Most US & UK businesses to REQUIRE at least some employees to get vaccinated against Covid-19, poll shows

© ASU Workplace Commons / rockefellerfoundation.org
RT | May 1, 2021
Many Americans and Brits will face de facto vaccine mandates, as a new poll shows that 56% of businesses will require at least some employees to be inoculated against Covid-19, in many cases under threat of losing their jobs.
The poll, which was conducted by Arizona State University and released on Thursday, showed that 40% of businesses will require all employees to be vaccinated against Covid-19, while 16% will mandate the jabs for at least some of their workers. All told, 88% of businesses will require or encourage their employees to be vaccinated, and 60% said they will demand some kind of proof of inoculation.
The survey, which was backed by the Rockefeller Foundation, paints a bleak picture for those who plan to resist getting the Covid-19 jabs. While the US and UK governments have refrained from making vaccines mandatory – and facing legal challenges that might ensue – the private sector may effectively do it for them. Businesses are already setting the stage to require so-called ‘vaccine passports,’ forcing customers to show proof of inoculation or a negative Covid test before accessing certain goods, services and events.
While many people can choose not to travel abroad or go to business venues that require proof of vaccination, an employer mandate could be more problematic. Arizona State said 31% of businesses plan to take disciplinary action, including possibly firing employees who refuse to comply with their vaccine policies.
A further 44% said non-compliant employees won’t be allowed to return to the workplace, while 27% said they will change the work responsibilities of those who fail to obey. Only 15% said there will be no consequences, even though the vaccines are being administered under emergency authorizations and so far lack the long-term study needed for full regulatory approval.
The survey was conducted at 1,168 companies, mostly large businesses with 250 or more employees based in the US and UK. The average business in the poll still has 57% of employees working remotely. About 75% expect workers to be back on site within the next one to six months, but 72% said they plan to offer more flexible work-from-home policies after the pandemic.
Employee wellbeing has suffered greatly during the pandemic. Nearly 58% of businesses said their concerns over employee mental health have increased, while 52% were more concerned about worker engagement. Other troubling issues included Covid-19’s impact on burnout, productivity and morale.
There is no scientific foundation to the concept of Vaccine Passports: Doctors for Covid Ethics
By Oliver May • THE DAILY EXPOSE • April 29, 2021
Doctors for Covid Ethics, a group of doctors across Europe and North America, say studies on Covid-19’s closest-related virus to infect humans, SARS, revealed that those who had acquired natural immunity in 2003 remain protected even now. They also maintain that, even before the onset of vaccination campaigns, most people had become immune to Covid-19, either through infection with the virus itself, often without symptoms or with only mild, uncharacteristic ones, or due to cross-immunity conferred by other, naturally occurring coronaviruses.
But under an Article of Law Decree just published by the European Union, its proposed Digital Green Pass will have validity for just six months. Once this expires the holder would need to be re-vaccinated or have had Covid in the last six months or take a test every 48 hours in order to regain their freedoms.
Doctors for Covid Ethics argue there is no rational case for such a pass, which is currently being used in Israel and proposed in the UK, adding that immunity from infection is likely to be durable and unaffected by variants.
Doctors for Covid Ethics said: “There is no scientific foundation to the concept of vaccine passports and no rational case at all for vaccine passports. To set a six-month cut-off is bizarre and arbitrary. Examining the time course of antibodies in blood samples is not a valid approach to the question of, ‘how long does immunity last?’.
“This is because antibodies aren’t the most important host defence mechanism in immunity to viruses. That’s considered to be T-cell memory (cytotoxic as well as ‘helper’ lymphocytes) and B-memory (antibody producing) cells. Antibodies naturally fall over time if you’re no longer constantly rechallenged with the infective pathogen. As community prevalence falls away, this re-exposure to the virus also diminishes.
“When durability of immunity to the closest known virus, SARS, was studied, those who had acquired immunity naturally, through infection in 2003, all retained immunity 17 years later. There is speculation that ‘variants’ of SARS-CoV-2 might ‘break through’ the immunity gained through natural infection or vaccination. There is absolutely no evidence for this at all.
“In fact, there is very strong evidence to the contrary – that no variant is sufficiently different from the original virus that it’s even possible for ‘immune escape’ to occur. Several groups of immunologists have shown convincingly that people immune to one variant have T-cells which recognise all the other variants tested. This isn’t a surprise, for no variant differs from the original sequence by more than 0.3 per cent.
“In fact, those who had retained immunity to SARS also possessed cross-immunity to SARS-CoV-2. These two viruses differ by approximately 20 per cent. Obviously, if our immune systems easily recognise two viruses which share 80 per cent similarity, it follows that differences of 0.3 per cent are completely irrelevant, from an immunological perspective.”
The group went on to add that focusing on antibodies in the context of vaccination against SARS-CoV-2 is “flawed” and so coercing people into so-called booster vaccines in order to regain their freedoms withdrawn by Governments is wholly inappropriate.
“The whole concept of antibody-based immunity against an air-borne pathogen is flawed because the antibodies are on the wrong side of the wall and cannot intercept viral entry into the respiratory tract epithelium,” added the group.
“Secreted IgA antibodies play no significant role either: selective IgA deficiency does not enhance susceptibility towards coronavirus infections.”
The group also highlights that vaccine companies have been exempt from legal liability for vaccine-induced harm, adding that, for the vast majority of people, SARS-CoV-2 is a non-lethal, typically mild to moderately severe illness. They said: “The overwhelming majority of people are not at risk from COVID-19 and do not require vaccination for their own protection.
“The vaccines have been touted as a means to prevent asymptomatic infection and, by extension, asymptomatic transmission. However, “asymptomatic transmission” is an artefact of invalid and unreliable PCR test procedures and interpretations, leading to high false-positive rates. Evidence indicates that PCR-positive, asymptomatic people are healthy false-positives, not carriers. A comprehensive study of 9,899,828 people in China found that asymptomatic individuals testing positive for COVID-19 never infected others.
“In contrast, the papers cited by the Centre for Disease Control to justify claims of asymptomatic transmission are based on hypothetical models, not empirical studies; they present assumptions and estimates rather than evidence. Preventing asymptomatic infection is not a viable rationale for promoting vaccination of the general population.”
They have written to MEP’s, putting them on notice that liability for adverse reactions to the vaccines will fall on them, should they vote for the Digital Green Pass, which was debated on Wednesday.
And last week, Doctors for Covid Ethics wrote their third letter to the European Medicines Agency, warning executive director Emer Cooke that cerebral venous sinus thrombosis (CVST) dominates the list of adverse reactions from the vaccines and is not as rare as the EMA suggests.
An exclusive interview with Dr Mike Yeadon

By Oliver May | The Daily Expose | April 25, 2021
Dr Yeadon, a former vice-president and chief scientific officer of the Allergy and Respiratory department at Pfizer, who has also provided a simple explanation of why lockdowns could never have worked, went on to explain that there is “zero” chance of incessantly reported new variants escaping immunity.
The 60-year-old, convinced the UK reached herd immunity last May, is now looking to move to Florida, where he hopes to work alongside Governor Ron DeSantis. He has expressed his severe concern over vaccine passports, saying that not only do healthy people under 60 not need a Covid 19 vaccine, but that the introduction of certification could lead to a society whereby, without such a pass, you may not even be permitted to leave your house.
In a passionate exclusive interview with The Daily Expose, he also criticised former Conservative MP Edwina Currie for her “uninformed” scattergun comments on Good Morning Britain in which she said she would not want anyone unvaccinated anywhere near her.
