Bill Seeks to Muzzle Doctors Who Tell the Truth About COVID
By Dr. Joseph Mercola | May 5, 2022
One of the most stunning parts of this pandemic has been the denial of basic science, and one of the most shocking developments from that has been the attack on medical doctors who try to set the record straight.
As reported by Dr. Jay Bhattacharya — professor of health policy at Stanford, research associate at the National Bureau of Economic Research and coauthor of the Great Barrington Declaration, which calls for focused protection of the most vulnerable1 — a California bill is now threatening to strip doctors of their medical licenses if they express medical views that the state does not agree with.2
Bhattacharya’s Personal Battle
Bhattacharya has first-hand experience with this kind of witch hunt. He was one of the first to investigate the prevalence of COVID-19 in 2020, and found that by April, the infection was already too prevalent for lockdowns to have any possibility of stopping the spread.
Bhattacharya has called the COVID-19 lockdowns the “biggest public health mistake ever made,”3 stressing that the harms caused have been “absolutely catastrophically devastating,” especially for children and the working class, worldwide.4
After Bhattacharya co-sponsored the Great Barrington Declaration, Dr. Anthony Fauci, director of the National Institutes of Allergy and Infectious Diseases (NIAID) and his former boss, now retired National Institutes of Health (NIH) director Francis Collins, colluded behind the scenes to quash the declaration from day 1.5
To that end, they set out to smear and destroy the reputations of Bhattacharya and the other coauthors of the declaration. In one email, Collins referred to the three highly credentialed and respected scientists as “fringe epidemiologists” and called for a press “takedown” of the trio.6,7,8,9 I detailed this treachery in “Authors of Barrington Declaration Speak Out.”
“Big tech outlets like Facebook and Google followed suit, suppressing our ideas, falsely deeming them ‘misinformation,’” Bhattacharya writes.10 “I started getting calls from reporters asking me why I wanted to ‘let the virus rip,’ when I had proposed nothing of the sort. I was the target of racist attacks and death threats.
Despite the false, defamatory and sometimes frightening attacks, we stood firm. And today many of our positions have been amply vindicated. Yet the soul searching this episode should have caused among public health officials has largely failed to occur. Instead, the lesson seems to be: Dissent at your own risk.
I do not practice medicine — I am a professor specializing in epidemiology and health policy at Stanford Medical School. But many friends who do practice have told me how they have censored their thoughts about COVID lockdowns, vaccines, and recommended treatment to avoid the mob …
This forced scientific groupthink — and the fear and self-censorship they produce — are bad enough. So far, though, the risk has been social and reputational. Now it could become literally career-ending.”
Do You Want Your Doctor To Be Muzzled by the State?
California Assembly Bill 209811 — introduced by Assemblyman Evan Low, a Silicon Valley Democrat, and coauthored by Assembly members Aguiar-Curry, Akilah Weber and Wicks, and Sens. Pan and Wiener — designates “the dissemination or promotion of misinformation or disinformation related to the SARS-CoV-2 coronavirus, or ‘COVID-19,’ as unprofessional conduct” warranting “disciplinary action” that could result in the loss of their medical license.
Misinformation or disinformation related to SARS-CoV-2 includes “false or misleading information regarding the nature and risks of the virus, its prevention and treatment; and the development, safety, and effectiveness of COVID-19 vaccines.” But as far as what might constitute “misinformation” or “disinformation” is unclear and basically left open for interpretation — by the state. As noted by Bhattacharya:12
“Doctors, fearing loss of their livelihoods, will need to hew closely to the government line on COVID science and policy, even if that line does not track the scientific evidence.
After all, until recently, top government science bureaucrats like Dr. Fauci claimed that the idea that COVID came from a Wuhan laboratory was a conspiracy theory, rather than a valid hypothesis that should be open to discussion. The government’s track record on discerning COVID truths is poor.
The bill claims that the spread of misinformation by physicians about the COVID vaccines ‘has weakened public confidence and placed lives at serious risk.’ But how significant is this problem in reality? Over 83% of Californians over the age of 50 are fully vaccinated (including the booster) …
What is abundantly clear is that this bill represents a chilling interference with the practice of medicine. The bill itself is full of misinformation and a demonstration of what a disaster it would be to have the legislature dictate the practice of medicine.”
The Shanghai Model
We don’t have to guess at what life might look like if this and other bills like it are implemented, Bhattacharya warns. The drama currently playing out in Shanghai offers a clear look into what can happen when public health is dictated by the state rather than by qualified medical professionals rooted in sound science.
“Shanghai is the model for the terrifying dangers of giving dictatorial powers to public health officials,” Bhattacharya writes.13 “The harrowing situation unfolding there is a testament to the folly of a virus containment strategy that relies on lockdown.
For two weeks, the Chinese government has locked nearly 25 million people in their homes, forcibly separated children from their parents, killed family pets, and limited access to food and life-saving medical care — all to no avail. COVID cases are still rising, yet the delusion of suppressing COVID persists.
In America, many of our officials still have not abandoned their delusions about COVID and the exercise of power this crisis has allowed. As the Shanghai debacle demonstrates, of all the many terrible consequences of our public health response to COVID, the stifling of dissenting scientific viewpoints by the state might be the most dangerous.”
The Science Deniers Are in Power
As stressed by Bhattacharya, the California bill includes a number falsehoods and fails to acknowledge basic science, starting with natural immunity. High-quality studies have repeatedly shown that natural immunity is equivalent or superior to the COVID shots. Were this bill to pass, a California doctor could lose his license for taking a patient’s COVID history into account when recommending the shot.
