FDA Authorizes Pfizer Booster for Kids 5 to 11, Bypasses Advisory Panel
By Megan Redshaw | The Defender | May 17, 2022
The U.S. Food and Drug Administration (FDA) today authorized a booster dose of the Pfizer-BioNTech COVID-19 vaccine for children ages 5 to 11, without convening its vaccine advisory panel of independent experts to discuss Pfizer’s data on 5- to 11-year-olds — and based on a study subset of only 67 children, CNBC reported.
The FDA granted Emergency Use Authorization (EUA) for the boosters despite data showing higher infection rates among fully vaccinated children in the 5 to 11 age group compared to unvaccinated children, no studies testing the efficacy of the vaccine against the current dominant BA.2 COVID-19 variant and two new studies showing that for vaccinated people who get Omicron, the infection provides better protection against future infections than a second booster dose.
The vaccine advisory panel for the Centers for Disease Control and Prevention (CDC) is scheduled to meet Thursday. The agency and its director, Dr. Rochelle Walensky, are expected to sign off on the boosters, The Washington Post reported.
Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, said data increasingly show protection provided by two shots wanes over time, but the agency determined a third shot could help boost protection for children in the 5 to 11 age group and the “benefits outweigh the risks.”
The FDA authorized the third shot after analyzing data from an ongoing Pfizer clinical trial in which a small subset of only 67 children in the age group had higher antibody levels one month after receiving a booster dose.
As The Defender reported, antibody levels alone are not indicative of immune protection. When it comes to COVID-19, T cell and natural killer cell responses are the crucial part of immune protection.
Pfizer has not published its actual data, precluding experts from conducting this analysis.
The authorized booster dose, the same strength as the first two doses, generated neutralizing antibodies to Omicron and the ancestral Wuhan version of the virus, according to The New York Times.
The FDA said it did not identify any new safety concerns and found the children in the trial experienced the same mild side effects other people do after receiving a booster.
However, a subset of only 67 children is not large enough to detect potential adverse events like myocarditis, and it is unknown how rapidly any protection provided wanes because trial participants were not followed beyond a 28-day period.
About 8.1 million, or 28%, of children ages 5 to 11, received their primary series of two COVID-19 vaccine doses as of May 11, according to data from the American Academy of Pediatrics.
Those children will now be eligible for a third dose five months after their second dose based on data obtained from the 67 children who were followed for only one month.
COVID cases higher in vaccinated children aged 5 to 11, CDC data show
According to the latest CDC data, since February, higher COVID-19 case rates were recorded among fully vaccinated children compared to unvaccinated children in the 5 to 11 age group.
The CDC on Feb. 12 reported a weekly case rate of 250.02 per 10,000 population in fully vaccinated children ages 5 to 11, compared to 245.82 for unvaccinated children in the same age group.
The trend continued through the third week of March, which is the latest week of available data.
“Several factors likely affect crude case rates by vaccination and booster dose status, making interpretation of recent trends difficult,” CDC spokesperson Jasmine Reed told The Epoch Times in an email.
“Limitations include higher prevalence of previous infection among the unvaccinated and unboosted groups, difficulty in accounting for time since vaccination and waning protection, and possible differences in testing practices (such as at-home tests) and prevention behaviors by age and vaccination status,” Reed said. “These limitations appear to have less impact on the death rates presented here.”
According to CDC data, the gap between fully vaccinated and unvaccinated individuals in all age groups has grown increasingly smaller, with the death rate showing the same trend for people over age 50.
For people under age 50, death rates are almost identical between the vaccinated and unvaccinated since the beginning of the vaccine rollout.
Data show COVID-19 vaccines have a “negligible effect” on people, said Dr. Peter McCullough, a prominent cardiologist and epidemiologist.
“With these results in hand, it is clear the vaccines are having a negligible effect in populations,” McCullough told The Epoch Times in an email.
“Given the overall poor safety profile and lack of any assurances on long-term safety, Americans should be cautious in considering additional injections of these products.”
Having COVID may be more effective than getting a booster, studies show
Two new studies show, for people who are vaccinated against COVID-19, getting a breakthrough Omicron infection may provide better protection than receiving a second booster, Fortune reported.
One study conducted by German biotechnology company BioNTech SE assessed vaccinated individuals who had breakthrough COVID-19 infection associated with the Omicron variant.
BioNTech found these individuals had a better B-cell response than individuals who had received a booster but had not been infected.
According to MD Anderson Center, B cells are a type of white blood cell that create antibodies that bind to pathogens or foreign substances and neutralize them. B cells bind to a virus and prevent it from entering a normal cell causing infection. They also recruit other cells to help destroy infected cells.
A second study by the University of Washington and Vir Biotechnology investigated the immune responses of various groups based on vaccination and infection status.
The study analyzed blood samples of individuals who had been vaccinated and then caught the Delta or Omicron variants and compared them with those who had COVID-19 first and were then vaccinated, those who had been vaccinated but were not previously infected and those who were infected but had never received a COVID-19 vaccine.
