Sen. Ron Johnson Shares COVID-19 Data from Public Health England, Refutes “Pandemic of The Unvaccinated” Narrative
The Last Refuge | October 3, 2021
Senator Ron Johnson (R-Wisconsin) used his time on the Senate floor to discuss recently released COVID-19 data from Public Health England in the U.K. [DATA pdf Here]
Ironically, Senator Johnson is forced to use the Senate floor to share the information in an effort to stop government and Big Tech censorship of the discussion. Unlike the rest of the nation, the House and Senate chamber rules create a free speech zone that prohibits anyone from censoring congressional debate and discussion.
Senator Johnson outlines data from the U.K. clearly showing the vaccines offer no protection from the claimed Delta variant. COVID-19 is carried and shed by vaccinated individuals. The subsequent rate of COVID-19 hospitalization and COVID-19 death appears unaffected by the vaccine itself. WATCH:
As Senator Johnson notes: 63% of the deaths in the U.K. during the 7 month period being discussed were among the vaccinated population.
The data Ron Johnson is sharing is available HERE in pdf form
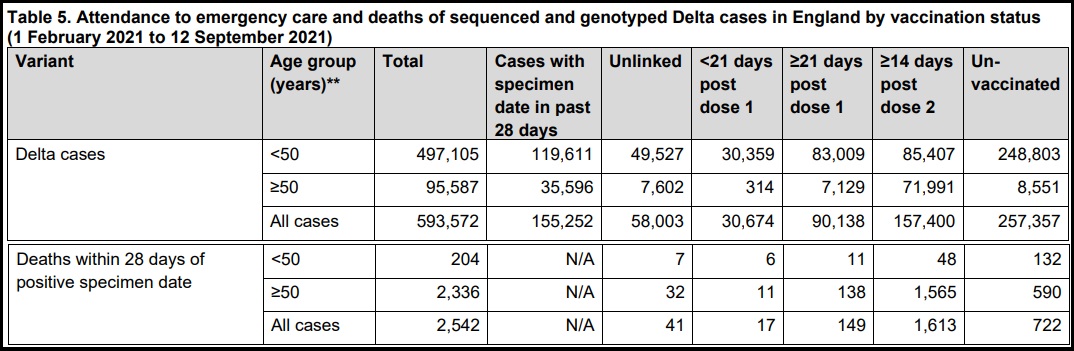
SOURCE: Page 19, 20 – Table 5

Natural Immunity and Covid-19: Twenty-Nine Scientific Studies to Share with Employers, Health Officials, and Politicians
BROWNSTONE INSTITUTE | OCTOBER 10, 2021
From the beginning of the March 2020 lockdowns for the SARS-CoV-2 virus, the subject of natural immunity (also called post-infection immunity) has been neglected. Once the vaccination became widely available, what began with near silence at the beginning turned nearly into a complete blackout of the topic.
Even now, there is an absence of open discussion, presumably in the interests of promoting universal vaccination and required documentation of such vaccination as a condition of participating in public life and even the jobs marketplace. Still, the science exists. Many studies exist. Their authors deserve credit, recognition, and to have their voices heard.
These studies demonstrate what was and is already known: natural immunity for a SARS-type virus is robust, long-lasting, and broadly effective even in the case of mutations, generally more so than vaccines. In fact, a major contribution of 20th-century science has been to expand upon and further elucidate this principle that has been known since the ancient world. Every expert presumably knew this long before the current debates. The effort to pretend otherwise is a scientific scandal of the highest order, especially because the continued neglect of the topic is affecting the rights and freedoms of billions of people.
People who have contracted the virus and recovered deserve recognition. For that matter, people who prefer an exposure risk to the virus in order to gain robust immunity deserve the freedom to make that choice. The realization that natural immunity – which pertains now to perhaps half of the US population and billions around the world – is effective in providing protection should have a dramatic effect on vaccine mandates.
Individuals whose livelihoods and liberties are being deprecated and deleted need access to the scientific literature as it pertains to this virus. They should send a link to this page far and wide. The scientists have not been silent; they just haven’t received the public attention they deserve. The preparation of this list was assisted by links provided by Paul Elias Alexander and Rational Ground’s own cheat sheet on natural immunity, which also includes links to popular articles on the topic.
1. One-year sustained cellular and humoral immunities of COVID-19 convalescents, by Jie Zhang, Hao Lin, Beiwei Ye, Min Zhao, Jianbo Zhan, et al. Clinical Infectious Diseases, October 5, 2021. “SARS-CoV-2-specific IgG antibodies, and also NAb can persist among over 95% COVID-19 convalescents from 6 months to 12 months after disease onset. At least 19/71 (26%) of COVID-19 convalescents (double positive in ELISA and MCLIA) had detectable circulating IgM antibody against SARS-CoV-2 at 12m post-disease onset. Notably, the percentages of convalescents with positive SARS-CoV-2-specific T-cell responses (at least one of the SARS-CoV-2 antigen S1, S2, M and N protein) were 71/76 (93%) and 67/73 (92%) at 6m and 12m, respectively. Furthermore, both antibody and T-cell memory levels of the convalescents were positively associated with their disease severity.”
2. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections, by Sivan Gazit, Roei Shlezinger, Galit Perez, Roni Lotan, Asaf Peretz, Amir Ben-Tov, Dani Cohen, Khitam Muhsen, Gabriel Chodick, Tal Patalon. MedRxiv, August 25, 2021. “Our analysis demonstrates that SARS-CoV-2-naïve vaccinees had a 13.06-fold increased risk for breakthrough infection with the Delta variant compared to those previously infected, when the first event (infection or vaccination) occurred during January and February of 2021. The increased risk was significant for a symptomatic disease as well…. This analysis demonstrated that natural immunity affords longer lasting and stronger protection against infection, symptomatic disease and hospitalization due to the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.”
3. Shedding of Infectious SARS-CoV-2 Despite Vaccination, by Kasen K. Riemersma, Brittany E. Grogan, Amanda Kita-Yarbro, Gunnar E. Jeppson, David H. O’Connor, Thomas C. Friedrich, Katarina M. Grande, MedRxiv, August 24, 2021. “The SARS-CoV-2 Delta variant might cause high viral loads, is highly transmissible, and contains mutations that confer partial immune escape. Outbreak investigations suggest that vaccinated persons can spread Delta. We compared RT-PCR cycle threshold (Ct) data from 699 swab specimens collected in Wisconsin 29 June through 31 July 2021 and tested with a qualitative assay by a single contract laboratory. Specimens came from residents of 36 counties, most in southern and southeastern Wisconsin, and 81% of cases were not associated with an outbreak. During this time, estimated prevalence of Delta variants in Wisconsin increased from 69% to over 95%. Vaccination status was determined via self-reporting and state immunization records.”
4. Necessity of COVID-19 vaccination in previously infected individuals, by Nabin K. Shrestha, Patrick C. Burke, Amy S. Nowacki, Paul Terpeluk, Steven M. Gordon, MedRxiv, June 5, 2021. “Individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before.”
5. Large-scale study of antibody titer decay following BNT162b2 mRNA vaccine or SARS-CoV-2 infection, by Ariel Israel, Yotam Shenhar, Ilan Green, Eugene Merzon, Avivit Golan-Cohen, Alejandro A Schäffer, Eytan Ruppin, Shlomo Vinker, Eli Magen. MedRxiv, August 22, 2021. “This study demonstrates individuals who received the Pfizer-BioNTech mRNA vaccine have different kinetics of antibody levels compared to patients who had been infected with the SARS-CoV-2 virus, with higher initial levels but a much faster exponential decrease in the first group.”
6. Discrete Immune Response Signature to SARS-CoV-2 mRNA Vaccination Versus Infection, by Ellie Ivanova, Joseph Devlin, et al. Cell, May 2021. “While both infection and vaccination induced robust innate and adaptive immune responses, our analysis revealed significant qualitative differences between the two types of immune challenges. In COVID-19 patients, immune responses were characterized by a highly augmented interferon response which was largely absent in vaccine recipients.”
7. SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans, by Jackson S. Turner, Wooseob Kim, Elizaveta Kalaidina, Charles W. Goss, Adriana M. Rauseo, Aaron J. Schmitz, Lena Hansen, Alem Haile, Michael K. Klebert, Iskra Pusic, Jane A. O’Halloran, Rachel M. Presti, Ali H. Ellebedy. Nature, May 24, 2021. “This study sought to determine whether infection with SARS-CoV-2 induces antigen-specific long-lived BMPCs in humans. We detected SARS-CoV-2 S-specific BMPCs in bone marrow aspirates from 15 out of 19 convalescent individuals, and in none from the 11 control participants…. Overall, our results are consistent with SARS-CoV-2 infection eliciting a canonical T-cell-dependent B cell response, in which an early transient burst of extrafollicular plasmablasts generates a wave of serum antibodies that decline relatively quickly. This is followed by more stably maintained levels of serum antibodies that are supported by long-lived BMPCs.”
8. Longitudinal analysis shows durable and broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells, by Kristen W. Cohen, Susanne L. Linderman, Zoe Moodie, Julie Czartoski, Lilin Lai, Grace Mantus, Carson Norwood, Lindsay E. Nyhoff, Venkata Viswanadh Edara, et al. MedRxiv, April 27, 2021. “Ending the COVID-19 pandemic will require long-lived immunity to SARS-CoV-2. We evaluated 254 COVID-19 patients longitudinally from early infection and for eight months thereafter and found a predominant broad-based immune memory response. SARS-CoV-2 spike binding and neutralizing antibodies exhibited a bi-phasic decay with an extended half-life of >200 days suggesting the generation of longer-lived plasma cells. In addition, there was a sustained IgG+ memory B cell response, which bodes well for a rapid antibody response upon virus re-exposure.”
