Drug harm reporting systems, like the MHRA’s yellow card system, are designed to alert the regulator to a potential issue. They are not designed to measure the size of the problem. If an issue is highlighted then the regulator has a responsibility to carry out an audit and see whether the incidence of the condition of concern has been higher than historical levels in the population who were vaccinated.
The Government appears to be treating the yellow card reports as if they are a record of every occurrence of a condition in the country, comparing the number of reports with background levels in the whole population. It is well known that reporting systems only capture a fraction of cases and it is very odd that the Government is treating this data as comprehensive.
As an example, let’s take Guillain-Barre Syndrome (GBS) which is a rare condition where the immune system attacks the nervous system. It is usually caused by a viral infection but has been attributed to vaccination adverse reactions in the past. There are 1,300 cases every year and 608 cases have been reported on the yellow card system.
A study by Hanson et al in the USA of 10 million patients showed that in the first 21 days after the Oxford-AstraZeneca vaccine the rates of GBS were 15 times higher than expected levels. Extrapolating from this figure we would expect 500 AZ vaccine related cases in the UK. There have been a total of 488 reported in the yellow card system but it is not clear whether these were within 3 weeks of vaccination.
In a three week period we would expect 29 background cases to have occurred co-incidentally. Based on the Hanson data of 500 cases after 24.9 million doses, the cause of someone having GBS within 3 weeks of the Oxford-AstraZeneca vaccine would be the vaccine 95% of the time and coincidental 5% of the time. The morally right thing to do for these people, is to accept that they have been vaccine injured and be wrong 5% of the time rather than claim these were coincidental and be wrong 95% of the time.
The Government appears to want to claim coincidence. A few of these patients have filed claims with the Vaccine Damage Payment Scheme. None of the claimants have been helped, even patients whose deaths have been investigated at inquest and where a coroner has determined the vaccine as the cause of death. When rolling out a £12bn vaccine programme it is naive not to set aside a budget for vaccine injury. The current claims system requires proof of “60% disability”, a ‘proof of cause’ and does not compensate for lost earnings or costs of care. Maria Caulfield, the minister for patient safety and primary care, said that they were employing people to look through the claimant’s medical records for a “causal link” as if vaccines write confession notes. Surely, this is the real waste of public funds and seems to point to a reluctance to compensate deserving victims.
As I described in my last article, the California Democratic Party and the Democratic National Committee have embraced the Pan Doctrine that is junk-science-eugenic-fascism with the added twist that they want everyone to be chronically ill in order to enrich their largest donors. This particular political machine works right up until the point at which the entire society collapses — which is fast approaching.
So what’s the alternative to the Pan Doctrine?
Actual Science.
What are the elements of actual science in connection with our current debate? These are the principles that came to mind for me but I imagine you’ll be able to add many more:
1. Nullius in verba which means “take nobody’s word for it.” Secondary sources are not a valid epistemology. One must read original source documents. Examine data and evidence. Draw your own conclusions. Think for yourself. Escape information bubbles and transcend dogma. Morality and ethics are vital. Skepticism, disinterestedness, transparency, and rigorous debate are the hallmarks of good science. Reductionism, censorship, and conflicts of interest are fatal to good science.
2. Civil engineers, not vaccines, produced the large gains in life expectancy over the 20th century. About 90% of the decline in infectious disease mortality among U.S. children occurred before the introduction of mass vaccination campaigns (Guyer et al. 2000). The large gains in life expectancy over the twentieth century were mostly the result of the construction of water and sewer systems, improvements in food safety, hand washing, improvements in housing, and reduced overcrowding in U.S. cities.
3. The best vaccine safety data set in the world shows that all vaccines on the U.S. childhood schedule produce more harms than benefits. The data show that only a few live attenuated vaccines produce more benefits than harms (oral polio, measles by itself, and tuberculosis) in regions where these viruses are endemic. None of those vaccines are available in the U.S. However, all live virus vaccines eventually revert to virulence and cause outbreaks of the disease that they are trying to protect against. The harms from coronavirus shots far exceed any benefits.
4. The human immune system is wondrous, more sophisticated than any man-made product, and not well understood by so-called “experts”. When our bodies need extra support, nature has given us a wide array of tools for treating disease. Community, a sense of connection, and meaning are key to health too. Allopathic medicine has a role to play in emergency treatment but over the long run the largest gains in health often come from lifestyle changes. Toxicants play a huge role in disease but they are poorly studied because government is captured by industry.
5. Science, technology, class, health, sex, wealth, and power are interwoven. From medieval witch trials through today, the wisest healers are often persecuted and the most effective treatments are often suppressed. Pure objectivity is impossible because the observer is always part of the world that is being observed. Science is always changing. Institutions exist to reproduce themselves. The purpose of the pharmaceutical industry is to enrich shareholders. It is essential to take personal responsibility for one’s own health.
This past week saw two high-profile Australians – cricketer Shane Warne and Labour senator Kimberley Kitching – both die of sudden heart attacks aged 52.
As such, heart disease is back in the headlines. Again.
We predicted in our new-years post that explaining heart attacks would be a big part of 2022’s news cycle, and only three months in it has been a torrent.
It actually started in December of 2021, with medical doctors theorising that the stress and anxiety of dealing with Covid was going to cause a huge spike in heart problems due to “post-pandemic stress disorder”.
At the beginning of February, a new reason was added to the list. As energy prices began to spike – do remember, that happened before the war – we were told the increased cold and stress could also cause heart disease.
Then, in mid-February scientific papers appeared claiming that “even a mild case of COVID” causes your “heart attack risk to soar”.
In short, and for many reasons, you’re much more likely to have a heart attack this year than you were last year.
Well, now the Sydney Morning Herald has joined in, with this article headlined “‘This is our biggest killer’: Shock deaths put spotlight on heart disease”, which warns:
The shock deaths of cricketer Shane Warne and Senator Kimberley Kitching should serve as a wake-up call to Australians about the prevalence of heart disease, doctors say, as a study shows COVID-19 may increase the risk for what was already one of the nation’s biggest killers.
Yes, having had covid – even if you just tested positive and had no symptoms – makes it more likely you’ll have a heart attack.
On top of that, warn the doctors quoted in the article, thousands of people will have missed their heart screenings due to lockdown, or have been sedantry and gained weight, not to mention the anxiety and stress.
All in all, Australians can expect a “rise in preventable heart disease deaths over the next five years”, according to health modellers.
But don’t worry, none of that is anything to do with the untested vaccines they’ve injected into literally millions of people.
Yes, all the major Covid vaccines are known to have “rare” side effects that impact the heart, such as blood clots and myocarditis, but clearly, that’s just a coincidence.
After all, the Sydney Morning Herald article doesn’t even use the word “vaccine”, not one single time. And they wouldn’t ignore anything that important, would they?
Data is the foundation of scientific analysis. Without data, researchers are left unable to draw conclusions, which leaves public health experts unable to accurately make recommendations. But that appears to be exactly what the CDC1 and Health and Human Services (HHS)2 are doing. The CDC is hiding data and the HHS is no longer collecting data, which one U.S. official has called “incomprehensible.”3
Since the World Health Organization announced a pandemic, multiple organizations began tracking data, including the number of people who were sick with COVID-19, in the hospital with or had died from it. As I have written, later the number of “cases” was reported. These were people who had a positive PCR test and did not necessarily have symptoms.
Whistleblowers working with attorney Thomas Renz, who is investigating hospital abuses,4 have reported that hospitals are incentivized to admit PCR positive patients, prescribe remdesivir,5 place patients on ventilators and include COVID on death certificates. All told, some believe hospitals could receive up to $100,000 for each patient who meets all the incentivized criteria.6
Of course, “fact” checkers immediately jumped on that claim in an effort to “debunk” what they call “false” information.7,8 But they simply contradicted themselves in the “fact” checking by changing the semantics of how COVID deaths are counted and rewording of how hospitals are compensated for COVID patients from “paid more” to receiving a “bump” in payment. So what’s the difference? They’re still getting paid more for COVID patients.
In analyzing this, it’s important to look at how data of all sorts are collected on you and everyone else in the world. For example:
Nearly everything people do is digitally recorded, analyzed and extrapolated for decision making. You leave a digital footprint each time you use your smartphone or computer. One study showed digital cookies may have lifetimes up to 8,000 years.9 In 2010, it was estimated there were 2 zettabytes (ZB) of data created.10
To put this into perspective, it would take 184 million football fields of 1 GB thumb drives laid end to end to contain the information. Data is so important that the organization that appears to be leading The Great Reset — the World Economic Forum — is also interested in data and estimates there would be 44 ZB of data collected in 2020.11
So, with all that in mind, in a world where data is king12,13,14 the HHS decision to hide COVID-19 data begs the question: What do they want to hide? Are they stopping the flow of data, as opposed to hiding data like the CDC, to reach the same end, where the data are not available for examination and analysis?