It also negates doctors’ ability to prescribe off-label drugs for the treatment of COVID, even though this has been a common and uncontroversial medical practice for many decades. It’s not uncommon for a drug intended for one condition to be used off-label for another. But for some reason, when it comes to COVID, this practice is now deemed hazardous and unprofessional.
The bill also falsely asserts that the “safety and efficacy of COVID vaccines have been confirmed through evaluation by the federal Food and Drug Administration.” Anyone who has followed this circus over the past year realizes that the FDA has completely ignored loud and clear warning bells showing the shots are far from safe and nowhere near as effective as initially claimed.
The bill also ignores the fact that the safety depends on the individual patient’s medical history and current state of health. “For example, there is an elevated risk of myocarditis in young men taking the vaccine, especially with the booster,” Bhattacharya notes.14
Doctors have an ethical obligation to treat each patient as an individual, and to ensure each patient receives the safest and best care. Bill 2098 will turn doctors into government agents, leaving no one to advocate for patients’ health.
“The false medical consensus enforced by AB 2098 will lead doctors to censor themselves to avoid government sanction. And it will be their patients, above all, who will be harmed by their silence,” Bhattacharya warns.
Californians, Vote NO on COVID Tyranny Bills
California Bill 2098 isn’t the only bill seeking to enshrine tyranny into law. Other pending California bills include:15
Senate Bill 1390,16 introduced by Sen. Pan, which seeks to criminalize “amplification of harmful content” on social media platforms.
Assembly Bill 1797,17 introduced by Assembly member Weber, which calls for the creation of a centralized vaccination registry.
Senate Bill 1464,18 introduced by Pan, which would strip state funding from any law enforcement agency that “publicly announces that they will not follow, or adopts a policy stating that they will not follow, a public health order.”
Those funds would instead be reallocated to the county public health department. Essentially, this bill would coerce sheriffs and police officers to violate their conscience or the law, or both, in the name of “public health policy.”
Senate Bill 871,19 introduced by Pan, which would mandate all school children, ages 5 and older, be “fully vaccinated” against COVID-19. The bill would also repeal exceptions to mandatory hepatitis B vaccination to attend school, and would remove the personal belief exemption against vaccination.
Senate Bill 866,20 introduced by Wiener and Pan, which would authorize minors, 12 years and older, to consent to vaccines without the consent of a parent or guardian.
Senate Bill 1479,21 introduced by Pan, which would expand “contagious, infectious, or communicable disease testing and other public health mitigation efforts to include prekindergarten, onsite after school programs, and child care centers,” and require each school district, county office of education, and charter school to create a COVID-19 testing plan, and report testing data to State Department of Public Health.
If you live in California, please review these bills and VOTE NO. In a Substack article, Margaret Anna Alice, offers the following guidance to Californians:22
“If you are a resident of California, please consider taking the additional step of contacting your respective senators and assembly members in addition to filling out the online portal. See Californians for Medical Freedom for step-by-step instructions on how to contact your local legislators as well as what to say if you decide to call (which is recommended).
The PERK website is also a very helpful way to track the hearing dates and status of these bills. In the comments, Donald Tipon has provided additional links for opposing AB2098 and AB1797 from A Voice for Choice Advocacy.”
Front Groups Marshal the Ignorant
Regulating the medical views a doctor can and cannot have is dangerous in the extreme, and hopefully the Californians who are left to vote in that state will quash such efforts. On the national level, we must also stay vigilant against similar legislative proposals, and push back against phony front groups that promote this kind of medical tyranny.
This includes the No License for Disinformation23 (NLFD) group, which promotes the false information disseminated by the dark-money group known as the Center for Countering Digital Hate (CCDH).
As most now know, U.S. Sen. Rand Paul, R-Ky., a medical doctor in his own right, has been the primary challenger of Fauci’s lies, and the NLFD has been instructing individuals to report him to the Kentucky Medical Board, with the aim of getting his medical license revoked.24
An Open War on the Public
We find ourselves in a situation where asking valid questions about public health measures are equated to acts of domestic terrorism. It’s unbelievable, yet here we are. Over the past two years, the rhetoric used against those who question the sanity of using unscientific pandemic countermeasures, such as face masks and lockdowns, or share data showing that COVID-19 gene therapies are really bad public health policy, has become increasingly violent.
Dr. Peter Hotez, a virologist who for years has been at the forefront of promoting vaccines of all kinds, for example, has publicly called for cyberwarfare assaults on American citizens who disagree with official COVID narratives, and this vile rhetoric was published in the prestigious science journal Nature, of all places.25
Doctors and nurses are now facing the untenable position of having to choose between doing right by their patients and toeing the line of totalitarianism. This simply cannot go on. It’s profoundly unhealthy and dangerous in a multitude of ways.
While frustrating and intimidating, we must all be relentless in our pursuit and sharing of the truth, and we must relentlessly demand our elected representatives stand up for freedom of speech and other Constitutional rights, including, and especially, the rights of medical doctors to express their medical opinions.
