What precisely happened in the month of February 2020, when Anthony Fauci and cohorts were plotting their pandemic response, is still a mystery. Jeremy Farrar, of the Wellcome Trust, in his book on the topic says that during these weeks, they went to burner phones, clandestine video calls, and warned family members that something terrible could happen to them.
Their top concern was the possibility of the lab leak from Wuhan. They needed to get to the bottom of it and prepare the spin. We know that the initial draft of the academic article denying the lab leak came out February 4, 2020, later published in the Lancet on March 16. But what happened in these three weeks – apart from the mid-February NIH junket to China to learn how to control a virus – remains foggy.
But this much we do know: by March 2, 2020, Fauci had his game plan lined up. Michael Gerson of the Washington Post wrote him on that day and asked about the purpose of social distancing. This was weeks before most Americans had even heard this euphemism for forced human separation. Was the idea to wait for a vaccine, Gerson asked?
Fauci answered in a private email as follows:
“Social distancing is not really geared to wait for a vaccine. The major point is to prevent easy spread of infections in schools (closing them), crowded events such as theaters, stadiums (cancel events), work places (do teleworking where possible… The goal of social distancing is to prevent a single person who is infected to readily spread to several others, which is facilitated by close contact in crowds. Close proximity of people will keep the R0 higher than 1 and even as high as 2 to 3. If we can get the R0 to less than 1, the epidemic will gradually decline and stop on its own without a vaccine.”

There we have it: the Fauci theory of how we get rid of the virus. We don’t need a vaccine. Just close things. Stay away from people. Don’t gather. Shut schools. Lock businesses and churches. All people stay away from all people. The R-naught will drop.
Then the virus will… and this is where the theory gets murky. Does it just vanish? Get bored? Get frustrated, give up, and vanish into the ether? And how long does this new social system of “social distancing” have to last? Years? Forever? And what happens once people start acting normally again?
This is very clearly crank science, one that confuses ex post data collection with causation itself and also seems to deny the workability of the human immune system. That such things would be written by a person in Fauci’s position is truly mind boggling. But the press went along, and still does after all this time.
What Fauci was imagining – and very few people picked up on it at the time – was the construction of a new social system. It was not just about this virus. It was about all pathogens and the whole functioning of society. He believed – or he decided to come to believe – that a re-engineering of the social order could successfully beat back common pathogens and bring about universal health.
He finally revealed this in his August 15, 2020, article for Cell that received very little attention at all. He was on his own attempting to implement an entire new social system based on a new ideology.
Living in greater harmony with nature will require changes in human behavior as well as other radical changes that may take decades to achieve: rebuilding the infrastructures of human existence, from cities to homes to workplaces, to water and sewer systems, to recreational and gatherings venues. In such a transformation we will need to prioritize changes in those human behaviors that constitute risks for the emergence of infectious diseases. Chief among them are reducing crowding at home, work, and in public places as well as minimizing environmental perturbations such as deforestation, intense urbanization, and intensive animal farming.
This article reveals the most important point. The pandemic response was not just about this one pathogen. It was about what amounts to a political, economic, social, and cultural revolution.
It’s not socialism or capitalism. It’s something else entirely, something very strange, like a Rousseauian technocracy, simultaneously primitive and high tech, as managed by a scientific elite, an untested dystopia worthy of the most terrifying literature in the English language.
No one has voted for such a thing. It is something Fauci and his friends dreamed up on their own and deployed all their enormous power to enact just as a test, until it fell apart. The US and many parts of the world were in their grip for the better part of a year and two years in some places.
This is a scandal for the ages, one that far outstrips issues of tax-funded gain-of-function research, as important as that is. It’s even more important than reports that Fauci has been earning personal royalty payments from pharmaceutical companies that receive grants that he has personally approved. The real problem comes down to his power and the ability of elected representatives and courts to control him for many decades.
Regardless of Fauci’s millenarian vision, the course of the virus took the usual path but for one major exception: the waves of infection occurred based on class rank in society. There was a political hierarchy of infection that started with the working classes, moved to the bourgeoisie, hit the professional classes, then high-end journalists, and finally, at the very end came for the elite ruling class itself – Trudeau, Psaki, Ardern, Gates, and finally Fauci – regardless of their multiple vaccines.
And here is why Fauci’s covid infection is significant, 28 months after the first lockdowns. It’s a sign and symbol that his entire theory of virus control was wrong. He got his way with policy and it did not work. The virus finally landed on him, as if to reenact Edgar Allan Poe’s fictional story of Prince Prospero in his castle that he believed would protect him.
And as a result of his exposure, Fauci will surely (unless his repeated injection of the same vaccine harmed the operation of his immune system) gain the natural immunity that is already possessed by 78 percent of kids and likely two thirds of the general population.
It should also alert us to three points of moral urgency:
- We need to replace Fauci-style feudalism with a new theory of how to reconcile the freely functioning society with the presence of infectious disease, so that neither he nor people in his pay or sway can attempt this again.
- We need to act to disable the unmitigated power of administrative-state bureaucrats to seize control of the machinery of government.
- We need a new system to decentralize science away from privileged elites so that they can never again have monopoly control over what is considered to be the science much less posses the power to censor dissent.
These are the lessons, at least the start of them. This virus is either endemic or at least almost so, but we are left with astonishing social, cultural, and economic destruction from Fauci’s attempt to implement an experimental plan on the whole population not only in the US but all over the world.
We will suffer for many years or generations from it. And yet, in the end, infection is individual and probably unavoidable for most people. The immune system adapts. That’s how we evolved to coexist. To pretend otherwise is the very essence of denying the science.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
June 17, 2022
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Malthusian Ideology, Phony Scarcity, Science and Pseudo-Science, Timeless or most popular | Covid-19, Human rights, United States |
Leave a comment
Presidents, senior leadership and trustees can’t say they didn’t know.
No College Mandates has launched a major letter campaign to put colleges on notice that continued Covid-19 vaccination mandates put their students, their reputations, and potentially their endowments at risk. The purpose of the letter is to make these policy makers aware of new information they likely did not know existed and to prompt them to further investigate.
To date, more than 60 college presidents have received this letter via certified mail. Across those 60 colleges, approximately 1400 individuals were copied. Many more college letters are in process. By the time we are finished, thousands of college administrators and trustees will be notified.
No College Mandates is so proud to have the following organizations as signatories on our letter: Health Freedom Defense Fund, The Mendenhall Law Group, Health Freedom Counsel, and The Unity Project.
The letter is below. If you are interested in working on this effort, email us at info@nocollegemandates.com. We’ll set you up to fight this fight with us and make change.
To College and University Presidents, Senior Leadership and Trustees:
We are writing to notify you of recently available information prompting concern that fraud has been committed by Pfizer and by the FDA in the development and continued distribution of Pfizer’s Covid-19 vaccine. Given that your institution mandates Covid-19 vaccination for students as a condition of enrollment, it is incumbent upon you to be fully informed about the safety and efficacy of these vaccines and the claims of fraud that call both into question.
If fraud or willful misconduct is proven, the manufacturers and those involved in the distribution or mandating of the vaccines will lose immunity from liability granted to them under the existing EUA and the PREP act.
We urge you to further investigate. We believe that once you do, you will see how continued Covid-19 vaccine mandates jeopardize the safety of your students and the reputation of your institution.
The new information consists of Pfizer’s biological product file used to obtain FDA approval of Comirnaty and data from the insurance industry showing a huge rise in excess deaths in Millennial and Gen X populations concurrent with the implementation of vaccine approvals and mandates. The excess death data is raising concerns in the insurance industry and on Wall Street. We are also including timely news about product safety, given the FDA’s recent restriction of the Johnson & Johnson vaccine due to blood clotting concerns.
Following is a brief overview of each category and starting points for further inquiry. We are standing by to provide you with additional information or to connect you to scientists, lawyers and investors who are reviewing the current and evolving data.
Pfizer Biological Product File – background and highlights:
The Public Health and Medical Professionals for Transparency (PHMPT) is a nonprofit group made up of public health professionals, medical professionals, scientists, and journalists. The group exists solely to obtain and disseminate the data relied upon by the FDA to license Covid-19 vaccines. Four days after the Pfizer Covid-19 vaccine was approved for children over 16, this group submitted a Freedom of Information Act for all data within Pfizer’s Covid-19 vaccine biological product file. When the FDA asked for 75 years to release that data, PHMPT sued to obtain it and won. Beginning in March 2022, the public has access to Pfizer’s clinical trial data, which is being downloaded in batches monthly. You can find the document releases to-date here.
Thousands of volunteers including scientists, statisticians, doctors, and lawyers continue to examine these downloads and publish their findings. For ready reference, below are just a few of the findings of greatest concern that call into question the safety and efficacy of the Pfizer product and support a thesis of fraud:
- Pfizer failed the all-cause mortality endpoint in their unprecedentedly short 28-day clinical trial. In brief, more people died in the vaccinated group than in the placebo group. This was known yet has still not been widely disclosed to the public.
- The CDC talking point that vaccines stopped transmission was based on no data, as this metric was not evaluated during Pfizer’s clinical trials. Pfizer and the FDA knew this yet did not disclose it to the public.
- Pfizer and the FDA knew as early as November 2020 that Pfizer’s clinical trials showed:
- Vaccine failure
- Waning vaccine efficacy
A baseline condition for granting a product Emergency Use Authorization is that it must be safe and effective. The data showed that the products are not effective. Yet, based on FDA approval, the CDC promoted them as such. From the initial roll-out in December 2020 through April 1, 2021, the public health messaging was that if you received the shot, you could not get infected and could not transmit the virus. The Pfizer documents are proof that they and the FDA colluded to lie to the American people and the CDC created false public health narratives based on these lies.
- Pfizer and the FDA most likely knew in May 2021 that the vaccines caused heart damage in teenagers based on a paper that was already in peer review at that time. The FDA approved the product for teenagers in June 2021 yet did not disclose this risk factor to consumers until August. During that time, all those who received this product did not have informed consent. Parents were not made aware of this known potential risk to their children.
- Brook Jackson, a regional director employed by Pfizer sub-contractor Ventavia Research Group, came forward in September 2020 with documented evidence that the company falsified data, unblinded patients and was slow to follow up on adverse events reported in Pfizer’s pivotal phase III trial conducted by Ventavia. Her findings call into question the integrity of not only Ventavia’s results but of all of the results from Pfizer’s other trial sites and the entire clinical trial. Further information is available in The British Medical Journal.
Excess death data and the insurance industry:
In December 2021, Midwest insurer One America CEO Scott Davidson disclosed a 40% increase in excess deaths over pre-pandemic levels in the working-age (18-64) population in the third quarter. Putting the number into context Davidson said, “The data is consistent across every player in this business . . . Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be a 10 percent increase over pre-pandemic. So 40 percent is just unheard of”. Other major insurers have subsequently reported increases in death claims ranging from 21–57 % over expected levels. Most of these deaths are not Covid-19 deaths. Long-term disability claims are also seeing an uptick.
These reports prompted a former institutional investor who was a #1 ranked Wall Street sell-side insurance analyst to confirm the numbers using CDC reported data. His findings, independently confirmed by others, show the spikes in excess deaths are related to the timing of vaccine approvals and mandates. This data is prompting concern at insurance and reinsurance companies, who will bear the financial brunt of this unexpected and unprecedented rise in mortality. It is raising questions about the safety of the Covid-19 vaccines in the investment community and beyond.
Of related interest is Pfizer’s amendment in February of its business risk disclosures in its Q4 2021 earnings report. The changes from the Q3 2021 report language center around disclosures of unfavorable safety data and “further information regarding the quality of pre-clinical, clinical or safety data, including by audit or inspection”.
It is likely that neither Pfizer nor the FDA anticipated the court-compelled release of their clinical trial and post-marketing surveillance data and the subsequent public scrutiny of it.
Additional product safety concerns:
The FDA announced on May 5 that they were restricting use of the Johnson & Johnson Covid-19 vaccine due to the risk of thrombosis with thrombocytopenia syndrome (TTS), a syndrome of rare and potentially life-threatening blood clots in combination with low levels of blood platelets. The decision to restrict was based on 60 reported cases and 9 fatalities. The Pfizer and Moderna vaccines also have serious risks and fatalities associated with them including but not limited to blood clots and myocarditis in college-aged populations. These are shown in Pfizer’s post-marketing surveillance data and in the CDC’s Vaccine Adverse Event Recording System (VAERS). As of April 29, 2022, there were approximately 1.2 million reports of adverse events following Covid-19 vaccination including more than 18,056 reports of deaths following the Pfizer vaccine, and 7,223 following the Moderna vaccine. Logic demands that Pfizer and Moderna products be restricted immediately as well. Why have they not been? Further, a recent Danish review of all three products in preprint in The Lancet showed that the J&J reduced all-cause mortality but that Pfizer and Moderna did not and may have increased it. Given all this, it is reasonable to think that Pfizer and Moderna products could be restricted or discontinued very soon due to safety concerns. This might well trigger a much higher level of scrutiny of the now-publicly available Pfizer data and the actions of our public health institutions. How would such a situation impact institutions such as yours that continue to mandate the products while knowing such risks exist?
One last thing to consider is the nature and associated secrecy of the contracts that Pfizer forced upon governments as conditions of sale and distribution of their Covid-19 vaccines in their respective countries. A review of some of these contracts can be found here. Terms included such things as the waiving of sovereign immunity, countries assuming full liability in the event that Pfizer was shown to have used another entity’s intellectual property, and that Pfizer be held harmless in the event of injury or death from the products. Why would a company require such terms if it knew its conduct and its products were sound?
We sincerely hope this information has been useful and that you will investigate this matter fully. We urge you to end your vaccine mandates to protect your institution’s students, reputation, and, in the event that fraud is proven, potentially your endowment.
Yours truly,
No College Mandates is a coalition of thousands of concerned students, parents, professors, staff, and community members working to end college Covid-19 vaccination mandates and restore medical choice on college campuses. Contact us at info@nocollegemandates.com
Health Freedom Defense Fund is a 501(c)(3) non-profit which seeks to protect and advance health freedom, educate Americans on informed consent, advocate for human rights and bodily autonomy for all people, and legally challenge unethical mandates, laws, and policies when necessary. (HealthFreedomDefense.org)
The Mendenhall Law Group is a mission-oriented practice focused on holding government, educational institutions and corporations accountable. The group is keenly interested in medical freedom and provides legal support for those concerned about Covid-19 mandates and policies. Mendenhall Law has offices in Ohio and Massachusetts and a national network of affiliated practices. (WarnerMendenhall.com)
Health Freedom Counsel believes in the right to medical choice and provides clients with the resources to stand up to mandates that infringe upon medical freedom. (HealthFreedomCounsel.com)
The Unity Project is a non-profit organization dedicated to fighting the Covid-19 Vaccine Mandate for students, kindergarten through 12th grade. We have enlisted globally esteemed physicians, scientists and business leaders and more than 150 grassroots groups and concerned individuals focused on preserving medical freedom.
June 17, 2022
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science, Solidarity and Activism | Human rights, United States |
Leave a comment
There are more than a dozen “smoking guns” that indicate that the Pfizer Phase 3 trial was not properly conducted

