COVID Vaccine Intended To Reduce World’s Population Without Anyone Suspecting Says Leading Doctor

Great Game India | November 27, 2021
The leading doctor credited with improving early treatment of COVID-19 said in a conference that the goal of vaccine transmission campaigns is to “control and kill off a large proportion of our population without anyone suspecting that we were poisoned.”
“The deaths that are meant to follow the vaccinations will never be able to be pinned on the poison. They will be too diverse, there will be too many, and they will be in too broad a timeframe for us to understand that we have been poisoned,” claims Dr. Shankara Chetty.
According to his website, South African family doctor Dr Shankara Chetty, “has treated 7,000 Covid-19 patients without a single hospitalization or death,” combining his insights with his medical background along with his observations of government censorship orders and censorship of medias to support its conclusions.
Joining the Zoom conference as a Doctor, Chetty began by asking the following questions:
“I think the perspective around what is happening is vitally important. We need to understand what the aim is. Everyone knows that there’s inconsistencies, that there’s coercion, but we need to understand why. Why is it there?”
He then identified the “most important” answer to these questions, “pathogen that was causing all the death in COVID illness,” the spike proteins common in both the vaccine and virus designed to be produced in a revivers body.
In my opinion of what’s going on in the world, spike protein is one of the most man-made toxins. And the purpose of this toxin is to kill billions of people without anyone noticing, he went on to add.
“What looks like transpired here, [is] they’ve engineered a virus and put this weapons-grade package onto it called ‘spike protein.’”
The allergic reaction with the initial release of the “most elaborately engineered toxin,” occurs in a small number of people, resulting in more severe cases and death when the vaccine is administered. According to Chetty, this usually happens eight days after the onset of symptoms.
Doctors say that due to the first 14-day international shutdown, people with the COVID-19 virus that caused it are arriving late to the hospital, and these facilities “to engineer death and damage in order to stir all the fear.”
“But the game that they played with this engineered virus was to justify the vaccination of the planet,” he continued.
Chetty added that these injections “expose us to the spike protein for a longer period.”
I often interview doctors online, and Dr. Pierre Kory, Ryan Cole, and Richard Urso have described how long a health risk begins to occur after death from an allergy in the first two weeks.
“We begin to see the endothelial [blood vessel lining] injuries that this vaccine causes with its spike protein, with its influence on its ACE2 receptors. Those are the deaths that are meant to follow. And they will never be pinned onto the spike protein, a very well-engineered toxin,” he said.
“Now spike protein is also a membrane protein. So, the mRNA will distribute this throughout our body. It will be made in various tissues around our body. It will be incorporated into those membranes around our body, and those specific tissues.”
“Those tissues will be recognized as foreign and will trigger a host of autoimmune responses. So, the deaths that are meant to follow the vaccinations will never be able to be pinned on the poison! They will be too diverse, there will be too many, and they will be in too broad a timeframe for us to understand that we have been poisoned,” he went on”
“Now this toxin in the long term is going to get people with pre-existing illness to have those illnesses exasperated,” the doctor explained.
With some toxins, including “bits of HIV protein” within this “definitely engineered” spike protein, Chetty states “people with cancers are going to have their cancers flareup, and they will say they died of the cancer.”
“People with vessel injuries or predisposition like our diabetics and [those with] hypertension are going to have strokes and heart attacks and the rest at varying times, and we’ll attribute those to their preexisting conditions,” he said.
“People are going to develop, over time, autoimmune conditions, the diversity of which will never be addressed by any pharmaceutical intervention because they’re far too targeted.”
“But I think if people understand what the intention is, then they’ll understand why what’s happened has happened. The ill logic, the coercion, the suppression, is all warranted if you understand that there is a bigger plan.
This plan is to make sure that we can control and kill off a large proportion of our population without anyone suspecting that we were poisoned,” the COVID specialist said.
“And so, I think the justification for everything we see is warranted in understanding the endgame,” he concluded.
“I think there’s a huge picture at play; otherwise the vaccines make absolutely no sense. We were sold the vaccine as our savior from the start, and if we look at the science, the science does not play out.”
Official Data shows Deaths of male Children are up 54% since they were offered the Covid-19 Vaccine
THE EXPOSÉ | DECEMBER 4, 2021
An investigation of official ONS data has revealed that since the Covid-19 vaccine was offered and administered to kids in England and Wales there has been a 54% rise in deaths among male children compared to the same period in 2020.
The UK’s Medicine and Healthcare product Regulatory Agency (MHRA) have openly admitted that they suspect myocarditis and pericarditis are potential side effects of the Pfizer and Moderna Covid-19 vaccines, especially among young males. A suspicion that has been strong enough for the UK Medicine Regulator to officially add warnings about myocarditis and pericarditis to the safety labels of the Covid-19 vaccines.
Myocarditis is inflammation of the heart muscle, whereas pericarditis is inflammation of the protective sacs surrounding the heart. Both are extremely serious conditions due to the vital role the heart plays in keeping a person alive, and the fact that the heart muscle cannot regenerate. Serious myocarditis can lead to cardiac arrest and knock years off a persons life.

The UK Government have now also admitted in official documents that a high percentage of all hospitalised children are presenting to hospital with Myocarditis following Covid-19 vaccination.

Source
This fact adds greater concern for data published by Public Health England on the number of 999 calls made requesting an ambulance due to cardiac arrest. The stats show that they have skyrocketed against the expected average since young adults and teens began receiving the Covid-19 vaccine.

Chris Whitty advised the UK Government to roll-out the Pfizer Covid-19 vaccine to all children over the age of 12 in week 37 of 2021. Thanks to preparations already being made by the NHS to intrude on education in schools and administer the jab to children, the roll-out got underway the following week (week 38).
The 2020 edition of ‘Deaths registered weekly in England and Wales, which can be downloaded here, and accessed on the ONS website here shows the number of deaths registered weekly by age group.

Source
The ONS data shows that between September 18th and November 13th 2020 a total of 24 deaths occurred among male children aged between 10 and 14.
However, the 2021 edition of ‘Deaths registered weekly in England and Wales, which can be downloaded here, and accessed on the ONS website here, shows a significantly higher number of deaths have occurred among male children in 2021 following Chris Whitty’s decision to offer them the Covid-19 vaccine.
The data shows that between week 38 (week beginning 18th September) and week 46 (week ending 19th November) of 2021, a total of 37 deaths occurred among male children aged between 10 and 14.

