BMJ Publishes Belated Attack on the Great Barrington Declaration, but It Doesn’t Hit the Target
By Noah Carl • The Daily Sceptic • October 13, 2021
The Great Barrington Declaration, which advocates a focused protection strategy for dealing with COVID-19, was published in October last year – before many countries around the world imposed their winter lockdowns.
Recently, The BMJ Opinion – a journalistic offshoot of the well-known medical journal – published a very belated hit piece against the authors. As you might expect, it’s light on scientific arguments and heavy on tactics like ad hominem, guilt by association and appeals to authority.
The authors, David Gorski and Gavin Yamey, really don’t mince words. For example, they describe the Declaration (which has been signed by hundreds of scientists and healthcare professionals) as a “well-funded sophisticated science denialist campaign based on ideological and corporate interests”.
Not exactly a respectful way to talk about your colleagues. But it’s hardly the first time the Declaration’s critics have sunk to this level. Just last month, Jay Bhattacharya became the subject of a censorious petition which claimed that he “sows mistrust of policies designed to protect the public health”.
Gorski and Yamey begin their article by criticising the Declaration’s authors for collaborating with the American Institute for Economic Research, which they claim is a “libertarian, climate-denialist, free market think tank”.
I’m not sure why this is a ‘gotcha’. Lockdown is about as un-libertarian a policy as you could imagine, so it’s not really surprising that a libertarian think tank would oppose it. And in any case, the Declaration’s website clearly states that the document was “was written and signed at the American Institute for Economic Research”.
Martin Kulldorff has since clarified that the AIER president and board did not know about the Declaration until after it was published. But even if they had done, so what? As Kulldorff notes, universities like Duke and Stanford have received money from the Koch brothers. Should we therefore completely disregard what their academics have to say?
Gorski and Yamey’s next move is to cite social media censorship of lockdown sceptics as evidence that their arguments constitute ‘misinformation’. (Incidentally, that term – which basically means ‘information that’s missing from the mainstream narrative’ – appears no fewer than six times in the article.)
However, this argument relies on circular logic: ‘Something was censored on social media? Therefore, it’s misinformation. How do we know? Well, misinformation is what social media companies censor.’ In reality, of course, the fact that something was censored is no indication whatsoever that it’s factually incorrect.
The authors then allege that when Sunetra Gupta and Carl Heneghan met Boris Johnson in September of last year, they were successful in “persuading him to delay” a ‘circuit breaker’ lockdown, which could have forestalled the second wave of infections.
As historian Phil Magness has already noted, this argument is deficient on two counts. It’s not clear that Gupta and Heneghan did persuade the Prime Minister to shelve the ‘circuit breaker’ idea. But even if they did, there’s no reason to believe that policy would’ve prevented a large number of deaths.
Finally, Gorski and Yamey compare lockdown sceptics to ‘climate science deniers’, insofar as both groups “argue that evidence-based public health measures do not work”. They call for experts to push back against the Great Barrington Declaration by highlighting “scientific consensus”, citing the John Snow Memorandum.
Of course, the pro-lockdown John Snow Memorandum is just another public statement signed by scientists and health professionals. If it constitutes “scientific consensus”, then so does the Great Barrington Declaration. I’m only aware of one attempt to gauge overall expert opinion on focused protection: the survey by Daniele Fanelli.
He asked scientists who’d published at least one relevant paper, “In light of current evidence, to what extent do you support a ‘focused protection’ policy against COVID-19, like that proposed in the Great Barrington Declaration?” Of those who responded, more than 50% said “partially”, “mostly” or “fully”.
Regardless of the exact number of experts who support focused protection, claiming there is a “scientific consensus” against it is simply false. Long before the Declaration itself was published, many scientists had proposed some version of precision shielding. In fact, this was basically the U.K.’s plan until the middle of March, 2020.
On March 5th, Chris Whitty told the Health and Social Care Committee that we are “very keen” to “minimise economic and social disruption”, and mentioned that “one of the best things we can do” is “isolate older people from the virus”.
Another prominent scientist who has argued in favour of focused protection is Sir David Spiegelhalter. In an article published on May 29th, he and George Davey Smith said that we ought to “stratify shielding according to risk” because lockdown is “seriously damaging many aspects of people’s lives”.
They noted that this would require “a shift away from the notion that we are all seriously threatened by the disease, which has led to levels of personal fear being strikingly mismatched to objective risk of death”.
Among the ad hominems, appeals to authority and repeated uses of ‘misinformation’, finding a scientific argument in Gorski and Yamey’s article is not easy. And given that the content’s almost a year out of date, I’m not sure why the authors felt the need to publish it.
In 20 Years of Practicing Medicine, ‘I’ve Never Witnessed So Many Vaccine-Related Injuries’
The Defender | October 13, 2021
In a letter dated Sept. 28 to officials at the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC), an ICU physician detailed her concerns about the adverse reactions, including deaths, she witnessed in people who had received a COVID vaccine.
Dr. Patricia Lee, a licensed physician in California, said her experience with patients harmed by the vaccine “does not comport with claims made by federal health authorities regarding the safety of COVID-19 vaccines.”
In the letter, Lee described observing “entirely healthy individuals suffering serious, often fatal, injuries,” including transverse myelitis, resulting in quadriplegia, pneumocystis pneumonia, multi-system organ failure, cerebral venous sinus thrombosis, postpartum hemorrhagic shock and septic shock.
Lee, a practicing physician for more than 20 years, said she “never witnessed so many vaccine-related injuries until this year.”
Lee told Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, and Dr. Tom Shimabukuro with the CDC’s COVID-19 Vaccine Task Force Vaccine Safety Team, that while “causation is difficult to prove definitively, it is my clinical judgment that each of these injuries were caused by a COVID-19 vaccine, because there was no other plausible explanation for these injuries other than the fact that the patients had recently been vaccinated.”
Lee acknowledged that her report reflects the experience of a single physician. However, she wrote, it appears “statistically improbable” that any one physician should witness this many COVID-19 vaccine injuries if the federal health authority claims regarding the vaccines’ safety were accurate.
“I can no longer silently accept the serious harm being caused by the COVID-19 vaccines,” Lee concluded. “It is my sincere hope that the reaction to this letter will not be to focus on me, but rather to focus on addressing the serious safety issues with these products that, without doubt, you have either missed or are choosing to ignore.”
Since the issuing of the original letter, Lee’s attorneys sent another letter to the CDC and FDA saying that the agencies’ “failure to respond is highly concerning,” adding that they are seeking a response so they can “arrange a discussion and information gathering session between Dr. Lee and the appropriate representatives at the CDC and FDA.”
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
SPECIAL BROADCAST: DR. ROBERT MALONE ON HIS MRNA CREATION
STEW PETERS | OCTOBER 13, 2021
Stew Peters sat down with Dr. Robert Malone, the creator of the mRNA technology being used in the shots being falsely referred to as “vaccines”, which have proven to be dangerous, and in many cases DEADLY.
