NYT Smears Dr. Mercola Again With Classic Orwellian Doublespeak
Video link
By Dr. Mercola | August 18, 2022
In July 2021, The New York Times (NYT) published the hit piece,1 “The Most Influential Spreader of Coronavirus Misinformation Online,” in which they made several blatantly false claims about me. Now, the NYT is upping the ante with an entire documentary dedicated to yours truly, titled “Superspreader.”
Ever since my book “The Truth About COVID-19” came out, the global cabal seems to have lost their collective minds. The New York Times has printed demonstrably false information about me on multiple occasions, CNN reporters have invaded my office and pursued me on my bicycle with unmarked vehicles, the president of the United States has utilized his federal agencies to target me — and my personal and business bank accounts were closed.
Twitter has banned anyone from sharing any link to my website, YouTube banned my account with over 15 years of content, while Facebook and Google have done everything possible to make me disappear. It certainly would be much easier to cave under the pressure, but if we don’t stand up for our rights and freedom now — when will it be too late? I will continue ‘superspreading’ truth and health until my last days.
NYT Hit Parade Continues With ‘Superspreader’
In an August 5, 2022, TV review, Alex Reif writes:2
“News can spread like a virus. In our fast-paced world, it doesn’t take long for either to spread around, which is why it’s so important to get your information from a good source.
In the latest installment of the FX series The New York Times Presents, viewers will get a perfect example of this with ‘Superspreader,’ which takes a look at one doctor with a massive following, who is credited as being the top spreader of misinformation regarding the COVID-19 and vaccine in the wellness industry …
One of the pre-credit notes at the end of the documentary states that FDA Commissioner Robert Califf considers misinformation to be the leading cause of death in the country and because of this …
[A]nother highlight of the film is an interview with Imran Ahmed, CEO of the Center for Encountering Digital Hate who ranked Mercola at the top of ‘The Disinformation Dozen,’ a numbers-based list of the twelve most influential people leading the COVID-19 anti-vaccination effort.
We also see how Mercola was de-platformed by several social media companies and how that hasn’t done all that much to stop the spread of misinformation.
At face value, The New York Times Presents ‘Superspreader’ is about Dr. Joseph Mercola, the empire he built, and the people who believe everything he says without question. But what viewers ultimately walk away with is a reminder that if something seems too good to be true, it most surely is.”
The NYT documentary premieres Friday, August 19, 2022, at 10 p.m. Eastern and 10 p.m. Pacific time, on FX and Hulu.
Truth Tellers Are Being Vindicated Every Day
In the NYT’s July 2021 hit piece, the author, Sheera Frenkel, cited an article I’d published in which she says I questioned “the legal definition of vaccines” and declared the COVID shots were “a medical fraud,” for the simple reason that they don’t prevent infections, they don’t provide immunity and don’t stop transmission of the infection.
According to Frenkel, that was misinformation. According to the U.S. government and its “experts,” the COVID jabs worked like any other vaccine. Check out the short video for a sampling of what Bill Gates, the Centers for Disease Control and Prevention, mainstream media, Dr. Anthony Fauci and President Biden were saying about the shots in early 2021.
The clear message — the promise — was that if you got the shots, you would not get COVID and you would not transmit it to others. Getting the population “vaccinated” would end the pandemic, for sure. Fast-forward to today, and the reality of the situation is beyond self-evident.
Biden, fully vaxxed and boosted has had COVID twice. Ditto for Fauci and a long list of government officials around the world. Outbreaks have repeatedly occurred at events where every single person present was fully vaxxed. So, the reality is that, back in February 2021, I warned that a medical fraud was being committed, and today, evidence from around the world show I was correct.
The shots do not prevent you from being infected, and they don’t prevent you from spreading it to others. As such, the COVID shots do not function as a vaccine at all, and mass vaccination cannot end the pandemic because you’re just as infectious if you get the shot and contract COVID as you would be if you were unjabbed.
Yet, despite the fact that time has vindicated me, the NYT has decided to double down and put out an entire documentary to cement the “superspreader of misinformation” label to my name when it really should be permanently attached to their own. It probably is important to note that they started their efforts on this video last year, in 2021.
‘Easily Disprovable’ Assertions Are in Fact True
In her 2021 hit piece, Frenkel also highlighted my comments about the COVID shots’ ability to “alter your genetic coding, essentially turning you into a bioweapon spike protein factory that has no off-switch.” According to Frenkel, these assertions “were easily disprovable.”
But did she disprove them? No. Here’s the reality: mRNA vaccines are by definition a genetic instruction set. That’s what messenger RNA (mRNA) is. And the mRNA created by Pfizer or Moderna are synthetic instructions that have never before existed in humans.
This is true for a variety of reasons, but the primary one is the substitution of pseudouridine for uridine to prevent the mRNA from being degraded. Natural mRNA is normally rapidly destroyed and this is by design as your body is very precise about producing proteins and does not produce them willy-nilly.
So is there an off switch? Absolutely not. There’s no off-switch programmed into these jabs. They are relying on your body’s normal degradation systems. The biotech industry has even referred to this reprogramming of your body as turning you into a “human bioreactor.”3
If an off-switch existed, the manufacturers would have assured us of that fact by now. In fact, they probably would have used the existence of a timed off-switch as the justification for boosters, but that has never come up. We know for sure that the mRNA jabs last at least 60 days and that is all we have for hard data. They more than likely last for six months and in some cases could last for years.
Asking Pointed, Nuanced Questions Is Bad?
Next, Frenkel went on to state that:4
“When the coronavirus hit last year, Dr. Mercola jumped on the news, with posts questioning the origins of the disease. In December, he used a study that examined mask-wearing by doctors to argue that masks did not stop the spread of the virus …
[R]ather than directly stating online that vaccines don’t work, Dr. Mercola’s posts often ask pointed questions about their safety and discuss studies that other doctors have refuted. Facebook and Twitter have allowed some of his posts to remain up with caution labels, and the companies have struggled to create rules to pull down posts that have nuance …”
So, I not only committed the “sin” of correctly warning people about the vaccine fraud committed, and had the audacity to follow science and reference published research, but I was also guilty of the “crime” of asking pointed, nuanced questions?
When merely asking questions is deemed a dangerous, if not criminal, act, you know you’re living under an authoritarian regime. It’s certainly far outside the accepted norms of “democracy” and “freedom” that the United States has been a beacon of since its inception.
Ineptitude at Its Finest
Further on in her hit piece, Frenkel makes a truly crucial error that no respectable journalist would ever dare make:
“In an email, Dr. Mercola said it was ‘quite peculiar to me that I am named as the #1 superspreader of misinformation.’ Some of his Facebook posts were only liked by hundreds of people, he said, so he didn’t understand ‘how the relatively small number of shares could possibly cause such calamity to Biden’s multibillion dollar vaccination campaign.’
The efforts against him are political, Dr. Mercola added, and he accused the White House of ‘illegal censorship by colluding with social media companies.’ He did not address whether his coronavirus claims were factual.
‘I am the lead author of a peer reviewed publication regarding vitamin D and the risk of COVID-19 and I have every right to inform the public by sharing my medical research,’ he said. He did not identify the publication, and The Times was unable to verify his claim.”
The problem with Frenkel’s assertion is that I did identify the publication. In fact, I emailed her the direct link. So, she lied. Secondly, my paper is beyond easy to locate. Just put my name into PubMed and you’ll find it. Believe it or not, you can even find it using the most biased search engine on earth, Google.
Daniel Engber, senior editor at the typically highly progressive mainstream media outlet, The Atlantic, commented on Frenkel’s clear ineptitude or malicious prevarication in a tweet:5
“A truly bizarre moment in the NYT piece on Joseph Mercola … you can literally verify the existence of this peer-reviewed publication in one second via googling. pubmed.ncbi.nlm.nih.gov/33142828/“
Legal Notice Sent to NYT
July 26, 2021, my attorneys sent the following legal notice to Frenkel at the NYT, demanding a retraction of her false statements:6
“Dear Ms. Frenkel,
The undersigned law firm represents Dr. Joseph Mercola in connection with the attached article that was widely published on July 24, 2021. We are providing notice that you have made several false and defamatory statements in this article:
1.You identified that you could not validate that Dr. Mercola published a peer reviewed study on Vitamin D in the severity of COVID-19. Dr. Mercola provided the direct link in response to you (attached) and any journalist or fact checker would simply find the study by searching “Mercola” in PubMed.
2.Your article falsely states Dr. Mercola has been fined “millions” by the FDA. This is completely fabricated, Dr. Mercola has never been fined by the FDA.
… On behalf of Dr. Mercola, we hereby demand you immediately retract the article. We also request that you preserve all communications and documents that relate to Dr. Mercola.”
Where’s the Proof That I Am the ‘No. 1’ Misinformant?
To this day, the NYT insists I’m the No.1 spreader of misinformation online, based on the fabrications of a group called Center for Countering Digital Hate (CCDH) — a “foreign dark money group,” to quote Missouri Sen. Josh Hawley,7 which sprang out of nowhere to create lists of people to be censored into oblivion.
