Steve’s fact-based COVID-19 hub

By Steve Kirsch | February 2, 2022
Spotify made a press release about their new platform policies which prohibits any information which in their sole opinion may cause offline harm or poses a direct threat to public health. They refer people to their “fact-based” COVID-19 hub for accurate information.
I think their “fact-based” hub is filled with misinformation, so I decided to write my own simplified version that takes just a couple of minutes to read.
Here it is:
- Early treatments using repurposed drugs in a proven protocol are the best way to treat COVID. Treating as soon as symptoms appear is key. Fareed and Tyson have now treated over 10,000 people infected with COVID without any deaths as long as the people arrived early in the disease. The NIH and CDC ignore these treatments. I recommend you choose an early treatment protocol where there have been at least 10,000 COVID patients treated early without a single death (such as the Fareed-Tyson protocol), and start it as soon as you have symptoms.
- The evidence is clear that all of the current COVID vaccines available in the US today are both unsafe and ineffective. They are not suitable for anyone because they are more likely to kill you than to save you. If they don’t kill you, they may permanently damage your immune system or leave you permanently disabled. Avoid these at all costs. After 90 days, it appears that the vaccines have negative efficacy against Omicron, making you up to twice as likely to be infected. This is likely why case rates are so high in highly vaccinated countries. See Incriminating Evidence for details.
- Cloth and surgical masks do not work. There have been just two randomized trials with masks and COVID (Denmark and Bangladesh) and they proved that surgical and cloth masks have no effect. Similarly, N95 masks do not work in practice either. The FAA rules basically require you to wear these masks on planes, mandating a medical intervention that is much more likely to make you sick and has no chance to protect you. See Incriminating Evidence for details.
- If you require PPE that might protect you from COVID, consider a 3M respirator with a P100 filter. Even better is to use a PAPR with your respirator (with a P100 or P3 filter). See this article on masks and respirators for details. These products that protect you do not protect others. The FAA will not allow these devices on a plane.
- Social distancing is not the right way to think about risk reduction. Think instead the 4 D’s: draft, distance, density, duration. Putting yourself in an unventilated small room at close distance to a source for a long duration will maximize your exposure. The 6 foot rule for standing in line is nonsensical since as soon as you enter the airspace of the person in front of you, you will be breathing the virus from people who were standing in that spot hours (to days) ago (depending on the ventilation in the area). There is absolutely nothing magical about 6 feet.
- Mitigation strategies such as testing, masking, isolation, and vaccination are largely ineffective. See this article for a convincing example.
- The best way to treat COVID is to do the opposite of what the CDC and FDA advises. So when they tell you to mask up, get boosted, avoid all repurposed drugs and supplements (including ivermectin, HCQ, fluvoxamine, vitamin D, zinc, aspirin, budesonide, etc), take paxlovid, molnupiravir, and remdesivir, you know what to do.
- There is only significant spread if you have symptoms. For example, in a study in China, they looked at 1,174 close contacts of these asymptomatic individuals and could not find ONE CASE of a person getting COVID from the asymptomatic people. Therefore, testing asymptomatic people is unnecessary because it is a lot of effort for near 0 gain.
- Omicron is very mild compared to Delta. After you recover from an Omicron infection, data shows you will be protected from Delta as well.
- As of December 3, 2021, Omicron had spread to 38 countries, but the WHO couldn’t find anyone who died from Omicron. How is this a national emergency?
- People who get the virus and recover are always better off than a vaccinated patient. Unlike vaccinated people, if a naturally infected patient is ever re-infected, they cannot transmit the virus to others (as far as we know so far).
- Censorship of COVID advice by social media (in particular the hazards of the vaccines and the effectiveness of early treatment protocols) has cost hundreds of thousands of lives.
- None of the health authorities issuing mandates and directives are willing to participate in a recorded scientific discussion with the so-called “misinformation spreaders” such as Robert Malone, Peter McCullough, Robert Kennedy, … Our authorities are afraid of the truth.
- The CDC, FDA, and NIH are all corrupt agencies that have looked the other way at safety signals. There are over 1M adverse events in VAERS and these represent over 40M adverse events in the real world. This is unprecedented, yet the CDC isn’t able to find a safety signal other than a “slightly elevated” risk of myocarditis. Attempts to bring the VAERS data to their attention is futile. They won’t even do a proper calculation of the underreporting factor which is required to do a proper risk-benefit analysis. They ignore the DMED data entirely.
Compare my fact-based COVID-19 hub to Spotify’s and let me know which one you like better.
EU Wants To Keep Vaccine Passports In Place For Another ENTIRE YEAR
By Steve Watson | Summit News | February 4, 2022
The unelected bureaucrat governors of the EU in the European Commission have proposed keeping the bloc’s COVID vaccine passport system in place for another entire year, despite the fact that many member countries are ramping down restrictions.
In a notice on its website, the Commission states “Today the European Commission is proposing to extend the EU Digital COVID Certificate by a year, until 30 June 2023.”
It continues, “The COVID-19 virus continues to be prevalent in Europe and at this stage it is not possible to determine the impact of a possible increase in infections in the second half of 2022 or of the emergence of new variants.”
“Extending the Regulation will ensure that travellers can continue using their EU Digital COVID Certificate when travelling in the EU where Member States maintain certain public health measures,” the statements adds.
It continues, “The Commission is adopting the proposal today to make sure the European Parliament and the Council can conclude the legislative procedure in time before the current Regulation expires.”
The move comes even as several countries, including Denmark, Norway, Italy, Sweden, France, in addition to non-EU countries such as Switzerland and England move to scrap restrictions including the vaccine passes.
The European Commission admits in its statement that it is up to the individual countries whether they carry on using the EU COVID vaccine passport scheme.
“The domestic use of EU Digital COVID Certificates remains a matter for Member States to decide, the statement notes, adding “The EU legislation on the EU Digital COVID Certificate neither prescribes nor prohibits the domestic use of EU Digital COVID Certificate (such as for access to events or restaurants).”
It also notes that “At the same time, where a Member State establishes a system of COVID-19 certificate for domestic purposes, it should continue to ensure that the EU Digital COVID Certificate is also fully accepted for those purposes. Beyond that, the Commission also encourages Member States to align their domestic validity periods with the validity period set at EU level for the purpose of travel.”
As we reported in November, despite vaccine passport schemes and high vaccination rates in many of the countries affected, COVID cases across Europe continued to surge as winter kicked in.
In addition, a recent investigation by experts in Spain concluded that vaccine passports have no significant impact on reducing COVID-19 infection rates.
The findings are similar to evidence found by the UK government that vaccine passports could actually increase Covid rates in the country.
The Spanish study noted that the only positives of such a scheme are that it “warns people that there is still danger from the pandemic and encourages vaccination uptake among the reticent.”
