Twenty Five Years Of Settled Science
By Tony Heller | Real Climate Science | March 17, 2021
“There is something fascinating about science. One gets such wholesale returns of conjecture out of such a trifling investment of fact.”
― Mark Twain
Twenty five years ago, experts blamed a huge snowstorm in New York on global warming.

TimesMachine: January 14, 1996 – NYTimes.com
In 2000, experts said snow was a thing of the past.
“According to Dr David Viner, a senior research scientist at the climatic research unit (CRU) of the University of East Anglia, within a few years winter snowfall will become “a very rare and exciting event”. “Children just aren’t going to know what snow is,” he said.”
Snowfalls are now just a thing of the past – Environment – The Independent
In 2003 experts said skiing was doomed because global warming was going to make it too hot to snow.

Reading Eagle – Google News Archive Search

On the rocks: the grim forecast for winter sports as global warming increases | World news | The Guardian
This story was repeated in 2012. Skiing was doomed because of global warming.
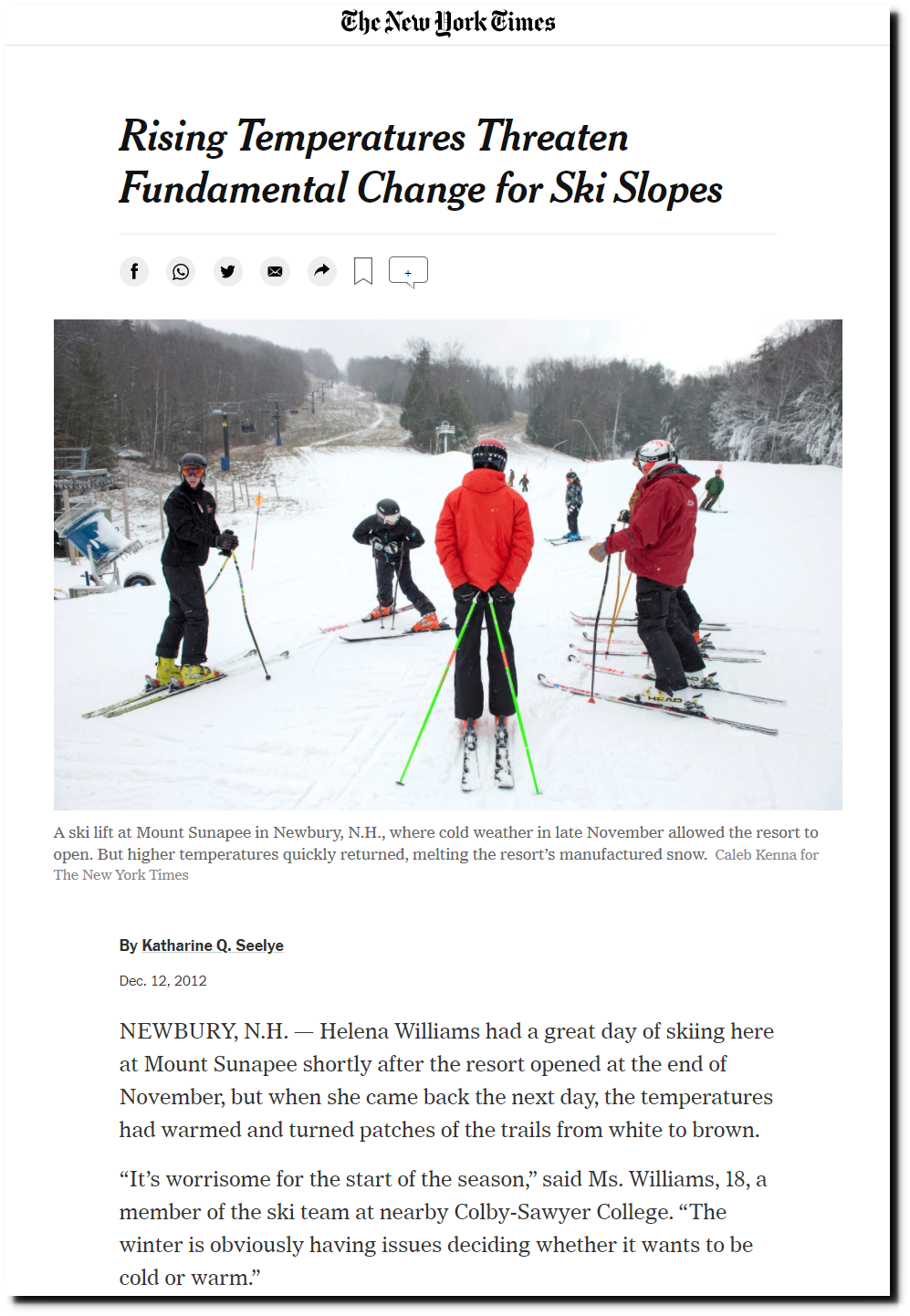
Climate Change Threatens Ski Industry’s Livelihood – The New York Times
And now experts say record cold and snow is caused by global warming, and they predicted it all along.

Record Northeast snow totals could be connected to climate change – The Washington Post
But the reality is that September-March snowfall has been increasing for 50 years, and climate academics and journalists are science fiction writers with no connection to reality.
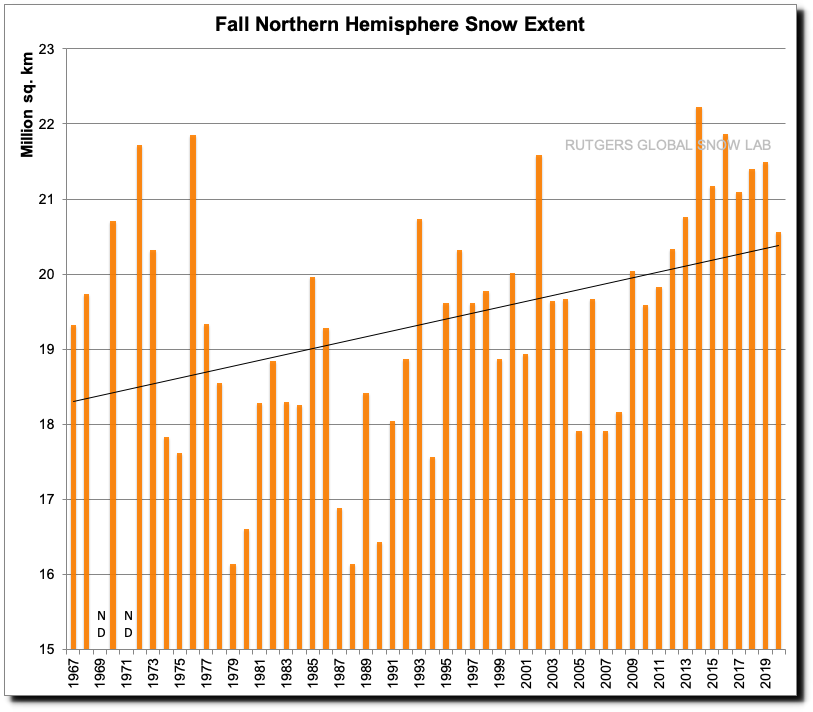

Rutgers University Climate Lab :: Global Snow Lab
This is what I saw when I stepped outside this morning.

