CDC director gives misleading testimony to Congress
Walensky misled Congress on vaccine effectiveness against viral transmission and on Cochrane review of face masks
BY MARYANNE DEMASI, PHD | APRIL 20, 2023
This week, CDC director Rochelle Walensky provided witness testimony to the House Committee on Appropriations responsible for overseeing the funding of various federal programs related to labour, health, education, and other related agencies.
But serious questions have been raised about the veracity of Walensky’s testimony.
Congressman Andrew Clyde (R-Ga) asked Walensky if her March 2021 public statement on MSNBC, in which she unequivocally said that “vaccinated people do not carry the virus, they do not get sick” was accurate.
“At the time it was [accurate]” Walensky replied confidently.
She then proceeded to explain, “We’ve had an evolution of the science and an evolution of the virus” and that “all the data at the time suggested that vaccinated people, even if they got sick, could not transmit the virus.”
However, there was no such evidence at the time and it prompted criticism from scientists who said there weren’t enough data to claim that vaccinated people were completely protected or that they could not transmit the virus to others.
One of those critics was Jay Bhattacharya, professor of health policy at Stanford University School of Medicine.
“Back then, Walensky didn’t know if it was true. It was just an irresponsible use of a bully pulpit as a CDC director to say something that she did not know for certain to be true at the time,” said Bhattacharya.
“Unfortunately, people used that information to discriminate against unvaccinated individuals and would certainly have been used as fuel for very destructive policies like vaccine mandates,” he added.
Notably, only days after Walensky made that statement to MSNBC, a spokesperson from her own agency had to walk back the comments saying, “Dr Walensky spoke broadly in this interview” adding that it was possible for fully vaccinated people to get COVID-19.
Walensky missed the memo
Walensky should have known that when mRNA vaccines were first authorised in 2020, the FDA listed critical ‘gaps’ in the knowledge base. One of them was the vaccine’s unknown effectiveness against viral transmission.
Also, in Pfizer’s and Moderna’s original pivotal trials, there were 8 and 11 people respectively, who developed symptomatic COVID-19 in the vaccine group, proving the vaccines never had absolute effectiveness, like Walensky had claimed.

Several months later, the FDA’s evaluation stayed the same. In a clinical review, the FDA wrote, “remaining uncertainties regarding the clinical benefits of BNT162b2 in individuals 16 years and older, include its level of protection against asymptomatic infection and transmission of SARS-CoV-2, including for the delta variant.”
Even today, the FDA remains clear that efficacy against transmission is unproven. The FDA’s website states, “While it is hoped this will be the case, the scientific community does not yet know if Comirnaty will reduce such transmission.”
Walensky says Cochrane summary ‘retracted’
Another astonishing falsehood made by Walensky was her response to Congressman Clyde’s question about the Cochrane review which found that wearing face masks in the community “probably makes little to no difference” in preventing viral transmission.
Walensky enthusiastically stated, “I think its notable, that the Editor-in-Chief of Cochrane, actually said that the summary of that review was…[stumble]..she retracted the summary of that review and said that it was inaccurate.”
However, the summary of the review was not retracted, nor have the authors of the review changed the language in the summary.
Misleading statements by New York Times columnist Zeynep Tufekci has likely led to this falsehood being repeated (which I cover in a previous article).
In response to Walensky’s comments, Tom Jefferson, lead author of the Cochrane study said, “Walensky is plain wrong. There has been no retraction of anything.”
“It’s worth reiterating that we are the copyright holders of the review, so we decide what goes in or out of the review and we will not change our review on the basis of what the media wants or what Walensky says,” remarked Jefferson.
Bhattacharya was also stunned by Walensky’s comments. “It’s irresponsible for her to claim that the Cochrane review [summary] was retracted when it was not. It damages her credibility and harms the scientific process, which requires public officials to be honest about scientific results,” he said.
Did Walensky lie to Congress or is she poorly informed?
Witnesses at these hearings are expected to provide truthful and accurate information to the committee and may be subject to legal penalties if they provide false information or knowingly make false statements.
But will Walensky be held accountable for misleading Congress? Unlikely.
The Novelty of mRNA Viral Vaccines and Potential Harms: A Scoping Review
By Peter A. McCullough, MD, MPH | Courageous Discourse | April 19, 2023
We all have the tendency to paint issues with a broad brush. That is to see things one way for intellectual simplicity. “All pharmaceuticals are bad” or “I don’t trust any vaccine.” It is even more tempting to take a negative view on all new technology when the product launch in humans fails to a large degree.
These old mental saws could apply to mRNA vaccines. Halma et al have published a scoping review of lipid nanoparticle-mRNA products with fair balance causing the reader to consider future possibilities. The COVID-19 vaccines are known to be unsafe for several reasons: 1) the Wuhan Spike protein damages cells, tissues, organs, and causes blood clotting, 2) the lipid nanoparticles may have toxicity from the PEG or polysorbate 80 or from syncytia formation, 3) the mRNA appears to be resistant to ribonucleases and is not broken down in the body. As some point the mRNA or fragments could interfere with gene function or alter other microRNAs that are managing the human genome.

Halma, M.T.J.; Rose, J.; Lawrie, T. The Novelty of mRNA Viral Vaccines and Potential Harms: A Scoping Review. J 2023, 6, 220-235. https://doi.org/10.3390/j6020017
The Halma paper points out that safe mRNA products are possible. For example, properly designed mRNA coding for normal proteins that are deficient or ones that are sufficiently humanized and not recognized by the body as foreign could indeed become part of the future pharmacopeia. But there is no doubt that the first use of mRNA on a mass, indiscriminate scale has been a disaster with the COVID-19 vaccine campaign.
The Emergency is Dead – Long Live the PREP Act
The Naked Emperor’s Newsletter | April 19, 2023
Did you think the Covid emergency was over? President Biden certainly did.

But the Public Readiness and Emergency Preparedness (PREP) Act didn’t get the memo. On Friday, Secretary Becerra at the US Department of Health & Human Services (HHS) announced that he intends to amend the declaration under the Act for medical countermeasures against COVID-19.
So instead of repealing the Act, parts of it are to be extended – never let a good crisis go to waste, even if it’s the end of the crisis.
The PREP Act declaration deals with vaccines, tests and treatments and provides flexibilities and protections to individuals and entities involved in providing them. This includes liability protections for entities engaged in manufacturing, distribution or administration of these Covid countermeasures.
The announcement says that even once vaccines, tests and treatments move away from being distributed under a US Government agreement and they transition to traditional pathways, the PREP Act still won’t automatically terminate.
So what will remain even after the “emergency” has finally ended?
- Coverage for Covid vaccines, seasonal influenza vaccines and Covid tests. Immunity from liability will be extended until December 2024 to pharmacists, pharmacy interns and pharmacy technicians to administer Covid and flu jabs (to over 3s) and Covid tests, regardless of any government agreement or emergency declaration;
- Federal agreements related to the provision of Covid countermeasures (including vaccines and treatments) will also be extended until December 2024;
- There will be no impact on government distributed Covid countermeasures;
- Coverage for prescribing and dispensing of Covid-19 oral antivirals will not change. This includes liability immunity for dispensing Covid treatments such as Paxlovid and Lagevrio; and
- There will be no change to the “test to treat” program.
They’ve managed to extend the crisis that has just ended to at least December 2024, more than another year and a half – bravo! And they’ve managed to sneak in flu vaccines as part of the emergency as well.
