Belgium has “overwhelming responsibility” for the killing of Prince Louis Rwagasore, the popular Burundian leader who sought to unite the country’s ethnic groups as it gained freedom from the colonial power, new evidence shows.
Weeks after being elected prime minister in a landslide, Rwagasore, the 29-year-old son of a former king, was assassinated in October 1961. The governing Belgian elite masterminded the shooting while Brussels turned a blind eye, according to archived records uncovered by Flemish sociologist Ludo De Witte.
Although the shooter, a Greek national, and five accomplices were executed, De Witte said that probes by the Belgian colonial court, the government of independent Burundi, and the UN all neglected Belgium’s role in the killing, which led to decades of war, ethnic tensions, and instability.
Publishing his findings in a book titled ‘Murder In Burundi’, De Witte noted that then-Belgian governor Roberto Regnier had told a post-election crisis meeting of senior Belgian officials and allies in the Belgium-friendly Christian Democrat party (CDC) that “Rwagasore must be killed.”
According to the author, the CDC saw his words as an invitation. Regnier’s remarks were apparently confirmed by four people at that meeting to a 1962 inquiry by prosecutors in Brussels. But that report had not been published until De Witte unearthed it during a five-year investigation into the murder.
It also appears the UK was at least aware of the danger faced by Rwagasore, with Britain’s then-ambassador James Murray writing in a 1962 dispatch that influential Belgians had “an almost pathological hatred” of the charismatic leader, who they believed would harm Belgian-Burundian relations. Murray noted that Regnier’s “words… go very far in the direction of incitement to murder,” according to De Witte.
The book also accuses then-Belgian foreign minister Paul-Henri Spaak – today celebrated as a founding father of the EU – of ignoring Regnier and other conspirators on a “war footing” with Rwagasore. It also finds fault with King Baudouin, who “moved heaven and earth” to commute the assassin’s death sentence to life imprisonment.
Last October, a special commission into Belgium’s colonial past admitted it paid “limited attention” to Burundi and Rwagasore’s killing. De Witte attributed this to a “reticence” among the country’s elite to “confront the reality” of colonization.
Meanwhile, a Belgian Foreign Ministry spokesperson did not respond to the book’s charges, but told The Guardian that the government was waiting for parliamentary recommendations before adopting a policy position.
During Tony Blair’s time in office, Downing Street allegedly ordered former defence secretary Geoff Hoon to burn a secret memo that questioned the legality of the 2003 Iraq invasion. Hoon makes the bombshell claim in a new memoir.
In disclosures that have boosted ongoing attempts to strip the former prime minister of his recently conferred knighthood, Hoon reportedly revealed that Blair’s chief of staff Jonathan Powell had instructed him “in no uncertain terms” to destroy the legal document.
When reports of the allegation first surfaced in 2015, they were dismissed by Blair as “nonsense.” But Hoon has resurrected the claim in a tell-all book, titled ‘See How They Run’, according to the Daily Mail. The paper said Hoon has provided details of a “cover-up” at Downing Street.
The former Labour minister said he was sent a copy of the “very long and very detailed legal opinion,” written by then-Attorney General Peter Goldsmith, “under conditions of considerable secrecy” and told he should “not discuss its contents with anyone else.”
Describing it as “not an easy read,” Hoon said he “came to the view” after several readings that the memo was “not exactly the ringing endorsement” of the war effort that the British government and military chiefs had hoped for. Goldsmith had apparently written that the invasion would be lawful only if Blair believed it was in the UK’s national interest.
“When my Principal Private Secretary, Peter Watkins, called Jonathan Powell in Downing St and asked what he should now do with the document, he was told in no uncertain terms that he should ‘burn it.’”
However, Hoon said he and Watkins defied the order and decided to lock the memo in a safe at the Ministry of Defence instead. He noted that the document is “probably still there.”
While Blair has yet to comment, Powell has denied ordering Hoon to burn the memo, telling the Daily Mail that, at Goldsmith’s request, he had asked the former defence secretary to “destroy” a separate “minute” on the legality of the invasion that had been sent months earlier.
The explosive claims come as over 750,000 people have signed an online petition to strip Blair of his knighthood. Anti-war activists have long accused Blair of war crimes for sending British troops into Iraq and Afghanistan.
Copyright Disclaimer Under Section 107 of the Copyright Act 1976, allowance is made for “fair use” for purposes such as criticism, comment, news reporting, teaching, scholarship, and research. Fair use is a use permitted by copyright statute that might otherwise be infringing. Non-profit, educational or personal use tips the balance in favor of fair use.
For many pilots who have chosen to remain unvaccinated for COVID-19, daily life has become a navigation of Catch-22s not seen since bombardiers were still stationed on Pianosa.
Jason Kunisch, a commercial airline pilot with 20 years experience and co-founder of the US Freedom Flyers, ponders whether OSHA can require him to take a newly approved vaccine, despite his long-held understanding that, “Traditionally pilots are not governed by OSHA… [but] by the FAA,” which prohibits pilots from taking newly approved drugs.
Sherry Walker, a United pilot with more than 24 years experience, and co-founder of Airline Employees for Health Freedom, copes with the reality that, according to her account, despite having received an exemption from United’s vaccine requirement in order to keep her job while unvaccinated, she can longer do her job or receive a paycheck, presumably until she is vaccinated.
Kate O’Brien, the Media Relations Director for the US Freedom Flyers, voices the frustration of her group’s members, as she describes how executive orders supposedly issued to keep Americans employed and maintain the integrity of the supply chain, have arguably led to increases in unemployment and the supply chain’s collapse.
Medical Freedom Organizations Takeoff in the Aviation Industry
Growing up in San Diego, Jason Kunisch learned to fly while still in high school. After earning his private pilot’s license, he attended a four year aeronautical university, graduating with degrees in aeronautical science and business, then went on and earned his instructor ratings before working dispatch for a charter corporation out of California and Texas. From there he went and flew regional jets prior to making his way over to one of the major airlines a little more than eight years ago.
However, over the course of the past year, life took an unexpected turn for Kunisch. Although still working for a major airline when interviewed for this article in late November, Kunisch was now spending a considerable portion of his time immersed in the day to day operations of the US Freedom Flyers, a medical freedom organization he co-founded with fellow pilots Jessica Sarkisian, Joshua Yoder, and Veronica Harris.
When asked to recount what led him to this role, Kunisch detailed the ever-shifting vaccination policies of the major airlines that went from tolerable to utterly unacceptable in his mind, as well as those of his compatriots in just under a year.
“Most of the airlines prior to September 9 [2021] were very reasonable in their approach,” Kunisch explained. “They said, ‘If you want to go and get vaccinated, that’s your personal choice. In fact we’re going to incentivize you to go do that. We’re going to give you days off. We’re going to give you cash. We’re going to give you extra vacation days next year.”
As for those who did not want to get vaccinated, Kunisch said, the companies and the unions took the approach of “‘Hey, we encourage you to do it but at the end of the day it’s a choice between you and your medical practitioner or you and your family doctor or you and your family. Really it’s a personal decision.’”
Yet, at the same time, Kunisch and others had their concerns about how long such a reasonable approach might last.
“We kind of saw the writing on the wall,” Kunisch recalled. The forced masking of individuals, social distancing, and the rules about what one could and could not do with regard to COVID were all disconcerting to him and many of his colleagues.
“So we’re like all right,” Kunisch said. “Really, the next logical thing is the vaccines and vaccine mandates.”
Then, before long, the mandates arrived. “So United Airlines comes out over the summer and says, ‘We’re going to impose our own vaccine mandate and those who don’t want to do it can submit for a religious or medical exemption,’” Kunisch explained.
Sherry Walker, co-founder of Airline Employees for Health Freedom, an organization similar to the US Freedom Flyers, was one such individual from United.
According to Walker, who spoke in an interview as a representative of Airline Employees for Health Freedom, the process of applying for an accommodation was so onerous that many at United who had reservations about taking a COVID vaccine simply acquiesced out of exasperation from the process or fear they might fail to navigate it properly in the time allowed.
Yet, for those that endured, Walker stated, “[United] put every one of us on unpaid indefinite leave.”
Jessica Sarkisian, a 24 year captain and US Freedom Flyers co-founder, had been concerned about something like this happening at her company for quite some time, having circulated a petition on the matter amongst her co-workers as early as January 2021.
In an interview, Sarkisian described the moment her grassroots activism transitioned from an intracompany endeavor to one with a more national scope. “When United announced their mandate, my company said, ‘Yeah, we’re going to mandate it also, but for the 20% who do not want to get the vaccine, [they’ll] get testing options’ and so immediately people started contacting me at my airline because… people already knew how I felt.”
From there the US Freedom Flyers began to take off. “I started collaborating with a few go getters,” Sarkisian explained. “Then I saw Josh Yoder, another co-founder, on the Stew Peters show and I reached out to him and we communicated and I also reached out to the gals at United and communicated with them and just started reaching out to people at other airlines.”
Likewise, Walker’s Airline Employees for Health Freedom saw their numbers grow during this period as well.
Yet, despite this grassroots success for Kunisch, Walker, Sarkisian, and the members of their nascent organizations, it was not long before they would have more to contend with than simply employer mandates.
Pilots Enter Dogfight with the Biden Administration
“So September 9 rolls around and President Biden says he’s going to have a number of mandates and executive orders,” Kunisch said. “[One] is covering employers of more than 100 employees and that is going to be handled through OSHA… That’s the OSHA case. Then there’s the federal contractor case. That’s another one… Initially our response was to raise funds and awareness and to sue the federal government on the grounds of the OSHA issue because that’s what we all thought was going to get us first.”
This though was despite the fact that there was initially some confusion amongst Kunisch and others in their organization regarding whether the OSHA mandate affected pilots specifically, given that they long understood that they were governed by the FAA, not OSHA.
But, before long, whether pilots were affected by a mandate enforced by an agency, that, according to Kunisch, traditionally did not have authority over them, Kunisch and the US Freedom Flyers realized that the OSHA mandate was not actually their most imminent threat.
