GAINESVILLE, Florida – Florida Gov. Ron DeSantis announced on Friday that the city of Gainesville has withdrawn a COVID-19 vaccine mandate for workers after pressure from his administration and a court ruling against the policy last month.
“We are not going to allow our first responders and government employees, many of whom have been on the front lines for over a year and a half, to be cast aside by local politicians’ mandates,” DeSantis said in a press release. “This reversal by the City of Gainesville is a victory for liberty.”
According to the press release, the Florida Department of Health (FDOH) received a letter from Gainesville last week informing the department that city commissioners “voided” a recent vaccination mandate for all public employees.
The FDOH had written to Gainesville mayor Lauren Poe days earlier, threatening to enforce a law signed by DeSantis in May that bans government entities, schools, and businesses from demanding COVID vaccination status. The law, S.B. 2006, allows up to $5,000 in fines per violation.
Gainesville told the health department in response that there are now “zero employees who are subject to a City COVID-19 employer vaccination requirement.”
“Please be advised that on September 23, 2021, the City Commission of the City of Gainesville took action to rescind their August 5th action related to COVID-19,” city manager Lee Feldman wrote, adding that the vaccine rules “have been voided.”
The day before the FDOH notice, a Florida judge temporarily halted Gainesville’s vaccine mandate following a lawsuit brought by city workers and backed by the DeSantis administration.
“The city failed to put on any evidence that the Vaccine Mandate serves a compelling state interest or that the Vaccine Mandate was the least restrictive means to accomplish that interest,” Circuit Judge Monica Brasington ruled September 22. Gainesville, in fact, “did not put on any evidence, at all, at the injunction hearing,” she noted.
The City Commission of Gainesville voted to rescind the rule the next day.
More than 200 city workers, including police officers, firefighters, and other first responders, sued to block the mandate, with the backing of Florida Attorney General Ashley Moody, a Republican who filed a brief in support of the workers in September.
Last month, Gov. DeSantis announced that Florida would move to penalize violations of the state’s ban on COVID-19 vaccine requirements, such as those in Gainesville, with “millions of dollars” in fines.
“If a government agency in the state of Florida forces a vaccine as a condition to employment, that violates Florida law, and you will face a $5,000 fine for every single violation,” the governor declared at a press conference near Gainesville. “If you look at places here in Alachua County, like the city of Gainesville, I mean, that’s millions and millions of dollars potentially in fines.”
“We will certainly move to impose the fines as the law requires when we see people that are denied access,” he said.
The DeSantis administration continues to fight local vaccine mandates in multiple counties, including Leon County, where city officials confirmed this weekend that they fired 14 employees who refused to disclose their vaccination status by Friday, in violation of S.B. 2006.
The FDOH had warned the county last week that it must “immediately rescind” the coercive vaccine policy and “refrain from terminating any employees who decline to produce proof of vaccination.”
“Fines may be assessed based on each employee who was required to submit proof of vaccination as a condition of continued employment,” wrote Doug Woodlief, FDOH division director for Emergency Preparedness and Community Support. Those fines could cost Leon County over $3.5 million, according to the Tallahassee Democrat.
Orange County also faces potential fines due to an ongoing COVID vaccine mandate, which prompted a lawsuit from dozens of firefighters last week, local news reported. The county downgraded the mandate days after Gov. DeSantis’ press conference last month, but has harassed unvaccinated employees and impeded them from being promoted, firefighters have said.
The Gainesville workers’ victory against compulsory COVID vaccination follows similar recent successes in other states. In Arizona, the city of Tucson backed down on a vaccine mandate last month after Republican Attorney General Mark Brnovich threatened to withhold up to $175 million in funding from the city, citing state laws enacted by Republicans earlier this year.
October 7, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Three US medical certifying boards have warned doctors that they risk losing their certification and licence if they spread covid vaccine misinformation.
Internists, family doctors, and paediatricians received an email on 9 September that quoted a warning from the Federation of State Medical Boards in July1 which read: “Providing misinformation about the covid-19 vaccine contradicts physicians’ ethical and professional responsibilities, and therefore may subject a physician to disciplinary actions, including suspension or revocation of their medical licence.”2
Richard Baron, president and chief executive of the American Board of Internal Medicine (ABIM), told The BMJ that the move was an attempt to establish a standard of care. “As standard setting organisations, we thought it was important to be on record, in a public way, to make clear that putting out flagrant misinformation is unethical and dangerous during a pandemic.” Baron said that the statement has been well received—“4 to 1 positive.” But community physicians contacted by The BMJ thought differently.
“When I got that email I thought I’d better not put anything on social media about vaccines,” said Shveta Raju, a community physician in the Atlanta, Georgia, area, who has treated covid patients and led the vaccination effort at her outpatient clinic.
“The email was sent more as a veiled threat to keep doctors on the official, established narrative, and that’s what I find chilling,” said a paediatrician who pseudonymously blogs under the name Elizabeth Bennett. “Pandemic or no, there is a problem with having an ill defined concept of misinformation that’s tied to public health messaging that hasn’t been consistent. How are physicians supposed to figure out what is misinformation when public health messaging swings so wildly?” Bennett asked.
Undefined offence
Baron said that the statement was also intended to signal the certifying boards’ support for physicians “trying to do the right thing.”
“We wanted to support that group and say ‘hey, we do have a standard of care here and you are doing the right thing when you uphold it,’” he said.
Raju responded, “If that was their intent, they should have defined misinformation. By leaving it undefined, the message was that we can’t talk about this at all.” She said that physicians are, by and large, a conservative group. “If they’re not sure what can be deemed misinformation, physicians would rather be quiet.”
Bennett concurred: “The thing I find most alarming is that they don’t define misinformation, but if they strip you of your board certification, you would lose your means of earning a living.”
Doctors spreading misinformation?
Official and social media company efforts to target “vaccine misinformation” predate the pandemic.3 But the new statement from ABIM, the American Board of Family Medicine, and the American Board of Paediatrics is one of several recent statements putting doctors in the spotlight for the first time.
In Canada, warnings about physician information began earlier, when in April the College of Physicians and Surgeons of Ontario declared that physicians “have a professional responsibility not to communicate anti-vaccine, anti-masking, anti-distancing, and anti-lockdown statements or promote unsupported, unproven treatments for covid-19.”4
The Canadian statement triggered an outcry, leading to a clarification that the statement was “not intended to stifle a healthy public debate about how best to address aspects of the pandemic.” But concerns continued. In June, a Canadian member of parliament held a press conference on censorship of Canadian clinicians and scientists. YouTube removed the video of the meeting.56
The BMJ asked ABIM about the size of the problem of board certified physicians spreading misinformation.
“We don’t have a sense of numbers of physicians spreading misinformation,” Baron said. “We’re at the beginning.” He believed it was only a “small number of doctors.” The medical boards opted to send the statement to all doctors, he said, because focusing on just the offending individuals would “miss the impact they’re having because of how much their voices are being amplified.”
As an example of “unprofessional or unethical behaviour,” Baron cited the case of a Florida doctor offering medical exemptions from mask wearing for $50 (£37; €43).7
Personalised medicine—or one-size-fits-all?
The BMJ asked whether physicians expressing doubt about the need for booster doses or vaccination of patients with natural immunity—two matters that have been the subject of debate and changing official guidance—would qualify as misinformation.8 “I don’t think we have concerns with doctors wrestling with areas where the science is unclear,” Baron said, “but there is no debate about whether people should get a primary vaccination series.”
Raju worries about the impact on personalised care. “The job of physicians is to take guidelines and apply them to the patient in front of them.” But now “physicians are basically being told that when it comes to covid vaccines it’s one-size-fits-all.”
Baron said, “We’re not trying to stifle conversations between doctors and patients. We understand that different people may look at evidence in different ways, but when you have an overwhelming preponderance of medical consensus in a certain area, you need at least to tell patients that there is an overwhelming professional consensus here.”
Cautious approach
Jeffrey Flier, former dean of Harvard Medical School, said that in the context of the pandemic, he was “not opposed to certain levels of misinformation triggering a decision to question somebody’s licence.” He said, “I can see this being an appropriate remedy at a time of public health emergency.
“But this is not how the system for licensure and certification has traditionally worked, and creates many opportunities for mistaken judgment about what is and is not misinformation, and those decisions would have to be rendered with extreme caution.”
Flier added, “We have to remember that there are legitimate areas of debate, and such matters should not fall within the scope of disciplinary actions.”