I just can’t think why they would have to extend liability immunity of these products for so long? (sarcasm).
Oh and unvaccinated non-citizens still won’t be able to travel to the US, even once the emergency is over.
Once the power-hungry politicians seize power they just can’t seem to let it go.
Doubled Pregnancy Loss Rate, Raised Foetal Abnormality Rate and Concentration of Lipid Nanoparticles in Ovaries – How Could They Call This Vaccine ‘Safe’?
BY ALEX KRIEL AND DR DAVID BELL | THE DAILY SCEPTIC | APRIL 14, 2023
The mRNA vaccines were released globally in early 2021 with the slogan ‘safe and effective’. Unusually for a new class of medicine, they were soon recommended by public health authorities for pregnant women. By late 2021, working age women, including those who were pregnant, were being thrown out of employment for not agreeing to be injected. Those who took the mRNA vaccines did so based on trust in health authorities – the assumption being that they would not have been approved if the evidence was not absolutely clear. The role of regulatory agencies was to protect the public and, therefore, if they were approved, the drugs were safe.
Recently, a lengthy vaccine evaluation report sponsored by Pfizer and submitted to the Australian regulator, the Therapeutic Goods Administration (TGA) dated January 2021 was released under a Freedom of Information request. The report contains significant new information that had been supressed by the TGA and by Pfizer itself. Much of this relates directly to the issues of safety in pregnancy and impacts on the fertility of women of child-bearing age. The whole report is important, but four key data points stand out:
- The rapid decline in antibody and T cells in monkeys following a second dose;
- Biodistribution studies (previously released in 2021 through an FOI request in Japan);
- Data on the impact of fertility outcomes for rats;
- Data on foetal abnormalities in rats.
We focus on the last three items as, for the first point, it is enough to quote the report itself: “Antibodies and T cells in monkeys declined quickly over five weeks after the second dose of [Pfizer Covid vaccine] BNT162b2 (V9), raising concerns over long term immunity.” This point indicates that the regulators should have anticipated the rapid decline in efficacy and must have known at the outset that the initial two dose course was unlikely to confer lasting immunity and would, therefore, require multiple repeat doses. This expectation of failure was recently highlighted by Dr. Anthony Fauci, former director at the U.S. NIH.
The three remaining items should be a major cause for concern with the pharmaceutical regulatory system. The first, as revealed in 2021, involved biodistribution studies of the lipid nanoparticle carrier in rats, using a luciferase enzyme to substitute for the mRNA vaccine. The study demonstrated that the vaccine will travel throughout the body after injection and is found not only at the injection site but in all organs tested, with high concentration in the ovaries, liver, adrenal glands and spleen. Authorities who assured vaccinated people in early 2021 that the vaccine stays in the arm were, as we have known for two years, not being honest.
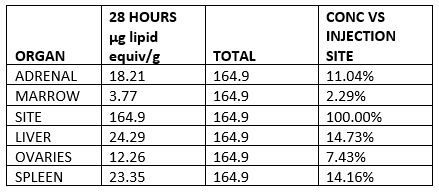
Lipid concentration per gram, recalculated as percentage of injection site.
In terms of the impact on fertility and foetal abnormalities, the report includes a study of 44 rats and describes two main metrics, the pre-implantation loss rate and the number of abnormalities per foetus (also expressed per litter). In both cases the metrics were significantly higher for vaccinated rats than for unvaccinated rats.
Roughly speaking, the pre-implantation loss ratio compares the estimated number of fertilised ova and the ova implanted in the uterus. The table below is taken from the report itself and clearly shows the loss rate for vaccinated (BNT162b2) is more than double the unvaccinated control group.

In a case control study, a doubling of pregnancy loss in the intervention group would represent a serious safety signal. Rather than take this seriously, the authors of the report then compared the outcomes to historical data on other rat populations – 27 studies of 568 rats – and ignored the outcome because other populations had recorded higher overall losses. This range is shown in the right hand column as 2.6% to 13.8%. This analysis is alarming as remaining below the highest previously recorded pregnancy loss levels in populations elsewhere is not a safe outcome when the intervention is also associated with double the harm of the control group.
A similar pattern is observed for foetal malformations with higher abnormality rate in each of the 12 categories studied. Of the 11 categories where Pfizer confirmed the data are correct, there are only two total abnormalities in the control group, versus 28 with the mRNA vaccine (BNT162b2). In the category which Pfizer labelled as unreliable (supernumerary lumbar ribs), there were three abnormalities in the control group and 12 in the vaccinated group.
As with the increased pregnancy losses, Pfizer simply ignored the trend and compared the results with historical data from other rat populations. This is very significant as it is seen across every malformation category. The case control nature of the study design is again ignored, in order to apparently hide the negative outcomes demonstrated.
These data indicate that there is no basis for saying the vaccine is safe in pregnancy. Concentration of lipid nanoparticles in ovaries, a doubled pregnancy loss rate and raised foetal abnormality rate across all measured categories indicates that designating a safe-in-pregnancy label (B1 category in Australia) was contrary to available evidence. The data imply that not only was the Government’s ‘safe and effective’ sloganeering not accurate, it was totally misleading with respect to the safety data available.
Despite the negative nature of these outcomes, the classification of this medicine as a ‘vaccine’ appears to have precluded further animal trials. Historically, new medicines, especially in classes never used in humans before, would require a very rigorous assessment. Vaccines, however, have a lower burden of proof requirement than ordinary medicines. By classifying mRNA injections as ‘vaccines’, this ensured regulatory approval with significantly less stringent safety requirements, as the TGA itself notes. In fact, these mRNA gene therapy products (to use the proper term) function more like medicines than vaccines in that they modify the internal functioning of cells, rather than stimulating an immune response to presence of an antigen. Labelling these gene therapy products as ‘vaccines’ means that, as far as we are aware, even today no genotoxicity or carcinogenicity studies have been carried out.
This report, which was only released after a FOI request, is extremely disturbing as it shows that authorities knew of major risks with mRNA COVID-19 vaccination while simultaneously assuring populations that it was safe. The fact that mainstream media have (as far as we are aware) completely ignored the newly released data should reinforce the need for caution when listening to the advice of public health messaging regarding COVID-19 vaccination.
Firstly, it is clear that regulators, drug companies and the Government would have known that vaccine induced immunity tails off very rapidly, with this being subsequently observed in real world data with efficacy against infection falling to zero. Accordingly, the single point in time figures of 95% and 62% efficacy against symptomatic PCR-positive infection quoted for Pfizer and AstraZeneca respectively meant almost nothing since a rapid decline was to be expected. Similarly, the concept of a two dose course was inaccurate as endless boosters would likely have been required given the rapid decline in antibodies and T-cells observed in the monkeys.
Most importantly, the data do not in any way support the ‘safe’ conclusion with respect to pregnancy; ‘dangerous’ would be much more accurate. The assurances of safety were, therefore, completely misleading given the data disclosures in the recent freedom of information release. Regulatory authorities knew that animal studies showed major red flags regarding both pregnancy loss and foetal abnormalities, consistent with the systemic distribution of the mRNA they had been hiding from the public. Even in March 2023, it is impossible to give these assurances, given the fact that important studies have not, to the best of our knowledge, been done. Pfizer elected not to follow up the vast majority of pregnancies in the original human trials, despite high miscarriage rates in the minority they did follow. Given all of the problems with efficacy and safety, the administration of these products to women of childbearing age and administration to healthy pregnant women is high risk and not justified.
