Comments in response to FDA’s license of Pfizer vax today for 16 years and up
By Meryl Nass, MD | August 23, 2021
The vaccine-induced protection provided by Covid vaccines starts fading within months. In late July, Israel’s Minister of Health said vaccine protection had dropped to 39%. It is not preventing severe illness in Israel and the UK either, though the US CDC changed its collecting methods for breakthrough cases on May 1 to disguise this fact.
While the US government has said it will begin booster doses of mRNA vaccines the week of September 20, there is actually NO evidence that Covid-19 boosters will provide increased protection against infection, or that they are effective against the delta variant or other new variants.
For other vaccines, such as mumps and pertussis, there is no evidence that booster doses after the initial course add measurable protection.
Boosters do raise antibody levels, briefly, which increases the risk of autoimmune adverse effects, immune overactivity and the dire possibility of antibody-enhanced disease (AED), a.k.a. vaccine-enhanced disease (VED), in which those who are vaccinated have a much more severe illness when exposed to Covid than do the unvaccinated.
Since the UK’s top vaccine expert Sir Andrew Pollard told Parliament 2 weeks ago that herd immunity cannot be obtained—in fact it is a “myth”– because the vaccine is not halting transmission, and since the CDC director confirmed this, there is no logical reason to mandate vaccinations for anyone, since the vaccines are not protecting the community.
Mandating vaccinations for the young and healthy, who are at minimal risk from Covid, but at increased risk from Covid vaccinations, is a travesty. The risk of myocarditis after vaccination in a male teenager is 50 times higher than the risk to a 65 year old, according to CDC data. The teenager has many years ahead of him, while the long-term side effects from Covid vaccines have yet to be identified.
Reported deaths following Covid vaccinations are at least 10 times higher than for any vaccine ever approved in the US. Yet FDA and CDC have never explained the causes of these deaths, and they pretend they do not exist.
This fact alone should have been sufficient to stop FDA granting a license to the Pfizer vaccine.
Here is the convoluted license-plus-authorization letter from FDA. This could be a bait and switch–see the next post.
21,766 Dead Over 2 Million Injured (50% Serious): EU’s Database of Adverse Reactions for COVID-19 Shots
By Brian Shilhavy | Health Impact News | August 18, 2021
The European Union database of suspected drug reaction reports is EudraVigilance, and they are now reporting 21,766 fatalities, and 2,074,410 injuries, following COVID-19 injections.
A Health Impact News subscriber from Europe reminded us that this database maintained at EudraVigilance is only for countries in Europe who are part of the European Union (EU), which comprises 27 countries.
The total number of countries in Europe is much higher, almost twice as many, numbering around 50. (There are some differences of opinion as to which countries are technically part of Europe.)
So as high as these numbers are, they do NOT reflect all of Europe. The actual number in Europe who are reported dead or injured due to COVID-19 shots would be much higher than what we are reporting here.
The EudraVigilance database reports that through August 14, 2021 there are 21,766 deaths and 2,074,410 injuries reported following injections of four experimental COVID-19 shots:
- COVID-19 MRNA VACCINE MODERNA (CX-024414)
- COVID-19 MRNA VACCINE PFIZER-BIONTECH
- COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19)
- COVID-19 VACCINE JANSSEN (AD26.COV2.S)
From the total of injuries recorded, half of them (1,021,867 ) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through August 14, 2021.
Total reactions for the experimental mRNA vaccine Tozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer – 10,616 deaths and 833,498 injuries to 14/08/2021
- 22,844 Blood and lymphatic system disorders incl. 135 deaths
- 22,132 Cardiac disorders incl. 1,591 deaths
- 208 Congenital, familial and genetic disorders incl. 16 deaths
- 10,953 Ear and labyrinth disorders incl. 8 deaths
- 563 Endocrine disorders incl. 5 deaths
- 12,887 Eye disorders incl. 24 deaths
- 75,021 Gastrointestinal disorders incl. 454 deaths
- 220,575 General disorders and administration site conditions incl. 3,013 deaths
- 893 Hepatobiliary disorders incl. 49 deaths
- 9,094 Immune system disorders incl. 58 deaths
- 27,018 Infections and infestations incl. 1037 deaths
- 10,454 Injury, poisoning and procedural complications incl. 158 deaths
- 20,892 Investigations incl. 342 deaths
- 6,172 Metabolism and nutrition disorders incl. 188 deaths
- 112,364 Musculoskeletal and connective tissue disorders incl. 133 deaths
- 605 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 51 deaths
- 148,477 Nervous system disorders incl. 1,171 deaths
- 910 Pregnancy, puerperium and perinatal conditions incl. 29 deaths
- 152 Product issues incl. 1 death
- 14,950 Psychiatric disorders incl. 141 deaths
- 2,763 Renal and urinary disorders incl. 169 deaths
- 10,909 Reproductive system and breast disorders incl. 3 deaths
- 36,913 Respiratory, thoracic and mediastinal disorders incl. 1,268 deaths
- 40,358 Skin and subcutaneous tissue disorders incl. 92 deaths
- 1,416 Social circumstances incl. 13 deaths
- 651 Surgical and medical procedures incl. 28 deaths
- 23,324 Vascular disorders incl. 439 deaths
Total reactions for the experimental mRNA vaccine mRNA-1273 (CX-024414) from Moderna – 5,600 deaths and 229,430 injuries to 14/08/2021
- 4,341 Blood and lymphatic system disorders incl. 49 deaths
- 6,744 Cardiac disorders incl. 614 deaths
- 89 Congenital, familial and genetic disorders incl. 1 deaths
- 2,916 Ear and labyrinth disorders
- 179 Endocrine disorders incl. 1 death
- 3,579 Eye disorders incl. 13 deaths
- 20,063 Gastrointestinal disorders incl. 205 deaths
- 61,894 General disorders and administration site conditions incl. 2,232 deaths
- 372 Hepatobiliary disorders incl. 20 deaths
- 1,926 Immune system disorders incl. 10 deaths
- 6,597 Infections and infestations incl. 340 deaths
- 4,944 Injury, poisoning and procedural complications incl. 105 deaths
- 4,556 Investigations incl. 107 deaths
- 2,230 Metabolism and nutrition disorders incl. 129 deaths
- 28,909 Musculoskeletal and connective tissue disorders incl. 111 deaths
- 275 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 29 deaths
- 40,922 Nervous system disorders incl. 572 deaths
- 463 Pregnancy, puerperium and perinatal conditions incl. 5 deaths
- 46 Product issues
- 4,510 Psychiatric disorders incl. 96 deaths
- 1,364 Renal and urinary disorders incl. 93 deaths
- 2,012 Reproductive system and breast disorders incl. 2 deaths
- 10,046 Respiratory, thoracic and mediastinal disorders incl. 528 deaths
- 12,375 Skin and subcutaneous tissue disorders incl. 47 deaths
- 966 Social circumstances incl. 20 deaths
- 732 Surgical and medical procedures incl. 56 deaths
- 6,380 Vascular disorders incl. 215 deaths
Total reactions for the experimental vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/ AstraZeneca: 4,740 deaths and 947,675 injuries to 14/08/2021
- 11,297 Blood and lymphatic system disorders incl. 194 deaths
- 15,757 Cardiac disorders incl. 550 deaths
- 137 Congenital familial and genetic disorders incl. 3 deaths
- 11,013 Ear and labyrinth disorders
- 457 Endocrine disorders incl. 4 deaths
- 16,608 Eye disorders incl. 19 deaths
- 93,703 Gastrointestinal disorders incl. 241 deaths
- 249,973 General disorders and administration site conditions incl. 1,166 deaths
- 770 Hepatobiliary disorders incl. 44 deaths
- 3,770 Immune system disorders incl. 19 deaths
- 23,056 Infections and infestations incl. 298 deaths
- 10,571 Injury poisoning and procedural complications incl. 130 deaths
- 20,678 Investigations incl. 108 deaths
- 11,336 Metabolism and nutrition disorders incl. 65 deaths
- 144,069 Musculoskeletal and connective tissue disorders incl. 66 deaths
