This is nuts, Moderna & Pfizer intentionally lost the clinical trial control group testing vaccine efficacy and safety
Conservative Treehouse | August 6, 2021
This is not just scientific madness, it appears to be very intentional and purposeful.
The Moderna and Pfizer vaccine tests were conducted, as customary, with a control group; a group within the trial who were given a placebo and not the test vaccine. However, during the trial -and after the untested vaccines were given emergency use authorization – the vaccine companies conducting the trial decided to break protocol and notify the control group they were not vaccinated. Almost all the control group were then given the vaccine.
Purposefully dissolving the placebo group violates the scientific purpose to test whether the vaccine has any efficacy; any actual benefit and/or safety issues. Without a control group there is nothing to compare the vaccinated group against. According to NPR, the doctors lost the control group in the Johnson County Clinicial Trial (Lexena, Kansas) on purpose:
(Via NPR) […] “Dr. Carlos Fierro, who runs the study there, says every participant was called back after the Food and Drug Administration authorized the vaccine.
“During that visit we discussed the options, which included staying in the study without the vaccine,” he says, “and amazingly there were people — a couple of people — who chose that.”
He suspects those individuals got spooked by rumors about the vaccine. But everybody else who had the placebo shot went ahead and got the actual vaccine. So now Fierro has essentially no comparison group left for the ongoing study. “It’s a loss from a scientific standpoint, but given the circumstances I think it’s the right thing to do,” he says.
People signing up for these studies were not promised special treatment, but once the FDA authorized the vaccines, their developers decided to offer the shots. (read more)
Just so we are clear, the final FDA authorization and approval for the vaccines are based on the outcome of these trials. As noted in the example above, the control group was intentionally lost under the auspices of “the right thing to do”, so there is no way for the efficacy, effectiveness or safety of the vaccine itself to be measured.
There’s no one left within the control group, of a statistically valid value, to give an adequate comparison of outcomes for vaxxed -vs- non-vaxxed.
Whiskey – Tango – Foxtrot !!! This is nuts.
That NPR article is one to bookmark when people start claiming the vaccination is effective.
How can the vaccine not be considered effective when there is no group of non-vaccinated people to compare the results to?
Good grief, the entire healthcare system is operating on a massive hive mindset where science, and the scientific method, is thrown out the window in favor of ideological outcomes and self-fulfilling prophecies. The fact that the researchers and doctors, apparently under the payroll of the pharmaceutical companies that have a vested financial interest in the vaccine outcome, lost the control group on purpose is alarming.
Of course, Big Pharma will promote the vaccine as beneficial, and the controlled media will promote that message with a complete disconnect from the clinical trial details, and the FDA will grant approval on results that were intentionally constructed to produce only one outcome.
Madness…. All of it.

Time is running out to stop the ‘vaccine’ control project
By Daniel Miller | TCW Defending Freedom | August 9, 2021
WE HAVE a limited time to act. The essence of the situation now is clear: what is still perceived by many as a medical emergency is in reality a highly organised global corporate and political agenda. This agenda is directed towards imposing unimaginable control over the global human population though mandatory vaccination, connected to a digital passport, which will be linked to digital currency and a social credit score.
These technologies enable power to be centralised to a level of intensity never seen before in history.
At the controls of the machine will be the network which has orchestrated everything that has unfolded over the past eighteen months.
Here is what has happened in Great Britain since March last year. The Ministry of Health under the direction of Matt Hancock has presided over the deaths of tens of thousands of the elderly in care homes. These deaths were not caused by deciding to lock down too slowly, but were the outcome of a series of political decisions.
These included turning care homes into prisons, and banning relatives from visiting, and placing an enormous order for Midazolam, a sedative which has been used for euthanasia.
At this time the government also reduced hospital capacity, emptied untested and sick patients into care homes, suppressed the early treatment use of safe generic drugs and initiated a behavioural control campaign directed towards increasing fear.
If there had been a premeditated plan to maximise deaths while retaining plausible deniability that this plan existed, how would it have unfolded differently?
The government has now converted hotels into prisons and incarcerates everyone who enters Britain from an arbitrary list of countries, drawn up without clear logic, and subject to sudden rapid changes. Leaving and returning to the country now involves submission to a regimen of humiliating, pointless and expensive testing based on Drosten’s defective PCR tests and a disinformation myth of asymptomatic spread.
Why are they doing this? To confuse and to humiliate, to deter travel, and to desensitise the population to a new normality of arbitrary imprisonment without trial.
Now the government has mandated the compulsory vaccination of care home workers even as evidence accumulates that the global universal vaccination programme, an unprecedented policy in the history of public health, following the unprecedented global lockdown, is a medical catastrophe with numbers of major side effects including death reported in the aftermath of vaccination climbing into tens of thousands, and still not ending the pandemic.