The Disease Models Were Tested and Failed, Massively
By Phillip W. Magness | AIER | March 19, 2021
One year ago this week the world embraced a lockdown strategy premised on the epidemiology modeling of Imperial College-London (ICL). In a March 16, 2020 report by physicist and computer modeler Neil Ferguson, the ICL team predicted catastrophic death tolls in the United Kingdom and United States unless both countries adopted an aggressive policy response of mandating social distancing, school and business closures, and ultimately sheltering in place.
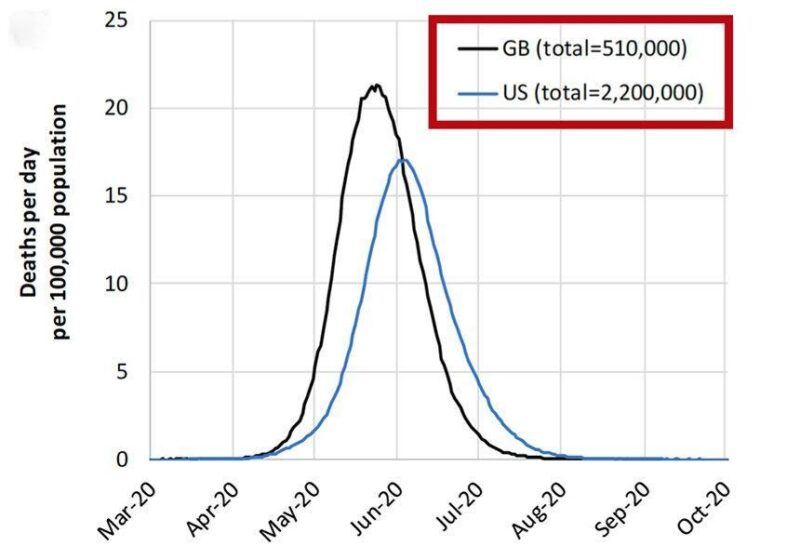
Ferguson’s model presented a range of scenarios under increasingly restrictive nonpharmaceutical interventions (NPIs). Under its “worst case” or “do nothing” model 2.2 million Americans would die, as would 510,000 people in Great Britain, with the peak daily death rate hitting somewhere around late May or June. At the same time, the ICL team promised salvation from the coronavirus if only governments would listen to and adopt its technocratic recommendations. Time was of the essence to act, so President Donald Trump and UK Prime Minister Boris Johnson both listened. And so began the first year of “two weeks to flatten the curve.”
It took a little over a month before we saw conclusive evidence that something was greatly amiss with the ICL model’s underlying assumptions. A team of researchers from Uppsala University in Sweden adapted Ferguson’s work to their country and ran the projections, getting similarly catastrophic results. Over 90,000 people would die by summer from Covid-19 if Sweden did not enter immediate lockdown. Sweden never locked down though. By May it was clear that the Uppsala adaptation of ICL’s model was off by an order of magnitude. A year later, Sweden has fared no worse than the average European lockdown country, and significantly better than the UK, which acted on Ferguson’s advice.
Pressed on this unexpected result, ICL tried to distance itself from the Swedish adaptation of its model in May. The records from the March 21st supercomputer run of the Uppsala team’s projections belie that assertion, linking directly to Ferguson’s March 16th report as the framework for its modeling design. But no matter – the ICL team’s own publications would soon succumb to a real-time testing against actual data.
A second ICL report, attempting to model the reopening of the United States from lockdowns, wildly exaggerated the death tolls that were expected to follow. By July, this model too had failed to even minimally correspond to observed reality. ICL attempted to save face by publishing an absurd exercise in circular reasoning in the journal Nature where they invoked the unrealized projections of their own model to supposedly “prove” multiple millions of lives had been saved by the lockdowns. That study soon failed basic robustness checks when the ICL team’s suite of models were applied to different geographies.
Another team of Swedish researchers then noticed oddities in the ICL team’s coding, suggesting they had modified a key line to bring data from their own comparative analysis of Sweden into sync with other European countries under lockdown after the models did not align. A published derivative of this discovery showed that ICL’s own attempts to validate the effectiveness of its lockdown strategies does not withstand empirical scrutiny.
Finally, in November, another team of researchers from the United States compared a related ICL team model for a broader swath of countries against five other international models of the pandemic, examining the performance of each against observed deaths. Their results contain a stunning indictment: “The Imperial model had larger errors, about 5-fold higher than other models by six weeks. This appears to be largely driven by the aforementioned tendency to overestimate mortality.”
The verdict is in. Imperial College’s Covid-19 modeling has an abysmal track record – a characteristic it unfortunately shares with Ferguson’s prior attempts to model mad cow disease, swine flu, avian flu, and countless other pathogens.
After a year of model-driven lockdowns, we may also look back to the original March 16, 2020 report to see yet another failure of its predictive ability. Recall that this is the model that fueled the alarmist rush to shut everything down last March, all to avert a 2.2 million death toll that would presumably peak around June.
(Source: Imperial College Report #9, March 16, 2020)
As noted above, the 2.2 million figure for the US (and corresponding 510,000 figure in Britain) were “worst case” scenarios in which the pandemic ran its course. According to the underlying theory of the ICL model, these catastrophic totals could be reduced by the adoption of NPIs – the escalating suite of social distancing measures, business and school closures, and ultimately full lockdowns that we observed in practice over the last year.
Aside from its 2.2 million worst case scenario, ICL offered no specific projections for how its proposed mitigation measures would work in the United States. Ferguson did however tell the New York Times on March 20, 2020 that a “best case” American scenario would still yield “about 1.1 million deaths,” giving us a glimpse of what he believed to be possible under NPI mitigation. The March 16th report similarly “predict[ed] there would still be in the order of…1.1-1.2 million in the US” under the most optimistic mitigation strategy, barring a large increase in hospital ICU bed capacity.
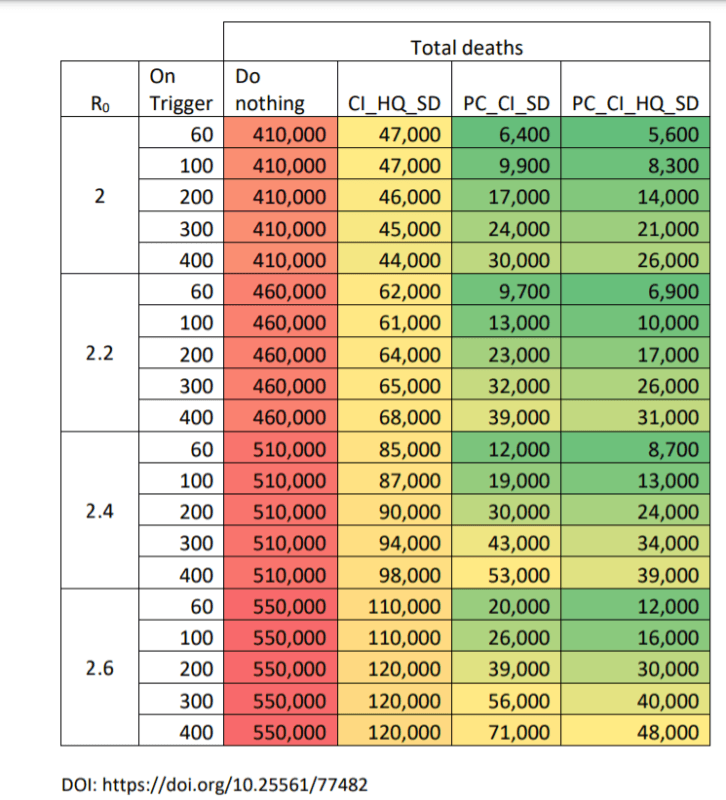
By contrast, ICL did publish an extensive table showing the results of its model run for Britain over a group of four increasingly stringent NPI scenarios. These range from the “worst case” projection with half a million deaths (the figures vary depending on assumptions about the virus’s reproduction rate) to a more stringent model where four NPIs (public school closures, case isolation, home quarantine, and social distancing) are simultaneously enacted. The results are depicted below.
(Source: Imperial College Report #9, March 16, 2020)
Note that the UK enacted policies based on all four measures recommended by the March 16th report, as well as an even more stringently enforced general lockdown on three separate occasions. After one year of following and expanding upon the Imperial College strategy, an unusual result appears in the data: not only have the UK’s numbers come up far short of Ferguson’s most alarmist scenario (depicted in the first column), but the UK has actually done much worse than the other NPI mitigation models in the ICL report.
As of the 1-year anniversary, the UK had a little over 125,000 confirmed Covid-19 deaths. By implication, the UK death toll has exceeded the mildest of the other three NPI scenarios from the ICL model (column 2) and blown past its heavier NPI recommendations (columns 3 and 4), even while operating under a more stringent set of lockdowns than ICL originally contemplated.
The implications are clear. While Ferguson wildly exaggerated the “worst case” scenario for the UK, he also severely overestimated the effectiveness of NPIs at controlling the pandemic.
By building its policy response around the Imperial College model, the UK government delivered the worst of both worlds. It imposed some of the most severe and long-lasting lockdowns in the world based on the premise that NPIs would work as Ferguson’s team predicted, and that such actions were needed to avert a catastrophe. Except the lockdowns did not work as intended, and the UK also ended up with an abnormally high death count compared to other countries – including locales that did not lock down, or that reopened earlier and for longer periods than the UK.
Why were the Ferguson/ICL predictions so far off base on both ends? The answer likely derives from two central flaws in their model design.
First, Ferguson adapted the model directly from a 2006 influenza pandemic model that he published in the journal Nature. As with the March 16th Covid report, this study aimed to predict the spread of a virus across the general population, subject to a suite of increasingly stringent NPI countermeasures. As the second-to-last paragraph of the study reveals though, it only modeled general population spread. In doing so, the authors acknowledged that “Lack of data prevent us from reliably modelling transmission in the important contexts of residential institutions (for example, care homes, prisons) and health care settings.”
With Covid-19 however, nursing homes have emerged as one of the greatest vulnerabilities in the pandemic. In many locales, nursing home deaths alone account for almost half of all Covid-19 fatalities despite housing only a tiny fraction of the population. While the latest nursing home figures for the UK are as of yet hard to come by, reports from last year suggest they are not only a large share of the country’s Covid-19 deaths but also severely undercounted in official records. Using a preliminary count from last year, the UK had one of the worst nursing home shielding ratios in Europe – a measure that compares a country’s death toll in its care facilities to the general population. The ICL projections likely missed this problem entirely due to a defect in the 2006 model it was built upon.
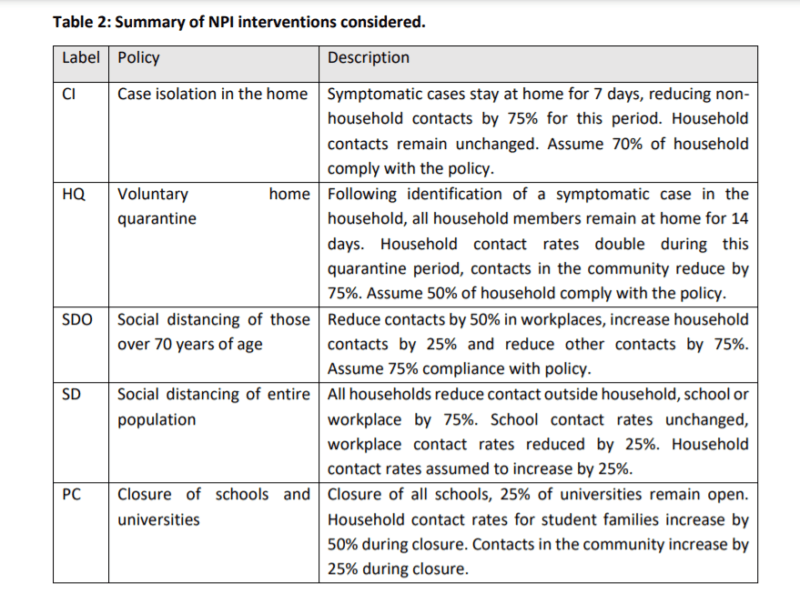
Second, Ferguson’s model severely overstated the effectiveness of NPIs at mitigating general population spread. Part of the appeal of the ICL report from last March came from its succinct portrayal of the available policy options and their claimed effects. The modelers presented political leaders with a menu of escalating measures to adopt with mathematical precision, each linked to an associated projection of its effectiveness at staving off the pandemic. All the politicians had to do was select from the menu and implement the prescribed course.
Except it wasn’t that simple in practice. ICL’s recommended NPI measures baked assumptions about their own effectiveness into the model. In reality, most of these assumptions had never been tested or even minimally quantified. As a key chart from the March 16th report illustrates, the supposed effect of each NPI was little more than a guesstimate – a set of nice, round numbers that purported to show the change in social interactions after its adoption.
A 2019 report by the World Health Organization (WHO) warned of the flimsy empirical basis for epidemiology models such as the one developed by ICL. “Simulation models provide a weak level of evidence,” the report noted, and lacked randomized controlled trials to test their assumptions. The same report designated mass quarantine measures – what we now know of as lockdowns – as “Not Recommended” due to lack of evidence for their effectiveness. Summarizing this literature, which included the same 2006 influenza model that Ferguson adapted to Covid-19, the WHO concluded: “Most of the currently available evidence on the effectiveness of quarantine on influenza control was drawn from simulation studies, which have a low strength of evidence.”
The UK’s experience under the ICL model therefore demonstrates not only Ferguson’s propensity toward wildly alarmist disease forecasting – it also illustrates the abject failure of lockdowns and related NPI measures to mitigate the pandemic. As a revealing point of comparison, the UK’s population-adjusted daily death toll under lockdowns has been consistently higher than no-lockdown Sweden for most of the pandemic, despite both countries following a nearly identical pattern of timing in both the first and second waves.
The relevant question, then, is not whether the UK failed to lock down stringently enough, but whether lockdowns offer any meaningful benefit whatsoever in mitigating the pandemic. A growing body of empirical data strongly suggests they do not.
The repeated failures of the Ferguson/ICL model point to a scientific error at the heart of the theory behind lockdowns and similar NPIs. They assume, without evidence, that their prescriptive approach is correct, and that it may be implemented by sheer will as one might achieve by clicking a check-box in a Sim City-style video game. After a year of real-time testing, it is now abundantly clear that this video game approach to pandemic management ranks among the most catastrophic public health policy failures in the last century.
Phil Magness is a Senior Research Fellow at the American Institute for Economic Research. He is the author of numerous works on economic history, taxation, economic inequality, the history of slavery, and education policy in the United States.
Hancock Is Terrified That Under-50’s Will Refuse Covid Vaccine
By Richie Allen | March 18, 2021
It’s a bit of a mystery. Speaking from Downing Street last night, UK Health Secretary Matt Hancock said that the under-50’s would have to wait a bit longer for their covid vaccine. He blamed production issues. The manufacturers said there are no issues. What’s going on?
A leaked letter suggested that the NHS is expecting a significant reduction in supply for a month from March 29. The letter said that local vaccination centres have been told not to make any new bookings from the end of this month.
This means that the under-50’s will have to wait until at least May, to get their first dose. Hancock said the country was still “on track” to hit vaccination targets to take England out of lockdown.
A fall in provision from AstraZeneca is being blamed for the shortage. Last night, the firm moved quickly to refute the claim. The company insisted that its UK supply chain was not experiencing disruption.
A spokesman said: “Our UK domestic supply chain is not experiencing any disruption and there is no impact on our delivery schedule.” Someone is lying.
I bet the government is anticipating widespread refusal among the under-50’s. I’ve been speculating for some time now, that the roll-out hasn’t been as successful as the government would have us believe.