“There are reasons to be concerned that state boards might be unprepared for these kinds of decisions at a time when so many aspects of covid policy have been enmeshed with political views.”
Footnotes
-
This article was updated on 4 October to make clear that it was medical certifying boards, rather than licensing boards, that emailed physicians. The email quoted an earlier warning from the Federation of State Medical Boards.
-
Competing interests: PD gave a public statement at a 17 September 2021 FDA advisory committee to discuss covid-19 vaccines, where he highlighted the joint statement. The views and opinions expressed here are those of the author and do not necessarily reflect official policy or position of the University of Maryland.
-
Provenance: commissioned; not externally peer reviewed.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usage
View Abstract
October 7, 2021
Posted by aletho |
Deception, Full Spectrum Dominance, Science and Pseudo-Science, War Crimes | Canada, Covid-19, COVID-19 Vaccine, Human rights, United States |
Leave a comment
Imagine you’re a doctor. You go into work every day for long hours and figure out how to treat Covid. You are saving lives and doing so patient by patient. Each patient has individual needs that sometimes require custom care, but you know early treatment works.
Suddenly, faraway bureaucrats demand that you abandon your best practices and fall into line around their grand plan. Suddenly your patients can’t get what you prescribe. Media apparatchiks diminish, invalidate or mock everything you’ve learned and are doing.
And all of it is being carried out in the name of “science.”
The Physicians’ Rebellion
More than 10,000 physicians and medical scientists have signed onto a Declaration that accuses public health authorities of, well, doing it wrong–and to devastating effect.
“WHEREAS, public policy makers have chosen to force a “one size fits all” treatment strategy, resulting in needless illness and death, rather than upholding fundamental concepts of the individualized, personalized approach to patient care which is proven to be safe and more effective;”
The Declaration goes on to assert that “thousands of physicians are being prevented from providing treatment to their patients, as a result of barriers put up by pharmacies, hospitals, and public health agencies” and that “These policies may actually constitute crimes against humanity.”
Local Knowledge
Such statements might strike non-physicians as hyperbolic. But consider that many of these doctors, such as Dr. Brian Tyson have each saved thousands of lives through early intervention and best practices developed in the field through trial-and-error, observation, and active communication among peers.
“We started seeing inflammation, so we used anti-inflammatories,” Dr. Tyson explains.
“We saw blood clots, so we used anticoagulants. We saw patients having trouble breathing, so we used asthma medications… It wasn’t just one drug. It was the art of what we see and how those patients responded to what we gave them.”
Despite treating more than 6,000 patients, Tyson can count the patients he’s lost to Covid on three fingers. And yet non-practicing officials are interfering with the work of doctors like Tyson.
The physicians and medical scientists who have signed the Declaration are also frustrated with the authoritarian measures supported by career bureaucrats such as Anthony Fauci. Indeed as more information trickles out, more and more observers suspect Fauci approved funding for dangerous research at the Wuhan Institute of Virology and then colluded with the bioethically disturbed Peter Daszak to propagate the unlikely “natural origins” theory.
Barriers to Treatment
Public health authorities have erected huge barriers to early treatment by:
- Putting pressure on major pharmacies not to fill essential prescriptions,
- Putting pressure on insurers not to cover proven therapies, and
- Putting pressure on Big Tech giants to censor and suppress eminent physicians such as cardiologist Peter A. McCullough, who has expressed concerns about vaccinating children.
Declaration signatories include physicians who figured out how to successfully reduce the death toll while public health authorities dithered and delayed their grand plan to roll out mRNA vaccines for everyone — including, apparently, low-risk populations.
All the doctors agree that greater access to early treatment could have saved thousands of lives–and could save thousands more. The Declaration suggests that public health authorities are trying to steamroll over clinical practitioners when these camps should complement each other.
“We are in a pandemic of undertreatment,” said intensive care specialist Pierre Kory, M.D., winner of the British Medical Association’s President’s Choice Award.
“Everything else that we’ve discovered, everything that’s in our protocols is because we have used good clinical sense, lots of experience, and we’ve used trial and error using our best judgments of risks and benefits.”
Clinicians or “Experts?”
Why should anyone trust thousands of doctors and medical researchers over public health authorities and other so-called experts trotted out in media campaigns?
- Physicians figured out how to save lives and control Covid by talking to each other and developing best practices.
- Physicians have more local knowledge and more direct experience with real patients.
- Physicians are not as beholden to pharmaceutical companies as public health authorities, particularly as these authorities have gone as far as mandating pharma products for millions.
- Physicians have learned to scale up their practices, including telemedicine, to avoid ‘hospital overwhelm.’
- Physicians have learned that early treatment and natural immunity is an effective way to reduce the dangers of a pandemic whose virus was probably funded by… public health authorities.
It’s no wonder these doctors are in open rebellion against authoritarian public health bodies who seek to implement monolithic mass behavioral control in place of a dynamic multi-pronged approach that includes clinical best practices.
Intimate, repeated, in-person care, which includes both observational and randomized control studies, has an underappreciated advantage over armchair analysis and “exciting, soul-capturing abstractions,” which have “extended themselves over the perception of world and self like plastic pillowcases.” And yet the doctors of the Physicians Declaration soldier on.
Nevermind. Fall into line. The government is here to help.
Note: The Declaration by the International Physicians and Medical Researchers is not affiliated with The Great Barrington Declaration hosted by AIER. Yet there are striking similarities in that each group represents a groundswell of opposition to authoritarian public health policies worldwide.
Max Borders is author of After Collapse: The End of America and the Rebirth of Her Ideals and The Social Singularity: A Decentralist Manifesto.
October 7, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19 |
Leave a comment

A study appeared in the Lancet this week confirming that vaccine effectiveness against infection is fading fast.
The study involved 3,436,957 people over the age of 12 who are members of the healthcare organisation Kaiser Permanente Southern California. It sought to assess the effectiveness of the Pfizer vaccine against SARS-CoV-2 infections and COVID-19-related hospital admissions for up to six months, with a study period covering December 14th, 2020, to August 8th, 2021.
Comparing fully vaccinated to unvaccinated, and controlling for confounders such as prior infection, the researchers found that effectiveness against infection plummeted from 88% (95% confidence interval 86-89%) during the first month after double-vaccination to 47% (43-51%) after five months. The variation by age (depicted above) was largely within the margins of error.
Among sequenced infections, the researchers found vaccine effectiveness against Delta infection was 93% (85-97%) during the first month after double-vaccination but dropped to 53% (39-65%) after four months. Effectiveness against infection from other variants the first month after double-vaccination was 97% (95-99%), but declined to 67% (45-80%) at 4-5 months.

Pfizer vaccine effectiveness by Covid variant
Vaccine effectiveness against hospital admissions for Delta infection held up at around 93% (84-96%) for the six months across all ages.

Pfizer vaccine effectiveness against Covid hospitalisation
However, the researchers note that the latest data from Israel “suggests that some reduction in effectiveness against hospital admissions has been observed among older people (65 years and over) roughly six months after receiving the second dose of [Pfizer]”.
One question that’s arisen recently is to what extent vaccine effectiveness estimates are affected by whether more people who have been previously infected decide not to be vaccinated. According to this study the answer is: not very much at all. Among the unvaccinated, 2.3% had one or more previous positive PCR tests, only slightly more than the 2% of the double-vaccinated who did.
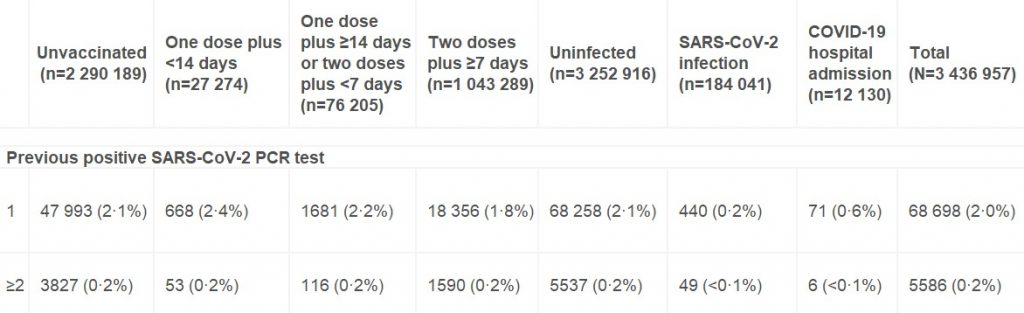
Number and percentage of individuals with one or more previous positive PCR tests
It’s also worth noting that although this study adjusts its raw estimates for no fewer than 22 potential confounding variables, the adjusted figures differ very little from the unadjusted figures in almost all cases. This suggests that unadjusted estimates from large population samples are often a fair approximation in the absence of sophisticated statistical analysis.