Sources and References
-
-
-
- 1 Great Barrington Declaration
- 2, 10, 12, 13, 14 Bariweiss.substack.com April 12, 2022
- 3 Newsweek March 8, 2021
- 4 Rumble, Ron DeSantis March 7, 2022, 32:00
- 5 Wall Street Journal December 21, 2021
- 6 YouTube Liberty Report, 7:13 minutes
- 7 The Blaze December 18, 2021
- 8 Daily Mail December 18, 2021, Updated December 19, 2021
- 9 ZeroHedge December 20, 2021
- 11 California Assembly Bill 2098
- 15, 22 Margaret Anna Alice Substack April 12, 2022
- 16 California SB1390
- 17 California AB1797
- 18 California SB-1464
- 19 California SB-871
- 20 California SB-866
- 21 California SB-1479
- 23 Twitter No License for Disinformation
- 24 Twitter Chass October 11, 2021
- 25 Nature April 27, 2021
-
-
Missouri and Louisiana Attorneys General sue Biden over Big Tech ‘collusion’

Samizdat | May 6, 2022
Attorneys General from two Republican-led US states, Missouri and Louisiana, have filed a lawsuit against the Biden administration, Fox News reported on Thursday. The states are accusing high-ranking officials, including President Joe Biden, of having “pressured and colluded” with social media companies to censor and suppress information on a number of big stories over the past two years.
Among the officials named as defendants are White House Press Secretary Jen Psaki and the President’s Chief Medical Advisor Dr. Anthony Fauci. They, and others, are accused of exerting undue pressure on, or working together, with a number of Big Tech companies such as Meta, Twitter and YouTube to suppress information regarding the Hunter Biden laptop controversy, the origins of Covid-19, and security concerns associated with mail-in voting during the pandemic.
Missouri Attorney General Eric Schmitt and Louisiana Attorney General Jeff Landry claim the Biden Administration has been doing so “under the guise of combating misinformation.”
The lawsuit, filed on Thursday in the U.S. District Court for the Western District of Louisiana, describes the administration’s supposed efforts to hush up certain information as “one of its greatest assaults by federal government officials in the Nation’s history” on Americans’ constitutional right to free speech.
The filing goes on to claim that “Having threatened and cajoled social-media platforms for years to censor viewpoints and speakers disfavored by the Left, senior government officials in the Executive Branch have moved into a phase of open collusion with social-media companies to suppress disfavored speakers, viewpoints, and content on social-media platforms under the Orwellian guise of halting so-called ‘disinformation,’ ‘misinformation,’ and ‘malinformation’.”
In an exclusive statement to Fox News Digital, Missouri Attorney General Eric Schmitt explained the decision to file the lawsuit by saying that he would “not stand idly by while the Biden Administration attempts to trample on the First Amendment rights of Missourians and Americans.”
His colleague from the state of Louisiana, Jeff Landry, went so far as to characterize Big Tech as an “extension of Biden’s Big Government,” which is busy “suppressing truth and demonizing those who think differently.” Landry compared Joe Biden to Joseph Stalin over the president’s policies that allegedly aim to “censor free speech and propagandize the masses.” The Attorney General said the lawsuit was seeking to “ensure the rule of law and prevent the government from unconstitutional banning, chilling, and stifling of speech.”
Among the cases brought up in the filing are Twitter’s decision to disable the sharing of a 2020 New York Post story revolving around the contents of Hunter Biden’s laptop that was recovered from a repair shop in Delaware. The report was later found to be accurate by the Washington Post and the New York Times, the two Attorneys General pointed out.
In a separate instance, Facebook supposedly censored posts suggesting that Covid-19 may have accidentally leaked from a laboratory in Wuhan, China. The Attorneys General claim that it was Anthony Fauci who orchestrated an effort to “discredit” the narrative while “exchanging emails with Mark Zuckerberg, the CEO of Facebook, regarding the control and dissemination of Covid-19 information.” The campaign only began to wind down after more media outlets started reporting on the viability of the theory, the lawsuit alleges.
In addition, according to the filing, YouTube effectively censored Republican Senator Rand Paul and Florida Governor Ron DeSantis for calling into question the effectiveness of wearing cloth masks during the Covid pandemic.
Another major case where “social-media platforms aggressively censored” speech, as Schmitt and Landry allege, was the run-up to the November 2020 presidential race. The Attorneys General claim that Donald Trump’s concerns regarding the security of mail-in voting were stifled by Big Tech at the time. Trump’s tweets were flagged, with a notice directing users to the facts surrounding the practice.
As further proof that the Biden administration has been exerting undue pressure on social media platforms to suppress free speech, the filing mentions Surgeon General Vivek Murthy’s statement back in June 2021, where he said “we expect more from our technology companies… We’re asking them to monitor misinformation more closely.” Moreover, the latest launch of the new DHS disinformation board just goes to show that the current US political leadership is intent on ramping up its “campaign of censorship,” the Attorneys General warn.
Fox News, which covered the lawsuit filing, reached out to Meta, Twitter, YouTube as well as the White House for comment, but apparently none of them have replied so far.
As Vaccine Demand Collapses, U.K. Faces £4 Billion of Waste, With 80% of its 650 Million Dose Stockpile Unused
By Nick Bowler | The Daily Sceptic | May 4, 2022
The U.K. has used just 142 million of the stockpile of 650 million vaccine doses it purchased, leaving an estimated £4 billion worth of vaccines unused and, at current levels of take-up, likely going to waste. The vaccines typically have an expiration date of six to 12 months after manufacture – though it’s not clear how many of the 650 million doses have already been manufactured and put in storage and how many are on order for future manufacture and delivery.
Officials have not revealed exactly how much was paid for the Pfizer vaccines, which comprise nearly a third of the total ordered, but the U.S. Government is reputed to have paid around $20 (£16) a dose.
The Moderna vaccine is said to have cost a bit less, perhaps about $15 (£12) per dose, and the Astra Zeneca considerably less, perhaps as low as $4 (£3) per dose as it was sold at cost. There are no data on the other five types ordered, all of which are as yet completely unused.
