“My name is Bill Gates, King of Kings”

Source: The next outbreak? We’re not ready | Bill Gates | INTIDOMAIN
By Richard Hugus | October 4, 2021
My name is Ozymandias, King of Kings,
Look on my Works, ye Mighty, and despair!
— Percy Bysshe Shelley, Ozymandias
The evidence is in. Gene-manipulating injections advertised as a “vaccine for covid 19” have killed and injured many thousands of people. Instead of providing immunity to an alleged virus, the shots actually harm the immune system and turn it against us. The spike proteins created by the shots spread out to attack major organs in the body, leading to a thousand and one different health problems, including heart attacks, myocarditis, pericarditis, strokes, blood clots, spontaneous abortions, neurological disorders, depression, and death. Yet the medical establishment is urging everyone, including pregnant women and children, to get the jab. The ghost standing in as US President recently decreed that if people refuse the shot they will lose their job. This is coercion to accept a medical intervention known to be a danger to human health — a crime against humanity. Half the population of the country is now facing this coercion.
This only makes sense if we reason that the authorities want to harm us, or that there is something so important in the injection that they don’t mind harming us, as long as we get the injection. Bill Gates said early in 2020 that everyone on the planet should be “vaccinated.” Perhaps his dream was that when that is accomplished there will be no one left who will not be genetically modified (to Gates’s secret specifications) and thus no one left to hold him to account.
One of the most insidious arguments put forward by the authorities is that we are facing a health crisis so serious that individual freedom must be sacrificed for the common good, and therefore no one has a moral right to refuse the Frankenshot. This argument quickly comes down to whether human beings have inalienable rights — rights given to us by God, which the state does not have the power to take away or overrule. To accept or reject any substance being given to us is obviously such a right. And after this we can discuss the details — that the purpose of the “vaccine” is unclear, that its contents are unknown, that it has proven harmful to thousands of people, that we were not informed of adverse effects, that natural immunity should be recognized, that tests establishing the alleged disease were fraudulent, that there is no emergency, that there are safe alternative treatments, et cetera. But if we understand that the state is a lesser power, then we understand that it does not have the authority to order substances injected into our bodies.
We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.
-U.S. Declaration of Independence
The cabal behind the medical tyranny we are facing doesn’t believe we have God-given rights because they don’t believe there’s a God in the first place. They apparently think that since they are billionaires, and billionaires have a lot of weight to throw around, that they can be gods. They also seem to believe there is nothing they are forbidden to do to other people because other people do not have souls — they are just biological entities evolved through random nature which the rich, by virtue of their power, are free to manipulate and improve upon. To technocrats, nothing is sacred. So it makes sense to them to risk injuring pregnant women and children and even experiment on the whole human race (beside their chosen few). Those who resist are now being segregated and punished, like Palestinians in their own land. Perhaps occupied Palestine is the oligarchs’ model for our future.
The ultimate goal may be the power that previous master-slave relationships were not able to achieve — a “read/write” capability in which the master has full surveillance power over the slaves and gives the orders for them to follow. Subtracted from the slave population, of course, will be those few billion dissidents and “useless eaters” who don’t fit in with the plan. They will be terminated. From this point of view it also follows that the genetic makeup of any living thing is just software which today’s sophisticated scientists can splice, delete, modify, or re-create as the masters see fit. From this point of view humans are no different than GM corn, soy, or cotton. GM humans can be used to bring in a nice profit as well because the masters will own their patents. Perhaps Monsanto agribusiness is another model for our future.
Taken to its logical extreme, reality itself is in the hands of our would-be masters. With proper control of the media, people can be made to believe anything, like that an illness similar to the flu is a “pandemic,” or that someone who has no symptoms of illness is actually sick, or that the unvaccinated are selfishly threatening everyone else with death, or that anyone who strays from the narrative is spreading “misinformation,” or that if someone goes into convulsions directly after getting jabbed it is not due to the poison that was just injected into them, or that a serum that injures and kills is “safe and effective.” In this world, the truth is what the powerful say it is, regardless of the facts. The powerful are a locomotive big enough to just run past any anomalies and contradictions, leaving us bewildered.
However, the ambitiousness of this insane program foretells its failure. History is full of great tyrants with grand plans who came in with spectacular fame but suddenly fell in disgrace, erased by time. The oligarchs’ main weakness is their lack of any sense of limits. Gaining some power, they then want it all. They reach too far, too soon, and expose themselves in the process. And then common humanity — always patient to a fault — finally decides to stand up and become a locomotive itself, running back over the entire plan and returning us to sanity.
If the world is going to see a great reset, it will not be the one Klaus Schwab and his Davos gangsters had in mind.
We should take heart. So much has been revealed! It’s as if the world’s worst criminals burst into the courtroom and offered up a horrendous public confession.
Another Study Links Low Vitamin D to Risk of COVID
By Dr. Joseph Mercola | October 4, 2021
Another preprint study, published September 25, 2021, shows the correlation between low vitamin D levels and the risk of getting COVID-19.
