As if the ongoing pandemics of COVID-19 and monkeypox aren’t enough, the New York health department is now urging residents to get vaccinated against polio, as the virus has been found in wastewater samples from two different counties.
Just two weeks prior to this, a 20-year-old in Rockland County was also diagnosed with polio.1 The case is reportedly the first in nearly a decade. The patient, identified as a “healthy young adult,” had not been vaccinated against polio as a child, and according to the New York health department, the positive water samples were genetically linked to this case. As reported by CBS News, August 5, 2022:2
“‘Based on earlier polio outbreaks, New Yorkers should know that for every one case of paralytic polio observed, there may be hundreds of other people infected,’ State Health Commissioner Dr. Mary T. Bassett said.
‘Coupled with the latest wastewater findings, the Department is treating the single case of polio as just the tip of the iceberg of much greater potential spread. As we learn more, what we do know is clear: the danger of polio is present in New York today’ …
Unvaccinated New Yorkers are encouraged to get immunized right away, the health department said. Unvaccinated people who live, work or spend time in Rockland County, Orange County and the greater New York metropolitan area are at the greatest risk …
According to the CDC’s most recent childhood vaccination data, about 93% of 2-year-olds in the U.S. had received at least three doses of polio vaccine. Meanwhile, adults who are not vaccinated would receive a three-dose immunization, and those who are vaccinated but at high risk can receive a lifetime booster shot, according to the health department.”
Orange County Health Commissioner Dr. Irina Gelman added:
“It is concerning that polio, a disease that has been largely eradicated through vaccination, is now circulating in our community, especially given the low rates of vaccination for this debilitating disease in certain areas of our County. I urge all unvaccinated Orange County residents to get vaccinated as soon as medically feasible.”
What They’re Not Telling You
In the U.S., polio was officially declared “eradicated” in 1979, and its eradication was attributed to a successful mass vaccination campaign. What the New York health department is not telling you, though, is that when polio strikes these days, it’s almost always caused by a vaccine strain. In contrast to CBS, the CNBC actually mentions this in its report:3
“The polio strain the adult in Rockland County caught suggests the chain of transmission did not begin in the United States. The strain the individual contracted is used in the oral polio vaccine, which contains a mild version of the virus that can still replicate. This means people who receive the oral vaccine can spread the virus to others.
But the U.S. hasn’t used the oral polio vaccine in more than 20 years. The U.S. uses an inactivated polio vaccine that is administered as [a] shot in the leg or arm …
The polio case in New York is genetically linked to the Rockland County wastewater sample as well as samples from the greater Jerusalem area in Israel and London in the United Kingdom.”
This is what’s called a delayed lede. Hard-news ledes give you the what, where, when, why and how in the first sentence or two. Here, the key point of the article — the fact that reemergence of polio is caused by the oral polio vaccine — is hidden further down the article than most people bother to read.
Wild Polio Has Been Replaced by Vaccine-Induced Polio
The fact that an oral vaccine strain is responsible for the New York polio case is an important detail. As explained by Vox:4
“Genetic sequencing shows that the recent case was a vaccine-derived poliovirus strain. This means the circulating virus isn’t from one of the few remaining pockets of endemic wild poliovirus, but rather from one of the many more countries with polio outbreaks that mutated from an oral, live-attenuated vaccine …
Although the live-attenuated poliovirus vaccine almost never causes polio itself … the fact that it contains a live virus inevitably carries some risk, unlike inactivated vaccines.
When live-attenuated polio vaccines are given in a community that contains a high fraction of unvaccinated people, the modified virus can infect others, and with enough generations of spread, it can … mutate back into a new virulent strain.”
The fact is, vaccine-derived polio has been the main circulating polio in most developing countries for years. And always, the response to vaccine-induced polio is — more polio vaccine.
Oral Live Polio Vaccines Shed
Cases of vaccine-derived polio have surged in recent years after global health authorities in 2016 decided to remove Type 2 poliovirus from the oral vaccine, leaving only Type 1 and Type 3.
The wild Type 2 poliovirus had been declared globally eradicated in 2015, and many felt it was unethical to expose children to a live poliovirus that no longer posed a threat.5 Moreover, the Type 2 portion of the vaccines was the source of most of the vaccine-derived strains that were by then causing paralysis.6
The change didn’t fix that problem, however. The live polio vaccine is still responsible for the vast majority of outbreaks.7 As explained by STAT News :8
“To understand the problem, you need to know some basics about polio vaccines — and, specifically, the oral vaccine, known as OPV. OPV contains the live but weakened viruses that Albert Sabin engineered in the late 1950s. This is the vaccine that is used in most of the developing world, unlike the United States, which uses IPV, or inactivated polio vaccine.
The strengths of Sabin’s vaccine … include: its pennies-a-dose price; its ease of administration; and the fact that the vaccine viruses spread from vaccinated children to others around them, which means vaccination campaigns protect many more children than just those the vaccination teams find.
Back in the day in the developing world, if you vaccinated some kids in a neighborhood, you pretty much vaccinated the neighborhood. But that last benefit, which was helpful when there were hundreds of thousands of polio cases a year, is a decidedly mixed blessing now.
The Sabin vaccine viruses, once released in a community, continue to spread if they encounter children who are not immune to polio … As they cycle from child to child, the vaccine viruses can regain the virulence traits that Sabin engineered out of them. If the vaccine viruses circulate long enough, they regain the power to paralyze.
The part of the oral vaccine that protected against type 2 viruses was removed in spring 2016 in a move synchronized around the world. Since then, the number of children with zero immunity to type 2 polio (and type 2 vaccine viruses) has grown daily. This cohort numbers in the tens of millions.
In parts of the world where type 2 vaccine viruses aren’t spreading, that lack of immunity doesn’t matter. But in countries in Central Africa, where the vaccine viruses are spreading over greater and greater territory, those unprotected children are at risk. Children without any type 2 polio protection give the vaccine viruses the chance to circulate enough to regain paralytic powers.”
Most Polio Today Is Caused by the Live Polio Vaccine
Importantly, while the inactivated polio vaccine prevents paralysis, it does not prevent infection. So, even those who have received the inactivated version can be infected by a vaccine-derived poliovirus, and can spread it to others. In Africa, the response to polio outbreaks has been to go in and broadly vaccinate as many children as possible with the original Type 2-containing polio vaccine.
But while this seems to work regionally, unvaccinated children in neighboring regions suddenly become targets as the vaccine viruses start to spread. So, essentially, these efforts merely reseed the transmission chain. For example, India’s polio eradication campaign in 2011 caused 47,500 cases of vaccine-induced polio paralysis — a condition that is twice as deadly as wild polio.9 And, as noted by the Global Polio Eradication Initiative:10
“[C]irculating vaccine-derived poliovirus, or cVDPV … have been increasing in recent years due to low immunization rates within communities. cVDPV type 2 (cVDPV2) are the most prevalent, with 959 cases occurring globally in 2020.
Notably, since the African Region was declared to have interrupted transmission of the wild poliovirus in August 2020, cVDPV are now the only form of the poliovirus that affects the African Region.”
Some believe the ultimate answer is a brand-new polio vaccine, and the Bill & Melinda Gates Foundation has spearheaded this development effort. Not surprisingly, upon hearing the news of a polio case in New York, Gates reminded his Twitter followers that “until we #EndPolio for good, it remains a threat to us all. The global eradication strategy must be fully supported to protect people everywhere.”11
Disturbingly, STAT News12 points out that “The plan is to use the vaccine under the WHO’s emergency use protocol, even before it is licensed.” Do children really need yet another experimental injection foisted into them? This seems like reckless folly at best. Be that as it may, this next-gen polio vaccine is predicted to be made available sometime in 2023.
Is the Official Polio Story True?
In “The Curios Case of Polio, DDT and Vaccines,” a guest-post posted to my Substack in February 2022, investigative journalist Tessa Lena takes a deeper look at the official history of polio. While polio is attributed to a viral infection, polio-like symptoms can also be caused by a number of toxic substances, including lead, arsenic and pesticides such as DDT.13
Indeed, DDT exposure may have been a major contributing factor to the polio epidemics of the 1950s. Lena cites a 1951 article14 by Dr. Ralph R. Scobey in the Archives of Pediatrics, titled “Is the Public Health Law Responsible for the Poliomyelitis Mystery?” in which he stressed that poliomyelitis “could be produced both by organic and inorganic poisons as well as by bacterial toxins.”
However, once polio was classified as a communicable viral disease, research into these other potential mechanisms ceased, as all funding for poliomyelitis research was “designated for the investigation of the infectious theory only.”
