Why are we so afraid of 1918?
What really happened that created this phantom behemoth?

Health Advisory & Recovery Team | October 4, 2023
Every time someone tries to whip up a frenzy about a new bug the 1918 influenza pandemic will be referenced. People will say there were a huge number of deaths including of the young and therefore you must be terrified. But what if this whole story was not what it seems?
The novel virus lie
1918 influenza did not spread like a tsunami as if everyone was susceptible. It came in 3 waves affecting 11% of the population each time. The deaths were spread over two years.
Similarly, seasonal influenza infect 5-15% of the population with each wave as does SARS-CoV-2.
The huge number of deaths
Kate Bingham trotted out the line that 50 million people died of the 1918 flu. (She also threw in that 20 million had died of COVID for good measure when the official figure is 6 million).
But 50 million is a lie.
Wellcome Trust would claim it was too low. In fact they claim the total was a stratospheric 100 million.
There were 1.8 billion people, of whom 600 million were infected. If 100 million really did die, that would mean an infection fatality rate of 1 in 6! If 50 million died, it would be an infection fatality rate of 1 in 12. Both are ludicrous claims that do not match with reality.
The consensus from every reasonable measure is that 1-3% of the infected died. This figure was based on extrapolating backwards from hospital fatality rates – people a hundred years ago were already very good at recording deaths and statistics.
Based on a mortality rate of 1-3% the deaths would have amounted to 6-18 million, still bad, but a fraction of the claim.
Estimates at the time were in that range. The US estimated 675,000 deaths from a population of 103 million. That means 0.65% of the population died.
The estimates for global mortality were exaggerated right from the start. China and Japan did not have the same problem as the West. However, when calculating global mortality it was assumed such places had fared as badly or worse than the USA and Europe. Consequently, modelling from 1920 already exaggerated deaths to 20 million globally.
Deaths in the young
Importantly there was more than one way to die in 1918. Some developed a viral pneumonia and then a bacterial pneumonia and then died. But there were unusual deaths in the young – unlike other pneumonias.
The second way to die was to develop a blue tinge – “heliotrope cyanosis” and then to die quite rapidly with haemorrhagic wet lungs. This is not the typical picture for a viral death.
Some have suggested other causes e.g. war related chemical exposure. There were huge movements of poorly nourished troops living in unsanitary conditions and thinking this was not a factor is surely naive. At the time there was a belief that influenza was a bacterial disease and a variety of bacterial based “vaccines” were concocted and injected during the second two waves. Whether that contributed to the harm is uncertain, other vaccines result in a temporary immune deficit to fight off infection, but it certainly couldn’t have helped. But aspirin toxicity is the most compelling argument.
Aspirin was new and was presented as the saviour drug. It was widely given in toxic doses of 8 to 31 grams per day, far beyond today’s maximum recommended dose of around 4 grams. It is now known that high doses can lead to lung damage, fever, seizures and death. The more fever the more aspirin would be given.
This story epitomises the problem:
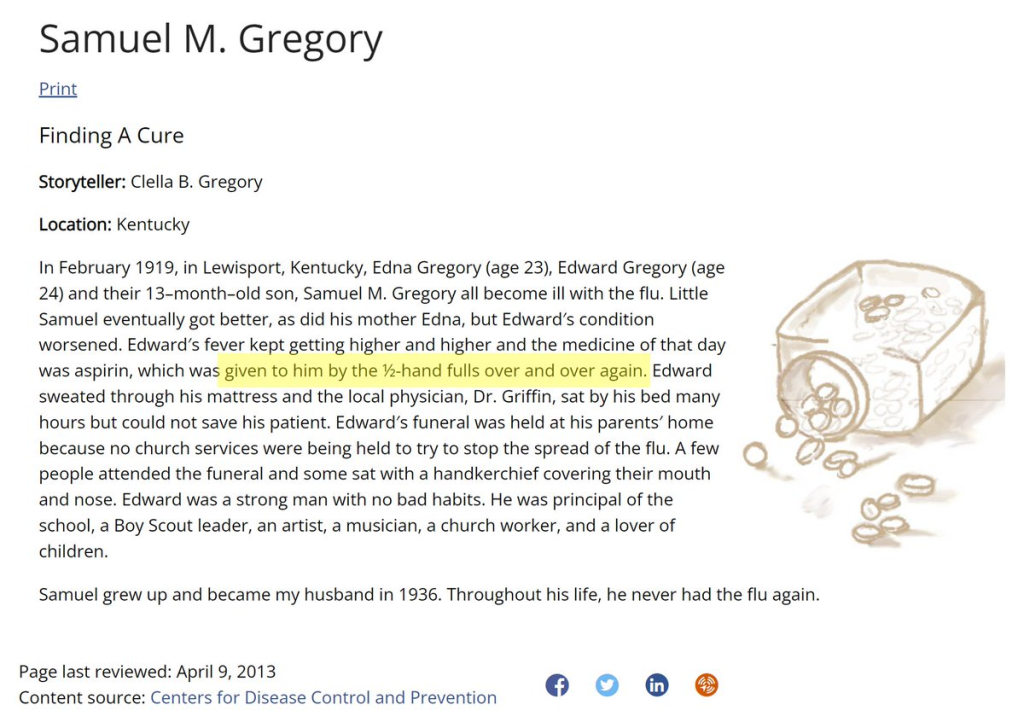
1918 was a story of iatrogenic harm (harm caused by medics). And yet it is being used to promote yet more iatrogenic harm. Do not be scared of 1918. It did not happen the way it was presented.
