Are Covid Fatalities Comparable with the 1918 Spanish Flu?
By Ethan Yang | AIER | April 27, 2021
On April 23, 2021 The New York Times published an article titled “How Covid Upended a Century of Patterns in U.S. Deaths.” The article lays out some data regarding the unprecedented uptick in the US death rate that occured in 2020.

As shown in the graph provided by the New York Times, US death rates have been steadily declining over the past century, likely due to advances in technology and living standards. Last year certainly signaled a noticeable break from this trend with a sizable increase in deaths, but not nearly the same as the 1918 Flu which is a universal benchmark for a killer influenza virus.
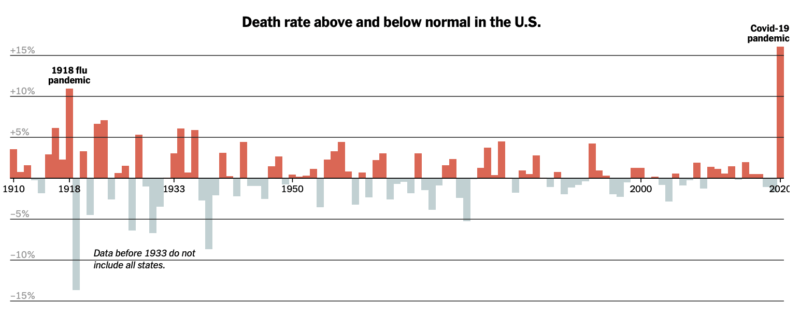
This graph provided by the New York Times indicates the spike in excess deaths in 2020, which is the number of deaths that have occured exceeding the predictions of standard death trends. This is of course all important information. Last year was certainly a horrific year with the outbreak of Covid-19, the lockdowns, and all the chaos that followed. It was a year of death and despair which should not be taken lightly.
Important Discussion: Deaths and Victims
It is common to invoke comparisons with the 1918 Flu Pandemic, as that was an extremely devastating virus that rocked the world. The article makes multiple references to the 1918 pandemic but there are a couple that raise interesting questions for further investigation. The first point is as follows,
“Combined with deaths in the first few months of this year, Covid-19 has now claimed more than half a million lives in the United States. The total number of Covid-19 deaths so far is on track to surpass the toll of the 1918 pandemic, which killed an estimated 675,000 nationwide.”
Comparing the death counts between the 1918 Flu and Covid-19 without adjusting for population growth is extremely misleading. In 1918 the population of the United States was roughly 103 million, while near the end of 2020 it stood at roughly 330 million. According to CDC statistics compiled by a study in JAMA Covid-19 killed 345,000 people in 2020 and now stands at around half a million as stated by the New York Times. Adjusted for the population growth of over 200 million people and holding the death rates constant, the 1918 Flu would have killed over 2 million people if it occured today, which is more than four times greater than Covid-19.
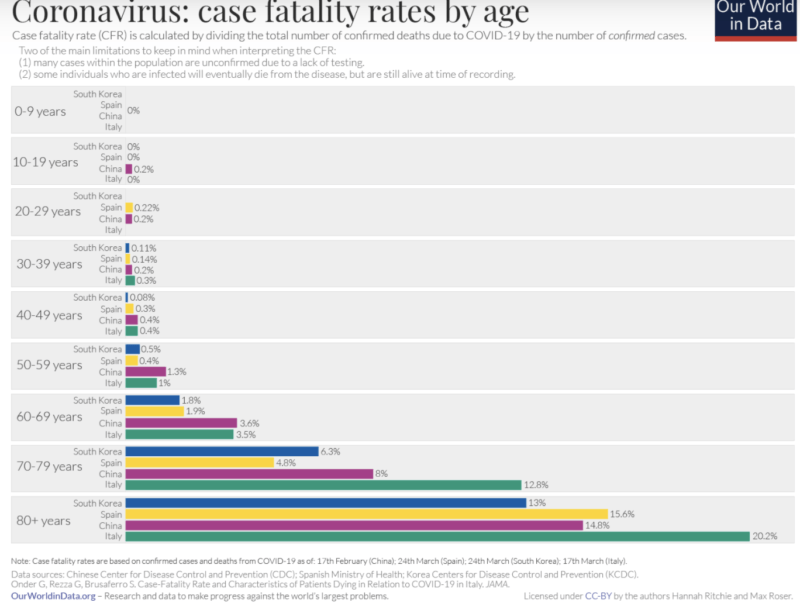
Furthermore, the two diseases are vastly different in terms of who is vulnerable. Covid-19’s severe outcomes almost exclusively affect the elderly and the immunocompromised, particularly those over the age of 65, which is also approaching the life expectancy of a human. Furthermore 94 percent of Covid deaths occurred with preexisting conditions. It poses virtually no risk to children, minimal risk to young adults, and only seems to kill more than 1 percent of victims with those over the age of 65.
On the other hand the Spanish Flu was devastating to virtually all age groups and did not discriminate between the healthy and the unwell. The CDC writes the following about the 1918 Flu:
“Mortality was high in people younger than 5 years old, 20-40 years old, and 65 years and older. The high mortality in healthy people, including those in the 20-40 year age group, was a unique feature of this pandemic.”
It is clear that the comparison is flawed between the 1918 Flu and Covid-19, as the former was a devastating killer virus whereas the latter only poses a threat to vulnerable populations.
Too Much Statistical Noise
It is certainly worth investigating the noted increase in excess deaths in 2020 as that is obviously a problem. However, the article seems to suggest that Covid-19 was the main causal factor driving increases in death. Although that is certainly a reasonable intuition given that it is a novel virus, clearly there is far more at play.
The main issue to point out is that there were two health crises, not one. Covid-19 is certainly one but we cannot simply ignore the absolutely devastating and unprecedented use of lockdown policies that drastically upended all of society in a way that a virus could never accomplish.
The effects of lockdowns have been thoroughly studied by AIER and in a series of articles I noted just some of the damage to the economy, young people, and the normal functioning of society. All these disruptions led to adverse outcomes whether it be mental health issues, decline in living standards, or even disrupted healthcare procedures. In a press release the CDC noted that in May 2020, it recorded the highest number of drug overdoses ever recorded in a 12-month period.
A study in JAMA notes that although there was a substantial increase in overall deaths in 2020, Covid-19 was only one part of the problem, assuming all Covid deaths are directly attributable to Covid and not a comorbidity.