“What really came to really bite us all was this federal contractor mandate,” Kunisch said. “Now because the airlines have contracts with the federal government to do troop lifts or evacuations and other flying we are considered federal contractors even though we don’t get any of the benefits of federal contractors like better benefits, better pay, etc., etc., holidays off, whatever… I guess we get none of the good, [although] we get all of the bad… Within the federal contractor mandate there’s no provision for testing. So it’s basically get vaccinated or get fired… So that’s a major concern and initially the companies were very strict in their wording. They more or less were saying ‘You get vaccinated because of the mandate or you are on the streets.’”
But the US Freedom Flyers and Airlines Employees for Health Freedom fought back. They continued to grow their numbers. They spread awareness. They became more vocal in the media and with their companies and their unions.
Because of this, Kunisch said, “The companies have started to kind of back off… Southwest was the first to come out and say, ‘We’re not going to fire anybody. We’re not going to let anybody go. We’re going to give medical and religious exemptions and you’re going to be able to continue to work.’ I think Jet Blue has done a similar thing… I think Alaska has done it. But the process is still rather arduous and there are still concerns, very specific grave concerns, with the process with these exemptions that everyone has to go through who chooses not to get vaccinated.”
To give greater context, Kunisch, explained that technically there’s a difference between an exemption and an accommodation. “An exemption is you are exempt from getting vaccinated. However, to comply or to be fully exempt, you need to participate in an accommodation. Now what is that accommodation? That’s the question?”
Depending on the specifics of the accommodation, Kunisch believes this could lead to some form of religious discrimination. If the accommodation is unvaccinated airline employees must wear a mask, while vaccinated ones do not, in essence, those who remain unvaccinated due to their religious beliefs would be getting forced by their employers to wear an outward sign of their religious affiliation.
Kunisch also pointed out how treating unvaccinated people differently from vaccinated people doesn’t even make sense scientifically given recent findings demonstrating that those who have been vaccinated against COVID can still contract and potentially spread COVID.
Possible Paths to Victory
Yet, whether groups like the US Freedom Flyers and Airline Employees for Health Freedom succeed likely will not come down to science, but, instead, a combination of legal technicalities and whether enough people will stand their ground and suffer the consequences while demonstrating their worth to their employers, and perhaps the rest of society, through their absence.
Given the key role the aviation industry plays in society and the narrow margins of personnel that facilitate its continued functioning, this should hypothetically be possible.
According to Sarkisian, it would not take a significant number of pilots or other personnel to cause a disruption for air travel by refusing to get vaccinated. “If you have an aircraft with… let’s call it a crew of seven: five flight attendants and two pilots. One of them calls out, or is not there anymore, that’s going to cause a delay or a cancellation. And then if that’s happening across the board like we’ve seen in the past, it’s going to be quite disruptive.”
Case in point, this is what we saw recently with Southwest and other airlines with alleged sickouts and across the commercial airline industry over Christmas when there were mass cancellations, seemingly on account of omicron.
Additionally, it is important to note that mandates impacting the aviation industry impact more than just commercial air travel.
A FedEx captain, who agreed to a phone interview on the condition of anonymity, described what the Biden administration’s vaccine mandates would mean for his company. “There is such a huge number [of pilots] that have not been vaccinated. And this is far bigger than the pilots. This is maintenance. This is the ground crews in Memphis.”
This FedEx captain went on to explain, “FedEx is centered in Memphis and [has] huge, huge ground crews in Memphis… and a huge percentage of our ground crew workforce is African American which, rightfully so, that group of people are very very distrusting of the government and the vaccine program because…[of] the Tuskegee experiments.”
“In comparison to the pilots,” the FedEx captain continued, “it’s a relatively low paying job where [FedEx is] having trouble having guys work anyway. There’s no possible way they’re going to stick around if a vaccine is mandated for them to work.”
O’Brien also emphasized the impact of vaccine mandates on the transportation of goods when discussing what she sees as the irrationality of the Biden administration’s rationale for their various mandates. “The administration itself has said, has outlined, you know, all the reasons why they feel the mandate is important, is imperative. Some of the reasons were to keep the supply chain intact. Well, we can see that the supply chain is currently in shambles. And why is that?”
Alternatively, on the legal front, both the US Freedom Flyers and Airline Employees for Health Freedom have cases working their way through the courts. There are also similar cases making their way to the Supreme Court. Yet, to be clear, these cases are not about some fundamental question of whether an individual has the right to make their own medical decisions in the absence of government or employer influence or coercion, but more narrow legal concerns such as which government agency has the right to mandate what medical interventions for whom.
Which path may ultimately be more fruitful, or if either will lead to a desirable outcome for the US Freedom Flyers and Airline Employees for Health Freedom, remains to be seen.
Looking Towards the Horizon
But according to the pilots fighting to preserve medical freedom, the simple fact that they are fighting the government on this is having an impact.
“The government put forward these mandates… not expecting the response,” Kunisch said. “I don’t know why they weren’t expecting that. We can come up with reasons. The fact that we are fighting this is the reason why they are kind of on their heels.”
According to Kunisch, this is why the government pushed back their initial deadlines for compliance with the OSHA and contractor mandates. “There’s a reason for [this] and that’s because we’re fighting back. We’re fighting back against these mandates. We’re saying no. We’re not going to do it. We’re not going to be coerced.”
As of November, Sarkisian said the US Freedom Flyers were working with employees from 26 airlines, Amtrak, and trucking companies, as well as the general public. Walker, when interviewed, estimated Airline Employees for Health Freedom had about 4000 members across the transportation industry.
“This isn’t just about crew members,” Sarkisian stated. “This is a fight for freedom for everyone because everybody is obviously affected.”
“The issue is not the vaccine,” Kunisch added. “The issue is medical freedom and anti-coercion.”
Walker, when speaking of the battle ahead, stated, “I have a 16 year old son,” before rhetorically asking, “If I do not fight this now, what world am I leaving him?”
Daniel Nuccio holds master’s degrees in both psychology and biology. Currently, he is pursuing a PhD in biology at Northern Illinois University studying host-microbe relationships. He is also a regular contributor to The College Fix where he writes about COVID, mental health, and other topics.
Almost one year on from the riot at the US Capitol Building, it continues to be used by those in positions of power to develop a culture of fear – yet another example of a threat being amplified and raising public insecurity.
There is no need for a pandemic for the hysterical ruling class to constantly turn on the engine of fear. Without blinking an eye, the American political establishment has casually catastrophised the Capitol protest in Washington on 6 January last year.
Almost immediately a political riot by angry protestors was reframed as an “insurrection” and an act of domestic terror. Leading Democratic Party figures even sought to link the so-called coup attempt to Russia, and House Speaker Nancy Pelosi declared that the rioters were “Putin’s puppets”.
Despite the relentless quest to uncover a malevolent conspiracy to overthrow the elected government of the United States, there is nothing to suggest that what occurred on January 6 was anything more than an instance of angry, violent rioters invading the Capitol Building. Despite their best efforts, the FBI and other agencies could find no proof of any conspiracy. Last August, Reutersreported that “the FBI has found scant evidence that the January 6 attack on the US Capitol was the result of an organized plot to overturn the presidential election result”.
This absence of evidence notwithstanding, America’s cultural elite, along with the leadership of the Democratic Party, continues to remain in hysteria mode. Indeed, its obsession with the threat of an insurrection or a coup has hardened during the past year to the point that it genuinely finds it difficult to distinguish between fantasy and reality.
The New York Times, once a serious news outlet, has become a slave of its paranoia about an impending civil war. Anyone reading its commentary would draw the conclusion that what happened on January 6 was akin to the violent rioting that accompanies a bloody coup d’etat.
On the first day of 2022, its Editorial Board published a piece titled “Every Day Is Jan. 6 Now”. In case anyone failed to get the point of the title, it added, “Jan. 6 is not in the past; it is every day”. The statement evokes a world where the American “Republic faces an existential threat” and insists that “we should stop underestimating the threat facing the country”. The threat it refers to constitutes the millions of voters who continue to support Donald Trump and deny the New York Times’ version of reality. In its typical alarmist tone, it states, “no self-governing society can survive such a threat by denying it exists”.
This feverish irrationality isn’t restricted to America. Across the Atlantic, The Guardian adopts a similar tone in its treatment of the legacy of January 6. “US could be under rightwing dictator by 2030, Canadian warns” runs one of its headlines. In this article, the scaremongering prediction of an academic in The Globe and Mail is presented as a sensible assessment of future possibilities. Political science professor Thomas Homer-Dixon from Royal Roads University in British Columbia urges Canada to protect itself against the “collapse of American democracy”. And he warns, “We mustn’t dismiss these possibilities just because they seem ludicrous or too horrible to imagine.”
Projecting a scene akin to one in a dystopian horror film, Homer-Dixon asserts, “By 2025, American democracy could collapse, causing extreme domestic political instability, including widespread civil violence. By 2030, if not sooner, the country could be governed by a right-wing dictatorship.”
The editorial team at The Guardian appears to have become addicted to the political pornography peddled by the likes of Homer-Dixon. It also features a piece by Jason Stanley, who imaginatively recasts the contemporary era as akin to the one that led to the rise of fascism in Weimar Germany. In a commentary titled “America is now in fascism’s legal phase”, Stanley paints a picture that looks depressingly similar to the months leading up to the rise of Adolf Hitler. For Stanley, there is a clear parallel between the behaviour of Trump and Hitler. He contends that “as in all fascist movements, these forces have found a popular leader unconstrained by the rules of democracy, this time in the figure of Donald Trump”.
At first sight, it is tempting to draw the conclusion that the catastrophising of January 6 or the constant evocation of the spirit of Nazi Germany haunting America is pure scaremongering propaganda. No doubt there is an element of media manipulation and conscious twisting of reality at play. But on closer inspection, it seems as if the ruling classes in Western societies have genuinely internalised the culture of fear. January 6 is simply one catastrophe amongst the many that preoccupy them.