Mandating any medical treatment as a condition of employment writes medical apartheid into law; the fact that this treatment might be useless (since the ‘vaccines’ do not prevent contracting, transmitting or even dying from the virus) as well as dangerous indicates a darker logic.
The extension of the vaccine programme to children, who are at less risk from the virus than they are from vaccines, suggests the vaccines have a function independent of their role in serving as a vaccine passport Trojan horse. Children will be harmed and die due to this policy, having already been tortured for a year with pointless mandatory testing and propaganda baselessly accusing them of potentially becoming accidental murderers if they did not comply with government decrees. Meanwhile Carrie Antoinette Ceaușescu is pregnant once again, with Johnson having done to her what he has been doing to the country.
For the vaccines to receive regulatory approval (if not for further reasons) effective, safe and cheap treatments have been ruthlessly suppressed. In March 2020 the Lancet, once the most reputable medical journal in the world, now a propaganda organ for the global network, published a fake paper claiming hydroxychloroquine had a negative effect; the paper was eventually retracted. One of the largest hydroxychloroquine factories in the world burned down after an explosion. The highly effective drug ivermectin remains suppressed in the UK and criminalised in other countries. If these drugs had been made available tens of thousands of people would be still alive today. Instead official policy has increased the death toll on the road to mandating vaccines.
Global government intends to make recurring vaccinations mandatory, indefinitely, to access social life. For this purpose they have stockpiled 450million doses of vaccines, enough to vaccinate each member of the British population seven times; other countries have similar figures. They will later order more. What is being implemented is compulsory repeated vaccination for perpetuity.
Towards this goal the facts about the danger of the virus and now the dangers of the vaccines have been ruthlessly suppressed, and bogus information, lies, neurolinguistic programming, and pseudo-scientific models promoted in their place.
A long and growing list of authoritative and conscientious scientists and doctors (including John Ioannidis, Mike Yeadon, Martin Kulldorff, Jay Bhattacharya, Sunetra Gupta, Didier Raoult, Scott Atlas, Peter McCullough, Dan Erickson and Artin Massihi, Sucharit Bhakdi, Robert Malone) have been censored and defamed. In their place we’ve been presented with charlatans, propaganda actors and fanatics.
Sweden, Florida and Texas, which have all defied the global line on lockdowns, are no longer mentioned, while Haiti’s Moise, Burundi’s Nkurunziza, and Tanzania’s John Magufuli are all dead, in Magufuli’s case weeks after the Guardian published a Gates Foundation-sponsored article demanding action.
This is a shameful period in human history and with every day that passes the shame of what we have already allowed to happen deepens. We have failed to stop a systematic policy which has killed millions around the world and will kill millions more. We have failed to stop the imposition of policy of child abuse on a national scale. We have failed to stop the imposition of lockdown policy which has achieved nothing but the immiseration of hard-working men and women. We are facing government by mercenaries, tyrants, propagandists and fanatics.
Men and women who have already shown courage must continue to do so, and others must now find their courage.
Doctors who have sacrificed their ethics to collaborate in this grotesque charade must redress the balance and remember their duty is to patients, not the government, and not to science.
Apathetic journalists who for eighteen months have functioned as the mindless relays of a criminal regime must recognise their duty is to truth and to the people.
The judiciary, who for eighteen months have deferred to rule by diktat and extended their goodwill to tyranny must recognise, like some of their colleagues in Spain, Alberta, Lisbon, Weimar and elsewhere, that their duty is to justice and human rights, and that these cannot be suspended under any circumstances whatsoever without being destroyed completely.
The vaccination programme must be stopped, or it will never end. Instead, it will become the basis of a new post-social contract modelled on the periodically updated terms of social media in which shared political and corporate interests will make humanity a resource to be farmed.
The Government, who answer to these interests, will seek to reimpose a lockdown with additional restrictions in the autumn. They must be stopped by every moral means.
DR RYAN N COLE: A PATHOLOGIST’S SUMMARY OF WHAT THESE INJECTIONS DO TO YOUR BRAIN & OTHER ORGANS
Free Speech Warrior
Extract presentation from America’s Front Line Doctors ‘White Coat Summit’ San Antonio TX July 28, 2021
Dr. Ryan Cole is the CEO and Medical Director of Cole Diagnostics, one of the largest independent labs in the State of Idaho. Dr. Cole is a Mayo Clinic trained Board Certified Pathologist.
He is Board Certified in anatomic and clinical pathology. He has expertise in immunology and virology and also has subspecialty expertise in skin pathology.