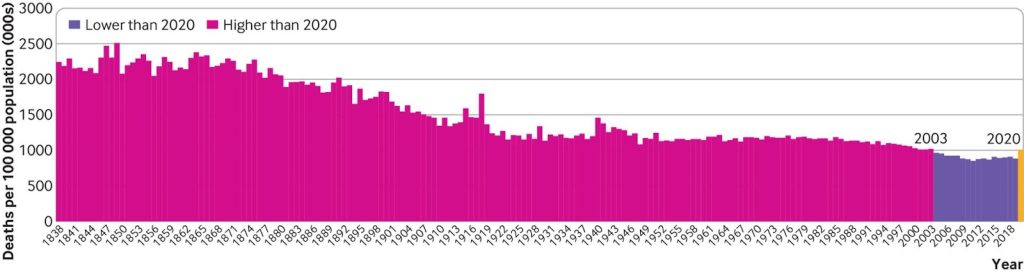
When looking at the bigger picture, 1918 does stand out as a bad year for deaths – as bad as 20 years before but better than almost every year preceding that.
The people exaggerating the claims about it all have something to gain from doing so. That’s how the deaths rose from 20 million (which assumed higher mortality in China and Japan than USA!) to 50-100 million. Stop believing them!
Connecticut School Board Faces Lawsuit for Rejecting School-Based Mental Health Clinic That Wanted to Treat Teens Without Parents’ Consent
By Brenda Baletti Ph.D. | The Defender | October 3, 2023
The Killingly Board of Education in Connecticut has been under fire since March 2022 when it refused to sign a five-year contract to install a federally funded school-based health center (SBHC) that would provide mental health services to minors without parental consent.
Instead, the board contracted for a similar center, but with month-to-month terms and parental consent required for treatment — and without federal grants or the rules they might impose.
The board’s rejection of the initial proposal, approved by the superintendent, led to the board and its members being slammed in local media, personally attacked, and subjected to a state investigation and a lawsuit.
Kelly Martin, vice chair of the Killingly Board of Education, and Sheila Matthews, founder of the nonprofit AbleChild, shared the board’s story with CHD.TV host Stephanie Locricchio on Monday’s “Good Morning CHD.”
Next week, the Killingly board faces a hearing, following a report last month — by attorney Michael McKeon, director of legal and governmental affairs for the Connecticut State Department of Education — criticizing the board’s actions.
The Killingly board rejected McKeon’s report as a “position statement,” and underscored the work they have taken to support Killingly children’s mental health.
The recent push by the U.S. federal government to rapidly expand the use of SBHCs across the country — largely justified as an intervention into a mental health crisis among young people —- has critics concerned children will receive unnecessary or unwanted medical interventions without their parents’ knowledge or consent.
School board beset by two-year battle including pandemic policies
Martin told Locricchio the controversy began when the school superintendent presented the school board with a proposal to put an SBHC in the school. The proposal provided only one possible service provider: Generations Family Health Center, which explicitly provided services without parental consent.
But many board members objected.
“The problem was never [with providing] mental health treatment,” Martin said. “We recognized that post-COVID children really, really need help. The problem was with the parents never being informed that the child was going to be treated.”
She added, “And that was something that was important to us — the parent doesn’t need to know what’s being discussed, [but they do] need to know that the child has a problem and is being treated and that they can actually keep a watchful eye on that child.”
The board voted down the SBHC, and a battle began. A group of parents represented by attorney Andrew A. Feinstein filed a complaint against the board seeking to overturn its vote, Martin said.
Once the board turned down the initial proposal, it interviewed alternative mental health services providers and set up a mental health clinic in the school where parents must opt-in to their child’s treatment.
But the state is not happy with that, she said. “They want that very first option, so it’s been an uphill battle since the lawsuit was actually filed,” she said.
The board had already come into conflict with the superintendent because it voted against an in-school COVID-19 vaccine clinic and then ended the in-school mask mandate.
Martin described the blowback:
“We have had people attack us constantly for the last two years. They’re making accusations that we don’t care about the mental health of children, [that] we don’t care about children at all. They’ve accused us of being racist, of being white supremacists. You name it, we’ve been accused of it.
“It’s been a very long two years. It all started when we started to give a little bit of pushback on some of these things.”
She said the group of people attacking them is small, “but they’re very vocal, they’re very loud,” and their actions have made board supporters afraid to speak out.Every Dollar has
Superintendent and attorney suing the board have conflicts of interest
The school board investigated the origins of the proposal and found the superintendent had put in a request for funding a mental health clinic without ever informing board members.
Martin said over the last few decades, power over schools has slowly been transferred from school boards to superintendents.
Because the clinic was to be grant-funded, they combed through the school board history to find which board policies had been changed to give power over grants to the superintendent — and reversed them.
In this case, the grant was part of ESSER II funding (Elementary and Secondary School Emergency Relief) — $54.3 billion made available by the Coronavirus Response and Relief Supplemental Appropriations Act of 2021 — with the requirement that it be awarded by September 2023.
She said the argument being made publicly and to parents was that this was a completely free, grant-funded clinic that would provide children with immediate assistance — so it was seen as a great idea all around.
But the clinics aren’t actually free, Martin pointed out. Once the grant ends, the cost burden shifts to the district.
Martin said children with mental health issues, of course, do need support as quickly as possible, but the only proposal made was for a clinic with a contract that was five years long and no parental consent.
She said the board wanted to review a variety of proposals, but they were only given that one.
In its investigations, the board also learned the superintendent sat on the board of the Northeast Early Childhood Council together with members of Generations — the one clinic he brought to the board.
After the board interviewed several other proposed clinics and selected one, she said Feinstein and a dissenting board member launched a media campaign smearing the clinic they selected, accusing it of bending to the board’s political agenda, which it implied was right-wing or “tea party.”
The selected clinic pulled out of the agreement with the board for fear its reputation would be ruined.
The board finally found another school-based mental health care provider, but the entire process dragged on for two years.
Little school board ‘up against Goliath’
Matthews, who works on national issues surrounding children’s mental health, became involved when she saw news stories that gave a disproportionate amount of negative attention to one small school board.
She began researching the issue and found that Feinstein is a registered lobbyist in the state of Connecticut and has received payments from a law firm dedicated to mergers and acquisitions in Big Pharma and to government grants that fund school-based clinics.
Matthews explained how government funding is funneled to different behavioral health vendors to set up clinics or provide medications, which make millions from children’s suffering.