In this retrospective examination of one population study and seven clinical studies where vitamin D3 levels were measured on the day of hospitalization, researchers said, “The two datasets provide strong evidence that low D3 is a predictor rather than a side effect of the infection.”
They suggested that it may be possible to “prevent or mitigate” new COVID outbreaks by simply raising people’s vitamin D3 levels to 50 ng/ml or above. Even though they said they believe vaccination is part of the fight against COVID, they added that the ongoing evidence of the part vitamin D plays in the risk for contracting the infection is especially important because the virus continues to mutate, which challenges the effectiveness of the vaccines.
New Zealand Abandons Controversial ‘Zero COVID’ Policy
But lockdowns will remain until 90% of population is vaxxed

By Paul Joseph Watson | Summit News | October 4, 2021
New Zealand has announced it is dropping its controversial ‘zero COVID’ policy after numerous critics pointed out that such an approach to eliminating the virus was impossible.
Prime Minister Jacinda Ardern made the announcement earlier today during a press conference in which she acknowledged, “The return to zero has been extremely difficult.”
“What we have called a long tail has been more like a tentacle that has been difficult to shake,” she added, noting that the delta variant of the virus forced a change in policy.
Critics had repeatedly asked how the country expected to maintain a ‘zero COVID’ policy given the emergence of new variants of the virus and decreasing efficacy of the initial round of vaccinations.
However, with 48% of the population fully vaccinated, no return to normal is expected anytime soon given that Ardern has said 90% will need to be fully vaxxed before the lockdowns will end.
Kiwis have faced continuous lockdown measures almost as brutal as their Aussie neighbors since the beginning of the pandemic.
As we highlighted in August, Ardern mimicked Australia’s top public health official by telling citizens, “Don’t talk to your neighbors,” after the country went into full lockdown as a result of just a single COVID case being detected.
Authorities also previously announced that they would put all coronavirus infectees and their close family members in “quarantine facilities” even if they refuse.
“Natural Immunity” Is a Political Problem for the Regime
By Ryan McMaken – Mises Wire – 09/21/2021
Since 2020, public health technocrats and their allies among elected officials have clung to the position that absolutely every person who can possibly get a covid vaccine should get one.
Both the Mayo Clinic website and the Centers for Disease Control and Prevention website, for example, insist that “research has not yet shown” that people who have recovered from covid have any sort of reliable protection. Moreover, the CDC page points to a single study from Kentucky claiming that people with natural immunity are more than twice as likely to contract covid again, compared to people who have been vaccinated.
This narrative is reflected in the fact that the Biden administration’s vaccine mandates are a one-size-fits-all policy insisting that virtually all adults, regardless of whether or not they’ve already had the disease, receive a covid vaccine. The official position is apparently this: nothing except the vaccine can provide any sort of resistance or immunity. So get a vaccine. No exceptions!
Health technocrats have repeatedly insisted that “the science” points unambiguously toward everyone receiving a vaccine, even to the point of pushing vaccines for children. All this in spite of the fact the risk to children from covid is far less than a dozen common daily risks, such as riding in an automobile.
The regime has attached itself closely to a vaccinate-everybody-no-matter-what policy, and a sudden u-turn would be politically problematic. So it’s no wonder there’s so little interest in the topic.
Indeed, in a September 10 interview, senior covid technocrat Anthony Fauci claimed that the matter of natural immunity was not even being discussed at government health agencies. Fauci’s response suggested that the facts of natural immunity warranted discussion at some point in the future. But the comment certainly fit the dominant regime narrative nonetheless: the facts of natural immunity don’t matter for now. Everyone should just get vaccinated:
CNN’s Sanjay Gupta asked if people who have already recovered from COVID-19 should still be required to get the vaccine.
“I don’t have a really firm answer for you on that,” [Fauci] said Thursday on CNN. “I think that is something that we need to sit down and discuss seriously.”
Maybe someday they’ll get to talking about it.
But some physicians aren’t as obsessed with pushing vaccine mandates as Anthony Fauci, and the evidence in favor of natural immunity is becoming so undeniable that even mainstream publications are starting to admit it.
In an op-ed for the Washington Post last week, Marty Makary of the Johns Hopkins School of Medicine argues that the medical profession has hurt its credibility in pretending that natural immunity is virtually irrelevant to the covid equation. Moreover, the dogmatic “get vaccinated” position constitutes a lack of honesty about the data. Rather, Makary concludes:
[W]e can encourage all Americans to get vaccinated while still being honest about the data. In my clinical experience, I have found patients to be extremely forgiving with evolving data if you are honest and transparent with them. Yet, when asked the common question, “I’ve recovered from covid, is it absolutely essential that I get vaccinated?” many public health officials have put aside the data and responded with a synchronized “yes,” even as studies have shown that reinfections are rare and often asymptomatic or mild when they do occur.