HHS Ends Hospital COVID Death Reports
January 6, 2022, the HHS announced15 changes to the reporting requirements for hospitals and acute care facilities. The new guidelines note “The retirement of fields which are no longer required to be reported,” which include the “previous day’s COVID-19 deaths.”
However, according to one news report, the guideline did not receive public attention until January 14, 2022, when it was tweeted by Dr. Jorge Caballero,16 who asked why the government no longer wanted these daily reports beginning February 2, 2022. By January 28, 2022, just like they did with the report on COVID-19 hospital reimbursements, fact-checkers were busy posting viral social media posts claiming Caballero’s conclusions were not correct.
Yet, as I mentioned, the announcement was published on the HHS website — so how could it be false? You can go to the website17 and read it for yourself. Under the section, “The retirement of fields which are no longer required to be reported,” it says: “previous day’s COVID-19 deaths.” So how could fact-checkers “debunk” that?
To create a fact check that claimed this was “false,” the fact-checkers simply changed the headline. So, while the HHS publicly announced they would no longer require hospitals to report deaths from COVID-19, fact-checkers reported the U.S. government was not ending daily COVID death reporting.
MSN18 fact-checkers reported that Nancy Foster from the American Hospital Association had suggested the change could “streamline data collection.” Yet, the HHS system used direct reporting from ICD medical diagnosis codes entered into the Electronic Medical Record (EMR) system.
In an emailed statement, Foster reported that she believes the HHS was no longer collecting data because they were receiving comprehensive data from public health agencies, including death certificates reported to the National Center for Health Statistics and used by the CDC in its death data reporting. Despite supporting the HHS decision, the agency did not respond to a request by MSN on the reason for the change.
HHS had worked with major electronic medical records (EMR) manufacturers, so 85% of hospital reporting was programmed into their computer, and you can’t get more streamlined than that. January 2021, Alex C. Madrigal, co-founder of the COVID Tracking Project,19 wrote:20
“In a series of analyses that we ran over the past several months, we came to nearly the opposite conclusion of other media outlets. The hospitalization data coming out of HHS are now the best and most granular publicly available data on the pandemic. This information has changed the response to the pandemic for the better.”
An unnamed federal health official spoke with a reporter from WSWS,21 calling the move to stop reporting COVID-29 hospital deaths “incomprehensible.” The official added, “It is the only consistent, reliable and actionable dataset at the federal level. Ninety-nine percent of hospitals report 100% of the data every day. I don’t know any scientists who want to have less data.”
CDC Is Hiding Data on Booster Shots
February 20, 2022, The New York Times 22 reported that the CDC has not published large parts of the data they collected during the COVID pandemic. In fact, most of the information they collected in the past year on hospitalizations has not been made public.
The CDC published data on the effectiveness of the COVID-19 boosters in people younger than 65 in early February 2022. However, as The New York Times points out, the data did not cover individuals from 18 to 49 years old.23 This also is the group least likely to benefit from the genetic therapy shot, since CDC data24 demonstrate they have some of the lowest rates of severe disease and death.
The New York Post25 notes that the FDA overruled an expert advisory committee and the CDC overruled their own experts to promote the boosters for all age groups. After ensuring the boosters would be open to all people, the CDC then did not release much of the data despite pleas from scientists.
A look at the published data for those 50 to 65 years shows the booster reduces the risk of death from 4 in 1 million to 1 in 1 million. Further analysis shows that 75% of the additional three people out of 1 million who are helped by the booster shot have at least four comorbidities.26
Unfortunately, since the CDC has not released the raw data, U.S. scientists have had to rely on Israeli data. One study27 published in The New England Journal of Medicine gathered information from 4.6 million people 16 years and older who had received two doses of the Pfizer vaccine. They then compared severe illness and death between those who had had a booster dose and those who had not.
The data showed the group of individuals from 16 to 29 years had zero deaths whether they were boosted or not boosted. Likewise, the group from 30 to 39 years had one death whether they were boosted or not boosted. In fact, the difference in death rate did not rise until the participants were 60 to 69 years, at which point the non-boosted group had 44 deaths and the boosted group had 32 deaths.
In addition to the number of deaths rising in the boosted and non-boosted groups, the percentage of people in those age categories also declined, much like you would find in the general population where the death rate rises as people age.
CDC Claims Data May Be Misinterpreted
Kristen Nordlund is a spokeswoman for the CDC. In her comments to The New York Times,28 she said the data are being slowly released since, “basically, at the end of the day, it’s not yet ready for prime time.” Another reason she cited was the information may be misinterpreted to mean the vaccines are ineffective.
Nordlund gave a third reason for not releasing the data, saying that the data they have is based on 10% of the U.S. population, which the Times reporter points out is the same sample size used to track influenza each year. Jessica Malaty Rivera is an epidemiologist. She spoke with the Times, saying,29 “We have been begging for that sort of granularity of data for two years.”
She went on to say, “We are at a much greater risk of misinterpreting the data with data vacuums, than sharing the data with proper science, communication and caveats.” In an opinion piece, Staten Island Advance’s Tom Wrobleski characterizes the CDC’s decision, writing about what has happened to most people who have been willing to speak out:30
“We’re told to have faith in the CDC, in Dr. Anthony Fauci, in all the experts who are trained to handle public health crises. But we can’t have trust if vital information is withheld from us.
Because then it becomes a case of, “Shut up and do what we say. We’re the experts. You don’t need to know how we come to our decisions. We know what’s best.” And if you question the received wisdom, you’re suddenly a dangerous person. You’re likened to a terrorist. You’re told you want people to die. You get banned from social media.
If you dare protest, you can have your bank account frozen and your vehicle insurance suspended, as we saw during the Freedom Convoy protest in Canada. You can get trampled by police on horseback.
Withholding information only makes people more skeptical. It breeds suspicion. Or mere doubt. The CDC needs to do better if it wants our trust.”
The Jab Is Deadlier Than COVID if You’re Under 80
With the end of the HHS COVID death reporting system, the only means of tracking COVID deaths will now rely on the collection of data from death certificates at the state level. However, as the unnamed official told the WSWS reporter:31
“… deaths are reported by the counties/states but the process is very slow and many coroners are actually not wanting to cite COVID as the reason, while hospitals rely on diagnoses.”
This last part of the sentence may refer to the hospital incentives for a COVID diagnosis, which increases the potential it would be listed in the ICD codes that were communicated to the HHS. Although the CDC and HHS would like the data to remain hidden, a cost-benefit analysis32 by Stephanie Seneff, Ph.D., and independent researcher Kathy Dopp revealed the jab is deadlier than the infection in anyone under the age of 80.
The analysis looked at publicly available official data from the U.S. and U.K. for all age groups and compared all-cause mortality to the risk of dying from COVID-19. Seneff and Dopp wrote:33
“As of 6 February 2022, based on publicly available official UK and US data, all age groups under 50 years old are at greater risk of fatality after receiving a COVID-19 inoculation than an unvaccinated person is at risk of a COVID-19 death.
All age groups under 80 years old have virtually no benefit from receiving a COVID-19 inoculation, and the younger ages incur significant risk. This analysis is conservative because it ignores the fact that inoculation-induced adverse events such as thrombosis, myocarditis, Bell’s palsy, and other vaccine-induced injuries can lead to shortened life span.”
Their analysis is upheld by OneAmerica’s announcement34 that the death rate in working-age Americans from 18 to 64 years in the third quarter of 2021 was 40% higher than prepandemic levels. This finding is stunning since one of the most reliable data points we have is all-cause mortality.
It is a very hard statistic to massage since people are either dead or they’re not. Their inclusion in the national death index database is based on one primary criterion — they’ve died — regardless of the cause. As noted in a (not peer-reviewed) study led by scientist Denis Rancourt, who looked at U.S. mortality between March 2020 and October 2021:35
“All-cause mortality by time is the most reliable data for detecting true catastrophic events causing death, and for gauging the population-level impact of any surge in deaths from any cause.”
