Putin makes a statement following the Security Council meeting on Donbass recognition
————————————————————————————————–
Freedom over censorship, truth over narrative.
Follow us on TikTok: https://www.tiktok.com/@rt.news
Follow us on Telegram: t.me/rtnews
February 24, 2022
Posted by aletho |
Timeless or most popular, Video | NATO, Russia, Ukraine, United States |
Leave a comment
Russia’s recognition of the ‘people’s republics’ of Luhansk and Donetsk in the eastern Ukrainian region of Donbass on Monday is a watershed event. In a manner of speaking, by this decision President Vladimir Putin crossed the Rubicon. But a tumultuous period lies ahead.
Moscow followed up by putting the legal underpinnings in place “to deploy troops to these regions,” concluding agreements on friendship, cooperation, and mutual assistance between Russia and the two Donbass republics, and, obtaining the authorisation by Russia’s Federation Council, or upper parliament house, for the use of armed forces outside Russia (as required under the constitution.)
The resolution by Federation Council, which was unanimously supported by all the 153 senators at an extraordinary session on Tuesday and coming into immediate effect, says:
“The Federation Council rules to give its consent to the Russian president for the use of armed forces outside Russia on the basis of generally recognised principles and norms of international law. The strength of army units, areas of deployment, tasks and the duration of their stay outside Russia are determined by the Russian president in compliance with the Russian constitution.”
Notably, this authorisation is not Donbass-specific, nor is there any timeline set here. It is also not conditional. Simply put, discretion lies with Putin entirely to make decisions.
Putin’s national address to the Russian people on Monday, which has been amplified further by him in comments to the Russian media on Tuesday, throws light on the “potential future steps.” What emerges from the national address are three things.
First, Moscow views the post-2014 political developments in Ukraine as having been engineered to create an anti-Russian regime in Kiev with hostile intentions, nurtured by the West. This regime is hopelessly compromised to the West and Ukraine has been turned into an American colony.
Second, the North Atlantic Treaty Organisation (Nato) has made deep inroads into Ukraine’s political and defence system. “The Ukrainian troop control system has already been integrated into NATO. This means that NATO headquarters can issue direct commands to the Ukrainian armed forces, even to their separate units and squads.”
Third, NATO is about to grant membership to Ukraine. That will increase the level of military threats to Russia dramatically, considering that American strategic planning documents allow preemptive strike at enemy missile systems. Putin said, “ballistic missiles from Kharkov will take seven to eight minutes; and hypersonic assault weapons, four to five minutes. It is like a knife to the throat.”
Much of this has been said before by Russian leaders but never in such details. Besides, Putin was directly addressing the Russian public and expecting their backing for his decision on Lugansk and Donetsk (which will undoubtedly be a very popular move) and thereby seeking legitimacy for his future course of action. Clearly, the western assessment that Russian public disapproves of any intervention in Ukraine is proven wrong.
For the international audience, Putin’s interaction with the media on Tuesday may be of greater interest. Putin has dropped an important hint that Moscow no longer considers the Minsk Agreements to be pertinent, as the Ukrainian leadership had publicly declared that they were not going to abide by these agreements.
A second point is about the borders of Lugansk and Donetsk. This is a complex issue and the germane seeds of future course of events, perhaps, lie here. This needs some explaining.
The borders of the breakaway regions underwent significant changes when war erupted between the government forces and the separatist forces. in particular, in May 2014, the government forces captured the strategic port of Mariupol (on the Sea of Azov) which used to be part of Donetsk from the separatists.
Putin said on Tuesday that Russian constitution stipulates the borders of Donetsk and Lugansk regions “at the time when they were part of Ukraine.” This is a carefully worded formulation. At issue is Donetsk’s claim to Mariupol, which is a major port for the industrialised rust belt region of Donbass for export of coal, iron ore, etc.
Indeed, retaking Mariupol and the coastal region could give a direct land route from mainland Russia to the Crimean peninsula, which is otherwise accessible only via a 19-km long rail-road sea bridge built in 2018.
Also, if Donetsk regains the lost territory, Ukraine will have no access to the Sea of Azov, which would strengthen Russia’s primacy in the Black Sea and enhance the security of its Black Sea Fleet. By the way, Crimea would also get assured supply of fresh water, since Kiev had shut off water from the so-called North Crimean Canal in 2014.
Putin said Russia’s expectation is that all disputes will be resolved during talks between the current Kiev authorities and the leaders of these republics, but he also acknowledged that “at this point in time, we realise that it is impossible to do so, since hostilities are still ongoing and, moreover, they are showing signs of escalating.”
From the remarks, it seems highly likely that conflict will erupt over Mariupol, as Donetsk forces, emboldened by Russian support, are sure to make a determined pitch to retake the port city and the adjacent coastal region, which have a big Russian population too. Of course, Russia is obliged to assist the Donetsk forces militarily if need arises.
Putin floated an idea that the vexed question of Ukraine’s membership can be addressed in such a way that the West does not “lose face”. He suggested that Kiev could instead “refuse to join NATO. In effect, in so doing, they would translate the idea of neutrality into life.”
This is a tantalising thought that has been aired previously also. But Putin linked this to “the demilitarisation, to a certain extent, of today’s Ukraine” — that is to say, the West should not “pump the current Kiev authorities full of modern types of weapons.”
Lastly, Putin drew a red line on any attempt by Ukraine to develop nuclear weapons. He said: “Ever since Soviet times, Ukraine has had fairly broad nuclear competencies… They only lack one thing – uranium enrichment systems. But this is a matter of technology, it is not unsolvable for Ukraine, it can be remedied quite easily.
“As to delivery vehicles,.. they have old Soviet-made Tochka-U missiles with a range of 100 plus kilometres, 110 kilometres. This is also not a problem in view of the competencies, say, at Yuzhmash, which used to manufacture intercontinental ballistic missiles for the Soviet Union.”
Putin seemed disinterested to have any direct interaction with the authorities in Kiev. In fact, Russian diplomats in the embassy in Kiev and the consulates in Lvov, Kharkiv and Odessa are being evacuated.
Putin is looking beyond the current regime in Kiev. Of course, if the Western military assistance to Kiev continues in any form, Washington knows that Russia will regard it as a hostile act and there will be severe consequences. Putin has made it clear that he is prepared to use force to counter any further western encroachments into Ukraine to challenge Russia’s security.
In these circumstances, the question of the return of military detachments of NATO to Ukraine in the garb of ‘advisors’ or ‘trainers’ also does not arise. That being so, the big question is: How long could Zelensky and his government hold out in Kiev? The countdown may have begun.
Putin remarked derisively that Zelensky may simply choose to leave Kiev for the US, Paris or Berlin. In a TV interview yesterday, Foreign Minister Lavrov called Zelensky “an unstable, dependent man, directly dependent on his American curators.” But what can the curators do to prop up Zelensky at such a critical stage? The elites in Kiev are known to have big bank accounts in the West.
Putin spoke with a lot of bitterness. At one point, he directly threatened the extreme nationalists who seized power in the 2014 coup and let loose a wave of violence and systematic persecution against ethnic Russians.
Putin said, “The criminals who committed that atrocity have never been punished, and no one is even looking for them. But we know their names and we will do everything to punish them, find them and bring them to justice.” Putin seems to anticipate a new regime in Kiev.
February 23, 2022
Posted by aletho |
Timeless or most popular | NATO, Russia, Ukraine |
Leave a comment
EACH week, members of the UK’s watchdog Medicines and Healthcare products Regulatory Agency publish their Yellow Card update on adverse reactions to the Covid vaccine.
Every time they do so, they repeat this claim: ‘Vaccination is the single most effective way to reduce deaths and severe illness from Covid-19.’
But how do they know?
The fact is as long as treatments such hydroxychloroquine and ivermectin continue to be banned in the UK, we are prevented from knowing whether treatment could be more effective than vaccines in preventing deaths and reducing severe illness. Published research indicates it could be.
Furthermore without a proper investigation into the thousands of hospital Covid fatalities, how can we know whether the chosen treatment protocols have not been as responsible a cause of death as the disease itself?
In the US, the National Institutes of Health treatment protocol guidance for Covid is based on two drugs, dexamethasone and remdesivir.
Yet at least one major study has called remdesivir into question. Published almost exactly a year ago, it found kidney disorders to be a serious adverse reaction of the drug in coronavirus disease.
It reported that compared with the use of chloroquine, dexamethasone, sarilumab, or tocilizumab, the use of remdesivir was associated with an increased reporting of kidney disorders.
The research states that ‘in the vast majority of cases (316 – 96.6 per cent), no other drug was suspected in the onset of kidney disorders. Reactions were serious in 301 cases (92 per cent) cases, with a fatal outcome for 15 patients (4.6 per cent).
The NHS ‘guidance pathways’ for severe Covid cases – which cover respiratory support to end of life support – are set out here. Other guidance states that ‘treatment with remdesivir may be considered in certain hospitalised patients with Covid‑19 pneumonia’.
Clinicians can also ‘offer dexamethasone to patients with Covid‑19 who need supplemental oxygen, or who have a level of hypoxia (lack of oxygen) that requires supplemental oxygen but are unable to have or tolerate it. If dexamethasone is unsuitable or unavailable, either hydrocortisone or prednisolone can be used.’
An Oxford Recovery Trial for hospitalised Covid patients found ‘the use of dexamethasone resulted in lower 28-day mortality among those who were receiving either invasive mechanical ventilation or oxygen alone at randomisation but not among those receiving no respiratory support.’
The perceived limitations of the data are set out here. But for all the glowing testimonials, the survival of the patients in the trial groups – a 22.9 per cent death rate – was not a huge improvement on that in the usual care group, 25.7 per cent
‘Overall, 482 patients (22.9 per cent) in the dexamethasone group and 1,110 patients (25.7 per cent) in the usual care group died within 28 days after randomisation (age-adjusted rate ratio, 0.83; 95 per cent confidence interval [CI], 0.75 to 0.93; P<0.001).’
What this drug treatment was not compared with was the efficacy of either hydroxychloroquine or ivermectin, two successful early intervention treatments that perversely remain banned here.
Sadly we will never know how many lives would have been saved had these drugs been introduced into community and hospital protocols a year ago? I rest my case.
Isn’t it high time the MHRA revised its claim to say: ‘Vaccine is the single most effective way to reduce deaths and severe illness from Covid-19 in the absence of potentially effective treatments which are banned in the UK.’
Below is the latest full Yellow Card adverse reaction breakdown. It follows a week marked by another seven deaths and a further 82 adverse reactions reported for children, all of which continue to go unremarked by the mainstream media.
MHRA Yellow Card reporting summary up to February 9, 2022 (Data published February 17, 2022)
Adult – primary and booster/third dose, child administration.
* Pfizer: 25.9million people, 49million doses. Yellow Card reporting rate, one in 157 people impacted.
* Astrazeneca: 24.9million people, 49.1million doses. Yellow Card reporting rate, one in 102 people impacted.
* Moderna: 1.6million people, three million doses. Yellow Card reporting rate, one in 45 people impacted.
Overall, one in 118 people injected experienced a Yellow Card adverse event, which may be less than ten per cent of actual figures, according to the MHRA.
The MHRA states that:
* Vaccination is the single most effective way to reduce deaths and severe illness from Covid-19.
* The expected benefits of the vaccines in preventing Covid-19 and serious complications associated with Covid-19 far outweigh any currently known side-effects in the majority of patients.
Adult booster or third doses given = 37,650,239.
Booster Yellow Card reports: 28,941 (Pfizer) + 466 (AZ) + 15,870 (Moderna) + 151 (Unknown) = 45,428.
Reactions: 472,956 (Pfizer) + 862,394 (AZ) + 118,425 (Moderna) + 4653 (Unknown) = 1,458,428.
Reports: 164,679 (Pfizer) + 243,491 (AZ) + 35,566 (Moderna) + 1520 (Unknown) = 445,256 people impacted.