Dr Yeadon said:
“I know enough about biotechnology to know that you can easily create, shall we say, pathogens, which don’t look like they’re related to what you’ve done. And what’s even more horrifying is you can separate them in time, so an injection which will later make you ill or kill you can be separated by design in time from that event. So you might die a year later of liver cancer or something and you wouldn’t connect that. And if you can imagine making a smorgasbord of different pathogens so not everybody is going to die of the same thing, you literally could do away with big slices of the population if you want. And we could all be running around like headless chickens. This is an attempt on global depopulation.
“I think vaccine passports are a gateway to numerous things and it is my belief that it will be a gateway to mass killing, in the billions. And the reason I say that is many of the key players, including Bill Gates and his father and Boris Johnson and his father, have all been maniacal – and possibly correct – about earth being overpopulated. Even if we said to people can you stop having children, the population would only start to fall in about 100 years. If you got birth rates down below replacement, it would still take a century given each new birth will probably live out 100 years.
“I accept the argument that, if we are on the verge of destroying the planet, the ecosystem and its non-renewables and biodiversity, if these things are true then, I’m not saying I endorse it, I can see the argument of ‘do you know what, the only possible way to save the earth is to get rid of 90 per cent of the people and then it will be a nice place to live’.
“I think a group of people over decades have said to each other, ‘this is an awful task that has fallen to us, which is to rescue the human species and its planet and there is no other way of doing it except for mass extermination. And it’s not something that anybody would want to do but we have to do it and it’s got to happen in this generation and these are the technological advances required’.
“There are some clever people who have taken it upon themselves to basically do God’s work and to do a violent readjustment of the population of the world to put it into a position where, once it sorts itself out from this utter bloody disaster, will be a place where 500million people maybe will be living on the planet and they can have comfortable sustainable lives with plenty of space, plenty of room for the animals. I will not support what they’re doing but that would provide a justification for those who are doing it.”
Dr Yeadon believes the proof lies in the correlation between deaths and the rollout of vaccines which have been rushed through via an Emergency Use Authorisation. He said:
“If you look at every regional health authority, they tick up on the same day, they peak at the same day and drop back in the same way and that’s because they’re sycned to vaccination. If it was the spreading of an epidemic, it could not possibly occur in Auchtermuchty on the same day as Aldershot. It can’t, it has to move.
“But the thing that moved was the vaccination squads. They started on December 8 everywhere in the NHS and then in the care homes, so that was the strong clue for me that what was correlating with the time and cause of deaths was not a geographical history and neither were the differences in timing, it was just the date of vaccination.
“Can it be stopped? I am not optimistic about the UK because as time has gone on there are fewer of me and most people have just put their heads down. I am fortunate in a number of ways, I have the breadth of a full career behind me and I love science and biology. There is nothing I can be fired from and I’m not doing it for money, so I can only be stopped if they arrest me or kill me.
“But I don’t fear for my life. It’s over anyway. This is not going to return to normal. It would be pointless. There is no way, with the amount of damage that has been done deliberately, would it then just be left. It would just be dumb. It would make no sense at all to have marched people up to the top of the hill and then say, ‘you can go back now’. And remember the drum beats for vaccine passports are very strong. And once that’s in then if they can transition an absolute majority that they already have who will be so delighted with their privileges, beeping their phones when they go in and out of shops, they are not going to pay any attention to someone like me who says, ‘excuse me what about the unvaccinated’?
“They will say, ‘well don’t you know, you’re the unclean people, you’re the ones brewing the variants, you’re going to kill us. Can you just go away or I might feel that I have to kill you’. I expect vaccine passport will come in and those who have already been vaccinated will whoop for joy, a large number of people yet to be vaccinated will rush to get vaccinated because they will see their horizons will be shrunk and they simply won’t realise they are being herded like cattle into a pen.
“I would fear next winter being an unvaccinated person in this country, there will be additional orchestrated events. They will need that in order to drive people to top-up vaccines. I’ve decided I’m not going to stop the fight, I’m going to leave the country. I’ll go wherever I have to because it’s not going to be safe for unvaccinated people indefinitely.”
Top-up vaccines is another thing that frightens Dr Yeadon, who highlighted the fact that these too will forego any further safety checks. He added that the driver for these will come in the form of new variants, which he says are barely any different from the original sequence.
“As soon as they started talking about it [new variants] I went to look at the source material and found that the variants most different from the Wuhan sequence are still 99.7 per cent identical. “And I can assure you that there is zero – not just implausible, but zero – chance something that would escape the immunity of someone who was immune from natural infection or vaccinated. It’s absolutely impossible, no matter what they tell you.
“We know for example that Sars 2003 is 20 per cent different – not 0.3, 180 times different – and the immune system has absolutely no trouble in recognising the two as brothers. I have empirical evidence, theoretical evidence and yet, countering that, we are being told by Sage, politicians, people around the world that you need these variant vaccines. We’ve closed our borders, we’re smashing our economy and depriving people of their liberty over the theoretical concern about variants, which is a lie. And now we are making variant vaccines. I became terrified when I knew they were actually making them and not just talking about it – and when all the large medicine regulators of the world put out a joint statement saying that, because vaccine variants are so similar to the parents from which they’re derived, we will not require the manufacturers to conduct any clinical safety studies.
“I have spoken to eight professors in the UK whose discipline includes immunology and they all agree with my analysis in terms of the technical side of it. Three months ago my fear levels went into the red and I begged them, ‘people like you have go to start writing letters to editors and getting pieces into the papers that this b******t about variants is fake because people are going to believe it’. Carl Heneghan [director of evidence based medicine at Oxford University] said that the world is in such a sort of panic at the moment, anything he could say would not have any breakthrough power at all.
“We’ve been trained to think that if anyone raises any question at all about vaccines, you automatically think ‘anti-vaxxer’. I’ve spent my entire professional career in the industry that produces these things. I would say I’m extremely pro innovative medicines. I don’t have an anti bloody anything in my body except I’m anti unsafe medicines. Why have we got vaccines that clearly are much more dangerous than other public health prophylactic vaccines, because they are if you just compare the number of people that have died within a month with the number of reported deaths after all other vaccines – it’s like 10 times worse.
“There have been 10 times more deaths from within a couple of months of any covid vaccination than in the entire year for all other vaccines combined. Most vaccines are very safe but there are rare idiosyncratic responses including fatal ones and I’m afraid that does happen. You might just drop dead tomorrow going out to your car. But as long as the numbers are very, very small it’s tolerable, because there is a benefit to it. But what we have here is that, even if the people being given the vaccines were at risk – and a lot of them are not – anyone 60 or younger who is in good physcial shape and does not have serious prior chronic conditions is not going to be killed by this virus, they’re just not. It’s unethical even to bloody offer it to them. There is no logic to the statement that we need to vaccinate everybody in order to stop this, it’s just nonsense.
“Now if Edwina Currie is vaccinated then she is fine. She might sincerely believe what she’s saying in which case she’s just uninformed and nuts. I’m sure lots of MPs have just been given the brief and they’re not very clever. I’ve personally spoken to about 60. Several get it reasonably well but some of them are just embarrassing.”
Reports have surfaced in the past week that trials mean venues might be able to open to capacity audiences on June 21, in keeping with the Government’s roadmap – but only if people agree to Covid passports. Dr Yeadon believes that introducing such a system will create a two-tier society and one which can be tweaked at a moment’s notice depending on the Government’s wishes.
Dr Yeadon said:
“There is absolutely no chance whatsoever that Westminster will save the people. They are the tools of our destruction. They will vote vaccine passports through, even those who know these are horrible things. They’ll be told it’s temporary and get their pat on the shoulder. But of course they won’t be temporary.
