An Essential Journey
My experience of international travel in Covid times
By Joanna Sharp | OffGuardian | June 19, 2021
I had not planned to travel abroad this year, especially after the UK government’s announcement in early 2021 that foreign holidays were forbidden. Even heading towards the airport with an intent to go on a foreign holiday could result in a £5000 fine or imprisonment! Surreal.
Where we live in London under a flight path to Heathrow, we notice that although there are fewer flights, they have not ceased completely. So how do people travel? It’s not something I have thought about.
One day at the end of April I receive a message that my elderly father’s condition is critical. Within an hour I am looking at flights back home in Eastern Europe and checking the UK government travel ‘advice’ webpages.
I say ‘advice’ but that word belongs to the past. Today, ‘command’ might be more appropriate. According to the government, only “essential” international travel is permitted for named valid reasons; ‘medical and compassionate’ is the category which applies to me.
I wonder whose compassion this is a reference to: mine, for wanting to be with my sick father, or the government’s for including this as a possibility. Reassured that I can go, it is now a question of buying the plane tickets, checking in and packing, right? Not quite.

WADING THROUGH THE RED TAPE
Since holiday travel has effectively been banned, the government created intricate webpages full of information on what is and what is not allowed, where citizens cannot travel, and if they must, what documents they need to prepare. So complicated travel advice alone has become that the webpage now includes a step by step flowchart with endless links within each step to be followed.
Getting through this information would take at least a day. It’s like a cross between a maze and a vortex. I soon understand that I cannot buy my tickets until I have uploaded the right Covid related paperwork onto the airline website!
First, I need to fill a Declaration for International Travel (since the 17th May it is no longer required) which asks for personal details including my date of birth, passport number, home address and destination.
The key question is the reason for international travel – and in the actual online questions, the phrase is: ‘What is your excuse for travel?’ My excuse? What kind of language is that? Am I asking a teacher to let me leave the classroom? Am I asked to explain why I haven’t done my homework?
That really shocks me, although I have already noticed my own reaction to the very idea that I need permission to leave the country, as if I was back in Eastern Europe before 1989…I read the following declaration and tick the right box out of the given options.
I hereby declare that my reason for being outside my home to travel internationally is for:
– Work
– Volunteering
– Education
– Medical or compassionate reasons
– Funeral
– Ending a temporary visit (non-UK resident)
– Allowing access to parents with children who do not live in the same country
– Other reasonable excuse – please specify
Next, I am required to sign to ‘certify that the information I have provided is true. I understand that if I provide false or misleading information, I may be issued with a fixed penalty notice and/or a direction to return home or be arrested’.
So, by signing this, and I have no choice not to if I want to get my ticket, I have given the UK authorities permission to arrest of fine me should my excuse to travel turn out to be incorrect. What if my father is not that ill, then what?
But of course, that is not enough. I now need to provide evidence of my father’s illness. How do you do that when the whole of the world is still in lockdown; imagine having to get a doctor’s note on demand. I am still just trying to get a ticket.
I want to travel tomorrow morning, my sister-in-law tells me, Dad is given a couple of days. I ask my brother to send me an email confirming the family crisis, he does that within an hour. He is also trying to copy the notes from my father’s last doctor’s visit and the most recent diagnosis.
Then, still before I buy a return ticket, I need to get a kit of two Covid tests which I will need to take upon return to UK. Another link takes me on to a list of government-approved Covid test providers. A whole list of them, each can be accessed via a separate link. I try a few. They average around £200 each. The cheapest ones are £99 but are sold out.
Why can’t I see any free NHS ones? The ones given out like sweets in schools and local pharmacies? Why are these not available? Why could I not just pick a free one at the airport?
But of course, there is no to answer these questions, I am desperate to leave so agree to this, too. No test, no flight. So, I order one of these almost £200 test kits, get an email confirming the order, upload all the documents and finally I can complete the purchase of my tickets which, as usual, turn out not so low cost after all.
I check in. My boarding card (lucky I had just bought a printer the previous week) says at the top of the page ‘Covid Documentation Uploaded’. So, now I have the boarding card and a pile of printed pages which presumably I will need to show at UK border control in order to prove my excuse for leaving the country is legitimate.
Finally, I download and fill in the compulsory Passenger Locator Form for the destination country that will enable the system to track and trace me. It is nearly bedtime and I now need to pack.
ON THE GO
My husband drives me to Stansted in the middle of the night. An early morning flight, no public transport available but at least it’s quiet and there is no traffic. The airport is still closed; a group of families with young children are waiting for the door to open.
These are not holidaymakers breaking the law to get some forbidden fun. No idea where they are travelling but they look like they are going home somewhere south, southeast perhaps? Turkey, Bulgaria or Ukraine? No idea but they do look like part of the globalised chain of workforce escaping poverty and perhaps the lockdown has pushed them to return. Better to be jobless and poor in your own village. The weather tends to be better and the environment less hostile.
Finally, the doors open. I push the scarf up over my face, my hand clutching a plastic folder with a wad of documents allowing me to leave. It is quiet, no waiting. I go through security, passport control seems non-existent, shops still closed so nothing to stop for. I wonder at which point someone will ask me to see the papers. Ask me what my excuse for leaving is. Strangely, that never happens. I am almost disappointed. I spent about four hours sorting out all that paperwork the night before and now this is not even checked!