Fatal: 718 (Pfizer) + 1,221 (AZ) + 38 (Moderna) + 40 (Unknown) = 2,017.
Blood disorders: 16,759 (Pfizer) + 7793 (AZ) + 2428 (Moderna) + 62 (Unknown) = 27,042.
Anaphylaxis: 649 (Pfizer) + 871 (AZ) + 87 (Moderna) + 2 (Unknown) = 1,609.
Pulmonary embolism and deep vein thrombosis: 875 (Pfizer) + 3,029 (AZ) + 106 (Moderna) + 25 (Unknown) = 4,035.
Acute cardiac: 12,273 (Pfizer) + 11,147 (AZ) + 3,009 (Moderna) + 90 (Unknown) = 26,519.
Eye disorders: 7,772 (Pfizer) + 14,797 (AZ) + 1,460 (Moderna) + 83 (Unknown) = 24,112
Blindness: 155 (Pfizer) + 317 (AZ) + 31 (Moderna) + 4 (Unknown) = 507.
Deafness: 288 (Pfizer) + 424 (AZ) + 50 (Moderna) + 5 (Unknown) = 767.
Spontaneous abortions: 471 + 1 premature baby death / 15 stillbirth/foetal deaths (11 recorded as fatal) (Pfizer) + 229 + 5 stillbirth (AZ) + 60 + 1 stillbirth (Moderna) + 5 (Unknown) = 765 miscarriages
Nervous system disorders: 78,872 (Pfizer) + 182,030 (AZ) + 19,215 (Moderna) + 839 (Unknown) = 280,956.
Seizures: 1,068 (Pfizer) + 2,050 (AZ) + 250 (Moderna) + 17 (Unknown) = 3,385.
Paralysis: 495 (Pfizer) + 871 (AZ) + 98 (Moderna) + 8 (Unknown) = 1,472.
Tremor: 2,117 (Pfizer) + 9,925 (AZ) + 637 (Moderna) + 50 (Unknown) = 12,729.
Vertigo and tinnitus: 4,078 (Pfizer) + 6,897 (AZ) + 684 (Moderna) + 39 (Unknown) = 11,698
Transverse myelitis: 34 (Pfizer) + 116 (AZ) + 2 (Moderna) = 152
BCG scar reactivation: 67 (Pfizer) + 38 (AZ) + 51 (Moderna) = 156
Headaches and migraines: 35,041 (Pfizer) + 93,844 (AZ) + 9,112 (Moderna) + 331 (Unknown) = 138,328
Vomiting: 5,134 (Pfizer) + 11,631 (AZ) + 1,727 (Moderna) + 59 (Unknown) = 18,551
Infections: 11,611 (Pfizer) + 20,089 (AZ) + 2,160 (Moderna) + 150 (Unknown) = 34,010.
Herpes: 2,149 (Pfizer) + 2,676 (AZ) + 240 (Moderna) + 23 (Unknown) = 5,088.
Immune system disorders: 2,369 (Pfizer) + 3,274 (AZ) + 593 (Moderna) + 21 (Unknown) = 6,257.
Skin disorders: 33,094 (Pfizer) + 53,154 (AZ) + 12,637 (Moderna) + 330 (Unknown) = 99,215.
Respiratory disorders: 20,950 (Pfizer) + 29,585 (AZ) + 4,015 (Moderna) + 196 (Unknown) = 54,746.
Epistaxis (nosebleeds): 1,063 (Pfizer) + 2302 (AZ) + 188 (Moderna) + 11 (Unknown) = 3,564.
Psychiatric disorders: 9,876 (Pfizer) + 18,289 (AZ) + 2,339 (Moderna) + 108 (Unknown) = 30,612.
Reproductive/breast disorders: 30,236 (Pfizer) + 20,649 (AZ) + 4,905 (Moderna) + 199 (Unknown) = 55,989
Children and young people special report – suspected side-effects reported in under-18s:
* Pfizer: 3,200,000 children (first doses) plus 1,500,000 second doses, resulting in 3,044 Yellow Cards.
* AZ: 12,400 children (first doses) resulting in 254 Yellow Cards. Reporting rate one in 49.
* Moderna: 2,000 children (first doses) resulting in 18 Yellow Cards.
* Brand unspecified: 18 Yellow Cards.
Total = 3,214,400 children injected
Total Yellow Cards for under-18s = 3,334
The MHRA states that all children aged five to 11 will be eligible for vaccination in the coming weeks.
For full reports, including 347 pages of specific reaction listings, see here.
February 23, 2022
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, COVID-19 Vaccine, HCQ, Human rights, Ivermectin, UK |
Leave a comment
The first thing I want to say here is that there should be nothing in science that is beyond analysis and potential criticism. Because, once this happens, we can find ourselves in a very dangerous situation indeed. A place of unquestioned acceptance of the accepted narrative, with criticism enforced by the authorities.
Unfortunately, I believe this is the place we have reached with COVID19 vaccination. Here is just one example from the UK.
‘GPs have been warned that criticising the Covid vaccine or other pandemic measures via social media could leave them ‘vulnerable’ to GMC* investigation.’1
*GMC = General Medical Council. This is the body that can strike doctors from the medical register so they cannot work as a doctor.
‘Vulnerable to GMC investigation’. What a deliciously creepy phrase that is, dripping with unspoken menace, whilst pretending to be helpful. It sounds like something the Mafia would come up with.
‘I would keep quiet about this, if I were you.’ Baseball bat tapping gently on the floor. ‘No, this is not a threat, think of it as advice from a friend. We don’t like to see anybody making themselves, or their family, vulnerable, and getting seriously injured now, would we?’
It seems that, unless you prostrate yourself before the mighty vaccine, and intone ‘Our vaccine, which art in heaven, hallowed be thy name…’ and suchlike, you will be attacked from all sides … simultaneously. Indeed, to suggest that vaccines are not perfect in every way is the twenty first century’s equivalent of blasphemy.
‘he said Jehovah. Stone him.’
This does make any discussion on vaccines somewhat tricky. To criticize any individual vaccine, indeed any aspect of any individual vaccine, is also to be instantly defined as an anti-vaxxer. Then you will be furiously fact-checked by someone with a fine arts degree, or suchlike, who will decree that you are ‘wrong’.
At which point you will be unceremoniously booted off various internet platforms – amongst other sanctions open to the ‘vulnerable’. This includes, for example, finding yourself struck off the medical register, and unable to earn any money:
‘Hell, we ain’t like that around here. We don’t just string people up, son. First, we have a trial to find ‘em guilty, only then do we string ‘em up. Yeeee Ha!’
Spit … ding!
Yes, it seems you must support the position that all vaccines are equally wonderful, no exceptions. Try this with any other pharmaceutical product. ‘He doesn’t think statins are that great, so he obviously believes that antibiotics are useless.’ Would this sound utterly ridiculous?
But with vaccines… All are the same, all are great, not a problem in sight? I said, NOT! a problem in sight. However, I genuinely believe there are some questions which still have not been answered and simply because of the different types of vaccines that are available, no, not all vaccines are the same.
Just for starters, vaccines come in many different forms. Live, dead, those only containing specific bits of the virus, and suchlike. Now we have the brand new, never used on humans before, messenger RNA (mRNA) vaccines. So no, all vaccines are not alike. Not even remotely.
In addition to the major difference between vaccines, the diseases we vaccinate against vary hugely. Some are viruses, others bacteria, others somewhere in between, TB for example.
Some, like influenza, mutate madly in all directions. Others, such as measles, do not. Some viruses are DNA viruses – which tend to remain unchanged over the years. Others, e.g. influenza, are single strand RNA viruses, and they mutate each year.
Adding to this variety, some of those viruses which mutate very little, also have no other host species to hide in. Smallpox, for example. Which means that the virus was unable to run away and hide in, say, a chicken, or a bat. Others are fully capable of flitting from animal species to animal species. Bird flu and Ebola spring to mind.
Some vaccines just haven’t worked at all. For over thirty years, people have tried to develop an HIV vaccine, and have thus far failed. Early trials on animal coronavirus vaccines also showed some concerning results. Here from the paper ‘Early death after feline infectious peritonitis virus challenge due to recombinant vaccinia virus immunization.’
‘The gene encoding the fusogenic spike protein of the coronavirus causing feline infectious peritonitis was recombined into the genome of vaccinia virus. The recombinant induced spike-protein-specific, in vitro neutralizing antibodies in mice. When kittens were immunized with the recombinant, low titers of neutralizing antibodies were obtained. After challenge with feline infectious peritonitis virus, these animals succumbed earlier than did the control group immunized with wild-type vaccinia virus (early death syndrome).’2
Yet, despite all this massive variety flying in all directions, with some spike protein vaccines found to increase the risk of death (in a few animal studies), attach the word vaccine to any substance, and it suddenly has miraculous properties that transcend all critical thought. Vaccines move in mysterious ways, their wonders to perform.
Yes, of course, some have worked extremely well. The polio vaccine, for example, although I have seen some valid criticisms. Smallpox… I am less certain about. Even though it is held up as the greatest vaccine success story of all. Maybe it was. Smallpox has certainly gone, for which we should be truly thankful. It was a truly terrible disease.
My doubts about the unmatched efficacy of smallpox vaccine simply arise from the fact that diseases come, and diseases go. The plague, for example. This was the scourge of mankind at one time. It tore round and round the world and leaving millions of dead in its wake, over a period of hundreds of years.
We do not vaccinate against the plague, yet it is virtually unknown today. Cholera killed millions and millions, thousands each year in the UK alone. Now … gone. In the UK at least. This had nothing to do with vaccination either. Measles. There seems little doubt that the measles vaccine is effective. But vaccination cannot explain the fact that measles deaths fell off a cliff and were bumping along the bottom for years and long before we started vaccination programmes.

In the US vaccination did not begin until 1963. So, what happened here? The virus did not mutate, so far as we know. It did not mutate because apparently it cannot. Or, if it did, it would no longer be able to be infective. At least not to humans:
‘While the influenza virus mutates constantly and requires a yearly shot that offers a certain percentage of protection, old reliable measles needs only a two-dose vaccine during childhood for lifelong immunity. A new study publishing May 21 in Cell Reports has an explanation: The surface proteins that the measles virus uses to enter cells are ineffective if they suffer any mutation, meaning that any changes to the virus come at a major cost.’3
So, measles didn’t change, but it did become far less damaging. From around ten deaths per one hundred thousand in the first two decades of the twentieth century, down to much less than one.
Why? What I believe happened with measles is primarily that the ‘terrain’ changed. Nutrition greatly improved. Vitamins, perhaps most importantly vitamin D, were discovered and added to the food supply. Rickets and other manifestation of vitamin D deficiency were rife in the late nineteenth and early twentieth centuries. Virtually gone by 1940.
Of course treatments improved as well, although antibiotics (to treat secondary bacteria pneumonia following measles), did not come into play until the late 1940s, at the earliest.
What we see with measles is simply the fact that infectious diseases have far less impact when they hit a healthy, well nourished person (healthy terrain), than when they hit an impoverished and undernourished child caught in the war in the Yemen, for example.
So, yes, vaccines have played a role in improving human health and wellbeing, but we shouldn’t inflate their impact to the point where they have become the unmatched saviours of humankind. They have certainly not been the only thing that reduced the impact of infectious diseases. They were probably not even the most important thing. ‘Yes … how dare you say this… string up the unbeliever, I know, I know.’
Moving on, and I think this is even more pertinant to the disucssion that follows. If we cannot accept the possiblility that, at least some vaccines, may have significant adverse effects, if we will not permit anyone to look into this, in any meaningful way. Then we can never improve them. Criticism is good, not bad.
Speaking personally, I do not criticize things that I do not care about. Primarily, because I don’t care if they improve, or not. I only criticize things when I want them to be as good as they possibly can be. It is a character trait of mine to hunt for flaws, and potential problems. Both real and imagined.