The CCDH’s data gathering is so questionable, even ultra-biased Facebook ended up publicly criticizing it. In an August 18, 2021, Facebook report, Monika Bickert, vice president of Facebook content policy, set the record straight:8
“In recent weeks, there has been a debate about whether the global problem of COVID-19 vaccine misinformation can be solved simply by removing 12 people from social media platforms. People who have advanced this narrative contend that these 12 people are responsible for 73% of online vaccine misinformation on Facebook. There isn’t any evidence to support this claim …
In fact, these 12 people are responsible for about just 0.05% of all views of vaccine-related content on Facebook. This includes all vaccine-related posts they’ve shared, whether true or false, as well as URLs associated with these people.”
At the time that Frenkel made her accusations, a Crowdtangle search for Facebook posts about the COVID jabs, from mid-June to mid-July 2021, also confirmed that my online reach was negligible. Topping the list of top performing Facebook posts expressing negative views about the COVID jabs was Candace Owens, followed by the mainstream news outlet ABC World News Tonight.9

The befuddling reality here is that most of the people identified as “top spreaders of misinformation” actually have negligible reach — at least compared to the people on this Crowdtangle list. None of the CCDH’s “top vaccine misinformants” are on the list above, and our reach certainly has not improved or expanded since then.
If You’re Targeted, You’re On-Target
This naturally raises the question, why were we targeted in the first place? Is it because we have high credibility from being one of the first natural health sites on the web with the most followers? Is it because we’ve spent a quarter of a century gaining people’s trust by mostly being correct about the health care system and criminal Big Pharma behavior?
Is it because we, more than others, have well-established credibility and are directly over the target? Is it because we have the experience and know-how to make accurate predictions? Is it because we see and explain the bigger picture?
Or is it some other reason entirely? It’s a mystery, really, but what is clear is that we’ve been deemed a threat to the official propaganda narrative, and I, for whatever reason, am at the very top of that threat identification list. Well, I’ve said this before, and I’ll say it again: I’m beyond truly honored to have been widely disparaged by one of the arms of the U.S. military and intelligence operations.
Being targeted in this fashion — tedious as it may be — is in fact a badge of honor. It tells me I’m doing the right thing, and that I’ve not misinterpreted the intentions behind the COVID machinations. More so than any intuition, it tells me I’m on target.
In the bright light of undeniable reality — as it is, a year later — it’s clear that Frenkel’s hit piece has not aged well. I doubt the NYT’s “Superspreader” documentary will fare much better. In the final analysis, if you want any hope of controlling your health, and that of your family, you’d be wise to understand legacy media speaks in Orwellian Doublespeak and reality is the opposite of virtually everything they are telling you.
Sources and References
How We Have Been Misled About Antidepressants
By Joanna Moncrieff | Brownstone Institute | August 18, 2022
Our umbrella review that revealed no links between serotonin and depression has caused shock waves among the general public, but has been dismissed as old news by psychiatric opinion leaders. This disjunction begs the questions of why the public has been fed this narrative for so long, and what antidepressants are actually doing if they are not reversing a chemical imbalance.
Before I go on, I should stress that I am not against the use of drugs for mental health problems per se. I believe some psychiatric drugs can be useful in some situations, but the way these drugs are presented both to the public and among the psychiatric community is, in my view, fundamentally misleading. This means we have not been using them carefully enough, and crucially, that people have not been able to make properly informed decisions about them.
Much public information still claims that depression, or mental disorders in general, are caused by a chemical imbalance and that drugs work by putting this right. The American Psychiatric Association currently tells people that: “differences in certain chemicals in the brain may contribute to symptoms of depression.” The Royal Australian & New Zealand College of Psychiatrists tells people: “Medications work by rebalancing the chemicals in the brain. Different types of medication act on different chemical pathways.”
In response to our paper finding that such statements are not supported by evidence, psychiatric experts have desperately tried to put the genie back in the bottle. There are other possible biological mechanisms that could explain how antidepressants exert their effects, they say, but what really matters is that antidepressants ‘work.’
This claim is based on randomised trials that show that antidepressants are marginally better than a placebo at reducing depression scores over a few weeks. However, the difference is so small that it is not clear it is even noticeable, and there is evidence that it may be explained by artefacts of the design of the studies rather than the effects of the drugs.
The experts go on to suggest that it does not matter how antidepressants work. After all, we do not understand exactly how every medical drug works, so this should not worry us.
This position reveals a deep-seated assumption about the nature of depression and the action of antidepressants, which helps to explain why the myth of the chemical imbalance has been allowed to survive for so long. These psychiatrists assume that depression must be the result of some specific biological processes that we will eventually be able to identify, and that antidepressants must work by targeting these.
These assumptions are neither supported nor helpful. They are not supported because, although there are numerous hypotheses (or speculations) other than the low serotonin theory, no consistent body of research demonstrates any specific biological mechanism underpinning depression that might explain antidepressant action; they are unhelpful because they lead to overly optimistic views about the actions of antidepressants that cause their benefits to be overstated and their adverse effects to be dismissed.
Depression is not the same as pain or other bodily symptoms. While biology is involved in all human activity and experience, it is not self-evident that manipulating the brain with drugs is the most useful level at which to deal with emotions. This may be something akin to soldering the hard drive to fix a problem with the software.
We normally think of moods and emotions as being personal reactions to the things going on in our lives, which are shaped by our individual history and predispositions (including our genes), and are intimately related to our personal values and inclinations.
Therefore we explain emotions in terms of the circumstances that provoke them and the personality of the individual. To override this common-sense understanding and claim that diagnosed depression is something different requires an established body of evidence, not an assortment of possible theories.
Models of drug action
The idea that psychiatric drugs might work by reversing an underlying brain abnormality is what I have called the ‘disease-centred’ model of drug action. It was first proposed in the 1960s when the serotonin theory of depression and other similar theories were advanced. Before this, drugs were implicitly understood to work differently, in what I have called a ‘drug-centred’ model of drug action.
In the early 20th century, it was recognised that drugs prescribed to people with mental disorders produce alterations to normal mental processes and states of consciousness, which are superimposed onto the individual’s preexisting thoughts and feelings.
This is much the same as we understand the effects of alcohol and other recreational drugs. We recognise that these can temporarily override unpleasant feelings. Although many psychiatric drugs, including antidepressants, are not enjoyable to take like alcohol, they do produce more or less subtle mental alterations that are relevant to their use.
This is different from how drugs work in the rest of medicine. Although only a minority of medical drugs target the ultimate underlying cause of a disease, they work by targeting the physiological processes that produce the symptoms of a condition in a disease-centred way.
Painkillers, for example, work by targeting the underlying biological mechanisms that produce pain. But opiate painkillers may work in a drug-centred way too, because, unlike other painkillers, they have mind-altering properties. One of their effects is to numb emotions, and people who have taken opiates for pain often say they still have some pain, but they do not care about it anymore.
In contrast, paracetamol (so often cited by those defending the idea that it does not matter how antidepressants work) does not have mind-altering properties, and therefore although we may not fully understand its mechanism of action, we can safely presume it works on pain mechanisms, because there is no other way for it to work.
Like alcohol and recreational drugs, psychiatric drugs produce general mental alterations that occur in everyone regardless of whether they have mental health problems or not. The alterations produced by antidepressants vary according to the nature of the drug (antidepressants come from many different chemical classes – another indication that they are unlikely to be acting on an underlying mechanism), but include lethargy, restlessness, mental clouding, sexual dysfunction, including loss of libido, and numbing of emotions.
This suggests they produce a generalised state of reduced sensitivity and feeling. These alterations will obviously influence how people feel and may explain the slight difference between antidepressants and placebo observed in randomised trials.
Influences
In my book, The Myth of the Chemical Cure, I show how this ‘drug-centred’ view of psychiatric drugs was gradually replaced by the disease-centred view during the 1960s and 70s. The older view was erased so completely that it seemed people simply forgot that psychiatric drugs have mind-changing properties.
This switch did not occur because of scientific evidence. It occurred because psychiatry wanted to present itself as a modern medical enterprise, whose treatments were the same as other medical treatments. From the 1990s, the pharmaceutical industry also started to promote this view, and the two forces combined to insert this idea into the minds of the general public in what has to go down as one of the most successful marketing campaigns in history.
As well as wanting to align with the rest of medicine, in the 1960s the psychiatric profession needed to distance its treatments from the recreational drug scene. Best-selling prescription drugs of the period, amphetamines and barbiturates, were being widely diverted onto the street (the popular ‘purple hearts’ were a mixture of the two). So it was important to emphasise that psychiatric drugs were targeting an underlying disease, and to gloss over how they might be changing people’s ordinary state of mind.
The pharmaceutical industry took up the baton following the benzodiazepine scandal in the late 1980s. At this time it became apparent that benzodiazepines (drugs like Valium- ‘mother’s little helper’) caused physical dependence just like the barbiturates they had replaced. It was also clear they were being doled out by the bucket load to people (mostly women) to medicate away the stresses of life.
So when the pharmaceutical industry developed its next set of misery pills, it needed to present them not as new ways of ‘drowning one’s sorrows,’ but as proper medical treatments that worked by rectifying an underlying physical abnormality. So Pharma launched a massive campaign to persuade people that depression was caused by a lack of serotonin that could be corrected by the new SSRI antidepressants.
Psychiatric and medical associations helped out, including the message in their information for patients on official websites. Although marketing has died down with most antidepressants no longer on patent, the idea that depression is caused by low serotonin is still widely disseminated on pharmaceutical websites and doctors are still telling people that it is the case (two doctors have said this on national TV and radio in the UK in the last few months).