Biden praises Southwest Covid vaccine mandate amid cancelation chaos, says it will help ‘eliminate this disease’

© REUTERS/Leah Millis
RT | October 14, 2021
In an address from the White House, President Joe Biden praised companies like Southwest Airlines enforcing his Covid-19 vaccine mandate, despite the CEO seemingly rebuking the requirement the day before.
Addressing the government’s effort to battle the coronavirus pandemic on Thursday through vaccine mandates, Biden praised private companies that have already been “stepping up” to combat misinformation about the Covid-19 vaccine and the implementation of their vaccine mandates.
“Southwest Airlines … the head of the pilots’ union and its CEO dismissed critics who claim vaccination mandates contributed to flight disruptions,” Biden said, referring to mass cancelations at Southwest Airlines that peaked on Sunday, shortly after the company began enforcing the vaccine mandate put forth by the president.
The company and the White House have denied the mandate and ensuing staffing shortages caused them to delay a third of their flights in the US. White House Press Secretary Jen Psaki even deemed the mandates “good for the economy” following the cancelations and speculation by critics.
In his address, Biden went on to praise school board members, doctors, and other healthcare workers for battling “misinformation” about vaccines.
“All of these efforts,” Biden said of the companies and individuals facing “misinformation” about vaccines and mandates, “are going to help us continue moving the dial to eliminate this disease.”
Biden’s comments came shortly after Southwest CEO Greg Kelly appeared to distance himself from the mandate, despite the company saying there was no connection between their scheduling troubles and the requirement.
The CEO told CNBC he had never “been in favor of corporations imposing that kind of a mandate,” though adding again it has nothing to do with the cancelations.
Biden pushed back against the divisive response his vaccine mandates have received from the public, saying mandates “should not be another issue that divides us” and is only part of the larger effort to battle the virus and get the still lagging, according to the president, vaccination rate up.
“Mandates work,” the president said, and companies like Southwest that have already implemented them prove that, he added.
The Department of Labor will be requiring all businesses with 100 or more employees to require Covid vaccinations, an order multiple companies have already said they will defy.
House of Commons Covid Report Gets Some Things Right, Most Things Wrong
By Toby Young • The Daily Sceptic • October 12, 2021
On Monday evening two House of Commons select committees – the Science and Technology Committee and the Health and Social Care Committee – published a joint report on the Government’s handling of the COVID-19 pandemic that was predictably damning. It was published in time to make the following day’s front pages – “Britain must learn from ‘big mistakes’ on Covid, says report”, reported the Times on its front page – but not in time for newspaper reporters or broadcast journalists to properly assess its findings. Not that that stopped all the usual suspects from using it as a stick to beat the Government with. For instance, Labour’s Shadow Health Secretary Jonathan Ashworth told the BBC that the “damning” findings showed that “monumental errors” had been made and called for the public inquiry – scheduled for next spring – to be brought forward.
The authors of the report say in the Executive Summary that the reason they’ve published it now, when there are still a large number of ‘known unknowns’ as well as ‘unknown unknowns’, is because we urgently need to learn from what the Government got right and what it got wrong so we are better prepared for the next pandemic, which might come along at any moment. But if it’s too soon to say what was a mistake and what wasn’t, that argument collapses. Indeed, a premature report that draws the wrong conclusions, e.g. that the Government didn’t lock down in March of last year early enough, which is one of the main findings of this report, is worse than useless since it may encourage future Governments to repeat the same mistakes.
I’ve now read the report – yes, all 145 pages – so you don’t have to.
What the report gets right
- It criticises the Government for discharging elderly patients from hospitals into care homes without testing them first to see if they had COVID-19 and without putting any measures in place in care homes to mitigate the impact of that policy, as well as for the lack of PPE in care homes. The report says these errors “led to many thousands of deaths which could have been avoided”. Hard to argue with that, although one of the oddities of the report is that it criticises the lack of infection control in care homes, but not in hospitals. Weird, given that ~20% of cases over the course of the U.K.’s epidemic have been hospital-acquired infections.
- The authors praise the RECOVERY trial for carrying out large randomised control trials of different COVID-19 treatments and identifying dexamethasone as an effective treatment. That too seems right.
- The report highlights the disproportionately high Covid death rates among black, Asian and minority ethnic populations and acknowledges that part of the explanation for that may be biological differences between those populations and the white British population. Even acknowledging that genetic factors may be part of the reason for these disparities makes a refreshing change. Unfortunately, the report goes on to play down these biological differences and claims that social, economic and health inequalities are much bigger factors.
- It criticises hospitals and care homes for issuing ‘Do Not Attempt CPR’ notices to patients/clients with learning disabilities and autism, often without the consent of their families. No argument there.
- Rather than blame Boris and other senior members of the Government for the decision not to lock down before March 23rd 2020, the report emphasises that they were just following the recommendations they were being given by their scientific advisors. As I’ve pointed out before, that is correct.
- The report is at least ambivalent about how effective a two-week ‘circuit breaker’ would have been in England in September of 2020.
It is impossible to know whether a circuit breaker in the early autumn of 2020 would have had a material effect in preventing a second lockdown given that the Kent (or Alpha) variant may already have been prevalent. Indeed such an approach was pursued in Wales, which still ended up having further restrictions in December 2020.
Unfortunately, having written this, the authors then go on to say:
It is likely that a “circuit break” of temporary lockdown measures if introduced in September 2020, and earlier lockdown measures during the winter, could have impeded the rapid seeding and spread of the Kent variant.
Make up your mind guys!
What the report gets wrong
- The report claims that the U.K.’s Pandemic Preparedness Strategy wasn’t fit for purpose because it prepared us for “an influenza-like pandemic” rather than a more serious infectious disease that was spread, in part, by asymptomatic transmission. Professor Devi Sridhar, who gave evidence to the joint committees, is quoted as saying the mistake our Government made was to assume COVID-19 was “just like a bad flu”. In fact, it was like a bad flu, as judged by the latest estimates of the infection fatality rate, and the jury’s still out on whether asymptomatic people who test positive for Covid are infectious.
- One of the reasons the Government didn’t lock down before March 23rd, according to the authors, is because its scientific advisors were guilty of following the flawed playbook of the Pandemic Preparedness Strategy. In particular, the initial advice was to try to ‘manage’ the spread of the virus through the general population rather than to suppress it altogether, which the authors believe would have been the correct strategy. They claim the Government didn’t realise this sooner because it had failed to learn the lessons of the SARS, Swine Flu and MERS pandemics and embed those lessons in its strategy. But, surely, one of the lessons of those pandemics is that national lockdowns aren’t necessary to contain pandemics – and that advice was embedded in the U.K. Government’s strategy document. The mistake the Government made was not to initially follow that advice; the mistake was to stop following it on March 23rd. The only time a government has tried quarantining entire regions as a strategy to mitigate the impact of a viral outbreak prior to 2020 was in Mexico in 2009 when something like a lockdown was imposed on April 27th in Mexico City, the State of Mexico and the State of San Luis Potosí. That was policy abandoned on May 6th because of the mounting social and economic costs.