Interestingly, Scobey points out that the polio contagion theory was almost entirely based on work done at the Rockefeller Institute. Afflicted children were kept in the general hospital ward, and not a single case of transmission occurred between patients. This detail contradicts the viral theory of polio, but it was ignored and the declaration that polio is a viral infection was quickly accepted and never successfully challenged again.
The case of the polio vaccine is in some ways reminiscent of what we’re now seeing with the mRNA COVID shots. Over time, the shots make you more prone to COVID. At the same time, they pressure the virus to mutate at a rapid clip, triggering outbreak after outbreak of increasingly resistant SARS-CoV-2 strains.
Today, the original SARS-CoV-2 Wuhan strain has been mutated out of existence, and all infections are caused by variants created in response to mass injection. On the one hand, these variants have mutated into far milder and less lethal forms, but on the other, they’ve developed resistance against both natural and jab-based antibodies, resulting in seemingly never-ending rounds of infection.
A silver lining of the COVID jab debacle is that more and more people are taking a second look at the theory of vaccination altogether, and are coming to the realization that many vaccines don’t work, and that none have been properly tested for safety using inert placebo controls.
Pfizer CEO Albert Bourla unironically tweeted that, despite catching COVID, he was grateful for getting jabbed four times and still requiring another one of his products to treat the infection.
“I would like to let you know that I have tested positive for COVID-19,” he tweeted. “I am thankful to have received four doses of the Pfizer-BioNTech vaccine, and I am feeling well while experiencing very mild symptoms. I am isolating and have started a course of Paxlovid.”
Following his statement, the ridicule via Twitter ratio came on quickly:
Liz Wheeler
Hahahahahahahahahaha remember that time you avoided taking your own vaxx because you knew it was garbage? Until you were found out when Israel refused you entry. I sincerely hope you recover quickly, but you & your 💉 are frauds.
Indeed, it’s harder than ever to take these talking heads seriously.
This is the same company that’s paid millions to settle allegations of bribing doctors and the same company that wanted to keep vaccine data hidden for 75 years, only to be forced by a court order to release nine pages worth of potential vaccine adverse effects.
Now, in this stunning tacit admission, Pfizer’s own CEO has revealed that two boosters can’t even stave off infection. Talk about a product flop.
Of course, Bourla isn’t the only one with a case of the quadruple vaxxed COVID blues. Recently, US President Joe Biden told the world that he’d caught COVID not once but twice despite receiving two boosters.
If there was still any doubt regarding a lack of vaccine efficacy, Pfizer’s CEO has proven that the vaccine can’t stop the spread — which is what everyone was promised when the vaccine was first rolled out.
According to a media report, the heirs to three US oil dynasties finance climate activists and non-governmental organizations that promote climate protest actions. Descendants of oil barons Getty and Rockefeller allegedly feel responsible for preventing “eradication” on Earth. That may not be the real reason however.
Descendants of the oil billionaires have been paying hundreds of green activists $25 000 a year each for their protests around the world, Britain’s Daily Mail reported August 10. Aileen Getty, Rebecca Rockefeller Lambert and Peter Gil Case fund such salaries through their non-governmental organizations (NGOs).
Aileen Getty, granddaughter of Getty Oil’s founder, now has over $1 million through her Climate Emergency Fund paid to activists. The wealthy heirs to the Rockefeller family, Rebecca Rockefeller Lambert and Peter Gil Case, whose ancestors founded Standard Oil in 1870, have spent over thirty million dollars on the Equation Campaign.
They all pay the activists, who, according to the Daily Mail, have caused disturbances with their actions around the world, especially in recent months, and finance the relevant NGOs. Lambert and Case, for example, put eco-activists from groups like Just Stop Oil on the payroll for $25 000 each and also funded the organization themselves. The descendants of oil baron John D. Rockefeller also established a fund to support anti-fossil fuel protests.
In recent months, thousands of activists have taken to the streets around the world to protest. The environmentalists also rioted and caused destruction, including in the US, Europe, the UK and Australia. Tires of SUVs were punctured in the US, UK and Australia, and famous oil paintings were vandalized in EU countries by the very activists who are on the payrolls of oil heirs’ non-profit organizations.
The Daily Mail questioned this type of funding: “Three American oil scions have been bankrolling mobs of eco-zealots who have terrorized the world by slashing tires, blocking traffic and attacking firms. Aileen Getty, Rebecca Rockefeller Lambert and Peter Gill Case, who are heirs to their families’ huge fortunes, are paying the salaries for thugs through their non-profits in an apparent bid to offset their relatives’ legacies.”
In 2019, Aileen Getty donated $500 000 to Extinction Rebellion climate activists. She herself is convinced that “a comprehensive disruption of everyday life” is necessary for actions. Getty conforms to the stereotype of idle, rich heirs: She contracted HIV from an extramarital affair and has survived numerous drug overdoses.
She told the New York Times that she wanted to support the effectiveness of the activists she sponsored and has so far donated $1 million from her own wealth to the Climate Emergency Fund. In her opinion, the civil disobedience spurned by such grassroots organizations is just a warning signal and the destruction is minimal compared to what is at stake.
She told the newspaper: “Let’s not forget that we’re talking about extinction. Don’t we have a responsibility to do everything we can to protect life on Earth?”
The Daily Mail also pointed out that scaremongering by various scientists are also financed by the oil heirs. In the US, the Climate Emergency Fund of the NGO Scientist Rebellion made $100 000 available for consultant salaries and travel expenses. Eco-warriors need money since they spend their lives protesting. Without funding, we would therefore not see the likes of Greta Thunberg making a fuss.
NASA climate researcher Peter Kalmus, who also belongs to this organization, brought together around 1000 scientists in 25 different countries who blocked traffic and chained themselves to landmark buildings.
‘Wreaking havoc on ordinary people’ to keep oil prices high
According to the Daily Mail, Kalmus justified his involvement in Scientist Rebellion’s concept of disrupting citizens’ everyday lives as follows: “He spent 16 years looking for ways to save the planet and came to the conclusion that the best way to do it is to wreak havoc on ordinary people.”
Last year in June, the Wall Street Journal reported that climate activists were driving up the price of oil: “Some investors are wagering that Wall Street’s preference for green energy will depress spending on oil extraction, setting the stage for supply shortages and higher fuel prices. The bets come as money managers line up trillions of dollars for wind, solar and other renewable programs and expenditures on oil projects tumble. The drop in fossil-fuel spending is becoming so severe that energy companies could struggle to quench the world’s thirst for oil, some analysts say.”
More recently, US sanctions against Russia have also helped to keep oil prices high.
I just sent the email below to nearly 300 people at the CDC who are known to be involved in the COVID vaccine program.
I pointed out that existing autopsy protocols cannot find vaccine deaths and asked why isn’t the CDC notifying medical examiner and pathologists how to find COVID vaccine-related deaths?
Do you think I’ll hear back? Do you think they will do anything differently?
Here is the full text of the email:
I wanted to make sure everyone who is involved in the COVID vaccination program understands exactly why the CDC isn’t finding any vaccine associated deaths.
The short answer is because they aren’t looking for them properly even though the methodology to do so is in plain sight. That methodology is ignored. This is why the pathologists find nothing.
A simple analogy: if the PCR test were run with just 5 cycles, we’d never find any COVID virus. We’re basically doing the same thing with the tests we do post-vaccine: we didn’t change the tests to FIND the vaccine.
This is unethical.
I wanted to make sure everyone who works at the CDC is aware of this.
At the very least, the CDC needs to publicly acknowledge this clear failing.
As I said recently on Fox News, hundreds of thousands of Americans have been killed by the COVID vaccines.
People who were skeptical of my numbers found that document very convincing.
Fox News REFUSED to look at my data or discuss it. Why not? Because they are paid not to challenge the narrative. Over $1B is being paid out to promote the vaccines and ignore anything that goes against the narrative.
Even worse, nobody will go on camera to try to refute any of this. Why not?
The reason the CDC finds no deaths is because they aren’t looking for them with tools that will find the deaths.
You need to run specialized tests to determine an association with the vaccine. The standard tests run by medical examiners are NEVER going to find an association. That was clear in their paper and it was independently validated by Dr. Ryan Cole who is a very experienced board certified pathologist.
The question you all should be asking is:
Why isn’t the CDC requiring that for anyone who dies 30 days after getting a vaccine an autopsy protocol that can find an association with the vaccine using the necessary specialized tests?
Such a protocol already exists and it is proven it works. See this article.
Dr. Cole points out that YOU NEED SPECIALIZED TESTS to find the association.
How many pathologists are doing these tests in America? Just one as far as he knows.
I am absolutely baffled as to why the CDC has never done any of these tests and why nobody has talked to Dr. Cole.