A striking illustration of how the self-catastrophising masochistic ruling elite thinks was offered by Belgian Prime Minister Alexander De Croo in a speech he gave to the United Nations General Assembly last September. Pointing to climate, vaccines, and terrorism’, he stated that “nobody is safe until everybody is safe”. By linking together three different and disparate elements, De Croo painted a picture of a world where threats to human existence are endemic. Add this scenario to the threat of American fascism and we end up with a 21st-century version of the Four Horsemen of the Apocalypse.
This distorted representation of reality promoted by insecure elites is having a cumulative impact on public life. Put simply, it is raising public insecurity – and at the same time diminishing the capacity of people to confront some of the very real problems they face.
Frank Furedi is an author and social commentator. He is an emeritus professor of sociology at the University of Kent in Canterbury. Author of How Fear Works: The Culture of Fear in the 21st Century.
Driven by climate madness, the environmental movement has become the greatest advocate of destructive industrial development in history.
As Kant said: “To will the end is to will the means”. In this case the means to the phantom end of climate control have led environmentalists to abandon all of their principles. Solar and wind require environmental destruction on an unprecedented scale. Electrification requires the use of toxic chemicals on a similar scale. The hazardous waste stream is enormous.
Solar is the worst because the destruction of forests and open land is complete. Perhaps something lives under these vast solar slabs but not much and certainly nothing like what they destroy and displace.
As I pointed out in my recent article on Virginia’s ill-named Clean Economy Act, we are talking about hundreds of square miles of solar devastation today, for just one state.
To actually meet our need for electricity would require several thousand square miles of destruction just for Virginia. For the whole country the numbers are staggering, easily the biggest environmental disaster in our history.
Wind is environmentally destructive too, just in a different way.
Let me make this personal. I live in the mountains, in far eastern West Virginia. When I drive to the county seat I get a grand view of the big mountain to the west. It is called the Allegheny Front, the height of land between the Atlantic and Mississippi watersheds. My magnificent natural view is now being industrialized, dotted with windmills and more on the way.
I am sure natural vistas are everywhere threatened, because that is where the best wind is. Mind you we almost never get sustained winds strong enough for full power, but that just means they need more intrusive industrial wind machines to produce the juice.
Even worse, there is a viewpoint up on the Front called Bear Rocks, where crowds gather every fall to watch the hawk migration. Great numbers of hawks come by in swirling groups called kettles, working their way slowly southward down the Front. Surely significant numbers will be killed by the growing phalanx of giant chopping blades.
West Texas has something like 10,000 choppers and other states are rapidly going the same way. That the environmentalists can allow the killing of enormous numbers of protected birds is a clear abandonment of their principles. This is Silent Spring in real life, with entire species threatened.
Then too, environmentalists fight hard for roadless areas. Scattering giant wind machines around a mountain top requires a dense system of access roads, one to every tower. In rugged terrain these systems can be complex and so big, destructive land users.
At the other end of the wire we have chemicals, especially enormous numbers of big batteries.
First come the huge battery arrays needed to turn highly intermittent wind and solar power into reliable juice. Then come the myriad batteries needed to electrify our transportation system, which also requires a lot more solar and wind devastation. Note that a lot of juice will go through batteries twice on its way to use.
Minimizing the use of toxic chemicals has been a cornerstone environmental principle. That the movement should now opt for chemical energy as a central feature of our energy system is a complete abandonment of that principle.
Then there is solid waste, which has always been a central environmental concern. Compared to conventional power plants, wind blades and solar panels are short lived, batteries are ridiculously so. In a solar, wind and battery world we are likely talking about billions of tons of toxic waste.
I think just about every principle of environmentalism is violated by the proposed massive buildout of wind, solar and electrification. Why the environmentalists are not screaming and suing to stop this vast open land destroying, wildlife killing and chemically intensive action is beyond me. Clearly environmentalism has lost its way.
David Wojick contributes Posts at the CFACT site. He is an independent analyst working at the intersection of science, technology and policy.
Over the past several decades, the progressive Left has successfully fulfilled Antonio Gramsci’s famed admonition of a “long march through the institutions”. In almost every Western country, its adherents now dominate the education system, media, cultural institutions, and financial behemoths.
But what do they have to show for it? Not as much as they might have expected. Rather than a Bolshevik-style assumption of power, there’s every chance this institutional triumph will not produce an enduring political victory, let alone substantially change public opinion.
Even before Biden’s botched Build Back Better initiative, American progressives faced opposition to their wildly impractical claims about achieving “zero Covid” and “zero emissions”, confronting “systemic racism” by defunding the police, regulating speech, and redefining two biological sexes into a multiplicity.
Increasingly, the “march” has started to falter. Like the French generals in 1940 who thought they could defeat the Germans by perfecting World War One tactics, the progressive establishment has built its own impressive Maginot Line which may be difficult to breach, but can still be flanked.
That is not to deny the progressives’ limited successes. It has certainly developed a remarkable ability to besmirch even the most respected institutions, including the US military. But that is where its achievements stop.
While the Pentagon’s top brass focused on “domestic terrorists” and a progressive social agenda, it calamitously bungled its withdrawal from Afghanistan and appears utterly unprepared for Chinese or Russian competitors. And the effect of this progressive march is plain to see: the percentage of Americans who feel “a great deal of trust and confidence in the military” has dropped in just three years to 45% from 70%.
This decline in trust in major institutions, so evident in America, is also rife across Europe and Australia. In Europe, for example, young people express less pride in their cultural and religious heritage, and are almost three times as likely as their elders to believe that democracy is failing.
The great paradox of progressivism is that nowhere are its shortcomings more evident than in its geographic heartland: the dense urban centre. Conventional wisdom has dictated that America’s high-tech economic future will be shaped in dense urban areas, where superstar companies stand the best chance of recruiting superstar employees.
But while the upper crust of the labour force continue to head to the dense urban cores, on the ground people are moving in the other direction. Across the high-income world, not only in America but Europe as well, the vast preponderance of growth has taken place in suburbs and exurbs. In the last decade over 90% of all US metropolitan population growth and 80% of job growth took place on the periphery. On the ground, then, the progressive dream is withering.
The pandemic has greatly enhanced these trends, with downtown neighbourhoods recovering far less quickly than suburban, exurban, and small towns. But even if these changes are not permanent, at least not entirely, city residents will still have to contend with another pitfall of the progressive agenda: rising crime. Twelve American cities have experienced record homicides this year; all are ruled by Democratic, often progressive, leaders, many of whom explain away crime and excused, even praised, the looting and mayhem caused by protestors in the summer of 2020.
Yet despite this visceral impact on urban neighbourhoods, it is in education that our new hegemony could have its most long-lasting impact. The West’s new educational mandarins, increasingly strident and increasingly influential, have no use for our liberal inheritance, which they consider little more than a screen for racists and misogynists.
In Canada, we have seen an instance of “flame purification” for everything from old encyclopaedias and maps to Depression-era cartoons. In America, the disconnect between the professoriate and the people also keeps growing, as conservatives head towards extinction on many campuses: on some well-regarded campuses such as Williams, Swarthmore and Bryn Mawr, the ratio of Democrats to Republicans reaches between 70 and 132 to 1.
These trends have long been evident in the fading humanities and social sciences, but now even the sciences are becoming politicised. Perhaps it’s no surprise, then, that universities are losing credibility even among some traditional Leftists, who marvel at how they burnish their progressive credentials while making huge profits off their endowments and seriously underpaying most of their employees.
And just as with the growing disaffection for the military, teachers, students and parents are starting to push back. A number of teachers who have been “cancelled” or otherwise threatened for dissenting are now fighting back in the courts. There’s also considerable criticism from parents and alumni, some of whom are now pledging not to contribute to their schools, and instead support well-publicised and well-funded efforts to start new initiatives, such as the recently announced University of Austin. Even more importantly, would-be students are also voting with their feet: after decades of rapid expansion, the number of college students enrolments fell by 5% last decade, and dropped an additional 6.5% since 2019.
Likewise, only one in three Americans have confidence in their public schools, where the education establishment’s goal seems to be to obliterate merit. In my adopted home state of California, this “post-colonial” approach includes deemphasising the importance of tests, excusing bad behaviour, and imposing ideology on often ill-educated students. The San Diego Unified School District, meanwhile, is busily getting rid of mandates for such things as knowing course material, taking tests, handing in work on time, or even showing up; all these, the district insists, are inherently “racist”. This in a state that ranked 49th in the performance of poor, largely minority students. (Still, the situation could be worse: neighbouring Oregon no longer requires any demonstrable proof of competence to graduate.)
In the past year, this blindness has incited considerable public outrage. Criticism of Critical Race Theory buoyed the Republican win in Virginia in November, and has become a rallying principle for parents around the country, including a recall drive against San Francisco school board members.
Other parents are trying to opt out of the public system altogether. The pandemic saw the departure of more than one million American students from public schools, while 1.2 million families switched to home-schooling last academic year, bringing the total number of home-schooled students to 3.1 million, roughly 11% of the total. According to the Census Bureau, Black and Hispanic families now have the highest estimated rates of home-schooling, at 16% and 12%, respectively.
Meanwhile, the mass media, particularly its legacy outlets, constitute another progressive bastion losing credibility. One recent survey found that barely one in three Americans trusts the media, including a majority of Democrats, while only 15% of Americans have confidence in newspapers. Part of this surely stems from their bias: although there remain some powerful conservative voices, notably on talk radio and Newscorp properties, the vast majority of journalistic power lies with the Left. It’s the same story with social media, which increasingly dominates news access and is also widely distrusted.
But the media’s Maginot Line may prove more vulnerable than expected, and this breach is certainly a far better prospect than those that came with the German flanking. There is a definite challenge not just from the traditional Right but a plethora of new publications which offer intelligent analysis outside the establishmentarian party line, as well as from Substack. Unless the media oligarchs find ways to repress these elements, a resurgence of free thinking may rescue journalism from progressive editors and journalism schools.