Other Insurance Companies Recording Similar Results
Other insurance companies that are citing higher mortality rates36 include Hartford Insurance Group, which announced mortality increased 32% from 2019 and 20% from 2020 before the shots. Lincoln National also reported death claims have increased 13.7% year over year and 54% in quarter 4 compared to 2019. Funeral homes are posting an increase in burials and cremations in 2021 over 2020.37
Similar numbers are also being reported in other countries. A large German health insurance company reported38,39 company data were nearly 14 times greater than the number of deaths reported by the German government. The insurance data are gathered directly from doctors applying for payment from a sample of 10.9 million people.
Despite mass injection campaigns, Silicon Valley software engineer Ben M. (@USMortality) revealed that in the 13 weeks before November 28, 2021, about 107,700 seniors died above the normal rate, despite a 98.7% vaccination rate.40
He also used data from the CDC, census.gov and his own calculations to show excess deaths rising in Vermont, even as the majority of adults have been injected. “Vermont had 71% of their entire population vaccinated by June 1, 2021,” he tweeted. “That’s 83% of their adult population, yet they are seeing the most excess deaths now since the pandemic!”41
It is easy to see why the HHS and CDC would like to hide these numbers from scrutiny. It is becoming more difficult to ignore with each passing day that the infection didn’t kill the number of people health experts claimed and the vaccine is killing far more than the virus.
15% of modern global warming (ocean) can be attributed to geothermal heat fluxes through the sea floor that persistently heat the ocean.
Evidence of more than 100,000 formerly or currently active volcanic vents permeate the Earth’s sea floor (Kelley, 2017).
Active volcanoes spew 380°C sulfuric acid and “metal-laden acidic fluids” into the bottom waters of the world ocean on a daily basis. Literal ocean acidification is thus a natural phenomenon.
The carbon dioxide concentrations present in these acidic floods reach “astounding” levels, dwarfing the potential for us to even begin to appreciate the impact this explosive geothermal activity has on the Earth’s carbon cycle.
Geothermal heating warms up the last 2000 m of the global ocean “by about 0.3°C to 0.5°C” (Emile-Gaey and Madec, 2009). The heat fluxes are systemically positive, span “the entire seafloor,” and the circulation is largely horizontal at these depths. Horizontal circulation allows the bottom waters “to feel the influence of geothermal heating for a long time.”
The rapidity of temperature changes near geothermal sources can be profound. Geothermal heating can induce warming rates of 0.02°C per year, or 0.2°C per decade, offsetting the abrupt (~0.25°C per year) cooling from “cold-seawater intrusions” (Becker et al., 2021).
Approximately 15% of modern global warming (ocean) can be attributed to geothermal heat fluxes through the sea floor that “persistently heat the ocean” (Gebbie, et al., 2021). The value attained for geothermal heating of the ocean, 87 mW/m², is similar to that which is required to end a glacial period (melt ice sheets) and transition into an interglacial.
Considering the ocean bottom waters warmed up 2°C from 19,000 to 17,000 years ago about 1,000 years before the surface warmed and CO2 began rising (Stott et al., 2007), geothermal heat fluxes could potentially explain a large portion of glacial-interglacial transitions – as well as millennial-scale global ocean temperature changes.
The most strenuous form of critique the media seem able to muster is to tell policymakers to apologize for “getting COVID wrong.”
Early on, Children’s Health Defense and other independent voices forcefully called out the government’s sub-rosa agenda as a deliberate, multisectoral effort spearheaded by central bankers and billionaire technocrats to ensnare the world in a global control grid — in other words, modern-day digital slavery.
Viewed from this angle, the “separate mind-boggling events” of the past two years “line up as sequential moves on a worldwide chessboard.”
Restrictive COVID policies and strange central bank maneuvers were no accident but rather the tools of a planned economic takedown of the most vibrant and independent segments of the economy, notably the small “retail, arts and entertainment, personal services, food services and hospitality businesses” that, together with other small business sectors, have “pretty much driven most economic activity throughout our known history.”
Even before this purposeful economic havoc, the developed world’s richest denizens were living at least 10 to 15 years longer than the world’s poorest.
When experimental injections were added in December 2020 to the mix of COVID interventions, the takedown began taking on even more gruesome dimensions.
Discussing far-reaching vaccine fraud allegedly perpetrated by Pfizer, acting in cahoots with the U.S. Food and Drug Administration, former BlackRock investor Edward Dowd has said:
“I think this is the greatest crime ever committed because most of the frauds I’ve been involved with are financial frauds where money’s lost; This has killed and maimed people.”
On March 1, shortly after a board member of German insurance company BKK ProVita expressed public alarm at the widespread killing and maiming — noting that Germany’s federal health agency was underreporting COVID vaccine injuries by a factor of 10 — the executive was summarily fired.
Prominent physician Dr. Vladimir Zelenko, who blazed a hopeful trail with his inexpensive and successful COVID treatment protocol, bluntly characterized the toxic jabs as instruments of “premeditated first-degree murder and genocide.”
Empty words and gestures
Of late, policymakers seem to have decided it’s time for some crocodile tears — and also time to make a show of putting a few COVID restrictions on hold.
For example, consider the recent remarks by Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC). Walensky said health officials “had perhaps too little caution and too much optimism” about the COVID shots.
For those paying attention, there can be little doubt these words and gestures are less about a policy one-eighty than about window dressing and distraction — as well as perhaps a clever move to “undercut” the momentum of the People’s Convoy currently demanding an end to all emergency measures.
As Jon Rappoport warned, “Although some governments … are lifting COVID restrictions and mandates, we should remember they still hold the power to re-impose those measures at the drop of a hat — for any reason they cook up.”
The key takeaway of the last two years, Rappoport clarified, is that governments’ COVID actions were expedient political decisions — designed to “advance tyranny” — and had “nothing to do with science or morality.”
New York City’s recent actions exemplify the duplicity of the policy rollbacks and the steady behind-the-scenes march of the control agenda. Remember — officials there willingly spent two years gutting the city’s famed restaurants, other small businesses and cultural institutions.
Now, while announcing an easing up of restrictions out of one side of his mouth, the new mayor fired almost 1,500 unvaccinated municipal workers, is insisting on continuing to mask 3- and 4-year-olds (defying widespread parental objections) and is advising businesses they “can still choose to require proof of vaccination.”
Maryland is another jurisdiction that has been indifferent to the distress caused by its policies, ignoring, for example, a leading trade group’s warning that politicians’ capricious on-again, off-again restrictions — promoted as protecting “well-being” — would permanently close four in 10 of the state’s restaurants.
In the state’s largest city, the Baltimore government is suddenly reopening some government services and lifting masking edicts. Yet at the same time, the prominent Baltimore Sun is beating the drum for joint COVID and influenza vaccine mandates.
In thinly veiled praise for coercion and segregation, the Sun argued, “employers and municipalities can certainly require flu vaccinations in order to engage in certain activities.”
Policy hypocrisy is also alive and well internationally. While the World Health Organization (WHO) issues parameters for “carefully relaxing the rules” — parameters so narrow as to be meaningless — Italy and China (the two countries that set the global precedent for lockdowns) are fining individuals who decline mandated interventions or denying them entry to workplaces, restaurants, stores, banks and post offices.
Vaccine passports and digital identities — full speed ahead
As Off-Guardian’s Kit Knightly noted on March 1, “Covid might be dying, but vaccine passports are still very much alive.”
In late February, Knightly also pointed out that the WHO, ominously, is working on an “international treaty on pandemic prevention and preparedness” that would invest the global health organization with the authority to preempt national sovereignty in the management of future pandemics and health challenges.
In a five-part series, Corey Lynn of Corey’s Digs outlined many disturbing implications of the push for vaccine passports. Falsely marketed as a “convenience,” the “passports” eventually will encompass far more than just vaccination records:
“From education to health records, finances, accounts, travel, contact info, and more, will all be linked to your QR code, along with biometrics and fingerprints, then stored on the Blockchain.”
The longer-term aim, said Lynn, is to achieve “full power and control,” down to the individual level, of spending, taxation, education, transportation, food, communications and healthcare, among other domains.
As writer Cherie Zaslawsky sees it, globalists “seek to enslave humanity worldwide in their long-dreamed-of totalitarian utopia. That’s utopia for them — as the ruling class that owns the world and everything in it — and dystopia for We the People.”
Knightly’s March 1 commentary drew readers’ attention to SMART Health Cards — “a covert federal vaccine passport” — rolled out in roughly half the country thus far, including in red states that previously had paid lip service to banning vaccine passports.
A late February article in Forbes boasted that more than 200 million Americans can already “download, print or store their vaccination records as a QR code.”