It is in the best interest of all parties to have transparency in these issues in order to restore public trust in the medical community and reduce vaccine hesitancy which are key goals of the CDC and FDA.
For example, Dr. Peter Marks recently stated:
“We do have a problem with vaccine uptake that is very serious in the United States and anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do,” said Dr. Peter Marks, director of the Center for Biologics Evaluation and Research.
There are two things Dr. Marks can do to achieve his goal:
- He can have an open discussion with the people who he alleges are the main spreaders of “misinformation.”
- He can open an official FDA investigation into allegations of fraud in the Pfizer trial and produce a written report responding to each allegation.
Dr. Marks, like every other public health official, will not do #1. I understand why he won’t: the data isn’t supportive of the government narrative so he’d lose the debate very badly. This is why nobody at the FDA, CDC, or NIH will talk to any of my colleagues. In ignoring us, he is acting in a way inconsistent with what is expected which was outlined by UCSF Professor Vinay Prasad in this op-ed published 2 years ago, Scientists who express different views on Covid-19 should be heard, not demonized
But #2 is critically important. If there is fraud/ willful misconduct, the liability protection is removed. If the FDA is truly working for the people, these allegations must be investigated.
In order to help facilitate option #2, I personally am aware of over a dozen fraud allegations that should be investigated. This is not a complete list. There are dozens of articles like this one that highlight irregularities in the data that need to be investigated.
My suggestion is that, in addition to the allegations in this article, the FDA should solicit a list of irregularities via an open public process to ensure that all of the key allegations are considered and investigated in order to restore trust in the system. Why would they not want to do that?
Here is only a partial list:
- Pfizer admitted in a US court proceeding that there was fraud and the FDA knew about it. An admission in a court like this of fraud is surely grounds for an investigation. Watch this 2 minute video where attorney Robert Barnes describes what happened in his federal court case against Pfizer. Read this article for more: Pfizer admits to COVID vaccine clinical trial fraud in federal court.
- 13-year old Maddie de Garay developed paralysis less than 24 hours after she was vaccinated. I know Maddie. I know her parents. Today, Maddie is confined to a wheelchair. She was perfectly healthy before she received the vaccine. Less than 24 hours after her second dose, she couldn’t walk off the school bus. Why were her symptoms reported to the FDA in the 12-15 trial results as “functional abdominal pain”? See FDA Buries Data on Seriously Injured Child in Pfizer’s Covid-19 Clinical Trial. I notified acting FDA Commissioner Janet Woodcock on Friday, June 25, 2021 6:21 AM. She promised me the FDA would investigate the fraud. To this day (Jun 14, 2022), the family was never contacted by anyone. I know the FDA is busy, but why has nobody reached out in the year since Commissioner Woodcock promised to investigate? If one child out of 1,000 ends up paralyzed for life, shouldn’t this be something the FDA should be concerned about?
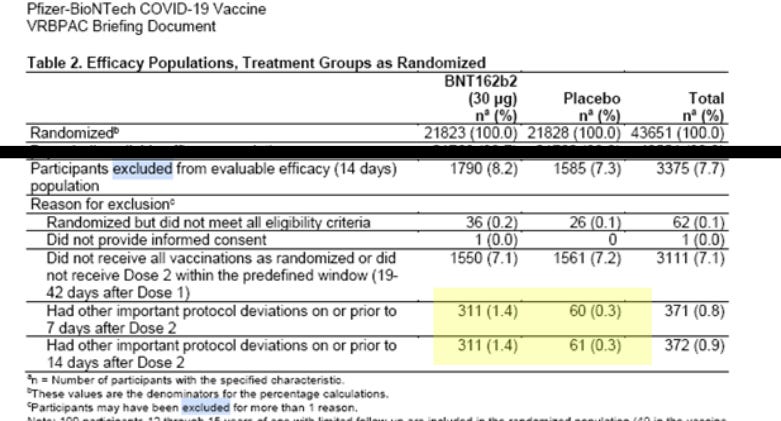
- There were 5 times as many exclusions in the treatment arm as in the placebo arm of the trial. It is statistically impossible for such an imbalanced number of exclusions to have happened by chance. It appears to be a deliberate culling of patients with adverse events which is not allowed. If it wasn’t a deliberate culling, then how do you explain such large numbers? The amount of the discrepancy is greater than the entire effect size of the trial. This is from page 18 of the December 10, 2020 VRBPAC meeting document:

- Why were the allegations of data integrity documented by the BMJ never investigated by the FDA? This is published in a major medical journal yet there was no follow up from the FDA at all. I just talked to Brook Jackson on the phone. She now has 20 lawyers on his whistleblower case. Pfizer was able to get the judge in her case to stay discovery for 6 months so an FDA investigation is the only way to compel discovery. I asked her if anyone at the FDA ever contacted her about her allegations and she said nobody ever called to talk to her. Instead, on the very same day that she emailed the FDA about what happened, she was fired. She emailed the FDA about the issues at 9am on September 25, 2020 and she was fired from her job at Ventavia at 3pm. This suggests that the FDA tipped off Pfizer who notified Ventavia. There was no other way Pfizer could have known: Brook only contacted the FDA. Period. The FDA needs to find out who at that FDA tipped off Pfizer, and then who at Pfizer told Ventavia to fire Brook instead of investigating the allegations. There has to be a chain of custody here. We deserve to know what actions the FDA is going to take against that employee who notified Pfizer. Or to notify the public that this is the proper behavior by FDA employees receiving whistleblower complaints is to take actions to get the whistleblower fired. We need to understand how the leadership of the FDA feels about what happened and whether they intend to get to the bottom of it or simply ignore it.

BMJ article documenting irregularities in the Pfizer trial. The whistleblower was fired 6 hours after notifying the FDA which must have leaked the information for Pfizer.
- Why are there more deaths in the trial report than the document Pfizer submitted to the FDA? Shouldn’t they be the same since they are reporting on the same Pfizer study? Here is another article questioning the numbers.
- There were more deaths in the treatment arm than in the placebo arm. How does the FDA know for certain that the people who died in the treatment arm did not die as a result of the drug? Did they ever look at the data from Pfizer on this? If so, what convinced them the deaths were not related? Can we see the written report which certified this? Pfizer says the deaths were unrelated, but we are never told how they determined this. Were the same tests done as Dr. Walter Lang did (see this video and also this article) and that Dr. Bhakdi and Dr. Burkhardt did? Dr. Peter Schirmacher also discovered that at least 30% to 40% of the deaths shortly after vaccination were likely caused by the vaccine. Schirmacher’s family’s life was then threatened if Schirmacher said anything more publicly. Did Pfizer use the same methodology as Dr. Schirmacher, Bhakdi, Burkhardt, and Lang? Why did Schirmacher, Bhakdi, Burkhart, and Lang all find a huge rate of causality but Pfizer found nothing. They cannot both be right. How will the FDA resolve the discrepancy and assure the public they found the truth?
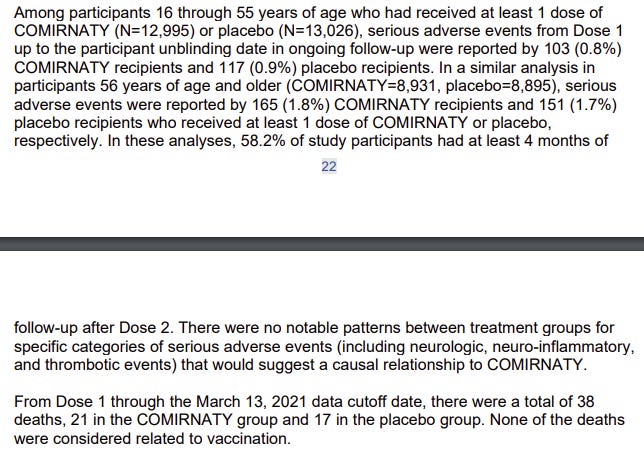
- A report Pfizer filed with the FDA entitled “Summary Basis for Regulatory Action” contains the following statements which are in conflict with data in the VAERS system which is reporting unprecedented increases in adverse events. There are more adverse and serious adverse events reported for the COVID vaccines than for all vaccines combined over the past 32 years. Therefore, the VAERS data and this report simply cannot both be true. The FDA needs to find out which is giving inaccurate data and correct the problem:

- Mysterious blood clots are only being found in vaccinated cadavers and have never been investigated by the CDC or FDA. Why are these blood clots only happening in vaccinated people if the vaccines are safe and effective? See also this article: EXCLUSIVE: Shocking microscopy photos of blood clots extracted from those who “suddenly died” – crystalline structures, nanowires, chalky particles and fibrous structures. Will someone at the FDA provide public assurances that they have investigated these clots and can explain them?
- If the vaccines are safe as represented then why does the blood of vaccinated patients look dramatically different under a darkfield microscope?
- If the vaccines worked as in the trials, how can double-masked, quadruply vaccinated Tony Fauci get COVID?
- The Pfizer data shows nobody became disabled, yet we had 1.8M people added to the disability system after the vaccines rolled out. If the trial data is correct, how did this happen? The trial was large enough to detect a signal this large, so how could it have gone undetected?
- The documents released by Pfizer show a large number of discrepancies that are impossible to explain if the trial was executed as stated. Can you investigate all the discrepancies pointed out in articles such as this and this?
- Brook Jackson’s whistleblower suit against Pfizer has not been dismissed by the court.
- The story of patient Augusto Roux needs to be thoroughly investigated. Please see Is Subject #12312982 the Key to Proving Pfizer Vaccine Trial Fraud?
- Why is Sudden Adult Death Syndrome only affecting people who have been vaccinated with the COVID vaccines? Is there a counter-example?
- Why are athletes dying at 22X the normal rate? And why is this only happening after the vaccines rolled out?
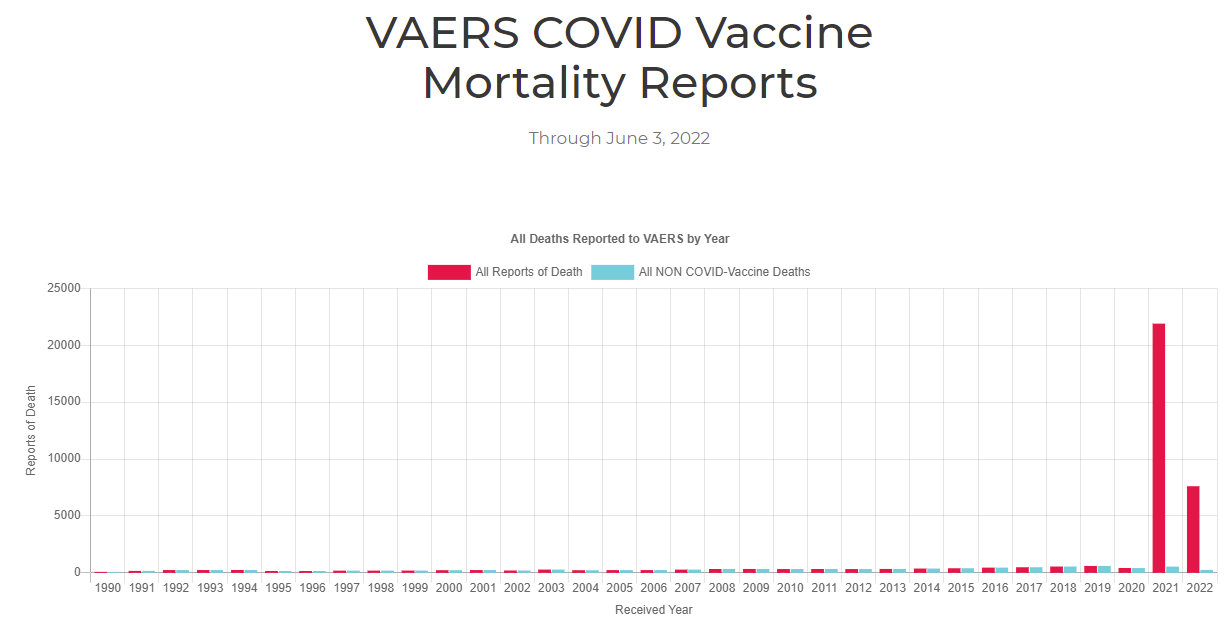
- Why are there more deaths reported associated with the COVID vaccines in VAERS than for all vaccines combined in the 32 year history of the VAERS system? It isn’t over-reporting because the deaths for all other vaccines for all years is still completely normal as you can see from this chart:

Mortality chart from OpenVAERS shows that the death reports are elevated only for the COVID vaccines and not for any other vaccines in the entire history of the VAERS system
- Shouldn’t the FDA and CDC call for a protective order to prevent retribution by state medical boards against physicians who are reporting adverse events and death following vaccination on social media? Clearly, the CDC and FDA are extremely safety conscious and would want to know about these incidents? So why not make a statement encouraging licensed MDs to speak out?
- Why are there so few autopsies? And why are the detailed autopsies showing causality ignored? And why is the CDC not warning people about the risk of death?
- Why is the public not permitted to see the assessments made of the 13,225 US deaths reported in the VAERS system that were determined to be not linked to the COVID vaccines?
- Nearly 500 articles in the peer-reviewed medical literature have been written about vaccine adverse events from the mRNA vaccines. That isn’t consistent with a vaccine found to have fewer adverse events than the placebo. Someone is lying. Is it hundreds of authors of peer-reviewed papers? Or was the study flawed? The FDA should investigate this because this needs to be resolved ASAP.
- Dr. John Su at the CDC appears to be a co-conspirator with Pfizer to hide the safety data. Whenever he presents, he never mentions that the VAERS data should be multiplied by the appropriate under-reporting factor (URF). This allows the vaccines to look 100 times safer than they actually are. He knows he shouldn’t be doing this, but this hasn’t inhibited his actions at all. The FDA and CDC refuse to acknowledge what the VAERS URF is for these vaccines and they stonewall newspaper reporters who ask about it. How is that being transparent?
- Anecdotal data from physicians. There is simply too much anecdotal data from formerly pro-vax physicians who report patients who are previously healthy become “unhealthy” (new disease, existing disease reoccurs, or cognitive decline, or menstrual issues) shortly after being vaccinated. How can that be if the rates are the same before and after the vaccine?
June 17, 2022
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, United States |
Leave a comment
MSN quickly removes article along with the study itself

I am back after a disruptive week, flight cancelled, tech stolen etc.
The bonus about having limited access to the internet is that by the time I started to write about a news article I was reading, it had been removed. Normally I wouldn’t have noticed but my sporadic typing meant going back and forth to the article over a number of days.
I was going to write about the study in the article but instead I will preserve the original article itself which was published on MSN.com
*UPDATE – As I type the actual study has been removed as well*
Severe COVID-19 ‘Rare’ In Unvaccinated People, Survey Reveals
A survey has found that people who did not get the vaccine had a lower rate of suffering severe COVID-19 amid the pandemic.
The survey uploaded to the preprint server ResearchGate presented data from more than 18,500 respondents from the “Control Group” project with more than 300,000 overall participants. An analysis revealed that compared to those who got jabbed, unvaccinated people reported fewer hospitalizations.
The international survey also found that the unvaccinated people from more than 175 countries were more likely to self-care to prevent and manage COVID-19 infection. They used natural products like vitamin D, vitamin C, zinc, quercetin, and drugs, such as ivermectin and hydroxychloroquine.
Many participants experienced discrimination for refusing the administration of “genetic vaccines” and struggled with mental health burdens due to the stigma in the mostly “vaccinated” society.
The participants admitted to avoiding vaccines due to their preference for natural medicine interventions and skepticism of pharmaceutical interventions. They also voiced distrust of government information and fear of the possible adverse effects of the vaccines in the long run.
The survey was conducted from September 2021 through February 2022. During the period, participants experienced mild to moderate COVID-19 infection and were infrequently hospitalized.
A number of female participants suffered menstrual and bleeding abnormalities, prompting the researchers who analyzed the data to surmise that the issues might have been caused by spike protein exposure and shedding, as per The Epoch Times.
Data collected from the survey were analyzed and interpreted by an independent, international team of scientists led by Robert Verkerk, Ph.D., the founder and executive and scientific director of Alliance for Natural Health International.
The link to the original article is here but as you can see this just diverts back to the home page.
Wayback Machine seems to be empty but fortunately Google has cached it for now.
The study itself can be read on ResearchGate. (Update – this has now been removed). However, this one is still available on the Wayback Machine.
It used data from a UK citizen-led cooperative called the Control Group Cooperative (CGC). This was formed in July 2021 “to represent the interests of individuals and families around the world who have chosen to not receive COVID-19 ‘vaccine’. Among the aims of the CGC is to evaluate long-term health outcomes among the COVID-19 vaccine-free, as well as linking its members to country support networks and online community groups. Participants who join the ‘control group’ may obtain an ID card (Fig. 1), in the relevant language. The card includes the statement that the individual is part of a SARS-CoV-2 Control Group and “must not be vaccinated”. Many members have reported that these ID cards have been successful in allowing travel, preventing forced vaccination (vaccination without informed consent) or avoiding the loss of liberties, such as access to venues otherwise limited to COVID-19-vaccinated individuals.”
There were around 300,000 members of the CGC which were predominantly from Europe (40.2%) with 25% from North America and 27% from Oceania. Approximately 18,500 were part of the survey on which the study was based.
The study was independent to the CGC and looked at the first five months of survey data. By using data from this group there is an obvious bias but interesting to see the results nevertheless.
Findings included the fact that the unvaccinated did not place a disproportionate burden on health systems. In fact only 0.4% of the cohort were hospitalised with COVID-19 which compared with 0.6% for the US population as a whole.
Reasons for individuals not wanting to be vaccinated was an almost equal five way split between preferring natural medication (16.8%), distrust of pharmaceutical intervention (16.4%), distrust of government information (16.4%), poor/limited trial study data (16.3%) and fear of long-term adverse reactions (15.4%).
Almost 75% of respondents, who had COVID-19, engaged in self-care using vitamins (such as D and C), minerals (zinc), quercetin, as well as ivermectin and hydroxychloroquine. The amount of people using dietary supplements was highest in the USA with 71% of respondents but still relatively high at 60-65% in the rest of the Western world.
A surprising finding was that there were common reports of menstrual disturbances and bleeding abnormalities in the unvaccinated female cohort. The authors suggest a number of reasons this may have occurred, including: COVID-19, pandemic lifestyle changes, shedding exposure or chronic stress.
Around 40% of respondents reported mental health problems due to the psychological stress of the pandemic. It is suggested that “the mental health burden may be associated more to the human response to the pandemic, rather than psychological, fear-based reactions to any threat posed by the SARS-CoV-2 virus itself. This includes discrimination in the workplace, by peers or by family members, as well as victimisation by states (governments/health authorities) owing to ‘unvaccinated’ status.
Much of this disproportionate and discriminatory treatment is likely the result of widespread misunderstandings about, and over-stated benefits of, COVID-19 ‘vaccines’, false claims over societal risks posed by the unvaccinated, media and state propaganda and coercion to ensure high rates of COVID-19 vaccination, institutional mandates, and the desire for in-group identity as explained by social identity theory (Scheepers and Derks, 2016).”
As I said above, the study is clearly biased. However, there is some interesting data to look at (which public health authorities have largely hidden or not collected) and so this study should not be disappeared. It should remain to be dissected and analysed and if others decide the findings are nonsense, it is for them to argue the reasons why.
June 17, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
Investigative Journalist with a popular Substack, Igor Chudov, explains his recent discoveries comparing the dramatic difference in Covid-19 death rates in both Portugal and South Africa, and what could be the cause.
Immune Dysfunction Expert, James Neuenschwander, joins Del to talk about the critical effect lockdowns and masking has had on our immune systems, particularly those of young people. Is there a direct link between the lack of exposure to germs and viruses in recent years and the current spike in deadly outbreaks of hepatitis and RSV?
June 17, 2022
Posted by aletho |
Science and Pseudo-Science, Video | Covid-19, COVID-19 Vaccine |
Leave a comment
The state government of Florida is standing up against the effort to indiscriminately inject experimental coronavirus “vaccine” shots into children four years old and younger. And, as reported Wednesday by Christopher O’Donnell and Ian Hodgson at the Tampa Bay Times, Florida is the only state to make this decision, every other state government having pre-ordered the shots from the United States government in anticipation of the granting of US regulatory approval.
Good for Florida. It is making the right choice in refusing to be a pusher for these shots promoted relentlessly by a collaboration of big business, big media, and big government.
In May of last year I wrote about the need for state and local governments to refuse to participate in the then new rollout of experimental coronavirus shots to 12 to 15 years old children. I concluded my comments on the matter with the following statement after addressing dangers of the shots and the very minimal risk coronavirus tends to pose for children:
It is one thing to stand aside as parents choose to have their children injected with experimental shots that carry significant known health risks and unknown potential negative consequences. It is another to actively encourage the giving of such shots through participating in their promotion and distribution. At some point, shouldn’t state and local governments admit that the risk and rewards related to shots are so out of whack that their taking part in pushing the shot-giving is a clear menace? Being presented with the opportunity to give experimental coronavirus vaccine shots to 12 to 15 years old children seems like a good time to declare ‘no more.’
A statement from the Florida Department of Health, reprinted at Fox 13 TV of Tampa Bay, makes clear that the state government’s decision not to preorder the shots was its way of saying “no more” based on the state having come to its own independent decision that the shots are not the safe and effective wonder for all young children that many people in government and the media proclaim them to be. Here is that statement from the Florida Department of Health:
The Florida Department of Health (Department) has made it clear to the federal government that states do not need to be involved in the convoluted vaccine distribution process, especially when the federal government has a track record of developing inconsistent and unsustainable COVID-19 policies.
It is also no surprise we chose not to participate in the distribution of the COVID-19 vaccine when the Department does not recommend it for all children. Doctors can order vaccines if they are in need, and there are currently no orders in the department’s ordering system for the COVID-19 vaccine for this age group.
The local television news report also provided these cogent comments regarding the decision from Joseph Ladapo, the state’s surgeon general:
‘We expect to have good data that the benefits outweigh the risks of any therapies or treatments before we recommend those therapies or treatments to Floridians. That is not going to change. I don’t think that is particularly radical. I think it’s very sensible,’ said Ladapo. ‘From what I have seen, there is just insufficient data to inform benefits and risk in children. I think that’s very unequivocal.’
Bravo to Florida and its surgeon general, about whom I wrote positively upon his appointment to the position in September.
Hopefully, we will see more state and local governments looking critically at the new shady approval of experimental coronavirus shots for young children and declaring their refusal to participate as well.
Copyright © 2022 by RonPaul Institute
June 16, 2022
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, Florida, Joseph Ladapo, United States |
Leave a comment