Matthews and Martin said the school assessed students’ mental health by having them fill out anonymous surveys in school, without parental knowledge or consent, which is a common practice.
The surveys ask serious questions — such as whether the children are experiencing suicidal ideation — without any follow-up.
Instead of addressing students’ mental health, the questionnaires are simply evidence-gathering mechanisms to justify funding requests, Matthews said.
Both women encouraged parents to talk to their children about these surveys and to exercise their parental rights to opt out of them. Mathews’ organization AbleChild provides a sample letter parents can use to do this.
According to Matthews, $258 billion has come into the states from these ESSER funds overall. States are compelled to distribute the funds quickly before deadlines pass, but involving parents and community organizations slows down that process, she said.
“And these vendors smell the money,” she added.
Matthews, who studies how federal funds are directed to distribute potentially dangerous medications to children — particularly among children in foster care and on Medicaid — said the funds are lining the pockets of industry, not supporting children’s mental health.
“These block grants, this is the Achilles heel we have to take a look at. We have to look at these behavioral health vendors that have already set up shop in our school system.”
She said at minimum there needs to be a way to track the grants awarded so that parents can research what is happening in their schools and make informed decisions.
She added:
“This little town in Connecticut, they are up against Goliath. Okay? They are up against the drug companies. They are up against the behavioral health vendors. They’re up against the state. They’re up against the federal government. They are swimming in, I want to say, an ocean of corruption when it comes to these grants.”
Martin said the next step in the school board’s case is an inquiry hearing at the state building in Hartford on Oct. 11 at 10 a.m. It is open to the public.
Locricchio appealed to CHD.TV’s audience to show support for the board, especially because local supporters have been scared into silence by the public attacks.
“We would love to see some of our CHD [Children’s Health Defense] supporters there to stand with Kelly and Sheila and all the people that are involved in this because it could be your school district tomorrow that’s going through it,” Locricchio said. “And we know that we are so much stronger together.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Ukraine’s Possible New Counteroffensive: ‘Camouflage’ for Zelensky to ‘Steal More Money From West’
By Oleg Burunov – Sputnik – 01.10.2023
Kiev’s alleged push for another counteroffensive, this time in the autumn, can be perceived as the West’s red herring, Scott Bennett, a former US Army psychological warfare officer and State Department counter-terrorism analyst, told Sputnik.
The Zelensky regime had elaborated a plan for a major offensive in the Kherson and Zaporozhye region in early October, securing the approval of Ukraine’s sponsors in Washington and London, an informed source told Sputnik earlier this week.
According to the source, Kiev’s special forces intend to seize control of the Zaporozhye Nuclear Power Plant (NPP) as part of the blueprint.
All this could be Western countries’ red herring, Scott Bennett suggested, pointing to the Ukrainian Army’s futile attempts to break through Russian defensive lines.
“As a result of the resounding defeat of Ukraine, the West is frantically searching for an opportunity to try and escape the coming judgement and potential crimes against humanity charges for the death and destruction the Biden Administration has recklessly unleashed. And the nearest opportunity for distraction may be the Zaporozhye Nuclear Power Plant,” Bennett argued.
He recalled that many perceive this facility as “a target for destruction in a kind of ‘doomsday’ button that the US might try and push, in an attempt to generate sufficient chaos and destruction to distract the world away from the small scale battles of Ukraine, to the global implications of a nuclear disaster.” According to the former psychological warfare officer, the potential destruction of the Zaporozhye NPP would be the “ultimate expression” of this chaos.
He warned that if the facility is destroyed, “the resulting tsunami of social, political, economic disruption would disorganize opposition parties and protests against the current political elites in Europe and America, and justify a lockdown or martial law and police state mentality which could be endlessly extended.”
Bennett didn’t rule out that “the West will combine its best liars in the CIA, the Mossad, the MI6 to blame the event on Russia, and perhaps also simultaneously initiate some self-inflicted false flag attacks at the same time—such as assassinate Joe Biden and Zelensky at the same time and blame this on Russia in order to justify ‘police action’ and a drafting of Americans into the military for conflict with Russia.”
“We’ve seen it in Vietnam, and the 9/11 war on terror, so they may try and do it again, sad to say. The American media, the most professional liars and propagandists since Germany’s Goebbels, have already planted in the minds of Americans that ‘Trump supporters’ are becoming Russia-sympathizing domestic terrorists who may try and assassinate Biden, so the writing is on the wall,” the former State Department analyst added.
Commenting on how Zelensky’s alleged new advance can be explained, given the failure of Kiev’s summer counteroffensive, Bennett claimed that the Ukrainian president is “a madman, or being told what to do by madmen—or both. I suspect the latter.”
When asked if it’s safe to say that the alleged October counteroffensive plan is an attempt to appease the Ukrainian people and justify Western demands, Bennett said that it is “camouflage for Zelensky’s scheme to steal more money from the West, and show some kind of a “good faith effort” that would invite future ‘re-construction’ donations and investments by the West.
“The military reality is that Ukraine is destroyed, the war is essentially over, and the Russian military and people have prevailed and been victorious. Of course, the West is trying to distract away from this reality and create all kinds of miniature flash-points and terrorist attacks upon innocent civilians in Crimea and Moscow and elsewhere, but this too shall end,” the ex-State Department analyst asserted.
Russian President Vladimir Putin stressed last month that Ukrainian troops had failed to achieve any tangible results on all the frontlines since the beginning of their counteroffensive on June 4, something that he said had claimed the lives of more than 71,000 Ukrainian soldiers by the time.
MRNA vaccines must be banned once and for all
By Angus Dalgleish | TCW Defending Freedom | September 29, 2023
Those of us who knew from the beginning that the sequence of CoV-SARS-2 contained inserts which could not have possibly occurred naturally, and were similar to ones that had already been published from the Wuhan laboratory, have had to endure unbelievable scorn, scientific ostracism and the ignominy of being ‘cancelled’ by the MSM as well as by professional colleagues for nearly three years now.