Some criticism is, of course, close to bonkers. Suggesting that COVID19 vaccines contain transhuman nanotechnology and microchips of some kind that will become activated by 5G phones … to what end? ‘World domination Mr Bond. Mwahahahahaha etc.’ Quantum dots? Yes, these do exist. But they would be pretty useless at collecting informaiton, and suchlike. Give it fifty years and … maybe.
The problem here is that wild conspiracy theories are simply gathered together with reasonable science-based criticism, to be dismissed as a package of equally mad, unscientific woo-woo tin-foil hat wearing, conspiracy theorist, gibberish.
Which means that, when people (such as me) suggested that COVID19 mRNA vaccination could, potentially, lead to an increased risk of blood clots – this was treated with utter scathing dismissal. I did not understand ‘the science’ apparently. Fact check number one. ‘Oh, look… clots.’
When people questioned the ‘fact’ that the safety phases of the normal clincial trial pathway had been seriously truncated, and that some parts were just non-existent, they were told that they knew nothing of ‘the science’ either.
I looked on the BBC website to find out the ‘official’ party line on vaccine safety information, sanctioned and approved by HM Govt, and SAGE I presume. It was an article entitled ‘How do I know if the vaccine is safe?’ The information rapidly contradicts reality. They say:
- There are different approved types and brands available and all have undergone rigorous testing and safety checks
- Safety trials begin in the lab, with tests and research on cells and animals, before moving on to human studies
- The principle is to start small and only move to the next stage of testing if there are no outstanding safety concerns
The article then looks at fast track approval for vaccines against new variants
- The UK’s drug regulator says new vaccines can be fast tracked for approval if needed.
- No corners will be cut, with safety paramount.
- But lengthy clinical trials with thousands of volunteers will not be needed4
What is wrong here? Well, ‘if the principle is to start small and only move to the next stage of testing if there are no outstanding safety concerns,’ then this principle was not followed. After pre-clinical and animal testing, we move onto trials in humans. Phase I, then II and then III.
Phase I may include as few as twenty people to check that humans don’t simply drop dead on contact with the new agent (it has happened).
Phase II may include a couple of hundred individuals, and usually lasts a few months… a bit more safety, and an attempt to establish the potential size of any health benefit.
Phase III may have up to thirty or forty thousand participants. This phase often lasts for several years.
Well, with the Pfizer Biontech vaccine, the concept of waiting to move to the next stage of testing did not truly occur. Because phase II and III were combined… and the phase III trials have now been, effectively abandoned. They were not supposed to finish until May 2022 at the earliest, and now apparently, they are not going to finish at all. At least not as a double-blind placebo controlled trial.
Yet, we are still informed by the BBC, in all seriousness, that no corners were cut, or will be cut. The fact is that corners were absolutely one hundred per cent cut. Slashed to the bone would perhaps be more accurate. To pretend otherwise is simply to deny reality.
It normally takes around ten years for any drug, or vaccine, to move through the clinical trials process, with each step done in series. COVID19 vaccines took around six months from start to finish, with critical steps done in parallel, and the animal testing was rushed – to say the least. To claim that no corners were cut is nonsense. Nonsense that we are virtually forced to believe?
It is possible/quite likely/probable that vaccine development can be shortened, but please do not tell us that all the normal processes were followed. No-one is that easily fooled.
‘Freedom is the freedom to say that two plus two make four[NK1] . If that is granted, all else follows.’ That freedom disappeared pretty early on in the COVID19 pandemic. I enjoyed the slant that ‘Important quotes explained’ had on the quote from Orwell’s 1984.
By weakening the independence and strength of individuals’ minds and forcing them to live in a constant state of propaganda-induced fear, the Party is able to force its subjects to accept anything it decrees, even if it is entirely illogical.
Of course, it could be that despite the speed with which these vaccines were pushed through nothing important was missed. It is almost certainly true that the standard ten years from start to finish in vaccine and drug development can be compressed, if everyone really wished. Bureaucracy expands to fill the space available.
But in general we are talking about a ten-year process, cut down to six months, or thereabouts. An additional concern is that this happened using mRNA vaccines, which represent a completely new form of technology. One that has never been used on humans before at all, ever.
We are not talking about the sixth drug in a long line of very similar drugs e.g. the statins.
- Lovastatin
- Fluvastatin
- Simvastatin
- Pravastatin
- Atorvastatin
- Cerivastatin
- Rosuvastatin etc.
Statins all do pretty much the exact same thing, in exactly the same way. Yet, each one of them still had to go through the entire laborious clincial trial process. Years and years.
‘Can we not just skip this phase…. please?’
‘No.’
‘Please?’
‘No.’
Hold on one moment, just step back, what was that at number six on this list, I hear you say… cerivastatin. You mean you’ve never heard of it. Well, it got through all the pre-clinical trials, then the animal trials. It then sailed through the human Phase II and III trials without a murmur. It was then was launched to wild acclaim. In truth that may be over-egging its real impact, which was a bit more ‘who cares, do we really need another one?’
Here from a 1998 paper: ‘Clinical efficacy and safety of cerivastatin: summary of pivotal phase IIb/III studies.’
‘In conclusion, these studies indicate that cerivastatin is a safe and effective long-term treatment for patients with primary hypercholesterolemia and also suggest that higher doses should be investigated.’ 5
Here from 2001, and an article entitled: ‘Withdrawal of cerivastatin from the world market.’
‘Rhabdomyolysis was 10 times more common with cerivastatin than the other five approved statins. We address three important questions raised by this withdrawal. Should we continue to approve drugs on surrogate efficacy? Are all statins interchangeable? Do the benefits outweigh the risks of statins? We conclude that decisions regarding the use of drugs should be based on direct evidence from long-term clinical outcome trials.’ 6
Yes, as it turns out, cerivastatin caused far more cases of severe muscle breakdown, and death, in a significant number of people. Which meant that it was hoiked from the market.
The moral of this particular story is that, even if you DO do all the clinical studies, fully and completely, one step at a time, over many years, in a widely used class of drug, your particular drug may still be found in the long term, not to be safe. Not even if it is the sixth of its class to launch.
The cerivastatin withdrawal is not an isolated event. You can, if you wish, read this paper ‘Post-marketing withdrawal of 462 medicinal products because of adverse drug reactions: a systematic review of the world literature.’7. So, what happens if you try to compress the entire ten year clinical trial process into around six months, on a completely new type of agent?
… Well then, it may be time to cross your fingers and hope for the best. But please do not insult my intelligence, or the intelligence of anyone else, by trying to tell me that vaccines have undergone: Rigorous testing and safety checks. Compared to what, exactly? Certainly not any other drug or vaccine launched in the last fifty years. ‘We rushed them through, and launched two years before the phase III clinical trials were due to finish.’ would be considerably more accurate.
Two plus two does not equal five, it never has, and it never will. However much you try to browbeat me, and everyone else, into accepting that it does. Indeed, as I write this, the simple fact is that not a single phase III clinical trial has yet ever been completed, on any mRNA COVID19 vaccine, and possibly not ever will be, in truth.
To repeat, this does not mean that mRNA vaccines may not be entirely safe. However, it has become impossible to claim that we have not seen significant adverse effects from the mRNA vaccines. Effects that were not picked up in any phase of the clincial trials. Here, from the Journal of the American Medical Association in February. One of the most highly cited medical journals in the world:
‘Based on passive surveillance reporting in the US, the risk of myocarditis after receiving mRNA-based COVID-19 vaccines was increased across multiple age and sex strata and was highest after the second vaccination dose in adolescent males and young men.’ 8
I highlighted the first bit here. Namely, the words ‘based on passive surveillance reporting in the US.’ Whilst this adverse effect was not seen, or reported in the clinical trials it was picked up by the passive surveillance reporting system a.k.a. spontaneous reporting systems.
Drug adverse event reporting systems
Frankly, it is surprising that anything at all is ever seen using passive surviellance. In the UK we have the passive/spontaneous reporting system, known as the ‘Yellow Card system.’ In this US (specifically for vaccines) there is ‘VAERS’ (Vaccine Adverse Event Reporting System).
When I use the term ‘spontaneous reporting’, I mean a system whereby someone may (or more likely may not) report an adverse effect to a healthcare professional. They may (or more likely may not) fill in a form, whereupon it goes through to VAERS, who then look at it and can decide whether or not the adverse effect may (or more likely may not) be due to the vaccine. Same basic principle in the UK.
How good are these types of spontaneous reporting system in picking up adverse effects?
Well, as far as I am aware, only one serious attempt has been made to look at how many drug and vaccine-related events were actually reported in the US. Here, from a study by The Agency for Healthcare Research and Quality:
‘Adverse events from drugs and vaccines are common, but under-reported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.’ 9
Fewer than one per cent of vaccine adverse events are reported. Their words, not mine. Even though, in the US, unlike the UK, there is a legal responsibility to report adverse events – I believe.
When the authors of this report tried to follow up with the CDC and perform further assessment of the system, with testing and evaluation, the doors quietly, but firmly, shut:
‘Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.’
This study was done over ten years ago, but nothing about the VAERS system has changed since, as far as I know, or can find out.
In the UK the Yellow Card system may be better, or it may not be. No-one has carried out the sort of detailed analysis that was attempted in the US. However it has been accepted that:
… all spontaneous reporting schemes have a problem with numbers: the MHRA (Medicines and Healthcare products Regulatory Agency) itself says that only 10% of serious reactions and 2 – 4% of all reactions are reported using the Yellow Card Scheme. This means that most iatrogenic* morbidity goes unreported.’ 10
*Iatrogenic means – damage/disease caused by the treatment itself.
Frankly, I see no reason why the Yellow Card system would be any better than VAERS. The barriers to reporting are exactly the same. As the US report states:
‘Barriers to reporting include a lack of clinician awareness, uncertainty about when and what to report, as well as the burdens of reporting: reporting is not part of clinicians’ usual workflow, takes time, and is duplicative.’9
In other words, reporting an adverse event takes an enormous amount of time and effort. You don’t get paid for doing it, you certainly don’t get thanked for it, and you have no idea if anyone paid any attention to it. All made worse if you are not sure if the adverse event was due to the vaccine, or not.
I have filled in yellow cards three times, and several hours of work followed each one. As directed, I searched though patient notes for all previous drugs prescribed, the patient’s medical conditions, a review of the consultations and on, and on. Back and forth from the pharmaceutical company the questions went. Until the will to live was very nearly lost.
If you wanted to devise a system to ensure that adverse effects were under-reported, you could not devise anything better. Yes, doctor, please do report adverse effects to us. The result will be endless hours of work, with no attempt to report back that what you did had the slightest effect, on anything. Thank you for your continued and future co-operation. And yet this, ladies and gentlemen, is the system we have in place to monitor and review all drug and vaccine-related adverse effects.
Which becomes even more worrying because, as mentioned before a couple of times so far, nothing else of much use is going to come out of the clinical trials. With the Pfizer BioNTech trial, crossover occurred in Oct 2020. By crossover I mean the point at which they started giving the vaccine to those in the placebo group as well. End of randomisation, end of useful data. End of … well of anything of any use.
mRNA vaccines and myocarditis
Anyway, getting back to the JAMA study. Even with all the formidable barriers in place to reporting adverse events, JAMA reported an increase in the rate of myocarditis of around thirty-two-fold, as reported via the VAERS system.
I should make it clear that this was the increase seen in the most highly affected population. Males aged eighteen to twenty-four. [Myocarditis = inflammation and damage to heart muscle]. The risk was lower in females, and also in other age groups, although still high. But, to keep things simple, I am going to focus on this, the highest risk group, as far as possible.
The first thing to say is that a thirty-two-fold increase probably does sound enormous. Another way to report this would be, a three thousand one hundred per cent increase, which may sound even more dramatic?