Immediately I catch myself: why am I disappointed? Because no one will give me the all-clear? Have I been conditioned to want to be waved through the green light already?
Perhaps that is how normalising oppression works. But of course, there is no need to check, the documents have been uploaded and recorded somewhere and someone now knows everything about me, my plans, my reason (“excuse”) for leaving the country. Or perhaps the intimate details of my family crisis; my father’s terminal illness and my attempt to get to him before it’s too late have now just been converted into big data slushing around the corpo-government’s control AI machine, and turned into useful predictions.
I guess this type of authoritarianism does not even need stern looks from border control officials, no need to divulge private dramas in public. Hours of stress of getting the documents turned into a discreet but vital small print on my boarding card; the only visible proof that my travel is acceptable to the corpo-state. It is all so neat, tidy, hi-tech and invisible that we can just pretend that all is just normal.
After all, the airport trimmings look all the same; with adverts, duty-free shopping, same old queues at departure gates and same safety drills on the plane, down to the irritating Ryanair voice thanking us for choosing to fly with them (no one chooses to fly with Ryanair, just like no one chooses to go to the dentist, you do it because you have to and you hope it won’t be too unpleasant).
We can pretend nothing has changed. Except the masks on faces, of course. Slow drinking and eating is my solution. During the flight many noses protrude against the regulations, of course. People do need to breathe.
We land on time. I send a message to my father, anxious, hoping he is still there. He is not responding. I am worried. From the tarmac I can see the arrivals hall is full. There is no way of entering so the crowd from my plane stops outside and waits in the drizzle. I wonder why that is. Is that Brexit or is it that people’s papers are now checked after all?
The queue moves very slowly, twenty minutes after landing I send my father another message saying that I’m still waiting for border control. I have no idea why this is so slow; each person seems to spend a good few minutes at the control desk. Finally, an hour and a half after landing I get into the taxi. As the driver pulls away, I notice a long queue of passengers outside the arrivals hall waiting to get a Covid test. I arrive home and find my father hanging on.
MY FATHER’S ILLNESS
There is a twist to this story. My father had been treated for cancer but has been still doing quite well and had been planning to spend the summer away from his flat, in the countryside. His sudden deterioration was unexpected for me but I have not had time to think of reasons. I only learnt of this yesterday. But now I am in the flat, taking my shoes off when my brother drops the bombshell: ‘you know, Dad took the vaccine’.
I am shocked. He told me he was not going to, because he found the registration process too difficult, so he decided to stop trying. I was relieved; I had been persuading him that he should not, that being immunocompromised, his system might not cope. I told him what I knew and what I worried about. My brother tells me another family member helped organize his jab and took him there. Jesus. But I am to pretend I don’t know about it; Dad asked my brother not to tell me.
So, I learn that the day after the Pfizer jab he started to feel weak, and within ten days he was prescribed blood thinning injections, a daily drip and he became bedbound. My brother has hired a hospital-style bed and an oxygen machine, set them up in father’s bedroom and organized a private nurse for daily visits. Dad had not wanted to go to hospital: he believed that hospitals were overrun by contagious Covid patients and that going to hospital would mean certain death under a ventilator.
Luckily (I never thought I would say this), unlike the UK, this ex-communist country never managed to build up its own national health service to a level able to deliver comprehensive care, so a secondary private sector filling the gaps exists and is not beyond the means of many people. So here he is, in his own bedroom and getting care at home.
He is happy to see me but asks me not to touch him. I feel sad, guessing he might worry I am bringing contagion. That hurts. I pretend I know nothing about the jab. Later, much later, I remember this moment and think that, he might have wanted to protect me. He knew the jab made him ill and he worried he was fighting vaccine induced-Covid and did not want to give it to me.
He never told me about the vaccine, I never told him I knew.

Sunset in Quaratine
QUARANTINE ONE: THE APP
The day after arriving I receive a text message telling me I am now under statute of law obliged to download a particular app and use it during my 10-day home quarantine. I start the download but can’t complete it. Something is stuck and I have no idea how to fix it. I try for a while and then abandon it. I spend most of the time caring for my father who now slips in and out of consciousness.
The next morning I get a phone call but it stops ringing before I have time to answer it. The following day the same happens. I realise this is the local track and trace. They ring but don’t wait for me to answer. Their call is logged, the box gets ticked but the robot or a human cannot be bothered to do the job properly. Actually, it must be a human as a robot would not give up. Good. The tyranny will fail due to human error or sheer laziness.
I don’t know what possessed me but somehow, I manage to complete installing the Quarantine App. The system springs into action. I get a message from the app that I must take a selfie within the next 30 minutes and submit it. I take a selfie from the app which gives me as many times as I like to choose the best shot. I choose the worst shot.
Of course, there is a way to cheat: after doing my selfie I could leave the phone at home and go out for a walk. Trouble is, the selfie demand comes at a different time each day, usually towards the end of the day. But I have no reason to go anywhere, really, I have come here to be with him, and his condition continues to be critical. And at some point, during this journey I decided that I would do everything by the book, just to see what the new normal travel feels and looks like, and what exactly they want us to experience.
