Lockdowns: the evidence revisited
Professor Marilyn James, Professor of Health Economics, Professor David Paton, Professor of Industrial Economics | Health Advisory & Recovery Team | June 10, 2022
“It is possible that lockdown will go down as one of the greatest peacetime policy failures in modern history” – Professor Douglas Allen[1]
In March 2021, we wrote two sections in ‘Covid-19 the evidence’, namely ‘Economic impacts – the true cost of lockdown’ and ‘Lockdowns – do they work?’. Over a year later, we have revisited not only the financial costs of lockdowns but also the societal costs, the impact on healthcare and the lack of evidence for overall benefit.
Assessing the economic costs of lockdowns and other Covid-19 restrictions is not easy, partly because the pandemic itself would have impacted economic activity independent of Government restrictions. However, we do now have considerable evidence that both voluntary behaviour change and government restrictions have significant economic effects.[2],[3] Further, voluntary changes tend to have most impact on the activity of groups most vulnerable to Covid, whilst Government restrictions have a disproportionate effect on those least vulnerable. This means that not only do most mandatory restrictions have a significant economic impact, but any benefits in terms of reductions in hospitalisations or deaths are minimal.[4]
Many of the immediate economic consequences of lockdowns were masked by the eye-watering amount of money spent by governments on furlough and business support schemes. Given the limited evidence that stay-at home measures and business closures have any significant impact on infection rates[5], the question needs to be asked whether the billions spent paying business to shut down and people not to work could have been used better by building up capacity in the health system. The stay at home message of “protect the NHS” may have been no more than elaborate code for don’t highlight years of dwindling funding that failed to keep pace with growing population and demand in health care, with the NHS entering the pandemic with spending per GDP at the lowest level since 2009.[6]
Although furlough and business support schemes have had success in limiting the impact on unemployment, the longer-term economic consequences of lockdowns are now becoming clear. The lack of spending opportunities during lockdown contributes to a build-up of personal and corporate savings. As restrictions have eased, people begin to spend these savings and, combined with the supply chain issues that have built up in the meantime, sustained inflation is the inevitable result. Even worse, having spent about £70 billion[7] paying healthy people not to work via the furlough scheme and some £150 billion in total on support measures[8], the ability of the government to respond to this lockdown-induced cost-of-living crisis via either tax cuts or increased benefits, is limited due to the hit to public finances caused by lockdown-induced government spending.
It is perhaps no surprise that a series of research papers looking at data from Australia[9], the UK[10], Canada[11] and the US[12], have concluded that the costs of lockdowns exceed any plausible estimate of the benefits many times over.
The pandemic saw one disease prioritised over all others. It is now painfully clear that the “all others” are set to suffer with longer and larger health consequences than those of the covid-19 crisis itself. The report issued by the BMA is terrifying in every sense.[13] At the start of the pandemic 4.24m were waiting for elective treatment this now stands at 6.18m. Ridsdale makes the point “stay home” may well have contributed to excess deaths as people died at home without access to care and government policy prioritised covid above all other health concerns[14]. This figure of 6.18m masks and continues to mask the lack of referrals that occurred. There is no reason to suppose demand has dropped for elective care, yet, since the pandemic there have been 4.51 m fewer elective referrals. The latest figures show some 300,000 are waiting over a year for treatment. Again, this figure is masked by GPs under referring, reporting their ability to make referrals is severely constrained, yet the patients are still sitting at primary care level needing care. If the elective surgical figure continues to remain well below pre pandemic levels, NHS waiting lists will only continue to rise. Add to this routinely soaring long waits of over 12 hours at emergency department level and the gap between target time for cancer surgery and actual time to getting surgery increasing, the health picture created by covid prioritisation in the UK is frightening.
Lockdowns created isolation from our social and working worlds. The latest report from MIND states “Isolation and loneliness have made people’s mental health worse – with young people particularly badly affected.”[15] Similar can be said for older people especially those in care homes. The unintended consequences of removing activity, family and social interaction from the elderly may be more serious than the direct disease consequences of covid, with isolation being listed as cause of death in a number of care homes in the USA.[16]
Given what we now know, it is hard to disagree with the conclusion of Professor Doug Allen’s analysis of lockdown costs and benefits in Canada that “lockdown will go down as one of the greatest peacetime policy failures in modern history.” 1
References
- https://doi.org/10.1080/13571516.2021.1976051
- www.sciencedirect.com/science/article/pii/S0047272720301754?dgcid=rss_sd_all
- https://direct.mit.edu/rest/article-abstract/doi/10.1162/rest_a_01108/107399/Do-Stay-at-Home-Orders-Cause-People-to-Stay-at
- https://link.springer.com/article/10.1007/s42973-021-00077-9
- https://onlinelibrary.wiley.com/doi/10.1111/eci.13484
- https://www.health.org.uk/news-and-comment/charts-and-infographics/health-spending-as-a-share-of-gdp-remains-at-lowest-level-in
- Coronavirus Job Retention Scheme: statistics – House of Commons Library (parliament.uk)
- https://commonslibrary.parliament.uk/research-briefings/cbp-9309/#:~:text=Current%20estimates%20of%20the%20cost,per%20person%20in%20the%20UK
- https://link.springer.com/content/pdf/10.1007/s40592-021-00148-y.pdf
- https://www.cambridge.org/core/journals/national-institute-economic-review/volume/87652BB968C8244B2E478DAA353C7DF9
- https://doi.org/10.1080/13571516.2021.1976051
- https://sites.krieger.jhu.edu/iae/files/2022/01/A-Literature-Review-and-Meta-Analysis-of-the-Effects-of-Lockdowns-on-COVID-19-Mortality.pdf
- https://www.bma.org.uk/advice-and-support/nhs-delivery-and-workforce/pressures/nhs-backlog-data-analysis
- http://dx.doi.org/10.1136/bmj.m3515
- https://www.mind.org.uk/media/8962/the-consequences-of-coronavirus-for-mental-health-final-report.pdf
- https://www.nbcnews.com/news/us-news/hidden-covid-19-health-crisis-elderly-people-are-dying-isolation-n1244853
Independent Pharmacovigilance Report Confirms Evidence for Recall of Covid-19 Vaccines
World Council for Health | June 11, 2022
Adverse Reactions for Novel Covid-19 Vaccines More Numerous Than for Similar Products by Factor of Between 10 and 169
BATH, UK — A new report prepared by the World Council for Health (WCH) has confirmed that data on adverse drug reactions from the experimental Covid-19 vaccines exist in an amount sufficient for the recall of similar products in the past.
The report was prepared to determine whether sufficient pharmacovigilance data exist on official and public databases (WHO VigiAccess, CDC VAERS, EudraVigilance, and UK Yellow Card Scheme) to establish a safety signal on the novel Covid-19 injections.
On all databases, it was found that adverse drug reaction (ADR) reports linked to Covid-19 injections are more numerous than other similar products by a factor of between 10 and 169 (see graph below). Many of the ADR reports are serious in nature and there exists sufficient evidence of associated harm on these databases to indicate a product recall.
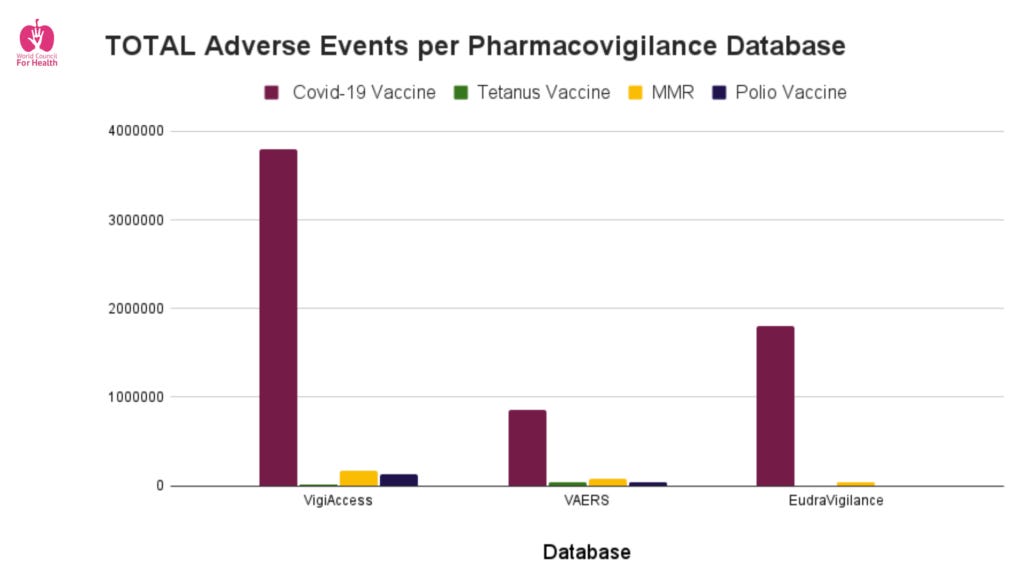
Total Adverse Events per Pharamacovigilance Database
In total, more than 40,000 deaths are linked to the novel Covid-19 vaccines in the official databases analysed.
In addition, the WCH pharmacovigilance report found that several thousand adverse drug reactions on official databases are related to the use of the experimental Covid-19 vaccines among young boys and girls for whom the vaccine had not been approved at the time.
The purpose of pharmacovigilance databases is to provide a signal of safety, and not to prove causality. To ensure that harms are detected in time, suspicion that an event is linked to the administration of the medicine is enough to register an event. “There is no need to prove that the medicine caused the adverse reaction, just the suspicion is good enough,” Dr. June Raine, head of the UK’s Medicines and Healthcare products Regulatory Agency, said in 2006. When sufficient pharmacovigilance data show a signal of harm, administration of the product should be ceased, the product recalled, and the safety signal investigated.
It should also be noted that such systems of passive surveillance result in significantly fewer ADR reports than active surveillance reporting. As a result, the actual number of adverse events that occurred in temporal relation to Covid-19 injections is likely to be much higher than revealed by the available official data.
In December 2021, World Council for Health called on regulators and governments around the world to immediately cease use of all experimental Covid-19 injections.
Dr. Tess Lawrie, co-founder of the World Council for Health, calls for people to come together to raise awareness of vaccine injury so that those harmed can get the help they deserve. “It is concerning that a grassroots organisation has had to do this work and point out that none of these experimental vaccines are safe according to publicly available official data. Why have the regulators not done their job and protected us?“
***
World Council for Health Covid-19 Vaccine Pharmacovigilance Report: https://worldcouncilforhealth.org/resources/covid-19-vaccine-pharmacovigilance-report/
World Council for Health Calls for an Immediate Stop to the Covid-19 Experimental “Vaccines”: https://worldcouncilforhealth.org/campaign/covid-19-vaccine-cease-and-desist/
World Council for Health Statement on Covid-19 Vaccines: https://worldcouncilforhealth.org/news/2021/12/covid-19-vaccines/14001/
World Council for Health Statement on Risk of Myocarditis in Children: https://worldcouncilforhealth.org/news/2022/01/risk-of-myocarditis-in-children/18570/
Contact: Dr. Katarina Lindley at katarina@thewc4h.org
Another nudge to vaccinate children and for whose benefit?