On June 8th 2022, I sent the following email to several reporters and one editor at al.com, which is the largest news organisation in my state of Alabama. I encourage other Daily Sceptic readers to send the same type of email to the major news organisations in their cities or states.
I don’t expect this news organisation to follow-up on my story suggestions and answer any of my questions, although I would be happy to be proven wrong. My main purpose is to create a record that shows that these reporters and editors are aware of many data points which strongly suggest that Covid vaccines are not ‘safe and effective’ (or necessary for children), and confirm that these ‘watchdog’ journalists will not share these types of stories with their readers. Nor will they pursue their own investigations that might corroborate (or impeach) these findings.
If enough readers participate in this similar experiment, this collective evidence (and the non-responses to our ‘story suggestions’) might provide strong evidence that the mainstream media are conspiring (or at least capitulating) in the cover-up of information that would debunk or challenge many elements of the alleged ‘settled science’ about Covid vaccines. In the opinion of this correspondent, such a finding – suggesting an obvious bias and censorship – would itself constitute an alarming and disturbing scandal.
Note: Story links and excerpts (several from the Daily Sceptic) are provided below this post.
Dear [journalists who routinely write Covid stories and an editor]:
I write to bring to your attention six articles that strongly suggest that Covid vaccines are not “safe and effective” nor necessary for many people. See story links below.
My real purpose in writing is to encourage al.com to do its own reporting to see if your reporters can confirm that the trends depicted in this quantifiable data are, perhaps, also being seen in Alabama.
Specifically:
- Are Alabama ambulance companies responding to more calls from individuals suffering health emergencies related to cardiac events than they did prior to widespread Covid vaccination?
- Are life insurance companies doing business in Alabama reporting more excess deaths in policy holders since vaccines became widespread, especially in the ages 18 to 64? What are these numbers?
- Are funeral homes in Alabama performing more funerals and cremations compared to time periods before Covid vaccines had been widely administered?
- Are doctors seeing more complications in vaccinated patients?
- Do vaccinated Alabamians now comprise the greatest percentage of PCR-confirmed Covid cases? Are the percentage of vaccinated patients being treated in hospitals now higher than the unvaccinated cohort (as appears to be the case in the U.K., whose data are much more comprehensive and transparent)? Are the percentages of deaths in older age groups (60 plus) now higher among the vaccinated class (as is also the case in the U.K. and other countries)?
- How many Alabama children under the age of 18 without serious pre-existing medical conditions have died from Covid in the past 27 months (this would be the mortality figure for ‘healthy’ children)? How many healthy Alabama children died from Covid in the first 12 months of the pandemic? Is death from Covid actually one of the ‘top eight’ or ‘top 10 causes of death of Alabama children in a given year (as has been quoted by public health officials and officials at pediatrician groups)? What are the top 10 annual killers of Alabama children with the number of annual deaths per year?
- If I wrote a 1,000-word article, listing several of the ‘accepted Covid narratives’ that I believe are false or dubious and why I believe they are, would you publish this piece?
I’ve come to believe that journalism or independent investigations that would challenge key parts of the ‘Covid narrative’ is not allowed at mainstream news organisations. Can you provide examples from your own reporting that would debunk or refute this theory? Is al.com going to follow up on these articles with your own reporting? If not, why not? Have reporters been told that certain Covid stories cannot be reported? Which al.com journalists have written any story that challenges or questions key parts of the CDC’s ‘settled science’?
Thank you for your consideration.
Bill Rice, Jr.
Supporting link and excerpts:
“Stop All Covid Vaccine Booster Programmes Now For Safety Reasons, Says Heart Surgeon in Virology Journal“:
Virology Journal has published a letter from a cardiovascular surgeon, Kenji Yamamoto, setting out the case for ceasing all Covid vaccine booster programmes on safety grounds, calling Covid vaccines a “major risk factor for infections in critically ill patients”. His own cardiovascular surgery department at Okamura Memorial Hospital, Japan, has seen numerous complications in vaccinated patients, including some deaths, he says.
“NHS reveals in FOI that Ambulance Call-Outs for Heart Illness have Doubled since COVID-19 Vaccination began among all age-groups“:
The National Health Service has confirmed in response to a freedom of information request that ambulance call-outs relating to immediate care required for a debilitating condition affecting the heart nearly doubled in the whole of 2021 and are still on the rise further in 2022. But the most concerning published figures show that they have also doubled among people under the age of 30.
“Indiana Life Insurance CEO Says Deaths Are Up Among people Ages 18-64“:
We are seeing, right now, the highest death rates we have seen in the history of this business – not just at OneAmerica,” the company’s CEO Scott Davison said during an online news conference this week. “The data is consistent across every player in that business.” …
Davison said the increase in deaths represents “huge, huge numbers,” and that’s it’s not elderly people who are dying, but “primarily working-age people 18 to 64” … “Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic,” he said. “So 40% is just unheard of.
“Long Funeral Homes, Short Life Insurers? Ex-Blackrock Fund Manager Discovers Disturbing Trends In Mortality“:
On Wednesday, Dowd noted that funeral home company Carriage Services saw a 28% increase in September 2021 vs. 2020, and a 13% increase in August vs. the same period. Funerals and cremations are up 12% and 13% respectively on the quarter.
“Unbelievable U.K. Vaccine Report Update“:
Already evident in previous weeks is that for all but the youngest group, the vaccinated were getting infected at higher rates than the unvaccinated … In several age groups, it would appear the double vaccinated are infected at four to five time the rate of the unvaccinated …
Looking at double (not triple) vaccinated, it appears they have higher rates of hospitalisation for all ages over 60, and comparable rates for ages 18-59.
In this case, the rate of death of the unboosted fully vaccinated is basically twice as high for the over 70 year olds.
“For Majority of U.K. children, Covid Mortality is 0.000“:
Only six of the 25 Covid deaths in the U.K. in the first 12 month of the pandemic occurred among children without pre-existing serious medical conditions … This represents a mortality risk to ‘healthy’ children of approximately 0.0001%.
June 16, 2022
Posted by aletho |
Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
I recently gave a lecture to 70 primary care physicians here in Stockholm, titled “should the patient really get the drug?”. The lecture seemed to generate quite a bit of cognitive dissonance among some in the audience, based on the somewhat aggressive discussion that followed the lecture, which suggests to me that much of what I was saying was stuff they had literally never been exposed to before – not at any point in medical school, and not at any point during their careers after medical school either. Cognitive dissonance is good. It’s the first step towards change.
I thought it would be interesting to re-write the lecture as an article, so that more people can hopefully achieve similar levels of cognitive dissonance. Please feel free to share it with any doctors you know that you think might benefit from an expanded perspective. Anyway, here we go.
Let’s imagine a common patient. Every primary care physician meets this patient, or someone much like her, on an almost daily basis. She’s 75 years old, and overweight. She experienced a wrist fracture two years ago, and was subsequently diagnosed with osteoporosis. She has high cholesterol levels, but she’s never had a heart attack or other “cardiovascular event”. On top of that, she has type 2 diabetes, chronic knee pain due to osteoarthritis, and high blood pressure. She was diagnosed with depression a few years ago, after her husband died.
Our patient takes seven drugs every day:
- Alendronate, because of her weak bones.
- Atorvastatin, because of her high cholesterol levels.
- Sertraline, because of her depression.
- Metformin, because of her type 2 diabetes.
- Insulin, also because of her type 2 diabetes.
- Paracetamol (a.k.a. acetaminophen), because of her knee pain.
- Enalapril, because of her high blood pressure.
So, the question is, are these drugs doing her any good?
Well, to answer that question, we need to consider NNT (Number Needed to Treat). NNT is the number of patients who need to take a drug for one patient to achieve a noticeable benefit.
For alendronate, the NNT is 20, i.e. if you treat 20 people for a couple of years, you prevent one fracture. For atorvastatin the NNT is 200, i.e. you need to treat 200 people for five years or so in order to prevent one heart attack. For sertraline, the NNT is 7, which means that you need to treat seven people in order to have a noticeable effect on depression in one patient. Note that this doesn’t mean that one out of seven gets cured of their depression, it just means that there is a noticeable difference on a rating scale for depression.
For metformin, the NNT is 14 – If you treat 14 type 2 diabetics with metformin for ten years, you prevent one death. For enalapril, the NNT is 70 – If you treat 70 people with high blood pressure with enalapril for five years or so, you prevent one stroke.
For insulin, however, there is no NNT, because insulin has not been shown to result in any benefit on any clinically relevant outcome, even though big studies have been carried out that have included thousands of patients and followed them for five or ten years. Note here that we’re talking about insulin for type 2 diabetics. When it comes to type 1 diabetes, insulin is pretty much magical – you don’t even need to do a randomised trial in order to show benefit. People with type 1 diabetes virtually return from the dead when treated with insulin. But when it comes to type 2 diabetes, there is no benefit, at least not to any hard outcomes. All insulin has been shown to do is reduce blood sugar, but it’s never been shown to result in any meaningful patient oriented benefit for type 2 diabetics.
The same is true for paracetamol/acetaminophen. When it comes to patients with knee pain due to osteoarthritis, the drug doesn’t provide any benefit whatsoever.
Ok, so we have seven drugs, and we know what their NNT’s are. If we plus the probabilities of benefit together, then we get the probability that our 75-year old woman will benefit in some way from at least one of the drugs she’s taking. So, what probability of benefit do we get?
We get 30%. Only 30%.
What that means is that there is a 70% probability that this woman doesn’t benefit at all from any of the seven drugs that she takes every day for years on end!
If you told her, I’d say there are pretty good odds she’d decide to stop taking her pills. Seven drugs a day, every day, and two to one odds of zero benefit.
And we haven’t even talked about harms yet. Because none of these pills are inert. All have widespread biological effects. And all can cause harms. So any rational treatment decision must include not just the potential benefits, but also the potential harms.
For figuring out harms, we have NNH (Number Needed to Harm), which is the counterpoint to NNT. NNH is the number of patients who need to get a drug for one to be harmed. Like I said, the drugs all have widespread biological effects, so there isn’t just one NNH – there is an NNH for each possible harm. That means that there are multiple NNH’s for each drug.
With our 75-year old woman and her seven drugs, we don’t have time to go through the NNH for every possible side effect, so we’re just going to look at a few, and put them side by side with the NNT, to get a somewhat more complete picture of benefits vs harms. I’ve tried to make sure that the NNH numbers apply to the same time period as the NNT numbers, since otherwise it’s an apples to oranges comparison.
If we do that, we get something like this:
Alendronate
NNT: 20 (fractures)
NNH: 200 (esophagitis), 260 (atrial fibrillation), 4,000 (osteonecrosis)
Atorvastatin
NNT: 200 (cardiac infarction)
NNH: 20 (myalgia), 20 (type 2 diabetes)
Sertraline
NNT: 7 (depression)
NNH: 2 (sexual disturbance), 10 (hyponatremia)
Metformin
NNT: 14 (death)
NNH: 2 (stomach upset), 5 (B12 deficiency), 1,000 (lactic acidosis)
Enalapril
NNT: 70 (stroke), 125 (death)
NNH: hyperkalemia (10), acute kidney failure (100)
Insulin
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: severe hypoglycemia (5), weight gain (1)
Paracetamol/acetaminophen
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: Hypertension (30), liver damage (?)
It’s possible to quibble here about specific NNT and NNH numbers. Different studies show different things. And many of the numbers come from studies carried out by pharmaceutical companies, which generally means that the risk of a certain side effect is massively underestimated (as we will discuss shortly). The point here isn’t to get hung up on any of the specific numbers. It’s to illustrate that we quickly end up with a very complex equation, where it in many cases isn’t clear at all whether the benefits outweigh the harms.
Take alendronate, as an example. We know that it decreases fractures in elderly osteoporotic women. But it doesn’t decrease hospitalisations. The only reasonable conclusion is that the reduction in hospitalisations that is seen due to the reduction in fractures is made up for by an increase in hospitalisations due to the many and varied side effects. So at the end of the day the only way to decide whether or not to take the drug is to have a detailed discussion with the patient and get them to decide which set of risks they’d rather be taking.
Hippocrates is supposed to have said “primum non nocere”, which is latin for “first, do no harm”. Actually he didn’t say that, and couldn’t have even if he wanted to. Hippocrates was greek, and didn’t speak latin. The quote comes from a 19th century American physician, Worthington Hooker.
Of course, as doctors, we all know that “first, do no harm” is completely unrealistic. Every intervention we do carries some measure of risk. If our primary guiding principle was to never do harm, we literally would never be able to do anything. A more reasonable principle is “only do something if the benefits clearly outweigh the risks”. If it isn’t clear to you that the benefits of a drug outweigh the harms, then don’t give it to the patient.
That’s a good general rule to stick by. However, it probably isn’t enough, for a few reasons we’re now going to discuss.
A study was published in JAMA Internal Medicine in 2021 that sought to establish how good physicians are at estimating the likelihood that a patient has a certain disease. 500 primary care physicians in the US were asked to consider various hypothetical scenarios, and then answer what they thought the probability of disease was. Here’s an example of a scenario that they were asked to consider:
Ms. Smith, a previously healthy 35-year-old woman who smokes tobacco presents with five days of fatigue, productive cough, worsening shortness of breath, fevers to 102 degrees Fahrenheit (38.9 degrees centigrade) and decreased breath sounds in the lower right field. She has a heart rate of 105 but otherwise vital signs are normal. She has no particular preference for testing and wants your advice.
How likely is it that Ms. Smith has pneumonia based on this information? ___%
Ms. Smith’s chest X-ray is consistent with pneumonia. How likely is she to have pneumonia? ___%
Ms. Smith’s chest X-ray is negative. How likely is she to have pneumonia? ___%
Go ahead and make your own guesses in relation to each of the three questions.
Once you’ve done that, you can take a look at the table below, and the answers will be revealed.

