New lawsuits have been filed against an array of Community Medical Centres in California over their covid care protocol…
Gilead’s Remdesivir is a drug that has received a lot of criticism, and rightly so.
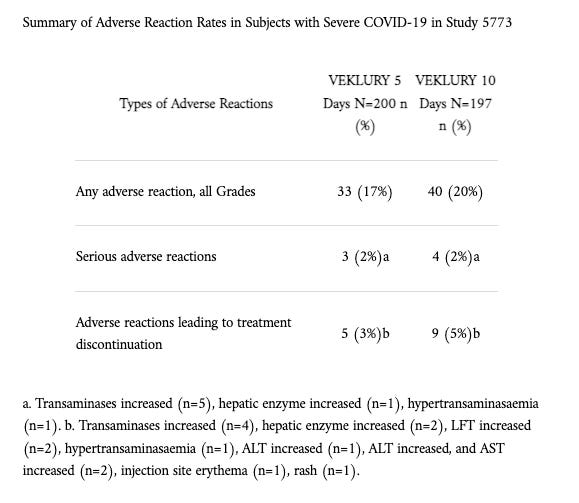
Prior to the pandemic, the World Health Organisation rejected its use due to poor trial studies abroad. NIAID-sponsored trials had likewise documented troubling issues. Reported adverse events were significant:
In short, a plethora of studies indicated it had potentially bizarre and fatal effects depending on the patient’s health. Patients who had a multi-organ impairment, for example, exhibited detrimental impacts on their renal function after the drug was administered. The FDA, nonetheless, granted its use under Emergency Use Authorisation (EUA) when a study showed it reduced COVID hospitalisation duration by 4 days.
From that point on, Remdesivir became part of every COVID-19 protocol across the country. Reports from 2020 have since revealed that if a vulnerable patient (aged 65 and over) came into a medical centre and tested positive, Remdesivir was the treatment most likely to be offered. That patient would then be placed or declared in the ICU as an inpatient.
Here is where the story turns very sinister.
According to local sources in California, hospitals that took on inpatient complex cases could charge up to 144x more than an outpatient case. As soon as they treated these patients within their facilities, they could apply for reimbursement from Medicare. In other words, there was a clear financial incentive for hospitals to “over-treat” patients to maximise profits.
With these reports now circulating, 14 Californian residents living in the Fresno area have filed lawsuits against various medical centres. These include Community Regional Medical Center, Clovis Community Medical Center, and St. Agnes Medical Center.
One plaintiff’s claim about a medical centre’s covid protocol is particularly reprehensible:
“A patient comes to the hospital often for problem unrelated to COVID-19. They are told they have COVID-19 or ‘COVID pneumonia’. They are immediately separated from their loved ones, and usually declared to be in ICU, even though they are often just placed in room. They are told that the deadly Remdesivir is the only available and safe treatment. They are usually told that if they leave the Hospital against ‘medical advice’ they will void their insurance. They are placed on BiPap machine at high rate, making it difficult for them to breathe. Their hands are often tied down so they can‘t take the BiPap machine off their face. After their hands are tied down, and sometimes before, [a] psychiatrist comes to the room and determines that they are ‘agitated.’ This results in the protocol patient being placed on morphine or something similar. Sedating the patient makes it more difficult for them to communicate and more difficult for them to fight the effects of Remdesivir especially as it relates to their ability to breathe….”
All the lawsuits are being funded by the Arizona-based medical advocacy nonprofit Truth For Health Foundation. The organisation is run by Elizabeth Lee Vliet MD. Currently, the three aforementioned lawsuits will return to court for case management in January.
Note: These claims do not concern ‘End-Of-Life Care Protocols’. They concern COVID care protocols in general. We’ve seen similar claims made in the UK regarding Midazolam but again this concerned ‘End-Of-Life’ care. These lawsuits could well lift the thickly-blackened veil (for the wider masses) on the medical industry’s capacity to treat patients like cattle.
February 23, 2023
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, Gilead, Human rights, remdesivir, United States |
Leave a comment
As reported last week by The Defender, federal monies from the 2020 and 2021 COVID stimulus bills dramatically reshaped K-12 educational priorities, turning American school officials into lackeys for federal agencies more intent on masking and vaccinating every last child than on supporting meaningful education.
So, too, with the stimulus-induced reshaping of hospital priorities.
In the second half of a January interview on Del Bigtree’s “The Highwire” — “COVID-19: Following the Money” — policy analyst A.J. DePriest reported on the untoward consequences set into motion as a result of COVID funds provided to hospitals.
Managed by the U.S. Department of Health and Human Services (HHS), the federal government allocated a total of $186.5 billion to the Provider Relief Fund (PRF), with two-thirds ($121.3 billion) disbursed as of January 2022.
