Can ‘Big Brother’ Save You From a Virus?
By Dr. Joseph Mercola | August 17, 2021
In June 2021, the U.S. National Security Council released a new “National Strategy for Countering Domestic Terrorism” document.1 While it’s being largely framed as a tool to fight White supremacy and political extremism, the definition of what constitutes a “domestic terrorist” is incredibly vague and based on ideologies rather than specific behaviors.
It’s not difficult to imagine this policy being used to silence political opposition simply by labeling anyone who disagrees with the government as a domestic terrorist and charging them with a hate crime.
We’re already seeing signs suggesting that this is the path we’re on. July 28, 2021, Dr. Peter Hotez published a paper2 in PLOS Biology titled “Mounting Antiscience Aggression in the United States,” in which he suggests criticizing Dr. Anthony Fauci and other scientists ought to be labeled a “hate crime.” Commenting on the paper, Paul Joseph Watson at Summit News writes:3
“This is yet another transparent effort to dehumanize anti-lockdown protesters and demonize people who merely want to exercise bodily autonomy while elevating Fauci and his ilk to Pope-like status. Science isn’t supposed to be a religious dogma that is set in stone, it’s an ever-evolving knowledge base that changes and improves thanks to dissent and skepticism.”
Science Depends on Questioning and Challenging Assumptions
Attorney Jonathan Turley also responded to Hotez’s paper in an August 4, 2021, blog post, saying:4
“’Religion is a culture of faith; science is a culture of doubt.’ Feynman’s statement captures how science depends upon constant questioning and challenging of assumptions …
[T]here remain important debates over not just the underlying science relation to Covid-19 but the implications for such science for public policies. Criminalizing aspects of that debate would ratchet up the threats against those with dissenting views, including some scientists. That would harm not just free speech but science in the long run.”
Should We Have Protected Classes That Cannot Be Questioned?
Turley also points out how making scientists a protected class (and one would assume only those with specific political leanings) is a slippery slope that will likely have unwieldy ramifications:5
“The federal hate crime laws focus on basis of a person’s characteristics of race, religion, ethnicity, nationality, gender, sexual orientation, and gender identity. We have seen calls for adding professions like police officers, which I also opposed.
As with police officers, the inclusion of such professions would have a direct and inimical impact on free speech in our society. Indeed, it would create a slippery slope as other professions demand inclusion from reporters to ministers to physicians. Hate crimes would quickly apply to a wide array of people due to their occupations.”
Will America Accept No-Fly List for Unvaccinated?
Writing for The Atlantic,6 former assistant secretary for Homeland Security Juliette Kayyem posits that people who do not want to be part of the COVID injection experiment “need to bear the burden” when it comes to preventing the spread of SARS-CoV-2.
“The number of COVID-19 cases keeps growing, even though remarkably safe, effective vaccines are widely available,” Kayyem writes.7 “Many public agencies are responding by reimposing masking rules on everyone.
But at this stage of the pandemic, tougher universal restrictions are not the solution to continuing viral spread. While flying, vaccinated people should no longer carry the burden for unvaccinated people.
The White House has rejected a nationwide vaccine mandate … but a no-fly list for unvaccinated adults is an obvious step that the federal government should take.
It will help limit the risk of transmission at destinations where unvaccinated people travel — and, by setting norms that restrict certain privileges to vaccinated people, will also help raise the stagnant vaccination rates that are keeping both the economy and society from fully recovering.”
Travel Ban Identified as Effective Coercion Strategy
According to Kayyem, traveling in general and flying in particular is not a human right, and putting unvaccinated individuals on a no-fly list is a matter of national security, in the sense that the country needs to protect itself from people capable of spreading this dangerous virus.
She makes no mention of the scientifically confirmed fact that none of the COVID shots actually prevent you from getting infected, and that “vaccinated” individuals carry the same viral load as the unvaccinated,8,9 which means they’re just as infectious. The main difference is that vaccinated individuals might not realize that they’re carriers, as the primary effect when the injections do work is lessening symptoms of infection.
Kayyem also cites a New York Times and Kaiser Family Foundation poll in which 41% of unvaccinated respondents had said prohibition on airline travel would sway their decision, including 11% of those “adamantly opposed” to vaccination. In other words, where free doughnuts and million-dollar lotteries have failed to coerce people to get the shot, an airline travel ban might do the trick.
Despite her former position within government, she makes no mention of laws forbidding coercion of medical volunteers, such as the U.S. Code of Federal Regulations 45 CFR 46 (subpart A, the Belmont report),10 the International Covenant on Civil and Political Rights treaty,11 the Declaration of Helsinki12 or the Nuremberg Code.13 Supreme court rulings have also clarified that Americans have the right to choose their own health care in general.14,15
Reframing to Confuse the Issue
Kayyem suggests circumventing such basic human rights by reframing the issue. She writes:16
“The public debate about making vaccination a precondition for travel, employment, and other activities has described this approach as vaccine mandates, a term that … suggests that unvaccinated people are being ordered around arbitrarily.
What is actually going on, mostly, is that institutions are shifting burdens to unvaccinated people … rather than imposing greater burdens on everyone.
Americans still have a choice to go unvaccinated, but that means giving up on certain societal benefits. Nobody has a constitutional right to attend The Lion King on Broadway or work at Disney or Walmart … People who still want to wait and see about the vaccines can continue doing so. They just can’t keep pushing all the costs on everyone else.”
As pointed out by Swift Headline,17 the owner of Atlantic magazine, Laurene Powell Jobs, the billionaire widow of Steve Jobs, owns two private jets herself, giving her the freedom to fly around the world at will, regardless what vaccine mandates might be in place. Many other ultra-rich individuals would also be able to ignore the rules due to wealth alone, essentially turning them into a protected class. Swift Headline points out this projection:18
“The Atlantic went on to say unvaccinated people who are exercising their individual rights as free Americans ‘do not deserve’ to be a ‘protected class’ …
Jobs’s wealth and class status is detailed in Breitbart News’ Editor-in-Chief Alex Marlow’s book, ‘Breaking the News: Exposing the Establishment Media’s Hidden Deals and Secret Corruptions,’ which ‘exposes the hidden connections between the establishment media and the activist left.’
