State Dept. Not Investigating Saudi Use of US Weapons in Alleged War Crimes: GAO

Samizdat | June 16, 2022
The Government Accountability Office (GAO) published a scathing report Monday which found that the Department of Defense and the Department of State “have not fully determined the extent to which U.S. military support has contributed to civilian harm in Yemen.” The news comes on the heels of the announcement that US President Joe Biden will be paying a visit next month to Saudi Arabia, a country which in 2019 he pledged to turn into a “pariah.”
“Despite several reports that airstrikes and other attacks by Saudi Arabia and UAE have caused extensive civilian harm in Yemen, [the Department of Defense] has not reported and [the State Department] could not provide evidence that it investigated any incidents of potential unauthorized use of equipment transferred to Saudi Arabia or UAE,” the GAO report concluded.
In February 2021, US President Joe Biden declared he was ending “all American support for offensive operations” in the Saudi war on Yemen. GAO monitors pointed out that while US Military Training Mission staff claimed that “all of the equipment the US sells… to Saudi Arabia must be for defensive purposes,” the “officials could not provide a definition for equipment that is defensive in nature when asked how they distinguish between equipment used for defensive purposes and equipment used for offensive purposes.”
Instead, the report’s authors noted, State Department officials “told us they have no specific definitions for what constitutes ‘offensive weapons’ and ‘defensive weapons’ to direct the sale of weapons to Saudi Arabia.”
The report also found that from fiscal year 2015 to 2021, the “Department of Defense administered at least $54.6 billion of military support to Saudi Arabia and the United Arab Emirates, of which over a third, or $18.3 billion, came in the form of missiles. The remaining military aid was reportedly spent as follows: $7.6 billion on equipment maintenance, $6.2 billion on aircraft, $4.9 billion on “special activities,” $4.6 billion on communication, detection, and coherent radiation equipment, $3.3 billion on ships, $2.8 billion on training, $1.4 billion on construction, $1.2 billion on ammunition, $1.1 billion on support equipment, $900 million on weapons, and $1.8 billion on other expenditures like combat, tactical, and support vehicles, as well as research and development.
Although “the United Nations has characterized the conflict in Yemen as one of the world’s worst humanitarian crises,” the report’s authors explain that the US has “long-standing security relationships with Saudi Arabia and UAE—two primary actors in the conflict—and has continued to provide them military support, including for operations in Yemen since 2015.”
In April, 32 US Congress members urged Secretary of State Anthony Blinken to commit to a “recalibration of the US-Saudi partnership,” noting that the US’ “continued unqualified support for the Saudi monarchy, which systematically, ruthlessly represses its own citizens, targets critics all over the world, carries out a brutal war in Yemen, and bolsters authoritarian regimes throughout the Middle East and North Africa, runs counter to US national interests and damages the credibility of the United States to uphold our values.”
But with Biden’s announcement that he’ll be flying to Riyadh next month for what the Saudi embassy described as “official talks” between Joe Biden and Prince Mohammed bin Salman, the odds of such an adjustment taking place–and of US agencies taking a more proactive approach towards American involvement in alleged Saudi war crimes–are growing ever-slimmer.
WHO Pandemic Treaty a “Power Grab at behest of Big Pharma and Big Donors”: Former UN Asst. Secretary-General
BY WILL JONES | THE DAILY SCEPTIC | JUNE 16, 2022
Former United Nations Assistant Secretary-General Ramesh Thakur has warned in the Spectator of the coming massive expansion of the international pandemic bureaucracy and the powers of the WHO to press countries towards authoritarian public health measures. The WHO’s track record during COVID-19 hardly merits reward with further powers, he says.
Health includes mental health and wellbeing and is highly dependent on a robust economy, yet the WHO-backed package of measures to fight Covid has been damaging to health, children’s immunisation programs in developing countries, mental health, food security, economies, poverty reduction, social and educational wellbeing of peoples. Their worst effects were grievous assaults on human rights, civil liberties, individual autonomy and bodily integrity. To make it worse, in promoting these policies the WHO violated, without providing any justification beyond China’s example, (1) the guidance from its own report in October 2019 that summarised a century’s worth of worldwide experience and science; and (2) its own constitution which defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. The vaccine push has similarly ignored accumulating safety signals about the scale of adverse reactions, on the one hand, and rapidly dwindling efficacy after successive doses, on the other.
Euro-U.S. efforts, backed by Australia, to amend legally binding international health regulations and adopt a new pandemic convention would confer extraordinary powers on the WHO to declare public health emergencies of international/regional concern and command governments to implement their recommendations. WHO inspectors would have the right to enter countries without consent and check compliance with their directives. They would lock in the lockdowns-vaccines narrative and preempt rigorous independent retrospective reviews of their costs and efficacy. The ‘reforms’ amount to a WHO power grab at the behest of Big Pharma and Big Donors. Whether approved as two separate instruments or folded into one overarching new treaty, the changed architecture will greatly strengthen the WHO’s core capabilities on public health surveillance, monitoring, reporting, notification, verification and response. The rush to amend the existing international health regulations encountered significant pushback last month from developing countries, China and Russia but will come up again for discussion and approval shortly. The new treaty under negotiation will be presented to the World Health Assembly in 2024.
The proposed reforms to international health agreements will only make things worse, he says.
On January 24th, Director-General Tedros Adhanom Ghebreyesus said an urgent priority was to “strengthen WHO as the leading and directing authority on global health”, for: “We are one world, we have one health, we are one WHO.” On April 12th, he said the Covid crisis had “exposed serious gaps in the global health security architecture”; the new treaty would be “a generational agreement” and “a gamechanger” for global health security. If adopted, it will consolidate the gains of those who have benefitted from COVID-19, concentrating private wealth, increasing national debts and decelerating poverty reduction; expand the international health bureaucracy under the WHO; shift the centre of gravity from common endemic diseases to relatively rare pandemic outbreaks; create a self-perpetuating global biopharmaceutical complex; shift the locus of health policy authority, decision-making and resources from the state to an enlarged corps of international technocrats, creating and empowering an international analogue of the administrative state that has already thinned national democracies. It will create a perverse incentive: the rise of an international bureaucracy whose defining purpose, existence, powers and budgets will depend on outbreaks of pandemics, the more the better.
Western media and politicians prefer to ignore the truth about civilians killed in Donetsk shelling

Remnants of the Uragan MLRS rocket which struck the Donetsk maternity hospital June 13. © Eva Bartlett / RT
By Eva Bartlett | Samizdat | June 16, 2022
Following intense Ukrainian shelling of Donetsk on June 13, some Western media sources, in tandem with outlets in Kiev, unsurprisingly claimed that the attack – which killed at least five civilians and struck a busy maternity hospital – was perpetrated by Russian forces.
Why Moscow would launch rockets at its own allies wasn’t explained, nor would it make much sense.
The Donetsk People’s Republic’s foreign ministry reported: “Such an unprecedented. in terms of power, density and duration of fire, raid on the DPR capital was not recorded during the entire period of the armed conflict [since 2014]. In two hours, almost 300 MLRS rockets and artillery shells were fired.”
