In the past few weeks, a series of analyses published by highly respected researchers have exposed a truth about public health officials during Covid: that much of the time, they were wrong – writes Dr. Marty Makary in the New York Post. He sets out “10 myths told by Covid experts — and now debunked”. Here are the first four.
Misinformation #1: Natural immunity offers little protection compared to vaccinated immunity
A Lancet study looked at 65 major studies in 19 countries on natural immunity. The researchers concluded that natural immunity was at least as effective as the primary Covid vaccine series.
In fact, the scientific data was there all along — from 160 studies, despite the findings of these studies violating Facebook’s ‘misinformation’ policy.
Since the Athenian plague of 430 BC, it has been observed that those who recovered after infection were protected against severe disease if reinfected.
That was also the observation of nearly every practicing physician during the first 18 months of the Covid pandemic.
Most Americans who were fired for not having the Covid vaccine already had antibodies that effectively neutralised the virus, but they were antibodies that the Government did not recognise.
Misinformation #2: Masks prevent Covid transmission
Cochrane Reviews are considered the most authoritative and independent assessment of the evidence in medicine.
And one published last month by a highly respected Oxford research team found that masks had no significant impact on Covid transmission.
When asked about this definitive review, CDC Director Dr. Rochelle Walensky downplayed it, arguing that it was flawed because it focused on randomised controlled studies.
But that was the greatest strength of the review! Randomised studies are considered the gold standard of medical evidence.
If all the energy used by public health officials to mask toddlers could have been channelled to reduce child obesity by encouraging outdoor activities, we would be better off.
Misinformation #3: School closures reduce Covid transmission
The CDC ignored the European experience of keeping schools open, most without mask mandates.
Transmission rates were no different, evidenced by studies conducted in Spain and Sweden.
Misinformation #4: Myocarditis from the vaccine is less common than from the infection
Public health officials downplayed concerns about vaccine-induced myocarditis — or inflammation of the heart muscle.
They cited poorly designed studies that under-captured complication rates.
A flurry of well-designed studies said the opposite.
We now know that myocarditis is six to 28 times more common after the Covid vaccine than after the infection among 16- to 24-year-old males.
Tens of thousands of children likely got myocarditis, mostly subclinical, from a Covid vaccine they did not need because they were entirely healthy or because they already had Covid.
Dr. Makary blasts the CDC for weaponising research by “putting out its own flawed studies in its own non-peer-reviewed medical journal, MMWR“.
“In the final analysis, public health officials actively propagated misinformation that ruined lives and forever damaged public trust in the medical profession,” he adds.
Worth reading in full.
March 1, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Data continues to emerge according to which not only were the mRNA shots ineffective at preventing infection and transmission of COVID-19, but they may have caused widespread harm to persons cajoled or coerced into undergoing vaccination, despite their own relative invulnerability to the worst effects of the virus. Anecdotal cases abound, but diehard regime narrative devotees continue to dismiss such “incidents”—thousands of which are recorded in the government’s own VAERS (Vaccine Adverse Effects Reporting System) database—as purely coincidental. It is more difficult to downplay reports involving entire cohorts, such as the increased incidence of myocarditis among young males, which the CDC itself has acknowledged. Some critics have suggested that a disproportionately high percentage of pregnant women in Pfizer’s initial trial of the shots suffered miscarriages.
Back in November 2021, in the midst of the widespread and aggressive “Vaccinate everyone!” campaign, I spoke with a woman in Oregon who matter-of-factly mentioned that her (vaccinated) daughter had suffered three recent miscarriages. Recognizing that it was too late to do anything anyway, given that the daughter had already been vaccinated, I did not dare to suggest that her troubles may have been caused by the shots she had no doubt been exhorted by her doctor to take. At that time, following the lead of CDC director Rochelle Walensky, health officials everywhere were in the midst of a marketing blitz according to which COVID-19 vaccination would protect mothers and their babies alike.
I said nothing to the woman in Oregon about the dangers of introducing foreign substances into pregnant women (although I had written about it), but I did naturally wonder at the time whether there might be a causal connection between the poor daughter’s miscarriages and the shots, given the biological activity of the spike protein already known to induce blood clotting and heart troubles. The mother of the young woman—who was pregnant again, for a fourth time—seemed optimistic that somehow there was nothing to worry about, even after three failed attempts to bring a baby into the world. It is possible, I realized then and continue to own, as I must, that the woman was simply unable, for unrelated reasons, to carry a child to term. But given that the biologically active spike protein is what the original virus used to access cells, and production of lots of it was induced by the injected mRNA, it would not take a tinfoil hat conspiracy theorist to surmise that the pregnancies may have been sabotaged by the shots.
Critics such as feminist scholar Naomi Wolf, who early on in the pandemic raised questions about the shot’s safety, given many reports of irregular menstrual cycles in women who under went vaccination, were denounced as purveyors of misinformation and immediately deplatformed by the social media giants. Only recently have such “conspiracy theorists” been permitted to articulate their concerns in the public sphere once again—and only on some platforms, including Twitter, which to Elon Musk’s credit reinstated thousands of accounts shut down for the crime of deviating from the narrative favored by the pharma-government alliance. If the shots are indeed dangerous to fetuses, it is needless to say too late for all of the pregnant women tricked into believing that because the CDC insisted that there was no evidence of risk to them and their offspring, they should therefore roll up their sleeves.
That Pfizer knew all along that their mRNA shots had effects upon women’s hormonal systems was corroborated through Project Veritas’ sting operation involving a Pfizer research director, Jordon Triston Walker. In the recorded interview thought by him to be a friendly conversation with a date, Walker observed that the shots seemed somehow to be affecting the endocrine systems of women. The delicate hormonal balance needed to maintain a pregnancy suggests an immediate connection between the widely reported menstruation irregularities of women and the incidence of miscarriages in some of the initial trial subjects.
The data interpreted by some critics to imply that miscarriage was one of the many possible side effects of the Pfizer shot were made public only recently, with the release of a large trove of court-ordered documents which the company is now required by law to provide, despite its initial insistence that it would take seventy-five years to do so. Setting aside the question of whether miscarriage is in fact a side effect of the shots, the very idea that it would take so many years to make public the documents said to have served as the basis for the FDA’s (Food and Drug Administration’s) decision to grant the Pfizer product Emergency Use Authorization (EUA), so that it could forego the customarily stringent multi-year testing program required of pharmaceutical products more generally, struck many people as absurd.
To my mind, the situation constituted a classic Charybdis and Scylla. If it was humanly impossible to process and assess all of the data (all 451,000 pages of it) in the short period between the creation of the vaccines and December 11, 2020, when the EUA was granted, this could be taken to imply that the persons on the committee incompetently executed their role and indeed based their decision to approve the shots primarily on Pfizer’s obvious wish that they do so. Alternatively, it was always possible to process the documents for publication, and the company’s resistance to doing so was due to the content of the documents themselves, which might harm the ambitious sales program to vaccinate everyone on the planet with the new product.
The director of the CDC, Rochelle Walensky, encouraged pregnant women from the beginning to get the shots, quite deceptively claiming that there was no cause for worry about possible health risks to fetuses. The safety information provided with the original shots itself indicated that pregnant women had been excluded from the initial trials, as they are for most pharmaceutical products. The reason why pregnant women are not included in early stage clinical trials of products intended for the general population is because they represent a special case, given the fragile chemical environment enveloping the fetus. It is a matter of common knowledge that developing human beings are highly sensitive to and often endangered by foreign substances—alcohol and nicotine being two well-documented examples. The vulnerability of fetuses was most notoriously and unforgettably demonstrated when pregnant women were prescribed Thalidomide on the basis of clinical trials which, again, excluded pregnant women. As in the case of the COVID-19 vaccines, Thalidomide was distributed by doctors under the misleading marketing line that there was no evidence that it would harm fetuses. Thalidomide killed thousands of babies and deformed thousands more before it was finally withdrawn from the market.