However, myocarditis is not exactly common. In this age group, over a seven-day period, you would expect to see around one and three-quarter cases per million of the population. Multiplying this by thirty-two still only gets you to fifty-six cases per million.
Which is not exactly the end of the world. In addition, most cases may fully recover. Although, having just said this, I have no long-term data to support that statement. The closest condition we have to go on as a comparator, is post-viral infectious myocarditis. And this has a mortality rate of 20% after one year and 50% after five years.11
Which means that myocarditis is certainly not a benign condition of little concern.
Anyway, at this point, you could argue that if around only one in twenty thousand men, in the highest risk population, suffer from myocarditis post-vaccination, then this does not represent a major problem.
It could indeed be worse to allow them to catch COVID19, where the risk of myocarditis is even higher than with vaccination. In reality, we may be protecting them from myocarditis through vaccination. This certainly seems to be the current party line. I might even agree with it… maybe. So, as is my wont, I looked deeper.
I looked for the highest rate of (reported) post-viral infection myocarditis, in younger people. I believe it can be found here. ‘Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis’ 12
Here, the reported rate was around four-hundred-and-fifty cases per million. On the face of it, this is much higher than the fifty-six cases per million post-vaccination. Approximately ten times as high. But … there are, as always, several very important buts here. There were two key factors that alter the equation.
First, in the JAMA post-vaccine study, the time period for reporting myocarditis was limited to seven days after vaccination. Any case appearing after that was not considered to be anything to do with the vaccine and was thus ‘censored’. In the study above, the time period was far longer. Anything up to ninety days post-infection was counted. A period thirteen times as long.
In addition, although it is difficult to work out exactly what was done from the details provided, the four-hundred-and fifty study only looked at young people who attended outpatients at hospital. These would have been the most severely affected by COVID19, or who had other underlying medical conditions. So, they represent a small proportion, of a small proportion …. of everyone who was actually infected. The vast majority of whom would only have suffered very mild symptoms, or none at all.
In short, we are not remotely comparing like with like here. I find that we very rarely are. We are not only going to vaccinate a small proportion, of a small proportion, of the population who are at high risk of myocarditis. We are going to vaccinate virtually everybody. So, the two populations are completely different.
Leaving that to one side, where else can we look for a comparison between the risk of post-vaccine myocarditis vs post-infection myocarditis. The CDC published this statement.
‘During March 2020–January 2021, patients with COVID-19 had nearly 16 times the risk for myocarditis compared with patients who did not have COVID-19, and risk varied by sex and age.’ 13
Their figure appears to have been entirely derived from a paper published in the British Medical Journal : ‘Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: retrospective cohort study’ 14. Different age groups were studied here which, again, makes any direct comparison tricky.
This study found a sixteen-fold increased risk, rather than a four hundred and fifty-times risk. A sixteen times risk is around half of the post-vaccination myocarditis risk reported in JAMA, in the eighteen-to twenty-four-year-old group.
Again, though, there were major differences. In the BMJ paper the observation period for inclusion of myocarditis considered to be ‘caused by’ COVID19, was one hundred- and forty-days post infection, not seven days. Twenty times as long for cases to build up.
Equally, after looking at nine million patients records over a year, slightly over two hundred thousand were diagnosed as having had COVID19. Of these, only fourteen thousand had post-infection problems, known as clinical sequelae. In this sub-group, which represents, one point two per-cent of one per-cent of the total, population there were so few cases of myocarditis that they didn’t even appear in the chart published in the main paper. You had to go to supplemental tables and figures 15
To be frank, there are far too many unknowns and uncontrolled variables kicking around here to make any accurate comparisons. However, I do not think it would be unreasonable to suggest that the risk of myocarditis post-vaccination, from these studies, is roughly the same as if you are infected with COVID19.
Once again though, we need to take a further step back. All of our figures here only make sense if all – or the majority of cases of myocarditis – are actually being picked up. What if they are not?
Worst case scenario
SAGE – the UK Governments scientific advisory group for emergencies – have been accused of scaremongering, and only presenting worst case scenarios for COVID19 hospital admissions and deaths. They are not the only ones. This is a worldwide phenomenon.
However, as Sir Patrick Vallance – one of the key members of (SAGE) – has stated, in response to such criticism.
‘It’s not my job to be an optimist’: Sir Patrick Vallance takes swipe at critics accusing scientists of scaremongering over Covid saying ministers need to ‘hear the information whether uncomfortable or encouraging.’ 16
SAGE believe it is their role to highlight the worst possible scenarios, the highest possible death tolls, and such like. So, let us now do the same, and focus on the worst-case scenario regarding mRNA vaccines and myocarditis. Whether ‘uncomfortable or encouraging’.
The worst-case scenario starts like this. If the VAERS system only picks up one per cent of vaccine related adverse effects, this means that we can start by multiplying the JAMA figures by one hundred.
Thus, instead of fifty-six cases per million, the reality is that we could be looking at five thousand six hundred cases per million, post-vaccination. Or very nearly one in two hundred.
If, in this model, we then include the possibility that post-vaccination myocarditis is as damaging as post-viral infection myocarditis, it means that one in four hundred eighteen to twenty-four-year-olds could be dead five years after vaccination.
Do I think that this is likely? I have to say that no, I don’t, really. Although this is where the figures, such as they can be relied upon, inevitably take you. Just to run you through the process a bit more slowly.
- Relying on the VAERS system, JAMA reported a thirty-three-fold increase in myocarditis post COVID19 vaccination. An increase from 1.76, to 56.31 cases per million (in the seven-day period post vaccination)
- It has been established that VAERS may pick up only one per cent of all vaccine related adverse effects
- Therefore, the actual number could be as high as five-thousand six-hundred cases per million ~ 1 in 200.
- Myocarditis (post viral infection) has a mortality rate of 50% over 5 years. So, we need to consider the possibility that post-vaccination myocarditis will carry the same mortality.
- Therefore, the rate of death after five years could be one in four hundred (males aged 18-24)
There are approximately sixteen million men aged between eighteen and twenty-four in the US.
Total number of deaths within five years (men aged eighteen to twenty-four in the US)
16,000,000 ÷ 400 = 40,000
(Divide by five for the UK) = 8,000.
Now, if I were in charge of anything, which I am not, which is probably a good thing, I would hope to have been made aware of these worst-case scenario figures. I would then immediately have begun to do everything I possibly could to verify them.
For starters I would want to know two critical things:
1: Is the VAERS system truly only picking up one per cent of vaccine related adverse effects?
2: Does vaccine related myocarditis lead to the same mortality and morbidity as caused by a viral infection?
If the answer to both of these questions were, yes, then I would have to decide what to do. And that could not possibly, be nothing. At least I would hope not. Yet, nothing appears to be exactly what is currently happening.
As you can tell, I still cling to the concept of ‘first do no harm.’ Today, with COVID19, it seems this this idea has become hopelessly naïve. The current attitude seems to be. ‘We are at war; you must expect casualties’ ‘Also, careless talk costs lives.’ So, my friend, I advise you to keep your ‘vulnerable’ mouth shut, if you know what is good for you.’
Well then, I just hope for everyone’s sake, that these figures are completely wrong. They are, after all, only a model. A worst-case scenario created using the most accurate information available at this time. However, as per the SAGE underlying philosophy, I believe it is important to present the information whether uncomfortable or encouraging.
The thing that concerns me the most is that we have a worrying signal emerging about the mRNA vaccines. A signal surrounded by a lot of noise, admittedly. Yet, the ‘official’ response continues to be to sweep the entire thing under the carpet. ‘Nothing to see here, move along.’
Postscript
As with regard to the GMC, and the threat of sanctions, as you can see, I am only following their guidance
‘Healthcare professionals must also be open and honest with their colleagues, employers and relevant organisations, and take part in reviews and investigations when requested. They must also be open and honest with their regulators, raising concerns where appropriate. They must support and encourage each other to be open and honest, and not stop someone from raising concerns.’ 17
What do you do if it is the GMC itself that may be stopping someone from raising concerns. Should I report the GMC to the GMC? I imagine they will find themselves innocent of any wrongdoing. Quis custodiet Ipsos custodes?
1: https://www.pulsetoday.co.uk/news/breaking-news/gps-who-criticise-covid-vaccine-on-social-media-vulnerable-to-gmc-investigation/
2: https://europepmc.org/article/MED/2154621
3: https://www.sciencedaily.com/releases/2015/05/150521133628.htm
4: https://www.bbc.co.uk/news/health-55056016
5: https://pubmed.ncbi.nlm.nih.gov/9737644/#:~:text=In%20conclusion%2C%20these%20studies%20indicate,higher%20doses%20should%20be%20investigated.
6: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC59524/
7: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4740994/
8: https://jamanetwork.com/journals/jama/fullarticle/2788346
9: https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
10: https://wchh.onlinelibrary.wiley.com/doi/pdf/10.1002/psb.1789
11: https://www.ncbi.nlm.nih.gov/books/NBK459259/#:~:text=Immediate%20complications%20of%20myocarditis%20include,and%2050%25%20at%205%20years.
12: https://pubmed.ncbi.nlm.nih.gov/34341797/
13: https://www.cdc.gov/mmwr/volumes/70/wr/mm7035e5.htm
14: https://www.bmj.com/content/373/bmj.n1098
15: https://www.bmj.com/content/bmj/suppl/2021/05/19/bmj.n1098.DC1/daus063716.wt.pdf
16: https://www.dailymail.co.uk/news/article-10341547/Sir-Patrick-Vallance-takes-swipe-critics-accusing-scientists-scaremongering-Covid.html
17: https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/candour—openness-and-honesty-when-things-go-wrong/the-professional-duty-of-candour
February 23, 2022
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, UK |
Leave a comment
Use of Covert Psychological Techniques to Promote Climate Change Dogma
Towards the end of last year, Laura Dodsworth and I complained to Ofcom about a collaboration between Sky U.K. and the Behavioural Insights Team – then part-owned by the Cabinet Office – to use “behavioural science principles”, including subliminal messaging, to encourage viewers to endorse and comply with the Government’s ‘Net Zero’ agenda. That is, Sky bragged about joining forces with a unit that was part-owned by the U.K. Government to use covert psychological techniques to try to persuade viewers to endorse one of the U.K. Government’s most politically contentious policies – and encouraged other broadcasters to do the same! Alarmingly, the joint report by Sky and the BIT also recommended broadcasters utilise these same covert techniques to change the behaviour of children “because of the important influence they have on the attitude and behaviours of their parents”.
In our complaint, Laura and I argued this was a breach of Ofcom’s Broadcasting code – in particular, paragraph 11 of section two, entitled ‘Harm and Offence’:
Broadcasters must not use techniques which exploit the possibility of conveying a message to viewers or listeners, or of otherwise influencing their minds without their being aware, or fully aware, of what has occurred.
Now, two months later, Ofcom has replied, effectively dismissing the complaint. You can read the full reply beneath our original complaint here, but this is the gist of it:
In the Guidance we outline that, among other things, whether an issue has “been broadly settled […] and whether the issue has already been scientifically established” should inform a broadcaster’s consideration of whether the special impartiality requirements in the Code apply to a particular issue. In our Guidance, we identify the scientific principles behind the theory of anthropogenic global warming as an example of an issue which we considered to be broadly settled. On this basis, we do not consider these principles in themselves to be matters of political or industrial controversy for the purposes of Section Five of our Code.
In other words, using covert psychological methods to persuade viewers to endorse climate change dogma and adapt their behaviour accordingly, e.g. switch to electric cars, is not a breach of the Broadcasting Code because the science of anthropogenic global warming is “broadly settled” and “scientifically established”.