The Ukrainian shelling began late morning, resumed in the afternoon, and continued for another two hours in the evening, a deafening series of blasts throughout the city, terrorizing residents and targeting apartment buildings, civilian infrastructure, the aforementioned hospital, and industrial buildings.
Locals say this was some of the heaviest bombing of Donetsk since 2014, when the eponymous region declared its independence from post-Maidan Kiev.
In the Budyonnovsky district in the south of the city, Ukrainian shelling of a market killed five civilians including one child. Just two months ago, Kiev’s forces hit another Donetsk market, leaving five civilians dead.
In the hard-hit Kievskiy district, to the north, the shelling caused fires at a water bottling plant and a warehouse for stationery, destroying it. The building was still in flames when journalist Roman Kosarev and I arrived about an hour after the attack. Apartment buildings in the area also came under firer, leaving doors and windows blown out and cars destroyed.
The destroyed gas station was on a street where I stayed in April, which is completely residential.
DPR head Denis Pushilin said, “The enemy literally crossed all the lines. Prohibited methods of warfare are being used, residential and central districts of Donetsk are being shelled, other cities and settlements of the DPR are also under fire now.”
Hypocritical silence after maternity hospital shelling
In a world where media reported honestly instead of manufacturing its own reality, there would be outrage over Ukraine’s attack on the Donetsk maternity hospital. But history shows that is not a world we live in.
As I wrote last year, Western media and talking heads also diligently avoided condemnation when terrorists attacked or destroyed Syrian hospitals, including the shelling of a maternity hospital in Aleppo, which killed three women.
At the damaged Donetsk hospital, I saw the gaping hole in the roof and remnants of the Uragan MLRS rocket which struck it. Most of the windows of both buildings were blown out.
Images shared on Twitter noted, “Both gynecology and intensive care have been bombed.” Other footage, taken by Donetsk war correspondent Dmitri Ashtrakhan, showed dozens of women, some heavily pregnant, taking shelter in the basement of the shelled maternity hospital.
Were these women and this hospital in Kiev, you can bet Western media would be loudly reporting it 24/7 for weeks. Instead, just as the West has steadfastly ignored Ukraine’s eight years of war on Donbass, they also omit reporting on the hospital.
Grotesquely, some Ukrainian and Western media instead disingenuously reported that it was a Russian attack, not Ukrainian, which terrorized, injured and killed civilians on June 13.
Just as Western media’s lack of reporting, or twisting of the narrative, on Ukraine’s shelling was to be expected, so too was the UN’s weak-worded condemnation, with the Spokesman for the Secretary-General, Antonio Guterres, calling it “extremely troubling.” You can bet that were the situation reversed and Russia responsible for bombing a Ukrainian maternity hospital, his words would have been far stronger.
In fact, they already have been: Three months ago, when Kiev accused Russia of an attack on a maternity hospital, in Mariupol.
Back then, the Guterres emphatically tweeted, “Today’s attack on a hospital in Mariupol, Ukraine, where maternity & children’s wards are located, is horrific. Civilians are paying the highest price for a war that has nothing to do with them. This senseless violence must stop. End the bloodshed now.”
A strong reaction to what later emerged to be a hoax claim, when the UN itself even admitted it could not verify the story. But a mild reaction to a documented reality in Donetsk.
The UN did, at least, rightly note the attack on the Donetsk maternity hospital was, “an obvious breach of the international humanitarian law.” So there’s that.
The thing is, Ukraine has violated international law for its eight years of waging war on the Donbass republics, using prohibited heavy weapons and targeting civilians and civilian infrastructure. This is only the latest incident.
Tears flow for hoax hospital bombing
In March, Western corporate-owned media supported Kiev’s claim that Russia had launched air strikes on a Mariupol maternity hospital, claiming three civilians had been killed. At the time, as reported, “The White House condemned the ‘barbaric’ use of force against innocent civilians, and UK Prime Minister Boris Johnson tweeted that ‘there are few things more depraved than targeting the vulnerable and defenceless’.”
As it turned out, witnesses reported there hadn’t been any air strike. There were explosions: just as terrorists bombed an Aleppo home in 2016 and used a mildly injured boy for their propaganda against Syria and Russia, so too did Ukrainian forces in Mariupol, setting the stage to incriminate Moscow.
Russia called the accusations “a completely staged provocation,” analyzing photos from the area and noting “evidence of two separate staged explosions near the hospital: An underground explosion and another of minor power, aimed at the hospital building,” and further noting that a “high-explosive aviation bomb would destroy the outer walls of the building.”
Russia also pointed out that the facility had stopped working when Ukraine’s neo-Nazi Azov Battalion expelled staff in late February and militarized the hospital, as Ukrainian forces did elsewhere in Donbass.
Marianna Vyshemirskaya, one of the women featured in the Western propaganda around the hospital, later spoke out and said there was no air strike, and that prior to the alleged event, Ukrainian soldiers expelled all the doctors and moved pregnant women to another building.
She also maintained that she and other women were filmed without warning by an Associated Press journalist dressed in a military uniform and wearing a helmet.
Even now, two days after Ukraine’s intense bombardment of Donetsk and targeting of the maternity hospital, when still more testimonies have emerged, Western media and politicians remain silent.
The suffering, and deaths, of the people of Donetsk doesn’t fit the Western narrative, so they misreport it or simply just don’t reference it at all, enabling Ukraine to continue to commit war crimes.
Eva Bartlett is a Canadian independent journalist. She has spent years on the ground covering conflict zones in the Middle East, especially in Syria and Palestine (where she lived for nearly four years).
Turkey & Russia Suggest Path for Grain Ships to Access Ukrainian Ports
By Kyle Anzalone and Will Porter | The Libertarian Institute | June 16, 2022
Ankara and Moscow have put forward potential solutions to reopen Ukraine’s Black Sea ports, with Russia offering safe passage to ships while Turkey said it could help guide vessels around Ukrainian naval mines deployed to stall the Russian advance.
Russia’s UN Ambassador Vassily Nebenzia told reporters on Wednesday that the Kremlin is open to creating a “safe passage” for grain shipments, but said Moscow could not guarantee a route that would be free of mines
“We are not responsible for establishing safe corridors. We said we could provide safe passage if these corridors are established,” he said. “It’s obvious it’s either de-mine the territory, which was mined by the Ukrainians, or ensure that the passage goes around those mines.”
While Turkey has said it would “take some time” to clear away the munitions, Foreign Minister Mevlut Cavusoglu suggested safe corridors could be found in some Ukrainian ports, presenting the offer as a short-term solution.
“Since the location of the mines is known, certain safe lines would be established at three ports,” the FM said earlier on Wednesday, adding that ships could “come and go safely to ports without a need to clear the mines.”
Cavusoglu went on to say that Ankara has not received a response from the Kremlin on the proposal, but is currently working with the United Nations on a plan. UN spokesman Stephane Dujarric confirmed that discussions were underway, though noted that an agreement from both Ukraine and Russia would be needed to move forward.