The study found vaccinated individuals with breakthrough Omicron infection produced antibodies that formed a strong defense against other variants of the virus. Unvaccinated people who caught Omicron did not have a similarly robust immune response.
Efficacy of Pfizer’s COVID vaccine wanes rapidly
A study published May 13 in the Journal of the American Medical Association (JAMA) found protection from Pfizer’s COVID-19 vaccine turned negatively effective among children and adolescents five months after receiving a second dose — meaning recipients were more likely to get COVID-19 five months after being vaccinated.
Vaccine effectiveness “was no longer significantly different from 0 during month 3 after the second dose,” the researchers wrote. They also found protection against hospitalization waned significantly over time.
In adolescents, the authors said, efficacy increased again with boosters.
Most non-randomized studies attempting to determine vaccine efficacy (VE) had “common flaws,” including no accounting for baseline prior COVID-19 infection, no reporting for those who received a booster within a six-month time window and no adjudication of hospitalization or death due to COVID-19 or other conditions, McCullough told The Epoch Times.
“As a result, most studies of COVID-19 VE have biases towards overestimating any clinical benefit of vaccination,” McCullough said.
As The Defender reported on May 13, a different study published in JAMA showed second and third doses of Pfizer’s COVID-19 vaccine provided protection against the Omicron variant for only a few weeks.
“Our study found a rapid decline in Omicron-specific serum neutralizing antibody titers only a few weeks after the second and third doses of [the Pfizer-BioNTech] BNT162b2,” the authors wrote.
A preprint study released in February showed Pfizer’s two-dose regimen of its COVID-19 vaccine for children was only 12% effective against Omicron in children ages 9 to 11, and the effectiveness of the vaccine “declined rapidly” for children 5 to 11.
Researchers at the New York State Department of Health and the University at Albany School of Public Health examined the effectiveness of the vaccine in children 5 to 11 and adolescents 12 to 17 from Dec. 13, 2021, to Jan. 30, 2022, and determined the effectiveness of Pfizer’s COVID-19 vaccine declined rapidly for children, particularly those 5-11 years.
According to a Danish study of 128 people who had received two or three doses of Pfizer’s COVID-19 vaccine, levels of Omicron-specific “neutralizing” antibodies decline rapidly after a second and third dose of Pfizer’s shot.
Compared to original and Delta variants, researchers found the proportion of Omicron-specific antibodies detected in participants’ blood dropped “rapidly” from 76% four weeks after the second dose to 53% at weeks 8 to 10 and 19% at weeks 12 to 14.
After the third shot, neutralizing antibodies against Omicron fell 5.4-fold between week 3 and week 8.
Last month, Moderna requested EUA for its COVID-19 vaccine for children aged 6 months to 6 years. Pfizer plans to seek EUA for a three-dose regimen for the same age group.
The FDA’s top vaccine official told a congressional committee on May 6 COVID-19 vaccines for children under 6 will not have to meet the agency’s 50% efficacy threshold required to obtain EUA.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Taking the milk out of babies’ mouths: Food shortages are the new globalist weapon
By Kate Dunlop | TCW Defending Freedom | May 18, 2022
ARE you getting used to the Great Reset? How are you liking the New World Order built on globalist diktat, infection, mass poisoning by inoculation, inaccessible healthcare, inflation, draconian policing, shortages, uncontrolled migration, fear, more fear, and war…
You’ll doubtless be prepared for what’s coming next. It’s not a secret – Bill Gates and his World Health Organisation cohorts have already told us. The next viral releases – Hantavirus, Nipah virus, Marburg, whatever – are all primed and ready to go, together with monkeypox and avian bird flu. All come packaged with their own ‘off the shelf treatments’ from Big Pharma, all guaranteed to be equally as effective as the Covid jabs.
Supply chain problems are already here and will worsen, depending on whatever the next emergency is, and the UK is as well prepared for them as it is for shortages of fuel, gas, and electricity – which is to say not at all.
Now we are being told that a major food crisis is inevitable. Speaking at a Nato conference in Brussels on March 25th of this year, Joe Biden said: ‘Regarding food shortages – yes, we did talk about shortages, and they’re going to be real.’ He’s a man of his word.
Previously the blame was put on ‘climate change’, Brexit, shortages of foreign hands to pick and harvest crops, not enough lorry drivers, lockdowns, the ‘management’ of Covid, and the mass culling of chickens due to bird flu.
Now the war in Ukraine and sanctions against Russia are delivering shortages of gas, oil, and wheat. Russia and Ukraine together are the largest exporters of wheat and other grains in the world and Russia the largest exporter of oil and gas. Their impact on global logistics and food supply is immense.
At the same time, food production and processing facilities in the US seem to be spontaneously combusting. Since August last year, more than 16 such plants have been damaged by fire.