Given that the adjusted figures were little different to the unadjusted figures, however, it’s not immediately clear why the vaccine effectiveness estimates in this study, while low and declining, are so much higher than the latest unadjusted estimates derived from Public Health England data (namely, negative vaccine effectiveness in the over-40s, including minus-66% in those in their 40s). It doesn’t appear to be merely a matter of additional time elapsing, as most people in the U.K. weren’t double vaccinated until April, May or June, meaning only four or five months have elapsed until September, the same time period as in the study.
Could it be because the study period ended on August 8th, when the Delta surge in California was just getting going (see below)?
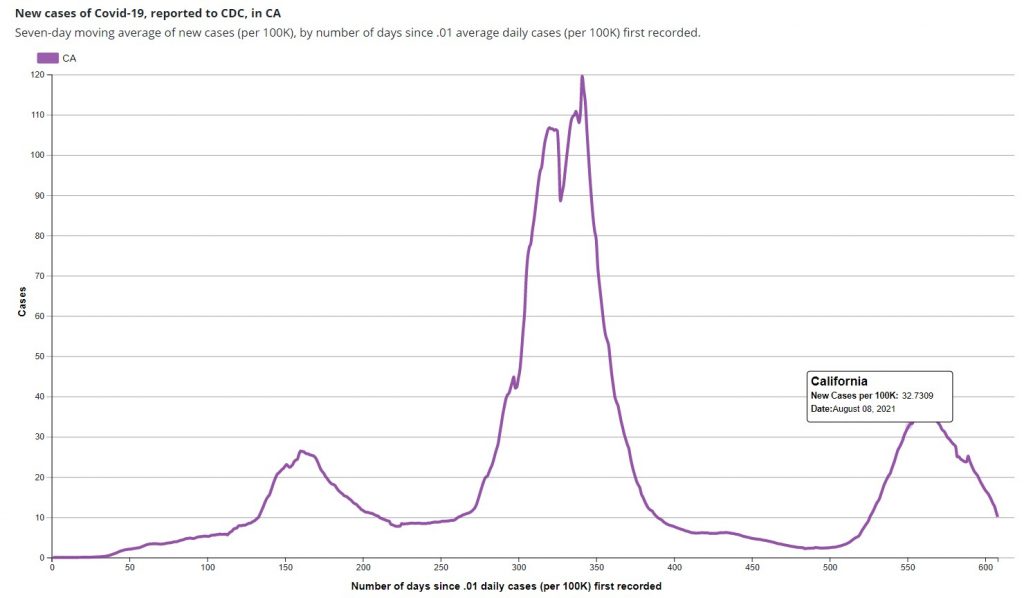
In the U.K. the vaccine effectiveness didn’t plunge until the second half of the Delta surge, the first part being dominated by infections in the unvaccinated (for reasons still not entirely clear). Did the new study finish too early to see the dramatic effect we’ve seen in England?
The authors say their study indicates that the decline in vaccine effectiveness is primarily a function of time rather than variant-related. However, the evidence from England would suggest otherwise, as in the same period of time, but later in the Delta surge, the decline has been far greater.
The decline in vaccine effectiveness in England was confirmed last week in a new Government-funded study (not yet peer-reviewed), which found that the reduction in transmission “declined over time since second vaccination, for Delta reaching similar levels to unvaccinated individuals by 12 weeks for [the AstraZeneca vaccine] and attenuating substantially for [Pfizer]”. In other words, within just three months AstraZeneca did nothing to prevent transmission, and Pfizer was scarcely better.
One of the main recommendations of the authors of both studies in light of their findings is for regular booster jabs – in the case of the first, where many of the authors are employees of and investors in Pfizer, this may be deemed hardly surprising. However, if effectiveness against serious disease is holding up, why give people boosters just to stop them getting and spreading what is effectively a cold, and which bestows more robust immunity as it goes? Furthermore, if the effectiveness declines after as little as three months, is it even possible to deliver enough boosters to have any impact on infection and transmission? Would it not be much better to say that the vaccines, by offering personal protection from serious disease to those who want it, have done their job? Better to move on and abandon any ideas of vaccine passports and mandates and boosters, and in general the now almost wholly pointless obsession with Covid vaccines.
October 7, 2021
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine |
Leave a comment
Right in the midst of a global political effort to reduce fossil fuel consumption, Japan is set to increase its fossil fuel use and imports as an expected colder-than-normal winter approaches.
The country’s meteorological department recently released its weather outlook for the upcoming winter, which expects that most regions will experience either 30-year-average or below average temperatures between December and February.
Climate Narrative vs. Energy Reality
Blind belief in the global warming narrative can catch nations off guard, risking severe energy crises due to unpreparedness. There is an old axiom that says, “Measure twice, cut once.” It reiterates the need for careful planning before embarking on a task. Doing so saves time and energy and prevents mistakes.
The axiom is extremely relevant in energy policy planning. With the ascendancy of the climate global warming narrative, many nations are susceptible to believing climate-model projections that may not reflect real climate, much less actual weather patterns.
On-the-ground weather forecasts contradict the narrative that winters will be milder. A Washington Post article read, “Winters are Shrinking.” Environmental Defense Fund claimed, “Winters are warmer” and “cold streaks are rarer.”
Such false climate forecasts can lead to chaos due to unpreparedness. Texas got suckered into this belief, making the great freeze of February 2021 shocking.
Japan, an energy-intensive country, is one such country where warmer world–milder winters can cause significant disruptions to energy planning. But this country is wise enough not to get caught in this global propaganda. It is aware of the importance of trusting regional weather patterns.
Fossil Fuels Deliver
Fossil fuels are the preferred energy source in many countries for tough winter conditions as they are the only dependable and affordable fuel source—alongside nuclear—in cold and snowy conditions.
Wind turbines work only in certain geographical regions and in certain months when wind speed is optimum. But in cold weather, they are not reliable. According to the government of Canada,
the operation of wind turbines in a cold climate such as Canada’s involves additional challenges not present in warmer locations, such as: Accumulation of ice on wind turbine blades resulting in reduced power output and increased rotor loads; Cold weather shutdown to prevent equipment failure; and Limited or reduced access for maintenance activities.
For these reasons countries like China and Japan depend heavily on coal, natural gas, and oil, instead of the highly unreliable wind and solar. The Japanese authorities know they cannot leave millions to freeze in the cold and have decided to stock up enough fossil fuels to sustain during the winter. S&P Global notes, “Japan’s demand for coal, LNG, crude and fuel oil for power generation as well as city gas and kerosene for heating was robust in January as a result of severe cold spells.” The scenario is likely to repeat this year.
Other Countries Too
Winter energy crises are of great concern the world over. The Japanese are very close to China, a country which in recent years has experienced severe energy shortages during winters due to its reluctance to increase coal consumption. A partial coal ban in northern provinces caused severe winter heating problems in recent years.
This year, news agencies in China predict widespread power blackouts in more than a dozen provinces as the country is critically short of coal and some power plants have stopped producing coal power due to high coal prices.
Japan, which has a bird’s eye view, is aware of the power shortage in China. So, to avoid a similar situation at home, Japan will not restrict the use of coal, natural gas and oil during winter months.
The demand for oil and gas is not just in Japan. The UK, too, is highly reliant on imported natural gas for winter heating needs, and analysts have urged the country to secure its resources before winter induces a power demand surge.
“If the winter is actually cold, my concern is we will not have enough gas for use for heating in parts of Europe. … it won’t only be a recessionary value, it will affect the ability to provide gas for heating. It touches everybody’s lives,” said Amos Hochstein, the US State Department’s senior adviser for energy security.
The Future is Now
The combined rise in demand for fossil fuels from Europe, China, India, Vietnam, and Japan has led to an increase in coal and natural gas prices. Investors see a “natural-gas crunch spilling into crude market, lifting oil prices.” OPEC, in its newly released World Oil Outlook 2045, observes that “oil will be leading energy source for decades (at least until 2045) as crude reaches 3-year highs.”
The demand for fossil fuels and the sharp increase in fossil fuels prices indicate that these energy fuels still dominate the global energy sector. The winter rush for fossil fuels also confirms their effectiveness in delivering reliable energy during cold weather.