Well, here I am, in a 10-day quarantine in a flat with my dying father. We are lucky. I have my brother to get the shopping in and kind neighbours ready to help. We are lucky my father is at home. What would be the point of coming here all this way, only to be stuck in quarantine if he was in a hospital with no visitors allowed? So, all in all, we are lucky.
DIFFICULT DAYS
Days go by, my father’s condition improves a little, I am his nurse, and of course I touch him – he stopped protesting as soon as he needed a glass of water; I continue to take my selfies. We talk, I read to him, feed him, then he sleeps. He dies two days after my quarantine ends. That is good timing.
There is a lot to do now, and I will not be breaking the law trying to organize the funeral… I remember my favourite literature lesson at school when we debated who was right: Creon or Antigone. Even then, I was in team Antigone.
A doctor arrives to certify death. She is nice and takes her time. Talks a little. Does not look like a corporate bot. She is sitting at a coffee table doing the paperwork. For the cause of death, she writes ‘Thrombosis’. I ponder for a bit and then hesitatingly say: ‘Did you know he was vaccinated?’.
Her face changes and she asks: ‘No, when?’ We tell her, ‘Four weeks ago, exactly’.
‘I am not allowed to say anything,’ she says, ‘but I can tell you I have seen a lot lately. A lot!’ We try to encourage her to talk more but she is cautious. I just ask her: ‘Why would a person on cancer treatment be given a vaccine? Surely that had not been done before?’ She looks at me and says: ‘Because they want to vaccinate us all.’ So, she knows.
This kind of conversation would have been typical in the days of strict communist authoritarianism before 1989. You never knew whom you could trust so you just dropped hints and checked for people’s response. In those days careless talk was dangerous, and I am too young to remember the worst times: the Stalinist years when children were encouraged to denounce their parents; many were imprisoned, tortured and killed.
Now the threat is only a loss of income and public humiliation and yet the new order based on lies, fraud and corrupt science is already in place. Everyone is just doing their job. A perfect example of Hannah Arendt’s banality of evil in which those, following orders in this elaborate house of cards, often do not even know their active contribution to harm inflicted on others. They do not realise because they refuse to look and to know. They stopped taking responsibility for their individual part in the whole.
There is a small group of doctors in the country who are challenging the official narrative, attempt to offer treatment for Covid patients and warn against the untested ‘vaccines’, particularly now that governments want to jab children. Their voices are censored, the people get smeared, ridiculed and shamed by the professional licensing medical body. The modern-day governance in Western democracies!

TRAVELLING HOME
As the funeral preparations get underway, I need to organise my return travel. I check the UK government website again. Travelling from an ‘amber’ coded country, I must test negative for Covid within 72 hours prior to departure. Tricky when the flight is on Monday afternoon.
I start to search for UK government-approved tests available in the city. Only a handful provide the specified UK approved antigen test with results in English. They are also open only in the mornings so if I test on Friday morning, I might be testing a few hours too early to fit within the 72 hours.
After hours of online searching, I find one that looks almost right. I pay the equivalent of £35 online and am told to come on the day, without an appointment. The laboratory website provides useful advice, how to prepare for the test. I learn that I should not brush my teeth or use mouthwash on the morning of test. So now I know what to do.
I arrive at the testing centre early, having heard that queues can be quite long. It is, and it is in the street. The lab’s waiting room only allows three people at a time so the rest stand outside. After about an hour it is my turn. I am allowed inside the surgery.
On the right, by the door, a masked man sitting at a desk behind a glass screen is checking my name and the type of test I have purchased. Then, a young tall, man in full white hazmat suit, his face covered, and in protective glasses ushers me to sit on a chair and tip my head backwards.
This is my first Covid test ever and I am terrified. I have rehearsed telling them how sensitive my face feels and asking not to go deep but there is no eye contact, no talk trying to help me feel comfortable, no attempt to put me at ease. He just tells me to tip my head back far.
I just manage to ask him to go into the left nostril as my right one is not straight. He happily obliges and shoves the long stick into my nostril. As soon as the tip enters my nose I feel shock, a feeling of something unnatural, wrong and threatening happening. The area he just touched is too soft, sensitive and the sensation so unfamiliar I involuntarily, and to my own shock, find myself pushing the man’s arm away. He moves back and looks at me, his body language (there is no face available) disapproves of my behaviour.
I say, please don’t go that deep, you already have some but he insists, tells me not to defend myself and does it again. And again, that feeling that a part of me which is vulnerable and should not be touched, gets scraped. He gets his sample and nods for me to go. I am frozen in that chair, unable to move for what seems like a while. I have tears in my eyes, and I am alone with two hazmat wearing robots. No word is uttered as I leave.
I get my negative result within hours. I recover with an old friend. By then I have a splitting headache and my left nostril is moist with a slight leak. The headache lasts for a couple of days but the leak persists for at least ten.