Some statistics of note are an increase in deaths due to heart disease, unintentional injuries, stroke, and diabetes. Although more investigation would be needed to understand how all of this comes together, it wouldn’t be absurd to believe that lockdown policies led to an increase in deaths due to their many disruptions to normal societal functions.
To cite one example of many, the Mackinac Center Legal Foundation recounts on one of its clients by writing,
“One of the affected medical practices, Grand Health Partners, operates in the Grand Rapids area. It performs endoscopies and other elective surgeries, many of which were deemed nonessential by executive order. Due to the shutdown, many of their patients were not able to receive treatment and have suffered because of it.”
Alongside exploring and cutting through the statistical noise posed by increases in death plausibly related to lockdowns, there still needs to be a discussion on quantifying the Covid-19 death count. Genevieve Briand, an economist at John Hopkins University, was subject to a massive degree of controversy for putting out a flawed but important lecture – later expanded into a research paper – that pointed out among other things that Covid-19 deaths may be inappropriately reclassified as deaths from other leading causes.
This is especially worthy of discussion given that the overwhelming majority of Covid deaths occur with comorbidities amongst eldery populations often nearing or exceeding life expectancy.
Key Takeaway
The data is clear; 2020 was a horrific year full of death and despair. The New York Times’ article certainly does a great job at starting a conversation about this topic. However, its comparisons of Covid-19 and the 1918 Flu raises more questions than answers. Furthermore its presentation of data regarding increases in deaths requires more context.
Upon further investigation, it is clear that Covid-19 claimed many lives. However, it is also clear that there is a substantial presence of statistical noise from comorbidities and increases in death from other causes. This raises many questions not just about the collateral damage of our policy response, but also about whether we are even operating with the appropriate information to be making such decisions with people’s lives in the first place.
ITV’s Lorraine Show Caught Lying! Photoshops Picture To Push For Climate Lockdowns
WE GOT A PROBLEM
Show was aired thursday 22/04/21 https://www.itv.com/hub/lorraine/1a93…
Australian MP blasts Facebook’s ‘interference’ after his OFFICIAL page was banned for Covid-19 ‘misinformation’
RT | April 26, 2021
After Facebook deleted the official page of Craig Kelly for spreading “misinformation” about the coronavirus and vaccines, the independent MP said the “book-burning” US social media giant was interfering in Australia’s democracy.
Kelly was informed of Facebook’s ban by text on Monday morning, he told the media, describing the move as “censorship.”
Banning the page with some 86,000 followers represents “interference in Australian democracy,” he said.
“This was the most popular, highly used political Facebook page in the country,” he said, in remarks quoted by ABC. “They have basically burnt and torched and incinerated and obliterated from the record, previous comments and previous things that I’d made.”
Kelly’s personal page and Instagram account remained active, for now. A Facebook spokesperson said in a statement that the Australian MP had “repeatedly” violated their policies.
“We don’t allow anyone, including elected officials, to share misinformation about Covid-19 that could lead to imminent physical harm or [Covid-19] vaccines that have been debunked by public health experts,” the spokesperson said.
“It is not misinformation if you have a difference of opinion,” Kelly shot back. “The idea that they are some purveyors of all truth is just absolutely outrageous.” The ban is not just outrageous but also violates the principles of free speech, he added.
Facebook did not just remove a few posts, but the entire page, he said, describing it as “like setting fire to a book, not just removing the pages they disagree with.”
These people are the heirs to those who used to go around burning books because that is effectively what they have done.
Kelly has represented Hughes, a parliamentary district south of Sydney in New South Wales, since 2010. He resigned from the ruling Liberal Party in February, after Facebook suspended him for “misinformation” about Covid-19 and someone from the office of Prime Minister Scott Morrison told him to “shut up” about the virus.
Flush from the success of “fortifying” the 2020 US presidential election, Facebook announced in December that it would ban any “false claims” and “misinformation” about Covid-19, even if posted by public officials.
In January, Mark Zuckerberg’s social media behemoth clashed with Canberra over a proposed law requiring social media to pay for news content. After a week-long Facebook ban on all news content in Australia, the government relented and proposed an amended law, which critics said favored major corporations over local and independent news outlets.
French Report Urges Halt to Covid Mass-Jabbing
By Stephen Lendman | April 26, 2021
There’s nothing remotely safe and effective about experimental/unapproved Pfizer/Moderna mRNA technology and J & J’s vaccine for covid mass-jabbing.
Translated into English, a report by an independent French drug assessment center — the Centre territorial d’Information indépendante et d’Avis pharmaceutiques — CTIAP) called for halting mass-jabbing for covid “as a matter of urgency.”
It stressed that experimental Pfizer, Moderna, AstraZeneca and J & J covid drugs lacked sufficient testing, adding:
Their excipients (coloring agents, preservatives, fillers and other ingredients) should be considered as new active substances.”
They were OK’d for emergency use — when no emergency exists — before there was “proof of quality for the active substance and the finished product.”
CTIAP also called their manufacturing processes problematic.
Its report stressed that “variabilities, which impact the very core of the product, could even invalidate any clinical trials conducted” ahead, adding:
“Can we imagine launching a car manufacturing line and putting vehicles on the road, despite the uncertainties noted in the official documents published?”
“These uncertainties are related to the quality of the parts making up the engine and the various other parts, including those related to safety, the manufacturing process, the reproducibility of the batches that are being marketed, etc.”
“In the field of medicines (including covid mRNA technology and vaccines), the pharmaceutical act of ‘release’ of the finished product (an authorized product intended for sale) constitutes the final stage of control that precedes the release of these products to the population.”
“This key step of ‘release’ is under the pharmaceutical responsibility of the manufacturers.”
“Prudence…dictate(s) that, in all countries where these vaccines against (covid) have been marketed, all the batches thus ‘released’ should be withdrawn immediately.”
“These MAs (marketing authorizations) that have been granted should be suspended, or even canceled, as a matter of urgency until further notice.”
European Medicines Agency (EMA) documents explain lack of sufficient evidence to show whether experimental covid drugs are safe and effective.
Marketing authorization granted them by the EMA is “conditional” for up to one year — based on “incomplete data.”
Separately on Friday, a CDC advisory panel recommended unrestricted use of J & J’s hazardous covid vaccine for individuals aged-18 and older.
If approved by the Pharma-connected CDC and FDA as expected, J & J covid mass-jabbing will resume.
Claiming benefits — that don’t exist — outweigh risks defies reality.
The same holds for Pfizer/Moderna mRNA technology and AstraZeneca’s covid vaccine.
They’re experimental, inadequately tested, rushed to market drugs that are too hazardous for human use.