The shift in the media parallels that in mass culture. As late as the Fifties, mass culture was seen as largely neutral. But in recent decades, it shifted towards a more monochromatic look — one which a significant portion of the public are fed up with. Gender flipping may excite progressive creatives, but politically correct remakes of household favourites have proved box offices disasters. Indeed, it’s striking that openly conservative presenters, such as Fox’s Greg Gutfeld, now do better in ratings than their more established network rivals like Jimmy Kimmel and Jimmy Fallon.
Yet perhaps nothing is more ironic, and potentially dangerous, than the takeover of the corporate suite by progressive ideology. Traditionally, the dispersion of ownership and the conflicting views of entrepreneurs and inheritors fuelled the dynamism of democracy: you had far-Left businessmen like George Soros and doctrinaire Right-wingers like the Kochs in competition. They fought it out, and sometimes even aligned. But they came from diverse viewpoints.
Today this diversity of viewpoints is being obliterated by design, with corporate behaviour now married closely to the notion of the “great reset” and “de-growth”: an economy where improving conditions for the masses is replaced with lowering carbon emissions and diversity tokenism. Such standards, of course, do not apply to snotty private schools attended by their offspring, or areas that are home to their mansions.
The oligarchs may feel they deserve dispensation from the masses by their “good deeds”, but people are not as stupid or malleable as the ruling elites believe. Trust in major corporations, never too robust, is below 20%, less than one third that for small businesses. It is slowly becoming apparent that ‘woke capitalism’ will never solve divisions which are essentially economic. The key, notes Richard Parsons, former President of Citigroup, lies not with racial quotas or hiring transgender workers but the economic growth and opportunity. There will never be “unity”, he suggests, until people “feel it in their pockets”.
The question now is whether there will be sufficient pushback to turn the tide. Unlike local school boards, online magazines, and even alternative colleges, it’s difficult to replace or challenge an Amazon, Apple, Microsoft, Google, or Morgan Stanley. Yet fortunately these institutions do not yet control all wealth. Big companies may have shamed themselves out of oil and gas, but investors are ramping up due to the soaring price of these assets.
So, here’s the good news. On what sometimes seems the inexorable course towards progressive capture, we can see multiple fronts of resistance, and the early congealing of independent-minded forces, from the rational Right to the traditional liberal-left. Our society may never regain the feistiness of previous eras, and our new elites might continue marching through our institutions. But as they become increasingly discredited, they would be unwise to forget that all long marches one day come to an end.
Joel Kotkin is the Presidential Fellow in Urban Futures at Chapman University and executive director of the Urban Reform Institute. His new book, The Coming of Neo-Feudalism, is now out from Encounter.
It’s been the most astonishing two weeks for American public life, with so many prescient changes, from new censorships, admissions, backtracks, experts speaking out, public outrage, and what strikes me as a progressive unraveling of every orthodoxy imposed nearly two years ago.
Not even the influential and powerful are in a position to defend what has happened to us. They seem to be gradually pulling away from public life, unable to say things that connect to what everyone knows.
Above all else, what’s remarkable right now is the undeniable arrival of Covid to a degree to which hardly anyone could have imagined all that time ago, when so many experts set out to deploy their fabulous new system for stopping the spread of a disease.
There was a goal (stop cases). There was a method (state compulsion). And there was a test (cases were supposed to go down and go away). There would be a war on a virus and the state would win! And now we look around and see the evidence of failure so pronounced, so impossible to deny, that we must face that which so many have worked so hard to deny for so long.
The best way I can describe this is by observation. In the Northeast of the US, and in many other parts of the country, everywhere you go, right now, you see sick people milling around. They don’t admit it and they don’t talk about it with strangers simply because there is such shame attached to having Covid. They complain of a cold, of a flu, or just suffer in silence. But there it is.
After nearly two years of work to control the spread, after brutal shutdowns of the whole country – shutdowns that happened two years too early, as judged by actual case trends (but of course lockdowns never should have been considered in the first place) – Covid is here. Not just here. It is everywhere. The case counts are beyond anything anyone on the planet could have imagined a year or two ago. The spikes make everything that came before look like child’s play.
Here is the global chart.
And we are talking really sick. Not so much death. Not even out-of-control hospitalization. We are talking about being sick in bed or walking around with misery. The nasty bug lasts maybe two days, maybe two weeks, maybe longer but it is vexing and wicked, not like a cold or flu but something more electric and strange.
Which variant? Two weeks ago, the CDC wanted to blame it all on Omicron. That is no longer possible. Perhaps that constitutes 20%; we just do not know for sure because tracking is so weak. Most of it is evidently Delta, meaning very sick but with no serious loss of taste and smell. Most everyone eventually gets well, and that’s what happens here.
We get to endemicity perhaps in a month or so and life will move on, my experts tell me, at least in some areas of the country. What’s striking and truly shocking is that all of the efforts, all of the propaganda, all of the astonishing spending and compulsion – the shutdowns, masking, size limits, travel restrictions, vaccination requirements, the track and trace, the endless testing, the enforcement, the intimidations, the censorship – and what do we have to show for it?
Lockdown architect Carter Mecher promised us as follows: “If you got everyone and locked each of them in their own room and didn’t let them talk to anyone, you would not have any disease.” They attempted a version of that, experimenting on the human population in ways without precedent. And let’s say that is true (it probably isn’t). That is not life. That is not society. That is not freedom. That is something else unimaginably horrific.
It was unsustainable. They pushed their theory without regard to the history of public health or, really, the whole of human experience. And now, the true pandemic finally arrived. And what is it? There are a ton of sick people. People are calling in sick because they cannot come to work. Institutions are having to shut down, not because government closed them but because people are too sick to come to work. This is the normal course of events – exactly what one would expect in a pandemic.
And it’s not just Covid. The head of an Indiana life insurance company reports that deaths among people aged 18-64 are up 40%, an astonishing increase. It’s suicide, drug overdoses, and every other manner of horror. And that’s just death. Many others are just sick from other things.
I personally know dozens and they each know many dozens of more people in the Northeast right now who are down for the count, miserable and pathetic, but still testing negative for Covid. Why would this be? It’s because immune systems have decayed over two years. The lack of vitamin D, the lack of exposure to normal germs in life, the isolation and depression, the overconsumption of liquor and drugs – it’s all been a terrible drain on health.
Meanwhile, the actual pandemic of Covid has certainly arrived. And it is far worse than the data indicated. Look at Massachusetts, New York, Pennsylvania, Rhode Island, Connecticut, any of these states, and including some Southern and Midwestern states, and what you find is increases of 500-1,000% in cases. And keep in mind that these are just cases as discovered by official testing spots.
Go to any CVS or Walgreens and you find long lines of people buying testing kits. If they are available. If they are not, the wait is weeks. They are $23 a kit and people are buying as many as possible. Why? Partially it’s because employers and schools are demanding negative tests, but it is also just curiosity. People are sick as dogs and want to confirm their illnesses.
People are estimating that real cases are 50x to 100x what the official data say.
But let’s talk now about a real scandal. When you are sick, you need treatment. Every competent medical professional I know is pretty darn sure that the best hope for dealing with Covid is a combination of Zinc, Vitamin D, and (sorry to mention the dreaded name) Ivermectin. This is not ideological. This is what experienced doctors are saying right now. I’m on many email lists with serious medical professionals and they are all saying the same thing. We can add HCQ to the list if you catch it early enough.
But here’s the kicker – and let me be clear that I’m NOT giving ANY medical advice here, merely just reporting the sense of the community out there. What’s remarkable is that people are having a very difficult time getting these basic therapeutics. Vaccines are everywhere but things to make you well once the virus penetrates the vaccine? Those are hard to come by.
There is a problem getting a prescription because state medical boards are actually barring people and preventing them from serving patients if they prescribe HCQ or Ivermectin, as incredible as that sounds. But once you get the prescription – if you have a doctor brave enough to risk it – finding a pharmacy to fill it is another challenge.
Most people in the UK today are getting their therapeutics from India. Americans get them from Mexico. And some are shipping to the US and they are being distributed via gray markets for anyone who is lucky enough to have a contact. It’s a speakeasy nation but this time for distributing basic therapies.
I feel like I’ve seen horrible things for almost two years now, and you feel the same way. But of all the scandals, and there are so many, this one seems to top the list, namely that once the real pandemic has arrived, there are no effective medicines that are widely available. Doctors are actually being blocked from doing their jobs.
Beyond belief. But you know this. I’m sure you have your own stories. I suspect that many of our readers have encountered this virus for the first time in the last two weeks and have dealt with the horrors of just getting basic medicines to get through this.
The NIH has funded almost no serious trials of these generic drugs. It is not in the interest of pharmaceutical companies to fund them either. As a result, we are truly at a loss – nearly two years into a pandemic at a time when people need meds more than ever.
Meanwhile, the FTC is spending its time cracking down on pharmacies that advertise that they have therapeutics available for people. They are sending cease and desist letters all over the country as a way of intimidating providers. I’ve seen these letters. They have invited me to post them but I’ve declined in the interest of keeping people out of trouble.
One merciful upside to all of this is that there is no more talk of lockdowns. At last, even the experts are saying that society must function. Lockdowns are not even being considered. The whole country is fed up with the phony baloney enterprise of virus control. It did not and cannot work.
Nearly two years ago, they deployed a new experiment in stopping a pathogen. It was a plan that was 15 years in the making, hatched by fanatics who imagined that state policy could outwit a virus.
The wreckage was astonishing, and yet what was the payoff? Here we are today with a wave of sickness that defies every prediction, and with collateral damage beyond even the worst predictions (including my own). And the truth of this is all over the data that anyone can see and the stories that anyone can hear.
The country is right now sicker than it has ever been in our lifetimes.
What a stunning repudiation of state policy – the worst failing of public health and public policy perhaps in the history of the US if not the entire world. We are right now living in its last days. Remember these days, my friends. They are legion and mark what is likely the end of the great fiasco.