I believe that they were largely successful in persuading OAP’s to have a jab, but began running into problems as they moved down the age groups.
Younger people are far more likely to refuse the vaccine or choose to wait and see if it causes harm. And it is causing harm. Unless you’ve been on Planet Mars for the last fortnight, you’ll have heard of the blood clotting.
The majority of under-50’s have Facebook, Twitter and Instagram accounts. They’ll be aware of reports that the vaccines are killing people, although it’s not known on what scale. But it’s happening.
And they’ll also be aware that 200,000 NHS workers have indicated that they will decline the jab. That was covered by mainstream media. Taking all this into account, my guess is that Matt Hancock is lying when he says that “supply is bumpy.”
He’s terrified that us under-50’s won’t be rolling up our sleeves. And why would we? Why would we need an experimental drug for an illness that most of us have never had, or may have had and didn’t even know about it?
I believe the government has bought itself a month, to try and figure out what to do. If it opens the door to booking under-50’s for their jabs and there is widespread refusal as I’ve suggested, the media will cover it, even if reluctantly.
Expect the dangling of more carrots in the weeks to come. We’ll hear a lot of talk about holidays and outdoor music festivals tied in with green passports or whatever name they give them. That’s their ace card.
At some stage though, they’ll have to go for it and open the doors to the young. What happens next will be fascinating.
Some Observations On the Efficacy of Masks in a #COVID19 World
By Kevin Kilty | Watts Up With That? | March 16, 2021
Some weeks ago, Pat Frank suggested that I might consider writing an essay about the efficacy of masks and mandates to wear masks during this pandemic. I hesitated doing so at first, but March 8th I noticed another research effort on the part of the CDC to justify masks as a prophylactic strategy.[1] This effort seems very deficient in my view and so this essay resulted. What I write here is a summary of a much larger work in progress.
Lincoln Moses and Frederick Mostellar long ago suggested that public policy be organized as experiments so that we might learn of its effectiveness, or lack thereof, and avoid successive failures.[2] When the COVID-19 pandemic arrived last spring, I wrote that we didn’t need to go through successive battles with exponential processes, but that we appeared not ready to gather useful data and evidence about the effectiveness of social distancing and other advice in this battle.[3] Considering the tendency of people to don a mask against all sorts of bad air is so universal that even screen writers employ it to add realism to a disaster scene, one would think we would know something about their effectiveness.[4] We do and we don’t. While I am told by some people employed in medicine along with many amateurs that masks are essential to controlling spread of SARS-COV-2; highly reputable authorities, many of them, thousands of them, make much more modest and even opposite claims.[5]
How might we analyze these competing claims? I see three avenues of attack: First, we can examine theoretical reasons for and against masks from a mechanical perspective. Second, there are limited experiments known as randomized clinical trials available, all of which have some deficiencies and limited pertinence. Third, we can examine observations of the progress of this epidemic as shown by cases in the light of local mandates. These observations and the methods used to evaluate them are quite deficient in many ways, but they do tend toward similar conclusions.
Mechanical Considerations
The CDC, WHO, and local departments of health have issued a variety of advisories about masks which they update periodically. A typical advisory begins as follows:
“Because the virus is transmitted predominantly by inhaling respiratory droplets from infected persons, universal mask use can help reduce transmission.”
As a rationale for masks this fails because it does not mention a necessary prior element. In order to work, masks have to attenuate the guilty aerosols. The individual aerosols involved could be only a micrometer or few micrometers in size. The individual virions are in the range of 50-130 nanometers.[6] I have looked at a number of cloth masks that one can purchase and found their pore sizes to be 0.05 to 0.15 millimeters. This is 1000 times larger than virions and hundreds of times larger than small aerosols. No wonder these packages of masks should come with disclaimers. Adding to this issue of excessive pore size is that cloth masks are not made of certified materials, are manufactured to no standard, are often ill-fitting displaying gaps aside the nose and on the cheeks, or pulled down below the nose, and sometimes placed over a beard. Flat surgical masks do better at times with the excessive pore size problem but still present issues with poor fit and gaps.
There is a mask that corrects most of these deficiencies. The N-95 mask is made of qualified materials and manufactured to a standard. These masks attenuate 95% of particles in the size range of 0.3 to 0.5 micrometers. However, they still require attention to fit to reduce gaps, and they are not guaranteed to halt very small aerosols the size of individual virions. A news article last summer in the Japanese newspaper, The Asahi Shimbun,[7] summarized measurements that researchers made on particle attenuation of cloth, gauze, and N-95 masks, supports what I have summarized here. Cloth and gauze masks have zero effectiveness; while N-95 masks perform to specification, but only if fitted and worn properly. And even then there is no guarantee they prevent the transmission of disease.
There is one more mechanical aspect to ponder. Often in a crisis people will offer what expertise they can – they recycle their expertise. Something I am doing here. Recently a number of researchers in the field of fluid dynamics have weighed in with measurements and simulations (as one would expect) using computational fluid dynamics (CFD). The AIP journal Physics of Fluids produced a special issue in October 2020 highlighting the physics of masks. One study uses CFD to model persons wearing masks inside and outside, in various conditions of air flow, to address ability of masks to attenuate aerosols ejected from a cough or a sneeze.[8] They state in conclusion…
“… our results suggest that, while in indoor environments wearing a mask is very effective to protect others, in outdoor conditions with ambient wind flow present wearing a mask might be essential to protect ourselves from pathogen-carrying saliva particulates escaping from another mask wearing individual in the vicinity.”
This means, I presume, that masks are useful in a situation when all around are sick, and sneezing, wheezing, and coughing — in other words, in a Covid ward of a health care facility. What does “very effective” mean? If it means a very great attenuation of particles, greater than 95% say, then this still has to be interpreted in the light of findings that as few as 300 virions can lead to disease.[9] However, one would think that if coughing and sneezing are the issue, then covering a cough or sneeze should do as well, or perhaps even better when one considers the problem of ill-fit and aerosol escaping through gaps. My experience since March 2020 is that I never encounter anyone in public who are so sick that they are simply sneezing and coughing with abandon.
This computational fluid dynamics approach to determining the efficacy of masks resembles the equivalent modeling approach to climate change. They imply that models define reality when, in fact, it should be that observations and measurements do. There is no means to turn CFD models into clinical outcomes.
In summary, there are mechanical reasons to suppose that masks could reduce the spread of virus in some settings, but none appear pertinent to the materials used to construct masks, or to the ways the public wear them in about 98% of situations. Opposed to supposing that masks might work, or modeling how they might work, we can only learn what efficacy they have by making experiments or observations.
Experiments
The closest thing I have found to true experiments regarding masks are a small number of randomized clinical trials (RCTs). A surprisingly few RCTs involving masks and respirators have been done.[10] I will summarize only two of these. Of these one is pre-COVID-19 and not controversial, and the other is post COVID-19 and subject to controversy and censorship.
There are many respiratory diseases which circulate in the human population. The recent epidemics of MERS, SARS, Ebola and influenza provoked a search for effective non-pharmaceutical interventions. In one example, a group of doctors became interested in how well cloth masks performed for preventing infection in hospitals because such masks are in wide use in the developing world. This trial involved 1607 volunteers at 14 hospitals in Hanoi, Vietnam working in high-risk wards. There were three arms in this RTC: cloth masks, surgical masks, and a control arm of “standard practice” which involved some mask usage but at about one-half the compliance rate of the two treatment arms. The study took place over a four week period, and was to the authors’ knowledge, the first RCT involving cloth masks. Among their findings were that particle attenuation was virtually nil in the cloth masks (97% infiltration), and surprisingly poor in these particular medical masks (44% infiltration). The rate of infection in the cloth mask wearers was double that in the medical mask wearers; medical masks showed some effectiveness, but this contradicted earlier studies showing no efficacy to the medical masks.[11] The researchers conclude that cloth masks should not be advocated for health-care workers, at least until a much better design of such is produced.[12]
The second RCT was performed in Denmark last spring and was subject to censorship by our social media as well as facing some publication resistance.[13] It involved 4862 participants who completed the study. It is more pertinent to this essay because it addressed the efficacy of masks outside of a health care setting. Participants were divided into a control group asked to refrain from wearing masks when out of their home and a treatment arm asked to wear a mask when out of the home for three hours per day. Both groups were ask to follow other social distancing guidelines in order to prevent confounding of masks and distancing which have similar if not identical effects. The primary measured outcome was the number of participants showing SARS-CoV-2 or other respiratory viral infections after one month as determined from PCR testing or hospital diagnosis.
The outcome produced an infection rate of 2.1% in the control arm against 1.8% in the treatment arm. However, the confidence interval of odds ratio (CI of 0.53 to 1.23) included a value of 1.0 almost at its center, suggesting no significant difference in outcomes. If one were to yet insist that the small difference in attack rate (42/2392=1.8% versus 53/2470=2.1%) is nonetheless an important risk reduction, the absolute risk reduction implied (0.003) translates into 30,000 hours (90 hours/0.003) of mask wearing to prevent one case of COVID-19 when community prevalence is around 2.0%. Take that as you may.
There is an interesting series of response letters to this study that are published along with it. These make some legitimate points about design deficiencies. It is certainly true that a study involving masks cannot be a “true RCT” because one cannot blind a study involving masks to a clinical end. The wearer knows they are wearing a mask, and so does the rest of the public. I won’t belabor this point by describing what can go wrong in an unblinded study. Another criticism focuses on using PCR tests, with their false positives and negatives, to measure outcome – a problem which will return in the next section about observations. However despite some criticism, one might note that the outcome of the CHAMP study, in which U.S. Marine Corps recruits were subjected to rigorous social distancing, hygiene and mask wearing resulted in just about the same attack rate as found in this study.[14] I doubt it is possible in the present politicized and hysterical atmosphere to do an RCT on any non-pharmaceutical intervention that could satisfy critics, but none that I know of have shown significant effectiveness of masks.[15]
Observations
Before launching into a discussion of what observations concerning the epidemic may mean, a brief segue into the incubation period and other influences on reporting is instructive. The incubation period of Sars-CoV-2 is probably ten or fourteen days long. Following exposure there is a probability on each successive day of someone becoming a case with half of the ultimate cases developing by day five or six.[16] The process behaves like a low pass filter with a delay. Figure 1 shows this. One-hundred exposures on day zero, presuming all result in cases, produces rising numbers until 19 cases occur on day five. Then they decline to zero.
This has two important considerations. First, it smooths the results of any factor producing a change to R, the reproductive ratio, and makes such changes harder to detect. That is, it reduces resolution. Second, it produces a correlation of cases day to day, so that counts of cases on successive days are not independent of one another, and this has the effect of reducing the degrees of freedom in observational data.[17]
Add to this the distortions resulting from common graphing options like 7 to 21 day averaging done with one-sided (causal) filters; and distortions which resulted from switching from clinical diagnosis to “lab confirmed” cases resting on PCR tests, and what one has is a mess. It is easy to reach a point where what a graph shows today is what might have happened three weeks earlier.