Alex Kriel is by training a physicist and was one of the first people to highlight the flawed nature of the Imperial Covid model; he is a founder of the Thinking Coalition which comprises a group of citizens who are concerned about Government overreach. David Bell is a public health physician with a PhD in population health and formerly worked as a scientific and medical officer at the World Health Organisation.
U.S. Approves First 3 COVID Vaccine Injury Claims — And Pays Out a Total of $4,634.89
By Brenda Baletti, Ph.D. | The Defender | April 13, 2023
The U.S. government approved its first three payments to people injured by COVID-19 vaccines — amounting to a total of $4,634.89.
The Health and Resources Service Administration (HRSA) vaccine injury claims report, updated monthly, shows one $2,019.55 payment for anaphylaxis and two payments — $1,582.65 and $1032.69 — for myocarditis.
The payments were made through HRSA’s Countermeasures Injury Compensation Program (CICP).
The CICP was established under the Public Readiness and Emergency Preparedness (PREP) Act, which protects pharmaceutical companies from liability for injuries sustained from “countermeasures,” such as vaccines and medications, administered during a public health emergency.
Since 2010, when it approved its first claim, the program has compensated a total of 33 claims for vaccine injuries — but these are the first awards for COVID-19 vaccines.
“These long-awaited awards were overdue, highly anticipated and speculated upon,” said Kim Mack Rosenberg, acting general counsel for Children’s Health Defense (CHD). “What is remarkable is that less than $5,000 was paid — total. This is a tragedy that highlights the severe limitations of the program.”
CHD Acting President Laura Bono called the payouts for myocarditis “insulting,” given that mortality rates increase to 50% within five years of diagnosis.
Bono said:
“The CICP is a pathetic, government-run program that gives complete liability protection to the very industries profiting from the COVID vaccine or product. While victims linger with their injuries, paying out-of-pocket for expenses, or at worst die, the industries run to the bank.”
Since the start of the pandemic, people claiming injuries related to COVID-19 vaccines and other countermeasures submitted 11,425 requests for compensation.
Of those, only 19 have been declared eligible for compensation and are undergoing a “medical benefits review” to determine payment.
The anaphylaxis case had been pending medical benefits review since the fall of 2021, and the two myocarditis cases had been pending review since January.
During the medical benefits review, HRSA determines any costs remaining after insurance, workers’ comp, disability or other reimbursements or payments.
Wayne Rohde, an expert in vaccine injury compensation, wrote on his Substack that given the “18+ months to review previous medical benefits that may have been awarded to the injured party [the anaphylaxis case], this process tells me it was a major injury that resulted in very large medical bills.”
Myocarditis is a serious condition that also requires a lot of medical attention, Rohde said.
To date, there have been 1,541,275 reports of adverse events following COVID-19 vaccination submitted to the Vaccine Adverse Event Reporting System (VAERS).
How does vaccine injury compensation work? the VICP and CICP
HRSA, which operates under the U.S. Department of Health and Human Services (HHS), administers two vaccine injury compensation programs: the National Vaccine Injury Compensation Program (VICP) and the Countermeasures Injury Compensation Program (CICP).
The VICP is a special, no-fault tribunal housed within the U.S. Court of Federal Claims that handles injury claims for 16 common vaccines on the childhood vaccination schedule. To date, it has awarded more than $4 billion for medical bills, lost wages, lawyer fees, and pain and suffering to thousands of people for vaccine injuries.
The program does not currently cover COVID-19 vaccine injuries. Should COVID-19 vaccines be moved into the program, any injuries would be handled by the already overwhelmed VICP.
The CICP, the only program that covers COVID-19 vaccine injuries at this time, is even less equipped to deal with them, Rohde told The Defender.
“For COVID-19 vaccine-injured people, the CICP is the worst place, it’s the worst option,” Rohde said, “because it is not really a compensation program, it’s a reimbursement program for medical costs.”
The CICP allows individuals to claim compensation only for unreimbursed medical expenses — meaning those not fully reimbursed by insurance or government programs, such as Medicaid — for death and for lost wages up to $50,000.
According to the Centers for Disease Control and Prevention, under the CICP:
“Eligible individuals may be compensated for certain reasonable and necessary medical expenses and for lost employment income at the time of the injury. Death benefits may be paid to certain survivors of covered countermeasures recipients who have died as a direct result of the covered countermeasure injury.
“The U.S. Department of Health and Human Services is the payer of last resort. Therefore, payments are reduced by those of other third-party payers.”
“There’s no pain and suffering here, there’s nothing,” Rohde said.
Because the CICP reviews and resolves claims through an administrative rather than a judicial process, no details other than the amount of the payments have to be shared with the public.
“It’s designed to be very convoluted, very non-transparent,” Rohde said.
The CICP was known for its cumbersome claims process and low likelihood of success for claimants even before the pandemic. Since then, it has seen unsustainable growth.
According to HRSA’s numbers, of the 11,941 claims filed with the CICP since 2010, nearly 11,000 of them are still under review.
The HRSA budget for COVID-19 vaccine injury compensation will increase in fiscal year 2023 — from approximately $1 million to $5 million — and its budget for staffing and contractors will jump from $5 million to $9.5 million.
How would COVID vaccine injury compensation change under the VICP?
For vaccine injury claims to be covered under the VICP rather than the CICP, three requirements must be met:
- The vaccine needs to be recommended for routine administration for children and/or pregnant women.
- It needs to have an excise tax imposed upon it through the legislature.
- There needs to be a notice of coverage published in the federal record.
The COVID-19 vaccine was added to the childhood immunization schedule earlier this year — but the next two steps in the process have yet to be completed and public health officials have not indicated when this might happen.
The National Academies of Science, Engineering, and Medicine met for three days last month — behind closed doors, except for a two-hour public comment period — to review the epidemiological, clinical and biological evidence on adverse events associated with COVID-19 vaccines.
The committee will generate a report that will be used to add injuries to the federal Vaccine Injury Table, which lists known adverse events associated with existing vaccines.
This list helps the VICP and the CICP decide whether to compensate vaccine injury claims.
At the National Academies meeting, Professor Renee Gentry, director of the Vaccine Injury Litigation Clinic at The George Washington University Law School, told the committee the stakeholders that created the VICP — vaccine manufacturers, lawyers and parents — set it up to be petitioner-friendly, informal, generous and non-adversarial.
But instead, she said, HHS has been “unrelenting” in its opposition to recognizing vaccine injuries.
“I believe the VICP as it exists today would be unrecognizable to those original stakeholders,” she said.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Biden Administration is sued, accused of pressuring Twitter to censor journalist Alex Berenson
By Dan Frieth | Reclaim The Net | April 13, 2023
Independent journalist Alex Berenson has filed a lawsuit against President Joe Biden, a Pfizer board member, and others for pressuring Twitter to ban his account.
His account was banned after posting a tweet questioning COVID-19 vaccines.
Initially, Twitter resisted the calls to ban Berenson. However, eventually the social media platform caved to the pressure.
Berenson sued Twitter in a federal court in California, accusing the company of violating its contract with him. The lawsuit resulted in a settlement and Twitter admitting it should not have banned him.
The defendants in the new lawsuit, filed on April 12, are President Biden, Surgeon General Vivek Murthy, former White House COVID-19 official Dr. Andrew Slavitt, Pfizer board member Dr. Scott Gottlieb, Pfizer CEO Albert Bourla, and the White House Director of Digital Strategy Rob Flaherty.