And yet it is not really the end. There will be decades of hell to pay for what has happened to us.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
The New York Times reportedly bases a book’s position on its bestseller list on what they call a proprietary algorithm. Whatever their method, they favor specific books, ignore others, and rankings are often disconnected from how many copies of a book were actually sold to consumers.
You probably thought the New York Times Best Sellers list reflected book sales, but it doesn’t. It’s an engine of censorship, corruption and misinformation.
How do we know this? Follow the numbers.
Can a book outsell every other book in the U.S. and not be the #1 New York Times Bestseller? Sure. Is that perhaps a form of censorship? Yup.
Robert F. Kennedy, Jr.’s latest book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health,” was published Nov. 16, 2021, by Skyhorse Publishing, Inc.
The New York Times reportedly bases a book’s position on its bestseller list on what it calls a proprietary algorithm. Whatever the method, the Times favor specific books, ignore others, and rankings are often bizarrely disconnected from how many copies of a book were actually sold to consumers.
As every publisher in America knows, you can’t make the Times’ list without selling a substantial number of books through Barnes & Noble, as well as “the independents.”
But what if Barnes & Noble decides to buy very few copies of a book based on its subject matter? And what if some independents exhibit similar bias by boycotting the book, refusing to carry it and telling customers that they won’t even special order the book?
That’s what happened in the case of Kennedy’s “The Real Anthony Fauci”: Barnes & Noble purchased an unusually small quantity, and they kept the book invisible in most of their stores.
Independent booksellers, such as the San Francisco-based City Lights, don’t list the book on their website, tell customers they “don’t carry the book” and refuse to order it, even upon request. These decisions have nothing to do with customer demand or interest in the book.
Perhaps because of the trend toward politicization by bookstores that report sales to the Times, Amazon now accounts for an increasingly large percentage of book sales in the U.S.
On the one hand, the Times’ list is inaccurate because it applies an outdated, and increasingly irrelevant, view of how books are sold. On the other hand, it appears the Times’ bestseller list intentionally misrepresents actual consumer sales and demand.
Let’s see that in action by using “The Real Anthony Fauci” as a case study. The book boldly challenges mainstream narratives. It’s a serious work that makes legitimate, meticulously researched arguments.
With more than 2,000 citations and references, the book asks readers to engage in dialog and debate. At the end of each chapter, there’s a QR code that links to a website containing updates, critiques and new information.
“The Real Anthony Fauci” was carefully vetted by doctors, scientists and lawyers. It has received substantial support from leading scientists, including at least one Nobel Prize-winning scientist.
This type of book cannot possibly be what any reasonable person has in mind when they seek to protect the public from “misinformation.”
Kennedy’s tour de force resonates so strongly with the American public that, despite epic censorship, “The Real Anthony Fauci” is one of the bestselling books in America.
It has achieved this status despite a total media blackout. There hasn’t been a single review in a major newspaper, online platforms have rejected advertising — some calling it “misinformation” before anyone could actually have read it — and bookstores are boycotting it.
In the past, people perused the New York Times Best Sellers list because they believed it represented an honest account of what people across the country were reading.
Today, alas, the New York Times Best Sellers list represents a political point of view and has become a way to encourage Times readers to buy and read books that the newspaper owners approve of — and to avoid books they don’t approve of.
The playbook from major newspapers and other media outlets is transparent: Attack the author, ignore the book.
In Kennedy’s case, the hit pieces have come from Town & Country, The New York Post, Vanity Fair, The Associated Press and others. (The Times hasn’t reviewed the book, of course, but describes it as a new book by an “anti-vaxxer.”)
Again, despite the epic censorship, there has been enormous grassroots demand for this book, and it’s burst through the blockade to hold the #1 spot on Amazon Charts and also become the #1 USA Today, #1 Publishers Weekly, and #1 Wall Street Journal bestseller.
The New York Times, however, listed it at #7 in the first week and #8 in the second. That must mean the book sold fewer copies than the books with higher rankings on the list, right? Wrong.
Few people ever see the actual numbers of books sold, so let’s break that tradition and share it all: The week Kennedy’s book was ranked #7 by the Times, it sold more than 92,000 hardcover copies.
That’s four-and-a-half times as many copies as two of the books ranked ahead of “The Real Anthony Fauci,” and more than double the average of all the books ranked ahead of it.
The fact is no book anywhere on the list sold more copies than “The Real Anthony Fauci.” (The book that earned the coveted #1 slot was the Times’ own “1619 Project,” which sold thousands fewer copies than Kennedy’s book.)
New York Times Best Sellers List
Nov. 21, 2021 (Reported Dec. 5)
The week after that, the Times again placed the “1619 Project” in the #1 position, as if it had sold the most books, even though it undersold Kennedy’s book by more than 20%.
And they moved “The Real Anthony Fauci” down to the #8 position — even though it outsold every other book on the list. It sold nearly three times as many copies as the book the Times listed as #3.
New York Times Best Sellers List
Nov. 28, 2021 (Reported Dec. 12)
The Times obviously doesn’t want its readers to know how well Kennedy’s book is selling, likely hoping that’ll stymie demand.
But Americans are smarter than the New York Times gives them credit for — in less than four weeks, “The Real Anthony Fauci” sold more than 400,000 copies in all formats.
Americans clearly don’t like to be told what to think or what to read — or what not to read. Buying “The Real Anthony Fauci” has become a vote, sort of like a straw poll, against the increasingly insidious censorship in America.
Tony Lyons, president and publisher at Skyhorse publishing, and an attorney, was publisher at The Lyons Press between 1997 and 2004. He founded Skyhorse Publishing in 2006 and has been involved with every aspect of the book publishing process.
In a Daily News Bulletin issued February 4, 1924, by the Jewish Telegraphic Agency, Jewish leaders across the nation publicly mourned the passing of former war-time president Woodrow Wilson, the self-described “staunch friend of the Jews.” The telegram goes on to commemorate Wilson’s “intense interest in Jewish questions” by reviewing his political deeds as president, appointing Louis D. Brandeis to the Supreme Court Bench despite vigorous opposition from the Court itself and urging the approval of the British Mandate over Palestine following the Balfour Declaration.[1]
Nearly a century later, this adulation of America’s twenty-eighth president continues to be echoed by prominent Jewish leaders and intellectuals. In Pulitzer Prize-winning biographer A. Scott Berg’s book, “Wilson,” this formidable Head of State has influenced the decision-making of each succeeding American president up to former President Donald Trump. Furthermore, Berg argues that Wilson is the most pro-Jewish president in US history.[2] This is attributed to Wilson’s breakaway from American isolationism, which guided the nation’s political function on the world stage for a hundred and twenty-five years.
Six months after winning a second consecutive term as president on the Democratic ticket (the first time since Andrew Jackson’s second term), Wilson asked the legislature to declare war on Germany in an imperative speech to Congress on April 2, 1917. His justification was to answer the question of the role the United States would play in the world – it was America’s duty to ensure that “the world must be safe for democracy.” This rhetoric has been repeated repeatedly by American politicians at all levels in subsequent generations, followed by military action.
As Wilson plunged the nation into Europe’s devastating four-year war which wrought 17 million deaths and 25 million wounded, he often portrayed himself as the beacon of progressive ideals, a missionary of self-determination, democracy, and multilateralism to the world and, by involuntary extension after the First World War, its conquered colonies from the ashes of the defeated German and Ottoman Empires. The question is on whose behalf and if foreign elements were acting abroad, at home, or both.
For example, it is entirely plausible today to assert that the invasion of Iraq was contrived almost entirely by high-ranking Jewish Zionists in the Bush administration for the long-anticipated purpose of removing Israel’s arch-nemesis at the time—Saddam Hussein—in another mission to destroy the Jewish State’s Arab neighbors and assert dominion over the region.[3]The catch was that Israel would not be fronting the 2 trillion dollar bill and sacrificing 190,000 lives; that was left to the Americans.[5]
Eighty years prior, before the founding of modern Israel, this similarly established Zionist paradigm in America’s political institutions persuaded the Wilson administration to do the same. Instead of winning the hearts and minds of the public through unbridled war propaganda and an unprecedented national tragedy for the specific purpose of creating a homeland for Jews, a cooperative network of Zionists in Britain, Russia, and the United States worked towards this goal through the imperial hand of the idealistic Wilson.
Jews long held Woodrow Wilson in high regard for his liberal politics and inclination to address their requests. When the former governor of New Jersey first ran for president in 1912, Boston’s Jewish Advocate published a political ad, pressing readers to join with “practically all the great Jewish leaders throughout the country” in endorsing him.[6]These leaders included financier Jacob H. Schiff, philanthropist Nathan Straus, and Ambassador Henry Morgenthau. At the time, beginning in 1906, the United States was faced with the difficult task of admitting roughly ten million immigrants, mainly from Eastern and Southern Europe.
This sudden influx overwhelmed several facets of the native populace, whereby the “restrictionists” emerged with literary test campaigns as a method by which to curtail subsequent waves of immigration. The American Jewish Committee was the most active and significant anti-restricionist lobby group in each of these battles through delay and outright blockage of the legislative passage. During his tenure as president, Wilson assisted by vetoing three restrictive measures he believed were aimed principally at Jews before being overridden by Congress. The AJC’s particular fixation on the plight of Russian-Jewish immigrants caused an extensive lobbying endeavor in America’s foreign policy.[7]
This emerging conflict of interest was sidestepped upon the outbreak of the First World War. The intense pogroms and anti-Jewish sentiment of Czar Nicholas II caused the American Jewish community to side more with Germany than with Allied forces. Immigrant Jews even prayed that the “more civilized” Germans would liberate their suppressed brethren in Eastern Europe from Russian harassment. In the Yiddish press, the enemy was portrayed vividly as: “The Jews support Germany because Russia bathes in Jewish blood.” Who will dare say that it is a crime for Jews to hate their torturers, their oppressors and murderers?”[8] The German Foreign Office took advantage of this position in order to maintain its favor in the Jewish community; in September, 1914, Dr. Isaac Straus was even sent to the United States to manage propaganda work among Jews for the German Information Bureau located in New York.