COP26 planners, are you listening?
———————————–
Vijay Jayaraj (M.Sc., Environmental Science, University of East Anglia, England), is a Research Contributor for the Cornwall Alliance for the Stewardship of Creation and resides in Bengaluru, India.
October 6, 2021
Posted by aletho |
Economics, Science and Pseudo-Science | Japan |
Leave a comment
Yesterday I noted that, 18 months after the start of the pandemic, a sizeable chunk of Americans still dramatically overestimate the risks of Covid. In a recent poll, more than one third said the risk of being hospitalised if you’re not vaccinated is at least 50%.
Of course, you’d expect some people to get the answer wrong just because we’re dealing with a small quantity, and there’s always going to be some degree of overestimation. But many people were off by a factor more than 10. What accounts for this?
Interestingly, Democrat voters’ guesses were much higher than Republican voters’ – about twice as many Democrats said the risk of being hospitalised if you’re not vaccinated is at least 50%. This suggests a role for ideology.
Throughout the pandemic, the ‘Democrat position’ has been to support restrictions and mandates, whereas the ‘Republican position’ has been to oppose such measures. This is clearly visible in a plot of U.S. states by average stringency index. Almost all the ‘red’ states are on the left-hand side, while almost all the ‘blue’ states are on the right.
Given that partisans (on all sides) like to avoid cognitive dissonance, they tend to adopt beliefs that are consistent with their party’s platform. Since Democrat politicians have been busy imposing all sorts of restrictions and mandates, Democrat voters have adopted beliefs that imply those measures were justified.
Most survey respondents don’t know numbers like ‘the risk of hospitalisation for people who aren’t vaccinated’ off the top of their head. Instead, they probably make a guess based on all the relevant information they can recall.
Democrat voters, who’ve spent the pandemic consuming media like MSNBC, CNN and NPR, will recall numerous incidents of pundits saying that Covid is extremely dangerous, and we have to do whatever we can to stop the spread.
They will also recall that they were locked down for months, that their kids’ schools were closed, and that they had to wear a mask whenever they went to the grocery store.
Putting all this information together, they will tend to assume that the risk of being hospitalised from Covid is extremely high. ‘Why else,’ they might ask, ‘would there have been so many restrictions?’
Note: Republicans also overestimated the risk of being hospitalised from Covid, albeit to a lesser extent than Democrats. This indicates that people’s skewed risk perceptions cannot be blamed solely on the content of left-wing media (or the policies implemented in ‘blue’ states).
The psychological quirk that may account for people’s skewed risk perceptions has a name in psychology: the availability heuristic. As Steven Pinker notes, “people estimate the probability of an event or the frequency of a kind of thing by the ease with which instances come to mind”.
Because plane crashes always make the news, people tend to overestimate the risks of air travel. And they may overestimate the risks of Covid for the same reason.
Since the start of the pandemic, we’ve been treated to morbid ‘daily death numbers’ – but for only one cause of death. Perhaps if these figures had been reported for all causes of death, people’s risk perceptions would be slightly less skewed. (Or perhaps they’d just be terrified of everything…)
During a pandemic, we obviously do want people to take precautions; we don’t want them nonchalantly walking into a care home when they have a high fever and a nasty cough. Yet – contrary to what some in government seem to believe – we don’t want people to be utterly terrified either.
There’s been so much attention on people claiming Covid is “just the flu” that the media has largely ignored the other end of the spectrum: people who believe Covid is the bubonic plague!
We can agree it’s bad if people underestimate the risks. But it’s also bad if they overestimate the risks. We want them to have the right risk perceptions. That way, they can make informed decisions.
October 6, 2021
Posted by aletho |
Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular | Covid-19 |
Leave a comment
CNN reporter Randi Kaye visited my home unannounced, then tracked me down as I bicycled around my home town in August 2021. Her purpose was to publish a hit piece further labeling me as a “super-spreader of COVID-19 misinformation,”1 based primarily on the opinions of foreign agent Imran Ahmed, founding CEO Center for Countering Digital Hate (CCDH),2 which is a recently spun up front group funded by dark money.
https://twitter.com/AC360/status/1445192038845227008?ref_src=twsrc%5Etfw%7Ctwcamp%5Etweetembed%7Ctwterm%5E1445192038845227008%7Ctwgr%5E%7Ctwcon%5Es1_&ref_url=https%3A%2F%2Fblogs.mercola.com%2Fsites%2Fvitalvotes%2Farchive%2F2021%2F10%2F05%2Fsee-my-latest-response-to-cnns-hit-piece.aspx
After that story aired, she again contacted me, this time via email, to request an interview regarding my latest book, “The Truth About COVID-19: Exposing The Great Reset, Lockdowns, Vaccine Passports, and the New Normal.” Interview questions were provided via email, as were my responses. CNN ran this new story October 4, 2021.
In the interest of transparency, below I’ll post the email exchange so you can read my response to her questions firsthand. You can tell from the leading questions that this “story” isn’t true journalism but rather another hit piece manipulated to fit a preformed agenda.
CNN Interview Request for My Latest Book
August 26, 2021, Kaye emailed, “Here are the questions we would like answered about Dr. Mercola’s new book. We would welcome responses by 5pm tomorrow, please.” The questions, which are clearly accusatory, are as follows:
“You say in your book that “A large amount of data strongly suggests the COVID – 19 vaccine may be completely unnecessary, which means the global population is being bamboozled into participating in a dangerous and unprecedented experiment for no good reason whatsoever.” Can you please point us to that data that suggests the covid vaccines are unnecessary or dangerous?
You say in your book that “vaccine trials are rigged.” What proof do you have of that? Which trials? How many? Who rigged them and for what purpose?
You say in your book, “Common sense dictates that if the vaccines cannot prevent or reduce infection and transmission, hospitalization, or death, then they cannot possibly end the pandemic.” And that “There’s no telling whether they will ultimately prevent hospitalizations and deaths.”
Can you please provide us with the source and support for your statements since the CDC says vaccines are nearly 100% effective at preventing severe disease and death and greatly reduce infection.
How do you explain statements from hospitals and government officials that nearly all those who are getting sick and dying now are the unvaccinated?
Do you feel responsible for the spread of misinformation by writing a book full of conspiracy theories and false claims?
What were you paid for this book deal by the publisher?
Are you donating 100% of the earnings from your book?
If so, to which organization? Are you concerned this book will cost people their lives?”
My Response to CNN
Media organizations contact Mercola.com regularly, sometimes to challenge us on the researched, fact-checked articles we post for our readers. In CNN’s case, the information they were seeking was directly related to my book, which was the No. 1 best seller in all categories for four straight days with thousands of five-star ratings.
Much like the information on Mercola.com, the information in my book is thoroughly referenced, but Kaye, ironically, engaged in the dissemination of misinformation herself by describing my book as being “full of conspiracy theories and false claims.” My response to her questions follows:
“Many studies and other literature offer support for my position in answering several of your questions, which are combined since they can be answered with the same literature. Here are the important points that drive my book:
The vaccines are just 39% effective and waning, and the CDC’s Advisory Committee on Immunization Practices has now advised booster doses to the mRNA vaccines in immunocompromised persons. CDC’s goal is to begin offering booster doses to everyone else beginning this fall.3,4,5,6
Additionally, breakthrough infections among fully vaccinated persons are becoming more and more prevalent around the world. Evidence is beginning to mount that people with breakthrough infections can spread the Delta variant more easily.7,8,9,10,11,12,13
Most recently, researchers in Israel report that fully vaccinated persons are up to 13 times more likely to get infected than those who have had a natural COVID infection.
As explained by ScienceMag: The study “found in two analyses that people who were vaccinated in January and February were, in June, July and the first half of August, six to 13 times more likely to get infected than unvaccinated people who were previously infected with the coronavirus.
In one analysis, comparing more than 32,000 people in the health system, the risk of developing symptomatic COVID-19 was 27 times higher among the vaccinated, and the risk of hospitalization eight times higher.”14
The study also said that, while vaccinated persons who also had natural infection did appear to have additional protection against the Delta variant, the vaccinated were still at a greater risk for COVID-19-related-hospitalizations compared to those without the vaccine, but who were previously infected.
Vaccinees who hadn’t had a natural infection also had a 5.96-fold increased risk for breakthrough infection and a 7.13-fold increased risk for symptomatic disease.