As Marlow details, Jobs’s past is a privileged one … Jobs ‘married well and inherited a lot of money, and her wealth is tied up in some of world’s biggest companies,’ Marlow continues. ‘She is the establishment.’”
The Price of Admission to Society
August 2, 2021, the San Francisco Chronicle also published an opinion piece19 by the Chronicle editorial board, in which they suggested we ought to “Make vaccination the price of admission to society.” One way to evaluate the reasonableness of such a proposition is to replace COVID “vaccination” with anything else. How about: “Make proof of contraception use the price of admission to bars and nightclubs.”
“Make clear skin the price of admission to gyms and public swimming pools.” “Make being taller than 5’ 9” the price of admission to theme parks.” “Make having a BMI below 25 the price of admission to airline flights.” “Make proof of not having an illness the price of admission to in-hospital care.”
According to the Chronicle editorial board, “the unvaccinated account for over 95% of hospitalizations and deaths.”20 The board does not cite where it got that data from, so let’s review the source of that data.
In an August 5, 2021, video statement, Centers for Disease Control and Prevention director Dr. Rochelle Walensky noted that this statistic was obtained by looking at hospitalization and mortality data from January through June 2021 — a timeframe during which the vast majority of the United States population were unvaccinated.
When you look at more recent data, the trend is swinging in the opposite direction.
January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,21 and as of June 15, 48.7% were fully “vaccinated.”22
The CDC has also pointed out that you are not considered “fully vaccinated” until two weeks after your second dose (in the case of Pfizer or Moderna), which is given six weeks after your first shot.23 This means that if you receive your first dose on June 1, you won’t be “fully vaccinated” until eight weeks later, around August 1.
So, the narrative that we’re in a “pandemic of the unvaccinated” was created by using statistics from a time period when the U.S. as a whole was largely unvaccinated. When you look at more recent data, the trend is swinging in the opposite direction.
Vaccinated Now Comprise the Bulk of Hospitalizations
For example, August 1, 2021, Dr. Sharon Alroy-Preis, director of Israel’s Public Health Services, announced half of all COVID-19 infections were among the fully vaccinated.24
A few days later, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID related hospitalizations overall.25
In Scotland, official data on hospitalizations and deaths show 87% of those who have died from COVID-19 in the third wave that began in early July were vaccinated,26 and in Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.27
A CDC investigation of an outbreak in Barnstable County, Massachusetts between July 6 through July 25, 2021, found 74% of those who received a diagnosis of COVID19, and 80% of hospitalizations, were among the fully vaccinated.28,29 Most, but not all, had the Delta variant.
“What the breakthrough cases appear to show is that the delta variant of the coronavirus is more easily carried and transmitted by vaccinated people than its predecessors,” the Chronicle editorial board writes.30
“In any case, the greater apparent transmissibility of the variant makes it that much more important to protect as many people as possible from severe COVID by increasing inoculation rates.”
What the board appears to be saying is that unvaccinated people must be protected against severe infection, against their will, if need be, and the best way to do that is to discriminate against them and treat them like second-class citizens.
Again, a simple way to check the reasonableness of this argument is to swap out the COVID reference for something else. How about, “It’s important to protect as many people as possible from dying in car accidents by raising car prices so fewer people can get behind the wheel.”
Can ‘Big Brother’ Save You From a Virus?
As early as April 2020, The Times in the U.K. weighed in with similar suggestions, stating “We need Big Brother to beat this virus.”31 Clare Foges, the author of the piece in question, went on to say, “Don’t let the civil liberties lobby blind us to the fact that greater state surveillance, including ID cards, is required.”
The argument that Big Brother can protect us from infection is ludicrous on its face, because no amount of people surveillance can prevent microscopic viruses from circulating.
The No. 1 place of viral spread is in institutions, such as nursing homes and hospitals, yet the staff within them are among the most well-trained in pathogenic control. If trained hospital staff can’t prevent the spread of viruses, how can government officials do it?
Importantly, the argument that we need vaccine passports to prove we’re “clean” enough to participate in society immediately falls apart when you take into account the fact that the COVID shots do not provide immunity. You can still be infected, carry the virus and spread it to others.
We’ve already seen several examples of situations where 100% of people were fully “vaccinated” against COVID-19 yet an outbreak occurred. We’ve even seen over 100 fully COVID injected people die from COVID in one state alone, Massachusetts,32 so it is likely there are now many thousands of fully “vaccinated” who have died from COVID.
Even a 100% Vaccination Rate Cannot Eliminate COVID
Most recently, Carnival cruise lines experienced an outbreak despite every last person on that ship having proof of COVID “vaccination.”33 The cruise liner had even intentionally reduced capacity from 4,000 to 2,800 to provide ample social distancing capability. None of the measures worked. People got sick anyway, which makes perfect sense if you remember that the shot doesn’t provide immunity, only symptom reduction.
Cases such as these clearly reveal that even if everyone gets the shot, SARS-CoV-2 will mutate and continue to circulate, taking people out here and there. To think that giving up basic rights and freedoms is the answer simply isn’t logical. Taking responsibility for your own health is, and that includes deciding if and how you want to protect yourself from SARS-CoV-2.
Not everyone is deathly afraid of COVID-19. Many realize there are safe and effective treatments available, such as the Front Line COVID-19 Critical Care Alliance’s I-MASS Prevention and At-Home Treatment protocol and I-MASK+ Early Outpatient Treatment protocol.
Nebulized hydrogen peroxide can also be used for prevention and treatment of COVID-19, as detailed in Dr. David Brownstein’s case paper34 and Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” And if there’s effective treatment, there’s little need to risk permanent side effects from an experimental gene technology that can only provide a narrow range of protection in the first place.