He has seen over 350,000 patients in his career.
PHE Data Confirms That New Infections Peaked and Dropped in the Unvaccinated Before They Did in the Vaccinated
By Will Jones • The Daily Sceptic • August 8, 2021
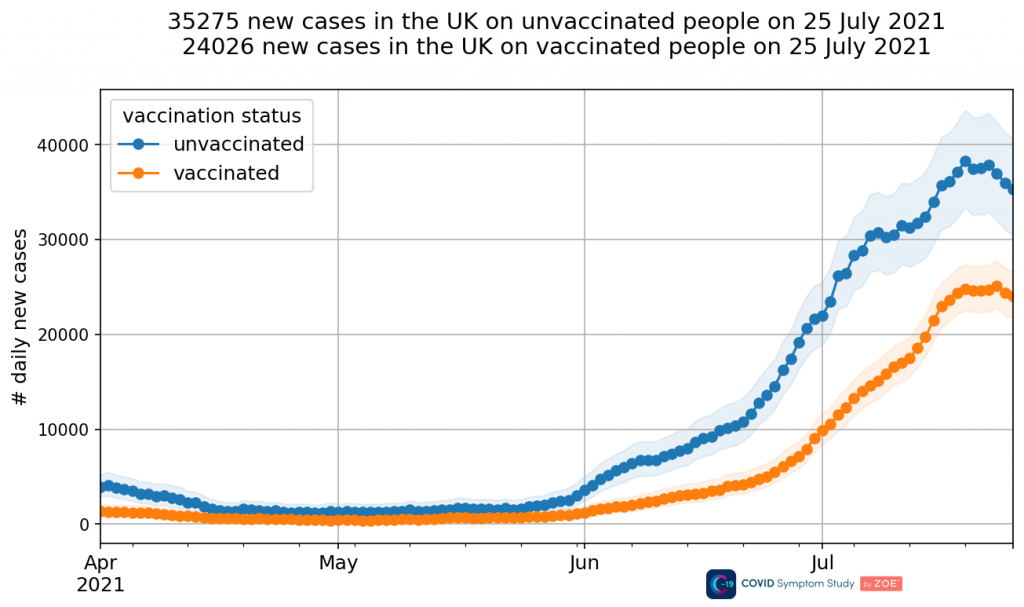
Back in early July I noted that data from the ZOE Covid Symptom Study was showing that new infections in the unvaccinated were peaking and falling while those in the vaccinated were still surging.
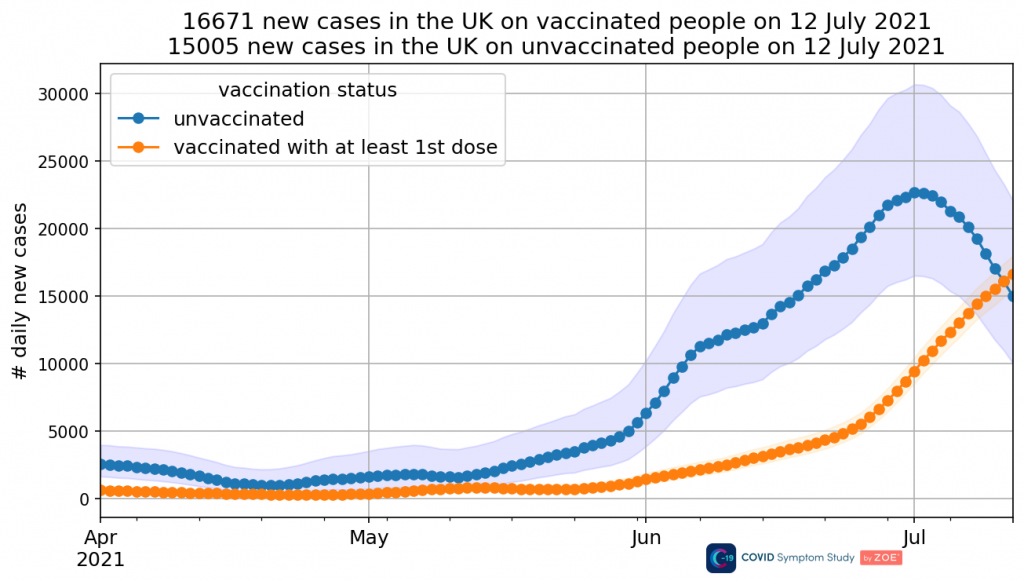
This was not a phenomenon noted elsewhere and prompted questions about whether it showed that the vaccines were delaying infection, or whether it was primarily an age-based phenomenon. Unfortunately, before anyone was able to investigate further, within a couple of weeks ZOE had ‘updated‘ their methodology and in their new data the phenomenon had oddly disappeared.