- 477 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 15 deaths
- 198,450 Nervous system disorders incl. 755 deaths
- 391 Pregnancy puerperium and perinatal conditions incl. 9 deaths
- 146 Product issues incl. 1 death
- 17,784 Psychiatric disorders incl. 40 deaths
- 3,449 Renal and urinary disorders incl. 45 deaths
- 12,080 Reproductive system and breast disorders incl. 1 death
- 33,058 Respiratory thoracic and mediastinal disorders incl. 560 deaths
- 43,592 Skin and subcutaneous tissue disorders incl. 31 deaths
- 1,182 Social circumstances incl. 6 deaths
- 1,040 Surgical and medical procedures incl. 21 deaths
- 22,831 Vascular disorders incl. 349 deaths
Total reactions for the experimental COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: – 810 deaths and 63,807 injuries to 14/08/2021
- 585 Blood and lymphatic system disorders incl. 24 deaths
- 988 Cardiac disorders incl. 103 deaths
- 24 Congenital, familial and genetic disorders
- 425 Ear and labyrinth disorders
- 27 Endocrine disorders incl. 1 death
- 836 Eye disorders incl. 3 deaths
- 6,041 Gastrointestinal disorders incl. 28 deaths
- 16,787 General disorders and administration site conditions incl. 201 deaths
- 80 Hepatobiliary disorders incl. 7 deaths
- 260 Immune system disorders incl. 5 deaths
- 1,086 Infections and infestations incl. 27 deaths
- 578 Injury, poisoning and procedural complications incl. 11 deaths
- 3,319 Investigations incl. 56 deaths
- 341 Metabolism and nutrition disorders incl. 13 deaths
- 10,533 Musculoskeletal and connective tissue disorders incl. 19 deaths
- 26 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 2 deaths
- 13,528 Nervous system disorders incl. 101 deaths
- 23 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 19 Product issues
- 794 Psychiatric disorders incl. 9 deaths
- 230 Renal and urinary disorders incl. 9 deaths
- 484 Reproductive system and breast disorders incl. 3 deaths
- 2,155 Respiratory, thoracic and mediastinal disorders incl. 64 deaths
- 1,893 Skin and subcutaneous tissue disorders incl. 3 deaths
- 164 Social circumstances incl. 3 deaths
- 490 Surgical and medical procedures incl. 31 deaths
- 2,091 Vascular disorders incl. 86 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
More COVID Shots on the Way
In spite of all these recorded injuries and deaths, most countries around the world are now preparing to roll out a 3rd Pfizer “booster” shot, as well as authorizing the COVID shots for young children, under the age of 12.
While the alleged COVID-19 “virus” has almost NO impact on deaths among young people, tragically, we cannot say the same for the experimental shots.
This Week in the New Normal #3
OffGuardian | August 22, 2021
1. UNIVERSITIES PUNISHING UNVACCINATED STUDENTS
Universities in the United States are issuing fines to any students who refused to take the Covid “vaccine”, according to a report from Zero Hedge.
West Virginia Wesleyan College, announced a few weeks ago that it will fine any unvaccinated student $750. Whilst Connecticut-based Quinnipiac University will fine them $100 per week increasing in $25 increments (equal to $2250 for the first semester).
Not only that, but unvaccinated students will also be denied internet access. In the modern age, attempting to function in an academic institution without access to the internet, emails or digital learning resources is almost impossible. So this is essentially a mandate under any other name.
Some bigger colleges have already started putting full-on mandates in place.
Other campuses are instituting “testing fees” of over $1500, but only for the unvaccinated. This is in spite of the fact vaccinated people are capable of testing positive for Covid.
2. “THE GREAT JOBS RESET”
The World Economic Forum (WEF) is the big daddy when it comes to pushing out the Great Reset, it’s the brainchild of their Chairman Klaus Schwab after all, and this past week they have unveiled their latest project. It’s called the “Jobs Reset Summit”.
The summit discusses, among other things, the alleged “impact of the pandemic” on employment. Bemoaning the loss of an estimated 255 million full-time jobs from the global economy, without ever mentioning (naturally) that these job losses had nothing to do with Covid, and everything to do with lockdown policies which were never intended to stop the spread of any virus.
The most alarming position to come out of this summit, however, was definitely a tweet that stated:
Get your COVID-19 jab – or you could face consequences from your employer #COVID19 #JobsReset21
Clearly supporting the idea that unvaccinated people should face censure, or even termination, from their employers. Just like they did with their “You’ll own nothing and be happy” article, they deleted the tweet and re-titled the article after a somewhat negative reaction.
Fortunately, once something is on the internet, it’s there forever.
3. YET MORE CASHLESS SOCIETY BS
The march toward a cashless society continues apace. We’ve been told already that cash is bad for the environment, and also contaminated with germs and drugs. Now the press is simply treating the cashless future as a fait acompli
This week alone there are articles about how Brazil, and India, and Saudi Arabia will all be cashless in the near future. China isn’t far behind.
Forgettable Guardian columnists are writing faux nostalgia puff-pieces about missing cash when it’s gone. Parishes are ditching collection plates for QR codes.
It seems the argument phase is over, definitely over. And what brought that on? Well Covid, of course. Multiple publications have been more than clear that the “pandemic” produced a “the viral spread of cashless society” and that a “cashless society is closer thanks to corona”.
It seems the totally real (and not-at-all agenda-driven) pandemic has accidentally facilitated the rise of a highly controlling government policy, which was around years before “Covid” even existed.
Weird how many times that’s happened in the last 18 months.
4. NO TRANSPLANTS FOR THE UNVAXXED
This week hospitals in both the USA and Ireland have admitted to removing unvaccinated patients from the donor organ waiting list.
Beaumont Hospital in Ireland sent out letters recommending doctors remove all unvaccinated patients from the kidney transplant waiting list. Whilst a man in Washington state was told he would not be considered for a heart transplant as long as he declined the Covid jab. Other patients in the same hospital, the University of Washington Medical Center, are reportedly in the same position.
The good news is that the public outcry was so intense, that the Beaumont hospital was forced to reverse its decision within days of the story breaking. But this policy will not go away, and just become more covert as it spreads.
BONUS: CREEPY SPEECH OF THE WEEK
Whoever runs the corporate puppet that lives inside Justin Trudeau’s skin has clearly decided it’s time for him to shake his rather inneffectual image and try and become a forceful public speaker. In a “strongman” speech in the run-up to the Canadian elections, Trudeau worked himself into a frenzy on vaccination:
“If you don’t want to get vaccinated, that’s your choice. But don’t think you can get on a plane or a train beside vaccinated people and put them at risk!”
A tip for the future though – if you’re going to have the blandest man in the world try and excite a crowd, give him more than 80 people to work with. That said, however poorly delivered and however lukewarm the reception, the sentiment itself is very unsettling. Full on segregation in Canada. As someone remarked to us on Telegram, “instead of the back of the bus, it’s now no bus at all.”
IT’S NOT ALL BAD…
We’ve got the usual protests in France, Australia and all over the world to report this week. It’s also in the news that Denmark will be abandoning all Coronavirus measures from October first… but whether that’s truly good news remains to be seen.
However, this week’s main entry for INAB comes in the form of a music video that tells the whole story:
You can follow Lukas Lion on youtube or Instagram, and stream the song on Spotify, Apple music and other platforms.