Mass-jabbing with them already caused countless numbers of adverse events, including deaths in the US, Europe and elsewhere.
Ignored by the CDC, FDA, and EMA is that no need or justification exists for use of these high-risk experimental drugs.
Safe, effective, low cost drugs, and alternative non-drug therapy, works to prevent, treat and cure seasonal flu-renamed covid as needed.
Defying reality, the pro-mass-jabbing NYT falsely claimed that “pause(d) (use of J & J’s covid vaccine) was widely considered a blow to national and global vaccination efforts (sic) and removed an effective vaccine (sic) that many states and countries had counted on to deploy in hard-to-reach places (sic).”
Experimental covid drugs don’t protect. They risk serious adverse events near-or-longer-term, including possible death.
Preserving and protecting health requires rejecting them.
The alternative is playing fast and loose with what’s too precious to lose.
“No Evidence Facemasks Keep Kids & Teachers Safe”
By Richie Allen | April 26, 2021
Speaking on Talk Radio this morning, Oxford University epidemiologist Carl Heneghan said that there is no evidence that face masks help to keep pupils and teachers safe in the classroom.
Heneghan told Julia Hartley-Brewer;
“What I would say to people is, in the absence of evidence, if you think they should be wearing them, go and talk to some children. That’s what I’ve done. And I’ve said, what’s the reality on the ground? What’s it like for you in class? How does it feel?
And I can tell you they hate them. They find it really difficult. They don’t adhere to the guidelines. So for instance at the end of class they go into their pocket. They pull them out. That’s a dangerous issue with co-infections and the potential of that to stay infected for a period of time.”
Heneghan went on to say that medical interventions must be backed by hard evidence that the intervention will work. He said;
“That’s all I ever do is say, where’s the evidence to inform what we do and if it’s lacking, you have to come down on the side of not intervening.
Now one of the key problems we’ve got when we intervene, is it becomes incredibly difficult to roll back interventions. And that’s what we are saying. That’s the great problem now, the just in-case approach. That’s not how to perform in healthcare.”
Should Unvaccinated and Obese Be Penalized by Government?
By Dr. Joseph Mercola | April 23, 2021
“Vaccine refusal will come at a cost — for all of us,” Edward-Isaac Dovere, a staff writer for The Atlantic, proclaims in an April 10, 2021, political commentary.1 Unvaccinated individuals “will have higher health care costs,” he says, and the vaccinated will have to foot the bill, either through taxes or insurance premiums.
This argument could have been made for decades, and can still be made today, for any number of groups. Obese individuals have far higher health care costs than those of normal weight. Insulin resistant people and those with Type 2 diabetes end up costing the health care system enormous sums. Who pays for them?
Overall, healthy individuals — people who generally do what they can to take good care of themselves to prevent chronic conditions — have always paid for those who are less particular about their diets and lifestyle.
The Economic Costs of Vaccination Vs. Vaccine Refusal
Dovere predicts the economic costs of vaccine refusal will begin to feature heavily as we move forward. He quotes Washington Gov. Jay Inslee, who told him,2 “You have a liberty right, and that unfortunately is imposing on everyone else and their liberty right not to have to pay for your stubbornness.” Not surprisingly, Dovere and Inslee both focus on just one side of what needs to be a two- if not four-sided equation.
When making public health policy, you have an obligation to analyze both the benefit and the cost of any given policy. In this case, what might be the cost of vaccine side effects, both in terms of health care costs and lives lost? As of April 1, 2021, VAERS had received 56,869 adverse events following COVID-19 vaccination, including 7,971 serious injuries and 2,342 deaths.3 By April 13, the had updated that death toll to 3,005.4
What might be the cost if the vaccines don’t work and you get sick anyway? As of April 15, 2021, some 5,800 Americans who had been fully vaccinated against COVID-19 had been diagnosed with COVID-19 post-vaccination; 396 (7%) required hospitalization and 74 died.5 These cases are popping up all over the world.
The vaccines are not foolproof. In fact, so-called “breakthrough cases,” meaning cases in which a fully vaccinated individual is diagnosed with COVID-19 are to be expected. I’m not sure why anyone is surprised, seeing how the vaccine makers have acknowledged that the mRNA injections are not designed to actually make you immune to SARS-CoV-2.
You can still contract the virus and spread it to others. What the shots may do is lessen your symptoms if and when you get infected with SARS-CoV-2. So, of course people can still get sick, as they did before. Some will require hospitalization. Some will die — just like they did previously, before the vaccine.
Then there’s the question of whether vaccinated individuals end up being more susceptible to variants of the virus than unvaccinated individuals. Preliminary research6,7,8,9 found that people who had received both doses of the Pfizer COVID-19 vaccine were eight times more susceptible to contracting the South African variant of SARS-CoV-2, called B.1.351, (5.4% compared to 0.7%).
Unfortunately, the study was too small to glean any information about outcomes, so we don’t know whether they developed milder or more serious illness than unvaccinated people sickened by the same variant.
Either way, if vaccinated people are more susceptible to more dangerous variants (which they claim B.1351 is), why assume that unvaccinated people would incur higher health care costs? Variants are now cropping up all over the place, so maybe vaccinated people will end up being responsible for a greater share of medical expenses. Maybe, if they have milder illness and unvaccinated have more serious illness, the costs might end up about the same for each group.
May There Be Economic Benefits to Vaccine Refusal?
In my view, the notion that COVID-19 vaccines will end this pandemic is an illogical fallacy since these shots do not provide actual immunity. The fizz in Dovere’s argument starts going flat on that basis alone. But there’s much more.
To really determine what’s best for public health, you’d also want to do the benefit and cost analysis of not vaccinating and relying on naturally-acquired immunity in combination with immune-boosting strategies instead, such as improving vitamin D levels across the entire population, for example.
Only when you have made all of those calculations — the benefit and cost of vaccinating, and the benefit and cost of not vaccinating — can you compare the two and begin to make statements about how certain groups of people may incur higher health care costs, and which strategy is likely to save the most lives. As of right now, it’s pure guesswork as to who’s going to cost more in the long run.
For example, I don’t know of any actual data showing that the health of people who are planning to forgo the vaccine place them at increased risk of serious COVID-19. If I were to guess, and this is pure speculation, people who have decided not to get vaccinated may be doing so because a) they know they’re in a low-risk category and/or b) they are health-conscious people who feel confident that they can prevent and/or treat COVID-19 in other cost-effective ways, should they get sick.
There are a lot of data that need to be compiled and analyzed before we can start declaring the COVID-19 vaccination campaign a public health care success, let alone a cost-saving imperative.