VCI was created by the federally funded MITRE Corporation (an MIT spin-off), which receives an estimated $2 billion a year from U.S. taxpayers to develop advanced surveillance technology, among other dubious national security pursuits.
MITRE received a $16.3 million CDC contract “to help construct an efficient game plan for the country during the health crisis,” and also spearheaded U.S. Department of Homeland Security efforts to “coordinate” responses among the nation’s mayors and governors.
Members of VCI’s public-private coalition include Amazon Web Services, Microsoft, Oracle, Salesforce, the Mayo Clinic, and the California and New York state governments, as well as “other health and tech heavyweights.” Additional organizations are contributing to the initiative as “data aggregators” and “health IT vendors.”
As an inner-circle member of VCI, New York State has been in the vanguard in building out a digital identity infrastructure intended to be interoperable (able to exchange or assemble data) “throughout the United States and abroad.”
New York’s “Digital Identity” policy, conveniently updated in July 2020, stipulates that citizens, businesses and government employees who conduct online business with the state must go through an “identity vetting” process that could involve authentication via “smart card” or “biometrics.”
Refuse totalitarian tyranny
Almost immediately after the COVID shots began being rolled out, Dr. Mike Yeadon, at one time a chief scientist and vice president at Pfizer, began protesting the push to inject children.
Yeadon also denounced vaccine passports, describing the apps as a sly vehicle for implementing “illegal, medical apartheid” and totalitarian tyranny.
In a more recent talk, Yeadon emphasized that the QR codes’ global interoperability will translate into 24/7 tracking of every person “in that moment, in that spot, down to the individual level.”
To impress upon the public the dangers of allowing a vaccine passport system to take hold, Yeadon described what it would mean to become an “out-person:”
“One example: Your VaxPass pings, instructing you to attend for your 3rd or 4th or 5th booster or variant vaccine. If you don’t, your VaxPass will expire & you’ll become an out-person, unable to access your own life.”
Fortunately, the globalists’ stark vision is becoming increasingly apparent to many members of the public, who are coming to understand, as Ron Paul said, that “authoritarian politicians will always lie to the people to protect and increase their own power.”
Mainstream media outlets also have begun openly worrying that “parents have a long memory when it comes to how their children have been treated.”
And, although it may not seem like it, governmental decisions “ARE affected by what citizens do or don’t do,” said Rappoport, arguing that it’s no time to “let up on pressure.”
The bottom line at this critical juncture is simple — rather than be lulled into complacency (or distraction) by the latest propaganda, just say no and don’t comply.
Don’t wear a mask. Don’t get tested. Don’t accept toxic jabs. And don’t download any QR codes or any other tools (no matter how “convenient”) that allow the build-out of digital tyranny.
AMD has to hide his/her identity or he/she will be fired. That’s how the medical system is designed: if you speak against the system, you lose your job. Period.
So to make things easier, I’ll assume AMD is a man.
The AEs documented by AMD were partly from his own patients, but mostly related by people who AMD directly knows. So no more than one step removed: a direct friend of a direct friend.
The results of his analysis (from the Conclusion section of the article):
Critical Injuries: 41
Severe Injuries: 39
Significant Reactions: 32
In AMD’s history, there were no critical injuries for all other vaccines combined. Zero.
But the important part was this statement:
Typically when a drug has between 10-100 critical injuries reported to the FDA, they strongly look at pulling it from the market or giving it a blackbox warning. I thus feel these vaccines are not being held to the adverse reporting standard we expect.
In other words, based on just the data AMD directly collected, the vaccine exceeds the stopping condition.
The numerator and denominator
AMD used more than his own patients: he also used friends of his friends.
AMD’s cases were split: 60% reached out to him with stories and 40% was due to his outreach.
How confident is he that every single case was vaccine related? For half of these cases, there was an extremely strong time correlation or other factors, so he’s extremely confident of a causality link. For the other half of the cases, the causality is extremely likely.
Because his sample includes only the direct friends of his friends, he estimates that the “denominator” in his case is less than 100,000 to be conservative (the average person has around 150 to 250 friends so this is quite conservative). There will be fewer than this due to overlap, but again, we aren’t trying to get to an exact number, just a rough engineering estimate.
AMD’s extended friend pool consists of a mix of vaxxed and unvaxxed people in our calculation. Since he’s a doctor, his mix of vaxxed patients will be higher than others so this may skew our extrapolation to be on the high side, but we are just trying to do a ballpark estimate of what the national rates might look like.
Let’s extrapolate that out to a population of 200M people who are over 18 years old and vax eligible. We’d have to multiply his numbers by 2,000 to get a lower bound on the number of events expected. This isn’t strictly accurate since AMD’s friend base is older and the AEs in the older group would not occur at the same rate as the younger group. So again, not trying to get a a super precise estimate since it isn’t needed as we’ll soon see.
So we have 41*2000 = a minimum of 82,000 estimated critical events caused by the vaccine in our crude estimate.
This is within a factor of 2 of the minimum of 150,000 deaths I’ve previously estimated for the vaccine (using over a dozen different methods). So it appears we were right in that our estimate was conservative. And our crude extrapolation also is well within numbers previously determined so it serves as a crude sanity check that the numbers reported by AMD were “reasonable.”
Comparing with our 10 to 100 critical event stopping condition, we find:
82,000 >> 10 to 100
The stopping condition for the vaccine is met not only from AMD’s direct observations alone (even adjusting a factor of 2 for causality doubts), but also for our conservative (and very crude) estimate of the total number of critical events in the US. QED.
Finally, let’s be clear: I am not claiming that we can extrapolate a single anecdote to an entire population to get an accurate rate estimate. I am only claiming that AMD’s observations alone justify halting the vaccines and that any extrapolation of that number to the entire population based on any reasonable assumptions shows that the stopping condition is exceeded by a large margin.
What other doctors are seeing
AMD polled his colleagues to see if they were seeing the same thing.
30% confirmed they were
70% said they either saw nothing at all and/or didn’t want to talk about it
He attributes the 70% seeing nothing as them not being aware of the possibility that the vaccines could be unsafe so any adverse reactions are immediately discounted and discarded; they don’t register.
Therefore, even if we further discount our calculation of 82,000 by 70% in the belief that these rates seen by AMD are inflated, the number critically harmed (24,600) is still way over our stopping threshold and that’s really the only thing I wanted to show.
The Pfizer Phase 3 clinical trial
AMD noted that when the shots were administered, people quickly discovered a high rate of anaphylaxis.
He asked, “How could the clinical trial not have found that?”
Indeed. Anaphylaxis wasn’t mentioned at all in the Phase 3 trial report despite the fact that it is life threatening.
It wasn’t mentioned in the 6 month follow up study either. That study would have included reactions of the placebo cohort who got the vaccine.
Anaphylaxis occurs at 2.47 events per 10,000 doses so there should have been around 10 events observed for the full-vaccinated treatment group (44,000 doses) and a similar number of events when the placebo group was vaccinated.
So we should have seen 21 anaphylaxis events on average yet there were none reported. This is extremely unlikely to happen by chance.
How does Pfizer explain that? This is, of course, a rhetorical question as nobody is going to ask them that question and they don’t have to answer it. That’s just the way it works in medicine. You are not allowed to ask questions like this. It’s “science.” We are teaching our kids to believe whatever the drug companies tell them and not ask questions.
One other “highlight”
This comment at the very end of AMD’s article deserves special mention:
Or as another commenter here wrote: I was a Midwestern nurse last year after the gene therapy roll out. Was a case mgr did discharge planning. Saw 10-12 side effects Daily. Everything you shared and more. 2 cases of amnesia ( one was a healthy anesthesiologist). 1 girl in her twenties with blood in her tears. Had to leave that job.
A girl with blood in her tears?!?! When was the last time you saw that?
Notes
In his writeup, AMD made the case write ups deliberately vague in order to protect patient confidentiality.
Reader feedback
Check out this comment on what is happening in Melbourne, Australia mirrors what was described in this article. She explains “doctors are very worried about what they’re seeing from the jabs but keeping quiet to save their jobs.” Makes perfect sense. A doctor’s first duty is to his/her family. I see this all the time. This is why the doctors I talk to stay quiet. I don’t blame them.
Another reader wrote this:
Steve,
I love your work. The physician in the Midwest is right. I am a practicing ophthalmologist in the southeast and have come across multiple catastrophic side effects from the shots. I have been sounding the alarm to my friends and colleagues for over a year. Most of these think I am crazy.