We’d also remind everyone in the UK that next Saturday, the 28th August, is the Unite for Freedom “Freedom Carnival” protest in London (and maybe other cities around the country). You can also follow their telegram channel for updates.
***
All told a pretty hectic week for the new normal crowd, and we didn’t even mention the Department of Homeland Security and Council on Foreign Relations dialling up the “terrorism threat”, or Australia’s new “national resilience centre”.
The Vapor, the Hot Hat, & the Witches’ Potion

By Margaret Anna Alice | Through The Looking Glass | August 3, 2021
Once upon a time in a prosperous land, a rumor swept across the kingdom that there was an invisible vapor floating through the air. Many vapors had come before, but this one was so extraordinary, it called for an extraordinary response.
This vapor, the town criers cried, could kill you at any time, anywhere. You could get it by talking, breathing, or singing. You could get it by standing or walking too closely to someone. You could even get it by playing. And the scariest thing of all—you could get it and not even know you had it.
The only way to escape was to hide indoors, keep away from people, and rub your hands with a clear jelly every time you touched something. Merchants stopped trading, apprentices stopped learning, and people stopped seeing people.

Every day, the town criers yelled out the number of people who had caught the vapor, although most didn’t know it since they felt the same as usual—just a lot more scared. They only learned they had it because of a certain spell a sorcerer had written down before the vapor came. The sorcerer had said it wasn’t supposed to be cast for vapors and couldn’t tell people if they had caught a vapor or not. But the sorcerer had died, and the king’s counselors decided to cast the spell, anyway, and that is how people found out they had the vapor.
The town criers shouted the latest death tolls so often their voices grew hoarse. Almost every one who died was very, very old or very, very sick or very, very fat. Hardly anyone else died, and at the end of the year, it would turn out about the same number had died as had in other years.

Still, it was a very scary vapor, and the entire kingdom had to change for the good of the public. The land was no longer prosperous, but the king just minted more coins and tossed them out to his subjects so they wouldn’t notice right away.
Eventually, people were told they could come out of hiding and the marketplace could open back up if everyone followed a few rules. They had to wear a hot, scratchy hat that covered their ears and eyes so the vapor couldn’t get into their earholes or eyeholes. They had to hop five times forward and five times backward if they accidentally got too close to another person. And, of course, they had to rub their hands with jelly after touching anything.

Some people thought the hats looked silly and were even a little dangerous since they made it hard for them to hear and see and made them sweat in the summer. The hopping took so much time, people weren’t able to get much done. When those people didn’t wear the hats or hop around, the rest of the people got very, very angry and said it was their fault people were dying and getting sick and couldn’t live the way they used to live. Some even took to wearing two or more hats for extra protection against the anti-hatters and anti-hoppers.

Every so often, the king would tell people to hide back inside again because too many people were catching the vapor. They couldn’t work or shop or visit people they loved. There wasn’t much to do besides lie around listening to the town criers, who always let people know how scared and angry and resentful they should all feel, especially toward the anti-hatters and anti-hoppers.
Suddenly, people started feeling more hopeful. A few witches who were richer than all the world’s kingdoms and queendoms combined offered to make a potion people would need to swallow every so often to keep them safe from the vapor—but it would only work if everyone drank it together.

It took a few months, but eventually the witches each had their own flavor—grape and orange and tropical punch—and they were ready to pour them into people’s mouths. Whenever potions had been made in the past, the witches had had to spend years and years making sure it was safe before giving it to people. This time, though, the vapor was so scary, they skipped all those steps so people could be saved sooner. They even got the king to issue a special decree so no one could hurt the witches if anything bad happened to them after drinking the potion. The king gathered three-quarters of the coins he had collected from the people that year and presented them to the witches.

Almost everybody couldn’t wait to drink the grape or orange or tropical punch potion. They bragged about going to get it and told everyone after they got their first and second drinks. When they came across someone who didn’t want to drink it, they got very, very cross. The town criers told everyone to yell at the anti-drinkers because it was their fault they couldn’t go back to life like it was before the vapor.
Something strange happened after people started drinking the potion. Some of them caught the vapor, anyway, but that was because it was a version of the vapor the witches hadn’t planned for—still, it was important to drink both doses of the potion because it was better than not drinking them. To be safe, though, the town criers said they should go back to wearing hot hats and hopping—although most hadn’t stopped to begin with because they were afraid of what would happen if they did (or worse, they might be mistaken for an anti-hatter, anti-hopper, or anti-drinker).

Even stranger, some of the people who had drunk the potion died either right after or not long after drinking it. Unlike the people who died from the vapor, these people were often very, very young or very, very healthy or very, very fit. The town criers never shouted about these deaths. If anyone brought it up, they called them an anti-hatter, anti-hopper, and anti-drinker.
Being an anti-drinker was the worst of all because everyone knows you need to drink to survive. If you’re against drinking the potion, you must surely be against drinking water, too, and we all know you can’t live without drinking water.
Not everyone who drank the potion died. Some just had peculiar things happen to their bodies. They shook all the time or got rare diseases or noticed parts of their bodies stopped working. They were bedridden or lame or hurt in different ways and couldn’t live the way they did before or even after the vapor. The town criers didn’t tell anyone about these people, either.

And then there were the drinkers who felt perfectly fine … for now. The potion had never been tried for longer than a few months, so no one was really sure what would happen in the next year or two or longer. It was also a different kind of potion than anyone had ever drunk before. This potion changed something inside you that could never be undone. People would also need to drink new versions of the potion every few months, and the king would need to continue giving three-quarters of the kingdom’s coins to the witches forever, or at least as long as the kingdom existed.

All the surviving drinkers were grateful to the witches and thanked them for saving their lives. They proudly displayed a mark on their chin that meant they’d drunk the potion. The ones who’d drunk it twice had two marks.
Those who didn’t have any marks were to blame for the kingdom’s problems. They weren’t permitted to shop in the marketplace or work or apprentice or take part in any public activities. They were shamed and shunned for being a threat to the people of the land. These people started to feel like they should leave the kingdom, but they weren’t allowed to travel without the double marks, and besides, all the other kingdoms and queendoms were the same as theirs, anyway. There wasn’t anyplace left where people weren’t afraid of the vapor and where they didn’t demand that everyone drink the potion.
Soon, the king decided the anti-drinkers were so dangerous, they would need to be locked in a dungeon until they agreed to drink the potion. They were free to choose whichever flavor they liked. If they decided not to drink, they would simply remain in the dungeon. It was entirely up to them.

One year passed, and then another. There were fewer and fewer people left in the kingdom. Eventually, so few people were left, the king could no longer collect enough coins to pay the witches. The rest of the kingdoms and queendoms around the world were in the same fix. They decided to join together into one king-queendom so they could collect enough coins to buy the potion.
After eight more years passed, there weren’t enough people left in all the world to cover the witches’ dues. The rulers decided everything that belonged to the people now belonged to the king-queendom. The people could still live in their hovels, but they wouldn’t own anything. They could earn their keep through labor—indeed, they might be put to work making the potion!

People no longer needed to decide what they wanted to do or be in life because the king-queendom would decide for them. People didn’t need to pay for anything because all the subjects got equally small amounts of the necessities. Everyone looked the same, acted the same, and thought the same.
Most people didn’t remember what it was like before the vapor. Some didn’t even know there was such a time.
The rulers, on the other hand, never wanted for anything. Nor did their friends, the town criers. The witches were the wealthiest of all—and deservedly so, as they had saved the world from the deadly vapor.

It wasn’t long before there were no more subjects. The rulers, the counselors, the town criers, and the witches had all the earth’s riches to themselves, and they lived happily ever after.