This left questions as to whether it had been entirely an artefact of problems with their previous methodology or whether it had been a real phenomenon.
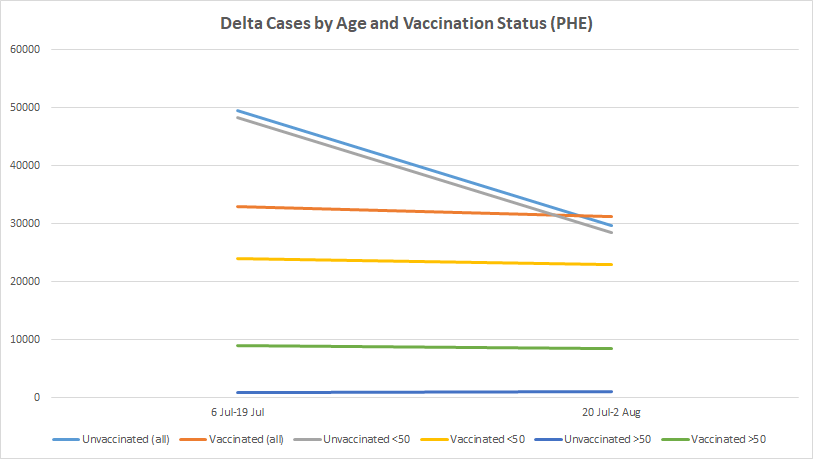
PHE data from the three most recent technical briefings (18, 19 and 20) allow us now to answer this question. Above (top of page) are the Delta case counts for the period July 6th to July 19th and then July 20th to August 2nd, broken down by vaccination status and age. (Actually, it’s not clear whether the initial date is July 6th or another date around then as briefing 18 appears to have a typo and says its data runs up to June 21st, even though briefing 17 also had data up to June 21st and the figures in briefing 18 are higher. However, for the purpose of this analysis it’s not important exactly what the start date is, and I have used July 6th as that is what it would be assuming briefing 18 has the equivalent date to the other briefings.)
The key lines to look at in the chart are the grey and yellow lines. They show that in the under-50s, Delta cases in the unvaccinated dramatically declined between early July and late July whereas those in the vaccinated (at least 21 days after the first dose) were stable. In the second half of the month there were actually more infections in the vaccinated of all ages than in the unvaccinated (the blue and orange lines).
This was the period when new infections nationwide peaked (on July 17th, by report date) and dropped quickly. This new analysis allows us to see that this fast drop was entirely in the unvaccinated under-50s (presumably the result of reaching herd immunity for the Delta variant). Infections in the vaccinated of all ages (and the unvaccinated over-50s) did not fall at the same time but remained stable. This helps explain why the drop ended around July 28th (by report date) and new infections have currently plateaued. What we are experiencing now is the ‘wave’ of infections in the vaccinated (along with the unvaccinated over 50s).
We can’t be sure that the explanation of the phenomenon is that the vaccines delayed infection. Another possibility is that the early surge was in the younger, less vaccinated portion of the under 50s (i.e., people under 30). What we really need is a finer breakdown by age. Unfortunately, despite all the data published during this crisis, very little of it is properly broken down by both vaccination status and age to allow us to do this kind of analysis.
Nonetheless, this confirms that ‘old ZOE’ was right to show infections in the unvaccinated falling during July while those in the vaccinated did not. The fact that ‘new ZOE’ no longer shows this phenomenon once again leads to questions about what changes were made and why, and whether the new methodology is really more reliable, or just more politically acceptable.
Does a high fibre diet prevent disease?

By Sebastian Rushworth | August 8, 2021
All doctors (and probably most non-doctors) have heard of Burkitt’s lymphoma, a type of cancer found primarily in children living in malaria-endemic areas in Africa. Denis Burkitt was the first person to describe the disease, and also the first person to propose that there was an environmental cause (now known to be simultaneous infection by both malaria and Epstein-Barr virus).
Most doctors probably don’t know that Denis Burkitt is also almost single-handedly responsible for the now widespread belief that dietary fibre is an important part of a healthy diet. Interestingly, Burkitt developed his ideas about dietary fibre after corresponding with a less well known doctor called Thomas Cleave (who hasn’t been allowed to give his name to any diseases).
Cleave was interested in the connection between diet and disease, and had noticed how the transition from a traditional diet to a modern diet, rich in refined carbohydrates, was associated with a massive increase in a large number of diseases, including cancer, diabetes, heart disease, and obesity. He even wrote a book on the subject. Burkitt was introduced to Cleave in the late 1960’s by epidemiologist Richard Doll (himself famous for discovering that smoking causes lung cancer).