The first tranche of $50 billion for hospitals and other Medicare providers — “for healthcare-related expenses or lost revenues … attributable to COVID-19” — began flying out the door in April 2020.
Almost immediately, alert doctors and astute journalists warned the Medicare add-on payments built into the relief package created perverse incentives unfriendly to patients’ interests.
As summarized by Dr. Scott Jensen — former Minnesota state senator and current gubernatorial candidate — “anytime healthcare intersects with dollars it gets awkward.”
Nearly two years down the road, the “awkwardness” is increasingly difficult to hide.
In the view of DePriest and many others, HHS’s stimulus slush fund has been every bit as dangerous for hospital patients as the U.S. Department of Education’s handouts have been for the nation’s schoolchildren.
Making out like bandits
Dr. Elizabeth Lee Vliet and Ali Shultz, J.D., who wrote a widely distributed op-ed in late 2021 for the Association of American Physicians and Surgeons (AAPS), summed up the disturbing situation prevailing in hospitals. The AAPS’s professional calling card is its “dedication to the highest ethical standards of the Oath of Hippocrates.”
Not mincing their words, the two argued that Centers for Medicare and Medicaid Services (CMS) payment directives turned hospitals and medical staff into “bounty hunters,” and COVID patients into “virtual prisoners.”
Highlighting the slew of CMS add-ons and other incentives established with the Coronavirus Aid, Relief and Economic Security (CARES) Act — and also the Paycheck Protection Program and Health Care Enhancement Act (PPPHCEA) — they emphasized the payments hinge on hospitals’ willingness to slavishly follow the National Institutes of Health’s (NIH’s) guidelines “for all things related to COVID-19.”
As itemized by Vliet and Shultz, compliant hospitals garner CMS payments for:
- Each completed diagnostic test (required in the emergency room or upon admission).
- Each COVID-19 diagnosis.
- Each COVID admission.
- Use of the intravenously administered Gilead drug remdesivir (brand name Veklury), which yields a 20% bonus payment on the entire hospital bill.
- Mechanical ventilation.
- COVID-19 listed as cause of death.
Citing a Becker’s Hospital Review breakdown, published in April 2020, of CARES Act payments to different states, DePriest told Bigtree payments ranged from $166,000 per COVID patient in Tennessee hospitals, for example, to far higher payments in states such as North Dakota ($339,000), Nebraska ($379,000) and West Virginia ($471,000).
In addition, for hospitals ascertained to be in COVID “hotspots,” HHS distributed special “high-impact” funds — $77,000 per admission initially, later downsized to $50,000 per admission.
HHS explained it used COVID admissions “as a proxy for the extent to which each facility experienced lost revenue and increased expenses associated with directly treating a substantial number of COVID-19 inpatient admission [sic].
The remdesivir ruse
The National Institute of Allergy and Infectious Diseases (NIAID) and the Centers for Disease Control and Prevention (CDC) spent $79 million developing remdesivir for Gilead, which itself dished out $2.45 million during the first quarter of 2020, to lobby for the drug’s use with COVID patients.
On May 1, 2020, the U.S. Food and Drug Administration (FDA) authorized remdesivir for emergency use in individuals hospitalized with severe COVID illness, and members of an NIH expert panel (many with financial ties to Gilead) added the drug to the agency’s treatment guidelines.
A scant five months later, FDA granted full approval to remdesivir for hospitalized COVID patients over age 12.
The World Health Organization (WHO), in contrast, advised against remdesivir, stating the drug has “no meaningful effect on mortality or on other important outcomes for patients.”
Remdesivir sailed through regulatory hoops in the U.S. despite an abysmal track record of “adverse effects serious enough to kill” any individual hapless enough to take it.
Children’s Health Defense Chairman Robert F. Kennedy, Jr. discusses remdesivir’s toxicity in his best-selling book, The Real Anthony Fauci, outlining the lethal problems — multiple organ failure, acute kidney failure, septic shock, hypotension and death — experienced by participants in NIAID’s clinical trial of remdesivir as an Ebola therapy.
When the trial, which compared remdesivir against three other drugs, killed more than half (54%) of the remdesivir recipients within 28 days — the highest mortality rate among the four groups — an oversight board forced the NIAID to end the prong of the study focused on remdesivir.
As if remdesivir alone weren’t bad enough, Vliet and Shultz estimate mechanical ventilation kills anywhere from 45% to 85% of COVID patients. Moreover, NIH’s skimpy treatment guidelines prescribe dexamethasone concurrently with ventilators.