In September, a meat processor in Nebraska lost five per cent of the country’s beef supply. In March this year, a frozen food plant in Arkansas and a potato processing site in Maine both burned down. Last month, two planes crashed into two food plants, causing massive destruction – one at a General Mills facility in Georgia and another at a potato processing unit in Idaho.
Florida is having its worst orange crop in 70 years, with 90 per cent of trees affected by ‘citrus greening,’ a disease spread by the invasive Asian citrus psyllid bug, which was first found in China, then India and Saudi Arabia. Today, every citrus grove is infected. The impact on farmers already suffering from Covid restrictions is disastrous.
Russia and Belarus are two of the biggest global exporters of fertiliser and fertiliser-related products, accounting for 10 billion dollars activity per annum. The war and the sanctions have damaged the fertiliser market, with prices hitting all-time highs in March.
China’s draconian ‘Zero Covid’ approach and its export ban on fertiliser since last summer has added to farmers’ woes and hit food production costs.
Now it’s baby formula milk, with shortages across the US since February this year. CBS News reports that some 40 per cent of top-selling formula products were ‘out of stock’ at the end of April, according to an analysis from Datasembly.
The Wall Street Journal suggests two reasons for the shortages. It says supply chain issues caused by the Covid-19 pandemic worsened after Abbott Labs, a major formula manufacturer, voluntarily recalled some products and closed a plant in Michigan. Then there was a Food and Drug Administration investigation into complaints related to four infants who were hospitalised, two of whom died.
The White House reaction last week was woeful, with the tone-deaf press secretary Jen Psaki saying the government is ‘doing its best’ and that manufacturers are working at full capacity. In a national health emergency she went on to hint that some mothers are hoarding formula.
But, as with everything in the Magic Kingdom of Biden, things are not what they seem. The legacy media are slow to show locked cabinets in Walmart and empty shelves in other stores, though news that the government is transporting supplies of baby formula to border migrants is beginning to leak, as Tucker Carlson reports.
Eric Boehm, writing in Reason, confirms that although some of the shortages stem from the closure of the Abbott plant, there were already longstanding market problems. A closer look at US trade and regulatory policies shows that government is primarily responsible for the shortages.
According to the New York Times, ‘baby formula is one of the most tightly regulated food products in the US, with the Food and Drug Administration dictating the nutrients and vitamins, and setting strict rules about how formula is produced, packaged, and labelled’.
The US formula market was valued at 3,653 million dollars in 2019 and projected to reach 5,811 million dollars by 2027. The Covid-19 pandemic brought an upsurge in demand due to panic buying on the back of shortage fears.
Rising numbers of American parents are sourcing ‘unapproved’ European formula, even though it attracts an 18 per cent tariff quota. Some are desperate for supply, but others choose European brands because they offer options such as goat’s milk or milk from pasture-raised cows, which are ‘rare or non-existent in an FDA-regulated form in the US’.
Others consider EU products to be of higher quality due to stricter content regulations, including important levels of DHA (an omega-3 fatty acid), which are not required in the US. Almost no American baby formula would meet EU standards and many parents worry about adulteration.
Americans pay well over the odds for European formula, with one website selling product from Germany at 26 dollars for a 400-gram box, about four times the price of the top US formulas.
In April 2021, US Customs and Border Protection agents in Philadelphia seized 588 cases of formula worth around 30,000 dollars. The formula was said to have violated the FDA’s ‘import safety regulations.’ According to Twitter chatter, the FDA issued a fake recall of European formulas in 2021 and has regularly seized legal personal-use shipments.
Plain old natural disaster coupled with bureaucratic interference is not what is going on here. The US baby formula shortage is neither due to incompetence nor maladministration – it is an attack on the most vulnerable in society; part of a deliberate policy to keep chaos bubbling at peak in the service of the Great Reset.
We know what is going on. In 1974, Henry Kissinger said: ‘Who controls the food supply controls the people; who controls the energy can control whole continents; who controls money can control the world.’
Bill Gates wants to build a dystopia

By Toby Green | UnHerd | May 9, 2022
It’s not easy being a regular multi-billionaire. Bill Gates used to be the simple guy-in-the-mansion next door, worried about virus outbreaks and global warming. Then, during the pandemic he became the point at which all conspiracy theories met.
Ever since March 2020, the memes have spread. Was Gates a mass murderer with a global depopulation agenda? Was he a “biofascist” seeking control over the world’s population through vaccine passports and microchips?
It didn’t stop there. Was the Covid-19 pandemic actually “plandemic”? Did the Microsoft founder and his acolytes create it through funding “gain of function” research in a biosecurity lab in Wuhan? Was it all war-gamed at Event 201 in October 2019?
Bill Gates has not much enjoyed being the focus of these stories for the past 18 months. He just wants to help out. He wants to solve problems so badly, he tells us early on in How To Prevent the Next Pandemic, that in February 2020, he flew from Seattle to South Africa to participate in a charity tennis match, no doubt on one of his four personal jets.