9. Incidence of Severe Acute Respiratory Syndrome Coronavirus-2 infection among previously infected or vaccinated employees, by N Kojima, A Roshani, M Brobeck, A Baca, JD Klausner. MedRxiv, July 8, 2021. “Previous SARS-CoV-2 infection and vaccination for SARS-CoV-2 were associated with decreased risk for infection or re-infection with SARS-CoV-2 in a routinely screened workforce. The was no difference in the infection incidence between vaccinated individuals and individuals with previous infection. Further research is needed to determine whether our results are consistent with the emergence of new SARS-CoV-2 variants.”
10. Single cell profiling of T and B cell repertoires following SARS-CoV-2 mRNA vaccine, by Suhas Sureshchandra, Sloan A. Lewis, Brianna Doratt, Allen Jankeel, Izabela Ibraim, Ilhem Messaoudi. BioRxiv, July 15, 2021. “Interestingly, clonally expanded CD8 T cells were observed in every vaccinee, as observed following natural infection. TCR gene usage, however, was variable, reflecting the diversity of repertoires and MHC polymorphism in the human population. Natural infection induced expansion of larger CD8 T cell clones occupied distinct clusters, likely due to the recognition of a broader set of viral epitopes presented by the virus not seen in the mRNA vaccine. Our study highlights a coordinated adaptive immune response where early CD4 T cell responses facilitate the development of the B cell response and substantial expansion of effector CD8 T cells, together capable of contributing to future recall responses.”
11. mRNA vaccine-induced T cells respond identically to SARS-CoV-2 variants of concern but differ in longevity and homing properties depending on prior infection status, Jason Neidleman, Xiaoyu Luo, Matthew McGregor, Guorui Xie, Victoria Murray, Warner C. Greene, Sulggi A. Lee, Nadia R. Roan. BioRxiv, July 29, 2021. “In infection-naïve individuals, the second dose boosted the quantity and altered the phenotypic properties of SARS-CoV-2-specific T cells, while in convalescents the second dose changed neither. Spike-specific T cells from convalescent vaccinees differed strikingly from those of infection-naïve vaccinees, with phenotypic features suggesting superior long-term persistence and ability to home to the respiratory tract including the nasopharynx. These results provide reassurance that vaccine-elicited T cells respond robustly to emerging viral variants, confirm that convalescents may not need a second vaccine dose, and suggest that vaccinated convalescents may have more persistent nasopharynx-homing SARS-CoV-2-specific T cells compared to their infection-naïve counterparts.”
12. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection, Jennifer M. Dan, Jose Mateus, Yu Kato, Kathryn M. Hastie, et al., Science, January 6, 2021. “Understanding immune memory to SARS-CoV-2 is critical for improving diagnostics and vaccines, and for assessing the likely future course of the COVID-19 pandemic. We analyzed multiple compartments of circulating immune memory to SARS-CoV-2 in 254 samples from 188 COVID-19 cases, including 43 samples at ≥ 6 months post-infection. IgG to the Spike protein was relatively stable over 6+ months. Spike-specific memory B cells were more abundant at 6 months than at 1 month post symptom onset. SARS-CoV-2-specific CD4+ T cells and CD8+ T cells declined with a half-life of 3-5 months. By studying antibody, memory B cell, CD4+ T cell, and CD8+ T cell memory to SARS-CoV-2 in an integrated manner, we observed that each component of SARS-CoV-2 immune memory exhibited distinct kinetics.”
13. Persistence of neutralizing antibodies a year after SARS-CoV-2 infection, by Anu Haveri, Nina Ekström, Anna Solastie, Camilla Virta, Pamela Österlund, Elina Isosaari, Hanna Nohynek, Arto A. Palmu, Merit Melin. MedRxiv, July 16, 2021. “We assessed the persistence of serum antibodies following wild-type SARS-CoV-2 infection six and twelve months after diagnosis in 367 individuals of whom 13% had severe disease requiring hospitalization. We determined the SARS-CoV-2 spike (S-IgG) and nucleoprotein IgG concentrations and the proportion of subjects with neutralizing antibodies (NAb).”
14. Quantifying the risk of SARS‐CoV‐2 reinfection over time, by Eamon O Murchu, Paula Byrne, Paul G. Carty, et al. Rev Med Virol. 2021. “Reinfection was an uncommon event (absolute rate 0%–1.1%), with no study reporting an increase in the risk of reinfection over time. Only one study esti- mated the population‐level risk of reinfection based on whole genome sequencing in a subset of patients; the estimated risk was low (0.1% [95% CI: 0.08–0.11%]) with no evidence of waning immunity for up to 7 months following primary infection. These data suggest that naturally acquired SARS‐CoV‐2 immunity does not wane for at least 10 months post‐infection. However, the applicability of these studies to new variants or to vaccine‐induced immunity remains uncertain.”
15. SARS-CoV-2 antibody-positivity protects against reinfection for at least seven months with 95% efficacy, by Laith J. Abu-Raddad, Hiam Chemaitelly, Peter Coyle, Joel A. Malek. The Lancet, July 27, 2021. “Reinfection is rare in the young and international population of Qatar. Natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months.”
16. Natural immunity against COVID-19 significantly reduces the risk of reinfection: findings from a cohort of sero-survey participants, by Bijaya Kumar Mishra, Debdutta Bhattacharya, Jaya Singh Kshatri, Sanghamitra Pati. MedRxiv, July 19, 2021. “These findings reinforce the strong plausibility that development of antibody following natural infection not only protects against re-infection by the virus to a great extent, but also safeguards against progression to severe COVID-19 disease.”
17. Protection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel, by Yair Goldberg, Micha Mandel, Yonatan Woodbridge, Ronen Fluss, Ilya Novikov, Rami Yaari, Arnona Ziv, Laurence Freedman, Amit Huppert, et al.. MedRxiv, April 24, 2021. “Similarly, the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94·8% (CI:[94·4, 95·1]); hospitalization 94·1% (CI:[91·9, 95·7]); and severe illness 96·4% (CI:[92·5, 98·3]). Our results question the need to vaccinate previously-infected individuals.”
18. Immune Memory in Mild COVID-19 Patients and Unexposed Donors Reveals Persistent T Cell Responses After SARS-CoV-2 Infection, by Asgar Ansari, Rakesh Arya, Shilpa Sachan, Someshwar Nath Jha, Anurag Kalia, Anupam Lall, Alessandro Sette, et al. Front Immunol. March 11, 2021. “Using HLA class II predicted peptide megapools, we identified SARS-CoV-2 cross-reactive CD4+ T cells in around 66% of the unexposed individuals. Moreover, we found detectable immune memory in mild COVID-19 patients several months after recovery in the crucial arms of protective adaptive immunity; CD4+ T cells and B cells, with a minimal contribution from CD8+ T cells. Interestingly, the persistent immune memory in COVID-19 patients is predominantly targeted towards the Spike glycoprotein of the SARS-CoV-2. This study provides the evidence of both high magnitude pre-existing and persistent immune memory in Indian population.”
19. Live virus neutralisation testing in convalescent patients and subjects vaccinated against 19A, 20B, 20I/501Y.V1 and 20H/501Y.V2 isolates of SARS-CoV-2, by Claudia Gonzalez, Carla Saade, Antonin Bal, Martine Valette, et al, MedRxiv, May 11, 2021. “ No significant difference was observed between the 20B and 19A isolates for HCWs with mild COVID-19 and critical patients. However, a significant decrease in neutralisation ability was found for 20I/501Y.V1 in comparison with 19A isolate for critical patients and HCWs 6-months post infection. Concerning 20H/501Y.V2, all populations had a significant reduction in neutralising antibody titres in comparison with the 19A isolate. Interestingly, a significant difference in neutralisation capacity was observed for vaccinated HCWs between the two variants whereas it was not significant for the convalescent groups.”
20. Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection, by Nina Le Bert, Hannah E. Clapham, Anthony T. Tan, Wan Ni Chia, et al, Journal of Experimental Medicine, March 1, 2021. “Thus, asymptomatic SARS-CoV-2–infected individuals are not characterized by weak antiviral immunity; on the contrary, they mount a highly functional virus-specific cellular immune response.”
21. SARS-CoV-2-specific T cell memory is sustained in COVID-19 convalescent patients for 10 months with successful development of stem cell-like memory T cells, Jae Hyung Jung, Min-Seok Rha, Moa Sa, Hee Kyoung Choi, Ji Hoon Jeon, et al, Nature Communications, June 30, 2021. “In particular, we observe sustained polyfunctionality and proliferation capacity of SARS-CoV-2-specific T cells. Among SARS-CoV-2-specific CD4+ and CD8+ T cells detected by activation-induced markers, the proportion of stem cell-like memory T (TSCM) cells is increased, peaking at approximately 120 DPSO. Development of TSCM cells is confirmed by SARS-CoV-2-specific MHC-I multimer staining. Considering the self-renewal capacity and multipotency of TSCM cells, our data suggest that SARS-CoV-2-specific T cells are long-lasting after recovery from COVID-19, thus support the feasibility of effective vaccination programs as a measure for COVID-19 control.”
22. Antibody Evolution after SARS-CoV-2 mRNA Vaccination, by Alice Cho, Frauke Muecksch, Dennis Schaefer-Babajew, Zijun Wang, et al, BioRxiv, et al, BioRxiv, July 29, 2021. “We conclude that memory antibodies selected over time by natural infection have greater potency and breadth than antibodies elicited by vaccination. These results suggest that boosting vaccinated individuals with currently available mRNA vaccines would produce a quantitative increase in plasma neutralizing activity but not the qualitative advantage against variants obtained by vaccinating convalescent individuals.” Newer version reads: “These results suggest that boosting vaccinated individuals with currently available mRNA vaccines will increase plasma neutralizing activity but may not produce antibodies with breadth equivalent to those obtained by vaccinating convalescent individuals.”