If you liked this post from Margaret Anna Alice Through the Looking Glass, why not share it? You can also Buy Me a Coffee, donate via PayPal,
© Margaret Anna Alice, LLC
Is Natural Immunity More Effective Than the COVID Shot?
By Dr. Joseph Mercola | August 18, 2021
According to Centers for Disease Control and Prevention data,1 COVID-19 “cases” have trended downward since peaking during the first and second week of January 2021.
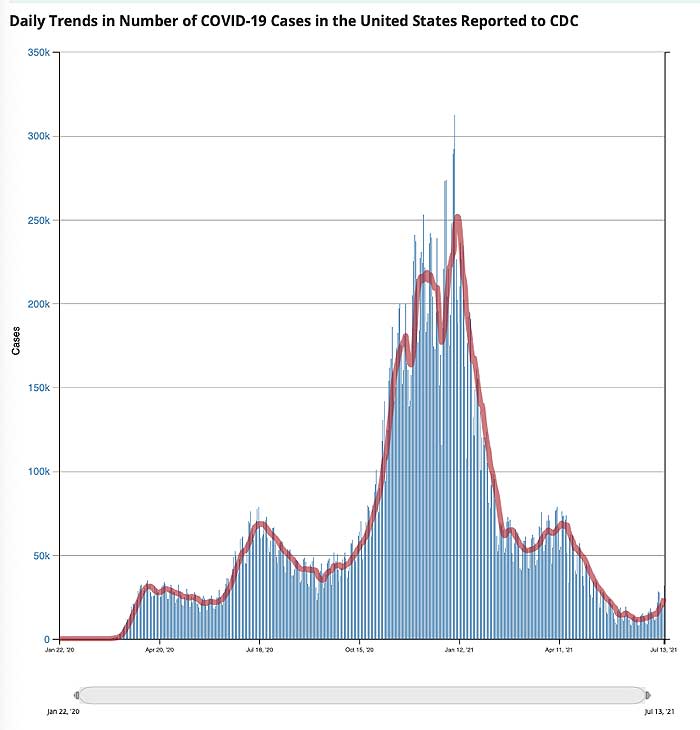
At first glance, this decline appears to be occurring in tandem with the rollout of COVID shots. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,2 and as of July 13, 48.3% were fully “vaccinated.”3
However, as noted in a July 12, 2021, STAT News article,4 “cases” had started their downward trend before COVID shots were widely used. “Following patterns from previous pandemics, the precipitous decline in new cases of Covid-19 started well before a meaningful number of people had been vaccinated,” Robert M. Kaplan, Professor Emeritus at the UCLA Fielding School of Public Health, writes. He continues:
“Nearly 50 years ago, medical sociologists John and Sonja McKinlay examined5 death rates from 10 serious diseases: tuberculosis, scarlet fever, influenzae, pneumonia, diphtheria, whooping cough, measles, smallpox, typhoid, and polio. In each case, the new therapy or vaccine credited with overcoming it was introduced well after the disease was in decline.
More recently, historian Thomas McKeown noted6 that deaths from bronchitis, pneumonia, and influenza had begun rapidly falling 35 years before the introduction of new medicines that were credited with their conquest. These historical analyses are relevant to the current pandemic.”
‘Case’ Decline Preceded Widespread Implementation of Jab
As noted by Kaplan, COVID-19 “cases” peaked in early January 2021. January 8, more than 300,000 new positive test results were recorded on a daily basis. By February 21, that had declined to a daily new case count of 55,000. COVID-19 gene modification injections were granted emergency use authorization at the end of December 2020, but by February 21, only 5.9% of American adults had been fully vaccinated with two doses.
Despite such a low vaccination rate, new “cases” had declined by 82%. Considering health authorities claim we need 70% of Americans vaccinated in order to achieve herd immunity and stop the spread of this virus, this simply makes no sense. Clearly, the COVID shots had nothing to do with the decline in positive test results.
To be clear, reported cases mean positive test results, and we now know the vast majority of positive PCR tests have been, and still are, false positives. They’re not sick. They simply had a false “positive.” Right now, we’re also faced with yet another situation that complicates attempts at data analysis, and Kaplan understandably did not address any of these confounding factors.
But just so you’re aware, if you have been fully “vaccinated,” then the CDC recommends running the PCR test at a cycle threshold (CT) of 28 or lower, which dramatically lowers your chance of a false positive result, but if you are unvaccinated, the PCR test is recommended to be run at a CT of 40 or higher, virtually guaranteeing a false positive.
This is just one way by which the CDC is manipulating data to make the COVID shots appear more effective than they are. This also allows them to falsely claim that the vast majority of new cases are among the unvaccinated.
Naturally, if unvaccinated are tested in such a way as to maximize false positives, then they’re going to make up the bulk of the so-called caseload. In reality, though, the vast majority of them aren’t sick.
Meanwhile, those who have received the jabs only count as a COVID case if they’re hospitalized and/or die with a positive test result. These widely differing testing strategies skew the data and allow for false interpretations to be made.
Natural Immunity Explains Decline in Cases
As noted by Kaplan, the most reasonable explanation for declining rates of SARS-CoV-2 appears to be natural immunity from previous infections, which vary considerably from state to state.7 He goes on to cite a study8 by the National Institutes of Health, which suggests SARS-CoV-2 prevalence was 4.8 times higher than previously thought, thanks to undiagnosed infection.
In other words, they claim that for every reported positive test result, there were likely nearly five additional people who had the infection but didn’t get a diagnosis. To analyze this data further, Kaplan calculated the natural immunity rate by dividing the new estimated number of people naturally infected by the population of any given state. He writes:9
“By mid-February 2021, an estimated 150 million people in the U.S. (30 million times five) may have had been infected with SARS-CoV-2. By April, I estimated the natural immunity rate to be above 55% in 10 states: Arizona, Iowa, Nebraska, North Dakota, Oklahoma, Rhode Island, South Dakota, Tennessee, Utah, and Wisconsin.
At the other end of the continuum, I estimated the natural immunity rate to be below 35% in the District of Columbia, Hawaii, Maine, Maryland, New Hampshire, Oregon, Puerto Rico, Vermont, Virginia, and Washington …
By the end of 2020, new infections were already rapidly declining in nearly all of the 10 states where the majority may have had natural immunity, well before more than a minuscule percentage of Americans were fully vaccinated. In 80% of these states, the day when new cases were at their peak occurred before vaccines were available.
In contrast, the 10 states with lower rates of previous infections were much more likely to experience new upticks in Covid-19 cases in March and April … By the end of May, states with fewer new infections had significantly lower vaccination rates than states with more new infections.”
COVID Shots Cannot Eliminate COVID-19
So, SARS-CoV-2 cases were actually higher in states where natural immunity was low but vaccination rates were high. Meanwhile, in states where natural immunity due to undiagnosed exposure was high, but vaccination rates were low, the daily new caseload was also lower.
This makes sense if natural immunity is highly effective (which, historically it has always been and there’s no reason to suspect SARS-CoV-2 is any different in that regard). It also makes sense if the COVID shots aren’t really offering any significant protection against infection, which we also know is the case.
Vaccine manufacturers have already admitted these COVID shots will not provide immunity, meaning they will not prevent you from being infected. The idea behind these gene modification injections is that if/when you do get infected, you’ll hopefully experience milder symptoms, even though you’re still infectious and can spread the virus to others.
Kaplan ends his analysis by saying that COVID shots are a safer way to achieve herd immunity, and that they are “the best tool available for assuring that the smoldering fire of [COVID-19] is extinguished.” I disagree, based on two major issues.