The German Information Bureau, despite official American neutrality, could not be more pleased following its meeting with the Jewish press. This came at a time when most Americans would rather side with French and British allies out of strong ancestral ties: “So far as our relations with the very influential Jewish press are concerned, they are in good shape, and will be carefully nourished. It is critical in this regard that all news pertaining to them elevate Jewish self-esteem; for example, the appointment of Jewish officers, the installation of Jewish professors, and honors bestowed upon Jewish professors should all be sent here.”
While war efforts were being bolstered in the Jewish press, American Zionist leaders adopted a policy of neutrality for the time being, stemming from Theodor Herzl’s stance on non-partisanship in a neutral country as war raged. During this time, it was Britain’s Grand Fleet that managed the naval blockade of supplies into Germany, starving 400,000 German civilians to death. For the first two years of the First World War, German war efforts nevertheless proved supreme thanks to their unexpected arsenal of submarines against the wealthier, more weaponized Allied Powers. Imperial German forces nearly captured Paris, expelled Russia from the war, and drove the French Army into mutiny, all before a Western Front victory was barely in their grasp by 1918. On three separate occasions throughout 1916, Germany pursued avenues to negotiate for peace, but both British and French resolve maintained that peace would only come about upon Germany’s defeat.[9]
Zionist leaders eventually came to the realization that Allied victory meant Russia’s influence would be amplified in the Near East. In early 1915, a conditional Entente agreement even allocated Constantinople to Russia. This posed an issue as Constantinople rested in the possession of the Ottoman Empire, an ally of Germany and Austro-Hungary. High-profile Zionists had their eyes eastbound on Palestine as a suitable place to lay the groundwork for a Jewish homeland. In 1896, the father of Zionism, Theodor Herzl, approached Sultan Abdul Hamid II and offered to pay off the Ottoman debt in exchange for a charter that permitted Zionists access to Palestine.[10] The Sultan outright refused.
The prospect of a promised land for Jews never escaped one highly influential man’s attention — Justice Louis D. Brandeis. Through Brandeis, Zionist leadership “passed into American hands by default.” He was considered one of the men of “light and lead” on whom Wilson relied.[11] Born in 1856 to secular Jewish immigrant parents from the present-day Czech Republic, he graduated from Harvard Law School at the age of 20 and settled in Boston to open a law firm focused on progressive social causes. In his early career, he was distinguished for his public advocacy against powerful corporations, mass consumerism, monopolies, and public corruption while advising methods to restrict the influence of big banks and money trusts in his collection of essays, Other People’s Money and How the Bankers Use It.[12]
These progressive positions would later be taken up by Democratic candidate Woodrow Wilson on the larger question of the role of the national government and the future of the American economic system. By that time, Louis Brandeis was head of both the Federation of American Zionists and the American Zionist Movement after meeting the English-born Zionist leader and close associate of the late Herzl, Jacob de Haas. The prominent Jewish lawyer was converted into a staunch Zionist under the mentorship of leading Zionists during that time, such as Aaron Aaronsohn, Horace Kallen, Shmarya Levin, Bernard Rosenblatt, and Nahum Sokolow.[13] From August 31, 1914, to October 1, 1916, Brandeis was also chairman of the Provisional Executive Committee for general Zionist affairs.
The Brandeis-Wilson coalition was the start of a political partnership with far-reaching consequences on the international scene until Wilson’s death. The opportunity for career advancement presented itself so visibly that Brandeis switched parties and carried his advocacies, including Zionism, into American political institutions as a high-ranking political figure with direct access to the newly elected U.S. president.
Upon Wilson’s presidential win in November, he noted to Brandeis, “You were yourself a great part of the victory.” During Wilson’s first year as president, Brandeis was instrumental in the behind-the-scenes creation of the Federal Reserve System in 1913. The ambitious president attempted to make Brandeis his Attorney General and later Secretary of Commerce, but intense resistance from corporate executives forced Wilson to rescind his plan to make the renowned radical part of his cabinet. Instead, he nominated him to the U.S. Supreme Court in 1916, and he was sworn in amid a public outcry.
At a time when correspondence between Zionist leaders and the American president was steadily rising, as the Great War intensified in its first year, Brandeis approached Wilson about Zionist plans, to which Wilson seemed receptive. By 1916, Brandeis established regular contact with the State Department on the future fate of the declining Turkish Empire following the war, with Hungarian-born leading Zionist and Rabbi Stephen S. Wise in communication with Wilson’s chief adviser on European politics and diplomacy during the First World War, Edward Mandell “Colonel” House, on Zionist objectives. Specifically, Wise functioned as an intermediary between Wilson and House from 1916 to 1919. Wise began his Zionist career in the late 1890’s by assisting the movement’s ideological development and organization of its membership. Another acquaintance of Herzl’s, he served as American secretary of the World Zionist Movement and was instrumental in producing the aforementioned Provisional Executive Committee for General Zionist Affairs.[14]
Opposition to American entry into the First World War cut across political, racial, and economic lines. Various factions of society, including socialists, anarchists, syndicalists, pacifists, civil libertarians, Marxists, rural southerners, Canadian and Irish nationalists, and women’s groups, were just some of the small but vocal minorities opposing American militarism. International socialist groups, for example, were keenly aware of the capitalist mobilization the war promised to big business rivals. The working class fought, while the ruling class profited.[15] This was America’s first debut as a global military power and pitted citizen against citizen until eventually the government itself grossly violated civil liberties under the Espionage and Sedition Acts.
In 1916, Wilson reignited his bid for re-election through his continued commitment to progressive change by calling for legislation regulating work hours and a minimum wage. Democrats campaigned on the slogan, “He Kept Us Out of War,” insisting to voters that a Republican victory would mean war with Germany. Just four months after his second inauguration, Wilson reneged on his campaign promise of neutrality and officially declared war. By this time, public resistance to this betrayal was minute. The preceding years of preparedness campaigns, patriotic zeal, and heavily propagandized press cycles swayed the consensus into viewing the war as just and necessary. Thousands more dissenters continued to be jailed, silenced, and deported under newly solidified justification.
Shortly after the U.S. entered into the war, the British Foreign Minister, Arthur J. Balfour, arrived in Washington. In a cable, James Rothschild urged Brandeis to discuss Zionism with Balfour on the viability of an English Zionist program to recognize Palestine as the Jewish national homeland. “Unanimous opinion is the only satisfactory solution for Jewish Palestine under British protectorate,” Rothschild explained in a telegram. Russian Zionists fully approve. Public opinion and competent authorities here are favorable… It would greatly help if American Jews would suggest this scheme to their government.[16]The charitable activity of the Zionist movement was over. Now an era of wielding political power has commenced to shift the tide of international conflict under the London-Moscow-New York axis.
Only one month after American entry into the war, Brandeis followed through with Rothschild’s request. Appealing to Wilson’s progressive vision for the globe, Brandeis explained that a Jewish Palestine would fulfill the conditions of the peace settlement Wilson desired; Turkish despotism would be swept aside for a democratic government where economic and cultural development would be undertaken by a historically suppressed people.[17]In reaction to the Balfour Declaration, Wilson said, “The allied nations, with the fullest concurrence of our government and people, agree that in Palestine shall be laid the foundations of a Jewish Commonwealth.”[18]
Partnered with Brandeis in courting Wilson was the Austrian-born Jewish lawyer and professor, Felix Frankfurter, a lifelong committed Zionist and member of the Zionist Organization of America. Frankfurter became acquainted with Brandeis in the Parushim, a secret Zionist society, reform movement, and arguably the first modern militant Zionist organization in America. Found by their former mentor, Horace M. Kallento, Zionist purpose was “a group much like the Peace Corps, young men and women who saw the Utopian opportunity that existed for the Jewish people in Palestine and who were willing to devote themselves to an ideal.”[19]
The ideological motivations for endorsing Zionism were personal for Wilson as well: “To think that I, the son of the manse, should be able to help restore the Holy Land to its people.” With Wilson formally persuaded, Brandeis passed along the good news via urgent cables to Rothschild in London. Two weeks later, Jacob de Haas, now advisor to Brandeis, cabled Russian born-Zionist leader and future president of the World Zionist Organization, Chaim Weizmann, not only outlining the plan for Palestine but to communicate “an accurate statement of the prevailing sentiment in the United States to be presented to the Allied Governments.”[20]
President Wilson was later asked directly by the British government about the likelihood of issuing a declaration of sympathy for the Zionist movement. Wilson responded that the time was not ripe. A month later, Wilson placed his full backing behind the affirmation as pressure mounted against Germany’s Turkish ally to make dispensations to the Zionists. The topic of the Balfour Declaration was on the table between the two world powers. Colonel House complained to Wilson in a note: “The Jews from every tribe have descended in force, and they seem determined to break in with a jimmy if they are not let in.”[21]
Brandeis’ influence over Wilson in regards to Zionist ambition could not be understated. Wilson once remarked that it was Brandeis to whom he owed his career. According to Frank Edward Manuel, Wilson’s interest in Zionism and including it as part of his foreign policy was “being slowly nurtured by Louis Brandeis, one of the men who stood closest to him in the early years of the administration and who became the key figure in future American intervention in Palestine.”[22]
A roadblock in the way of the highly anticipated declaration was the Counselor to the State Department, Robert Lansing. Lansing was completely bypassed in House and Wilson’s correspondence on the Balfour Declaration. In response, Lansing argued in a letter to Wilson why America must decline Balfour’s promise, noting that, among several reasons, “many Christian sects and individuals would undoubtedly resent turning the Holy Land over to the absolute control of the race credited with the death of Christ,” a flagrant secession from the protracted Christian support for the prophetic restoration of Israel.