“This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity,” study authors said.15
A majority of gravely ill patients in Israel are double vaccinated.16 A majority of deaths over 50 in England are also double vaccinated.17 Also, mass vaccination of the population with the highly mutating coronavirus will only evolve perfectly vaccine-resistant strains of the virus.”18
Injection Trials Included COVID-19 Infections as Successes
The next part of my response focused more specifically on the vaccine trials, which were problematic from the start since they did not include prevention of infection as an endpoint. Instead, all study endpoints required infection with SARS-CoV-2, and “successes” included subjects with confirmed COVID-19 cases. The difference measured wasn’t whether or not the vaccines prevented COVID-19 but whether, and how, they modified symptoms among those infected.19
Also problematic is the unblinding of the vaccine trials, which means the placebo groups were removed. As medical investigative journalist Jeanne Lenzer wrote in the BMJ, “The data are now likely to be scanty and less reliable given that the trials are effectively being unblinded.”20 This is the next section of my response to Kaye:
“Regarding the vaccine trials: The vaccine trials were designed specifically to succeed for profit. The public health authorities and media like CNN are utilizing fear of the virus to induce psychological stress that promotes obedience and servitude.21
Additionally, proof that the trials are “rigged” can be shown by virtue of the fact that they’ve done away with the control groups — who were getting a placebo but who were then offered the vaccine, which virtually does away with the ability to compare adverse reactions including deaths. Pfizer’s own vaccine insert for Comirnaty admits that the control group hasn’t existed since December 2020:
Section 6.1 — “Upon issuance of the Emergency Use Authorization (December 11, 2020) for COMIRNATY, participants were unblinded to offer placebo participants COMIRNATY. Participants were unblinded in a phased manner over a period of months to offer placebo participants COMIRNATY.”22
NPR has noted that removing the placebo groups from vaccine trials will prevent accurate data from long-term studies from being known.23
Additionally, the CDC is being dishonest by utilizing data from the beginning of this year when the vaccine campaign had just been initiated to conflate their claim. They are using data that were scant early in the year because so few were vaccinated, as opposed to using current information.24
Proceeding with the FDA approval of Comirnaty this week was unprecedented. No other vaccine has ever received approval this fast — and without public comment being allowed through ACIP [the CDC’s Advisory Committee on Immunization Practices] or VRBPAC [the FDA’s Vaccines and Related Biological Products Advisory Committee] before approval was issued.
The approval is unconscionable because over 600,000 adverse reactions and 6,000 deaths [now over 14,500 deaths25] have been reported in the U.S. to VAERS. A majority of these reports are filed by medical professionals.
This shows that the safety of these vaccines is not proven. Besides, the experiments are continuing through 2027 as the FDA APPROVAL requires Pfizer to submit study results analyzing risk of myocarditis and pericarditis, and risk to long-term infant development in pregnant women. Study results will be submitted to the FDA for review on Oct 31, 2025 and May 31, 2027 respectively.”26
Lifesaving Information That CNN Won’t Share
CNN and other media outlets have the power to share lifesaving information that could turn the pandemic around and save lives in the process — but they won’t. Instead, the media are ignoring the basics of healthy immune function and the importance of early COVID-19 treatment to continue to push the narrative that the only solution is to get an injection.
The last part of my response to Kaye includes empowering steps that virtually everyone can take to support their health and reduce their risk of infectious disease. This includes having supplies from the Front Line COVID-19 Critical Care Working Group (FLCCC) I-MASK+ protocol on hand in the event you do get COVID-19.
FLCCC’s I-MASK+ protocol can be downloaded in full,27 giving you step-by-step instructions on how to prevent and treat the early symptoms of COVID-19. FLCCC also has protocols for at-home prevention and early treatment, called I-MASS, which involves ivermectin, vitamin D3, a multivitamin and a digital thermometer to watch your body temperature in the prevention phase and ivermectin, melatonin, aspirin and antiseptic mouthwash for early at-home treatment.
I also recommend getting a nebulizer, and the moment you feel a sniffle or something coming on, use nebulized hydrogen peroxide. Having a pulse oximeter on hand is also wise, as it’s a noninvasive way to measure the oxygen levels in your blood, allowing you to monitor your levels and help gauge whether a trip to the ER is truly in order.
As I told Kaye, taking control of your health continues to be the “secret” that I strive to share with the masses. The remainder of my response to CNN follows:
“I am donating all proceeds to the National Vaccine Information Center. I encourage every person to fully educate themselves to make individual decisions about medical risk-taking by talking with their personal physician and comparing the risks and benefits to make an informed decision that includes all the information on how these vaccines are working (or not working) and what all the possible side effects may be.
This pandemic is a direct reflection of the health of our population: 95% of COVID deaths have multiple comorbidities. Obesity, vitamin D deficiency and metabolic dysfunction are at the core of this pandemic and can be resolved by taking control of your health by following science-based dietary and lifestyle recommendations.
Since building up your health can’t be done overnight, what you can do beginning right now is avoid linoleic acid, check to ensure your vitamin D levels are above 40ng/ml, exercise, get fresh air and proper sun exposure, and restrict your eating window to a 6- to 8-hour time frame each day.
If you do get COVID-19, early treatment is crucial. Follow the Front Line Critical Care Alliance iMASK+ or MATH+ treatment protocols.”28
Sources and References
October 6, 2021
Posted by aletho |
Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science | CDC, COVID-19 Vaccine |
Leave a comment
- Nick Karl, Pfizer Scientist: “When somebody is naturally immune — like they got COVID — they probably have more antibodies against the virus…When you actually get the virus, you’re going to start producing antibodies against multiple pieces of the virus… So, your antibodies are probably better at that point than the [COVID] vaccination.”
- Chris Croce, Pfizer Senior Associate Scientist: “You’re protected for longer” if you have natural COVID antibodies compared to the COVID vaccine.
- Croce: “I work for an evil corporation… Our organization is run on COVID money.”
- Rahul Khandke, Pfizer Scientist: “If you have [COVID] antibodies built up, you should be able to prove that you have those built up.”
[NEW YORK – Project Veritas released the fourth video in its COVID vaccine investigative series today which exposed three Pfizer officials saying that antibodies lead to equal, if not better, protection against the virus compared to the vaccine.
Nick Karl, a scientist who is directly involved in the production of Pfizer’s COVID vaccine, said that natural immunity is more effective than the very vaccine he works on, and Pfizer produces.
“When somebody is naturally immune — like they got COVID — they probably have more antibodies against the virus… When you actually get the virus, you’re going to start producing antibodies against multiple pieces of the virus… So, your antibodies are probably better at that point than the [COVID] vaccination,” Karl said. Notwithstanding, Karl still believes that vaccine mandates are positive for society.
“The city [of New York] needs like vax cards and everything. It’s just about making it so inconvenient for unvaccinated people to the point where they’re just like, ‘F*ck it. I’ll get it.’ You know?”
A second Pfizer official, Senior Associate Scientist, Chris Croce, corroborated Karl’s assertion about COVID immunity derivative of antibodies:
Veritas Journalist: “So, I am well-protected [with antibodies]?”
Chris Croce, Pfizer Senior Associate Scientist: “Yeah.”
Veritas Journalist: “Like as much as the vaccine?”
Croce: “Probably more.”
Veritas Journalist: “How so? Like, how much more?”
Croce: “You’re protected most likely for longer since there was a natural response.”
Croce expressed dismay with his company’s direction and moral compass:
Veritas Journalist: “So, what happened to the monoclonal antibody treatments?”
Croce: “[It got] pushed to the side.”
Veritas Journalist: “Why?”
Croce: “Money. It’s disgusting.”
…
Croce: “I still feel like I work for an evil corporation because it comes down to profits in the end. I mean, I’m there to help people, not to make millions and millions of dollars. So, I mean, that’s the moral dilemma.”
Veritas Journalist: “Isn’t it billions and billions?”
Croce: “I’m trying to be nice.”
Veritas Journalist: “No, I hear you. I hear you. I do. I mean, I’ll still give you a hard time about it.”
Croce: “Basically, our organization is run on COVID money now.”
The third Pfizer scientist, Rahul Khandke, admitted his company demands that its employees keep information from the public.
“We’re bred and taught to be like, ‘vaccine is safer than actually getting COVID.’ Honestly, we had to do so many seminars on this. You have no idea. Like, we have to sit there for hours and hours and listen to like — be like, ‘you cannot talk about this in public,’” Khandke said.