Neither Pharma nor the psychiatric profession has had any interest in bursting the chemical imbalance bubble. It is quite clear from psychiatrists’ responses to our serotonin paper that the profession wishes people to continue under the misapprehension that mental disorders such as depression have been shown to be biological conditions that can be treated with drugs that target the underlying mechanisms.
We haven’t worked out what those mechanisms are yet, they admit, but we have plenty of research that suggests this or that possibility. They do not want to contemplate that there might be other explanations for what drugs like antidepressants are actually doing, and they do not want the public to do so either.
And there is good reason for this. Millions of people are now taking antidepressants, and the implications of discarding the disease-centred view of their action are profound. If antidepressants are not reversing an underlying imbalance, but we know that they are modifying the serotonin system in some way (though we are not sure how), we have to conclude they are changing our normal brain chemistry – just like recreational drugs do.
Some of the mental alterations that result, such as emotional numbing, may bring short-term relief. But when we look at antidepressants in this light we immediately understand that taking them for a long time is probably not a good idea. Although there is little research on the consequences of long-term use, increasing evidence points to the occurrence of withdrawal effects which can be severe and prolonged, and cases of persistent sexual dysfunction.
Replacing the serotonin theory with vague assurances that more complex biological mechanisms can explain drug action only continues the obfuscation, and enables the marketing of other psychiatric drugs on equally spurious grounds.
Johns Hopkins, for example, is telling people that ‘untreated depression causes long-term brain damage’ and that ‘esketamine may counteract the harmful effects of depression.’ Quite apart from the damage to people’s mental health by being told they have, or will soon get brain damage, this message encourages the use of a drug with a flimsy evidence base and a worrying adverse effect profile.
The serotonin hypothesis was inspired by the desire of the psychiatric profession to regard its treatments as proper medical treatments and the need of the pharmaceutical industry to distinguish its new drugs from the benzodiazepines that, by the late 1980s, had brought the medicating of misery into disrepute.
It exemplifies the way that psychiatric drugs have been misunderstood and misrepresented in the interests of profit and professional status. It is time to let people know not only that the serotonin story is a myth, but that antidepressants change the normal state of the body, brain and mind in ways that may occasionally be experienced as useful, but may be harmful too.
Joanna Moncrieff is a Professor of Critical and Social Psychiatry at University College London, and works as a consultant psychiatrist in the NHS. She researchers and writes about the over-use and misrepresentation of psychiatric drugs and about the history, politics and philosophy of psychiatry more generally. She is currently leading UK government-funded research on reducing and discontinuing antipsychotic drug treatment (the RADAR study), and collaborating on a study to support antidepressant discontinuation. In the 1990s she co-founded the Critical Psychiatry Network to link up with other, like-minded psychiatrists. She is author of numerous papers and her books include A Straight Talking Introduction to Psychiatric Drugs Second edition (PCCS Books), published in September 2020, as well as The Bitterest Pills: The Troubling Story of Antipsychotic Drugs (2013) and The Myth of the Chemical Cure (2009) (Palgrave Macmillan). Her website is https://joannamoncrieff.com/.
Climate change is not making children obese

BY MARY HARRINGTON | UNHERD | AUGUST 15, 2022
If you’re a hammer, everything looks like a nail. And if you’re a media ecosystem with a fixation on hammers, you will do your best to make anything look like a nail.
This is the inescapable conclusion from the reporting around a recent study, published in the peer-reviewed journal Temperature, which looked at the relationship between climate change and children’s fitness — and reported the findings entirely backwards to fit a pre-existing political narrative.
The study pointed out that children’s aerobic physical fitness is 30% lower than that of their parents at the same age, arguing that this is a problem because aerobic physical fitness is vital for tolerating higher temperatures. This in turn means that where climate change is causing temperatures to increase, obese individuals will find it harder to cope.
This is sensible stuff — but the study was reported as stating that climate change had caused reduced fitness in children. The study itself pointed to Covid lockdown measures, among many other factors, as having exacerbated an already-existing issue of poor fitness in children. But headlines suggested children are staying indoors because it’s too hot and that this is why they’re less fit than their parents.
You don’t have to be a scientist to know that reduced aerobic fitness in this generation of children long precedes measurably rising outdoor temperatures of the kind that could be attributed to climate change. Here’s a report from 2013 on the topic, for example, that describes aerobic fitness in children decreasing every decade from 1975 onward.
Nor do you have to be a scientist to come up with multiple factors that are plausibly contributing to this unhappy situation. Anyone with young children, or just rudimentary powers of observation, needs only a moment’s reflection to think of multiple ways in which 21st-century life militates against physically active childhood, compared to the world just a few decades ago. But we mustn’t let minor considerations like the patent absurdity of a claim, or its rampant misreading of an actual scientific paper, get in the way of a clickbait mass-media narrative on a much-hyped topic.
A sensible paper discussing the importance of physical fitness in ensuring resilience in the face of changing climate has been reported entirely backwards. Obesity, discussed as a cause of difficulty in adapting to climate change, is reported as the effect of climate change itself, while ignoring politically inconvenient factors cited in the paper itself as contributing to poor fitness.
But this is only an especially egregious example of how even supposedly respectable media can’t be relied on to read even the abstract of a research paper, before editorialising on it in terms that align with established political narratives. And arguably whether or not such specious editorialising qualifies as “misinformation” mostly depends on your political priors.
Given this, the now-widespread cynicism that increasingly greets “expert” opinion in the press is perhaps understandable. It’s all very well saying “follow the science” – but the average Joe may be forgiven for concluding that “the science” is not so much a reliable source of truth as a pick n’mix array of talking-points for a pre-determined political agenda.
White House “Climate Adviser” Banned from the National Academy of Science for Science Fraud
… while White House Officials Beg Social Media to Silence Opponents
By Igor Chudov | August 18, 2022
Climate change is a very important topic! According to Bill Gates-sponsored scientist Kari Nadeau, climate change is responsible for the recent rise in heart attacks, stillbirths, and cardiovascular disease, especially in children. So, knowing how important climate change is, I am paying attention to news about it, though with lesser intensity than I devote to Covid news.
Finally, we have a great climate change story! White House “climate official” Jane Lubchenco was just banned by the National Academy of Science (archive link) for science fraud. She was an editor of a paper written by her brother-in-law. Jane did not disclose this family relationship and promoted her brother-in-law’s article. The article itself contained false data that was known to be out of date at the time the article was written, and thus the paper was fraudulent.

Jane is now not allowed to participate in many scientific activities due to violating ethics rules meant to prevent fraud in science.
What is the White House’s biggest priority right now, when it comes to climate change? Perhaps it is cleaning up the place and making sure that we have honest science? Not really. The priority is demanding that major social networks silence climate change skeptics. Watch this video at 11:10:
The White House adviser says in the interview:
And frankly, the tech companies have to stop allowing specific individuals over and over again to spread disinformation.
I am not a big climate change skeptic — I do not care about climate change all that much right now — but coincidentally, Twitter recently suspended my dog’s account for 7 days.
So, I am not allowed to spread misinformation. The White House, on the other hand, has climate change advisors who perpetrate scientific fraud.
On a more serious note, my dog’s Twitter account was not alone and was suspended among hundreds of others last week, ostensibly for antivax misinformation. Why is this happening now? Why the urgency? It certainly is NOT about helping to vaccinate the public, as COVID vaccine uptake is at historic lows and everyone made up their mind already. Censorship would not help much with vaccination! Why, then, is it intensifying?
My own guess is that these suspensions are not so much related to Covid, but are happening due to the fact that the White House and the woke social networks are preparing for the November elections and want to silence dissent in advance. Why?
- to influence the election, and
- to prevent people from questioning election conduct and fairness afterward
They — the White House, Twitter, Facebook and Google — know that they will have to face very uncomfortable questions about their role in forcing the so-called “Covid vaccine” onto young people, as they “own” the outcome of this. They want to postpone that moment of reckoning and thus are deleting as many dissenting voices as they can.
The CDC Failed, So Spin It Off and Make It More Powerful?
BY JEFFREY A. TUCKER | BROWNSTONE INSTITUTE | AUGUST 17, 2022
The failure of the CDC to manage Covid-19 was baked in from the first moments of its response. A government agency was never going to mitigate much less get rid of this sort of pathogen. This is because the virus never cared a whit about prestige degrees, job descriptions, big budgets, high-end connections, media agitprop, or polls. It went on its merry way, hit everyone, and immune systems adapted as they always have done.
The great experiment was an enormous flop.
The costs of the experiment we know: it is the catastrophe that Donald Henderson predicted it would be in 2006.
Thus does it make sense that the present overlords of the agency have admitted at least partially to have made some errors. The question is what were these errors. From the latest news concerning some impending shakeup, I see no evidence of any serious rethinking of the crazed and cockamamie lockdown orders it issued from March 2020 onward. Not even preposterous mandates like plexiglass at retail counters, two years of school closures, “six feet of distance,” one-way grocery aisles, band members in bubbles, mask mandates, and limits on how many people you can have in your home have prompted remorse.
Instead, every indication is that the CDC believes the real problem was that it did not have a high-enough budget and enough power. Plenty of lawmakers are willing to go along – not that anyone is asking them. Therefore, its tremendous pandemic powers need to be tweaked and invested mainly in a division known as the Office of the Assistant Secretary for Preparedness and Response, or ASPR.