Figure 1. From a single exposure event cases climb for many days afterward in the incubation period. This behaves like a low-pass filter with a delay.
One does not have to search extensively to find evidence suggesting that epidemics proceed unhindered despite all sorts of mandates. I know of no epicurve showing a clear effect. Figure 2, using data drawn from the Covid Tracking Project, for example, shows a comparison among Colorado, New Mexico, and Utah. Despite mandates of various rigor, introduced at different times, the epicurves are virtually the same.[18] The Swiss Policy Research Group produced a nice twelve-paned panel, found here, which makes comparisons among various countries, with the same result – masks have no obvious benefit. A more detailed time series of cases in four German cities during April, 2020 also shows no benefit;[18] however, I would criticize these time series as being of such short duration following the mandatory mask order as to have possibly missed the period of greatest effect, if there is one, just over incubation delay.

Figure 2. Comparison of epicurves from three neighboring states, with timing of mask mandates shown. This was done by @ianmSC on Twitter using data drawn from the Covid Tracking Project.
The global data firm Dynata reported that by the first of July mask wearing in Houston and south Florida was likely to be 80% even before mandates; yet these places saw multiple large waves of infection thereafter.[20] California and New York applied rigorous mask mandates, yet still went through several large waves in the summer and autumn. The USA as a whole, in which 39 states imposed mask mandates in April or before, exhibits an epicurve almost identical, except for vertical scale, to Wyoming, the smallest state, even though Wyoming applied no state-wide mandate until November 9. The CDC reported that most people contracting COVID had worn masks, although self-reporting is notoriously inaccurate.[21]
There are many problems with our observational data. Death counts have been biased by incentives provided to hospitals over payments for COVID-19 deaths.[22] While many states tried to build useful epicurves by placing cases on date of symptom onset, many publically available data sets were built by date of case report and become dominated by the cycle of bureaucratic testing and reporting rather than by characteristics of the disease. To see how these differ Figure 3 shows Colorado data from 08/02/20. The difference is stark with a dominant seven day cycle which some people have confused with a dynamic of the disease and which disappears in the date of onset rendition. A subtle effect like mask usage is likely to be lost in these extraneous influences.