So, for our pneumonia example above, we see that the actual initial risk of disease based on the presented information was around 35%. If we then move along and look at what the doctors answered, they thought the risk was 80-85%. In other words, they thought pneumonia was more than twice as likely as it actually was!
The same phenomenon was seen in all clinical scenarios tested. The doctors consistently overestimated the initial risk, and they continued to overestimate the risk after both a positive and a negative test result. In some cases the difference between reality and what the doctors thought was huge, with the doctors overestimating risk by a factor of ten or more.
What can we conclude from this?
Doctors consistently overestimate disease risk.
Hold that thought, as we move on to take a quick look at another study, which was published in BMJ Open in 2015. This study sought to do something about a problem inherent in statin trials (and for that matter, all trials in medicine), which is that the results they produce, in the form of percent absolute risk, percent relative risk, and NNT, are so abstract that they’re completely meaningless to patients (and for that matter, to doctors as well). We know that statins have an NNT of 200 when used for primary prevention (to prevent a heart attack in someone who has risk factors but hasn’t already has a heart attack), and 40 when used for secondary prevention (to prevent additional heart attacks in someone who has already experienced a heart attack). But what do those numbers actually mean? Are they good or bad?
What the patient really wants to know is “how much longer will I live if I take this drug?”
So, what the researchers did was gather together data from all the big randomised trials of statins, and use the survival curves provided to estimate how much longer the patients actually lived. Here’s what they came up with:

All the big statin trials are included here. What’s interesting to do is look at the NNT provided, and then compare that with the number to the right of it, which is how much longer the patients actually lived, on average. So, for the ALLHAT trial, to take the topmost example, we have an NNT (for primary prevention) of 250, which comes down to a postponement of death of 4.96… well, 4.96 what?
Is it years? No.
Is it months? No
The patients in the statin group lived 4.96 days longer than the patients in the placebo group. That is what the NNT of 250 means in real terms.
Let’s look instead at 4S, which was published in 1994 and is the statin trial that has produced the best results of any statin trial ever. It’s the trial that initiated the massive boom in statin prescribing that we still see today. In 4S, the NNT (for secondary prevention) is 27.8. So, in other words, one in 27.8 patients benefited from the treatment.
But what does that actually mean in terms of life extension?
It means 27 days.
Not as impressive as you would have thought, right?
When the researchers put all the data together, from all the trials, in order to get an overall average, what they found was that when statins are used for primary prevention they prolong life by 3 days. When they are used for secondary prevention, they prolong life by 4 days.
I can imagine quite a few patients turning down the offer of a statin if they knew that it will on average only prolong their life by days.
The purpose of bringing up this study was to illustrate the following general point:
Doctors consistently overestimate the benefit of the drugs they prescribe.
Hold that thought in your mind as we move on and look at a third study.
This one was published in The Lancet Healthy Longevity in 2021. It compared the rate of serious side effects seen in randomised trials with that seen in the real world. If randomised trials give us good information about what to expect in reality, then the rate of serious side effects in the trials should be the same as that seen in reality.
But that isn’t what the researchers found. What they found was that serious side effects were three to four times more common in reality than they are in the randomised trials! Three to four times!
How is this possible?
Well it’s important to remember that the randomised trials are funded and run by the drug companies, and the drug companies want to sell their drugs, so they will do what they can to make side effects appear as rare as possible.
Why is this a problem? Because it’s the randomised trials that doctors mostly use as a basis for determining whether a drug is safe to give to a patient or not.
So, what can we conclude from the study?
Doctors consistently underestimate side effects of drugs.
Ok, so we have three conclusions, that are all pointing us in the same direction:
- Doctors consistently overestimate disease risk.
- Doctors consistently overestimate drug benefit.
- Doctors consistently underestimate drug harm.
What does this lead to?
Massive overprescribing of drugs.
Peter Gotzche, a founding member of the Cochrane Collaboration and former director of the Nordic Cochrane Center, has estimated that prescription drugs are now the third biggest cause of death in the western world, after heart disease and cancer.
That on its own should lead to massive humility among all doctors about our drug prescribing. It should make us much more careful every time we think about prescribing a drug to a patient.
Ok, so we’ve identified the problem. The causes of this problem are many and complex, so I’m just going to bring up one that each of us as doctors can actually do something about – industry sponsored meals.
A study was published in JAMA Internal Medicine in August 2016 that sought to estimate the extent to which physicians are influenced by partaking in industry sponsored meals, which often take the form of a lecture about a specific drug given by an drug company salesperson, which the physician is supposed to sit and listen to in return for getting a free meal. Industry sponsored meals are very common. Most physicians probably take part in at least a couple of these per year, and many take part in far more than that.
As the saying goes, “there’s no such thing as a free lunch”. The drug companies are not charities whose goal it is to keep starving doctors alive. If they spend vast sums of money of sponsored meals, it’s because they’re pretty damn sure that it increases sales of their drugs, and thereby their profits.
So, anyway, the study sought to estimate the extent to which industry sponsored meals influence physician prescribing patterns, by comparing participation in such meals with later prescribing behaviour. Here’s what they found:

They looked at four different drugs. As I think is clear from the tables, participation in industry sponsored meals increased prescribing of the drug the meal was about, and the more such meals a doctor participated in, the more often he or she prescribed that drug.
The purpose of these meals is not to educate us, or make us better doctors. It’s the opposite – the purpose is to make us do a specific profit-driven company’s bidding. And it works.
If you’re a doctor, and you think you don’t get influenced by participating in industry sponsored meals, then you are very naive. The more industry sponsored meals we participate in, the worse doctors we become.
Doctors in general massively underestimate the extent to which their thoughts, beliefs, and opinions are influenced by the pharmaceutical industry. We like to think that we are evidence based. But the truth is that much of what we think we know is not based on sound scientific knowledge, but on pharmaceutical industry propaganda, which quickly becomes clear to anyone who starts going through the studies in detail themselves.
On that note, I strongly recommend reading these three books, all written by physicians, to help get some perspective on the scale of the problem we face in relation to the pharmaceutical industry.
- Bad Pharma by Dr. Ben Goldacre
- Doctoring data by Dr. Malcolm Kendrick
- Deadly medicines and organised crime by Dr. Peter Gotzsche
There is one very simple thing every doctor can do, to at least partially free themselves from the onslaught of drug company propaganda, and that is to refuse to take part in industry sponsored lunches, and all other forms of industry sponsored “education”. Just say No.
Ok, so, that’s number one: refuse to take part in industry sponsored lunches.
What else can you do as a doctor?
Well, something that was once considered standard, but has fallen by the wayside in recent decades, is to never have a patient on more than five drugs at the same time. With drugs, as with everything else, there is a state of diminishing returns – the more you add, the less benefit (and more harm) each additional drug confers. So try to keep a patient on at most five simultaneous drugs. If you want to add a sixth, then rank them all, and get rid of the one that you think is least important. Most likely, the sixth least important drug in a list of six is not going to do anything useful for the patient anyway, just increase their risk of harm.
Ok, so that’s number two: try to avoid having your patients on more than five drugs simultaneously.
Number three: go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit. As any doctor will know, it’s common for patients to stay on drugs for years, even though the original reason they were put on the drug resolved itself a long time ago. The patient often doesn’t remember why they were put on the drug in the first place, but they keep taking it dutifully. Drug lists require regular pruning or they will become increasingly bloated as the years go by, which is one reason why so many elderly people are on 15 simultaneous drugs or more.
Number four: only prescribe a drug if the benefits clearly outweigh the harms. This should be obvious, but it requires a deep knowledge of the size of both potential benefit and potential harm, which unfortunately most doctors lack. And what they think they know is often incorrect because it’s based more on pharma propaganda than real science.
As a doctor, the only way to get around this is to start doing your due diligence and getting in to the weeds of the scientific studies. Do that for the ten drugs you prescribe most commonly, so that you’re an expert on those ten drugs, and you’ve already done a lot. If a patient asks you about the probability of benefit and the probability of harm, you should be able to answer that question correctly, at least for the ten drugs you use most frequently. It requires an up-front investment of time, but it will pay massive dividends to your patients over the remainder of your career.
Ok, so that was number four: only prescribe a drug if the benefit clearly outweighs the harm.
Here’s number five: prioritise lifestyle changes. Most of the diseases that doctors spend most of their time dealing with are caused by poor lifestyle choices. And most can be rectified by switching to good lifestyle choices, which invariably produce greater benefits than any drug can, with less risk of harm.
Doctors can accomplish a lot with their patients with simple lifestyle coaching. To take one example, a primary care clinic in the UK decided to try putting their type 2 diabetic patients on a ketogenic diet, since the drugs they were using clearly weren’t making the patients better. They published their six year follow up results in BMJ Nutrition, Prevention, and Health in 2020.
Over six years, the patients following the ketogenic diet decreased their median HbA1c (a measure of average blood sugar over the preceding few months) from 66 to 48. Normally, that would be unheard of. HbA1c doesn’t decrease over time in a type 2 diabetic. It increases. Yet here it was far better at the end of the six years than at the beginning. The same goes for body weight. Normally it goes up over time. But here the median decreased from 99 kg to 91 kg. And on top of that, median systolic blood pressure dropped from 152 to 141.
All this just with a simple diet intervention. Thanks to the improvements in all health markers, the patients were able to get off a lot of their drugs. This meant that after six years, the clinic was spending less than half as much money on anti-diabetic drugs as the other primary care clinics in the region.
To take another example of a simple lifestyle intervention, a randomised trial published in BMJ in 2021 that was carried out in nursing homes in Australia found that a diet high in protein has an effect on fracture risk that is equivalent to that seen with bisphosphonates.
There is a massive amount that can be accomplished with simple lifestyle interventions, and since they are much less risky than drugs, and actually treat the underlying problem rather than just putting a patch on top of it, they should be the primary intervention we use whenever possible. Drugs should be viewed as a complement to lifestyle interventions. It shouldn’t be the other way around.
Ok, so that was my fifth and final point. I’ll repeat the five points here again. These are five things that you as a doctor can do about the situation we currently find ourselves in, where prescription drugs are the third biggest killer in the western world:
- Refuse to participate in industry sponsored lunches and other industry sponsored “education”.
- Try to avoid having your patients on more than five drugs simultaneously.
- Go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit.
- Only prescribe a drug if the benefits clearly outweigh the harms.
- Prioritise lifestyle changes.
June 16, 2022
Posted by aletho |
Book Review, Science and Pseudo-Science, Timeless or most popular |
Leave a comment
Just like ‘Vaxxed’, this A grade documentary was successfully stopped from being aired on tv, by some jews who have lots to lose. After watching it, you can see why the jewish drug pushers would not want people to see this. This video could be said to be the precursor to Vaxxed. It includes Dr Andrew Wakefield and how he has cured many children who were Autistic, in addition to making the link between vaccines and neurological harm/damage.
Related
Vaxxed
Vaxxed World (channel)
Watch Mercury Kill The Brain – Vaccines And Neurodegeneration
June 16, 2022
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, Video |
Leave a comment
Government-funded research of lab-engineered viruses to create contagious self-spreading vaccines that bypass the consent of citizens. What could go wrong?
For two decades scientists have been quietly developing self-spreading contagious vaccines. The NIH funded this research, in which either DNA from a deadly pathogen is packaged in a contagious but less harmful virus, or the deadly virus’s lethality is weakened by engineering it in a lab. The resultant “vaccines” spread from one person to the next just like a contagious respiratory virus. Only five percent of regional populations would need to be immunized; the other ninety-five percent would “catch” the vaccine as it spread person-to-person through community transmission.
This technology bypasses the inconvenience of recalcitrant citizens who may refuse to give consent. Its advocates highlight that a mass vaccination campaign that would ordinarily take months of expensive effort to immunize everyone could be shortened to only a few weeks. Scientists have already shown proof of concept in animal populations: in 2000, Spanish researchers injected seventy rabbits with a transmissible vaccine and returned them to the wild, where they quickly passed the vaccine on to hundreds more, reportedly stopping a viral outbreak. European countries are now testing the technology on pigs.
In the wake of the covid pandemic, about a dozen research institutions in the U.S., Europe, and Australia are investigating the potential human uses for self-spreading vaccines. The federal Defense Advanced Research Projects Agency (DARPA), for example, is examining this technology for U.S. military to protect against the West Africa lassa fever, a virus spread by rats to humans. This project, it should be noted, does not require the consent of our military service men and women.
In 2019 the U.K. government began exploring this technology to address the seasonal flu. A research paper from Britain’s Department of Health and Social Care advised that university students could be an obvious target group:
They do not work so [vaccinating them] will not cause much economic disruption and most have second homes to go to, thereby spreading the vaccine.
Researchers admitted a contagious vaccine for an attenuated flu virus would cause some deaths but estimated these would be less than the original influenza virus. As the U.K. government report described:
Self-spreading vaccines are less lethal but not non-lethal: they can still kill. Some people will die who would otherwise have lived, though fewer people die overall.
As the saying goes, you can’t make an omelet without breaking a few eggs. Or in Lenin’s formulation, if you are going to chop down a forest then wood chips will fly. Contagious vaccines are in our future, their champions claim, and are no different than putting fluoride in drinking water. Plus, for those who find jabs unpleasant there are fewer needles required.
Government-funded research of lab-engineered viruses to create contagious self-spreading vaccines that bypass the consent of citizens. What could go wrong?
June 15, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Australia, Darpa, Human rights, NIH, UK, United States |
Leave a comment
Pfizer wants Babies to be Exposed to SIX Vaccine Shots!
I will explain that
- Children of Covid vaccinated mothers were never tested for developmental disorders
- CDC recently revised and lowered developmental milestones, and removed some entirely
- Newly born babies will be exposed to SIX doses of mRNA vaccines if the FDA’ approves the Pfizer vaccine.
An interesting article came out:
This article found that at one year of age, babies born to mothers who had COVID (not vaccine), had a roughly twice-higher rate of neurodevelopmental disorders:
those born to the 222 mothers with a positive SARS-CoV-2 polymerase chain reaction test during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first 12 months after delivery, even after accounting for preterm delivery.
Considering that COVID is a bad disease for a sizable minority of people, there is no surprise. Covid is bad and gives people all sorts of problems. Then I started thinking: a lot of adverse effects of Covid vaccines mimic the adverse effects of Covid. The younger is the vaccine recipient, the worse some effects of vaccination (such as myocarditis) are.
A great number of expectant mothers received up to three Covid vaccine shots during pregnancy. Did anyone bother testing one-year-old children of vaccinated and boosted (during pregnancy) women for neurodevelopmental disorders, before approving this vaccine for all pregnant women?
The question is, obviously, rhetorical, since “mRNA Babies” of triple-vaxed-during-pregnancy mothers are only beginning to get born right now and are at most a few months old. Not one such baby reached a year of age. So nobody tested them for developmental disorders at one year of age, before approving the three vaccine shots for expectant mothers.
The usual argument of vaccinators that “since Covid does it too, you should take the vaccine” does not hold water. To a woman who decided to take the vaccine, the probability of getting a vaccine is 100%. The probability of her getting Covid is much less. In the above study, out of 7,772 births, only 222 (2.8%) were exposed to Covid during pregnancy. So while vaccination is 100% guaranteed for those who elect to vaccinate, the chance of Covid is over 30 times less likely. And the “vaccine” does not prevent Covid anyway and does not even reduce the viral load.
There is literally zero data on one-year-old children of triple-vaccinated mothers because the oldest ones are 3-4 months old as of today.
However, there are disturbing developments regarding newborns. Vaccination does seem to have an effect on births and pregnancies.
The best data I found regarding recently born newborns happens to come from Scotland. They have an interesting “wider impacts” page that I am quoting below.
Infant deaths are way above average and exceeded “Alert Limits” twice.