Khandke also signaled that proof of antibodies is on par with proof of vaccination.
“If you have [COVID] antibodies built up, you should be able to prove that you have those built up,” he said.
Project Veritas will be releasing more Pfizer tapes in the very near future. To receive updates straight into your email inbox, click here.
October 5, 2021
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science, Timeless or most popular, Video | COVID-19 Vaccine, Pfizer |
Leave a comment
A patient with Type 1 diabetes called to tell me the pharmacist at our local Walgreens refused to fill the prescription I had written for ivermectin, so I called to ask why.
The young pharmacist, a few years out of pharmacy school, informed me he did not understand why I was using ivermectin for early treatment of COVID because “SARS-CoV-2 does not have an exoskeleton.”
I explained I was not using ivermectin as an anti-parasitic medication, but that it had impressive data as an anti-inflammatory and anti-viral.
Furthermore, as a pediatrician, I have more than 40 years of experience managing multiple viral illnesses. There is value in treating viruses early, often with inexpensive natural remedies, rather than “staying at home until you have problems breathing then go to the hospital” as U.S. public officials have advised for COVID.
The pharmacist was not buying my initial explanation. “I am not going to fill prescriptions for ivermectin that are used in pseudo vaccine doses,” he told me.
I was surprised a young pharmacist was able to override an experienced physician’s prescription, effectively removing an inexpensive prevention and treatment option for selected patients in the middle of a pandemic.
The medical educator in me kicked in. “I would be happy to send you some references about the use of ivermectin for treatment and prevention. There are impressive studies from Argentina, Peru, Africa and India that suggest much better outcomes than we are achieving here in the U.S. with our single-minded focus on vaccines.”
He told me the U.S. Food and Drug Administration (FDA) did not recommend ivermectin for COVID. I asked to see the documentation and he agreed to fax it to me.
I hand-delivered 93 references and a great review article to the Walgreens.
The pharmacist faxed back a post from March 5, on the FDA website entitled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.”
The next day, I received notice that a pharmacy in Northern Virginia would not fill any prescriptions for ivermectin if the diagnosis code mentioned COVID.
I had written an ivermectin prescription for a patient who has a history of bad reactions to vaccines and significant autoimmune illness. His adolescent age means that he is at very low risk of death from COVID itself.
Based on my experience as his doctor for over a decade, I was worried about potential adverse events if he got the COVID vaccine. I dug into the data about ivermectin, and it seemed like a great option for him to have on hand for early treatment of COVID if he got sick.
A pharmacist in a drug store, who never examined my patient or learned his extensive medical history, got to trump my best medical judgment by refusing to fill the prescription.
The same day, in a conversation with a compounding pharmacy, we learned of a case in which a patient’s family had to take a hospital to court to obtain treatment with ivermectin.
Bear in mind that the safety profile for ivermectin is excellent and the drug is spectacularly less expensive than the vast majority of hospital interventions.
Three days later, on a zoom call with a colleague whose parents live in Colorado, I learned that a pharmacist at a major drugstore was not only refusing to fill ivermectin for 86- and 87-year-old patients who held valid prescriptions, but the pharmacist was taking the initiative to remind the other King Soopers pharmacies in the state not to fill those prescriptions either.
My analysis of the medical literature is that ivermectin has an impressive safety record and there are multiple studies from around the globe suggesting it can decrease morbidity and mortality from COVID 19.
Two doctors who were actually in the ICU treating real patients, Dr. Paul Marik and Dr. Pierre Kory, looked at their prior experience with similarly sick patients and reviewed treatment strategies to determine what could be helpful.
As Dr. Anthony Fauci advised us to “stay home and wait for the vaccine,” frontline doctors took care of the patients before them, learning valuable lessons about what worked and what did not.
Let’s hit the highlights, quoting directly from the review paper by Kory et al, Jan 2021:
- Since 2012, multiple in vitro studies have demonstrated that ivermectin inhibits the replication of many viruses, including influenza, Zika, Dengue and others (Mastrangelo et al., 2012; Wagstaff et al., 2012; Tay et al., 2013; Götz et al., 2016; Varghese et al., 2016; Atkinson et al., 2018; Lv et al., 2018; King et al., 2020; Yang et al., 2020).
- ivermectin inhibits SARS-CoV-2 replication and binding to host tissue via several observed and proposed mechanisms (Caly et al., 2020a).
- ivermectin has potent anti-inflammatory properties with in vitro data demonstrating profound inhibition of both cytokine production and transcription of nuclear factor-κB (NF-κB), the most potent mediator of inflammation (Zhang et al., 2008; Ci et al., 2009; Zhang et al., 2009).
- ivermectin significantly diminishes viral load and protects against organ damage in multiple animal models when infected with SARS-CoV-2 or similar coronaviruses (Arevalo et al., 2020; de Melo et al., 2020).
- ivermectin prevents transmission and development of COVID-19 disease in those exposed to infected patients (Behera et al., 2020; Bernigaud et al., 2020; Carvallo et al., 2020b; Elgazzar et al., 2020; Hellwig and Maia, 2020; Shouman, 2020).
- ivermectin hastens recovery and prevents deterioration in patients with mild to moderate disease treated early after symptoms (Carvallo et al., 2020a; Elgazzar et al., 2020; Gorial et al., 2020; Khan et al., 2020; Mahmud, 2020; Morgenstern et al., 2020; Robin et al., 2020).
- ivermectin hastens recovery and avoidance of ICU admission and death in hospitalized patients (Elgazzar et al., 2020; Hashim et al., 2020; Khan et al., 2020; Niaee et al., 2020; Portmann-Baracco et al., 2020; Rajter et al., 2020; Spoorthi V, 2020).
- ivermectin reduces mortality in critically ill patients with COVID-19 (Elgazzar et al., 2020; Hashim et al., 2020; Rajter et al., 2020).
- ivermectin leads to striking reductions in case-fatality rates in regions with widespread use (Chamie, Juan, 2020).
- The safety, availability, and cost of ivermectin is nearly unparalleled given its near nil drug interactions along with only mild and rare side effects observed over almost 40 years of use and billions of doses administered (Kircik et al., 2016).
- ivermectin was successful at controlling several diseases which blighted the lives of billions living in poverty in the tropics.
- ivermectin’s discoverers were awarded the Nobel Prize in Medicine in 2015.
- ivermectin is included in the World Health Organization’s “List of Essential Medicines.” It has been widely distributed in countries like India for pennies a day. The out-of-pocket cost of ivermectin at my Walgreen’s is more than$1,000.
Kory and Marik compiled eight studies (three randomized controlled studies and five observational controlled studies) demonstrating efficacy in prevention of COVID-19 with significant decreased transmission.
They found 19 controlled studies that showed significant impacts on time to recovery, hospital stay, decrease in viral loads, reductions in duration of cough and decreased mortality.
In medical history pre-COVID, this body of research about ivermectin would be applauded for bringing value in the midst of a pandemic. In the medical era pre-COVID, the judgment and experience of clinicians at the patient’s bedside counted for something.
Pre-COVID, we taught medical students to use keen observational skills and keep accurate records of whether the patient improved or deteriorated after the treatment strategies used.
In the Age of COVID, pharmacists who chide doctors that “COVID does not have an exoskeleton” deny patients ivermectin — a safe, cheap, effective and potentially life-saving early treatment.
If you or your patients are having trouble getting ivermectin prescriptions filled for COVID 19 prevention or treatment, see this excellent resource from the Front Line COVID 19 Critical Care Alliance.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
October 5, 2021
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Ivermectin, United States |
Leave a comment
The UK government’s Winter Plan is rife with nudges
There’s a chill in the air. Not from the changing seasons, it’s still beautifully balmy, but because the behavioural scientists’ fingertips have traced a hoar frost of psychocratic nudge on the government’s “Autumn and Winter Plan”.
The UK government’s Winter Plan plan contained some welcome news. The most draconian schedules of the Coronavirus Act will be revoked, including the powers to close schools, allow potentially infectious people to be detained, and restrictions on gatherings and events. The language around the plan’s launch was thankfully more cool-headed. The times are “challenging” but it is no longer claimed that Covid is the “biggest threat this country has faced in peacetime history”.
But the plan is also rife with “nudges” – sneaky ways to prime, prepare and prod you into the desired mindset and course of action.
The contents are freighted with the sunk cost fallacy; we’ve come so far, we mustn’t allow our good work to be undone. This also taps into people’s innate sensitivity to loss.