Says The Washington Post :
The Biden administration is reorganizing the federal health department [HHS] to create an independent division that would lead the nation’s pandemic response, amid frustrations with the Centers for Disease Control and Prevention.
Joy!
The new head of this high-level division (same level as FDA/CDC) is Dawn O’Connell who has a background in literature (Vanderbilt) and law (Tulane), not science or medicine. She is a political appointee who took the reins as Assistant Secretary of Health and Human Services for Preparedness and Response, as confirmed by the Senate in 2021. She is now elated to report that her division will be elevated to become just as important as the CDC and the FDA.
Here is her memo to the staff:
ASPR Team:
As you know firsthand, ASPR is at the forefront of many of HHS’s and the Biden-Harris Administration’s top priorities. Whether your work involves strengthening our core preparedness and response capabilities, tackling new and emerging challenges, or providing essential support services to the team, please know that the work that you do matters and that it is making a big difference.
In recognition of the tremendous value this team brings to the Department and the American people – and due to the increasing size and scope of what we do – I asked Secretary Becerra to consider making us an Operating Division and I am pleased to report that Secretary Becerra has made the critically important decision to elevate our team from a Staff Division to an Operating Division (OpDiv)!
This change allows ASPR to mobilize a coordinated national response more quickly and stably during future disasters and emergencies while equipping us with greater hiring and contracting capabilities. As an OpDiv, we are now in the same category as other large HHS teams with core operational responsibilities such as CDC, NIH, FDA, CMS, and ACF. This change is an important next step for our organization which has continued to grow and evolve since its creation in 2006 – the pace of which has quickened over the past year. This change is also a recognition of the good work you all have been and continue to do on behalf of the American People…
Along with this reclassification, moving forward we will be known as the Administration for Strategic Preparedness and Response (ASPR). The adjustment to our name signals our elevation to an OpDiv, while maintaining the equity and brand recognition we have built with key internal and external stakeholders, particularly over the course of the pandemic.
Thus must we ask: what the heck is going on here? The Biden administration has no idea. Indeed the Washington Post reports that “some senior Biden administration officials said they were unaware of the plan to reorganize the department, which was approved by HHS Secretary Xavier Becerra and has been held close by his deputies.”
This point is crucial. This is how the administrative state works. It cares nothing for the elected officials who come and go. It moves on its own, fueled by money baked into the budgets and with power hardly anyone dares to challenge. There is never any accountability. There is only one path forward: more power. Elections be damned.
The most important part of the memo here is the idea of mobilizing a “coordinated national response.” It drove these people utterly bonkers that during the pandemic, several states went their own way. South Dakota never shut down. Georgia opened a month after the shutdowns. Florida and Texas were next. Finally all the states with Republican governors opened while most states with Democratic governors remained closed to some degree.
The empirical results are incredibly obvious. The open states performed as well and often better on disease demographics. Meanwhile their economies did not suffer nearly as much. The kids stayed in school. The churches functioned. There were live musical performances. The museums, libraries, and playgrounds opened. People are less traumatized.
The migration of people from blue to red tells the whole story. Masses of people fled the lockdown states for the open states.
A “coordinated national response” would make such federalist solutions impossible. Forget the 9th and 10th Amendments. These agencies and these people care nothing for them, nor actual science which would encourage a plethora of experiments in the management of a pathogen. These bureaucrats in Washington think they have all the answers, and they demand complete compliance.
Meanwhile, the CDC itself is being reorganized. But don’t be fooled by any appearance of contrition. They still have a legal appeal in process that would put a mask back on your face when traveling. The new agency to which some of its pandemic responsibilities will be transferred will have a 1,000-person staff to start, people paid the big bucks to sit around coming up with new ways to whip up disease panic and start another crackdown.
A better solution would be to abolish the CDC. States can handle all its responsibilities. It did not even exist until 1947. Its purpose was mosquito control, spraying a now-banned chemical (DDT) everywhere. These days we handle that by going to Home Depot.
The CDC as an agency grew out of the 1944 Public Health Services Act that permitted nationally ordered quarantines for the first time. The legislative history of that thing remains a mystery to me. Regardless, it is nowhere justified in the US Constitution. This act needs to go too. So too all the federal agencies to which it gave rise. This is the only real solution.
Certainly creating a new agency is not the answer. And note that ASPR has its roots in 2006 as an outgrowth of the Bush administration’s obsessive panic over bioterrorism. It was also the first year that anyone imagined that lockdowns could be an appropriate path for any free society. It was the year that “social distancing” was invented by a cabal of computer scientists with zero experience in infectious disease.
These fanatics need to be out of power completely, and the regulations, laws, and agencies that enabled them to ruin the country and its freedoms must be ended. This is what any responsive government in a modern society would do. It would see failure and call it and then do something about it. It certainly would not go in this new direction and reward the disease planners with more power and money!
We must learn real lessons and act on them.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown. He is also the editor of The Best of Mises. He writes a daily column on economics at The Epoch Times, and speaks widely on topics of economics, technology, social philosophy, and culture.
CDC’s Ludicrous Makeover
BY HARVEY RISCH | BROWNSTONE INSTITUTE | AUGUST 18, 2022
CDC announced that the institutes have done an external/self-study and proposed a makeover “to restore public trust.” Dr. Walensky said that she “plans to remake the culture to help the agency move faster when it responds to a public health crisis. She also wants to make it easier for other parts of the government to work with the CDC, and wants to simplify and streamline the website to get rid of overlapping and contradictory public health guidance.”
The CDC’s announcement covers everything except the fundamental problem to which the director and the external reviewer are blind: industry subservience and epidemiologic incompetence.
CDC has published numbers of fatally flawed study reports over the last two years in MMWR, its captive journal. No amounts of “moving faster” will fix this problem. It took CDC two years to figure out that the vaccines are not an effective public health tool for reducing infection spread, something that I and numerous colleagues have been saying for more than a year.
CDC has still not recognized that for Covid, masks are useless, that distancing is useless, that general population testing is virtually useless for managing the population pandemic.
That the CDC has reviewed itself and only found trivialities and not the systematic problems that caused it to produce repeatedly failing policies shows that this review exercise was only window dressing. It was not a serious review.
The CDC needs a completely different independent external review to understand how it as a public health agency with MD and PhD epidemiologists could get so much science wrong for so long. The current makeover plans are ludicrous, will fool no one, and will not restore any of the large amount of public trust that has been lost by its poor performance over the last 2.5 years.
Harvey Risch is Professor of Epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and Yale School of Medicine. Dr. Risch received his MD degree from the University of California San Diego and PhD from the University of Chicago. After serving as a postdoctoral fellow in epidemiology at the University of Washington, Dr. Risch was a faculty member in epidemiology and biostatistics at the University of Toronto before coming to Yale.
(Yet) more worrying data on myocarditis in children
Thai data shows alarming signal
Health Advisory & Recovery Team | August 18, 2022
HART recently published an article summarising the results of a study performed in the US military which found that nearly 3% of those vaccinated with smallpox vaccine developed subclinical myocarditis (defined by an increased troponin level – which was prospectively measured in all subjects).
It should be emphasised that no “safe” level of increased troponin has been identified. Any increase is a potential cause for concern in any age group, let alone young people.
In that article, we expressed alarm that – given the worrying data regarding myocarditis and Covid mRNA vaccination – a simple prospective before and after study of troponin levels had never been performed in any age group.
It turns out that we weren’t the only people suggesting such a study needs performing. The FDA thought so too.
As Vinay Prasad writes – apparently the FDA made it a condition of the Emergency Authorisation.

The agreed dates for such a study are frankly bizarre, given how simple and quick such a study would be to perform and how many billions of doses of this product have / are being injected into people of all ages, with no (official) abatement in enthusiasm yet apparent.
However, such a study has in fact now been performed. Not by any investigators in the wealthy Western world, for whom carrying out such an exercise would have been like a proverbial “cake-walk”.
No, instead we have had to rely on a publication out of Thailand, which can be found here. In this study, they measured troponin levels in ~300 teenagers aged 13 to 18 in 2 schools, both before and after their second dose of Pfizer mRNA vaccine.
A lot has now been written about this study already, and we will therefore refer you to the best summaries published to date, which are those from Vinay Prasad and Brian Mowery although the former analysis is, in our opinion, far too muted given the gravity of the situation.
The bottom line is that troponin elevation or cardiac symptoms indicative of myocarditis/pericarditis were identified in 7 (3.5%) of 200 boys, 5 of whom (2.5%) had elevated troponin levels.
(Troponin is a substance released from heart cells which is indicative of damage to heart muscle cells, which have no repair mechanism. Testing for its presence is commonly performed when patients present with chest pain suggestive of a possible heart attack.)
There was a zero signal (for either symptoms or raised troponin) in girls.
John Campbell – who has around 2.5m followers and had previously been extremely enthusiastic about the mRNA covid vaccines – appears visibly shocked by this data in his video covering it.
He points out that anyone with a raised troponin level would ordinarily be ordered to rest due to the association between myocardial damage and fatal arrhythmia on exertion. The implication must surely be that the administration of these agents to children and young people must cease, since the notion that all will routinely be troponin-tested is clearly ridiculous.