CDC Records: 12,791 DEAD and 682,873 Injuries Following COVID-19 Experimental Shots
By Brian Shilhavy | Health Impact News | August 16, 2021
According to the most recent stats released by the CDC this past Saturday, August 14, 2021, their Vaccine Adverse Event Reporting System (VAERS) now has recorded more than twice as many deaths following the non-FDA approved experimental COVID-19 shots during the past 8 and a half months, than deaths recorded following ALL FDA approved vaccines for the past 30 years.
This has to be the most censored information in the U.S. right now, even though these statistics come directly from the CDC.
They have now recorded 12,791 deaths, 16,044 permanent disabilities, 70,667 emergency room visits, 51,242 hospitalizations, 13,139 life threatening events, among 682,873 reported injuries from 571,831 cases.

The CDC’s official response to these statistics is that they are basically coincidences, and are not related to the experimental COVID-19 shots.
Reports of adverse events to VAERS following vaccination, including deaths, do not necessarily mean that a vaccine caused a health problem. A review of available clinical information, including death certificates, autopsy, and medical records, has not established a causal link to COVID-19 vaccines. (Source.)
Trusting in the CDC for COVID-19 safety information is quite obviously deadly. Because it is widely known that these statistics that they admit to are but a fraction of actual cases, as very few medical professionals are willing to classify an injury or death as caused by COVID-19 injections.
By way of contrast, deaths following all FDA-approved vaccines for the 30 years prior to the emergency use authorizations of the COVID-19 shots total 6,068 over 30 years according to the CDC.

What are NOT included in these 12,791 deaths the CDC is reporting following COVID-19 shots, are the number of fetal deaths following COVID-19 injections into pregnant women, which now numbers 1,360 deaths according to the CDC.

Source
The FDA and CDC Serve Big Pharma – Not the Public
The Big Pharma cartel is now fully in control of just about every aspect of our lives. They own the corporate media which is not reporting any of these statistics from VAERS, and they control the health agencies like the NIH, the CDC, and the FDA.
They are rushing now to remove the emergency use authorization on these COVID-19 shots, so that they can legally be mandated, and the Pentagon has already stated that they will mandate them for the U.S. Military in September.
The FDA has also just recently approved a 3rd booster COVID-19 shot “for those who are immunocompromised.”
Los Angeles County started offering these 3rd Pfizer COVID-19 shots this past weekend.
Anthony Fauci did the Sunday talk show tour yesterday, and stated that Americans need to surrender their liberties (yes, he actually said that) because we are all fighting a common enemy, “the virus.”
In addition, the Department of Homeland Security has now issued a bulletin declaring that anyone who questions COVID-19 measures like masks and “vaccines” are potential “domestic terrorists.”
They are using a bogus COVID-19 “outbreak” called the “Delta variant,” and the CDC has already been caught lying about who are actually being hospitalized right now, falsely stating that the “unvaccinated” are filling up hospitals, when almost the exact opposite is happening around the world.
Israel, Australia Report 95-99% Hospitalized are Fully Vaccinated
The Lies Behind the ‘Pandemic of Unvaxxed’
By Dr. Joseph Mercola | August 16, 2021
According to the Centers for Disease Control and Prevention, the White House and most mainstream media, what we have now is a “pandemic of the unvaccinated.”1
According to the official narrative, 99% of COVID-19 deaths and 95% of COVID-related hospitalizations are occurring among the unvaccinated. In a July 16, 2021, White House press briefing,2 CDC director Dr. Rochelle Walensky claimed “over 97% of people who are entering the hospital right now are unvaccinated.”
But as reported by Fox News anchor Laura Ingraham on “The Ingraham Angle,” “that statistic is grossly misleading,”3 and in an August 5, 2021, video statement, Walensky inadvertently revealed how that 95% to 99% statistic was created.
Grossly Misleading Data Manipulation
As it turns out, to achieve those statistics, the CDC included hospitalization and mortality data from January through June 2021. It does not include more recent data or data related to the Delta variant, which is now the most prevalent strain in circulation. The problem is, the vast majority of the United States population was unvaccinated during that timeframe.
January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,4 and as of June 15, 48.7% were fully “vaccinated.”5 Keep in mind that you’re not “fully vaccinated” until two weeks after your second dose (in the case of Pfizer or Moderna), which is given six weeks after your first shot. This is according to the CDC.6
So, those receiving an initial dose in June, for example, won’t be “fully vaccinated” until eight weeks later, sometime in July or August.
By using statistics from a time period when the U.S. as a whole was largely unvaccinated, the CDC is now claiming we’re in a “pandemic of the unvaccinated,” in an effort to demonize those who still have not agreed to receive this experimental gene modification injection.
Selective Pressure Promotes Emergence of New Variants
Here’s what Canadian viral immunologist and vaccine researcher Dr. Byram Bridle told Ingraham about the claim that we’re in a pandemic of the unvaxxed, and that the unvaccinated are hotbeds for dangerous variants:
“Absolutely, it’s untrue to be calling this a pandemic of the unvaccinated. And it’s certainly untrue … that the unvaccinated are somehow driving the emergence of the novel variants. This goes against every scientific principle that we understand.
The reality is, the nature of the vaccines we are using right now, and the way we’re rolling them out, are going to be applying selective pressure to this virus to promote the emergence of new variants. Again, this is based on sound principles.
We have to look no further than … the emergence of antibiotic resistance … The principle is this: If you have a biological entity that is prone to mutation — and the SARS-CoV-2, like all coronaviruses is prone to mutation — and you apply a narrowly focused selective pressure that is nonlethal, and you do this over a long period of time, this is the recipe for driving the emergence of novel variants.
This is exactly what we’re doing. Our vaccines are focused on a single protein of the virus, so the virus only has to alter one protein, and the vaccines don’t come close to providing sterilizing immunity.
People who are vaccinated still get infected, it only seems particularly good at blunting the disease, and what that tells you therefore is that these vaccines in the vast majority of people are applying a nonlethal pressure, narrowly focused on one protein, and the vaccine rollout is occurring over a long period of time. That’s the recipe for driving variants.”