The runaway train that refuses to be knocked off course
Health Advisory & Recovery Team | June 10, 2022
When the JCVI considered covid vaccines for children in July 2021, they stated, “JCVI is of the view that the health benefits of universal vaccination in children and young people below the age of 18 years do not outweigh the potential risks”. Even in September 2021, they still said, “A precautionary approach was agreed given the very low risk of serious disease in those aged 12 to 15 years without an underlying health condition that puts them at increased risk.” As HART bulletin readers will know, the Chief Medical Officers eventually recommended the vaccine for 12-15s, in the vain hope of reducing school closures, which of course could have been achieved by simply stopping routine testing of asymptomatic school children and the sending home of healthy contacts.
Roll on to February 2022, when a ‘non-urgent offer’ was made of Pfizer vaccine for 5-11-year-olds, JCVI stated, “This advice on the offer of vaccination to 5 to 11-year olds who are not in a clinical risk group is considered by JCVI as a one-off pandemic response programme. As the COVID-19 pandemic moves further towards endemicity in the UK, JCVI will review whether, in the longer term, an offer of vaccination to this, and other paediatric age groups, continues to be advised.”
If any of our readers has seen this review, we would be pleased to know, as it might help us clarify the surprising appearance of Covid-19 on the NHS routine immunisation programme. Placing an unlicenced preparation onto the routine schedule is unprecedented. It raises serious questions of the legality, given the conditional authorisation was predicated on there being an emergency. It is also of course a subtle way of making parents think this vaccine is just run-of-the-mill. The current low uptake (53% of 12-15s and a mere 8.5% of 5-11s) suggests that at present, parents are well aware that covid-19 vaccines are not the same as other vaccines, either in terms of the risk of the disease for children or in terms of drug safety. They will also be well aware that lots of their triple vaccinated adult friends and family, have been catching covid regardless.
Not content with slipping this drug into the schedule under cover of the 4-day Jubilee holiday, the Local Government Association has been pushing behavioural psychology techniques to increase vaccine uptake in the young. Their opening gambit is, “Younger generations are more likely to be vaccine hesitant partly because they perceive themselves to be at lower risk of developing a severe form of COVID-19”. Surely, this is not a ‘perception’, it is a ‘fact’, which should surely have been viewed as a blessing, rather than an annoyance.
It gets worse: “Highlight the pro-social benefits of vaccination
Behavioural Insight: Emphasising the pro-social benefits of vaccination is particularly effective among young people. Prosocial benefits include achieving herd immunity and protecting others, especially those that are vulnerable and cannot get vaccinated. Combining both informational and emotional content can be effective.” Another one for the fact checkers – the JCVI say, “the benefits to the wider population are highly uncertain.”
And worse: “Highlight social norms about vaccination
Behavioural Insight: Highlighting that there are growing intentions to get vaccinated, that most people are getting vaccinated and that they approve doing so, can effectively encourage vaccine take up. Since young people tend to be more susceptible to peer influence, it is likely that social norms can be particularly effective when targeting this group.
Potential application: Emphasise Social norms in communications targeted towards young people. Make vaccination visible to other young people by setting up vaccination centres in university campuses or schools. Launch an ‘I will get vaccinated’-pledge on social media.”
And faintly ridiculous: “Second vaccine jab compliance
Ensuring residents take their second vaccine dose could be a challenge with which councils can support PHE and the NHS. This could be especially the case if news on vaccine efficacy and new strains undermines the perceived value of the second jab.” Again, the use of the word ‘perceived’ implies that the ‘news’ on vaccine efficacy and new strains is somehow irrelevant to informed consent. No wonder the powers that be don’t want people to see this graph from week 13 of 2022, dropped from the more recent weekly vaccine reports.

Weird that the “I-Believe-The-Science(TM)” crowd has completely given up on science
The NY Times announces that henceforth, clinical trials for Covid-19 shots must be abandoned because real world data makes the cartel look bad
By Toby Rogers | June 9, 2022
I. Pharma is losing the game so they are throwing the chess board across the room
The NY Times published a vile piece of fascist Pharma propaganda today. Berenson flagged the online version of the article yesterday. As you know, I have been yelling about the FDA’s Orwellian “Future Framework” for weeks because it’s literally the worst idea in the history of public health.
It turns out that it’s even worse than I thought.
Pharma has already begun a PR offensive to get it across the line and Sharon LaFraniere of the NY Times was eager to do their bidding.
Here’s what’s happening. The mRNA shots are not working against SARS-CoV-2. Everyone knows this. So Moderna and Pfizer are racing to reformulate these shots. The reformulated shots are not working either. Just last week Moderna was touting a bivalent shot that combined Alpha + Beta, but now, apparently, they’ve abandoned that approach. The NY Times article hypes a Moderna shot targeting earlier Omicron variants (it does not say, but perhaps BA.2 and BA.2.12.1?). However evidence from South Africa shows that BA.4 and BA.5 are outcompeting the earlier Omicron variants and the reformulated Moderna shot probably won’t work against the new strains (the virus evolved for a reason — to evade vaccines).
So what are predatory pharmaceutical companies and their feckless government enablers supposed to do!? Abandon clinical trials altogether!
Here’s how the NY Times describes this scheme:
… many experts worry that the virus is evolving so quickly that it is outpacing the ability to modify vaccines, at least as long as the United States relies on human clinical trials for results.
See, it’s not that coronavirus vaccine have failed over and over again (even though they have). It’s that This Wily Virus(TM) is just evolving so quickly that we could not possibly allow human clinical trials of coronavirus vaccines ever again. The only way to beat This Wily Virus(TM) at this point is to abandon science.
Of course it gets worse. The NY Times elaborates:
The problem is that Moderna and Pfizer — the maker of the other main coronavirus vaccine in the United States — do not have enough time now to run more human clinical trials and still manufacture shots before the fall, when the Biden administration is hoping to be able to offer an updated vaccine to counter what public health experts predict will be a winter surge.
See, it’s not that rapacious pharmaceutical companies want to suck all wealth out of the world and put it into their own pockets while setting up a 1,000 year Pharma Reich. No, no, no, silly. It’s just that they “do not have enough time” to do actual science anymore so they are just going to skip all that. Don’t you worry your little head about it.
Furthermore, only a conspiracy theorist would believe that the FDA has abandoned all of its statutory responsibilities to protect public health in order to prostitute themselves to Pharma. The Correct Understanding(TM) is that the FDA is being forced by circumstances outside their control to abandon science. This is not a problem because the cartel is truth, the cartel has always been truth, and since the cartel has decided to abandon science altogether then that’s the new science.
Henceforth, quite literally, the peasants will be forced every six months to inject whatever they are told, with no questions asked, and “they will be [required by law to be] happy about it”.
Instead of human clinical trials the FDA will rely on a few test tube and mouse studies. In the article, Fauci describes this as, “alternative pathways of decision.” That guy just oozes totalitarianism at this point.
So if the “Future Framework” is approved on June 28 the new rules will be: a pharmaceutical company can claim that some new injection creates antibodies in a test tube or mouse (that no one else can see or audit). Done! Ship it and inject it! That’s it. Even though the FDA admits that there are no “correlates of protection.”
In the replies to my earlier articles about the Future Framework some astute readers have pointed out that the FDA has already abandoned human trials when it comes to Covid-19 shots in kids. None of the Moderna or Pfizer clinical trials in kids showed any real world health benefit at all. So they switched to looking at antibodies in the blood and use this tortured mental gymnastics called “immunobridging” to conjure up hypothetical future benefits that never materialize in the real world. Abandoning even the pretense of human trials and moving to test tubes and mice is the obvious next step in this complete abandonment of science.
When people say “I Believe The Science(TM)” what they really mean is “I Support The Genocide.” That’s what’s happening. The FDA has not done science in two years, probably much longer than that.
There is no left and right in politics anymore. Just, the FDA Pharma Fascist Party where members are expected to participate in self-genocide for “the good of society” (read: the profits of the cartel)
vs.
the Rebel Alliance where we practice actual science, critical thinking, logic, and reason, and work every day to protect human health and dignity.
Any politician who wants the 18 million votes of single-issue medical freedom voters in November needs to know that there must be hearings, arrests, and trials of the bureaucrats at FDA, CDC, NIAID, HHS, and NIH who did this to us.
II. What is to be done?
In the meantime, here are the email addresses for all of the public health political appointees, FDA staff, and VRBPAC members who have a say in connection with the “Future Framework”. Please contact them to urge them to reject this nonsense (proposed subject line and email text below — or share your own personal story).
Subject line: The “Future Framework” is the WORST idea in the history of public health. Please vote NO.
1. No Covid-19 shots for kids that failed clinical trials. According to the journal Nature Medicine, children and young people have a 99.995% recovery rate. According to the CDC, the overwhelming majority of children already have natural immunity. The harms from Covid-19 shots in kids are catastrophic.
2. The FDA and CDC must pivot to therapeutics. About twenty off-the-shelf treatments are more effective than vaccines (if used for prophylaxis or early intervention). Get these safe and effective medicines to people who need them and let doctors be doctors again and treat patients based on their own best clinical judgment.
3. Any reformulated Covid-19 shots MUST go through proper HUMAN clinical trials and FDA review. That means:
• large (50,000+ person) double-blind randomized controlled trials with inert saline placebos conducted by an independent third party;
• safety and efficacy studies for two years prior to any application; monitor the treatment and control group for the rest of their lives to record non-specific effects;
• must provide sterilizing immunity with greater than 90% efficacy and less than 0.1% Grade 3 Adverse Events; and
• proper monitoring for carcinogenesis, mutagenesis, and impairment of fertility.