- Bizarrely, the authors of the report claim the reason the British Government didn’t abandon the Pandemic Preparedness Strategy sooner was because of “groupthink”. But, surely, the reason for putting a carefully thought out strategy document in place, incorporating the lessons from the mistakes made during previous pandemics, was precisely to avoid Government decisions being influenced by groupthink. And that approach was successful until mid-March, at which point Boris Johnson and his closest political allies abandoned it and decided to copy what other Western leaders were doing, i.e. lockdown. In other words, it was groupthink that was responsible for the disastrous U-turn, not the comparatively sensible initial approach.
- One of the main conclusions of the report is that the Government should have locked down earlier than it did – that’s one of the “big mistakes” in all the headlines – and they quote Professor Neil Ferguson to that effect:
The initial U.K. policy was to take a gradual and incremental approach to introducing non-pharmaceutical interventions. A comprehensive lockdown was not ordered until March 23rd 2020 – two months after SAGE first met to consider the national response to COVID- 19. This slow and gradualist approach was not inadvertent, nor did it reflect bureaucratic delay or disagreement between Ministers and their advisers. It was a deliberate policy – proposed by official scientific advisers and adopted by the Governments of all of the nations of the United Kingdom. It is now clear that this was the wrong policy, and that it led to a higher initial death toll than would have resulted from a more emphatic early policy. In a pandemic spreading rapidly and exponentially every week counted. The former SAGE participant Professor Neil Ferguson told the Science and Technology Committee that if the national lockdown had been instituted even a week earlier “we would have reduced the final death toll by at least a half”.
- In fact, it’s far from clear that “this was the wrong policy” or that it “led to a higher initial death toll”. The authors of this report take it for granted that – in the words of Professor David Paton – “governments can turn infections on or off like a tap by imposing or lifting restrictions”, when all the real-world data we’ve accumulated in the past 18 months suggests that is hopelessly naive (see these 30 studies, for instance). Governments around the world, including ours, have been guilty of wildly over-estimating the impact of non-pharmaceutical interventions on the spread of the virus.
- In the British case, there’s no reason to believe that locking down earlier would have reduced the final death toll at all, let alone by half. As David Paton points out, the Czech Republic locked down on March 16th, imposed hard border controls and rolled out the first national mask mandate in Europe. Yet it had a second surge in the Autumn of 2020, prompting it to lock down again, and then an even bigger one in December, leading to a third lockdown. Cases surged again in Czechia in February and March of this year and, six months ago, it had the second-highest per capita Covid death toll in the world, according to Reuters.
More damning still is the comparison with Sweden, which didn’t lock down at all in 2020 and, as of today, is ranked 50th in Worldometers’ table ranking countries according to per capita deaths. The U.K., by contrast, is ranked 25th.

- There are only three mentions of Sweden in this report, two of them in a single footnote. Any assessment of the U.K. Government’s response to the pandemic that fails to compare it with that of the Swedish Government – particularly one advocating we should have locked down sooner and for longer – doesn’t deserve to be taken seriously.
- The report’s authors take at face value the “reasonable worst-case” scenarios that various modellers (including a sidekick of Dominic Cummings’) came up with in mid-March to show that if the Government continued to follow Plan A, i.e. the Pandemic Preparedness Strategy, the NHS was on track to become overwhelmed many times over. Here is Matt Hancock giving evidence on June 8th 2021, appealing to a prediction of “slightly below” 820,000 deaths, absent a lockdown:
I asked for a reasonable worst-case scenario planning assumption. I was given the planning assumption based on Spanish flu, and it was signed off at Cobra on January 31st. That was a planning assumption for 820,000 deaths. […]
In the week beginning March 9th, what happened is that the data started to follow the reasonable worst-case scenario. By the end of that week, the updated modelling showed that we were on the track of something close to that reasonable worst-case scenario. I think the numbers were slightly below that, but they were of a scale that was unconscionable.
- Rather than just take those projections at face value, couldn’t the House of Commons committees have interrogated the models a little bit? The report’s most damning criticism – that the Government’s delay in imposing the first lockdown resulted in thousands of unnecessary deaths – is contingent on not questioning those forecasts. In light of SAGE’s over-estimate of the likely uptick in cases following the easing of restrictions on July 19th of this year, as well as its more recent over-estimate of hospitalisations this autumn, wouldn’t it have been prudent to scrutinise those models? That’s a particularly glaring omission, given that the authors of the report criticise members of the Government for not challenging the scientific advice they were given: “Those in Government have a duty to question and probe the assumptions behind any scientific advice given, particularly in a national emergency, but there is little evidence sufficient challenge took place.” Why do “those in Government” have a duty to do this, but not those serving on select committees who are supposed to be holding the Government to account?
- In case further evidence is required that the authors of the report have credulously lapped up the doom-mongering of SPI-M and others, consider this passage:
It seems astonishing looking back that – despite the documented experiences of other countries; despite the then Secretary of State referring to data with a Reasonable Worst Case Scenario of 820,000 deaths; despite the raw mathematics of a virus which, if it affected two-thirds of the adult population and if one percent of people contracting it died would lead to 400,000 deaths – it was not until March 16th that SAGE advised the Government to embark on a full lockdown (having said on March 13th that “it was unanimous that measures seeking to completely suppress the spread of COVID-19 will cause a second peak”) and not until March 23rd that the Government announced it.
- Note the appeal to an IFR of 1% when even Neil Ferguson’s team at Imperial College, which predicted 510,000 deaths if the Government stuck with Plan A in its famous March 16th paper, assumed an IFR of 0.9%. In fact, a WHO bulletin put the IFR at 0.23% as long ago as October 2020.
- This unwillingness to interrogate the modelling data that underpins the report’s conclusions is particularly odd, given that the authors acknowledge the limitations of modelling elsewhere – “Models can be useful and informative to policymakers, but they come with limitations” – and at one point try to blame the delay in lockdown down on an “overreliance on specific mathematical models”! Again it’s a case of one rule for me and another for thee.
- The report compares the response of the British government in the first months of the pandemic unfavourably to that of various East Asian and South East Asian governments, but overlooks the fact that many Asian countries that successfully suppressed infection by closing borders at the beginning of 2020, and rolling out successful test, trace and isolate programmes, are now in the grip of devastating waves in spite of having vaccinated large swathes of their populations. That suggests their non-pharmaceutical interventions only succeeded in postponing the impact of SARS-CoV-2, not avoiding it. (It also fails to note that these supposed role models didn’t issue stay-at-home orders, close schools or shutter businesses in their initial responses to the pandemic.)
- The report criticises the Government for stopping community testing in March 2020 due to PHE’s lack of testing capacity and praises Matt Hancock for setting the 100,000 tests a day target to galvanise the system into massively ramping up that capacity. Indeed, the authors claim that had a proper test-and-trace system been in place at the beginning of 2020, the initial lockdown might have been avoided. That, too, is a shaky assumption. After all, the Government has spent £37 billion and counting on a ‘world-beating’ test, trace and isolate programme but that didn’t stop us locking down for a second and third time. The authors of the report acknowledge this point, but blame Baroness Harding for not doing a better job of running NHS Test and Trace. That seems a tad harsh, particularly as the authors repeatedly say – Uriah Heap-like – that it’s not their intention to apportion blame for the mistakes they’ve identified.