Natural Immunity Offers Far Superior Protection
Bridle also explains why natural immunity offers robust protection against all variants, whereas vaccine-induced immunity can’t. When you acquire the infection naturally, your body develops antibodies against ALL of the viral proteins whereas the COVID shots only trigger antibodies against one, namely the spike protein.
As mentioned above, when you have antibodies against just one of the viral proteins, the virus only needs to mutate that one protein in order to evade your immune system. When you have natural immunity, on the other hand, your antibodies will recognize all parts of the virus, so even if the spike protein is mutated, your body will recognize other parts of the virus and mount an attack against those.
That SARS-CoV-2 works the same way other viruses do was shown in a Nature Reviews Immunology study7 by Alessandro Sette and Shane Crotty, published in October 2020. The study, “Cross-Reactive Memory T Cells and Herd Immunity to SARS-CoV-2” argued that naturally-acquired immunity against SARS-CoV-2 is potent, long-lasting and very broad in scope, as you develop both antibodies and T cells that target multiple components of the virus and not just one.
If we are to depend on vaccine-induced immunity, as public health officials are urging us to do, we’ll end up on a never-ending booster treadmill. Boosters will absolutely be necessary, as the shot offers such narrow protection against a single protein of the virus. Already, data around the world show vaccine-induced protection is waning rapidly in the face of new variants, and Moderna has publicly stated that the need for additional boosters is expected.8
How Dangerous Is the Delta Variant?
According to Dr. Anthony Fauci, the Delta variant is both more transmissible and more dangerous than the original virus and previous variants. July 4, 2021, he told NBC News:9
“It is more effective and efficient in its ability to transmit from person to person. And studies that we’ve seen where they have been the variant that’s dominated in other countries, it’s clear that it appears to be more lethal in the sense of more serious — allow you to get more serious disease leading to hospitalization, and in some cases leading to deaths.”
In a June 29, 2021, interview,10 Fauci called the Delta variant “a game-changer” for unvaccinated people, warning it will devastate the unvaccinated population while vaccinated individuals are protected against it.
Remember, Fauci is not a clinician and has never treated someone infected with SARS-CoV-2. Other health experts and practicing physicians who treat COVID-19 patients disagree with Fauci’s claims, arguing that not only is the Delta variant not more dangerous, it’s certainly not more dangerous for the unvaccinated.
As reported by Ingraham in June 2021 (video above), there’s an evolutionary genetics theory called Muller’s Ratchet, which states that as an outbreak starts to peter out, the virus tends to mutate into a more transmissible form, but at the same time it grows weaker, causing far less serious infection. According to epidemiologist and cardiologist Dr. Peter McCullough, this is exactly what we’re seeing. He told Ingraham:
“The good news is on the 18th of June, the United Kingdom presented their 16th report11 on the mutations — and they’re doing a great job, much better than our CDC — and what they demonstrated is that the Delta is more contagious but it’s far less deadly, far less worrisome. In fact, it’s a much weaker virus than both the U.K. [Alpha] and the South African [Beta] variants.”
Spike Mutations Render Vaccinated Vulnerable to Delta
Importantly, the Delta variant contains three different mutations, all in the spike protein. This, McCullough explains, allows this variant to evade the immune responses in those who have received the COVID jabs — but not those who have natural immunity which, again, is much broader. In a June 30, 2021, appearance on Fox News, McCullough stated:12
“It is very clear from the UK Technical Briefing13 that was published June 18th that the vaccine provides no protection against the Delta variant. It’s a very mild variant.
Whether you get the vaccine or not, patients will get some very mild symptoms like a cold and they can be easily managed … Patients who have severe symptoms or at high risk, we can use simple drug combinations at home and get them through the illness. So, there’s no reason now to push vaccinations.”
Children’s Health Defense chief scientific officer Brian Hooker, Ph.D., has echoed McCullough’s sentiments. The Defender quotes Hooker:14
“What we’re seeing is virus evolution 101. Viruses like to survive, so killing the host (i.e. the human who is infected) defeats the purpose because killing the host kills the virus, too. For this reason, new variants of viruses that circulate widely through the population tend to become more transmissive but less pathogenic. In other words, they will spread more easily from person to person, but they will cause less damage to the host.
The vaccine focuses on the spike protein, whereas natural immunity focuses on the entire virus.
Natural immunity — with a more diverse array of antibodies and T-cell receptors — will provide better protection overall as it has more targets in which to attack the virus, whereas vaccine-derived immunity only focuses on one portion of the virus, in this case, the spike protein. Once that portion of the virus has mutated sufficiently, the vaccine no longer is effective.”
Real-World Data Show Most of Infected are Fully ‘Vaccinated’
Real-world data from areas with high COVID jab rates show the complete converse of what media, the CDC and White House officials are telling us. In addition to the British Technical Briefing No. 16,15 cited above, we have additional data from Israel, Scotland, Massachusetts and Gibraltar:
•August 1, 2021, director of Israel’s Public Health Services, Dr. Sharon Alroy-Preis, announced half of all COVID-19 infections were among the fully vaccinated.16 Signs of more serious disease among fully vaccinated are also emerging, she said, particularly in those over the age of 60.
A few days later, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID-related hospitalizations overall.17 As of August 2, 2021, 66.9% of Israelis had received at least one dose of Pfizer’s injection, which is used exclusively in Israel; 62.2% had received two doses.18
•In Scotland, official data on hospitalizations and deaths show 87% of those who have died from COVID-19 in the third wave that began in early July were vaccinated.19
•A CDC investigation of an outbreak in Barnstable County, Massachusetts, between July 6 through July 25, 2021, found 74% of those who received a diagnosis of COVID19, and 80% of hospitalizations, were among the fully vaccinated.20,21 Most, but not all, had the Delta variant of the virus.
The CDC also found that fully vaccinated individuals who contract the infection have as high a viral load in their nasal passages as unvaccinated individuals who get infected.22 This means the vaccinated are just as infectious as the unvaccinated.