[Contact list:]
sean.mccluskie@hhs.gov, commissioner@fda.hhs.gov, DeanofPublicHealth@brown.edu, Aux7@cdc.gov, Peter.Marks@fda.hhs.gov, Hong.Yang@fda.hhs.gov, Richard.Forshee@fda.hhs.gov, Huilee.Wong@fda.hhs.gov, Leslie.Ball@fda.hhs.gov, Doran.Fink@fda.hhs.gov, CBERVRBPAC@fda.hhs.gov, hanae@bcm.edu, paula.annunziato@merck.com, adam.berger@nih.gov, hbernstein@northwell.edu, acohn@cdc.gov, anc0@cdc.gov, hjanes@fredhutch.org, hgans@stanford.edu, david.kim@hhs.gov, asmonto@umich.edu, offit@chop.edu, spergam@fredhutch.org, Jportnoy@cmh.edu, erubin@hsph.harvard.edu, erubin@nejm.org, ashane@emory.edu, swamy002@mc.duke.edu, fullerao@umich.edu, bgellin@rockfound.org, RandyHawkins@cdrewu.edu, officeofthepresident@mmc.edu, JYLee@uams.edu, ofer.levy@childrens.harvard.edu, wayne_marasco@dfci.harvard.edu, cmeissner@tuftsmedicalcenter.org, mrn8d@virginia.edu, stanley-perlman@uiowa.edu, reingold@berkeley.edu, mhsawyer@ucsd.edu, mew2@cdc.gov
III. The FDA has opened the formal comment portal for the “Future Framework”
If you prefer the official route, you can lodge a formal comment with the FDA by following the instructions (here). Enter docket number FDA-2022-N-0905 at https://www.regulations.gov by June 22 to tell the FDA what you think of their proposed plan to abandon clinical trials for Covid-19 shots in perpetuity.
THE WHO, PANDEMIC PREPAREDNESS, AND THE IMPORTANCE OF FALSE MESSAGING
By Dr David Bell | Pandemics – Data and Analytics | June 9, 2022
The World Health Organization (WHO), and the growing pandemic preparedness industry sponsoring it, has faced considerable challenges in maintaining support for its COVID-19 response. It has addressed this difficult situation with simple and uniform messaging. The compliance thus achieved by the WHO has been vital to achieving a successful concentration of wealth, benefitting not just its major sponsors, but also the army of global health staff who have remained obedient throughout.
Threatening this progress, a skeptical minority within the public sphere have been using evidence and rational argument to undermine the pandemic industry’s potential. As the pandemic preparedness and response narrative is poorly defensible on rational criteria, such criticism and opposition must be dealt with and dismissed by other means. This is being achieved through the creation of a dogma around mass COVID-19 vaccination sufficiently separated from reality as to render the normal processes of debate irrelevant. If the gap between pandemic messaging and reality can be kept sufficiently wide, few passengers can step off, and this lucrative gravy train becomes unstoppable.
Small lies can be argued against, big lies become matters of faith
The development and mass deployment of vaccines has been a key component of the COVID-19 response, underpinning much of the transfer of wealth from lower-income people and countries to large Pharma, their investors and the global health workforce they sponsor. Against a background of rapidly increasing global poverty, this unprecedented increase in wealth has in turn raised the potential for unprecedented funding to global health institutions – the mostly Western-based industry that fills offices and drains aid budgets in Europe and North America. A significant cognitive decoupling has been necessary across this sector to achieve sufficient uniformity of voice and purpose, as the institutions involved were ostensibly intended to improve the health and uphold the rights of those less financially fortunate. To achieve success, staff of the WHO and other international organizations therefore had to be enabled to signal virtuous intent while acting in concert for corporate gain.
Vaccines traditionally protect the vaccinated against a target pathogen and humans tend to develop good immunity after respiratory virus infections. These two realities create an urgent problem for the pandemic preparedness industry, as the increased financing set to expand their reach is dependent on successfully convincing the world that these truths are indeed fallacies. Thus, to sell COVAX, the WHO’s financing facility for mass COVID-19 vaccination and the model for future pandemic responses, it was vital for the WHO to ensure that the obvious nonsensical nature of the programme would be ignored. This required coordination and adherence to a single simple message, repeated incessantly to stifle external opinion; a slogan so ridiculous that it becomes inarguable. In other words, it required propaganda.
It is essential to focus people on simplistic slogans if the aim is to suppress their tendency for independent thought and to make any venture in that direction a cause of stress. If people can see their respected authority figures standing behind a statement that is otherwise obviously false, it becomes easier to accept that the false must be true than to stand alone against authority and the crowd. Once one’s colleagues are on-board, the Asch conformity phenomenon kicks in – if everyone else is saying ‘X’, then it surely must be ‘X’, even if it looks like ‘Y’. If a health programme flies in the face of all existing medical knowledge, it must therefore be supported by a sufficiently strong dogma to negate evidence-based arguments. It is a testament to the power of group-think, loyalty to sponsors and the allure of money that this has, thus far, been brilliantly achieved.

COVAX – Selling the golden goose
“No one is safe, until everyone is safe”, the WHO’s COVAX motto, fulfills all the above criteria.
Most people want to be safe – and to achieve industry aims, the public must be convinced that others, not just themselves, are the key to their personal safety. They must support the blame or coercion being applied to these others. But the brilliance of ‘No one is safe, until everyone is safe’ is not just in its appeal to self-preservation and its divisiveness, but in its simple stupidity.
1) For the slogan to be true, the vaccine must be transmission-blocking only. It must not protect the vaccinated individual. Otherwise, their safety will not be dependent on the vaccination of others. However, the WHO and its partners also claim that “COVID-19 vaccines provide strong protection against serious illness, hospitalization and death”. Therefore, in promoting its ‘No one is safe’ slogan, WHO staff must collectively proclaim a falsehood. This builds loyalty and cohesion, as a lie is more easily maintained within a like-minded group.
2) To be ‘safe’ from a virus, one must either be intrinsically at very low risk (as most people are to most viruses) or gain immunity.
- ‘Intrinsic low risk’ created a huge problem for the mass-vaccination narrative early in the COVID-19 outbreak, as data from China showed the very strong skew of severe COVID-19 towards old age, and association with certain comorbidities. Most people are clearly at minimal risk. This had to be suppressed to enable mass-vaccination – all must consider themselves at risk. Public health agencies and their corporate backers even proclaimed impending catastrophe for the people of sub-Saharan Africa, more than half of whom are under 20 years of age. The use of age-based disease metrics, standard for disease-burden assessments up to 2019, were put aside and ‘COVID-19’ mortality reported as raw mortality numbers only.
- Immunity presents a problem, as it is both the pathway through which vaccines work, and the way we naturally gain protection. Immunity makes us safe, but natural immunity is useless to investors. While a safe vaccine would be preferable to a dangerous virus, once infection has occurred the gain from vaccination is minimal. This poses an immediate threat to profits and share price. The response to this dilemma included one of history’s more ludicrous statements from a global institution, when the WHO modified its herd immunity definition to only recognize immunity resulting from pharmaceutical intervention. This is nonsense to anyone with even a rudimentary understanding of immunology, and of course the WHO’s staff have at least rudimentary knowledge.
Inevitably, SARS-CoV-2 has continued spreading, including from the vaccinated. Based on serology from Africa, India and the USA, and the highly transmissible Omicron variant, we can now be confident that nearly all the world’s population have post-infection immunity. It is no biological surprise that immunity gained from a respiratory tract infection with whole virus reduces disease severity more effectively than injection with spike-protein or its mRNA precursors. Claiming that mass vaccination still has public health relevance in these populations requires both abandonment of logic, and a willingness to dispense with decades of prior scientific learning. It requires acceptance of dogma.
A final component of the COVAX strategy, to lock-in celebrity support and enable those promoting the vaccine to still feel virtuous, is ‘vaccine equity’. People in rich countries are having boosters whilst many of the ‘global poor’ still await their first doses. The lack of benefit to be obtained from these doses, and the requirement of coercion to attain high coverage, are irrelevant – inequity in vaccine distribution simply has to be ‘bad’. Whilst pushing more boosters on high income markets, the same Pharma companies can look good by demanding vaccine equity, advocating for the ‘disadvantaged’. In reality this diverts resources from areas of greater need, thereby killing more children, but such fine print will never make the front pages. Commodity equity expands markets and provides returns, while health equity does not. Fear of being vilified as anti-equity helps keep skeptics quiet.
Bolting down the golden goose
Science, including public health, were previously held to be based on processes of logic, based on an acceptance that aspects of our world are grounded in discoverable truth. This concept is a threat to COVAX and the wider pandemic preparedness narrative. It is a threat to the return on investment of the pandemic industry’s sponsors. Greed is a stronger driver than truth, and it must be allowed to run free if society is to be truly reset in favor of those who wish to concentrate and control its wealth.
Despite its massive internal contradictions, disproportionate cost, coercion, and requirement for its promoters to live obvious lies, COVAX and the entire mass-vaccination paradigm has created a strong model for the success of the wider pandemic preparedness project. If truth in public health can be so readily dispensed with, and those working in the field so willingly corralled, the potential for milking the public’s trust and desire for safety presents unprecedented potential for profit. As this wealth accumulates, it supports the continuing advocacy and manipulation required to keep its adherents loyal. This creates a self-perpetuating cycle – we can expect to see more outbreaks, health emergencies and pandemics declared, more vaccines rolled out, and more wealth concentrated as a result. An unstoppable cycle burying truth under a growing fog of fear and falsehood.
That, at least, is the plan. The eventual outcome will depend on whether truth, human rights, equality and trust were ever fundamental to maintaining societal cohesion and peace. If they were, then let us hope the chaos that follows their abandonment is somehow contained. For now, business is business, and the golden goose, bolted down in a hall of lies, will keep on laying.
Research Confirms Statins Are a Colossal Waste of Money
This article was previously published December 8, 2021, and has been updated with new information.
By Dr. Joseph Mercola | June 9, 2022
The lecturer in the featured video, Maryanne Demasi, Ph.D., produced the 2014 Australian Catalyst documentary, “Heart of the Matter: Dietary Villains,” which exposed the cholesterol/saturated fat myths behind the statin fad and the financial links which lurk underneath.
The documentary was so thorough that vested interests actually convinced ABC TV to rescind the two-part series.1 The Australian Heart Foundation, the three largest statin makers (Pfizer, AstraZeneca and Merck Sharp & Dohme) and Medicines Australia, Australia’s drug lobby group, complained2 and got the documentary expunged from ABC TV.
Cholesterol and saturated fat have been the villains of heart disease for the past four decades, despite the many studies showing neither has an adverse effect on heart health.
The entire food industry shifted away from saturated fat and cholesterol, ostensibly to improve public health, and the medical industry has massively promoted the use of cholesterol-lowering statin drugs for the same reason. Despite all of that, the rate of heart disease deaths continues to be high.3 That really should tell us something.
Statins Are a Colossal Waste of Money
Since the release of Demasi’s documentary, the evidence against the cholesterol theory and statins has only grown. As noted in an August 4, 2020, op-ed by Dr. Malcolm Kendrick, a general practitioner with the British National Health Service:4
“New research shows that the most widely prescribed type of drug in the history of medicine is a waste of money. One major study found that the more ‘bad’ cholesterol was lowered, the greater the risk of heart attacks and strokes.