- The report praises the speed at which the Nightingale hospitals were created, although it acknowledges that, for the most part, they weren’t used. But the reason they weren’t used is partly because the NHS lacked the trained employees to staff them with – ICU nurses, for instance. Perhaps if they’d been built with less speed – at a cost to the taxpayer of roughly half a billion pounds, don’t forget – the Government would have had time to spot this obvious flaw in the plan. Or, more realistically, those aware of it from the start would have had more time to organise and obstruct this expensive PR stunt.
- The authors praise the Government – and the NHS – for at no point running out of ICU beds and becoming overwhelmed, as the health system did in some parts of Italy during the first phase of the pandemic. But given the enormous cost of protecting the NHS – both in terms of seriously ill people who were either discharged or went untreated, as well as the collateral damage inflicted by the lockdowns on the economy, education, family life, mental health, etc. – it’s impossible to say whether prioritising the NHS at the expense of absolutely everything else was in fact the right strategy. To bottom that out you need to do some cost-benefit analysis, of which there is precisely none in this report.
- The report concludes by praising the Vaccine Taskforce under the leadership of Kate Bingham and highlights the ‘success’ of the U.K.’s vaccine programme – “one of the most effective in Europe and, for a country of our size one of the most effective in the world”. But they ignore the fact that the efficacy of the Covid vaccines is much less impressive than the initial trial data indicated and looks less impressive with each passing week, something Dr. Will Jones has been meticulously documenting for the Daily Sceptic. So was the massive Government expenditure on the development and trialling of home grown vaccines, as well as procuring hundreds of millions of vaccines manufactured overseas, worth it? One notable omission from the report is any acknowledgement of the risks associated with a fast-tracked vaccine approval process – it just breathlessly praises the speed with which vaccines were made available to the public and expresses the hope that “in the future this could be conducted in much shorter time still”.
Conclusion
This is a pretty feeble document that seems to have been written with an eye on getting Jeremy Hunt and Greg Clark – the chairs of the two select committees involved – on the BBC news rather than making a serious contribution to understanding what the Government got right and what it got wrong over the past 18 months. It’s hard to argue with some of its findings, but its headline conclusion – that the Government should have locked down earlier – isn’t based on any serious analysis, let alone a careful consideration of the evidence that seems to point in the opposite direction. Talk about groupthink!
I hope the official inquiry, when it comes, is a bit more intellectually weighty than this.
We need a Covid champion to defy Big Pharma like the thalidomide heroine
By Mary McGreechin | TCW Defending Freedom | October 13, 2021
IN 1960, Frances Oldham Kelsey prevented thousands of American babies from facing a life of severe disability.
A medical officer with the US Food and Drugs Administration (FDA), Kelsey refused to buckle under relentless pressure from the pharmaceutical company Merrell to approve the drug thalidomide for use as a sedative and, off-label, as a treatment for morning sickness.
From 1957, the drug had been used in Europe to ease extreme nausea in the early stages of pregnancy. But by 1961, mounting reports from concerned doctors revealed devastating birth defects in the babies of women who had taken thalidomide.
Determined to break into the lucrative American drug market, Merrell had claimed stringent testing showed the drug to be safe as well as efficacious.
Kelsey, however, was suspicious of incomplete data and the omission of tests on the drug’s prolonged use and refused to give her approval. Despite harassment and intimidation by the company – ‘most of the things they called me you wouldn’t print’ – Kelsey had remained resolute.
Today, as the Covid agenda aims to vaccinate every man, woman and child, minimising, or ignoring, often fatal side-effects, we need a Frances Kelsey to say: ‘No.’ Or even: ‘Not yet.’ Despite some courageous voices within the medical community speaking out at great personal cost, no influential figure has voiced the level of dissent needed to halt this programme.
Medical advances have, undeniably, delivered life-enhancing and life-saving treatments. Yet countless lawsuits against the pharmaceutical industry demonstrate that medicine can have an iatrogenic (illness-causing), as well as a therapeutic, effect. In the US alone, billions of dollars are paid annually in damages by pharmaceutical companies.
The industry has sought to temper such negative perceptions by cultivating a philanthropic image, portraying itself as a benevolent entity driven by altruism rather than a competitive industry whose investors salivate at ever-increasing share prices.
Despite these endeavours, it is astonishing that a large proportion of the public have failed to be concerned that drug companies which have been fined astronomical sums in multiple lawsuits have been granted liability immunity on Covid vaccines. With pharmaceutical firms typically afforded limited liability protection, this indemnity has been described as ‘very rare.’
Should we be surprised at the lack of public suspicion? The NHS has been elevated to such a degree that any condemnation of this behemoth is considered blasphemy. A 2020 Ipsos MORI poll revealed that more than 90 per cent of Britons trusted doctors and nurses ‘to tell the truth.’
Yet medics may be untruthful, or unaware of the full facts behind the medicine they prescribe. UK doctors believed thalidomide could be given ‘with complete safety to pregnant women and nursing mothers without adverse effect on mother or child’, yet it was later acknowledged that no tests were done involving pregnant women.
The effect of Covid vaccines on fertility and the unborn child are unknown. However, more than 30,000 women have, at present, reported changes in their menstrual cycle post-vaccination.
The vice-president of the Royal College of Obstetricians and Gynaecologists stated: ‘We support calls for more research to understand why women may be experiencing changes to their menstrual cycle after having the vaccine.’ Stable door, horse and bolted come to mind.
And whilst pregnant women were excluded from the Covid vaccine trials, the Journal of the American Medical Association (JAMA) had these reassuring words to ‘pregnant people’: ‘Reproductive toxicity studies with the Moderna vaccine in rats haven’t uncovered any worrisome signals.’
Are we to place our trust in pharmaceutical companies whose employees’ emails reveal such statements as:
‘I am not 100 per cent comfortable with this data being made publicly available.’
‘Thus far we have buried trials 15, 31, 56 … how do we face the outside world when they begin to criticise us for suppressing data?’
‘Lisa has done a great “smoke and mirrors” job.’
All this correspondence was made public when litigation against AstraZeneca’s anti-psychotic drug Seroquel began. The company, now most famously known for the development and production of Covid vaccines, faced a major lawsuit in 2009 brought by thousands of Seroquel users who claimed they had developed diabetes whilst taking the drug.
The damning emails proved the pharmaceutical giant had been aware of the risk a decade earlier. Moreover, AstraZeneca had suppressed research which showed its earlier anti-psychotic treatment, Haloperidol, was more effective, and much cheaper, than Seroquel.
Employee John Tumas messaged concerns to colleagues that ‘our own analysis supports the “view out there” that we are less effective than Haloperidol.’
Promoting expensive treatments over cheaper alternatives has also caused debate regarding Covid-19. Those advocating for the use of Ivermectin, more commonly used as an anti-parasitic in animals, to treat the virus, have been relentlessly mocked. But studies have shown the drug can provide ‘an increase in clinical recovery … and a decrease in mortality rates even when used in patients with severe Covid-19.’