It was in South Africa that he first began to join the Covid-19 dots. The tech entrepreneur delivers the story with characteristic flair: “A couple of days after returning from South Africa, I sent an email about scheduling something for the coming Friday night: ‘We could try and do a dinner with the people involved with coronavirus work to touch base.’” Gates is happy, “everyone was nice enough to say yes — despite the timing and their busy schedules”. His work on the pandemic begins.
Now Gates is tired of all the conspiracies. He asks his critics to judge him by his actions. And the best way to do so is by reading the book: does Gates have anything sensible to say about the best way to combat future pathogenic outbreaks?
His model for the future is built on what he feels has worked over the past two years: isolate contacts, close borders, lockdown as quickly as possible, then remove restrictions slowly and cautiously. He cites Dr Anthony Fauci, who Gates says he spoke to once a month during the pandemic: “Not only should you appear to overreact at first, as Tony Fauci said, but you also have to be careful about relaxing all NPIs [non-pharmaceutical interventions] too soon.” Meanwhile, you should invest enormous sums in boosting global public health systems, vaccine production in poor and rich countries, and fund a Global Pandemic Emergency Response Unit to monitor potential outbreaks. The aim, says Gates, is to vaccinate the entire world — twice if necessary — within six months while lockdown measures restrict the spread of the new pathogen.
It all sounds so reasonable, doesn’t it? Or it might do to those who haven’t seen the footage of Shanghai’s lockdown circulating on social media, to those who can work online in relative comfort, or indeed to billionaires with comfortable gardens and libraries in which to while away those six months. With the Gates model, a little translation is in order.
The massive investment required to make this vision happen is a good starting point. Where will it come from? Gates is a well-known philanthropist, and makes much of the more than US$2 billion which the Bill and Melinda Gates Foundation have ploughed into fighting Covid-19. Yet this is a small amount compared to the US$6 billion that the US government has invested in the Moderna vaccine alone. As Gates points out, “Most of the world’s greatest talent for translating research into commercial products is in the private sector… It’s the government’s role to invest in the basic research that leads to major innovations, adopt policies that let new ideas flourish.”
Translation: taxpayers invest in developing products through government agencies, and private companies and their shareholders reap the profits. How does this work in practice? Gates does not give what we might call full disclosure. He offers the example of the antiviral Molnupiravir which “Merck and its partners developed”. It was authorised to great fanfare as a Covid treatment in November 2021.
Yet Merck did not develop this drug. It was initially developed as a veterinary drug for horses at Emory University, with a US$19 million grant from Fauci’s NIAID and funding from other sectors of the US government. Molnupiravir costs US$17.74 per dose to manufacture, according to an estimate from researchers at Harvard and King’s College London, but is being retailed to the US government for US$712 per course — a profit of 4,000%.
Another example of Gates’s eye for detail is his discussion of Remdesivir, which was approved as “Standard of Care” for Covid in the US by the Federal Drug Agency. Again, like Molnupiravir, much of the funding and institutional support for the drug originally came from the US government. Remdesivir was the baby of the drug company Gilead.
Gates describes how one study showed that “it may have a major impact in patients who aren’t yet sick enough to be in the hospital”. But other details are ignored. He doesn’t tell us that in an earlier, peer-reviewed study from China, published in the Lancet in May 2020, “Remdesivir was not associated with statistically significant clinical benefits”, and that the trial was “stopped early because of adverse events in 18 (12%) patients versus four (5%) patients who stopped placebo early”. All the same, the profits were good: while the drug cost Gilead just US$10 per dose to manufacture, it was being retailed to US taxpayers at US$3,120.
Maybe Gates knows nothing about the Lancet study. Perhaps he doesn’t know that in both of these cases, public investment has funded enormous private profits — and that in the case of one of the drugs, there’s little evidence that this was to any benefit. He’s just a software engineer after all.
For Gates, technology really does provide all the answers, as it certainly has in his own life. He believes humanity belongs online: “once people learn the digital approach, they generally stick to it”. Post-Covid, he envisages a world of flexible working, in which regular guys like him with large mansions and decent living space can languidly choose between going into the office on Wednesdays or Thursdays. The problem with Gates’s digital utopia — full of virtual spaces where 3D avatars attend business meetings — is that I suspect many of us will not want to live in it.
Gates tries to show in this book that he gets it, while at the same time demonstrating on every page that he just doesn’t. As he draws up his elaborate plans for global governance, Gates writes that he does so knowing that he hasn’t been elected. He tells us he wouldn’t want to be anyway (after all, we can surmise, if he were elected, he might be accountable).
Gracefully, Gates understands that people are angry at the huge increases in wealth disparities during the pandemic, and pledges to return his profits to “make the world a fairer place”. He recognises that poor people across the world have suffered, and are far less able to deal with lockdowns, and even acknowledges that harsh measures might not be a good idea for some of them… And yet he recently went on record as saying that “if every country does what Australia did, then you wouldn’t be calling it a pandemic”. We can, in fact, judge him by his actions, and his words: he says one thing, and funds and promotes others.