Turkey’s National Defense Minister Hulusi Akar, meanwhile, told TRT that the three nations recently created an “emergency communication mechanism” to resolve the problem and reopen Ukraine’s ports, but it’s not yet clear whether any progress had been made in negotiations. Last Sunday, President Recep Tayyip Erdogan also announced that he plans to hold a three-way dialogue on the issue with his Russian and Ukrainian counterparts sometime in the coming weeks, after Ankara hosted several rounds of lower-level peace talks.
Kiev, however, has signaled that it will not accept the Russian or Turkish proposals. Speaking at an event in Washington on Wednesday, David Arakhamia, a lawmaker and the head of Ukraine’s negotiation team, said “Our military people are against [de-mining the ports], so that’s why we have very, very limited optimism for this model.”
The UN has warned that the disruption of grain exports from Ukraine could have a massive impact on global food supplies. Together, Moscow and Kiev provide up to 40% of Eastern Europe’s grain purchases, and make up an even greater part of some countries’ total imports.
While Ukrainian and American officials have repeatedly blamed Russia for the shortages, Moscow has rejected the charge, instead pinning the scarcities on US sanctions and the explosives still deployed at key Ukrainian seaports. The Kremlin previously offered to help establish a safe route for shipping vessels in exchange for sanctions relief, but Washington refused to take up the deal.
The US and its Western partners have attempted to cripple the Russian economy through heavy sanctions in response to the invasion, some pledging outright embargoes on the country’s energy exports. While the penalties initially sent the ruble tumbling, it has since made a significant comeback and is now among the best performing currencies against the dollar in 2022. Meanwhile, the White House is now quietly pushing US shipping companies to do business with Russian fertilizer suppliers.
The conflict raging in Eastern Europe has not severed all business ties between Moscow and Kiev, as Ukraine’s state-run Naftogaz has continued to work with its Russian equivalent, Gazprom. Though the two firms have reportedly done hundreds of millions of dollars in trade since the war kicked off in February, the shaky truce could soon fracture, as Naftogaz is now pursuing a lawsuit against Gazprom for alleged underpayment.
Google, Twitter, Meta, TikTok and more just signed the EU’s “anti-disinformation” code
By Dan Frieth | Reclaim The Net | June 16, 2022
Big Tech companies have signed a new version of the European Union’s “anti-disinformation” code. Some of the companies that signed include Google, Twitter, Meta, TikTok, and Twitch – but also smaller players such as Vimeo and Clubhouse.
There are 34 signatories in total:
- Adobe
- Avaaz
- Clubhouse
- Crisp Thinking
- Demagog
- DOT Europe
- European Association of Communication Agencies (EACA)
- Faktograf
- Globsec
- Interactive Advertising Bureau (IAB Europe
- Kinzen
- Kreativitet & Kommunikation
- Logically
- Maldita.es
- MediaMath
- Meta
- Microsoft
- Neeva
- Newsback
- NewsGuard
- PagellaPoltica
- Reporters without Borders (RSF)
- Seznam
- The Bright App
- The GARM Initiative
- TikTok
- Twitch
- Vimeo
- VOST Europe
- WhoTargetsMe
- World Federation of Advertisers (WFA)
Apple declined to sign.
The “code of practice on disinformation,” will require online platforms to show how they are tackling “harmful content.”
It will also require platforms to fight “harmful misinformation” by forming partnerships with fact-checkers and developing tools. They will be forced to include “indicators of trustworthiness” on information verified independently on hot-button issues like COVID-19 and Russia’s invasion of Ukraine.
Perhaps the most notable requirement is providing their efforts to tackle harmful content and disinformation on a country-by-country basis. The move was opposed by online platforms, but national regulators demanded that they need more specific data to better address the spread of disinformation.
The EU’s vice president for values and transparency Věra Jourová, who is in charge of the code, said “to respond to disinformation effectively, there is a need for the country- and language-specific data. We know disinformation is different in every country, and the big platforms will now have to provide meaningful data that would allow to understand better the situation on the country level.”
“Russia’s actions have informed to shape the anti-disinformation code,” she said. “Once the code is operational, we will be better prepared to address disinformation, also coming from Russia.”
The new code also requires online platforms to provide other data, including the AI systems deployed to tackle “disinformation,” number of bots removed, and the number of content moderators in each country.
The code applies immediately but allows for a six-month implementation period for platforms to adhere to the strict rules.
Russia to export agricultural products to ‘friendly countries’ only
Samizdat | June 16, 2022
Russian Minister for Agriculture Dmitry Patrushev said on Thursday that the country’s grain harvest could reach 130 million tons this year, which would be enough to cover both domestic needs and ensure export potential.
Speaking on the sidelines of the St. Petersburg International Economic Forum (SPIEF), he pointed to numerous challenges including broken supply chains and difficulties with financial calculations.
Patrushev said Russia has to overcome these obstacles in order to provide food to the countries that need it most. “Our [agricultural] products will be on foreign markets, but only in those countries that are friendly to us, that do not create hurdles and difficulties for us,” he told reporters.
Russia is expecting a bumper grain crop this year, including a record wheat harvest, President Vladimir Putin said last month. He added that a number of countries are facing the threat of famine, stressing that the blame for this situation lies entirely with “the Western elites.”
The grain crisis is being felt across the globe as wheat prices have surged to record highs over the past two months. The global food market, already affected by weather and the Covid pandemic, was dealt another blow due to the Russia-Ukraine conflict and Western sanctions on Moscow. This has sparked fears of global food insecurity and hunger.
Nord Stream Can Stall Completely in the Event of New Turbine Problems: Russian UN Envoy
Samizdat | 16.06.2022
The pipeline, which supplies a significant proportion of the natural gas imported by Germany, reduced its output to just 60% after its operator failed to receive one of the turbines that pump the gas from maintenance in Canada due to anti-Russia sanctions. The warnings of a further reduction in the capacity prompted a 25% spike in EU gas prices.
Further problems with the repair and maintenance of turbines that pump the gas flowing through the Nord Stream pipeline could bring a halt to its operation, Russia’s Permanent UN Ambassador Vladimir Chizhov has warned in his speech at the St. Petersburg International Economic Forum (SPIEF).
Such scenario would be a disaster for Germany, which significantly depends on gas supplies from this pipeline, Chizhov added.
“We should ask [the turbine’s manufacturer] Siemens, why the turbines must undergo maintenance in Canada. […] I don’t want to give any advice, but I think they could have learnt by now how to repair [turbines] themselves”, Chizhov said.
The UN envoy further called EU plans for a seventh sanctions package against Russia a “strategic mistake”. He added that Russia will start dealing with its consequences once the sanctions package is adopted.
The anti-Russia sanctions are the reason why German giant Siemens can’t return Russia’s Nord Stream turbines, which had been sent to Canada for maintenance. Siemens said that it was looking into ways to solve the problem.
While the German company is looking for a solution, the Russian company Gazprom announced on 14 June that Nord Stream’s output capacity had fallen to 60% due to an inability to retrieve the turbine which had undergone maintenance. Its output dropped to 100 million cubic metres versus 167 million per day at peak. The company warned that it would be further reduced on 16 June to 67 million cubic metres per day for the same reason.