In the summer of 2020 a paper I co-authored, describing the findings of an Anglo-Norwegian team of scientists who had demonstrated unique ‘fingerprints’ of laboratory manipulation in the Covid virus, was suppressed in both the US and UK. This was at the time that the World Health Organization, leading science journals and others were going to huge lengths to persuade us that Covid was a natural occurrence, and that we should spend a lot more money to fight any such future threats.
Only now does the Telegraph (uncritically) report that the US government is no longer going to fund the research it denied doing for nearly three years and the MSM sat on. Yet it has been an open secret for anyone who follows primary sources of information (the ones ignored by the MSM and the BBC specifically, reported as misinformation by Ofcom and targeted by the Orwellian Counter-Disinformation Cell of the UK government) that mRNA vaccines did not do what it says on the vial, as it were.
First the ‘vaccine’ did not stay at the site of injection as promised but travelled throughout the body and were found at post-mortems to be everywhere.
Accusations of dramatic variations in batch-to-batch variability – an absolute ‘no no’ in vaccine manufacture protocols – which could explain why side effects were more common in some batches than others were denied but were borne out by definitive Danish research reported here. These alarming concerns seem to have been brushed off by the regulators when they should have immediately begun investigating them in depth.
All the while the regulatory authorities and politicians, parroting their ‘highest standards’ assurances, have repeatedly declared the mounting disturbing UK Yellow Card and US VAERS adverse event reports to be nothing to be worried about.
Last June, whistleblowers led by the scientists Sucharit Bhakdi and Kevin McKernan raised an entirely new issue of concern – that of serious levels of DNA contamination. Once again this was ignored by the MSM. Though quite happy to report the odd side effect from the vaccines as an excuse to point out that they are extremely rare, they have never addressed the increasingly problematic official ‘safe and effective’ mantra.
Finally there was a small breakthrough. An isolated but braver branch of the MSM in the form of the Spectator Australia has finally blown the lid on serious levels of contamination of both Pfizer and Moderna mRNA Covid vaccines. The article describes how the genomics scientist Kevin McKernan from Boston used Pfizer and Moderna vials as controls in a study only to find that they contained highly significant DNA plasmid contamination. It reports that McKernan was alarmed to find the presence of an SV40 promoter in the Pfizer vaccine vials, a sequence that is ‘used to drive DNA into the nucleus, especially in gene therapies’ and that this is ‘something that regulatory agencies around the world have specifically said is not possible with the mRNA vaccines’. These SV40 promoters are also well recognised as being oncogenic or cancer-inducing.
Others have confirmed these findings. A German biologist whistleblower has found contamination rates of up to 354 times the recommended limit. All this has been reported to the US Food and Drug Administration (FDA). It is highly significant.
To put it bluntly, this means that they are not vaccines at all but Genetically Modified Organisms that should have been subject to totally different regulatory conditions and certainly not be classed as vaccines. This has been recognised by the Australian version of the FDA, the TGA, which has changed the picture so much that the Premier of Victoria Dan Andrews, who was the greatest proponent of the vaccine and of its mandatory use, has resigned – though at the time of writing the vaccine has not been mentioned as the reason for his resignation. (Paula Jardine reported in these pages in December 2021 on this regulatory sleight of hand in granting vaccine Emergency Use Authorisations for what were gene therapies.)
All this data, which is slowly breaking through into the public domain, comes hard on the heels of the latest findings that booster vaccines actually increase the chance of getting infected by 3.6 times. This is according to an in-depth study published by the Cleveland Clinic, one of the largest health care organisations in the world, who monitored their staff as well as patients.
It gets worse. Supporters of this technology have claimed that it can be adapted to chase new variants. But it can’t. The results of bivalent vaccines (with components against at least two variants) are seeing the same result. Authors of the Cleveland study say that ‘there is not a single study that has shown that the Covid-19 bivalent vaccine protects against severe disease or death caused by the XBB lineages of the Omicron variant. At least one prior study has failed to find a protective effect of the bivalent vaccine against the XBB lineages of SARS-CoV-2.’
In one study, all bivalent-vaccinated mice which were challenged with Covid became ill.
This was predicted by many of us as the SARS viruses are subject to immunological imprinting: that is, once they have seen a vaccine they will make the same response to any close variant (this is also known as ‘antigenic sin‘) making further vaccines not only useless but more dangerous as they induce antibodies that enhance infection (ADE antibodies), not cross reactivity as has been claimed by the manufacturers.
This is not the end of the issues with the mRNA ‘vaccines’. Several immunology studies have shown that the boosters induce an antibody switch from neutralising subtypes to tolerising subtypes as well as inducing significant T cell suppression, all of which will encourage new infections and suppress the immune response to cancer.
At the end of last year I reported that I was seeing melanoma patients who had been stable for years relapse after their first booster (their third injection). I was told it was merely a coincidence and to keep quiet about it, but it became impossible to do so. The number of my patients affected has been rising ever since. I saw two more cases of cancer relapse post booster vaccination in my patients just this last week.
Other oncologists have contacted me from all over the world including from Australia and the US. The consensus is that it is no longer confined to melanoma but that increased incidence of lymphomas, leukaemias and kidney cancers is being seen after booster injections. Additionally my colorectal cancer colleagues report an epidemic of explosive cancers (those presenting with multiple metastatic spread in the liver and elsewhere). All these cancers are occurring (with very few exceptions) in patients who have been forced to have a Covid booster whether they were keen or not, for many so they could travel.
So why are these cancers occurring? T cell suppression was my first likely explanation given that immunotherapy is so effective in these cancers. However we must also now consider DNA plasmid and SV40 integration in promoting cancer development, a feature made even more concerning by reports that mRNA spike protein binds p53 and other cancer suppressor genes. It is very clear and very frightening that these vaccines have several elements to cause a perfect storm in cancer development in those patients lucky enough to have avoided heart attacks, clots, strokes, autoimmune diseases and other common adverse reactions to the Covid vaccines.