“For example, you might even be told as from next month it will be illegal to leave your house without a valid vaccine passport. That’s how easy it would be. We are following “the science”, capital T, capital S. I’m not saying they will do that but they can exclude non-vaccinated people from civil society wholly and that is what is happening in Israel. Once this system comes in I cannot see a way in which it can be undone. They might say initially you can’t enter a sports ground or a large shopping complex, but then in a couple of weeks they might say, ‘as of Tuesday all large supermarkets will use vaccine passports on the door’, so that’s them out. And eventually they can say, ‘as from Wednesday week, all cashless transactions must be preceded by demonstration of a vaccine pass’ – so you can’t even fill your car with petrol. It could happen.
“The idea would be for me to be in America, educating and essentially immunising populations and politicians against what is happening, so that when they’re told next time that you need to lock down your businesses and your state, they won’t. That’s the goal. My preferred one would be to go and work for either Governor DeSantis or his scientific advisory team.”
Dr Yeadon has criticised his peers for failing to speak out against the problems he sees with following only one line of enquiry. He explains that the UK’s official figures of 4,395,703 positive cases and 127,000 simply cannot be believed due to the countless levels of contamination in testing and the unprecedented change in how deaths are certified.
He said:
“I am disappointed that almost no one in the scientific community has said anything. What about recently retired professors, people who are not being paid by universities, why aren’t you saying something? Is it cowardice? Death certification has been radically changed in a way that has never been done anywhere for any disease. And we have never used PCR on an industrial scale and it is my opinion – confirmed by people who do this professionally – that it could never be done reliably. So whatever they tell you it’s a lie. You cannot run three quarters of a million PCR tests and not have cross contamination all over the place.
“Why were the doctors not complaining about the death certification? If you have a positive in this ropey test at any time 28 days up to your death then that is on your death certificate. It’s just not even logical. It’s like saying if you had biro on your finger at any point 28 days prior to your death, we’ll say you died of biro ink poisoning. It’s absurd. But they went along with it.”
And he has a message for those who no doubt once would have agreed that you cannot trust a politician but who know hang on their every word.
“If you spot an inconsistency, something you think, ‘that doesn’t sound right’, pursue it, because if you pursue it to a point where you think, ‘I’m not being told the truth’ – which you’re not – once you spot that, then the question would be, ‘if your Government has lied to you about one thing, don’t you think it’s quite likely it has lied to you about other things?’ I believe they are lying to you about everything.
“Let’s look at pubs; you can only take a drink outside and you can only pay for it outside. Hold on, have the supermarkets not been open continuously through this process? Sometimes it’s really busy and you might be in the shop an hour. Isn’t that an inconsistency? And why are we OK with that? I don’t believe that any outbreaks have ever been linked to a supermarket. And that is another odd one. That’s about the only place you meet. Surely all the outbreaks that aren’t linked to hospitals and care homes must be linked to common places of commerce and they are supermarkets and essential shops – there aren’t any others, none.”
And he uses supermarkets in his insight as to why lockdowns are pointless; in a nutshell, if you are full of virus, you feel very ill, so you would be at home, curled up on the sofa, in bed or in hospital. If not, you do not have enough virus in your body to be a threat of transmission. Indeed, a global study, cited by Jay Bhattacharya, Professor of Medicine at Stanford University and co-author of the Great Barrington Declaration, to a court in Manitoba, found that asymptomatic transmission is close to zero in an outside setting, given it is about 0.7 per cent inside.
Dr Yeadon says:
“We will lock down again. They will want to do it as early as possible, so October.
“But the reason why lockdowns could never have worked is combined with one of the other lies, asymptomatic transmission. The reason it’s a lie is that, in order to be a good source of infection, you need to have lots of virus in your body. If you’ve only got a little bit, the chances that you would infect another person is very low, even if you were close to them – maybe even if you kissed them – you just don’t have that much virus in and around your body.
“But if you had a thousand times more virus, maybe you could put a droplet on a person and they might inhale it or whatever. But if you have lots of virus you must have symptoms. You cannot have a situation where your body is growing huge amounts of virus in the airwaves and producing no symptoms and this is because the virus will attack you, it’s damaging your tissues, every cell it multiplies in and then escapes from is destroyed. It’s not just a theory, it’s inevitable you will have symptoms. And furthermore you need symptoms like coughing in order to propel infected droplets out of your body. They don’t come out when you’re just passively breathing. If you have lots of virus and it’s attacking you and making you ill and your immune system is fighting it back, which is also making you feel ill, those symptoms are called ‘I don’t feel well’.
“So if you’re a good source of infection, you’re symptomatic, you don’t feel well, you probably feel very ill, possibly bad enough to be in your bed and we’re giving you chicken soup and cups of tea every few hours. And if you’re a bit older you might be in hospital. But what you’re not going to be doing is dashing up and down the aisles in Sainsbury’s. Or sitting in the pub. You’re ill. So that’s the whole point. In the general community, almost no one who met the conditions to be pretty sure of infection was out there. It’s just simply not possible. You need to be full of virus, you need to get the symptoms to get the stuff out of your body but you need to be completely unwell despite those two things.
“And those things do not overlap, you can’t have ‘feeling fine out and about, looking normal but full of virus’. And we are trained to notice if someone has a cold or they look ill. We have known this stuff for tens of thousands of years. You can spot someone who is a respiratory threat to you. It’s very uncommon for people with good sources of infection to be walking about in the community and, even if they were there, you would usually avoid them. And as a result hardly any transmission occurred in the general population. And as a result shutting down the general population made f**k all difference to transmission. And that is why lockdowns don’t work and they never did. They never worked anywhere because lockdown isn’t really lockdown, it just smashes the economy.”
Australian MP blasts Facebook’s ‘interference’ after his OFFICIAL page was banned for Covid-19 ‘misinformation’
RT | April 26, 2021
After Facebook deleted the official page of Craig Kelly for spreading “misinformation” about the coronavirus and vaccines, the independent MP said the “book-burning” US social media giant was interfering in Australia’s democracy.
Kelly was informed of Facebook’s ban by text on Monday morning, he told the media, describing the move as “censorship.”
Banning the page with some 86,000 followers represents “interference in Australian democracy,” he said.
“This was the most popular, highly used political Facebook page in the country,” he said, in remarks quoted by ABC. “They have basically burnt and torched and incinerated and obliterated from the record, previous comments and previous things that I’d made.”
Kelly’s personal page and Instagram account remained active, for now. A Facebook spokesperson said in a statement that the Australian MP had “repeatedly” violated their policies.
“We don’t allow anyone, including elected officials, to share misinformation about Covid-19 that could lead to imminent physical harm or [Covid-19] vaccines that have been debunked by public health experts,” the spokesperson said.
“It is not misinformation if you have a difference of opinion,” Kelly shot back. “The idea that they are some purveyors of all truth is just absolutely outrageous.” The ban is not just outrageous but also violates the principles of free speech, he added.
Facebook did not just remove a few posts, but the entire page, he said, describing it as “like setting fire to a book, not just removing the pages they disagree with.”
These people are the heirs to those who used to go around burning books because that is effectively what they have done.
Kelly has represented Hughes, a parliamentary district south of Sydney in New South Wales, since 2010. He resigned from the ruling Liberal Party in February, after Facebook suspended him for “misinformation” about Covid-19 and someone from the office of Prime Minister Scott Morrison told him to “shut up” about the virus.
Flush from the success of “fortifying” the 2020 US presidential election, Facebook announced in December that it would ban any “false claims” and “misinformation” about Covid-19, even if posted by public officials.