I arrive at the airport early because I have difficulties completing the UK Passenger Locator Form which UK needs from all passengers. I pass through a manned gate with an automatic wrist temperature check. The airport is unusually quiet, and the staff help me identify the problem which stops me from completing the form. The reference number for the double Covid test needed for the Passenger Locator Form is wrong. I ring home and ask my husband to read the reference number off the Covid test kit. Surely it has arrived now. It hasn’t. It looks like the Day 2 and 8 Test I ordered has not been paid for.
I am told I need to buy a new kit if I want to get this flight. I do as I’m told. No form, no flight. I stand next to the luggage drop off counter feeling sweats, and with my hands shaking I battle the website on my phone. Again, all the ‘cheap’ ones are sold out and somehow, at the last minute I manage to make a purchase for £180, get an email, a reference number, complete the form and have my luggage accepted.
I hurry to my gate and make it just in time as passengers are starting to board. I slow down to join the Ryanair herd waiting on the tarmac for the aircraft to be processed before we are told we can travel.
The pavement is marked with lines at 2-meter intervals. Two men behind me are joking loudly that we must stand on the lines correctly, otherwise the virus will jump on us. I turn and smile (no mask, we are still outside) and make eye contact with the fellow humans.

QUARANTINE TWO: TRACK AND TRACE
Back home in London, the following day I get my first out of ten phone calls from Track and Trace. Each time a different voice reads the same script.
I am contacting you on behalf of the NHS Test and Trace as you have recently travelled into the UK from abroad. Are you happy to continue in English?”
No idea what would happen if I said ‘no’.
Before we proceed, I need to make you aware that this call will be recorded for training and quality improvement purposes and should just take a few minutes of your time. I can confirm I have completed the necessary data security training and all information you provide today will be stored securely. NHS Test and Trace may need to share your details with other organisations including the Home Office, and further information on data security and privacy can be found on http://www.gov.uk/coronavirus. Sharing information in the call today means you consent for it to be stored in the ways I have described. Are you happy to proceed with the call?”
I wish I could say, no, I am not. Once or twice I ask how long the data is going to be stored. The caller is not sure and advises me to find this out from the government website. The call proceeds with them checking my year of birth. Then they ask if I have opted into a ‘test to release’ – I frankly don’t even know it is my option, so I say ‘no’.
I later learn that the Test to Release scheme does not replace the compulsory Day 2 and 8 test. The ten-day quarantine can be shortened to 5 days by ‘opting into’ Test to Release for an additional £99. I realise they ask this question to advertise another product!
Can you confirm that you are quarantining at the address you provided on the passenger locator form and will continue to do so for ten days starting on the day after you arrive in the UK.”
So, again, I confirm, yes. What would happen if I said no?
As part of the Covid 19 response you are legally required to take the test on Day 2 and Day 8 and a failure to do so may result in prosecution.”
That answers my previous question…
Has your test arrived? And have you taken or do you intend to take your test?”
Yes.
Then I am asked if I got my test from the NHS or from a private provider. I am confused as I had no option to get an NHS test and I tell the caller. They seem happy with my answer and continue:
If your Day 2 test is positive confirming Covid 19, you do not need to take another test on Day 8.”
I think, on one occasion, I ask how I am expected to post the test if I am not allowed to leave the house. Of course, the assumption is there is someone else in the house, and if I still have difficulties, again, the go-to place is another NHS number. Amazing what they can do these days; they can even pick up your mail for you!
The call continues:
If you develop any of the three coronavirus symptoms which are: a new continuous cough, a high temperature, or a loss or change to your sense of taste or smell, please visit http://www.gov.uk/coronavirus for further advice. You should not go to the GP, hospital or a pharmacy. If you require medical advice, please ring the NHS on 111 or in an emergency dial 999”.
So here we have the admission of medical malpractice: if I fall ill, I must not seek help from NHS, not even by going to my local pharmacy. I must stay home without help, except of course, if I qualify for 999 ie, a ventilator…
The call continues:
I must advise you that if you test positive for coronavirus or are identified as a close contact of someone who has coronavirus you will be notified by NHS Test and Trace and may be contacted again. Is there anything you would like me to repeat?”
Of course, if someone I sat next to on the (half-empty) plane gets a positive result, my quarantine will stretch to a fortnight or longer! Each time, the call ends with a friendly, youthful, ‘have a great day’. All those who have called me are young voices, all kinds of accents, probably desperate for any job in the current climate. They are trained to stick to the script and any departure from it by my questions seems to trip them up.
And most of them probably think they are doing something socially useful and valuable.

THE QUARANTINE DIY TESTS
The one I have purchased in haste at the airport is a kit with two PCR tests to be administered at home on Day 2 and Day 8. The instructions tell me that the test is run at less than a 30-cycle value threshold.
The first thing to say about the swab is that it is long. It looks like a cotton bud used for everyday use, but on closer inspection it is different. The stick itself is about 12 cm long, that’s 6”, and designed to break off after the sample is collected and put into a small tube provided. The tip itself is 2 cm long, quite thin and covered in almost translucent spiky bristles protruding outwards. It looks a bit like a miniature harsh brush designed to scratch the delicate tissue inside the mouth and nose.
I am told to swab the back of the throat for 3-5 seconds over the posterior pharynx and tonsillar areas but to avoid tongue, teeth and the sides of the mouth. Then I am told to insert the same swab to each nostril about 2 cm deep and to rotate it for 3-5 seconds each time.