It started last year in roughly March when I walked into a patient’s preposition room to have a mom sign a consent. She apologises to me that she had trouble writing for she had just recently had a stroke. I told her I was glad she was here then asked if she knew what the cause was. “It was that shot” she said. She was in the hospital that night. I then went to the OR and told my CRNA the story. She proceeded to tell me her friends daughter died (39) died with a pulmonary embolus 1 month after getting one. I told this to one of my partners who said his friend was in the hospital with myocarditis after having a shot.
I also know of a physician in a nearby practice dropping dead at 52 with a heart attack. He had recently been vaccinated according to his front desk.
I also know of 3 breast cancer diagnosis after vaccinations as well as a transverse myelitis and a brain stem glioma. All of these had been vaccinated but I cannot say that these were caused by the shots.
One of my parent’s good friend’s son in law died suddenly from a heart attack at 39. He was also recently vaccinated.
In my own practice, I have 3 patients with side effects. 1 with increased intracranial pressure . Almost immediately after the second Pfizer dose the patient started experiencing headaches. I saw the child about a week after and she had swollen optic nerves.
A second had uveitis roughly 2 weeks after the first dose.
A third patient had a “spontaneous “ vitreous hemorrhage within 2 weeks of a dose.
There are some others I know of too…
If I mention these to most doctors, they just look at me with blank stares. I have been ridiculed, reprimanded and threatened for just telling physicians my observations.
These need to be stopped yesterday.
Summary
Based on the number of just this one physician’s observations, the vaccines should be immediately halted.
AMD is not an isolated data point. He discovered that 30% of his colleagues are seeing similar things.
I can also personally confirm that speaking confidentially with other physicians (who fear retribution such as loss of medical licenses if they speak out), that AMD is hardly alone. The doctors I know have never before needed to report an event to VAERS in the past and this year have had 20 and 1,000 case reports to make. They won’t talk to the FDA about what they see because they don’t want to have their licenses revoked.
As AMD’s case shows, the medical community makes it impossible for these doctors to speak freely and tell what they know. Doctors are forced to hide in the shadows to tell their story or simply remain silent.
The days of colleagues having open friendly discussions to resolve conflicts are gone. The medical community now uses fear and intimidation techniques to silence any scientific dissent. For example, in Canada, an entire university ganged up on Dr. Byram Bridle to discredit him for speaking out. Would any of the University of Guelph faculty debate him? Of course not! No chance. Some faculty members even signed the joint faculty letter denigrating him without even reading the document he wrote. In their mind, Professor Bridle was wrong and they didn’t even have to bother to take the time to understand his position.
In California today, the legislature is seeking to further empower the medical boards to remove the license of any physician who speaks out against the vaccines. It is a top down dictatorship with the Medical Boards holding all the cards. They are not accountable to anyone. They will not be questioned. In many cases, the doctors who are having their license revoked don’t even know who is examining them and are not allowed to question the authorities on the record. So the boards cannot be held accountable for their actions.
Even though the evidence is clear that these vaccines are harmful and should be stopped, we, as a society, are doing the opposite today with vaccine mandates requiring people to be boosted or be fired. We are requiring doctors like AMD to keep their mouths shut.
There is even a US government form now so you can turn in any doctor who challenges the official narrative. Basically, the government is asking us to be spies to help them eliminate people who disagree with the narrative.
Someone isn’t telling you the truth here, and it isn’t A Midwestern Doctor.
You should be upset. Very upset. This is unconscionable.
Unfortunately, no public health official in America wants to talk about it, and the mainstream press isn’t going to cover it either.
Neatly nestled behind the Ukraine headlines plastered all over the front pages, this past week has seen the World Health Organization meeting to discuss the global legislation to empowering the WHO to combat “future pandemics”.
The first consultation was held on March 1st. The EU passed a motion authorizing the bloc to negotiate such a treaty on March 3rd.
Nobody knows exactly what the hypothetical international regulations – dubbed the “Pandemic Treaty” – would entail, but there are hints.
It’s almost certainly going to involve some kind of international vaccine passport, possibly based on the SMART Health Cards currently rolling out all across the US.
It’s also interesting to note that this treaty is being developed in parallel to the UK “reforming” their Human Rights Act 1998 into a new “UK bill of rights” which seeks to prevent the “abuse” of “rights culture” and place a new emphasis on “social responsibility”.
However, the specifics will remain a mystery until the final proposal is published later this year.
One thing we do know though, is that a big part of the proposed “strengthening” of our pandemic response will be increased funding and resources for developing vaccines even faster than the Covid vaccine.
This aim was announced at the recent Global Pandemic Preparedness Summit in London, where the Coalition for Epidemic Preparedness Innovations (CEPI) announced their “100 Days Mission”.
CEPI, for those who don’t know, is a foundation jointly funded by (among others) the Bill and Melinda Gates Foundation and the World Economic Forum, whose stated aim is “to develop vaccines to stop future epidemics”.
The 100 Days Mission, which already has its own website and a trending hashtag (#100DaysMission), is pretty much exactly what it sounds like.
In future CEPI wants to produce new vaccines for unknown emerging diseases – what they call Disease X – within 100 days of the pathogen being isolated.
They’ve already secured 1.5 BILLION pounds sterling to further this effort.
Let that percolate.
Over a billion pounds to produce vaccines for a disease that – as yet – does not even exist, and may never exist.
This looks like a further step in the process, begun by the ‘pandemic’ narrative, of redefining everything we previously understood about how infective agents and vaccines interact.
Covid, let’s remember, was a disease-narrative totally removed from all social, scientific and historical context to create a fluid, agenda-driven alternate reality. And it looks as if this is intended to be the ‘new normal’.
Here’s a little refresher course on just how fast the Covid vaccines sped through the usual scientific process:
The paper that all the PCR tests were based on was peer-reviewed in less than 24 hours.
After decades of failure, the human race produced a dozen effective coronavirus vaccines in less than three months.
These vaccines were then “safety tested” in less than six months.
All told, from ‘discovering’ the virus to getting the vaccine(s) approved for use on people, it took 300 days.
This process normally takes at least 3-10 years.
It usually takes at least 5-10 years to bring a fully-tested vaccine to market. A paper by Pronker et al, “Risk in vaccine research and development quantified” (PubMed 2013), estimates the average development time for a new vaccine to be over 10 years.
Simply put, it has never been possible to make a vaccine for a new disease in 1000 days, let alone 100.
The speed with which the covid vacines were produced is totally unprecedented in the history of vaccines.
The idea you could further reduce this unprecedented time frame, and produce a safe and effective vaccine in only 100 days is frankly absurd. It’s surreal. Fictional.
For one thing, the vast majority of candidate vaccines don’t work.
The Pronker paper, found that of all potential vaccines products being researched, only about 6% ever actually hit the market.
So, back in the real world, a vaccine manufacturer will go through that 5-10 year process knowing there is a ~94% chance there will be nothing to show for it in the end.
After decades of trying they haven’t managed to produce a vaccine against AIDs, or the flu, or malaria or many other common diseases. These are conditions they know and (allegedly) understand, but they cannot make vaccines for them.
So, in that old world of veridical reality, even if you managed to make a vaccine in 100 days, the odds are it either won’t produce immunity, or it will but will also produce harmful side effects, or maybe it will do literally nothing.
Now, granted, science and technology are not static. We are always moving forward and making progress… but that’s irrelevant to this issue, because even if vaccine manufacturing technology really did take a huge leap forward just in time to battle covid, you still can’t produce a safe vaccine in 100 days, or even 300 days – because the process NEEDS time.
It takes time to test rigorously, it takes time – a lot of it – to a assess long term side effects. The clue is right there in the name.
No amount of new tech is going to permit you to know the ten-year effects of a vaccine in under three months.
With the public eye fixed on Ukraine, and Covid now firmly in the collective unconsciousness’s rearview mirror the powers that be are trying to normalise what was, inherently, an abnormal, unreal (if not impossible) process. To make it easier “next time”.
We’ve already seen Bill Gates lament that the vaccine was too slow, and he was partially right. The Covid story didn’t keep people hypnotized enough to secure everything they needed, in part because their “vaccine” rollout took almost a year.
But for the future “Disease X” waiting in the wings, it will officially only take three months, and the fear will still be fresh. The fact the process will be completely incompatible with reality or sense will not matter in the slightest.
To be clear: You cannot develop a “safe and effective” vaccine for a brand new disease in three months.
You can’t do it in one year.