In January, Mark Zuckerberg’s social media behemoth clashed with Canberra over a proposed law requiring social media to pay for news content. After a week-long Facebook ban on all news content in Australia, the government relented and proposed an amended law, which critics said favored major corporations over local and independent news outlets.
French Report Urges Halt to Covid Mass-Jabbing
By Stephen Lendman | April 26, 2021
There’s nothing remotely safe and effective about experimental/unapproved Pfizer/Moderna mRNA technology and J & J’s vaccine for covid mass-jabbing.
Translated into English, a report by an independent French drug assessment center — the Centre territorial d’Information indépendante et d’Avis pharmaceutiques — CTIAP) called for halting mass-jabbing for covid “as a matter of urgency.”
It stressed that experimental Pfizer, Moderna, AstraZeneca and J & J covid drugs lacked sufficient testing, adding:
Their excipients (coloring agents, preservatives, fillers and other ingredients) should be considered as new active substances.”
They were OK’d for emergency use — when no emergency exists — before there was “proof of quality for the active substance and the finished product.”
CTIAP also called their manufacturing processes problematic.
Its report stressed that “variabilities, which impact the very core of the product, could even invalidate any clinical trials conducted” ahead, adding:
“Can we imagine launching a car manufacturing line and putting vehicles on the road, despite the uncertainties noted in the official documents published?”
“These uncertainties are related to the quality of the parts making up the engine and the various other parts, including those related to safety, the manufacturing process, the reproducibility of the batches that are being marketed, etc.”
“In the field of medicines (including covid mRNA technology and vaccines), the pharmaceutical act of ‘release’ of the finished product (an authorized product intended for sale) constitutes the final stage of control that precedes the release of these products to the population.”
“This key step of ‘release’ is under the pharmaceutical responsibility of the manufacturers.”
“Prudence…dictate(s) that, in all countries where these vaccines against (covid) have been marketed, all the batches thus ‘released’ should be withdrawn immediately.”
“These MAs (marketing authorizations) that have been granted should be suspended, or even canceled, as a matter of urgency until further notice.”
European Medicines Agency (EMA) documents explain lack of sufficient evidence to show whether experimental covid drugs are safe and effective.
Marketing authorization granted them by the EMA is “conditional” for up to one year — based on “incomplete data.”
Separately on Friday, a CDC advisory panel recommended unrestricted use of J & J’s hazardous covid vaccine for individuals aged-18 and older.
If approved by the Pharma-connected CDC and FDA as expected, J & J covid mass-jabbing will resume.
Claiming benefits — that don’t exist — outweigh risks defies reality.
The same holds for Pfizer/Moderna mRNA technology and AstraZeneca’s covid vaccine.
They’re experimental, inadequately tested, rushed to market drugs that are too hazardous for human use.
Mass-jabbing with them already caused countless numbers of adverse events, including deaths in the US, Europe and elsewhere.
Ignored by the CDC, FDA, and EMA is that no need or justification exists for use of these high-risk experimental drugs.
Safe, effective, low cost drugs, and alternative non-drug therapy, works to prevent, treat and cure seasonal flu-renamed covid as needed.
Defying reality, the pro-mass-jabbing NYT falsely claimed that “pause(d) (use of J & J’s covid vaccine) was widely considered a blow to national and global vaccination efforts (sic) and removed an effective vaccine (sic) that many states and countries had counted on to deploy in hard-to-reach places (sic).”
Experimental covid drugs don’t protect. They risk serious adverse events near-or-longer-term, including possible death.
Preserving and protecting health requires rejecting them.
The alternative is playing fast and loose with what’s too precious to lose.
Should Unvaccinated and Obese Be Penalized by Government?
By Dr. Joseph Mercola | April 23, 2021
“Vaccine refusal will come at a cost — for all of us,” Edward-Isaac Dovere, a staff writer for The Atlantic, proclaims in an April 10, 2021, political commentary.1 Unvaccinated individuals “will have higher health care costs,” he says, and the vaccinated will have to foot the bill, either through taxes or insurance premiums.
This argument could have been made for decades, and can still be made today, for any number of groups. Obese individuals have far higher health care costs than those of normal weight. Insulin resistant people and those with Type 2 diabetes end up costing the health care system enormous sums. Who pays for them?
Overall, healthy individuals — people who generally do what they can to take good care of themselves to prevent chronic conditions — have always paid for those who are less particular about their diets and lifestyle.
The Economic Costs of Vaccination Vs. Vaccine Refusal
Dovere predicts the economic costs of vaccine refusal will begin to feature heavily as we move forward. He quotes Washington Gov. Jay Inslee, who told him,2 “You have a liberty right, and that unfortunately is imposing on everyone else and their liberty right not to have to pay for your stubbornness.” Not surprisingly, Dovere and Inslee both focus on just one side of what needs to be a two- if not four-sided equation.
When making public health policy, you have an obligation to analyze both the benefit and the cost of any given policy. In this case, what might be the cost of vaccine side effects, both in terms of health care costs and lives lost? As of April 1, 2021, VAERS had received 56,869 adverse events following COVID-19 vaccination, including 7,971 serious injuries and 2,342 deaths.3 By April 13, the had updated that death toll to 3,005.4
What might be the cost if the vaccines don’t work and you get sick anyway? As of April 15, 2021, some 5,800 Americans who had been fully vaccinated against COVID-19 had been diagnosed with COVID-19 post-vaccination; 396 (7%) required hospitalization and 74 died.5 These cases are popping up all over the world.
The vaccines are not foolproof. In fact, so-called “breakthrough cases,” meaning cases in which a fully vaccinated individual is diagnosed with COVID-19 are to be expected. I’m not sure why anyone is surprised, seeing how the vaccine makers have acknowledged that the mRNA injections are not designed to actually make you immune to SARS-CoV-2.
You can still contract the virus and spread it to others. What the shots may do is lessen your symptoms if and when you get infected with SARS-CoV-2. So, of course people can still get sick, as they did before. Some will require hospitalization. Some will die — just like they did previously, before the vaccine.
Then there’s the question of whether vaccinated individuals end up being more susceptible to variants of the virus than unvaccinated individuals. Preliminary research6,7,8,9 found that people who had received both doses of the Pfizer COVID-19 vaccine were eight times more susceptible to contracting the South African variant of SARS-CoV-2, called B.1.351, (5.4% compared to 0.7%).
Unfortunately, the study was too small to glean any information about outcomes, so we don’t know whether they developed milder or more serious illness than unvaccinated people sickened by the same variant.
Either way, if vaccinated people are more susceptible to more dangerous variants (which they claim B.1351 is), why assume that unvaccinated people would incur higher health care costs? Variants are now cropping up all over the place, so maybe vaccinated people will end up being responsible for a greater share of medical expenses. Maybe, if they have milder illness and unvaccinated have more serious illness, the costs might end up about the same for each group.
May There Be Economic Benefits to Vaccine Refusal?
In my view, the notion that COVID-19 vaccines will end this pandemic is an illogical fallacy since these shots do not provide actual immunity. The fizz in Dovere’s argument starts going flat on that basis alone. But there’s much more.
To really determine what’s best for public health, you’d also want to do the benefit and cost analysis of not vaccinating and relying on naturally-acquired immunity in combination with immune-boosting strategies instead, such as improving vitamin D levels across the entire population, for example.
Only when you have made all of those calculations — the benefit and cost of vaccinating, and the benefit and cost of not vaccinating — can you compare the two and begin to make statements about how certain groups of people may incur higher health care costs, and which strategy is likely to save the most lives. As of right now, it’s pure guesswork as to who’s going to cost more in the long run.