What about the fact that many of the behavioural changes Sky is trying to persuade viewers to make also happen to be changes the current Government is promoting under the banner of ‘Net Zero’? On that point, Ofcom is slightly more ambivalent, leaving the door open to another complaint:
The U.K. Government’s position on net zero covers a wide range of policy areas around which there may be a degree of controversy. Policies on how governments deal with crises or controversies in general can be a “matter or major matter of political controversy or relating to current public policy”, even if the U.K. Government has a settled policy position on it. It is possible, depending on the specific content and context, that a broadcast programme containing discussion of specific net zero policy decisions by the UK Government may engage Section Five of the Code, and require consideration under the special impartiality rules.
Ofcom goes on to say that it has raised our complaint with Sky, but has been assured by Sky’s response, and for that reason, among others, won’t be taking our complaint any further:
Turning to your complaint, you did not identify any specific programmes broadcast by Sky which you considered to be in breach of the Code. As I have explained, Ofcom is a post-transmission broadcast regulator and as such, does not usually consider general complaints about a broadcaster’s policies. On this occasion, we drew Sky’s attention to your complaint. Sky has assured us that they retain full control of all editorial broadcast content on their channels, and they are aware of their obligations under the Code.
It is also important to note that, broadcasters have the editorial freedom to analyse, discuss and challenge issues across the board, including topics related to net zero policies. As set out above, a broadcaster’s right to freedom of expression can only be subject to restrictions which are in pursuit of legitimate aims, in accordance with the law, necessary, and proportionate. We must exercise our regulatory functions in a way which is compatible with those rights, and in line with our regulatory principles.
For these reasons, in light of the assurances given by Sky, and in the absence of a complaint about specific broadcast content, there are no grounds for opening an investigation into Sky’s editorial policies and general organisational strategy related to net zero carbon emissions under the Code.
Accordingly, we will not be taking any further action in relation to the general matters which you raised with us about Sky. However, if you do wish to make a complaint about a specific programme that you consider raises issues under the Code, then you can do this by submitting a complaint on Ofcom’s website.
Disappointingly, at no point does Ofcom address our concern about Sky’s use of covert psychological techniques to prosecute its green agenda or its intention to use these methods to bend the minds of children.
Needless to say, Laura and I have no intention of letting the matter drop. If you see a programme on Sky that you think uses covert psychological methods to brainwash you (or your children) into accepting ‘Net Zero’ gobbledegook please bring it to our attention by emailing us here.
You can subscribe to Laura’s Substack newsletter here.
February 23, 2022
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular | Ofcom, UK |
Leave a comment
After maneuvering Russia into choosing either (1) to permit the U.S. to install its missiles, bases, troops, tanks, and weaponry along Russia’s border in Ukraine or (2) to invade Ukraine to prevent that from happening, President Biden, the Pentagon, and the CIA are now responding to Russia’s choice of (2) by imposing brutal sanctions on the Russian people.
Oh sure, they are making out like the sanctions are targeting Russian President Putin and the Russian “elites” in the government that are supporting the invasion. But that’s just another lie. In fact, the sanctions are designed to do the same thing as the sanctions against Iran, Cuba (i.e., the embargo), North Korea, China, Iraq, Afghanistan, and elsewhere. They are designed to squeeze the Russian people with impoverishment and even death in the hope that they will protest and cause Russian President Vladimir Putin to change course or even violently revolt against Putin’s regime.
Of course, never mind that some protestors are likely to get killed or that a revolution would mean thousands of deaths. That never matters to U.S. officials. What matters is the political goal they are striving to achieve with their sanctions. Any number of foreigners who get killed in the process of trying to achieve that goal is entirely acceptable. That’s why, for example, U.S. Ambassador to the UN Madeleine Albright exclaimed that the deaths of half-a-million Iraqi children from the sanctions on Iraq were “worth it.”
The first thing that must be recognized is the fundamental evil of targeting innocent people with death and impoverishment as a way to achieve a political goal. Isn’t that why we condemn terrorism? Where is the moral justification for targeting the Russian people with death and impoverishment simply because their government is doing something that is illegal or unjustifiable?
The problem is that the American people have become so accustomed to sanctions and embargoes as a foreign policy tool that they unable to recognize the evil on which they are based. But the fact is that sanctions and embargoes are no different in principle from terrorism, in that they both target innocent people with death and suffering as a way to achieve a political goal.
The second thing that must be recognized: Sanctions don’t achieve their political goal, which means that the death and suffering they inflict is useless.
Consider the 60-year embargo on Cuba. It was intended to oust Fidel Castro from power and, after he died, to oust Cuba’s communist regime from power and replace it with another pro-U.S. dictatorship. It still hasn’t achieved its goal, notwithstanding the death and suffering it has inflicted on the Cuban people for six decades.
Consider the brutal system of sanctions on Iraq. It contributed to the deaths of hundreds of thousands of children — yes, children! — and it still did not succeed in ousting the Pentagon’s longtime partner and ally, Saddam Hussein, from power.
Consider the brutal sanctions against Iran. U.S. officials have targeted the Iranian people with death and suffering in the hope that they will rise up and oust Iran’s anti-U.S. regime and replace it with with another pro-U.S. dictatorship, similar to that of the Shah of Iran, who the CIA installed into power with a coup in 1953. Despite the death and suffering among the Iranian people, Iran’s theoretic ‘dictatorship’ remains in power.
Third is a point that Biden’s, the Pentagon’s, and the CIA’s Operation Mockingbird assets in the mainstream press just don’t get or don’t care about: U.S. sanctions imposed on Russia and other countries constitute a direct infringement on the liberty of the American people.
Under principles of liberty, people have the right to trade with whomever they want and to travel wherever they want. Those are fundamental, natural, God-given rights that no government, not even the U.S. government, can legitimately infringe.
Yet, that is precisely what U.S. sanctions do. They contribute to the destruction of our own rights and liberties at the hands of our own government.
Thus, we have the spectacle of the U.S. national-security establishment, through its NATO machinations, making Russia one of its official enemies, then cornering Russia into invading Ukraine (versus permitting U.S. missiles, bases, tanks, and troops to be established on Russia’s border), and then using this manufactured crisis to further destroy the rights and liberties of the American citizenry.
Our ancestors warned us about this type of thing. That’s why they called into existence a limited-government republic and rejected the national-security state form of governmental structure under which we now live. That’s why there was no Pentagon, military-industrial complex, CIA, or NSA for the first 150 years of American history. George Washington and Thomas Jefferson warned us against “entangling alliances,” such as NATO. John Quincy Adams, in his 1821 speech “In Search of Monsters to Destroy,” explained the reasons for America’s founding foreign policy of non-interventionism into the affairs and crises of foreign nations.
An updated warning came in President Eisenhower’s Farewell Address where he pointed out that the “military-industrial complex” posed a grave threat to the freedom and democratic processes of the American people. His warning was followed by that of President Kennedy, the last president who was wiling to stand up against the overwhelming power of the national-security establishment. Kennedy’s warning was followed by that of former President Truman, who, thirty days after JFK was killed, pointed out that the CIA had become a sinister force in American life.
It’s time for Americans to do some serious soul-searching. The question should not be what to do about Russia’s invasion of Ukraine. The big question to be discussed and debated shoud instead be: Should America restore its founding systems of a limited-government republic and a non-interventionist foreign policy and get America back on the road toward liberty, peace, prosperity, and harmony with the people of the world?
February 23, 2022
Posted by aletho |
Civil Liberties, Timeless or most popular, War Crimes | Human rights, Sanctions against Iran, United States |
Leave a comment
Today I’m publishing the first draft of a guide I’ve prepared to help with all the Covid hospitalization problems, based on my legal and practice experience dealing with clients and help-seekers from all over the country. The guide is meant to be studied BEFORE you get to the hospital, and provides suggestions for folks who are already hospitalized.
I hope this helps save someone’s life.
This is a first draft. I will be refining and expanding this guide, and will post subsequent versions when they are available. If you have any suggestions for improvements to the guide, post them in the comments.
The single most common call we are getting in our office these days is the scenario where a loved-one has been admitted to the hospital, diagnosed with SARS-CoV-2 infection, often attached to a ventilator, and has become concerned about their course of treatment. In many cases the hospitals have refused to release the patient, citing their unstable condition, meaning that at some point, it can become impossible to get off the Covid express.
The most common complaints we get include that patients are being pressured to accept Remdesivir, have been given Remdesivir even though they objected to it, or the hospital will not administer alternative widely-used treatments even though the patient is in critical condition where side effects are less risky than imminent death. I have personally seen hospitals spend tens of thousands of dollars on lawyers to keep patients in their facility.
Here are some suggestions, starting with the time before admission. You should read this now and you might want to bookmark it for later. It could save your life.
## Common Suggestions
[1] Document everything when working with a hospital. Keep or make all paperwork. Take pictures and video of everything. Be organized.
[2] Determine whether you are in a one-party consent or two-party consent state for recordings, and then record meetings with hospital staff. If in a two-party state, you must notify the other party they are being recorded or it may be a felony. Record everything. One option for notice is to just put up a handwritten sign near the patient’s bed notifying folks that recordings are being made for quality assurance. Obviously document the existence of the sign.
[3] Keep a log of the names of all hospital staff involved in the patient’s care.
[4] Before getting anywhere near the hospital, or as soon as you read this if in the hospital, you MUST complete a medical health surrogacy form. This will legally designate the person who can direct your care if you become unable to do so.
Here’s the example form for the State of Florida: http://www.myfloridalegal.com/desigsurrogfaq.pdf
Do some googling for your area.
[5] If you’re in the hospital, or are considering admission, request a copy of the hospital’s current Covid protocol IN WRITING.
[6] Allied doctors have suggested that if you are in the hospital for Covid treatment, the things to focus on are the optimal use of anticoagulants, steroids, and the inpatient setting, meaning the overall day-to-day care (hydration, bedsore prevention, nutrition, etc.).
[7] Consider researching whether you want to receive glucose (sugar water) at all, since some studies suggest this can worsen Covid outcomes. This may be particularly important for diabetics and pre-diabetics. If not, make your wishes known in writing as described above.
[8] If any treating staff — nurses or doctors — make disparaging comments about your vaccination status, directly or indirectly, consider immediately instructing the hospital in writing that person may NOT be involved in your care.
[9] Always remember the old saw about catching more flies with honey. Hospital staff are stressed and unhappy about Covid; I know of many who feel they cannot speak or act freely out of fear of professional reprisal. So the nurse or doctor that you think is an opponent may in fact be an ally willing to help wherever possible, but having to parrot the party line in the meantime. Never show anger or frustration. Keep it together. This is important.
## Emergency Room
The most common scenario that we are hearing is that folks go to the ER for Covid infection and are sent home without treatment if the symptoms aren’t serious enough, and then later are admitted after the patient’s condition has worsened to the point they require hospitalization. An increasing number of reports include folks who go to the ER for a separate reason and wind up testing positive in the ER, or become positive after admission — then get bunged right into the Covid ward and — boom! — they’re on the Covid express.
[1] If you test positive in the ER, whether you were there FOR Covid or for a different reason, and are told you will be admitted, ask about at-home care alternatives. Most corporate hospitals do NOT have home-care protocols. I’ve listed websites below that provide information about alternatives for home treatment. With a little effort, you can find a local doctor or community hospital who will arrange and oversee at-home oxygen if needed.
Ask about the hospital’s Covid protocol BEFORE you agree to be admitted. Is it based on remdesivir and the ventilator? If so, you may want to review the literature on those two treatments before you agree.
[2] If you’re in the ER for a non-Covid critical condition but test positive, you’ll be admitted to the Covid ward. See the notes below, and consider discharging yourself for at-home Covid care the instant your primary issue has been stabilized.
## Pre-Surgery
If you are going in for a non-Covid-related surgery, be aware that nosocomial (hospital-acquired) Covid infections appear to be very common. In other words, even though you are there to have your appendix out, the hospital is going to start testing you for Covid about every ten seconds from the time you arrive until discharge. If you test positive, you’ll be on the Covid express before you know what happened.