We now know from Pfizer safety data recently released that some of the women in the initial trial were in fact pregnant—apparently without having known that this was the case at the time, which was why they were not excluded from the trial. The vaccines may or may not have caused their reported miscarriages, but the fact that the CDC would encourage pregnant women, on the basis of nearly no data, to undergo vaccination betrays a reckless disregard and their true goals in injecting everyone everywhere, even members of low risk cohorts, with the mRNA treatment. Ignorance is bliss for pharmaceutical companies, which can continue to market and sell products for years, reaping billions of dollars of profits, before finally halting sales on the basis of widely reported and what come eventually to be undeniable post-launch problems, as in the cases of Vioxx, Belviq, Baycol, etc.
Above and beyond the profit motive was plausibly the desire to test the newfangled mRNA technology on the largest sample of human beings possible—whether or not they actually needed any treatment whatsoever in contending with COVID-19. Of course, if the desire on the part of Pfizer CEO Albert Bourla and Moderna CEO Stéphane Bancel was to make strides ahead in the research and development of other lucrative medications, then the quest for data, too, was ultimately driven by the profit motive—albeit looking forward, to future possible blockbuster drugs.
Certainly, the steadfast resistance, indeed, the outright refusal on the part of public health authorities such as Dr. Anthony Fauci and Dr. Rochelle Walensky, for more than a year after the launch of the COVID-19 vaccines, to acknowledge the relevance of natural immunity in those persons previously infected, and to recommend appropriate adjustments to the U.S. government’s mandates—for both health care workers and military personnel—supports the hypothesis that one of the overarching aims of the aggressive, relentless vaccine campaign was not to save the lives of the small percentage of human beings vulnerable to the virus, but to amass data.
Corroborating this interpretation, according to which the companies hoped not only to reap a windfall of profits but also to collect a huge amount of data, is the explanation by many critics (including Robert F. Kennedy, Jr. and Dr. Peter McCullough) of the assiduous suppression of any and every other therapeutic which the vaccine salespersons recognized would compete with and diminish the uptake of the newly patented products. Most importantly of all, ivermectin and hydroxychloroquine were dismissed and denounced by public health authorities, and ridiculed by parroting pundits throughout the media, because EUA cannot be granted to products when alternative therapies are available.
In his conversation with a Project Veritas reporter, Dr. Jordon Triston Walker also shared the potentially explosive piece of information that Pfizer executives had floated ideas such as mutating the COVID-19 virus so as to be able to develop vaccines preemptively. It was not entirely clear from Walker’s remarks whether the intention would be to release those mutated viruses so as to direct the course of the disease in populations, or simply to predict which variants would pop up on the scene naturally, through mutations of the virus in its effort to self-propagate by evading the antibodies induced by the latest shots.
Pfizer responded to the bombshell revelation by effectively minimizing the story through suggesting that the process described by their (now former, I presume) employee was essentially part of the normal, necessary research conducted in producing, for example, the flu shot each year. Nearly everyone by now is more or less aware that the flu shot is a gamble, involving researchers predicting which strains will be most prevalent and virulent. People who undergo inoculation against those versions may still fall ill because they may or may not come in contact with the predicted dominant strains. Some individuals report anecdotally that they were never more ill than during a year when they opted for the “free” flu shot, which clearly indicates that they encountered versions of the pathogen not expected by the researchers who determined the ingredients for the products distributed during that particular flu season. Unsurprisingly, neither anecdotal reports, nor adverse effects, nor even consistently poor efficacy rates have deterred pharmaceutical firms from pushing for widespread uptake of their mediocre flu shot products in very public and misleading advertising campaigns fronted by government health authorities.
Needless to say, if the intention of Pfizer in mutating the COVID-19 virus was to release it into the human population in order to induce countless numbers of persons to seek protection by purchasing (or obtaining from their government) the “vaccine” developed in order to stop that strain, then that would constitute a flagrant violation of any decent person’s basic sense of ethics. Such a possibility would moreover, and disconcertingly, be taken by some to accrue a degree of plausibility to the conspiratorial notion according to which the original COVID-19 virus was not only a gain-of-function product, created by researchers in a lab, but also intentionally released into the world in order to initiate The Great Reset being promoted by members of the World Economic Forum (WEF), led by Klaus Schwab.
More plausible, I believe, is that Pfizer and Moderna, et al., are primarily focused on the future of their other new mRNA products in the works. It is not at all far-fetched to surmise that the relentless, divisive push to vaccinate everyone everywhere with the first mRNA treatment ever tested on a population of human beings, made possible only by the FDA’s EUA, was spearheaded by companies with much broader goals in mind. The CEOs of these companies have publicly vaunted their plans to use mRNA to cure cancer and other intractable diseases, which in fact best explains their manifest fervor to acquire as much data as possible, by all means necessary. Such a program, albeit less explicitly heinous than creating illnesses in order to be able to sell patented cures for the symptoms caused by them, nonetheless involved using all of the people coerced into undergoing treatments for which they had no need as the means to the companies’ mercenary ends.
Further evidence for this admittedly unsavory interpretation can be seen in the push to vaccinate children, even infants, despite the minimal danger posed to them by the COVID-19 virus. If, in reality, the chances of a child dying from COVID-19 is less than the chance of their being hit by a bolt of lightning, then it is hard to see why anyone would push for uptake under a public health pretext. Yet those who wish to foist the product on young persons, including infants, have continued to press the line according to which the virus poses a serious health risk to everyone, and the vaccine will help to protect children along with their parents, this despite data according to which the protection provided by the shots, even to the vulnerable persons who might be said to benefit, plummets to nothing after only a few months. (Preposterously enough, according to one recent study at the Cleveland Clinic, in the longterm, the more shots one has received, the greater become one’s chances of contracting COVID-19!)
A second reason why children have been important for the product companies is peculiar to the United States, where the PREP Act (Public Readiness and Emergency Preparedness Act) protecting companies from liability in the event of adverse effects covers any product approved as a part of the child immunization schedule. Demonstrating their complete capture by pharmaceutical industry forces, on February 9, 2023, the CDC added the COVID-19 shots to the long list of those recommended in the childhood vaccination schedule (which now includes dozens of shots), thus ensuring the product companies massive profits for years to come through the inoculation of persons not at significant risk from the virus, using a product whose already nearly negligible protective capacity for invulnerable persons (a risk reduction of ~1%—or less) spans less than a few months.
Unbelievably enough, the new CDC recommendation for children (beginning at six months) includes the original COVID-19 vaccine, though the wild strain of the virus may no longer exist, along with booster shots, for which the only clinical trial on human beings is currently underway—on the millions of persons who rolled up their sleeves on the basis of safety data gathered from only animal trials. The results are trickling in on the first-round of “bivalent” booster shots, which have so far been demonstrated to have only middling (30%) efficacy in preventing infection by the variant they are attended to address. But the virus will continue to mutate, thus serving as the pretext for producing new booster formulas. This implies that, under the CDC’s immunization guidelines, each new booster shot will of necessity constitute yet another experimental trial, to be conducted, shockingly enough, upon children throughout the years of their development into adults. In other words, children have been set up to serve as test subjects (i.e., human guinea pigs) for each newly developed “booster” to follow in the future as the virus continues to mutate, despite the fact that they make up the least vulnerable cohort of them all.
Why should “vaccines” which do not offer longterm immunity to anyone and are not even necessary for children—the CDC itself explicitly claims that most children will experience only mild symptoms from COVID-19—be included in the battery of time-tested vaccines such as those against polio, measles, etc.? Along with the desire to sell products, and to be able to test new products on children, is, again, scandalously enough, the fact that the CDC’s addition of the mRNA shots to the children’s immunization schedule protects the manufacturers in perpetuity from lawsuits, even after the State of Emergency has ended. President Biden has announced that the State of Emergency will be lifted on May 11, 2023, two months after the CDC added the COVID-19 shots to the children’s immunization schedule.
Because state and local officials follow the cues of the CDC, we can expect to see its recommendation for childhood inoculation by the COVID-19 shots swiftly transformed into mandates for public school children in states throughout the country. This will likely happen in places such as Massachusetts, California, and New York, where health authorities have persisted in retaining laws which restrict the behavior of residents even as new data continues to refute the erroneous premises widely embraced by officials in the spring of 2020 regarding masks, social distancing, etc. Although states such as Florida rescinded the COVID-19 emergency laws, and have passed legislation to protect children, the fact remains: with the federal level CDC recommendation in place, the product companies will retain their protection from future litigation arising from adverse effects, even if the data currently being collected and analyzed eventually demonstrate widespread harm to either children or adults.