And if in the future they claim to have done so, they will be lying.
Full Title: Omega-6 Apocalypse 2: Are Seed Oil Excesses the Unifying Mechanism for Overweight and Virtually All Chronic Disease? – Chris Knobbe (AHS21)
Over the past 150 years, we’ve witnessed the evolution of pandemics of chronic degenerative, metabolic, and noncommunicable disease (NCD). Ample evidence supports the conclusion that coronary heart disease, cancers, metabolic disease, type 2 diabetes, obesity, age-related macular degeneration (AMD), and many other chronic diseases have risen from medical rarity to the most common causes of chronic disease and death.
During this same time frame, we’ve witnessed industrially produced seed oils, rich in omega-6 fatty acids, elevate to occupy up to one-fourth to one-third of human consumption, or more. Such oils rarely existed anywhere prior to the American Civil War, globally. Virtually all chronic degenerative diseases have in common one primary metabolic defect, namely, mitochondrial dysfunction. Seed oil and high omega-6 is a known driver of mitochondrial dysfunction, as evidenced in many studies.
Furthermore, an examination of food consumption patterns in many nations strongly indicates that seed oils are by far the greatest factor in such chronic disease. An examination of food consumption in Japan leads to no other obvious conclusion. Could omega-6 rich seed oils, consumed to excess, be the common precipitating factor for most all chronic disease, via multiple mechanisms, including the fact that they are pro-oxidative, proinflammatory, cytotoxic, genotoxic, mutagenic, atherogenic, thrombogenic, and obesogenic? The evidence is compelling.
A study funded by the Centers for Disease Control and Prevention (CDC) and published Monday in The Lancet concluded most COVID-19 vaccine-related adverse events reported during the first six months after the vaccines were rolled out in the U.S were “mild and short in duration.”
For the study, researchers analyzed data captured between Dec. 14, 2020, and June 14, 2021, by two reporting systems, the Vaccine Adverse Event Reporting System (VAERS) and v-safe, both of which are overseen by the CDC. Nearly 300 million doses of COVID vaccines were administered during the study period.
The authors found that of the 340,522 adverse events reported to VAERS, 27,023 (8%) were serious, 4,496 of which were deaths.
The U.S. Food and Drug Administration (FDA) defines a Serious Adverse Event (SAE) as an outcome that is life-threatening or one that results in hospitalization (immediate or prolonged), permanent injury, birth defect or death.
Authors suggest vaccines didn’t cause deaths
As an event capturing system VAERS is not designed to attribute causation. However, the authors noted that there was a “… concentrated reporting of deaths on the first few days after vaccination..”
The temporal relationship of the death to the time of vaccination was demonstrated here:
The correlation in time between inoculation and death is highly suggestive of causation. Instead, the authors chose to explain it as follows:
“This pattern might represent reporting bias because the likelihood to report a serious adverse event might increase when it occurs in close temporal proximity to vaccination.”
The authors suggest that if a death occurs soon after vaccination it will be more likely reported than if the death occurred later. This, they believe, is why the number of deaths asymptotically approaches zero as more time elapses since inoculation.
Independent researcher unable to duplicate study’s VAERS findings
Jessica Rose, Ph.D., attempted to duplicate the Lancet authors’ findings through her independent analysis of the VAERS data.
Despite filtering the database using three different date stamps (Vaccination Date, Onset Date and Received Date), none returned the number of reports published in the Lancet.
From her analysis:
“The closest I got to their estimate when I filtered using the RD (Received Date) data was 371,775.
“For the VD (Vaccination Date) data filter I got 545,275 reports and for OD (Onset Date) data filter I got 499,432 reports.”
In other words, using every date option, Rose found tens (sometimes hundreds) of thousands more reports than the authors of the Lancet study found.
The most conservative number, 371,775, is still nearly 30,000 more than reported. Nevertheless, using the Received Date as the date filter still returned 6,114 deaths — 36% more than the CDC study claimed.
Furthermore, Rose’s most conservative search parameters returned 68,124 SAEs, or three times more than the Lance study.
Rose said she believes using the Received Date field will unavoidably lead to an undercount of actual reports because this field is left blank more often than the other timestamps in a given record.
How can this large difference be reconciled?
One clue is Pfizer’s “Cumulative Analysis of Post Authorization Adverse Event Reports,” a document released through a Freedom of Information Act request submitted in August 2021, by the Public Health and Medical Professionals for Transparency.
In it, approximately 50% of adverse events reported to Pfizer were SAEs. The adverse events tabulated in this document were passively reported, as they are in VAERS. This further suggests that the authors of the Lancet report may have undercounted SAEs for an unexplained reason.
What about the v-safe findings?
The authors reported separately on their analysis of v-safe data.
V-safe is an active reporting system. Enrolled participants are contacted by phone and are asked to complete a survey. Active surveys are expected to return more complete data. Subjects agree to enroll voluntarily.
Of the 5,674,420 vaccinated subjects that received a second dose and responded through the v-safe system, 26.5% reported they were unable to do normal activities at the time of survey completion.
Additionally, 16.1% were unable to work, 0.9% received medical care and 2,053 were hospitalized.
“In an accompanying editorial, Matthew Krantz, MD, and Elizabeth Phillips, MD, both of Vanderbilt University School of Medicine in Nashville, Tennessee, characterized the report as ‘reassuring,’ noting that, ‘there were no unexpected signals other than myopericarditis and anaphylaxis, already known to be associated with mRNA vaccines.’”
Krantz and Phillips stated myopericarditis and anaphylaxis were “unexpected” signals but were already known to be a problem.
Nonetheless, the Lancet study found that the incidence of myopericarditis and anaphylaxis were 4.4 and 5.5 per million vaccine doses administered respectively.
Yet coagulopathies (clotting disorders including pulmonary embolism), seizures, strokes and Bell’s Palsy (paralysis of the facial nerve) all occurred at higher incidence rates than myopericarditis according to the Lancet study.
Why aren’t these considered unexpected signals to be further investigated or at least acknowledged?
Anaphylaxis, though reported at an incidence of 5.5 per million in the Lancet study, is known to occur at a much higher rate from COVID vaccines.
In a paper published in March 2021, anaphylaxis following COVID vaccines was found to occur at a rate of 250 per million. These findings are a foundational argument for the existence of a significant and calculable underreporting factor (URF) with regard to all events reported in VAERS.
Steve Kirsch estimated the URF to be approximately 41. It is not possible to know what the URF is for every adverse event. Nevertheless, the 4,496 deaths reported in the Lancet are most likely grossly under-representative of the true number of vaccine-related fatalities.
Late in the summer of 1971, a young man was taken from his home in Palo Alto, California. Then another. And another. Nine in all, they were each spirited away. Eventually brought to a place with no windows and no clocks, they were stripped and they were chained. They were costumed in dress-like gowns. They were given numbers to be used in place of their names. Minor pleasures were redefined as privileges, as were such basic acts as bathing, brushing one’s teeth, and using a proper toilet when one pleased.
In essence, they had become the playthings of the nine other young men who now kept them in that windowless place. Uniformly dressed in khakis pants and shirts, along with large reflective sunglasses, wearing whistles around their necks and brandishing clubs, these nine other young men could have been their classmates, their co-workers, their friends had they met in another place or time, but instead now possessed near absolute control over them, often exercising it for no other purpose than to humiliate and emasculate, to remind their prisoners of their subordinate state.
These uniformly dressed young men in khakis and sunglasses were the guards of the “Stanford County Prison.” They were acting at the behest of Dr. Phillip G. Zimbardo.
The research that Zimbardo carried out that August would go on to become one of the most renowned and most infamous studies in the history of psychology.
As the story is told in most introductory psychology texts, Zimbardo set out to study the power of situational forces and social roles on identity and behavior. To do this, he randomly assigned seemingly normal college students with no criminal history or mental illness to the role of guard or prisoner in a simulated prison, providing little to no instruction.
However, due to the spontaneous and increasingly sadistic actions of the guards and the extreme emotional breakdowns of the prisoners, Zimbardo had to call off the experiment prematurely – but not before making some important discoveries about how social roles and oppressive environments can alter the psyches and actions of normal people in pathological ways.
Zimbardo’s own descriptions of his work tend to be somewhat more grandiose, sometimes bordering on a telling of a Greek myth or biblical tale, a story of something surreal, or as Zimbardo once put, something “Kafkaesque.”