•In Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.23
While those who benefit from keeping the pandemic going would like you to cower in fear at the thought of the Delta variant, there’s really no evidence that it’s any worse than the original. It’s more transmissible, yes, but far less dangerous, as its primary symptoms are that of a regular cold.
According to Harvard and Stanford professors, the actual number of Americans dying from or with COVID-19 are actually at an all-time low, so alarmism is uncalled for.24
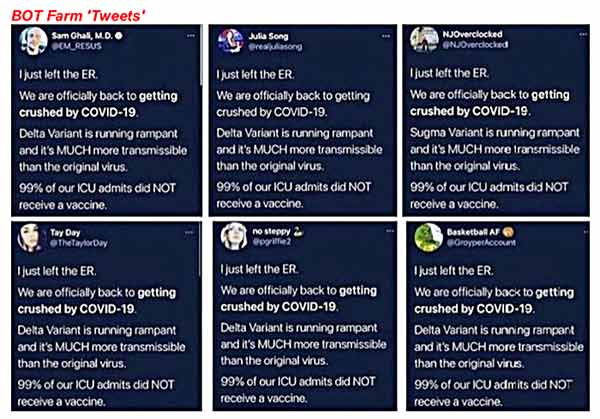
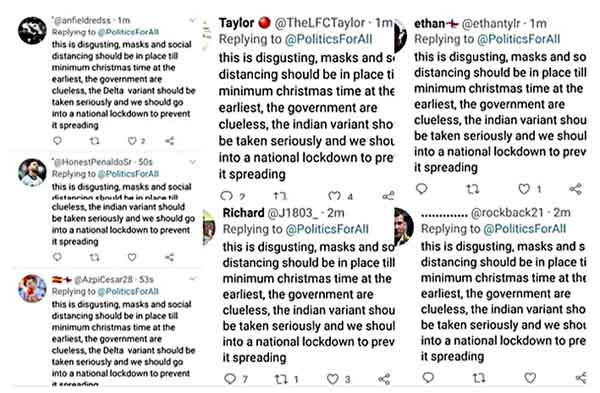
And, as for viral social media posts by doctors and nurses claiming hospitals are overflowing with unvaccinated COVID patients, don’t believe them. Most are bots. We’ve repeatedly seen evidence that fearmongering is being spread not by real people but by fake accounts run by artificial intelligence. This includes blue check accounts. Here’s a sampling of recent bot farm tweets trying to scare everyone:25
Don’t Fear It, Just Treat It
In closing, remember there are several different treatment protocols for COVID-19 that appear just as effective for variants as for the original virus, including the following:
- Front Line COVID-19 Critical Care Alliance’s I-MASS Prevention and At-Home Treatment protocol
- The FLCCC’s I-MASK+ Prevention and Early Outpatient Treatment protocol
- The FLCCC’s I-RECOVER management protocol for long-haul COVID-19 syndrome
- Nebulized hydrogen peroxide for prevention and treatment of COVID-19, as detailed in Dr. David Brownstein’s case paper26 and Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” Levy believes nebulized hydrogen peroxide can also be an invaluable strategy for combating spike protein toxicity27 because, in addition to being a powerful antiviral, it will also augment and speed up cellular healing, in part by improving oxygenation
Sources and References
- 1 The New York Times July 16, 2021
- 2 WH.gov Press Briefing July 16, 2021
- 3 Fox News
- 4 Bloomberg COVID Vaccine Tracker, see US Vaccinations vs Cases graph, top portion
- 5 Mayo Clinic COVID Vaccine Tracker
- 6 CDC.gov When You’ve Been Fully Vaccinated Updated July 27, 2021
- 7 Nature Reviews Immunology October 6, 2020; 20: 709-713
- 8 The Hill August 5, 2021
- 9 NBC News July 4, 2021
- 10 PBS June 29, 2021
- 11, 13, 15 Public Health England, SARS-CoV-2 Variants Technical Briefing 16, June 18, 2021 (PDF)
- 12 Covidcalltohumanity.org July 5, 2021
- 14 The Defender August 3, 2021
- 16 Bloomberg August 1, 2021 (Archived)
- 17 American Faith August 8, 2021
- 18 Our World in Data, Data for Israel
- 19 The Daily Expose July 29, 2021
- 20 CDC MMWR July 30, 2021; 70
- 21 CNBC July 30, 2021
- 22 NBC News August 7, 2021
- 23 Big League Politics August 4, 2021
- 24 FEE.org July 28, 2021
- 25 Padrak.com Vaccine Propaganda Bot Farms (PDF)
- 26 Science, Public Health Policy and The Law July 2020; 1: 4-22 (PDF)
- 27 Orthomolecular Medicine News Service, June 21, 2021
California Hospitals Require Proof of Visitors’ COVID Vaccine or Negative Test to Enter

21st Century Wire | August 16, 2021
Since the very beginning of the ‘global pandemic,’ the state of California has led the way as one of the most aggressive violators of its citizens Constitutional rights and freedoms. Like many governments, the state has sought to justify its authoritarian policies and coercive measures by claiming these are necessary in order to ‘stop the spread of virus’ – despite the fact that there exists no scientific basis for such broad claims on the efficacy of such interventions. Regardless, governments everywhere are pushing forward even harder in the race to implement Vaccine Passports as a mechanism to to force the entire population to accept an unending series of unlicensed, experimental corporate products – in this case, brand new COVID-19 vaccines. Once again, government is claiming these are absolutely necessary to ‘stop the spread of virus,’ and again, there exists no scientific basis for these broad claims either.
Regardless of these facts, American healthcare providers are now pushing ahead by banning visitors from their facilities who do no submit to either COVID-19 corporate PCR testing or experimental vaccine regimes.
Given the state’s already abysmal record in protecting its residents’ civil liberties, it should be no surprise that California is now leading the way in the United States in denying freedom of movement of the unvaccinated.