This shows that since the Covid-19 vaccines began being given to kids over the age of 12, deaths among male children have increased by 54% compared to the same period in 2020.
We compiled the following graph on ONS figures so that we were able to easily compare the number of deaths per week among male children in 2020 and 2021.

The data is there now for the authorities to see, a 54% increase in deaths of male children compared to 2020 since they started to be given the Covid-19 vaccine, they must investigate this and cease the roll-out of the jabs to kids immediately.
2,809 Dead Babies in VAERS Following COVID Shots as New Documents Prove Pfizer, the FDA, and the CDC Knew the Shots Were Not Safe for Pregnant Women
By Brian Shilhavy | Health Impact News | December 4, 2021
The latest data dump into the U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) happened yesterday (12/3/21) and covers data through 11/26/2021.
There are now 927,740 cases reported to VAERS following COVID-19 shots for the past 11 months, out of the total of 1,782,453 cases in the entire VAERS database filed for the past 30+ years.
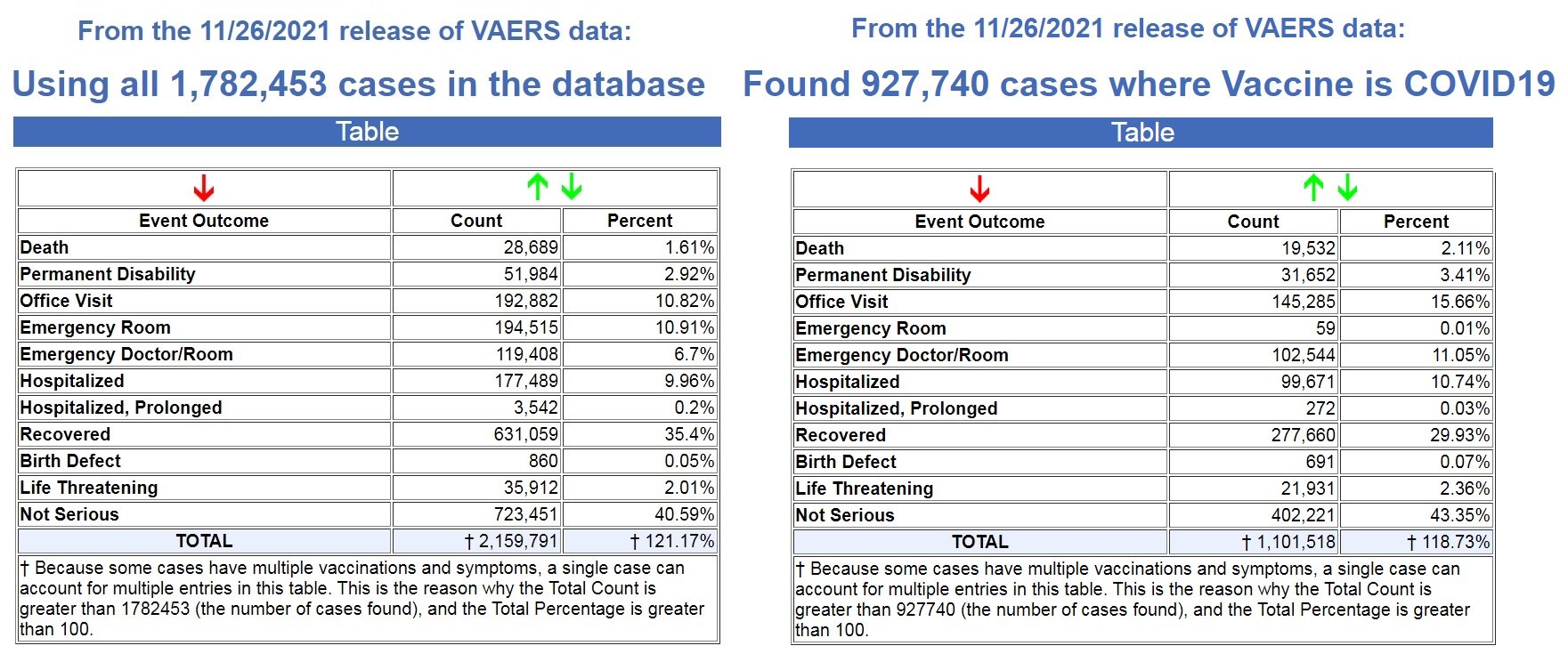
Left image source, Right image source.
That means that 52% off ALL vaccine adverse reaction cases in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
In addition, 68% of all deaths following vaccines reported in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
We are on pace to see 21,307 deaths reported in the first year following the experimental COVID-19 shots, while the average yearly deaths reported after FDA-approved vaccines for the past 30+ years is 305 deaths.
That is an astounding 86% increase in reported deaths following the COVID-19 shots, a 70X increase over the average reported deaths following vaccinations for the past 30+ years!
- FDA-approved vaccines: 305 deaths per year
- COVID-19 EUA shots: 21,307 deaths per year
And as Dr. Jessica Rose has previously reported, the under-reporting factor in VAERS for the COVID-19 shots is 41X, as a conservative number, which means that at least 800,812 people have now died following COVID-19 shots based on the VAERS data.
Most, if not all, of those deaths are being reported in the pharma-owned corporate media as “COVID” deaths, as there are now more recorded “COVID deaths” for the first 11 months of 2021 than there were for the entire year in 2020, when there were no COVID vaccines until December. (Source.)