Looking forward, the outlook is bleak. Preventing pandemics in Gates-World means shutting down immediately at the “next major outbreak” — a favourite, and alarming turn of phrase. Future semi-permanent global lockdowns are baked-in as the new normal, something I warned of in the conclusion to my book The Covid Consensus. As Gates notes, the WHO have identified 1,500 new pathogens in the past 50 years, and thus the “next major outbreak” surely cannot be far off. In the past 20 years, pre-Covid, there were already three of note (SARS — 2003; Avian Flu — 2005; Swine Flu — 2009). In each case enormous fatalities were falsely predicted, and would surely have led to six month shutdowns in the Gates model.
Gates-World is one where citizens make sacrifices for his model to work. And it’s also one where class is totally ignored. Does Gates know what it was like for Angolan children to be forced to stay at home for seven months in 2020? He admits that internet connections need to be improved to make digital schooling possible — but does he understand that no IT in the world can help children of sex workers in Mumbai slums with their homework? Can he comprehend what it is like to be incarcerated in a flat with small children for months on end in New York, Shanghai or London?
Gates wants to be respected, and understood. His world is one of innovative scientists having dinner with one another. They solve the world’s problems by the pool, or near the barbecue. It’s what he likes doing best, because “I’ve had some of the best conversations of my working life with a fork in my hand and a napkin in my lap” (p4). He wants to fund more and more work leading to experiences like this, and meanwhile turn the rest of human society into a digital avatar of itself.
No doubt he means well. But you don’t need to indulge the conspiracy theories to realise that the road to hell is paved with good intentions.
Toby Green is a Professor of History at King’s College, London.
American Airlines Captain Robert Snow speaks out about his vaccine injury