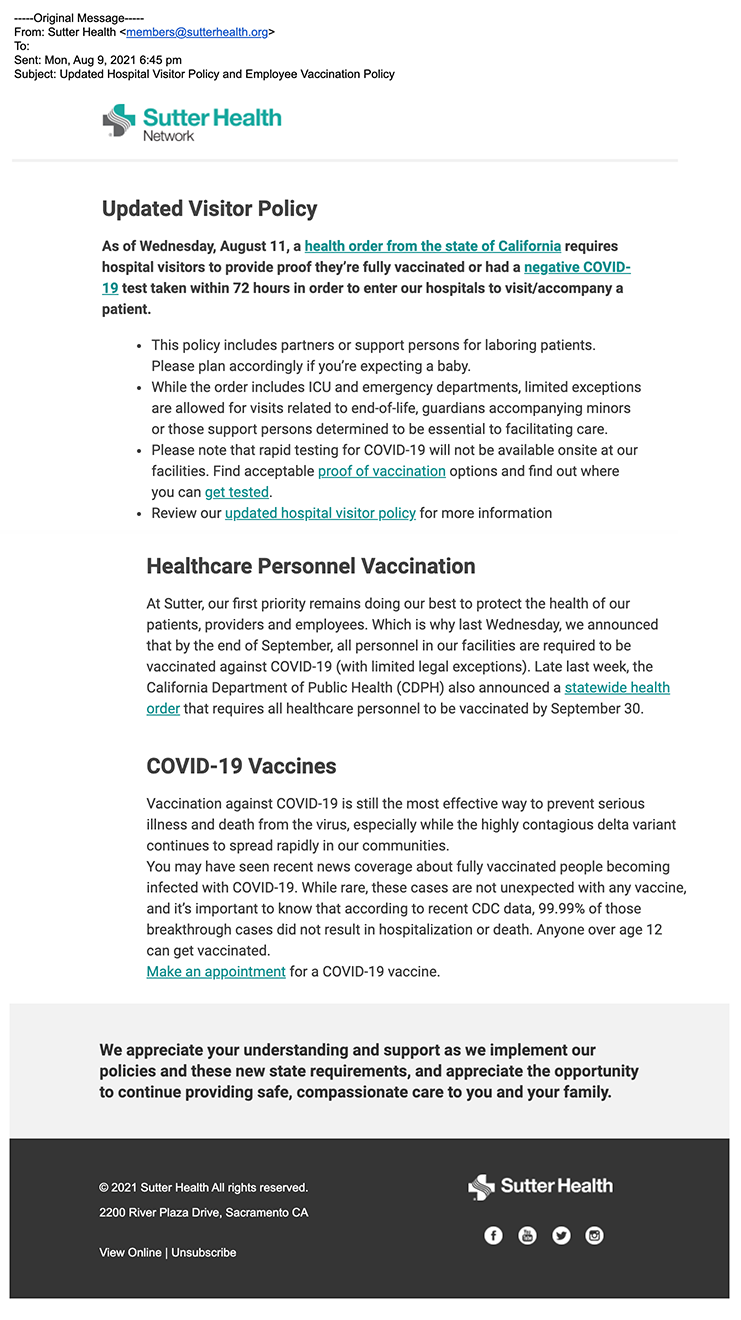
According to an email (see below) sent out this week to the members of Sutter Health Network, the state public health’ officials have issued a new decree that visitors to facilities will no longer be able to enter hospitals or retirement care homes – without a COVID-19 vaccine, or a negative COVID-19 test. The announcement began with the following text:
———————
- This policy includes partners or support persons for laboring patients. Please plan accordingly if you’re expecting a baby.
- While the order includes ICU and emergency departments, limited exceptions are allowed for visits related to end-of-life, guardians accompanying minors or those support persons determined to be essential to facilitating care.
- Please note that rapid testing for COVID-19 will not be available onsite at our facilities. Find acceptable proof of vaccination options and find out where you can get tested.
- Review our updated hospital visitor policy for more information
———————
Thank you to News From Underground for this tip.
The claims made by state health officers are simply breathtaking – in the sense that their statements do not correspond at all with the reality, even according to widely known official data.
In order to give the impression that the state is still in the grips of a ‘pandemic,’ it is relying on fabricated ‘case’ numbers gleaned from corrupted false positive test data from non-diagnostic PCR test. Even so, it’s still struggling to show significant ‘infection’ numbers:
California is currently experiencing the fastest increase in COVID-19 cases during the entire pandemic with 18.3 new cases per 100,000 people per day, with case rates increasing ninefold within two months.
By pursing completely arbitrary, non science-based policies, the state appears to following in the footsteps Australia’s failing “Zero COVID” policy.
State officials then go on to claim California is now under viral siege from an uncontrollable and “possibly” more deadly ‘Delta Variant’:
The Delta variant, which is very highly contagious and possibly more virulent, is currently the most common variant causing new infections in California.
The fabrications continue with the government making the now widely discredited false claim that “Unvaccinated persons are more likely to get infected and spread the virus” (official data from Israel, Iceland and numerous other regions clearly show that the vaccinated are actually driving the alleged outbreaks), a commonly repeated canard disseminated by the Biden Administration and mainstream media outlets:
Unvaccinated persons are more likely to get infected and spread the virus, which is transmitted through the air. Most current hospitalizations and deaths are among unvaccinated persons.
So at present, the only real epidemic appears to be an epidemic of medical misinformation’ being promulgated by government itself.
The catastrophic catalogue of vaccine reactions
By Sally Beck | TCW Defending Freedom | August 16, 2021
THE Medicines and Healthcare products Regulatory Agency (MHRA), the government body which approved the experimental Covid vaccines for emergency use, is receiving unprecedented numbers of Yellow Card Scheme reports about the vaccines. The self-reporting system, which receives approximately 10 per cent of adverse events, monitors the vaccine damage numbers reported by the public and health professionals. It is intended to be an early warning system which flags up problems that might not have come to light in clinical trials so that authorities can act.