Yet a trial conducted on those with mild symptoms concluded it had little effect. Doctor Eduardo Lopez-Medina published his findings in JAMA, maintaining that Ivermectin had delivered negligible benefits.
However, a ‘conflict of interest disclosure’ revealed Dr Lopez-Medina was in receipt of grants and ‘personal fees’ from pharmaceutical giants GlaxoSmithKline, Janssen and Sanofi Pasteur – all involved in the production of Covid-19 vaccines.
Countless stories have emerged in the past 18 months which should raise serious questions over transparency and truthfulness within the medical field – from doctors wrongly claiming intensive care units are full of unvaccinated 20 and 30-year-olds on ventilators, to hospital matrons inventing stories of children’s wards full of Covid patients.
And yet we are expected to have faith that such medics, and the pharmaceutical industry, have our best interests at heart in their pursuit of global vaccination against Covid-19.
Like Frances Oldham Kelsey, we should remain steadfast against coercion and duress. We should ask more questions and seek more answers. If we do not like the answers we find, then we must hold the line. For our own sake and that of our children.
Preventing Covid Infections Among Healthy Children Is Pointless
By Noah Carl • The Daily Sceptic • October 12, 2021
Thanks to school closures, children missed out on in-person teaching, as well as regular face-to-face interaction with their friends, for the best part of a year.
The main rationale for closing schools was to help ‘flatten the curve’ of total infections, and thereby prevent the NHS from being overwhelmed. (We’ve known since early on in the pandemic that children’s risk of death from Covid is vanishingly small – lower even than their chance of dying from seasonal flu.)
However, evidence suggests that neither lockdowns in general, nor school closures in particular, were necessary to prevent healthcare systems from being overwhelmed; and the harms from school closures were substantial.
Once the Government conceded it was time for schools to reopen, there came a new justification to keep them closed: protecting teachers. Yet studies have repeatedly shown that teachers are not at elevated risk of death from Covid.
Even after schools finally did open up, pupils faced a rigamarole of mask mandates, regular testing and stints of mandatory self-isolation. Since the vast majority of vulnerable people (and most teachers) had been vaccinated by this point, it’s unclear exactly why things couldn’t just return to normal.
As far as one can discern, the specific rationale seems to be: ‘something to do with case numbers and/or long Covid’. Why we should care about case numbers in an age-group that faces a higher risk of death from season flu has not been explained.
As to long Covid, the latest data suggest that only a tiny number of children (less than 2%) continue to report symptoms 12 weeks after infection. One study found that symptoms were no more common among children who’d had the virus than among those who’d never been infected.
Despite all this, demands for more restrictions in schools can still be heard. On 3rd September, scientists associated with Independent SAGE, as well as various other individuals and organisations, co-signed a letter in The BMJ Opinion calling for the Government “to protect children, our wider communities, and the NHS”.
Their “nine point plan” includes such measures as: reinstating face coverings; offering vaccines to all 12–15 year-olds; and reinstating contact tracing “with a strict policy on mandatory isolation”.
But according to Chris Whitty, “roughly half” of children have already have Covid, and it’s reasonable to assume that “the great majority” are “going to get it at some point” because “this is incredibly infectious”.
Now that almost all vulnerable people have been vaccinated, why are we trying to stop children getting the virus if “the great majority” of them are going to get it at some point anyway? Offering the vaccine to those with an underlying health condition makes sense, but apart from that, why do anything at all?
In fact, shouldn’t we actively encourage young people to get the virus, so as to build up more population immunity before the winter?
Ex-Pfizer Employee Warns Vaccine Increases COVID By Over 300%
By Lance D Johnson | Humans Are Free | October 1, 2021
The fraudulence of covid-19 vaccines is on full display, and the evidence is sitting right out in the open. The full FDA approval for Pfizer’s COMIRNATY vaccine contained clinical proof that the inoculation increases COVID infection by over 300 percent!

Varitage.com
A former Pfizer employee named Karen Kingston is blowing the whistle on her former employer. Kingston is currently a pharmaceutical marketing expert and biotech analyst. When she scrutinized the full FDA approval for COMIRNATY, she found blatant fraud in Pfizer’s clinical studies.
FDA Approves Pfizer’s Covid-19 Vaccine, Even Though It Increases Infection By 300 Percent
Kingston brought forth a Briefing Document from the FDA’s advisory committee meeting that took place on September 17, 2021. The title of the document is, “Application for licensure of a booster dose for COMIRNATY (COVID-19 Vaccine, mRNA).” The document includes clinical studies conducted by Pfizer. These studies track the durability of immunity offered by the COMIRNATY vaccine and compare it to immunity observed in unvaccinated people.
“If you get the Pfizer vax, you’re more likely to get COVID” said Kingston, “So, when they weren’t injected, their infection rate was 1.3% and when they got injected, it was 4.34%. It went up by over 300%.” How could the FDA have glossed over this evidence and approved blatant fraud?
Since the vaccine was officially approved, the federal government started applying pressure on businesses across the US, threatening them with extortion and fines if they do not impose vaccine mandates on their employees.
The covid-19 vaccines have been injected almost 225 million times into the arms of Americans, causing severe injury and death along the way. Real world observations also support clinical data showing that the vaccines increase one’s susceptibility to covid-19.
In fact, the vaccines increase viral load in the nostrils of the vaccinated. An August 26 article by Dr. Peter McCullough shows that the covid vaccines allow the vaccinated to carry 251 times the viral load of covid-19 in their nostrils, turning them into the asymptomatic super spreaders they once feared.
Pfizer Studies Show That Being Unvaccinated Offers Greater Protection
Medical freedom rights attorney, Thomas Renz, went public with the Pfizer fraud. The Pfizer study involved over 36,000 people. Those who were injected earlier in the study were more likely to come down with covid infections later on, showing a clear trend of waning immunity. Those put in “high priority” groups, who were vaccinated earlier on, have a 36 percent greater chance of infection, compared to the group that vaccinated later on.
The group that vaccinated later on went unvaccinated for 5.1 months longer than the group that got vaccinated early on. This placebo group did not have high rates of infection while they were unvaccinated, even though they went longer without any “protection.”
Because of this, Kingston stated that the vaccinated group “have an even higher chance of being infected with COVID-19 than the 36 percent difference indicated by this portion of the study.”
The study even admitted in its conclusion: “An additional analysis appears to indicate that incidence of COVID-19 generally increased in each group of study participants with increasing time post-Dose 2.” Kingston clarified that infection rates “increase over time” when people get two doses of Pfizer mRNA.
Most shocking was the data on the placebo group. In the first four months, the placebo group had “no vaccine protection” and recorded an infection rate of 12.6 cases per 1,000 person-years. The infection rate for the unvaccinated was a meager 1.3 percent.
After their placebo period, the group got “fully vaccinated.” In just a few months, this group became more infectious and showed 43.4 cases per 1,000 person-years. Their infection rate went UP by over 300 percent to a 4.34% infection rate. Mrs. Kingston called this “super alarming.”