For example, I don’t know of any actual data showing that the health of people who are planning to forgo the vaccine place them at increased risk of serious COVID-19. If I were to guess, and this is pure speculation, people who have decided not to get vaccinated may be doing so because a) they know they’re in a low-risk category and/or b) they are health-conscious people who feel confident that they can prevent and/or treat COVID-19 in other cost-effective ways, should they get sick.
There are a lot of data that need to be compiled and analyzed before we can start declaring the COVID-19 vaccination campaign a public health care success, let alone a cost-saving imperative.
Appeal to Illogical Reasoning
Dovere goes on to discuss some of the messaging campaigns employed to lure people out of their vaccine hesitancy:10
“Two appeals seem to work best: First, the vaccines are safe, and they’re more effective than the flu vaccine. Second, you deserve this, and getting vaccinated will help preserve your liberty and encourage the government to lift restrictions.
(That last idea is what Jerry Falwell Jr. focused on in the vaccination selfie he posted11 this week, captioned, ‘Please get vaccinated so our nutcase of a governor will have less reasons for mindless restrictions!’) Inslee hopes that emphasizing those points will persuade more Republican men to get their shots.”
Sometimes it can help to spell out a logical fallacy using different words. (Personally, I believe Falwell was simply trying to be funny, but Dovere and Inslee have apparently seized the “lift restrictions” angle as a social conditioning opportunity, so that’s really what I’m addressing here.)
One rewrite of Falwell’s plea could be: “Please ignore your current health status and potential vaccine risks and just obey so that our governor will have less reason to impose unconstitutional and unscientific limitations on our basic rights and freedoms.”
In my view, a more appropriate way to prevent “mindless restrictions” would be to peacefully disobey and/or take the governor to court, as has been done to California Gov. Gavin Newsom. The Supreme Court has ruled against him no less than six times, finding he abused his power, overstepped his authority and violated the Constitution with his pandemic restrictions on churches.12
Urging someone to take a vaccine to prevent an elected official — who can be unseated — from implementing unscientific and/or unconstitutional restrictions is hardly rational. Let’s not forget that cost-benefit analyses13 have actually been done for lockdowns — perhaps one of the most mindless of restrictions — and the cost is far greater than the benefit.
The cost of the lockdowns in the U.K., in terms of Wellbeing Years (WELLBY), is five times greater than might optimistically be saved, and may in reality be anywhere from 50 times to 87 times greater. The cost for lockdowns in Canada is at least 10 times greater than the benefit.
In Australia, the minimum cost is 6.6 times higher, and in the U.S., the cost is estimated to be at least 5.2 times higher than the benefit of lockdowns. A cost-benefit analysis performed for New Zealand, which looked at the cost of adding just five extra days of “COVID-19 alert level 4” found the cost in Quality Adjusted Life Years (QALY) was 94.9 times higher than the benefit.
Should We Penalize Obesity and Vitamin D Deficiency?
If it’s determined that unvaccinated individuals need to be penalized socially, financially or otherwise, then how can we not also penalize other choices that significantly add to the COVID-19 burden? We know, for example, that vitamin D deficiency significantly raises your risk of COVID-19. In one analysis,14 82.2% of COVID-19 patients were vitamin D deficient.
I published a scientific review15 on the impact of vitamin D in COVID-19 in October 2020, co-written with William Grant, Ph.D., and Dr. Carol Wagner, both of whom are part of the GrassrootsHealth expert vitamin D panel. You can read the paper for free on the journal’s website.
Another major COVID-19 factor is obesity. As reported by CNN16 March 5, 2021, the COVID-19 death rates were more than 10 times higher in countries where more than half the adult population was overweight, compared to countries in which the obesity rate was below 50%. The COVID-19 death rates also rose in tandem with the prevalence of obesity, thereby strengthening the link, according to the report, released by the World Obesity Federation.
At the lowest end is Vietnam, which has an obesity rate of 18.3% and a COVID-19 death rate of 0.04 per 100,000. Toward the high end is the U.S., which has an obesity rate of 67.9% and a COVID-19 death rate of 152.49 per 100,000. (Of course, this report used COVID-19 mortality statistics that have been proven to be wildly exaggerated, as detailed in my interview with Dr. Henele.)
Making an already dire situation worse, recent data17 show 42% of U.S. adults have packed on unwanted pounds, with an average weight gain of 29 pounds, since the start of the pandemic. Only 18% report undesired weight loss, with an average weight loss of 26 pounds.
Government Has Ignored the Value of Healthy Population
According to the World Obesity Federation report, obesity was the second most important risk factor for hospitalization and death from COVID-19 — old age being the primary risk factor — and as noted by Johanna Ralston, CEO of the World Obesity Federation:18
“Old age is unavoidable, but the conditions that contribute to overweight and obesity can be highly avoidable if governments step up and we all join forces to reduce the impact of this disease. The failure to address the root causes of obesity over many decades is clearly responsible for hundreds of thousands of preventable deaths.”
Lead author of the report, Dr. Tim Lobstein, added:19
“Governments have been negligent, and ignored the economic value of a healthy population at their peril. For the last decade they have failed to tackle obesity, despite setting themselves targets at United Nations meetings. COVID-19 is only the latest infection exacerbated by weight issues, but the warning signs were there. We have seen it in the past with MERS, H1N1 and other respiratory diseases.”
Let’s Not Accept Hypocrisy and Double Standards
Even WHO Director-General Tedros Adhanom Ghebreyesus commented on the report saying it “must act as a wake-up call to governments globally,” as “The correlation between obesity and mortality rates from COVID-19 is clear and compelling.”
That said, let’s get back to Dovere’s argument that unvaccinated people are bound to incur higher health care costs due to COVID-19, and therefore there must be some way to penalize those people or force them into compliance.
Using that logic, what, then, do we need to do about obese individuals, whose risk of hospitalization due to COVID-19 is anywhere from 40% to 113% greater, and their chances of requiring intensive care 74% higher,20 than that of their non-obese peers? What do we need to do about people who just refuse to get their vitamin D levels up, and end up taking up the lion’s share of hospital beds?
To be clear, I am NOT proposing we penalize people based on their weight, metabolic flexibility or vitamin D status. I do not support that any more than I support penalizing unvaccinated people — and that is the whole point. Most would agree that this would be completely ridiculous.
My point is, if you cannot fathom penalizing obesity, insulin resistance, diabetes or vitamin D deficiency — conditions known to significantly raise your risk of severe COVID-19 — then how could you possibly consider penalizing an unvaccinated person based on that single parameter alone?
The question is especially valid because, again, vaccinated persons can contract and spread SARS-CoV-2 like anyone else. It’s really unclear how vaccinated people are “safer” than unvaccinated ones, when the only person standing to gain from these shots is the person getting it (in the form of milder symptoms when sickened).
Are You ‘Pure’ Enough for Your Government?
I think it’s important to realize that the COVID-19 vaccine campaign is less about protecting public health and more about creating the infrastructure and psychological climate required for the implementation of global tyranny, which will likely begin with the introduction of vaccine passports that are very similar to the China social credit system.
As discussed in “Vaccines Are the New ‘Purity Test,’” it can almost be likened to a loyalty test. Or perhaps it could best be described as a totalitarian submission test?
Getting private companies to require these vaccine passports only makes sense if there is a strong vaccine push, and this is one of many clues as to what’s really behind the stated “need” for the whole world to get vaccinated.