The trigger from Plan A to Plan B will be “unsustainable pressure” on the NHS rather than deaths. It’s under serious pressure every winter so consider yourselves to be put on notice.
There are other indications of the inevitability of Plan B. I spoke to behavioural scientist Patrick Fagan, who observed that:
“the Plan A / Plan B approach is a classic example of the foot-in-the-door technique. Firstly it makes us accept Plan A because, compared to Plan B, it looks more reasonable; then, once we have accepted and acclimatised to Plan A, we are more likely to then accept Plan B, because it is just one extra step on top of the commitment we’ve already made. The announcement of Plan B may also be an example of the mere exposure effect: simply by talking about the measures (even if, ironically, saying they won’t be implemented), the government makes them more familiar and therefore more psychologically acceptable.”
Bizarrely, after 18 months we’re trapped in a Groundhog Day of modelling and worst case scenarios. Almost a year ago, on the 21st September, Chris Whitty and Patrick Vallance warned of infections hitting 50,000 per day by mid-October in their “Shock and Awe” presentation. When the day arrived, the moving average was 16,228.
According to the doom-mongers at SAGE, up to 7,000 people could be hospitalised per day within the month. And this September the modellers were wrong once again – hospitalisations peaked at about a 1,000 a day and are now falling.
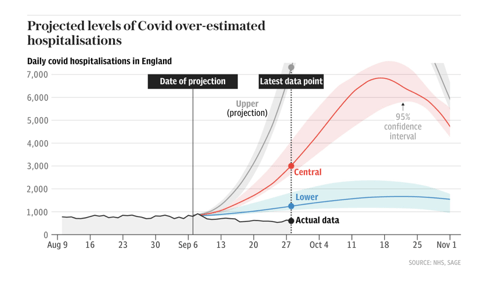
Source: The Telegraph
The big numbers both fuel the policies and justify them. It doesn’t matter that there are more optimistic scenarios, or that the modelling has limitations, because the first supine headline sticks in the brain. The behavioural psychology principle of “salience” draws your attention to what is novel and risky.
Dr Alex De Figueiredo, who conducts mathematical and statistical analyses for the Vaccine Confidence Project, told me that:
“Since the beginning of the pandemic it seems many modelling assumptions, such as the infection fatality rate, have been quite pessimistic. I think this has been why many of the predictions — such as hospitalisations and deaths — have been overstated. It also appears there has been little effort to validate forecasts out-of-sample, such as applying the models to Sweden or Florida, who have had far fewer restrictions.”
There are no quantifiable measures for what justifies each step from Plan A to Plan B. The parameters are fluid, unspecified. This creates confusion and stress, which infantilises people and makes them look to the government for direction. Essentially, confusion increases compliance.
The threat of lockdown hangs like a Sword of Damocles. Will we, or won’t we? It seems unlikely that the public and businesses could be persuaded again. Regardless, the threat of lockdown might be leveraged to justify the introduction of Covid Passports, in what is known as a “reciprocation nudge” – we appear to be given a concession in return for reduced resistance to another option.
Covid Passports have been vigorously opposed by MPs and civil liberties groups, and there hasn’t been a vote in Parliament yet. Despite this, they squat in Plan B as a fait accompli, in the denouement of the “door in the face” technique. This is when a huge request is made, then refused, to be followed by a second smaller request, in this case relegation to Plan B and for limited venues only. Boris Johnson said that it’s “not sensible to rule out this kind of option now when it might still make the difference between keeping businesses open or not.” But why would it be sensible when the Public Administration and Constitutional Affairs Committee produced a damning report against them and found the government could make no scientific case in their favour?
Covid Passports appear to be a behavioural science tool, used to increase vaccine uptake. This may backfire. ‘A Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19’ found that vaccine passports deter a significant minority of people who want autonomy over their bodies. This also chimes with the research conducted by De Figueiredo and colleagues at The Vaccine Confidence Project. The bullying and resultant mistrust may impact Covid-19 vaccine uptake as well as other public health initiatives.
When my book A State of Fear: how the UK government weaponised fear during the Covid-19 pandemic was published some people believed, quite quaintly, that public health measures and messaging were unrelated to behavioural science. I think that the book and the writings of other academics and journalists have moved the dial. Once nudge is seen it can’t be unseen. The public increasingly see the nudge. If the behavioural scientists have been dazzling people with card tricks they have over-played their hand.
As such, there is more honesty about the purpose Covid Passports serve. Nicola Sturgeon, Scotland’s First Minister, said that the passport scheme
“will not eradicate transmission completely but it will help reduce it in some higher risk settings, and it will maximise protection against serious illness. And we believe – as we have seen already in some other countries – it will help encourage take-up of the vaccine.”
Similarly, Linda Bauld, Professor of Public Health and Interim Social Policy Adviser to the Scottish Government, also admitted that Covid Passports are “to increase uptake in vaccination” and the “rationale” is that it particularly boosts vaccination in 18 to 29 year olds.
While Covid Passports are in Plan B, Ministers say different things about them each day. Within the space of a week, Sajid Javid scrapped them but also didn’t rule them out for pubs. Javid admitted there’s “no evidence” for them but Boris Johnson called them “sensible”. Does the left hand not know what the right hand is doing? Or maybe a big behavioural science brain lurks in between. The epidemic management is reminiscent of the uncertainty created by Vladislav Surkov in the Soviet Union to deliberately turn politics into a performance of confusion – you don’t know what’s real anymore.
There are never-ending question marks over travel, although double-vaccinated travellers will no longer need expensive and inconvenient PCR tests. The double-jabbed will delight in the news, and it sounds sensible on the surface. However, this is not about “following the science”, since the previously infected do not benefit from the exemption. This is an incentive, a classic nudge, to encourage jabs. The vaccinated are rewarded and the unvaccinated are punished. Bearing in mind that negative tests and prior infection could suffice, this decision reeks of disdain for personal autonomy.
Vaccines for 12 to 15 year olds have been authorised. Politicians have stirred up debate amongst all corners regarding whether children should be jabbed with their parents’ consent or not. This utilises what Patrick Fagan calls “the leapfrog effect”. He says,
“it leapfrogs one stage of the debate and in doing so, sets the baseline assumptions which become accepted implicitly. Specifically, by having people debate whether or not parents’ consent should be sought, they are establishing the unspoken assumption that children should receive the jab in the first place. Those who think they are debating the government, arguing that parents’ consent is needed, are actually accepting its true goal, to jab kids.”
The government might be more in control of the narrative than many people like to believe. (Of course, chaos and confusion are alternatives…)
Worryingly, can teens truly provide informed consent? Throughout 2020 they were exhorted not to “kill granny”, which would provoke fear, shame and stress. Ads on Tiktok tell youngsters that the way to get back to normal is to take the vaccine. The vaccine will be rolled out in schools which will create peer pressure, in a particularly egregious use of “norms”. Finally, if the JCVI found the decision difficult, how is a 12 year old supposed to weigh up the evidence? (Nudging teens is the subject matter of my next article.)
Since the Cabinet reshuffle, Michael Gove has been informally dubbed the ‘Minister for Christmas’. Boris Johnson joked that he “didn’t want to have to cancel Christmas again”. Did you know Christmas might be cancelled and needs saving? You do now, the idea has been “seeded”.
Although it is ostensibly supply chains which threaten Christmas, the joke draws a comparison with last year’s Covid reasons. Again, you are put on notice. The nudges are still focussed on increasing vaccination, for now, but the threat to Christmas might hint at the beginning of a behavioural science approach to meet green targets.
We must be good boys and girls if we want Santa to come. And be aware, the nudgers are drafting our collective New Year’s Resolutions.