To advise booster vaccines, as is the current case, is no more and no less than medical incompetence; to continue to do so with the above information is medical negligence which can carry a custodial sentence.
No ifs or buts any longer. All mRNA vaccines must be halted and banned now.
MHRA Finally Admits it Failed to Test the Safety of Mass Manufactured Covid Vaccine Batches
UK’s medicines regulator comes clean
By JJ Starky| The Stark Naked Brief | September 28, 2023
On December 8th, 2020, June Raine, the Head of the Medicines and Healthcare products Regulatory Agency (MHRA), publicly declared that “no corners have been cut” during the temporary authorisation of the Pfizer Covid vaccine. However, thanks to the persistence of former Ministry of Defence employee, Nick Hunt, recent findings prove Raine’s statement was not true.
For context, it’s common in development trials across various sectors to first use products made in small-scale facilities or laboratories. Investing in mass production usually comes later, once there’s sufficient confidence in the product’s design. Scaling up, naturally, introduces new risks.
With pharmaceuticals, regulations are in place to manage this process. This is to ensure the final product remains consistent and effective.
Concerns first arose in 2022 regarding the Pfizer Covid vaccine. There were suspicions that the vaccine MHRA approved in December 2020, manufactured using “Process 2”, differs from the version tested in Pfizer’s clinical trials, manufactured using “Process 1”. Josh Guetzkow, an Israeli academic, brought the difference to light, referencing Freedom of Information requests from various countries and Pfizer documents released by U.S. courts.
In May 2023, he published this rapid response in the British Medical Journal alongside Professor Retsef Levi, airing his concerns.

Guetzkow highlighted two things. First, there is a lack of publicly available reports comparing vaccines produced by both processes. Second, there is significant variability in the rate of serious adverse events across different vaccine lots, underscoring the need to better understand variability in the production process.
In October 2020, Pfizer had committed to comparing safety and immunogenicity results between vaccines produced by both processes. Yet, when Hunt submitted his initial FOI request concerning the latter to MHRA in July, their initial response directed him to the European Medicine Agency’s archive without specific guidance.
Here’s the bombshell.
Nick then requested an internal review. In their response, MHRA admit their replies “were not compliant with the (FOI) Act and did not provide or address the specific information (Nick) asked for”.
They then confess they do not possess the “Process 2” report.
The document goes on to state the “Process 2 drug… was shown to be comparable through side-by-side comparability studies and heightened characterisation testing”. In short, trust us, we’ve seen the data but we can’t show it to you and we don’t have it.
Worse yet, MHRA also revealed they failed to chase Pfizer on the promised report that the company should have published comparing the products. This was because of the “extensive usage of vaccines manufactured via Process 2”.
Family investigated for keeping teen home after school-based health center gave bag of unlabeled Zoloft to 17-year-old
By Brenda Baletti, Ph.D. | The Defender | September 28, 2023
A federally funded school-based health center (SBHC) in Maine reportedly gave prescription anti-depressant pills in a plastic baggy to a 17-year-old girl without her parents’ knowledge or consent, her father told The Maine Wire.
When the girl’s father, Eric Sack, found the pills — which his daughter told him were Zoloft — he complained to the school.
Zoloft carries a black box warning — which warns of possible serious adverse reactions — indicating the drug can cause suicidal ideation, particularly in people under age 24, when they first start taking the drug.
Sack kept his daughter home from school the following week to make appointments with a doctor and therapist — a decision that resulted in someone at the school or the health center reportedly contacting Child Protective Services, which investigated the family.
The recent push by the U.S. federal government to rapidly expand the number of SBHCs across the country to improve healthcare for children by offering “primary care, mental health care, and other health services in schools” — particularly in underserved communities — is raising red flags.
Critics say they’re concerned children might receive, or be pressured into receiving, unnecessary or unwanted medical interventions without their parents’ knowledge or consent.
Georgia attorney Nicole Johnson, co-director of Georgia Coalition for Vaccine Choice and a consultant to the Children’s Health Defense (CHD) legal team, told The Defender :
“This case in Maine really is everything we worried about. It is almost the worst-case scenario. A young person is getting a drug with a black box warning. They come home with it. It doesn’t even have any warning label on it. The parents haven’t been told, and the drug is in some plastic bag that anybody — any other child in the house, or their peers — could have access to. It could be a very dangerous situation.”
Maine goes all in on SBHCs
The Bulldog Health Center at Lawrence High School in Fairfield, Maine, which reportedly gave the Zoloft to Sack’s daughter, offers primary care services onsite to middle and high school students.
It is operated by Maine’s HealthReach Community Health Centers, a nonprofit funded largely by patient fees and grants. HealthReach reported it also received $4.8 million from the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS), although further grant details are not available.
HRSA also awarded approximately $25 million in 2022 to expand 125 SBHCs, including $81,728 to HealthReach. HRSA also awarded $5 million to 27 centers in 2021.
Those grants came in addition to $50 million in HHS grants authorized by the Biden administration and Congress in 2022 to states “for the purpose of implementing, enhancing, or expanding the provision” of healthcare assistance through SBHCs using Medicaid or the Children’s Health Insurance Program, The Defender reported.
In Maine, the Department of Education and Department of Health and Human Services (DHHS) announced in March 2022 plans to expand SBHCs across the state through the use of one-time federal American Rescue Plan funding for $2.4 million.
Funds are being distributed in two-year grants during 2021-24 to establish 12-15 new centers in Maine.
In 2022, there were at least 22 SBHCs in the state.
State funding covers startup costs plus costs for uninsured and underinsured students, for additional time needed during visits and for “confidential care that may not be billed to insurance,” according to a presentation by DHHS.
In the SBHC partnership, the school district acts as the “host,” coordinating enrollment in the SBHC program, parental consent and services. The healthcare provider is the “sponsor,” which receives the funding and provides the services.