Do you know why? Can you tell me?
While there may be a better protocol, this protocol is proven to detect vaccine involvement in 93% of the cases studied. These are all tissue samples from people dying shortly after vaccination where the medical examiners were unable to find any association.
If this protocol is insufficient, where is the CDC document explaining why and proposing a better one that finds more association?
If the CDC has been doing adequate tests, where is the documentation of that?
It seems pretty clear to me that the CDC isn’t finding vaccine-caused deaths because they refuse to look.
They can even go back to the autopsy tissue samples they already have and re-stain them to see how many were missed in the initial analysis as documented in the Rosenblum paper in Lancet.
The Rosenblum paper should have reported that none of the autopsies used stains that were necessary to show an association. But this was never mentioned. Shouldn’t that paper be corrected?
I tried to talk to the authors, but Martha Sharan at the CDC ignored every email and phone call I left for her.
Is this how science is done? By not allowing anyone to challenge your work?
My article also explains very clearly why doctors are not finding vaccine-related deaths. The interview with Gina Doane makes it clear her dad died from the vaccine yet the doctor in charge refused to even consider this as a possibility even though NONE of his other explanations fit, and the vaccine hypothesis fit perfectly. That’s not how science works. This is corruption. You don’t need a medical degree to figure it out. It’s all in the video.
But that second video shows you first hand how doctors are looking the other way.
I hope you will find the two videos and the content of the post eye opening. One commenter wrote: ” One of the best and most revealing pieces of research on the net….very telling. Thank you.”
It’s well worth your time. I’ve written over 700 articles on the COVID vaccines and the content presented in these two interviews are the most important interviews for everyone at the CDC to watch because it shows you how 1) the tests are inadequate and 2) even with overwhelming evidence, the doctors are deliberately NOT acknowledging vaccine death.
If you want to chat, I can be reached at <redacted>.
-steve
Am I flogging a dead horse?
No. I’m just putting hundreds of people at the CDC on the record as having been notified of what is going on.
And who knows. Maybe ONE person is honest.
The CDC has backed off their earlier “guidance” and have removed things from their website that were untrue.
After a landmark court ruling in December, the name “Keira Bell” was cited worldwide, admiringly by some, with hostility by others. (Photo: Paul Cooper/Shutterstock)
From the earliest days, my home life was unhappy. My parents—a white Englishwoman and a black American who got together while he was in Britain with the U.S. Air Force—divorced when I was about 5. My mother, who was on welfare, descended into alcoholism and mental illness. Although my father remained in England, he was emotionally distant to me and my younger sister.
I was a classic tomboy, which was one of the healthier parts of my early life in Letchworth, a town of about 30,000 people, an hour outside London. Early in childhood, I was accepted by the boys—I dressed in typically boy clothing and was athletic. I never had an issue with my gender; it wasn’t on my mind.
(Courtesy: Keira Bell)
Then puberty hit, and everything changed for the worse. A lot of teenagers, especially girls, have a hard time with puberty, but I didn’t know this. I thought I was the only one who hated how my hips and breasts were growing. Then my periods started, and they were disabling. I was often in pain and drained of energy.
Also, I could no longer pass as “one of the boys,” so lost my community of male friends. But I didn’t feel I really belonged with the girls either. My mother’s alcoholism had gotten so bad that I didn’t want to bring friends home. Eventually, I had no friends to invite. I became more alienated and solitary. I had been moving a lot too, and I had to start over at different schools, which compounded my problems.
By the time I was 14, I was severely depressed and had given up: I stopped going to school; I stopped going outside. I just stayed in my room, avoiding my mother, playing video games, getting lost in my favorite music, and surfing the internet.
Something else was happening: I became attracted to girls. I had never had a positive association with the term “lesbian” or the idea that two girls could be in a relationship. This made me wonder if there was something inherently wrong with me. Around this time, out of the blue, my mother asked if I wanted to be a boy, something that hadn’t even crossed my mind. I then found some websites about females transitioning to male. Shortly after, I moved in with my father and his then-partner. She asked me the same question my mother had. I told her that I thought I was a boy and that I wanted to become one.
As I look back, I see how everything led me to conclude it would be best if I stopped becoming a woman. My thinking was that, if I took hormones, I’d grow taller and wouldn’t look much different from biological men.
I began seeing a psychologist through the National Health Service, or NHS. When I was 15—because I kept insisting that I wanted to be a boy—I was referred to the Gender Identity Development Service, at the Tavistock and Portman clinic in London. There, I was diagnosed with gender dysphoria, which is psychological distress because of a mismatch between your biological sex and your perceived gender identity.
By the time I got to the Tavistock, I was adamant that I needed to transition. It was the kind of brash assertion that’s typical of teenagers. What was really going on was that I was a girl insecure in my body who had experienced parental abandonment, felt alienated from my peers, suffered from anxiety and depression, and struggled with my sexual orientation.
After a series of superficial conversations with social workers, I was put on puberty blockers at age 16. A year later, I was receiving testosterone shots. When 20, I had a double mastectomy. By then, I appeared to have a more masculine build, as well as a man’s voice, a man’s beard, and a man’s name: Quincy, after Quincy Jones.
(Courtesy: Keira Bell)
But the further my transition went, the more I realized that I wasn’t a man, and never would be. We are told these days that when someone presents with gender dysphoria, this reflects a person’s “real” or “true” self, that the desire to change genders is set. But this was not the case for me. As I matured, I recognized that gender dysphoria was a symptom of my overall misery, not its cause.
Five years after beginning my medical transition to becoming male, I began the process of detransitioning. A lot of trans men talk about how you can’t cry with a high dose of testosterone in your body, and this affected me too: I couldn’t release my emotions. One of the first signs that I was becoming Keira again was that—thankfully, at last—I was able to cry. And I had a lot to cry about.
The consequences of what happened to me have been profound: possible infertility, loss of my breasts and inability to breastfeed, atrophied genitals, a permanently changed voice, facial hair. When I was seen at the Tavistock clinic, I had so many issues that it was comforting to think I really had only one that needed solving: I was a male in a female body. But it was the job of the professionals to consider all my co-morbidities, not just to affirm my naïve hope that everything could be solved with hormones and surgery.
Last year, I became a claimant against the Tavistock and Portman NHS Foundation Trust in a judicial-review case, which allows petitioners in Britain to bring action against a public body they deem to have violated its legal duties. Few judicial reviews get anywhere; only a fraction obtain a full hearing. But ours did, with a panel of three High Court judges considering whether youths under treatment at the clinic could meaningfully consent to such medical interventions.
Bell in January 2020, after she brought legal action against the clinic. (Photo: Sam Tobin/PA Wire)
My team argued that the Tavistock had failed to protect young patients who sought its services, and that—instead of careful, individualized treatment—the clinic had conducted what amounted to uncontrolled experiments on us. Last December, we won a unanimous verdict. The judges expressed serious doubts that the clinic’s youngest patients could understand the implications of what amounted to experimental treatment with life-altering outcomes.
In their ruling, the judges repeatedly expressed surprise at what had been going on at the Tavistock, particularly its failure to gather basic data on its patients. They noted the lack of evidence for putting children as young as 10 years old on drugs to block puberty, a treatment that is almost universally followed by cross-sex hormones, which must be taken for life to maintain the transition. They also had concerns about the lack of follow-up data, given “the experimental nature of the treatment and the profound impact that it has.”
Notably, a growing wave of girls has been seeking treatment for gender dysphoria. In 2009-10, 77 children were referred to the Gender Identity Development Service, 52% of whom were boys. That ratio started to reverse a few years later as the overall number of referrals soared. In England in 2018-19, 624 boys were referred and 1,740 girls, or 74% of the total. Over half of referrals were for those aged 14 or under; some were as young as 3 years old. The court noted the practitioners at the Tavistock did not put forward “any clinical explanation” for the dramatic rise in girls, and expressed surprise at its failure to collate data on the age of patients when they began puberty blockers.
The ruling does not completely prevent a minor from beginning a medical transition. But the judges recommended that doctors consider getting court permission before starting such treatment for those 16 to 17; they concluded it was “very doubtful” that patients aged 14 and 15 could have sufficient understanding of the consequences of the treatment to give consent; and that it was “highly unlikely” for those aged 13 and under.
In response, the NHS said that the Tavistock had “immediately suspended new referrals for puberty blockers and cross-sex hormones for the under-16s, which in future will only be permitted where a court specifically authorizes it.” The Tavistock appealed the ruling, and the court will hear its appeal in June.
The puberty blockers that I received at 16 were designed to stop my sexual maturation: The idea was that this would give me a “pause” to think about whether I wanted to continue to a further gender transition. This so-called “pause” put me into what felt like menopause, with hot flushes, night sweats, and brain fog. All this made it more difficult to think clearly about what I should do.