The form which I have to complete for each test is yet another mandated opportunity for the corpo-government to harvest my personal data, to store it for as long as it sees fit, yet, as is often the case in abusive relationships I have to (I repeat:) I have to give my consent for all this to happen, and even consent for my possible positive test result which may include my personal details: name, date of birth, gender, home address, telephone number, occupation, place of work, ethnicity and the fact that I have tested positive for Covid 19 to be communicated to Public Health England. Luckily, both of my test results are negative.
Eleven days after arrival in the UK my quarantine is officially over. It takes me a couple of days before I venture outside, I detect a bit of agoraphobia. In the last six weeks I spent twenty days in house arrest. They say it takes six weeks to develop a new habit.
POSTSCRIPTUM
I doubt very much I will travel internationally any time soon. Not planning to take the experimental Covid jab and so will not be enjoying the privilege of freedom promised to those with the vaccine passport. At the time of writing, it is no longer illegal to leave England but the elaborate hoops and the red tape remain and the government website reminds us that “to protect public health in the UK and the vaccine rollout, you should not travel to countries or territories on the red or amber lists”.
The ‘red and amber’ lists cover most countries of the world and returning from an amber list country will involve three or four tests which could come to £240-£340 per person plus the time spent completing all the online forms.
As to the red list countries; even a short spell there ends in an expensive £1750 per person prison-like stay at an airport hotel, as can be seen here.
So whilst not forbidden, even essential travel has been made into a series of expensive, degrading and time-consuming obstacles. Vaccine passports are being rolled out precisely to convince people they will magically bring freedom back to their lives. Do they not realise, that once they have their passports, the vaccine will need regular boosters?
Those still asleep; trusting the governments and the mainstream media think that easy travel is only temporarily put on hold but once the pandemic is ‘under control’, things will get back to the way they used to be. They do not realise the plan is to make travel an exclusive and rare event beyond reach of ordinary people.
This is done to us not just by the predatory elite class. Disappointingly, the pro-lockdown left continues to cheer these restrictions on and dismiss people’s desire and need to travel, as undeserved indulgence or middle-class privilege (interestingly, unrestricted travel around Europe was, until so recently, one of the main reasons for their fierce anti-Brexit position. What happened to their cherished principle of freedom of movement?). They could not be further from the truth.
They forget that, according to official migration data for the end of 2019, the UK is home to 6.2 million people – that is 9% of the total population – who have the nationality of a different country! And that data does not even include naturalised UK citizens like me, first-generation settled migrants who have close relatives all over the world and that unrestricted travel is an essential means to family life, something which is protected by Human Rights Act 1998.
The irony for those like myself, who grew up in communist Eastern Europe, is that freedom of movement, so taken for granted in the West, the right to travel and to have your own passport at home at all times is what we did not have then. The state set limits on where ‘citizens’, treated like its property, could travel.
For many who experienced those times, even as children, a return to state-mandated travel restrictions will feel like going back into tyranny.
As for my own journey: I will never forgive those responsible and all those lockdown fanatics for stealing my Dad’s, and so many other elderly people’s, last year by locking them up in the prison of fear and isolation, and then for pushing them to take the dangerous experimental jab which – for so many – was the last straw in their already weakened bodies.
Nerd immunity is the way forward
By Andy Lambeth | The Conservative Woman | June 19, 2021
WE learnt on Monday that lockdown restrictions are being extended for one more month. Like millions of others up and down the country I was shocked and quite deflated by this depressing news. However, having had time to reflect, I feel certain that there is a very cunning plan behind Boris Johnson’s seemingly pointless and cowardly dithering. You may disagree and be of the opinion that if someone looks and sounds like a pathetic, spineless, lying nincompoop then he is indeed a pathetic, spineless, lying nincompoop. It’s a fair point, but please hear me out on this one.
People are still very frightened. They have been queuing up in their thousands to get vaccinated and now eighty per cent of the population has had at least one jab. But this still is not enough to make us feel safe, hence the substantial support for vaccine passports and now child vaccination. Face masks are still everywhere. Not only do we see masks where they are a legal requirement but also on the high street and in the park. Many people are wearing them in their cars and on their bicycles. The other day I saw my neighbour wearing one in his back garden. The really worrying thing is that he was in his swimming pool at the time. Recent polls suggest that eighty per cent of people are completely behind Covid restrictions and a large majority want them to continue until we are all completely safe from the virus. There is genuine fear amongst people everywhere and there is a very good reason for this: They have all become nerds.
This pandemic of nerdishness has completely beleaguered this once brave nation of ours. We have become a society of hopeless, wretched supernerds. We put on our nerdy masks to go to the pub, where we check in with our nerdy apps and clean our hands with nerdy hand sanitiser. When inside we greet our friends with a nerdy elbow rub. We take our nerdy mask off to sit down and socialise and then we put it on again to go to the loo. Our level of nerdishness makes Mr Bean look like James Bond. Many of us who find all of this weird do it anyway because we are too nerdy to realise nothing will happen to us if we refuse. Nerdishness has become ingrained into our psyche and our British way of life.