Dexamethasone, often described as a “double-edged sword,” is a highly potent corticosteroid that suppresses the innate immune system.
Like remdesivir, dexamethasone’s potentially significant adverse impacts include kidney damage. Additional side effects include interference with the normal function of other organ systems such as the cardiovascular, digestive, endocrine, musculoskeletal and nervous systems.
Ironically, dexamethasone can also increase the need for mechanical ventilation as well as for blood pressure intervention.
Therapies like these are a large part of why, as Vliet and Shultz note, the U.S. COVID mortality rate is so “shockingly high” compared to the rest of the world.
Remdesivir’s trail of destruction could get worse — on Jan. 21, FDA expanded use of remdesivir to “high-risk” adult and pediatric outpatients (age 12 and older) “for the treatment of mid-to-moderate COVID-19 disease,” permitting administration of the intravenous drug in various outpatient facilities.
FDA’s side effects warnings include possible liver injury and allergic reactions such as “changes in blood pressure and heart rate, low blood oxygen level, fever, shortness of breath, wheezing, swelling …, rash, nausea, sweating or shivering.”
Getting involved and bringing transparency
Referring to the 20% add-on payment that hospitals receive for administering remdesivir to COVID patients, DePriest commented that a “bonus” is a “weird thing to call something when you’re murdering people.”
Journalist Jon Rappoport agreed, preferring to characterize hospitals’ behavior toward COVID patients as “a federally incentivized protocol for murder” — or “cash for death.”
All of the above parties concur that the best-case scenario is to treat COVID early at home and avoid hospitals — “because we know from experience what happens there.”
In cases where hospitalization is unavoidable, DePriest encourages communities to get more involved:
“[W]hen you know these hospitals are doing that, the people of that community need to show up at that hospital en masse and start telling them that you, as a community, are going to be advocating for every single COVID patient that walks through those doors, and you are going to hold that hospital accountable — to their patient bill of rights, to their stated visitation policies — and if your state is not in a state of emergency anymore, there shouldn’t be any reason why patients are medically kidnapped and separated from their families and isolated.
“There’s absolutely no reason for it, but the communities have to get involved and they have to confront these hospitals and tell them, ‘We’re done, you’re not killing any more of us.’”
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
January 25, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, remdesivir, United States |
Leave a comment
A 2003 analysis lists three ways in which doctors earn money from drug companies. Some are hired to conduct research. Some get paid for referring patients to clinical trials. Others are incentivized to write more prescriptions.
These incentives can take the form of annual consultant’s fees. Or speaker’s fees at drug company events. Or expense-paid conferences in exotic locales (travel), dinners at fancy restaurants, tickets to sporting events, and tickets to music concerts.
Research suggests even small gifts and small amounts of money affect physician behaviour to a surprising degree, and that most physicians believe their colleagues are influenced by drug company promotions.
Which brings us to COVID-19. A very public conflict has arisen between those who favour treating patients with inexpensive, off-patent drugs such as hydroxychloroquine (HCQ), and those who favour the use of expensive, proprietary drugs such as remdesivir/veklury, which is manufactured by Gilead Sciences.
A recent paper examines what 98 French professors/physicians who specialize in infectious diseases have said publicly about HCQ. Titled Influence of conflicts of interest on public positions in the COVID-19 era, the case of Gilead Sciences, it reports that 54 of these academics have taken no public position on HCQ. 14 others have remained carefully neutral.
Which leaves 30 more. 14 have said favourable or very favourable things about HCQ. 16 have said unfavourable or very unfavourable things.
In France, drug companies are required to report, via a government website, how much financial support they provide to doctors. This paper reveals a startling difference between pro- and anti-HCQ academics. Generally speaking, doctors who are more favourable toward HCQ take less money from Gilead Sciences. And vice versa.
The paper treats the 14 pro-HCQ academics as two sub-groups (favourable and very favourable), rather than as identifiable individuals. Some of these people had no financial links to Gilead Sciences over the past seven years (2013-2019). The most any individual benefited was to the tune of €4,773.
All 16 of the (likewise unidentified) anti-HCQ academics were financially linked to Gilead during the same time frame. Those who’ve made unfavourable public comments received, on average, €11,085 (with individual cases ranging from €234 to €31,731). Those who’ve made very unfavourable comments received, on average, €24,048 (with individual cases ranging from €122 to €52,812).
In France, the less financially connected to Gilead Sciences experts happen to be, the more likely they are to support the use of HCQ. The greater the financial connection to Gilead, the greater the hostility toward HCQ.
The ‘Results’ section of this paper further reports that, of the 98 academics studied, only 13 had no financial links whatsoever to Gilead. Four of those 13 have taken no public position on HCQ. One has remained neutral. The majority (62%) are pro-HCQ – with one being favourable, and seven being very favourable.