By the end of a year of this treatment, when I was presented with the option of moving on to testosterone, I jumped at it—I wanted to feel like a young man, not an old woman. I was eager for the shots to start, and the changes this would bring. At first, the testosterone gave me a big boost in confidence. One of the earliest effects was that my voice dropped, which made me feel more commanding.
Over the next couple of years, my voice deepened further, my beard came in, and my fat redistributed. I continued to wear my breast binder every day, especially now that I was completely passing as male, but it was painful and obstructed my breathing. By the time I was 20, I was being treated at the adult clinic. The testosterone and the binder affected the appearance of my breasts, and I hated them even more. I also wanted to align my face and my body, so got a referral for a double mastectomy.
My relationship with my parents continued to be difficult. I was no longer speaking to my mother. My father had kicked me out of his apartment shortly after I turned 17, and I went to live in a youth hostel. He and I were still in touch, though he was adamantly opposed to my transition. Reluctantly, he took me for the surgery. I was a legal adult when it took place, and I don’t relieve myself of responsibility. But I had been put on a pathway—puberty blockers to testosterone to surgery—when I was a troubled teen. As a result of the surgery, there’s nerve damage to my chest, and I don’t have sensation the way I used to. If I am able to have children, I will never breastfeed them.
Around the end of that first year post-surgery, something started happening: My brain was maturing. I thought about how I’d gotten where I was, and gave myself questions to contemplate. A big one was: “What makes me a man?”
I started realizing how many flaws there had been in my thought process, and how they had interacted with claims about gender that are increasingly found in the larger culture and that have been adopted at the Tavistock. I remembered my idea as a 14-year-old, that hormones and surgery would turn me into someone who appeared to be a man. Now, I was that person. But I recognized that I was very physically different from men. Living as a trans man helped me acknowledge that I was still a woman.
I also started to see what I was living out was based on stereotypes, that I was trying to assume the narrow identity of “masculine guy.” It was all making less and less sense. I was also concerned about the effect my transition would have on my ability to find a sexual partner.
Then there was the fact that no one really knew the long-term effects of the treatment. For instance, the puberty blockers and testosterone caused me to have to deal with vaginal atrophy, a thinning and fragility of the vaginal walls that normally occurs after menopause. I started feeling really bad about myself again.
I decided to stop, cold turkey. When I was due for my next testosterone shot, I canceled the appointment.
After I came to this decision, I found a subreddit for detransitioners. The number of people on it started rising, as if all these young women had come to a collective realization of the medical scandal we had been a part of. It was a place we could talk about our experiences and support each other. I felt liberated.
What happened to me is happening across the Western world. Little of my case was a surprise to those paying attention to the Tavistock whistle-blowers who in recent years have spoken out in alarm to the media, sometimes anonymously. Some have left the service because of these concerns. But the transgender issue is now highly political and wrapped up in questions of identity politics. It can be perilous to raise questions or doubts about young people’s medical gender transitions. Some who have done so have been vilified and had their careers threatened.
At the Tavistock, practitioners provide “gender affirmative care”—in practice, this means that when children and teens declare a desire to transition, their assertions are typically accepted as conclusive. Affirmative care is being adopted as a model in many places. In 2018, the American Academy of Pediatrics released a policy statement on the treatment of young people who identify as transgender and gender diverse that advocated for “gender-affirmative care.”
But former Tavistock practitioners have cited varied problems suffered by the kids who sought help, such as sexual abuse, trauma, parental abandonment, homophobia in the family or at school, depression, anxiety, being on the autism spectrum, having ADHD. These profound issues, and how they might be tied up with feelings of dysphoria, have often been ignored in favor of making transition the all-purpose solution.
As the High Court found, much of the clinic’s treatment is not even based on solid evidence. At the time our case was accepted, the NHS was asserting that the effects of puberty blockers are “fully reversible.” But recently, the NHS reversed itself, acknowledging “that ‘little is known about the long-term side-effects’ on a teenager’s body or brain.” That didn’t stop them from prescribing these drugs to people like me.
Dr. Christopher Gillberg, a professor of child and adolescent psychiatry at Gothenburg University in Sweden and a specialist in autism, was an expert witness for our case. Gillberg said in his court statement that over his 45 years of treating children with autism, it was rare to have patients with gender dysphoria—but their numbers started exploding in 2013, and most were biological girls. Gillberg told the court that what was happening at the Tavistock was a “live experiment” on children and adolescents.
Parents who are reluctant or even alarmed about starting their children on a medical transition may be warned, “Would you rather have a dead daughter or a live son?” (Or vice versa.) I had suicidal thoughts as a teen. Suicidal thoughts indicate serious mental health problems that need assessment and proper care. When I told them at the Tavistock about these thoughts, that became another reason to put me on hormones quickly to improve my well-being. But after the court ruling, the Tavistock released an internal study of a group of 44 patients who had started taking puberty blockers at ages 12 to 15. It said that this treatment had failed to improve the mental state of patients, having “no significant effect on their psychological function, thoughts of self-harm, or body image.” Additionally, of those 44 patients, 43 went on to cross-sex hormones. This suggests blocking puberty isn’t providing a pause. It is giving a push.
Before beginning on testosterone, I was asked if I wanted children, or if I wanted to consider freezing my eggs because of the possibility that transition would make me infertile. As a teenager, I couldn’t imagine having kids, and the procedure wouldn’t have been covered by the NHS. I said I was fine if I couldn’t, and I didn’t need to freeze my eggs. But now as a young adult, I see that I didn’t truly understand back then the implications of infertility. Having children is a basic right, and I don’t know if that has been taken from me.
As part of its defense, the Tavistock put forth statements from a few young trans people who are happy with their care. One is S, a 13-year-old trans boy who got puberty blockers from a private provider because the waiting list at the Gender Identity Development Service was so long. S told the court that he had “no idea what me in the future is going to think” about being able to have children and that since he has never been in “a romantic relationship,” the idea of one is not “on my radar at the moment.”
Lots of teenagers, when contemplating future sexual relationships, feel baffled and even disturbed at the thought. Those same people, when adults, often feel very differently. I know, because this happened to me. I’d never been in a sexual relationship at the time of my transition, so I didn’t truly understand what the transition would mean sexually.
S’s statementdemonstrates how difficult it is for minors to give consent for procedures they can’t yet understand. As the judges wrote, “There is no age-appropriate way to explain to many of these children what losing their fertility or full sexual function may mean to them in later years.”
Bell speaking to the media after the court ruling last December. (Photo: Sam Tobin/PA Wire)
Today, at 24, I’m in my first serious relationship. My partner is very supportive of everything I do, and I am the same for her. She has a large group of female friends who accept me; it’s been very healing. For now, I don’t speak to either of my parents or have a relationship with them.
I still get taken for male sometimes. I expect that, and I’m not angry about it. I know that I will live with that for the rest of my life. What I am angry about is how my body was changed at such a young age. People want to know if I’m going to have reconstructive surgery of my breasts or do other things to make me look more female. But I haven’t fully processed the surgery I had to remove my breasts. For now, I want to avoid more such surgical procedures.
When I joined the case, I didn’t realize how big it would become. What has happened since the ruling has been a rollercoaster. Many people have thanked me. I have also been attacked online. If you’re someone who regrets transitioning and decides to speak out about your experiences, you’re considered a bigot. You may be told that you’re trying to take away trans rights, that children know what’s best for themselves and their bodies, and that you’re ruining kids’ lives.
But I am focused on what is best for distressed young people. A lot of girls are transitioning because they’re in pain, whether it’s from mental-health disorders, or life trauma, or other reasons. I know what it’s like to get caught up in dreaming that transitioning will fix all of this.
Although sharing my story has been cathartic, I still struggle, and have yet to receive appropriate therapy. As I go on with my life, I plan to continue to be an activist on behalf of this cause. I want the message of cases like mine to help protect other kids from taking a mistaken path. This year, I helped create the first Detrans Awareness Day, on March 12. I hope that, in years to come, this day can be a beacon to empower others.
I do not believe in rigid gender expression. People should be comfortable and feel accepted if they explore different ways of presenting themselves. As I said in my statement after the ruling, this means stopping the homophobia, the misogyny, and the bullying of those who are different.
I also call on professionals and clinicians to create better mental health services and models to help those dealing with gender dysphoria. I do not want any other young person who is distressed, confused, and lonely as I was to be driven to conclude transition is the only possible answer.
I was an unhappy girl who needed help. Instead, I was treated like an experiment.
But for the programme itself the BBC commissoned a large survey which, we show, revealed that 26% were unvacinated.