The figures to August 4 included 1,536 deaths, which should provoke outrage in the government and a press conference to explain, but instead we’ve had an uncomfortable silence. No one in power wants to talk about the vaccine damage elephant in the room.
We know a ‘rare’ event is attributed to AstraZeneca’s ‘clotshot’, the jab which has the nasty and sometimes fatal side effect of vaccine-induced thrombosis (VITT), but the 73 deaths accepted as VITT deaths by the MHRA so far, are in the minority of the serious reactions that have been reported.
The other serious issue which is developing with Pfizer and Moderna, but is almost double if you receive the AstraZeneca vaccine, is heart problems. There are 13,838 reports of acute cardiac problems and 712 reports of heart attacks and heart failure, with 9,440 acute cardiac events attributed to AZ; 4,644 to Pfizer; Moderna, the new kid on the block, have clocked up 38 while 1,715 are unknown.
Perhaps the best way to bring home what it means if you develop inflammation of the heart muscle (myocarditis), inflammation of the sac protecting the heart (pericarditis) or any other heart problem is to join the 5.3k people following the Mark Briggs Updates page on Facebook.
Mark Briggs, 55, is a miner and loving father and grandfather from Rockhampton, Queensland, Australia. He received an AstraZeneca shot on June 15 and developed heart symptoms that night.
His partner Sammy said: ‘He started getting pains between his shoulder blades so took some ibuprofen and came good. He went to his seven-day shift at the mine and on the last shift began getting pains between the shoulder blades again. He drove home and on 23rd June had chest pain. He called the vaccine clinic and said, “I’ve got chest pain, is there anything to worry about?” They said don’t ring us, ring your GP. The GP said don’t ring us, call an ambulance. We called an ambulance, and he was in hospital all day. They couldn’t find anything wrong so sent him home. That night he was in pain and restless and woke at 5am with severe pain in his arms. He went back into hospital and has been there ever since.’
After two weeks Mr Briggs was airlifted from the hospital in Rockhampton to Brisbane, where he could receive specialist treatment. Sammy said: ‘We were all called to say goodbye before he left, in case he didn’t make it. He was in Brisbane for two weeks then sent back to Rockhampton where he crashed again, and he’s been ventilated and heavily medicated since.
‘He didn’t normally get sick, was on no medication, was fit and healthy, played lots of sport and didn’t get the flu vaccine.’
Initially, Mr Briggs was diagnosed with mild pericarditis and since then has developed heart failure, septicaemia and pneumonia. He has had spinal taps, blood tests, bone marrow biopsies, CT scans and other X-rays. He’s been seen by cardiologists, cardiothoracic surgeons, neurologists, rheumatologists, immunologists, but no one can work out what’s wrong with him. He’s been in an artificially induced coma, ventilated, and given the strongest pain medication such as fentanyl and morphine, which barely relieved his discomfort.
So far there is no official diagnosis of vaccine damage. Sammy said: ‘Initially a doctor will say that there is no link with the vaccine because the problem they know with the AstraZeneca is blood clotting, but by the end of the five-day roster they have with him they then say they think it is. One doctor said if it wasn’t Q fever [bacterial infection with severe flu-like symptoms] he was sure it was the vaccine. But no one will officially say until the TGA [Therapeutic Goods Administration, part of the Australian government department of health responsible for monitoring medicines] has investigated and said it is an official case of vaccine damage.’
He has been in hospital for 52 days. The family don’t know if he will recover, but if he does they’ve been told he’ll need at least six months’ rehabilitation because his muscle wastage is so bad. He has developed anxiety too, which he’s never had, and he was the main earner but on a casual wage, so the family have no money coming in.
Yesterday’s Facebook post from his daughter Jayde Jamieson said that Mark had been flown back to Brisbane and that on Saturday night his heart rate and blood pressure had dropped before going up again on Sunday morning. Both are irregular and all anyone can do currently is pray for his recovery.
Updated Yellow Card report published by MHRA on August 13, covering reports up to August 4, 2021
Pfizer: 20.8million people, 35.5million doses. Yellow Card reporting rate: 1 in 205 people impacted
AstraZeneca: 24.8million people, 48.6million doses. Yellow Card reporting rate: 1 in 109 people impacted
Moderna: 1.4million people, 1.9million doses. Yellow Card reporting rate: 1 in 111 people impacted
Overall 1 in 137 people experience a Yellow Card Adverse Event after vaccination. This may be a reporting rate of approximately 10 per cent, according to MHRA.