In the midst of the COVID-19 pandemic, almost every other medical condition has been shoved onto the sidelines. However, in the UK last year, heart attacks and strokes (CVD) killed well over 100,000 people — which is at least twice as many as have died from COVID-19.
CVD will kill just as many this year, which makes it significantly more important than COVID-19, even if no one is paying much attention to it right now.”
According to a scientific review5 published online August 4, 2020, in BMJ Evidence-Based Medicine, lowering LDL is not going to lower your risk of heart disease and stroke. “Decades of research has failed to show any consistent benefit for this approach,” the authors note.
Since the commercialization of statin drugs in the late ’80s (lovastatin being the first one, gaining approval in 19876), total sales have reached nearly $1 trillion.7,8 Lipitor — which is just one of several brand name statin drugs — was named the most profitable drug in the history of medicine.9,10 Yet these drugs have done nothing to derail the rising trend of heart disease.
Lowering Cholesterol Does Not Show a Beneficial Impact
According to a press release announcing the BMJ Evidence-Based Medicine review, the analysis found that:11
“… over three quarters of all the trials reported no positive impact on the risk of death and nearly half reported no positive impact on risk of future cardiovascular disease.
And the amount of LDL cholesterol reduction achieved didn’t correspond to the size of the resulting benefits, with even very small changes in LDL cholesterol sometimes associated with larger reductions in risk of death or cardiovascular ‘events,’ and vice versa. Thirteen of the clinical trials met the LDL cholesterol reduction target, but only one reported a positive impact on risk of death …”
In their paper,12 the study authors argue that since dozens of randomized controlled trials looking at LDL-cholesterol reduction “have failed to demonstrate a consistent benefit, we should question the validity of this theory.”
They also cite the Minnesota Coronary Experiment,13 a double-blind randomized controlled trial involving 9,423 subjects that sought to determine whether replacing saturated fat with omega-6 rich vegetable oil (corn oil and margarine) would reduce the death rate from heart disease by lowering cholesterol.
It didn’t. Mortality and cardiovascular events increased even though total cholesterol was lowered by 13.8%. For each 30 mg/dL reduction in serum cholesterol, the death risk rose by 22%. In conclusion, the Evidence-Based Medicine study authors note that:14
“In most fields of science the existence of contradictory evidence usually leads to a paradigm shift or modification of the theory in question, but in this case the contradictory evidence has been largely ignored, simply because it doesn’t fit the prevailing paradigm.”
Deception Through Statistics
If lowering cholesterol doesn’t reduce mortality or cardiovascular events, there’s little reason to use them, considering they come with a long list of adverse side effects. Sure, there are studies claiming to show benefit, but many involve misleading plays on statistics.
One common statistic used to promote statins is that they lower your risk of heart attack by about 36%.15 This statistic is derived from a 2008 study16 in the European Heart Journal. One of the authors on this study is Rory Collins, who heads up the CTT Collaboration (Cholesterol Treatment Trialists’ Collaboration), a group of doctors and scientists who analyze study data17 and report their findings to regulators and policymakers.
Table 4 in this study shows the rate of heart attack in the placebo group was 3.1% while the statin group’s rate was 2% — a 36% reduction in relative risk. However, the absolute risk reduction — the actual difference between the two groups, i.e., 3.1% minus 2% — is only 1.1%, which really isn’t very impressive.
In other words, in the real world, if you take a statin, your chance of a heart attack is only 1.1% lower than if you’re not taking it. At the end of the day, what really matters is what your risk of death is the absolute risk. The study, however, only stresses the relative risk (36%), not the absolute risk (1.1%).
As noted in the review18 “How Statistical Deception Created the Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular Disease,” it’s very easy to confuse and mislead people with relative risks.
Statins Sabotage Your Health
A stunning review of statin trials published in 2015 found that in primary prevention trials, the median postponement of death in those taking statins was a mere 3.2 days. While potentially extending life span by 3.2 days, those taking statins are also at increased risk for:
- Diabetes (if taken for more than two years, your risk for diabetes triples)
- Dementia, neurodegenerative diseases and psychiatric problems such as depression, anxiety and aggression
- Musculoskeletal disorders
- Osteoporosis
- Cataracts
- Heart disease
- Liver damage
- Immune system suppression
Oftentimes statins do not have any immediate side effects, and they are quite effective, capable of lowering cholesterol levels by 50 points or more. This is often viewed as evidence that your health is improving. Side effects that develop over time are frequently misinterpreted as brand-new, separate health problems.
Crimes Against Humanity
The harm perpetuated by the promotion of the low-fat, low-cholesterol myth is so significant, it could easily be described as a crime against humanity. Ancel Keys’ 1963 “Seven Countries Study” was instrumental in creating the saturated fat myth.19,20
He claimed to have found a correlation between total cholesterol concentration and heart disease, but in reality this was the result of cherry picking data. When data from 16 excluded countries are added back in, the association between saturated fat consumption and mortality vanishes.
In fact, the full data set suggests that those who eat the most saturated animal fat tend to have a lower incidence of heart disease, which is precisely what other, more recent studies have concluded.
Procter & Gamble Co.21 (the maker of Crisco22), the American Heart Association and the Center for Science in the Public Interest (CSPI) all promoted the fallacy for decades, despite mounting evidence that Keys had gotten it all wrong.
The AHA was issuing stern warnings against butter, steak and coconut oil as recently as 2017.23 That same year, Procter & Gamble partnered with University Hospitals Harrington Heart & Vascular Institute to promote heart health by lowering cholesterol.24
CSPI was also instrumental in driving heart disease skyward with its wildly successful pro-trans fat campaign. It was largely the result of CSPI’s campaign that fast-food restaurants replace beef tallow, palm oil and coconut oil with partially hydrogenated vegetable oils, which were high in synthetic trans fats linked to heart disease and other chronic diseases.
As late as 1988, CSPI praised trans fats, saying “there is little good evidence that trans fats cause any more harm than other fats” and that “much of the anxiety over trans fats stems from their reputation as ‘unnatural.'”25
CSPI and AHA Omit Their Role in Heart Disease Epidemic
Today, you’ll have to dig deep to unearth CSPI’s devastating public health campaign. In an act of deception, they erased it from their history to make people believe they’ve been doing the right thing all along. Their historical timeline26 of trans fat starts at 1993 — the year CSPI decided to change course and start supporting the elimination of the same trans fat they’d spent years promoting.
![]()
Similarly, the AHA conveniently omits saturated fat and cholesterol from its history of “lifesaving” breakthroughs and achievements.27 It makes sense, though, considering the AHA’s and CSPI’s recommendations to swap saturated fat for vegetable oils and synthetic trans fat never resulted in anything but an epidemic of heart disease.
The idea that the harms of trans fats were unknown until the 1990s is simply a lie. The late Dr. Fred Kummerow started publishing evidence showing trans fat, not saturated fat, was the cause of heart disease in 1957. He also linked trans fat to Type 2 diabetes.
The Truth About Saturated Fat
In addition to the more recent studies mentioned earlier, many others have also debunked the idea that cholesterol and/or saturated fat impacts your risk of heart disease. For example:
•In a 1992 editorial published in the Archives of Internal Medicine,28 Dr. William Castelli, a former director of the Framingham Heart study, stated:
“In Framingham, Mass., the more saturated fat one ate, the more cholesterol one ate, the more calories one ate, the lower the person’s serum cholesterol. The opposite of what … Keys et al [said] …”
•A 2010 meta-analysis,29 which pooled data from 21 studies and included 347,747 adults, found no difference in the risks of heart disease and stroke between people with the lowest and highest intakes of saturated fat.
•Another 2010 study30 published in the American Journal of Clinical Nutrition found that a reduction in saturated fat intake must be evaluated in the context of replacement by other macronutrients, such as carbohydrates.
When you replace saturated fat with a higher carbohydrate intake, particularly refined carbohydrate, you exacerbate insulin resistance and obesity, increase triglycerides and small LDL particles, and reduce beneficial HDL cholesterol. According to the authors, dietary efforts to improve your cardiovascular disease risk should primarily emphasize the limitation of refined carbohydrate intake, and weight reduction.
•A 2014 meta-analysis31 of 76 studies by researchers at Cambridge University found no basis for guidelines that advise low saturated fat consumption to lower your cardiac risk, calling into question all of the standard nutritional guidelines related to heart health. According to the authors:
“Current evidence does not clearly support cardiovascular guidelines that encourage high consumption of polyunsaturated fatty acids and low consumption of total saturated fats.”
Will Saturated Fat Myth Soon Be Upended?
Nina Teicholz, a science journalist, adjunct professor at NYU’s Wagner Graduate School of Public Service and the executive director of The Nutrition Coalition, is the author of “The Big Fat Surprise: Why Butter, Meat and Cheese Belong in a Healthy Diet,” which reviews the many myths surrounding saturated fat and cholesterol.
In an interview I did with Dr. Paul Saladino and Teicholz, they reviewed the history of the demonization of saturated fat and cholesterol, starting with Keys, and how the introduction of the first Dietary Guidelines for Americans in 1980 (which recommended limiting saturated fat and cholesterol) coincided with a rapid rise in obesity and chronic diseases such as heart disease.
Teicholz also reviewed a paper32 in the Journal of the American College of Cardiology, published online June 17, 2020, which actually admits the long-standing nutritional guideline to limit saturated fat has been incorrect. This is a rather stunning admission, and a huge step forward. As noted in the abstract:
“The recommendation to limit dietary saturated fatty acid (SFA) intake has persisted despite mounting evidence to the contrary. Most recent meta-analyses of randomized trials and observational studies found no beneficial effects of reducing SFA intake on cardiovascular disease (CVD) and total mortality, and instead found protective effects against stroke.
Although SFAs increase low-density lipoprotein (LDL)-cholesterol, in most individuals, this is not due to increasing levels of small, dense LDL particles, but rather larger LDL which are much less strongly related to CVD risk.
It is also apparent that the health effects of foods cannot be predicted by their content in any nutrient group, without considering the overall macronutrient distribution.
Whole-fat dairy, unprocessed meat, eggs and dark chocolate are SFA-rich foods with a complex matrix that are not associated with increased risk of CVD. The totality of available evidence does not support further limiting the intake of such foods.”