Burkitt was deeply affected by Cleave’s ideas, and in particular his conception that all the “diseases of civilization” had a single underlying cause, but he took the data and went off in a different direction with it. While Cleave believed that it was the refined carbohydrates in the modern diet that were causing harm, Burkitt came to believe instead that it was the absence of dietary fibre that was responsible. Since refined carbohydrates are by definition low in dietary fibre, the two things track together perfectly, and it becomes almost impossible to say from observational data which is the causative factor and which is the confounder.
There was a big fly in the ointment of Burkitt’s hypothesis from the start, however, and that was the fact that the Maasai tribespeople in Kenya and Tanzania, who lived on a diet consisting almost entirely of meat, milk, and blood, showed none of the diseases of modern civilization, even though they had virtually no fibre in their diet. Burkitt, who spent much of his career in Africa, was well aware of this fact, but seemingly chose to ignore it because it didn’t fit his hypothesis.
The world of nutrition was at this time (the late 1970’s) focusing increasingly on dietary fat as the cause of modern diseases (based on atrociously low quality evidence and forceful lobbying by diet-heart hypothesis originator Ancel Keys), and Cleave’s hypothesis was inconvenient, because telling people to cut down on both fats and carbohydrates wouldn’t work – people had to eat something. Burkitt’s fibre hypothesis could however be made to fit together with the diet-heart hypothesis without too much trouble. The two were thus wedded and came to dominate dietary advice for the next couple of decades.
That is how breakfast cereals came to be considered a health food, and why we’ve all been told to increase our intake of dietary fibre. Anyway, it’s now a couple of decades later. One would think that by now there would be plenty of data from actual randomized trials to tell us whether we should be eating more dietary fibre or not. Unfortunately we’re still to a large extent stuck with crappy and confounder-riddled observational studies that cannot separate the presence of refined carbohydrates from the absence of dietary fibre, and that therefore cannot actually say anything about what causes what.
The Cochrane Collaboration tried to do a systematic review and meta-analysis in 2016 to look at the state of the evidence when it comes to the ability of dietary fibre to prevent cardiovascular disease. They found 23 randomized controlled trials with a total of only 1,513 participants. Most of the studies ran for only 12 weeks (the minimum length of time the reviewers had set for inclusion in the review, since short term effects are meaningless from a public health standpoint), and the longest ran for only six months. That’s why I say they tried – there simply isn’t enough data to draw any firm conclusions about what effect dietary fibre has on cardiovascular disease risk. 1,513 people followed for a few months provides far too little data to be able to say anything certain.
With that being the case, the reviewers decided to look at surrogate markers for cardiovascular risk instead of looking at hard outcomes like heart attacks and deaths. In other words, they looked at blood lipids and blood pressure. They included trials of both dietary interventions (i.e. that had people eat more food rich in dietary fibre) and trials of fibre containing supplements. I prefer the fibre supplement trials, since the dietary intervention trials have the same confounding issue that the observational studies have – i.e. that an increase in intake of foods rich in dietary fibre virtually always also means a decrease in intake of foods rich in refined carbohydrates. The supplement trials are also at lower risk of bias, since they can be placebo-controlled and thereby blinded. But I’ll report what the diet modification studies showed too, for the sake of completeness. In total, there were fifteen fibre supplement trials and eight diet modification trials.
Let’s get to the results. The fibre supplements were associated with a marginal 0.04 mmol/L reduction in LDL (“bad cholesterol” – yes I know that description is dumb and technically incorrect) that was just about statistically significant. The effect was similar (0.03 mmol/L) in the diet modification trials. For an average person with an LDL of 4 mmol/L this would represent a reduction of just 1%, in other words nowhere near enough to be expected to have any noticeable impact on cardiovascular disease risk.
And LDL is anyway a poor predictor of risk of cardiovascular disease. A much better predictor is triglycerides. The fibre supplements were associated with a 0,03 mmol/L reduction in triglycerides (not statistically significant), while diet modification was associated with a 0,02 mmol/L increase in triglycerides (also not statistically significant). Considering that the average person has a triglyceride level of around 2 mmol/L, this amounts to no noticeable effect on triglycerides whatsoever (and when the supplement and diet modification trials were meta-analyzed together, the difference between high-fibre and low-fibre was exactly zero mmol/L).
When analyzing blood lipids, the final piece of the puzzle is HDL (“good cholesterol”). While you want LDL and triglycerides to be low, you want HDL to be high. Unfortunately, fibre was associated with a reduction in HDL – 0,04 mmol/L in the supplement trials and 0,03 mmol/L in the diet modification trials. Fortunately, that difference was again so small as to be utterly inconsequential.