It would be a mistake to judge corporations by the moral standards appropriate to individual persons. Corporations are beholden only to their stockholders, and their sole goal is to maximize profit. But the spokespersons for such companies are themselves individual human beings, as are all of the authorities representing public health organizations whose ostensible raison d’être is to protect members of society, not to maximize the profits of their sponsors. When institutions such as the FDA are coopted by mercenary forces, they cease to perform the function which citizens are depending upon them to execute. Because this already happened in the case of the opioid crisis, the fact that people fell for the trick once again in the case of the COVID-19 “vaccines” is best and perhaps only explained by the fearmongering campaign used to psychologically traumatize them to the point where they lost all critical bearings and agreed to undergo an experimental treatment of which most of them had no need.
Every healthy, nonobese person under the age of seventy who underwent COVID-19 vaccination was deceived into serving as a pro bono experimental subject in a pharmaceutical product trial. That millions of well-meaning parents, believing that they are doing the right thing, will on the basis of the CDC’s addition of the COVID-19 shots to the children’s immunization schedule, enroll their progeny in an entire series of such experimental trials, using substances never before tested on human beings, is nothing less than tragic.
Laurie Calhoun is the author of We Kill Because We Can: From Soldiering to Assassination in the Drone Age, War and Delusion: A Critical Examination, Theodicy: A Metaphilosophical Investigation, You Can Leave, Laminated Souls, and Philosophy Unmasked: A Skeptic’s Critique, in addition to many essays and book chapters.
February 27, 2023
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, COVID-19 Vaccine, FDA, Moderna, Pfizer, United States, WEF |
Leave a comment
The agency must have told some truths, but it’s hard to identify those statements.

Substack All-Star Igor Chudov just published another important article. This article asks if the CDC was lying all along about “vaccine effectiveness?”
My question (and it’s a serious one) is this: Can someone name ONE pronouncement of CDC officials that either wasn’t a lie or of highly-dubious veracity?
Per my assessment, the CDC and other national public health agencies and their key experts …
Lied about there being no evidence of early cases in America.
Lied when they said there was no possibility this virus leaked from a lab.
Lied about the effectiveness of masks.
Lied when they said the virus could be spread on physical surfaces.
Lied when they said it would take only two weeks to “flatten the curve.”
Lied when they said that virus transmission could easily happen outside.
Lied about the stats of “cases” and “deaths.”
Lied about the mortality risk to children and healthy young adults.
Lied about ivermectin and HCQ being worthless drugs for treatment.
Lied about remdesivir being a safe drug.
Lied about the vaccines being “safe and effective.”
Lied when they labeled these shots as “vaccines.”
Lied about the “vaccines” and boosters preventing “severe” cases and deaths.
Lied about the necessity or importance of testing people (including the asymptomatic) over and over.
Lied when they attacked and sought to censor people who were telling the truth.
Lied when they “adjusted” estimates of ILI in the Flu Season of 2019-2020 … to make it seem this flu season did not produce “widespread” and “severe” ILI (Covid?) outbreaks.
Before Covid, lied about the effectiveness of the flu vaccines.
Do liars continue to lie? Will liars lie again?
Do liars often try to cover-up their lies?
Do liars in positions of great power often attack people who try to expose their lies?
Is it smart to continue to trust proven or known liars?
How many lies does some person or agency have to tell before people start to realize they are listening to a liar?
February 27, 2023
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | CDC, Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Three years ago few of us knew the impending storm that was brewing; one that would upend the very fabric of global democracy, destroy whole communities, businesses and families and cause a vast number of children and adolescents to become unmoored and disengage from society, among many other deleterious outcomes.
Perhaps most chilling of all has been the sinister turn in those three years of what was once seemingly a force for good, “public health;” which changed into a punitive and authoritarian entity that wilfully engages in iatrogenesis and the disenfranchisement of those skeptical of the medical-industrial complex through widespread and draconian vaccine mandates.
In retrospect, America in February of 2020 seems like a libertarian, innocent age compared to our current one. We did not live under the shadow of possible nuclear holocaust. Everyday life was devoid of the nanny-state elements of our current age. Many of us had gone through life never quite knowing what the destructive power of a government run amok looked like.
Now we know.
Not only do we once again live under the imminent threat of atomic annihilation, as our global “leaders” continue to play out a 21st-century version of Dr. Strangelove, but Covid offered an opportunity to further militarize and subordinate society. For let’s call lockdowns what they were: martial law.
Moreover, the government and the security state during the last few years has proved itself to be in the service of only a tiny sliver of shadowy and in some cases invisible elites and “experts” whose actions have, in America most especially, been held to little accountability. In the face of lockdowns, which happened to be the most universally undemocratic and destructive event of my lifetime, regular citizens were held in contempt and with little more agency than the serfs of the Middle Ages. Some of us were made completely irrelevant and “non-essential.”
Yet, amongst this wreckage and horror, many skeptical people, who once believed in benevolent leaders, have been freed from the flawed faith in “good” government. In this freedom lie several important lessons for how to move forward into a (hopefully) less totalitarian future.
Lesson #1: We need to hold the medical-industrial complex accountable.
My skepticism about the medical-industrial complex felt inchoate and somehow unfounded pre-Covid. Sure, I knew I’d be given a lecture at every doctor’s appointment about how I needed to schedule colonoscopies (in my early 40s!), buy new medicines, get blood work done, no questions about my holistic well-being, diet, etc. It didn’t matter which doctor I saw, they were all like that. There was always a feeling that these big buildings and office parks that housed the machinery of the medical industrial complex were, like consolidated public schools or prisons, quite anti-human. But I still . . . believed, more or less.
What the Covid mania revealed is that much of the medical-industrial complex, like the military-industrial complex, is part of a system of hierarchical relationships that only truly benefits those in power. The beneficiaries being Big Pharma, massive corporate health systems, wealthy physicians and even a security state/biodefense apparatus that sees vast swaths of the global population as dots on a chart to be manipulated, vaccinated and medicalized.
Even worse, iatrogenesis – the massive health harms caused by Covid medical interventions – generates unseemly and massive profits, again for a tiny segment of individuals with unfathomable power and wealth (Bill Gates is the prime example). This sinister complex relies on sickness, not health to make their profits. I believe this is one reason why Covid was so intensely medicalized and why we all became pawns of the vaccine industry, instead of public health pursuing more holistic attempts for better outcomes for people with Covid.
None of us has to take this lying down, though. Health consumers can take back their rights through the great work of organizations such as the Children’s Defense Fund and No College Mandates, two groups with writers affiliated with Brownstone Institute.
Lesson #2: The “real” American left is not MSNBC and has perhaps vanished entirely
The American liberal-left is a coalition that has deteriorated so far as to be unrecognizable, filled with purity tests, blind obedience to secret service agencies like the FBI, the CIA and shadow organizations in the military like DARPA, with authoritarian leaders who constantly virtue signal and who will censor and cancel those they do not agree with.
For many years, since the late Obama years particularly, I’ve felt more and more out of place within the cultural ideology of the American left, which has placed identity politics above economic fairness, and in many instances is entirely unrecognizable from the “left” of old.
Covid remains the demarcation point–when I and millions of others abandoned the movement entirely.
Nothing about being a cheerleader for lockdowns represented traditional leftist values. In fact, I would argue that the natural place for the American left was to viciously oppose lockdowns, because they so deleteriously affected the working class, working poor, and minorities. And yet the silence on the left in the mid-part of 2020, much to my horror, soon became derision and then full scale hatred toward those of us who proclaimed our opposition to lockdowns, even with reasoned analysis or proposals such as the Great Barrington Declaration.
That we were brutally censored and that all protestations ended up falling on deaf ears was such an alienating experience, many of us who at one time proclaimed to be “of the left” have abandoned the project entirely, and most especially the political party that was supposed to represent us in America, the Democrats. We have emerged politically homeless; some having even established alliances within the welcoming arms of the libertarian and conservative movements.
This begs the question that many of us have pondered: what is the political left now? And what has it always been?