Steve Kirsch | May 14, 2022
Ever wonder why so many flights are delayed or canceled? A lot of it is due to injuries caused by the vaccine mandates.
Today, there are many pilots who are vaccine injured and not saying anything, endangering the public.
Here’s what happened to one vaccine injured pilot who now has to retire because he’s unable to fly anymore.
He speaks freely, right after being released from the hospital.
And no, the CEO of American Airlines, working just 10 minutes away didn’t call or come visit him. That’s the way they treat “family” at American Airlines.
Other articles about the vaccine and pilots
I wonder if the vaccine is causing all these incidents. I’m told they are safe and effective. But that’s not what the data says.
THREE KILLED, AS PLANE CRASHES INTO MEXICAN SUPERMARKET
PLANE CRASHES ONTO A STREET IN SAN DIEGO
PILOT SUFFERS MID-AIR HEART ATTACK
CO-PILOT LANDS PLANE AFTER PILOT HAS HEART ATTACK:
TRAFFIC CONTROL HELPS PASSENGER LAND PLANE, AFTER PILOT HAS HEART ATTACK
Conspiracies about conspiracy theories
A little trip down memory lane
el gato malo – bad cattitude – may 16, 2022
My goodness, these “conspiracy theorists” certainly do have vivid imaginations, don’t they?

i mean, that would be terribly divisive, counter to rights, and directly antagonistic to people who just want bodily autonomy. can you even imagine public officials doing something like that?
pretty far fetched…
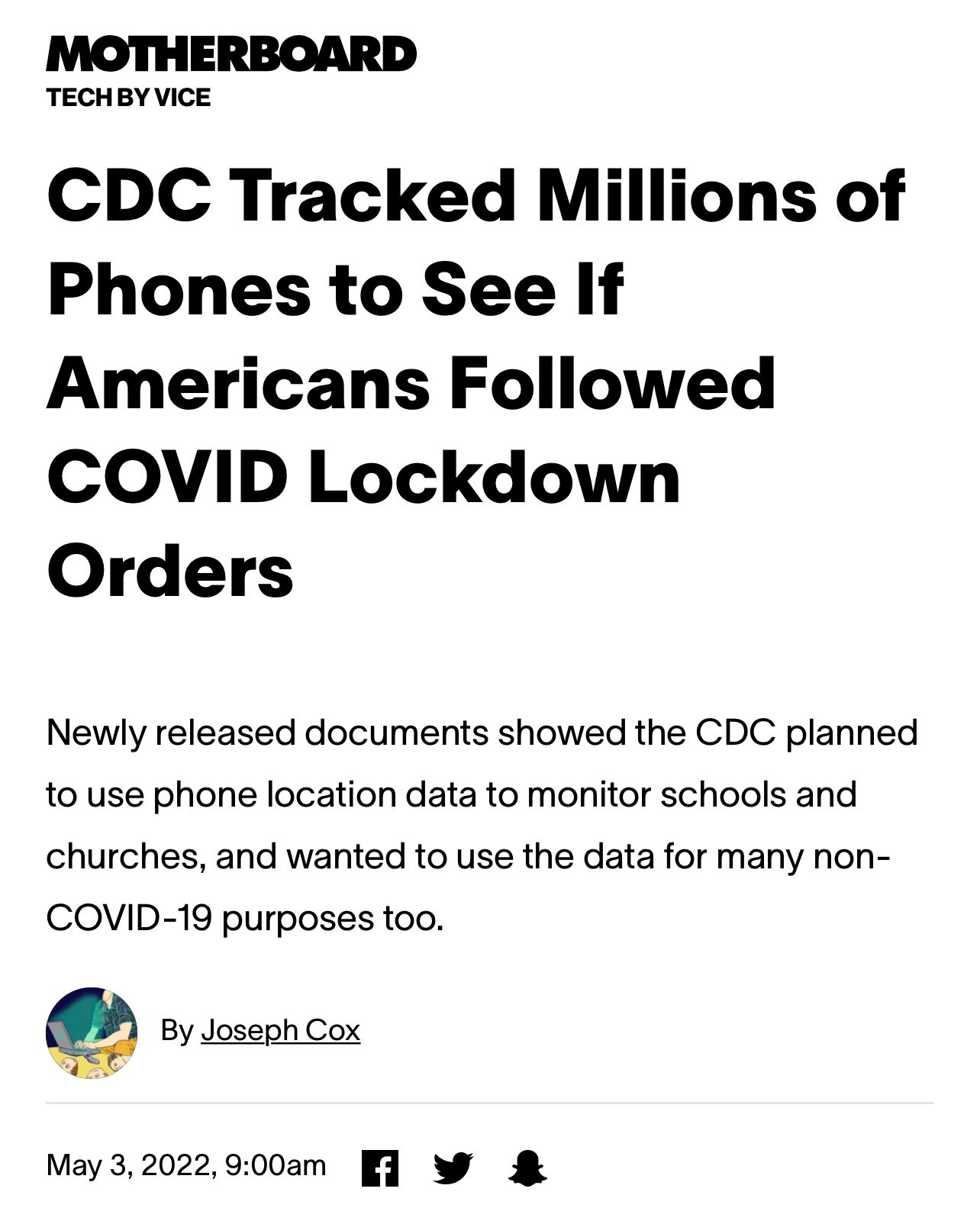
or health bodies using disease to engage in surveillance?
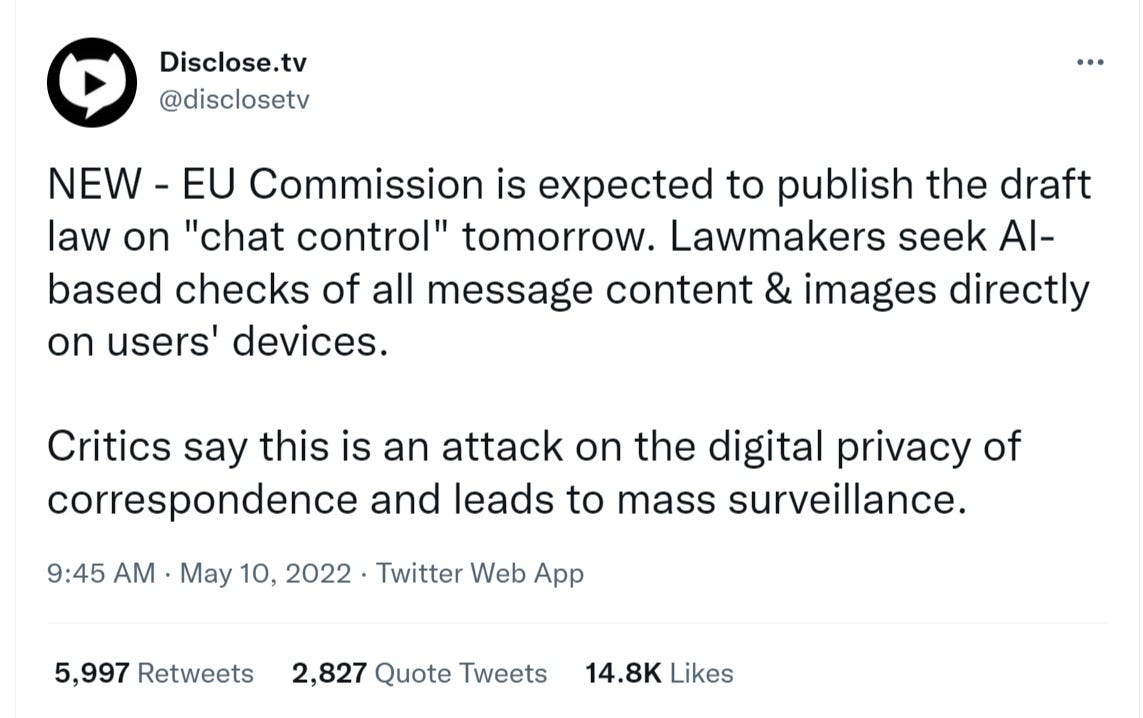
or governments seeking to do the same and mitigate privacy altogether?
i mean, that’s just silly!
what next, some wild eyed claims that they want universal digital ID?
that they have been quietly rolling out the standards for
![]()
and making international and inescapable?
i mean, what will these prolific conspiracy boffins think up next, some sort of state run digital currencies to link to this new ID and surveillance state?
i mean, who would even suggest something like that?