23. Differential effects of the second SARS-CoV-2 mRNA vaccine dose on T cell immunity in naïve and COVID-19 recovered individuals, by Carmen Camara, Daniel Lozano-Ojalvo, Eduardo Lopez-Granados. Et al., BioRxiv, March 27, 2021. “While a two-dose immunization regimen with the BNT162b2 vaccine has been demonstrated to provide a 95% efficacy in naïve individuals, the effects of the second vaccine dose in individuals who have previously recovered from natural SARS-CoV-2 infection has been questioned. Here we characterized SARS-CoV-2 spike-specific humoral and cellular immunity in naïve and previously infected individuals during full BNT162b2 vaccination. Our results demonstrate that the second dose increases both the humoral and cellular immunity in naïve individuals. On the contrary, the second BNT162b2 vaccine dose results in a reduction of cellular immunity in COVID-19 recovered individuals, which suggests that a second dose, according to the current standard regimen of vaccination, may be not necessary in individuals previously infected with SARS-CoV-2.”
24. COVID-19 natural immunity: Scientific Brief. World Health Organization. May 10, 2021. “Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months). Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein.”
25. SARS-CoV-2 re-infection risk in Austria, by Stefan Pilz, Ali Chakeri, John Pa Ioannidis, et al. Eur J Clin Invest. April 2021. “We recorded 40 tentative re-infections in 14 840 COVID-19 survivors of the first wave (0.27%) and 253 581 infections in 8 885 640 individuals of the remaining general population (2.85%) translating into an odds ratio (95% confidence interval) of 0.09 (0.07 to 0.13). We observed a relatively low re-infection rate of SARS-CoV-2 in Austria. Protection against SARS-CoV-2 after natural infection is comparable with the highest available estimates on vaccine efficacies. Further well-designed research on this issue is urgently needed for improving evidence-based decisions on public health measures and vaccination strategies.”
26. Anti-spike antibody response to natural SARS-CoV-2 infection in the general population, by Jia Wei, Philippa C. Matthews, Nicole Stoesser, et al, MedRxiv, July 5, 2021. “We estimated antibody levels associated with protection against reinfection likely last 1.5-2 years on average, with levels associated with protection from severe infection present for several years. These estimates could inform planning for vaccination booster strategies.”
27. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN), by Victoria Jane Hall, FFPH, Sarah Foulkes, MSc, Andre Charlett, PhD, Ana Atti, MSc, et al. The Lancet, April 29, 2021. “A previous history of SARS-CoV-2 infection was associated with an 84% lower risk of infection, with median protective effect observed 7 months following primary infection. This time period is the minimum probable effect because seroconversions were not included. This study shows that previous infection with SARS-CoV-2 induces effective immunity to future infections in most individuals.”
28. SARS-CoV-2 Natural Antibody Response Persists for at Least 12 Months in a Nationwide Study From the Faroe Islands, by Maria Skaalum Petersen, Cecilie Bo Hansen, Marnar Fríheim Kristiansen, et al, Open Forum Infectious Diseases, Volume 8, Issue 8, August 2021. “Although the protective role of antibodies is currently unknown, our results show that SARS-CoV-2 antibodies persisted at least 12 months after symptom onset and maybe even longer, indicating that COVID-19-convalescent individuals may be protected from reinfection. Our results represent SARS-CoV-2 antibody immunity in nationwide cohorts in a setting with few undetected cases, and we believe that our results add to the understanding of natural immunity and the expected durability of SARS-CoV-2 vaccine immune responses. Moreover, they can help with public health policy and ongoing strategies for vaccine delivery.
29. Associations of Vaccination and of Prior Infection With Positive PCR Test Results for SARS-CoV-2 in Airline Passengers Arriving in Qatar, by Roberto Bertollini, MD, MPH1; Hiam Chemaitelly, MSc2; Hadi M. Yassine. JAMA Research Letter, June 9, 2021. “Of 9180 individuals with no record of vaccination but with a record of prior infection at least 90 days before the PCR test (group 3), 7694 could be matched to individuals with no record of vaccination or prior infection (group 2), among whom PCR positivity was 1.01% (95% CI, 0.80%-1.26%) and 3.81% (95% CI, 3.39%-4.26%), respectively. The relative risk for PCR positivity was 0.22 (95% CI, 0.17-0.28) for vaccinated individuals and 0.26 (95% CI, 0.21-0.34) for individuals with prior infection compared with no record of vaccination or prior infection.”
Articles in the popular media
Why COVID-19 Vaccines Should Not Be Required for All Americans, by Marty Makary, US News, August 21, 2021
Having SARS-CoV-2 once confers much greater immunity than a vaccine—but vaccination remains vital, by Meredith Wadson, Science, August 26, 2021
Natural infection vs vaccination: Which gives more protection? By David Rosenberg, Israeli National News, July 13, 2021.
Flu survivors still immune after 90 years, by Ed Yong, National Geographic, August 17, 2008.
Rescind Vaccine Mandates: Open Letter to Medical Societies, Hospitals, Clinics, and Other Healthcare Facilities, Association of American Physicians and Surgeons, August 31, 2021.
University Vaccine Mandates Violate Medical Ethics, By Aaron Kheriaty and Gerard V. Bradley, Wall Street Journal, June 14, 2021.
Immunity to the Coronavirus May Last Years, New Data Hint, by Apoorva Mandavilli, New York Times, November 17, 2020.
COVID-19 induces lasting antibody protection, Tamari Bhandara, Washington University School of Medicine, May 24, 2021.
The World Health Organization Oversold the Vaccine and Deprecated Natural Immunity, by Jeffrey Tucker, Brownstone Institute, August 29, 2021.
Why Does the CDC Recognize Natural Immunity for Chicken Pox but Not Covid? By Paul Elias Alexander, Brownstone Institute, September 17, 2021.
Rand Paul and Xavier Becerra Square Off on Natural Immunity, with Devastating Results, by Brownstone Institute, October 2, 2021.
Lockdowns, Mandates, and Natural Immunity: Kulldorff vs. Offit, by Brownstone Institute, October 6, 2021.
Hospitals Should Hire, Not Fire, Nurses with Natural Immunity, by Martin Kulldorff, October 1, 2021.
The Strange Neglect of Natural Immunity, by Jayanta Bhattacharya, Brownstone Institute, July 28, 2021.
The Brownstone Institute for Social and Economic Research is a nonprofit organization conceived of in May 2021 in support of a society that minimizes the role of violence in public life.
Critics love Fauci’s new documentary, but audience hate it and accuse Rotten Tomatoes of ‘hiding’ low score

RT | October 11, 2021
Critics have almost universally praised the new documentary on Dr. Anthony Fauci, but audiences have seemingly hated it, even accusing review aggregator Rotten Tomatoes of trying to hide the movie’s unpopularity.
National Geographic’s ‘Fauci’ has been playing in select cinemas since September 10 and premiered on the Disney Plus streaming service last week. Trailers for the film focus heavily on Fauci and his work combating Covid-19, during which time he has become one of the more controversial figures in American politics.
The film, however, takes a positive look at Fauci and focuses more on tales about the health figure from his family, as well as public figures the infectious disease expert has worked with in the past, such as U2 frontman Bono and former President George W. Bush.
On Rotten Tomatoes, which aggregates reviews from selected critics and then gives a ‘rotten’ or ‘fresh’ score, the film holds a 91% positive rating, based on 30 positive reviews and three negative. The rating from audience members, however, was conspicuously missing from the website until Monday. As of Sunday, only one review, which was negative, had been posted despite the film being out for weeks.
The site was accused of ‘hiding’ the audience score in an effort to spin the movie’s increasingly negative coverage.
On Monday, an audience score did appear, and it showed valleys of difference in opinion from critics to the audience, with users awarding the film a 2% average from over 250 ratings (though it began with a 4% rating that has continually dropped). Despite the average now showing, there is still a lack of actual user reviews on the site, though many users may have chosen to simply drop a rating instead of writing a review.
“Two Americas,” writer Josh Jordan tweeted, including a screenshot of the ‘Tomatometer’ for ‘Fauci’ along with the recently-released comedy special from Dave Chappelle, which has been labeled transphobic by critics, but has been a popular title on Netflix. Critics on Rotten Tomatoes gave the movie a ‘rotten’ score of 33% while audiences awarded a near perfect score.
Fauci critics were quick to mock the film’s near-universal panning from audience members.
The Rotten Tomatoes score for ‘Fauci’ is just the tip of the iceberg when it comes to negative reviews. On IMDB, the movie has a 1.5 rating from over 6000 users.
Trailers for the movie on YouTube haven’t fared much better. One posted by National Geographic has over 100,000 ‘dislikes’ and less than 8000 ‘likes’, as of this writing.
A Disney Plus trailer, on the other hand, has just over 1000 ‘likes’ and over 20,000 ‘dislikes’.
Rotten Tomatoes has been accused of bias in the past, and the company has often chalked up near-universal negative reactions from audiences to trolls’ review-bombing.
In 2019, the company disabled pre-release comments and removed their ‘Want to See’ function – which allowed ratings based on how excited users were for a film – in response to early backlash against franchise pictures accused by critics of going ‘woke’, such as ‘Star Wars: The Last Jedi’ and ‘Captain Marvel’.
Two years before that decision, debate around Rotten Tomatoes and the political influence the audience can have was still a heated debate. Outspoken liberal and comedian Amy Schumer claimed in 2017 that her comedy special ‘The Leather Special’ was review-bombed by the “alt-right” over her comments on Donald Trump and other Republicans (50% critic rating/4% audience). At the time, the site responded again by limiting user functions by removing a five-star system in favor of a positive or negative rating from audiences.