Mr Johnson is faced with the impossible task of putting an end to all this strange behaviour. He cannot simply say the virus has disappeared, because no one would believe him. On the other hand it would be political suicide for him to admit that the whole thing was an overreaction in the first place. His only option is to give people the opportunity, one by one, to come to that realisation themselves and to develop the confidence to start acting like normal people. In other words we need to develop nerd immunity. This cannot be achieved by the government lifting restrictions: it can only be achieved by them doing the very opposite and pushing our patience and tolerance to its limits. Johnson must therefore ensure that we all have continued exposure to never-ending, ridiculous coronavirus regulations until we build up a natural resistance to it and stop acting like frightened little nerds.
So how does the human body actually develop nerd immunity? I put this question to Professor Dai Ifyougettit, Head of Immunology at Cardiff University Hospital. The professor recounted the story of Kevin, one of the volunteers in his clinical study group, who has fully recovered from being a nerd. When this all started back in March 2020, like many people Kevin thought the pandemic was just as deadly as the Spanish flu of 1918. However, increased exposure to Covid news conferences on the BBC made Kevin start to wonder if things were being exaggerated. As restrictions became more ludicrous and unnecessary Kevin began to start questioning things. The official narrative just didn’t add up and even David Icke began to make a bit more sense than Matt Hancock. ‘I hadn’t become a Covid denier or a conspiracy theorist as such,’ Kevin said, ‘but I had serious doubts about what the Government was telling us.’
Professor Ifyougettit explained how Kevin’s change in perception was the body’s immune system doing its job. To protect him from nerdishness Kevin’s internal defences had forced him to do something that did not come naturally: critical thinking. Some individuals may have major concerns about the adverse side effects of critical thinking and are therefore hesitant. However, if we are to achieve nerd immunity we will all have to be more open to thinking critically. Just one application of critical thinking would be enough to give someone sixty per cent nerd immunity but another one a few weeks later would give up to ninety per cent. After that, critical thinking boosters might be needed. I asked the professor if a stronger dose of critical thinking would offer complete protection from nerdishness. ‘No, it is important to get the dose exactly right,’ he said. ‘Too much critical thinking can cause adverse side effects, such as making you even nerdier.’
Many people are asking why the situation is so different in the US. In particular, states such as Florida and Texas have already made excellent progress with their levels of nerd immunity. I questioned one of the epidemiologists working with the Government advisory body NERDTAG (New and Emerging Really Dorkish Threats Advisory Group). She told me it is likely that progress in some American states has been possible due to pre-existing levels of immunity against nerdishness. On average Americans are a little less nerdy than Brits so they may have had some protection already. She said that the estimated level of nerd immunity in the UK is currently standing at about ten per cent but this has to rise to at least fifty per cent if we are ever to return to normal.
Clearly we have some way to go and so Boris Johnson is doing exactly the right thing in having us on for a little longer until the penny drops. If restrictions are simply lifted at this stage we are under serious threat of a third wave of nerdishness. This would be utterly disastrous for both the country and the Government. Mr Johnson really has no choice but to remain in lockdown and continue his Simple Simon routine until all age groups have been given the opportunity and the incentive to think critically about their nerdish compliance.
Of course some people might argue that although this is a clever and pragmatic strategy there is a hefty price to pay for it. UK debt is over two trillion pounds already and it is rising all the time. More financial compensation will be necessary for any continuation of lockdown measures and so we will undoubtedly need to borrow even more money. However, anyone who knows anything about getting into debt will tell you what you need to do when you cannot afford to pay off what you owe. You borrow more. Then you keep borrowing more and more until paying it back is absolutely inconceivable. That is the only way you can get your debt written off.
So we’re in this for the long haul. There are no easy solutions and we are all going to have to grin and bear it. But don’t despair because if we go through enough pain, nerd immunity will be the light at the end of the tunnel.
Willem Engel Interview – The Fight For Freedom In The COVID Age & The Battle For Our Very Humanity
Willem Engel has been neutralized by the Netherlands/EU Totalitarian Regime
By Taylor Hudak | The Last American Vagabond | June 16, 2021
Joining me today is scientist and activist Willem Engel, here to discuss his ongoing legal efforts to fight back against what many are referring to as ‘crimes against humanity’ being committed under the guise of fighting COVID-19 – and rightly so – as well as what’s at the center of this battle, and that is the fight for humanity itself.
(https://www.rokfin.com/TLAVagabond)
(https://odysee.com/@TLAVagabond:5)
(https://www.bitchute.com/channel/24yVcta8zEjY/)
Source Links:
https://www.irishtimes.com/topics/topics-7.1213540?article=true&tag_person=Willem+Engel
https://www.bbc.com/news/world-europe-56084466
https://www.dutchnews.nl/news/2021/02/police-backpedal-on-congratulations-for-curfew-court-case-win/
Are the Covid-19 vaccines “safe and effective”?
Steve Kirsch | Trial Site News | June 16, 2021
A video presentation by Steve Kirsch, Executive Director of the Covid-19 Early Treatment Fund.