And what are these studies? Makary continues:
More than 15 studies have demonstrated the power of immunity acquired by previously having the virus. A 700,000-person study from Israel two weeks ago found that those who had experienced prior infections were 27 times less likely to get a second symptomatic covid infection than those who were vaccinated. This affirmed a June Cleveland Clinic study of health-care workers (who are often exposed to the virus), in which none who had previously tested positive for the coronavirus got reinfected. The study authors concluded that “individuals who have had SARS-CoV-2 infection are unlikely to benefit from covid-19 vaccination.” And in May, a Washington University study found that even a mild covid infection resulted in long-lasting immunity.
The policy bias in favor of vaccines ignores many other facts as well, such as the relative risks of vaccines, especially for the young:
The current Centers for Disease Control and Prevention position about vaccinating children also dismisses the benefits of natural immunity. The Los Angeles County School District recently mandated vaccines for students ages 12 and up who want to learn in person. But young people are less likely to suffer severe or long-lasting symptoms from covid-19 than adults, and have experienced rare heart complications from the vaccines. In Israel, heart inflammation has been observed in between 1 in 3,000 and 1 in 6,000 males age 16 to 24; the CDC has confirmed 854 reports nationally in people age 30 and younger who got the vaccine.
A second dose of the two-shot mRNA vaccine like that produced by Pfizer and Moderna may not even be necessary in children who had covid. Since February, Israel’s Health Ministry has been recommending that anyone, adult or adolescent, who has recovered from covid-19 receive a only single mRNA vaccine dose, instead of two. Even though the risk of severe illness during a reinfection is exceedingly low, some data has demonstrated a slight benefit to one dose in this situation. Other countries use a similar approach. The United States could adopt this strategy now as a reasonable next step in transitioning from an overly rigid to a more flexible vaccine requirement policy. For comparison, the CDC has long recommended that kids do not get the chickenpox vaccine if they had chickenpox infection in the past.
The nonscientific, ideology-induced blind spot for natural immunity also prompted The BMJ (the journal of the British Medical Association) to note that “[w]hen the vaccine rollout began in mid-December 2020, more than one quarter of Americans—91 million—had been infected with SARS-CoV-2…. As of this May, that proportion had risen to more than a third of the population, including 44% of adults aged 18–59.”
And yet, the authors note this fact doesn’t appear to be a part of any policy discussion at all:
The substantial number of infections, coupled with the increasing scientific evidence that natural immunity was durable, led some medical observers to ask why natural immunity didn’t seem to be factored into decisions about prioritising vaccination.
This problem is reflected in the Biden administration’s drive for booster shots—announced in mid-August—even before there was any clinical research on booster shots at all. Even by mid-September, as one hospital’s chief medical officer put it, “the data is not compelling one way or another.”
But those sorts of details don’t trouble federal “public health” officials, and the Biden administration quickly moved toward pushing booster shots for everyone.
This Is Why There Should Be No Mandatory Medical Treatment
Of course, mandating vaccines—like mandating any medical treatment—would still be immoral even if we could list a dozen studies suggesting boosters are a boon and that natural immunity is no good.
What if there were twenty-five studies “proving” vaccines are better than natural immunity, but only twenty studies “proving” natural immunity is better? Would coercive vaccine mandates then suddenly be justified? Unfortunately, that’s exactly how many advocates for repressive covid policies think the world should work. For these people, policy is just a matter of adding up the number of studies “proving” their side is right, and then claiming this justifies forcing mandatory medications on millions of human beings.
(It never works in reverse, of course. The fact that there’s a lot of evidence—as Makary points out—against vaccines for those who have natural immunity, the dominant narrative is nonetheless that vaccines are “necessary” and “worth it” for everybody, always and everywhere.)
In the real world, however, many medications—including these new vaccines—come with risks that must be weighed against potential benefits. These decisions can only be made at the individual level, where patients must make their own decisions about what substances to put into their own bodies. In other words, blanket policies proclaiming “everyone must receive this medical treatment immediately, or else” contradicts the realities of the uncertainties and varying risk levels that affect individuals. The facts of uncertainty and informed consent were once considered a mainstay of medical ethics—and of any political ideology that actually respects self-determination and basic human rights. Unfortunately, the philosophy of “public health” appears to be uninterested in such trivialities.
At this point, it would be embarrassing for the regime to admit what actual scientific inquiry has shown: that natural immunity is generally superior to receiving the vaccine. The regime doesn’t like to be embarrassed, and neither do the countless doctors and nurses who have long toed the regime’s political line. So expect more of the same.
Covid in Sweden: Everything on the table
Sebastian Rushworth, M.D. | October 2, 2021
A group of German celebrities have started the campaign “alles auf den tisch”, which literally means “everything on the table”. It’s a reaction to the shocking lack of indepence and critical oversight that has been exhibited by journalists ever since the pandemic began. The purpose of the campaign is to break through the blinkered media narrative that exists in relation to covid, and allow a wider range of thoughts and opinions to get out.