In other words, although vaccine passports have no discernible impact on their stated goal – reducing the spread of COVID-19 – they do succeed in keeping people fearful and compliant.
That conclusion dovetails with a recent admission by French Minister of Health Olivier Véran that the vaccine passports are “a disguised form of vaccination obligation,” but are “more effective.”
Since when was heart trouble ‘non-serious’?
By Guy Hatchard | TCW Defending Freedom | February 4, 2022
New Zealand – The Medsafe report Adverse events following immunisation with COVID-19 vaccines: Safety Report #39 – 31 December 2021 lists 46,000 adverse events reported since the start of the Pfizer vaccine rollout in New Zealand. Historically this is 30 times the rate of adverse effects reported for flu vaccines. More than 50 per cent of these adverse effects are reported by medical professionals and about 40 per cent by affected members of the public via the CARM (Centre for Adverse Reactions Monitoring) website. Prior experience published by Medsafe concludes that only 5 per cent of adverse events are reported to CARM. A total of 8.1million doses have been administered in NZ.
The ten most common adverse events
Some 44,000 of the 46,000 adverse events are dismissed by Medsafe as ‘non-serious’—a number which has been echoed by politicians across the NZ political spectrum and by our Ministry of Health as evidence that the Pfizer vaccine is safe. The ten most common adverse events (all rated as non-serious) are as follows (from Medsafe). The total number of events below is more than 44,000 because many people experienced multiple symptoms.
The Mayo Clinic in USA reported before the pandemic that the risk of developing myocarditis is rare and lists the following concerning symptoms of myocarditis:
Mayo Clinic—Myocarditis Symptoms
If you’re in the early stages of myocarditis, you might have mild symptoms such as chest pain, rapid or irregular heartbeats, or shortness of breath. Some people with early-stage myocarditis don’t have any symptoms. The signs and symptoms of myocarditis vary, depending on the cause of the disease. Common myocarditis signs and symptoms include:
• Chest pain
• Rapid or irregular heartbeat (arrhythmias)
• Shortness of breath, at rest or during activity
• Fluid buildup with swelling of the legs, ankles and feet
• Fatigue
• Other signs and symptoms of a viral infection such as a headache, body aches, joint pain, fever, child dizziness, a sore throat or diarrhea
Sometimes, myocarditis symptoms may be similar to a heart attack. If you are having unexplained chest pain and shortness of breath, seek emergency medical help.
Of the ten most common adverse effects of Covid-19 vaccination reported to CARM in NZ, you can see eight are listed as symptoms of myocarditis by the Mayo Clinic. Given that myocarditis is the most common known severe outcome of Covid-19, why have the eight common vaccine adverse effects also known to be symptoms of myocarditis been characterised as ‘non-serious’? Is this a glaring case of misdiagnosis? If so, why?
NZ GPs and medical personnel had a naive expectation of vaccine safety
The first point to note is that most NZ medical professionals had expectations of vaccine safety based both on years of experience with vaccination programmes and the extensive medical education they had received. They had no prior experience with drugs or vaccines which had not already completed years of testing and safety evaluation. It was for them therefore virtually unthinkablethat the Pfizer vaccine was unsafe. Moreover the Pfizer vaccine trial results had already characterised the common adverse effects as non-serious. For this reason the very common reports of chest discomfort and shortness of breathfollowing Covid-19 vaccination, which according to prior protocols should have led to intensive investigation and treatment, were dismissed as non-serious without investigation and in most cases without reporting to CARM. Perhaps their very common occurrence fostered an attitude of indifference and dismissal which many victims suffered in NZ when they reported such symptoms to their GP or to hospital staff.
Rates of Myocarditis symptoms are higher than realised
The prevalence of a wide range of known myocarditis symptoms is probably indicative of a very high rate of subclinical and mild myocarditis following Pfizer vaccination. The important point to note is that the recommended treatment for mild myocarditis is rest. Most people recover if it is treated early with sufficient prolonged rest. If left untreated, myocarditis can restrict the capacity of the heart to pump blood which can lead to serious cardiac events such as heart attack, stroke, and arrhythmia. It is wrong to undertake vigorous physical activity including sport while suffering from myocarditis. It is clear from this that insufficient precautionary instructions were given to vaccine recipients about the risks they faced and the steps that they needed to take to avoid these risks. This may have contributed to cardiac problems including among some recipients undertaking vigorous physical exercise.
The possible extent of these cardiac events is indicated by multiple reports to voluntary organisations. An important point to note here is that reporting to CARM is not mandatory, a very unfortunate yet unforgivably deliberate omission. Medsafe attempts in its Safety Report #39 (referenced above) to dismiss the significance of adverse events by comparing their rate to population norms. In the absence of mandatory reporting, especially considering that Medsafe knows adverse events are grossly under-reported, all such comparisons are statistically meaningless.
A public information campaign is essential
Belatedly Dr Ashley Bloomfield, Director General of the Ministry of the Health, struck a note of alarm about myocarditis in his December 15 2021 letter to directors of district health boards, but this concern did not alter much the processes being applied. Individuals experiencing myocarditis following their first vaccination are still being denied exemptions. Those suffering strokes and heart attacks are in some if not most cases being denied Accident Compensation Commission (ACC) assistance. There is also a virtual data black-out on rates of cardiac events and hospitalisations and on ACC claims. Anecdotal and whistleblower reports here and overseas suggest these might be high but considering that data collection has been haphazard due to the ‘non-serious’ label, these might be hard to quantify unless the government makes an honest attempt to inform the public of risks and ask people to come forward who are already affected. This is particularly important as many stroke, cardiac and other serious adverse event sufferers have already been emphatically informed by their GP or other medical professionals that their symptoms must be unrelated to the Pfizer vaccination – an egregious form of victim-blaming lacking any scientific basis.
For more information: HatchardReport.com
Stop ‘harmful’ mass testing of children now, demand MPs
TCW Defending Freedom – February 4, 2022
THE cross-party Pandemic Response and Recovery All-Party Parliamentary Group of MPs met this week to hear whether there is a case for the continued mass testing of healthy children by schools and nurseries.
The committee is co-chaired by Conservative MP Esther McVey and Labour MP Graham Stringer. The group examined the pros and cons of testing in schools, and growing concerns about the likely physical and mental health harms caused by constant testing. Their uncompromising conclusion was that the mass testing of healthy children is ‘harmful, invasive and unevidenced’.
Ms McVey told the group something few of the public outside parents are aware of, which is that children are still routinely being asked to take tests, even at primary school, regardless of whether they have symptoms.
Though the threat of school closures has been lifted and the requirement for children to wear masks rescinded, hundreds of thousands of children are still missing schooling, she said, owing to constant testing and the government requirement for healthy children to isolate.