Figure 3. Comparison of epicurves by date of onset vs. report date.
The case data is a mess because when it began early in 2020 cases were confirmed through symptoms or at least a probable contact with another case, but eventually became dominated by mass testing of people without symptoms using PCR tests. Once this mass testing took hold even states trying to maintain an epicurve by date of onset could no longer do so. Figure 4 shows the curve for the state of Wyoming which became dominated by the weekly cycle of PCR testing which began at the University in Laramie in mid-august, but really took effect with return of students around September 1. Because so many of the “lab confirmed” cases had no associated symptoms a full one-third of cases remained always under investigation and the date of report became the de facto date of onset.[23]
This university provides an interesting case study in itself. The total number of cases from the start of the epidemic to the 31st of August in the entire county was134 – less than one case per day. The university instituted a very rigorous set of rules for reopening including mask wearing in all settings inside and out, rules for limiting number of persons in university vehicles, foot traffic patterns inside buildings, dedicated entrances and exits, periodic sanitation of all surfaces, social distance guidelines and even a web site to report persons not following rules. I did a few informal surveys around campus in September and October and thought mask compliance was between 80 and 90%.
Nevertheless by October 15, six weeks later, the county had added 780 cases of which 551 (71%) were connected to the U.W. campus. The rules and masks appeared to present no barrier to the spread of our mini-epidemic.[24]