October 5, 2021
Posted by aletho |
Book Review, Deception, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, UK |
Leave a comment
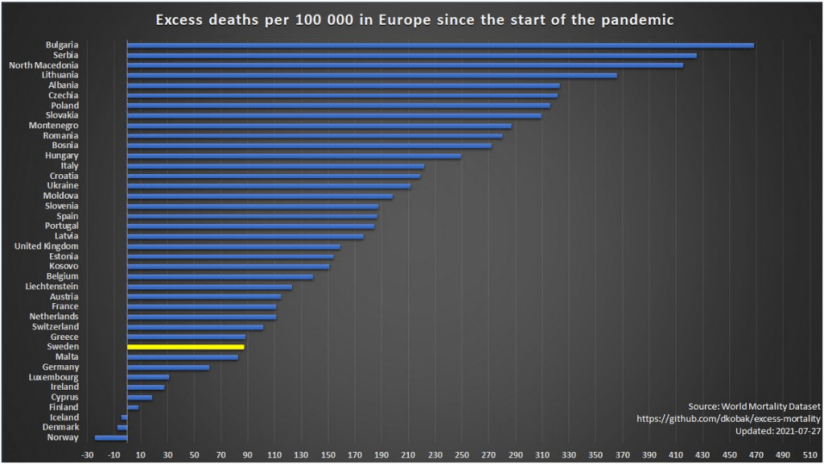
There follows a guest post by a subeditor and long-time Daily Sceptic reader who is keeping his identity anonymous. He has spotted that spectacular healthcare spending and impressive vaccination rates have not brought the U.K. obvious rewards against Covid. (Sweden is highlighted in the graph above because, by imposing the fewest restrictions, it is the closest Europe has to a control.)
Recent figures for European countries from the World Mortality Dataset, depicted in the graph above, reveal that island nations have fared particularly well during the pandemic: Iceland, Cyprus, Ireland and Malta have all recorded low levels of excess deaths. However, there is one noteworthy exception – the U.K.
In fact, even the third poorest country in Europe, Kosovo, riven by war in the late 1990s, and only an independent state since 2008, has performed better. This is despite the Balkan country having, per capita, a fraction of our health service facilities, staff and expertise.
The double-vaccination rate in Kosovo, currently 30% of the population, is a long way behind the U.K. on 66%.
Excess mortality is widely regarded as the best measure of a country’s success in coping with a prolonged health crisis, such as a bad flu season, as it allows for differing evaluations of the causes of death, notably whether they have been ‘with’ or ‘of’ Covid, and disregards arbitrary time limits, such as within 28 days of a positive PCR test. All other deaths, such as those brought on by lockdown measures, are also, of course, included in these statistics.
This evidence shows that spending billions of pounds above normal on health services and staff, and enticing a large proportion of a population to get vaccinated, do not necessarily correlate with a lower number of deaths.
October 5, 2021
Posted by aletho |
Economics, Science and Pseudo-Science | European Union, UK |
Leave a comment
The publisher Springer Nature has released an “expression of concern” for more than four hundred papers they published in the Arabian Journal of Geosciences. All these papers supposedly passed through both peer review and editorial control, yet no expertise in geoscience is required to notice the problem:

The paper can’t decide if it’s about organic pollutants or the beauty of Latin dancing, and switches instantly from one to the other half way through the abstract.
The publisher claims this went through about two months of review, during which time the editors proved their value by assigning it helpful keywords:

If you’re intrigued by this fusion of environmental science and fun hobbies, you’ll be overjoyed to learn that the full article will only cost you about £30 and there are many more available if that one doesn’t take your fancy, e.g.
Background
Peer-reviewed science is the type of evidence policymakers respect most. Nonetheless, a frequent topic on this site is scientific reports containing errors so basic that any layman can spot them immediately, leading to the question of whether anyone actually read the papers before publication. An example is the recent article by Imperial College London, published in Nature Scientific Reports, in which the first sentence was a factually false claim about public statistics.
Evidence is now accruing that it’s indeed possible for “peer reviewed” scientific papers to be published which have not only never been reviewed by anybody at all, but might not have even been written by anybody, and that these papers can be published by well known firms like Springer Nature and Elsevier. In August we wrote about the phenomenon of nonsensical “tortured phrases” that indicate the usage of thesaurus-driven paper rewriting programs, probably the work of professional science forging operations called “paper mills”. Thousands of papers have been spotted using this technique; the true extent of the problem is unknown. In July, I reported on the prevalence of Photoshopped images and Chinese paper-forging efforts in the medical literature. Papers are often found that are entirely unintelligible, for example this paper, or this one whose abstract ends by saying, “Clean the information for the preparation set for finding valuable highlights to speak to the information by relying upon the objective of the undertaking.” – a random stream of words that means nothing.
Where does this kind of text come from?
The most plausible explanation is that these papers are being auto-generated using something called a context-free grammar. The goal is probably to create the appearance of interest in the authors they cite. In academia promotions are linked to publications and citations, creating a financial incentive to engage in this sort of metric gaming. The signs are all there: inexplicable topic switches half way through sentences or paragraphs, rampant grammatical errors, the repetitive title structure, citations of real papers and so on. Another sign is the explanation the journal supplied for how it occurred: the editor claims that his email address was hacked.
In this case, something probably went wrong during the production process that caused different databases of pre-canned phrases to be mixed together incorrectly. The people generating these papers are doing it on an industrial scale, so they didn’t notice because they don’t bother reading their own output. The buyers didn’t notice – perhaps they can’t actually read English, or don’t exist. Then the journal didn’t notice because, apparently, it’s enough for just one person to get “hacked” for the journal to publish entire editions filled with nonsense. And finally none of the journal’s readers noticed either, leading to the suspicion that maybe there aren’t any.
The volunteers spotting these papers are uncovering an entire science-laundering ecosystem, hiding in plain sight.
We know randomly generated papers can get published because it’s happened hundreds of times before. Perhaps the most famous example is SCIgen, “a program that generates random Computer Science research papers, including graphs, figures, and citations” using context-free grammars. It was created in 2005 by MIT grad students as a joke, with the aim to “maximize amusement, rather than coherence“. SCIgen papers are buzzword salads that might be convincing to someone unfamiliar with computer science, albeit only if they aren’t paying attention.
Despite this origin, in 2014 over 120 SCIgen papers were withdrawn by leading publishers like the IEEE after outsiders noticed them. In 2020 two professors of computer science observed that the problem was still occurring and wrote an automatic SCIgen detector. Although it’s only about 80% reliable, it nonetheless spotted hundreds more. Their detector is now being run across a subset of new publications and finds new papers on a regular basis.
Root cause analysis
On its face, this phenomenon is extraordinary. Why can’t journals stop themselves publishing machine-generated gibberish? It’s impossible to imagine any normal newspaper or magazine publishing thousands of pages of literally random text and then blaming IT problems for it, yet this is happening repeatedly in the world of academic publishing.
The surface level problem is that many scientific journals appear to be almost or entirely automated, including journals that have been around for decades. Once papers are submitted, the reviewing, editorial and publishing process becomes handled by computers. If the system stops working properly editors can seem oblivious – they routinely discover they published nonsense only because people who don’t even subscribe to their journal complained about it.
Strong evidence for this comes from the “fixes” journals present when put under pressure. As an explanation for why the 436 “expressions of concern” wouldn’t be repeated the publisher said:
The dedicated Research Integrity team at Springer Nature is constantly searching for any irregularities in the publication process, supported by a range of tools, including an in-house-developed detection tool.
The same firm also proudly trumpeted in a press release that:
Springer announces the release of SciDetect, a new software program that automatically checks for fake scientific papers. The open source software discovers text that has been generated with the SCIgen computer program and other fake-paper generators like Mathgen and Physgen. Springer uses the software in its production workflow to provide additional, fail-safe checking.
A different journal proposed an even more ridiculous solution: ban people from submitting papers from webmail accounts. The more obvious solution of paying people to read the articles before they get published is apparently unthinkable – the problem of fake auto-generated papers is so prevalent, and the scientific peer review process so useless, that they are resorting to these feeble attempts to automate the editing process.
Diving below the surface, the problem may be that journals face functional irrelevance in the era of search engines. Clearly nobody can be reading the Arabian Journal of Geosciences, including its own editors, yet according to an interesting essay by Prof Igor Pak “publisher’s contracts with [university] libraries require them to deliver a certain number of pages each year“. What’s in those pages? The editors don’t care because the libraries pay regardless. The librarians don’t care because the universities pay. The universities don’t care because the students and granting bodies pay. The students and granting bodies don’t care because the government pays. The government doesn’t care because the citizens pay, and the citizens DO care – when they find out about this stuff – but generally can’t do anything about it because they’re forced to pay through taxes, student loan laws and a (socially engineered) culture in which people are told they must have a degree or else they won’t be able to get a professional job.
This seems to be zombie-fying scientific publishing. Non-top tier journals live on as third party proof that some work was done, which in a centrally planned economy has value for justifying funding requests to committees. But in any sort of actual market-based economy many of them would have disappeared a long time ago.
October 4, 2021
Posted by aletho |
Corruption, Deception, Environmentalism, Science and Pseudo-Science, Timeless or most popular |
Leave a comment