We’re not all at risk for COVID-19. For a vast majority of individuals, the vaccines make little or no sense, as for young, healthy individuals, their risks outweigh the benefit. Now they are pushing to vaccinate children, whose risk of getting COVID-19 is well-established as being profoundly minuscule.
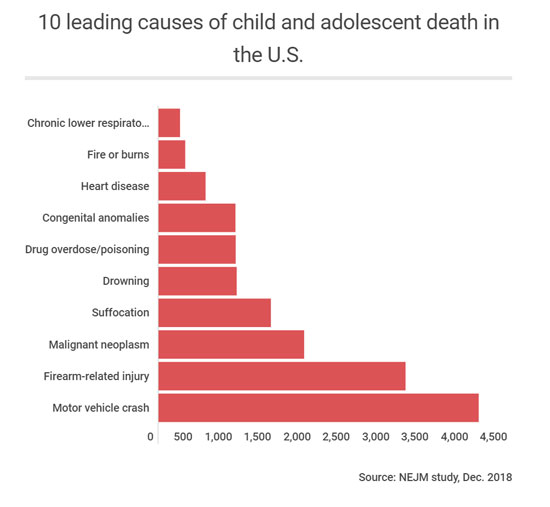
They are at exponentially higher risk from many other factors. There are currently fewer than 500 children who are reported to have died from COVID-19, even with the massively manipulated causes of death. Remember, if you had a positive COVID test and died from terminal cancer or a motorcycle accident, you were classified as a COVID-19 death.
As you can see from the graph below, there are 10 higher risks of death than COVID-19 for children. To be logically consistent, the government would need to be equally rigid about addressing all of these causes as aggressively as they are pursuing COVID-19 vaccination for children.
But it’s not about simply getting a vaccine into your arm. Ultimately, it’s about getting you tied into the digital system being launched in the form of vaccine passports. As explained by former Clinton adviser and author Naomi Wolf (whom I will be interviewing shortly) in a March 28, 2021, interview with Fox News’ Steve Hilton:21,22
“‘Vaccine passport’ sounds like a fine thing if you don’t understand what those platforms can do. I’m [the] CEO of a tech company, I understand what these platforms can do. It is not about the vaccine, it’s not about the virus, it’s about your data.
Once this rolls out, you don’t have a choice about being part of the system. What people have to understand is that any other functionality can be loaded onto that platform with no problem at all. It can be merged with your Paypal account, with your digital currency. Microsoft is already talking about merging it with payment plans.
Your network can be sucked up. It geolocates you everywhere you go. Your credit history can be included. All of your medical and health history can be included … It is absolutely so much more than a vaccine pass … I cannot stress enough that it has the power to turn off your life, or to turn on your life, to let you engage in society or be marginalized.”
Dangerous Curves Ahead
Wolf also points out the horrific history of IBM, which developed a sophisticated system of punch cards that allowed Nazi Germany to create a two-tier society and ultimately facilitated the rounding up of Jews for extermination. Fast-forward to today, and IBM is now a leader in the vaccine passport business. I wrote about this in “IBM Colluded With Hitler, Now Makes Vaccine Passports.”
In Nazi Germany, the obsession with purity — both in terms of hygiene and race theory — drove the genocide of Jews, the old, the handicapped and the mentally challenged.
In present day, the public narrative has eerily followed Nazi Germany’s playbook for genocide, starting with the scapegoating of healthy people, as the rapid spread of COVID-19 was blamed on asymptomatic individuals not properly masking, social distancing and self-isolating.
That then grew into the nurturing of prejudice against people who refuse to wear masks, and now we’re seeing the narrative building toward persecution of those who do not want to get the vaccine. It will start with discrimination, and already, we’re hearing talk of how only vaccinated people ought to have the right to partake in certain social activities. If that is tolerated, then outright persecution will be the inevitable next step.
This is why I reject and counter commentaries such as that by Dovere. These half-baked, one-sided, persecutory arguments must be challenged at every turn, because they only lead us one way. And unless you’re part of the technocratic elite, you — regardless of how you feel about vaccination right now — do not want to end up there.
Sources and References
- 1, 2, 10 The Atlantic April 10, 2021
- 3 The Defender April 9, 2021
- 4 CDC, Selected Adverse Events Reported after COVID-19 Vaccination April 13, 2021
- 5 The Defender April 15, 2021
- 6 Epoch Times April 11, 2021
- 7 Reuters April 10, 2021
- 8 Washington Examiner April 11, 2021
- 9 Medical Xpress April 11, 2021
- 11 Twitter Ruth Graham April 8, 2021
- 12 Townhall April 13, 2021
- 13 Preprints.org 2020: 2020100330 DOI: 10.20944/preprints202010.0330.v2
- 14 The Journal of Clinical Endocrinology & Metabolism October 27, 2020; dgaa733 [Epub ahead of print], Results
- 15 Nutrients October 31, 2020;12, 3361; doi:10.3390/nu12113361
- 16, 18, 19, 20 CNN March 5, 2021
- 17 APA.org Undesired Weight Change Since Start of Pandemic
- 21 Real Clear Politics March 29, 2021
- 22 The Epoch Times March 29, 2021
The Capture of Goodness

By Sinead Murphy | OffGuardian | April 25, 2021
‘Goodness’ is not the word I wanted to use in this article. But ‘ethics’ sounded too abstract, ‘morality’ too rule-bound, ‘virtue’ too archaic, and ‘kindness’ too corporate (at least since ‘random acts of kindness’).
The ubiquity of that dreaded term ‘safety,’ brayed at us from every angle, has made all the old names for concern for each other’s welfare seem ill-fitting and out of date. ‘Goodness,’ for all its faults, will have to do.
*
On Tuesday 30th March, leaders of 23 countries, including the UK, France and Germany, issued a statement on the matter of ‘pandemic preparedness.’
Its key phrase was reprinted across the media: Nobody is safe until everyone is safe.
As we embark on our second Covid year, the sentiment is chilling.
Nobody is safe until everyone is safe is the latest phase in the capture of human goodness that has been the most profound effect of Covid.
At first, we were asked to keep our distance. Other people, for whose sake we do most of the good things we do, were put beyond our reach.
We no longer held the door for the next person to pass through. We no longer offered to carry an old lady’s shopping. We stopped shaking one another’s hand and patting each other on the back. We no longer hugged.
Almost all of the ways in which we knew how to be good to each other were paused; the bonds of mutual support were severed.
Then, for the first time uncertain about how to do good – then, we were asked to mask up. Not for our own sake. For the sake of the other person – I mask for you, you mask for me. Being good to other people was returned to us. But it was not quite like it had been before.
Other people, still at a distance, were now also without faces, and faces are so important in arousing our pity, commanding our assistance, eliciting our smile. Goodness had been readmitted, but for the sake of newly anonymous beings.
Then, still at a distance, still masked up, we were encouraged to take the jab. Not for our own sake – at least, not directly. For the sake of the herd. For herd immunity.
This concept, so energetically rejected as cruel during the first months of Covid, was returned to us. But it was not quite like it had been before. It was cleansed of its natural components, redefined by the World Health Organisation as an achievement of vaccination, its taint of ‘let it rip’ buried under a great enthusiasm for pharmaceutical engineering. Herd immunity was back. And goodness was redirected towards an anonymous crowd.
And now we are told that nobody is safe until everyone is safe. Now we are to be good, not even to a masked and distanced other, not even to an anonymous herd, but to everyone.
Everyone? All seven billion inhabitants of the earth? It is worse than that. The statement issued by world leaders on 30th March champions a concept of ‘One Health,’ which is described as encompassing ‘humans, animals and our planet.’