Record Number of Fetal Deaths Following COVID-19 Shots
As of this most recent update in VAERS, we have now found 2,809 fetal deaths following COVID-19 shots injected into pregnant and child-bearing women for the past 11 months. (Source.)
By way of contrast, using the exact same search parameters in VAERS, but excluding the COVID-19 shots, we found 2,168 fetal deaths following all FDA-approved vaccines for the past 30+ years. (Source.)
That’s an average of 72 fetal deaths per year following all FDA-approved vaccines for the past 30+ years, compared to what is on pace to be 3064 fetal deaths in 1 year following COVID-19 shots.
- FDA-approved vaccines: 72 fetal deaths per year
- COVID-19 EUA shots: 3064 fetal deaths per year
That is an 80% increase in fetal deaths recorded in VAERS following the COVID-19 shots. And yet, the CDC and FDA continue to recommend these EUA shots for pregnant women and nursing mothers.
Not only do they recommend these shots for pregnant women, we now have ample evidence that they have known since earlier this year that these shots are dangerous to pregnant women, and causing fetal deaths.
In a March 4, 2021 Advisory Commission on Childhood Vaccines (ACCV) meeting, the CDC submitted a report that contained a section titled: Maternal vaccination safety summary (starting on p. 39).
They stated (emphasis mine – my comments in red):
* Pregnant women were not specifically included in pre-authorization clinical trials of COVID-19 vaccines
– Post-authorization safety monitoring and research are the primary ways to obtain safety data on COVID-19 vaccination during pregnancy
* Larger than expected numbers of self-reported pregnant women have registered in v-safe
* The reactogenicity profile and adverse events observed among pregnant women in v-safe did not indicate any safety problems (based on what criteria???)
* Most reports to VAERS among pregnant women (73%) involved non-pregnancy specific adverse events (e.g., local and systemic reactions)
* Miscarriage was the most frequently reported pregnancy-specific adverse event to VAERS; numbers are within the known background rates based on presumed COVID-19 vaccine doses administered to pregnant women (no supporting evidence to backup these claims)
It is important to note through all of this reporting by the CDC that these are based on self-reporting data from pregnant women.
We know that it is politically incorrect to blame any health issue on a COVID-19 “vaccine,” and that doctors and nurses are pressured to NOT report these, so how many pregnant women had an adverse reaction, like a miscarriage, and never even thought to link it to their COVID-19 shot?
So back in March of this year (2021), there were already major concerns about the effects of the shots on pregnant women, as “larger than expected” pregnant women were reporting adverse reactions, and “the most frequently reported pregnancy-specific adverse event to VAERS” was “miscarriage.”
Then in August of this year (2021), the CDC presented a “new study” with “new data.”
Again, this “data” is dependent on pregnant women “self-reporting” adverse reactions, so we know these reports will be well below what was actually happening in the population, as it is politically incorrect to report any adverse reactions related to the experimental COVID-19 shots. To do so is to be branded an “anti-vaxxer” and shame you for life.
The August update admitted that 13% of the pregnant women who had received a COVID-19 shot reported a miscarriage. The CDC brushed this aside by stating “miscarriage typically occurs in about 11-16% of pregnancies.”
But of course ALL miscarriages are reported somewhere in the medical files, which is why they can even come up with a number range like this. So this figure is based on 100% of the reported data, while the COVID-19 related miscarriages are only based on what was self-reported, and we have no idea how many women never reported their miscarriages because they never related it to their COVID-19 shot.
One the main studies the CDC allegedly relied upon to declare that COVID-19 shots were safe for pregnant women, was a study published in the New England Journal of Medicine on June 17, 2021.
But on October 14, 2021, they issued a statement stating that some of their data was wrong in the June 17th study. (Source.) It dealt specifically with pregnancies in their 20th week or earlier.
“No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for gestational week–specific risk of spontaneous abortion.” (Source.)
The chilling new ‘advice’ on vaccine heart risk for children
By Kathy Gyngell | TCW Defending Freedom | December 3, 2021
I HAVE just been alerted to the Government’s new Myocarditis and pericarditis after Covid 19 vaccination: guidance for healthcare professionals, published four days ago on Monday. It makes chilling reading.
You can read it here.
First, it is a clear admission of that myocarditis is a serious post-vaccine adverse reaction risk. Second, amongst the usual and increasingly implausible disclaimers like ‘it is a rare condition’ and ‘it is usually mild or stable and most patients typically recover fully without medical treatment’, comes the terrifying admission that ‘a high percentage of children admitted to hospital with myocarditis have significant left ventricular fibrosis and no follow-up data is available yet on hospitalised patients.’
So does it recommend halting the vaccine programme for children, given ‘that no follow-up data is available yet on hospitalised patients’?
No.
In complete defiance of any precautionary principle the subtext of this disturbing document is that these are reactions that are expected, not to be alarmed by and to be lived with as an inevitable consequence of the vaccination, giving what should be self-evident advice that though ‘the majority of cases appear to be mild and self-limiting; any acutely ill or unstable patients should be referred to hospital directly’. As though an acutely ill child was not normally treated as an emergency and rushed to hospital.
Furthermore, how they can claim to know at this stage that ‘ the majority of cases are mild and self-limiting’ in the absence of rigorous and systematic follow-up health checks on such children? It beggars belief and betrays an astonishingly cavalier attitude to children.
Even more chilling, if that were possible, is the publication of this document on the very same day that the JCVI decided to recommend second vaccine doses for 12-15s.
The opening few bullet points include these gems:
· Myocarditis – significant left ventricular (LV) fibrosis has been described in a high percentage of children admitted to hospital, with a small percentage of these having non-sustained ventricular tachycardia (VT);
· No follow-up data is available yet on hospitalised patients;
· The long-term consequences of this condition secondary to vaccination are yet unknown, so any screening recommendations need to be balanced against the frequency and severity of the disease with the aim to prevent complications, in particular of myocarditis (arrhythmias, long term myocardial damage or heart failure).
The question is also raised as to why would a GP not refer every child or youth with suspected myocarditis or pericarditis to the paediatric team for a full assessment, especially given this is a vaccine still under emergency use authorisation requiring proper post marketing surveillance? Perhaps the government doesn’t want to find too many cases?
Please, please do anything and everything you can to bring this to the attention of parents.
Some 80 per cent of school children* are estimated to have had Covid already and so have nothing to gain from vaccination, only the potential risk of harm.
*MRC Biostatistics Unit’s statistics on infections and deaths, which are updated once a week using ONS data, estimates that 5.53 million 5-14-year-olds in England have had Covid. This is of a total population of 6,975,037.
Scenarios in Response to the New War Against Humanity
By Doug E. Steil | December 2, 2021
In light of recent developments in the western world it has become abundantly evident to most informed observers that a war against the general population has been launched under the guise of counteracting a viral pandemic. Through a process of coordinated incrementalism governmental efforts have focused on implementing a totalitarian population control system rather than appropriately targeting public health problems associated with a limited viral outbreak.
A key mechanism in this control process has involved coercive means to inject as many people as possible with an experimental gene therapy concoction with proven toxicity, in some cases deadly, which however has been ineffective in its claimed suppression of viral infection and transmission to others. The established term “vaccination” was misappropriated to mislead the public into believing that getting these shots would lead to salvation by protecting themselves and others around them. These toxic doses were authorized for emergency use a year ago based on various fraudulent misrepresentations, which included relying on false test results, suppressing viable treatment protocols, such as those published by physician Dr. Peter McCullough, rigging trial designs and aborting prematurely, and manipulating statistical interpretations in a manner that created the impression they were effective when they were not. Though their producers acknowledged unforeseen effects they demanded contractual indemnification against bad outcomes. The failure to properly inform the public about the facts surrounding these substances, including known and potential adverse effects, in conjunction with the aggressively coercive measures to compel millions of people to submit to receiving them into their bodies, constitutes crimes against humanity in accordance with the Nuremberg Code, established in 1947.
At least technically, thus far getting these toxic injections was voluntary, but a substantial portion of the public saw through the scam or were reservedly skeptical, for which they have been publicly vilified in a vicious defamation campaign propagated by the mass media, operating in concert with the pharmaceutical industry and governments. Only a few days ago – November 19 in Austria and November 30 in Germany – a critical red line was crossed through announcements by public officials, of impending requirements for everybody, including kids, to get these toxic injections, purportedly against a virus from Wuhan that has long since mutated. Today Angela Merkel expressed her endorsement of such measures, though she will no longer be in power to vote for them. The mantra has been simply that this was necessary – indeed “the only solution” – in order to increase the overall so-called “vaccination rate” in the population, as if though that could somehow solve ongoing health problems. Since there is no substantive evidence for these sensationalistic claims, it equates to pure political demagoguery. Yet, contrary to this transparently false claim, mandatory injections, possibly on a repetitive basis, would only exacerbate the current situation purportedly occurring in emergency rooms or intensive care units at hospitals because the shots do not provide any remedy but cause harm instead, in some cases almost immediately, in many cases cumulatively. Essentially, this highly controversial mandate amounts to a subversive extermination campaign in the long run, deriving from likely cases of infertility and decreased life expectancy. In order to deflect from their previous lies, officials have chosen to raise the stakes an thus declared war against humanity.
Such an egregious attack as this is unprecedented in recent memory, so it may be difficult for many to understand what is occurring, right in front of their eyes. There may be a prevailing inclination toward cognitive dissonance, but it is preferable to assess various means to counteract such ominous developments within the full scope of possible scenarios that may arise. Below are five situations, beginning with the most obvious. Subsequent response scenarios represent an escalatory progression. Though they are not equally likely to occur and may be less specific to some regions, such results cannot be ruled out entirely when considering the volatile social conditions that are caused by governments that have intentionally gone rogue. In the pursuit of conquest, they have split and destabilized society, a recurring modus operandi when regarded in a historical context, back to Philip II of Macedon and Julius Caesar – divide et impera.
• Legal Challenges