On the opposite end of the spectrum, conservative artists have often pointed to the fact that films aimed at right-leaning audiences often score much lower with critics than audiences as proof the company is more open to ‘certifying’ liberal critics than right-of-center or conservative ones.
Producer John Aglialoro blamed near-universal bad reviews from “hateful” critics on Rotten Tomatoes for his 2011 film ‘Atlas Shrugged: Part I’ struggling to find an audience in theaters (he would go on to produce two sequels covering the last two thirds of Ayn Rand’s influential novel).
Trudeau Bans the Unvaccinated from Leaving the Country and from Earning a Living
The Justice Centre – October 7, 2021
CALGARY: The Justice Centre today responded to the federal government announcement that unvaccinated Canadians will lose their right to move and travel freely within Canada, their right to leave Canada, and their right to earn a living and participate in society without discrimination.
“The government is seeking to have 100% of Canadians injected with the experimental mRNA vaccine, which has not been subjected to any long-term testing on humans,” states lawyer John Carpay, President of the Justice Centre.
With the Canada-U.S. land border closed to non-essential travel, this Covid-19 vaccine travel mandate will effectively prevent unvaccinated people from leaving Canada in any way. In addition to denying unvaccinated Canadians the right to travel by plane or train, the federal government has also announced that federal employees and contractors will lose their jobs unless they participate in the world-wide experiment with new mRNA vaccines.
“We were recently promised, this past summer, that life would go back to normal once 70% of Canadians were injected with mRNA. This high vaccination rate has been achieved but has not stopped the spread of the virus. The new mRNA vaccine also provides no guarantee against the Delta variant,” continues Mr. Carpay.
According to media reports, Prime Minister Trudeau declared that these discriminatory measures against unvaccinated Canadians are needed to keep people “safe,” including children.
“Government data and statistics from every Canadian province, and from countries around the world, tell us that children, teenagers and young adults face no serious threat from Covid, which makes the Prime Minister’s rhetoric about saving children highly misleading,” continues Mr. Carpay.
“Medical reports and scientific studies make it clear that both vaccinated and unvaccinated people spread Covid-19. There is no scientific basis for turning unvaccinated Canadians into second-class citizens,” stated Allison Pejovic, Justice Centre Staff Lawyer.
Currently, Canada’s provincial and federal governments accept two injections as enough to qualify for “full” vaccination. But this may soon change to requiring three, four and more injections to maintain one’s legal status as “fully” vaccinated, as has been demonstrated in Israel and the Netherlands.
“Governments throughout history have used the notion of ‘science’ to support their policies, along with various appeals to public health, safety, security, morality, and so on. No government will violate human rights without putting forward a good-sounding justification, such as the war on terrorism, communism, online hate, drugs, or a nasty virus,” continues Mr. Carpay.
The government’s own data and statistics tell us that Covid is much closer to the annual flu than to the Spanish Flu of 1918. This matters because the entire world was put into a state of panic by the dire predictions of Dr. Neil Ferguson of Imperial College, who claimed in March of 2020 that Covid would be like the Spanish Flu of 1918, killing tens of millions of people.
“Canada’s vaccine passports, and the creation of first-class and second-class citizenship, are founded on Neil Ferguson’s demonstrably false claim that Covid is an unusually deadly killer,” states Mr. Carpay.
“Covid is real. Fear of Covid is wildly exaggerated. Over the past 18 months, government-funded media have been very successful in persuading the majority that vaccine passports (and lockdown policies preceding them) are based on science. When people hear a message thousands of times, they believe it to be true,” continues Mr. Carpay.
“The Justice Centre is profoundly disturbed that these federal mandates will prevent unvaccinated Canadians from leaving the country. Such a mandate is an egregious and unacceptable infringement of Canadians’ constitutionally protected mobility rights. There is no scientific justification for this,” concludes Ms. Pejovic.
These new government restrictions on civil liberties are still announcements at this stage, and no law has been passed by Parliament or by way of cabinet regulation (Order-in-Council). So, no legal challenge is possible at this time. If the government intends to implement these vaccine travel mandates and give them the force of law, these policies can then be challenged in court.
Doctor Says Physicians Are Being “Hunted” For Speaking Out by Press & Medical Boards
Dr Robert Malone branded a “terrorist” by Italian media

By Paul Joseph Watson | Summit News | October 7, 2021
Dr Robert Malone, the inventor of mRNA vaccines, says he was branded a “terrorist” by the media in Italy and warns that physicians who speak out are being “hunted via medical boards and the press.”
“I am going to speak bluntly,” tweeted Malone. “Physicians who speak out are being actively hunted via medical boards and the press. They are trying to deligitimize and pick us off one by one. This is not a conspiracy theory – this is a fact. Please wake up. This is happening globally.”
“I was labeled as a ‘terrorist’ in the Italian press when I was in Rome for the International COVID Summit. My crime? Advocating for early treatment of COVID-19 disease. I suggest that merits a bit of meditation,” he added.
Malone is one of many doctors who have been completely persecuted merely for discussing issues relating to COVID treatments and vaccine side-effects.
He has faced fierce opposition for his assertion that children shouldn’t be given COVID-19 vaccines and has also consistently highlighted concerns over links to myocarditis risk.
Those concerns are now being justified by Finland, Denmark and Sweden halting the Moderna jab for for younger males after reports of cardiovascular side effects.
Despite such concerns being regularly voiced by doctors, the Federation of State Medical Boards announced back in July that it would consider pulling medical licenses of doctors who traffic in “misinformation” about COVID.
In another stunning development, Malone’s IP address was blocked by the New England Journal of Medicine so he couldn’t read studies on their website.
The doctor said he was aware of how to get around the IP block, but called the move a “petty act.”
The War Against Ivermectin Intensifies
By Joel S. Hirschhorn | Principia Scientific | October 11, 2021
The unrelenting opposition to using ivermectin to treat and prevent COVID-19 is stronger than ever. This has resulted from a gigantic increase in demand for IVM by much of the public.
Despite big media tirades against IVM, the truth about its effectiveness (together with failure of COVID vaccines) has reached the public through many articles on alternative news websites and truth-tellers on countless podcasts. Its success has forced Big Pharma to create expensive copies of it.
And in my book Pandemic Blunder I made the case with data that using cheap, safe and effective generics like IVM and hydroxychloroquine would save 80 percent or more of COVID deaths. Esteemed physician Peter McCollough later said 85 percent. For the US, that means over 500,000 lives could have been saved, and globally over four million lives.
Meanwhile, hundreds of thousands of people worldwide have died from COVID vaccines, the failed solution to the pandemic.
Merck, a maker of IVM, is getting much positive press coverage for its forthcoming prescription oral antiviral (molnupiravir). It is designed to replace IVM that they cannot make big money from. FDA will soon give it emergency use authorization because of the emerging clarity that COVID vaccines do NOT work effectively or safely.
That the Washington Post says that what Merck has created is the “first covid-fighting pill” illustrates how awful big media has been in ignoring the proven benefits of the IVM and HCQ generics. And ignoring the many failures of COVID vaccines. In its October 2 front-page story on the new Merck pill, it did not even mention IVM or present any data showing IVM as proven even more effective than the new expensive drug tested on only hundreds of people for a short period.
In contrast, IVM has been used successfully on hundreds of thousands of people to treat and prevent COVID.
Speaking as someone who is using IVM as a prophylactic, here is what I have seen in recent times. Though getting a prescription for it is very difficult and stressful it can be done through a number of websites. But then the battle just begins. Many pharmacies, especially big chain ones, will not fill IVM prescriptions if there is any evidence that it is being used to fight COVID.
And then you will likely discover, as I did, that virtually no pharmacy (typically small community ones) that will fill such prescriptions has any IVM. That’s right. There is a national shortage of IVM because of huge demand in recent months and because US makers have not escalated production.
Probably, millions of vaccine resisters are using IVM, especially those resisting booster shots.
Can you still get it? Yes, and even without a prescription. It will have to come from India, with many makers of IVM. It can take many weeks to get it. But the cost is a tiny fraction of what US pharmacies have been charging when they did have it in stock. Rather than $4 or $5 for a 3 mg pill, you can buy 12 mg pills for way under $1 a pill.
But there is more to the IVM story.
There is absolutely no doubt whatsoever that there is massive medical science data showing absolute reliable data that IVM is safe and effective for both treating and preventing COVID. This is what should be a bold large headline in newspapers if we had honest big media: IVM SAFE AND EFFECTIVE ALTERNATIVE TO COVID VACCINES.
But instead, there is a constant barrage of articles and statements from government agencies asserting IVM should not be used to fight COVID. They argue it is unsafe and ineffective. Both are lies aimed solely at protecting the mass vaccination effort and the profits of big drug companies. And now protecting the new Big Pharma market for antiviral pills.
FDA has issued very strong warnings against using IVM for COVID. Nothing it has said follows the true science and mountains of data supporting safe and effective IVM use. Like other IVM opponents, it has conflated personal IVM use with the use of IVM products designed for animals.
This is even more infuriating. Merck, despite being a maker of IVM discredited its use for COVID by irresponsibly stating, “We do not believe that the data available support the safety and efficacy of ivermectin beyond the doses and populations indicated in the regulatory agency-approved prescribing information.”
Clearly, Merck, Pfizer and other vaccine makers are developing their own oral antivirals to directly compete with the cheap and effective IVM. These antivirals, unlike cheap generic IVM, would be patented so expensive pills could be sold worldwide. They will find some ingenious ways to copy IVM but make enough changes to get patents.