If an average price of $10 (£8) per dose is assumed, the total bill for all the unused vaccine doses will amount to around $5 billion or £4 billion. Will the public be forgiving of this massive waste of public funds on account of it occurring with good intentions during a state of emergency? That remains to be seen.
It is however far from the only example of pandemic profligacy. The losses due to fraud and delinquent business loans are colossal, with City AM reporting that the Treasury’s £4.3bn fraud write-off is likely to be eclipsed by £20bn of Covid loan defaults. The Government has also written off £8.7bn it spent on protective equipment bought during the pandemic, with £673m of equipment unusable, £750m not used before its expiry date, £2.6bn of equipment judged to be unsuitable for use in the NHS, and £4.7bn being due to the Government paying more for it during the acute global shortage than it is now worth. The Government also spent £569m buying 20,900 ventilators, of which only 2,150 (10%) were used, the rest being left idle in a Ministry of Defence warehouse.
This gross misuse of taxpayers’ money must be examined in the independent inquiry and by Government so the lessons can be learned and in future a robust management system applied in real time so that even stocks purchased in haste and with urgency are kept in reasonable proportion to anticipated demand.
The over-reaction and panic in spring 2020 resulted in decisions that have now turned out to be a huge waste of public money. If there was perceived to be a shortage of anything that might conceivably be needed to fulfil the needs of the public emergency, the public purse was always open.
Actually, the purse appeared to be treated more like Mary Poppins’ bottomless magic carpet bag, with no sign of any prudent oversight applied to funding decisions as long as they served the purpose of proving to the public that the Government was ‘doing something’ about Covid. The results of that fiscal incontinence are now clear for all to see.
Reminder: Respiratory viruses infect huge numbers of people all the time, and nobody cared about this until 2020
Perspective from a 2018 New York study that tested a bunch of healthy adults for common respiratory viruses. Over 6% tested positive.
eugyppius | May 2, 2022
The ever-sharp Zacki on Twitter points to this intriguing 2018 study out of New York. The authors administered PCR tests to 2,685 people at a tourist attraction in New York City, between the months of January and July. Over 6% tested positive for one of seven common human respiratory viruses. In the winter, human coronaviruses were the most common; in the summer, rhinoviruses took the lead. By design, the study targeted healthy populations, and so we must imagine that it substantially understates the true rate of virus infection.
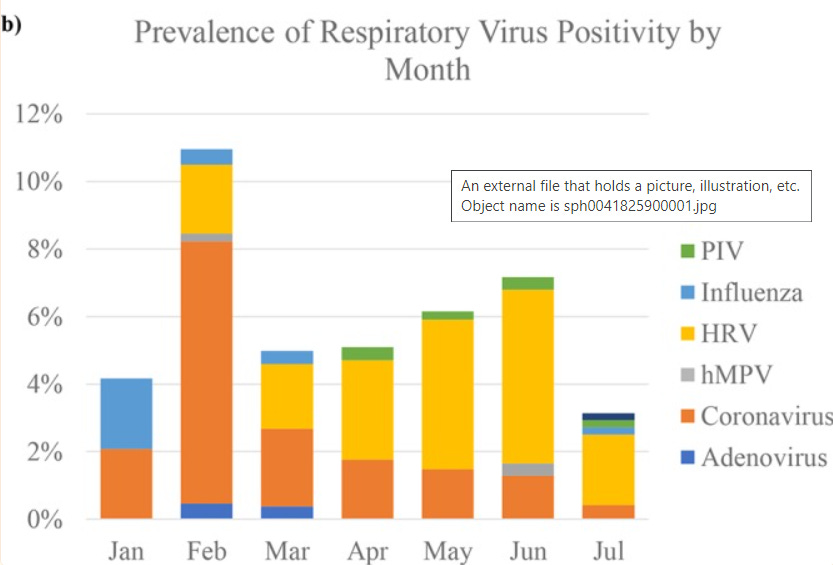
The authors don’t find a significant difference in the overall prevalence of positivity between winter and summer. In their small sample, it’s only the mix of viruses that changes. This is another piece of evidence in favour of my crazy theory, that a great part – perhaps a majority – of spring and summer allergies are in fact persistent low-grade rhinovirus infections.
Other studies, particularly on rhinovirus, find even larger incidences of infection. There is this paper, which looks at rhinovirus in infants and finds that 20% of their sample are asymptomatic positives; or this case-control study of all ages, which finds rhinovirus in 17% of their asymptomatic controls.
For perspective: At the height of the alpha wave in the United Kingdom, only about 0.3% of the population was testing positive for SARS-2 every day. School antigen testing in Germany, which is done multiple times a week and finds nearly every detectable infection in school-age children, found Delta 7-day incidences of around 1%, and Omicron 7-day incidences peaking in February at near 4% in specific age cohorts (see the the graph on p. 5). The allegedly hypercontagious SARS-2 looks like it was doing substantially worse, in other words, than garden-variety human coronaviruses in the same month in the New York study.
Respiratory viruses are extremely pervasive; they’re everywhere and this is totally normal. What isn’t pervasive, is virus testing. We’ve only ever tested widely for a single virus. So much of Corona mythology depends upon presenting data in isolation from what we know about the behaviour of all the other pathogens we’ve lived with for centuries. Our governments have spent two years hyperventilating about incidences of infection that turn out to be minuscule, or at worst normal, when compared to the other pathogens that infect us. This should also make you very, very sceptical of uncontrolled studies cataloguing alleged Long-Covid symptoms. If we tested this widely for rhinovirus, imagine all the totally unrelated symptoms we’d find in our vast pool of positive results.