She informed the group that the evidence presented by their experts found no benefits to mass testing and that the children are not drivers of transmission. They have been disrupted, harmed and distressed despite the absence of any robust randomised control trial evidence of the benefits of mass testing them: ‘The evidence we have heard is clear. Testing in schools must stop, especially in the absence of any sort of study on the impact it has on our children’s physical and mental health. Evidence sessions such as this one are so important, to allow us to get a full picture before we make a decision and put our case to the Government.’
Mr Stringer said: ‘We cannot continue to force such an invasive procedure and we have heard today of children as young as two being physically restrained by their parents, put in headlocks or vomiting after the tests. As I have said before, the evidence to impose these sorts of measures must be overwhelming and I’m not aware the evidence exists that testing healthy children is beneficial and will help stop the spread of SAR-CoV-2. Not to mention the eye-watering sums spent on testing which could have been so much better spent on redressing some of the damage already caused to child mental health. Surely the time has come to stop the mass testing of healthy children?’
The group heard from Dr Angela E Raffle, honorary senior lecturer, University of Bristol Medical School Department of Population Health Sciences, Dr Allyson Pollock, clinical professor of public health at the University of Newcastle, child and adolescent clinical psychologist Dr Zenobia Storah, Professor Ellen Townsend, professor of psychology at the University of Nottingham and Mark Ward, a parent who spoke about the traumatic experiences of testing his toddler.
They all argued against the mass testing of healthy children in schools, highlighting the insufficient scientific and clinical evidence and arguing that, far from being of any public health benefit, mass testing causes significant damage to children.
Dr Raffle said: ‘SARS-CoV-2 testing of healthy school children needs to stop. The World Health Organisation cautions against mass symptomless testing because of high costs, lack of evidence on impact, and risk of diverting resources from more important activities. There is no sound evidence that testing children leads to reduction in serious cases of Covid-19. The policy decision in England to introduce school testing appears to have been a political decision, to create the impression of safety, rather than investing in staffing and ventilation which would have made an impact. The tests being used have not been properly evaluated as self-tests or for use in children. Children are low transmitters compared with adults. The net effect of the school testing is harmful because of the trauma of repeated testing and the disruption to children’s lives through repeated exclusion and isolation. Testing is important when done under medical supervision in order to guide decisions about the best way to treat a child who is ill, but the indiscriminate use of tests in children who are well is unjustified.’
Professor Pollock said: ‘Many of the so-called public health measures applied over the last two years have been no more than blanket measures applied with no evidence but with serious consequences, such as mass testing healthy school children. The tests are inappropriate and in the UK we completely ignored the Wilson and Junger 1968 principles of screening. They are not tests of infectiousness so children were and are being isolated unnecessarily. We know from studies that infected children do not spread the virus to others readily, not other children, their families nor their teachers. Now with the milder Omicron variant, many of them will be asymptomatic, so constantly mass testing healthy children is not only a traumatic experience but an appalling waste of time and is something that should only be done if clinically necessary, such as if a child is ill enough to need medical attention.’
Dr Storah described mass testing of healthy children as ‘harmful, invasive and unevidenced’ and ‘nothing short of state-sponsored child abuse’. She said: ‘I have been working with young people throughout the last two years and have seen a steep rise in mental health conditions as a result of measures like testing. These obsessive infection control measures are causing worrying levels of highly anxious behaviour. They maintain and amplify the fear messaging, further exacerbated when children are surrounded by adults, their parents or teachers, also constantly testing. It is utterly extraordinary for a society to treat their young in such an abusive way, to throw decades of understanding about normal child development out of the window without having considered the risk factors. One in six young people now meets the diagnostic criteria for at least one mental health disorder but there is still time to lessen and even reverse the long-term psychological impact this is having on our children. Children and adolescents need to be prioritised and mass testing, like face coverings, must be consigned to the policy bin, once and for all. What is required immediately is a return to normality for all children and all school and extra-curricular environments.’
Professor of Psychology Ellen Townsend told the group: ‘It is unclear what mass testing healthy children is achieving from a Public Health perspective. No studies have been carried out to understand if there are any benefits and no evaluation has been done on the psychological impact of testing – this is a grave and unethical oversight. We must recognise that children are at minimal risk to others but the harms caused to children, the disruption of testing protocols in schools and the resulting absences, are completely disproportionate to the proclaimed benefits of indiscriminate mass testing. The president of the Royal College of Paediatrics and Child Health was quite correct when she said last year that testing in schools was causing unnecessary chaos.’
You can find information about the APPG and its membership here and here.
No question the vaccines increase your susceptibility to COVID. What else do they do?
By Meryl Nass, MD | February 3, 2022

https://www.publichealthscotland.scot/media/11404/22-02-02-covid19-winter_publication_report.pdf
If you live in Scotland, a small country, the government, with its NHS, is like Santa: it knows if you’ve been bad or good. Scotland has 5.5 million residents. Over 5 million of them are listed in Scotland’s report of cases, above. The rest are kids too young for the vaccine. Sadly for Scots, 80% went along with the jab. It didn’t help them. And you can’t dispute these numbers: look at the narrow confidence intervals.
So now we know the jabbed get more COVID. What we suspect is that they also get more heart attacks, strokes, blood clots, autoimmune diseases and myocarditis. Will Scotland release those data, ever?
Different vaccines reveal different side effects
MHRA should release the raw data for public scrutiny
Health Advisory & Recovery Team | February 1, 2022
The MHRA Yellow Card reporting system is designed to provide a signal of possible problems with new drugs based on reports of suspected adverse reactions from qualified medical practitioners. The data collected could be of much more value if more details were published. The MHRA shares such information with the pharmaceutical industry but, despite its role being to protect the public and relying on public funding, this data is not put into the public domain.
To make the most of what information is available the reports on different vaccine types can be compared. Any side effects that are a result of the production of the spike protein itself may be similar between all vaccine types. However, if one vaccine type has a much higher rate of a particular adverse effect than other vaccine types then this is suggestive of a genuine causal relationship. Confounders such as age may account for part of these differences, which is why publishing the raw data is so important.
Data sharing
The Yellow Card scheme is administered by the MHRA, a government body funded, at least in part, by the public. The data for the scheme is collected largely by NHS staff, who are again funded by the public. However, despite public finance being crucial to the generation of Yellow Card data, the MHRA have refused to release the anonymised individual patient data from this scheme for independent analysis (FOI 21/640). The MHRA argue that release of these data would be too onerous, yet paradoxically these same data are passed on to the vaccine manufacturers for analysis as a matter of routine (FOI 21/942). All that the public can access from Yellow Card is a rudimentary summary of the total numbers of adverse events recorded for each vaccine type in particular medical categories.