Watch Video at Trial Site News
Are there any risks associated with the COVID-19 vaccines currently authorized on an emergency use basis by the U.S. Food and Drug Administration (FDA)? Presently three genetic-based vaccines have been authorized via the emergency order including two mRNA-based vaccines (Moderna and Pfizer-BioNTech) as well as the adenovirus-based Johnson and Johnson product. Developed at historical speed under Operation Warp Speed, the mRNA-based technology foretells enormous implications for healthcare including the prospect of vaccines for cancer. An amazing research prowess has unfolded in response to the COVID-19 pandemic heralding profound breakthroughs that’ll benefit society for years to come. Governmental authorities have declared the vaccines both safe and effective and as TrialSite recently reported based on a change of law that waives the need for informed consent with investigational products. Both the U.S. Centers for Disease Control and Prevention (CDC) and FDA have declared that the risk-benefit analyses strongly indicate the risks of not getting a vaccination outweigh any risk of vaccination. They argue that the risks associated with COVID-19 are materially greater. Moreover, health authorities are on record that there is absolutely no correlation associated with the COVID-19 vaccines to any deaths as indicated by the CDC declaration. But have they sufficiently probed and pursued granular investigation into their own data? Have they undertaken the comprehensive analyses associated with what in the CDC VAERS is now close to 6,000 deaths. Are all of these unrelated to the vaccines? Steve Kirsch, the founder and executive director of the COVID-19 Early Treatment Fund (CETF), a regular contributor to the TrialSite recently conducted a more systematic and thorough analysis of the VAERS and CDC adverse event and death numbers reported in conjunction with the COVID-19 vaccines. The results are disturbing to say the least. TrialSite offers no opinion here other than the presentation of the highly successful MIT-trained engineer who has invested millions of his own funds into early stage treatment options targeting COVID-19. What follows is a summary of his deep dive into VAERS presented in this video.
Official CDC Position
The CDC is on the record that the now nearly 6,000 deaths reported in VAERS since December 2020, including “A review of available clinical information, including death certificates, autopsy, and medical records, has not established a causal link to COVID-19 vaccine.”
The analysis provided by Kirsch suggests that while nearly 6,000 are now entered into the voluntary system, he suggests the actual number could be undercounted by a magnitude of up to 5 times and a review of direct CDC excess death data indicates what the notable entrepreneur counts as 25,000 deaths that could be associated with the coronavirus vaccines.
The Presentation
The Kirsch presentation starts with an introduction to the CDC Vaccine Adverse Event Reporting System known as VAERS with a review of some key indicators including reported deaths. Open to the public, he reveals by June 4th the following adverse events were associated with the COVID-19 vaccines:
Reported Event #s Deaths 5,088 Hospitalizations 19,587 Urgent Care 43,891 Office Visits 58,800 Heart Attacks 2,190 Anaphylaxis 1,459 Bells Palsy 1,737 Thrombocytopenia/Low Platelet 1,564 Myocarditis/Pericarditis 1,087
A review of available clinical information, including death certificates, autopsy, and medical records, has not established a causal link to COVID-19 vaccines.
At 12:15 into the presentation Mr. Kirsch reveals a data distribution revealing a dramatic spike in deaths associated with the COVID-19. Moreover in this data analysis it’s revealed that the majority of deaths occur closer to the actual time of the vaccination event indicating a higher probability of a causal relationship.
At 12:49 he presents the data findings indicating that overwhelming the incidents of heart attacks associated with the VAERS COVID-19 vaccine spike within a day to three days after the vaccination event. He also emphasizes that the indication of Myocarditis/Pericarditis actually increases with vaccination as age decreases which is counter intuitive in that young people should have less probability of experiencing such heart related troubles. Is the vaccine causally connected to this data?
At 15:51 in the presentation Kirsch depicts again the growing numbers of deaths corresponding to the release of the vaccines under emergency use authorization by mid-December 2020. At 18:55 he reveals a corresponding increase in excess deaths reported by the CDC.
Kirsch goes on at 26:13 to discuss the imperative to consider a time out in the process to at least investigate these safety data signals. At 28:09 Kirsch raises the imperative for informed consent under the Declaration of Helsinki. Although as TrialSite reported the law was changed in 2016 thus waiving the need for informed consent with investigational products deemed safe.
At 32:22 Mr. Kirsch discusses early treatment options for COVID-19. He shares that considerable research has gone on pointing to a number of potential treatments for early onset COVID-19 that can serve to help combat COVID-19. A risk-benefit comparison at 41:50 showcases at least one argument that early stage treatments currently under study should be accelerated.
The presenter offers a plethora of other information that merits review for those interested in a debate on this topic.
Kirsch commented on the findings “The narrative is that the COVID-19 vaccines are safe and effective but the truth is that the data points to an otherwise alternative conclusion.” Kirsch declared that “if anyone was paying attention they would have picked up these safety signals by the end of January.”
Data-Driven Truth or Random Coincidence?
TrialSIte cannot advocate one position over another but rather can serve to share information that fits within the guidelines of the platform for purposes of discussion and hopefully healthy debate. This isn’t a platform for attacking others but rather one that fosters awareness, transparency and engagement. The data present in the CDC VAERS database as well as the CDC death reports do indicate a material spike in activity associated with the coronavirus vaccines. Does the CDC’s position that none of these deaths are conclusively correlated to the vaccine itself despite the data in this presentation revealing a disturbing trend of adverse events and death within a day to three days within the vaccination event? It’s not clear but TrialSite invites the CDC and others on to the platform to put forth an explanation.