“They had less infection when they had no protection. So, that’s a problem,” she said.
References:
Are leaky vaccines driving delta variant evolution and making it more deadly?
by el gato malo – bad cattitude – october 10, 2021
one of the great fears in any vaccination campaign is that the vaccine can wind up becoming the driver viral evolution and making the virus more dangerous. this is a special concern around imperfect (so called “leaky”) vaccines that are non-sterilizing. such vaccines do not stop spread or contagion of the virus. this means the virus will have lots of chances to replicate.
when you combine this with a vaccine that reduces severity of cases and prevents deaths in the vaccinated, it’s a bit of a perfect storm. you get full spread but break the evolutionary gradient towards mildness that viruses tend to follow (and that protects humanity from them).
all a virus wants is to replicate. “make a copy of me and pass it on.” that’s the biological imperative of the selfish gene. excel at it, you win. fail, you disappear. simple as that.
killing or harming the host is maladaptive to viral spread. it’s like burning down your own house with your car in the garage. now you have nowhere to live and no way to get around. that’s not a recipe for reproductive fitness.
this is a property of the world, not of the viruses themselves. so it applies to all of them, evolved and lab hotwired alike.
so viruses evolve to become less, not more virulent. they do not want to kill you. ideally, they’d like to help you. figure out how to be a useful symbiote, and you get a huge boost in propagation. (mitochondria were probably bacteria that were so useful, all our cells incorporated them.) so seeing case fatality rate (CFR) rise in a variant of a virus is like watching water flow uphill. it’s not supposed to do that and when it does, you need to suspect some external force acting on it.
and we’re seeing water flow uphill here.
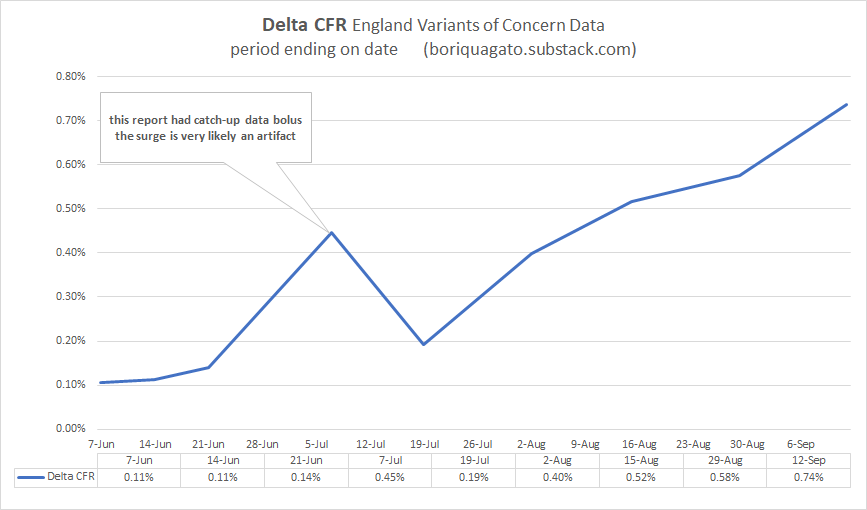
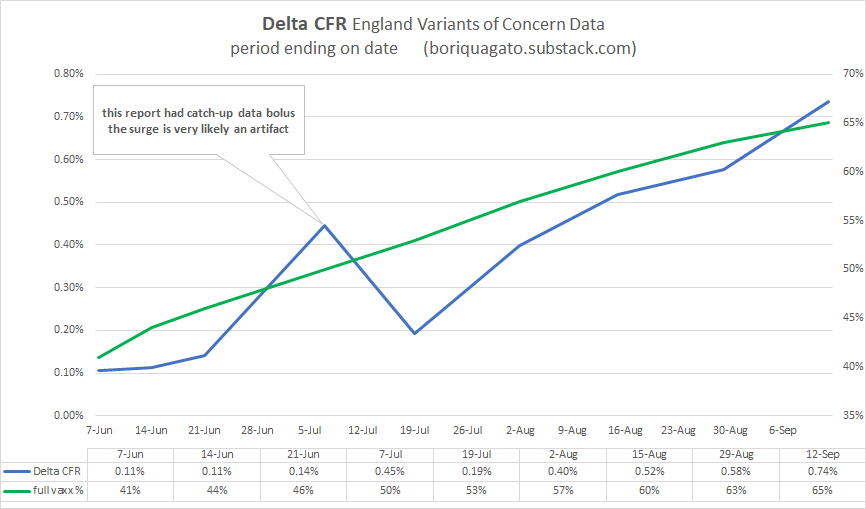
i started with the england variants of concern (VoC) data. it’s the best quality and the best broken out. (the US data is just plain broken. it’s being deliberately scrubbed to prevent analysis like this.) because this data is always aggregated from feb to current period, it does not provide good temporal snapshots, but this can be fixed by subtracting the penultimate report from the current one etc. you subtract report 22’s totals from report 23 and you get just what happened in the last 2 weeks (it used to be a weekly report, now it’s bi-weekly)
what we see is not what one would expect from a virus. none of the other variants (pre vaccine) worked like this. none saw CFR rise like this. and no jump from major variant to variant saw a statistically significant rise in deadliness.
this IS however what one would expect if a virus were undergoing vaccine mediated evolution (as mareks disease did in chickens) and selecting for hotter strains because vaccinated people can carry and spread them and not die.
experienced CFR on delta is nearly 7X what it was in the beginning of june and has been galloping since the middle of july.
(note that pretty much all this data has a large artifact in it from the 21 june report (VoC 17). there was a “data-dump” in it where they caught up on a bolus of past data. it’s an artifact, not a signal. best to ignore it. i suspect the curve from mid june to mid july was smooth.)
put simply: this is not good.
delta is rapidly approaching alpha (1.1%) in terms of CFR whereas it used to be 90% lower. (it also means that the reports on delta CFR in these VoC updates are FAR too low because they are a blend of all cases and deaths back to feb, so they are averaging in the low CFR past and are slow to respond to current dynamics)
this is consistent with, but not proof of vaccines mediated evolution. to get there, we need to do better.
so now we need to start ruling things out and validating this claim to see if it’s meaningful.