It certainly does not resemble the George Orwell version, which had so much influence on me as a college student. The spirit of the left contained in “The Road to Wigan Pier,” for instance, feels like a world gone by, infused as it was with a healthy skepticism, admiration and reverence for the working classes, and the mutually supportive ideas of liberty and egalitarianism. Such humility and nuance have almost wholly disappeared from our current rendition of “leftism.”
Some of us have even wondered (and indeed Orwell pondered the same thing): does leftism, if unchecked, always loop into something horrendous, the inevitable conclusion not being utopia but the graveyards of Cheong Ek or tendentious, censorious authoritarianism?
Does dialectical materialism only go down one road in the end, and that toward Stalinism or fascism?
Yet, despite the loneliness of becoming a dissenter within one’s old political home, the complete destruction of what used to be “left” and in some instances “right” political spheres is in itself freeing. Many of us are carving out new political identities and in some cases new political parties and alliances are forming. This outcome will ultimately be very healthy for the future of democracy.
Lesson #3: We have proof that “experts” are often wrong.
A healthy skepticism of the “experts” and elites has always been a hallmark of American life, especially out here in the provinces where I reside. Yet, as Christopher Lasch pointed out in Revolt of the Elites and the Betrayal of Democracy – the last book he published and maybe most prescient – many American elites and professional “experts” have now completely abandoned their advisory roles to become de facto rulers in themselves, worshiped in almost a religious sense by a segment of completely secularized, well-to-do liberals. These elites, however, mostly hold contempt toward the working and middle class. This has been happening for quite some time (Lasch’s book was published in 1996).
The most egregious recent example of this worship and the power of the 21st century technocrat is embodied by the former Director of NIAID, Anthony Fauci, who was the public face of the disastrous Covid response for nearly three full years. The myopic reverence for this man is dangerous on many levels, but it also showcases a grave weakness of modern humanity; many of us will give up even the most basic freedoms because we blindly trust a technocratic “savior” who just may have all the wrong data or simply be a mendacious, cunning bureaucrat.
Yet, before Covid many of us, including myself, trusted unelected bureaucrats like Fauci far too often with little questioning of their motives. Lockdowns showed their hand and tipped the balance toward egregious authoritarianism. Unelected administrative-state actors should not have any ability to create policy by fiat, and groups such as the NCLA are fighting many of the unconstitutional edicts pushed forward by the Centers for Disease Control and Prevention and the NIH as part of the Covid response.
Lesson #4: The technology that was supposed to lessen inequality actually increases societal rifts.
The modern worship of technology has created an undemocratic information ecosystem rife with inequity, which helped smooth the way for authoritarian and coercive lockdown policies. In fact, with the aforementioned DARPA heavily involved in the Covid response and Big Tech gaining nearly unfettered power during the pandemic, technology’s tentacles are lodged in every classroom, courthouse and boardroom across the country. It seems likely that the architecture for future lockdowns is now firmly in place.
We should never, at any moment moving forward, accept this as our future. The Western world imitated China’s brutal, authoritarian lockdowns because digital technology facilitated it. These policies would have been impossible as little as 25 years ago.
And in the end it was all a sham.
Millions still had to keep the sewers clear, emergency services running, the lights on and our grocery stores stocked. Working class people, many of whom were rightly skeptical of the Covid vaccine, and who subsequently lost their jobs because of the illegal vaccine mandates, were completely ignored by the laptop class who were able to work from home. In the midst of receiving endless curbside deliveries, virtue signaling on social media about “anti-vaxxers,” and sidelining those who actually had to leave their homes and work for a living, Big Tech only fueled the culture wars and ultimately hurt the working class.
Lesson #5: The most meaningful things are still the most meaningful things.
If we cannot trust the experts, the government, the global order, or technology, who can we trust? This is perhaps the most important question of all, and one that has been asked from time immemorial. In intense readings of Leo Tolstoy’s non-fiction work during this strange and awful time, especially Patriotism and Government and The Kingdom of God is Within You, I’ve come to realize that in the very act of trusting monolithic institutions or the state in general, we are looking for all the wrong answers and even perhaps asking the wrong questions.
For, like all of the material world, institutions are fallible and crumble. The right questions are much larger and far more personal, and the answers are immutable and have been there forever.
Outside the bounds of our fallible institutions, the most important answers to nearly every question are to be found in authentic feelings of love and belonging. Love for your family, or the little plot of land and house that you own, or the tiny farming community that you live in, the church you belong to, or the group of kind-hearted and supportive friends and writers, like those who have found one another in Brownstone Institute and other grassroots communities.
Faceless federal institutions and their representatives do not deserve our love, nor in most cases do they deserve even admiration or respect. They are the products of very flawed, uncaring systems and are ultimately artificial creations of a flawed humankind.
Despite the anguish and pain we have all felt–and the divisions the last three years of authoritarianism have created–don’t let the elites and their petty politics divide your friendships and family. Love is still the ultimate answer.
Seth Smith is an avid outdoorsman and public librarian based in Missouri.
February 25, 2023
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Supremacism, Social Darwinism, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
In retrospect, it was surprisingly easy. Here are some of the key features that explain what happened to our world.
For almost three years I’ve been researching Covid topics. Based on this deep dive, I feel qualified to offer opinions on the question of how all the events of the last three years actually materialized.
Stated differently, how did all of this madness actually happen?
I quickly identified several big themes or pivotal events that help explain how so many nonsensical and harmful policies became a reality.
Readers can identify other features that that were important in getting us to where we are today. As always, feedback is appreciated and welcome.
Note: “They” = public health officials, establishment authority figures and leaders, myriad vested interests who were all “on the same page” when it comes to Covid policies and narratives.
They sold fear … hard, incessantly, shamelessly, brazenly, unapologetically.
In short, hyper fear of a novel (and “deadly”) virus was THE prerequisite for everything that followed. So how was this mass fear/panic actually produced?
The groundwork must have begun many months and years before the “Wuhan outbreak.”
Multiple “table top” exercises (like Event 201) were conducted to lay the groundwork for what would follow.
All the key “stakeholders” were recruited to participate in these events, often organized by groups like the Bill and Melinda Gates Foundation. Politicians, bureaucrats, key media members, physicians, scientists, and representatives of all they key agencies and key organizations were recruited and then participated in these exercises.
Main-Takeaway: Advance “buy in” had already been achieved regarding the key premises of these table-top planning exercises. An event like Covid-19 had already been predicted and this was the blueprint for dealing with this … if you were going to be a part of the enlightened group that was going to help save the world.
Significantly, no participants ever questioned any of the assumptions built-in to these exercises and when Covid was announced nobody wanted to challenge any of the responses.
Appeals to authority, groupthink, wanting to support the “current thing” (to protect your status and career advancement opportunities) helped ensure that no significant dissenting voices would come forward to thwart or block the agreed-upon course of action.
Logistical and legislative actions had already been implemented to ensure nothing or no one could block the response. “Emergency orders” of bureaucrats trumped the need for legislative votes, which were not even required to implement policies that turned the world upside down.
It now seems that the Department of Defense played a larger role (than most realized) in making the key decisions.
Still, Fauci, Birx (a former military doctor), and Collins played a large role in orchestrating policy and getting the president to go along with their recommendations.
At some point, China’s response – locking down parts of their country – was endorsed as the bold and effective solution that should be used everywhere. The outbreak in northern Italy helped create more fear.
I’ve written many articles about “early spread.” However, one of the key planks explaining how what happened in America actually happened was the wide-spread belief that “late spread” of this virus was occurring.
That is, the virus had not yet spread through America (and other countries) and thus it was wise and proactive to implement draconian lockdowns and non-pharmaceutical interventions to slow or stop the spread of the virus. The public was told that that they could “flatten the curve” with just two weeks of inconvenience.
Significantly, nobody in official capacity or the mainstream press ever questioned whether the virus may have already spread throughout much of the country or the world (even though case of Influenza like Illness were rampant in many sections of the country/world).
Organizers of the response, per their table top exercises and research, knew that physicians were among the “most trusted” people in the world. Officials quickly got all the leading medical associations to sign off on the grave threat.
Once the physicians groups were on board, the guidance or marketing became “listen to your physicians.”
The vast majority of leading scientists also quickly came on board … perhaps because they knew going against Anthony Fauci would jeopardize their future research grants.