Hospital and Care Home Visiting Restrictions Are “Cruel, Inhumane and Unnecessary”, Doctors Tell MPs
By Will Jones | The Daily Sceptic | April 29, 2022
The Pandemic Response and Recovery All-Party Parliamentary Group met this week to hear about visiting restrictions still being imposed by many care homes and NHS Trusts. Co-chaired by Rt Hon Esther McVey MP and Graham Stringer MP, the Group listened to evidence about the devastating effects visiting restrictions in hospitals have on patients and their loved ones. MPs also heard how visiting restrictions in care homes, along with the continued use of rolling lockdowns and over interpretation of testing guidelines, is leading to isolation, neglect and abuse of the residents.
Leandra Ashton, who co-founded The People’s Care Watchdog, Dr. Ammar Waraich, a medical registrar in the West Midlands, Carol Munt, experienced Patient Partner and Advocate and Dr. Ali Haggett, community mental health and wellbeing specialist, told MPs of the obstacles still in place when trying to visit a loved one and the shocking impact on vulnerable hospital patients, care home residents and their families.
All the speakers voiced serious concerns that obstacles are still in place in some healthcare settings. Politicians heard harrowing accounts of the harmful effects of isolation and loss of social contact on physical and mental health, safeguarding problems with medication, dehydration, hygiene and lack of basic care and the failures to uphold existing legislation to protect those who lack capacity.
Leandra Ashton’s mother was arrested in November 2020 for taking her grandmother out of her care home a day before the second lockdown. Two years on, many residents are still being isolated from their loved ones. She told MPs:
When I took the video of my mum being arrested taking my nan out of her care home, I did not think it would go viral. So many families got in touch and it led to us setting up the People’s Care Watchdog. We were struck by how much legislation is in place, such as Article 8 of the Human Rights Act, Deprivation of Liberty and the Mental Capacity Act, to protect those in care homes. These laws are simply not being upheld and instead guidelines are being over-interpreted and the legislation even used to keep people in care homes and hospitals as if they were prisons. The public bodies that are supposed to uphold the protective legislation are not doing so.
There are still obstacles in place when trying to visit a loved one in a care home and the impact has been and continues to be devastating. The safeguarding issues I am seeing and hearing about are atrocious. Residents left for hours in dirty, wet incontinence pads leading to dangerous pressure ulcers. Malnutrition. Dehydration. End of life medication given to patients without their or their family’s consent. Psychological trauma, post-traumatic stress and suicides have resulted because of this. Multiple systems are failing, including Local Authorities and the CQC. It is a complex situation that needs a bold approach by both empowering families and galvanising Government action to hold public bodies to account and stop private equity firms placing profit over people.
Listening to the evidence, Esther McVey said:
I am troubled by the evidence presented by our speakers, particularly the safeguarding issues and neglect that care home residents are suffering as a result. In hospitals, we have heard about patients losing hope and refusing treatment without the encouragement of family. We know patients have much better treatment outcomes when they have support from relatives and friends around them.
Most of the infection control measures that restricted visiting in healthcare settings have been removed, most recently NHS Trusts were told healthcare workers, patients and visitors no longer need to distance in hospitals, so I fail to see why and how these visiting restrictions are still in place in any healthcare setting. I shall be writing to the Secretary of State for Health and Social Care to ask that he makes it absolutely clear that all patients and residents must be able to see visitors.
Highlighting how visitation is an important and necessary part of healthcare, Carol Munt said:
In the same way that we would not stop prescribed medication and treatments, we should not have stopped visits. Why were decisions taken without any consideration for the need of patients and their families to connect? Why do we still have such variation in compassionate care across the country? There is no uniformity among care homes apart from the need to be profitable for their owners. Some care homes made a superhuman effort to arrange visiting, as did the Bristol Nightingale Hospital. There was good practice in some places so there should be good practice everywhere. We should expect more of these endemic situations and we must be prepared for them.
I could not comprehend how any Minister for Health and Social Care could allow this to happen and not make the effort to get his department to look at ways that visiting could be facilitated. I heard and continue to hear the most callous reports of relatives dying alone with no visitors. The same goes for hospital patients. Ultimately, I think we need legislation to ensure that visiting rights are enshrined and protected.
Medical Registrar Dr. Ammar Waraich reported that many hospitals are still preventing visits due to the potential risk of Covid spread:
The policy is cruel, inhumane and unnecessary. Seeing loved ones can be immensely therapeutic and give struggling patients the will to survive. It is deeply traumatic for families to lose loved ones suddenly or see them go through difficult treatment without being there in person. Video calls are not a good enough replacement and we do not have the staff, the time or resources to facilitate calls for all our patients.
Most infection control measures have been lifted as the level of risk is no longer there. Hospitals can no longer function as detention centres and an inpatient stay should not become a sentence. The policy was one of the major mistakes of lockdown. Visiting sick relatives in hospital is, and must remain, a fundamental right, not to be given up.
Co-chair Graham Stringer said:
I find it extraordinary that no visiting is allowed in some healthcare settings, even to this day. It is cruel that family members are being denied access to sick and vulnerable loved ones, often not getting regular updates, living in anxiety about what their relatives may be going through, but knowing they are going through frightening and difficult treatment, often at the end of their lives, without being able to be with them in person.
“At the height of the pandemic it was understandable that there were precautions but there is no longer a basis to that argument. All the restrictions have been lifted and NHS Trusts across England have now been told to ‘return to pre-pandemic physical distancing in all areas’. The government must take action to resolve this situation.