This study tells us nothing, of course, about the circumstances in which HCQ might be an effective COVID treatment. But it reminds us that governments rely on the judgment of fallible human beings. Even in the midst of a pandemic, when everyone should be trying hardest to think clearly, infectious disease experts are prone to multiple kinds of bias.
November 9, 2020
Posted by aletho |
Corruption, Science and Pseudo-Science, Timeless or most popular | Covid-19, Gilead Sciences, HCQ, remdesivir |
Leave a comment
In late May, Russia registered the world’s first anti-COVID-19 drug, based on favipiravir, an antiviral medication. The medicine has been extensively used in Russian clinics to treat coronavirus disease since June, and has since been obtained by hospitals in Belarus, Kazakhstan, Bolivia and a number of other countries.
The Russian Direct Investment Fund (RDIF), the investor which funded the development of the world’s first vaccine against coronavirus, and Moscow-based ChemRar Group have agreed to supply the anti-COVID drug Avifavir to 17 countries.
Avifavir, the world’s first favipiravir-based drug to be approved for the treatment of COVID-19, will now be delivered to Saudi Arabia, Brazil, Bulgaria, Serbia, Argentina, Chile, Colombia, Ecuador, El Salvador, Honduras, Kuwait, Panama, Paraguay, Slovakia, South Africa, the UAE and Uruguay.
After being first registered in Russia on 29 May 2020, it has already been used for COVID-19 treatment in more than 70 Russian regions and subsequently purchased by Belarus, Bolivia, Kazakhstan, Kyrgyzstan, Turkmenistan and Uzbekistan.The efficacy of favipiravir against COVID-19 has been confirmed by Japan’s Fujifilm Holdings Corp, several months after Avifavir trials in Russia.
Avifavir as the Leading Anti-Covid Drug in the Russian Market
RDIF notes that in comparison to other Russian manufacturers of favipiravir, Avifavir has proven to be more effective when treating more than 400 patients, who fell ill with the coronavirus disease since April. The drug has now been approved by European, Middle Eastern and Asian regulators, becoming Russia’s number one anti-coronavirus medication for export.
According to RDIF, it is also a much cheaper option in comparison to Remdesivir, a favipiravir-based drug produced in the United States.
“When we registered the first anti-coronavirus drug in the world based on favipiravir, there was a lot of scepticism as people were wondering how we could register it when Japan had not registered it yet,” says Kirill Dmitriev, CEO of the Russian Direct Investment Fund. “Now five months after our clinical trials, we see that Japan has confirmed the clinical efficacy of favipiravir.”
The RDIF CEO stresses that apart from clinical trials which were conducted at 35 medical centres in Russia, Avifavir’s efficiency has also been tested by 940 patients in observational post-registration studies, which made it “the largest clinical trial of a favipiravir-based drug against coronavirus in the world”.
“Based on our extensive clinical trials and the research in Japan confirming favipiravir’s efficacy against coronavirus we believe that Avifavir and other favipiravir-based products will be the leading antiviral medicines against COVID-19 in the world,” Dmitriev adds. “In addition to proven efficacy and safety Avifavir is also three to four times cheaper than Remdesivir.”
Trials Confirm Avifavir’s Efficiency
According to the results of post-registration clinical trials, those patients taking Avifavir recovered more quickly from COVID-19 symptoms, as in 30% of cases the virus was eliminated at an early stage, while the level of oxygen saturation in the patient’s blood was also restored to normal two times more quickly than when traditional therapy was applied. No adverse effects from the drug’s use have been reported. Meanwhile, the third phase of clinical trials of the Japanese favipiravir-based drug Avigan also showed a shorter time of recovery among patients with non-severe pneumonia, according to the results published on 23 September.
RDIF, Russia’s sovereign wealth fund, has also been involved in the development of the world’s first anti-coronavirus vaccine, dubbed Sputnik V, which was registered in Russia on 11 August. The country has now received a request for 1 billion doses of the vaccine from at least 20 countries, including the UAE, Saudi Arabia, Indonesia, Philippines, Mexico, Brazil and India.
September 24, 2020
Posted by aletho |
Aletho News | Avifavir, Covid-19, remdesivir |
Leave a comment
Fake news is keeping us away from the treatment to end the coronavirus crisis
The anti-hydroxychloroquine media has been full of the supposed dangers of hydroxychloroquine and its failure as a treatment for the virus. Does hydroxychloroquine work or does it not, is it safe or dangerous, and should we be using it as a treatment for the virus? Here we examine the evidence for and against it.