It doesn’t matter whether you’ve been vaccinated. You can still test positive and will be treated for Covid infection.
You need to consider this risk in planning your surgery. If you test positive but don’t want remdesivir or ventilation, you need to make that clear in WRITTEN INSTRUCTIONS provided to the hospital IN ADVANCE of your surgery. They need to be part of your medical record. Otherwise you could be on remdesivir even before you come out of anesthesia.
Some people may not have options because of insurance constraints and so forth. Explore your options. And if you DO have options, consider whether your surgery would be better handled in a facility where they don’t also provide Covid treatment, in order to reduce the risk of Covid hospitalization.
Finally, can your surgery be safely deferred? Don’t defer necessary surgery unnecessarily. But if you can wait, that might be a good idea.
## Early Interventions (post-admission)
This section applies to folks or their loved ones who are in the hospital with a Covid diagnosis but remain conscious.
[1] If you haven’t yet received Remdesivir, and DO NOT want it, state that in writing and give it to your doctors. Post a copy by your hospital bed.
[2] If you DO NOT want to be placed on a ventilator, state that in writing and give it to your doctors. Post a copy by your hospital bed.
Be prepared for the hospital to try, hard, to change your mind about those two treatments. This pressure may come when you are weakest. Be ready.
[3] Many people believe that Covid is best treated at home. Your circumstances may vary. Get an opinion from a telemedicine specialist in at-home Covid care like www.jamesclinic.com, or consult www.myfreedoctor.com.
Other online places to check include: aapsonline.org, AFLDS.com, https://covid19criticalcare.com (FLCCC), and GlobalCovidSummit.org.
[4] If you decide that you prefer to treat your Covid at home, or can find a non-corporate independent clinic somewhere that will accept you, discharge yourself. If the hospital pushes back on discharge, you may need to discharge yourself “Against Medical Advice,” or AMA. Ask if your hospital has its own form, otherwise google one.
## Late Interventions
In this section, the patient is no longer conscious or capable of directing their own care. Many times these patients are, unfortunately, already on the ventilator. Therefore relatives or a surrogate are making decisions for the patient. Many patients in this condition are essentially just waiting to die.
[1] If you are concerned about the quality of care, immediately get the hospital’s “Patient Advocate” involved. Most hospitals have one.
[2] Get a second opinion. You’ll need to find a local independent doctor to provide a second treatment opinion. Obviously you will need a doctor who specializes in Covid treatment. You should request the doctor be allowed to evaluate the patient even if they lack admitting privileges for purposes of a second opinion. Request that the doctor be permitted to participate in patient conferences even if by phone.
[3] If at all possible, arrange for someone to be in the room with the patient at all times to ensure consistent high quality of care. At ALL times. Do it in shifts. Even in the middle of the night. Things can happen over the night shift. This person should be checking hydration levels and conferring when possible with nurses and doctors assigned to the patient.
[4] Advocate continually for alternative treatments (iv.mectin, fluvoxamine, and/or monoclonal antibody treatments), if approved by the outside physician.
[5] Some people have successfully arranged to have alternative treatment providers see the patient; or have managed transfers to other hospitals with more flexible Covid treatment, specialized clinics, or even at-home treatment. You may have to insist on the patient being discharged AMA.
[6] Right-To-Try. Consider drug treatments still in clinical trials with right-to-try programs. You MUST use the magic words “I am requesting this against medical advice,” or the hospital will usually reject or ignore your request. Note that iv.mectin and fluvoxamine are APPROVED drugs and are excluded from right-to-try.
For example, one drug in this category that has been frequently mentioned is Zysemi. See (https://tinyurl.com/2p84528z).
[7] You might want to familiarize yourself with successful hospital protocols from 2020, like placing ventilated patients on their stomach.
[8] Your primary goal is to wean the patient off the ventilator. The longer they are on the ventilator, the more likely it is that their condition will continue to deteriorate. Once off the ventilator, you can transition to at-home care.
## Legal Options
[1] Court Options. Court options are limited, and expensive, but have worked in some places. Laws vary widely state-by-state. In Florida, the applicable law is Probate Rule 5.900, which provides for an emergency hearing about patient treatment within 72 hours. My suggestion is that the Court be asked ONLY that the patient (a) be allowed to be treated by the outside physician, or (b) that the patient be released AMA.
As an example, here is a link to Florida Rule 5.900: (https://tinyurl.com/2p8hm8kx).
Your lawyer should carefully consider that asking a Court to order administration of iv.mectin is a risky ask. There have been some successes with this approach, but also many, many failures. Courts have wide latitude in what they can do (or not do) in these situations. Adding a controversial drug into the equation makes the case significantly harder, and since judges are people too, the judge’s preconceived notions about iv.mectin will be a factor. You do NOT want to get into a giant evidentiary battle over the efficacy of iv.mectin.
In other words, simpler and less intrusive requests are more likely to be granted by the Court.
[2] Police Reports. If the patient was given Remdesivir against instructions, that may be a battery, and you might want to consider filing a police report against the hospital and involved staff. If the patient passed away, the stakes are even higher. Although it is hard to say whether the police report will amount to anything, it may be very helpful documentation later. Obviously, provide the police with all paperwork and evidence that you have and keep a file copy of the police report.
I hope this helps. These cases are the worst, most heart-breaking cases I have ever handled in my career. The stakes are literally life-and-death. I don’t mean this guide to be critical of well-meaning doctors and nurses in corporate hospitals — many, if not most are heroic professionals who want the best for patients. Unfortunately, the incentives (e.g. government payments to hospitals) are totally perverse.
Finally, remember that you are not alone! There are more and more advocacy groups forming to help people trapped in hospitals receiving ineffective or harmful treatment. But time is short. The best defense is a good offense; be prepared BEFORE you reach the emergency room.
DISCLAIMER: This is not medical advice. I’m a lawyer, not a doctor. You should always follow the advice of a trusted physician and make your own independent decisions about your healthcare, especially when it is critical. This guide is presented only as an outline to help inform you about options that may be available.
February 23, 2022
Posted by aletho |
Civil Liberties, Timeless or most popular | Covid-19, Human rights, United States |
Leave a comment
While the decision to eliminate President Kennedy undoubtedly took place after his resolution of the Cuban Missile Crisis, it was without a doubt solidified when Kennedy ambushed his enemies within the U.S. national-security establishment with his Peace Speech at American University on June 10, 1963. With his Peace Speech, JFK was upsetting the Cold War apple cart that the Pentagon and the CIA were convinced would last forever.
What was so significant about that speech?
After the end of World War II, the U.S. government was converted from its founding system of a limited-government republic to a governmental structure called a national-security state. The justification for this radical change, which was accomplished without even the semblance of a constitutional amendment, was that the United States now faced an enemy that was said to be even more threatening than Nazi Germany. That new enemy was “godless communism” as well as a supposed international communist conspiracy to take over the United States and the rest of the world — a conspiracy that was supposedly based in Moscow, Russia — yes, that Russia!
With the conversion to a national-security state, the U.S. government acquired many of the same totalitarian powers that were being wielded by the totalitarian communist states, such as the Soviet Union and Red China — powers that had been prohibited when the government was a limited-government republic. Such powers included state-sponsored assassinations, torture, kidnapping, indefinite detention, and coups.
Equally important, the Cold War brought ever-increasing taxpayer-funded largess flowing into the coffers of the “defense” industry, along with the ever-increasing power and influence of the Pentagon, the CIA, and the NSA within the overall federal structure. Over time, the national-security branch of the federal government would become the most powerful branch, the one to which the other three would inevitably defer.
After the Cuban Missile Crisis, Kennedy achieved a breakthrough, one that threatened not only the ever-increasing power, money, and influence of the national-security branch, but also its very existence. Kennedy came to realize that the Cold War was just one great big racket — and a highly dangerous one at that.
That danger was manifested during the Cuban Missile Crisis. U.S. officials and their loyalists in the mainstream press have always maintained that the crisis was brought on by the Soviet Union and Cuba. Not so! It was brought on by the Pentagon and the CIA. It was those two entities that brought the world to within an inch of all-out nuclear war.
The Soviets and the Cubans knew that the Pentagon and the CIA wanted to invade Cuba and effect a regime-change operation there, one that would oust Cuban leader Fidel Castro from power and replace him with another pro-U.S. dictator, similar to Fulgencio Batista, the corrupt pro-U.S. brute that ruled Cuba before the revolutionaries ousted him in 1959.
That was why the Soviets installed those nuclear missiles in Cuba — to deter U.S. officials from attacking or, if deterrence failed, to enable Soviet and Cuban forces to defend themselves from a U.S. attack.
There is something important to note about the invasion that the Pentagon and the CIA wanted Kennedy to initiate against Cuba: It was illegaL The U.S. had no legal right to invade the island either before the crisis or during the crisis.
What was the justification for invading Cuba before the Cuban Missile Crisis? They said that because Cuba was befriending the Soviet Union, that constituted a grave threat to U.S. national security. But the fact is that under international law, Cuba had the right to befriend anyone it wanted. Its decision to befriend the Soviet Union did not constitute legal justification for invading the island and effecting regime change there.
What about during the crisis? Well, here is where the irony appears with respect to what it happening in Ukraine today. Throughout the crisis, the Pentagon and the CIA were pressuring Kennedy to bomb Cuba and follow up the bombing with a ground invasion. Their position was that America could not permit the Soviet Union to install nuclear missiles pointed at the United States from only 90 miles away.
But the fact is that Cuba was a sovereign and independent regime. Under international law, it had the authority to invite the Soviet Union to install whatever missiles it wanted on the island.
But from a practical standpoint, U.S. officials said no — that the United States would not permit Soviet nuclear missies to be installed so near to America’s borders. Obviously, it is a rather ironic position, given that that’s precisely why Russia today does not want Ukraine to be admitted into NATO, which would enable the Pentagon and the CIA to install their nuclear missiles pointed at Russia on Russia’s border.
Kennedy had a unique ability to put himself into the shoes of his opponent in order to figure out a satisfactory resolution to a crisis. He figured out that if he pledged that the U.S. would not invade Cuba, the Soviets would not need to keep their missiles in Cuba. Thus, after tense negotiations, that was the deal that he struck with Soviet leader Nikita Khrushchev — except for one thing.
It turned out that the Pentagon had U.S. nuclear missiles stationed in Turkey that were pointed at the Soviet Union. Yes, you read that right: The Pentagon’s position was that it was okay for the Pentagon to have U.S. nuclear missiles pointing at the Soviet Union in a country bordering the Soviet Union but it was not okay for the Soviet Union to have missiles pointing at the U.S. in a country 90 miles away from America’s borders.
Unlike President Biden, who would never think of bucking the Pentagon and the CIA, Kennedy saw the hypocrisy of that position. He secretly agreed with the Soviets that he would quietly withdraw the missiles from Turkey later on.
The crisis was over. The U.S. would not invade Cuba. The Soviets withdrew their missiles. Kennedy withdrew the U.S. missiles from Turkey six months later.
But the Pentagon and the CIA were livid. They considered Kennedy’s resolution of the crisis to be the “biggest defeat in U.S. history.” Those were the words of Gen. Curtis LeMay, chief of staff of the Air Force. During the crisis, LeMay compared Kennedy’s handling of it to Neville Chamberlain’s appeasement of Hitler at Munich.
Why was the national-security establishment so filled with rage? Because Kennedy essentially agreed that Cuba would remain permanently under communist rule and, even worse, headed by a regime that would continue befriending the Soviet Union. In other words, in their eyes, with his agreement with the Soviets, Kennedy had ensured that Cuba would pose a permanent grave threat to U.S. national security.