How in the world is any of us to act for the good of this everyone? The idea is sublime. It may strike us with awe, even admiration, but there is nothing we can do for its sake. Our good deeds, already scrambled by distancing and masking and herding, are now, at last, out of play.
One year ago, we were tempted from the well-trodden paths of goodness onto a seemingly higher road, emblazoned with slogans of sacrifice, decorated with rainbows and resounding with the clapping of people pulling together. But the road leads nowhere. It is a dead end.
In January, in the northern snow, I was saying hello to my neighbour over the low garden wall. So that she could find her key, she placed her little girl, ten months old and all wrapped up in her snowsuit, onto the soft ground. While my neighbour was searching in her bag, her baby slowly keeled over. Without thinking, I stepped across and leaned down to lift her. But it was the wrong thing to do. Her mother snatched her up and I retreated in vague apology.
What is now the right thing to do when a small baby falls sideways onto the snow? The answer: nothing. Goodness is cancelled. Or, rather, it is redirected through an idea so sublime that nothing follows from it for mere humans with their merely human faculties. Everyone means nothing to us. For the sake of everyone, we can do nothing.
But there is a problem about doing nothing. Because it may just be that human beings are only good insofar as they do good things. Goodness requires practice and wastes away from lack of practice. It is more like playing the piano than riding a bike; you have to keep it up or you can no longer really do it. How long before our good natures grow rusty and flake away? How long before we no longer know how to be good?
Which is why, I presume, we now have these badges of goodness: masks, certificates.
Our enthusiasm for both may have little to do with their dubious efficacy in stopping the spread of a respiratory virus, and much to do with our need for reassurance that, even though we no longer do good things, we still really are good people.
Sinead Murphy teaches Philosophy at Newcastle University. Her most recent publication is Zombie University: Thinking Under Control (Repeater, 2017).
Did Bill Gates Reveal the Reason Behind the Lock-Downs?
By Rosemary Frei | OffGuardian | April 4, 2020
In a candid interview, Bill Gates has outlined that, despite the comparatively small threat of Coronavirus, he and his colleagues “don’t want a lot of recovered people” who have acquired natural immunity. They instead are hoping we become reliant on vaccines and anti-viral medication.
Shockingly, Gates also suggests people be made to have a digital ID showing their vaccination status, and that people without this “digital immunity proof” would not be allowed to travel. Such an approach would mean very big money for vaccine producers.
On March 24, 2020 Bill Gates gave a highly revelatory 50-minute interview (above) to Chris Anderson. Anderson is the Curator of TED, the non-profit that runs the TED Talks.
The Gates interview is the second in a new series of daily ‘Ted Connects’ interviews focused on COVID-19. The series’s website says that:
TED Connects: Community and Hope is a free, live, daily conversation series featuring experts whose ideas can help us reflect and work through this uncertain time with a sense of responsibility, compassion and wisdom.”
Anderson asked Gates at 3:49 in the video of the interview – which is quickly climbing to three million views – about a ‘Perspective’ article by Gates that was published February 28 in the New England Journal of Medicine.
“You wrote that this could be the once-in-a-century pandemic that people have been fearing. Is that how you think of it, still?” queried Anderson.
“Well, it’s awful to say this but, we could have a respiratory virus whose case fatality rate was even higher. If this was something like smallpox, that kills 30 percent of people. So this is horrific,” responded Gates.
“But, in fact, most people even who get the COVID disease are able to survive. So in that, it’s quite infectious – way more infectious than MERS [Middle East Respiratory Syndrome] or SARS [Severe Acute Respiratory Syndrome] were. [But] it’s not as fatal as they were. And yet the disruption we’re seeing in order to knock it down is really completely unprecedented.”
Gates reiterates the dire consequences for the global economy later in the interview.
“We need a clear message about that,” Gates said starting at 26:52.
“It is really tragic that the economic effects of this are very dramatic. I mean, nothing like this has ever happened to the economy in our lifetimes. But … bringing the economy back and doing [sic] money, that’s more of a reversible thing than bringing people back to life. So we’re going to take the pain in the economic dimension, huge pain, in order to minimize the pain in disease and death dimension.”
However, this goes directly against the imperative to balance the benefits and costs of the screening, testing and treatment measures for each ailment – as successfully promulgated for years by, for example, the Choosing Wisely campaign – to provide the maximum benefit to individual patients and society as a whole.
Even more importantly, as noted in an April 1, 2020 article in OffGuardian, there may be dramatically more deaths from the economic breakdown than from COVID-19 itself.
“By all accounts, the impact of the response will be great, far-reaching, and long-lasting,”
Kevin Ryan wrote in the article. Ryan estimated that well over two million people will likely die from the sequelae of the lock-downs and other drastic measures to enforce ‘social distancing.’
Millions could potentially die from suicide, drug abuse, lack of medical coverage or treatment, poverty and lack of food access, on top of other predictable social, medical and public-health problems stemming from the response to COVID-19.
Gates and Anderson did not touch on any of those sequelae. Instead, they focused on rapidly ramping up testing and medical interventions for COVID-19.
Gates said at 30:29 in the interview that he and a large team are moving fast to test anti-virals, vaccines and other therapeutics and to bring them to market as quickly as possible.
The Gates Foundation and Wellcome Trust with support from Mastercard and now others, created this therapeutic accelerator to really triage out [candidate therapeutics]…You have hundreds of people showing up and saying, ‘Try this, try that.’ So we look at lab assays, animal models, and so we understand which things should be prioritized for these very quick human trials that need to be done all over the world.”
The accelerator was launched March 10 with approximately $125 million in seed funding. Three days later Gates left Microsoft.
Not long before that, on January 23, Gates’s organization the Coalition for Epidemic Preparedness Innovations (CEPI) announced it will fund three programs to develop COVID-19 vaccines. These are the advancing of DNA-vaccine candidates against MERS and Lassa fever, the development of a “‘molecular clamp’ platform” that “enables targeted and rapid vaccine production against multiple viral pathogens,” and the manufacture and Phase 1 clinical study of an mRNA vaccine against COVID.
“The programmes will leverage rapid response platforms already supported by CEPI as well as a new partnership. The aim is to advance nCoV-2019 vaccine candidates into clinical testing as quickly as possible,” according to a news release.
Then at 32:50 in the video, Anderson asked whether the blood serum from people who have recovered from a COVID infection can be used to treat others.
“I heard you mention that one possibility might be treatments from the serum, the blood serum of people who had had the disease and then recovered. So I guess they’re carrying antibodies,” said Anderson. “Talk a bit about that and how that could work and what it would take to accelerate that.”
[Note that Anderson did not ask Gates about, instead, just letting most of the population – aside from people most vulnerable to serious illness from the infection, who should be quarantined — be exposed to COVID-19 and as a result very likely recover and develop life-long immunity. As at least one expert has observed, “as much as ninety-nine percent of active cases [of COVID-19] in the general population are ‘mild’ and do not require specific medical treatment” to recover.]
“This has always been discussed as, ‘How could you pull that off?’” replied Gates. “So people who are recovered, it appears, have very effective antibodies in their blood. So you could go, transfuse them and only take out white cells, the immune cells.”
However, Gates continued, he and his colleagues have dismissed that possibility because it’s “fairly complicated – compared to a drug we can make in high volume, you know, the cost of taking it out and putting it back in probably doesn’t scale as well.”
Then a few seconds later, at 33:45, Gates drops another bomb:
We don’t want to have a lot of recovered people […] To be clear, we’re trying – through the shut-down in the United States – to not get to one percent of the population infected. We’re well below that today, but with exponentiation, you could get past that three million [people or approximately one percent of the U.S. population being infected with COVID-19 and the vast majority recovering]. I believe we will be able to avoid that with having this economic pain.”