No one in the mainstream press ever questioned the doomsday scenarios and indeed actively promoted the “this-must-be-done” narrative.
Censorship and cancellation of dissenting voices slowly and then rapidly became a priority. All social media, Big Tech companies and legacy media companies implemented “misinformation” guidelines that had rarely if ever been utilized.
Seeding, funding and establishing “misinformation” experts had actually begun months or years earlier. Almost all at once, these disinformation gurus sprung into action, further muzzling any significant “push back” against the authorized narrative.
I think a key event, rarely mentioned or remembered, was the decision of the Ivy League to cancel its conference basketball tournament in early March. The Ivy League is supposedly a repository of the brightest minds in the world. Once the Ivy League did this, the NBA and other organizations (The PGA cancelled a big golf tournament after one round) quickly followed. The dominoes started to fall and the momentum was set in motion.
Lesson: Be wary of the actions of the Ivy League or elite colleges.
The federal government actually could not compel any citizen, state or city to comply with its “guidance” but this didn’t matter as governors and mayors almost all at once implemented their own, more specific, lockdown orders. Or: They simply followed the federal “guidance.”
In retrospect, it’s quite fascinating that almost 100 percent of state and local officials “signed off” on such draconian mandates. It’s also worth noting that Gov. Ron DeSantis, the one prominent politician who did challenge the narrative, became a political superstar almost overnight.
To make it more likely that hospitals and medical clinics signed off on the various treatment guidelines and protocols, the federal government came up with numerous financial incentives (payouts) to get the hospitals and doctors to go along with their program. So hospitals received extra money for treating a Covid patients or if someone was placed on a ventilator.
Congress enacted emergency funding to mollify many groups that might otherwise have suffered economic damages. New money was printed out of thin air. State governments were compensated for implementing the federal program.
Media organizations began to receive advertising funding for promoting Covid safety and, later promoting the vaccines.
Mandatory masking was ordered, which further promoted the requisite fear of the virus.
All big companies signed off on the proposals even while many of their smaller competitors were put out of business, which was fine with the big guys.
Somehow the churches put up no resistance. No meaningful organization put up any resistance.
How did the organizers get virtually 100-percent compliance from all key stakeholders? The answer is found in psychological and sociological reasons: Nobody in a “leadership” role wanted to be a contrarian as this would be dangerous to their careers.
“We are all in this together” was the implied or explicit message. This was a great event in history (like fighting WWII) and the only way to defeat the “enemy” (the virus) was for all citizens to act together … and do what the experts said must be done. In other words, comply.
The fear was ramped up to a new level thanks to 40 to 45-cycle PCR tests suddenly flooding the market (as well as mandatory testing).
The media daily reported “new cases” and “new deaths,” most of which probably weren’t caused by this novel coronavirus.
It was rarely if ever mentioned that the average age of death of a Covid victim was around 82 – which is at or beyond the average life expectancy.
Anyone who questioned the narrative was met with a rejoinder that “XXX,000” people have already died. Unspoken was the fact very few people personally knew one person under the age of 60 who had died, and these official deaths “from” Covid were massively inflated.
In late March 2020 through April 2020 massive spikes of deaths in certain cities like New York City, New Orleans and Detroit received massive media coverage.
Receiving virtually no media attention was the hundreds of other hospitals that were almost ghost towns.
The lockdowns lasted many months (even years) in some states … not “two weeks.”
Nobody questioned why the check-out girls at the “essential” super markets were not becoming casualties of Covid even though they came in close contact with hundreds of customers every day and touched every item the customer had put in their buggies.
At some point, the narrative (pushed by the experts) became that the only thing that would stop or end this pandemic was mass vaccination … so people just had to hold on until Pfizer and Moderna saved the world and ended the pandemic.
The vaccines arrived in “warp speed” and the world got a non-stop dose of this is a “pandemic of the unvaccinated” stories.
People were fired for not getting vaccinated or pressured into getting vaccinated (although after the non-stop fear campaign, 75 percent of the country was rushing to their pharmacy to get their shots). Plus, all the medical experts recommended this and everyone trusted their doctors.
At some point, officials no longer needed to pressure the public into “fighting Covid.” Citizens took up the charge themselves. America became an “us against them” society – and the skeptics were the mangy dog “thems.”
When people continued to get sick or infected after vaccination, the narrative became the shots lowered the likelihood you’d have a “severe case.”
The fact the vaccines did not work as advertised actually didn’t damper enthusiasm for the vaccines at all. The Covid vaccines became the only product in world history that was a colossal bust – but still generated record sales and demand.
A spike in “all-cause” deaths began days, weeks or months after the roll-out of the vaccines, but these spikes in deaths were either not reported or were blamed on Covid. Never mentioned was that the vaccines were supposed to make Covid deaths an impossibility.
The “narrative” that the vaccines were “safe and effective” – probably repeated a billion times – was never challenged by anyone in official capacity. In many states and cities, the lockdowns and restrictions were never challenged.
In a nutshell, Project Massive Fear worked.
All the key stakeholders “bought in.” Even if some people eventually realized some of the narratives may have been dubious or false, they’d already risked their reputations and careers by zealously pushing or endorsing these narratives … so they weren’t going to suddenly admit they might have been wrong.
In retrospect, how “they” made all the madness happen was surprisingly easy.
February 25, 2023
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
New lawsuits have been filed against an array of Community Medical Centres in California over their covid care protocol…
Gilead’s Remdesivir is a drug that has received a lot of criticism, and rightly so.
Prior to the pandemic, the World Health Organisation rejected its use due to poor trial studies abroad. NIAID-sponsored trials had likewise documented troubling issues. Reported adverse events were significant:
In short, a plethora of studies indicated it had potentially bizarre and fatal effects depending on the patient’s health. Patients who had a multi-organ impairment, for example, exhibited detrimental impacts on their renal function after the drug was administered. The FDA, nonetheless, granted its use under Emergency Use Authorisation (EUA) when a study showed it reduced COVID hospitalisation duration by 4 days.
From that point on, Remdesivir became part of every COVID-19 protocol across the country. Reports from 2020 have since revealed that if a vulnerable patient (aged 65 and over) came into a medical centre and tested positive, Remdesivir was the treatment most likely to be offered. That patient would then be placed or declared in the ICU as an inpatient.
Here is where the story turns very sinister.
According to local sources in California, hospitals that took on inpatient complex cases could charge up to 144x more than an outpatient case. As soon as they treated these patients within their facilities, they could apply for reimbursement from Medicare. In other words, there was a clear financial incentive for hospitals to “over-treat” patients to maximise profits.
With these reports now circulating, 14 Californian residents living in the Fresno area have filed lawsuits against various medical centres. These include Community Regional Medical Center, Clovis Community Medical Center, and St. Agnes Medical Center.
One plaintiff’s claim about a medical centre’s covid protocol is particularly reprehensible:
“A patient comes to the hospital often for problem unrelated to COVID-19. They are told they have COVID-19 or ‘COVID pneumonia’. They are immediately separated from their loved ones, and usually declared to be in ICU, even though they are often just placed in room. They are told that the deadly Remdesivir is the only available and safe treatment. They are usually told that if they leave the Hospital against ‘medical advice’ they will void their insurance. They are placed on BiPap machine at high rate, making it difficult for them to breathe. Their hands are often tied down so they can‘t take the BiPap machine off their face. After their hands are tied down, and sometimes before, [a] psychiatrist comes to the room and determines that they are ‘agitated.’ This results in the protocol patient being placed on morphine or something similar. Sedating the patient makes it more difficult for them to communicate and more difficult for them to fight the effects of Remdesivir especially as it relates to their ability to breathe….”
All the lawsuits are being funded by the Arizona-based medical advocacy nonprofit Truth For Health Foundation. The organisation is run by Elizabeth Lee Vliet MD. Currently, the three aforementioned lawsuits will return to court for case management in January.
Note: These claims do not concern ‘End-Of-Life Care Protocols’. They concern COVID care protocols in general. We’ve seen similar claims made in the UK regarding Midazolam but again this concerned ‘End-Of-Life’ care. These lawsuits could well lift the thickly-blackened veil (for the wider masses) on the medical industry’s capacity to treat patients like cattle.