federalreserve.gov/cbdc-faqs.htm
and anyhow, what’s the worst that could happen?

i mean, they told us this is all benign, right?
and it’s not like they ever lied to us before! (or if they did, i’m sure it was for our own good…)

and it’s not like they are seeking to give this power to deeply compromised and captured transnational agencies with no accountability whatsoever and grant them authority over citizens who had no say in the matter…

“The Biggest Global Power Grab We Have Seen in Our Lifetimes”: How Serious is the Threat From the WHO Pandemic Treaty?
so let’s all take a breath. i’m sure you’re just overwrought and imagining things.
there are no conspiracies.
no one is out to get you, least of all some shadowy davos cabal.
and come on, if they were really trying to do this to you, i’m sure they would not just come right out and tell you in some sort of james bond villain megalomaniacal monologue.
i mean, this is real life. no one actually does that…
and hey, i’m sure they’ll probably manage to keep those first 2 promises.
watch out for that third one though.
i have some real doubts about it it…
Data From Iceland and Australia Confirm: Vaccine Effectiveness Is Overstated
By Noah Carl | The Daily Sceptic | May 16, 2022
Back in March, I wrote a post noting that excess mortality data from Europe and Israel were hard to reconcile with claims of 95% vaccine effectiveness against death. However, I also noted that some countries data were consistent with very high vaccine effectiveness against death.
The two examples I gave were Australia and Iceland – both countries with very high vaccination rates. By the end of 2021, each country had double-vaccinated 77% of its population, compared to only 70% in the U.K. and only 63% in the U.S. (see below).

At the time I wrote the post, Iceland had only seen a minor uptick in excess mortality, while Australia had not seen any at all – despite both countries experiencing major outbreaks in the winter/spring of 2022. If countries like Germany, the Netherlands and Israel had seen deadly post-vaccination waves, why hadn’t Iceland and Australia? That was the puzzle.
It appears that ‘puzzle’ is now solved – we just needed to wait for more data. The latest figures from Iceland and Australia show sizeable upticks in excess mortality. First, let’s look at Iceland:

After bouncing around the zero mark for the first two years of the pandemic, excess mortality jumped to 74% in the first week of March. And it has now been above zero for eleven of the last thirteen weeks. Next, let’s consider Australia:

Over the first two years of the pandemic, excess morality averaged roughly zero – dipping lower in the summer and rising higher in the winter. Yet since the start of October, it has been consistently positive, jumping to 26% in the third week of January.
It should be noted: these upticks in excess mortality are not as large as those seen in European countries during 2020 and 2021.
However, they indicate that even very high vaccination rates are not sufficient to prevent mortality from rising when there’s a major outbreak. And they cast further doubt on claims that the vaccines are 95% effective against death. If they were 95% effective against death, excess mortality should hardly have risen at all in Iceland and Australia.
Given that 77% of the entire population was double vaccinated before the latest outbreaks began (and that’s the entire population, not just over 16s), you’d have to believe that excess mortality would have been many, manty times higher in the absence of vaccination to rescue the claim of 95% effectiveness against death.
What’s probably true instead is that the vaccines do reduce mortality from Covid – but not by 95%.
Investigation Launched After ‘Mystery’ Surge in Deaths of Newborn Babies
By Paul Joseph Watson | Summit News | May 16, 2022
Health authorities in Scotland have launched an investigation after a mystery surge in deaths of newborn babies, the second time the phenomenon has been recorded in the space of six months.
A report by the Herald newspaper highlights the “very unusual” spike in deaths of babies, with the alarm being raised after 18 infants died within four weeks of birth in March.
That same control limit was also breached in September last year, when 21 neonatal deaths were reported, the first time this had occurred since records began.
“The neonatal mortality rate was 5.1 per 1,000 live births in September and 4.6 per 1,000 in March, against an average of 1.49 per 1000 in 2019,” reports the newspaper.
Public Health Scotland (PHS) said the deaths could not have been down to chance, while the cause behind the previous spike in September also “remained a mystery.”
The report notes that vaccination uptake has increased in expectant mothers and that COVID infections during pregnancy are associated with a higher chance of premature birth, but found no “direct link” between COVID surges and the deaths.
PHS Scotland says COVID infections “did not appear to have played a role” in the September spate of deaths.
Edinburgh University’s Dr. Sarah Stock said, “The numbers are really troubling,” but admitted she didn’t know the cause of the deaths.
No sympathy for widows from the vaccine zealots

By Laura Perrins | TCW Defending Freedom | May 16, 2022
DEAR reader, I’m going to tell you something and you are not going to like it. People don’t care about you. Deep down, deep, deep down, people who don’t know you don’t really care about you. Not really. Not in any way that matters.