First, and perhaps most importantly, this is an untested “vaccine” and we have no idea of the short-term let alone long-term damage it will cause, as any reasonable effort at collecting this data has been actively suppressed. Secondly, the survivability of COVID-19 outside of nursing homes is 99.74%. If you’re under the age of 40, your chance of surviving a bout of COVID-19 is 99.99%.10,11,12
You can’t really improve your chances of surviving beyond that, so COVID shots cannot realistically end the pandemic. Meanwhile, the COVID shots come with an ever-growing list of potential side effects that can take years if not decades off your natural life span. The shots are particularly unnecessary for anyone with natural immunity,13 yet that’s what the CDC recommends.14
Why Push COVID Jab on Those with Natural Immunity?
In January 2021, Dr. Hooman Noorchashm, a cardiac surgeon and patient advocate, sent a public letter15 to the U.S. Food and Drug Administration commissioner detailing the risks of vaccinating individuals who have previously been infected with SARS-CoV-2, or who have an active SARS-CoV-2 infection.
He urged the FDA to require prescreening for SARS-CoV-2 viral proteins to reduce the risk of injuries and deaths following vaccination, as the vaccine may trigger an adverse immune response in those who have already been infected with the virus. In March 2021, Fox TV host Tucker Carlson interviewed him about these risks. In that interview, Noorchashm said:16
“I think it’s a dramatic error on part of public health officials to try to put this vaccine into a one-size-fits-all paradigm … We’re going to take this problem we have with the COVID-19 pandemic, where a half-percent of the population is susceptible to dying, and compound it by causing totally avoidable harm by vaccinating people who are already infected …
The signal is deafening, the people who are having complications or adverse events are the people who have recently or are currently or previously infected [with COVID]. I don’t think we can ignore this.”
In an email to The Defender, Noorchashm fleshed out his concerns, saying:17
“Viral antigens persist in the tissues of the naturally infected for months. When the vaccine is used too early after a natural infection, or worse during an active infection, the vaccine force activates a powerful immune response that attacks the tissues where the natural viral antigens are persisting. This, I suggest, is the cause of the high level of adverse events and, likely deaths, we are seeing in the recently infected following vaccination.”
Despite being widely ignored, Noorchashm continues to push for the implementation of prevaccine screening using PCR or rapid antigen testing to determine whether the individual has an active infection, and an IgG antibody test to determine past infection.
If either test is positive, he recommends delaying vaccination for a minimum of three to six months to allow your IgG levels to wane. At that point, he recommends testing your blood IgG level and use that as a guide to decide the timing of your vaccination.
Those with Natural Immunity Have Higher Risk of Side Effects
Mere weeks after Noorchashm’s letter to the FDA, an international survey18 confirmed his concerns. After surveying 2,002 people who had received a first dose of COVID-19 vaccine, they found that those who had previously had COVID-19 experienced “significantly increased incidence and severity” of side effects, compared to those who did not have natural immunity.
The mRNA COVID-19 vaccines were linked to a higher incidence of side effects compared to the viral vector-based COVID-19 vaccines, but tended to be milder, local reactions. Systemic reactions, such as anaphylaxis, flu-like illness and breathlessness, were more likely to occur with the viral vector COVID-19 vaccines.
Like Noorchashm before them, the researchers called on health officials to reevaluate their vaccination recommendations for people who’ve had COVID-19:19
“People with prior COVID-19 exposure were largely excluded from the vaccine trials and, as a result, the safety and reactogenicity of the vaccines in this population have not been previously fully evaluated. For the first time, this study demonstrates a significant association between prior COVID19 infection and a significantly higher incidence and severity of self-reported side effects after vaccination for COVID-19.
Consistently, compared to the first dose of the vaccine, we found an increased incidence and severity of self-reported side effects after the second dose, when recipients had been previously exposed to viral antigen.
In view of the rapidly accumulating data demonstrating that COVID-19 survivors generally have adequate natural immunity for at least 6 months, it may be appropriate to re-evaluate the recommendation for immediate vaccination of this group.”
CDC Misrepresents Data to Push Jab on Those with Immunity
So far, the CDC has refused to change its stance on the matter. Instead, officials at the agency seem to have doubled down and actually go out of their way to misrepresent data in an effort to harass those with natural immunity to inappropriately take the jab, which is clearly clinically unnecessary.
In a report issued by the CDC’s Advisory Committee on Immunization Practices (ACIP) December 18, 2020, the Pfizer-BioNTech COVID-19 vaccine was said to have “consistent high efficacy” of 92% or more among people with evidence of previous SARS-CoV-2 infection.20
After looking at the Pfizer trial data, Rep. Thomas Massie — a Republican Congressman for Kentucky and an award-winning scientist in his own right — discovered that’s completely wrong. In a January 30, 2021, Full Measure report, investigative journalist Sharyl Attkisson described how Massie tried, in vain, to get the CDC to correct its error. According to Massie:21,22
“There is no efficacy demonstrated in the Pfizer trial among participants with evidence of previous SARS-CoV-2 infections and actually there’s no proof in the Moderna trial either …
It [the CDC report] says the exact opposite of what the data says. They’re giving people the impression that this vaccine will save your life, or save you from suffering, even if you’ve already had the virus and recovered, which has not been demonstrated in either the Pfizer or the Moderna trial.”
After multiple phone calls, CDC deputy director Dr. Anne Schuchat finally acknowledged the error and told Massie it would be fixed. “As you note correctly, there is not sufficient analysis to show that in the subset of only the people with prior infection, there’s efficacy. So, you’re correct that that sentence is wrong and that we need to make a correction of it,” Schuchat said in the recorded call.
January 29, 2021, the CDC issued its supposed correction, but rather than fix the error, they simply rephrased the mistake in a different way. This was the “correction” they issued:
“Consistent high efficacy (≥92%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions. Efficacy was similarly high in a secondary analysis including participants both with or without evidence of previous SARS-CoV-2 infection.”
As you can see, the “correction” still misleadingly suggests that vaccination is effective for those previously infected, even though the data showed no such thing. Children of ever-younger ages are also being pushed to get the COVID jab, even though they have the absolute lowest risk of dying from COVID-19 of any group.
Data23 from the first 12 months of the pandemic in the U.K. show just 25 people under the age of 18 died from or with COVID-19.24 In all, 251 children under 18 were admitted to intensive care between March 2020 and February 2021. The absolute risk of death from COVID-19 in children is 2 in 1 million.
Vaccine Provides Far Less Protection Than Natural Immunity
While some claim vaccine-induced immunity offers greater protection against SARS-CoV-2 infection than natural immunity, historical and current real-world data simply fail to support this non-common sense assertion.
As recently reported by Attkisson25,26 and David Rosenberg 7 Israeli National News,27 recent Israeli data show those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection.
Among the 7,700 new COVID cases diagnosed so far during the current wave of infections that began in May 2021, 39% were vaccinated (about 3,000 cases), 1% (72 patients) had recovered from a previous SARS-CoV-2 infection and 60% were neither vaccinated nor previously infected. Israeli National News notes:28
“With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.”
Breakthrough Infections Are on the Rise
Other Israeli data also suggest the limited protection offered by the COVID shot is rapidly eroding. August 1, 2021, director of Israel’s Public Health Services, Dr. Sharon Alroy-Preis, announced half of all COVID-19 infections were among the fully vaccinated.29 Signs of more serious disease among fully vaccinated are also emerging, she said, particularly in those over the age of 60.
Even worse, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID-related hospitalizations overall.30
Other areas where a clear majority of residents have been vaccinated are also seeing spikes in breakthrough cases. In Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.31
US Outbreak Shatters ‘Pandemic of Unvaccinated’ Narrative
An investigation by the CDC32,33 also dispels the narrative that we’re in a “pandemic of the unvaccinated.” An outbreak in Barnstable County, Massachusetts, resulted in 469 new COVID cases among residents who had traveled into town between July 3 and July 17, 2021.