Figure 4. Confirming cases using lab PCR tests caused the appearance of a seven day period in the epicurve.
Evidence provided to support mask mandates consisted mainly of a single study.[25] There have been many criticisms of this study, including one which suggested it be retracted.[26] However, ignoring its controversy for the moment, let’s just focus on what the authors have to say.
They state, first of all, that masks may have effectiveness as large as 85%, but that this estimate has low confidence – precise number but narrow confidence interval. Second, they notice a diminished effectiveness between N95 respirators on the one hand and cloth masks with 12 to 16 plies on the other. No one wears cloth masks with even one-fourth as many plies. Thus, this can’t be an endorsement of cloth masks. No one has unlimited access to N95 respirators,[27] and couldn’t because there is not enough manufacturing capacity to supply them to the public in general. Thus, this “essential” study does no more than reiterate what the other sources of information, including the measurements of particle attenuation reported in the Asahi Shimbun article, have to say. Its recommendations are not pertinent to reality of mask wearing by the general public. This is an unscientific rationale.
A more recent effort to promote masks as essential to controlling the pandemic appears to me to have many shortcomings.[28] This is a retrospective study of the history of the epidemic on a county level, referenced to timing of mask mandates and orders to close or limit restaurant traffic between March 2020 and October 2020. It is what economists would call an “event study”.[29] Problems with the study include:
- The event involved in an event study should be independent of the data. It is not in this case. Mask mandates were generally applied through political pressure during a pandemic wave. Often applied when the wave had begun to wane.
- Mask mandates are probably hopelessly confounded with other orders such as closure of restaurants. According to the researchers themselves, the mask mandates began in April in 39 states, and restaurant closures began in 49 states in March and April. Two influences atop one another. The claim to having a mask measurement unconfounded by closures cannot be true, or there was a lot of data sorting involved which becomes another confounder.
- The paper is missing details about the statistical methods and calculation of significance.
- Even if significant in a statistical sense, the effect seems very small.
The worst flaw seems to me to be a subtle one. The underlying data of the CDC study are curves of cumulative cases and deaths, which I have already explained are flawed to begin with. However, the typical cumulative curve, being a logistic curve, has a particular shape that begins as an almost exponential rise but quickly passes through an inflection with constantly diminishing slope as it approaches a horizontal asymptote. Such a curve will display a long sequence of days in which the case rate declines. An average of daily changes over segments of this decline, even with noise added, which are then referred to an earlier time period, will produce results just like those in the CDC study. No matter what the cause of the limit to an epidemic, the result is the same. What has happened is the CDC has chosen a statistic having a nearly perfect expectation to the characteristics of a logistic curve from any limiting influence, and cannot draw a distinction between the null hypothesis and a particular alternative. It is like circular logic.
Conclusions
There are situations, health care settings mainly or situations of extreme community prevalence with a lot of coughing and sneezing in public, where masks serve a useful purpose. Yet, people who insisted last spring that the epidemic would go away with mask mandates could not have been more wrong. Every consideration shows this.
Nearly all the masks we see people wearing are constructed to no standard, made of varying sorts of cloth, are poorly fitting, are worn with near complete disregard for effectiveness, reused who knows how many times, used for what else we know not, and are often completely open at the cheeks, nose, chin and beard. They appear mainly useful for making a person touch their face constantly.
How about experimental or observational evidence from the present pandemic? The only experimental evidence is consistent with the benefits being so small they cannot be distinguished from occurrence by chance. Probably no new experimental evidence will become available for the following reason: People have probably changed their behavior drastically during this pandemic leading to too many confounding factors to identify the effect of just one. As the epidemic wanes recruiting sufficient subjects for RTCs becomes difficult.
Masks mandates are not a risk free intervention. They have a poor effect of civil society, they absorb resources, they possibly carry health risks of their own, and they certainly contribute to mistaken notions of safety and risk. Masks seem to me like a solution to a political problem which should alone raise skepticism about all claims.
References/Notes:
1- Gery P. Guy,Jr. et al, Association of State-issued Mask Mandates and Allowing On-Premises Dining with County-level COVID-19 Case and Death Growth Rates, https://www.cdc.gov/mmwr/volumes/70/wr/mm7010e3.htm?s_cid=mm7010e3_w, last accessed 3/8/2021.
2-Lincoln Moses and Frederick Mostellar, Experimentation: Just do it!, In Statistics and Public Policy, Bruce D. Spencer Ed., Oxford U Press, 1997.
3-Futile Fussings: A history of Graphical Failure from Cattle to #coronavirus https://wattsupwiththat.com/2020/03/31/futile-fussings, last accessed 03/13/2021.
4-Close Encounters of the Third Kind, for example.
5-I have a collection including about three-dozen essay, opinion pieces, and research papers, discussing the topics of social distancing, mask mandates, lockdowns, school closures. These include contributions by Dr.s Scott Atlas, John Ioannidis, Paul Alexander, Donald Henderson, Jay Battacharya, Sunetra Gupta, Carl Henehgan, Tom Jefferson, Martin Kulldorff, and others; and almost all of these have been ignored, scorned, or censored in some way.
[6]-Individual virions are mentioned as having various sizes ranging from 50 to 130 nanometers in various internet sources. Corona viruses are pleomorphic which means they have a variety of shapes.
7- Cloth face masks offer zero shield against virus, a study shows, Nayon Kon, The Asahi Shimbun, July 7, 2020.
8-Ali Khosronejad, et al, Fluid Dynamics simulations show that facial masks can suppress the spread of COVID-19 in indoor environments, AIP Advances 10, 125109, (2020); https://doi.org/10.1063/5.0035414;
9-Referenced in Imke Schroeder, COVID-19: A Risk Assessment Perspective, J Chem Health Saf., 2020 May 11: acs:chas.0c00035
10-Tom Jefferson, and Carl Heneghan, Masking lack of evidence with politics, Center for Evidence Based Medicine, July 23, 2020. In particular the authors note the surprisingly small number of RTCs considering the great importance of controlling respiratory disease.
11-C. Raina MacIntyre, et al, A cluster randomized trial of cloth masks compared with medical masks in healthcare workers. BMJ Open 2015;5;e006577. doi.org/10.1136/bmjopen-2014-006577. Two earlier studies conducted in China by same group found no effectiveness for medical masks.
12-By significant in this context the authors mean a 95% confidence interval that does not enclose a relative risk of infection of 1.0, but is entirely above or below 1.0.
13-Henning Bundgaard, et.al. Effectiveness of adding a mask recommendation to other public health measures to prevent SARS-CoV-2 infection in Danish mask wearers, Annals of Internal Medicine, 18 November 2020. https://doi.org/10.7326/M20-6817
14-Andrew G. Letizia, et al, SARS-CoV-2 Transmission among Marine Recruits during Quarantine, N Engl J Med 2020; 383:2407-2416. DOI: 10.1056/NEJMoa2029717
15- Not finding significant protection, significant in the statistical sense, does not mean masks are completely ineffective, or counter-effective, but rather that their effect was not so large that it could be distinguished from a chance outcome at some level, usually 95%, of confidence.
16-P.E. Sartwell, The distribution of incubation periods of infectious disease, Amer. Jour. Hyg., 1950, 51:310-318. Sartwell lists coronaviruses as having a log mean of 0.4 (2.5 days) and dispersion of 1.5. However, a recent training class stated a median of 5-6 days for SARS-CoV-2. I used 5 days for purposes of producing Figure 1.
17-swprs.org/2018/10/01/covid-19-intro/ search for the English language version.
18- This panel of four German city graphs can be found at swprs.org/face-masks-evidence/ last accessed on 3/12/2021
19-This is well known, but see for example, chaamjamal, Illusory Statistical Power in Time Series Analysis, April 30, 2019, https://tambonthongchai.com/2019/40/30/illusory-statistical-power-in-time-series-analysis/ last accessed 1/18/2020
20-WSJ July 29, 2020.
21-CDC report referenced in article at The Federalist, CDC Study Finds Overwhelming Majority Of People Getting Coronavirus Wore Masks, October 12, 2020 https://thefederalist.com/2020/10/12/cdc-study-finds-overwhelming-majority-of-people-getting-coronavirus-wore-masks/
22-Payments for covid deaths, but not for others is incentive enough to bias results.
23-My attempts to learn how many cycles were being employed to report PCR results revealed that no one at any responsible agency in my state knew. All they would do is refer me to a misleading and wrong page at the supplier of the tests. However, a news item reported that researchers at Wayne State University a variety of cycle numbers are used to report results nationally including numbers from 25 to above 37. Viral Loads In COVID-19 Infected Patients Drop, Along With Death Rate, Study Finds Researchers find “a downward trend in the amount of virus detected.” Joseph Curl, DailyWire.com, Sep 27, 2020
24-UW to implement enhanced covid-19 testing program Monday, UW press release, Oct. 15. Data from this also mentions the university expects to perform 15000 tests per week. Yet my asking questions revealed that no one seemed to know what to expect from false positive and negative results. Amazingly few people recognize that interpreting the outcomes of PCR tests is a matter of conditional probability and cannot be done reliably without other information. Even one-half of the faculty and students at Harvard medical school did not know this according to an example from Julian L. Simon in his book “Resampling: The New Statistics, 1997.”
25-Derek K Chu, MD, et al, Physical distancing, face masks, and eye protection to prevent person to person transmission of SARS-CoV-2 and COVID-19: a systematic
review and meta-analysis, The Lancet, v 395, issue 10242, p1973-1987, June 27, 2020 https://doi.org/10.1016/S0140-6736(20)31142-9
26-For example, the Center for Evidence Based Medicine (CEBM) at Oxford University objects to its social distancing conclusions.
27-The term “N95 Respirator” is ambiguous. These respirators are designed to be tight fitting, but most N95s are manufactured for construction, while there are N95s specifically manufactured to prevent disease transmission. Unfortunately the studies cited do not present a clear picture of which N95s were employed.
28-Refer to note #1 above. But in addition to my concerns listed here more were raised in Paul E. Alexander, The CDC’s Mask Mandate Study: Debunked, AIER, March 4, 2021 https://www.aier.org/article/the-cdcs-mask-mandate-study-debunked/ last accessed 3/13/2021
29-John Staddon, Scientific Research: How Science Works, Fails to Work, and Pretends to Work, Routledge, 2018, p. 124.
Are Doctors Failing To Record Bad Reactions To Covid Jabs?
Conservative Woman | March 16, 2021
This article was written by ‘a frontline NHS consultant’.
I HAVE just logged on to enter a patient with a fatal flare-up of malignant melanoma (originally diagnosed and surgically excised in 2014) manifesting as a suspected stroke with unilateral arm paralysis at the end of February, exactly one month after the patient’s first dose of the AstraZeneca coronavirus jab. This is the sixth Yellow Card report I have made in a month.
It seems entirely plausible to me, from a biological perspective, that natural tumour-suppressing activity of our lymphatic cells (NK cells and various classes of T Cell) could be temporarily suppressed by the surge of spike protein induced by the vaccine. As this is a new class of drug, which was rushed to market at breakneck speed, it is my clinical instinct that we should err on the side of over-caution as regards reporting observational anomalies or potential adverse reactions. With this week’s news that Denmark and other countries have suspended the use of the AstraZeneca vaccine, this approach seems even more sensible.
As a doctor with more than three decades of experience, this observational practice defines a long tradition of proper science.
But just how accurate and usable is the adverse event Yellow Card reporting system in the UK? Given the highly experimental nature of the Covid-19 vaccine, was due diligence given to making sure those rolling it out, and indeed those receiving it, were well versed in this system of reporting?
I have noticed that young doctors I work with are rather perversely trained not to respond to their instincts and clinical observations. The strict and immovable hierarchy within the NHS quickly instructs them that in this environment, the squeaky wheel definitely does not get the grease. It may find itself rolled out of the door, never to return. Working in a sector with only one potential employer, viz the NHS, this is not a risk many young medics would be prepared to take.
Using the MHRA (Medicines and Healthcare products Regulatory Agency) reporting system for adverse effects following the vaccine is a shockingly unlikely thing to happen among hospital doctors where I work. From many discussions I have had over the years, I know that this is also the case in various hospitals where colleagues work. None have had any training in using the online system and many seem surprised to learn of its existence.
The net result is that many adverse events do not get reported by medics. Most are not even noticed. There is no tradition of timelining the appearance of a problem and remarking any possible connection to the vaccine. Because the mantra ‘vaccines are safe’ is so embedded, both societally and medically, most in the medical fraternity struggle to envisage that a vaccine could have deleterious effects past the first 15 minutes of being injected. There is a collective spirit of self-censorship with respect to the Covid-jabs in particular. It is disquieting to say the least.
Members of the public, as well as healthcare professionals, are free to lodge a Yellow Card event at this site. Has every person getting the jab received clear instructions on how to do this? Did every individual really receive the information necessary to give informed consent? In a world where patient safety was the primary objective, this would be a bare minimum for an entirely novel medical product, particularly when being rolled out to millions of people at once. Were care home managers educated on the reporting system and trained in observing changes and possible symptoms? From enquiries made to care home managers, it seems this did not happen.
It is also possible to lodge an event on behalf of a relative you care for, or for an elderly relative who cannot perhaps navigate the labyrinthine online reporting system. When making the report, you can register so that any future reporting you do may be accessible by putting in your email and password to bring up the reporting system. However, you may lodge a report without doing this.
The online form is poorly designed. I know numerous computer-literate clinical colleagues who find it time-consuming and cumbersome. For something as simple as a headache one has to choose from 50 different types of headache. For insulin, 20 types. Such systems need to be simple and slick to avoid further unnecessary blocks for busy medics.
The issues cited above are reflected in the fact that adverse effects have been reported for only 0.3 per cent of Pfizer vaccinations and 0.5 per cent of AstraZeneca vaccinations. In their phase 1 and 2 trials, adverse events were reported at least 100 times more often (Pfizer 84 per cent pain, 63 per cent fatigue; AstraZeneca 50 per cent moderate symptoms). With these kind of percentages slipping through the cracks, it seems that the entire reporting system is in dire need of an overhaul.
Surprise, Surprise – MP’s and Scientific Advisors are heavily invested in Vaccine Industry
The Daily Expose | March 8, 2021
The UK Government is on a mission to vaccinate the entire population of the UK with an experimental gene therapy. Their supposed reasoning is to protect us all against a “deadly” virus. But that just isn’t the case, the resulting disease statistically kills only 0.2% of those it infects and the majority of those deaths are aged over 85 and have underlying health conditions.
So the question remains, ‘Why does the Government and it’s scientific advisors so desperately want to vaccinate every man, woman and child in the United Kingdom?’.
Well The Daily Expose investigated by following the money, and this is what we found…
In April 2020, the ‘Chief Scientific Advisor’ to the UK Government – Sir Patrick Vallance was placed in charge of the new ‘Vaccine Taskforce’. The aim of this taskforce was to “drive forward, expedite and co-ordinate efforts to research and then produce a coronavirus vaccine.”
So isn’t it interesting how by July 2020 the UK Government signed a contract with GlaxoSmithKline to secure 60 million doses of an untested, experimental “vaccine” treatment that was still being developed to combat SARS-CoV-2? Interesting because the chief scientific advisor and head of the ‘Vaccine Taskforce’ has £600,000 worth of shares in the pharmaceutical giant, GlaxoSmithKline.
Sir Patrick, who has had huge influence in dictating the Government’s response to the alleged SARS-CoV-2 pandemic, has over 43,111 shares in the company. But the conflict of interest doesn’t end there. Sir Patrick Vallance used to be the president of GlaxoSmithKline.
He joined the company in May 2006 as ‘Head of Drug Discovery’, going on to become Senior Vice President of Medicines Discovery and Development, before finally becoming President in 2006.
When the pompous Health Secretary, Matt Hancock found out about this he said “Well, I didn’t know about it until I read it in the newspapers,”. Pushed on whether he thought he should have been informed as Health Secretary, he replied: “No, not particularly”.