Lansing ordered Ambassador Walter Hines Page to investigate and report prudently the British reasons for the Balfour Declaration. In spite of political opposition within the State Department, the declaration was officially signed by Lord Balfour after a two-year process of edits by British and American Zionists and officials. Despite its official status as a British document, it was Brandeis who spearheaded its drafting and application through Wilson.
News rapidly spread worldwide upon the issuance of the Balfour Declaration, with heaps of telegrams addressed to Wilson expressing their gratitude for his contributions. Leaflets were dropped over German and Austrian territory announcing, “The hour of Jewish redemption has arrived…” The Allies are giving the land of Israel to the people of Israel… Will you join them and help to build a Jewish homeland in Palestine? Stop fighting the allies who are fighting for you, for all the Jews… An Allied victory means the Jewish people’s return to Zion.”[23]
By the summer of 1918, Turkish resistance was waning and President Wilson took this time to formally announce his public endorsement of the Balfour Declaration in August. Three months later, Germany was the last of the Central Powers to sign an armistice agreement with the Allies. The war was over. The next battle would be held in Paris.
The ambitions of Wilson’s liberal internationalist foreign policy were outlined in the Fourteen Points and used as the basis of terms for Germany’s surrender at the Paris Peace Conference. The Peace Conference produced five treaties, one of which was the notorious Treaty of Versailles. There were a number of high-profile Jews present, not just in diplomatic positions but in many senior and important functions within the Allied delegations.[24] This included Baron Sonnino for Italy, Edwin Montagu for Britain, Louis Klotz for France, and Paul Mantoux as the interpreter for the “Big Three”—United States, Britain, and France.
Wilson also endorsed Rabbi Wise to promote the Jewish program for Palestine in Paris. Another Zionist delegate was Frankfurter, who was among the nearly one hundred intellectuals that signed a statement of principles for the formation of the League of Free Nations Associations. This formally enacted Wilson’s mission to dispel isolationism in favor of increasing American participation in international affairs.[25]
In the midst of empirical savagery slicing up Germany and parceling out Europe’s colonial holdings, the case for a Jewish homeland in Palestine was presented by a delegation of the Zionist Organization led by Weizmann. The terms of the newly established British Mandate involved promoting Jewish immigration and settlement, suggesting boundaries, self-government, and the assurance of religious liberty.
At the request of President Wilson, Jewish statesman and Wall Street financier Bernard Baruch attended the Paris Peace Conference as an advisor to negotiate a deal with the victorious Allied powers on the destiny of Germany.[26] He served as a member of the American Delegation to the Preliminary Peace Conference and on the Committee on Form of Payments of Reparations. Baruch is credited with managing America’s economic mobilization in the First World War while chairman of the War Industries Board. While Baruch opposed the strenuous financial tenets of punishing Germany, he nonetheless attempted to assist the Senate in passing the Treaty of Versailles.
Baruch also played a significant role in securing France’s vote in favor of the Palestine Partition Plan. He swayed their vote by visiting France’s UN delegate and heavily suggesting that failure to support the resolution could result in America withholding desperately needed monetary support as the war devastated France’s financial market.[27]
The renowned English economist, John Maynard Keynes, was also in attendance at the Peace Conference as a delegate of the British Treasury. Disgusted by the ravenous nature of the treaties, particularly the Versailles Treaty, Keynes publicized a negative portrayal of the treaties in his book, The Economic Consequences of the Peace. In response, Baruch paid John Foster Dulles $10,000 to ghostwrite his own book, The Making of the Reparation and Economic Sections of the Treaty, to counter Keynes by exalting the treaties.[28]
The most significant of American Jewish attendees, however, was Justice Brandeis himself, whose task at the world’s peace tables was to assist Colonel House “in collecting peace data for President Wilson.” The task was clear: “Colonel House will devote his attention to problems concerning the war in the west, while Justice Brandeis will study the near eastern question.” Their work will form the basis for the country’s contention.”[29]
For a liberal president known for endorsing and exporting democratic ideals even through coercion, its inconsistent implementation was noted during the peace talks and formally addressed on August 28, 1919, through the presentation of the King-Crane Commission. The commission argued that the establishment of a Jewish state in Palestine would inevitably lead to an immediate violation of the right of the indigenous Palestinian people to self-determination and deemed the Zionist program incompatible.
The report also stated that meetings with Jewish representatives led them to conclude that “the Zionists looked forward to a practically complete dispossession of the present non-Jewish inhabitants of Palestine through armed forces” and begged the Peace Conference to reject Zionist proposals. The findings of this report were suppressed for three years by Brandeis until after the Peace Accords were passed. Working diligently to ensure the stipulations of the Balfour Declaration were incorporated into the final arrangement was Frankfurter, who found the findings of the commission to “cheat Jewry of Palestine.”[30]
As the dissolution of the former Ottoman Empire began via the Treaty of Sevres, the vehicle for colonizing Palestine as spelled out by the Balfour Declaration was put into effect under the Brandeis-guided Wilson. The Council of the League of Nations and the United States both approved the Mandate for Palestine in July of 1922. It was clear from the beginning that the flagrant denial of self-government for the Palestinian population would continue until the Jews were strong enough to take the reins of government in the region.
For four days in April 1922, Congress debated resolutions brought forth to reaffirm the colonial implications of the Balfour Declaration as urged by Zionists. One of the vocal participants of its opposition was Professor Edward Bliss Reed, who testified in a prophetic hearing before Congress about the outcome of what American support entailed: “If you indorse the Balfour declaration, you are caught absolutely in the mandate…” What I want to warn you against is getting caught up in the mandate in what I consider an impasse. It will devastate this country, Palestine. I want to prevent my country from doing something that will bring it untold trouble.”[31]
Nevertheless, Congress was subjected to endless Zionist pressure and passed the Lodge-Fish Resolution endorsing the British Mandate for Palestine as laid out by the Balfour Declaration, which was signed by Wilson’s presidential successor, Warren G. Harding, on September 21, 1922.
When Wilson died two years later, the President of the Zionist Organization of America, Louis Lipsky, stated publicly, “Mr. Wilson followed with interest the progress of the Zionist movement even after he retired to private life.” In 1921, when informed that the Mandate for Palestine had been finally ratified, he telegraphed to the Zionist Organization of America: “I am proud that it should be thought that I have been of service to the Jewish people.”[32]
The First World War was proclaimed to represent “the war to end all wars”, bringing about a golden future on the promise of self-determination, democracy, mutual security, and peace. The cost would only be the blood and ashes of young, idealistic men committed to the service of their nation. What resulted was the pervasive indifference and lack of cohesive understanding of the memory of the war in spite of its devastating cost. As Steven Trout tried to explain the lack of American consciousness toward the war, “What exactly should the nation recall about the war? Is neutrality failing? The bravery of the combat soldier? The futility of trench warfare? The racial discrimination that permeated the ranks? Are there domestic attacks on German Americans? The botched peace processes? ”
Not to mention the American public that had opposed entry into Europe’s war was forced to grapple with the casualties of 120,000 soldiers and the reintegration of 200,000 wounded men, crippled of mind and body. For Wilson, it was his lifelong and close political partnerships with notable Jewish Zionists fully entrenched in American institutions that prompted his breakaway from isolationism—to which the United States has never returned. More consequential was Wilson’s setting the pattern for amplifying and servicing the dominance of a foreign state as the costs continue to rise.
Footnotes
[1] Jewish Telegraphic Agency, INC., “Leaders Pay Tribute To The Passing Of A Great Statesman,” Daily News Bulletin, last modified February 4, 1924, https://pdfs.jta.org/1924/02-04_025.pdf.
[7] Joseph Rappaport, “The American Yiddish Press and the European Conflict in 1914.” 113–28 in Jewish Social Studies 19, no. 3/4 (1957).http://www.jstor.org/stable/4465551.
[16] Rothschild and Chaim Weizmann to Brandeis (cable), April 21, 1917 (received April 25), Zionist Archives, New York City, Jacob de Haas Archives.
[17] Lebow, Richard Ned. “Woodrow Wilson and the Balfour Declaration.” The Journal of Modern History, 40, no. 4 (1968): 507 http://www.jstor.org/stable/1878450.
[19] Schmidt, Sarah. “The ‘Parushim’: A Secret Episode in American Zionist History.” American Jewish Historical Quarterly 65, no. 2 (1975): 122. http://www.jstor.org/stable/23880453
[20] De Haas Archives, Brandeis to Rothschild (cable), May 9, 1917.
[22] Ahmed, Hisham H. “From the Balfour Declaration to World War II: The U.S. Stand on Palestinian Self-Determination.” Arab Studies Quarterly 12, no. 1/2 (1990): 9–41. http://www.jstor.org/stable/41858937.
[24] Levene, Mark. “Nationalism and Its Alternatives in the International Arena: The Jewish Question in Paris, 1919.” Journal of Contemporary History 28, no. 3 (1993): 522. http://www.jstor.org/stable/260644.
[25] Gunther, Learned Hand: The Man and the Judge, 261.
[31] United States. Congress. House. Committee on Foreign Affairs, Hearings Before the Committee on Foreign Affairs, House of Representatives, Sixty-seventh Congress, Second Session, on H. Con. Res. 52, Expressing Satisfaction with the Re-creation of Palestine as the National Home of the Jewish Race April 18, 19, 20, and 21, 1922 (Kessinger Publishing, 1922), 23–24.
I was totally shocked to hear the claims by a fire scientist I had once admired and often quoted in my blog posts about wildfire. In a National Public Radio interview Jennifer Balch said, “Climate change has lengthened the state’s fire season”. Then she said “”Climate change is essentially keeping our fuels drier longer. These grasses that were burning, they’ve been baked all fall and all winter.”
Having studied fire ecology for 30 years and knowing her published science, I could only believe she had been corrupted by the need to attract large amounts of funding, and these days that comes to those who blame the climate crisis. And here’s why I now hold that opinion so strongly.