The way the story is presented in the transcript of a slideshow put together by Zimbardo, all who entered that mock prison he constructed seemingly drifted into a dream. The minds of those who stayed too long fractured. Soon, everyone who remained began to metamorphose into nightmarish vermin.
Fortunately though, the good doctor was awakened by the pleas of a young man, who, in the midst of a mental breakdown, begged not to be released so he could prove he was a good prisoner. This is when Zimbardo knew it was time to bring the world he had created to an end.
Critics, however, have questioned many aspects of Zimbardo’s telling of the tale and its often uncritical, albeit less dramatic, retelling in psychology texts.
Only a third of the guards actually behaved sadistically. Some of the prisoners may have faked their emotional breakdowns for early release after being led to believe that as volunteer prisoners they were not permitted to leave the pretend prison.
But perhaps the most damning critique is that from the beginning, Zimbardo, who took on the role of prison superintendent, made it clear that he was on the side of the guards. He did this along with his undergraduate warden, who had researched and designed a rudimentary dormroom version of the simulation three months prior for a project in one of Zimbardo’s classes. He provided the guards with detailed instructions for how to manage the prisoners at the start, then continuously pressed them to be tougher on the inmates as the Stanford experiment went on.
In a documentary, Zimbardo acknowledged that, although he forbade the guards from hitting the prisoners, he explained to them they could instill boredom and frustration. Video from orientation day shows the charismatic professor in his prime instructing his guards, “We can create fear in them, to some degree. We can create a notion of arbitrariness, that their life is totally controlled by us, by the system.”
Some participants later admitted to leaning into their assigned roles deliberately. Given that Zimbardo was paying them $15 per day for their participation, he was essentially their boss at their summer job.
Despite these additional details though, it remains difficult to deny that Zimbardo’s study can tell us something important about human nature.
Maybe like the pre-teen boys with whom Muzafer Sherif played Lord of the Flies in the summers of 1949, 1953, and 1954, the young men of Stanford County Prison came to internalize the identities associated with their arbitrarily assigned groups, but here in an environment intelligently designed for oppression and with a pre-established social hierarchy.
Maybe like the seemingly normal Americans Stanley Milgram instructed to deliver what they thought were increasingly painful shocks to forgetful learners in an alleged memory experiment, they were just obeying authority.
Maybe they simply knew they were getting paid by the day and wanted this arrangement to continue.
Maybe it was a combination of the above.
In the end though, at least a portion of guards and prisoners acted in accordance with their arbitrarily assigned roles, with perhaps members of both groups accepting the authority of those above them, even if it meant behaving with casual cruelty or accepting degradation.
The Current Experiment: Year One
In the early days of the Pandemic Era, our superintendents and wardens took control over all aspects of daily life. They costumed us in masks. Minor pleasures, as well as basic acts such as spending time with family and friends were redefined as privileges. They created fear. They instilled boredom and frustration. They created a notion of arbitrariness, that our lives were totally controlled by them, by the system. We were their prisoners. We were their playthings.
In the early days of the Pandemic Era, there weren’t true guards or arbitrary groupings beyond authorities and prisoners – at least not any with which many truly came to identify.
We had actual law enforcement who could be said to have acted as guards in some places, following the orders of the superintendents and wardens, arresting lone paddle boarders and harassing parents for letting their children have playdates. Yet, most people throughout much of the United States, at least, never quite experienced that level of direct tyranny.
Early on we had the designations of essential and nonessential, but no one really knew what those categories meant. No one derived real power or status from them.
The only distinctions that could be said to have meant anything for Year One of the Pandemic Era were obedient and dissident, masked and unmasked, good prisoner and bad prisoner, although even these lost some meaning by virtue of the fact they were impermanent and fluid and that revealing one’s affiliation was generally a matter of personal choice.
The obedient granted themselves the occasional indulgence, meeting up with romantic partners and taking off their masks in the company of intimates. The unmasked reluctantly donned the symbol of their oppression when required. No one had to state their cognitive dissonance.
It was not until the Covid vaccines became available that more meaningful groups began to emerge.
The Current Experiment: Year Two
As the Covid vaccines became widely available, the objective groups of vaccinated and unvaccinated took shape and it was clear which group our superintendents and wardens favored from the start.
Sometimes they provided direct instructions. Sometimes they did not. But, in locations and institutions where their power was strongest, our superintendents and wardens encouraged and coerced their prisoners to be part of the favored group, allowing them to earn back such privileges as education, employment, and minor pleasures from the lives they once lived. They also made it clear that no one could fully rise from their present state until virtually everyone chose to do so.
Before long presumably normal people came to support vaccination requirements for travel, work, and education.
Some, however, seemed to go a step further and began to fancy themselves as guards.
As in the Stanford County Prison, physical violence was out of the question. So was the kind of pushing, shoving, and nighttime raids Sherif observed among the arbitrarily divided boys chosen for his summer camps. However, various forms of ostracism were deemed fully acceptable, if not encouraged and condoned.
Yet, more subtly, it also took the form of a kind of casual cruelty within families, offices, and schools.
Loved ones required one another to show proof of vaccination to attend weddings and holiday gatherings.
Those who had received medical or religious exemptions from employers and universities with vaccine mandates had, in some places, supervisors that barred them from certain corners of their workplaces and co-workers and classmates, who long ago stopped masking and social distancing around one another, reminded them to keep their distance and demanded that before entering a room they stand in the doorway and give those present time to mask up.
Although maybe not sufficient to foment the kind of alleged breakdowns noted by Superintendent Zimbardo at the Stanford County Prison, at least in the short term, it does not take much to imagine how such day-to-day humiliations could erode one’s sense of belonging or meaning. Long-term, it would seem only natural for such constant reminders of one’s subordinate state to engender feelings of depression, alienation, and worthlessness.
A considerable body of research on ostracism and social exclusion would suggest such feelings would be only natural.
Additional work in the area indicates that those that have been ostracized, to some degree, come to see themselves and their social aggressors as losing elements of their human nature, changing into cold and rigid things lacking agency and emotion.
In other words, our modern prisoners, with time, come to see themselves and their guards as metamorphosing into nightmarish vermin.
Future Directions: Year Three
As time passes though, it is becoming increasingly clear that the effectiveness of the Covid vaccines is not quite what was initially promised.
Numerous studies from California, Israel, Ontario, and Qatar, along with others, have consistently shown that fully vaccinated individuals can still contract and presumably transmit SARS-CoV-2, especially following the rise of the Omicron variant.
Hence the basis for ascribing any real meaning to the groups of vaccinated and unvaccinated, or at least any real meaning from which the former could be granted or derive some form of social or moral superiority over the other, has been demolished.
Subsequently it would only make sense that these groupings dissolve.
Yet, research has shown that people still find meaning in even the most meaningless groupings even when there is no objective reason to do so.
After a year of our superintendents and wardens publicly impugning the unvaccinated as a literal and figurative blight on society standing in the way of a return to normalcy, it is even more understandable that some continue to find meaning in these designations.
Thus, even as some cities and companies drop vaccine mandates, not all have been willing to return the same rights, now termed privileges, to both vaccinated and unvaccinated alike.
Additionally, the family, friends, co-workers, and classmates of some unvaccinated individuals still experience no qualms about behaving with casual cruelty towards them. Some unvaccinated individuals are even still willing to accept their casual degradation.
Maybe like the pre-teen boys with whom Muzafer Sherif played Lord of the Flies, these modern guards and prisoners have come to internalize their new identities, but in an environment intelligently designed for oppression and with an implied social hierarchy.
Maybe like the seemingly normal Americans, Stanley Milgram instructed to deliver what they thought were increasingly painful shocks to forgetful learners in an alleged memory experiment, they are just obeying authority.
Maybe they are trying to do their part to please their superintendents and wardens in the hope of earning some imagined reward.
Maybe it is a combination of the above.
A Final Lesson from Superintendent Zimbardo
Given the world in which we have been living for the past two years, despite the numerous flaws critics have found in both Zimbardo’s work, as well as Zimbardo the man and Zimbardo the legend, it would seem that both he and other members of social psychology’s golden age can still tell us a lot about how social roles, oppressive environments and powerful authorities can alter the psyches and actions of normal people in pathological ways.
But perhaps one of the last lessons Zimbardo can teach us is more a reminder of something George Orwell wrote in 1984 : “Who controls the past controls the future; who controls the present controls the past”.
Throughout his career Zimbardo appears to have actively worked to write his own myth and influenced the fields of psychology and criminal justice for decades.