Speaking about her experience working in the community throughout the pandemic, Dr. Ali Haggett said:
I have spent the last eighteen months with the support group Unlock Care Homes, uncovering the plight of many thousands of families who are still denied regular, meaningful contact with care home residents and hospital patients. Even before Covid, we knew that isolating people, particularly older people, has a serious impact on physical and psychological health. We have continued to isolate adults in care and in some hospitals almost continuously for two years. The effects have been felt particularly badly by those with dementia. Many residents no longer recognise their families and have been denied the most basic of human needs.
My concern is that this situation is concealing neglect and abuse on a significant scale. One of my community members sadly died and the hospital has admitted liability partly because he was completely blind and couldn’t reach his food or drink. Had his wife been allowed to visit, this wouldn’t have happened. Families I work with report numerous issues still affecting them, not just visiting restrictions. Rolling lockdowns, over-interpretation of testing, PPE requirements resulting in poor communication and fear, lack of ancillary services such as podiatry or physiotherapy leading to huge health problems, residents asked to isolate when one person tests positive, sometimes for 10 days or more and the one significant visitor recommendation being ignored or rejected. Families must be able to visit openly and check the wellbeing of residents.
Stop Press: MPs and Peers including Esther McVey, Lord Frost, Sir Iain Duncan Smith, Sir Graham Brady, Emma Lewell-Buck, Graham Stringer and Sammy Wilson have written to the Telegraph to say they are “deeply concerned” that visiting is still forbidden in many institutions where “over-interpretation of testing guidelines is leading to isolation, neglect and abuse of vulnerable residents”. They point out that Article 8 of the Human Rights Act and the Mental Capacity Act “could and should have protected against this situation arising” but this legislation is being “wilfully misinterpreted as an excuse” to keep people isolated in care homes and hospitals “as if they were prisons”.
Masks may have caused MORE Covid deaths
The Naked Emperor’s Newsletter | April 30, 2022
A newly published, peer-reviewed study in Cureus looked to see if there was a correlation between mask compliance and COVID-19 outcomes in Europe. The study was undertaken at the University of Sao Paulo in Brazil.
The authors noted that previous trials about mask effectiveness had produced mixed results and those that concluded that masks were associated with a reduction in transmission and cases were conducted out of season.
“The World Health Organization (WHO) as well as other public institutions…strongly recommend the use of masks as a tool to curb COVID-19 transmission. These mandates and recommendations took place despite the fact that most randomised controlled trials carried out before and during the COVID-19 pandemic concluded that the role of masks in preventing respiratory viral transmission was small, null, or inconclusive. Conversely, ecological studies, performed during the first months of the pandemic, comparing countries, states, and provinces before and after the implementation of mask mandates almost unanimously concluded that masks reduced COVID-19 propagation.
However, mask mandates were normally implemented after the peak of COVID-19 cases in the first wave, which might have given the impression that the drop in the number of cases was caused by the increment in mask usage. For instance, the peak of cases in Germany’s first wave occurred in the first week of April 2020, while masks became mandatory in all of Germany’s federal states between the 20th and 29th of April, at a time when the propagation of COVID-19 was already declining.
Furthermore, the mask mandate was still in place in the subsequent autumn-winter wave of 2020-2021, but it did not help preventing the outburst of cases and deaths in Germany that was several-fold more severe than in the first wave.”
Due to the different levels of masking in Europe (5% – 95% compliance), it gave the authors the opportunity to test masking during a strong COVID-19 wave.
“Data were collected from the following Eastern and Western European countries: Albania, Bosnia and Herzegovina, Bulgaria, Croatia, Czechia, Hungary, North Macedonia, Poland, Romania, Serbia, Slovakia, Slovenia, Belarus, Estonia, Latvia, Lithuania, Republic of Moldova, Ukraine, Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, United Kingdom, and Northern Ireland. The inclusion criterion was a population size higher than one million people.”
Analysis was undertaken to verify if masking correlated with COVID-19 morbidity and mortality. The data looked at were between October 2020 and March 2021, in the 35 European countries listed above, during which all the countries went through a peak COVID-19 infection wave.
The average proportion of masking was 60.9% with Eastern Europe being slightly higher than Western Europe. However, compliance was much more homogeneous in the East than the West.
Importantly, results showed a weak positive correlation for mask compliance versus morbidity (cases) and mortality (deaths).
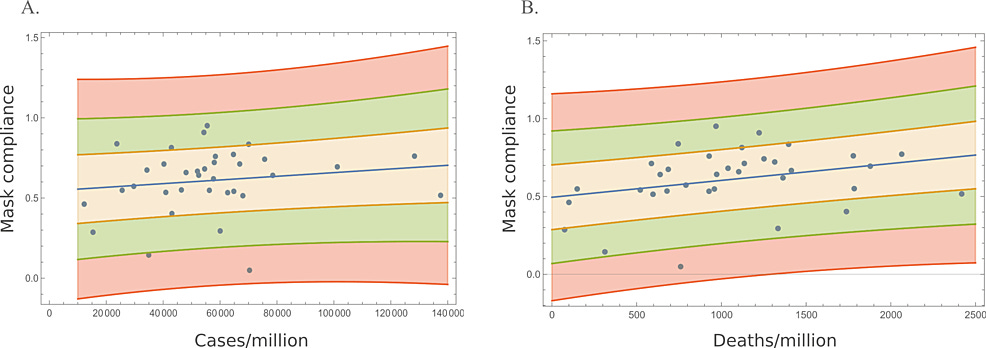
Each dot in the diagrams above represent a different country. As you can see, as mask compliance goes up, so do cases/million and deaths/million.
Please note, the positive correlation for mask usage and cases was not statistically significant. However, the correlation for masks and deaths WAS statistically significant.