Sources and References
- 1 Highstreaks May 21, 2014
- 2 YouTube Dr. Maryanne Demasi: My Experience of Exposing the Statin Con
- 3 Cardiovascular Business August 27, 2019
- 4, 7 RT August 4, 2020
- 5, 12, 14 BMJ Evidence-Based Medicine August 4, 2020 DOI: 10.1136/bmjebm-2020-111413
- 6 News-Medical.net History of Statins
- 8 BMJ January 21, 2018
- 9 Youtube.com Maryanne Demasi, Statin Wars: Have We Been Misled by the Evidence?, 1:40 minutes
- 10 Kiplinger December 1, 2017
- 11 Medical Xpress August 3, 2020
- 13 BMJ 2016;353:i1246
- 15 Youtube.com Maryanne Demasi, Statin Wars: Have We Been Misled by the Evidence?, 14:40 minutes
- 16 European Heart Journal February 1, 2008; 29(4): 499-508
- 17 CTT Collaboration, About
- 18 Expert Review of Clinical Pharmacology March 2015:8(2); 201-210
- 19 Carnivore Aurelius June 16, 2019
- 20 Institute for Science in Society April 13, 2015
- 21 The Atlantic April 26, 2012
- 22 Weston A. Price February 23, 2009
- 23 Los Angeles Times July 23, 2017
- 24 UH Hospitals August 17, 2017
- 25 The Free Library, The Truth About Trans Fat, CSPI 1988
- 26 CSPI Timeline for Trans Fat
- 27 Heart.org Our Lifesaving History
- 28 Archives of Internal Medicine 1992 Jul;152(7):1371-2
- 29 American Journal of Clinical Nutrition 2010 Mar;91(3):535-46
- 30 American Journal of Clinical Nutrition March 2010: 91(3); 502-509
- 31 Annals of Internal Medicine March 18, 2014
- 32 Journal of the American College of Cardiology June 17, 2020 [Epub ahead of print]
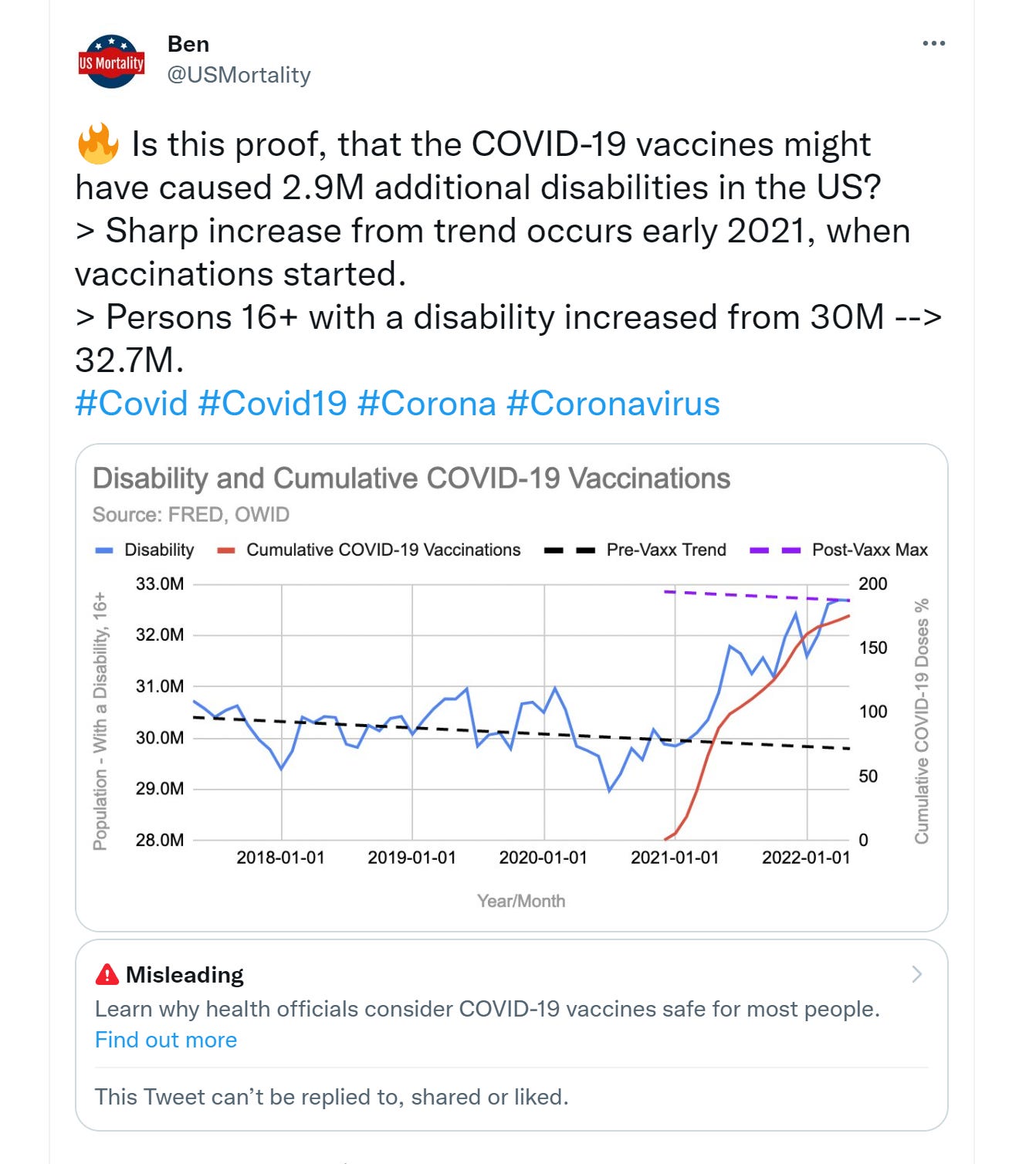
Do vaccine rollouts correlate to disabled americans?
el gato malo – bad cattitude – june 10, 2022
i have long been friends with ben. he’s done a lot of great work, runs a fantastic site on US all cause mortality, and has broken open a number of important issues around covid.
this may be another.
and it was not up for an hour before twitter not only marked the tweet as disinformation and locked ben out of his account all for asking a simple question that pretty much leaps out of this data.
the data comes from the FRED tool run by the st louis federal reserve bank. they are a well respected and high quality government run data source.
hard to see the problem with the data.
clearly, their issue is with the conclusion.
and, well, streisand effect and all, well, it caught my attention because naughty kitties love reading banned books.
correlation does not and cannot prove causality, but it can sure give us some strong hints, especially when we already know how off the charts the adverse event rate from these vaccines have been.
and boy is this timing provocative…
so, being the kind of gato to want to play with the data myself, i downloaded the set and graphed it.
as can be seen, this series was very stable for the prior 5 years. the dotted red line is the average value from 6/16 to 2/20, right before covid starting having effect.
this data comes from the current household survey. the drop for covid is likely a drop in survey response but as can be seen, it rapidly normalized.
then covid vaccination started.
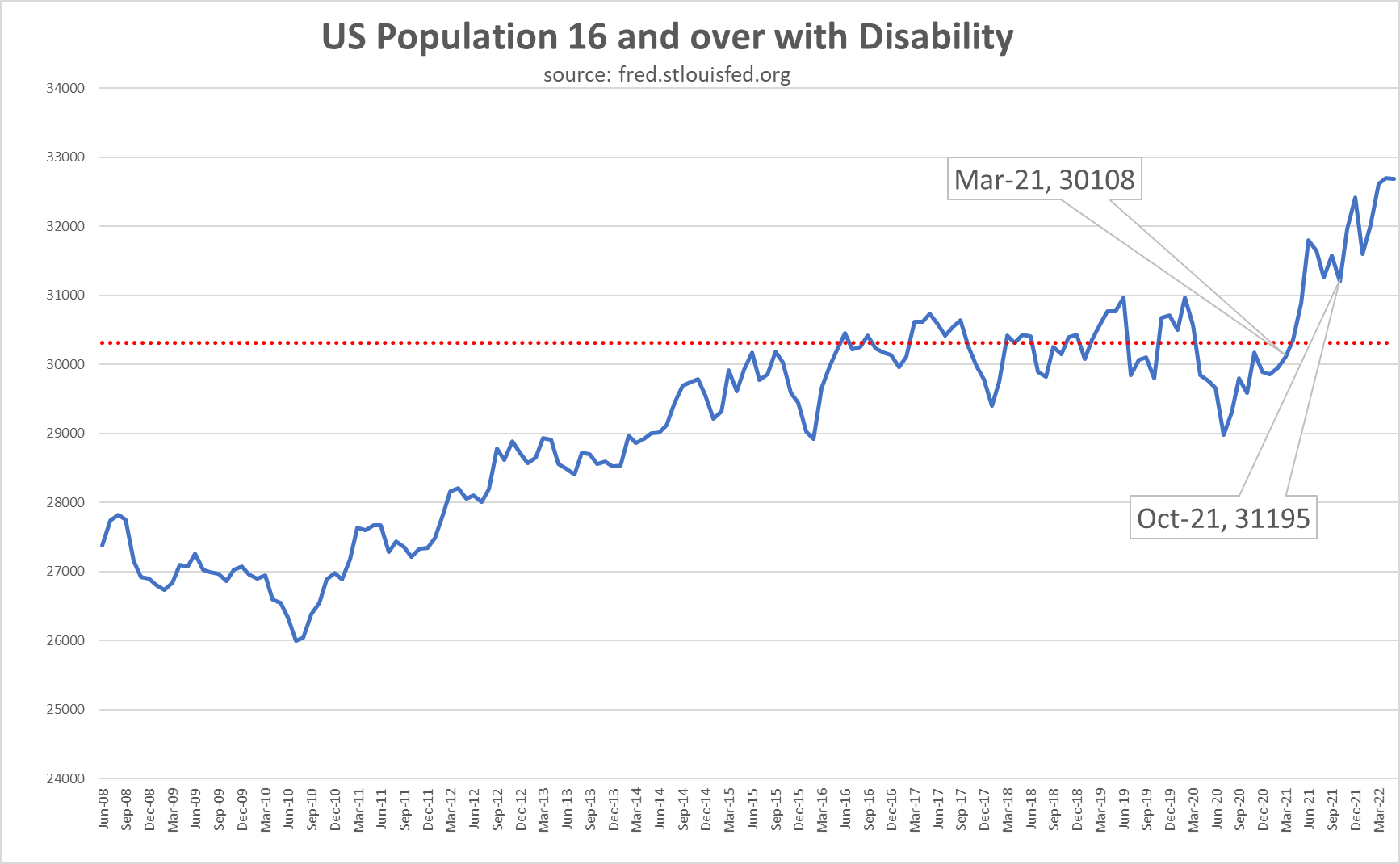
the first callout is when vaccinated reached 1%.
the second is when boosters reached 1%.
i chose this convention because each has a sort of long tail at a very low level leading in but rose rapidly after reaching 1% so it seemed like the best inflection point for maximum relevance.
as can be seen, the timing is highly suggestive.
and it makes sense.