In order to accomplish this, the celebrities have interviewed a large number of doctors and scientists who have thus far been sidelined by the mainstream media, and put the interviews up on their site allesaufdentisch.tv. The campaign appears to have been pretty effective so far, since the site crashed on launch due to the massive amount of traffic it was getting. Luckily it’s up and running again now. As a part of the campaign, I was interviewed by violinist Linus Roth. We talked about happenings in Sweden, the covid death rate, and lockdowns. The interview is short but sweet, only around twenty minutes long.
Vaccine Effectiveness Hits as Low as Minus-66% in the Over 40s, New PHE Data Shows

By Will Jones • The Daily Sceptic • October 3, 2021
The new Public Health England (PHE) Vaccine Surveillance report was released on Thursday, allowing us to update our estimates of unadjusted vaccine effectiveness from real-world data.
Oddly, the report appeared on a new webpage this week, but the old page didn’t include a note to let you know, so it took me a while to discover it had appeared and where it was.
Following last week’s ‘fact check‘ from Full Fatuous – ostensibly of my piece but with some words of admonition for PHE as well, particularly over the accuracy of the population data – a new note appeared in the report: “Interpretation of the case rates in vaccinated and unvaccinated population is particularly susceptible to changes in denominators and should be interpreted with extra caution.” So there you go. All estimates in this post are based on the data PHE uses and are valid insofar as that data is accurate.
As before, the data is just for a four-week period, which, given that the early part of the Delta surge was dominated by the unvaccinated and the latter part has seen infections rise in the vaccinated, seems to me a mistake. A fairer view would cover the whole Delta surge (as with the estimates I make from the data in the Technical Briefings), but in any case the report gives a snapshot of current relative infection rates.
As Full Fatuous pointed out, PHE don’t recommend using this data to estimate vaccine effectiveness, saying it’s “not the most appropriate method” because it’s unadjusted for risk factors (and, inevitably, they don’t provide the data you’d need to adjust it). However, even if not recommended by PHE, it is certainly a valid method of calculating vaccine effectiveness, which is just a figure which states the relative risk reduction in the vaccinated group, as long as you bear in mind its limitations. All vaccine effectiveness estimates have limitations, and while adjusting for confounding factors is in principle important, it is helpful only if done well, and many studies do not do it well. Unadjusted estimates from raw data are a necessary starting point.
Perhaps the key confounder for the estimates of vaccine effectiveness against infection given here is whether people have been previously infected, with a common assumption being that a higher proportion of the unvaccinated will be previously infected, due to it being a potential factor in people’s decision not to be vaccinated. This may well artificially lower the vaccine effectiveness estimates, but since no one has yet produced data showing how antibodies-from-infection split between vaccinated and unvaccinated it is hard to know how far this is the case.
Unvaccinated here means actually unvaccinated, not partially vaccinated or post-jab. Hospitalisation means “cases presenting to emergency care (within 28 days of a positive specimen) resulting in an overnight inpatient admission”.
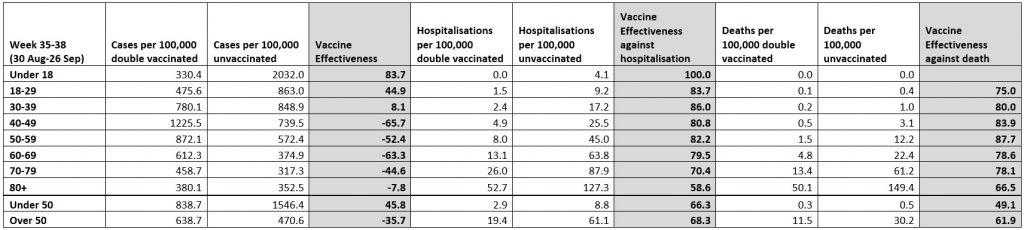
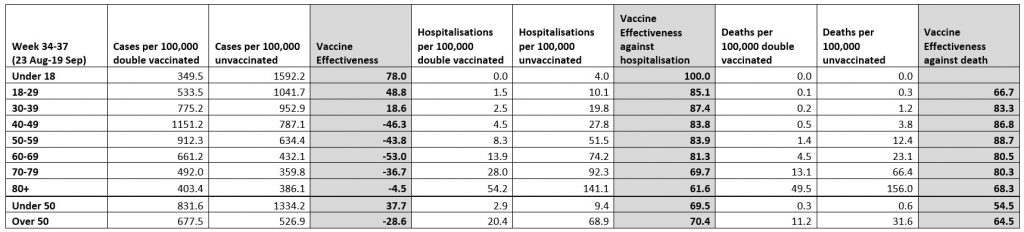
As England’s drawn-out Delta outbreak drags on, the infection rates in the vaccinated continue to outpace those in the unvaccinated, reducing (unadjusted) vaccine effectiveness further. For the 60s age group, infection rates are 63% higher in the vaccinated than in the unvaccinated, up from 53% last week, giving an (unadjusted) vaccine effectiveness of minus-63%. But that has been topped this week by the 40s age group, the vaccinated among whom now have an infection rate no less than 66% higher than the unvaccinated, up from 46% in last week’s report and 27% in the report for the month ending September 5th. Vaccine effectiveness has been heading downward in the 30s age group as well, now just 8%, though interestingly it has actually been increasing in the under 18s. On this data, vaccine protection against serious illness and death appears to be holding up. I have included the two previous tables below for comparison.