The correlation was even higher in the West compared to Eastern countries. It is suggested that this could be because larger countries are located in the West. However, even when the largest countries were removed, the correlations hardly changed.
Various other analyses were performed, e.g. using smaller and larger countries but no tests resulted in negative correlations.
The authors conclude by saying that “while no cause-effect conclusions could be inferred from this observational analysis, the lack of negative correlations between mask usage and COVID-19 cases and deaths suggest that the widespread use of masks at a time when an effective intervention was most needed, i.e., during the strong 2020-2021 autumn-winter peak, was not able to reduce COVID-19 transmission. Moreover, the moderate positive correlation between mask usage and deaths in Western Europe also suggests that the universal use of masks may have had harmful unintended consequences.”
Science is finally catching up with the science that disappeared two years ago. Whilst this study is not conclusive, it is quite damning and will be interesting to see what masking mandates or recommendations are brought back, next winter, after this.
Blame the unjabbed – whatever the facts
By Guy Hatchard | TCW Defending Freedom | April 29, 2022
The writer is in New Zealand
THE business magazine Forbes has published a story with the arresting headline: ‘Unvaccinated People Increase Risk Of Covid Infection Among Vaccinated, Study Finds.’
The work to which it refers is not in the normal sense a study but is actually a modelling exercise published by the journal of the Canadian Medical Association. Did the Forbes staff writer read the paper very well? I am quite sure not. At the end of paragraph one of the Method section of the original paper, it describes its model, saying: ‘A vaccine that is 80 per cent efficacious would result in 80 per cent of vaccinated people becoming immune, with the remaining 20 per cent being susceptible to infection. We did not model waning immunity.’
Now I am sure you know that the mRNA vaccines do not stop infection and also wane in effectiveness. In other words mRNA vaccination does not confer immunity and its effectiveness does not remain constant as the paper assumes. So what use is this paper and to what do its conclusions apply? Apparently not to the mRNA Covid vaccines.
Lo and behold, one of the paper’s authors, David Fisman, declares competing interests: ‘He has served on advisory boards related to SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca and Sanofi-Pasteur Vaccines.’
Another author, Ashleigh Tuite, was ‘employed by the Public Health Agency of Canada when the research was conducted’ (aka the domain of Justin Trudeau).
So why publish this story which on the face of it has little relevance to the real-world data of the current pandemic? Forbes magazine is 51 per cent owned by a Hong Kong-based company, Integrated Whale Investments, about which little is known. The Washington Post has suggested that Forbes’s editorial policy has been influenced as a result, but by whom no one really knows.
At this point in the pandemic, it has become clear that boosted individuals are becoming more vulnerable to Omicron than the unvaccinated. So I can only suggest that it might be advantageous for some scientists and politicians to blame the unvaccinated for everything in order to cover up their own mistaken ideas. Or perhaps there are commercial interests anxious to sell more arguably useless vaccines for billions of dollars. You decide.
If the government and their compliant media friends are our one source of truth, as has happened in New Zealand (by decree), then you have no option except to blame the unvaccinated whatever happens.
The actual situation is that the unvaccinated are currently less likely to be hospitalised than the boosted. Thank you to Grant Dixon for compiling and graphing NZ Ministry of Health data, below.

This morning my mask-exempt friend entered a haberdashery shop, whereupon two other potential customers turned and fled. Yesterday she was turned away from a fabric store. I am sure many of you have had similar experiences. The fact of the matter is that almost the whole of the New Zealand population has become subject to fear-based government-sponsored groupthink.
Are we all being conditioned to vote for Jacinda Ardern in next year’s election based on the carefully constructed myth that she is keeping us all safe? We should be keeping our feet on the ground. We should recognise that public relations experts and propaganda promoters are at work full-time, but they are working out of touch with reality.
Meanwhile our whole economy is becoming ever more dysfunctional. As people are too afraid to associate with one another in public, the whole basis of commercial activity is being undermined.
The two large supermarket chains are laughing all the way to the bank. As small businesses are forced to close and their monopoly grows, supermarket prices and profits are entering the stratosphere. Smart individuals are now ordering their vegetables and groceries direct from Australia (as far away from us as Moscow is from London) because they are so much cheaper.
The government is clueless to control this rampant price inflation, along with most things including the pandemic. The public is hoodwinked, queueing fully masked and fully vaccinated to pay through the nose for everyday items without a squeak of dissent.
The ten-year-old son of a friend asked his mother the other day: ‘Which do you think our society is more like – Brave New World or 1984?’ I doubt if either Aldous Huxley or George Orwell could ever have imagined anything so incomprehensibly doublethinking as 2022 New Zealand.
This is the state we have reached through our government’s careful rationing of information and saturation conditioning.
Time we reopened the floodgates of free speech and social media – hold your horses, we might endanger our one source of truth.
Strike off the truth tellers? No, strike out Whitty & Co!

By Angus Dalgleish | TCW Defending Freedom | April 30, 2022
THE recent announcement from the General Medical Council that doctors face being struck off for spreading fake news on vaccines and lockdowns is somewhat frightening given the recent experience of Dr Sam White, a GP in Hampshire. It has a chilling Orwellian overtone to it.
It seems to imply that fake news is anything not approved by the Government and any of its agencies such as Public Health England and the NHS plus the mainstream media, who have been bribed throughout the pandemic with lucrative advertising contracts.