A key justification for the expansion of the centers, in Maine and nationally, is an “increased need for mental health care.” The demand for mental health services for children and youth were at “an all-time high,” according to DHHS’ presentation, and the COVID-19 pandemic made disparities in access to healthcare more severe.
In the 2020-21 school year, 77% of the reported SBHC visits were for mental health services. DHHS also indicated that increased emergency department use by youth was driven by suicidal ideation among adolescent females.
‘I’m looking out for the best interests of my daughter’
The Maine Wire reported that when Sack found a zip-close bag containing small blue pills in his family home, his daughter told him she had been prescribed the pills by the Bulldog SBHC.
He said he was concerned the prescription given to his daughter violated his parental rights, but also that the center sent unlabeled drugs with no child-resistant container home with his daughter to a household where two younger children also lived.
Sack said he contacted Lawrence High School Principal Dan Bowers, who told him the clinic was a separate entity that he had no control over.
Sack also said a representative from the Bulldog Health Center told him they could legally prescribe the medication to his daughter without informing him. They did not comment on the lack of a label or safety container, he said.
Concerned, Sack pulled his daughter out of school the following week.
“I’m looking out for the best interests of my daughter. That’s why I pulled her out of school,” Sack told The Maine Wire. “Because I don’t think she really ought to be there if they’re going to start giving her pills, you know? Until I sit down with a doctor that I pick for my daughter, not through the school.”
The Maine Wire reported what happened next:
“On Thursday, an agent from Child Protective Services (CPS) called Sack and informed him that he would be arriving shortly to make a surprise visit to his home to conduct a child welfare investigation.
“‘They called and said it was an emergency situation at my house, that I was pretty near holding my daughter hostage, is what the gentleman that came yesterday told me,’ Sack said.
“‘He had information that only the school and Bulldog Health Center had,’ he said.”
Members of the family were questioned individually and as a group by CPS Agent Dylan Wood, who eventually indicated the complaint against him was unfounded, Sack said.
The Defender reached out to Sack, who said he is seeking legal counsel and declined to be interviewed at this time. The Bulldog Health Center and Bower did not respond to a request for comment.
SBHC consent forms may be confusing for parents
Sack told The Maine Wire that he or his wife may have signed a consent form at the start of the school year, but he still thought the incident violated his rights.
Justine Tanguay, an attorney with nearly 20 years of experience advocating for children in various areas of the law, told The Defender these consent forms are a key issue for parents to be aware of.
At the start of each school year, parents are given many forms to sign and they likely don’t realize they are signing away their rights over their children’s healthcare, she said.
Most parents, she said, tend to assume that school medical consent forms allow a school nurse to administer first aid, treatment for minor illnesses or emergency treatment.
“But that is not what this is,” Tanguay said. “It’s something much more nefarious.”
Unlike school nurses, SBHCs function as primary care clinics. By signing consent forms, parents may unknowingly give those who run the SBHC the legal authorization to provide “comprehensive healthcare.”
This could include — but may not be limited to — “the ability to provide preventative treatment, behavioral and mental health services, reproductive counseling, lab and prescription services, various medical screenings, immunizations and disease management,” Tanguay said.
She said parents should know:
“One form they may receive at the start of the school year is a blanket consent form, and if they sign it, they are basically abdicating their parental rights to make medical decisions for their kids.
“The school won’t need to reach out and ask, ‘Hey, can we test your child for whatever thing?’ No, they’ve signed the form, they’ve already said, ‘Do whatever you want.’”
But, she said, parents who signed such a form have the right to revoke it.
Tanguay added that consent forms can be difficult to understand and the forms are not all the same.
She suggested parents whose children go to schools with SBHCs should find out what the forms they are signing say and decide what they want to opt out of.
Tanguay also said Bower’s alleged statement that the clinic is not under his control is true. These clinics are inside of the school, but are separate entities not administered by the school, she said.
Yet, the school is responsible for obtaining signed consent forms from the parents, which generates confusion.
That means parents are not giving informed consent, Tanguay said.
“Did the father in this case know what he was signing? Was there a warning on the document that stated ‘You are abdicating your parental rights to make medical decisions’? So did he understand the implications of the form? I doubt it,” she said.
Teen mental health crisis spurred federal funding for SBHCs
At least since the start of the COVID-19 pandemic, public health officials and organizations have been sounding the alarm about a mental health crisis among children.
The American Association of Pediatrics (AAP) declared the children’s mental health crisis a national emergency in October 2021 and the surgeon general in May of this year issued a public advisory warning that social media can pose a “profound risk of harm to the mental health and well-being of children and adolescents.”
In fact, suicide rates, particularly among teenage girls, have been on the rise since 2008.
Those public announcements pointed to the COVID-19 pandemic, racism, and social media as the causes of higher rates of mental illness among teens.
But other experts, including Vinay Prasad, M.D., MPH, have cautioned against those assumed links, instead pointing to policies such as lockdowns and school closures that isolated kids and teens and forced them online for large periods of time, compromising their education and their social lives.
Groups like the AAP, a strong supporter of SBHCs, have used the mental health crisis to call on the Biden administration to fund expanded access to screening, diagnosing and treatment for children, arguing access to “school-based mental health care” should be a priority.
The administration responded with new policy measures, including the Bipartisan Safer Communities Act — which made $11 billion available for mental health services — and the American Rescue Plan Act. Both offer funding explicitly for school-based mental health services for students, KFF Health News reported.
Many of these resources have funded the expansion of SBHCs.
Professional associations including the AAP and the American Academy of Family Physicians recommend antidepressants, often combined with therapy, to treat moderate-to-severe mental health issues in young people.
But the use of antidepressants for young people — one tool for addressing mental health issues by the healthcare industry — has been controversial, with many advocates arguing for decades that the “heavily-marketed mind-altering agents” are prescribed too frequently to children and the drugs’ effects are understudied.
A 2016 review of over 70 trials published in The BMJ found an increase in self-harm and aggression in children and adolescents taking antidepressants, but not in adults.