The MHRA’s attitude to data sharing stands in stark contrast to the situation in the USA, where the VAERS reporting system [2] provides anonymised individual patient data, and the detailed analyses that this allows has been crucial for recognising important safety signals [3] — albeit US Regulators have been slow off the mark in making full use of the data available to them. We note that the MHRA’s refusal to share the information that they hold within the Yellow Card database would not be tolerated in the general science community where access to raw data is now a prerequisite for publication in peer reviewed journals.
Despite the intransigence of the MHRA over the issue of releasing raw data from the Yellow Card scheme to the general public, it is incumbent upon the scientific community to make the maximum use of the data released from the scheme to scrutinise the validity of the conclusions that the MHRA reach in their weekly reports. This is particularly important to achieve because, despite FOI requests to see the scientific analyses on which their conclusions are based, the MHRA have been unable to produce any such reports (FOI 21/942).
Comparing frequency of reports by vaccine type
The weekly data released from the Yellow Card scheme takes the form of the total number of doses of each of the vaccines given, the total number of reports filed for each vaccine type, and the total number of adverse reactions recorded for each of a huge range of medical conditions compiled separately for each of the vaccine types. What insights can we gain from analysis of this information?
A simple question that we can ask is whether the different vaccines elicit the same or different rates of reporting of adverse reactions or number of reactions per report. The answer is clear (Table 1). There is something about a Moderna injection that generates a higher frequency of adverse event reports with less reactions per report than an Astrazeneca vaccination, which in turn generates a higher frequency of reports and more reactions per report than a Pfizer injection. The figures involved are so huge that these differences cannot be due to chance. There is something important happening that needs to be explained.

Table 1. Percentage of vaccinations resulting in a Yellow card report, and mean number of adverse events per report for three covid-19 vaccines administered in the UK
Risk of misinterpretation
Unfortunately, however, our interpretation can never be secure. The results we see could be due to the vaccines themselves. Alternatively, they could also be due to some confounding factor like the differences in age profile of the patients who were injected with different vaccine types, or to certain vaccine types being injected predominantly as boosters, or some combination of such factors. Yet distinguishing between alternative explanations is vital. If the effects we see are indeed due predominantly to vaccine type, this would have serious implications for vaccination policy and optimum choice of vaccine for minimising adverse reactions. However, analysis of confounding effects can only be achieved if the raw, anonymised individual patient data from the Yellow Card scheme are released by MHRA.
Comparing type of report by vaccine type
The second type of question that we can address using the Yellow Card data is whether choice of vaccines affects the spectrum of medical conditions recorded as adverse reactions. To answer this question, we can first sum up the number of adverse events elicited by each vaccine under the broad headings Blood & Vascular, Cardiac, Immune, Reproductive & Breast, Respiratory, Skin, Nervous System, Eye, Muscle and Other. A simple test for heterogeneity indicates that the relative frequency with which these classes of adverse reactions occur is highly dependent on the type of vaccine administered (χ2(18) = 29508, P<<0.001). Figure 1 illustrates the percentage by which the observed numbers of adverse reactions differ from the number expected if all vaccines elicited the same spectrum of adverse reactions. It is clear from the figure that departures from expectations are particularly large in the categories Blood & Vascular, Cardiac, Reproductive & Breast, and Skin; the different vaccines are eliciting quite different relative frequencies of adverse reaction in these categories.
For the categories Blood & Vascular, Cardiac, and to a lesser extent Immune and Reproductive & Breast, much higher than expected numbers of adverse reactions are elicited when the mRNA vaccines are administered, and lower than expected numbers of adverse reactions are found when the virus vectored Astrazeneca vaccine is used. Given that the same spike protein is encoded in the mRNA and virus vectored vaccines, this suggests that differences in the observed spectra of adverse reactions may be related to the mode of delivery of the spike encoding nucleic acid sequence in the vaccine. This observation for the Cardiac category is in agreement with a recent case series analysis which found that the risk of myocarditis is greater following sequential doses of mRNA vaccine than sequential doses of the adenovirus vaccine [4]. The role of the mRNA vaccine delivery system itself in eliciting adverse reactions must therefore come under scrutiny.

Figure 1. Percentage deviation of observed number of adverse reactions from the number expected if the spectrum of adverse events was the same for all vaccines. Data from nine different categories of adverse events are shown
While this example shows that the Yellow Card data may be helpful for generating ideas and supporting other studies, the inadequacy of the partial information currently released by the MHRA means that our interpretation of such data will always be compromised. Again, we do not possess the means to control for possible confounding factors (age and sex of individual, vaccine dose number etc.) that could contribute to the results observed. Nevertheless, in this example, the sheer size of the apparent effects of vaccine type on the spectrum of adverse effects indicates that a thorough investigation is essential. If the vaccine effect were confirmed, this would have serious real-world implications for the Covid-19 vaccination programme and the safety and health of the UK population.
Conclusion
The data we need to carry out the necessary analysis to maximise the usefulness of the Yellow Card scheme has already been collected at the public expense and is currently held by the MHRA. We call upon the MHRA immediately to release the raw, anonymised, individual patient data from the Yellow Card reporting scheme to enable rigorous scrutiny of Covid-19 vaccine adverse events by doctors, researchers and the public. This echoes the recent call by BMJ editors for immediate release of raw data from trials conducted by vaccine manufacturers [5].
2. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vaers/index.html
3. https://jessicar.substack.com/p/a-report-on-myocarditis-adverse-events
4. https://www.medrxiv.org/content/10.1101/2021.12.23.21268276v1
5. Doshi P, Godlee F, Abbasi K. Covid-19 vaccines and treatments: we must have raw data, now BMJ 2022; 376 Covid-19 vaccines and treatments: we must have raw data, now | The BMJ
Am I immune to Omicron if I have already become infected with the Delta variant?
Q&A #12 with Geert Vanden Bossche | February 3, 2022
Question
“Those who became infected with the Delta variant are therefore not immune to the Omicron,” says Frank Vandenbroucke, Minister of Public Health Belgium. Is this correct? Will my T cells then not recognize the coronavirus? Or will my antibodies not protect me? Or maybe I will be infected asymptomatically and thus not get sick and then this is equivalent to “after vaccination”?
Answer
When you get infected with another variant there is always a chance that you will get sick. However, if you are in good health, the chance that SARS-CoV-2 will make you seriously ill is negligible. We owe this to our innate immunity which – especially in young people – is the first line of defense to clean up and eliminate large amounts of the virus (vacuum cleaner!). Young people, but even all healthy people who are in excellent health (e.g. no excess weight and regular exercise / sport), will often not even get sick or at best develop some vague, mild symptoms. If the first line of defense is broken, then our acquired immune system rushes to the rescue whereby our T cells ensure that the sick, virus-infected cells are eliminated. This allows us to recover from illness.