A New York doctor Vladimir Zelenko looked at treatments being used in China and Korea and gave it to 405 patients over 60 or with high-risk problems such as diabetes, asthma, obesity, hypertension or shortness of breath. In this high risk group he claimed to have cut hospital admission and mortality rates compared to what could be expected without treatment by 80 to 90%.
Dr Zelenko sent a letter to President Trump urging him to issue an executive order to roll out the treatment which the FDA was blocking. Trump announced that hydroxychloroquine looked like it could be a “game-changer”, and thus the politicization of hydroxychloroquine began.
Dr Fauci the director of the National Institute of Allergy and Infectious Diseases who was supposed to be advising Trump disagreed with him and backed Gilead’s rival treatment Remdesivir. YouTube deleted a video of Dr. Zelenko talking about the treatment on his Rabbi’s channel and despite objections that there was nothing wrong with the video YouTube never reinstated it.
In this YouTube video interview with Rudy Giulliani from July 1, which hopefully will not be deleted by the time you read this, Dr. Zelenko claims 99,3% survival rate for the high-risk patients he has treated.
Professor Didier Raoult of Marseilles used a similar protocol to Dr. Zelenko without the zinc. His study with a small group using hydroxychloroquine and azithromycin showed a fifty-fold benefit. He then went on to get similar results with a much larger group of 1,061 patients. Contrary to the warnings the media had been running that hydroxychloroquine would cause heart problems, no cardiac toxicity was observed and he achieved a mortality rate of only 0.5%.
The media quickly found critics who claimed that the only valid proof any treatment worked was a “gold-standard” double-blind clinical trial and dismissed Dr. Zelenko’s and Raoult’s results. Dr. Zelenko and Prof. Raoult both refused on ethical grounds to give placebos to half the patients in clinical trials and they defended their data as sufficient to show the treatment did work. They both stressed that the urgency of the situation made it necessary to act on available evidence, not clinical trials which would take months to produce results and be verified. There have subsequently been over a dozen studies which confirm that Dr. Zelenko’s and Prof. Raoult’s protocols do work.
A study from the New York University Grossman school of Medicine published in May found patients given hydroxychloroquine and azithromycin at an early stage had a lower need for hospitalization than those who were not. The addition of zinc improved the results even more.
“I’ll tell you what. If this is me, and I am me, and I end up getting this thing, I am going to want Zinc plus Hydroxychloroquine plus Azithromycin. I would want that treatment.” Commented Chris Martenson, PhD, in his video series about COVID-19 where he talks about this study.
Yale Professor Harvey Risch submitted a report of five trials and studies using hydroxychloroquine in the American Journal of Epistemology titled “Early Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis.
Prof. Risch agreed that, in an ideal world, randomized double-blinded controlled clinical trials would be preferable but in the meantime “for the great majority I conclude that hydroxychloroquine and azithromycin, preferably with zinc can be this outpatient treatment, at least until we find or add something better. It is our obligation not to stand by as the old and infirm are killed by this disease and our economy is destroyed by it and we have nothing to offer except high-mortality hospital treatment. Available evidence of efficacy of HCQ+AZ has been repeatedly described in the media as anecdotal, but most certainly is not”
A Brazilian study found 4.6 times less hospitalization in patients who took hydroxychloroquine and azithromycin within seven days of infection. Professor Paolo Zanotto reported that there were “41% of deaths among those who did not choose therapy and were hospitalized against 0% among those who chose by therapy.”
A retrospective study of 2,541 Detroit cases showed up to 71% reduction in mortality in early treatment with hydroxychloroquine azithromycin.
A retrospective study of 3,737 cases in Marseille showed a reduction of 50% in mortality without any adverse effects in the Hydroxychloroquine and Azithromycin group.
A meta-analysis of 105,040 cases from 20 studies in 9 countries found a reduction in mortality by up to three times in groups treated early with Hydroxychloroquine and Azithromycin: https://doi.org/10.1016/j.nmni.2020.100709
A study of 6,493 patients with COVID-19 at Mount Sinai Hospital, New York, showed that hydroxychloroquine helped to reduce mortality in hospitalized patients.
On July 3 a study by a Michigan team at Henry Ford Health System found that 13 percent of patients who were given the drug early on died while 26 percent of patients who were not given the drug died. The study which included 2,541 patients was published in the International Journal of Infectious Diseases and determined that hydroxychloroquine and azithromycin provided a 71% hazard ratio reduction. “Our results do differ from some other studies. What we think was important in ours … is that patients were treated early. For hydroxychloroquine to have a benefit, it needs to begin before the patients begin to suffer some of the severe immune reactions that patients can have with COVID” said Dr. Marcus Zervos, head of infectious disease for Henry Ford Health System.