Colorado’s Marshall Fire was a grassfire that happened with temperatures hovering around freezing. All fire experts and fire managers know grasses are 1-hour lag fuels. That means in dry conditions grasses can become flammable within hours. Attempting to link CO2 global warming, she and other alarmists were now blaming the Boulder area’s grass flammability on the warm dry conditions from July through November. But dry conditions in the past months are totally irrelevant. Those months could have also been cold and wet, but just one day of dry conditions is all that is needed for grasses to burn.
To minimize recklessly set fire that often occurs as people burn away unwanted dead vegetation, the Nova Scotia government felt the need to counter the Myth that “It’s safe to burn grass as long as there is still some snow on the ground.”
The Fact is: “Within hours of snow melting, dead grass becomes flammable, especially if there have been drying winds. Grass fires burn hot and fast and spread quickly around, and even over, patches of snow.” That’s a fact that Balch and every other fire expert should know!
Apparently, Daniel Swain, a climate scientist at the University of California Los Angeles and the Nature Conservancy and acolyte of climate alarmist Michael Mann and Noah Diffenbaugh, also failed to understand grasses are 1-hour fuel. He stated in an interview for NBC’s article How climate change primed Colorado for a rare December wildfire that “Climate change is clearly making the pre-conditions for wildfires worse across most fire-prone regions of the world,”
But dry grasses are not the pre-condition to be worried about. The pre-conditions that neither Swain nor Balch shared with the public is well known: Boulder County’s invasive grasses increase fire danger. The “main offender is cheatgrass, which was likely introduced to the area alongside agriculture and ranching” and “is increasing fire danger by 29%”
In fact, in 2013 Balch published, Introduced annual grass increases regional fire activity across the arid western USA (1980–2009), writing “Cheatgrass was disproportionately represented in the largest fires, comprising 24% of the land area of the 50 largest fires” and that “multi-date fires that burned across multiple vegetation types were significantly more likely to have started in cheatgrass.”
It was also very disingenuous for Balch to say “Climate change has lengthened the state’s fire season”. It is the very same meme that every climate alarmist regurgitates that climate change has made “a year-long fire season the new normal”. But in 2017 Balch published in Human-started wildfires expand the fire niche across the United Statesthat human ignitions “have vastly expanded the spatial and seasonal ‘fire niche’ in the coterminous United States, accounting for 84% of all wildfires”. Balch’s published graph clearly shows that human ignitions have extended fire season all year long. Based on her own research, a more relevant comment would have mentioned that Louisville, Colorado’s population had jumped 10-fold; from 2,000 in 1950 to about 20,000 today. Does a 10-fold increase in population create a 10-fold increase in fire probability. The Marshall Fire was not naturally started by Lightning.
In 2015, Balch created the Earth Lab program at Colorado University. In 2017 it became part of CIRES, a partnership of NOAA and CU Boulder. Earth Lab, got increasing attention from mass media that’s always seeking click-bait. As Earth Lab’s team began blaming more fires on climate change, it got more attention and Balch got more interviews.
Earth Lab hired Natasha Stavros as Earth Lab’s Analytics Hub Director. In videos posted by the Washington Post, she claimed climate change causes “longer, hotter, and drier fire seasons” reflecting Balch’s conversion to a climate crisis narrative. To get around Balch’s earlier scientific research Stavros deflected, “We are not talking about the ignition source” or the “availability of fuels”, “what we are talking about are the conditions of those fuels”. But in the case of the Marshall Fire, 1-hour grass fuels have nothing to do with climate change. It only takes a few hours to be in highly flammable conditions. That’s weather, not climate!
Although lacking in scientific integrity, pivoting to a climate crisis narrative worked in Balch’s favor. The U.S. Geological Survey has selected the University of Colorado Boulder to host the North Central Climate Adaptation Science Center (NCCASC) for the next five years. Balch, as director of CIRES’ Earth Lab, and now NCCASC Director had attracted $4.5 million in funding. Universities around the country similarly create such centers to attract such major funding. Certainly, blaming fires on a climate crisis attracts more funding than if its director sounded like a “denier” blaming invasive grasses and human ignitions.
The politics of funding research requires a major level of group think. Daniel Shechtman won the Nobel Prize for discovering quasi-crystals that are now used in surgical instruments. But when he first announced his observations, he was kicked out of his lab by his colleagues. They saw him as a threat to the lab’s prestige and funding because observing quasi-crystals contradicted the consensus that was enforced by Linus Pauling that quasi-crystal did NOT exist.
Similarly, esteemed atmospheric scientist Dr Cliff Mass was criticized by Washington University administrator’s for detailing how an episode of problematic acidic waters that had been pumped into the state’s oyster’s hatcheries, was due to natural upwelling events, not climate change. But contradicting the climate crisis angle threatened funding to WU’s Ocean Acidification Center. Up until then Mass had been the Seattle Times go-to person for all weather events, but that stopped when his one analysis didn’t support climate crisis groupthink. Dr Peter Ridd was fired for presenting evidence showing his colleague’s claims of coral reef destruction were exaggerated. So, all savvy university professors know you can’t contradict the meme if you want funding, or worse, keep your job.
Climate crisis groupthink, also ignores natural climate change, as did Balch and Swain. But one meteorologist confidently blamed the lack of snow and dryness on a natural La Nina. The science is well established that depending on how colder Pacific surface waters set up during a La Nina, atmospheric currents can carry higher or lower amounts of moisture to different regions. California had record snowfall this December while Colorado snowfall was very low. And if the Marshall Fire had been ignited just 2 days later, there would have been a snowfall to suppress the fire.
However too often, alarmist scientists cherry-pick one-year events. They weaponized this year’s low snowfall while ignoring that last year’s Colorado snowfall was far above normal. In November last year, Fort Collins received more than 15 inches of snow on its way to 80 inches, which is 25 inches more than normal. Again, such variations in snowfall are weather, not climate.
Alarmists also weaponized the dry conditions as solely due to global warming drought. They ignored the drying and warming effects of the Chinook winds that are very common in Colorado. Chinooks are known as “snow eaters” because as the winds pass over the mountains of the western USA they are forced upward and precipitate all their moisture. When those winds descend from the Rockies down to Boulder, temperatures rise adiabatically (due to pressure not added heat) and the warm dry air quickly removes moisture or snow from the surface. Southern California’s Santa Anna winds are similar and drive large fires.
Sometimes Boulder’s winds reach speeds of 100+ mile per hour. NOAA reported The Chinook Wind Events Winter of 1982 during which peak wind gusts more than 100 mph damaged areas around Boulder. Weatherwise journal reported 100+MPH winds over Boulder on January 7, 1969, which snapped power poles and toppled planes as seen in the photographs below. In November 2021 the weather service gave a red flag warming due to the high winds from a Chinook event. But without a coinciding human ignition, there was no rapidly spreading fire.
I would like to believe that Balch’s Earth Lab scientists have been campaigning for the housing developments in Boulder’s suburbs of Louisville and Superior to create a system of firebreaks and defensible space. Those suburbs had built into easily ignited grassland in a region where fires are rapidly spread by the dry Chinooks descending from the Rockies. Such natural fire danger is not always obvious to the public looking for affordable housing. But it is not obvious that was ever done, at least not as obvious as faulty climate change narratives.
Fire experts should have pushed for building codes, requiring adequate spacing between new houses. As a story in Wildfire Today reported today, one common feature of the surviving homes was they were more distant from neighboring homes. Many houses in the devastated subdivisions were only 10 to 20 feet apart. Without adequate fire breaks or defensible space, if just one house allowed the fire to reach it, the heat of that burning house is enough to ignite any house next to it. Similar dynamics were seen in California’s Tubbs and Camp Fires that demolished neighborhoods.
But perhaps local governments were greedy. Eager to build a tax base a growing Louisville population was most important. Politicians had worked hard to present Louisville as one of the top 10 most livable little cities. Putting natural fire danger front and center, might put a damper on the city’s attractiveness. And not surprisingly the Denver Democrats didn’t waste time to capitalize on the Marshall Fire devastation. The released a statement claiming “This fire has also punctuated our climate crisis and made abundantly clear the need for bold action. The science is clear, and the impacts are very real. We will continue to work with our community and legislators to ensure climate change is treated with the urgency and attention it deserves.”
But the science does not show a connection between the Marshall Fire and Climate Change. And due to the greed of the media, politicians, and selfish scientists, only scientific integrity is facing a real crisis.
Finally, it is worth noting that some scientists are acutely aware of the increasing fire danger presented by the build-up of dead vegetation. To remove that hazard prescribed burns are being performed. But sometimes prescribed burns get away and burn down people’s homes. So prescribed burns are carefully planned for times when fires are most easily controlled. So, one must wonder just how unusually dangerous local conditions were if the City of Boulder planned a prescribed burn on Monday, December 13, 2021, just 2 weeks before the Marshall Fire. Had climate change really made conditions so dangerous?
Jim Steele is Director emeritus of San Francisco State University’s Sierra Nevada Field Campus, authored Landscapes and Cycles: An Environmentalist’s Journey to Climate Skepticism, and proud member of the CO2 Coalition.
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

 During Tony Blair’s time in office, Downing Street allegedly ordered former defence secretary Geoff Hoon to burn a secret memo that questioned the legality of the 2003 Iraq invasion. Hoon makes the bombshell claim in a new memoir.
During Tony Blair’s time in office, Downing Street allegedly ordered former defence secretary Geoff Hoon to burn a secret memo that questioned the legality of the 2003 Iraq invasion. Hoon makes the bombshell claim in a new memoir.

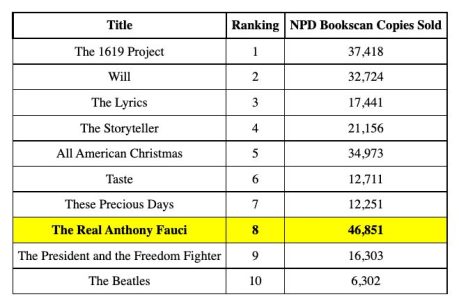







 Aletho News
Aletho News