But whenever our innate immune system is exposed and eliminates the virus (with or without the help of the acquired immune system) it also immediately learns to recognize the virus better in the future. While it continues to recognize all SARS-CoV-2 variants (and even all CoVs), it now does so with more efficiency/affinity. This phenomenon is called “training” of the innate immune system. It is a form of adaptive immunity caused by epigenetic changes that effect a reprogramming of immune cells that secrete innate antibodies. That is, with subsequent exposure to the virus, there is an increasing chance that that person will develop an asymptomatic infection and actually not get sick at all, even if the virus undergoes antigenic drift (antigenic drift). If the virus undergoes an antigenic shift (i.e., severe change due to multiple mutations as in the case of Omicron), then the innate immunity will have to train again for a while before being able to withstand an infection with such a variant without giving rise to illness.
A pandemic is of course an excellent opportunity to train the innate immune system against SARS-CoV-2. However, it also means that if a variant with an antigenic shift (e.g. Omicron) dominates, more people may become ill anyway and within a short period of time the virus will be under pressure due to the induced natural antibodies, which are not able to suppress the virus at high infection pressure. Reducing the infection pressure is possible via (one-time) antiviral chemoprophylaxis. On the contrary, continued vaccination will increase the immune pressure and ensure that the vicious circle of the pandemic is maintained.
Thus, trained innate immunity to SARS-CoV-2 is not equivalent to COVID-19 vaccination but is superior because
- It is effective against all variants
- It has a sterilizing effect in contrast to vaccine antibodies
- Because of its non-varying character it does not lead to the selection of more infectious or resistant variants.
In other words, it benefits both individual and public health. It is the only way to acquire group immunity (independent of the circulating SARS-CoV-2 variant) and thus to move the pandemic into the endemic phase.
Former Pfizer VP Michael Yeadon demands apology from media over ‘lies’ asserting vaccine safety

Dr Michael Yeadon, former Pfizer vice president and co-founder of Doctors for COVID-19 Ethics
By Patrick Delaney | LifeSiteNews | February 2, 2022
After being excoriated by mainstream media outlets regarding his concern that COVID-19 gene-based vaccines could cause fertility issues in young women, Dr. Michael Yeadon is now requesting contrition on the part of media outlets as leaked data from the U.S. military indicates heavy spikes in these tragic outcomes.
“I’m not vindictive, but I want some humility and contrition from the BBC and all other media outlets that lied to their audiences,” said the former Pfizer vice president and Chief Scientist for allergy and respiratory.
Yeadon, who spent 32 years in the industry leading new medicines research and retired from the pharmaceutical giant with the most senior research position in his field, was an author of a submitted petition to the European Medicines Agency (EMA) in December 2020 that raised substantial concerns regarding a lack of sufficient testing of the experimental COVID-19 gene-based vaccines, prior to their emergency use authorizations.
With regard to the possibility of the shots endangering the fertility of women, Yeadon and his colleague, Dr. Wolfgang Wodarg, wrote, “There is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would then also prevent the formation of a placenta which would result in vaccinated women essentially becoming infertile.”
Such a possibility would need to be ruled out through standard experimentation prior to imposing such substances onto the entire population, according to the doctors.
“It’s important to note that none of these gene-based agents had completed what’s called ‘reproductive toxicology,’” Yeadon wrote in his recent statement. “Over a year later, this battery of tests in animals still has not been done. So there was and still is no data package supporting safety in pregnancy or prior to conception.”
Media response to valid concerns: attacks, smears, vilifications
“As a society, we’ve practiced the precautionary principle most assiduously in relation to conception and pregnancy ever since the tragedy of thalidomide, over 60 years ago. So we had hoped that some at least in the media would take this [concern] with the seriousness it deserved,” he wrote.
“Did that happen? No. Instead, we were attacked, smeared and vilified in every medium, from Twitter to the BBC,” the British national wrote. “[M]ajor broadcasters actively lied to the public, explicitly stating that these agents were completely safe in pregnancy.”
Indeed, Reuters excoriated the doctors for making their inquiry “without providing evidence, that the vaccines could cause infertility in women,” shifting the burden of proof onto the petitioners from the regulators whose job it is to ensure proper safety trials are completed before the release of such drugs.
The article quoted an anonymous spokesman for Britain’s Department of Health & Social Care, saying, “These claims are false, dangerous and deeply irresponsible.”
Reuters later attempted to “fact-check” Yeadon as well over several concerns including the danger to fertility, to which he simply reiterated common ethical principles with regard to human experimentation: “No one in their right mind thinks giving experimental treatments to pregnant women is other than reckless. Especially when reproductive toxicity testing is incomplete.”
Of special note for Yeadon was BBC Radio talk show hostess Emma Barnett, who “directly attacked me by name on air in the most unpleasant terms,” which also led to his charging the program with slander. In response, after a bit of investigation, the program editor conceded, apologized to Yeadon, and cut their false representation of the former Pfizer scientist from their recorded podcast.
“[Barnett] also had her guest, who was from the Royal College of Obstetrics and Gynecology, repeat the lies that it was perfectly safe for young women to be injected,” Yeadon called out in his statement.
Preprint paper reveals placental-damaging antibodies increased 2.5 fold after shots
Also of note for the former executive was a preprint study published last May that appeared to attempt a rebuttal of his concern that anti-Syncytin-1 antibodies could be developed due to the shots, but instead reinforced them showing a 2.5 fold increase of the placental-damaging antibodies in days 1 to 4 after COVID-19 gene-therapy injections.
The paper, which claimed a conflict of interest in being funded by Johnson & Johnson, went on to explain that though they had observed this major increase, they did not examine its “clinical significance,” thus admitting they didn’t know if these higher levels of the antibody flagged an actual safety problem with regards to fertility and miscarriage.
At the same time, the study’s authors acknowledged data showing “spontaneous miscarriage as the most common obstetric outcome after COVID-19 mRNA vaccination.”
Based on the outcome of this study alone, Yeadon said “all of these experimental products as a class should have been completely contraindicated in women younger than menopause.”
Pfizer & Moderna ‘definitely knew’ these mRNA products would ‘accumulate in the ovaries’
An additional source of concern regarding fertility was that “the mRNA products (Pfizer and Moderna) would accumulate in ovaries,” the British national explained.
“An FOI request to the Japanese Medicines Agency revealed that product accumulation in ovaries occurred in experiments in rodents. I searched the literature based on these specific concerns and found a 2012 review [here], explicitly drawing attention to the evidence that the lipid nanoparticle formulations as a class do, in fact, accumulate in ovaries and may represent an unappreciated reproductive risk to humans. This was ‘a well-known problem’ to experts in that field,” Yeadon explained.