The stated rationales for implementing compulsory injections of toxic substances, euphemistically referred to as “mass vaccination”, cannot be legally justified under any circumstances under existing protections, therefore the arguments presented to the public are all based on provably false premises or wishful thinking. They have been repeated so often, that many have already internalized them to be functionally true. At their core have been false promises of immunity, appeals to social solidarity, moral self-righteousness, and an unproven notion of easing the potential demand for medical services. If only everybody had volunteered to get the shots, the claim goes, the outbreak would have been eradicated; therefore mandatory injections are the only solution. None of this is true; on the contrary the data show that case hospitalization rates increase in correlation with the proportion of administered injections. Yet even if it were true, there are basic legal protections in place worldwide that forbid such mandates.
Many people understand this as self-evident and therefore expect the legal process to work, as it should, in theory. They may regard the announcements as typical hot air from politicians as a tactical means of leveraging their authority to exert additional pressure on those people who had not made up their minds yet about this vital question and presume the judicial reviews will enforce a reversal. Though this would be a reasonable expectation if the facts and the law were followed, the problem is that the legal process has become hopelessly corrupted. Reiner Füllmich, one of the founders of the Corona Investigative Committee, which has broadcast the 80 weekly sessions it has held thus far, has repeatedly confirmed that the German legal system has been so thoroughly corrupted, that bringing forth such matters before a system with an Anglo-American legal tradition makes more sense. Contemporary judicial rulings in Germany can be so out of touch with reality that it is difficult to imagine that decisions in prior totalitarian regimes could have possibly been any worse. Even so, it is still necessary to formally proceed through this avenue in order to be able to justify taking additional steps if it should turn out that cynical expectations of an inherently corrupted system are confirmed. There is also the possibility that the time it takes to submit to the judicial review process will result in the matter becoming moot, so that the stated premises for the mandates no longer obtain and are formally withdrawn.
The sheer suddenness and public lying that accompanied these announcements, which were completely contrary to repeated promises made by these same politicians who then proclaimed there was no alternative, shows they deserve no trust. They will say and do whatever they feel will defer the truth from emerging and in the meantime protect themselves from embarrassment. Once they have gone so far as to thrown aside basic principles – having in effect become criminals of the worst kind – one can no longer expect to reverse themselves in response to appeals to decency.
• Passive Resistance
This is an effective path that many skeptics and opponents of totalitarian edicts have already chosen. Examples of this have been the numerous work stopages among US airline pilots, or hospital staff quitting their jobs. In the Italian port cities of Trieste and Genoa dock workers have gone on extended strikes in response to onerous governmental impositions still falling short of universal mandates to submit to toxic injections.
During the most recent session of the Corona Investigative Committee four specialists working in Austria, of which three are physicians, presented responses to the Austrian announcement of future mandates a week earlier, which was followed by large demonstrations in Vienna on the next day, which were said to have involved the participation of more than a hundred thousand protesters. The fourth guest , an attorney, started a political party that immediately received sufficient acclaim to be represented in the provincial government of Upper Austria. He stressed the importance of mass resistance and announced liaison efforts with various unions in addition to forming new union representation.
Mass strikes and roadblocks associated with the yellow vest movement in France have shown how determined efforts by a coordinated group of dedicated individuals can force the government to back down under persistent pressure. For people who understand why they have adamantly refused to be injected with a toxic substance for the sake of a failing mass experiment the imposition of a mandate would be regarded as an existential issue. Sane people do not risk the threat of premature death, severe sickness or disability for the sake of satisfying the power egos of corrupted political puppets and greedy profiteers.
Big demonstrations have recently taken place in numerous cities in the Netherlands, France, Britain, Australia, Croatia, Warsaw, and many other locations. Even during the cold winter months hundreds of thousands of protesters will go out onto the streets to show their strength.
• Active Rebellion
On July 20, 1944, as part of Operation Valkyrie, Claus Von Stauffenberg participated in a plot to kill Adolf Hitler and other leading cohorts by means of a suitcase bomb placed in a conference room. The bombing killed a stenographer instantly but the coup failed because the intended targets survived. After the follow-up arrests nearly five thousand individuals, including Von Stauffenberg were executed. That particular assassination attempt continues to be commemorated in contemporary times on the date of the anniversary. Von Stauffenberg is glorified in the German media as a hero even though he was a German nationalist and purportedly expected to replace Hitler with another authoritarian government, though ruled instead by aristocrats like himself. Moreover, his co-plotters had earlier helped Hitler come to power and shared many of the same policy goals. In other words, the disagreement they had with the government was about methodology and style, along with certain details, rather than wanting to transform society along a new democratic course of redemption. In other words, had their coup attempt been successful, there was likely to be far less ideological change than occurred as a consequence of the coup against John F Kennedy nearly six decades ago in Dallas, in which Lyndon B Johnson was a plotter and beneficiary. From a judicial perspective, it is said, the German government had not blatantly broken any existing laws. In any case, an implicit question that the German media do not appear to have answered in this context is: from what specific time onward in the history of that regime would it have been legitimate, without possessing any benefit of foresight, for Von Stauffenberg to have participated in multiple assassinations, and how many additional functionaries would they likely have executed subsequently?
It is relevant to bear in mind such conjecture because the fourth part in Article 20 of Germany’s Basic Law contains an essential element that explicitly states that all Germans have a right to resistance against anyone who proceeds to eliminate the specific democratic and social order enumerated in the prior three sentences, if other remedies are not possible. The first twenty articles have a special status; they cannot be revoked. What was openly suggested by the next chancellor and successor to Merkel, Olaf Scholz from the Social Democratic Party, was a significant milestone in German post-war history because this unprecedented proposal, which was universally acknowledged by everyone to be unconstitutional and unworkable, would constitute a blatant violation of Article 2, guaranteeing bodily integrity, in case it were ever to be imposed upon the population. This explains why nobody has ever gone this far, to step over the red line. They were previously reluctant to do so, but now they are playing with fire. If legal challenges to this usurpation of the most basic human principles are thwarted under some imaginary and invalid pretext, the circumstances premised in Article 20 will legally enable and authorize Germans to resist against all those who brought about the transgression. It should be noted that exercising such resistance does not – and logically cannot – rule out the use of force.
Understandably there is little legal precedence for how the right to resistance may play out, except for abiding by the general principle of proportionality, which itself is somewhat vague in the context of potentially existential measures being threatened against a substantial portion of the population. It is known that there are clandestine groups who are armed because they have been anticipating a potential situation like this, just as in the United States millions of Americans bear firearms to protect against potential tyranny pursuant to the Second Amendment of the US Constitution. One can imagine that the imposition of an illegal law that would essentially force virtually the entire population to get toxic injections, against their will, so that their life span will be shortened, will simply not be accepted by many. Official jurists may claim now that they are not threatening to forcibly inject dissenters, this is just a “cute” technicality, and there is no way to know if that claim will be revoked a few weeks or months later, as the totalitarian escalation continues. Though utilizing violence as a means of exercising the right to resist, as distinct from self defense, is not rooted in jurisprudence, its use is fueled instead by image ideation in the media as well as historical narratives. This can lower the threshold level for some individuals to criminally act out their rage. Only a few weeks ago, in late September, a person not wearing a face mask got triggered at a gas station by being told to wear one, based on a valid ordinance. This made him so angry that he came back with a gun and killed the employee, a student who was working there part-time. While some may act out their resentment impulsively, others might choose to express their resistance selectively. If a top-level politician were to be targeted in a violent way, this would surely provoke a disproportionate and unwelcome response.
An episode in German history highlights how easily and quickly things can get out of control. On November 7, 1938 Herschel Grynszpan, then a 17-year old Jew, assassinated the German diplomat Ernst Vom Rath at the German embassy in Paris, through five shots into the abdomen, on behalf of persecuted Jewry, as he claimed immediately thereafter. Grynszpan was living in Paris illegally as a stateless person and had gained access to the embassy by falsely claiming that he had valuable secret information that he wanted to share with a top official. That was the event that triggered the Kristallnacht in various cities in Germany two days later.
An important prerequisite for introducing and enhancing totalitarianism is to manufacture and cultivate a scapegoat group that is to be reviled by the general population. Over the past few months German media have been denouncing all those who refuse to get toxic shots as somehow being primarily responsible for the fact that hospitals are having to deal with patients complaining of respiratory problems, most of whom, if they are below seventy years old, have a weakened immune system due to overweight or obesity issues. A common media ploy to reinforce this fabricated hatred is to have reporters go around town with camera and microphone and film ordinary people on the street giving their opinion about these awful “unvaccinated” people. The negative attitudes will then be selected to be shown on television, providing a feedback loop to convey that such opinions are perfectly legitimate. The next phase in this perception management scheme then entails presenting the public with skewed opinion poll results, based on undisclosed methodology, which embolden legislators to invoke public support for unpopular and inherently illegitimate measures.