Worse still: this 2.5% (which is bad enough) only represents the cases where the troponin levels exceeded a specific threshold of 13 pc/mg. The authors have not provided the raw data and it is perfectly possible that there were many more boys (and possibly girls) in whom some clinically relevant elevated troponin might have been evident but not to this level.
It is to be noted that as described here the cut-off of 13 pc/ml (based on the 99th percentile for a normal reference population) appears to relate to the use of troponin levels to determine a differential diagnosis of chest pain when a myocardial infarction (“heart attack”) is suspected – ie to answer the typical question facing ER doctors (and one which is not as easy to answer merely based on symptoms as many might imagine): “has there been cardiac involvement, or is this just indigestion?”
Because of the mechanism of a typical heart attack (blockage of an artery) you’d actually expect a heterogeneous response – either an amount of heart muscle has been damaged sufficient to result in high troponin elevation, or not (resulting in no elevation). Hence the use of a certain cut-off can reasonably reliably rule out an incident such as heart attack.
However, with myocarditis, we should surely be concerned with identifying any myocardial damage at all, not screening for MI as a differential diagnosis. In this context, a completely safe level is unknown. It may be that any elevation means there has been myocardial damage. Depending on where this is, it may be associated with an increased chance of suffering a fatal arrhythmia.
We don’t know the answers to these questions. Given where we are, that’s alarming.
In the absence of comorbidities, young people were never at risk from covid and certainly are not at risk from omicron. Most have been infected and have natural immunity. The mass administration of these agents to the young was always completely unjustifiable; this latest data brings the decision to continue with this program into the more serious realm of malfeasance.
What to Know Before Deciding to Take The Novavax Injection
Accepting an injection of spike protein hoping it is safe or effective is absurd. Yet, many are again forced to make a decision threatening their health and ability to support their family.
By Pierre Kory, MD, MPA | August 17, 2022
A subscriber asked me to write a post about my thoughts on Novavax because she “really trusts my judgement.” Flattered, I felt like I should share what they are. So here goes.
Before any medical intervention, but especially in the case of a novel or barely tested one, a long standing practice of medical ethics is that informed consent must be obtained. The emphasis should be on the informed part and not the consent part. Note that informed consent has been one of the foundations of medical ethics, essentially an inviolable standard, or at least it used to be before this “emergency” came along where now you have pharmacists injecting children with barely a mention of the risks, “because they might be too scared to take the shot.”
Informed consent discussions are simple in structure but often complex and time-consuming to conduct. It relies on providing the patient with as detailed and comprehensive a knowledge of the risks, benefits, and alternatives to the intervention.
So, should we go through an informed consent discussion with the novel Novavax injection? Actually, I would not. Why? Because I don’t hold informed consent discussions for interventions I do not recommend or would not want my patient to consider. I instead tell them not to consider and give them my reasons for that recommendation. Thus, I only conduct informed consent discussion for interventions that I feel would bring about greater benefits than risks (generally much greater), and I would only do so for patients with active illness in order to get them better. A vaccine is a much different proposition as they are given to patients without disease.
Why would I not even consider Novavax as a reasonable option? Simple:
- There has never been a successful or safe coronavirus vaccine. The last 18 months have shown that COVID vaccines lead to increased chances of getting ill, equal or increased chances of transmitting, and higher likelihood of entering hospital and dying. And that is leaving unmentioned the lethality and toxicity of the mRNA platform ones. See my “Vaccine Exemption Letter” post for the data to support these statements. The coronavirus is a rapidly mutating virus, thus vaccines will always be non-neutralizing because by the time they are manufactured and ready for injection, the virus has mutated into forms poorly responsive to older, narrower antibodies.
- Novavax is still formulated with a two and a half year-old protein for this rapidly mutagenic coronavirus, so it would be like giving a two and a half year old flu shot for this years flu (worse actually). Yet our health system, including every single academic medical center in the country is still mandating and eager to adopt use of an outdated viral protein. I would love to say this is beyond belief, but this is the world we live in now.
- We now have the omicron variant circulating, which is generally well tolerated by most, particularly those who are healthy or young (and even the old), and especially those with natural immunity.
- The country now has abundant natural immunity, which even the CDC now admits offers equal protection (actually, natural immunity offers better protection but let’s give the CDC some credit for telling at least a partial truth). So why are we still vaccinating and/or mandating in those who have recovered from COVID?
- Vaccinating against respiratory viruses works very poorly as the antibodies do not reach high concentrations in the nasal and respiratory mucosa which is where the virus enters. The flu vaccine is almost completely ineffective, even when you get this years flu shot. Not known by most.
- Vaccinating against respiratory viruses with non-neutralizing vaccines actually weakens and warps the immune system such that you are more likely to get other respiratory viruses or illnesses as well (this has been well reported after flu vaccinations given that those vaccinated against the flu are more susceptible to other respiratory viral infections).
- Proposing a novel and barely tested product coming out of the pharmaceutical industry to a patient is a wicked proposition in modern times. Note the pharmaceutical industry is a documented criminal industry which has repeatedly put out unsafe and ineffective products (even deadly, i.e opioids, Avandia, Vioxx, Bextra, the list goes on), followed by burying the adverse event data while pushing their wares through control of professional societies, federal/state legislation, and captured agencies. They have paid over $12 billion in criminal fines and over $16 billion in civil fines, just in the last 20 years across the 20 largest settlements. Their history of these actions stretches even longer.
- The history of criminality around the COVID vaccines dwarfs any actions the industry has done in the past. The Pfizer documents that the PFDA (the P is not a typo) tried to hide for 75 years reveal insane amounts of manipulations to try to show they work and are safe. They didn’t and weren’t. Further the testimony from the Ventavia/Pfizer whistleblower Brook Jackson reveals that the studies were so poorly done with such little follow-up of patients that they are simply not credible. Remember, Pharma. Does. Not. Care. About. Your. Health. Just your wallet (actually the government’s wallet, which I suppose is also your wallet).
So, conceptually, I think the idea of getting any coronavirus vaccine at this point is preposterous. However, let’s try to do a more traditional informed consent using the structure of risks/benefits/alternatives. The following is what I think other providers (or pharmacists egads) should be telling people prior to offering them Novavax, or more accurately, in order to get them to avoid it.
Yes, Novavax is a “non-mRNA” vaccine and is designed more along the line of a traditional vaccine in that an amount of viral protein is injected into the arm, it is then recognized as a “foreign” protein by our immune system which then makes antibodies against it. These antibodies are then thought (“hoped” remember) to help clear the virus rapidly and efficiently after exposure such that we avoid illness. Sounds good on paper. Not. Just ask Geert Vanden Bossche, one of the worlds top immunologists and vaccine experts.
RISKS
Novavax delivers the spike protein. As a self-described clinical expert in spike-protein induced disease, the spike protein is a pathogen. A pathogen is a substance or organism that is capable of inducing illness. Note that I call myself an expert because there are very few of us out here studying it’s pathogenicity, however I would argue Professor Paul Marik has taken the lead across the globe in amassing all the basic science and clinical research underlying the knowledge of the mechanisms and treatments of spike-protein induced diseases. That scholarly document is in evolution, and has over 300 scientific references at this point, with rapid evolutions and additions each week. Note that it appears to be the world’s sole “comprehensive” scholarly work on spike protein pathogenicity and empirically proposed treatments.
Another great sadness about the US COVID response is that almost the entire health system and all of academia have yet to recognize the spike as a pathogen or formulate any approach to treating Long-Haul or Post-Vaccine Injury. Until they do, they will continue to fail to recognize the causes or mechanisms of these syndromes as well as to offer effective treatments. And, it goes without saying, they will not be able to discuss this in thier ill-informed consent discussions. Their deplorable failure at treating these disabling diseases is astounding and will continue for the foreseeable future. Remember, the system docs won’t treat because they are all members of the Church of RCT Fundamentalism (a.k.a “evidence based medicine.”) You know, where they will sit there paralyzed until some massive randomized controlled trial is published in a high-impact medical journal and then is recommended by a federal agency or national medical society. You know what that system produces by now if you read my Substack. Not only will it leave patients untreated for months to years, but while the docs sit around waiting, Pharma, via the agencies and media, will suppress or attack any generic medicines or supplements that front-line doctors and patients have found effective. They will do this with ferocity and depravity until such a time they can “save the day” with the massive promotion of a novel, pricey Big Pharma pill which they will get our government to pay for at a price they set. Think about what happened to ivermectin and hydroxychloroquine until Pharma saved the day with the pathetic and poisonous Paxlovid using our government coffers. Rinse repeat here.
The two major and complex diseases unleashed by the spike are what we call “long haul” and “post-vaccine injury” syndromes. I probably should differentiate post-vaccine into two subtypes, with one being an acute, sudden death syndrome caused by massive heart attacks, myocarditis (which can cause lethal arrhythmias or pump failure), and/or massive strokes. Excess mortality amongst the vaccinated in 2021 skyrocketed and is showing up in Life Insurance industry data in both the U.S and other countries. However I don’t see those events in my practice because they are sudden deaths occurring in asymptomatic patients (who are often swimming or running or doing something else fun until they suddenly drop dead). My practice instead sees patients who suffer with the more chronic subtype consisting of myriad, disabling symptoms across multiple organ systems. Now, whether there is enough spike in Novavax to produce similar deadly events or chronic syndromes in the future, who knows. More on that below.