To understand why it is so critical to get an accurate estimate of the proportion of unvaccinated see this 2 minute accompanying video: https://youtu.be/8It4qI9yhzQ
This report is all over the media, and all with virtually the same wording, suggesting a carefully coordinated, manufactured story, almost certainly from one of the well funded, climate misinformation organisations.
The BBC headline is grossly misleading, as the 30cm is the water under the boat; As Captain Kempl comments, the river depth is actually 1.5m.
The river gauge measurement of 42cm at Kaub is also widely reported, but is equally misleading, as this measurement is taken near the river bank, rather than at the deepest part of the stream.
In none of the dozens of reports I have read is there any actual historical data to compare against this event, whether rainfall or water level data. We are told this is the lowest water level since 2018, as if this means anything at all. There is no evidence presented to show that this drought is in any way unprecedented, or that droughts are becoming more extreme; merely this claim that appears in most of the articles:
“HGK and other shipping companies are preparing for a “new normal” in which low water levels become more common as global warming makes droughts more severe, sapping water along the length of the Rhine from the Swiss Alps to the North Sea.
“There’s no denying climate change and the industry is adjusting to it,”
However, annual rainfall trends at Mainz, which is just upstream of Kalb, show that while recent years have been drier than the 1980s and 90s, they are no drier than the 1950s. We also see exactly the same trends with April to September rainfall:
And finally, WUWT offers an insight to some of the megadroughts in Germany in the past, notably in 1540.
There is therefore nothing to suggest that this is not just another weather event.
In 2015 a team of researchers employed by the medical services of the US military published a peer-reviewed paper on the incidence of myocarditis and pericarditis after smallpox vaccination (SPX) and vaccination with an inactivated trivalent influenza vaccine (TIV).
Despite being published 7 years ago before anyone had heard of “covid”, the findings in this study could have very significant implications for the Covid-19 mRNA injections.
In this study, the researchers found that:
When active surveillance systems are used, significantly more myocarditis cases were identified than in earlier studies which had relied on more passive reporting.
The incidence of cases of possible myocarditis without symptoms – detected by testing all subjects vaccinated regardless of symptoms – was far higher than the cases in which subjects developed symptoms such that they would seek medical help.
Given these observations, it seems highly likely that the incidence rates of myocarditis following Covid vaccination have to date been severely underestimated.
The background to the study was that the US military rolled out a limited program of SPX following a perceived threat that smallpox might be used as a weapon in a bioterrorism incident. By the time of the paper’s publication, >2m doses had been administered, but the US had 290m doses in reserve to use for the general population if required. Concerns had been raised about a possible risk of myocarditis after this vaccination. This study sought to quantify these risks.
Key aspects of the study design:
Subjects were selected from previously healthy military personnel presenting for either SPX (1081 subjects) or TIV (189 subjects). A battery of baseline tests were performed and these were repeated either once or twice 5-8 days after vaccination and / or 9-28 after vaccination.
The notable difference between this and other studies assessing myocarditis and pericarditis rates was that the assessments were performed on all subjects and they included measurements of cardiac troponin levels (a protein which is released by damaged heart muscle cells) and ECG, in an attempt to detect possible “subclinical” cases of myocarditis – ie those which did not result in symptoms and so ordinarily would not gain the attention of healthcare systems.
Clinical myocarditis and pericarditis were determined according to published epidemiological case definitions that require the development of new onset cardiac symptoms soon after vaccine exposure, and each case was confirmed by an independent adjudicator.
Possible subclinical myocarditis and pericarditis were diagnosed whenever troponin levels rose by or to a certain level[1], or by ECG changes respectively, in the absence of symptoms.
Incidence rates were compared to background incidence rates calculated from a 2002 study among 1,390,352 service members (no exposure to any vaccines).
Key results:
Subjects receiving SPX were predominantly young (mean 23 years) and male (88%), those in the TIV cohort were more evenly balanced (54% male) and older (mean 36 years)
8.8% of the SPX recipients reported severe cardiac symptoms (defined as >3 out of 10 on a visual scale for at least 2 days).The most frequently reported cardiac symptoms were chest pain and dyspnea on exertion.
Despite no significant differences in pre-vaccine health self-assessment between the cohorts and fewer reported physical limitations in the SPX cohort, there was a significantly higher incidence of new onset cardiac symptom(s) post-SPX (10.6%) compared to the older post-TIV cohort (2.6%), p<0.001. These differences remained 4-5 fold higher in the SPX cohort after adjusting for group differences in age, sex, weight, race, smoking, and physical limitations, and also when symptoms were limited to consideration of those above 3 out of 10 on the visual scale.
The incidence rate of clinical myocarditis / pericarditis after SPX was 5 cases out of 1081 (4 were myocarditis and one pericarditis), equating to 463 per 100,000, which was >200 x background expected rates.
The incidence of possible subclinical myocarditis / pericarditis after SPX was 2868 per 100,000, or nearly 3%, which was 6 x the rate of clinical myocarditis.[2] This could not be compared to an expected background rate as this had never been measured before in this way.
No cases of either clinical or subclinical myocarditis were detected after TIV.
Implications.
Before going on to discuss the implications of this study for the Covid-era, it must be emphasised that “full recovery” from myocarditis is a misleading term: whilst the patients may initially become symptom-free, all should ideally receive regular cardiological follow-up to detect cardiomyopathy and / or arrhythmias later in life, and there is a significantly raised risk of cardiac morbidity and mortality.
Moreover, in several case series, for example this one published in JAMA, “Late Gadolinium Enhancement” on cardiac MRI[3] indicative of long term heart damage was found in the majority of clinical myocarditis cases which underwent detailed investigation. This finding is not consistent with mRNA-induced myocarditis having a more benign course than other forms, as was originally hoped.
For the above reasons, it is important to try to accurately capture all possible cases of myocarditis, both for the individuals concerned (so they can receive proper follow-up) and for calculating the extent of any added risks from vaccination.
In respect of the accurate detection of myocarditis cases, this study raises several important concerns relevant to the Covid injections:
Passive surveillance misses many cases.
Before this study, the rate of clinically diagnosed myocarditis / pericarditis had been previously estimated to be 16.1 cases per 100,000 in a cohort of US service members receiving smallpox vaccination, nearly 7.5-fold higher than the expected background rate of 2.16 per 100,000 observed among comparable unvaccinated service members.
The rate of clinical myocarditis observed in this SPX study was approximately 28 times higher than the previous estimate, at 463 per 100,000 – several hundred times the expected background rate. The higher incidence rate detected is almost certainly due to the active surveillance systems in place, where cases were pro-actively sought out and participants and their physicians made aware of their possibility.
As the authors state:
Prior to the present study, the incidence of myocarditis / pericarditis following smallpox vaccination was estimated from passive surveillance registries and population databases, with an inherent bias towards underestimation of disease incidence.
Myocarditis cases may be easily dismissed as musculoskeletal in origin.
Myocarditis is usually self-limiting in its acute phase, improving with self-treatment by a non-steroidal anti-inflammatory drug such as ibuprofen. It could quite easily be confused with “expected” aches and pains following injection, or with musculoskeletal injury, and this would be more frequent in the young, especially if active in sport.
The authors make the point that:
“3 of the 5 clinical cases would not have sought medical care without study interventions including enhanced education and surveillance.”
With the Covid mRNA injections, not only have we experienced a lack of active surveillance and a reliance on passive adverse event reporting, but there has been an atmosphere of discouragement of reporting. Many physicians have reported censure by hospitals or other health authorities for even discussing a possible vaccine origin for adverse events, and even subjects themselves have received opprobrium online after questioning the origin of their symptoms.
Hence, whatever factors the authors noted in 2015 in relation to underreporting of myocarditis following SPX are likely to be even more in evidence now for the Covid vaccines.
Because of this, there must be a very significant possibility that the actual numbers of clinical myocarditis cases caused by the mRNA injections have to date been very significantly underestimated.
The frequency of subclinical cases may dwarf the clinical cases.
This was actually the first study to attempt to detect possible subclinical cases of myocarditis (ie those without discernible symptoms) following vaccination. It is highly likely that, just as there is a spectrum of outcomes with symptomatic cases, such that a proportion have zero long-term problems, so with the subclinical cases an unknown proportion may well go on to have cardiac problems. Given that heart cells are irreplaceable and that scar tissue in the heart can disrupt electrical conduction the degree of concern about heart damage must be much more than with, say, damage to the skin, which can self-repair and still perform its primary function.