Appeal to Illogical Reasoning
Dovere goes on to discuss some of the messaging campaigns employed to lure people out of their vaccine hesitancy:10
“Two appeals seem to work best: First, the vaccines are safe, and they’re more effective than the flu vaccine. Second, you deserve this, and getting vaccinated will help preserve your liberty and encourage the government to lift restrictions.
(That last idea is what Jerry Falwell Jr. focused on in the vaccination selfie he posted11 this week, captioned, ‘Please get vaccinated so our nutcase of a governor will have less reasons for mindless restrictions!’) Inslee hopes that emphasizing those points will persuade more Republican men to get their shots.”
Sometimes it can help to spell out a logical fallacy using different words. (Personally, I believe Falwell was simply trying to be funny, but Dovere and Inslee have apparently seized the “lift restrictions” angle as a social conditioning opportunity, so that’s really what I’m addressing here.)
One rewrite of Falwell’s plea could be: “Please ignore your current health status and potential vaccine risks and just obey so that our governor will have less reason to impose unconstitutional and unscientific limitations on our basic rights and freedoms.”
In my view, a more appropriate way to prevent “mindless restrictions” would be to peacefully disobey and/or take the governor to court, as has been done to California Gov. Gavin Newsom. The Supreme Court has ruled against him no less than six times, finding he abused his power, overstepped his authority and violated the Constitution with his pandemic restrictions on churches.12
Urging someone to take a vaccine to prevent an elected official — who can be unseated — from implementing unscientific and/or unconstitutional restrictions is hardly rational. Let’s not forget that cost-benefit analyses13 have actually been done for lockdowns — perhaps one of the most mindless of restrictions — and the cost is far greater than the benefit.
The cost of the lockdowns in the U.K., in terms of Wellbeing Years (WELLBY), is five times greater than might optimistically be saved, and may in reality be anywhere from 50 times to 87 times greater. The cost for lockdowns in Canada is at least 10 times greater than the benefit.
In Australia, the minimum cost is 6.6 times higher, and in the U.S., the cost is estimated to be at least 5.2 times higher than the benefit of lockdowns. A cost-benefit analysis performed for New Zealand, which looked at the cost of adding just five extra days of “COVID-19 alert level 4” found the cost in Quality Adjusted Life Years (QALY) was 94.9 times higher than the benefit.
Should We Penalize Obesity and Vitamin D Deficiency?
If it’s determined that unvaccinated individuals need to be penalized socially, financially or otherwise, then how can we not also penalize other choices that significantly add to the COVID-19 burden? We know, for example, that vitamin D deficiency significantly raises your risk of COVID-19. In one analysis,14 82.2% of COVID-19 patients were vitamin D deficient.
I published a scientific review15 on the impact of vitamin D in COVID-19 in October 2020, co-written with William Grant, Ph.D., and Dr. Carol Wagner, both of whom are part of the GrassrootsHealth expert vitamin D panel. You can read the paper for free on the journal’s website.
Another major COVID-19 factor is obesity. As reported by CNN16 March 5, 2021, the COVID-19 death rates were more than 10 times higher in countries where more than half the adult population was overweight, compared to countries in which the obesity rate was below 50%. The COVID-19 death rates also rose in tandem with the prevalence of obesity, thereby strengthening the link, according to the report, released by the World Obesity Federation.
At the lowest end is Vietnam, which has an obesity rate of 18.3% and a COVID-19 death rate of 0.04 per 100,000. Toward the high end is the U.S., which has an obesity rate of 67.9% and a COVID-19 death rate of 152.49 per 100,000. (Of course, this report used COVID-19 mortality statistics that have been proven to be wildly exaggerated, as detailed in my interview with Dr. Henele.)
Making an already dire situation worse, recent data17 show 42% of U.S. adults have packed on unwanted pounds, with an average weight gain of 29 pounds, since the start of the pandemic. Only 18% report undesired weight loss, with an average weight loss of 26 pounds.
Government Has Ignored the Value of Healthy Population
According to the World Obesity Federation report, obesity was the second most important risk factor for hospitalization and death from COVID-19 — old age being the primary risk factor — and as noted by Johanna Ralston, CEO of the World Obesity Federation:18
“Old age is unavoidable, but the conditions that contribute to overweight and obesity can be highly avoidable if governments step up and we all join forces to reduce the impact of this disease. The failure to address the root causes of obesity over many decades is clearly responsible for hundreds of thousands of preventable deaths.”
Lead author of the report, Dr. Tim Lobstein, added:19
“Governments have been negligent, and ignored the economic value of a healthy population at their peril. For the last decade they have failed to tackle obesity, despite setting themselves targets at United Nations meetings. COVID-19 is only the latest infection exacerbated by weight issues, but the warning signs were there. We have seen it in the past with MERS, H1N1 and other respiratory diseases.”
Let’s Not Accept Hypocrisy and Double Standards
Even WHO Director-General Tedros Adhanom Ghebreyesus commented on the report saying it “must act as a wake-up call to governments globally,” as “The correlation between obesity and mortality rates from COVID-19 is clear and compelling.”
That said, let’s get back to Dovere’s argument that unvaccinated people are bound to incur higher health care costs due to COVID-19, and therefore there must be some way to penalize those people or force them into compliance.
Using that logic, what, then, do we need to do about obese individuals, whose risk of hospitalization due to COVID-19 is anywhere from 40% to 113% greater, and their chances of requiring intensive care 74% higher,20 than that of their non-obese peers? What do we need to do about people who just refuse to get their vitamin D levels up, and end up taking up the lion’s share of hospital beds?
To be clear, I am NOT proposing we penalize people based on their weight, metabolic flexibility or vitamin D status. I do not support that any more than I support penalizing unvaccinated people — and that is the whole point. Most would agree that this would be completely ridiculous.
My point is, if you cannot fathom penalizing obesity, insulin resistance, diabetes or vitamin D deficiency — conditions known to significantly raise your risk of severe COVID-19 — then how could you possibly consider penalizing an unvaccinated person based on that single parameter alone?
The question is especially valid because, again, vaccinated persons can contract and spread SARS-CoV-2 like anyone else. It’s really unclear how vaccinated people are “safer” than unvaccinated ones, when the only person standing to gain from these shots is the person getting it (in the form of milder symptoms when sickened).
Are You ‘Pure’ Enough for Your Government?
I think it’s important to realize that the COVID-19 vaccine campaign is less about protecting public health and more about creating the infrastructure and psychological climate required for the implementation of global tyranny, which will likely begin with the introduction of vaccine passports that are very similar to the China social credit system.