February 23, 2023
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, Gilead, Human rights, remdesivir, United States |
Leave a comment
Immunity acquired from past COVID-19 infection provides strong, lasting protection against severe outcomes from the illness at a level “as high if not higher” than that provided by mRNA vaccines, according to a study published Thursday in The Lancet.
Researchers conducted a systematic review and meta-analysis of 65 studies worldwide, providing overwhelming evidence to support what many scientists, doctors and studies have said since early in the COVID-19 pandemic.
“The Lancet is finally acknowledging what doctors and scientists have been gaslit for saying for years — that natural immunity provides superior protection to experimental vaccines,” said Robert F. Kennedy, Jr., chairman and chief litigation counsel for Children’s Health Defense.
“Only the tsunami of propaganda and censorship from the pharma/government biosecurity cartel and the controlled media persuaded the public that Pfizer and Moderna were better at protecting the human immune system than God and evolution,” he added.
The study found that immunity acquired from infection was often far more robust and consistently waned more slowly than the immunity from two doses of an mRNA vaccine.
The researchers found that natural immunity was at least 88.9% effective against severe disease, hospitalization and death for all COVID-19 variants 10 months after infection.
It also provided 78.6% protection against reinfection for all variants except omicron BA.1, for which protection was 45.3%.
At an October 2022 Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices meeting, the CDC presented data showing that vaccine-acquired immunity after two or three injections dropped to zero six months after injection, and then became negative.
The Lancet study stated that “although protection from reinfection from all variants wanes over time, our analysis of the available data suggests that the level of protection afforded by previous infection is at least as high, if not higher than that provided by two-dose vaccination using high-quality mRNA vaccines (Moderna and Pfizer-BioNTech).”
The study was funded in part by the Bill and Melinda Gates Foundation. Authors included Dr. Christopher Murray, director of The Institute for Health Metrics and Evaluation, the Gates-funded institute that was “largely responsible for the notoriously exaggerated mortality calculations that overestimated COVID deaths by 20-fold at the COVID pandemic’s outset,” according to Kennedy.
The authors argued, based on their findings, that natural immunity should be recognized along with vaccines when authorities are considering restricting travel, access to venues and work based on immunization status.
Commenting on these conclusions, Dr. Meryl Nass, internist and epidemiologist, said:
“While framing this as an acknowledgment that natural immunity confers protection, what it is also doing is providing tacit agreement that government-imposed policies restricting travel are acceptable. It furthermore provides tacit approval of vaccine passports.”
The ‘cartel’s’ war on natural immunity
In October 2020, The Lancet published an article — “Scientific consensus on the COVID-19 pandemic: we need to act now” — by authors including CDC Director Rochelle Walensky, which was widely covered in the mainstream press. They stated that “there is no evidence for lasting protective immunity to SARS-CoV-2 following natural infection” and that “the consequence of waning immunity would present a risk to vulnerable populations for the indefinite future.”
But in November 2021, a Freedom of Information Act (FOIA) request forced the CDC to admit that it didn’t even collect data on natural immunity.
Then, in January 2022, the CDC was compelled to revise its position on natural immunity, acknowledging in a report that natural immunity against COVID-19 was at least three times as effective as vaccination at preventing people from becoming infected with the Delta variant.
The pharmaceutical companies were also aware of the benefits of naturally acquired immunity, although they suppressed that information, documents revealed.
In October 2021, Project Veritas exposed three Pfizer officials saying that antibodies lead to equal if not better protection against the virus compared to the vaccine, The Defender reported.
Later, in April 2022, Pfizer documents held by the U.S. Food and Drug Administration (FDA) and released under court order confirmed Pfizer knew natural immunity was as effective as the company’s COVID-19 vaccine at preventing severe illness, journalist Kim Iversen reported.
Most recently, the Twitter files revealed that a Pfizer board member who used to head the FDA lobbied Twitter to take action against a post accurately pointing out that natural immunity is superior to COVID-19 vaccination, The Epoch Times reported.
FOIA requests also revealed that Dr. Anthony Fauci and his boss, National Institutes of Health Director Francis Collins, colluded to suppress the Great Barrington Declaration, which argues that natural immunity plays an important role in mitigating public harm from COVID-19, The Defender reported.
The vaccines are failing, which means we need more vaccines
Media that reported on the study, including NBC, ABC and U.S. News & World Report, continue to advocate for vaccination as the more important way to protect against severe disease and death from COVID-19.
This is despite the fact that even vaccine advocates Bill Gates and Fauci admitted that COVID-19 vaccines perform poorly.
In a paper published last month in Cell Host and Microbe, Fauci and his co-authors confirmed that the predominantly mucosal respiratory viruses, including influenza, coronaviruses, respiratory syncytial virus, or RSV, and common colds “have not to date been effectively controlled by licensed or experimental vaccines.”
They concluded, “Durably protective vaccines against non-systemic mucosal respiratory viruses with high mortality rates have thus far eluded vaccine development efforts.”
Nass said that while it is quite significant for The Lancet to publish these findings about natural immunity, the authors’ framing, like the admissions by Gates and Fauci, “is intended to quietly, without apology, veer away from current COVID vaccines, while implying that more money is needed to develop new types of vaccines. No one made any mistakes. No one accepts any blame. Chris Murray never erred with his outlandish estimates. No, just send money and let us do the science.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
February 18, 2023
Posted by aletho |
Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Gates Foundation |
Leave a comment
Pfizer enrolled 44,000 people across 270 clinical sites in the phase 3 clinical trials for the Pfizer/BioNTech Comirnaty vaccine. The largest of these sites by far was number 1231 in Buenos Aires, under the direction of the pediatric infectious diseases specialist Fernando Polack. The Argentine operation appears to have been plagued by substantial irregularities and is the subject of an ongoing inquiry by the Argentinian parliament.
Yesterday, Welt reporter Elke Bodderas published a report shedding further light on what appear to be systematic efforts to cover up or reclassify adverse events among trial participants.
The centrepiece of their reporting is patient number 12312982, a 36 year-old Buenos Aires resident named Augusto Roux, who participated in the vaccine arm of the trial and experienced significant adverse reactions following both doses of the vaccine. His most severe symptoms followed the second jab; they included shortness of breath, nausea, fever and darkened urine, and required hospitalisation. Throughout both sets of reactions, he tested negative for Covid. A trial doctor judged his symptoms very likely to be an adverse reaction to vaccination, and there are compelling reasons to think he suffered pericarditis. Roux promptly dropped out of the trial, and his lawyers succeeded in gaining access to internal Pfizer records his case. These reveal that Buenos Aires researchers recorded Roux as testing positive for Covid following dose 1, despite multiple negative PCR tests. To cover for his September hospitalisation, meanwhile, they listed him as suffering from a “severe anxiety attack.”
Welt finds other irregularities in data from the the Argentine clinical site as well. Following the first dose at the end of August, they removed 53 trial participants; internal documents give nothing but vague, contradictory excuses for the purge. Following the second dose, Buenos Aires researchers removed a further 200 participants – two-thirds of all removals across the entire trial.
Irregularities appear to extend beyond the shady Buenos Aires operation. As a friend notes on Twitter, the fact that there were more deaths in the vaccine than the placebo arm of the Pfizer trial has always been considered an awkward coincidence by the fact checkers. Upon closer examination, though, it begins to look like deaths from severe vaccine injuries were actually what put the vaccine arm over the top:
[Pharmacology expert and head of the “Data Based Medicine” network and the vaccine injury support organisation React-19] David Healy has … questions about the trial beyond the Augusto Roux case and other events at Buenos Aires. He wonders about a total of 21 vaccine group deaths that are said to be “not due to vaccination.” In at least two of these deaths, this conclusion doesn’t seem to be fully justified. WELT has documents showing that patient No. 11621327 was found dead in his home three days after the second dose, apparently a stroke. Patient No. 11521497 died 20 days after vaccination, diagnosed with cardiac arrest. “According to the current understandings, these two cases would be attributed to vaccination,” says Berlin-based pharmaceutical specialist Susanne Wagner, “especially since the US health authority CDC is currently investigating strokes in vaccinated people and it is known that blood clots can trigger sudden deaths following vaccination.”