The actual proportion of subclinical cases which go on to manifest in cardiac disease later in life is unknown, however the authors selected a threshold for the measured troponin levels by which to define a subclinical case which is known to be associated with an increased risk of adverse outcomes. In the paper cited by the authors in support of their chosen troponin criterion it had been concluded that:
“In the general population, cTnT [troponin – protein released from heart damage] elevation is rare in subjects without CHF, LVH, CKD, or DM, [Congestive Heart Failure, Left Ventricular Hypertrophy, Chronic Kidney Disease or Diabetes Mellitus] suggesting that the upper limit of normal for the immunoassay should be <0.01 μg/L. Even minimally increased cTnT may represent subclinical cardiac injury and have important clinical implications, a hypothesis that should be tested in longitudinal outcome studies.”
*Definitions in [ ] with bold added by this author
The rate of possible subclinical myocarditis detected after SPX (3% of subjects) was 6 x the rate of symptomatic myocarditis. That these findings are or might be significant rather than chance fluctuations is supported by the fact that zero such cases were detected in the TIV cohort.
Moreover, the authors point out that even this may be an underestimate (bold added):
“While assumptions about benign troponin release from the myocardium have been made, there is a growing body of literature suggesting that even in generally healthy populations with no known cardiac disease risk, small elevations in troponin (stratified below the levels measured by the assay in this study) are associated with increased risk of all cause and cardiovascular mortality. Therefore, the rate of reported elevations in this study may actually be an underestimate of the true incidence of vaccine related subclinical myocarditis.“
There seem no reasons to suggest that possible subclinical myocarditis might not also be occurring after Covid injections, and also at higher rates than clinical cases. In fact, given the use of active surveillance for clinical cases employed in the SPX study, it is likely that the ratio between possible subclinical and reported clinical myocarditis cases for the Covid vaccines may in fact be higher than the 6-fold seen after SPX, because of the significant underreporting of clinical cases after Covid vaccines for the reasons mentioned above.
It should be stressed that little is known about the long-term prognosis of myocarditis / pericarditis, whether infective in origin or otherwise. No follow-up to the Engler et al paper (now 7 years old) measuring cardiac status in either the clinical or possible subclinical cases has been published to date.
A 2005 paper reported a well-conducted follow-up study of 67 cases detected following smallpox vaccination of 540k military personnel and found normalisation of echocardiography, ECG, and functional status (measured by ECG exercise-testing) in all subjects including those who initially had depressed cardiac function. This is encouraging, although the median follow-up period was just a few months and none were followed for more than one year after the myocarditis; hence concerns must remain regarding cardiac function in later life, especially in those in whom cardiac reserve falls secondary to other cardiac pathology such as coronary artery disease.
Concluding remarks
The authors conclude their paper with this warning:
Our study identified a rate of myocarditis/pericarditis following SPX immunization that is significantly higher than previously described, and highlights the challenges of post-licensure vaccine safety surveillance to identify adverse events that are not well understood or previously unrecognized.
Applying the incidence described in this study to a SPX immunization program that has delivered over 2 million doses, largely to young, healthy primary vaccinees, there are potentially thousands of vaccine associated cases, many undiagnosed because of self-medication or lack of provider awareness].
In our study, 3 of the 5 clinical cases would not have sought medical care without study interventions including enhanced education and surveillance. The recognition of potential adverse events following immunization requires accurate diagnosis of new onset clinical symptoms.
Our study reinforces the need, as part of all post-vaccine (and potentially new drug related) adverse events surveillance, to include specific standardized inquiry about new onset cardiac symptoms and to highlight the value of dynamic pre to post immunization cardiac troponin increases as a potential biomarker of risk in future safety surveillance studies.
Two million doses of SPX sounds a large number, but it is sobering to consider where we are today in respect of our understanding of the association of the Covid vaccines to myocarditis, having rolled out several billion doses, a program which is now continuing with 3rd or even 4th doses (whereas the incidence studies published to date have been based on 2 doses only).
It is accepted now that there is a definite association between mRNA vaccination and myocarditis, yet the precise rates of increased risks reported vary hugely between different studies, which probably reflect vastly different methodologies between investigators and countries according to prevailing local reporting standards and customs.
Moreover, initial claims that myocarditis risk might be higher after Covid infection compared to vaccination have not held up to scrutiny. The latest study – based on a large (~200k) cohort of adults in Israel – found no increase in the incidence of pericarditis or myocarditis in adult patients recovering from COVID-19.
In addition to the high, yet underreported, rates of clinical myocarditis, there remains a distinct possibility that there may have been very large numbers of subclinical myocarditis cases caused by Covid vaccines, the long-term outcomes for which are uncertain.
Approximately 3% of those receiving a single SPX vaccination met the criteria for having developed possible subclinical myocarditis, and given that billions have now received Covid mRNA products (many multiple times), if the frequency is similar to SPX the number of such cases following mRNA injections could well be in the millions.
Despite these worrying data, we have inexplicably witnessed the rollout of multiple booster doses, including in many countries to young adults and even children, despite there having been:
No active surveillance for myocarditis, only passive reporting
No prospective studies of troponin levels (which would be relatively simple to perform).
No standardised inquiries about new onset cardiac symptoms
One could be forgiven for thinking that the reason for this is that those who have relentlessly pushed this program into younger and younger people at little to no risk from Covid, simply do not want to know, and prefer to maintain a degree of “plausible deniability”.
Footnotes:
For subclinical myocarditis, the criteria for diagnosis were: the development of any one of the following: a) elevated post-vaccine levels of cTnT ≥ 0.02 ng/ml with pre-vaccine cTnT levels <0.01 ng/ml; or b) a post-vaccine cTnT level of 0.02 ng/ml greater than the pre-vaccine level based on the imprecision profiles of the assay.
The absolute subclinical cTnT elevations post SPX vaccine ranged from 0.02 to 0.24 ng/ml with the majority (n = 28, 90.3%) ranging from 0.02 to 0.07 ng/ml
This is a radiological feature seen on cardiac imaging which is indicative of myocardial damage consistent with a high risk of poor long-term prognosis.
In 2020, government orders to stay home — along with lockdown-produced job losses, public fear of COVID-19 and other factors — led to dramatic declines in in-person utilization of healthcare services among adults and children, both in the United States and globally.
“Well-baby” and “well-child” visits were some of the noteworthy casualties.
In the U.S., children’s and teen’s vaccination rates plummeted dramatically, falling that year by as much as 91% depending on the age group, including a noticeably lower uptake of diphtheria, tetanus and pertussis vaccines (DTaP or DTP), meningitis shots and human papillomavirus (HPV) vaccines.
Public health officials expected this “pandemic hangover” to dissipate by 2021, but instead, the change in parents’ vaccine-seeking behavior for their kids persisted.
Internationally, 6 million fewer children worldwide got at least one dose of DTP vaccine in 2021 versus 2019, causing the head of UNICEF to lament “the largest sustained drop in childhood immunization in a generation.”
And in the Philippines — where the president threatened to jail COVID-19 vaccine refusers — 2021’s percentage of children receiving a first DTP dose was just 57% versus 92% a decade previously.
Stateside, Washington State reported flu shot uptake in children under age 5 was down by around 25% in November 2021, compared to the two previous flu seasons. And Michigan’s state registry for March 2022 showed that 24% fewer toddlers “were considered vaccinated” compared to March 2020.
When Michigan compared its 2020 vaccination data against the 2016-2019 period, it found vaccination coverage had declined in “all milestone age cohorts, except for birth-dose hepatitis B coverage.”
At this juncture, state officials are openly speculating that COVID-19 shots — thus far rejected by the parents of 97% of under-5-year-olds — are the reason parents are increasingly ambivalent about childhood vaccination more generally.
Referring to this “spillover doubt,” a Michigander public health spokesperson said parents who once accepted childhood vaccination without question are now saying, “Wait a minute. Do I really need these vaccines?” and asking, “How are these vaccines made?”
According to another Michigan official, “vaccination” — the “V-word” — has become a “trigger word” for irate parents who believe government not only overstepped its authority during COVID-19 but is fraudulently pushing unsafe vaccines on their little ones.
Fewer babies dying is no ‘disaster’
In October 2020, three scientists from the U.S. and U.K. authored the Great Barrington Declaration and condemned — quite gloomily — the steep decline in childhood vaccination resulting from COVID-19 lockdowns.
As long-time proponents of vaccination — professionally involved in vaccine development, promotion of the dangerous HPV vaccine and accepting of COVID-19 vaccines as a solution to lockdowns — the three declaration authors positioned the decline in childhood vaccination rates at the head of their list of “disastrous” lockdown consequences.
Far from witnessing a disaster, however, observers by June 2020 had begun noticing a wonderful silver lining — a “surprising” pandemic effect on the death rate among infants, in particular, with 200-plus fewer infants dying per week, amounting to a 30% reduction in expected child deaths within a few months.