With infection rates now, on this data, much higher in the vaccinated than the unvaccinated, what remaining justification can there be for vaccine passports, vaccine mandates, and any other policy based on the assumption that vaccines protect other people? When will the Government face up to the reality that vaccines provide poor protection against infection, poor protection against transmission, and thus poor protection of others, and so there is no justification for continuing to build-up the infrastructure of a two-tier, discriminatory state?
This Week in the New Normal #7
OffGuardian | October 3, 2021
This Week in the New Normal is our weekly chart of the progress of autocracy, authoritarianism and economic restructuring around the world.
1.THE WORST ARTICLE I’VE EVER READ.
The demonisation campaign against those who decline to partake in the untested gene therapy is pervasive and seemingly limitless. Article’s pop up claiming unvaxxed people should be banned from flying, banned from healthcare, banned from state benefits, and even fired from their jobs.
But this article in The Mirror is the worst of the worst. Quite honestly the worst, most hate-filled and insidious article I have ever read, and it is literally my job to search out and read hate-filled and insidious articles.
It’s titled:
Anti-vaxxers want to kill your babies, stage a coup and cause another lockdown!”
… and you don’t really need any more information than that. Read at your own risk.
2. THE RETURN OF LAB-GROWN MEAT
… well, not “the return” exactly, because it never went away. I guess “resurgence” is the better word. There’s certainly a sudden bump in the coverage.
The Guardian “asks the expert” if lab-grown meat will replace the real thing. The “expert” in question makes and sells lab-grown meat and, rather unsurprisingly, they say “yes!”.
And then the Times, with a tone of reluctant surrender, tells us we “must embrace lab-grown meat” whether “we like it or not”.
At the same time, Sky hosts a “climate debate” on lab-grown meat. One of those fake “debates” which serves a pre-determined agenda by basing a staged disagreement on fundamental assumptions which neither side questions.
In this case, it’s just assumed that LGM is good for the planet, and that actual meat is bad for it. Neither of those things are proven to be true.
But good news everyone! Your genetically synthesised meat-like protein paste is one step closer…whether you like it not.
3. “TREAT VIOLENCE AGAINST WOMEN AS SERIOUSLY AS TERRORISM”
The result of the Sarah Everard trial in the UK has kicked off a wave of fear-based propaganda concerning just how much violence against women goes on, and what we need to do about it. Over and over again a list of very predictable names in very predictable publications talk up the idea that women are “still not safe”, or never “feel safe” (which is not the same thing).
Clearly, any murder is a tragedy for the victim and their family, but to present our country, or society, as inherently violent or dangerous is completely disengenuous.
Let’s just check the stats, for the sake of reality.
In the UK, and most of the Western world, violent crime has been generally on the decline for decades. In 2019, EU statistics found a 32% drop in homicides since 2008. In 2020, the UK suffered ~750 murders in a population of 68 million people, meaning a crude murder rate of 0.001% (or 1 per 100,000). Less than one-third of those killed were women, and only 20% of them were attacked on the street.
Our society is not perfect, but violent crime (against either gender) has literally never been less of a danger in the history of the country. In terms of violent crime, the streets are as safe for women as they have ever been. If they don’t feel safe, well that’s probably because the media keep telling them how much “danger” they’re in.
But why? Why the massive exaggeration of the danger? And why the clarion calls for “action” on violence against women?
Well, the same exact reasons behind the “pandemic” narrative. Because hysteria is always useful. Because the people in charge need us to be afraid all the time. Because they want to make sure different genders, races and orientations are constantly mistrustful of one another. And, obviously, because it can be manipulated into increased powers for the state.
Social media companies are already being pressured to “do more to protect women”. After Everard’s murder first in the news in March, people were suggesting male-only curfews so women feel safe on the streets. If Covid has taught us anything, it’s that well-stoked public panic can be parlayed into exactly that kind of insane policy.
The title of this section is taken from a tweet by British Labour MP David Lammy:
It’s not clear what (if anything) David means by this. It’s entirely possible he’s just an idiot playing to the gallery, but anyone familiar with the real purpose, and disastrous societal fallout, of the “War on Terror” should probably be concerned about just how far those in charge could go to (allegedly) “make women feel safe.”
BONUS: THE TOTALLY-NOT-A-CULT OF THE WEEK
Just want to point out that the vaccine-pushers of the New Normal are totally not in a cult.
Whether it’s dressing up dancers like syringes to prance around with glassy-eyed soul-dead TV hosts:
Or literally citing God as the source of the vaccine:
This is all very normal behaviour, and if you perceive it as creepy or cultlike, it’s only because you are a heretic…sorry, I mean a science denier.