A statement from the Trump campaign hailed the study as fantastic news. “Fortunately, the Trump Administration secured a massive supply of hydroxychloroquine for the national stockpile months ago, yet this is the same drug that the media and the Biden campaign spent weeks trying to discredit and spread fear and doubt around because President Trump dared to mention it as a potential treatment for coronavirus. The new study from the Henry Ford Health System should be a clear message to the media and the Democrats: stop the bizarre attempts to discredit hydroxychloroquine to satisfy your own anti-Trump agenda. It may be costing lives.”
Also on July 3 results from another study by Dr. Takahisa Mikami and his team at Icahn School of Medicine at Mount Sinai in New York, was published in the Journal of General Internal Medicine. The study analyzed the outcomes of 6,493 patients who had laboratory-confirmed COVID-19 in the New York City metropolitan area and found that hydroxychloroquine decreased mortality hazard ratio by 47% percent.
Many more studies in addition to those above also show that treating early with hydroxychloroquine and azithromycin and preferably also zinc is the key to ending hospitalization and death.
The trials that confirm Dr. Zelenko’s and Prof. Raoult’s finding have been mostly ignored or dismissed by the anti-hydroxychloroquine media. The trials that they have given attention to are those that supposedly show that hydroxychloroquine doesn’t help or even increases the death rate.
Statistics from the US Veterans hospital study (Magagnoli, 2020) showed patients who were given hydroxychloroquine died more frequently than those who did not.
In this study hydroxychloroquine was only given to patients who were already seriously ill and those who were getting better without any treatment were not given it. Predictably those given hydroxychloroquine did worse than the untreated group but those conducting the study claimed it as proof that hydroxychloroquine did not work. Professor Raoult commented “In the current period, it seems that passion dominates rigorous and balanced scientific analysis and may lead to scientific misconduct. The study by Magagnoli et al is an absolutely spectacular example of this,”
One of the collaborators in the trial reportedly received a $260 million grant from Gilead Sciences Inc. which produces the rival treatment Remdesivir.
The US Secretary of Veteran Affairs Robert Wilkie, acknowledged that the drug was given to veterans at their last stages of life and added “We know the drug has been working on middle-age and young veterans … it is working in stopping the progression of the disease.”
Another study that supposedly showed that hydroxychloroquine was dangerous and didn’t work came from a group that claimed to have data on hydroxychloroquine use for Covid-19 from hospitals around the world The study was published on 22 May in the Lancet medical journal. The results were immediately disputed by one of the Australian hospitals from which Surgisphere, the company which supplied the data claimed to have obtained it.
Following this a group of 140 scientists, researchers, and statisticians wrote an open letter to the Lancet and the authors of the study questioning the data used. A Guardian investigation revealed that Surgisphere was run by employees who lacked any scientific background. One was a science fiction author and fantasy artist and another was an “adult model and events hostess.” The Lancet conducted an independent investigation, retracted the study and in an interview with The New York Times, Dr. Richard Horton, the editor in chief admitted that the study should never have appeared in his journal.
On the basis of the flawed Lancet study the WHO suspended the hydroxychloroquine trials it was sponsoring. When the study was retracted they resumed them briefly but soon after suspended them again on the results of another faulty study, the Oxford University’s “RECOVERY Trial”.
The researchers in this trial gave patients massive doses of hydroxychloroquine without the necessary addition of azithromycin and they started treatment too late. That the RECOVERY Trial was never going to work was pointed out on the Covexit website two months before it started.
Prof. Raoult compared the Oxford academics who carried out the hydroxychloroquine section of the RECOVERY trial to the Marx Brothers in a video interview titled “The Marx Brothers are Doing Science – the Example of RECOVERY”
Prof. Raoult sarcastically commented that the good news that came out of the trial was that hydroxychloroquine is not toxic. The RECOVERY trial used a 2,400 mg dose on the first day compared to Dr.Raoult’s 600 mg. Even with such high dosage there were no cardiac side effects with any of the participants. Prof. Raoult recalled that “two weeks ago one was told everybody was dying because of cardiac issues. At least, this trial is good to assess the toxicity of hydroxychloroquine as they did not announce any toxicity, even at such high dosage”.
Although by now it should have been abundantly clear that hydroxychloroquine and azithromycin only worked in combination and if given early, not to patients in hospital more than seven days after infection, in April the US National Heart, Lung, and Blood Institute (NHLBI) at the National Institutes of Health (NIH) started hydroxychloroquine trials on hospitalized patients too late, some already in emergency wards, and then abandoned the trials with the conclusion that “hydroxychloroquine does no harm but provides no benefit”. The FDA cancelled its emergency use authorization and the NIH halted their clinical trials of hydroxychloroquine
The media hostile to hydroxychloroquine successfully whipped up hysteria about its supposed dangers although it has an excellent safety record and it is not even alongside aspirin on the WHO list of the 100 most dangerous drugs. Specialists and doctors prescribing hydroxychloroquine for Rheumatoid Arthritis and Lupus have confirmed that thousands of patients are being prescribed the same dose Dr. Zelenko is giving for five days for years on end without problems.