Ok, so the overall picture is that fibre doesn’t meaningfully impact blood lipids one way or the other. What about blood pressure?
Both the supplement studies and the diet modification studies reported a 2 mmHg reduction in systolic blod pressure and a 2 mmHg reduction in diastolic blood pressure. Considering that the average person has a systolic blood pressure of around 130 and a diastolic blood pressure of 80, this again amounts to such a marginal difference that it’s not going to have any noticeable impact whatsoever on an individual’s risk of cardiovascular disease (in other words, the story when it comes to fibre is the same as the story when it comes to salt – the impact of diet change is far too small to have any noticeable impact on an individual’s heart disease risk).
So the evidence to support the notion that fibre is “heart healthy” is weak. Kellogg’s should definitely stop marketing bran flakes as a “heart healthy” food.
Fifty years ago, when Denis Burkitt started researching fibre and it’s possible health benefits, the first thing he focused on was it’s potential to prevent colon cancer. The notion that fibre might have a role in preventing colon cancer makes a lot more intuitive sense than the notion that it might prevent heart disease, for the simple reason that fibre doesn’t move from the intestine into the body proper (technically the contents of the intestine are considered to be outside the body), but fibre does have various effects on the intestine, not least of which is the fact that it interacts with the bacteria that reside in the colon.
Colon cancer is thus a good test case for the many claims made about dietary fibre’s health benefits. The Cochrane Collaboration carried out a systematic review in 2017 that looked at the ability of dietary fibre to prevent colon cancer. The review included randomized trials of people who had had polyps removed and that then followed them over time to see if they developed new polyps and/or colon cancer.
Colon cancer usually progresses in an orderly fashion, beginning as a polyp that over time (if you’re unlucky) progresses to full blown cancer, so studies that want to determine risk of colon cancer progression can usually get away with looking at whether new polyps develop rather than having to wait and see whether the participants develop cancer (which saves time and allows for shorter, smaller studies).
Five trials were identified, with a total of 4,798 participants. The average age of the participants was around 60 years at the start of the studies, and they were followed for two to four years. As with the heart disease studies, there was quite a bit of variation in terms of the intervention used, with four trials providing dietary supplements while one attempted diet modification. The trials were for the most part able to at least double people’s fibre intake.
Ok, let’s take a look at the results.
Over the course of follow-up, participants in the high fibre group were 4% more likely to develop at least one new polyp in their colon than participants in the control group, although the difference wasn’t statistically significant. Hmm. Odd. We’d have expected at least some signal of benefit. The trend definitely shouldn’t be towards harm.
But polyps are really just a surrogate marker, like blood pressure is when it comes to heart disease. What we really want to know is whether the high fibre diet protects against colon cancer. Two of the studies were big enough to provide data on this more meaningful outcome.
In these two studies, participants in the high fibre group were 170% more likely to develop colon cancer than participants in the control group. Yes, more. Not less. That difference was statistically significant. So… that’s strange. Admittedly, this result is based on a few thousand participants followed for a few years. It could be wrong. But what it means is that the highest quality evidence currently available suggests that a high fibre diet might actually increase your risk of colon cancer, not decrease it.
How do we square this finding with the observational data that shows a decrease in colon cancer risk with a high fibre diet? As mentioned, the observational data is heavily affected by confounding variables, not least of which is the fact that a high fibre diet usually means a diet low in refined carbohydrates. These results support the notion that Burkitt was wrong and Cleave was right – that the harms associated with a diet rich in refined carbohydrates are due to the presence of refined carbohydrates, not due to the absence of fibre.
So, what can we conclude from all this? Does fibre prevent the so-called “diseases of civilization”?
Well, maybe. That is certainly the impression you would get if you look at the observational data, which find a correlation between a low fibre diet and pretty much any chronic disease you care to look at. The randomized trials that have been done have however for the most part failed to show evidence of a benefit of increasing intake of dietary fibre.
Alarming PHE data shows the fatality rate in vaccinated under-50s is 57% greater than in the unvaccinated
By Will Jones | The Daily Sceptic | August 8, 2021
Yesterday I wrote about the new data from Public Health England that allows us to make a (rough) calculation of vaccine efficacy during the Delta surge. Using data from technical briefings 17 and 20 I calculated that vaccine efficacy against infection with the Delta variant in the over-50s was a disappointing 17%. Vaccine efficacy against mortality was a better (if lower than expected) 77%.