It appears that rather than let the population be exposed to the virus and most develop antibodies that give them natural, long-lasting immunity to COVID-19, Gates and his colleagues far prefer to create a vast, hugely expensive, new system of manufacturing and selling billions of test kits, and in parallel very quickly developing and selling billions of antivirals and vaccines.
And then, when the virus comes back again a few months later and most of the population is unexposed and therefore vulnerable, selling billions more test kits and medical interventions.
Right after that, at 34:14, Gates talked about how he sees things rolling out from there.
Eventually what we’ll have to have is certificates of who’s a recovered person, who’s a vaccinated person […] Because you don’t want people moving around the world where you’ll have some countries that won’t have it under control, sadly. You don’t want to completely block off the ability for people to go there and come back and move around. So eventually there will be this digital immunity proof that will help facilitate the global reopening up.”
[Sometime on the afternoon of March 31 the last sentence of this quote was edited out of the official TED video of the interview. Fortunately, recordings of the complete interview are archived elsewhere.]
In the October 2019 Event 201 novel-corona virus-pandemic simulation co-sponsored by the Bill & Melinda Gates Foundation, the World Economic Forum and a division of the Johns Hopkins Bloomberg School of Public Health, a poll that was part of the simulation said that 65% of people in the U.S. would be eager to take a vaccine for COVID-19, “even if it’s experimental.”
This will be tremendously lucrative.
Vaccines are very big business: this Feb. 23 CNBC article, for example, describes the vaccine market as six times bigger than it was 20 years ago, at more than $35 billion annually today, and providing a $44 return for every $1 invested in the world’s 94 lowest-income countries.
Notably, the Bill & Melinda Gates Foundation – which has an endowment of $52 billion – has given more than $2.4 billion to the World Health Organization (WHO) since 2000, according to a 2017 Politico article. (While over the same time frame countries have reduced their contributions to the world body, particularly after the 2008-2009 depression, and now account for less than one-quarter of the WHO’s budget.) The WHO is now coordinating approximately 50 groups around the world that are working on candidate vaccines against COVID-19.
The Politico article quotes a Geneva-based NGO representative as saying Gates is “treated liked a head of state, not only at the WHO, but also at the G20,” and that Gates is one of the most influential people in global health.
Meanwhile, officials around the world are doing their part to make sure everyone social distances, self-isolates and/or stays locked down.
For example, here’s Toronto’s Medical Officer of Health, Dr. Eileen de Villa, at her and Toronto Mayor John Tory’s March 30 press briefing:
“We find ourselves in the midst of a global pandemic. We should expect some more people will get sick – and for some, sadly, will die. This is why it is so important to stay at home to reduce virus spread. And to protect front-line workers, healthcare workers and our essential workers, so they can continue to protect us. People shouldn’t have to die, people shouldn’t have to risk death taking care of us because others won’t practice social distancing or physical distancing.”
Yet look how close Ontario’s Chief Medical Officer of Health, Dr. David Williams, is sitting to Haley Chazan, Senior Manager, Media Relations, for Christine Elliott, Deputy Premier and Minister of Health of Ontario.
This was on Friday, March 27, just before the start of that day’s daily press conference by Dr. Williams and Ontario’s Associate Medical Officer of Health Dr. Barbara Yaffe:

They were sitting two seats, or just a couple of feet, apart. A short time later Chazan got up and stood even closer to Dr. Williams for a little while:

Dr. Williams and Chazan do not live together. Rather, Dr. Williams very likely knows – just as Gates knows – that there is little if any reason to worry about being in close contact with other people unless you or they are vulnerable to developing a severe illness from COVID-19. He surely knows, also, that if you contract COVID-19 and you’re otherwise healthy you’ll very likely have few symptoms, if any, and recover quickly. And that this exposure in fact is beneficial because in the process you will develop antibodies to the virus and have natural, long-lasting immunity to it.
Yet in the March 27 press conference, just like all the others he has participated in during the COVID-19 crisis, Dr. Williams lectured the public about maintaining social distancing. He told people not to go outside on the coming weekend to enjoy the nice weather because, otherwise, they might walk past someone and not be two metres apart.
Dr. Williams is among the large cadre of powerful officials who’ve crashed the global economy by forcing tens of millions of small- and medium-sized businesses to close in the name of the need for forced, severe, social distancing and lock-downs.
They’ve shattered society, suspended most civil liberties and prohibited most activities and connections that keep people mentally and physically healthy. At the same time the officials have prioritized COVID-19 care over everything else and, as a result, severely limited billions of people’s access to life-saving healthcare services ranging from acquiring medication and blood transfusions to having organ transplants and cancer surgeries.
Rosemary Frei has an MSc in molecular biology from a faculty of medicine and was a freelance medical journalist for 22 years. She is now an independent investigative journalist in Canada. You can find her recent detailed investigative analysis of COVID here.
Facebook deletes 120,000-member group where people posted stories of alleged adverse vaccine reactions
By Tom Parker – RECLAIM THE NET – April 23, 2021
Facebook has removed a popular, rapidly growing group where members would post stories about alleged negative COVID-19 vaccine side effects.
The group, “COVID19 VACCINE VICTIMS AND FAMILIES,” had over 120,000 followers when it was shut down and had been gaining more than 10,000 followers per week.
The shutdown of the page follows Facebook introducing a ban on a wide range of claims about the coronavirus vaccine in February. The list of prohibited claims includes claims that the vaccines cause blood clots and claims that the coronavirus vaccines change people’s DNA (something that even Facebook CEO Mark Zuckerberg told Facebook staff during a July 2020 internal meeting).
Not only is Facebook restricting a wide range of vaccine-related claims but it’s also adding labels to all posts about coronavirus vaccines. These labels state that vaccines are safe and direct users to sources that Facebook has deemed “authoritative” such as the World Health Organization (WHO).
Facebook’s actions are similar to those of other Big Tech platforms which have also cracked down on vaccine-related conversations over the last few months. YouTube prohibits videos that go against the WHO “consensus” on coronavirus vaccines and adds information panels to some videos that direct viewers to the WHO and the Centers for Disease Control and Prevention (CDC). Twitter also bans “harmful misleading” posts about vaccines.
Politicians have actively encouraged this Big Tech crackdown on vaccine skepticism. Days ago, Democrats pushed Facebook and Twitter to “address” 12 prominent vaccine skeptics. State Attorneys General also told Facebook and Twitter to kill vaccine skepticism earlier this month.
These crackdowns on vaccine skeptic conversations come amid mass pushes from global governments to introduce digital vaccine passports that force people to prove their vaccination or test status to enter business premises.
Featured Video

Iran Blockade Complications
or go to
Aletho News Archives – Video-Images
Book Review
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
Blog Roll
 Aletho News
Aletho News- Left in Disbelief: Israel in Panic over Hezbollah FPV Drone Nightmare
- Trump Taps Israel Lobbyist From Mossad Cutout FDD To Join Iran Negotiations
- Trump’s Blockade Snatches Defeat from the Jaws of Victory
- Geopolitics and Geoeconomics of the Strait of Hormuz
- Mali: a new front in the Western war on multipolarism
- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- COVID Conniving Receives First Federal Indictment
- Iran Blockade Complications /Lt Col Daniel Davis & Nima Alkhorshid
- Pirates of Mediterranean: Israel does as it pleases in the Sea of Three Continents
- Minab children massacre not ‘unfortunate situation’ but ‘heinous war crime’: Tehran
- If Americans Knew
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