seeing this:
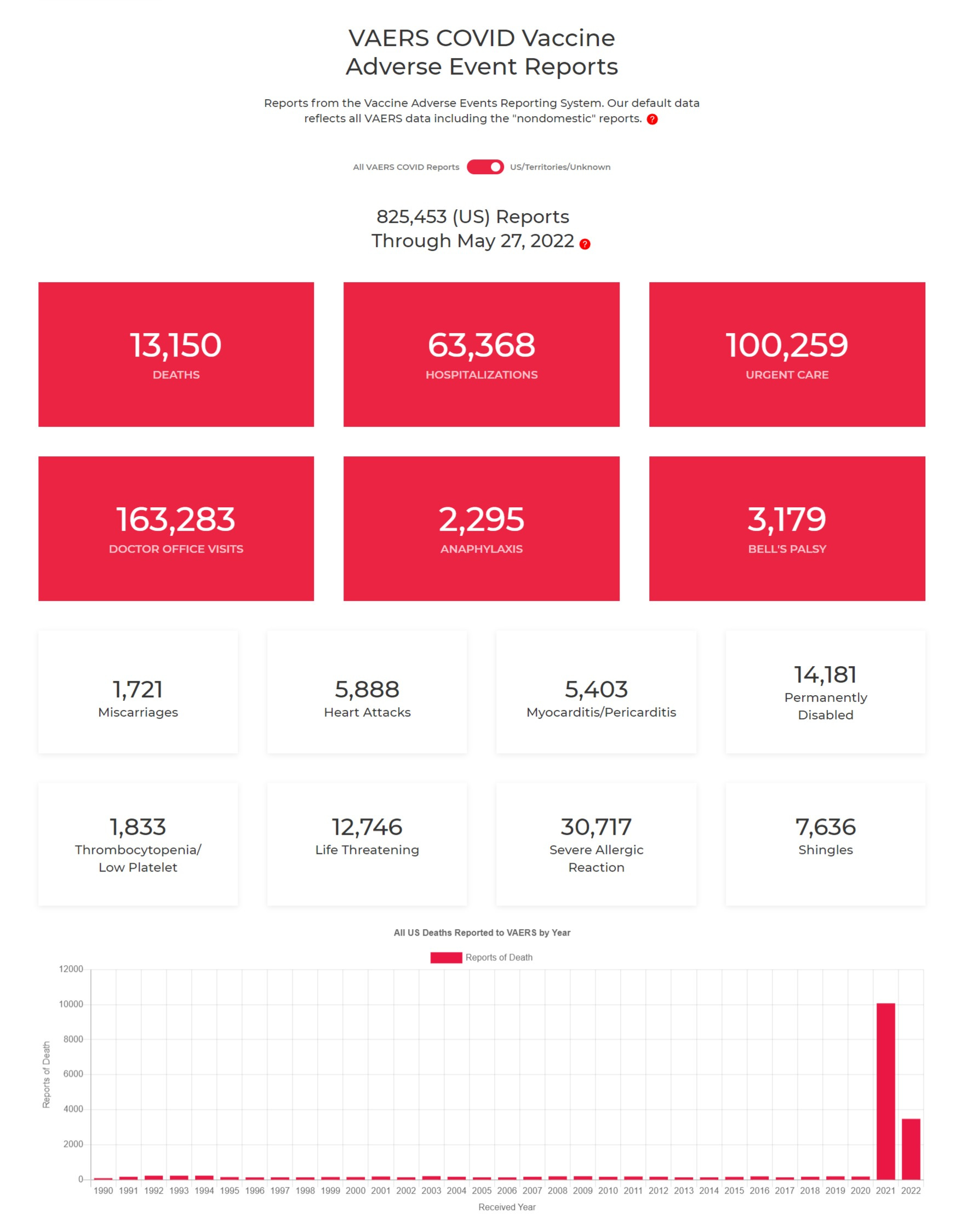
without a rise in disability reports would be surprising. we see 14k permanently disabled in VAERS. and we see a rise in the disabled rolls of 1.8 million. that’s pretty close to the 1-2% capture rate (more like 1%, but also likely capturing other categories as well, so hard to be precise) for reporting we’ve seen around other VAERS issues (besides death which seems to get better counted)
so it feels like we’re in a ballpark here.
and it does not look like “long covid” because the original covid strains were more severe and yet we saw no evidence of this disability spike pre-vaccines.
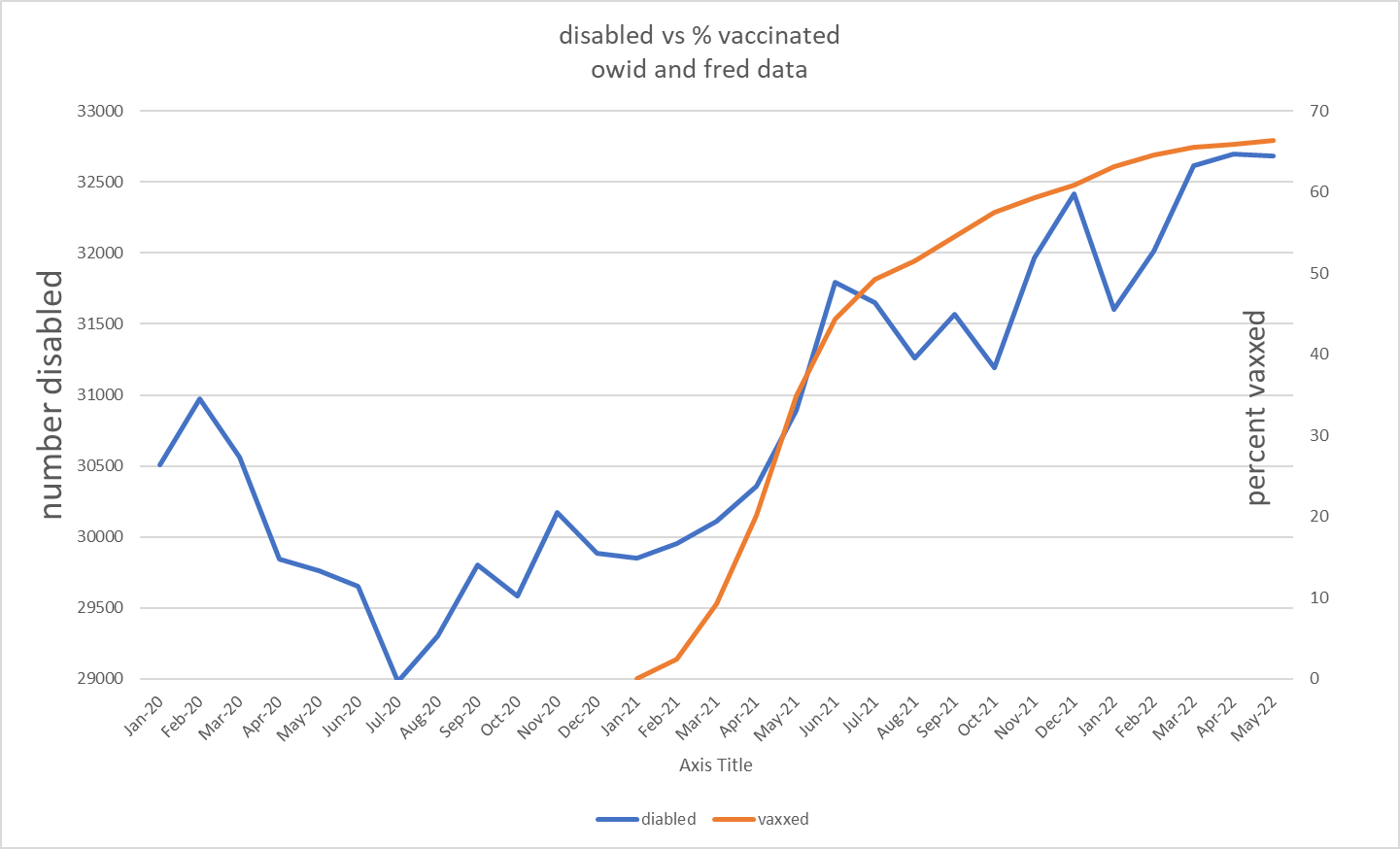
we can zoom in and really see the issue. data used is fred and owid. obviously, there is some chart crime here with the scaling, but the overall relationship is remarkable. this is basically what ben plotted.
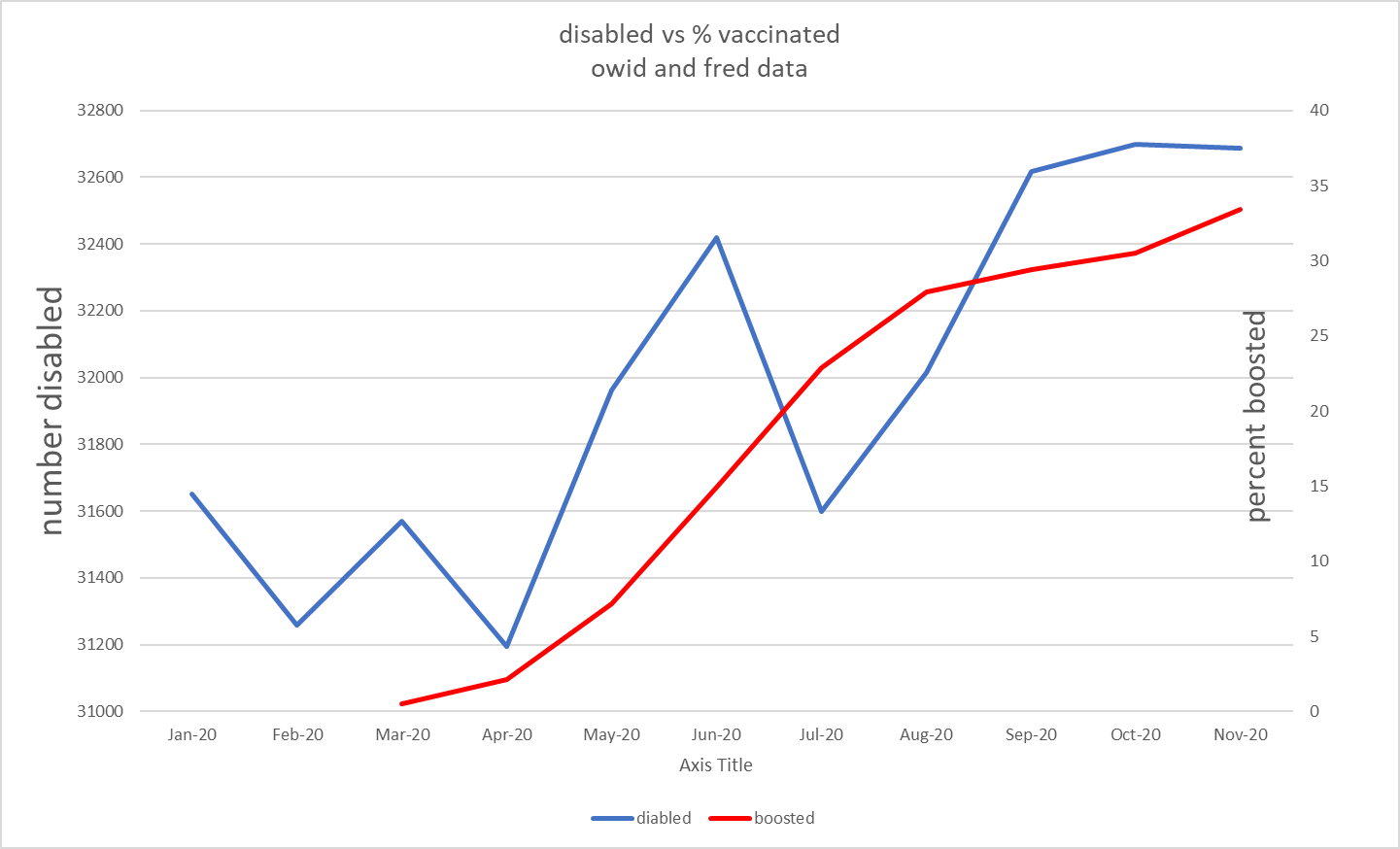
the second sharp upleg in october also interested me so i checked it against this:
it’s easy to take up trending series and lay their scales so they look correlated. the real test is bi-directionality. and this looks to be most damning of all. i took % vaxxed each month and subtracted the prior month to get “% of population vaxxed in month.” this should give us a sense of the people at risk of vaccine complications at any given time. to this i added the same treatment to the booster series to get a total % of population getting a vaccine each month.
i then plotted this series against disability.