By the time the missile crisis was over, however, Kennedy had achieved his breakthrough. Determined to bring an end to the national-security establishment’s Cold War, Kennedy went to American University and essentially declared an end to the Cold War racket. He announced that from that day forward, the United States would live in peaceful and friendly coexistence with the Soviet Union and the rest of the communist world. Reflecting his new vision for America, he entered into a nuclear test-ban treaty with the Soviets, ordered a withdrawal of U.S. troops from Vietnam, and proposed a joint trip to the moon with the Soviets. At the moment he was assassinated, he had an emissary meeting with Fidel Castro, while the CIA was conspiring to commit yet another assassination attempt against Castro without JFK’s knowledge or consent.
After JFK’s Peace Speech, the war between him and the U.S. national-security establishment over the future direction of the United States was on. There could be no compromise. There was going to be a winner and a loser. Kennedy’s enemies in the national-security establishment hated him for what he was doing. In their eyes, this neophyte, incompetent, naive, womanizing president was leading America to a communist takeover of the United States. In their eyes, what Kennedy was doing as president, after all, constituted a much graver threat to national security than President Arbenz in Guatemala, who the CIA had violently ousted in a coup in 1954 because Arbenz, like Kennedy, was befriending the Soviet Union and the communist world. (See FFF’s book JFK’s War with the National Security Establishment: Why Kennedy Was Assassinated by Douglas Horne, who served on the Assassination Records Review Board in the 1990s.)
Take a look at this advertisement in the Dallas Morning News on the morning of JFK’s assassination. And then take a look at this flier that was being circulated in Dallas on the day of his assassination. The sentiments expressed in those two documents reflected the views of the U.S. national-security establishment. In their eyes, Kennedy was a cowardly traitor whose policies of appeasement were leading America to doom.
They knew that it was a virtual certainly that Kennedy would win the 1964 election. They also knew that he would never permit them to go into the Middle East and begin killing people, thereby producing terrorist blowback that would justify a perpetual “war on terrorism” to replace the “war on communism.”
They knew that if Kennedy’s vision were to prevail, the national-security establishment would have nothing to do. With no big official enemy, they would be left twiddling their thumbs. People would begin wondering about all that taxpayer-funded largess flowing into the “defense” industry. Even worse, the American people might begin demanding the restoration of their founding governmental system of a limited-government republic.
But as we all know, Kennedy’s vision did not prevail. He lost the war against his enemies within the military and the CIA when they killed him just 5 1/2 months after his Peace Speech. His assassination elevated to the presidency Lyndon Johnson, whose Cold War mindset matched that of the Pentagon, the CIA, and the NSA. The taxpayer-funded largess continued flowing into the coffers of the “defense” industry. The war on communism was ultimately replaced by the war on terrorism. And now, with its NATO machinations in Eastern Europe, the national-security establishment has succeeded in achieving Cold War II.
Who says the Kennedy assassination isn’t relevant today?
February 22, 2022
Posted by aletho |
Militarism, Timeless or most popular | CIA, JFK Assassination, United States |
Leave a comment

Historically, the claim of consensus is the first refuge of the scoundrel; it is a way to avoid debate by claiming the matter is already settled. Whenever you hear the consensus of scientists agrees on something or other, reach for your wallet, because you’re being had. Let’s be clear: the work of science has nothing whatever to do with consensus. Consensus is the business of politics.
Michael Crichton, PhD, MD, author, screenwriter and academic
Humans cause all or most of the changes in the climate by burning fossil fuel. We must stop using the most efficient fuel we have, one that supplies 85% of our energy needs, and sign up for a so-called Net Zero future. The rich will get richer, since they will control state-mandated transfers of once-productive capital into new untried technologies, and the poor will get poorer. Holidays, personal travel and energy will be rationed (for the masses), while meat-free diets will be the order of the day. There are disadvantages, admit the green, politically motivated zealots, but it has to be done. The Earth is on fire – the science is settled.
Except that it isn’t. The idea that humans are largely responsible for climate change is an unproven hypothesis. The claim that it is ‘settled science’ on which all specialists in the field agree is a political con. Over 40 years, climate models have produced wildly inaccurate warming forecasts that have never been right.
The political narrative of global warming got going in the 1980s, following the failure of the 1970s global cooling scare. The warming narrative had a good ride for 15 years, until the recent warming started to run out of steam. Over the last seven years, there has been a standstill in temperatures. This is part of what lies behind the recent rebranding of bad weather as ‘extreme’, and unscientific attempts to link solo events to long-term aggregate climate change. Record high temperatures among the jet aircraft at Heathrow, record “gusts” of wind off isolated sea cliffs – all are used to craft a political Armageddon narrative.
At the heart of the debate, or rather the public non-debate, is the role of carbon dioxide as a warming gas. CO2 does warm the planet and the Earth would be about 33°C cooler without it and the other greenhouse gases. But its warming properties become less effective as more of it enters the atmosphere. Doubling atmospheric CO2 does not double the warming – a point which the IPCC accepts. Climate models guess that such doubling causes global temperature to rise in a range from 1.5°C to 6°C. Recent scientific work suggests this estimate is way too high. The simple ‘settled’ science deduction that rising CO2 levels automatically lead to significantly higher temperatures fails to take much account of natural climatic variations. In addition, little cause and effect between CO2 and temperature can be seen in current, historical or geological records.
CO2, methane and ozone, along with the much more common water vapour, produce a greenhouse effect of reflecting heat back to the Earth only within certain bands on the infrared spectrum. This has led some scientists to suggest that CO2 becomes ‘saturated’ once it reaches a certain level. Most of the heat that is going to be trapped is already being radiated back by the CO2 molecules evenly distributed in the existing atmosphere.
It is fascinating science, but it is conducted away from mainstream media, most political circles and the Earth Sciences/Geography university departments. It is the last that seem to provide many of the vocal scientists promoting the ‘settled science’ narrative. Such ground-breaking work holds out the promise of a better understanding of the role of CO2 in the atmosphere. Only a blinkered following of a political agenda can explain why it is ignored.
The idea that the science surrounding changes in the climate is settled goes back a long time. In 2006, the BBC ran a one day seminar in secret to decide on its future climate editorial policy. The meeting was crucial in plotting future editorial guidelines. According to the former Sunday Telegraph journalist Christopher Booker, the new guidelines “would allow it to make its coverage of any issues relating to climate change more actively partisan than ever”. Booker continued: “Its obligations to remain impartial could be put aside, it argued, on the grounds that the official orthodoxy was now so overwhelmingly accepted that any dissent from it could be dismissed as too insignificant to be worthy of notice.”
In 2013, John Cook came up with the suggestion that 97% of scientists believed that humans cause global warming. Mr. Cook is a green activist, who runs a site called Skeptical Science with the intriguing strapline: “Getting sceptical about global warming scepticism”. His notion was given a huge boost when Barack Obama tweeted that 97% of scientists agree that climate change is “real, man-made and dangerous”. In fact the 97% figure, which is still widely quoted today, was quickly debunked. It was found that of the 12,000 abstracts rated, only 0.5%, or 65 papers, suggested that humans were responsible for more than 50% of global warming.
Since scientists differ widely in their view on the human contribution to climate change, the attempt to put a number on a so-called consensus is futile and meaningless. But it makes a good headline. Step forward Mark Lynas, with a recent raise on 97% to 99%. In fact, his study found only that 99% of scientists failed to explicitly quantify the effect humans were having on the climate.
Mr. Lynas has had a lively career in green activism and journalism, first coming to attention in 2001 when he threw a pie into the face of the sceptical climate economist, Bjørn Lomborg. He was behind the PR stunt in 2009 when the Government of the Maldives met under water to draw attention to rising sea levels. Happily, this is not a problem for the Maldives, since overall the islands have grown in recent years. In 2007 he wrote an article in the Guardian reporting on the possibility of global warming producing fuel air bombs caused by oceanic methane eruptions. These would be equivalent to 10,000 times the world’s stockpile of nuclear weapons, he claimed.
These days, Mr. Lynas is the Communications Strategist and Climate Lead for the Alliance for Science, a non-profit operation linked with Cornell University. Its primary source of funding is said to be the Bill and Melinda Gates Foundation – another case, it appears, of following the money to find the billionaires pushing their pet green narratives and causes.
February 22, 2022
Posted by aletho |
Corruption, Science and Pseudo-Science, Timeless or most popular | Gates Foundation |
Leave a comment
The 2020-2022 pandemic split parties and ideologues, separated friend from friend and family members from family members. Neighbors were dangerous, and strangers even more so: the invisible enemy stalking our lands overturned every other concern in life: The conflicts it spurred replaced bonds of affection with fear and hatred.
More than ever, we need calm and level-headed thinkers, honest and willing to admit past errors, with eyes wide open for the corruption of industry or government itself. In other words, we need as little politics as humanly possible. As I wrote in a previous piece: we need “people without a clear ideological position, and who can thus appeal to audiences across the political spectrum.”
Two sane figures recently attempted the impossible: to speak calmly to the other side, trying earnestly to explain what happened – Konstantin Kisin, of the popular show Triggernometry, and Columbia sociology professor Musa al-Gharbi.
Kisin begins his monologue with “You’re struggling to understand why some people are vaccine hesitant. Let me help you.”
He uses no study result, no appeal to the biological effect of the drug that has become the main symbol of the Covid conflict; no death rates or R0; no projection of spread or what number of lives lockdowns may or may not have saved. Instead Kisin, for 13 spellbinding minutes, walks us through the many good reasons that people had – before and during Covid – to distrust the elites in politics, business, and media. If this is a question of (dis)trusting the establishment (including “the” Science), you must ask what the establishment did to no longer deserve that trust.
The tale begins years ago, with the Brexit vote and with the election of Donald Trump. Those events shocked the pompous leaders of the universities, the pollsters who confidently said it wouldn’t happen, the media pundits who so convincingly described to us the madness of such prospects.
For a brief moment after the unthinkable had happened, if you recall, there was an earnest desire for inclusivity – for inviting in the views that had gone overlooked in the other half of these countries. Outlets like the New York Times made an effort to portray conservative views and show the kinds of people who had long felt alienated and ostracized from civilized society. As despicable and difficult it was for their core audience to see, revealing perspectives and objections is better than silencing and hiding them.
The efforts didn’t last long and in 2019 and 2020, the monolithic thoughts that dominate these institutions willingly put their blinders on – tighter and more aggressively than before.
Kisin’s final minute is the most powerful thing in these disease-ridden past two years:
“The same people who told you Brexit would never happen; Trump would never win, and that when he did win, it was because of Russian collusion, then because of racism; that you must follow lockdown rules while they don’t; that masks don’t work and then that they do; that protests during lockdowns are a health intervention; that ransacking Black communities in the name of fighting racism is mostly peaceful justice; that Jussie Smollett was the victim of a hate crime; that men are toxic; that there’s an infinite number of genders; that Covid didn’t come from a lab, and then that it probably did; that closing borders is racist, and then that it’s the most important thing to do; that the Hunter Biden story is Russian disinformation, and then that it’s not; that they would not take Trump’s vaccine, and then that you must take the vaccine; that Governor Cuomo is a great Covid leader, and then that he’s a granny killer and a sex pest; that the number of Covid deaths is one thing and then another; that hospitals are filled with Covid patients, and then that many of them caught Covid in hospital.
These are the same people now telling you that the vaccines are safe, you must take it, and if you don’t you will be a second-class citizen.
Understand vaccine hesitancy now?”
Like Steve Carell’s character says in that glorious scene from The Big Short, “Short everything that guy has touched.” These guys have fooled us once too many times: we will not comply.
The long-read for the British newspaper The Guardian by Musa al-Gharbi is even more important, partly because he speaks to his own side and partly because the piece runs in an outlet that has been heavily on the vaccine-cherishing train. Building bridges begins by showing those on your own side of the river what the land looks like on its far side.
And al-Gharbi perfectly captured the mind of the current skeptic. He lists, bullet-point by bullet-point, the clear and sensible reasons why anyone would refuse to follow along. To most of his audience, these vaccines are fantastic miracles, life-saving devices, their impact ending the pandemic in one fell swoop: “failure to comply with the directives of public health officials,” writes al-Gharbi, has thus seemed insane to the audience he addresses – probably “driven by some pathology or deficit.”