The Daily Expose also published a piece looking at the new PHE data and argued that it showed vaccination was actually increasing the risk of hospitalisation and death. Their analysis did not break the results down by age, however, and so did not take into account that most of the infections are in the young, who are less vaccinated, and most of the deaths are in the old, who are much more vaccinated. That’s why my analysis focused on the over-50s, and when you do that you find the vaccines reduced mortality during the Delta surge in that age group by around 77%.
The Daily Expose article helpfully drew attention to the fact that in a recently published document, the Government advisers on SAGE themselves appear to admit that the vaccines do not prevent infection and transmission. In paragraph eight, they write:
While we feel that current vaccines are excellent for reducing the risk of hospital admission and disease, we propose that research be focused on vaccines that also induce high and durable levels of mucosal immunity in order to reduce infection of and transmission from vaccinated individuals. This could also reduce the possibility of variant selection in vaccinated individuals.
This being the case, why is SAGE not advising the Government to cease all aspects of the vaccination programme based on the idea of reducing transmission and protecting others (vaccine passports, the coercion of young people, vaccination of children and so on) as its members clearly don’t believe that these things are backed up by sound scientific evidence?
The Daily Expose article also highlights that there is another way of using the data in the PHE report to calculate the vaccine effectiveness against death. This is by calculating the case fatality rates (CFRs) in the vaccinated and unvaccinated groups respectively and taking the ratio.
Doing this for the over-50s, between June 22nd and August 2nd there were 339 deaths from 17,926 cases in the double vaccinated, giving a CFR of 1.9%, and 167 deaths from 2,464 cases in the unvaccinated, giving a CFR of 6.8%. One minus the ratio of these gives a vaccine effectiveness against death of 72% (1-(1.9%/6.8%)). Unlike the figure I calculated yesterday using population vaccination coverage, this is the vaccine effectiveness against death once infected, so doesn’t include any protection the vaccines provide against infection in the first place, meaning it is not surprising that it is lower. That it is not much lower is a further indication that the vaccines do little to prevent infection.
Because with this method we don’t need to worry about vaccination coverage in the population, we don’t need to restrict ourselves to the period June 22nd to August 2nd, which I selected because it was when the vaccination programme in the over-50s was basically complete. This means we can use all the Delta cases up to August 2nd as found in technical briefing 20. Again, for the over-50s, up to August 2nd there were 389 deaths from 21,472 cases in the double vaccinated, giving a CFR of 1.8%, and 205 deaths from 3,440 cases, giving a CFR of 6%. One minus the ratio of these gives a vaccine effectiveness against death (once infected) of 70%. So vaccine effectiveness against death in the over-50s rose slightly during the recent surge.
We can also use this method for the under-50s. Up to August 2nd there were 13 deaths from 25,536 cases in the double vaccinated, giving a CFR of 0.05%, and 48 deaths from 147,612 cases in the unvaccinated, giving a CFR of 0.03%. Strikingly, the CFR in the vaccinated here is higher than in the unvaccinated. In fact, it is 57% higher, meaning the vaccine effectiveness is negative 57%, i.e., in the under-50s the vaccine increases the risk of death once infected by 57%. This is in line with the Daily Expose‘s report, albeit the effect is found only in the younger population.
One caveat is that this doesn’t allow for any protection the vaccine might offer against infection, which may be higher in the under-50s (I haven’t attempted to calculate this as the vaccine coverage in that age group is constantly rising meaning I can’t pin down a figure). But even so, the fact that the case fatality rate among the vaccinated under-50s is 57% higher than among the unvaccinated under-50s is not just disappointing, it is alarming.
It’s worth bearing in mind that we are dealing with very small numbers here. There were only 61 deaths in these two groups (double vaccinated and unvaccinated under-50s) and only 13 of them were in the double vaccinated. One possible explanation is that these 13 deaths are highly vulnerable people who were vaccinated to try to protect them, while the CFR in the unvaccinated was driven down by the high infection rate among socially active young people. A more reassuring statistic, using data from the same report, is that the vaccine effectiveness against A&E attendance (once infected) among under-50s is 35%, and against an overnight hospital stay is 43%. These are not exactly stunning results, but do at least indicate a positive effect. Interestingly, the same statistics for the over-50s are a vaccine effectiveness against A&E attendance once infected of 71% and against an overnight hospital stay of 73%, indicating again an unexpectedly higher efficacy in the older population. Is this an artefact of higher risk younger people being vaccinated first?
Since, then, the disturbing statistic arises from just 13 deaths, perhaps the most sensible course of action would be for PHE to investigate these 13 deaths and publish a report assessing what role if any the vaccine may have played in them. More generally, given that the number of Covid deaths in vaccinated under-50s is small, a report filling out details on each would be illuminating. It would help to address what is otherwise a worrying sign that the vaccines may be counterproductive for younger people.