BONUS II: PROJECTION OF THE WEEK
For those of you who don’t know who Keith Olbermann is, well I envy you..and apologise for introducing you to his existence. He’s a petty, ill-informed, opinionated loudmouth who takes up irrational and bigoted positions on pretty much everything, and trumpets those views loudly to anyone who’ll listen.
And yesterday, he tweeted this…
It takes a serious lack of self-awareness to get your third untested vaccination against a disease you have a 99.5% chance of surviving, and then lambast everyone not worried about the disease for being scaredy cats.
IT’S NOT ALL BAD…
The world of sport, especially American sports, is somewhat of a hotbed of “vaccine hesitancy”. This is down to several factors, most probably to do with many US athletes coming from working-class demographics with longstanding (and entirely justified) suspicions of both the media and big pharma.
By way of contrast with Olbermann’s spittle-spraying diatribe, we present the calm and rational position of NBA star Jonathan Isaac, speaking at a press conference on September 27th:
The NBA has already said they will dock the pay of unvaxxed players who refuse to comply with local mandates. And both the NBA and NFL have put in place massive restrictions on unvaccinated players to pressure them into getting the shot. The media, likewise, is piling on the pressure to conform.
All the players resisting in the face of such a powerful campaign deserve respect. And they serve as a reminder that Covid sceptics, or even just those people who want nothing to do with the vaccine, are not anything like the tiny minority the media tries to pretend we are. And our arguments are rational and informed, not based on the insults and mindless frothing outrage of those trying to pressure us into conforming.
All told a pretty hectic week for the new normal crowd, and we didn’t even mention the “mysterious rise in heart attacks” or the UK’s entirely manufactured “fuel crisis”.
A Robust Balance
By Willis Eschenbach | Watts Up With That? | October 3, 2021
Albedo is the percentage of incident light that is reflected by an object. For years, I’ve read claims that the loss of Arctic sea ice is a positive feedback. It is logical—warming leads to less ice, less ice reduces the surface albedo; reduced surface albedo means more sunlight is absorbed; more sunlight absorbed leads to increased warming. Positive feedback. What’s not to like?
For example, in 2019 the IPCC said:
Feedbacks from the loss of summer sea ice and spring snow cover on land have contributed to amplified warming in the Arctic (high confidence).
Wim Rost pointed me to an interesting 2007 NASA article about Arctic albedo which says:
Although sea ice and snow cover had noticeably declined in the Arctic from 2000 to 2004, there had been no detectable change in the albedo measured at the top of the atmosphere: the proportion of light the Arctic reflected hadn’t changed. In other words, the ice albedo feedback that most climate models predict will ultimately amplify global warming apparently hadn’t yet kicked in.
Kato quickly understood why: not only is the Arctic’s average cloud fraction on summer days large enough—on average 0.8, or 80 percent—to mask sea ice changes, but an increase in cloudiness between 2000 and 2004 further hid any impact that sea ice and snow losses might have had on the Arctic’s ability to reflect incoming light. According to the MODIS observations, cloud fraction had increased at a rate of 0.65 percent per year between 2000 and 2004. If the trend continues, it will amount to a relative increase of about 6.5 percent per decade. At least during this short time period, says Kato, increased cloudiness in the Arctic appears to have offset the expected decline in albedo from melting sea ice and snow.
Wim suggested that I take a look to see if this process, of the changes in cloud albedo counteracting the changes in surface albedo, had continued up to the present.
Fortunately, the CERES data allows us to calculate the trends in both the surface albedo and the top-of-atmosphere (TOA) albedo. First, here’s the trend in surface albedo in percent per year, on a 1° latitude by 1° longitude basis.


Figure 1. Atlantic and Pacific centered views of the trend in surface albedo, in percent per year. Seasonal variations removed.
As expected, due to the reduction in Arctic sea ice, the albedo in the Arctic has indeed decreased significantly over the 21-year period. It’s decreased at a rate of 0.28% per year, a total of almost 6% over the 21 year period. Note also that the poles are the only part of the surface with a significant trend.
Next, here’s the top-of-atmosphere (TOA) albedo trend.


Figure 2. Atlantic and Pacific centered views of the trend in TOA albedo, in percent per year. Seasonal variations removed.
Amazing. The increase in cloud albedo has almost totally counteracted the decrease in Arctic surface albedo. The change is only six-hundredths of a percent per year, basically lost in the noise. The effect of the clouds has brought the polar regions back into line with the rest of the planet.
This inspired me to look at the correlation of the surface albedo and the cloud albedo over the period. Positive correlation of two variables means generally that when one increases, so does the other. Negative correlation means that they move in opposite directions. Figure 3 shows that result.


Figure 3. Correlation, surface albedo and cloud albedo.
This is also most interesting. It shows that the cloud albedo not only counteracts the sea ice albedo changes. It also counteracts the changes in surface albedo from snow and land ice. Not only that, but in the area of the sea ice, the correlation is around -1, meaning that surface albedo and cloud albedo move in nearly total opposition..