Already, Merck has begun production of its new pill to be taken twice daily for five days. Even more significant: The US government has made an advance purchase of 1.7 million treatment courses for $1.2 billion! That is over $700 per treatment. So much more profitable than making IVM. Forget the billions of dollars spent on vaccines that are injuring and killing many people.
I am confident in predicting that as more and more bad news about the ineffectiveness and dangerous side effects of COVID vaccines become increasingly known to more of the public, the big drug companies will increasingly switch from vaccines to prescription antiviral medicines.
This is what smart corporate business strategic planning is all about. With Merck, it has already started. And FDA, CDC and NIH will go along with this strategic switch.
This will preserve a trillion-dollar market for pharmaceutical companies. How the government and public health establishment weasel word their switch from COVID vaccines to antiviral pills will be a marvelous magical trick to watch. Do you think that they will admit that millions of people worldwide have lost their health and lives from vaccine use? Of course not. Expensive antiviral pills will simply be sold as a better solution.
Be clear about the science explaining why IVM and HCQ have worked. They both (along with zinc) interfere at the earliest stage of COVID infection with viral replication. Stop infection in its tracks. They work as prophylactics for the same reason.
If you keep a modest amount of IVM and HCQ in your body (and take zinc, vitamins C and D, and quercetin) any virus that enters your body can be stopped before major viral replication. The new prescription medicines coming from Merck and other Big Pharma are designed to serve the same function as the cheap generics.
This is the big truth coming to fruition: All the emerging information on COVID vaccine ineffectiveness and dangerous and often lethal side effects is forcing a major strategic shift to antivirals.
Congressman Louie Gohmert has recently made a number of solid observations about IVM:
“Almost 4 billion doses of ivermectin have been prescribed for humans, not horses, over the past 40 years. In fact, the CDC recommends all refugees coming to the U.S. from the Middle East, Asia, North Africa, Latin America, and the Caribbean receive this so-called dangerous horse medicine as a preemptive therapy.
Ivermectin is considered by the World Health Organization (WHO) to be an ‘essential medicine.’
The Department of Homeland Security’s ‘quick reference’ tool on COVID-19 mentioned how this life-saving drug reduced viral shedding duration in a clinical trial.”
“To date, there are at least 63 trials and 31 randomized controlled trials showing benefits to the use of ivermectin to fight COVID-19 prophylactically as well as for early and late-stage treatment. Ivermectin has been shown to inhibit the replication of many viruses, including SARS-CoV-2. It has strong anti-inflammatory properties and prevents transmission of COVID-19 when taken either before or after exposure to the virus.”
“Ivermectin also speeds up recovery and decreases hospitalization and mortality in COVID-19 patients. It has been FDA approved for decades and has very few and mild side effects. It has an average of 160 adverse events reported every year, which indicates ivermectin has a better safety record than several vitamins. In short, there is no humane, logical reason why it should not be widely used to fight against the China Virus should a patient and doctor decide it is appropriate to try in that patient’s case.”
And that small number of adverse events pales in comparison to hundreds of thousands for COVID vaccines.
A new, comprehensive report noted that 63 studies have confirmed the effectiveness of IVM in treating COVID-19. This is a great website to see positive IVM data.
And consider what former Director of Intellectual Property at Gilead Pharmaceuticals, Brian Remy, said about the necessity of implementing Ivermectin. “It is simple – use what works and is most effective – period. Ivermectin used in combination with other therapeutics is a no-brainer and should be the standard of care for COVID-19. Not only would this be good for business and help avoid the criticism and bad PR, and potential civil/criminal liability for censorship, scientific misconduct, etc. for misrepresentation of Ivermectin and other generics, but most importantly it would save countless lives and end the pandemic for good.” Amen.
Want even more positive facts? Consider the India experience. In India’s deadly second pandemic surge, Ivermectin obliterated their crisis. Within weeks after adopting IVM cases were down 90 percent. Those states with more aggressive IVM use were down more dramatically. Daily cases in Goa, Uttarakhand, Uttar Pradesh, and Delhi were down 95, 98, 99, and 99 percent, respectively.
And appreciate this: Dr. Kory and the FLCCC published a narrative review in May 2021, showing the massive effectiveness of IVM against COVID-19 in reducing death and cases. They concluded that it must be adopted globally immediately. Yet big media without respect for public health waged war against IVM. Now it is going crazy in support of the expensive Merck antiviral pill.
To sum up: The IVM story is far from over. We now have a pandemic of the vaccinated. From all over the world the fractions of people said to have died from COVID who were fully vaccinated are very high, often 80 percent. Many people with breakthrough COVID infections die.
Blame those deaths on the vaccines. Big media suppresses all the negative information on the vaccines and all the positive information on IVM.
This double whammy is pure evil. It is designed to pave the way for the new, expensive generation of antiviral pills once the medical and public health establishments backtrack from their vaccine advocacy and coercion.
About the author: Dr. Joel S. Hirschhorn, author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.
Cultural Warfare in the 20th Century: How Western Civilization Came Undone
By Matthew Ehret | Strategic Culture Foundation | October 9, 2021
In my last article “Guterres and the Great Reset: How Capitalism Became a Time Bomb”, I made the case that the time bomb justifying a Great Reset of civilization was set into motion over 50 years ago. In that location, we were introduced to a cast of characters surrounding the World Economic Forum and Trilateral Commission who played instrumental roles in bringing about a controlled disintegration of western civilization.
Despite the fact that this un-natural transformation occurred over the dead bodies of great statesmen of the 1960s, a question still lingers: HOW did the western nations… especially the United States, so deeply shaped by a love of freedom, wilfully relinquish its democratic institutions in favor of a new system of supranational governance and de-growth? How did the very people who were targeted for destruction not only let this happen but in some cases even aide and abet the perpetrators?
Epistemological Warfare in America
Here it helps to look to the writings of an imperial grand strategist who is too often championed as a defender of freedom: Aldous Huxley.
While Aldous’ brother Julian was reshaping the global paradigm by re-packaging eugenics under several new costumes post-1945, Aldous’ creative juices were driven entirely by his role as a cultural warrior.
Grand children of Thomas Huxley who was commissioned to re-organize the British Empire in the late 1850s, both grandchildren vigorously embraced the family business working closely with the elite Bloomsbury Group of Bertrand Russell, and John Maynard Keynes between 1914-1937.
Among these creative misanthropes, Lord Bertrand Russell (another celebrated pacifist) had gone far in outlining the sort of bone chilling ideal that Darwinian laws of evolution demanded be humanity’s destiny under a scientifically managed priesthood. In his 1930 Scientific Outlook, Russell stated:
“The scientific rulers will provide one kind of education for ordinary men and women, and another for those who are to become holders of scientific power. Ordinary men and women will be expected to be docile, industrious, punctual, thoughtless, and contented. Of these qualities probably contentment will be considered the most important. In order to produce it, all the researchers of psycho-analysis, behaviourism, and biochemistry will be brought into play…. All the boys and girls will learn from an early age to be what is called `co-operative,’ i.e., to do exactly what everybody is doing. Initiative will be discouraged in these children, and insubordination, without being punished, will be scientifically trained out of them.”
“Except for the one matter of loyalty to the world state and to their own order, members of the governing class will be encouraged to be adventurous, and full of initiative. It will be recognized that it is their business to improve scientific techniques and to keep the manual workers contented by means of continual new amusements”.
Huxley would have Russell’s thesis firmly in mind when he began writing his Brave New World in 1931.
Aldous Goes to Work
Having set up his base of operations in Hollywood in 1937, Aldous lived out his days in the USA writing scripts for Hollywood, exploring psychotropic drugs and coordinating a new cultural movement that would soon overtake the youth growing up amidst the insanity of the Cold War.
In an infamous 1962 speech titled “The Ultimate Revolution”, Aldous Huxley outlined the principles of this new science of governance telling adoring fans amidst the wannabe alphas in the Berkeley auditorium:
“If you are going to control any population for any length of time, you must have some measure of consent. It’s exceedingly difficult to see how pure terrorism can function indefinitely. It can function for a fairly long time, but I think sooner or later you have to bring in an element of persuasion, an element of getting people to consent to what is happening to them. Well, it seems to me that the nature of The Ultimate Revolution with which we are now faced is precisely this: That we are in process of developing a whole series of techniques, which will enable the controlling oligarchy who have always existed and presumably always will exist, to get people, actually, to love their servitude.”
Getting people to love their servitude would be made possible by an array of new techniques outlined in both Huxley’s fiction and non-fiction writings and put into motion by the hard work of CIA-funded laboratories working under secretive umbrella of Allan Dulles’ MK Ultra. Utilizing many techniques pioneered by Nazi psychiatrists in WWII, one of the primary objectives of MK Ultra was to deconstruct the human psyche using a mix of electroshock therapy, psychotropic drugs and other conditioning in order to reconstruct personalities from scratch by professional psychiatrists. As Naomi Klein demonstrated in her famous book The Shock Doctrine, the idea behind MK Ultra was always to extend these behavioral techniques to reprogramming entire groups, societies and nations.
Within Huxley’s Brave New World, psychotropic drugs (soma), cultural norms driven by pre-adolescent sensualism, constant Tinder-esque sexual escapades, the disintegration of family units and hyper-sensualized entertainment (dubbed “feelies”) did the job nicely. Huxley’s dystopia featured a society which had successfully evolved to become a total oligarchy with a scientific priesthood managing the test tube babies bio engineered to become alphas, betas, gammas or the lowly toilet cleaning epsilons reminiscent of the sub-human Morlocks described in H.G. Wells’ earlier Time Machine. In Huxley’s world, family units have long since disintegrated with the nation state and any belief in God.