A necessary premise for maintaining democracy is for the population to be properly informed, not brainwashed with lies and hate, so they can make valid decisions based on facts. Yet democracy is in the process of being subverted. Two of Germany’s top weekly publications with a daily online presence, Der Spiegel and Die Zeit, based in Hamburg, have both received generous direct funding from the Bill and Melinda Gates Foundation, according to their web site. Not surprisingly, these publications have been among the more vicious disseminators of lies and vituperations against conscientious dissidents. German politicians in conjunction with the media have thus already prepared the stage for future expressions of street violence by disgruntled individuals and may themselves become caught up in such activity due to their undermining of law and democracy. For instance, as in the United States, especially as occurred during riots in the summer of 2020, it is not uncommon for one political group to stage a peaceful public demonstration. An opposing group, virtually always self-proclaimed “leftists”, nowadays including hoodlums with an affinity toward Antifa, will announce a counter-demonstration with the goal of preventing the first group to exercise their right to march along a predetermined route. Police and journalists often get caught up in the violence perpetrated by the second group of counter-demonstrators, for which the first group then gets blamed. Such activity on the streets is representative of an unfortunate societal breakdown on a larger scale. This development is exactly what enemies of Germany, such as the Green Party, which has been characterized by distinctive totalitarian flavors since its inception in 1980, would relish to spread. Its activists seek to capitalize on such situations to attain increasingly tighter control. It will be interesting to see how exercising the right to resistance will play out next year.
• Paramilitary Rejection
In a few cases a ruling elite exercising power through government can become so corrupt and disliked that the military temporarily takes over and becomes welcomed for their intercession by a substantial portion of the population. The best example of this practice is Thailand, where perennial military takeovers have a different manifestation than in African or Latin American nations. In many smaller European countries the military has taken on a more subdued role since the likelihood of fighting defensive wars to defend their own territory has decreased. This may be one explanation for a recent trend toward female defense ministers who lack military experience. Yet this should not mean they should feel or become irrelevant. They can assert themselves in special emergency situations such as natural weather catastrophes but also as a necessary back-up of police force activity. They are also particularly well equipped to secure borders to neighboring countries and airports, as well as their national radio and television broadcasting facilities, just in case a corrupt government were to become carried away with excessively abusing power to the detriment of a large segment of the population. This readiness for such contingencies may be because its leadership and soldiers have taken an oath that they tend to take more seriously than career politicians do.
A few hours after it was announced that the Austrian government would aim to implement a general requirement for experimental gene therapy through toxic shots, and a call by a leading opposition politician for large demonstrations against such plans the following day in the center of Vienna, there was an interesting report from The Free Thought Project under the following headline:
The following is excerpted from the news story:
“The police and the army refuse to control the health pass in the name of ‘freedom and human dignity.’ They will join a large demonstration against compulsory confinement on November 20, 2021 in Vienna” […]
“Austrian Armed Forces Union (FGÖ) President Manfred Haidinger followed suit and joined in a letter published on 14 November. He intends to “defend fundamental rights and freedoms”. The FGÖ specifies that “everyone” is authorized to demonstrate, even in the event of confinement! The obligation of control imposed by the Minister of the Interior, Karl Nehammer has already been rejected by the police union. In addition, the Union of Austrian Armed Forces announces that they will participate in this great gathering in Vienna.”
The chairman of the Social Democratic Trade Unions (FSG) and the Police Union, Hermann Greylinger said in an interview that the police don’t want to carry out these checks.
Legislators in parliaments propose and pass laws with the tacit presumption that such legislation will ultimately be enforced by the state power apparatus. However, if such legislators or judges should step too far out of bounds by attempting to prevent large demonstrations, as was the case in Berlin a few months ago, or by announcing a determination to implement potentially dangerous and transparently illegal mandates, then it is a duty for those who would be encumbered with the repercussions to announce that they will refuse to play along. This public rejection by the union organization, on behalf of the armed forces and police, appears to have been suppressed by the Austrian state media because it obviously represented a slap in the face of governmental overreach.
In Austria a larger segment of the population has refused to get their recommended shots than in Germany, where the population is more compliant toward authority. It remains to be seen whether the current crew of party leaders who went along with the announced mandates will retain their functions in the wake of planned public resistance and police rejection of these government plans.
• Indicting Instigators
 Based on numerous media presentations, no group of individuals is more strongly associated with the ongoing totalitarian campaign to push toxic shots onto the world’s population, to bring on a new era, than Anthony Fauci, Bill Gates, and Klaus Schwab, head of the World Economic Forum organization, which has hosted annual assemblies in the Swiss mountain resort of Davos in January, attended by influential business people, economists, top politicians, media, and technical functionaries from non-governmental organizations among others. Schwab provoked much controversy and revulsion for the contents of his book Great Reset, published last year. If the self-contradictory pronouncements in the wake of the fabricated virus pandemic made little sense it was because they were merely part of a larger playbook, according to which the population is to be manipulated to accept a new utopian order referred to as Trans-humanism. A reduced population surviving the envisaged transformation is to merge with new technology and thereby extend themselves. Trans-humanism is the fantasy goal and Technocracy is the ideological basis to get there.
Based on numerous media presentations, no group of individuals is more strongly associated with the ongoing totalitarian campaign to push toxic shots onto the world’s population, to bring on a new era, than Anthony Fauci, Bill Gates, and Klaus Schwab, head of the World Economic Forum organization, which has hosted annual assemblies in the Swiss mountain resort of Davos in January, attended by influential business people, economists, top politicians, media, and technical functionaries from non-governmental organizations among others. Schwab provoked much controversy and revulsion for the contents of his book Great Reset, published last year. If the self-contradictory pronouncements in the wake of the fabricated virus pandemic made little sense it was because they were merely part of a larger playbook, according to which the population is to be manipulated to accept a new utopian order referred to as Trans-humanism. A reduced population surviving the envisaged transformation is to merge with new technology and thereby extend themselves. Trans-humanism is the fantasy goal and Technocracy is the ideological basis to get there.
At the end of Session #79 in the weekly Corona Investigative Committee meeting Patrick M Wood, author of Technocracy Rising, explained the genesis of this movement in the early 1930s, which for a while was centered at Columbia University. It has merged with the Trilateral Commission, the UN Sustainability initiative, and runs on a parallel track with the “Climate Change” cult. As a few privileged elitists will be able to extend their lives, everybody else is regarded as cattle. This ideological movement is indeed inhumane, and everybody is supposed to accept this. In this regard one is reminded of the book Animal Farm by George Orwell, or just the most basic Talmudic principles. Wood provides a cohesive explanation detailing how various observed political phenomena, that do not fall within a binary left / right paradigm, fit together within the overarching scheme of Technocracy. Klaus Schwab takes on the role of cult leader, or guru, and attendees of the World Economic Forum are the devotees.
As has been the case with other cultist leaders, affluent people tend to be attracted to the exclusive movement and donate much of their wealth to spread the message. As a totalitarian ideology Technocracy stipulates that the entire world population must become injected with one of the toxic substances being foisted onto the public. Many of the world’s current leaders, such as Merkel, Macron, Newsom, Blair, and many more, began their political careers in the World Economic Forum’s Young Global Leaders program many years ago and are now collectively well networked. They have long since become activist devotees serving the Technocracy agenda.
It is not hard to surmise that Schwab is regarded as a most odious individual. A couple of years ago his request to receive regular or at least honorary Swiss citizenship was rejected, even though he has purportedly lived there for six decades from the time he studied at the university in Zurich. (By contrast, pop singer Tina Turner got full Swiss citizenship a few years ago without apparent difficulty.) While at Harvard University, he became a protégée of Henry Kissinger. Under his tutelage Schwab began his career by organizing a meeting for executives. Subsequent gatherings eventually became the annual World Economic Forum.
There are plenty of industry groups that have lost out to both the “Climate Change” and “Corona Pandemic” constructs, including oil and gas, airlines, aviation, automobiles, hotels, casinos, cruise ships, restaurants, and entertainment, among others. The executives from these organizations are not likely to be Schwab devotees and would presumably be happy to see his influence neutralized. In Switzerland, where high-end tourism still plays an important economic role, business has gone down significantly due to measures that restrict personal contacts. It is unclear why all these sectors have not seemed to have been able to organize a coordinated response to the pernicious agenda of Schwab and his cohorts.
Just a few weeks ago, in mid-November, rumors were circulating that Schwab had been arrested at his residence in Cologny in the canton of Geneva, due to a criminal complaint, and was charged with fraud for his involvement in the Covid scandal. The initial report was not officially corroborated, and multiple fact-checker sites then claimed it was a case of false news. The denials were very specific, which left open the possibility that perhaps he may have been subject to questioning in an investigation. However, given that crimes against humanity are serious transgressions, so also are acts that aid and abet such major crimes. In view of Schwab’s central position in this criminal enterprise in association with Nuremberg Code violations, it is hard to conceive that there would not be sufficient evidence upon which to indict Schwab as a titular coordinator or crime boss.
Though the annual meeting early this year was cancelled, as was a planned event in Singapore, the World Economic Forum web site shows the date for its next meeting to be between 17-22 January in 2022, only a few weeks away. The theme is to be “Working Together, Restoring Trust”, which at least tacitly acknowledges a loss of trust. The quickest way to end the loss of trust of the thinking and critical people toward their governments would be to arrest and charge Schwab and his collaborators at the upcoming Davos meeting under criminal charges that would lead to prosecutions. This would be an easy operation since there are only two access roads to the town, from the north and south, when the Flüela Pass, which connects to the Engadin Valley, is closed for the winter. Last Sunday Swiss citizens held a referendum on the issue of a tightened Covid policy proposal, including required documentation, which a majority of voters endorsed. Based on the election results, a majority of voters in many rural regions were opposed. People who join the police forces, which would execute a mass arrest order, tend to come from these more conservative regions, especially in the eastern and central parts of the country.