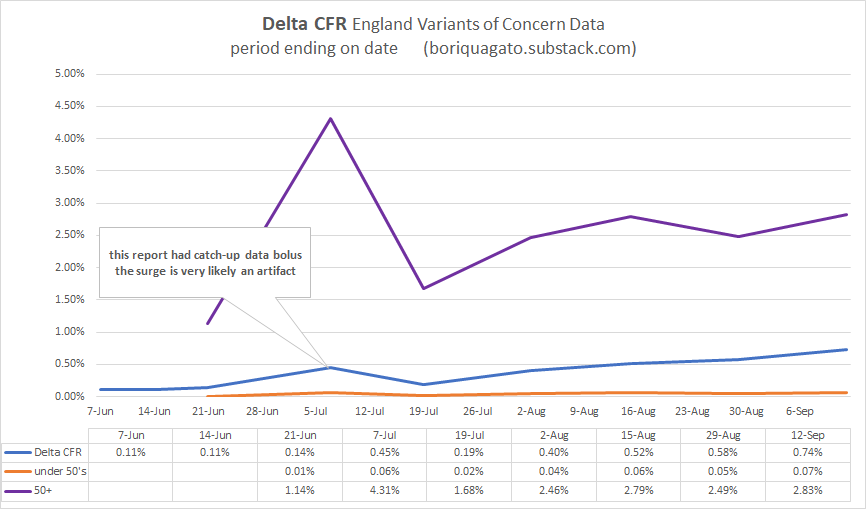
first, it’s not a simpson’s paradox in age data. CFR is rising in over and under 50’s. it’s not mix shift alone. CFR in over 50’s is up 2.5X. it’s up 4-7X in under 50’s.
we’re at about a 3X rise in CFR overall in delta since the summer once we adjust for shifts in age. not as worrying as 7, but still worrying.
and the deaths are real. it’s not made up counting. this can be clearly seen when we comp CFR to the euro-momo Z scores (thoughtfully provided by frequent gato collaborator ben m at USmortality.com. z score is just a measure of deviation from expected all cause deaths. (explained HERE)
alignment is quite strong.
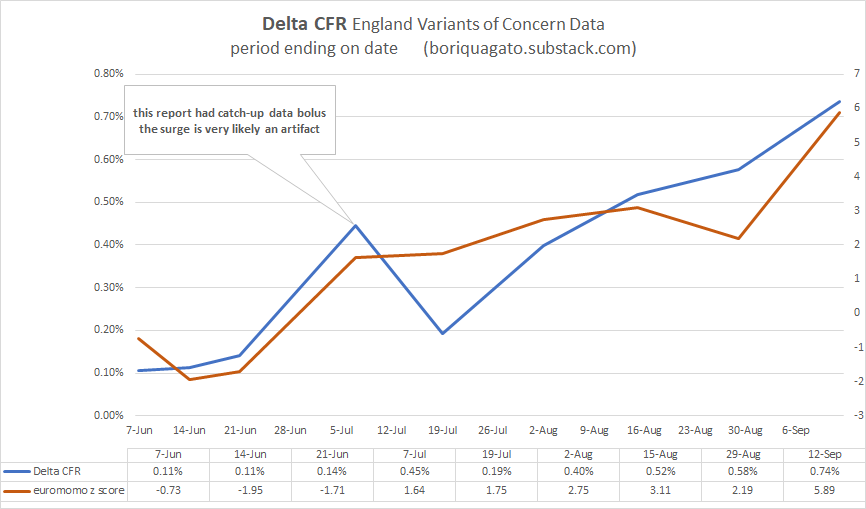
z score was trending negative and spiked to high levels just as CFR really started to ramp up.
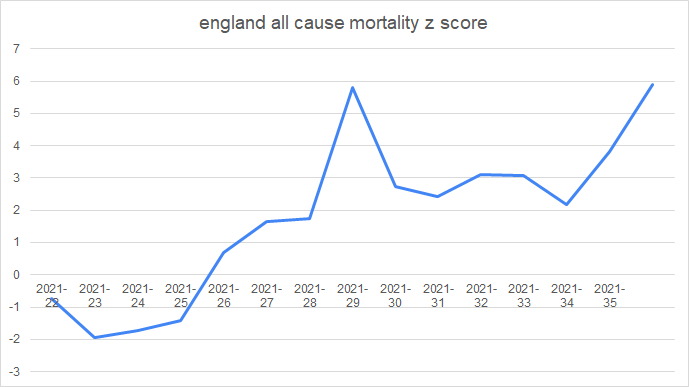
z score for the year can be seen here. starting in wk 22 (may 31) (numbers after the year are weeks)
and given that we know that vaccines DO work to stop deaths in the UK (seemingly in the 50-60% range) it’s even more unexpected that CFR would be rising like this. but it is and the rise in the vaxx rate is not hampering it.
(the precise alignment here is more chart crime than signal, so i’d caution against inferring too much from it)
none of this is what one would expect. not remotely. it bucks evolution, it bucks the other variants, and it flies in the face of late stage pandemic dynamics like increase in acquired immunity (which IS sterilizing), depletion of high risk cohorts, improvements in treatment, etc. all these should be pushing CFR down.
instead, water is flowing uphill.
the question is “why?”
the other day, i discussed ADE (antibody dependent enhancement) where antibodies wind up acting as passkeys for a virus to enter cells and also the fetchingly biblically named OAS (original antigenic sin) whereby preferential training to one antibody response leads to its use against new variants of a pathogen and thereby prevents adaptation to more effective modalities.
note that these two phenomena are by no means mutually exclusive and are actually strongly synergistic.
but are they driving this issue?
i do not not think so.
- if they were, we’d be seeing the CFR rise in the vaccinated but not in the unvaccinated and if it were ALL antibodies, we’d be seeing the previously infected getting hit too. but they are not.
- we’d also likely be seeing low or negative vaccine efficacy (VE) for deaths. but we aren’t. it’s clear the vaccinated are doing better.
CFR is (and has been) much better in the vaccinated than the unvaxxed in UK over 50’s (the highest risk category). trends are similar, but absolute values durably disparate.
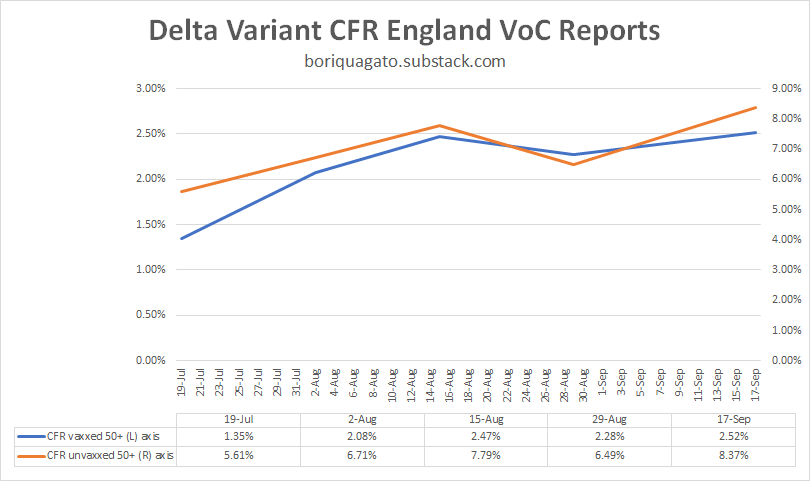
whether and to what extent this is real vaccine efficacy vs cohort bias in a place where 90% of this demographic is vaccinated remains an open issue. it may simply be that only those with the weakest/most compromised immunes systems have not gotten the jab. but this is not really material here.
what IS material is the fact that CFR in the unvaxxed is trending up significantly and so is CFR in the vaxxed. but we’re not seeing many cases of re-infection and almost none of those are serious. this does not look like ADE or OAS as a major driver. if it were, there’s no reason the CFR in the unvaccinated would be rising too.
what this IS consistent with is a variant heating up and getting more and more deadly because it is not checked by normal biological limitations. vaccine mediated evolution (VME) would be very bad news for us.