“debates turn around identifying the primary malfunction of ‘those people’: Are they ignorant? Brainwashed? Stupid? Selfish and apathetic? All of the above? Left off the menu is the possibility that hesitancy and non-compliance may actually be reasonable responses to how experts and other elites have conducted themselves, both before and during the pandemic.”
The vaccines were developed too fast, without the long and rigorous testing regimes we usually apply to pharmaceuticals to ensure efficacy, correct dosage, the target demographics, safety, and observation of long-term harm (if those safeguards are optional and superfluous, why do we have them in normal times…?). Both Biden and Harris vocally pushed against “Trump’s vaccine,” but when the power of government passed into their hands, the tune was suddenly very different. Many people smelled a political rat.
Dr. Fauci himself has engaged in noble lie after noble lie to get people to do what he says is crucial for them: if he lied about the masks and then the Wuhan lab financing and then herd-immunity targets, why should anyone believe that he hasn’t lied about more things? That the advice his agency gives out is sound? That the science he says he represents is as all-encompassing and definitive as he and others deferring to him let on?
Step by step, month by month, and variant by variant, writes al-Gharbi, the figures of vaccine efficacy kept dropping:
“the main benefit of vaccination has been revised down dramatically – from outright preventing infections to reducing severe infections – even as people are encouraged to get more and more shots in order to achieve that benefit.”
But the official advice remained, intensified even, as did the public’s discourse. Somehow, the anger against the unvaccinated strengthened.
This is not what we were promised when, in early 2020, we stoically and proudly began sacrificing aspects of our personal lives for the public good. On top of that al-Gharbi points to the billions that Big Pharma makes out of vaccines – a point that should weigh heavily on The Guardian’s readership. And harms stemming from vaccines cannot be pursued in court, as the US government shielded the companies from liabilities in order to speed up the vaccine-creation process.
Add misleading statistics, former MSNBC hosts losing their minds, modeling predictions gone haywire and it isn’t hard to see why many people want to opt out. Something is rotten in the state of Denmark, and the only tangible act of dissent that most people have is refusing a needle in their arm.
In genuine scientific efforts, admits al-Gharbi, people are routinely wrong – that’s how the process works and how the sum knowledge of humanity improves. Instead, in the plague years we received
“spokespeople (and “Trust the Science” stans) [who] regularly concealed uncertainties, suppressed inconvenient information and squashed internal dissent in an ill-conceived effort to seem maximally authoritative. Rather than enhancing confidence among skeptics, these moves often made authorities seem incompetent or dishonest when they were forced to change their positions.”
There are few public officials who haven’t shunned the rules they themselves made, but of course we all shun the rules – they’re impossible to live under. The hypocrisy just looks so much worse when it’s the rulemaker himself or herself doing it. al-Gharbi’s summarizing paragraph is almost as powerful as Kisin’s:
“In a world where the experts are regularly wrong but continue to project high levels of confidence even as they change their minds and update their policies, where elite narratives about the crisis often seem to be inappropriately colored by political and financial considerations, where those who share one’s own background, values and interests do not seem to have a seat at the table in making the rules – and especially among populations that have a long history of neglect and mistreatment by the elite class (leading to high levels of pre-existing and well-founded mistrust even before the pandemic) – it would actually be bizarre to unquestioningly believe and unwaveringly conform to elite guidance.”
This is the story that those skeptical of vaccines see: a dissonance between official words and reality that no amount of social ostracism or edicts from on high can eliminate. This is the story of a tribe of navel-gazing authoritarians imposing rules on the rest of us, rules that don’t make sense, that are routinely flaunted by their proponents, and in aggregate don’t achieve the goals they’re said to achieve.
There is no reason to puzzle about the loss of trust and the rise of grave skepticism about elite plans for our lives.
February 22, 2022
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
The World Economic Forum (WEF), an international organization that works to “shape global, regional and industry agendas,” recently published its latest dystopian proposal – a far-reaching digital ID system that will collect as much data as possible on individuals and then use this data to determine their level of access to various services.
This digital ID proposal is outlined in a report titled “Advancing Digital Agency: The Power of Data Intermediaries” and builds upon a digital ID framework that the WEF has published previously.
Under this framework, the WEF proposes collecting data from many aspects of people’s “everyday lives” through their devices, telecommunications networks, and third-party service providers.
The WEF suggests that this data collection dragnet would allow a digital ID to scoop up data on people’s online behavior, purchase history, network usage, credit history, biometrics, names, national identity numbers, medical history, travel history, social accounts, e-government accounts, bank accounts, energy usage, health stats, education, and more.
Once the digital ID has access to this huge, highly personal data set, the WEF proposes using it to decide whether users are allowed to “own and use devices,” “open bank accounts,” “carry out online financial transactions,” “conduct business transactions,” “access insurance, treatment,” “book trips,” “go through border control between countries or regions,” “access third-party services that rely on social media logins,” “file taxes, vote, collect benefits,” and more.

In this Advancing Digital Agency: The Power of Data Intermediaries report, the WEF positions this digital ID framework as the part of the solution to a “trust gap in data sharing” and notes that vaccine passports, which were mandated across the world during the COVID-19 pandemic, do “by nature serve as a form of digital identity.”
The WEF also praises the way vaccine passports have allowed governments to harvest data from their populations without “notice and consent”:
“At a collective level, vaccine data is an incredible public health asset. The United Kingdom Government in particular has acknowledged this and has suggested that anonymization, pseudonymization and data shielding techniques could be harnessed in a controlled environment to allow for the reuse of that highly sensitive data. In such cases, notice and consent is not required per se for the reuse of the data but the intermediary processes the data undergoes must be done in a controlled environment so that the findings of the data set are made available rather than the data itself.”
Additionally, the WEF provides a specific example of how digital IDs could be used to authenticate a user (by using fingerprints, a password, or identity verification technology) and decide whether they should be granted access to a bank loan by judging their profile (which may include their biometrics, name, and national identity number) and history (which may include their credit, medical, and online purchasing history).
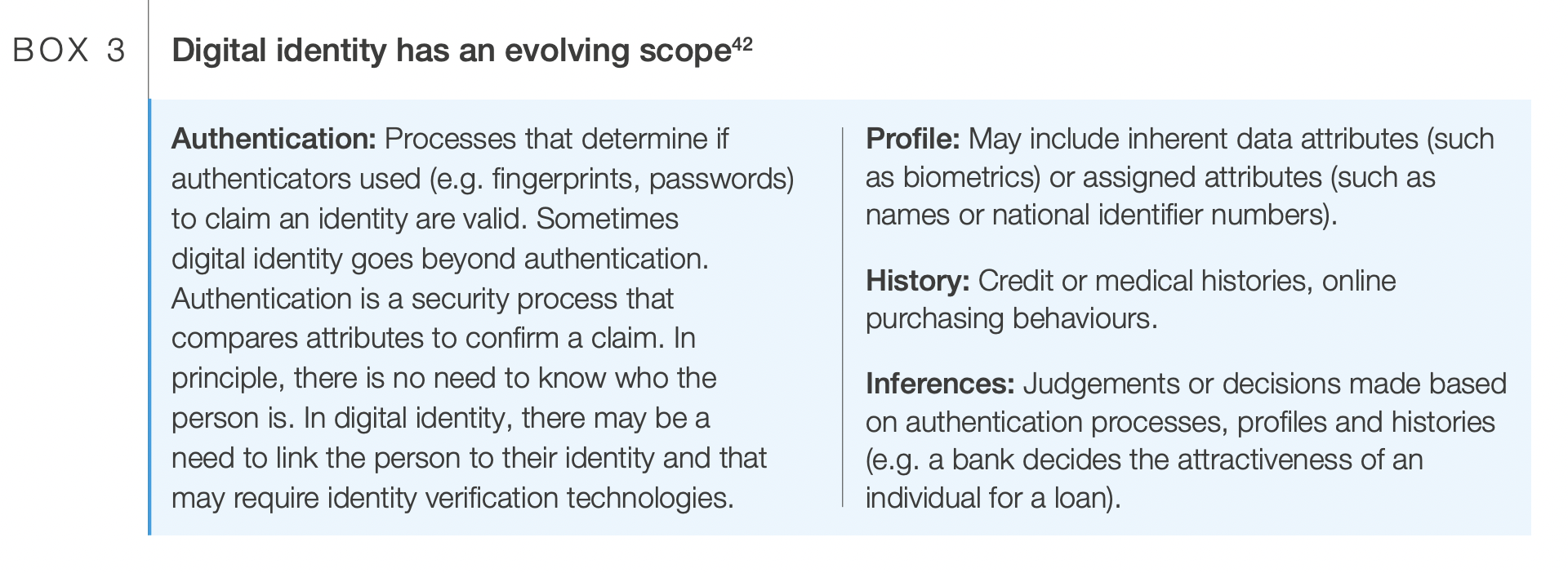
The WEF goes on to suggest that digital IDs will “allow for the selection of preferences and the making of certain choices in advance” and ultimately pave the way for “automated decision-making” where a “trusted digital assistant” “automates permissions for people and effectively manages their data across different services” to “overcome the limitations of notice and consent.”
This push for an invasive digital ID system from the WEF follows it proposing other similar surveillance systems such as turning your heartbeat into a digital ID. Throughout the pandemic, the WEF has consistently advocated for vaccine passports and digital ID.
Beyond these specific proposals, the WEF is infamous for its globalist and transhumanist agendas such as the “Great Reset” (which proposes that people will “own nothing” and “be happy”) and the “Fourth Industrial Revolution” (which, according to WEF founder and chairman Klaus Schwab, will lead to “a fusion of our physical, our digital, and our biological identities”).
Governments and private corporations are increasingly embracing digital IDs. Some governments are also pushing a similar notion – social credit-style apps that monitor citizens’ behavior and reward them for engaging in state-approved actions.
February 22, 2022
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights, WEF |
Leave a comment

 Aletho News
Aletho News
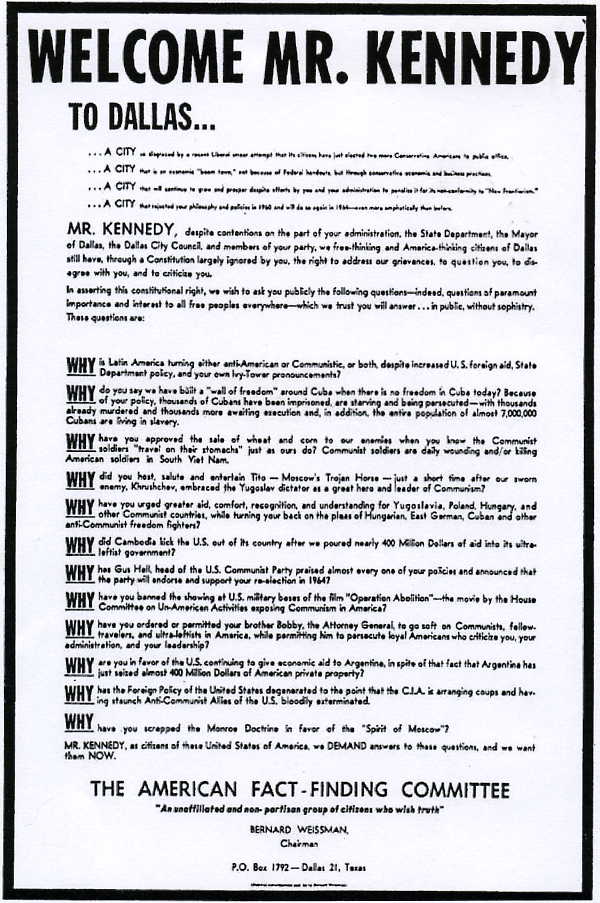{kind=link}
{kind=link}