SHORT TERM RISK DATA
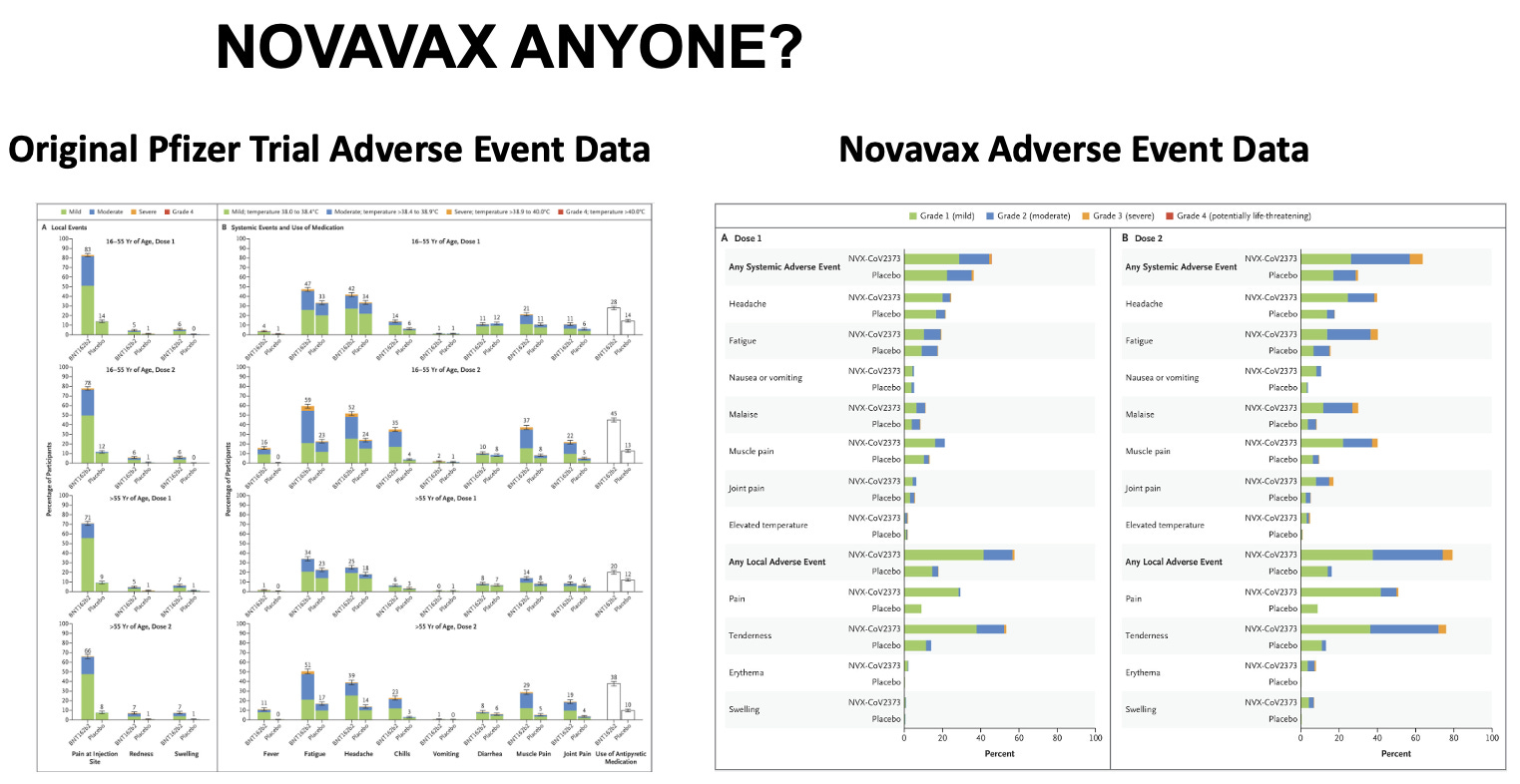
Not looking good here folks. Let’s take a look at the actual published trial of Novavax, and their chart detailing the “side effects.” Then let’s compare it to Pfizers mRNA “vaccine” trial published in December 2020. Look carefully. I will interpret these charts below.
Click for full size
Here is how I interpret the data:
- The “local” and “systemic” adverse events are absurdly high in both. I remember thinking back in December 2020 when I was reading the Pfizer trial, I said to myself, “Wow, that does NOT look friendly!” Not just the wickedly high frequency of really sore arms with redness and swelling, but the very high rates of “systemic symptoms” of fatigue, headache, chills, vomiting, muscle pain. Very high rates of those. Ouch.
- Next, look at the “dose response,” meaning look at the incidence of adverse events after the 2nd shot compared to the 1st shot. If it is higher after the 2nd, it indicates a “dose-response relationship,” which, when we are talking about a therapeutic, is a pillar of evidence to support the efficacy of the drug. For instance, ivermectin in COVID has a strong dose response relationship, meaning the higher the dose, the more effective it is (that is why all the high impact trials tried as much as they could to limit the dose of ivermectin, in particular during history’s most fraudulent trial called the TOGETHER trial).
Conversely, a dose-response in terms of side effects is a pillar of the measure of toxicity. The more you give, the sicker you get. Not cool. Now take a look at Pfizers published chart above, keeping in mind, these are only the short term systemic side effects.
- Pfizer: fatigue goes from 47% after the 1st to 59% after the 2nd in young folks and 34% up to 51% in older folks. Chills: 14% to 35% in young, 6% to 23% in old. Same pattern and increases with muscle pains and also joint pains and use of anti-pyretic medications.
- Now, take a look at Novavax. Note how they don’t give you the numeral percentages and instead make you crane your neck and use a ruler to estimate the actual incidences and increases. But just looking at the height of the bars from shot 1 to shot 2 and the increases in the yellow at the tops of the bars (yellow = “Grade 3” reactions – i.e. more severe), you see again what looks like a scary shot to me with some of the local and systemic events reported even higher than with Pfizer’s mRNA shot! So, is Novavax safer?
LONG TERM SIDE EFFECTS. Unknown. Remember the famous, “I guess we will just have to give it to see how safe it is” by one of the nations top vaccine experts. I swear, again, and I say this often, you just cannot make this stuff up. So, an informed consent discussion should relate that long term side effects are unknown. Remember as well, we are not in a supposed “emergency” anymore, despite the fact our government keeps renewing its emergency powers. If the person conducting this discussion tries to argue that in terms of long term effects, it is safe and effective because the mRNA vaccines were safe and effective, that is so categorically ridiculous it does not even bare addressing. Again, read my “Vaccine Exemption Letter” post for the data on toxicity and lethality of those vaccines. Do not proceed. My caution would be that spike protein is a pathogen with sequences that we know generate antibodies that then are capable of attacking many tissues (what are called autoantibodies which cause a category of diseases called “auto-immune” diseases). Also, spike protein, when broken down by the body is known to generate amyloid like fragments which are highly thrombogenic (i.e. cause clotting). Spike protein also stimulates immune cells called monocytes and macrophages which disturb numerous organ functions. Spike protein is also toxic to mitochondria which are the energy producing parts of each cell. In summary, don’t sign up for any more spike protein than is already circulating in the world.
Also, Novavax, like the mRNA vaccines uses “nanoparticles” in a “saponin-based adjuvant” solution which is novel and proprietary, patented only in 2020. Well, thats reassuring no? Their published paper states that the adjuvant and the vaccine was found to be “safe and immunogenic” in Phase 1 and 2 trials. Then I found this in the supplementary appendix from one of the earlier trials, ”the mechanism of Matrix-M1 (the adjuvant) is not well defined, but it has been associated with a potent induction of leukocyte activation and migration into the draining lymph nodes in their previous study.” Not reassuring.
EFFICACY
Unknown, but likely ineffective as it has not been tested against Omicron, or any of its sub-variants or whatever future variant will be circulating when it rolls out. Plus, as we know now, all the predicted efficacy reported from COVID-19 vaccine trials were never observed in the real-world, again likely due to trial shenanigans and data manipulations and removal and/or miscategorization of those who fell ill during the trial or simply due to the fact the virus is rapidly mutating. Even if it were effective, we know from the past two years, it would be short lived. I again have to mention natural immunity. It already protects against severe disease and reasonably well from re-infection, and there is no credible data to suggest adding an even older spike protein vaccine using a newly patented adjuvant will better protect you or make you healthier.
ALTERNATIVES TO VACCINATION
For readers of my Substack, you all know that you can always just skip the vaccine and instead just rely on early treatment which has been shown to be near perfectly effective in achieving rapid recovery and avoidance of hospitalization and death, especially when given in synergistic combinations like the FLCCC’s or the AAPS’s protocols. In fact, as you know, no vaccine would ever get an EUA or approval if effective treatments were available. Further, there are now over three dozen effective treatments supported by controlled trials, with many of them repurposed and/or over the counter. I suppose you could also just rely on Paxlovid given its demonstration of such incredible efficacy in treating President Biden and Dr. Fauci.
Hope this helps.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S. I am getting professional help (hah!) to write a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:

RNA for Moderna’s Omicron Booster Manufactured by CIA-Linked Company
BY WHITNEY WEBB |
UNLIMITED HANGOUT| AUGUST 17, 2022
Since late last year, messenger RNA for Moderna’s COVID-19 vaccines, including its recently reformulated Omicron booster, has been exclusively manufactured by a little known company with significant ties to US intelligence.