Hence, perhaps as long as those who worked to give social or moral meaning to the groupings of vaccinated and unvaccinated are allowed to write the myth of how the public policies and interpersonal behaviors that followed contributed to delivering us to our returning semblance of normalcy, the more likely we will be to continue to have a society of guards and prisoners who act with casual cruelty and accept degradation as we move forward into the future.
Daniel Nuccio holds master’s degrees in both psychology and biology. Currently, he is pursuing a PhD in biology at Northern Illinois University studying host-microbe relationships. He is also a regular contributor to The College Fix where he writes about COVID, mental health, and other topics.
This is a scandal of immense proportions that warrants an immediate investigation.
First, let’s set the stage:
— Over one year ago, there were ample peer-reviewed, randomized controlled trials that provided strong evidence on ivermectin’s efficacy as a treatment for COVID in every disease phase.
— A paper considering these many studies was written by lead author Dr. Andrew Hill at the University of Liverpool for the World Health Organization’s COVID Guideline Development Group. Hill was an early and vigorous proponent for ivermectin. His paper showed that ivermectin could reduce deaths by 75% if used throughout the world.
— Inexplicably, just days before its publication, the paper appeared on a pre-print server, with its conclusions changed. Instead of concluding that ivermectin—one of the world’s safest and most inexpensive drugs— should be rolled out globally, it now concluded that more studies on ivermectin were needed before it could be recommended worldwide. Given the totality of scientific evidence for ivermectin, it was a stunning—actually shocking—reversal by Dr. Hill.
—In an urgent Zoom call to Dr. Hill initiated by Dr. Tess Lawrie, Director of the Evidence-based Medicine Consultancy, Dr. Hill admitted to her that one of his study’s sponsors, Unitaid, had a say in the conclusions of his paper. But he would not divulge the name(s) of those who altered the paper’s conclusions.
But now, “The Digger” on Substack (aka producer/director Phil Harper) has revealed the name of the person who could have edited the paper’s conclusions—which led to the WHO’s non-recommendation of the use of ivermectin. That decision could have led to the unnecessary deaths of millions across the world.
GASP.
Mr. Harper studied the PDF of the paper, wanting to learn the identity of its “ghost” author. “The hope was that some artifact on the PDF would reveal something, maybe a font was different, maybe there was a hidden comment, maybe some tracked changes had been saved to the document,” said Harper. “None of those lines of inquiry came to anything.”
Then it came to him. Was it in the PDF’s metadata? “Sometimes it’s the most obvious of things,” Harper writes. “The ‘v1_stamped’ version of the paper did indeed have metadata. It even had author information inside the metadata. Expecting to see Andrew Hill listed as the author, instead, I saw a name I recognized. Andrew Owen.
“Unless someone used his computer, Andrew Owen has his digital fingerprint on the Andrew Hill paper.”
Professor Andrew Owen is the person who allegedly edited the critical Andrew Hill paper on Ivermectin. He was also in receipt of consultancy fees from pharmaceutical companies with competing products.
As it turns out, Andrew Owen is a Professor of Pharmacology & Therapeutics and co-Director of the Centre of Excellence in Long-acting Therapeutics (CELT) at the University of Liverpool. He is also scientific advisor to the WHO’s COVID-19 Guideline Development Group. Just days before Dr. Hill’s paper was to be published, a $40M grant from Unitaid, the paper’s sponsor, was given to CELT —of which Owen is the project lead. “The $40 million contract was actually a commercial agreement between Unitaid, the University of Liverpool and Tandem Nano Ltd (a start-up company that commercializes ‘Solid Lipid Nanoparticle’ delivery mechanisms)— for which Andrew Owen is a top shareholder,” says Harper.
Furthermore, Harper writes that, “Andrew Owen is prolific in the art of receiving money from pharmaceutical companies. He’s received research funding from ViiV Healthcare, Merck, Janssen, Boehringer Ingelheim, GlaxoSmithKline, Abbott Laboratories, Pfizer, AstraZeneca, Tibotec, Roche Pharmaceuticals and Bristol-Myers Squibb.”
GASP.
Read the entire essay HERE. In it, Harper reveals much, much more. This is just the latest in a series of postings on ‘The Digger’ exposing the machinations and the backdoor wheeling and dealing to prevent ivermectin from saving lives so that other, more profitable (and scientifically proven more dangerous) designer drugs could take center stage and make bank.
By Lisa Pease | Consortium News | September 16, 2013
More than a half century ago, just after midnight on Sept. 18, 1961, the plane carrying UN Secretary-General Dag Hammarskjöld and 15 others went down in a plane crash over Northern Rhodesia (now Zambia). All 16 died, but the facts of the crash were provocatively mysterious. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.









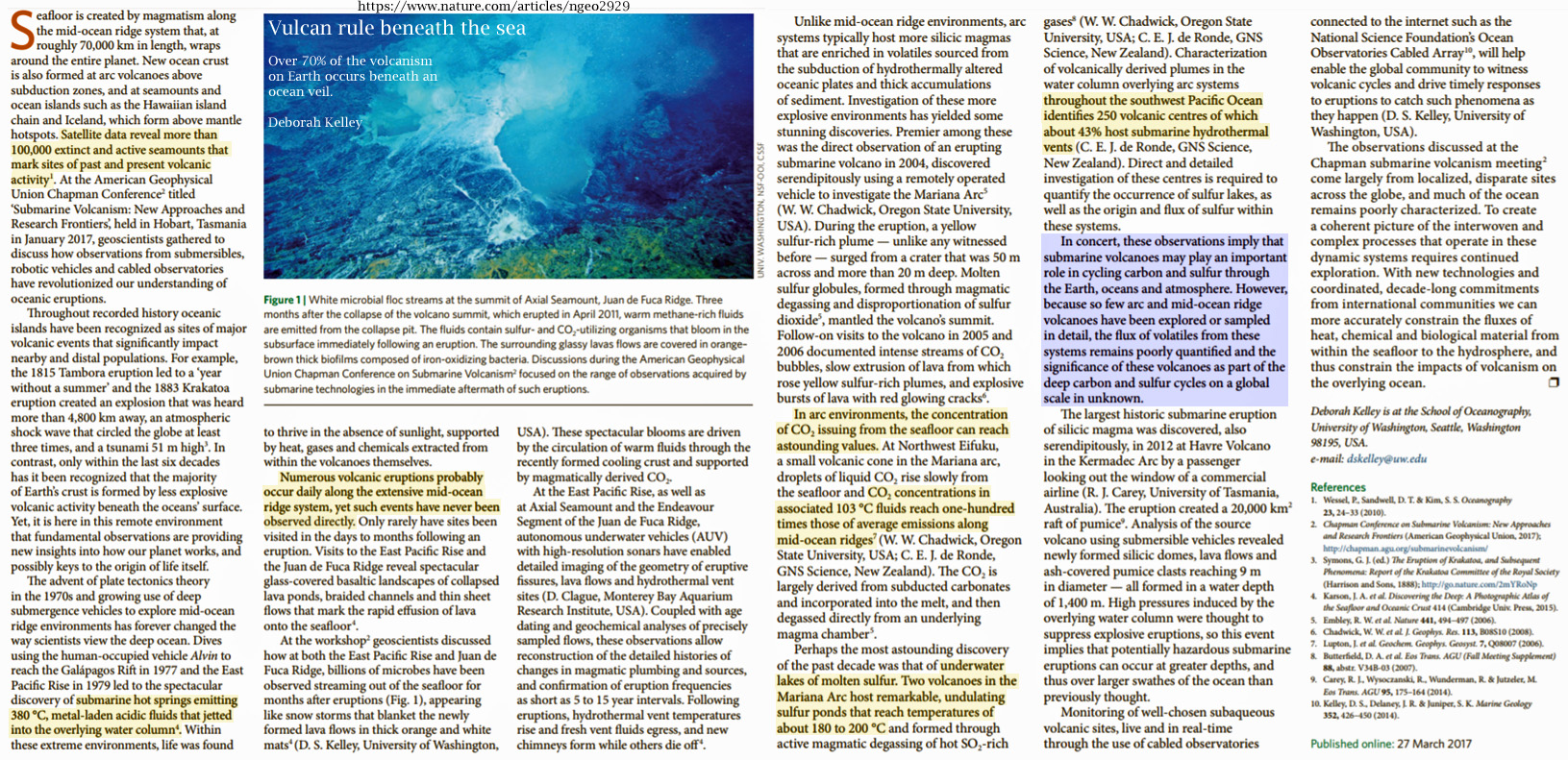{kind=link}