On the news of a further reduction in Nord Stream output capacities, the price of gas in Europe jumped 25% in one day (15 June) exceeding $1,300 per thousand cubic metres. On the trading day’s opening the price was up 2% compared to around $1,069 per thousand cubic metres as of the close of the previous day’s trading.
Should the patient really get the drug?
By Sebastian Rushworth, M.D. | June 14, 2022
I recently gave a lecture to 70 primary care physicians here in Stockholm, titled “should the patient really get the drug?”. The lecture seemed to generate quite a bit of cognitive dissonance among some in the audience, based on the somewhat aggressive discussion that followed the lecture, which suggests to me that much of what I was saying was stuff they had literally never been exposed to before – not at any point in medical school, and not at any point during their careers after medical school either. Cognitive dissonance is good. It’s the first step towards change.
I thought it would be interesting to re-write the lecture as an article, so that more people can hopefully achieve similar levels of cognitive dissonance. Please feel free to share it with any doctors you know that you think might benefit from an expanded perspective. Anyway, here we go.
Let’s imagine a common patient. Every primary care physician meets this patient, or someone much like her, on an almost daily basis. She’s 75 years old, and overweight. She experienced a wrist fracture two years ago, and was subsequently diagnosed with osteoporosis. She has high cholesterol levels, but she’s never had a heart attack or other “cardiovascular event”. On top of that, she has type 2 diabetes, chronic knee pain due to osteoarthritis, and high blood pressure. She was diagnosed with depression a few years ago, after her husband died.
Our patient takes seven drugs every day:
- Alendronate, because of her weak bones.
- Atorvastatin, because of her high cholesterol levels.
- Sertraline, because of her depression.
- Metformin, because of her type 2 diabetes.
- Insulin, also because of her type 2 diabetes.
- Paracetamol (a.k.a. acetaminophen), because of her knee pain.
- Enalapril, because of her high blood pressure.
So, the question is, are these drugs doing her any good?
Well, to answer that question, we need to consider NNT (Number Needed to Treat). NNT is the number of patients who need to take a drug for one patient to achieve a noticeable benefit.
For alendronate, the NNT is 20, i.e. if you treat 20 people for a couple of years, you prevent one fracture. For atorvastatin the NNT is 200, i.e. you need to treat 200 people for five years or so in order to prevent one heart attack. For sertraline, the NNT is 7, which means that you need to treat seven people in order to have a noticeable effect on depression in one patient. Note that this doesn’t mean that one out of seven gets cured of their depression, it just means that there is a noticeable difference on a rating scale for depression.
For metformin, the NNT is 14 – If you treat 14 type 2 diabetics with metformin for ten years, you prevent one death. For enalapril, the NNT is 70 – If you treat 70 people with high blood pressure with enalapril for five years or so, you prevent one stroke.
For insulin, however, there is no NNT, because insulin has not been shown to result in any benefit on any clinically relevant outcome, even though big studies have been carried out that have included thousands of patients and followed them for five or ten years. Note here that we’re talking about insulin for type 2 diabetics. When it comes to type 1 diabetes, insulin is pretty much magical – you don’t even need to do a randomised trial in order to show benefit. People with type 1 diabetes virtually return from the dead when treated with insulin. But when it comes to type 2 diabetes, there is no benefit, at least not to any hard outcomes. All insulin has been shown to do is reduce blood sugar, but it’s never been shown to result in any meaningful patient oriented benefit for type 2 diabetics.
The same is true for paracetamol/acetaminophen. When it comes to patients with knee pain due to osteoarthritis, the drug doesn’t provide any benefit whatsoever.
Ok, so we have seven drugs, and we know what their NNT’s are. If we plus the probabilities of benefit together, then we get the probability that our 75-year old woman will benefit in some way from at least one of the drugs she’s taking. So, what probability of benefit do we get?
We get 30%. Only 30%.
What that means is that there is a 70% probability that this woman doesn’t benefit at all from any of the seven drugs that she takes every day for years on end!
If you told her, I’d say there are pretty good odds she’d decide to stop taking her pills. Seven drugs a day, every day, and two to one odds of zero benefit.
And we haven’t even talked about harms yet. Because none of these pills are inert. All have widespread biological effects. And all can cause harms. So any rational treatment decision must include not just the potential benefits, but also the potential harms.
For figuring out harms, we have NNH (Number Needed to Harm), which is the counterpoint to NNT. NNH is the number of patients who need to get a drug for one to be harmed. Like I said, the drugs all have widespread biological effects, so there isn’t just one NNH – there is an NNH for each possible harm. That means that there are multiple NNH’s for each drug.
With our 75-year old woman and her seven drugs, we don’t have time to go through the NNH for every possible side effect, so we’re just going to look at a few, and put them side by side with the NNT, to get a somewhat more complete picture of benefits vs harms. I’ve tried to make sure that the NNH numbers apply to the same time period as the NNT numbers, since otherwise it’s an apples to oranges comparison.
If we do that, we get something like this:
Alendronate
NNT: 20 (fractures)
NNH: 200 (esophagitis), 260 (atrial fibrillation), 4,000 (osteonecrosis)
Atorvastatin
NNT: 200 (cardiac infarction)
NNH: 20 (myalgia), 20 (type 2 diabetes)
Sertraline
NNT: 7 (depression)
NNH: 2 (sexual disturbance), 10 (hyponatremia)
Metformin
NNT: 14 (death)
NNH: 2 (stomach upset), 5 (B12 deficiency), 1,000 (lactic acidosis)
Enalapril
NNT: 70 (stroke), 125 (death)
NNH: hyperkalemia (10), acute kidney failure (100)
Insulin
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: severe hypoglycemia (5), weight gain (1)
Paracetamol/acetaminophen
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: Hypertension (30), liver damage (?)
It’s possible to quibble here about specific NNT and NNH numbers. Different studies show different things. And many of the numbers come from studies carried out by pharmaceutical companies, which generally means that the risk of a certain side effect is massively underestimated (as we will discuss shortly). The point here isn’t to get hung up on any of the specific numbers. It’s to illustrate that we quickly end up with a very complex equation, where it in many cases isn’t clear at all whether the benefits outweigh the harms.
Take alendronate, as an example. We know that it decreases fractures in elderly osteoporotic women. But it doesn’t decrease hospitalisations. The only reasonable conclusion is that the reduction in hospitalisations that is seen due to the reduction in fractures is made up for by an increase in hospitalisations due to the many and varied side effects. So at the end of the day the only way to decide whether or not to take the drug is to have a detailed discussion with the patient and get them to decide which set of risks they’d rather be taking.
Hippocrates is supposed to have said “primum non nocere”, which is latin for “first, do no harm”. Actually he didn’t say that, and couldn’t have even if he wanted to. Hippocrates was greek, and didn’t speak latin. The quote comes from a 19th century American physician, Worthington Hooker.
Of course, as doctors, we all know that “first, do no harm” is completely unrealistic. Every intervention we do carries some measure of risk. If our primary guiding principle was to never do harm, we literally would never be able to do anything. A more reasonable principle is “only do something if the benefits clearly outweigh the risks”. If it isn’t clear to you that the benefits of a drug outweigh the harms, then don’t give it to the patient.