Of these cases, 74% were fully vaccinated, as were 80% of those requiring hospitalization.Most, but not all, had the Delta variant of the virus. The CDC also found that fully vaccinated individuals who contract the infection had as high a viral load in their nasal passages as unvaccinated individuals who got infected.34 This means the vaccinated are just as infectious as the unvaccinated. According to Attkisson:35
“CDC’s newest findings on so-called ‘breakthrough’ infections in vaccinated people are mirrored by other data releases. Illinois health officials recently announced36 more than 160 fully-vaccinated people have died of Covid-19, and at least 644 been hospitalized; 10 deaths and 51 hospitalizations counted in the prior week …
In July, New Jersey reported 49 fully vaccinated residents had died of Covid; 27 in Louisiana; 80 in Massachusetts … Nationally, as of July 12, CDC said it was aware of more than 4,400 people who got Covid-19 after being fully vaccinated and had to be hospitalized; and 1,063 fully vaccinated people who died of Covid.”
It is important to note this data is over 1 month old now and it is likely that many thousands of fully “vaccinated” have now died from COVID-19.
Natural Immunity Appears Robust and Long-Lasting
An argument we’re starting to hear more of now is that even though natural immunity after recovery from infection appears to be quite good, “we don’t know how long it’ll last.” This is rather disingenuous, seeing how natural immunity is typically lifelong, and studies have shown natural immunity against SARS-CoV-2 is at bare minimum longer lasting than vaccine-induced immunity.
Here’s a sampling of scholarly publications that have investigated natural immunity as it pertains to SARS-CoV-2 infection. There are several more in addition to these:
Science Immunology October 202038 found that “RBD-targeted antibodies are excellent markers of previous and recent infection, that differential isotype measurements can help distinguish between recent and older infections, and that IgG responses persist over the first few months after infection and are highly correlated with neutralizing antibodies.”
The BMJ January 202139 concluded that “Of 11, 000 health care workers who had proved evidence of infection during the first wave of the pandemic in the U.K. between March and April 2020, none had symptomatic reinfection in the second wave of the virus between October and November 2020.”
Science February 202140 reported that “Substantial immune memory is generated after COVID-19, involving all four major types of immune memory [antibodies, memory B cells, memory CD8+ T cells, and memory CD4+ T cells]. About 95% of subjects retained immune memory at ~6 months after infection. Circulating antibody titers were not predictive of T cell memory.
Thus, simple serological tests for SARS-CoV-2 antibodies do not reflect the richness and durability of immune memory to SARS-CoV-2.” A 2,800-person study found no symptomatic reinfections over a ~118-day window, and a 1,246-person study observed no symptomatic reinfections over 6 months.
A February 2021 study posted on the prepublication server medRxiv41 concluded that “Natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months.”
An April 2021 study posted on medRxiv42 reported “the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94.8%; hospitalization 94.1%; and severe illness 96·4%. Our results question the need to vaccinate previously-infected individuals.”
Another April 2021 study posted on the preprint server BioRxiv43 concluded that “following a typical case of mild COVID-19, SARS-CoV-2-specific CD8+ T cells not only persist but continuously differentiate in a coordinated fashion well into convalescence, into a state characteristic of long-lived, self-renewing memory.”
A May 2020 report in the journal Immunity 44 confirmed that SARS-CoV-2-specific neutralizing antibodies are detected in COVID-19 convalescent subjects, as well as cellular immune responses. Here, they found that neutralizing antibody titers do correlate with the number of virus-specific T cells.
A May 2021 Nature article45 found SARS-CoV-2 infection induces long-lived bone marrow plasma cells, which are a crucial source of protective antibodies. Even after mild infection, anti-SARS-CoV-2 spike protein antibodies were detectable beyond 11 months’ post-infection.
A May 2021 study in E Clinical Medicine 46 found “antibody detection is possible for almost a year post-natural infection of COVID-19.” According to the authors, “Based on current evidence, we hypothesize that antibodies to both S and N-proteins after natural infection may persist for longer than previously thought, thereby providing evidence of sustainability that may influence post-pandemic planning.”
Cure-Hub data47 confirm that while COVID shots can generate higher antibody levels than natural infection, this does not mean vaccine-induced immunity is more protective. Importantly, natural immunity confers much wider protection as your body recognizes all five proteins of the virus and not just one. With the COVID shot, your body only recognizes one of these proteins, the spike protein.
A June 2021 Nature article48 points out that “Wang et al. show that, between 6 and 12 months after infection, the concentration of neutralizing antibodies remains unchanged. That the acute immune reaction extends even beyond six months is suggested by the authors’ analysis of SARS-CoV-2-specific memory B cells in the blood of the convalescent individuals over the course of the year.
These memory B cells continuously enhance the reactivity of their SARS-CoV-2-specific antibodies through a process known as somatic hypermutation. The good news is that the evidence thus far predicts that infection with SARS-CoV-2 induces long-term immunity in most individuals.”
Another June Nature paper concluded that “In the absence of vaccination antibody reactivity [to the receptor binding domain (RBD) of SARS-CoV-2], neutralizing activity and the number of RBD-specific memory B cells remain relatively stable from 6 to 12 months.” According to the authors, the data suggest “immunity in convalescent individuals will be very long lasting.”
What Makes Natural Immunity Superior?
The reason natural immunity is superior to vaccine-induced immunity is because viruses contain five different proteins. The COVID shot induces antibodies against just one of those proteins, the spike protein, and no T cell immunity. When you’re infected with the whole virus, you develop antibodies against all parts of the virus, plus memory T cells.
This also means natural immunity offers better protection against variants, as it recognizes several parts of the virus. If there are significant alternations to the spike protein, as with the Delta variant, vaccine-induced immunity can be evaded. Not so with natural immunity, as the other proteins are still recognized and attacked.
Not only that but the COVID jabs actually actively promote the production of variants for which they provide virtually no protection at all, while those with natural immunity do not cause variants and are nearly universally protected against them.
If we are to depend on vaccine-induced immunity, as public health officials are urging us to do, we’ll end up on a never-ending booster treadmill. Boosters will absolutely be necessary, as the shot offers such narrow protection against a single protein of the virus. Already, Moderna has publicly stated that the need for additional boosters is expected.
Ultimately It’s About Wealth Transfer, Power and Control
Government agencies typically don’t issue recommendations without ulterior motives. Since current recommendations make absolutely no sense from a medical and scientific standpoint, what might the reason be for these illogical and reprehensibly unethical recommendations to inject people who don’t need it with experimental gene modification technology?
Why are they so hell-bent on getting a needle in every arm? And why are they refusing to perform any kind of risk-benefit analysis?
Data already indicate these COVID-19 injections could be the most dangerous medical product we’ve ever seen, and a June 24, 2021, peer-reviewed study published in the medical journal Vaccines warned we are in fact killing nearly as many with the shots as would die from COVID-19 itself.50
Using data from a large Israeli field study and two European drug reactions databases, they recalculated the NNTV for Pfizer’s mRNA shot. To prevent one case of COVID-19, anywhere between 200 and 700 had to be injected. To prevent a single death, the NNTV was between 9,000 and 50,000, with 16,000 as a point estimate.
Meanwhile, the number of people reporting adverse reactions from the shots was 700 per 100,000 vaccinations. For serious side effects, there were 16 reports per 100,000 vaccinations, and the number of fatal side effects was 4.11 per 100,000 vaccinations.
The final calculation suggested that for every three COVID-19 deaths prevented, two died from the shots. “This lack of clear benefit should cause governments to rethink their vaccination policy,” the authors concluded.