CDC Director “What our vaccines can’t do any more is prevent transmission”
By Meryl Nass, MD | August 7, 2021
Here is a 15 second clip of Rochelle Walensky talking to Wolf Blitzer.
She lies in the same sentence, claiming the vaccines still work “exceptionally well.”
If they don’t prevent transmission, you CANNOT USE PUBLIC HEALTH AND HERD IMMUNITY AS THE JUSTIFICATION FOR A MANDATE. At best, the vaccines might provide the recipient with some protection for a few months. But the downside is they might increase susceptibility or severity of disease later.
And when you add on the known and unknown short and long-term side effects, vaccination with an experimental product that went through minimal testing and poorly designed clinical trials just doesn’t make sense.
All the bluster about mandates was designed to trick the public into getting vaccinated before the truth came out. Now it’s out. Help your friends and family avoid these shots.
Remember: Your vaccine does NOT protect me, and it might not protect you either. Not for long. Then it might make things worse for you.
UK uses TikTok influencers to urge teens to get jab after Pfizer-linked vaccine committee chair admits policy lacks evidence
RT | August 6, 2021
Downing Street will enlist TikTok stars to push teens to get vaccinated, even as critics note that the committee behind the decision to expand the inoculation drive has admitted it had sparse evidence for doing so.
The Joint Committee on Vaccination and Immunisation (JCVI) announced on Thursday that the first dose of the Pfizer Covid vaccine will be offered to all 16- and 17-year-olds without needing the consent of their parents, reversing its own recommendation from just two weeks ago.
The independent panel of experts, which advises the UK government on immunisation, had earlier said that the jab should not be given to minors unless they were over 12 and suffered from medical conditions that would make them vulnerable to Covid-19, or lived with someone deemed high-risk. JCVI said it will issue a recommendation about when the second dose should be administered at a later date.
The NHS is now gearing up to give the shot to about 1.4 million children. To help with the effort, the government plans to assemble an army of Instagram and TikTok stars, as well as a fleet of ‘vaccine buses’ to drum up enthusiasm for the jab and make it easy for teens to get, iNews reported.
The kid-friendly approach to promoting the Pfizer jab comes after social media observers highlighted the fact that JCVI chair Wei Shen Lim sent mixed signals about how the decision to offer the jab to teens was made.
During a press briefing on Thursday announcing the policy, Lim said his committee decided to reverse its recommendation after “carefully considering the latest data.”
But he appeared to back-pedal after a journalist asked if the committee would be publishing “the evidence” used in making its decision to allow 16- and 17-year olds to get the shot, in order to help reassure parents. Lim responded by stating that there was currently no evidence available to share with the public.
The intention is for all the evidence to be published. The evidence isn’t necessarily in the hands of JCVI. We have spoken to academic partners and to other people in other countries as well. So wherever possible we encourage that the evidence is published, but the timing is not in our hands.
The committee’s attempt to explain its decision led to head-scratching from the media. Sarah Knapton, the Science Editor at The Daily Telegraph, said that after sitting through two press briefings, “I’m none the wiser about why JCVI has changed their advice. Not convinced they know either.”
Others pointed to what appears to be a rather straightforward conflict of interest. While the JCVI claims to be an independent body, Professor Wei Shen Lim is part of a department at the British Thoracic Society that received more than £25,000 ($34,760) in funding from Pfizer. Lim declared the “departmental interests” in a 2021 audit, which stated that he had “direct responsibility” over the Pfizer-gifted funds. The British Thoracic Society is a charity that aims to improve treatments for respiratory and associated disorders.
Governments around the world have urged people of all ages to get vaccinated, claiming that the more transmissible Delta variant may pose a greater risk. However, the disease has had a negligible effect on mortality among children. In the first 12 months of the pandemic, NHS data shows only 25 under-18s died from the illness.
Featured Video
House Resolution Calls for Tech Companies to Censor Speech
or go to
Aletho News Archives – Video-Images
Book Review
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran unveils new control measures over Strait of Hormuz transit
- House Resolution Calls for Tech Companies to Censor Speech
- Ceasefire no longer viable after 200 days of Israeli violations: Hamas
- Israeli strikes intensify across southern Lebanon, casualties reported
- Left in Disbelief: Israel in Panic over Hezbollah FPV Drone Nightmare
- Trump Taps Israel Lobbyist From Mossad Cutout FDD To Join Iran Negotiations
- Trump’s Blockade Snatches Defeat from the Jaws of Victory
- Geopolitics and Geoeconomics of the Strait of Hormuz
- Mali: a new front in the Western war on multipolarism
- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- If Americans Knew
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- No Tricks Zone
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