That’s a good general rule to stick by. However, it probably isn’t enough, for a few reasons we’re now going to discuss.
A study was published in JAMA Internal Medicine in 2021 that sought to establish how good physicians are at estimating the likelihood that a patient has a certain disease. 500 primary care physicians in the US were asked to consider various hypothetical scenarios, and then answer what they thought the probability of disease was. Here’s an example of a scenario that they were asked to consider:
Ms. Smith, a previously healthy 35-year-old woman who smokes tobacco presents with five days of fatigue, productive cough, worsening shortness of breath, fevers to 102 degrees Fahrenheit (38.9 degrees centigrade) and decreased breath sounds in the lower right field. She has a heart rate of 105 but otherwise vital signs are normal. She has no particular preference for testing and wants your advice.
How likely is it that Ms. Smith has pneumonia based on this information? ___%
Ms. Smith’s chest X-ray is consistent with pneumonia. How likely is she to have pneumonia? ___%
Ms. Smith’s chest X-ray is negative. How likely is she to have pneumonia? ___%
Go ahead and make your own guesses in relation to each of the three questions.
Once you’ve done that, you can take a look at the table below, and the answers will be revealed.

So, for our pneumonia example above, we see that the actual initial risk of disease based on the presented information was around 35%. If we then move along and look at what the doctors answered, they thought the risk was 80-85%. In other words, they thought pneumonia was more than twice as likely as it actually was!
The same phenomenon was seen in all clinical scenarios tested. The doctors consistently overestimated the initial risk, and they continued to overestimate the risk after both a positive and a negative test result. In some cases the difference between reality and what the doctors thought was huge, with the doctors overestimating risk by a factor of ten or more.
What can we conclude from this?
Doctors consistently overestimate disease risk.
Hold that thought, as we move on to take a quick look at another study, which was published in BMJ Open in 2015. This study sought to do something about a problem inherent in statin trials (and for that matter, all trials in medicine), which is that the results they produce, in the form of percent absolute risk, percent relative risk, and NNT, are so abstract that they’re completely meaningless to patients (and for that matter, to doctors as well). We know that statins have an NNT of 200 when used for primary prevention (to prevent a heart attack in someone who has risk factors but hasn’t already has a heart attack), and 40 when used for secondary prevention (to prevent additional heart attacks in someone who has already experienced a heart attack). But what do those numbers actually mean? Are they good or bad?
What the patient really wants to know is “how much longer will I live if I take this drug?”
So, what the researchers did was gather together data from all the big randomised trials of statins, and use the survival curves provided to estimate how much longer the patients actually lived. Here’s what they came up with:

All the big statin trials are included here. What’s interesting to do is look at the NNT provided, and then compare that with the number to the right of it, which is how much longer the patients actually lived, on average. So, for the ALLHAT trial, to take the topmost example, we have an NNT (for primary prevention) of 250, which comes down to a postponement of death of 4.96… well, 4.96 what?
Is it years? No.
Is it months? No
The patients in the statin group lived 4.96 days longer than the patients in the placebo group. That is what the NNT of 250 means in real terms.
Let’s look instead at 4S, which was published in 1994 and is the statin trial that has produced the best results of any statin trial ever. It’s the trial that initiated the massive boom in statin prescribing that we still see today. In 4S, the NNT (for secondary prevention) is 27.8. So, in other words, one in 27.8 patients benefited from the treatment.
But what does that actually mean in terms of life extension?
It means 27 days.
Not as impressive as you would have thought, right?
When the researchers put all the data together, from all the trials, in order to get an overall average, what they found was that when statins are used for primary prevention they prolong life by 3 days. When they are used for secondary prevention, they prolong life by 4 days.
I can imagine quite a few patients turning down the offer of a statin if they knew that it will on average only prolong their life by days.
The purpose of bringing up this study was to illustrate the following general point:
Doctors consistently overestimate the benefit of the drugs they prescribe.
Hold that thought in your mind as we move on and look at a third study.
This one was published in The Lancet Healthy Longevity in 2021. It compared the rate of serious side effects seen in randomised trials with that seen in the real world. If randomised trials give us good information about what to expect in reality, then the rate of serious side effects in the trials should be the same as that seen in reality.
But that isn’t what the researchers found. What they found was that serious side effects were three to four times more common in reality than they are in the randomised trials! Three to four times!
How is this possible?
Well it’s important to remember that the randomised trials are funded and run by the drug companies, and the drug companies want to sell their drugs, so they will do what they can to make side effects appear as rare as possible.
Why is this a problem? Because it’s the randomised trials that doctors mostly use as a basis for determining whether a drug is safe to give to a patient or not.
So, what can we conclude from the study?
Doctors consistently underestimate side effects of drugs.
Ok, so we have three conclusions, that are all pointing us in the same direction:
- Doctors consistently overestimate disease risk.
- Doctors consistently overestimate drug benefit.
- Doctors consistently underestimate drug harm.
What does this lead to?
Massive overprescribing of drugs.
Peter Gotzche, a founding member of the Cochrane Collaboration and former director of the Nordic Cochrane Center, has estimated that prescription drugs are now the third biggest cause of death in the western world, after heart disease and cancer.
That on its own should lead to massive humility among all doctors about our drug prescribing. It should make us much more careful every time we think about prescribing a drug to a patient.
Ok, so we’ve identified the problem. The causes of this problem are many and complex, so I’m just going to bring up one that each of us as doctors can actually do something about – industry sponsored meals.
A study was published in JAMA Internal Medicine in August 2016 that sought to estimate the extent to which physicians are influenced by partaking in industry sponsored meals, which often take the form of a lecture about a specific drug given by an drug company salesperson, which the physician is supposed to sit and listen to in return for getting a free meal. Industry sponsored meals are very common. Most physicians probably take part in at least a couple of these per year, and many take part in far more than that.
As the saying goes, “there’s no such thing as a free lunch”. The drug companies are not charities whose goal it is to keep starving doctors alive. If they spend vast sums of money of sponsored meals, it’s because they’re pretty damn sure that it increases sales of their drugs, and thereby their profits.
So, anyway, the study sought to estimate the extent to which industry sponsored meals influence physician prescribing patterns, by comparing participation in such meals with later prescribing behaviour. Here’s what they found:

They looked at four different drugs. As I think is clear from the tables, participation in industry sponsored meals increased prescribing of the drug the meal was about, and the more such meals a doctor participated in, the more often he or she prescribed that drug.
The purpose of these meals is not to educate us, or make us better doctors. It’s the opposite – the purpose is to make us do a specific profit-driven company’s bidding. And it works.
If you’re a doctor, and you think you don’t get influenced by participating in industry sponsored meals, then you are very naive. The more industry sponsored meals we participate in, the worse doctors we become.
Doctors in general massively underestimate the extent to which their thoughts, beliefs, and opinions are influenced by the pharmaceutical industry. We like to think that we are evidence based. But the truth is that much of what we think we know is not based on sound scientific knowledge, but on pharmaceutical industry propaganda, which quickly becomes clear to anyone who starts going through the studies in detail themselves.