To explain the “something mysterious” saving the lives of infants, these analysts, along with Children’s Health Defense (CHD) Chief Scientific Officer Brian Hooker, pointed out how the missed infant vaccines coincided with a “precipitous drop” in reports of sudden infant death syndrome (SIDS) to the Vaccine Adverse Event Reporting System (VAERS).
SIDS deaths — which by definition affect children who are normal and healthy — and sudden unexplained deaths in children over age 1 typically occur in close temporal proximity to vaccination, with nine out of 10 SIDS deaths following two- and four-month “well-baby” visits.
An analysis of three decades of VAERS data found 75% of reported post-vaccination SIDS cases occurred within seven days of childhood shots.
Japanese pathologists who identified SIDS cases taking place within a week of vaccination agree that “suspicious cases do exist,” leading them to encourage forensic pathologists to “devote more attention to vaccination” in SIDS events.
Naturally, “fact-checkers” dispute the hypothesized association between 2020’s lower vaccination rates and the decreased deaths in young children.
Additional clues
CHD has reviewed dozens of studies showing dramatically better health in unvaccinated children while finding “no studies that show superior health outcomes in vaccinated children.”
However, because the effects of vaccination are complex, cumulative and synergistic with other toxic exposures — and because most chronic disease data sets have not yet caught up to the pandemic — it is not so easy to tease out other upsides resulting from 2020’s lower childhood vaccination rates.
There are a few clues, however.
Consider the decline in emergency department (ED) visits and the fact that the largest declines were in persons under age 15.
Ordinarily, an estimated one in seven children experiences an ED visit every year.
An analysis comparing 2020’s pediatric ED visits to ED encounters over the previous decade found “substantial” decreases for certain diagnoses — notably abdominal pain, ear infections, asthma, pneumonia, upper respiratory and urinary tract infections and trauma — while visits for diagnoses such as seizures and complications of diabetes held steadier.
Although there is no surefire way to know why ED visits declined for those specific conditions, all of the diagnoses in question show up in vaccine package inserts as post-vaccination occurrences — along with nearly 400 other acute and chronic symptoms and conditions.
Abdominal pain may not sound serious, but it can be a sign of acute pancreatitis (sudden-onset inflammation of the pancreas), so much so that clinicians advise “always” considering acute pancreatitis “in the differential diagnosis of abdominal pain in children.
And case reports are now flooding in (for example, from the U.S., Japan, Poland and New Zealand) describing severe pancreatitis in the aftermath of COVID-19 vaccination.
Moreover, acute and chronic pancreatitis began mysteriously surging in children following the childhood vaccine schedule’s expansion in the 1990s and 2000s, and juvenile diabetes and pancreatic cancers in young adults — two conditions associated with pancreatitis — began escalating soon thereafter.
COVID vaccines — a line in the sand?
Most observers attributed the sudden drop-off in routine childhood vaccination in 2020 purely to circumstance-imposed foregone care (“the gap between perceived need and actual utilization of healthcare services”).
Now, however, it is COVID-19 vaccines — and particularly the unscientific authorization of the jabs for teens and young children — that appear to be the principal reason many parents no longer “perceive a need” to rush back into the vaccine fold.
Even the propagandistic New York Timesadmitted to a hardy new contingent of vaccine “skeptics” whose questioning was forged in the crucible of COVID-19 restrictions, COVID-19 vaccine mandates and, tragically for some, a child’s adverse reaction to the COVID-19 shots.
As a physician tweeted from the “frontlines of medicine” in early August, “Parents are DONE with giving their kids any and all [syringe emoji]. Not only that but they’re disgusted with what they had already allowed to be injected into their kids. They wish they could turn back.”
Public health’s tired old strategy for recapturing these wayward parents appears to be (surprise, surprise) badgering parents to “catch up as many vaccines as possible in a single visit” — bolstered by the false claim that it is to a child’s advantage to get a bunch of shots at once — while also stoking worries about a resurgence of so-called “vaccine-preventable” illnesses.
Thus, following a single case of paralysis ascribed to “polio,” New York State is busily trying to conjure up a polio outbreak, never mentioning the decades of manipulation of the “polio” diagnosis intended to mask nonviral causes of paralysis that include vaccination and poisoning.
Florida, meanwhile, is urging college students and other groups to get meningococcal vaccines following the deaths of seven gay and bisexual men, allegedly from meningococcal disease.
Why did the deceased men develop meningitis to begin with? No one has shared information about their COVID-19 vaccination status, but researchers around the world are reporting meningitis as a post-COVID-vaccination adverse event in adolescents and adults — for example, in Japan, Singapore, Korea, Iraq, Belgium and Germany.
Meningitis also is a listed adverse event for DTaP, hepatitis A and B, influenza and MMR vaccines, and vaccines containing Haemophilus influenzae type b (Hib) and polio components.
And a 28-year-old physician who volunteered in Brazil’s clinical trials for AstraZeneca’s COVID-19 vaccine died after receiving the meningitis vaccine given to the “control group.”
What kids really need
Sadly, whatever temporary or longer-lasting silver lining may have emerged from the COVID-19-induced lull in childhood vaccination, children and their parents still face many challenges.
According to a Centers for Disease Control and Prevention study, the weight status of children and adolescents who were already overweight or obese worsened significantly during 2020, and children’s food insecurity is rising both domestically and internationally.
In addition, the massive social and behavioral changes commanded through government restrictions have prompted dire headlines about young people’s mental health — although experts caution these could counterproductively lead to overdiagnosis and overmedication with black-box-warning drugs known to cause violence and suicide.
Rather than more vaccines or drugs that have never delivered on their hype or promises, what children and youth need to thrive are the slower-but-surer public health fundamentals — such as solid nutrition, safe housing and economic security — and the loving attention of their parents.
In 2013, the CNN presenter Deborah Feyerick asked if asteroids falling to earth were caused by climate change. Earlier this year, CBS anchor Nate Burleson commented on the Tonga earthquake by saying: “We talk about climate change… these stories are a harsh reality of what we are going through. We have to do our part because these are more frequent.” Last week, the academic networking blog The Conversation discussed the Fagradalsfjall volcano eruption in Iceland and asked: “Is climate change causing more eruptions?”, adding that it had the potential to increase volcanic eruptions and affect their size.
In the climate change show, jumping the shark is now a daily occurrence, particularly in the mainstream media. Gaslighting on a global scale is evident as the media push the command-and-control Net Zero agenda. Bad weather incidents and natural disasters are catastrophised to promote this increasingly hard-left political agenda. But the distinguished atmospheric scientist Emeritus Professor Richard Lindzen of MIT recently voiced the views of an increasing number of people when he said the current climate narrative was “absurd”. Yet he acknowledged that it had universal acceptance, despite the fact that in a normal world the counter-arguments would be compelling. “Perhaps it is the trillions of dollars being diverted into every green project under the sun, and the relentless propaganda from grant-dependent academics and agenda-driven journalists, along with the political control offered to elite groups in society by Net Zero, that currently says it is not absurd,” he speculated.
The Daily Sceptic has written numerous articles presenting evidence that global warming started to run out of steam over 20 years ago, despite the frequent, back-dated and upward temperature adjustments made by state-funded weather services. No science paper exists that proves conclusively that humans cause noticeable changes in the climate by burning fossil fuel. Despite years of research, scientists are no nearer knowing how much temperatures will rise if carbon dioxide doubles in the atmosphere. No link has been shown directly connecting temperatures and CO2 rises (and falls) over the entire paleoclimatic record. Countless natural processes play a part in determining climate conditions. And attempts to link individual weather events to long-term changes in the climate are produced by climate modellers and green activists giving vent to wishful thinking.
In the absence of credible science, there has been a resort to the name-calling, shaming and appeals to authority, common in previous ages. The recent news that the Great Barrier Reef (GBR) had returned to blooming health, and was showing record growth, was a disaster for most mainstream media outlets. All parts had reported for years that the coral was on its last legs due to human-induced climate change. During this time, the GBR observer Professor Peter Ridd was vilified for stating that the reef was a vibrant and healthy ecosystem. He was fired from his post at James Cook University for pointing out the deficiencies in the output of reef science institutions.
In August 2019, the Guardian reported that the former Australian chief scientist Ian Chubb had accused Ridd of “misrepresenting robust science” about the plight of the GBR. Shamefully, it repeated without comment Chubb’s slur that Ridd was relying on the “strategy used by the tobacco industry to raise doubts about the impact of smoking”.
Professor Ridd emerges from the whole sorry affair with his reputation restored and an acknowledgement that true scientists report their findings without fear of the mob, or seeking the favour of the Establishment.