It assumes that ideas and speculation from discredited sources such as Neil Ferguson and Sage were correct and accepted by the senior medical officers such as Chris Whitty and Patrick Vallance, with all other inputs ignored or treated with contempt. Many of us suggested that as Covid was an airborne virus which affected mainly the old and those with other medical conditions it should be treated as such. This was based on knowledge accrued from years of treating such unknown upper respiratory tract infections (URTIs) which involves correcting the hideously low levels of vitamin D3 in the population and treating symptoms with regular gargling of aspirin and mouthwash and intranasal sprays. In short, vitamin D3 and topical anti-inflammatory medicines abort colds and flu when given early and frequently.
Why was this not made official policy? I observed severe Covid symptoms melt with such a regimen in many friends and colleagues.
Secondly, why were doctors not allowed to give dexamethasone, which is known to be life-saving in cases of lung inflammation? No, we had to wait for a trial to tell us it worked. A colleague calculated that 4,000 to 5,000 patients died unnecessarily through this decision, which the Chief Medical Officer has to own.
Also why did they stamp on any original idea such as ivermectin, which was dismissed as ‘worm treatment for horses’ when it clearly has some benefit in some Covid cases?
What I am driving at here is that common sense can be classified as fake news by the ever-increasingly power-crazed authorities. The greatest example of this ill-informed madness was the decision to enforce lockdowns not once but twice. It has been calculated that lockdown probably averted 200 Covid deaths but the advisers took no account of the effects on other conditions by denying screening and early treatment of cancer, heart attacks, strokes, not to mention the infliction of severe mental health problems and chronic stress (I personally know of four suicides, two of them medical colleagues). This is before we get on to the big picture – the destruction of young lives, education and the economy.
For what? Sweden refused to follow the lockdown route and not a single child lost a day’s education.
Our experts who felt entitled to tell us what to do and conspired to denigrate those of us with an alternative take such as Professor Sunetra Gupta, myself and other Great Barrington declarants. They cruelly derided Sweden’s state epidemiologist Anders Tegnell for refusing to back lockdown, with 2,000 of his own condemning him.
It has now been accepted by all bar the CCP in China that lockdown was an absolute and avoidable disaster. Yet those of us who were right would be persecuted and prosecuted and struck off by this new emanation from the GMC. Dr Sam White also thought that masks were a waste of time, something every one of the government advisers has agreed with at some time, but they were insisted upon by the Department of Fear, Intimidation and Control of the Population.
Next comes the ‘vaccine’ project. In spite of our warning that a good vaccine needs a powerful T-cell adjuvant, and that the 80 per cent of the spike which mimicked human sequences and was likely to induce side-effects should be omitted, we were dismissed as not important or eminent enough to heed. The vaccines that the establishment backed were experimental medicines designed to reduce morbidity and death in the older population and of course to save the NHS.
So why were they imposed on the whole population without testing to see if they were needed? Even the BCG vaccine was given only to non-tuberculin reactors after a test.
My colleagues started to see serious reactions especially in those below 55 years, which have now been accepted to be real, such as blood clots, strokes, heart inflammation and death. Our original report highlighted the sequence in the spike similar to a neurological protein and severe neurological damage has now been officially recognised. For pointing this out early we were accused of being anti-vaxxers. No, we were not! We were just trying to save people from serious side-effects from a disease with an 0.085 per cent fatality rate.
Presumably the GMC would now strike off anyone, such as Sam White, trying to do the best for their patients. No, they should be looking at the real culprits for this mayhem and whether they had the skills and experience to make these decisions (they did not).
Bizarrely, in this brave new world they were given knighthoods.
Featured Video

Roosevelt’s Partnership with Stalin
or go to
Aletho News Archives – Video-Images
From the Archives
“Democratic Institutions?” – 10 Lessons from history that will destroy your trust in the CIA
By Kit | OffGuardian | July 20, 2018
… At every corner, we are urged to simply believe what we are told. Whether it is about believing Porton Down and MI6 about “novichok”, or believing the White Helmets about Sarin, or believing the FBI about “collusion”, we are presented with no facts, just assertions from authority. Those who question those assertions are deemed “bots” at best or “traitors” at worst.
Well here, fellow traitors, are the Top Ten reasons to question anything and everything the CIA – or any intelligence agency – has ever told you. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran Beat Back The Greater Israel Project
- Roosevelt’s Partnership with Stalin
- Strategic Ambiguity (If We Must)
- Finland shreds nuclear weapons ban
- Kiev turns to ‘systematic killing’ of Zaporozhye plant staff – Russia’s nuclear chief
- Censored Lavrov article Politico refused to publish (FULL TEXT)
- Israel’s censor silenced 5,700 reports in 2025
- After US-Iran deal, Israeli minister threatens war on Syria ‘sooner or later’
- When the Iran War is over: Why the West Bank may be Netanyahu’s next front
- Israeli forces launch fresh ground incursions into Syria’s Quneitra, interrogate locals
- If Americans Knew
- What Ceasefire? Israel Has Now Killed Over 1,000 Palestinians in Gaza Since October
- U.S. Whole-of-Government Takeover by Israel
- Netanyahu’s Mouthpieces Turn on Trump, Revealing a Deeper Israeli Ingratitude
- Senate wants to force US to share sensitive intel with Israel
- Trump ended his idiotic Iran war. Good.
- Khanna Becomes First in Congress to Sign ‘Peace Pledge’ Promising to Reject AIPAC Funds
- Look who’s losing it over Trump’s Iran deal
- Israel has killed over 1,000 Gazans during 8-month “ceasefire” – Daily Update
- REVEALED: Former Top DEA Official Says Israel Spies on US Law Enforcement
- What would happen if US actually cut off military aid to Israel?
- No Tricks Zone
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