In a meeting with Twitter, Slavitt and other White House officials asked why Berenson had not been “kicked off” Twitter. Slavitt has previously called Berenson a conspiracy theorist.
Flaherty recently said that he remembered Slavitt “expressing his view that Twitter was not enforcing its content guidelines with respect to Alex Berenson’s tweets, and that employees from Twitter disagreed with that view.”
Gottlieb also asked Twitter to suspend Berenson. He has also previously called for the suspension of other people, including former acting FDA commissioner Dr. Brett Girior.
In the offending tweet, Berenson wrote, “It doesn’t stop infection. Or Transmission. And we want to mandate it? Insanity.”
According to his lawsuit, the defendants violated his First Amendment rights.
We obtained a copy of the complaint for you here.
“The government Defendants specifically targeted Mr. Berenson’s constitutionally protected speech and journalism,” the suit states.
“Members of [the Biden] administration engaged in a nearly unprecedented conspiracy to suppress Mr. Berenson’s First Amendment rights.
“Through 2021, they—and a senior board member at Pfizer, Inc. which has made more than $70 billion selling COVID-19 vaccines—worked together to pressure Twitter to suspend Mr. Berenson’s account and mute his voice as a leading COVID-19 vaccine skeptic. The White House and the Biden Administration did this at the same time government officials promoted their views on the necessity of COVID19 vaccination on Twitter, effectively blocking Mr. Berenson from commenting on their own statements or making his own.”
It adds that the permanent suspension “harmed both Mr. Berenson and a clearly identifiable class of nearly 100 million Americans whose interests he helped represent—Americans who either had questions about the vaccine or did not want to be forced to take a shot that they feared had been rushed through development and lost its ability to prevent COVID-19 infections within months.”
The suit is asking the court to stop the government from targeting the journalist and to award him damages.
Bad Pfizer Vaccine Batches Account for 4.2% of doses but 71% of Serious Adverse Events
Explains Why Some Have Severe Side Effects and Others Do Not
By Peter A. McCullough, MD, MPH | Courageous Discourse | April 13, 2023
I am routinely asked: why are so many people who took the COVID-19 vaccines apparently fine while others are suffering heart damage, strokes, blood clots and are ending up disabled or dead? It has been suspected for many months that there may be variations in vaccine lots or batches that could partially explain these observations. In other words, not everyone is getting the same dose of mRNA.
Under Emergency Use Authorization, the vaccine companies and their subcontractors do not have any inspections of the final filled and finished vials. This is unprecedented for a widely used product of any type. It is possible that lipid nanoparticles aggregate in suspension and so some batches may contain more mRNA than others. Likewise, since lot size has varied over time, it is possible that contaminants from the manufacturing process may be concentrated in some smaller lots compared to larger ones. Finally, there may be product transport, storage, and use factors that denature mRNA including heating, air injected into vials, and multiple needles dipped into the suspension.
The contaminant issue came to light as Japan returned millions of doses when visible debris was seen in the bottom of the vials. Additionally, since metallic beads are used by the biodefense contactors, it is possible that smaller initial lots could have had magnetic debris that explained “magnetism” in the arm where the shot was given as reported early in the vaccine campaign.
A report from Schmeling and coworkers using Pfizer BNT162b2 mRNA COVID-19 vaccine found that 71% of serious adverse events came from 4.2% of doses (high risk batches) conversely <1% of these events came from 32.1% of doses (low risk batches). The variation explained for the high and moderate risk batches was 78 and 89%, respectively. Thus as more doses were given out of those vials, the greater the number of side effects were reported. This means that the majority of risk is in the shot and not the person who received it.

Schmeling, M, Manniche, V, Hansen, PR. Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Eur J Clin Invest. 2023; 00:e13998. doi:10.1111/eci.13998
These are critically important results. They imply the COVID-19 vaccine debacle is indeed a product problem and not due to patient susceptibility in most circumstances. Additionally, the lack of inspections has led to a safety disaster. Some unfortunate patients are getting too much mRNA, contaminants, or both and thus are exposed to damaging and in some cases, lethal injections.
Reuters Aug 2021, Japan suspends 1.6 mln doses of Moderna shot after contamination reports
World Vaccine Congress: A Report From the Belly of the Beast

Photo credit: @vaccinenation/Twitter
By Madhava Setty, M.D. | The Defender | April 11, 2023
Last week I attended the 23rd World Vaccine Congress in Washington, D.C. — which bills itself as “The Most Important Vaccine Event of the Year”:
“Our event format allows for whole-sector topics, giving an opportunity for people to find out more about their specific area of research and their job-function. By running parallel niche conference channels over the 3 days, it increases the relevance of the whole event for everyone who attends.
“During the sessions you will learn how cutting-edge research efforts can be integrated with
-
- Pharma
- Biotech
- Academia
- Government
“to produce more and better vaccines to the market.”
More than 3,100 people, largely from the pharma and biotech industries and regulatory affairs, attended the event.
Keynote speakers included prominent figures from public health agencies, including Peter Marks, M.D., Ph.D., director of the Center for Biologics Evaluation and Research (CBER) at the U.S. Food and Drug Administration (FDA); various directors of research at BioNTech and Moderna; and academic bigwigs like Peter Hotez, M.D., Ph.D., dean of the National School of Tropical Medicine and co-director of Texas Children’s Hospital Center for Vaccine Development at Baylor College of Medicine (my own alma mater).
During the three full days of the conference, neither I nor Dr. Elizabeth Mumper encountered another physician presently in clinical practice.
The event was open to anyone willing to pay the entry fee, which started at $495 for students and went up to $1,000+. But from what I could tell, this was largely a gathering of big and small pharma, biotech and leaders in regulatory affairs.
General impressions
- The majority of attendees truly believe they are doing the right thing.
- The majority of attendees look no further than recommendations from agencies of public health to guide their opinions. In other words, they fully believe COVID-19 mRNA (and other) vaccines are exceedingly safe and have saved millions of lives.
- Beyond members of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) and officers from the UK Health Security Agency (UKHSA), few, if any, are aware of vaccine trial and post-marketing observational data around COVID-19 vaccine safety and efficacy.
- The keynote speakers and expert panel moderators who raised the topic of “vaccine hesitancy” were dismissive of those who managed to avoid vaccination and were openly contemptuous of those who encouraged others to do the same.
- Except for a few instances, the tone of the presentations and round table discussions were collegial. Aside from the pointed questions that Mumper and I were able to pose, there were no open hints that any of the attendees questioned the conventional narratives around the COVID-19 pandemic response.
- One-on-one exchanges revealed encouraging signs that not everyone there has bought the conventional narratives around the pandemic.
- Calls for public-private “partnerships” were a common theme.
I was able to attend only a fraction of the hundreds of presentations and panel discussions during the conference. Below I summarize the most important points from the sessions I attended and key conversations I had with the presenters.
Note: Throughout this article I have quoted myself and others. I do not have access to any audio or video recordings from the sessions, if there are any. Quotations are paraphrased from my own recollection and are not to be taken verbatim.
Introduction to the conference: Anti-vaxxers are dangerous, expect annual COVID vaccinations
Dr. Gregory Poland, director of vaccine research at the Mayo Clinic, delivered the opening remarks. He then moderated a panel discussion with Marks; Paul Burton, chief medical officer at Moderna; Isabel Oliver, chief scientific advisor transition lead at UKHSA; and Dr. Penny Heaton, vaccines global therapeutic area head, Johnson & Johnson.