On that note, I strongly recommend reading these three books, all written by physicians, to help get some perspective on the scale of the problem we face in relation to the pharmaceutical industry.
- Bad Pharma by Dr. Ben Goldacre
- Doctoring data by Dr. Malcolm Kendrick
- Deadly medicines and organised crime by Dr. Peter Gotzsche
There is one very simple thing every doctor can do, to at least partially free themselves from the onslaught of drug company propaganda, and that is to refuse to take part in industry sponsored lunches, and all other forms of industry sponsored “education”. Just say No.
Ok, so, that’s number one: refuse to take part in industry sponsored lunches.
What else can you do as a doctor?
Well, something that was once considered standard, but has fallen by the wayside in recent decades, is to never have a patient on more than five drugs at the same time. With drugs, as with everything else, there is a state of diminishing returns – the more you add, the less benefit (and more harm) each additional drug confers. So try to keep a patient on at most five simultaneous drugs. If you want to add a sixth, then rank them all, and get rid of the one that you think is least important. Most likely, the sixth least important drug in a list of six is not going to do anything useful for the patient anyway, just increase their risk of harm.
Ok, so that’s number two: try to avoid having your patients on more than five drugs simultaneously.
Number three: go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit. As any doctor will know, it’s common for patients to stay on drugs for years, even though the original reason they were put on the drug resolved itself a long time ago. The patient often doesn’t remember why they were put on the drug in the first place, but they keep taking it dutifully. Drug lists require regular pruning or they will become increasingly bloated as the years go by, which is one reason why so many elderly people are on 15 simultaneous drugs or more.
Number four: only prescribe a drug if the benefits clearly outweigh the harms. This should be obvious, but it requires a deep knowledge of the size of both potential benefit and potential harm, which unfortunately most doctors lack. And what they think they know is often incorrect because it’s based more on pharma propaganda than real science.
As a doctor, the only way to get around this is to start doing your due diligence and getting in to the weeds of the scientific studies. Do that for the ten drugs you prescribe most commonly, so that you’re an expert on those ten drugs, and you’ve already done a lot. If a patient asks you about the probability of benefit and the probability of harm, you should be able to answer that question correctly, at least for the ten drugs you use most frequently. It requires an up-front investment of time, but it will pay massive dividends to your patients over the remainder of your career.
Ok, so that was number four: only prescribe a drug if the benefit clearly outweighs the harm.
Here’s number five: prioritise lifestyle changes. Most of the diseases that doctors spend most of their time dealing with are caused by poor lifestyle choices. And most can be rectified by switching to good lifestyle choices, which invariably produce greater benefits than any drug can, with less risk of harm.
Doctors can accomplish a lot with their patients with simple lifestyle coaching. To take one example, a primary care clinic in the UK decided to try putting their type 2 diabetic patients on a ketogenic diet, since the drugs they were using clearly weren’t making the patients better. They published their six year follow up results in BMJ Nutrition, Prevention, and Health in 2020.
Over six years, the patients following the ketogenic diet decreased their median HbA1c (a measure of average blood sugar over the preceding few months) from 66 to 48. Normally, that would be unheard of. HbA1c doesn’t decrease over time in a type 2 diabetic. It increases. Yet here it was far better at the end of the six years than at the beginning. The same goes for body weight. Normally it goes up over time. But here the median decreased from 99 kg to 91 kg. And on top of that, median systolic blood pressure dropped from 152 to 141.
All this just with a simple diet intervention. Thanks to the improvements in all health markers, the patients were able to get off a lot of their drugs. This meant that after six years, the clinic was spending less than half as much money on anti-diabetic drugs as the other primary care clinics in the region.
To take another example of a simple lifestyle intervention, a randomised trial published in BMJ in 2021 that was carried out in nursing homes in Australia found that a diet high in protein has an effect on fracture risk that is equivalent to that seen with bisphosphonates.
There is a massive amount that can be accomplished with simple lifestyle interventions, and since they are much less risky than drugs, and actually treat the underlying problem rather than just putting a patch on top of it, they should be the primary intervention we use whenever possible. Drugs should be viewed as a complement to lifestyle interventions. It shouldn’t be the other way around.
Ok, so that was my fifth and final point. I’ll repeat the five points here again. These are five things that you as a doctor can do about the situation we currently find ourselves in, where prescription drugs are the third biggest killer in the western world:
- Refuse to participate in industry sponsored lunches and other industry sponsored “education”.
- Try to avoid having your patients on more than five drugs simultaneously.
- Go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit.
- Only prescribe a drug if the benefits clearly outweigh the harms.
- Prioritise lifestyle changes.
Senators want DHS chief Mayorkas to answer for “misleading” testimony about disinformation board
By Dan Frieth | Reclaim The Net | June 15, 2022
In a letter to Senate Homeland Security Committee Chairman Gary Peters, senate Republicans are demanding that Department of Homeland Security Secretary Alejandro Mayorkas answer for his testimony about the paused Disinformation Governance Board that contradicts newly-discovered documents.
We obtained a copy of the letter for you here.
According to the letter, Senators Josh Hawley and Chuck Grassley obtained documents from a whistleblower with detailed information about the disinformation board that contradicts what Mayorkas testified.
According to the documents, the disinformation board was created to to monitor online speech about “conspiracy theories about the validity of elections” and “disinformation related to the origins of effects of COVID-19 vaccines or the efficacy of masks.” It also said that the controversial board wanted to partner with Twitter to suppress certain speech and wanted to meet with Twitter executives to determine how this could be done.
Under oath on May 4, Mayorkas said that the disinformation board had not yet started working. Speaking to media outlets, Mayorkas said that the board would focus on cartels and foreign adversaries and would not spy on Americans, something that was contradicted by the leaked documents.
The letter demands that Mayorkas testify again to clear the contradictions between his previous testimony, his public statements, and the documents provided by the whistleblower.
The letter states: “We are deeply concerned that documents recently obtained by Senators Josh Hawley and Chuck Grassley contradict the Secretary’s testimony and public statements about the Board. The American public deserves transparency and honest answers to important questions about the true nature and purpose of the Disinformation Governance Board and it is clear that Secretary Mayorkas has not provided them – to the public or this Committee.
“Therefore, we request you hold a hearing with Secretary Mayorkas and join us in insisting that all records related to the Board be provided to the Committee prior to the hearing.”
Developmental Disorders in Babies born to Vaccinated Mothers?
Pfizer wants Babies to be Exposed to SIX Vaccine Shots!
By Igor Chudov | June 10, 2022
I will explain that
- Children of Covid vaccinated mothers were never tested for developmental disorders
- CDC recently revised and lowered developmental milestones, and removed some entirely
- Newly born babies will be exposed to SIX doses of mRNA vaccines if the FDA’ approves the Pfizer vaccine.
An interesting article came out:
This article found that at one year of age, babies born to mothers who had COVID (not vaccine), had a roughly twice-higher rate of neurodevelopmental disorders:
those born to the 222 mothers with a positive SARS-CoV-2 polymerase chain reaction test during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first 12 months after delivery, even after accounting for preterm delivery.