As discussed in “Vaccines Are the New ‘Purity Test,’” it can almost be likened to a loyalty test. Or perhaps it could best be described as a totalitarian submission test?
Getting private companies to require these vaccine passports only makes sense if there is a strong vaccine push, and this is one of many clues as to what’s really behind the stated “need” for the whole world to get vaccinated.
We’re not all at risk for COVID-19. For a vast majority of individuals, the vaccines make little or no sense, as for young, healthy individuals, their risks outweigh the benefit. Now they are pushing to vaccinate children, whose risk of getting COVID-19 is well-established as being profoundly minuscule.
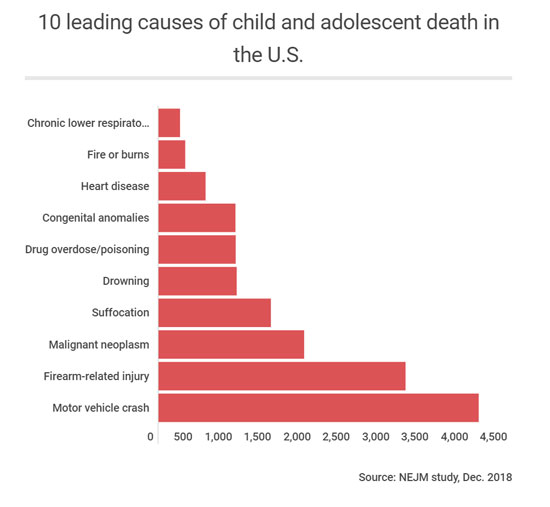
They are at exponentially higher risk from many other factors. There are currently fewer than 500 children who are reported to have died from COVID-19, even with the massively manipulated causes of death. Remember, if you had a positive COVID test and died from terminal cancer or a motorcycle accident, you were classified as a COVID-19 death.
As you can see from the graph below, there are 10 higher risks of death than COVID-19 for children. To be logically consistent, the government would need to be equally rigid about addressing all of these causes as aggressively as they are pursuing COVID-19 vaccination for children.
But it’s not about simply getting a vaccine into your arm. Ultimately, it’s about getting you tied into the digital system being launched in the form of vaccine passports. As explained by former Clinton adviser and author Naomi Wolf (whom I will be interviewing shortly) in a March 28, 2021, interview with Fox News’ Steve Hilton:21,22
“‘Vaccine passport’ sounds like a fine thing if you don’t understand what those platforms can do. I’m [the] CEO of a tech company, I understand what these platforms can do. It is not about the vaccine, it’s not about the virus, it’s about your data.
Once this rolls out, you don’t have a choice about being part of the system. What people have to understand is that any other functionality can be loaded onto that platform with no problem at all. It can be merged with your Paypal account, with your digital currency. Microsoft is already talking about merging it with payment plans.
Your network can be sucked up. It geolocates you everywhere you go. Your credit history can be included. All of your medical and health history can be included … It is absolutely so much more than a vaccine pass … I cannot stress enough that it has the power to turn off your life, or to turn on your life, to let you engage in society or be marginalized.”
Dangerous Curves Ahead
Wolf also points out the horrific history of IBM, which developed a sophisticated system of punch cards that allowed Nazi Germany to create a two-tier society and ultimately facilitated the rounding up of Jews for extermination. Fast-forward to today, and IBM is now a leader in the vaccine passport business. I wrote about this in “IBM Colluded With Hitler, Now Makes Vaccine Passports.”
In Nazi Germany, the obsession with purity — both in terms of hygiene and race theory — drove the genocide of Jews, the old, the handicapped and the mentally challenged.
In present day, the public narrative has eerily followed Nazi Germany’s playbook for genocide, starting with the scapegoating of healthy people, as the rapid spread of COVID-19 was blamed on asymptomatic individuals not properly masking, social distancing and self-isolating.
That then grew into the nurturing of prejudice against people who refuse to wear masks, and now we’re seeing the narrative building toward persecution of those who do not want to get the vaccine. It will start with discrimination, and already, we’re hearing talk of how only vaccinated people ought to have the right to partake in certain social activities. If that is tolerated, then outright persecution will be the inevitable next step.
This is why I reject and counter commentaries such as that by Dovere. These half-baked, one-sided, persecutory arguments must be challenged at every turn, because they only lead us one way. And unless you’re part of the technocratic elite, you — regardless of how you feel about vaccination right now — do not want to end up there.
Sources and References
- 1, 2, 10 The Atlantic April 10, 2021
- 3 The Defender April 9, 2021
- 4 CDC, Selected Adverse Events Reported after COVID-19 Vaccination April 13, 2021
- 5 The Defender April 15, 2021
- 6 Epoch Times April 11, 2021
- 7 Reuters April 10, 2021
- 8 Washington Examiner April 11, 2021
- 9 Medical Xpress April 11, 2021
- 11 Twitter Ruth Graham April 8, 2021
- 12 Townhall April 13, 2021
- 13 Preprints.org 2020: 2020100330 DOI: 10.20944/preprints202010.0330.v2
- 14 The Journal of Clinical Endocrinology & Metabolism October 27, 2020; dgaa733 [Epub ahead of print], Results
- 15 Nutrients October 31, 2020;12, 3361; doi:10.3390/nu12113361
- 16, 18, 19, 20 CNN March 5, 2021
- 17 APA.org Undesired Weight Change Since Start of Pandemic
- 21 Real Clear Politics March 29, 2021
- 22 The Epoch Times March 29, 2021
The Capture of Goodness

By Sinead Murphy | OffGuardian | April 25, 2021
‘Goodness’ is not the word I wanted to use in this article. But ‘ethics’ sounded too abstract, ‘morality’ too rule-bound, ‘virtue’ too archaic, and ‘kindness’ too corporate (at least since ‘random acts of kindness’).
The ubiquity of that dreaded term ‘safety,’ brayed at us from every angle, has made all the old names for concern for each other’s welfare seem ill-fitting and out of date. ‘Goodness,’ for all its faults, will have to do.
*
On Tuesday 30th March, leaders of 23 countries, including the UK, France and Germany, issued a statement on the matter of ‘pandemic preparedness.’
Its key phrase was reprinted across the media: Nobody is safe until everyone is safe.
As we embark on our second Covid year, the sentiment is chilling.
Nobody is safe until everyone is safe is the latest phase in the capture of human goodness that has been the most profound effect of Covid.