This first session was possibly the most fascinating 90 minutes of the entire week. Poland, I learned in a brief conversation with him after the conference, is also a pastor. His oratory skills were on full display during his opening and closing remarks. He also is vaccine-injured.
In February 2022, Poland reported suffering from significant tinnitus after receiving the second dose of “an mRNA vaccine.” At the time, Poland described his symptoms as “extraordinarily bothersome.” Nevertheless, he chose to receive a third dose (monovalent booster).
Poland’s commentary on the COVID-19 mRNA vaccines was extremely positive. He said the rapid deployment of the new therapy saved millions of lives and would have saved millions more if it weren’t for the disturbing trend of growing vaccine hesitancy.
I assumed that his vaccine-induced tinnitus had resolved over the last year. It was only at the end of the conference, several days later, when he told me personally that his symptoms were still debilitating, making his unmitigated support of these products even more astonishing.
Poland set the tone for the four-day conference in the first 10 minutes. In his mind, the COVID-19 pandemic was halted through the hard work of our regulatory agencies and the remarkable products borne of the mRNA platform.
The only failure came in the form of “inexplicable” vaccine hesitancy, a phenomenon driven by anti-vax pseudoscientists who are profiting from spreading baseless, fear-driven propaganda.
Combatting vaccine hesitancy is as big a challenge as protecting the world from the next deadly pathogen. Indeed, a significant portion of the events focused on strategies to dismantle the troubling “anti-vaxxers.”
Marks supported Poland’s position that the vaccine-hesitant are irrational, “It’s crazy that they don’t get how great vaccines are,” he said. “I am past trying to argue with people who think that vaccines are not safe.”
I found this remark to be particularly disquieting. What is it going to take for the director of the FDA’s CBER to reassess the safety profile of the mRNA shots?
The panelists expressed shock that some states (Idaho and North Dakota) are considering bills making the administration of COVID-19 mRNA vaccines illegal.
“How can we get the public to understand that science is iterative?” Heaton asked. “COVID vaccines save lives!”
Poland responded: “Can we get an amen?!!”
Marks, flanked by his partners — I mean counterparts — in industry let the audience know what the future would look like. “I am not going to hold my breath waiting for a sterilizing vaccine, protecting against severe disease is enough,” he said.
Marks predicted COVID-19 vaccines would be administered annually or even biannually.
He noted that the challenge will be to identify the strain of interest in June so that we can have a vaccine by September. A 100-day turnaround is possible as long as we have manufacturing ready to go, he said. Heaton (J&J) and Burton (Moderna) nodded in response.
To summarize, leaders of the vaccine industry and the regulatory agencies are, in my impression, convinced that they have offered the world an amazing product and are frustrated that it is not being readily and universally accepted.
They cited the fact that although 70% of Americans received the primary series, only 15% have chosen to receive the bivalent booster that became available in September 2022.
The reluctance of the public to accept the shot, they think, is due to the perceived reduction of threat of the disease, which can be overcome by “proper messaging.”
Of course, the public is correct. The pathogenicity of the strains now circulating is less than the original ancestral strain from 2020. The possibility that reduced uptake could be linked to a poor safety profile was never mentioned.
In their minds, vaccine injuries and serious adverse events are extremely rare. Their incidence has been exaggerated by anti-vax rumor mills. Poland joked that “maybe we should start a rumor that microchips are in ivermectin!”
His rejoinder was met with only sparse, nervous laughter.
Roundtable discussion: ‘Insights and tools to counter vaccine hesitancy’
Though the speakers at the introductory session were clearly entrenched in the “safe and effective” position, they acknowledged that there was a strong and growing swath of the population that was vaccine-hesitant.
More importantly, they were interested in dismantling this movement and not ignoring it. It was an opportunity to engage with them, perhaps in smaller groups or individually. I made my first attempt at a roundtable discussion where people could offer ways to convince the “anti-vaxxers” that they were wrong.
I found myself sitting next to Dame Jennifer Margaret Harries, a British public health physician and chief executive of the UKHSA. The UKHSA has been publishing U.K. health surveillance data with more granularity and frequency than our own Centers for Disease Control and Prevention (CDC).
I let her know that I appreciated the data coming from her agency and that I began following the agency’s regular surveillance reports two years ago. She was grateful for the acknowledgment and appreciated my interest in her work.
It was the UKHSA that offered the first glimpse of negative efficacy of the COVID-19 vaccines in a public dataset in September 2021.
I asked Harries about that and her tone immediately shifted. She said she was aware of no such thing and that she would have to look into it before commenting.
I was surprised by her response. The report from September 2021 wasn’t an aberration. Subsequent reports from the agency over which she presides indicated there was a large and growing incidence of COVID-19 among the vaccinated compared to the unvaccinated.
The UKHSA stopped making that data available several months later. I wanted to know why, but she was unwilling to answer.
I changed tactics and asked her about Tess Lawrie, Ph.D., of the Evidence-Based Medicine Consultancy who notably saw safety signals in the U.K.’s Yellow Card system and, in an open letter in June 2021, urged the director of the Medicines and Healthcare products Regulatory Agency to halt the British vaccination campaign.
Harries looked at me sternly and said, “There are a number of prominent physicians in my country who are gaining fame for their unfounded positions around vaccine dangers, most recently a cardiologist.”
“Do you mean Dr. Aseem Malhotra?”
“Yes. He has gotten a lot of attention of late.”
Harries didn’t think Malhotra or Lawrie held credible opinions, or at least that’s what she told me. It wasn’t easy for me to accept this. We didn’t have a chance to speak about this further. I had another brief interaction with Harries later in the week (see below).
An American pediatrician chaired the roundtable. He opened the discussion with a request for ideas on how to counter vaccine hesitancy.
I had one:
“It’s obvious that the Krispy Kreme doughnuts and travel restrictions are carrots and sticks that have only partially worked. Those that remain hesitant are steadfast in their position because they have looked harder than most.
“They aren’t believing rumors. They are listening to credentialed physicians and scientists who have authored numerous peer-reviewed papers and who happen to be COVID-19 vaccine critics. Why don’t we engage them openly and see what they have to say?”
Katie Attwell, Ph.D., a professor from the University of Western Australia whose interest is in vaccine policy and uptake, shot down that idea. I didn’t know who she was at the time. I did manage to speak with her personally later in the week. Her rebuke was curt and to the point, “We cannot give any voice to the critic,” she told me. “Once the public sees them on equal footing with us they may believe what they are saying.”
Implicit in her strategy is the idea that the public cannot separate information from misinformation. Truth, in her mind, cannot stand on its own. It needs to be identified by those who know better.
Of course, there is another possibility. Perhaps she knows what the truth is and wants to hide it. My initial impressions were that she was earnestly doing her duty to protect the public through whatever means necessary. It would all come down to assessing her breadth of knowledge on the topic.
Chris Graves, the founder of Ogilvy Center for Behavioral Science, supported Attwell’s position. He was a smiling, gregarious fellow, who, I found out later, was hired by Merck to analyze different personality types and value/belief systems among the “anti-vax” camp.