Because of these concerns, the U.S. Food and Drug Administration (FDA) put a black box warning on many antidepressants in 2004, warning that they increase the risk of suicidality (defined as serious thoughts about taking one’s own life or planning or attempting suicide) among children, adolescents and young adults.
Despite those concerns, there has been a steady increase in the last decade in the number of antidepressants prescribed to children.
Many medical researchers have called on the FDA to eliminate these warnings, alleging they led to a reduction in the number of young people who take antidepressants. Others have found these claims are based on “weak evidence.”
Advocates for children’s mental health, such as Tom Madders, director of campaigns at the U.K.-based YoungMinds, a children and young person’s mental health nonprofit, said antidepressants could play a role in some young people’s mental health, but that it is “crucial” they be coupled with other therapies and that they are not used as a substitute for other treatments.
Even those who strongly advocate for the use of antidepressants for children caution about side effects and the importance of parental education and informed consent.
A 2019 article in Current Psychiatry underscored that:
“It is important that clinicians and families be educated about possible adverse effects and their time course in order to anticipate difficulties, ensure adequate informed consent, and monitor appropriately.
“The black-box warning regarding treatment-emergent suicidal thoughts or behaviors must be discussed.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
The Anglo-American War on Russia – Part Ten (NATO Lies at Minsk)
Tales of the American Empire | September 28, 2023
The United States CIA organized a coup to overthrow the neutral government of Ukraine and installed a Russian hating regime in 2014 that wanted to drive millions of ethnic Russians out of Ukraine. This led to a rebellion in eastern Ukraine where the Russian majority took up arms to protect themselves. This led to a small civil war that was quickly settled with a peace agreement. These 2015 Minsk agreements were brokered by France and Germany, agreed to by Ukraine and Russia, and accepted by the United States. Ukraine would retain official ownership of this rebellious region called the Donbas that would be granted full autonomy for internal rule. The Minsk agreements were endorsed unanimously with United Nation’s Security Council Resolution 2202, see the link in the description.
Ukraine never complied by withdrawing its heavy weapons from the Donbas region and continued random artillery and tank fire into Donbas cities. The Donbas rebel’s ability to retaliate was limited because the Ukrainians fired from urban areas mostly inhabited by ethnic Russians. Russian President Vladimir Putin appealed to the United Nations, United States, France, and Germany to apply economic and diplomatic pressure on Ukraine to abide by Minsk. They promised to help and the occasional terror bombardments into Donbas cities lessened, but never stopped as they killed thousands of civilians, mostly ethnic Russians.
NATO refused to pressure Ukraine to adhere to the Minsk agreements and continued massive economic and military assistance. Ukraine possessed only 6000 combat-ready soldiers in April 2014 but NATO help allowed it to build its military into the second largest in Europe comprising about 250,000 active-duty troops and 80,000 reservists who were trained at the billion dollar American built base at Yavoriv where hundreds of American soldiers were based. Ukraine soon had more tanks than France, the United Kingdom, and Germany combined.
President Putin began to understand that NATO had no interest in peace. He correctly concluded that the United States planned for war on Russia. We now know this for certain because in 2022, Minsk agreement signers, former Ukrainian President Pyotr Poroshenko, former German Chancellor Angela Merkel, and former French President François Hollande, admitted that the Minsk agreements were a deception to trick Russia into a ceasefire with the promise of a peaceful settlement to buy Ukraine and NATO time to build up its military to attack Russia.
_________________________________
“Unanimously Adopting Resolution 2202 (2015); Security Council Calls on Parties to Implement Accords Aimed at Peaceful Settlement in Eastern Ukraine”; United Nations; February 17, 2015; https://press.un.org/en/2015/sc11785….
“Children Living in Bombshelters Entire Lives”; Patrick Lancaster; YouTube; March 10, 2022;  • Children Living In Bombshelters Entir…
• Children Living In Bombshelters Entir…
“Ukrainian/NATO Training Centre”; NATO; October 20, 2003; https://www.nato.int/structur/nmlo/li…
Related Tales: “The Anglo-American War on Russia”; • The Anglo-American War on Russia
Top Japanese Virologist Takes to the Street to Warn of Manufactured Omicron Strain
BY JEFFEREY JAXEN | SEPTEMBER 28, 2023
What if the world learned that the Omicron strain was manufactured?
An emotionally alarming video has just been posted. A man in a suit stands alone on a busy Japanese street trying to get the attention of people passing by. He is Japanese professor Takayuki Miyazawa from Kyoto University. A top virologist and associate professor at the university’s Institute for Life and Medical Sciences. The Japanese language clip of Professor Miyazaawa’s warning has over 8 million views on X at the time of this writing.

“We often appear on TV but there are many things that cannot be said on TV. There are many things that cannot be said on YouTube. There are many things that cannot be said on Twitter.”
“Only researchers know what is true. Researchers can directly obtain data and analyze it. And when they analyze it, they can learn a lot of things. We can’t communicate that. So I’m not sure what Japan is doing.”
“By examining the amino acid sequences you can immediately understand what is being done. If you analyze it, it’s obvious.”
[Watch the full video here and turn on closed caption translations]
Professor Miyazawa has published over 250 academic papers and studies in the areas of virology, disease, veterinary medicine, and microbial ecology. Yet his most recent paper has the world talking and deeply moved him into action to alert others to what he has found. Even if it means losing his longstanding position at the very highly regarded Kyoto University.
Researchers and virologists around the world were baffled at the evolution and rapid dominance of the Omicron variant of SARAS-CoV-2 after being first identified in November of 2021.
An outlier with no explanation for its wildly divorced trajectory from the rest of the lineages. Just an unnatural, red rocket line perched above the rest of the natural virus evolution. What happened?
Japanese professors Miyazawa and Tanaka set out on a year of research to find out.
The evidence presented in their paper titled Unnatural evolutionary processes of SARS-CoV-2 variants and possibility of deliberate natural selection, published in September of 2023, was potentially earth-shattering. Using the Basic Local Alignment Search Tool (BLAST) program, the pair of researchers looked at nearly 400 Omicron-related variants to identify regions of similarity between protein or nucleotide sequences to understand the order of mutations leading to their formation.