At first, we were asked to keep our distance. Other people, for whose sake we do most of the good things we do, were put beyond our reach.
We no longer held the door for the next person to pass through. We no longer offered to carry an old lady’s shopping. We stopped shaking one another’s hand and patting each other on the back. We no longer hugged.
Almost all of the ways in which we knew how to be good to each other were paused; the bonds of mutual support were severed.
Then, for the first time uncertain about how to do good – then, we were asked to mask up. Not for our own sake. For the sake of the other person – I mask for you, you mask for me. Being good to other people was returned to us. But it was not quite like it had been before.
Other people, still at a distance, were now also without faces, and faces are so important in arousing our pity, commanding our assistance, eliciting our smile. Goodness had been readmitted, but for the sake of newly anonymous beings.
Then, still at a distance, still masked up, we were encouraged to take the jab. Not for our own sake – at least, not directly. For the sake of the herd. For herd immunity.
This concept, so energetically rejected as cruel during the first months of Covid, was returned to us. But it was not quite like it had been before. It was cleansed of its natural components, redefined by the World Health Organisation as an achievement of vaccination, its taint of ‘let it rip’ buried under a great enthusiasm for pharmaceutical engineering. Herd immunity was back. And goodness was redirected towards an anonymous crowd.
And now we are told that nobody is safe until everyone is safe. Now we are to be good, not even to a masked and distanced other, not even to an anonymous herd, but to everyone.
Everyone? All seven billion inhabitants of the earth? It is worse than that. The statement issued by world leaders on 30th March champions a concept of ‘One Health,’ which is described as encompassing ‘humans, animals and our planet.’
How in the world is any of us to act for the good of this everyone? The idea is sublime. It may strike us with awe, even admiration, but there is nothing we can do for its sake. Our good deeds, already scrambled by distancing and masking and herding, are now, at last, out of play.
One year ago, we were tempted from the well-trodden paths of goodness onto a seemingly higher road, emblazoned with slogans of sacrifice, decorated with rainbows and resounding with the clapping of people pulling together. But the road leads nowhere. It is a dead end.
In January, in the northern snow, I was saying hello to my neighbour over the low garden wall. So that she could find her key, she placed her little girl, ten months old and all wrapped up in her snowsuit, onto the soft ground. While my neighbour was searching in her bag, her baby slowly keeled over. Without thinking, I stepped across and leaned down to lift her. But it was the wrong thing to do. Her mother snatched her up and I retreated in vague apology.
What is now the right thing to do when a small baby falls sideways onto the snow? The answer: nothing. Goodness is cancelled. Or, rather, it is redirected through an idea so sublime that nothing follows from it for mere humans with their merely human faculties. Everyone means nothing to us. For the sake of everyone, we can do nothing.
But there is a problem about doing nothing. Because it may just be that human beings are only good insofar as they do good things. Goodness requires practice and wastes away from lack of practice. It is more like playing the piano than riding a bike; you have to keep it up or you can no longer really do it. How long before our good natures grow rusty and flake away? How long before we no longer know how to be good?
Which is why, I presume, we now have these badges of goodness: masks, certificates.
Our enthusiasm for both may have little to do with their dubious efficacy in stopping the spread of a respiratory virus, and much to do with our need for reassurance that, even though we no longer do good things, we still really are good people.
Sinead Murphy teaches Philosophy at Newcastle University. Her most recent publication is Zombie University: Thinking Under Control (Repeater, 2017).
Did Bill Gates Reveal the Reason Behind the Lock-Downs?
By Rosemary Frei | OffGuardian | April 4, 2020
In a candid interview, Bill Gates has outlined that, despite the comparatively small threat of Coronavirus, he and his colleagues “don’t want a lot of recovered people” who have acquired natural immunity. They instead are hoping we become reliant on vaccines and anti-viral medication.
Shockingly, Gates also suggests people be made to have a digital ID showing their vaccination status, and that people without this “digital immunity proof” would not be allowed to travel. Such an approach would mean very big money for vaccine producers.
On March 24, 2020 Bill Gates gave a highly revelatory 50-minute interview (above) to Chris Anderson. Anderson is the Curator of TED, the non-profit that runs the TED Talks.
The Gates interview is the second in a new series of daily ‘Ted Connects’ interviews focused on COVID-19. The series’s website says that:
TED Connects: Community and Hope is a free, live, daily conversation series featuring experts whose ideas can help us reflect and work through this uncertain time with a sense of responsibility, compassion and wisdom.”
Anderson asked Gates at 3:49 in the video of the interview – which is quickly climbing to three million views – about a ‘Perspective’ article by Gates that was published February 28 in the New England Journal of Medicine.
“You wrote that this could be the once-in-a-century pandemic that people have been fearing. Is that how you think of it, still?” queried Anderson.
“Well, it’s awful to say this but, we could have a respiratory virus whose case fatality rate was even higher. If this was something like smallpox, that kills 30 percent of people. So this is horrific,” responded Gates.
“But, in fact, most people even who get the COVID disease are able to survive. So in that, it’s quite infectious – way more infectious than MERS [Middle East Respiratory Syndrome] or SARS [Severe Acute Respiratory Syndrome] were. [But] it’s not as fatal as they were. And yet the disruption we’re seeing in order to knock it down is really completely unprecedented.”
Gates reiterates the dire consequences for the global economy later in the interview.
“We need a clear message about that,” Gates said starting at 26:52.
“It is really tragic that the economic effects of this are very dramatic. I mean, nothing like this has ever happened to the economy in our lifetimes. But … bringing the economy back and doing [sic] money, that’s more of a reversible thing than bringing people back to life. So we’re going to take the pain in the economic dimension, huge pain, in order to minimize the pain in disease and death dimension.”
However, this goes directly against the imperative to balance the benefits and costs of the screening, testing and treatment measures for each ailment – as successfully promulgated for years by, for example, the Choosing Wisely campaign – to provide the maximum benefit to individual patients and society as a whole.
Even more importantly, as noted in an April 1, 2020 article in OffGuardian, there may be dramatically more deaths from the economic breakdown than from COVID-19 itself.
“By all accounts, the impact of the response will be great, far-reaching, and long-lasting,”
Kevin Ryan wrote in the article. Ryan estimated that well over two million people will likely die from the sequelae of the lock-downs and other drastic measures to enforce ‘social distancing.’
Millions could potentially die from suicide, drug abuse, lack of medical coverage or treatment, poverty and lack of food access, on top of other predictable social, medical and public-health problems stemming from the response to COVID-19.