Examining Figure 3, it is obvious that over the land the correlation is negative almost everywhere. However, over the ocean, the correlation is clearly related to the temperature. As the Figure 4 scatterplot below shows, wherever the ocean is below about 22°C, the clouds tend to oppose any change in surface albedo.

Figure 4. Scatterplot showing the correlation of cloud and surface albedo trends versus surface temperature. Data is the gridcell-by-gridcell 21-year average values. Yellow/black line is a LOWESS smooth of the data.
Again, in the sea ice area where 21-year average temperatures are around zero, the negative correlation is almost perfect.
Discussion
With those results in mind, let me return to the 2019 IPCC claim:
Feedbacks from the loss of summer sea ice and spring snow cover on land have contributed to amplified warming in the Arctic (high confidence).
Note that despite the IPCC claim of “high confidence”, the 2007 findings of Kato and the more recent CERES data shown above demonstrate that feedback from changes in sea ice and snow cover have NOT contributed in any significant way to amplified warming in the Arctic. Cloud changes offset these sea ice and snow changes almost entirely. In short, the IPCC claim is overstated.
This highlights the problem with the claim that we should all listen to the “97% consensus” … it’s meaningless. Science is the process of overthrowing the consensus.
Journal Rebuked for Publishing Biased Letter Signed by EcoHealth President
By Dr. Joseph Mercola | October 2, 2021
In July 2021 and February 2021 the medical journal The Lancet printed letters signed by 24 scientists, physicians, epidemiologists and virologists that denied the possibility that SARS-CoV-2, the virus that causes COVID-19, originated in a lab.
One of those signers was Peter Daszak, president of EcoHealth Alliance, which received grant funds from the National Institute of Allergy and Infectious Diseases (NIAID) for gain-of-function research. The information on Daszak’s, EcoHealth Alliance’s and the NIAID’s involvement in research that possibly could have led to a lab origin was revealed in late-summer, 2021.
Previously, any suggestion that a lab leak could have occurred was resoundly proclaimed a conspiracy theory.
But now, in a rebuke of The Lancet for allowing the letters to be published when there “is so far no scientifically validated evidence that directly supports a natural origin,” 16 other scientists are calling for The Lancet to “open their columns to in-depth analyses of all hypotheses.”
“As scientists, we need to evaluate all hypotheses on a rational basis, and to weigh their likelihood based on facts and evidence, devoid of speculation concerning possible political impacts” they add. “More importantly, science embraces alternative hypotheses, contradictory arguments, verification, refutability, and controversy. Departing from this principle risks establishing dogmas, abandoning the essence of science, and, even worse, paving the way for conspiracy theories.”
SOURCES:
Hospitals Should Hire, Not Fire, Nurses with Natural Immunity
BY MARTIN KULLDORFF | BROWNSTONE INSTITUTE | OCTOBER 1, 2021
Among many surprising developments during this pandemic, the most stunning has been the questioning of naturally acquired immunity after a person has had the Covid disease.
We have understood natural immunity since at least the Athenian Plague in 430 BC. Here is Thucydides:
‘Yet it was with those who had recovered from the disease that the sick and the dying found most compassion. These knew what it was from experience and had no fear for themselves; for the same man was never attacked twice—never at least fatally.’ – Thucydides
We have lived with endemic coronaviruses for at least a hundred years, for which we have long-lasting natural immunity. As expected, we also have natural immunity after Covid-19 disease, as there have been exceedingly few reinfections with serious illness or death, despite a widely circulating virus.
For most viruses, natural immunity is better than vaccine-induced immunity, and that is also true for Covid. In the best study to date, the vaccinated were around 27 times more likely to have symptomatic disease than those with natural immunity, with an estimated range between 13 and 57. With no Covid deaths in either group, both natural and vaccine immunity protect well against death.
During the last decade, I have worked closely with hospital epidemiologists. While the role of physicians is to treat patients and make them well, the task of the hospital epidemiologist is to ensure that patients do not get sick while in the hospital, such as catching a deadly virus from another patient or a caretaker.
For that purpose, hospitals employ a variety of measures, from frequent hand washing to full infection control regalia when caring for an Ebola patient. Vaccinations are a key component of these control efforts. For example, two weeks before spleen surgery, patients are given the pneumococcal vaccine to minimize postoperative infections, and most clinical staff are immunized against influenza every year.
Infection control measures are especially critical for older frail hospital patients with a weakened immune system. They can become infected and die from a virus that most people would easily survive. A key rationale for immunizing nurses and physicians against influenza is to ensure that they do not infect such patients.
How can hospitals best protect their patients from Covid disease? It is an enormously important question, also relevant for nursing homes. There are some obvious standard solutions, such as separating Covid patients from other patients, minimizing staff rotation, and providing generous sick leave for staff with Covid-like symptoms.