In response to Welt inquiries, Pfizer responded that “Regulatory authorities around the world have approved our Covid-19 vaccine. These approvals are based on a robust and independent assessment of the scientific data on quality, safety, and efficacy, including the phase 3 clinical trial.” Thomas Mertens, head of the German vaccine regulator STIKO, demanded clarification from Pfizer, while the Berlin Charité immunologist Andreas Radbruch suggested the pharmaceutical should be sanctioned to preserve faith in vaccination and trust in regulators.
I doubt very much that will happen.
February 18, 2023
Posted by aletho |
Deception, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
CBS joins the chorus of mainstream media outlets promoting the false narrative that covid is the cause of a sharp increase in excess heart failure deaths around the world. The concept of “covid heart” has been thoroughly debunked by multiple studies, yet the lie continues to persist because of media disinformation.
An early report that set in motion fears of a Covid-heart disease connection was published in JAMA Cardiology on July 27, 2020. German researchers claimed that 78% of recently recovered Covid-19 patients had “abnormal” signs on their cardiac magnetic resonance scans and 60% showed signs of inflamed heart muscle, a condition known as myocarditis. Those astonishing numbers were covered in nearly 400 news outlets. The report has so far been viewed more than 900,000 times — a rarity for academic papers.
Soon after its publication, however, the paper was criticized for statistical and methodologic errors. It eventually underwent a long but much quieter correction that indicated that many of the abnormalities were only marginally more common among those recovering from Covid-19 than among similar control individuals who had not had Covid-19.
The assertion of the existence of covid heart serves a useful purpose, however, as it conveniently helps to distract from the very real threat of myocarditis caused by mRNA vaccines. Studies show a direct connection between covid vaccination, boosters, and risk of heart failure, specifically in younger people. The corporate media continues to ignore these studies in favor of the covid heart claim.
The CBS report presents a correlation as proof of causation: The explosion in heart failure happened in parallel with the pandemic, therefore, they say it “must be covid” that is causing the damage. But there was one other event that also happened in parallel with the heart failure spike – The introduction of experimental mRNA vaccines which have never been used before.
In reality, there is no evidence of a significant increase in risk of heart problems from contraction of covid, and there are no studies yet that use unvaccinated people as a control group to determine if vaccines help or hurt a patient’s chances. Medical officials simply assume that the deaths of younger people are due to them being “less likely” to have been vaccinated. The complete absence of objective scientific analysis has contributed to a lack of understanding surrounding covid risks versus vaccine risks. Mainstream outlets have consistently proven they are only interested in repeating establishment positions and protecting the status quo.
Why don’t medical authorities use unvaccinated people as a control group for their observations? Why do they continue to promote assumptions rather than definitive evidence? One can only theorize, but this behavior suggests a desire to hide certain findings and mislead the public rather than uncover the facts.
February 18, 2023
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science, Video | Covid-19, COVID-19 Vaccine |
Leave a comment
Eight leading critics of the United States’s COVID-19 response have called for an investigation of the many failures of policy architects and key decision makers — at institutions ranging from the Centers for Disease Control and Prevention and Food and Drug Administration to universities and hospitals — over their repeated mishandling of the pandemic.
Given the immense harm inflicted on our society by the follies of a ruling class and their expert advisers who never failed to make a wrong decision when presented with the opportunity, as well as the fact that lives are still being destroyed by their lingering policies, we can only hope this blueprint does not go ignored.
Dubbing themselves the “Norfolk Group,” the association of scholars includes such prominent names as Stanford epidemiologist Jay Bhattacharya, Harvard epidemiologist Martin Kulldorff, UCSF physician Tracy Beth Høeg, Johns Hopkins University surgeon Marty Makary, and Indiana University School of Medicine immunologist Steven Templeton.
According to the Norfolk Group’s website, although initially organized by the Brownstone Institute in May 2022, the eight members of the group have since worked free from outside influence to draft the 80-page document they published earlier this year, “Questions for a COVID-19 Commission.”
Presented as a series of summaries and questions pertaining to key elements of U.S. COVID policy, the document, in effect, lays out a thorough indictment of the consistent incompetence of our ruling class while also raising concerns over the possible influence on policy by special interests such as teachers unions and drug companies.
Regarding natural immunity, the authors ask, “Why did the CDC downplay infection-acquired immunity, despite robust evidence for it?”
In respect to school closures, they ask, “Why were schools and universities closed despite early evidence about the enormous age-gradient in COVID-19 mortality … and early evidence that school closures would cause enormous collateral damage to the education and mental health of children and young adults?”
On that matter, they also wonder, “Why did the CDC incorporate policy language proposed by leaders of teachers unions on the scientific and public health aspects of school reopening without soliciting expertise of outside scientists in public health, infectious diseases, or other related fields?”
When discussing lockdowns, they inquire, “Why was so much influence on public health policy accorded to Drs. [Francis] Collins and [Anthony] Fauci? They control the largest source of infectious disease research funding in the world. How many infectious disease scientists, who should have been strong voices during the pandemic, kept quiet for fear of losing the research funding on which their livelihood depends?”
In their section on epidemiologic modeling, they demand, “Why did world leaders overly rely on models that made unverified assumptions about the pandemic’s trajectory rather than trying to verify these assumptions and their implications?”
When addressing COVID-19 vaccines, they raise questions such as, “Why did many organizations continue with mandates through summer and fall of 2021, despite data demonstrating both waning efficacy of symptomatic infection and reduced long term ability to curb viral spread?”
Regarding masks, they state, “Prior to the COVID-19 pandemic, the evidence that masks did little if anything to stop the spread of respiratory viruses was uncontroversial,” before summarizing a few studies demonstrating this and asking the obvious: “[W]hy did public health officials and agencies promote the idea that masks would be effective against SARS-CoV2?”
In its entirety, the Norfolk Group’s “Questions for a COVID-19 Commission” serves as a blueprint for the kind of investigation our country needs. Just don’t expect the Biden administration to do anything about it.
Daniel Nuccio holds master’s degrees in both psychology and biology. Currently, he is pursuing a PhD in biology at Northern Illinois University studying host-microbe relationships. He is also a regular contributor to The College Fix where he writes about COVID, mental health, and other topics.
February 16, 2023
Posted by aletho |
Corruption, Science and Pseudo-Science | CDC, Covid-19, COVID-19 Vaccine, FDA, United States |
Leave a comment
In late 2019 and early 2020, I was asked to work on the front line in an emergency department to help with the ‘war effort’. We had no idea what was going on, apart from a few videos of the Chinese suddenly collapsing due to this new contagion. We were waiting for it to hit the U.K.
It hit, I saw what it did to people, they became unwell, x-ray x-ray x-ray, PPE, barriers, red lights, code words, panic, panic. Our world changed overnight, and my world changed especially. One minute we were told not to wear masks, the next moment it was made mandatory etc.
At this point, my sole focus was to protect myself and my family, so I began studying in order to do so successfully. I read papers during my breaks and at night before work. I reflected on what I saw at work and made a mental note of the real-life evidence.
The emergency department warped as time went on; I saw a lot of errors and mismanagement of resources. Patient care was being delayed, which led to staff burnout and medical errors. I could see that if this went on, people would needlessly die.
I knew something had to change. So in efforts to bring about some change, I wrote a book outlining how Toyota’s lean manufacturing methods could aid in improving patient safety as well as reducing costs in emergency departments. The book was called Saving A&E The Toyota Way. While researching for it, I learned a lot about healthcare infrastructure, artificial intelligence and preventative medicine. I knew what the national health situation was like; I knew we had to change as a species.
I presented that book to my hospital; my consultants liked it, but as an academic piece. That was not my intention, but hey ho, life goes on. There were more pressing matters at hand.
As the pandemic was progressing, I continued to research, write blogs and share what I saw. And I saw a lot of unscientific rubbish, unethical practices and poor care. The research papers said one thing, and yet we were doing something completely different. I knew very early on that not everyone needed to be jabbed. Something seemed fishy.
I worked in the emergency department and then paediatrics during the second peak. There was one child admitted due to COVID-19 who was later discharged. The ward was largely empty. And yet many doctors online were saying that COVID-19 was extremely dangerous to children. Nonsense.