As has become the trend, a letter expressing “concern” about the study was published June 28, 2021, resulting in the paper being abruptly retracted July 2, 2021, against the authors’ objections. They disagreed with the accusation that their data and subsequent conclusion were misrepresentative, but the paper was retracted before they had time to publish a rebuttal.
Based on everything we’ve discovered so far, it seems a pandemic virus industrial complex is running the show, with a goal to eliminate medical rights and personal freedoms in order to centralize power, control and wealth.
By the looks of things, the COVID-19 mass psychosis and loss of any rational thinking by nearly half the population will continue to persist as long as the propaganda continues. Fear will continue and if need be, other engineered viruses may be released, for which they’ll create even more gene modification injections.
I believe the truth will eventually be so overwhelming, it’ll sweep away the confusion and the lies.
Sources and References
- 1 COVID.CDC.gov, COVID Cases in the US Reported to the CDC, Viewed July 15, 2021
- 2 Bloomberg COVID Vaccine Tracker, see US Vaccinations vs Cases graph, top portion
- 3 Mayo Clinic COVID Vaccine Tracker
- 4, 7, 9 STAT News July 12, 2021
- 5 Health and Society 1977; 55(3): 405-428
- 6 Population Studies, A Journal of Demography 1975; 29(3): 391-422
- 8 NIH.gov June 22, 2021
- 10 Annals of Internal Medicine September 2, 2020 DOI: 10.7326/M20-5352
- 11 Greek Reporter June 27, 2020
- 12 WFAE.org July 2, 2020
- 13 medRxiv June 1, 2021
- 14 U.S. CDC, COVID-19 Vaccination FAQs April 30, 2021
- 15 Medium February 15, 2021
- 16, 17 The Defender March 23, 2021
- 18 Life 2021; 11(3): 249
- 19 Life 2021; 11(3): 249, Discussion
- 20 MMWR December 18, 2020
- 21 Full Measure After Hours Podcast January 30, 2021
- 22 Full Measure News January 31, 2021
- 23 Research Square July 7, 2021
- 24 BBC July 9, 2021
- 25 Sharylattkisson.com August 8, 2021
- 26, 35 Sharylattkisson.com August 6, 2021
- 27, 28 David Rosenberg 7 July 13, 2021
- 29 Bloomberg August 1, 2021 (Archived)
- 30 American Faith August 8, 2021
- 31 Big League Politics August 4, 2021
- 32 CDC MMWR July 30, 2021; 70
- 33 CNBC July 30, 2021
- 34 NBC News August 7, 2021
- 36 NBC Chicago July 28, 2021
- 37 Reddit COVID-19 and Immunity
- 38 Science Immunology October 8, 2020; 5(52): eabe0367
- 39 BMJ 2021;372:n99
- 40 Science February 5, 2021; 371(6529): eabf4063
- 41 medrxiv February 8, 2021 DOI: 10.1101/2021.01.15.21249731
- 42 medRxiv April 24, 2021 (PDF)
- 43 BioRxiv April 29, 2021 DOI: 10.1101/2021.04.28.441880
- 44 Immunity June 16, 2020; 52(6): 971-977.E3
- 45 Nature 2021; 595: 421-425
- 46 E Clinical Medicine 2021; 36: 100902 (PDF)
- 47 Cure-hub June 11, 2021
- 48 Nature June 14, 2021
- 49 The Hill August 5, 2021
- 50 Vaccines 2021; 9(7): 693
Businesses Are Refusing to Enforce France’s Vaccine Passport
By Paul Joseph Watson | Summit News | August 16, 2021
Anecdotal evidence detailed by former Google software engineer Mike Hearn strongly suggests that most restaurants, cafes and other businesses in France are not enforcing the country’s controversial vaccine passport system.
As we highlighted last week, on the first day the new program was in place, police were visibly patrolling bars and cafes demanding customers show proof they’ve had the jab.
However, this seems to have largely been a bluff as just days later, businesses and venues have become very lax at checking people’s papers despite the threat of large fines.
“I decided to do a simple experiment to find out: always present an expired test even though I had a valid negative one, and see what happens,” writes Hearn.
“Over a four day stay I was required to show a valid pass exactly zero times; that includes at the airports in both directions. Compliance is absolutely min viable and often lower.”
“At small businesses enforcement was non-existent: sometimes the pass requirement was ignored entirely, other times we were asked “do you have a pass” and our answer wasn’t checked. One restaurant had come up with a clever way to detect police stings without requiring customers to actually present a pass. As expected, enforcement was stricter by larger firms, however even there we saw the following:
– Test certificates being checked once and then swapped for a token that doesn’t expire.
– Expired tests being accepted.
– People accepting paper test certificates without scanning them.
– Scanning tests and then not looking at the screen to see the results.
– Accepting QR codes that failed to scan.”
Hearn also reveals how mask mandates in theme parks and other venues are also not being followed, despite signs everywhere ordering people to cover their faces, while social distancing is also a “forgotten memory.”
Images showing empty cafes and bars on the first day the system was introduced may have spooked venues into taking a hands off approach.
In passing the law but failing to ensure that it is enforced, France is following the same model as Israel, where the point of introducing the system wasn’t really to enforce it, but merely as a means of bullying young people into getting the vaccine.
As we highlighted last week, despite the odious and draconian nature of the vaccine passport system, President Macron asserted that the it was actually introduced to protect people’s “freedom,” which is like saying putting you in prison is for your own safety.
Escape from New York: Mayor Decrees Vaccine Mandate for All Businesses, Venues
21st Century Wire | August 17, 2021
New York City is the latest casualty in the current wave of fascism sweeping through the major western countries.
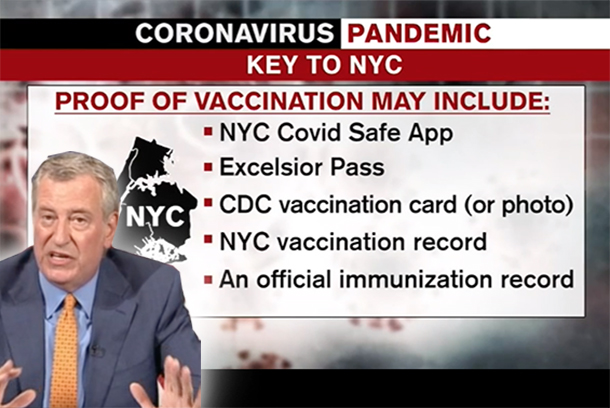
This week, the Mayor of New York declared his to be the first major city in the United States to mandate mandatory vaccines for all indoor facilities and businesses, including all entertainment venues, gyms, pools, indoor dining, cafes, bars, museums, and retail outlets. All of these premises will soon be ‘off-limits’ for any employees and customers who refuse to be injected with the unlicensed experimental GMO ‘vaccine’ gene-jab.
Mayor Bill de Blasio, a Democrat, declared his unprecedented unitary rule over the city, bypassing the normal democratic process by signing an executive order which is said to begin on Tuesday, August 17th with enforcement of his decree coming into full effect on Monday, September 13th.
In true Orwellian fashion, he has named this new medical apartheid regime the “Key to NYC.”
De Blasio is threatening harsh punishments for any resident who defies his executive diktat, with fines starting at $1,000 for failure to comply with his vaccine mandate, and with fines that will increase progressively for repeat offenses. The Mayor has not yet specified whether or not punishments will include arrest and imprisonment for any repeat offenders.
“We made a decision a few weeks ago, the whole ball game is vaccination and once you make that kind of profound strategic decision you throw everything you got at it,” said De Blasio during the press announcement.
Stating he will only accept full compliance from the city’s 8 million residents, he warned, “We’re not interested in half measures.”
The Mayor openly admitted that his decree is especially targeting young people in their 20s and 30s, stating that he intends to coerce them into accepting the experimental COVID injection, as they are the primary target demographic “who needs to be convinced that it’s so powerful to be vaccinated.”