Once a person is properly categorized, “personalized messaging” can be used to bring them back to “reality.” According to the abstract of his study:
“Just as precision medicine treats individuals, this study of 3000 parents (inclusive of all demographics) in the USA sought to identify the most effective personalized messaging to address vaccine hesitancy among parents. First, it sought correlations between: demographics; stated specific reasons for vaccine hesitancy; cognitive biases; cognitive styles; identity-linked worldviews; and personality traits.
“Second, it tested 16 messages in the form of mini-narratives, each embodied with a behavioral science principle, to find if certain messages resonated better than others depending on the many factors above.”
I later asked him how he would respond to someone who looked at the trial and observational data and found that it told a different story about the vaccines’ safety. He smiled, “Oh, those are the ones that have a higher need for cognitive closure. Yes. They are stuck because they cannot move forward if there is any uncertainty.”
Graves couldn’t describe what the “personalized messaging” would look like for this group specifically, only that it existed and had been proven to be more effective than the other types of messaging
I asked him if he was aware of how many reports of adverse events had been registered in the Vaccine Adverse Event Reporting System. “No,” he said, still smiling.
Panel discussion: ‘What vaccines and COVID have taught us about the science of immunology’
The panel included Ofer Levy, M.D., Ph.D., director of the Precision Vaccines Program at Boston Children’s Hospital and VRBPAC member.
This discussion centered around the lack of good biological markers for vaccine efficacy. According to the consensus position of the VRBPAC, antibody levels are not a surrogate for protection.
In other words, an immune response to the vaccine in the form of antibodies should not be used to judge whether the vaccine will do anything useful. Nevertheless, pediatric trials of the original formulation used them as proof of efficacy.
One of the expert panel members was Sharon Benzeno, Ph.D., chief commercial officer of Immune Medicine at Adaptive Biotechnologies, who offered encouraging information. She felt that our approach was too centered on antibody responses and that it would be possible to identify biochemical markers of vaccine-induced cellular immunity in the future.
Levy agreed that this would be an important addition to our fund of knowledge moving forward.
When it came time for questions, I asked the panel:
“As we all know, uptake of the bivalent booster is very low. People are unwilling to subject themselves to another shot because there are no trials that look at outcomes, only immunogenicity, which you yourself are saying is insufficient. Why not insist on trials that can prove an outcome benefit?”
Levy responded that the advisory panel had no say in what kind of studies were required. His advisory committee could only vote yes, no or abstain with regard to approval/authorization.
Another panel member, Alessandro Sette, doctor of biological science, head of Sette Lab and professor at La Jolla Institute for Immunology, piped in, “It wouldn’t be practical. The signal is too small because we are no longer dealing with a non-naive population.”
Sette had taken the bait. He was saying that most people have either been vaccinated or exposed to the virus already. The booster would have little benefit, if any, on a population that was already protected.
I asked the obvious follow-up: “So why then are we insisting that everyone get boosted?”
Harries, the moderator, immediately stepped in, “Okay, we have veered off topic. Next question.”
I was beginning to understand how this conference was being managed. I don’t believe the sponsors of this meeting expected to encounter many probing questions about the quality of the COVID-19 vaccines from the audience who paid for their expensive tickets. When and if they arose, moderators were quick to intervene.
Was it possible that others in the audience saw what was happening? I believe it to be so. Every time I asked a question, people seated near me told me that they appreciated the question and wondered why it went unanswered.
Even a non-scientist from Moderna approached me several times throughout the conference to let me know she agreed that responding to these issues would be the best way to “increase uptake” and that she was planning on forwarding my questions to her scientific staff.
Panel discussion: How does vaccine law impact uptake and access?
This group was moderated by a lawyer, Brian Dean Abramson, “a leading expert on vaccine law, teaching the subject as adjunct professor of vaccine law at the Florida International University College of Law.”
His opening remarks demonstrated his contempt of the vaccine-hesitant:
“We didn’t get to herd immunity because of these anti-vaxxers.
“They are dangerous. In 2021, they received $4 million in donations. It is estimated that in 2022, more than $20 million have been funneled to their movement.”
The panel included Attwell, whose position was clear from her flat response to my suggestion earlier. Her public page indicates that she has received approximately $2 million in funding for her research into increasing vaccine access and uptake.
Attwell is not a physician or a medical scientist. However, also on this panel was a public health physician from Johns Hopkins Bloomberg School of Public Health, Chizoba Wonodi, Ph.D., who has 27 years of experience in Africa, Asia and America.
I was encouraged by the flexibility in the audience from my prior challenges and when offered the microphone, I opened with a more aggressive salvo directed at the moderator:
“‘Anti-vax’ is pejorative and reflects ignorance about who the vaccine-hesitant are and why they believe what they believe. This is further reflected when you insert terms like ‘herd immunity’ with regard to this pandemic. Without a sterilizing vaccine, or even one that can prevent infection, herd immunity is an impossibility.
“Rather than inflaming the situation, why don’t we engage with the doctors and scientists who are vaccine-cautionary and hear their arguments in a fair, open and public discussion?”
Once again, Attwell politely but sternly warned the audience that this would be too dangerous in her opinion. I expected that. And I also was again encouraged that the three people sitting around me acknowledged that my point was valid and that it was puzzling that the panelists would not address the merits of my position.
Afterward, Chizoba approached me and let me know she appreciated my question. In her work, she has found that education is the most important thing. She was kind; she believed that many of the vaccine-hesitant physicians could be reached by providing them with the proper information.
I asked her how she would address a physician who simply felt that authorizing a therapy where the double-blinded trial demonstrated a greater all-cause mortality than the placebo was not only unprecedented but illogical.
She stared at me blankly. “Is this from a new study?” she asked.
I told her that this was from the published interim results from the Pfizer/BioNTech trial, the trial that launched the worldwide vaccination campaign. She was not aware of the results.
To her credit, she admitted that she hadn’t looked at the paper but planned on doing so.
The final day
I attended a session titled “Let’s Talk Shots” where Daniel Salmon, Ph.D., presented the work being done at Johns Hopkins Institute for Vaccine Safety.
“LetsTalkShots is designed to support vaccine decision-making. It shares engaging animated content based on a person’s questions or concerns.”
Suffice it to say that there is a lot of thought, money and energy behind the campaign to vaccinate the public. The approach once again is around targeted messaging, which acknowledges that different people need to hear different types of information.
Attwell also presented to the same audience. In this forum, she pointed out that the U.S. government was more tolerant of the vaccine-hesitant than in her country. She suggested that our religious and philosophical exemptions should be eliminated entirely. Only the strictest medical exemptions should be permitted. This will lead to better outcomes.
After her talk, I approached her. She looked up as if she was expecting me to ask her some questions. I asked her if she would be willing to have a more open conversation about her research and opinions. She was.
I let her know that I thought she was smart enough to realize that I was, in fact, a vaccine skeptic. She nodded her head.
“So,” I said, “the number one disinformation spreader may be running for President of the United States. What do you think should be done?”
She smiled uncomfortably and said, “Yes, it’s going to be hard to keep him from getting oxygen.”
In other words, her proposed approach to suffocate the anti-vax spokespersons becomes much harder when they are running for the highest office in the land. I thought she might be willing to reconsider her strategy. She wasn’t.
I tried a different approach. I explained that in my investigation, I haven’t found enough evidence that the COVID-19 mRNA shots were safe or effective, however, I was open to the possibility that the mRNA platform may eventually prove to be a powerful way to create therapies that are safe and effective in the future.
What good would it be to have this technology if half of the public no longer trusts it or the people who are shoving it down their throats while denying them an opportunity to debate them?