What they found led them to conclude that the formation of a part of Omicron isolates BA.1, BA.1.1, and BA.2 was not the product of genome evolution. They conclude by writing:
“This study aims to point out that SARS-CoV-2 has undergone unthinkable mutations based on conventional coronavirus mutation mechanisms, and we hope that the possibility of artificial creation is included in serious discussions on the formation of SARS-CoV-2 variants.”
The variants, when displayed in graphical form, displayed an incremental and methodically stepped-down ordering. Something nature doesn’t do. Natural mutations are random, and once they mutate, they don’t revert back. However, what professors Miyazawa and Tanaka found was that the Omicron mutations were switched off, and then back on step by step down the evolutionary ladder.
A separate article analyzing their findings stated:
“Perfect reversion of mutations like this, on such a scale, is completely implausible by any natural process. The variants found by Tanaka and Miyazawa can best be described as a “panel” of reversion mutations. This kind of panel is exactly what a researcher would create to systematically test the contribution of different elements of a virus to its activity.”
Viruses undergo only two types of mutations. Synonymous, functionally silent, and evolutionarily neutral mutations accrue in the background whereas non-synonymous mutations are the prime movers that can change the function and abilities of a virus. In natural evolution, the ratio of synonymous (silent) mutations is always higher than the rarer non-synonymous mutations.
Yet when it came to the spike protein, the business end of the SARS-CoV-2 virus, the researchers write:
“Concerning the genetic variation in the S protein of these variants, most of the mutations were non-synonymous (Fig. 1). There were no synonymous mutations in the Alpha, Beta, Gamma, Delta, or Mu variants, but only one each in the Lambda and Omicron variants.”
The paper has yet to be peer-reviewed, however, this isn’t because of the merits of the research. Speaking exclusively to The HighWire, one of the authors shared the correspondence they received from a journal upon submitting their research for publication.
“During our initial checks, some issues were identified regarding potential inflammatory language in the manuscript. The authors have not amended this in line with the suggestions to make the text more objective. This prevents the manuscript from proceeding further into review.”
Whether the data discovered and the passionate pleas by one of the paper’s authors will be further investigated, understood, or disseminated remains to be seen. In a world where many in the medical, health, and research communities are still in the dark about the virus’ origins such striking evolutionary data presented by the Japanese researcher should at least spark more investigation and serious debate about what appears to be the real possibility of a lab-created variant.
Highwire | September 15, 2023
Cost of Living Crisis to Cause ‘Thousands of Extra Deaths’ in UK – Report
By Chimauchem Nwosu – Sputnik – 27.09.2023
 Some UK military personnel and their families have been turning to food banks because of the increasing pressures from the cost of living crisis, a British news network has reported.
Some UK military personnel and their families have been turning to food banks because of the increasing pressures from the cost of living crisis, a British news network has reported.
The raging cost of living crisis that has had the UK in its stifling grasp is going to cause thousands of extra deaths this year, according to new research, as life expectancy across the UK will plummet by 6.5 percent this year.
The research suggests that untimely mortalities in the United Kingdom are expected to rise from 463 to 493 per 100,000 inhabitants.
The findings have shone a light on critical concern for the populace at large. The unrelenting cost-of-living crisis, combined with a prolonged period of soaring prices, is anticipated to result in a significant 6.5 percent drop in life expectancy throughout the nation this year.
Furthermore, the report highlights a stark disparity: the most economically disadvantaged households are projected to face a four times higher death toll than their wealthier neighbours. This discrepancy arises from the fact that the less affluent must allocate a more significant portion of their income to pay for energy, the cost of which has rocketed.
Recent statistics from the previous month indicate that the UK’s inflation rate stood at 6.7 percent. Despite this reduction from its peak of 11.1 percent, Britain continues to have the worst inflation of all G7 member states.
“The mortality effects of inflation and real-terms income reduction are likely to be large and negative, with marked inequalities in how these are experienced. Implemented public policy responses are not sufficient to protect health and prevent widening inequalities,” researchers noted.
These findings come on the heels of a recent alert from the UK-based consumer association ‘Which’ last month, when it pointed out that rising food prices had left low-income households in the country in dire straits and having to make painful decisions about whether to pay the utility bills or put food on the table.
House Panel Releases Emails Showing US Attorney Blocked FARA Probe Into Joe Biden
Sputnik – 28.09.2023
WASHINGTON – The House of Representatives Oversight Committee released redacted emails it claims show that Delaware Assistant US Attorney Lesley Wolf blocked federal agents from conducting a FARA (Foreign Agents Registration Act) investigation into then-Democratic presidential nominee Joe Biden in August 2020.
“Newly released emails and documents show that Delaware Assistant US Attorney Lesley Wolf did not allow agents to investigate Joe Biden as part of a FARA probe,” the Oversight Committee said via X (formerly Twitter) on Wednesday.
In the email, dated August 7, 2020, it appears Lesley told federal investigators they made a mistake in their search warrant request by including Biden. Lesley purportedly claims Biden falls outside of the scope of their FARA investigation.
The House Oversight Committee will hold the first hearing of the impeachment inquiry against President Joe Biden on Thursday to begin further examining alleged criminal activity involving Hunter Biden and his foreign business dealings.
The committee has been investigating alleged foreign bribery and influence peddling involving the Biden family and entities in countries including Ukraine and China. Biden denies ever having discussed foreign business affairs with his son.
Citing bank records, the committee on Tuesday revealed that Hunter Biden in 2019 received two payments wired from China totaling $260,000 with President Joe Biden’s Delaware home listed as the beneficiary address.
McCarthy, in light of the new findings, said the Republican impeachment inquiry against Biden will uncover the whole truth.
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- Press TV reporter wounded in Israeli drone strike on southern Lebanon
- Time for Trump to Tell Benjamin Netanyahu to Go Away!
- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- If Americans Knew
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