De Blassio went on to say, “New Yorkers, we love our arts, culture, entertainment, restaurants…. knowing that is the way you connect with these things through vaccination – is going to move people to get vaccinated.”
De Blasio then announced he intends to run a multimillion dollar propaganda campaign, paid for by city taxpayers, designed to condition residents to comply with his new executive decree.
Technocrats in the city’s public health coterie also added that they would pursue serious fraud charges against anyone caught using a fake vaccination card.
“A fake vaccination card constitutes fraud and will be prosecuted as fraud by that individual,” said Dr. David Chokshi, NYC Health Commissioner.
Chokshi added that a special line has been set up to report on any residents suspected of faking their proof of vaccination, warning, “We will have recourse for people to report if they are encountering fake vaccination cards, both at the city level through 311 as well as through the state attorney general’s office.”
Businesses and venues will be expected to ask members of the public for both proof of vaccination along with a photo ID ‘to prove they are who they say they are.’ … Full article
Massive fraud in reporting vaccine injuries; withheld data, pretense of “safe and effective”
By Jon Rappoport | No More Fake News | August 17, 2021
ONE: A bombshell. Alex Berenson, former New York Times reporter, August 6: “Covid vaccine maker Moderna received 300,000 reports of side effects after vaccinations over a three-month period following the launch of its shot, according to an internal report from a company that helps Moderna manage the reports.”
“That figure is far higher than the number of side effect reports about Moderna’s vaccine publicly available in the federal system that tracks such adverse events.”
BOOM. 300,000 vaccine adverse effects NOT reported to VAERS, the federal database.
Berenson: “The 300,000 figure comes from an internal update provided to employees by IQVIA, a little-known but enormous company that helps drugmakers manage clinical trials. Headquartered in North Carolina, IQVIA has 74,000 employees worldwide and had $11 billion in sales last year.”
“Earlier this week, Richard Staub, the president of IQVIA’s Research & Development Solutions division, sent a ‘Q2 2021 update’ which was labeled ‘Confidential – For internal distribution only’.”
“A person with access to the presentation provided screenshots of the relevant slide, which clearly explains the 300,000 side effect reports were received over ‘a three-month span’ – not since the introduction of the vaccine in December…”
TWO: Independent researcher Virginia Stoner has issued a stunning new report on the VAERS numbers, and the effort by mainstream scientists to minimize the destructive effects of the COVID vaccines. Here are key quotes from her report:
“More deaths have been reported to VAERS from the covid shots than from all other vaccines combined for the last 30 years.”
“There’s a code of silence shielding the massive increase in deaths (and other serious injuries) reported to VAERS from the covid shots. Not only do CDC web pages and press releases omit that inconvenient fact—vaccine research studies omit it as well.”
“The number of covid shots [in the US] administered so far in 2021 (309 million) is roughly the same as all other vaccines administered in 2020 (316 million). But a shocking 36-times more deaths were reported this year from the covid shots than were reported last year from all other vaccines.”
“Someone died from a vaccine they [a medical provider] administered…could it potentially call their professional judgment into question, or result in a malpractice lawsuit? If you were a doctor, or supervisor at a drive-thru covid vaccination clinic, and you were given a choice between spending the evening filing a VAERS report, or having dinner with friends, which would you choose?”
“There are reasons to think death may be one of the most underreported vaccine injuries of all—mainly because the victim is dead, and can’t file a VAERS report. Nor can they prod their doctor into filing a VAERS report. Unless they’re fortunate enough to have a relative or doctor who knows they got the vaccine, knows about VAERS, understands the potential for vaccine injury, and is willing to go through the onerous process of filing a VAERS report, it won’t happen.”
THREE: Open letter from Doctors for COVID Ethics accusing governments and media of lying to the people:
“Official sources, namely EudraVigilance (EU, EEA, Switzerland), MHRA (UK) and VAERS (USA), have now recorded more Injuries and Deaths from the ‘Covid’ vaccine roll-out than from all previous vaccines combined since records began.”
“TOTAL for EU/UK/USA – 34,052 Covid-19 injection related deaths and over 5.46 million injuries reported as of 1 August 2021.”
“It is important to be aware that the official figures above (reported to the health authorities) are but a small percentage of the actual figures. Furthermore, people continue to die (and suffer injury) from the injections with every day which passes.”
“This catastrophic situation has not been reported by the mainstream media, despite the official figures above being publicly available.”
“The Signal of Harm is now indisputably overwhelming, and, in line with universally accepted ethical standards for clinical trials, Doctors for Covid Ethics demands that the ‘Covid’ vaccine programme be halted immediately.”
“Continuation of the programme in the full knowledge of ongoing serious Harm and Death to both adults and children constitutes a Crime Against Humanity/Genocide for which those found to be responsible or complicit will ultimately be held personally liable.”
“Governments worldwide are lying to you the people, to the populations they purportedly serve.”
“The figures above demonstrate that the mRNA vaccines are deadly.”
FOUR: The well-known 2010 Harvard Pilgrim Health Care, Inc. study of VAERS bluntly stated: “Adverse events from vaccines are common but underreported, with less than one percent reported to the Food and Drug Administration (FDA). Low reporting rates preclude or delay the identification of ‘problem’ vaccines, potentially endangering the health of the public.”
Following the finding of that study, you would multiply the number of reported vaccine injuries by 100 to arrive at a proper figure.
FIVE: In view of the massive number of vaccine injuries and deaths, how would we expect the public to react? Here is a major clue. Stat News, July 21: “Millions of unused Covid-19 vaccines are set to go to waste as demand dwindles across the United States and doses likely expire this summer, according to public health officials…”
“Currently, states have administered 52.36 million fewer doses than have been distributed to them, according to federal data.”
“A significant tranche of Pfizer doses is expected to expire in August… Given waning domestic vaccine demand, those doses are unlikely to be fully used before they must be tossed.”
“’We’re seeing demand [for the vaccine] falling off across all the states,’ said Marcus Plescia, chief medical officer at the Association of State and Territorial Health Officials.”
SIX: Understanding this, government, media, and corporate criminals are ramping up vaccine mandates wherever and however they can, to force the needle into your arm.
“You’re aware that our product is highly dangerous and destructive? We’ll make you take it.”
SEVEN: RESIST. REBEL.
SOURCES:
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
A low-fat, high-carb diet has been the largest public health experiment in history. It’s past time for a rethink.
By Malcolm Kendrick | RT | November 25, 2020
New research suggests that four billion people globally will be overweight in 2050. This trend can be traced back to the ‘low-fat, high-carb’ guidelines first issued in the 70s, and should prompt a major U-turn on dietary advice.
A recent report from the Potsdam Institute predicts that by 2050 there will be four billion overweight people in the world, with one-and-a-half billion of them obese. This is not entirely surprising. The world has been getting fatter for years, and things do not seem to be slowing down.
Why is this happening? … continue
Blog Roll
 Aletho News
Aletho News- OPCW Forced To Pay Damages To Whistleblower Who Found Evidence Of False Flag In Syria
- Iran can thrive under blockade, the US and its allies cannot
- Iran slams US leadership, debunking fabrications, false war costs
- Here’s why Iran is sovereign and Germany is not
- Israel pours $730m into global propaganda machine as reputation collapses
- Leaked audios reveal pro-Israel groups ‘paid’ for US pardon of convicted drug trafficker Juan Orlando Hernandez
- Congress Extends Section 702 Spy Program 45 Days
- Zionists Are Gunning for Your Freedom of Speech
- Larry Johnson: U.S. Desperation Grows as Iran Is Winning
- Why don’t UK media mention the Israel lobby?
- If Americans Knew
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