“I’ll say that again. The pharmaceutical industry definitely knew, in 2012, that formulating these agents in lipid nanoparticles would lead them to accumulate in the ovaries of women to whom these were given.
“No one in the industry or in leading media could claim ‘they didn’t know about these risks to successful pregnancy,’” he emphasized.
Results from the U.S. military leak confirm damage done to unborn children and fertility
“So it’s with tremendous anger and sorrow that I heard of military physicians blowing the whistle about the evidence of harms in pregnancy that their proprietary safety monitoring database had thrown out,” Yeadon said, referring to last week’s revelations during a U.S. Senate panel discussion.
“In the intervening months since journalists (including but definitely not limited to Emma Barnett) chose to downplay or downright lie about our concerns, we learned that women in the U.S. military were experiencing 3X normal rates of miscarriage,” he explained.
In fact, these data leaks, given by three “decorated high-ranking soldiers who are doctors and public health officials,” in sworn declarations under penalty of perjury, show several increases in negative impacts upon fertility, including spontaneous abortion, among this military population where enforcement of an experimental COVID gene-vaccine mandate is strictly observed.
As presented by these soldiers, the following 2021 increases only include the first 10 months of the year (January through October) and are compared with the full five-year average of figures taken from 2016 through 2020.
- Miscarriages — increase of 279%
- Female infertility – increase of 471%
- Male infertility — increase of 344%
- Congenital malformations (birth defects) – increase of 156%
And considering most children conceived after these injections had not been born before November 2021, the final figure of birth defects is likely to significantly increase as well.
Journalists, regulators and manufacturers: ‘You are way out over thin ice and deep water’
After Yeadon’s request for contrition from the BBC and other media outlets, he went on to implore readers, “please do not get injected with these inherently dangerous and ineffective experimental products. Warn anyone you know about the risks to pregnancy, now confirmed by whistleblowers from physicians in the U.S. military.
“Please also tell them there are likely to be other reproductive health consequences, even in young girls, because of accumulation [of lipid nanoparticles] in their ovaries.“
Having originally alerted the EMA of several other possible toxic outcomes due to the injections, Yeadon highlighted that he and Dr. Wodarg were sadly also right about their warning of “allergic, potentially fatal reactions to the vaccination,” citing examples from the UK of emergency interventions and tragic deaths.
“Having had two of two serious harms we warned about, prior to regulatory authorisations, come to pass,” he said. “I humbly recommend that governments and journalists everywhere recognise what you’ve done and lobby for or directly decide to immediately and completely withdraw all these experimental products from the market, before some of the other specified concerns (or issues we didn’t think of) show up in the safety monitoring systems.”
“Journalists, regulators, healthcare professionals and politicians, as well [as], of course, the manufacturers, you are way out over thin ice and deep water. I don’t know how you’re planning to get out from under this before the wider public more fully appreciates what you’ve done,” Yeadon wrote.
“One possibility is that you won’t be able to hide your complicity in the massed harms you’ve done to millions of people. In this case, I look forward to giving evidence against you in a court of law,” he concluded.
Dr. Yeadon’s full statement can be accessed here.
These 5 Studies Reveal a Disturbing Trend — Researchers Presenting Conclusions That Don’t Match the Data
By Josh Mitteldorf, Ph.D. and Madhava Setty, M.D. | The Defender | February 2, 2022
It was January 2020, the very beginning of COVID, when news articles began appearing that connected the genetics of the virus with gain-of-function research on bat coronaviruses at the Wuhan Institute of Virology.
These speculations were put to rest by an authoritative statement in the prestigious journal Nature Medicine, echoed by a summary in Science and an unusual affidavit in the Lancet signed by an impressive list of prominent scientists.
The message in the Nature Medicine article was dispositive: “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.”
But where was the support for this confident conclusion in the article itself?
The 2,200-word article in Nature Medicine (Anderson, et al) contained a lot of natural history and sociological speculation, but only one tepid argument against laboratory origin: that the virus’s spike protein was not a perfect fit to the human ACE-2 receptor.
The authors expressed confidence that any genetic engineers would certainly have computer-optimized the virus in this regard, and since the virus was not so optimized, it could not have come from a laboratory. That was the full content of their argument.
Most readers, even most scientists, take in the executive summary of an article and do not wade through the technical details. But for careful readers of the article, there was a stark disconnect between the Cliff Notes and the novel, between the article’s succinct (and specious) conclusion and its detailed scientific content.
This was the beginning of a new practice in the write-up of medical research. Recent revelations in the Fauci/Collins emails shed light on the origins of this tactic and the motives behind it.
In the past, if a company wanted, for example, to make a drug look more effective than it really was, it would choose a statistical technique that masked its downside, or it would tamper with the data.
What companies would not do, in the past, was describe the results of a statistical analysis that proves X is false, then publish it with an Abstract that claims X is true.
But this strange practice has become more common in the last two years. Academic papers are being published in which the abstract, the discussion section and even the title flatly contradict the content within.
Why is this happening? There are at least three possibilities:
- The authors cannot understand their own data.
- The authors are being impelled by the editorial staff to arrive at conclusions that match the ascendant narrative.
- The authors and editors realize the only way to get their results into publication is to avoid a censorship net that gets activated by any statement critical of vaccination efficacy or safety.
Before reaching any conclusions, let’s take a closer look at some examples of this troubling phenomenon arising in what should be the foundation of what is known: published scientific data.
In this article, we present five different published studies. Each to varying degrees exemplifies a disconnect between the data and the conclusions.
Example 1: ‘Phase I Study of High-Dose L-Methylfolate in updates Combination with Temozolomide and Bevacizumab in Recurrent IDH Wild-Type High-Grade Glioma’
This example is unrelated to the pandemic, but it typifies a common practice in the pharma-dominated world of medical research. If a remedy is cheap and out of patent, there is no one motivated to study its efficacy.
But research practice has gone well beyond neglect. In fact, investigators are skewing statistics to make cheap, effective treatments look ineffective if they are in competition with expensive pharma products.
This is ridiculously easy to do — all it requires is incompetence. Using the wrong statistical test, using a weak test when a stronger one applies — or just about any mistake in parsing the data — is far more likely to make compelling data appear random than the opposite.
Is it always incompetence? Or is it more often a well-thought-out deception that uses seemingly erudite analysis to lead the undiscerning reader into believing the wrong conclusion?
In the case of this article, a simple B vitamin (L-Methylfolate) was shown to double the life expectancy of 6 out of 14 brain cancer patients who received it, while showing no benefit (and no harm) to the other half of the patients.