More likely than such a mass arrest would be for an international tribunal to be held, to collect evidence, in a similar manner that the Corona Investigative Committee has been engaging in fact-finding sessions for over a year. As more people understand the direct link between ongoing totalitarian offensives by numerous governments and the influence that Schwab and his associates have over these totalitarian public officials, it will become increasingly difficult for the remaining people of good conscience who are in a position to act, to do a favor for humanity and help end this new war.
To summarize, everybody concerned about the future of humanity can play at least a minor role in spreading the message of resistance to increase public awareness about what is unfolding and what ought to be done in response.
Australia has recorded 11 times more Deaths in 8 months following Covid-19 Vaccination than it has Deaths following every other Vaccine combined in over 50 years
THE EXPOSÉ | NOVEMBER 25, 2021
Serious questions have been raised as to why medicine regulators have not pulled the Covid-19 vaccines from distribution to the general public after data on the Australian Government site revealed that there have been eleven times as many deaths reported as adverse reactions to the Covid-19 vaccines over a period of 8 months than deaths reported as adverse reactions to every other available vaccine combined over a period of 50 years.

The Department of Health Therapeutic Goods Administration (TGA) is the medicine regulator for the Australian Government, and as part of the Department of Health, the TGA regulates the quality, supply, and advertising of medicines, pathology devices, medical devices, blood products and most other therapeutics.
However, a Freedom of Information request made by Doctors for Covid Ethics back in February 2021 revealed that the TGA never saw the extremely limited study data for the Pfizer mRNA Covid-19 vaccine prior to granting it emergency approval and deeming it safe to be injected into the arms of Australians.