In his 1958 Brave New World Revisited, Aldous decries the ultimate evil caused by faith in scientific and technological progress as an illusion which cannot provide an escape from the ultimate determining law of humanity: overpopulation. Citing creative breakthroughs in atomic power, space exploration and medicine, Huxley bemoans how each time humanity solves a problem that allows us to save more lives, the species replicates at faster rates bringing about the inevitable Malthusian problems of future wars for resources, diseases and the breeding of the inferior races.
Huxley writes:
“In this second half of the twentieth century we do nothing systematic about our breeding; but in our random and unregulated way we are not only over-populating our planet, we are also, it would seem, making sure that these greater numbers shall be of biologically poorer quality. In the bad old days children with considerable, or even with slight, hereditary defects rarely survived. Today, thanks to sanitation, modern pharmacology and the social conscience, most of the children born with hereditary defects reach maturity and multiply their kind.”
In another speech delivered to the University of California in 1961, Huxley elaborated on this bone chilling plan saying:
“There will be in the next generation or so a pharmacological method of making people love their servitude and producing dictatorship without tears, so to speak. Producing a kind of painless concentration camp for entire societies, so that people will in fact have their liberties taken away from them but will rather enjoy it, because they will be distracted from any desire to rebel – by propaganda, or brainwashing, or brainwashing enhanced by pharmacological methods. And this seems to be the final revolution.”
Huxley knew that if this sort of brainwashing were successfully induced, the ruling oligarchy could ensure that the hedonistic identities of those coming of age within this controlled environment would detach themselves from outdated concepts like nationalism, love of family, or religion, in order to create LSD-driven personal “micro-realities”. Honoring the past and sacrificing for the future became replaced with a new wisdom of “living in the now”.
Huxley was happy to discover that LSD-25 mixed with cannabis, hashish and mescaline was a perfect supplement for soma writing in his 1958 Revisited:
“In LSD-25 (lysergic acid diethylamide) the pharmacologists have recently created another aspect of soma – a perception-improver and vision-producer that is, physiologically speaking, almost costless. This extraordinary drug, which is effective in doses as small as fifty or even twenty-five millionths of a gram, has power (like peyote) to transport people into the other world. In the majority of cases, the other world to which LSD-25 gives access is heavenly; alternatively it may be purgatorial or even infernal. But, positive, or negative, the lysergic acid experience is felt by almost everyone who undergoes it to be profoundly significant and enlightening. In any event, the fact that minds can be changed so radically at so little cost to the body is altogether astonishing.”
During his time in the United States coordinating this new countercultural insurgency, Aldous recruited a young professor of psychiatry named Timothy Leary to his cause. Describing his interaction with Huxley as the two planned this final revolution, Leary wrote in 1983:
“We had run up against the Judeo-Christian commitment to one God, one religion, one reality, that has cursed Europe for centuries and America since our founding days. Drugs that open the mind to multiple realities inevitably lead to a polytheistic view of the universe. We sensed that the time for a new humanist religion based on intelligence, good natured pluralism and scientific paganism had arrived.”
The Creation of Organized Schizophrenia
How the counter-culture was formed in the bowels of such oligarchical psychiatric mental meatgrinders like London’s Tavistock Institute and was applied by psychiatric shock troops strategically placed across all schools, military, unions, corporate boards and government bureaucracies throughout the years is beyond the scope of this present article, although it was explored in a recent video by this author.
What must be kept in mind for our present purposes is that cultural warfare during this intense post WW2 period was full spectrum in nature- taking every major branch of human life into account and extracting all traces of creative reason, universality, Freedom, and Truth anywhere it could be found.
Whether it was in the fine arts and music or whether it was in scientific practice, new dualisms were imposed severing logical thinking from the “pollution” of subjective emotions. Where the arts became shaped increasingly by hedonism liberated from reason (with a “high” post-modern art for the elites and a “low” populist art for the dumb masses), the sciences became governed by the dogmatic faith in cold mathematical sterility governed by “statistics”, entropy, and blind fatalism.
Random paint splashes of CIA-funded artists like Jackson Pollock or the fuzzy squares of Mark Rothko became the new artistic ideal while scientists found themselves trained to think like computers modelling their minds of the methods of Bertrand Russell’s Principia, Norbert Weiner’s Cybernetics and John von Neumann’s Information Theory. Bertrand Russell’s role coordinating the CIA’s Congress for Cultural Freedom should not be lost on anyone.
With the severing of creativity from reason, the minds of those processed by this new cultural field was increasingly shaped by blind rules and axioms enforced by expert consensus rather than personal acts of discovery. Computer modelling thus found itself replacing acts of genuine human thought and within this sterile intellectual climate, a new cult of artificial intelligence began to find fertile soil to grow its perverse roots.
When mixed with heavy doses of imperial wars, assassinations, coups, and the looming threat of nuclear annihilation, the parents of the baby boomers had no clue what evil they were dealing with as their children were absorbed into a new drug/sex-ridden cultural field that no one had ever experienced before. Schizophrenic chaos in the world bred schizophrenic chaos in the culture as increasingly large arrays of youth gave up on reality in order to “tune in, turn on and drop out”.
Throughout the 1960s, patriotic forces around the world rallied to revive the spirit of scientific and technological progress which these neo-Malthusians despised so much. President John F Kennedy attempted to amplify Eisenhower’s Atoms for Peace along with large scale investments into Africa, Asia and Ibero America alongside leaders of the Pan African and Pan Arab world who were committed to ending colonialism and bringing their people into the 21st century.
After Kennedy’s murder, Charles de Gaulle worked with international co-thinkers like Quebec Premier Daniel Johnson, Canadian Prime Minister John Diefenbaker and German Chancellor Adenauer to bring about a coalition of progress which peaked in 1968 with Bobby Kennedy’s inevitable leadership of the United States.
Just as in the period of the late 19th century when a win-win system of international cooperation was threatening to replace the dying Hobbesian system of the British Empire, a dense string of coups, color revolutions and assassinations ensured the crushing of this dynamic as a new age of post-industrialism, Anglo-American imperialism and monetarism was unleashed onto an unsuspecting society.
The Club of Rome Takes the Stage
In this new post-1968 political climate, new scientific conferences were organized in an attempt to impose statistic modelling premised on systems analysis onto biological, economic and especially ecological systems. Extrapolating present trends into the future and disregarding the sorts of non-linear qualitative leaps caused by creative thought allowed this new breed of scientist to “predict” the inevitable crises caused by population growth and the diminishing returns on finite resources.
The iconic study for this new scientific movement was the Club of Rome-commission MIT report Limits to Growth that “predicted”, as Malthus had done two centuries earlier, the point of crisis when population pressures would outstrip nature’s bounty- giving technocrats managing humanity the tools needed to make the proper sacrifices in the present.
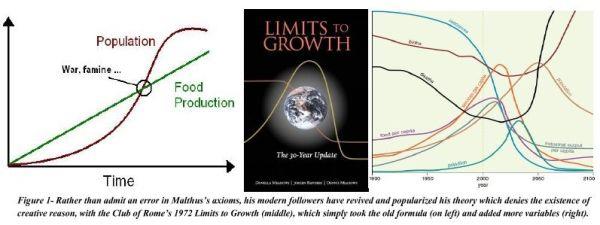
When figures like Mark Carney discuss the “greening of global finance” and placing monetary values upon the reduction of carbon footprints, this is the sick and unscientific foundation of their thinking. Where formerly, humanity valued economic growth via scientific and technological progress (and implicitly the support of increased numbers of people at higher standards of life), the new system of “values” promoted by these misanthropes demanded that profit be tied to the reduction of human activity on the earth.
Club of Rome co-founder Aurelio Peccei, who presented at the inaugural World Economic Forum meetings in Davos, stated:
“The economy and the ecology are inextricably united… A strategy of generating wealth and one of safeguarding this patrimony are opposed. Activities that generate wealth but destroy the natural patrimony even more, create negative value”.
Former President of the World Federation of Mental Health during the high point of MK Ultra, Margaret Mead (wife of MK Ultra controller Gregory Bateson) presided over one such 1975 conference on the environment and atmosphere sponsored by the Club of Rome (this club also being an early sponsor of the World Economic Forum in 1971). Echoing the spirit of Russell and Huxley earlier, Mead called for the creation of a new science of statistics premised on equating pollution to climate change that would become internally consistent and shape the behavior of humanity going into the 21st century. The focus was always population control. In her speech Mead said:
“The unparalleled increase in the human population and its demands for food, energy, and resources is clearly the most important destabilizing influences in the biosphere. We are facing a period when society must make decisions on a planetary scale.”
“What we need from scientists are estimates, presented with sufficient conservatism and plausibility but at the same time as free as possible from internal disagreements that can be exploited by political interests, that will allow us to start building a system of artificial but effective warnings, warnings which will parallel the instincts of animals who flee before the hurricane. [We must] draw from the necessary capacity for sacrifice. It is therefore a statement of major possibilities of danger, which may overtake humankind, on which it is important to concentrate attention”.
Rather than seeing science as a field for optimistic problem solving, this misanthropic cult of elitists demanded that science be redefined around a “new wisdom” of adapting to problems real or imagined. This cynical science of “problematique” (the science of problems) assumed that since all creative discovery caused population growth, the real enemy was found in the naïve optimists who believe it good to promote discoveries. Mead ridiculed those cultural optimists who rejected this cynical view of science saying:
“Those who react against prophets of doom, believing that there is not adequate scientific basis for their melancholy prophecies, [for they] tend to become in turn prophets of paradisiacal impossibilities, guaranteed utopias of technological bliss, or benign interventions on behalf of mankind that are none the less irrational just because they are couched as ‘rational.’ They express a kind of faith in the built-in human instinct for survival, or a faith in some magical technological panacea.”