The purple jagged line extending out to the right represents 40% of patients who lived dramatically longer when treated with L-Methylfolate (LMF).
The abstract reports that “LMF-treated patients had median overall survival of 9.5 months [95% confidence interval (CI), 9.1–35.4] comparable with bevacizumab historical control 8.6 months (95% CI, 6.8–10.8).”
The increase in median survival time is just a few months and not statistically significant. But the average survival time of the folate-treated group was more than double, and the difference was statistically significant (by my calculation, not in the article).
But the average is what is more commonly reported, and most readers don’t understand the difference between average and median.
The longest surviving patient on the B vitamin was still alive at the end of the study (3.5 years) when every one of the patients treated only with traditional chemo was dead before 1.5 years.
There were three different dosages in the study, (30, 60, 90 mg) and it was not reported whether the longest-living patients were receiving the highest dosages.
This is, in fact, a hugely promising pilot study about treating a common, fatal cancer with a simple vitamin. If it were an expensive chemotherapy drug instead of a cheap vitamin, you can be sure it would have been hailed as a breakthrough.
But this study will not create much excitement, and few oncologists will even know to prescribe methylfolate for their glioma patients.
Example 2: ‘Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons’
Earlier this year, MacLeod et al used data from a prominent Centers for Disease Control and Prevention (CDC) study to calculate that for women in their first trimester, the rate of miscarriage following administration of an mRNA COVID vaccine was an alarming 82%.
On Jan. 7, the CDC released a report designed to dispel our misgivings about vaccinating pregnant women. Its conclusions were unequivocal:
“These data support the safety of COVID-19 vaccination during pregnancy. CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant, who are trying to become pregnant now, or who might become pregnant in the future.”
The Defender reported on the numerous flaws in this study. The most egregious deficiency was the dearth of pregnant women in the study who were vaccinated early in their pregnancy (less than 2%).
The authors admit their study could not quantify the risk of vaccine exposure in the first trimester: “First trimester vaccinations are not included in analyses stratified by trimester because few exposures occurred…”
How then can they recommend COVID vaccination for women who are “recently pregnant” if their analyses excluded women in their first trimester?
This report serves a purpose. People who read it superficially will find the reported results reassuring — including front-line doctors who don’t have time to evaluate the research critically.
The CDC chose to paint over troubling safety concerns with reassuring words that are unsupported by clear science.
Example 3: ‘Public Health Scotland COVID-19 & Winter Statistical Report’
There is a section of this report comparing vaccinated and unvaccinated rates of disease, preceded by a warning to the reader not to take the data at face value.
“PLEASE READ BEFORE REVIEWING THE FOLLOWING TABLES AND FIGURES There is a large risk of misinterpretation of the data presented in this section due to the complexities of vaccination data …”
The data the authors don’t want us to misinterpret say that people who have been vaccinated with one shot or three shots are 50% more likely to contract COVID-19 compared to people who are unvaccinated.
People who receive two shots are more than twice as likely to contract COVID-19. This is according to the authors’ own method of calculating age-standardized disease rates.

The authors emphasize it’s not about case numbers — it’s about severe outcomes, hospitalizations and deaths:
“Evidence suggests the COVID-19 vaccines are 90% effective at preventing a severe outcome of COVID-19. COVID-19 hospitalizations and deaths are strongly driven by older age, with most deaths occurring in those over 70 years old and having multiple other illnesses. But overall, you are less likely to be hospitalized if you are vaccinated with a booster.”
What data are they talking about? Here are results from their own data table:
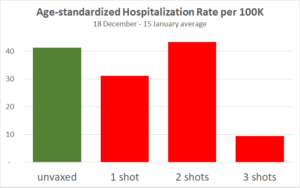
The only substantial reduction is from people who received the third shot, which has only recently been available in Scotland. But for the three-shot cohort only, vaccination effectiveness is declining over the four weeks.
This adds to previous evidence that protection from the vaccine is short-lived, and each injection provides a shorter window of protection than the previous one. Also, note the hospitalization statistics may have been gamed.
Since the publication of this article, England but not Scotland has backed off requirements for vaccination IDs.
Example 4: ‘Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults’
Myocarditis, or inflammation of the heart, is a severe and life-shortening disease. It is virtually unknown in young people, but it is a recognized side effect of the COVID vaccines, especially in boys and young men.
This article summarizes the experience of 139 young patients (ages 12 to 20) who were hospitalized for myocarditis following vaccination.
19% of them were taken into intensive care.
Two required infusions of pressors and inotropes (potent intravenous drugs used to raise critically low blood pressure).
Every patient had an elevated Troponin I level. Troponin is an enzyme specific to cardiac myocytes. Levels above 0.4 ng/ml are strongly suggestive of heart damage. These young patients had a median Troponin I level of 8.12 ng/ml — over 20 times greater than the levels found in people suffering heart attacks.
“Conclusions: Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms.”
“Mild clinical course” — We suppose this refers to the 81% who did not go to the ICU or the fact that none died or required ECMO (Extracorporeal Membrane Oxygenation, a desperate means to keep the body oxygenated when a patient’s heart or lungs have completely failed).
In any case, every single person in this study was hospitalized. When does a “mild clinical course” require hospitalization for a two-day median length of stay?
“Rapid resolution of symptoms” — How would anyone know this? Myocarditis in older patients doubles the probability of death for the long term.
We don’t know what it will do to young boys in the long term, especially since every patient had some damage to their heart as evidenced by significantly abnormal troponin levels. And we don’t fully understand the mechanism by which the vaccines cause myocarditis.
Example 5: ‘Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States’
This is the title of a paper by two statisticians from the Harvard School of Public Health, published on Sept. 30, 2021, in the European Journal of Epidemiology.
The title makes the important claim that there is no public health benefit from vaccination. COVID-19 is spreading at the same rate in different populations, unrelated to whether the population is mostly vaccinated or mostly unvaccinated.
It’s a powerful counterpoint to the ubiquitous demand that more people should undergo vaccination for the sake of their community.
The paper completely undermines the requirement of vaccination to attend meetings, concerts, theater and other public gatherings. It says there is no legitimacy to the creeping government vaccine mandates for travel.

But the data in the paper don’t show that vaccination and spread of COVID-19 are “unrelated.” In fact, there is a paradoxical relationship, an insidious relationship: The more vaccinated countries had more new COVID-19 cases (during the week when the survey was conducted). The correlation is significant (p=0.04).
Still, the authors conclude by explicitly recommending propagandizing of the unvaccinated: “In summary, even as efforts should be made to encourage populations to get vaccinated it should be done so with humility and respect.”
It may sometimes be wrong to promote flawed health policy, but apparently, it’s a good thing, so long as it is done with humility and respect.