“Yes. That’s a good point.”
I told her that in this country, doctors are unwilling to write religious or philosophical exemptions to COVID-19 vaccines for fear of backlash. Many employers won’t accept them anyway, so her position is moot.
“Yes. That’s true.”
I asked her what would be a cause for a medical exemption. She didn’t know. I explained that medical exemptions are considered valid ONLY if the person has evidence of a prior reaction to an mRNA vaccine or to one or more of the ingredients in them. Nobody but a handful of people on the planet knows what exactly is in these things.
How would a doctor (or anyone else) know whether a given person was at an increased risk for an untoward event?
“I don’t know.”
I asked her if she was aware of the evidence of medical fraud around the Pfizer vaccine trials. She said she read something about it a while ago but didn’t think it was important.
Finally, I asked her why she thought vaccinating everyone was the right thing to do.
“Vaccination rates in my country are higher than in yours and we fared better.”
But there are countries whose vaccination rates are much lower than both countries and mortality rates are even lower. How could she explain that? She couldn’t.
Observations from Dr. Elizabeth Mumper
Mumper attended “Partnering for Vaccine Equity Program,” chaired by Joe Smyser, Ph.D., CEO of The Public Good Projects.
She shared this with me:
“This lecture was about vaccine acceptance and demand, specifically social and behavioral drivers, and how to link action and policy through the use of the social sciences.
“The strategy was to empower community leaders to take public health messages to communities. The research showed that disparities in vaccine acceptance decreased in black and brown communities which had the program. Research shows that now the most vaccine-hesitant are white, rural and right-wing.
“In the program described, they worked with social media influencers (like young women who did beauty blogs) to repeat public health messages to their audiences. They identified 212,700,000 disinformation messages about vaccines, most of which came from the United States.
“In this project, they worked closely with Twitter and facilitated the removal of what they deemed misinformation. They recruited 495 influencers who would share information voluntarily with their followers. As a result, they reached 60 million people.
“They know that so-called ‘anti-vaxxers will not come after social media influencers.’ The program provided training and webinars to educate how to compose effective public health messages.
“This public health social scientist called anti-vaxxers ‘idiots and jerks.’
“During the question and answer period, I said that in my experience, many parents who were vaccine-hesitant were very smart and had advanced degrees. People like doctors and lawyers and engineers knew someone in their family who had an adverse vaccine reaction. I suggested it would be more effective to engage with the vaccine-hesitant and discover what data they are relying on rather than using vitriolic name-calling.
“I am paraphrasing the speaker’s response below. He said, ‘We work upstream. We want to know where they are getting their misinformation. I can call people idiots and jerks if they are giving out misinformation. If you even raise questions like about the HPV vaccine, you will get speaker invitation and book deals. People are getting rich from spreading misinformation. We know what the right information is.’”
Mumper summarized:
“It was profoundly disturbing for me to hear details about how social scientists and public health officials worked directly with Twitter to remove content they deemed to be misinformation. Their assertion ‘that we know what is true’ did not ring true. Their efforts were directed at increasing vaccine uptake in all age groups for which emergency use authorization had been granted.
“The speaker did not seem to take into account the First Amendment rights for free speech of those who posted data questioning the effectiveness of COVID vaccines.
“I was surprised by the vitriolic rhetoric directed at those who reported side effects from the vaccine or who questioned the risk-benefit ratio.
“It was unsettling to hear how public health officials courted social media influencers to spread messages for their followers to get vaccinated. Yet they scrubbed messages from doctors and scientists who posted inconvenient data about COVID-19 vaccines.”
The last question of the symposium
The final day wound down with another plenary session. Once again, Poland moderated a panel of vaccine researchers who discussed how to quickly manufacture more durable vaccines, i.e., ones that would have longer-lasting protection.
One of the researchers made a remarkable observation. Early in the pandemic, prior to vaccine availability, young infants who contracted COVID-19 were found to have robust and enduring immunity by every measure even three years later. Perhaps some clues lay within this interesting cohort.
Mumper saw a great opportunity to pull the rug from under their feet. She said:
“I am a pediatrician in Virginia. I have been shocked at how well my infant patients did with COVID-19. The CDC has told us that the survival rate from COVID-19 is 99.997% in these infants. Now you, too, are telling us that we know these kids have great protection two years after infection.
“I am wondering why I should be pushing these vaccines on a 6-month-old when I don’t have any long-term data on what things like lipid nanoparticles do to babies. So convince me!”
(Laughter from audience.)
Poland to the panelist: “You have 30 seconds to answer.”
(More laughter.)
Panelist: “That would require more time and a bottle of wine.”
(Laughter.)
Panelist: “I don’t think I can answer that question.”
Mumper: “OK, Anybody else?”
Panelist Andrea Carfi, Ph.D., chief scientific officer at Moderna, took a shot at it, pointing out that Mumper is under the “misconception” that long-term effects of COVID-19 are less than that of the vaccines while admitting that he didn’t know what the long-term sequelae of infection were either.
Poland accepted Carfi’s response as sufficient and closed the discussion.
Those sitting next to us once again noted the merits of Mumper’s concern. Moreover, Carfi’s response didn’t resolve the issue at all. If the long-term effects of both the vaccine and the infection are unknown, on what grounds are we pushing the jab on these children?
Final thoughts
This was a rare opportunity to engage with vaccine proponents in their own house on their own terms. In my assessment, their foundation is crumbling and their structure will eventually collapse.
The big players must see this, which is why they are quick to squelch any lines of inquiry that will expose the hypocrisy.
This wasn’t lost on the audience. As I mentioned, some of them were able to realize that simple questions were not met with clear answers.
It is clear to me that the “pro-vaccine” camp is not as monolithic as we often think. There is a spectrum of skepticism amongst them. They also recognize that the vaccine-hesitant range the full continuum from “SARS-CoV-2 virus deniers” to the “wait and seers.”
They have the means to construct sophisticated “information” campaigns that target the vaccine-cautionary with specific messaging.
I suggest we use their model to at least acknowledge that we can be more precise in how we bring them to their senses.
In my first open comment in a roundtable discussion, I summarized the situation as follows:
“There are many people who are vaccine-hesitant that do not have the capacity to read scientific papers and analyze data. They see two groups who are mirror images of each other. Both sides think the other side is incredibly gullible, that they are listening to misinformation spreaders and are endangering the rest of us for their own personal gain.
“They can also see the one big difference between the two. One side is asking for an open discussion around this important issue. The other believes that only their side should have the right to express themselves while the other needs to be silenced.
“How do you think this is going to play out? Why would the undecided ever choose to follow the group that advocates censorship over open debate?”
By refusing to engage us in any meaningful exchange they may be able to bring over a few of the vaccine-hesitant to their side by what can be best described as “conversion therapy.”
However, in the end, their tower will topple because it is not based on logic, the scientific method or the unassailable facts. It relies on censorship of the voices of those who are qualified to speak on the matter to manufacture “consensus.”
It is incumbent on us to decide what should be done to hasten the inevitable emergence of sensibility around this matter.
I am quite certain there are people who know vaccines are causing incalculable harm but advocate their widespread use anyway. A few of them were likely at the conference. They won’t be swayed by open debate, however, they represent only a tiny minority of all vaccine advocates.
I suggest that we begin by not regarding every vaccine proponent as an engineer of mass murder. Most are woefully uninformed. In attempting to achieve herd immunity they have succumbed to herd mentality. They need to be reached.