Reactions: 284,776 Pfizer; 806,489 AZ; 38,285 Moderna; 3,029 unknown. Total 1,132,579
Reports: 101,483 Pfizer; 226,959 AZ; 12,569 Moderna; 1,003 unknown. Total 342,014
Fatal: 486 Pfizer; 1,036 AZ; 10 Moderna; 27 unknown. Total 1,559
Acute cardiac: 4,425 Pfizer; 8,964 AZ; 417 Moderna; 32 unknown. Total 13,838
Myocardial infarction and heart failure: 219 Pfizer; 476 AZ; 11 Moderna; 6 unknown. Total 712
Anaphylaxis: 453 Pfizer; 803 AZ; 30 Moderna; 1 unknown. Total 1,287
Blood disorders: 9,545 Pfizer; 7,283 AZ; 734 Moderna; 42 unknown. Total 17,604
Infections: 6,718 Pfizer; 17,843 AZ; 617 Moderna; 87 unknown. Total 25,265
Headaches: 20,686 Pfizer; 83,141 AZ; 2,150 Moderna; 223 unknown. Total 106,200
Migraine: 2,319 Pfizer; 7,948 AZ; 245 Moderna; 29 unknown. Total 10,541
Eye Disorders: 4,711 Pfizer; 13,526 AZ; 404 Moderna; 50 unknown. Total 18,691
Blindness: 93 Pfizer; 271 AZ; 10 Moderna; 3 unknown. Total 377
Deafness: 177 Pfizer; 348 AZ; 13 Moderna; 1 unknown. Total 539
Psychiatric disorders: 5,692 Pfizer; 16,802 AZ; 759 Moderna; 73 unknown. Total 23,326
Skin disorders: 20,211 Pfizer; 49,841 AZ; 6,102 Moderna; 207 unknown. Total 76,361
Spontaneous abortions: 242 + 6 stillbirth/foetal death Pfizer; 177 + 2 stillbirth AZ; 21 + 1 foetal death Moderna; 1 unknown. Total 441 + 9 (figures imply 14 related maternal deaths)
Vomiting: 3,069 Pfizer; 11,299 AZ; 404 Moderna; 39 unknown. Total 14,811
Facial paralysis including Bell’s palsy: 658 Pfizer; 843 AZ; 44 Moderna; 5 unknown. Total 1,550
Nervous system disorders: 50,230 Pfizer; 172,644 AZ; 5,891 Moderna; 576 unknown. Total 229,341
Strokes and CNS haemorrhages: 484 Pfizer; 1,945 AZ; 13 Moderna; 6 unknown. Total 2,448
Guillain Barré Syndrome: 39 Pfizer; 377 AZ; 2 Moderna; 5 unknown. Total 423
Dizziness: 7,892 Pfizer; 24,041 AZ; 1,252 Moderna; 81 unknown. Total 33,266
Tremor: 1,198 Pfizer; 9,636 AZ; 132 Moderna; 37 unknown. Total 11,003
Pulmonary embolism & deep vein thrombosis: 549 Pfizer; 2,630 AZ; 23 Moderna; 17 unknown. Total 3,219
Respiratory disorders: 12,238 Pfizer; 27,129 AZ; 978 Moderna; 105 unknown. Total 40,450
Seizures: 668 Pfizer; 1,841 AZ; 94 Moderna; 8 unknown. Total 2,611
Paralysis: 282 Pfizer; 719 AZ; 33 Moderna; 5 unknown. Total 1039
Haemorrhage (all types): 2,332 Pfizer; 4,605 AZ; 114 Moderna; 22 unnknown. Total 7,073
Vertigo/Tinnitus: 2,535 Pfizer; 6,199 AZ; 238 Moderna; 21 unknown. Total 8,993
Reproductive/breast: 15,471 Pfizer; 16,103 AZ; 1,969 Moderna; 108 unknown. Total 33,651
See Annex One for full reports.
Canada to introduce vaccine passports for crossing provincial borders
By Dan Frieth | Reclaim The Net | August 14, 2021
Canada’s Minister for Transport Omar Alghabra announced the introduction of vaccine passports for transport across provincial borders via plane, trains, and large water vessels.
The move underscores the growing adaptation of digital vaccine passports across the globe, particularly in developed countries.
“Vaccine requirements in the transportation sector will help protect the safety of employees, their families, passengers, their communities and all Canadians. And more broadly, it will hasten Canada’s recovery from the COVID-19 pandemic,” Alghabra said during a press conference on Thursday.
For those who cannot get the jabs, the minister said they will still be able to travel by showing proof of recent negative tests.
Alghabra said that the government was looking into practical ways to implement the vaccine passes “as quickly as possible.”
Alghabra’s announcement coincided with an announcement from the Privy Council that the government would be mandating vaccination for federal employees. The employees will be required to show proof of having received both doses of the COVID-19 vaccines.
The Evolving Definition of “Vaccine” in the Merriam-Webster Dictionary for 2021
By Brian Shilhavy | Health Impact News | August 13, 2021
The popular online dictionary, Merriam-Webster.com, has had the same definition for “vaccine” for several years.
Here is the definition until early to mid-January, 2021:

By January 26, 2021 it was changed to include a section on “genetic material” and mRNA:

Apparently that was not quite good enough to silence the critics who were claiming that the COVID-19 shots did not meet the definition of a “vaccine,” so it was changed again by June 1, 2021 to include examples of mRNA “vaccines” such as Moderna and Pfizer, “viral vector” vaccines such as J&J and AstraZeneca, and a completely new definition to cover some “vaccines” the military is working on: a preparation or immunotherapy that is used to stimulate the body’s immune response against noninfectious substances, agents, or diseases.

I wonder what this “definition” of “vaccines” will be expanded to include next?
Noah Webster Jr. was the original founder of America’s most famous dictionary, and in 1831, George and Charles Merriam founded the company as G & C Merriam Co.
In 1964, Encyclopædia Britannica, Inc. acquired Merriam-Webster, Inc.
In 1996, Britannica was purchased by Jacob E. Safra, a Jewish Swiss-bank financier.
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
A low-fat, high-carb diet has been the largest public health experiment in history. It’s past time for a rethink.
By Malcolm Kendrick | RT | November 25, 2020
New research suggests that four billion people globally will be overweight in 2050. This trend can be traced back to the ‘low-fat, high-carb’ guidelines first issued in the 70s, and should prompt a major U-turn on dietary advice.
A recent report from the Potsdam Institute predicts that by 2050 there will be four billion overweight people in the world, with one-and-a-half billion of them obese. This is not entirely surprising. The world has been getting fatter for years, and things do not seem to be slowing down.
Why is this happening? … continue
Blog Roll
 Aletho News
Aletho News- OPCW Forced To Pay Damages To Whistleblower Who Found Evidence Of False Flag In Syria
- Iran can thrive under blockade, the US and its allies cannot
- Iran slams US leadership, debunking fabrications, false war costs
- Here’s why Iran is sovereign and Germany is not
- Israel pours $730m into global propaganda machine as reputation collapses
- Leaked audios reveal pro-Israel groups ‘paid’ for US pardon of convicted drug trafficker Juan Orlando Hernandez
- Congress Extends Section 702 Spy Program 45 Days
- Zionists Are Gunning for Your Freedom of Speech
- Larry Johnson: U.S. Desperation Grows as Iran Is Winning
- Why don’t UK media mention the Israel lobby?
- If Americans Knew
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