Using more truthful language, Club of Rome co-founder Sir Alexander King stated in the preface of The First Global Revolution (1991):
“In searching for a common enemy against whom we can unite, we came up with the idea that pollution, the threat of global warming, water shortages, famine and the like, would fit the bill. In their totality and their interactions these phenomena do constitute a common threat which must be confronted by everyone together. But in designating these dangers as the enemy, we fall into the trap, which we have already warned readers about, namely mistaking symptoms for causes. All these dangers are caused by human intervention in natural processes, and it is only through changed attitudes and behaviour that they can be overcome. The real enemy then is humanity itself.”
Today’s world is being pulled by two opposing dynamics.
The prophets of doom who set the time bomb in place half a century ago giddily prepare their utopian Great Reset which demands vast bloodletting as an overpopulated humanity is to be sacrificed by a modern pagan scientific priesthood devoted to Gaia and computer models. On the other hand, the spirit of progress and open system thinking has come alive in the form of the multipolar alliance which premises its planning on an opposing set of assumptions about the nature of humanity, creative thought, value, economics, progress and natural law.
Which future wins out in this battle over humanity will be shaped by the decisions and discoveries we make (or fail to make) in the days ahead.
Vaccine Effectiveness Drops Again, Now as Low as Minus-86% in Over-40s, Latest PHE Data Shows
By Will Jones • The Daily Sceptic • October 10, 2021
The latest Public Health England (PHE) Vaccine Surveillance report was released on Thursday, meaning we can update our estimates of unadjusted vaccine effectiveness from real-world data.
As before, the report itself states this is “not the most appropriate method” to assess vaccine effectiveness as it is not adjusted for various confounders (and they do not provide the data that would allow such adjustments to be made). ‘Fact-checking’ website Full Fact (funded by Big Tech) are currently trying to censor the Daily Sceptic because, they claim, this means it is ‘incorrect’ to use the data in the report to calculate vaccine effectiveness. This is not true, however: regardless of what PHE deems to be the “most appropriate method”, vaccine effectiveness is defined as the reduction in the proportion of infections in the vaccinated group compared to the unvaccinated group, and it is perfectly acceptable to estimate it from population data, as long as any limitations in the data are acknowledged.
It is certainly not ‘incorrect’ to use the latest population-based data to get an up-to-date estimate of unadjusted vaccine effectiveness as part of tracking how the vaccines are performing on the ground.
Perhaps the most important limitations in this data are that the high-risk were originally prioritised for vaccination and that those who have been previously infected may be more likely to decline vaccination. Both of these would artificially lower the estimate of vaccine effectiveness. However, a recent population study in the Lancet adjusted its vaccine effectiveness estimates to take account of no fewer than 22 different confounding factors, including these, and in almost all cases this resulted in very little change. For instance, here are the adjusted and unadjusted estimates against infection by age. (Note that the high values here are for the whole study period; what the study showed overall is that in more recent months vaccine effectiveness has been dropping fast.)
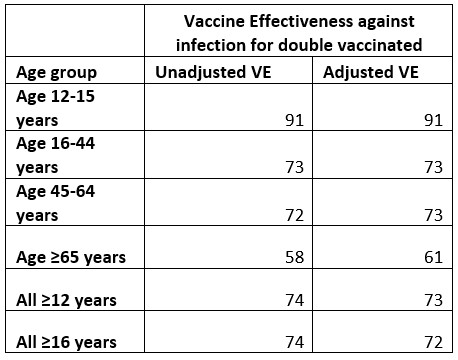
Tartof SY, Slezak JM, Fischer H, et al (2021)
Two stay the same, two change by one point, one changes by two points and one changes by three points. This is typical of the vaccine effectiveness estimates in the study, with very few exceptions. This suggests that the unadjusted estimates from large population studies like this are already very close to the mark in most cases, with any adjustments being small. This gives us reason for confidence that the unadjusted estimates from the PHE data, even if, according to them, not “the most appropriate method”, will be sufficiently close to be useful.
So here, without further ado, is the table with the latest unadjusted vaccine effectiveness estimates, for the period September 6th to October 3rd. (For the previous three tables see my previous post.)
Note that unvaccinated here means actually unvaccinated, not partially vaccinated or post-jab. Hospitalisation means “cases presenting to emergency care (within 28 days of a positive specimen) resulting in an overnight inpatient admission”.

Strikingly, the (unadjusted) vaccine effectiveness (VE) in over-18s continues to drop. For those in their 40s it hits nearly minus-86% this week, down from minus-66% in last week’s report. This means the double-vaccinated in their 40s are now getting on for being almost twice as likely to be infected as the unvaccinated of the same age. Those in their 50s, 60s and 70s have similarly super-low VE estimates, while the unadjusted VE for those in their 30s goes negative for the first time, having been dropping for some weeks. For the under-18s, on the other hand – which is the group currently being vaccinated – it actually went up, from 84% to 88%.
Public health officials should be making a priority of investigating the reasons for this alarming inversion of vaccine effect in the over-30s. The fact that instead we have an effort from Government-approved ‘fact-checkers’ to suppress the reporting of it is disturbing, to say the least.
Vaccine effectiveness against serious disease and death continues to hold up well, save in the over-80s, where VE against hospitalisation has dropped from 59% to 51% since last week’s report, which is worrying as most of the deaths are in the over-80s. Effectiveness against death in the over-80s has been sliding more gradually from 70% in weeks 32-35 down to 64% in weeks 36-39, a month later.
Oddly, the text of the report contains an error. It states: “The rate of a positive COVID-19 test is substantially lower in vaccinated individuals compared to unvaccinated individuals up to the age of 39.” This is the same statement (word-for-word) the surveillance reports have made since they started reporting this data in week 36. However, it clearly is no longer true for those in their 30s, where the infection rate in the vaccinated is now slightly higher than in the unvaccinated, and needs updating.
A new PHE Technical Briefing has also been published recently, but we cannot update our VE estimates from that data as we usually do as they have decided to discontinue including it. A note explains:
Cases, hospitalisation, attendance and deaths by vaccination status are now presented in the COVID-19 vaccine surveillance report and therefore this data will not be produced in future editions of the variant technical briefing. These tables will be reinstated in the technical briefing if new variants of concern arise.
This is a pity as the Technical Briefing data, while limited to sequenced Delta positive tests, was useful because it went back to February and was published with a fortnight added at a time, allowing data for each two-week period to be analysed. The Vaccine Surveillance report data, on the other hand, only appears in four-week chunks a week at a time, preventing finer analysis, and only goes back to August.
What is really needed, of course, is for the full anonymised data to be released so that it can be analysed independently of Government and its favoured scientists. This is what those in Government and Parliament who care about transparency and truth should be pushing hard for, as without such full transparency the scope for real accountability is limited.
In the meantime, this real-world data from PHE, with infection rates in the double-vaccinated hugely outpacing those in the unvaccinated across many age groups, continues to make a mockery of the vaccine passports and mandates that have become oddly popular even as the data mounts-up that they are pointless.
Some Ontario towns won’t let couples get a marriage license without a vaccine passport
By Ken Macon | Reclaim The Net | October 10, 2021
In Oakville, Ontario in Canada, engaged couples will have to show a vaccine passport to attend a meeting for a marriage license. The only way around the requirement is to get married in a different town.
“Appointments for marriage licenses and ceremonies that have already been booked prior to September 22 will not require proof of full vaccination,” the city website says. “…however, any new appointments for marriage licences and ceremonies will be required. Ceremonies will be held inside town hall as of November 4, 2021.”
A marriage license is a requirement to be recognized as legally married in Canada. In Oakville, a marriage license cannot be obtained online.
“You must schedule an appointment to receive your marriage licence,” the city’s website says. “To be eligible for an appointment, please ensure that the intended date of your marriage is finalized and you have an officiant that has agreed to perform the marriage.”
Additionally, a couple might not get married if they do not pass a screening at the city’s building.
“When you arrive at Town Hall for your scheduled appointment, you will be required to complete a COVID-19 self-assessment,” the city said. “If you do not successfully meet the screening criteria, you will not be allowed to enter the building and your appointment will be canceled.”
The city’s requirement for proof of vaccination for marriages is in line with the vaccination mandate implemented in Ontario last month.
Related: How vaccine passports are crushing freedom, privacy, and civil liberties
A Message To Fauci: You Are In No Position To Dictate The “Greater Good”

By Brandon Smith | Alt-Market | October 6, 2021
How does a fraud like Anthony Fauci find himself in the highest paid position in US bureaucracy? Well, Fauci’s career is a rather shocking testament to the reality of our government and our era – The more corrupt you are the more favors and promotions you will receive.
Fauci is well known as a shameless opportunist among many within the medical research community. For example, the creator of the Polymerase Chain Reaction (PCR) Test, Kary Mullis, had nothing but disdain for Fauci. Mullis was an interesting figure who valued scientific honesty above all else. He often warned that his PCR test could be exploited to inflate infection numbers by identifying remnants of a virus in a person’s body without distinguishing whether or not they are actually “infected” (sick). Sadly, his test is now being used in this exact manner today to exaggerate infection rates of the covid-19 virus.
In interviews Mullis has referred to Anthony Fauci as a “liar”, arguing that he is a bureaucrat that “doesn’t know anything about anything”. Mullis noted that people like Fauci have an agenda that is outside of the public good, and that they have no problem misrepresenting the science to the populace to achieve their goals. It should also be noted that YouTube has made it their mission to consistently erase any traces of the Mullis interviews mentioning Fauci from their website.
It is also not surprising that Fauci’s rampant fear mongering over AIDS in the 1980’s has gone mostly unmentioned by the mainstream media. His claim that 1 in 5 heterosexual Americans would be dead from AIDS by 1990 has been summarily memory-holed and the guy is treated like a scientific genius by the journalistic community in 2021.