Gates and Anderson did not touch on any of those sequelae. Instead, they focused on rapidly ramping up testing and medical interventions for COVID-19.
Gates said at 30:29 in the interview that he and a large team are moving fast to test anti-virals, vaccines and other therapeutics and to bring them to market as quickly as possible.
The Gates Foundation and Wellcome Trust with support from Mastercard and now others, created this therapeutic accelerator to really triage out [candidate therapeutics]…You have hundreds of people showing up and saying, ‘Try this, try that.’ So we look at lab assays, animal models, and so we understand which things should be prioritized for these very quick human trials that need to be done all over the world.”
The accelerator was launched March 10 with approximately $125 million in seed funding. Three days later Gates left Microsoft.
Not long before that, on January 23, Gates’s organization the Coalition for Epidemic Preparedness Innovations (CEPI) announced it will fund three programs to develop COVID-19 vaccines. These are the advancing of DNA-vaccine candidates against MERS and Lassa fever, the development of a “‘molecular clamp’ platform” that “enables targeted and rapid vaccine production against multiple viral pathogens,” and the manufacture and Phase 1 clinical study of an mRNA vaccine against COVID.
“The programmes will leverage rapid response platforms already supported by CEPI as well as a new partnership. The aim is to advance nCoV-2019 vaccine candidates into clinical testing as quickly as possible,” according to a news release.
Then at 32:50 in the video, Anderson asked whether the blood serum from people who have recovered from a COVID infection can be used to treat others.
“I heard you mention that one possibility might be treatments from the serum, the blood serum of people who had had the disease and then recovered. So I guess they’re carrying antibodies,” said Anderson. “Talk a bit about that and how that could work and what it would take to accelerate that.”
[Note that Anderson did not ask Gates about, instead, just letting most of the population – aside from people most vulnerable to serious illness from the infection, who should be quarantined — be exposed to COVID-19 and as a result very likely recover and develop life-long immunity. As at least one expert has observed, “as much as ninety-nine percent of active cases [of COVID-19] in the general population are ‘mild’ and do not require specific medical treatment” to recover.]
“This has always been discussed as, ‘How could you pull that off?’” replied Gates. “So people who are recovered, it appears, have very effective antibodies in their blood. So you could go, transfuse them and only take out white cells, the immune cells.”
However, Gates continued, he and his colleagues have dismissed that possibility because it’s “fairly complicated – compared to a drug we can make in high volume, you know, the cost of taking it out and putting it back in probably doesn’t scale as well.”
Then a few seconds later, at 33:45, Gates drops another bomb:
We don’t want to have a lot of recovered people […] To be clear, we’re trying – through the shut-down in the United States – to not get to one percent of the population infected. We’re well below that today, but with exponentiation, you could get past that three million [people or approximately one percent of the U.S. population being infected with COVID-19 and the vast majority recovering]. I believe we will be able to avoid that with having this economic pain.”
It appears that rather than let the population be exposed to the virus and most develop antibodies that give them natural, long-lasting immunity to COVID-19, Gates and his colleagues far prefer to create a vast, hugely expensive, new system of manufacturing and selling billions of test kits, and in parallel very quickly developing and selling billions of antivirals and vaccines.
And then, when the virus comes back again a few months later and most of the population is unexposed and therefore vulnerable, selling billions more test kits and medical interventions.
Right after that, at 34:14, Gates talked about how he sees things rolling out from there.
Eventually what we’ll have to have is certificates of who’s a recovered person, who’s a vaccinated person […] Because you don’t want people moving around the world where you’ll have some countries that won’t have it under control, sadly. You don’t want to completely block off the ability for people to go there and come back and move around. So eventually there will be this digital immunity proof that will help facilitate the global reopening up.”
[Sometime on the afternoon of March 31 the last sentence of this quote was edited out of the official TED video of the interview. Fortunately, recordings of the complete interview are archived elsewhere.]
In the October 2019 Event 201 novel-corona virus-pandemic simulation co-sponsored by the Bill & Melinda Gates Foundation, the World Economic Forum and a division of the Johns Hopkins Bloomberg School of Public Health, a poll that was part of the simulation said that 65% of people in the U.S. would be eager to take a vaccine for COVID-19, “even if it’s experimental.”
This will be tremendously lucrative.
Vaccines are very big business: this Feb. 23 CNBC article, for example, describes the vaccine market as six times bigger than it was 20 years ago, at more than $35 billion annually today, and providing a $44 return for every $1 invested in the world’s 94 lowest-income countries.
Notably, the Bill & Melinda Gates Foundation – which has an endowment of $52 billion – has given more than $2.4 billion to the World Health Organization (WHO) since 2000, according to a 2017 Politico article. (While over the same time frame countries have reduced their contributions to the world body, particularly after the 2008-2009 depression, and now account for less than one-quarter of the WHO’s budget.) The WHO is now coordinating approximately 50 groups around the world that are working on candidate vaccines against COVID-19.
The Politico article quotes a Geneva-based NGO representative as saying Gates is “treated liked a head of state, not only at the WHO, but also at the G20,” and that Gates is one of the most influential people in global health.
Meanwhile, officials around the world are doing their part to make sure everyone social distances, self-isolates and/or stays locked down.
For example, here’s Toronto’s Medical Officer of Health, Dr. Eileen de Villa, at her and Toronto Mayor John Tory’s March 30 press briefing:
“We find ourselves in the midst of a global pandemic. We should expect some more people will get sick – and for some, sadly, will die. This is why it is so important to stay at home to reduce virus spread. And to protect front-line workers, healthcare workers and our essential workers, so they can continue to protect us. People shouldn’t have to die, people shouldn’t have to risk death taking care of us because others won’t practice social distancing or physical distancing.”
Yet look how close Ontario’s Chief Medical Officer of Health, Dr. David Williams, is sitting to Haley Chazan, Senior Manager, Media Relations, for Christine Elliott, Deputy Premier and Minister of Health of Ontario.
This was on Friday, March 27, just before the start of that day’s daily press conference by Dr. Williams and Ontario’s Associate Medical Officer of Health Dr. Barbara Yaffe:

They were sitting two seats, or just a couple of feet, apart. A short time later Chazan got up and stood even closer to Dr. Williams for a little while:

Dr. Williams and Chazan do not live together. Rather, Dr. Williams very likely knows – just as Gates knows – that there is little if any reason to worry about being in close contact with other people unless you or they are vulnerable to developing a severe illness from COVID-19. He surely knows, also, that if you contract COVID-19 and you’re otherwise healthy you’ll very likely have few symptoms, if any, and recover quickly. And that this exposure in fact is beneficial because in the process you will develop antibodies to the virus and have natural, long-lasting immunity to it.