Considering that COVID is a bad disease for a sizable minority of people, there is no surprise. Covid is bad and gives people all sorts of problems. Then I started thinking: a lot of adverse effects of Covid vaccines mimic the adverse effects of Covid. The younger is the vaccine recipient, the worse some effects of vaccination (such as myocarditis) are.
A great number of expectant mothers received up to three Covid vaccine shots during pregnancy. Did anyone bother testing one-year-old children of vaccinated and boosted (during pregnancy) women for neurodevelopmental disorders, before approving this vaccine for all pregnant women?
The question is, obviously, rhetorical, since “mRNA Babies” of triple-vaxed-during-pregnancy mothers are only beginning to get born right now and are at most a few months old. Not one such baby reached a year of age. So nobody tested them for developmental disorders at one year of age, before approving the three vaccine shots for expectant mothers.
The usual argument of vaccinators that “since Covid does it too, you should take the vaccine” does not hold water. To a woman who decided to take the vaccine, the probability of getting a vaccine is 100%. The probability of her getting Covid is much less. In the above study, out of 7,772 births, only 222 (2.8%) were exposed to Covid during pregnancy. So while vaccination is 100% guaranteed for those who elect to vaccinate, the chance of Covid is over 30 times less likely. And the “vaccine” does not prevent Covid anyway and does not even reduce the viral load.
There is literally zero data on one-year-old children of triple-vaccinated mothers because the oldest ones are 3-4 months old as of today.
However, there are disturbing developments regarding newborns. Vaccination does seem to have an effect on births and pregnancies.
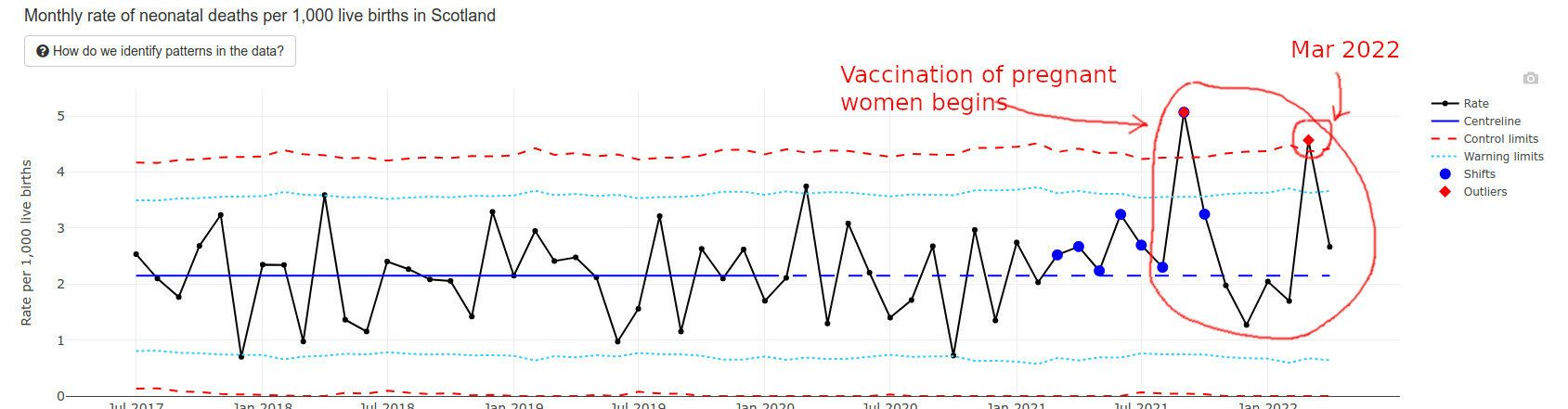
The best data I found regarding recently born newborns happens to come from Scotland. They have an interesting “wider impacts” page that I am quoting below.
Infant deaths are way above average and exceeded “Alert Limits” twice.
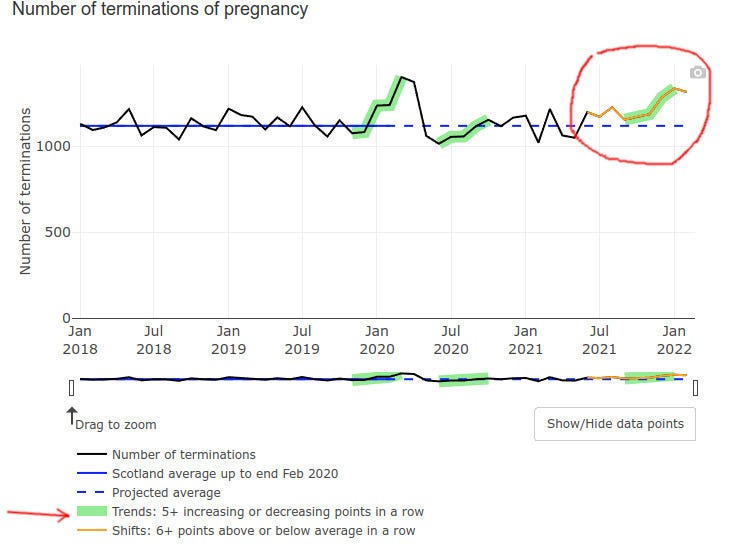
Even pregnancy terminations went up at the end of 2021, possibly but not certainly explained by prenatal vax problems:
Low Apgar score births (for those readers who do not have kids, Apgar score is how healthy is the baby at birth, the best being a score of 10) triggered a green alarm signal:
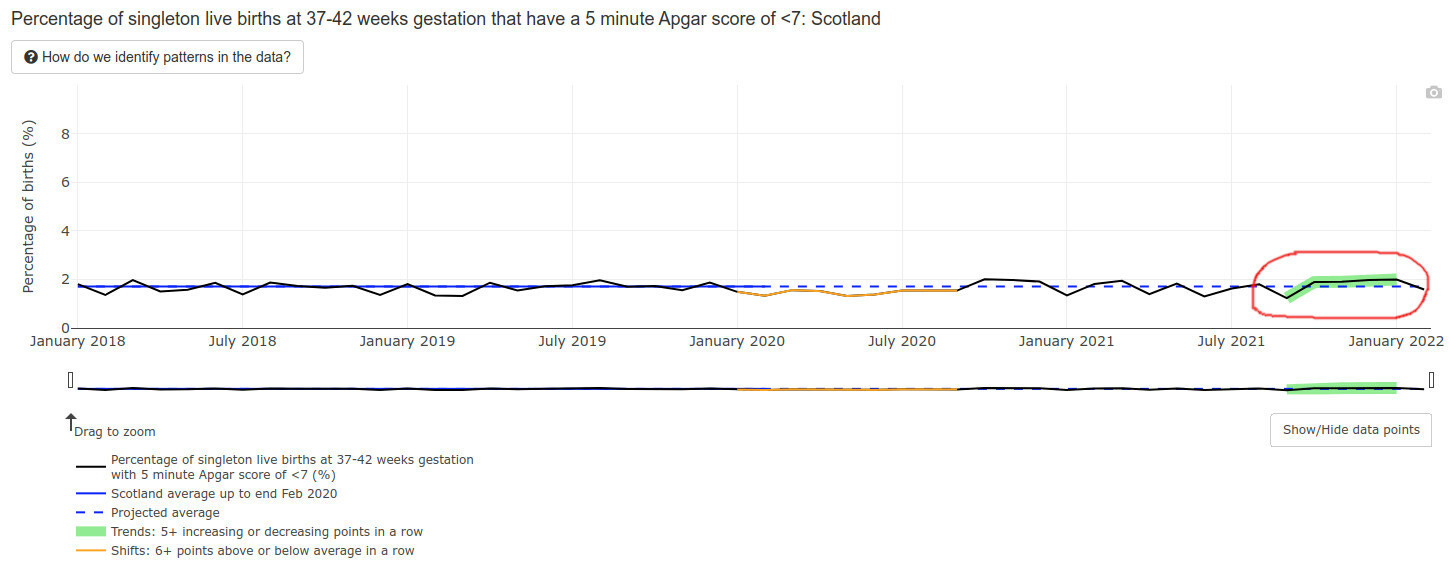
Mind you, an Apgar score is also a developmental evaluation of sorts — at 5 minutes after birth. What will happen to the developmental milestones of those lucky babies of vaccinated mothers, who survived the pregnancies, did not die postnatally, and lived to one year of age? I literally have no idea and nobody else in the world does — the time has not passed yet.