Even pregnancy terminations went up at the end of 2021, possibly but not certainly explained by prenatal vax problems:
Low Apgar score births (for those readers who do not have kids, Apgar score is how healthy is the baby at birth, the best being a score of 10) triggered a green alarm signal:

Mind you, an Apgar score is also a developmental evaluation of sorts — at 5 minutes after birth. What will happen to the developmental milestones of those lucky babies of vaccinated mothers, who survived the pregnancies, did not die postnatally, and lived to one year of age? I literally have no idea and nobody else in the world does — the time has not passed yet.
The data we have is NOT encouraging.
CDC Solution: Remove and Lower Milestones
The CDC possibly caught a whiff of this, because in February of 2022 they literally removed half the developmental milestones, bumped some others to higher ages, and lowered standards for yet more of them. (Hat tip @CLesterwood)

About one-third of milestones like fine motor skills have been bumped up to older ages. Because of the setback, children may worsen their developmental delay, making it harder to provide early intervention, explains Jessica Hatfield, MS, OTR/L, a pediatric occupational therapist for TheraTree Pediatric Therapy.

Removing crawling as a milestone??? Are you kidding us? For those of my readers who are parents, do you think that crawling is unimportant as a milestone?
Vaccinated Infants Exposed to SIX Doses of Covid Vaxx in a Year!
Imagine a vaccine enthusiast mother, who gets three doses during her pregnancy. Say, two doses during month 4 and one during the last week of pregnancy. The unborn baby is, obviously, exposed to all that.
Then the baby is born.
If the June 14-15 FDA meeting goes as planned, FDA will approve a three-dose Pfizer vaccine for infants and toddlers. So shortly after being exposed to THREE doses of mRNA vaccines prenatally, the recently born 6 months old baby will get THREE MORE Pfizer mRNA shots.
That’s a total of, drumroll, six spike protein, and nanoparticle exposures. For a tiny newborn, all during one first year of her life.
And what if the mom has several Covids while being pregnant and vaccinated?

They will ask the mom to vaccinate the baby regardless of those covid infections. This literally amounts to six doses within a year or close to, without even counting actual covids that the vaxed moms have. Pfizer will make $132 from these six shots. Not sure if the baby will eventually need much more expensive treatments.
Do you think that it is a little bit too much? Do you think Pfizer or the FDA care?
June 15, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | CDC, COVID-19 Vaccine, FDA, Human rights, UK, United States |
Leave a comment
Labour and the SNP are planning on a new amendment
Civil libertarians often talk about a phenomenon known as the “ratcheting effect”. This is the idea that when it comes to the erosion of our liberties, the trajectory tends to head in one direction; in favour of state power at the expense of our rights and freedoms.
It is the reason why we draw red lines that should not be crossed. If you breach the principle of non-interference in people’s rights with a relatively minor incursion, what is to stop that minor incursion from escalating to something more significant in the future?
Yet with the Online Safety Bill, a censor’s charter, which has been so long in the making, the ratcheting effect is happening in real time. Last week, SNP and Labour politicians on the Committee currently scrutinising the Bill laid an amendment to include “health-related misinformation and disinformation’ as a recognised form of lawful but ‘harmful’” speech. This threatens to open a Pandora’s box of censorship.
The terms ‘misinformation’ and ‘disinformation’ have grown to become part of the political lexicon in recent years. The concepts of being incorrect or misleading have been left behind for alternative terms, with loaded connotations. Yet they are malleable terms, often deployed in ways to discredit or silence another individual’s argument in the course of public debate.
Stoked by these fears, we have seen Big Tech increasingly taking on the role of online speech police in recent years. During the coronavirus era, this reached new extremes. At the beginning of the pandemic, Facebook took the step of removing content which promoted face masks as a tool to combat the spread of Covid-19.
Yet within a short space of time, the medical consensus on masks changed. But rather than acknowledge that it was wrong, Facebook flipped its position and censored in the other direction. A high-profile example saw Facebook label, discredit and suppress an article in The Spectator, written by the Oxford academic Carl Heneghan, disputing the efficacy of masks. What grounds or competency Silicon Valley’s fact-checkers had to overrule reasoned arguments by a Professor of Evidence-Based Medicine remains to be seen.
This approach is a direct threat to the epistemic process, so central to the free and open development of knowledge and ideas in liberal democracies. The fact that not even academics can escape this kind of truth arbitration speaks volumes.
Proponents of the Online Safety Bill perform mental gymnastics in trying to defend the legislation by arguing that hard and soft censorship is already happening online. They fail to provide how an approach which sees the state support these systems and even designate some categories of free speech as ‘harmful’, will do anything but compound this issue.
All of this highlights a problem that the Government are yet to acknowledge; this Bill could end up strangling our rights and freedoms online. The misinformation amendment is unlikely to carry much traction for now, but it is a sign of things to come. We should all be concerned.
June 15, 2022
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | Online Safety Bill, SNP, UK |
Leave a comment