If there is any justice in this world then Fauci should really go down in history as one of the primary initiators of the Covid pandemic, being that he was a director of the NIAD and the National Institutes of Health (NIH) while overseeing the funding of Gain of Function research on corona-viruses at the Wuhan Lab in China. This is the same research that Fauci blatantly lied about to congress on multiple occasions. And, the Wuhan lab is the same lab that evidence suggests was the ground zero source of the Covid-19 outbreak.
It is important to note that it was Fauci and the NIH that LIFTED the ban on gain of function research on deadly viruses in 2017, and it was well known around this time that the Level 4 Wuhan lab in China was not secure.
If anyone is responsible for global covid deaths, it is Fauci, the Chinese government and anyone else involved in that gain of function research which is primarily used to WEAPONIZE viruses under the guise of creating “therapeutics.” Gain of function research was originally banned under the Biological Weapons Convention which went into effect in 1975, unless it was being used for therapeutics. Now ALL gain of function research that is revealed publicly is labeled as therapeutics even if it is actually designed to produce biological weapons. This is sometimes referred to as “dual use research.”
The prevailing narrative continues to be that even if the virus came from the Wuhan lab then it was surely an accident. I continue to believe according to the available evidence that Covid-19 was deliberately released in order to create a global crisis which could then be exploited by the establishment to introduce extreme controls over the populace to the point of medical totalitarianism. But of course, there is no smoking gun to prove this, only common sense.
If we take the notorious Event 201 into account things get a little weird. Event 201 was a war game held by the World Economic Forum and the Bill and Melinda Gates Foundation. Its claimed purpose was to simulate the effects of a deadly coronavirus pandemic “spread by animals” to humans and to develop the policies governments and their corporate partners should employ to deal with it. Interestingly, this simulation was held in October of 2019, only two months before the REAL THING happened. Nearly every policy suggested by the participants of Event 201 has now been adopted by most governments, including the social media censorship campaign against anyone that questions the origins of the virus and the safety of the experimental mRNA vaccines.

Anthony Fauci and friends….
WEF founder Klaus Schwab was quick to announce at the start of the pandemic that Covid-19 was the “perfect opportunity” to launch the “Great Reset”, which is a globalist plan to completely erase free market systems and replace them with a highly centralized socialist framework. The WEF envisions a world in which carbon related power is banned, all financial transactions become digital and are monitored and controlled by central authorities, and they have even suggested that one day people will “own nothing and be happy”. This is a reference to the so-called “shared economy” of the future, where the concept of personal property is abolished and all people will live in communal housing collectives where necessities are rationed or rented out to them by the government.
Something must have went wrong with covid, however, because the Event 201 death estimates for such a virus were around 65 million within the first year of the outbreak. This of course never happened with Covid-19. So, the resistance to the mandates has been high, or much higher apparently than the globalists expected. They have been forced to engage in an endless fear campaign for the past 18 months over a virus with a mere 0.26% median death rate. It is a virus that well over 99.7% of all people will survive and it has an extremely low chance of long term effects on those who do actually end up hospitalized. In the majority of states the hospitalization rates are between 10-35 people for every 100,000 people infected.
These numbers come from the CDC and the medical establishment at large, yet they are ignored by propagandists like Fauci, just as Fauci has continued to ignore natural immunity as a factor in covid mandates. It might seem bizarre to almost any scientist, doctor and virologist not paid by the government, but Fauci has argued that natural immunity should be ignored when compared to vaccination. Multiple studies from around the world now show that natural immunity is up to 27 times more effective at preventing covid infection than the vaccines, but those with natural immunity are considered a threat to others under the new mandates unless they are also vaxxed.
This simply makes no sense from a scientific perspective until you realize that the mandates are not about science, they are about authoritarianism. Fauci is the US front man for a campaign of medical tyranny being imposed in every nation; this is why he does not care about natural immunity. The idea of it is inconvenient to his narrative, so he pretends it is inconsequential.
It is perhaps ironic that Fauci himself is becoming inconsequential as he is slowly fading away from the media limelight. I have noticed that ever since the NIH gain of function information was released to the public Fauci has been in the media less prominently. A documentary produced by National Geographic and soon to be distributed by Disney+ portrays the conman as a misunderstood savior and is sure to be a trash fire. That said, it does represent a clear last-ditch effort to save the man’s false reputation.
There is a good reason for all of this. Fauci’s distaste for personal freedom has been well documented and is making him extremely unpopular. He even recently argued on CNN in favor of vaccine mandates using this perverse position:
“There comes a time when you do have to give up what you consider your individual right of making your own decision for the greater good of society.”
Fauci and his globalist ilk can be distilled down to this single mantra: Do as you are told for the greater good. But who gets to determine what the “greater good” is? Isn’t it disturbing that it’s always the same elitists that end up in that position? I know that leftists in particular love the idea of the vaccine mandates and worship Fauci, and they say we skeptics should “listen to the science”, but Fauci is not a scientist, he’s a door-to-door salesman, and as I’ve noted above the REAL science does not support the arguments for forced vaccinations or lockdowns.
Hell, I keep asking the same questions on the mandates in these articles and not a single leftist or pro-vax proponent has come up with a valid or logical response, but out of morbid curiosity I would love to see Fauci give his answers:
1) Covid has a median death rate of only 0.26%, so why should we take ANY risk on an experimental mRNA vaccine with no long term testing to prove its safety?
2) Why not give support to the 0.26% of people actually at risk from dying due to covid instead of spending billions of dollars on Big Pharma producing a rushed vaccine that you plan to force on the 99.7% of people who are not at risk?
3) In majority vaccinated countries like Israel, over 60% of covid hospitalizations are fully vaccinated people. The exponential rise of fully vaccinated patients in multiple nations suggests that the vaccines do not work. Why should we take a vaccine that has been proven not to be effective?
4) If you believe the vaccines actually do work despite all evidence to the contrary, then why should vaccinated people fear anything from unvaccinated people? How are we a threat to them?
5) If the vaccines don’t work, then doesn’t this mean the mandates are pointless and the people that are most safe are the people with natural immunity? Shouldn’t we be applauding the naturally immune and encouraging treatment instead of useless vaccination?
6) Since the vaccines actually don’t work according to the data, isn’t it time to stop blindly dismissing treatments like Ivermectin and focus on trials and studies that research these alternatives? Why the vitriolic propaganda campaign to label Ivermectin nothing more than “horse paste” when it is actually a long used Nobel Prize winning treatment for human ailments? Is it because the experimental covid vaccines would lose their emergency authorization status under the FDA if effective treatments exist?
7) Why are government funded scientists so keen on defending Big Pharma to the point of ignoring all data that contradicts their claims? Are you just embarrassed of being wrong, or are you corrupt?
8) Who decided you are qualified to determine what constitutes the “greater good?”
Globalists and errand boys like Fauci will never be able to answer these questions without twisting the narrative. They will say “What about the 700,000 dead in the US?” to play on the idea that the freedom minded lack empathy for their fellow man. Of course, around 40% of those deaths are patients from nursing homes with preexisting conditions, so we have no idea if they died from covid or from their previous ailments. Also, millions of people die every year from a plethora of communicable diseases including the flu and pneumonia, and we never tried to lock down the entire country and crush people’s civil rights because of this.
If we maintained a running tally of flu and pneumonia deaths year after year as we are doing with covid, then the ever increasing number of bodies would seem just as forbidding. Society cannot function when it is preoccupied with death.
Yes, around 0.26% of people die from covid, but life goes on for everyone else. Our freedoms are more important than your irrational fears. Our freedoms are more important than globalist agendas for centralization. Our freedoms ARE the greater good. Without them our society dies, and as our society dies millions more people will die from the inevitable collapse and tyranny that will follow; far more than will ever die from covid.
This is why nothing Fauci says has any relevance to us. He is so transparent in his corruption that he might as well be invisible. We will continue to ignore his declarations and admonitions and we will continue to fight back against the vaccine passports and restrictions. When all is said and done, if Fauci, Biden and other globalist puppets try to use force to impose their agenda upon us then there will come a day very soon when they will be held accountable for their crimes against humanity, and then they will wish they were invisible.
You can contact Brandon Smith at: brandon@alt-market.com
Featured Video

Iran Blockade Complications
or go to
Aletho News Archives – Video-Images
From the Archives
A low-fat, high-carb diet has been the largest public health experiment in history. It’s past time for a rethink.
By Malcolm Kendrick | RT | November 25, 2020
New research suggests that four billion people globally will be overweight in 2050. This trend can be traced back to the ‘low-fat, high-carb’ guidelines first issued in the 70s, and should prompt a major U-turn on dietary advice.
A recent report from the Potsdam Institute predicts that by 2050 there will be four billion overweight people in the world, with one-and-a-half billion of them obese. This is not entirely surprising. The world has been getting fatter for years, and things do not seem to be slowing down.
Why is this happening? … continue
Blog Roll
 Aletho News
Aletho News- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- COVID Conniving Receives First Federal Indictment
- Iran Blockade Complications /Lt Col Daniel Davis & Nima Alkhorshid
- Pirates of Mediterranean: Israel does as it pleases in the Sea of Three Continents
- Minab children massacre not ‘unfortunate situation’ but ‘heinous war crime’: Tehran
- OPCW Forced To Pay Damages To Whistleblower Who Found Evidence Of False Flag In Syria
- Iran can thrive under blockade, the US and its allies cannot
- Iran slams US leadership, debunking fabrications, false war costs
- Here’s why Iran is sovereign and Germany is not
- Israel pours $730m into global propaganda machine as reputation collapses
- If Americans Knew
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