Were the failed studies faulty because of ignorance or by design? Who gains from them? The drug companies can’t make much money on a generic drug, and they found in the media and the scientific community willing accomplices to stop its use. Gilead Sciences Inc. gives grants in addition to those mentioned above to Oxford University and the WHO. Is it possible that people in these prestigious institutions may have their integrity compromised by money, or is it mere coincidence that Gilead with their rival treatment is funding them?
Some of the media will do anything to make Trump look like a fool and these faulty trials were the perfect opportunity. The media hostile to hydroxychloroquine downplayed or cast doubt on the many successful studies and trials with hydroxychloroquine and made the most of the faulty trials as proof that the drug Trump had touted didn’t work.
For the media it seems to have been more about scoring political points and increasing their audience ratings rather than investigative reporting which uncovers the truth. For those who are dying and their families and friends as a result of this treatment not being used because of media misinformation it is lives tragically lost, and for the rest of us it is our economies sinking, businesses failing, and unemployment, poverty and suffering rising.
Hundreds of thousands of lives could be saved, and loss ruin, suffering and devastation to our economies and societies avoided if we simply started using this safe, cheap and readily available treatment. It is a ludicrous and tragic farce that because of the massive misinformation on behalf of corporate greed and political point scoring that we are not.
July 12, 2020
Posted by aletho |
Corruption, Deception, Full Spectrum Dominance, Science and Pseudo-Science, Timeless or most popular | Covid-19, remdesivir, WHO, YouTube |
Leave a comment
Evidence that a cheap, over-the-counter anti-malarial drug costing £7 combats Covid-19 gets trashed. Why? Because the pharmaceutical giants want to sell you a treatment costing nearly £2,000. It’s criminal.
A few years ago, I wrote a book called ‘Doctoring Data’. This was an attempt to help people understand the background to the tidal wave of medical information that crashes over us each and every day. Information that is often completely contradictory, viz ‘Coffee is good for you… no, wait it’s bad for you… no, wait, it’s good for you again,’ repeated ad nauseam.
I also pointed out some of the tricks, games and manipulations that are used to make medications seem far more effective than they truly are, or vice versa. This, I have to say, can be a very dispiriting world to enter. When I give talks on this subject, I often start with a few quotes.
For example, here is Dr Marcia Angell, who edited the New England Journal of Medicine for over 20 years, writing in 2009:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgement of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as editor.”
Have things got better? No, I believe they’ve got worse – if that were, indeed, possible. I was recently sent the following email about a closed-door, no-recording-allowed discussion, held in May of this year under no-disclosure Chatham House rules:
“A secretly recorded meeting between the editors-in-chief of The Lancet and the New England Journal of Medicine reveal both men bemoaning the ‘criminal’ influence big pharma has on scientific research. According to Philippe Douste-Blazy, France’s former health minister and 2017 candidate for WHO director, the leaked 2020 Chatham House closed-door discussion was between the [editor-in-chiefs], whose publications both retracted papers favorable to big pharma over fraudulent data.
The email continued with a quote from that recording: ‘Now we are not going to be able to … publish any more clinical research data because the pharmaceutical companies are so financially powerful today, and are able to use such methodologies, as to have us accept papers which are apparently methodologically perfect, but which, in reality, manage to conclude what they want them to conclude,’ said The Lancet’s editor-in-chief, Richard Horton.”
A YouTube video where this issue is discussed can be found here. It’s in French, but there are English subtitles.
The New England Journal of Medicine and The Lancet are the two most influential, most highly resourced medical journals in the world. If they no longer have the ability to detect what is essentially fraudulent research, then… Then what? Then what, indeed?
In fact, things have generally taken a sharp turn for the worse since the Covid-19 pandemic struck. New studies, new data, new information is arriving at breakneck speed, often with little or no effective review. What can you believe? Who can you believe? Almost nothing would be the safest course of action.
One issue has played out over the past few months, stripping away any remaining vestiges of my trust in medical research. It concerns the anti-malarial drug hydroxychloroquine. You may well be aware that Donald Trump endorsed it – which presents a whole series of problems for many people.