Sir Patrick Vallance
Just recently, the Deputy Chief Medical Officer for England – Jonathan Van Tam said that it was “perfectly possible” a “Covid” vaccine could be licensed for children by the end of the year. Stating that he believes “most of the major manufacturers are beginning to turn their attention “to licensing vaccines for under-18’s”.
But we’ve been repeatedly told that children are at no risk to the Covid-19 disease, so why on earth do we need to vaccinate them?
Well Professor Van Tam’s career history can possibly clarify why he is so eager to see children vaccinated against a disease they supposedly don’t suffer from.
Van Tam joined the pharmaceutical industry in 1997 as an associate director at SmithKline Beecham. He then went on to become Head of Medical Affairs at Roche in April 2001, before joining Aventis Pasteur MSD in February 2002 as the UK medical director.
In 2010 he became an advisor to the World Health Organisation, during the over exaggerated H5N1 influenza pandemic. His advice was to roll out a mass vaccination programme to combat the H5N1 influenza virus, and that advice was followed. But guess who manufactured the H5N1 influenza vaccines and made billions of pounds? SmithKline Beecham and Roche, two pharmaceutical giants that Van Tam worked for.
So do you think Van Tam wants to vaccinate children for the good of their health? Against a disease we’ve been told they don’t suffer from. Or do you think he wants to vaccinate children in order to make billions for the companies he serves?