Earlier this week, the United Kingdom became the first country to approve Moderna’s reformulated version of its COVID-19 vaccine, which claims to provide protection against both the original form of the virus and the significantly less lethal but more transmissible Omicron variant. The product was approved by the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) with the support of the UK government’s Commission on Human Medicines.
Described by UK officials as a “sharpened tool” in the nation’s continued vaccination campaign, the reformulated vaccine combines the previously approved COVID-19 vaccine with a “vaccine candidate” targeting the Omicron variant BA.1. That vaccine candidate has never been previously approved and has not been the subject of independent study. The MHRA approved the vaccine based on a single, incomplete human trial currently being conducted by Moderna. The company promoted incomplete data from that trial in company press releases in June and July. The study has yet to be published in a medical journal or peer reviewed. No concerns have been raised by any regulatory agency, including the MHRA, regarding Moderna’s past history of engaging in suspect and likely illegal activity in past product trials, including for its original COVID-19 vaccine.
The approval comes shortly before several Western countries, including the UK, plan to conduct a massive COVID-19 booster vaccination campaign this fall. Moderna has also noted that approval for its Omicron booster vaccine are pending in the US, EU, Australia and Canada – all of which are also planning fall vaccination campaigns focused on COVID-19. The company’s CEO, Stéphane Bancel, has called the reformulated vaccine “our lead candidate for a Fall 2022 booster.”

Moderna CEO Stéphane Bancel, Source: ClockworkOrange
However, unlike the company’s original COVID-19 vaccine, the genetic material, or messenger RNA (mRNA), for this new vaccine, including the newly formulated genetic material meant to provide protection against the Omicron variant, is being manufactured, not by Moderna, but by a relatively new company that has received hardly any media attention, despite its overt links to US intelligence. Last September, it was quietly announced that a company called National Resilience (often referred to simply as Resilience) would begin manufacturing the mRNA for Moderna COVID-19 vaccine products. Under the terms of the multi-year agreement, “Resilience will produce mRNA for the Moderna COVID-19 vaccine at its facility in Mississauga, Ontario, for distribution worldwide.”
“Reinventing Biomanufacturing”
National Resilience was founded relatively recently, in November 2020, and describes itself as “a manufacturing and technology company dedicated to broadening access to complex medicines and protecting biopharmaceutical supply chains against disruption.” It has since been building “a sustainable network of high-tech, end-to-end manufacturing solutions with the aim to ensure the medicines of today and tomorrow can be made quickly, safely, and at scale.” It further plans to “reinvent biomanufacturing” and “democratize access to medicines,” namely gene therapies, experimental vaccines and other “medicines of tomorrow.”
In pursuit of those goals, the company announced it would “actively invest in developing powerful new technologies to manufacture complex medicines that are defining the future of therapeutics, including cell and gene therapies, viral vectors, vaccines, and proteins.” It was founded with the reported intention “to build a better system for manufacturing complex medicines to fight deadly diseases” as a way to improve post-COVID “pandemic preparedness.”
The company initially marketed its manufacturing capabilities as “the Resilience platform”, and offers principally “RNA Modalities”, including RNA development for vaccines, gene editing and therapeutics; and “Virus Production”, including viral vectors, oncolytic viruses (i.e. a virus engineered to preferentially attack cancer cells), viruses for use in vaccine development and gene-edited viruses for unspecified purposes. It is worth noting that, to date, many controversial “gain-of-function” experiments have justified modifying viruses for the same purposes as described by National Resilience’s Virus Production capabilities. In addition, National Resilience offers product formulations and other modalities, such as biologics and cell therapies, to its clientele and the “Virus Production” of its website has since been removed.

Resilience CEO Rahul Singhvi, Source: Resilience
National Resilience, being such a young company, has very few clients and there is little publicly available information on its manufacturing capabilities aside from the company’s website. The firm only acquired its first commercial manufacturing plant in March 2021, located in Boston, MA and purchased from Sanofi, followed shortly thereafter by the acquisition of another separate plant located in Mississauga, Ontario, Canada. Makeovers were announced for the plants, but little is publicly known about their progress. Prior to the acquisitions, the company had been subleasing a Bay area facility in Fremont, California. Reporters were puzzled at the time as to why a company with roughly 700 employees at the time had acquired a total of 599,00 square feet of manufacturing space after having only emerged from stealth less than 6 months prior.
In April 2021, National Resilience acquired Ology Bioservices Inc., which had received a $37 million contract from the US military the previous November to develop an advanced anti-COVID-19 monoclonal antibody treatment. This acquisition also provided National Resilience with its first Biosafety Level 3 (BSL-3) laboratory and the ability to manufacture cell and gene therapies, live viral vaccines and vectors and oncolytic viruses.
Despite being in the earliest stages of developing its “revolutionary” manufacturing capabilities, National Resilience entered into a partnership with the Government of Canada in July of last year. Per that agreement, the Canadian government plans to invest CAD 199.2 million (about $154.9 million) into National Resilience’s Ontario-based subsidiary, Resilience Biotechnologies Inc. Most of those funds are destined for use in expanding the Ontario facility that Resilience acquired last March and which is now manufacturing the mRNA for Moderna’s COVID-19 products. Canada’s Minister of Innovation, Science and Industry, François-Philippe Champagne, asserted at the time that the investment would “build future pandemic preparedness” and help “to grow Canada’s life science ecosystem as an engine for our economic recovery.” More recently, in 2022, the company has announced a few new clients – Takeda, Opus Genetics and the US Department of Defense.
According to National Resilience’s executives, the company’s ambitions apparently go far beyond manufacturing RNA and viruses. For instance, Resilience CEO Rahul Singhvi has claimed that the company is seeking to build “the world’s most advanced biopharmaceutical manufacturing ecosystem.” Yet, Singhvi has declined to offer much in the way of specifics when it comes to exactly how the company plans to become the planet’s most elite biomanufacturing company.
In an interview with The San Francisco Business Times, Singhvi states that Resilience is looking to fill its massive manufacturing plants with “technologies and people that can set and apply new standards for manufacturing cell therapies and gene therapies as well as RNA-based treatments.” Prior to Resilience, Singhvi was CEO of NovaVax and an operating partner at Flagship Pioneering, which played a major role in the creation and rise of Moderna.
Singhvi has further insisted that National Resilience is “not a therapeutics company, not a contractor and not a tools company” and instead aims “to boost production using the new therapeutic modalities” such as RNA-based treatments, which have become normalized in the COVID-19 era. Whereas contract manufacturers “are like kitchens, with pots and pans ready for any recipe,” “what we’re trying to do is fix the recipes,” Singhvi has explained. One member of Resilience’s board of directors, former FDA Commissioner and Pfizer Board member Scott Gottlieb, has described the company as seeking to act as the equivalent of Amazon Web Services for the biotechnology industry.
Essentially, Resilience bills itself as offering solutions that will allow “futuristic” medicines, including mRNA vaccines, to be produced more quickly and more efficiently, with the apparent goal of monopolizing certain parts of the biomanufacturing process. It also appears poised to become the manufacturer of choice for mRNA vaccines and experimental therapeutics in the event of a future pandemic, which some public health “philanthropists” like Bill Gates have said is imminent.
Perhaps the company’s most noteworthy ambition relates to their claims that they support clients through the government regulatory process. Given the company’s emphasis on speedy mass production of experimental gene therapies, its stated intention of getting the “futuristic” medical products it manufactures to market as quickly as possible seems at odds with the slower, traditional regulatory processes. Indeed, one could easily argue that the approvals of mRNA vaccines for the first time in human history during the COVID-19 crisis were only possible because of the major relaxing of regulatory procedurse and safety testing due to the perceived urgency of the situation.
Resilience seems intent on seeing that phenomenon repeat itself. As previously mentioned, the company claims to allow for the setting and application of “new standards for manufacturing cell therapies and gene therapies” and also says it plans to become a “technology-aggregating standards bearer that helps therapies come to market more efficiently.” It previously offered on its website “regulatory support” and “strategy consulting” to clients, suggesting that it would seek to mediate between clients and government regulators in order to fulfill its goal of having the products it manufactures taken to market more quickly. In addition, upon launch, the company claimed it planned to obtain unspecified “regulatory capabilities.” If so, it is certainly notable that former top Food and Drug Administration (FDA) officials are either on the company’s board or, as will be noted shortly, played a major role in the company’s creation.
The People Behind Resilience
Resilience was co-founded by Biotech venture capitalist Robert Nelsen, who is known for listening “to science’s earliest whispers, even when data are too early for just about anyone else.” Nelsen was one of the earliest investors in Illumina, a California-based gene-sequencing hardware and software giant that is believed to currently dominate the field of genomics. As mentioned in a previous Unlimited Hangout investigation, Illumina is closely tied to the DARPA-equivalent of the Wellcome Trust known as Wellcome Leap, which is also focused on “futuristic” and transhumanist “medicines.” Nelsen is now chairman of National Resilience’s board, which is a “Who’s Who” of big players from the US National Security State, Big Pharma and Pharma-related “philanthropy.”

Bob Nelsen of ARCH Venture Partners, Source: ARCH Venture Partners
However, while Nelsen has been given much of the credit for creating Resilience, he revealed in one interview that the idea for the company had actually come from someone else – Luciana Borio. In July of last year, Nelsen revealed that it was while talking to Borio about “her work running pandemic preparedness on the NSC [National Security Council]” that had “helped lead to the launch of Nelsen’s $800 million biologics manufacturing startup Resilience.”