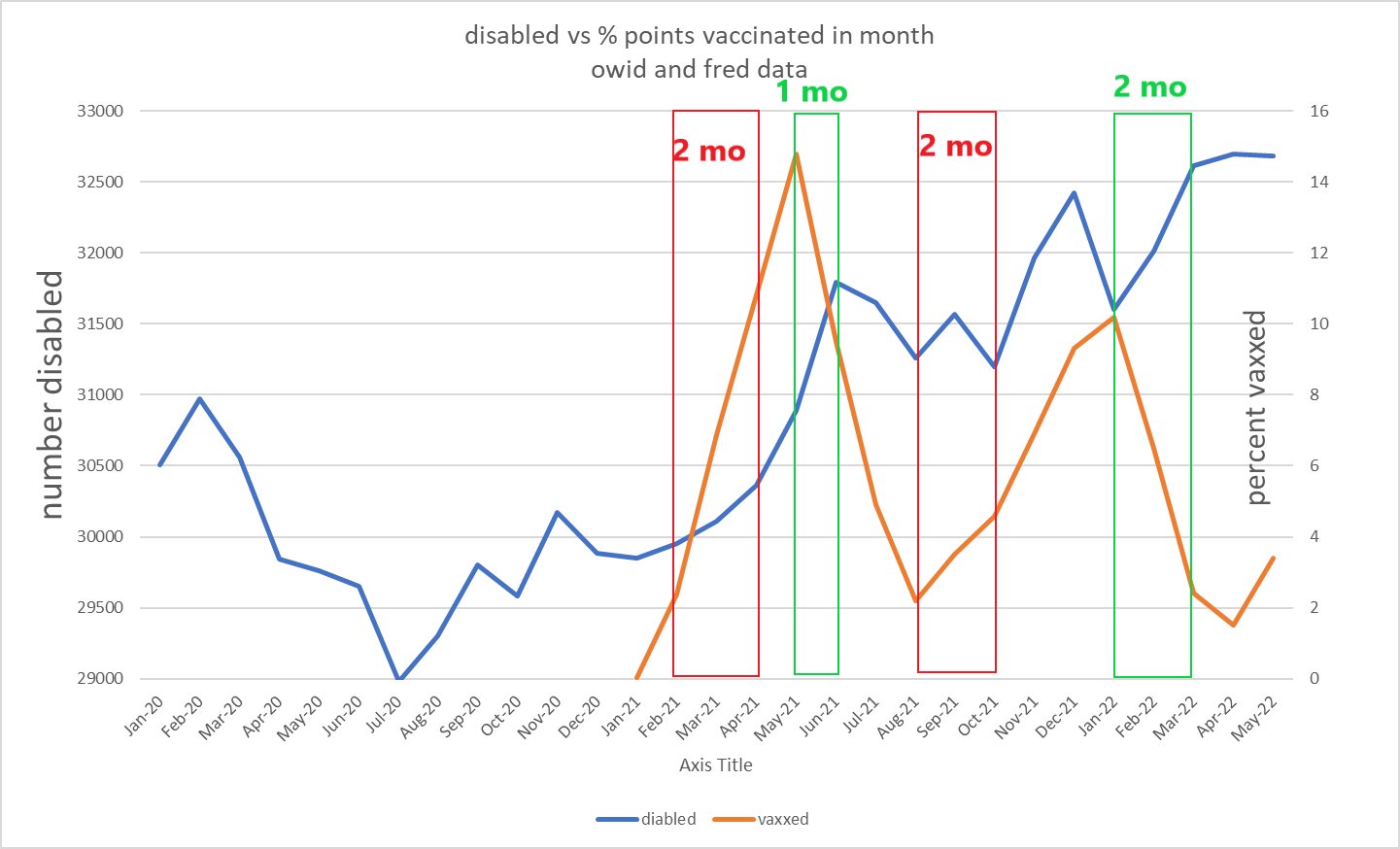
- the vaccination series started to get steep in feb 21. disability got steep in april 21.
- vaccination peaked in may. disability peaked in june.
- vaccination started to rise again after august.
- disability began to rise again after october.
- then vaxx dropped off after jan 2022 and disability flattened out in mar 2022.
2 month lag, 1 month lag, 2 month lag, 2 month lag. 4 separate inflections all tracked in near identical and highly plausible timeframes for vaccine injury. we’re starting to get past “suggestive” here.
this zigs, zags, then zigs again, then zags again all as predicted if it were causal and all with the sort of lag you’d associate with reporting, 1-2 months. (all 2 mo save may-jun 21)
the disability series can be a little noisy month to month, but the big trends are all there.
based on what we know about side effects this looks to be an odds on hypothesis at this point. i can see no better fit to the data.
anyone seeing flaws here? what are we missing? is there another explanation?
“the vaccines just put 1.8 million americans into disability” is a big claim.
i want to stress, this is still a hypothesis and this is my first run through with this data so i want to let people chew on it and see what else emerges before making claims that are too strong.
but this is also REALLY provocative and unless i have really missed something, warrants research and explication, not censorship.
please spread the word and let’s get some eyes on this.
Monkeypox is following the Covid playbook step by step
By Kit Knightly | OffGuardian | June 8, 2022
Monkeypox is back in the headlines as of yesterday, back to work after a short break.
It burst onto the front pages, with concomitant BIG RED NUMBERS and daily case updates a couple of weeks ago, and then went quiet. The press pretty much stopped talking about it.
… until they started again.
Yesterday it was reported that the UK Health Security Agency (UKHSA) has “upgraded” monkeypox to a “notifiable disease”, meaning any positive test must be immediately reported to the government agency.
Ever one for subtlety, the Telegraph’s front page reports this as “monkeypox upgraded to same level as leprosy and the plague”
Across the pond, the US CDC has made the curiously synchronised decision to increase their travel alert on Monkeypox to level 2, which recommends people “practice enhanced precautions”.
Let’s be clear here – the “monkeypox outbreak” is a joke.
Anybody actually taking any of this seriously after the last two years of Covid hysteria needs a major reality check.
At this point you should be assuming any disease “outbreak” is a hoax until proven otherwise. Really proven, not “trust me, I’m an expert” proven.
For those who haven’t got to that stage yet, consider all the ways that monkeypox is following the exact same path as “Covid”…
- The monkeypox outbreak was “predicted” by an exercise a few months before it happened. Just like Covid.
- We’ve seen the narrative re-inforced by rumours that it’s a bio-weapon. These accusations have gone both ways, with the Western press saying Monkeypox is a Russian bio-weapon and Chinese rumours claiming it was deliberately released by the US. Just like Covid
- We’re seeing institutions revising history in order to inflate the potential threat of the disease. just like Covid.
- Monkeypox is being diagnosed via a PCR test. These tests are going to become more widely available as test-makers “seize the new market” and governments plan to “ramp up testing”. Increased testing (with an unreliable test) could artificially inflate “cases”, and feed the panic. Just like covid.
- The monkeypox narrative is being pushed by countries on both sides of the “New Cold War”. Just like covid.
They’re already resorting to the “new variant” headline, that wasn’t a thing for Covid for almost a year. Is this due to desperation or impatience? Who can say, but there must be some reason for the accelerated timeline.
They’re even trying to bring masks back into style by claiming monkeypox may have become airborne.
And, of course, the biggest similarity is in the solution: “vaccines”.
It has already been decided that vaccines originally designed for smallpox work for monkeypox too, and that they are best way to stop the spread of the disease.
Meanwhile, the monkeypox story over at Science tells us…
As monkeypox threat grows, scientists debate best vaccine strategy”
It seems the “experts” can’t decide between “ring vaccination” – where you vaccinate every close contact of a confirmed monkeypox case – or “broader vaccination campaigns”.
Note, they don’t debate if we need a vaccine strategy at all.
The US government is already set to spend at least 180 million dollars on smallpox vaccines.
In Europe, pharmaceutical company Bavarian Nordic is seeing a huge up-tick in its contracts as EU nations treat monkeypox as a “wake-up call”.
So, vaccine manufacturers are set to make a tidy profit… Just like covid.
Whatever eventually comes of this story, it certainly seems that Covid has put a “pandemic” playbook in place, one that each new scare-disease will follow.
It’s all so predictable… and yet the people in charge actually expect us to believe it. Worst of all, some people actually will.
I started by calling monkeypox a joke, and that might be literally true. It’s hard not to feel like they’re making fun of us.
And if that’s the case then, just like at school, the best thing we can do is simply ignore it.
French President Macron: “Vaccinate Everything That Can Be Vaccinated”
By Robert Kogon | Brownstone Institute | June 8, 2022
In another sign that the campaign of C-19 vaccination in Europe is far from over, French President Emmanuel Macron suggested last week that the appropriate response to the crisis in France’s overstrained emergency healthcare services is to “vaccinate everything that can be vaccinated.”
“Vaccinate everything that can be vaccinated,” Macron said, “because we avoid the virus. That’s the best response for unburdening the healthcare system and having a healthy population. So, we’re going to continue to work on this aspect.”
Macron’s word choice has attracted particular attention in the French Twittersphere and other online media, since he literally said that it was necessary to vaccinate “every-thing” (tout ce) and not, say, “everyone” (tous ceux) that can be vaccinated. But even if he had chosen to refer to people as people rather than things, the very idea of “having to vaccinate” people clearly denies them agency – to say nothing of any possibility of informed consent.