Professor Jonathan Van Tam
That’s two of the main influencers on UK Government policy so far who have major ties to the pharmaceutical giants, with both Vallance and Van Tam having ties to GlaxoSmithKline, and Van Tam also have ties to pharmaceutical company ‘Roche’. Well there’s another man who has had great influence on the Government’s “Covid” strategy, and he also has major shares in ‘Roche’.
His name is Sir John Irving Bell, and he is a Canadian immunologist and geneticist. Sir Bell also had a role in the ‘Vaccine Taskforce’ alongside Sir Patrick, but there’s another role he held that is of particular interest to our investigation.
Sir John Irving Bell has worked as an adviser to the Department of Health and Social Care since 2017, and headed the ‘National Covid Testing Scientific Advisor Panel. He also chaired the Government’s new test approvals group, which assesses virus diagnostic tests. One of the tests assessed and approved, back in May 2020, was an antibody test. The manufacturer of this antibody test being the pharmaceutical giant ‘Roche’. So it must just be a coincidence that Professor Van Tam has ties to the firm, and Sir John Irving Bell has shares amounting to £773,000 in Roche?
£13.5 million of the British taxpayer’s money was spent on these antibody tests but Public Health England later declared they were “unreliable”.

Sir John Irving Bell
Which brings us to the elected members of parliament who are voted in to serve the people of the United Kingdom. The one’s who have had the final say on the policy to combat the alleged Covid-19 pandemic.
The Health Secretary – Matt Hancock received a £10,000 donation for his leadership campaign in 2019 from Wol Kolade, the head of Livingbridge private equity firm. This firm owns Vanguard Healthcare, which provides mobile facilities such as operating theaters and wards. We wonder if Vanguard had anything to do with the Nightingale hospitals that were erected, never used and dismantled at a cost of half-a-billion pounds?
Mr Hancock has also awarded a contract to the tune of £5.5 million of taxpayer’s money to a family friend for the provision of mobile testing units. The contract was awarded to EMS Healthcare, which is run by an Iain Johnston – the former business partner of Shirley and Robert Carter, Hancock’s mother and stepfather.

Matt Hancock pictured with Wendy Maisey
Education secretary Gavin Williamson received £3000 from St Philips Care Caledonia Ltd in November 2019, while Waveney MP Peter Aldous registered a donation of £2000 to the General Election Fighting Fund from Althea Healthcare Properties.
Mike Freer, MP for Finchley and Golders Green, registered a £10,000 donation in January from Advinia Health Care, which operates care homes.
Steve Brine , MP for Winchester, who is listed as an event speaker for Sigma pharmaceuticals company, receiving £1667 a month for up to 16 hours of “speeches, networking and Q&A sessions”. He is also a strategic adviser to Remedium Partners, a healthcare recruitment firm, working on an “ad-hoc basis” at a rate of £800 a day. Brine states in the register he consulted ACoBA about both of the appointments.
Finally we come to the Vaccine Deployment Minister, Nadhim Zahawi. Mr Zahawi’s wife, Lana Saib is the owner and director of ‘Warren Medical Limited’, which was incorporated under the name ‘Zahawi Warren Limited’ on the 10th June 2020. The company has another two directors named Ahmad Shanshal and Jaafar Shanshal – who are the sons of Nadhim Zahawi. It is not clear what this newly formed company currently does in the healthcare sector but we’re sure the vaccine roll out will have something to do with it.

Nadhim Zawahi
We could go on forever as the corruption doesn’t end there. But perhaps we’ll save Professors Neil Ferguson and Chris Whitty for another day.
The question was ‘Why does the Government and it’s scientific advisors so desperately want to vaccinate every man, woman and child in the United Kingdom?‘.
We think we’ve just answered it for you.
The Lockdown, the Vaccine, and the Corruption Endemic in Modern Democracy
By Andrew Anglin | The Daily Stormer | March 16, 2021
We’ve got some new information about Pfizer, the pharmaceutical company that has designed one of the deadly coronavirus vaccines from The Intercept’s Lee Fang. He’s gotten ahold of internal documents, which were intended for investors.
Currently, Pfizer claims that you need two injections of the “vaccine” in order for it to work. However, Fang has revealed that the company is pushing for a third injection, even before they begin with the annual “boosters.”
Fang got video of executives talking on Zoom, with Pfizer executive Frank D’Amelio talking about all of the money they are going to make with these shots as the coronavirus hoax shifts from “pandemic” to endemic.
This should be breaking global news, that this vaccine company is trying to inject people with as many shots as possible.
Endemic Corruption in the Vaccine Industry
The fact that these companies are making such huge amounts of money from these vaccines should bring into question a conflict of interests among the medical establishment, which is so heavily funded by these companies.
Outside of any questions about what the vaccine is, what the virus is, and whatever else we can talk about, this is just very straightforward, simple corruption in action.
Pfizer has their annual reports of “charitable donations” available on their website, and the list includes hundreds of different organizations, all of which are aggressively in support of the vaccine program.
I took the time to browse through the 2020 Q1-Q2 (half the year) “U.S. Medical, Scientific, Patient and Civic Organizations Funding Report” report, and it is 37 pages long.
Note that this is only one type of bribe. They have several other categories of “funding” of various private institutions.
This will be the situation not just with Pfizer, but with any of the big pharma entities – they make sure to send money to everyone, in order that everyone has a good opinion of them. The government considers this bribery to be “charitable work.”
Beyond the medical establishment being fueled by big pharma, the governments that are trying to force these injections on us, claiming we are immoral if we don’t take them, are also heavily funded by these companies.
According to OpenSecrets, a site that tracks political donations and lobbying, Pfizer was number 25 in the United States in government lobbying in 2020.
They made millions in contributions directly to candidates, with Joe Biden being the number one recipient. … continue
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Who Runs Our World?

Netanyahu addresses US Congress
By Richard Hugus | January 4, 2019
Our world is run by oligarchs, the holders of vast wealth from monopolies in banking, resource extraction, manufacturing, and technology. Oligarchs have such power that most of the world doesn’t even know of their influence over our lives. Their overall agenda is global power — a world government, run by them — to be achieved through planned steps of social engineering. The oligarchs remain in the background and have heads of state and entire governments acting in their service. Presidents and prime ministers are their puppets. Bureaucrats and politicians are their factotums.
Who are politicians? Politicians are people who work for the powerful while pretending to represent the people who voted for them. This double-dealing involves a lot of lying, so successful politicians must be good at it. It’s not an easy job to make the insane agenda of the powerful seem reasonable. Politicians can’t reveal this agenda because it almost always goes against the interests of their constituents, so they become adept at sophistry, mystification, and the appearance of authority. For example, wars for Israel have been part of the agenda of the powerful for years. Since 2001, wars for Israel have been sold as “the war on terror” and lots of lies had to be made up as to why the war on terror was a real thing. The visible faces promoting the war on terror were neoconservatives in the US, almost all of whom were advocates for Israel, or Zionists. Zionists are not the only members of the oligarchy, but they seem to be its lead actors. ... continue
Blog Roll
 Aletho News
Aletho News- Palantir touts record expansion and ‘battlefield’ AI value
- Israeli telecom networks used for mass surveillance across countries
- US claim of sinking Iranian boats ‘a lie’, senior military official tells IRIB
- New KC-46 Supertankers Promise Israel Conventional Samson Option Strike Сapability
- No, New York Times, We Don’t Need to Dam the Bering Strait
- Gates-Funded ‘Big Catch-Up’ Delivers 100 Million Vaccine Doses — Including High-Risk DTP Vaccine Not Used in U.S.
- No commercial ship or oil tanker transited Strait of Hormuz in past hours: IRGC
- Russia warns of escalating NATO military activity in Baltic region
- Government Kills the Spirit
- How ‘Israel’s’ Iran regime change plot failed – again
- If Americans Knew
- As in Gaza, Israel is targeting rescue workers in South Lebanon, killing more than 100 since March
- Israel’s Obliteration Ecocide from Gaza to Lebanon and Beyond
- Israel Said It’s Applying the Gaza Model in Lebanon. This Is What the Devastation Looks Like.
- New Member of Trump’s Iran Negotiating Team Comes From Notoriously Pro-Israel Think Tank
- Israeli army demolishes Christian monastery, nuns’ school in southern Lebanon
- Tokenizing Christians In Israel
- One Gaza is not enough: Israel is turning southern Lebanon into another Gaza – Daily Update
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- No Tricks Zone
- 46 IPCC Scientists Break Rank, Publicly Challenge Long-Standing Dogmatic Climate Claims
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