At the time of their conversation, Borio was the vice president of In-Q-tel, the venture capital arm of the CIA that has been used since its creation in the early 2000s to found a number of companies, many of which act as Agency fronts. Prior to In-Q-Tel, she served as director for medical and biodefense preparedness at the National Security Council during the Trump administration and had previously been the acting chief scientist at the FDA from 2015 to 2017.
Borio is currently a senior fellow for global health at the Council on Foreign Relations, a consultant to Goldman Sachs, a member of the Bill Gates-funded vaccine alliance CEPI, and a partner at Nelsen’s venture capital firm ARCH Venture Partners, which funds Resilience. Nelsen’s ARCH previously funded Nanosys, the company of the controversial scientist Charles Lieber. Around the time of her conversation with Nelsen that led to Resilience’s creation, Borio was co-writing a policy paper for the Johns Hopkins Center for Health Security that recommended linking COVID-19 vaccination status with food stamp programs and rent assistance as a possible means of coercing certain populations to take the experimental vaccine.
Borio is hardly Resilience’s only In-Q-Tel connection, as the CEO of In-Q-Tel, Chris Darby, sits on the company’s board of directors. Darby is also on the board of directors of the CIA Officers Memorial Foundation. Darby was also recently a member of the National Security Commission on Artificial Intelligence (NSCAI), where members of the military, intelligence community and Silicon Valley’s top firms argued for the need to reduce the use of “legacy systems” in favor of AI-focused alternatives as a national security imperative. Among those “legacy systems” identified by the NSCAI were in-person doctor visits and even receiving medical care from a human doctor, as opposed to an AI “doctor.” The NSCAI also argued for the removal of “regulatory barriers” that prevent these new technologies from replacing “legacy systems.”

Resilience Board Member Drew Oetting, Source: 8VC
Another notable board member, in discussing Resilience’s intelligence ties, is Drew Oetting. Oetting works for Cerberus Capital Management, the firm headed by Steve Feinberg who previously led the President’s Intelligence Advisory Board under the Trump administration. Cerberus is notably the parent company of DynCorp, a controversial US national security contractor tied to numerous scandals, including scandals related to sex trafficking in conflict zones. Oetting is also part of the CIA-linked Thorn NGO ostensibly focused on tackling child trafficking that was the subject of a previous Unlimited Hangout investigation.
Oetting is also the co-founder of 8VC, a venture capital firm that is one of the main investors in Resilience. 8VC’s other co-founder is Joe Lonsdale and Oetting “started his career” as Lonsdale’s chief of staff. Lonsdale is the co-founder, alongside Peter Thiel and Alex Karp, of Palantir, a CIA front company and intelligence contractor that is the successor to DARPA’s controversial Total Information Awareness (TIA) mass surveillance and data-mining program. In addition, Oetting previously worked for Bill Gates’ investment fund.
Also worth noting is the presence of Joseph Robert Kerrey, former US Senator for Nebraska and a former member of the conflict-of-interest-ridden 9/11 Commission, on Resilience’s board. Kerrey is currently managing director of Allen & Co., a New York investment banking firm which has hosted an annual “summer camp for billionaires” since 1983. Allen & Co. has long been a major player in networks where organized crime and intelligence intersect, and is mentioned repeatedly throughout my upcoming book One Nation Under Blackmail. For instance, Charles and Herbert Allen, who ran the firm for decades, had considerable business dealings with organized crime kingpins and frontmen for notorious gangsters like Meyer Lansky, particularly in the Bahamas. They were also business partners of Leslie Wexner’s mentors A. Alfred Taubman and Max Fisher as well as associates of Earl Brian, one of the architects of the PROMIS software scandal – which saw organized crime and intelligence networks cooperate to steal and then compromise the PROMIS software for blackmail and clandestine intelligence-gathering purposes. Allen & Co. was a major investor in Brian’s business interests in the technology industry that Brian used in attempts to bankrupt the developers of PROMIS, Inslaw Inc. and to market versions of PROMIS that had been compromised first by Israeli intelligence and, later, the CIA.
In addition to these intelligence-linked individuals, the rest of Resilience’s board includes the former CEO of the Bill & Melinda Gates Foundation, Susan Desmond-Hellmann; former FDA Commissioner and Pfizer board member, Scott Gottlieb; two former executives at Johnson & Johnson; former president and CEO of Teva Pharmaceuticals North American branch, George Barrett; CalTech professor and board member of Alphabet (i.e. Google) and Illumina, Frances Arnold; former executive at Genentech and Merck, Patrick Yang; and Resilience CEO Rahul Singhvi.
To Boost or Not to Boost
It is certainly telling that the normally publicity hungry Moderna has said so little about its partnership with Resilience and that Resilience, despite its ambitious plans, has also avoided the media limelight. Considering Moderna’s history and Resilience’s connections, there may be more to this partnership that meets the eye and concerned members of the public would do well to keep a very close eye on Resilience, its partnerships, and the products it is manufacturing.
Given that we now live in a world where government regulatory decisions on the approval of medicines are increasingly influenced by corporate press releases and normal regulatory procedures have fallen by the wayside for being too “slow,” there is likely to be little scrutiny of the genetic material that Resilience produces for the “medicines of tomorrow.” This seems to be already true for Moderna’s recently retooled COVID-19 vaccine, as there has been no independent examination of the new genetic sequence of mRNA used in the Omicron-specific vaccine candidate or its effects on the human body in the short, medium or long term. For those who are skeptical of the outsized role that intelligence-linked companies are playing in the attempted technological “revolution” in the medical field, it is best to consider Resilience’s role in the upcoming fall vaccination campaign and in future pandemic and public health scenarios before trying its “futuristic” products.
Whitney Webb has been a professional writer, researcher and journalist since 2016. She has written for several websites and, from 2017 to 2020, was a staff writer and senior investigative reporter for Mint Press News. She currently writes for The Last American Vagabond.
Do the smallpox vaccines work to prevent monkeypox?
By Meryl Nass, MD | August 16, 2022
181 monkeypox patients (average age 37) were studied in Spain, and their illnesses described in the Lancet.
Mitjà and co-authors noted that 32 individuals in their cohort (18%) acquired monkeypox infection despite a smallpox vaccination history, which “warrants further investigation to better understand the protection provided by vaccination in the context of the current outbreak.”
Smallpox vaccination of infants ended over 50 years ago. Smallpox was declared eradicated 45 years ago. So few people in a cohort whose average age is 37 would be expected to have been vaccinated—and the vaccine they received would have preceded both ACAM-2000 and Jynneos, and been reliable at preventing smallpox. But it apparently did not prevent recent monkeypox.
In 2002 it was suggested that vaccination-induced immunity to smallpox was long-lasting.
We can thank Tony Fauci’s NIAID for sponsoring the original trial (2003) in which 20 plus year old (expired) smallpox vaccine was diluted to see how much you really needed. You didn’t need that much. This study presumably provided the underpinning for the dilution decision regarding Jynneos.
- When will a public health agency tell us whether the vaccines they are indiscriminately providing to MSM actually work?
- When will they tell us the side effects vaccinees are experiencing?
- And when will they tell us the results of the CDC study of 1600 Congolese healthcare workers that CDC jabbed between 2017 and 2020?
Featured Video

US Middle East Policy: The Growing Propensity for Genocide
or go to
Aletho News Archives – Video-Images
From the Archives
The New Baghdad Pact
By Dr Bouthaina Shaaban | February 23, 2017
A recently declassified CIA document prepared in 1983, and released on 20 January 2017, shows that the United States had at the time encouraged Saddam Hussein to attack Syria, which would have led to a vicious conflict between the two countries, thus draining their resources.
The report, which was then prepared by CIA officer Graham Fuller, indicates that the US tried adamantly to convince Saddam to attack Syria under any pretense available, in order to get the two most powerful countries in the Arab East to destroy each other, turning their attention away from the Arab-Israeli conflict. … continue
Blog Roll
 Aletho News
Aletho News- The Gratitude of the Captured
- Hezbollah denies involvement in deadly attack on UNIFIL in south Lebanon
- The prospect of an expanded and far more violent war
- Canada’s Carney Revives Online Censorship Bill
- Israeli soldiers kill UNICEF truck drivers delivering water to Gaza families
- Iran defends limits on Strait of Hormuz passage
- ‘We warned you’: Hormuz Strait back to pervious state amid US blockade
- Iran rejects uranium transfer, warns of response to naval blockade
- US Middle East Policy: The Growing Propensity for Genocide
- Daniel Davis: Iran Reopens the Strait of Hormuz
- If Americans Knew
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- Think the Iran war is a disaster? Blame these DC think tanks first.
- Number of Palestinian Prisoners Rises By 83% Since October 2023
- With multiple “ceasefires” in place, Israel keeps on killing in Gaza and Lebanon – Daily Update
- Mearsheimer: Israel Owns Trump
- Mark Levin and Jonathan Pollard Push for Nuking Iran
- TCN: America Enables Israel’s Crimes
- Israel’s Next Leader Will Be Just Like Bibi – but Without the Corruption
- Born into war, raised across borders: The story of Gaza’s premature babies separated from their parents amid Israel’s genocide
- No Tricks Zone
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