A clip of Macron’s remarks, which were broadcast on the French news channel BFM TV, is available here. They form part of more wide-ranging remarks, complete video of which does not appear to be available online.
But another extract posted on the BFM website appears to show the immediate lead-up to the “vaccinate everything” comment and suggests that Macron was responding to a question, more precisely, about whether reintegrating hospital staff who were suspended for having refused to get vaccinated against Covid-19 might help to address staffing shortages in French emergency rooms.
“Reintegrating unvaccinated healthcare workers is absolutely not an answer to the problem,” Macron says, not only because, according to him, they represent just a “tiny minority,” but also because – “if we’re honest” – the unvaccinated staff have “a dubious relationship to care and to ethics.” The French government made Covid-19 vaccination mandatory for healthcare workers in September 2021.
Macron’s remarks on “vaccinating everything that can be vaccinated” come after European Commission President Ursula von der Leyen’s recent call to “further step up vaccination” throughout the EU and the Commission’s issuing of a detailed strategy for doing so starting in the fall.
Robert Kogon is a pen name for a widely-published financial journalist, a translator, and researcher working in Europe. He writes at edv1694.substack.com.
Doctors Sue FDA, Allege Crusade Against Ivermectin ‘Unlawfully Interfered’ With Their Ability to Treat Patients
The Defender | June 6, 2022
Three physicians are suing the U.S. Food and Drug Administration (FDA) for launching what they allege is a “crusade” against ivermectin as a treatment for COVID-19 that “unlawfully interfered” with the doctors’ ability to practice medicine.
In a lawsuit filed June 2, Drs. Robert L. Apter, Mary Talley Bowden and Paul E. Marik argued the FDA acted outside of its authority by directing the public, including health professionals and patients, to not use ivermectin — even though the drug is fully approved by the FDA for human use.
The suit, filed in the U.S. District Court, Southern District of Texas, Galveston Division, also names the U.S. Department of Health and Human Services (HHS), HHS Secretary Xavier Becerra and Robert Califf, acting FDA commissioner.
According to the complaint:
“The FDA generally cannot ban particular uses of human drugs once they are otherwise approved and admitted to the market, even if such use differs from the labeling — commonly referred to as ‘off-label’ use.
“The FDA also can not advise whether a patient should take an approved drug for a particular purpose. Those decisions fall within the scope of the doctor-patient relationship.
“Attempts by the FDA to influence or intervene in the doctor-patient relationship amount to interference with the practice of medicine, the regulation of which is — and always has been — reserved to states.”
The plaintiffs said their lawsuit isn’t about whether ivermectin is an effective treatment for COVID-19. It’s about who determines the appropriate treatment for each unique patient and whether the FDA can interfere with that process.
In their complaint, they site an FDA publication, “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19,” and tweets from the FDA — including one implying that ivermectin is intended only for animals — among examples of the FDA discouraging the use of ivermectin.
The plaintiffs also argued if the FDA is allowed to interfere with the practice of medicine now, using the pandemic as a cover, “this interference will metastasize to other circumstances, destroying the carefully constructed statutory wall between federal and state regulatory powers, and between the FDA and the professional judgment of health professionals.”
“This lawsuit, brought by three eminently qualified physicians, is a welcome development,” said Mary Holland, Children’s Health Defense president and general counsel.
Holland told The Defender :
“These doctors rightfully assert that the FDA, assisted by corporate media, have unlawfully interfered in the doctor-patient relationship and the appropriate treatment for individual patients. Regulating the doctor-patient relationship is an area of well-established state, not federal, law.
“I hope these plaintiffs will enjoin the FDA from continuing to restrict access to ivermectin and from penalizing healthcare practitioners who use this licensed drug for their patients.”
The plaintiffs: well-respected in their field, high success rate treating COVID patients
Apter, who is licensed to practice medicine in Arizona and Washington and has a COVID-19 patient survival rate of more than 99.98%, was referred to the Washington Medical Commission and Arizona Medical Board for disciplinary proceedings for prescribing ivermectin to treat COVID-19.
In a press release, Apter said, “If doctors are freed to treat patients according to their best judgment and unprejudiced evaluation of the medical literature, many thousands more deaths and serious disabilities will be averted.”
Apter said the FDA’s pronouncements against the use of ivermectin “have been the basis for disciplinary actions against doctors, interfere with the doctor-patient relationship, and have had a severe chilling effect on the use of life-saving medication for a deadly disease.”
In the lawsuit, Apter argued that government pressure, “largely through the FDA,” also led pharmacies — especially in large corporate chains — to refuse to fill ivermectin prescriptions for COVID-19, because that position is supported by the FDA.
Bowden, who according to the lawsuit has 40 years of experience in emergency medicine, began recommending ivermectin to treat COVID-19 in early 2020. She treated more than 3,900 patients for COVID-19, with a success rate of over 99.97%.
She said the FDA’s actions regarding ivermectin, specifically its directives to stop using the drug to treat COVID-19, harmed Bowden’s ability to practice medicine and treat patients.
Bowden’s employer, Houston Methodist Hospital, last year forced her to resign by suspending her privileges for spreading “COVID misinformation.”
Bowden said she is “fighting back — the public needs to understand what the FDA has done is illegal, and I hope this suit will prevent them from continuing to interfere in the doctor-patient relationship.”
In an interview earlier this year with The Defender, Bowden said she was all for the COVID vaccines when they first came out — it was only when she started seeing what was happening with all the breakthrough cases that she wondered, “Why am I seeing so many COVID cases among the fully vaccinated?”
Then her patients began having adverse reactions. “If I hadn’t seen that firsthand, I would still think the vaccine was the way to go,” she said.
As the pandemic evolved, Bowden developed protocols for preventing and treating COVID patients. She said she’s seen excellent results.
“The basis of it is ivermectin,” she said. “And also vitamins C and D, quercetin and zinc, and black seed oil. It’s nothing complicated — and it’s just like with anything in medicine — not one size fits all — protocols are guidelines.”
The controversy over prescribing ivermectin was initially “intimidating and isolating,” she said. “I thought I was a little bitty island in a huge ocean, and now I realize that I’m part of at least half a continent.”
Marik, author of more than 750 publications, was professor of medicine and chief of pulmonary and critical care medicine at Eastern Virginia Medical School (EVMS) in Norfolk, Virginia, from 2009 through 2021. He also served as a director of the intensive care unit at Sentara Norfolk General Hospital.
He developed a protocol for EVMS for treating COVID-19, called the EVMS COVID-19 Management Protocol, which included the MATH+ Protocol.
However, according to the lawsuit, Marik was forced to resign from his positions at EVMS and Sentara Norfolk General Hospital for promoting the use of ivermectin — “as well as other safe, cheap, and effective off-label FDA-approved drugs” — to treat COVID-19 following the FDA’s attempts to stop use of those drugs for that purpose.
Marik alleged in the lawsuit that refusing to allow patients to receive effective early treatment for COVID-19 “led to innumerable hospitalizations and deaths, and caused extreme distress for patients, their families, and health professionals.”
Boyden, Gray & Associates, a Washington, DC-based law firm, is representing the plaintiffs.
Ivermectin was developed in the 1970s as a veterinary medicine to treat parasitic diseases in livestock, but a decade or so later was hailed as a “wonder drug” and received approval for human use as a therapeutic against diseases such as river blindness — or onchocerciasis — and lymphatic filariasis, according to Newsmax.
Since 1987, it has been used safely in 3.7 billion doses worldwide. William Campbell and Satoshi Omura won the 2015 Nobel Prize in Physiology or Medicine for their research on the drug.
Studies show ivermectin is associated with lower COVID-19 death rates, but the FDA — with help from mainstream media — continues to state the drug is ineffective for treating COVID.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Featured Video

Russia and China quietly take over natural gas markets in Asia, with Qatar gone
or go to
Aletho News Archives – Video-Images
Book Review
Palantir CEO Calls for Draft to Fight the Empire’s Wars
Involuntary servitude is good for business
By Kurt Nimmo | Another Day in the Empire | April 20, 2026
In 2025, Alex Karp, the CEO of government and military tech contractor Palantir, published The New York Times best-seller, The Technological Republic: Hard Power, Soft Belief, and the Future of the West. The Wall Street Journal praised the book as a cri de coeur, a passionate appeal “that takes aim at the tech industry for abandoning its history of helping America and its allies,” while Wired praised the book as a “readable polemic that skewers Silicon Valley for insufficient patriotism.”
On April 18, 2026, Palantir posted twenty-two points to social media summarizing the book. In addition to taking Silicon Valley to task for insufficient patriotism, advocating a role for AI in forever war, and denouncing the “psychologization of modern politics,” the Palantir post on X declares: “National service should be a universal duty. We should, as a society, seriously consider moving away from an all-volunteer force and only fight the next war if everyone shares in the risk and the cost.”
National conscription, a form of involuntary servitude, and the wars it portends, is good for business, especially for corporations within the orbit of the Pentagon, the CIA, and the national security state. Palantir fits comfortably within this amalgamation. … continue
Blog Roll
 Aletho News
Aletho News- Israeli army blows up school in southern Lebanon in violation of ceasefire
- The desalination front: Water as Israel’s Achilles heel
- Washington cuts flow of US dollars to Iraqi central bank until ‘acceptable’ government formed
- China blames US for diplomatic impasse with Iran, urges it to show ‘sincerity’ in talks
- Iran announces new Hormuz restrictions after US ceasefire violations
- After Islamabad: How the Global South Is Reshaping Eurasian Geopolitics
- Is Trump Going for Armageddon?
- Palantir CEO Calls for Draft to Fight the Empire’s Wars
- Iran War fallout: Russia and China quietly take over natural gas markets in Asia, with Qatar gone
- Hamas dismisses US-backed disarmament plan as ‘collective suicide’
- If Americans Knew
- 5 times Israelis desecrated Christian sites in the past two years
- US running out of weaponry for Israel’s war; Iran has plenty – Daily Update
- Israel is (still) killing aid workers in Gaza
- Catholics finally splitting with Trump over Iran war and Israel
- Israel’s “Black Wednesday” Massacre Leaves Lebanese Families Giving DNA To ID Loved One’s Remains
- ‘I Felt I Was a Monster’: IDF Soldiers Talk About the ‘Moral Injury’ – and the Silence
- ‘I thought I might die’: A Palestinian mother’s account of Israeli detention
- Mom whose daughter was killed by Israeli bulldozer 23 years ago pleaded with Congress to finally stop funding
- Israeli soldier takes sledgehammer to Jesus statue in Lebanon – Daily Update
- Israel employs ‘Gaza tactics’ in Lebanon, destroying 1,000 homes per day – Daily Update
- No Tricks Zone
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