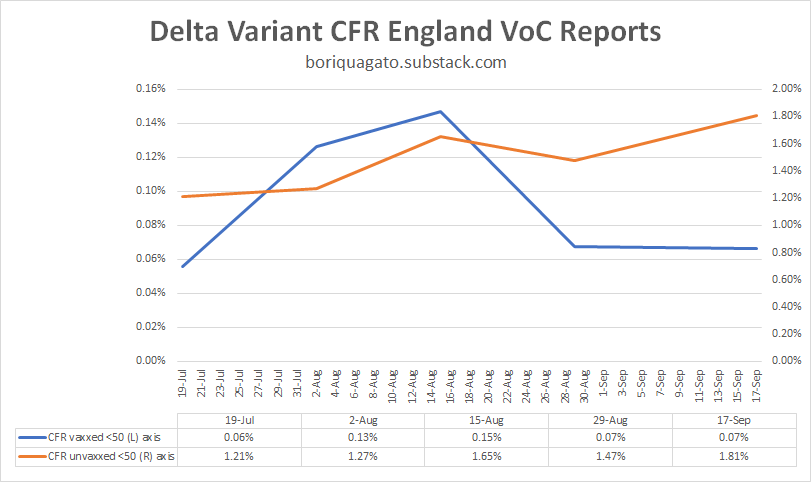
we can see similar in the under 50’s, though the data here is a bit of a mess as during this period, so many very low risk under 50’s (those under 18) got vaccinated that it moved a material risk profile reduction from unvaxxed to vaxxed. i suspect that is why “CFR vaxxed” dropped. it was not vaccines working, it was the vaccinated category being “salted” with large number of the lowest risk folks around. (it also means that group left the unvaxxed, so you get an effect on both)
so i view this data as much lower quality than over 50’s, but it still looks like VME, not ADE or OAS.
this is EXACTLY what leaky vaccines did in chickens.
(read these links. THIS in particular. it’s important.)
such vaccines change the evolutionary gradient for a virus. instead of becoming less virulent/deadly, they can tend the other way because the maladaptiveness of killing the host is mitigated in the vaccinated population. this is what happened with marek’s disease in chickens.
not only is it now more lethal to them than ebola is to humans, making it one of if not THE hottest persistent disease known (killing 100% of unvaxxed birds in 10 days), but, it’s now a disease so hot that an unvaccinated chicken cannot spread it. they die too quickly. only the vaccinated birds spread the nasty strains of mareks. they’re the only ones who live long enough to shed virus.
“Previously, a hot strain was so nasty, it wiped itself out. Now, you keep its host alive with a vaccine, then it can transmit and spread in the world,” Read said. “So it’s got an evolutionary future, which it didn’t have before.”

this is an awful lot of puzzle pieces snapping together and i think we’re really starting to see what this is a picture of.
leaky vaccines that stop severe illness and death but not spread look to be affecting the evolution of the covid 19 virus.
this is an established, predictable, and well supported risk from such vaccines.
this has become my leading hypothesis.
it also explains why we’re seeing such a large rise in deaths relative to cases and deaths and hospitalization overall in so many places. it’s the virus adapting to a stressor we put on it and becoming much more dangerous as a result.
the CFR is a function of the virus, but the virus has become a function of the leaky vaccines.
and it also means the vaccine is protecting no one. yes, it seems to have 50-60% protection against death. but what good is that against a CFR that’s up 300% or more (and rising)? everyone is worse off.

negative VE’s on spread are accelerating cases and this is multiplicative with higher CFR. this is the nightmare scenario and no one is left better off as a result. the CFR among the high risk vaccinated groups is way up too.
everyone is harmed but the brunt is borne by the unvaccinated which perversely winds up looking like better vaccine efficacy. the very fact that vaccines made everyone worse off but spread the misery unevenly makes it look like vaccines are a good idea.
it’s just simple math. if we do something to one group that makes their death rate rise from 1 to 2 per 100 but that also makes the death rate in another group rise from 1 to 4 per 100, that looks like a VE of 50%. in reality, it’s killing 100% more vaxxed people and 300% more of the unvaxxed.
mistaking that gas pedal for the brake and pushing ever harder when you fail to slow would represent an accelerating disaster curve.
that’s the problem with relative measures that ignore absolute changes. you can hide all manner of calamity in such analyses.
it’s still, of course, possible that i’m wrong, but this is looking more and more like it has to be the answer. i can find nothing else fits the facts and the facts themselves are weird enough that “it’s just normal” does not look like a satisfying explanation either and we have enough features here that we can really start testing our puzzle pieces. this one aligns in an AWFUL lot of places.
for something this odd to happen, it takes a truly uncommon exogenous stressor.
i’m just not seeing what else it could be than vaccine mediated selection for hotter variants driving pernicious delta evolution.
so, i’m putting this out to you all to see if you can find some other explanation for what’s going on that fits these facts.
looking forward to the peer review as, honestly, i hope i’m wrong here. this is not an outcome that anyone wants. it’s the nightmare scenario both as a pandemic and as a political horror in the making as if this was an “own-goal”, what would the experts and politicians that pushed this plan not be willing to do to avoid accepting the blame?
because this is career or pharma franchise polonium, and that’s if you’re lucky.
let’s keep at this. one way or the other, we need to know.
the facts do not care about our feelings and epidemiology data is a lousy fabric from which to spin a wubbie to hide under.
we need to get at the truth.
(even if it makes us make a face like this)

Featured Video

Iran Blockade Complications
or go to
Aletho News Archives – Video-Images
From the Archives
A low-fat, high-carb diet has been the largest public health experiment in history. It’s past time for a rethink.
By Malcolm Kendrick | RT | November 25, 2020
New research suggests that four billion people globally will be overweight in 2050. This trend can be traced back to the ‘low-fat, high-carb’ guidelines first issued in the 70s, and should prompt a major U-turn on dietary advice.
A recent report from the Potsdam Institute predicts that by 2050 there will be four billion overweight people in the world, with one-and-a-half billion of them obese. This is not entirely surprising. The world has been getting fatter for years, and things do not seem to be slowing down.
Why is this happening? … continue
Blog Roll
 Aletho News
Aletho News- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- COVID Conniving Receives First Federal Indictment
- Iran Blockade Complications /Lt Col Daniel Davis & Nima Alkhorshid
- Pirates of Mediterranean: Israel does as it pleases in the Sea of Three Continents
- Minab children massacre not ‘unfortunate situation’ but ‘heinous war crime’: Tehran
- OPCW Forced To Pay Damages To Whistleblower Who Found Evidence Of False Flag In Syria
- Iran can thrive under blockade, the US and its allies cannot
- Iran slams US leadership, debunking fabrications, false war costs
- Here’s why Iran is sovereign and Germany is not
- Israel pours $730m into global propaganda machine as reputation collapses
- If Americans Knew
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