Yet in the March 27 press conference, just like all the others he has participated in during the COVID-19 crisis, Dr. Williams lectured the public about maintaining social distancing. He told people not to go outside on the coming weekend to enjoy the nice weather because, otherwise, they might walk past someone and not be two metres apart.
Dr. Williams is among the large cadre of powerful officials who’ve crashed the global economy by forcing tens of millions of small- and medium-sized businesses to close in the name of the need for forced, severe, social distancing and lock-downs.
They’ve shattered society, suspended most civil liberties and prohibited most activities and connections that keep people mentally and physically healthy. At the same time the officials have prioritized COVID-19 care over everything else and, as a result, severely limited billions of people’s access to life-saving healthcare services ranging from acquiring medication and blood transfusions to having organ transplants and cancer surgeries.
Rosemary Frei has an MSc in molecular biology from a faculty of medicine and was a freelance medical journalist for 22 years. She is now an independent investigative journalist in Canada. You can find her recent detailed investigative analysis of COVID here.
NIH plays legal games while US citizens die
By Peter Yim | Trial Site News | April 24, 2021
On January 14, 2021, the NIH updated its recommendation on the use of ivermectin in COVID-19. It removed its recommendation against the use of ivermectin in COVID-19. However it stated:
“There are insufficient data for the COVID-19 Treatment Guidelines Panel (the Panel) to recommend either for or against the use of ivermectin for the treatment of COVID-19.”
The “Panel” consists of 47 medical experts and patient advocates. Presumably, recommendations in the Guidelines are endorsed by a vote of the Panel. However, there is ambiguity about voting since the Guidelines state:
“Updates to existing sections that do not affect the rated recommendations are approved by Panel co-chairs without a Panel vote.”
I submitted a Freedom of Information Act (FOIA) request to the NIH on January 25 to find out if there was a vote:
“On January 6, 2021, the NIH COVID-19 Treatment Guidelines Panel met to consider updating their recommendation on the use of Ivermectin in COVID-19. Please answer the following question. As of today, has that Panel taken a vote on whether to change its recommendation? (Date Range for Record Search: From 01/06/2021 To 01/25/2021)”
The NIH responded:
“Please be advised that the FOIA is not intended to answer questions, but rather it is meant for the public to request specifically identified and searchable Federal records that are already in existence, i.e. a record cannot be created in response to a FOIA request. Considering this, your request is not deemed a proper FOIA request as it is in the form of a question, and your NIH FOIA case has been administratively closed.”
I rephrased and resubmitted the FOIA request on January 28:
“All updates to the Coronavirus Disease 2019 (COVID-19) Treatment Guidelines that were endorsed by a vote of the Panel. (Date Range for Record Search: From 01/01/2021 To 01/28/2021)”
There was only one update to the Guidelines in that time period and that update was for the ivermectin recommendation. Therefore, if there was a vote on the ivermectin recommendation, the NIH should provide that update. If there was not a vote, the NIH should state that no record is available.
The NIH did not respond to this request within 20 business days as required by law. I have challenged that non-response by the NIH in federal court. The NIH did just provide this response:
“You requested all updates to the Coronavirus Disease 2019 (COVID-19) Treatment Guidelines that were endorsed by a vote of the Panel (Date range for record search from 01/01/2021 to 01/28/2021). All approved updates to the guidelines are posted online and can be found at https://www.covid19treatmentguidelines.nih.gov/whats-new/. The documents posted on this website respond to your request in full.”
Whether that is a legally adequate response to the FOIA request remains to be seen in the federal court proceeding. What is obvious is that the NIH is playing legal games while US citizens suffer and die from COVID-19.
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Who Runs Our World?

Netanyahu addresses US Congress
By Richard Hugus | January 4, 2019
Our world is run by oligarchs, the holders of vast wealth from monopolies in banking, resource extraction, manufacturing, and technology. Oligarchs have such power that most of the world doesn’t even know of their influence over our lives. Their overall agenda is global power — a world government, run by them — to be achieved through planned steps of social engineering. The oligarchs remain in the background and have heads of state and entire governments acting in their service. Presidents and prime ministers are their puppets. Bureaucrats and politicians are their factotums.
Who are politicians? Politicians are people who work for the powerful while pretending to represent the people who voted for them. This double-dealing involves a lot of lying, so successful politicians must be good at it. It’s not an easy job to make the insane agenda of the powerful seem reasonable. Politicians can’t reveal this agenda because it almost always goes against the interests of their constituents, so they become adept at sophistry, mystification, and the appearance of authority. For example, wars for Israel have been part of the agenda of the powerful for years. Since 2001, wars for Israel have been sold as “the war on terror” and lots of lies had to be made up as to why the war on terror was a real thing. The visible faces promoting the war on terror were neoconservatives in the US, almost all of whom were advocates for Israel, or Zionists. Zionists are not the only members of the oligarchy, but they seem to be its lead actors. ... continue
Blog Roll
 Aletho News
Aletho News- Israeli telecom networks used for mass surveillance across countries
- US claim of sinking Iranian boats ‘a lie’, senior military official tells IRIB
- New KC-46 Supertankers Promise Israel Conventional Samson Option Strike Сapability
- No, New York Times, We Don’t Need to Dam the Bering Strait
- Gates-Funded ‘Big Catch-Up’ Delivers 100 Million Vaccine Doses — Including High-Risk DTP Vaccine Not Used in U.S.
- No commercial ship or oil tanker transited Strait of Hormuz in past hours: IRGC
- Russia warns of escalating NATO military activity in Baltic region
- Government Kills the Spirit
- How ‘Israel’s’ Iran regime change plot failed – again
- 1977 Influenza Pandemic Sequence Shows Signs of Laboratory Creation: Journal ‘Cell’
- If Americans Knew
- As in Gaza, Israel is targeting rescue workers in South Lebanon, killing more than 100 since March
- Israel’s Obliteration Ecocide from Gaza to Lebanon and Beyond
- Israel Said It’s Applying the Gaza Model in Lebanon. This Is What the Devastation Looks Like.
- New Member of Trump’s Iran Negotiating Team Comes From Notoriously Pro-Israel Think Tank
- Israeli army demolishes Christian monastery, nuns’ school in southern Lebanon
- Tokenizing Christians In Israel
- One Gaza is not enough: Israel is turning southern Lebanon into another Gaza – Daily Update
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- No Tricks Zone
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