The TGA originally attempted to suppress the FOI request by requesting a 6-month extension in view of the amount of work required to respond satisfactorily. But after a complaint was made to the Office of the Information Commissioner the TGA responded confirming that they had never seen or requested the patient data from Pfizer and simply accepted Pfizer’s report of their study as fact, despite their proven history of fraudulent claims.
Pharmaceutical giant Pfizer Inc., have been fined £3,573,465,793.97p since the year 2000 for over 80 offences / violations.
This includes over £26.1million in Kickbacks and Bribery offences, £870million in False Claims offences and £2.5billion in healthcare related offences.

The TGA’s admission that they have never seen the raw trial data for the Pfizer jab prior to granting it approval, and Pfizer’s scandalous history of fraudulent claims and bribes, may go some way to explaining why the TGA have so far refused to pull the Covid-19 injections from distribution to the public, despite 6.5 times more adverse reactions, and 11 times more deaths being reported due to the jabs over a period of 8 months than have been reported to all other available vaccines combined since the 1st January 1971.
The TGA has a ‘Database of Adverse Event Notifications‘ that allows visitors to search adverse events reported for medicines including vaccines. The reports come from a wide range of sources, including members of the public, GPs, other health professionals and the therapeutic goods industry.
By searching the database for ‘Vaccine’ and deselecting the four available Covid-19 vaccines, with a date parameter of ‘1st January 1971 – 11th November 2021‘ the following results can be found –

Source
Over those 50 years and 9 and a half months there have been 76 different vaccines available to the Australian public (excluding Covid-19 vaccines), and there have been 19,205 individual reports to all 76 vaccines combined, including 59 deaths. The TGA state that they think there is a possibility that the available vaccines caused 12,366 of those reported adverse reactions.
By carrying out a new search on the database for ‘Covid-19 Vaccine‘, with a date parameter of ‘1st December 2020 – 11th November 2021’ the following results can be found –

Source
The results shows that there have been 81,318 reports made against the available Covid-19 vaccines, including 656 deaths. The TGA state that they they think there is a possibility that the Covid-19 vaccines caused 79.953 of those reported adverse reactions.
The first Covid-19 vaccine was administered in Australia in February 2021. This means that there have been been 11 times more deaths, 4 times more reports of adverse reactions, and 6.5 times more reports of adverse reactions that the TGA suspects were more than likely due to the Covid-19 vaccines, than have been reported to all other available vaccines combined over a period of 50 years and 9.5 months.
According to the TGA database, the leading cause of death due to the Covid-19 vaccines has been an ‘adverse event following immunisation’. The second leading cause of death has been dyspnoea (difficulty breathing), followed by pulmonary embolism (blocked blood vessel in the lung), then cerebrovascular accident (stroke), and then cardiac arrest.