Something was off: doctors weren’t being doctors, autopsies weren’t being done, the medical field was ignoring anyone who didn’t have COVID-19, and yet staff were doing TikTok dances. They asked me to join. I refused.
While all this was happening, I lost my grandma. The doctors didn’t want to see her in her home; her infection got bad; she didn’t want to go to the hospital; she became septic; she had to go in. I visited her after my shifts and fed her during my breaks.
I got the bad news from a doctor on the night she died. I asked the doctor if we could see her as a family, and he approved. We saw her one after the other, in tears and trying not to wake the other patients. Midway through, a matron I used to work with told us we couldn’t see her due to hospital policy and warned us that if we carried on she would call security on us. I told her we had approval already. She didn’t care. I saw evil in her eyes.
I asked her why she became a nurse. It was surely to treat and help people with compassion. She didn’t budge. I said, “Go ahead and call security then.”
Thank God, we had enough time for our family to all say their goodbyes. I made sure I was the last one. I knew and saw that many others weren’t as lucky as I was. Many had to FaceTime their dying family members. We were treated so badly and healthcare professionals encouraged it. I also knew the evils that lurked inside mankind that day.
During paediatrics I asked my colleagues about masks and jabs. Why did we only allow one parent to see their newborn child while wearing a mask, whereas we could all snuggle up together in the staff room maskless? I’d get responses that sounded like parrots. “It’s the rules”; “Policy”; “To stop infection”; “We just have to do it”. No science. No debate. No conversation. No brain.
I later worked in a children’s psychiatric ward, and what I witnessed was truly backward. Many children, many of whom wanted to commit suicide, were placed in solitary confinement so that useless PCR swabs could be taken. Two would need to be done, and the nurses would sometimes forget to do these. I actually had to make them a table so they would remember. Children were required to be swabbed, but staff members who would go wherever they pleased over the weekend were not.
I told my seniors that none of this made sense and that children did not suffer with COVID-19, but they just told me it was policy. The hospital trust actually recruited people to make sure staff were changing into scrubs before work too. The worst of it was when we had a ward round on one occasion. In psychiatry, the patient would sit in the room with the rest of the staff. This particular time my consultant found out that the young person who was in the room with us wasn’t swabbed. After the patient had left, she made us all stay in the room and asked us to lock the door and find ways to disinfect the room. She was seriously considering bleaching all surfaces. In disbelief, I asked her if we had to all strip down naked and shower together too. I had work to do, so I left.
The mental health of children and adults during lockdown was the lowest I’ve ever seen it in my career. Children were arriving with life disruption-related issues such as trauma, abuse, etc. all related to lockdowns.
My next job was in general practice. I was working towards becoming a GP. I enjoyed understanding and caring for all sorts of patients. I’m a generalist at heart. However, this transition marked another difficult time for me.
On the last day of hospital medicine and just before the first day of GP work, a close work colleague of mine went to play football, collapsed and never woke up. Deep down, I knew what had caused this. I knew the link between mRNA technology and myocarditis early on.
I cried finding this information out. I cried in front of my mother for the first time in my adult life. I’m in fact tearing up typing this. My friend was killed.
I went to his parents’ house to give my condolences. His parents were there, broken. He recently proposed to his fiancée. She was there too, broken. We viewed his funeral via Zoom.
There’s a spot in the park I dip into regularly while looking up at the leaves. I am reminded of him when I do this. I am reminded of how lucky I am to be alive. Deep down, I was terrified about what this meant for people around the world.
Time went on, and I worked in general practice. There was discussion about making vaccinations mandatory for all healthcare workers. I knew this was not only unscientific and unethical, but murderous. Yet my colleagues didn’t seem to care. They were safe, I guess.
Regardless, I could not do anything about it, so I plodded along. I never stopped reading papers, writing, tweeting and sharing information. I saw patients; I saw jab-related side effects, missed periods, new-onset whole-body inflammation, hair loss, etc. I saw cognitive dissonance too.
All of a sudden, one day, my practice asked me for my full jab status. This puzzled me because the managers knew I had to be jabbed with everything else in order to work in all the other specialties. I knew they wanted to know only one result. Whether or not I had taken the COVID-19.
I didn’t lie. I told them the truth. The next day, in a panic, they asked me to stop seeing patients face-to-face. They had made a team decision as a team, without me, that I was no longer able to see patients. They felt that I was a threat to them and that I would scare them away.
I have never had COVID-19. I worked on my health and immunity every day, and I purposely breathed in the virus in the emergency department to stimulate T cells. I knew jabs increased one’s risk of infection and showed them evidence. I was the least risky person in the practice and I knew it.
They didn’t care. They didn’t care about evidence. They didn’t care about ethics, about immunity, about anything. I shrugged this off and called patients instead. I was ostracised at work and many colleagues acted coldly towards me. I was alone, but not lonely; I knew I had evidence on my side.
Many doctors had to take sick leave from work multiple times due to COVID-19. I had meetings discussing my jab status. A doctor with myocarditis on long-term meds post-jab urged me to get the shot. One said I was “too principled”, It was surreal.
They admitted it was all politics. I asked them why they didn’t read papers? I asked them about T cells. Silence.
I have wanted to become a doctor since the age of six. I love biology and enjoy helping people using my knowledge. But I understood that I was working in an environment that was harming people. I had many sleepless nights thinking about leaving.
One morning, after parking my car at work, I felt a warmth around my head. It had no words, but if it did, it told me that everything would be okay. As soon as I had that experience, my decision was made, and I felt light; a colossal weight had been lifted.
I asked to quit, and a few meetings later (carried out to make sure I wasn’t crazy), I left healthcare and then deregistered myself from the medical register. I wanted to be totally free. I needed to be.
The flat my girlfriend and I were planning to buy fell through. I was in financial turmoil. My mother cried for weeks. I was lost, but I was free. I wasn’t part of the killing system.
I did what I only knew – I began writing. I started a Patreon and am grateful for those who did and continue to contribute to that. But it wasn’t enough. I ended up being on the dole for just less than a year. The guy I had to call every two weeks was surprised I was once a doctor.
I began learning and researching everything I could to help people who had been jabbed. I knew what was going on and I didn’t want another pandemic to happen. I wanted to save as many lives as possible.
I would take my bike, cycle across the park to my local library, and work feverishly every day till close. Around this time, I was permanently suspended on Twitter for stating facts.
I see this as a blessing now, as it made me work even harder to produce something that could never be banned. A book. I worked and researched to make sure I got this book out before 2023.
I was blessed around this time to come into contact with Alex Mitchell. He introduced me to other people injured by the shots. I was determined to make sure their voices got heard. I included their stories in the book.
During this time, on my walks, I had many insights and extraordinary experiences that many people may not believe or might dismiss as crazy. I saw light, and I ended my fears.
Before the new year, I released my book, Calling Out The Shots. It goes through what genetic agents are, what they do to our bodies, how we can improve our immunity, ways we may mitigate jab damage and what we need to do as a society to heal.
The book marks my first gift to the world. I am working on many more and other projects. I will fight for humanity until my final breath.
Dr. Eashwarran Kohilathas is a medical doctor, qualified personal trainer and author who aims to help people achieve physiological, psychological and spiritual freedom. This article first appeared as a Twitter thread.
February 16, 2023
Posted by aletho |
Book Review, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights, UK |
Leave a comment
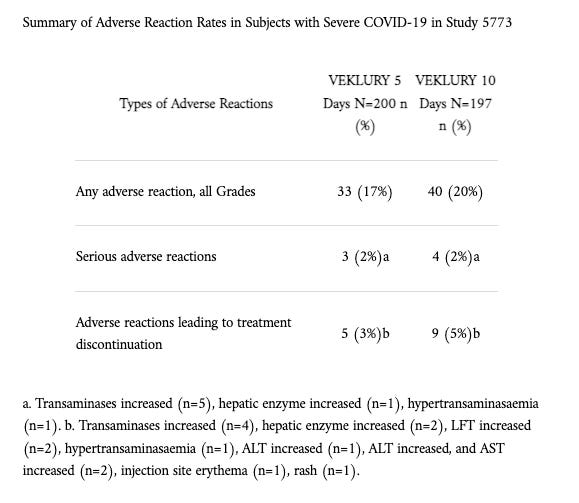


 Aletho News
Aletho News