Why would these researchers take the trouble to publish data that is so damning to the vaccine narrative, and then pull punches in the title and in the conclusions?
Are we to assume that these authors who have assiduously extracted data from 68 different countries and nearly 3,000 U.S. counties were unable to notice their meticulous scatter plot unequivocally demonstrates high vaccination uptake is associated with higher (NOT lower) prevalence of COVID-19?
This seems to be a different case from the first example, where shills for the pharmaceutical industry set out to create a deceptive narrative. We think it’s probable that in this case, soft-pedaling the implications of these glaring data may not have been the authors’ choice, but rather a decision by the journal’s editors.
We know from personal experience how difficult it is to get an article through peer review at most “reputable” medical journals when the results are out of sync with the COVID narrative.
It may well be that these authors fought hard to get their subversive message into print, and in order to get past peer review, they softened the language, especially, the title.
Conclusions
The church was once the most trusted institution in Europe. Then the bishops started selling indulgences — a kind of get-out-of-hell-free pass for rich sinners.
Today the most trusted institution is science.

Sources: Gallup, Gallup, Gallup, Pew
This is true despite the fact that scientists are human, subject to error and to corruption.
Medical journals have become financially dependent on their advertisers, which are almost exclusively the pharmaceutical giants.
For several decades now, the “Church of Science” has been selling indulgences. With enough money, you could buy a scientific study that says what you want it to say.
Darell Huff’s book, “How to Lie with Statistics,” first published in 1954, remains the all-time best-seller in its field.
Recently, Gerald Posner documented the way in which the pharmaceutical industry has used its profits to affect science at every level, from medical researchers to journal editors to government regulatory agencies to the journalists who interpret science for the public.
Pressure is being placed on independent researchers by the journal editors and peer reviewers, many of whom have ties to Big Pharma. Valid studies, honestly reported, can be rejected for publication if they send a message that threatens corporate profits.
In the age of COVID, we see three reasons that an article’s conclusions might become detached from its statistical findings:
- Scientists have suddenly abandoned basic logic and reason. This is an implausible explanation because, as has been demonstrated above, these examples demonstrate diligence in gathering data. There is no reason why they would abandon diligence in arriving at reasonable conclusions.
- Shortcuts by pharmaceutical companies and their shills in academia. Rigging clinical trials the old-fashioned way is expensive and time-consuming. It’s also uncertain. Sometimes the truth rears its head even if a study is designed to conceal it. Even a study that is designed to fail might succeed when the inconvenient truths are sufficiently stubborn. How much easier it is to report the results and then tack on an abstract and a discussion section that say what you want to say, regardless of the data tables in the body of the article!
- Scientist authors are well aware of the pernicious censorship in scientific publication that has emerged in recent days. This is perhaps the most intriguing possibility. If researchers behind the study have some prestige and some influence, they still may find they have to soften their rhetoric in order to pass peer review. However, what we are witnessing today is more than a tendency to be “diplomatic” in their choice of words. What does it mean when their conclusions do not match the findings? Are they trying to tell us that they are gagged? Are they silently screaming at us to look at the data and not their interpretation of them?
The Nature Medicine article on the origins of the SARS-CoV-2 virus (reviewed first) seems to be an example of researcher corruption.
The article in the European Journal of Epidemiology (Example 5), which relates vaccination rates to COVID prevalence, is more likely an example of corruption by journal editors and peer reviewers.
In this instance, the data and conclusions are so disparate that it begs us to reconsider the cynical position that all scientists have been corrupted. Is there a better way for conscientious scientists to signal their community that they are being censored than by compiling solid data that tell a compelling story and then arriving at a nonsensical conclusion? Are they imploring us to read between the lines?
For the other four articles reviewed above, we leave it to your judgment — how do you think the conclusions came to be so disconnected from the statistical findings in these same articles?
Obviously, this blatant distortion of scientific write-ups is not a long-range strategy, but the world is moving fast, and people who count on their ability to shape scientific conclusions to their financial interests will be successful for long enough to do a great deal of mischief.
What will be the damage to the credibility of science when the dust clears?
Josh Mitteldorf, Ph.D., has a background in theoretical physics. Since the 1990s, he is best known for his contributions to the biology of aging, including many articles and two books.
Madhava Setty, M.D. is senior science editor for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Featured Video
Israel and the Palestinians — It’s about Mind Over Matter
or go to
Aletho News Archives – Video-Images
Book Review
The Greatest Threat to World Peace? A Review of Daniele Ganser’s ‘USA: The Ruthless Empire’
Review by Marilyn Langlois | November 10, 2023
 If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you scoff at the notion that the US, a republic founded on principles of freedom and democracy, has morphed into a world empire, perpetrating assassinations, coups d’état, acts of terror and illegal warfare . . .
If you want to promote peace but haven’t yet explored deceptive events that precipitate US warmongering . . .
. . . here is a volume that will clear the air and paint an honest picture of the significant, not-so-rosy impact US foreign policy and actions have had in the world around us.
USA: The Ruthless Empire, by Swiss historian and peace researcher Daniele Ganser, is the newly published English language translation of his book Imperium USA, originally written in German and published in 2020. Here is a summary of key points — including some lesser-known ones — along with remedies for a more peaceful future, that are covered in the book. … continue
Blog Roll
 Aletho News
Aletho News- Talks would resume if US accepts 3-phase framework Iran put forward
- Israeli forces raid Syria’s Dara’a, Quneitra countryside, set up checkpoints
- IRGC says to reverse engineer 15 undetonated US missiles uncovered in southern Iran
- Liberation From War
- Major fire erupts at UK base used for US bombers
- What Is Asthma?
- When a Train Ticket Costs Your Passport: The Eurail Breach and the Digital ID Problem
- Seyed M. Marandi: The Strike That Wiped Out Trump’s Plan (It’s Over)
- Court Forces German Chancellor Merz to Open Files on 300 “Insult the Chancellor” Cases
- ‘Territorial Theft With Better Branding’: Israel Keeps Advancing Its ‘Yellow Line’ in Gaza
- If Americans Knew
- Six Months into Gaza Ceasefire, Setting the Record Straight About Aid
- ‘Silent suffering’: Why children in Gaza are losing their ability to speak
- In Gaza, 17,000 infections linked to rodents and external parasites – Daily Update
- Lobby group taking journalists on propaganda tours of Israel
- The Shattered Figure of Jesus Is Not an Exception. It’s a Pattern
- Israel’s idea of ceasefire includes killing 21 in one day – Daily Update
- Christians in Israel and Palestine, past and present
- Israel eager to restart Iran war, Gaza genocide – Daily Update
- Meet the Top “Content” Producers Linked to Canary Mission
- Lebanese Journalist Amal Khalil Bombed and Left to Die by Israel
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