These numbers raise serious questions as to why the Covid-19 vaccines have not been pulled from distribution to the public when just four separate vaccines for Covid-19 have caused over 11 times as many deaths in just 8 months, than 76 separate vaccines combined have caused over a period of nearly 51 years.
French troops violently disrespect African populations during anti-occupation demonstrations
By Lucas Leiroz | December 1, 2021
Paris has always had Africa as a route for its political and economic expansionism, advancing on the continent and making it part of its international sphere of influence. However, it is possible to see that the African people are increasingly indignant with the constant presence of French military personnel in the region, which has resulted in protests taking to the streets of African cities, clamoring for a change. Now, French forces are seeing such demonstrations as a real threat and treating the population in a violent and disrespectful way, with the sole intention of asserting power and demonstrating the strength of the Paris’ agenda.
In recent days, thousands of people have taken to the streets to protest against the French expansionism in many African countries. This week, at least two people died in western Niger due to the brutality of French troops trying to stop a demonstration. During the action of the military convoy that tried to prevent the people from protesting, several shots were fired, leaving, in addition to the fatalities, eighteen injured people – eleven of them seriously wounded. This same convoy had previously performed similar scenes in Burkina Faso, where French military personnel shot at four protesters last week, generating a wave of indignation and revolt on the part of the local population.
According to what has been reported by Agence France-Presse, the convoy has a force of around 100 soldiers and has departed from Côte d’Ivoire and, after circling through Burkina Faso and Niger, is on its way to Mali, where it will be joining a French military base in the Gao region. Apparently, this convoy is making an international tour of the western part of the African continent, acting as a kind of “police force” in the containment of demonstrations, ignoring local authorities and the right of the citizens of these states to demand changes in the security policies that are being implemented in their countries.
The French forces reported that the shooting in Niger was motivated by the protesters’ own actions. According to the troops, the protesters tried to block the convoy’s passage, which was why the soldiers, trying to open the way, acted with the use of force. Obviously, regardless of the actions taken by the protesters, it is inconceivable for trained military personnel armed with war equipment to act with total force against unarmed civilians. Although it is admitted to partially use military power to disperse protesters, it is absolutely reprehensible that this resulted in lethal gunshots, killing innocent citizens who only exercised their civil right to protest against the presence of foreign troops in their country.
Also, there are images and videos circulating on the internet recording the horror scenes that took place in Niger this week, where it is possible to note that the use of force by the French far exceeded the reasonable line to simply disperse a human barricade of protesters. In one of the videos, it is possible to see a French Mirage 2000 strike aircraft dropping flares and tear gas bombs in a high-speed, low altitude pass over the protesters. There are also reports of shootings from military drones.
Commenting on the case, the Nigerien Interior Ministry said in a statement that “an investigation has been opened to determine the exact circumstances of this tragedy and determine responsibility”. However, it should be noted that this is not the first time that such actions have been carried out with impunity by French forces. Not only are the African people tired of the immeasurable violence perpetrated by French troops, but the very governments that “allow” such actions also wish to put an end to them, however, they lack the power to do so.
Faced with immense military asymmetry, with African countries being much weaker than France and still sharing a problematic heritage from the colonial ties of past centuries, West African governments do not have many options to respond to the suffering of their own people. There are no ways to retaliate or punish the French for their criminal acts – and there are no viable ways to expel the Europeans either.
In Mali, the military tried to end the French presence through a coup d’état last year, but the Paris’ forces continue to act freely against the local population in many situations, such as the massacre of 22 civilians during an attack to a Malian village earlier this year. In fact, there seems to be no alternative path for the African states, which, as long as they do not have a political, economic, and military structure strong enough to coercively expel foreign troops, will continue to suffer the consequences of Paris’ neo-colonial expansionism.
France, on its part, has diminished its interest in the African continent. The failure of the occupation of the Sahel showed that the French project for Africa was unfeasible and that, therefore, Paris should change its focus on international projection – which has gradually turned to the European and Mediterranean space itself. On the other hand, France does not want to simply “abandon” Africa, as this would open the way for another world power to occupy this space.
The French project, therefore, consists of reducing the presence of their troops in the African space, but preventing a real “independence” on the part of African governments, preventing them from seeking new alliances. In practice, this materializes in actions such as the ones of this convoy, which spread chaos and instability in the region. The French objective in Côte d’Ivoire, Burkina Faso and Niger is to prevent, through intimidation, a maneuver such as the one that happened in Mali – and, in Mali, the aim is to prevent the military’s plan to succeed.
Indeed, France “does not want” Africa at the moment, but it is not willing to allow Africans to follow their own path of independence. Fostering social chaos, disorder and violence seems to be the French tactic in this regard.
Lucas Leiroz is a research fellow in international law at the Federal University of Rio de Janeiro.
France sends military police to Martinique amid vaccine mandate protests
RT | December 1, 2021
France has sent police reinforcements to overseas territory Martinique, after riots broke out in response to a mandatory Covid-19 vaccine policy for healthcare workers.
Around 70 armed French police officers, known in France as gendarmes, arrived in Martinique on Tuesday to tackle the violent protests, which were marred by arson, looting, and vandalism.
French Minister of Overseas Territories Sebastien Lecornu said in a press conference that “social dialogue is not possible without a sound basis and that sound basis is the re-establishment of freedoms… and our capacity to re-establish order.”
Civil unrest broke out after France imposed a vaccine mandate for healthcare workers in Martinique, which has reported low vaccination rates amid high levels of mistrust in the government and faith in natural medicine
As a result of the riots – which included an attack on the residence of France’s most senior official on the island – France revealed on Friday that it would be postponing its vaccine mandate.
Lecornu has blamed Martinique’s vaccine hesitancy on the island’s culture, saying, “I don’t want to stigmatise but the mistrust over vaccines is cultural.”
Protesters, however, say they are unable to trust officials with their health after previous cases of misconduct – 95% of adults in Martinique have traces of a pesticide with links to cancer in their blood after it was consistently sprayed on the island for several decades.
Martinique was colonized by France in 1635 and has remained under French control despite independence efforts.
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- Press TV reporter wounded in Israeli drone strike on southern Lebanon
- Time for Trump to Tell Benjamin Netanyahu to Go Away!
- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- If Americans Knew
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