The data we have is NOT encouraging.
CDC Solution: Remove and Lower Milestones
The CDC possibly caught a whiff of this, because in February of 2022 they literally removed half the developmental milestones, bumped some others to higher ages, and lowered standards for yet more of them. (Hat tip @CLesterwood)
About one-third of milestones like fine motor skills have been bumped up to older ages. Because of the setback, children may worsen their developmental delay, making it harder to provide early intervention, explains Jessica Hatfield, MS, OTR/L, a pediatric occupational therapist for TheraTree Pediatric Therapy.
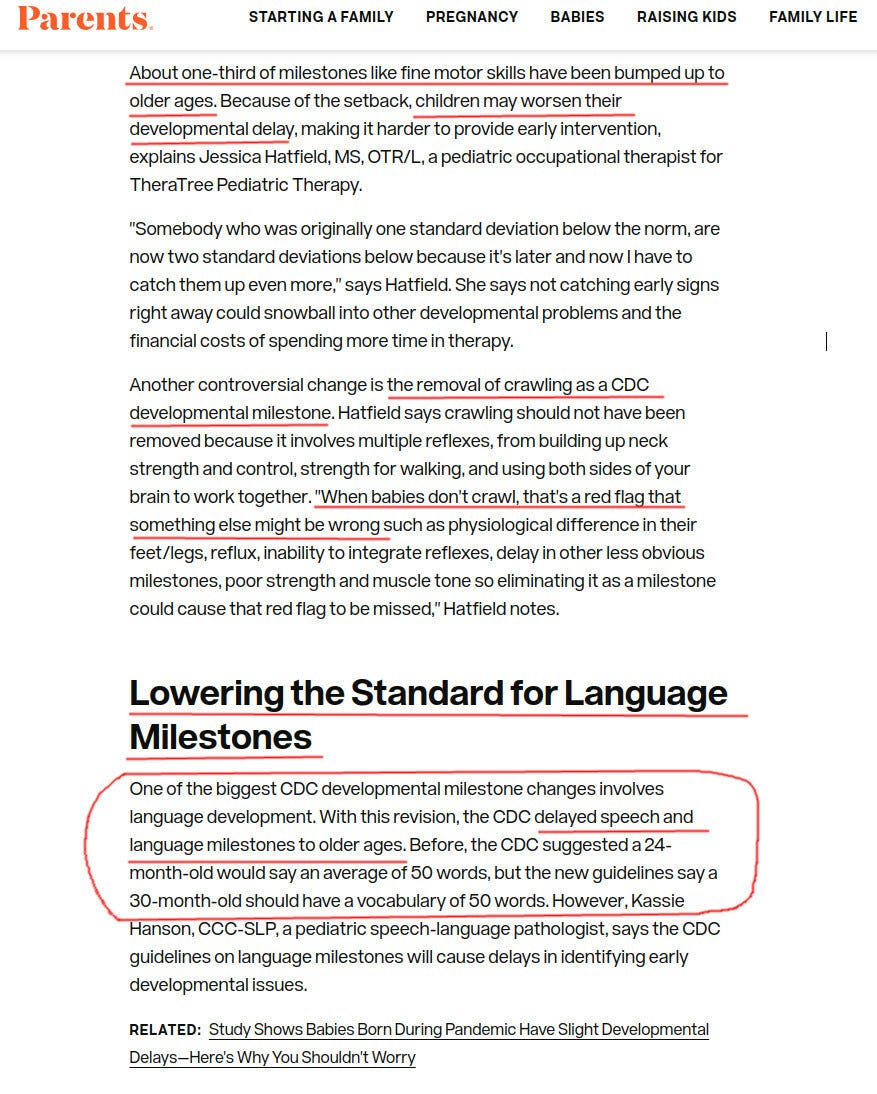
Removing crawling as a milestone??? Are you kidding us? For those of my readers who are parents, do you think that crawling is unimportant as a milestone?
Vaccinated Infants Exposed to SIX Doses of Covid Vaxx in a Year!
Imagine a vaccine enthusiast mother, who gets three doses during her pregnancy. Say, two doses during month 4 and one during the last week of pregnancy. The unborn baby is, obviously, exposed to all that.
Then the baby is born.
If the June 14-15 FDA meeting goes as planned, FDA will approve a three-dose Pfizer vaccine for infants and toddlers. So shortly after being exposed to THREE doses of mRNA vaccines prenatally, the recently born 6 months old baby will get THREE MORE Pfizer mRNA shots.
That’s a total of, drumroll, six spike protein, and nanoparticle exposures. For a tiny newborn, all during one first year of her life.
And what if the mom has several Covids while being pregnant and vaccinated?
They will ask the mom to vaccinate the baby regardless of those covid infections. This literally amounts to six doses within a year or close to, without even counting actual covids that the vaxed moms have. Pfizer will make $132 from these six shots. Not sure if the baby will eventually need much more expensive treatments.
Do you think that it is a little bit too much? Do you think Pfizer or the FDA care?
Featured Video

Language is a Weapon
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- The 12 Screenings That Manufacture the Patients They Claim to Find
- Iran deputy FM says MoU with US finalized, to be signed in Geneva on Friday
- With one strike, Netanyahu tries to kill two peace deals
- Iran warns ‘no point’ in deal with US if Israel remains unrestrained
- Ukraine as a laboratory of ‘techno-fascism’
- Desperate Starmer choosing piracy as distraction over UK crime crisis – Putin envoy
- The Crusades – colliding narratives
- Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
- What Is SIDS?
- If Americans Knew
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- Israel is changing the face of Lebanon, mainstream media is normalizing it – 3 articles
- Genocide lobby benefits from EU anti-racist fund
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