Another goal should be to employ staff with the strongest possible immunity against Covid, as they are less likely to catch it and spread it to their patients. This means that hospitals and nursing homes should actively seek to hire staff that have natural immunity from prior Covid disease and use such staff for their most vulnerable patients.
Hence, we are now seeing a fierce competition where hospitals and nursing homes are desperately trying to hire people with natural immunity. Well, actually, not.
Instead, hospitals are firing nurses and other staff with superior natural immunity while retaining those with weaker vaccine-induced immunity. By doing so, they are betraying their patients, increasing their risk for hospital-acquired infections.
By pushing vaccine mandates, White House chief medical advisor Dr. Anthony Fauci is questioning the existence of natural immunity after Covid disease. In doing so, he is following the lead of CDC director Rochelle Walensky, who questioned natural immunity in a 2020 Memorandum published by The Lancet. By instituting vaccine mandates, university hospitals are now also questioning the existence of natural immunity after Covid disease.
This is astonishing.
I work at Brigham and Women’s Hospital in Boston, which has announced that all nurses, doctors and other health care providers will be fired if they do not get a Covid vaccine. Last week I spoke with one of our nurses. She worked hard caring for Covid patients, even as some of her colleagues left in fear at the beginning of the pandemic.
Unsurprisingly, she got infected, but then recovered. Now she has stronger and longer-lasting immunity than the vaccinated work-from-home hospital administrators who are firing her for not being vaccinated.
If university hospitals cannot get the medical evidence right on the basic science of immunity, how can we trust them with any other aspects of our health?
What’s next? Universities questioning whether the earth is round or flat? That, at least, would do less harm.
Martin Kulldorff, Senior Scholar of Brownstone Institute, is a professor of medicine at Harvard Medical School. kulldorff@brownstone.org
Rep. Adam Schiff says YouTube’s ban of vaccine skepticism doesn’t go far enough

By Christina Maas | Reclaim The Net | October 2, 2021
Rep. Adam Schiff praised YouTube’s decision to ban all vaccine skepticism but said it was not the “end of our fight against misinformation.”
On Wednesday afternoon, YouTube announced that it will ban all vaccine skepticism to stop the spread of what it says is misinformation. The ban not only applies to COVID vaccines but also any other vaccines that pharmaceutical companies produce.
While making the announcement, YouTube said: “Today’s policy update is an important step to address vaccine and health misinformation on our platform, and we’ll continue to invest across the board.”
YouTube’s decision was applauded by many, including Rep. Adam Schiff.
“YouTube’s curbing of anti-vaccine content is a strong first step,” the Democrat congressman wrote on Twitter. But this doesn’t mark the end of our fight against deadly misinformation. These policies must be enforced. And we must keep pushing for other companies to follow suit. What do you say, @Amazon and @Facebook?” hinting at his demands for more censorship.
YouTube Bans Mercola, Others Without Warning but Tips Off Media First
By Dr. Joseph Mercola | October 1, 2021
In a move to override the First Amendment with its own interpretation of what constitutes free speech, YouTube spent the last few days of September planning and executing a coup that included notifying major media of what they were doing before they pulled it off.
The coup was a sudden strike against Mercola.com, the National Vaccine Information Center (NVIC), Robert F. Kennedy Jr. and others whose channels YouTube decided to shut down without as much as a single word of warning — except to news agencies that obviously were tipped off in advance.
According to the Washington Post, YouTube was specifically targeting channels “associated with high-profile anti-vaccine activists … who experts say are partially responsible for helping seed the skepticism that’s contributed to slowing vaccination rates across the country.”
Early in the work day September 29, the Post gave Dr. Mercola exactly 23 minutes to respond to a story they had to have already had written about. They contacted Mercola’s media department just after 9 a.m.; they broke the story at 9:35 a.m.
CNBC’s Jim Forkin must have had a tip too, from YouTube, as he contacted Mercola at 9:12 a.m., with just two sentences: “Have your videos been removed from YouTube?” and “Do you have a statement or comment?”
YouTube, meanwhile, quietly changed their policies regarding who gets to publish on their server and who gets banned. It was a deviously brilliant move: Just change the rules to match the (previously compliant) content of the individuals you want to remove, and provide users no time to remain in compliance of the new rules.
Featured Video

Iran Blockade Complications
or go to
Aletho News Archives – Video-Images
Book Review
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
Blog Roll
 Aletho News
Aletho News- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- COVID Conniving Receives First Federal Indictment
- Iran Blockade Complications /Lt Col Daniel Davis & Nima Alkhorshid
- Pirates of Mediterranean: Israel does as it pleases in the Sea of Three Continents
- Minab children massacre not ‘unfortunate situation’ but ‘heinous war crime’: Tehran
- OPCW Forced To Pay Damages To Whistleblower Who Found Evidence Of False Flag In Syria
- Iran can thrive under blockade, the US and its allies cannot
- Iran slams US leadership, debunking fabrications, false war costs
- Here’s why Iran is sovereign and Germany is not
- Israel pours $730m into global propaganda machine as reputation collapses
- If Americans Knew
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