Just days before the news was confirmed that the GBR was continuing to grow back in record amounts, the Guardian ran a long article saying that scientists had demonstrated “beyond any doubt” that humanity is forcing the climate to disastrous new extremes, They hadn’t, of course, and “beyond any doubt” is a phrase borrowed from the criminal law, not science. Professor Terry Hughes from the National Coral Bleaching Taskforce estimated that close to 50% of the GBR coral is already dead. Attribution science is said to show that the hot March weather in 2016 that caused a “catastrophic die-off” in 2016 was made “at least 175 times more likely” by the human influence on the climate. A more realistic explanation, invariably ignored in mainstream media, is that the powerful El Nino experienced in that year warmed sea waters temporarily, and led to a natural burst of bleaching. Full reef health was quickly restored when the effect of the natural oscillation was removed.
The global media gaslighting over political climate change is easier to understand if you follow the money. Earlier this year, the Daily Scepticreported that the Associated Press was adding two dozen journalists to cover “climate issues”. Five billionaire foundations, including the left-wing Rockefeller operation, supplied $8 million. AP now says over 50 jobs are funded from these sources. The BBC and the Guardian regularly receive multi-million dollar contributions from the trusts of wealthy donors. It is estimated that Bill Gates has given more than $300 million over the past decade to a wide variety of media outlets. Democrat power couple James and Kathryn Murdoch also help pay the staff’s wages at AP. On their Foundation web site, it is noted that there is an investment in Climate Central, where meteorologists are used as “trusted messengers” of the links between extreme weather and climate change.
Meanwhile, the foundation of the green technology-funding Spanish bank BBVA hands out annual €100,000 payments. Last year the cash went to Marlow Hood of Agence France-Presse, who describes himself as the “Herald of the Anthropocene”, the latter being a political renaming of the current Holocene era. In 2019 Matt McGrath of the BBC took home the annual prize, while in 2020 it ended up in the coffers of the Guardian.
The White Queen tried to believe in six impossible things before breakfast. It’s a shame climate change wasn’t around in Alice’s day.
Chris Morrison is the Daily Sceptic’s Environment Editor
The CDC has dropped special quarantine recommendations for unvaccinated persons, finally admitting that natural immunity should be considered and that vaccines don’t stop infection.
“CDC’s COVID-19 prevention recommendations no longer differentiate based on a person’s vaccination status because breakthrough infections occur, though they are generally mild, and persons who have had COVID-19 but are not vaccinated have some degree of protection against severe illness from their previous infection,” their update reads.
The CDC removed the recommendation that unvaccinated persons quarantine after they’re exposed to the virus. They now recommend that individuals wear a mask for ten days post-exposure and get tested after five days.
The CDC further acknowledged that the Omicron variant of COVID poses a smaller risk of hospitalization and death than previous variants.
This announcement will likely pressure Canada’s health authorities (and Trudeau) to follow suit. Although numerous countries dropped their medical segregation policies long ago, Canada remains one of the last to do so.
Moreover, each consecutive variant appears to be weakening, with immunity (including natural immunity) being widespread. Although Canada has an abnormally high amount of mask and vaccine fanatics, the remaining medical segregation could soon be a thing of the past.
With that said, Canada’s health authorities have done nothing but warn of a return to restrictions and upcoming waves of COVID, telling Canadians that the pandemic is not over.
Additionally, the University of Toronto recently mandated that young health students living on residence get a 3rd vaccine.
A recently declassified CIA document prepared in 1983, and released on 20 January 2017, shows that the United States had at the time encouraged Saddam Hussein to attack Syria, which would have led to a vicious conflict between the two countries, thus draining their resources.
The report, which was then prepared by CIA officer Graham Fuller, indicates that the US tried adamantly to convince Saddam to attack Syria under any pretense available, in order to get the two most powerful countries in the Arab East to destroy each other, turning their attention away from the Arab-Israeli conflict. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.





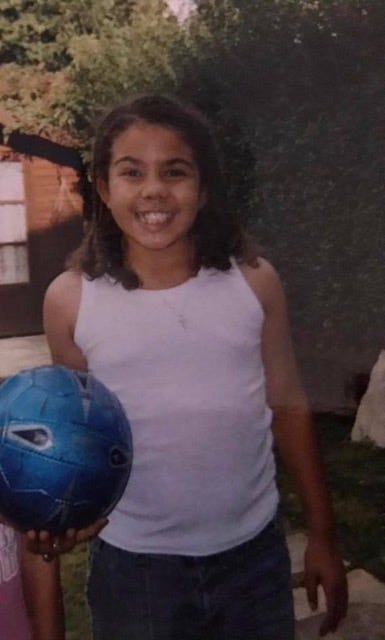

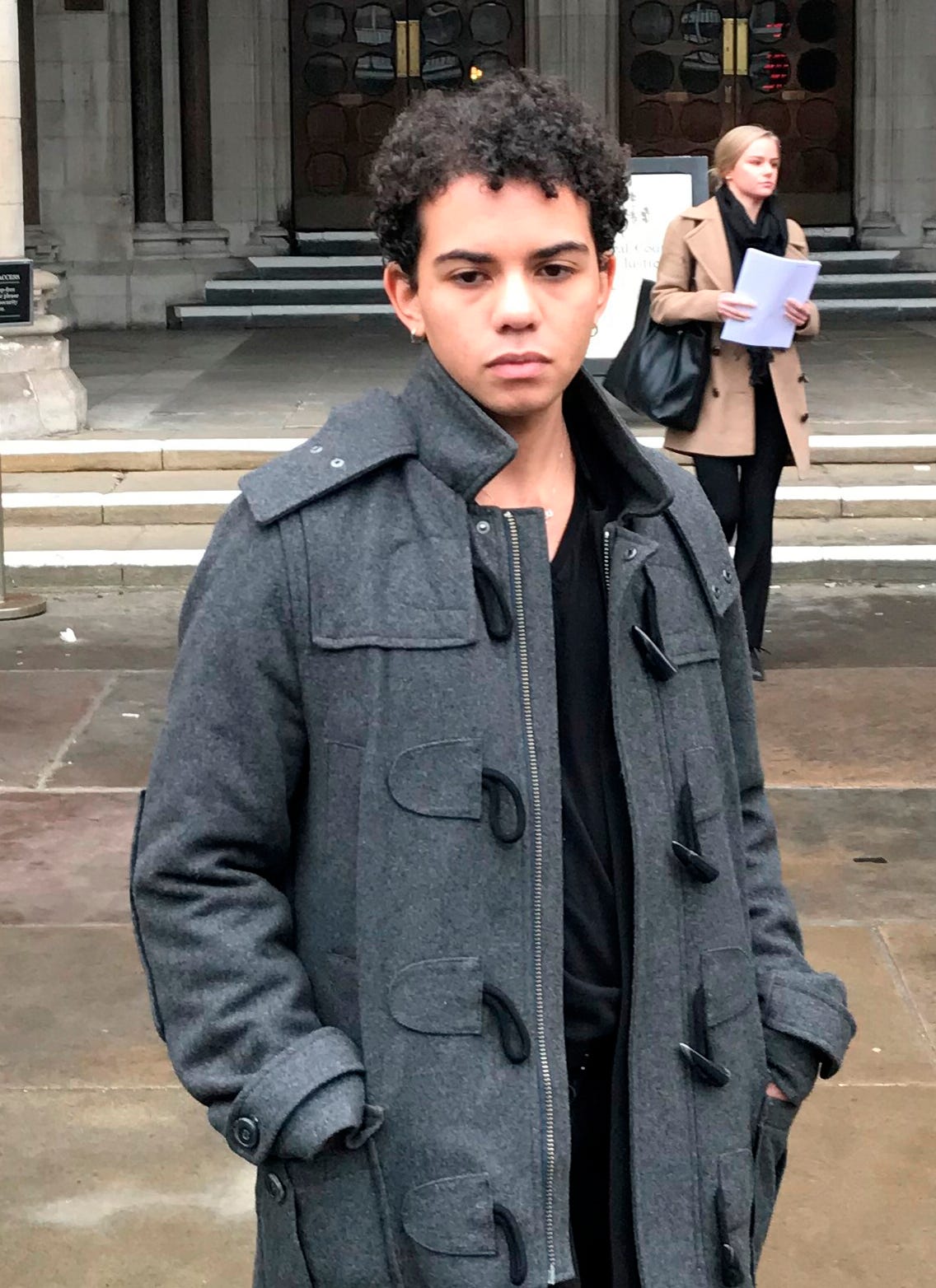




 Aletho News
Aletho News