In my recent experience, I see that it is possible through open dialogue. This is precisely why the engineers of this pandemic and its response want to make sure this never happens. Despite what they say publicly, I don’t think they are worried about the vaccine skeptics remaining hesitant — they are worried about losing members of their own herd to the truth.
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Doctors in Kentucky, California Received Millions in Bonus Payments for Vaccinating Medicaid Patients Against COVID
By Brenda Baletti, Ph.D. | The Defender | April 11, 2023
The federal government and insurers incentivized healthcare providers in Kentucky and California to vaccinate Medicaid patients against COVID-19 by offering bonuses based on the percentage of patients successfully vaccinated.
“[This is] truly sickening and I am embarrassed for my profession by this,” Dr. Meryl Nass, an internist and biological warfare epidemiologist, wrote on her Substack, where she posted several documents relating to the COVID-19 vaccine provider incentive programs.
The documents help to draw a picture of the broader effort at the federal, state and local levels to unleash a range of strategies targeting low-income and people-of-color communities, which tended to have lower vaccination rates.
The strategies included providing hundreds of millions of dollars for the creation of “culturally tailored” pro-vaccine materials and for training “trusted” and “influential messengers” to promote COVID-19 and flu vaccines to communities of color in every state.
Nass’ revelations showed these efforts went beyond advertising, fear campaigns, payments to patients and payments to trusted community actors and included, in some cases, direct financial incentives to healthcare providers.
Kentucky: Medicaid paid doctors up to $250 per vaccinated Medicaid patient
Anthem Blue Cross and Blue Shield Medicaid in Kentucky told physicians in 2021 it would “recognize your hard work by offering incentives for helping patients make the choice to become vaccinated.”
The more people vaccinated, the higher the per-person incentive.
For physicians who treated an Anthem Medicaid cohort with a minimum of 25 patients in their practice, Anthem Medicaid offered incentives for vaccination by Sept. 1, 2021, that ranged from a $20 bonus per vaccinated person for physicians who vaccinated 30% of the cohort, to $125 per vaccinated person for those who vaccinated 75% of the cohort, with several incremental steps in between.
As time went on, the rates increased.
Between Sept. 1 to Dec. 31, 2021, physicians received payments ranging from $100 per newly vaccinated person for those who vaccinated 30% of their patient cohort, to $250 per newly vaccinated person for those who vaccinated 75% of their patient cohort.
In 2022, the Anthem provider incentive program changed to a flat rate. Providers received $50 per newly vaccinated Medicaid patient. This included children ages 6 months to 4 years and kids 12 and older vaccinated between Jan. 1 and Dec. 31, 2022, and children ages 5 to 11 vaccinated between June 1 and Dec. 31, 2022.
Medi-Cal: $350 million in incentives to vaccinate low-income children, people of color
The California Department of Health Care Services (DHCS) on Aug. 6, 2021, announced $350 million in incentive payments — $250 million to providers and $100 million for direct non-monetary payments, such as gift cards, to vaccine recipients — to encourage vaccination among Medi-Cal’s 14 million beneficiaries.
Of the $350 million, $175 million came from state general funds and $175 million from federal funding. The funding period lasted from Sept. 2, 2021, through Feb. 29, 2022.
The program offered incentives to managed care plans in the name of “health equity.” In the press release, DHCS Director Will Lightborne said that raising rates among Medi-Cal beneficiaries was essential because “California will only be safe when everyone is safe.”
Nass noted that this program was rolled out one day after Centers for Disease Control and Prevention Director Rochelle Walensky told CNN the vaccines don’t prevent virus transmission. “That’s clearly a contradiction,” Nass told The Defender.
The funding targeted Medicaid recipients with low vaccine uptake — the homebound, communities of color, youth ages 12 to 25 and people ages 50 to 64 with multiple chronic conditions — and incentivized outreach and vaccination activities for providers and pharmacies.
At the time of the announcement, only 45.6% of Medi-Cal beneficiaries age 12 and over had received at least one dose of the COVID-19 vaccine, compared to over 76% of Californians overall.
The DHCS funding included payments to community-based organizations, food banks, advocacy groups and faith-based organizations. This key strategy of funding grassroots leaders to act as “grassroots” proxies spreading the federal government’s vaccine message was widespread throughout the pandemic.
Providers could also couple this grant with a CAIRVaxGrant, which offered providers up to $10,000 to enter all of their historical electronic health record immunizations into the California Immunization Registry (CAIR).
The grant stipulated that after startup costs, payments would be directly tied to “meeting specific vaccination goals,” similar to the Kentucky program.
The incentive payment structure under the California plan was complex, paying a financial reward to healthcare providers who met particular benchmarks that varied by county and demographic but overall increased the percentage of vaccinated patients among their Medicare beneficiaries.
Under this incentive structure, providers had to meet particular vaccination targets in order to get paid. Those who were especially successful in increasing vaccination rates in the target groups would be entered into a “high performance pool,” receiving extra money for substantially moving the vaccination rates for Medicaid recipients 75% higher than baseline or within 10% of a given county’s general rate.
In the equation that determined the incentive payment structure, different demographic groups were weighted differently. For example, vaccine recipients ages 12 to 25 were weighted more highly than older recipients and those in the two racial/ethnic groups with the lowest uptake were also given greater weight.
By Jan. 21 of this year, despite this $250 million push, Medi-Cal vaccination had only increased to 52.9%.
Medicaid pays doctors more to administer COVID vaccines than other shots
As part of the American Rescue Plan Act, the Biden administration fully funded the COVID-19 vaccination program, making vaccines free regardless of health insurance status.
To cover the costs of the uninsured and underinsured, the Health Resources and Services Administration (HRSA) paid provider costs of vaccine administration through an Uninsured Program and a COVID-19 Coverage Assistance Fund.
Reimbursements were based on national Medicare rates, but the Centers for Medicare & Medicaid Services (CMS), which sets those rates, increased the reimbursement rate over time. Through March 14, 2021, HRSA paid $28.93 for a single-dose vaccine or for the second dose in a series of 2, and $16.94 for the first dose in a series of two.
On March 15, 2021, those rates increased to $40 per dose and $75.50 for an “in-home” dose of the vaccine.
Nass said the initial payments were in line with Medicaid payments for other vaccines, but the increased payment marked a departure from the usual reimbursement structure.
Usually, all CMS changes to Medicare payments for specific services must go through notice and comment rulemaking, but “to save time during the COVID-19 pandemic, the agency bypassed that route before increasing payments for administering the vaccines,” JAMA reported.
CMS said the higher payments were meant to help expand COVID-19 vaccination, supporting “actions taken by providers, such as growing existing vaccination sites, conducting patient outreach and education, and hiring additional staff,” Healthcare Finance News reported.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

Language is a Weapon
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- The 12 Screenings That Manufacture the Patients They Claim to Find
- Iran deputy FM says MoU with US finalized, to be signed in Geneva on Friday
- With one strike, Netanyahu tries to kill two peace deals
- Iran warns ‘no point’ in deal with US if Israel remains unrestrained
- Ukraine as a laboratory of ‘techno-fascism’
- Desperate Starmer choosing piracy as distraction over UK crime crisis – Putin envoy
- If Americans Knew
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- Israel is changing the face of Lebanon, mainstream media is normalizing it – 3 articles
- Genocide lobby benefits from EU anti-racist fund
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