As many readers will know, all last week Mark Steyn interviewed victims of the Covid vaccine. They include widows whose husbands were killed by the vaccine, and survivors who were left with life-changing injuries from the vaccine. If you haven’t watched them, please do try to catch up on YouTube, or at Mark’s website.
As I sat through these testimonies, what struck me was the quiet dignity of the widows and survivors. They were all articulate and dignified. Some were careful to say they were not anti-vax; they just wanted to be listened to, their loss acknowledged and adequately compensated for by a government that forced them to take this vaccine. (And once we look at the propaganda and emotional blackmail it was coercion.)
Some other disgusting journalist took issue with Mark interviewing these victims, saying he was ‘exploiting’ them. Nothing could be further from the truth. The only reason Mark Steyn ended up with these interviews is because every other media outlet ignored them. The government ignored them, the vaccine manufacturers ignored them and the media, who usually would be all over stories like this, ignored them.
There was no rage or anger but plenty of bemusement, bewilderment and hurt as to why and how these victims could be treated like this. The most repeated phrase was that the victims were not scared about getting Covid themselves, but they did not want to spread it to others, they were told to get the vaccine, and they wanted to do the ‘right thing’.
At this point, I felt genuine pity for them. They trusted the government, they trusted the mainstream media and they were injured for it. I especially felt for Charlotte Wright whose husband, Dr Stephen Wright, had died leaving sons aged seven and one.
Those boys, Izaac and Elijah, will grow up without their father because he took a vaccine he did not need. Those boys were told, Daddy is not coming home, ever. To lose a father is bad enough. To lose a father because your government coerced him to have a vaccine is an outrage. Not even to compensate the family is evil.
We now know the vaccines do not stop transmission. As such, why healthy people who had no underlying conditions were told to take them should be subject to a public inquiry. In fact, the population were not just told to take them – they were shamed, bullied and threatened with dismissal from their jobs and civil society itself if they didn’t take them. Leading commentators – Andrew Neil, Piers Morgan, Claire Cohen – advocated for a system of apartheid and punishment for ‘vaccine refuseniks.’ These vaccine victims didn’t stand a chance.
At one point I did seriously consider getting the vaccine. I had just the baby and the government propaganda was seeping even into our No BBC house. I also worried about my husband. I worried that one of us would catch Covid and die leaving the four kids. It didn’t make any sense, but everyone breaks sometimes. Everyone. Luckily, a friend called me and told me to pull myself together and that I stood a much greater chance of being injured by the vaccine than Covid. So that moment passed.
Which brings me back to people not caring. When I considered getting this vaccine, what also stopped me is that for all the talk of ‘do the right thing’, I knew that if my husband died from it, no one other than close family and friends would care. Ultimately Matt Hancock was not going to call at my door and say, Don’t worry you are not going to starve to death even though your husband has died.
If I got injured and couldn’t drive, which would devastate the workings of the family, Claire Cohen wasn’t going to rock up and say, Don’t worry, I’ll do the school run. Childless Andrew ‘Punish refuseniks’ Neil certainly wasn’t going to take the baby if I could barely carry him. Neil had his house in the South of France to retreat to – so shut up and take your vaccine.
Ultimately, these people don’t care. They don’t care because they have never once recognised the injuries caused by the vaccine they so passionately advocated for. They don’t care because from my viewpoint they have never once written about it, or had the victims on their shows.
The same goes for the ordinary public. The bottom line is we all have a limited supply of sympathy and empathy to go around, and if we felt every loss we couldn’t get out of bed. But to advocate in such strong terms for a vaccine that has killed and injured people – that was morally abhorrent.
Featured Video

IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
or go to
Aletho News Archives – Video-Images
From the Archives
Because no animal reservoir has been found for SARS-CoV-2, it cannot properly be termed a zoonosis.* Should we call it a labnosis? And what does that mean?
By Meryl Nass, MD | July 12, 2021
After a year and a half of seeking but not finding SARS-2 in any wildlife anywhere (apart from domesticated or zoo animals that appear to have caught it from humans) is it time to say, yes, it didn’t just escape from a lab. It was created, built, assembled in a lab. Or many labs
Coronavirus scientists have been constructing new viruses out of bits and pieces of other viruses for a long time.
Why did they do it? … continue
Blog Roll
 Aletho News
Aletho News- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- Strait of Hormuz closed over Israeli aggression on Lebanon
- Keir Starmer arson mysteries multiply
- IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
- Zelensky threatens to attack Belarus
- UK to send Ukraine 150,000 drones
- ‘Biased censorship’: Iran deputy FM slams X for stripping him of blue tick
- Hezbollah lawmaker says Israel has 60 days to withdraw from Lebanon
- Iran rules out IAEA inspections of war-damaged nuclear sites
- If Americans Knew
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- Old Iraq war architects rise up against Trump’s Iran deal
- Unmasking Axios, its Israeli ties and agenda
- No Tricks Zone
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