However, before the pandemic hit, I was recommending to my local NHS trust that we should look to stock up on hydroxychloroquine. There had been a great deal of research over the years strongly suggesting it could inhibit the entry of viruses into cells, and that it also interfered with viral replication once inside the cell.
This mechanism of action explains why it can help stop the malaria parasite from gaining entry into red blood cells. The science is complex, but many researchers felt there was good reason for thinking hydroxychloroquine may have some real, if not earth-shattering, benefits in Covid-19.
This idea was further reinforced by the knowledge that it has some effects on reducing the so-called ‘cytokine storm’ that is considered deadly with Covid-19. It’s prescribed in rheumatoid arthritis to reduce the immune attack on joints.
The other reason for recommending hydroxychloroquine is that it’s extremely safe. It is, for example, the most widely prescribed drug in India. Billions upon billions of doses have been prescribed. It is available over the counter in most countries. So, I felt pretty comfortable in recommending that it could be tried. At worst, no harm would be done.
Then hydroxychloroquine became the center of a worldwide storm. On one side, wearing the white hats, were the researchers who’d used it early on, where it seemed to show some significant benefits. For example, Professor Didier Raoult, of the Institut Hospitalo-universitaire Méditerranée Infection, in France:
“A renowned research professor in France has reported successful results from a new treatment for Covid-19, with early tests suggesting it can stop the virus from being contagious in just six days.”
Then came this research from a Moroccan scientist at the University of Lille:
“Jaouad Zemmouri … believes that 78 percent of Europe’s Covid-19 deaths could have been prevented if Europe had used hydroxychloroquine… Morocco, with a population of 36 million [roughly one tenth that of the US], has only 10,079 confirmed cases of Covid-19 and only 214 deaths.
“Professor Zemmouri believes that Morocco’s use of hydroxychloroquine has resulted in an 82.5 percent recovery rate from Covid-19 and only a 2.1 percent fatality rate, in those admitted to hospital.”
Just prior to this, on May 22, a study was published in The Lancet, stating that hydroxychloroquine actually increased deaths. It then turned out that the data used could not be verified and was most likely made up. The authors had major conflicts of interest with pharmaceutical companies making anti-viral drugs. In early June, the entire article was retracted by Horton.
Then a UK study came out suggesting that hydroxychloroquine did not work at all. Discussing the results, Professor Martin Landray, an Oxford University professor who is co-leading the Randomised Evaluation of Covid-19 Therapy (RECOVERY) trial, stated:
“This is not a treatment for Covid-19. It doesn’t work. This result should change medical practice worldwide. We can now stop using a drug that is useless.”
The study has since been heavily criticized by other researchers, who state that the dose of hydroxychloroquine used was potentially toxic. It was also given far too late to have any positive effect. Many of the patients were already on ventilators.
This week, I was sent a pre-proof copy of an article about a study that will be published in the International Journal of Infectious Diseases. Its author has found that hydroxychloroquine “significantly” decreased the death rate of patients involved in the analysis. The study analyzed 2,541 patients hospitalized in six hospitals between March 10 and May 2 2020, and found 13 percent of those treated with hydroxychloroquine died and 26 percent of those who did not receive the drug died.
When things get this messed up, I tend to look for the potential conflicts of interest. By which I mean, who stands to make money from slamming the use of hydroxychloroquine, which is a generic drug that’s been around since 1934 and costs about £7 for a bottle of 60 tablets?
In this case, first, it’s those companies who make the hugely expensive antiviral drugs such as Gilead Sciences’ remdesivir, which, in the US, costs $2,340 for a typical five-day course. Second, it’s the companies that are striving to get a vaccine to market. There are billions and billions of dollars at stake here.
In this world, cheap drugs such as hydroxychloroquine don’t stand much chance. Neither do cheap vitamins, such as vitamin C and vitamin D. Do they have benefits for Covid-19 sufferers? I’m sure they do. Will such benefits be dismissed in studies that have been carefully manipulated to ensure they don’t work? Of course. Remember these words: “Pharmaceutical companies are so financially powerful today, and are able to use such methodologies, as to have us accept papers which are apparently methodologically perfect, but which, in reality, manage to conclude what they want them to conclude.”
Unless and until governments and medical bodies act decisively to permanently sever the financial ties between researchers and Big Pharma, these distortions and manipulations in the pursuit of Big Profit will continue. Just please don’t hold your breath in anticipation.
Malcolm Kendrick is a doctor and author who works as a GP in the National Health Service in England. His blog can be read here and his book, ‘Doctoring Data – How to Sort Out Medical Advice from Medical Nonsense,’ is available here.
July 4, 2020
Posted by aletho |
Book Review, Corruption, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, Gilead Science, remdesivir |
Leave a comment


 Aletho News
Aletho News