Perspex Screens Installed to Stop COVID May Have Actually Increased Its Spread

Al Seib / Contributor via Getty Images
By Paul Joseph Watson | Summit News | June 16, 2021
A leaked Whitehall document seen by Politico suggests that perspex screens installed to stop the transmission of COVID-19 may actually have increased its spread.
Businesses and schools were told by the government to install the screens as a condition of re-opening after the first lockdown and they were widely used by ‘essential’ shops throughout the entire period.
Politico’s Alex Wickham writes that the perspex screens could be about to be scrapped given new information the government has received on their efficacy.
“Ministers are also being advised that those perspex screens that have appeared in some offices and restaurants are unlikely to have any benefit in terms of preventing transmission,” states the report.
“Problems include them not being positioned correctly, with the possibility that they actually increase the risk of transmission by blocking airflow. Therefore there is clear guidance to ministers that these perspex screens should be scrapped.”
Despite the report, government ministers say there is no plan to change advice on installing the screens in businesses.
What other COVID-19 measures put in place to fight the spread of the virus have been utterly useless or actually made it worse?
A study on the effectiveness of face masks involving 6,000 participants in Denmark found “there was no statistically significant difference between those who wore masks and those who did not when it came to being infected by Covid-19.”
New EPA Climate Change Indicator Is Deceptive
Science Under Attack | May 31, 2021
New climate change indicators on the U.S. EPA (Environmental Protection Agency) website are intended to inform science-based decision-making by presenting climate science transparently. But many of the indicators are misleading or deceptive, being based on incomplete evidence or selective data.
A typical example is the indicator for heat waves. This is illustrated in the top panel of the figure below, depicting the EPA’s representation of heat wave frequency in the U.S. from 1961 to 2019. The figure purports to show a steady increase in the occurrence of heat waves, which supposedly tripled from an average of two per year during the 1960s to six per year during the 2010s.
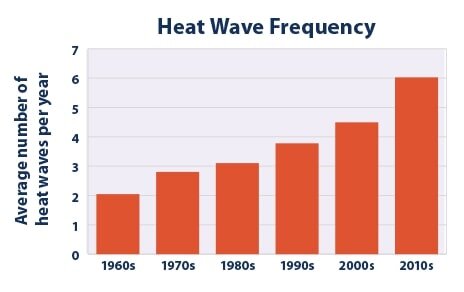
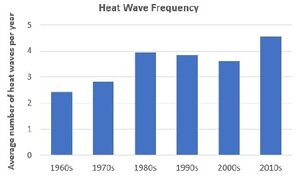
Unfortunately, the chart on the top is highly deceptive in several ways. First, the data is derived from minimum, not maximum, temperatures averaged across 50 American cities. The corresponding chart for maximum temperatures, shown in the bottom panel above, paints a rather different picture – one in which the heat wave frequency less than doubled from 2.5 per year in the 1960s to 4.5 per year in the 2010s, and actually declined from the 1980s to the 2000s.
This maximum-temperature graph revealing a much smaller increase in heat waves than the minimum-temperature graph displayed so boldly on the EPA website is dishonestly hidden away in its technical documentation.
A second deception is that the starting date of 1961 for both graphs is conveniently cherry-picked during a 30-year period of global cooling from 1940 to 1970. That in itself exaggerates the warming effect since then. Starting instead in 1980, after the current bout of global warming had begun, it can be seen that the heat wave frequency based on maximum temperatures (bottom panel) barely increased at all from 1981 to 2019. Similar exaggeration and sleight of hand can be seen in the EPA indicators for heat wave duration, season length and intensity.
A third deception is that the 1961 start date ignores the record U.S. heat of the 1930s, a decade characterized by persistent, searing heat waves across North America, especially in 1934 and 1936. The next figure shows the frequency and magnitude of U.S. heatwaves from 1900 to 2018.
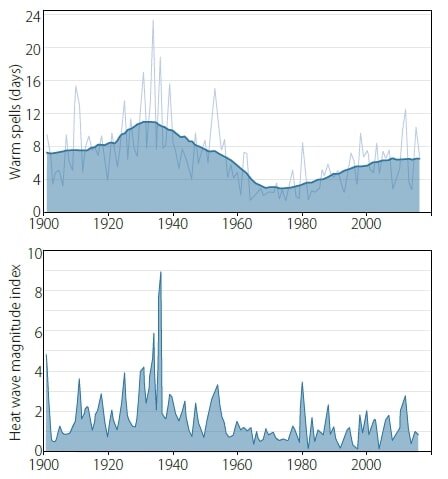
The frequency (top panel) is the annual number of calendar days the maximum temperature exceeded the 90th percentile for 1961–1990 for at least six consecutive days. The EPA’s data is calculated for a period of at least four days, while the heat wave index (lower panel) measures the annual magnitude of all heat waves of at least three days in that year combined.
Despite the differences in definition, it’s abundantly clear that heat waves over the last few decades – the ones publicized by the EPA – pale in comparison to those of the 1930s, and even those of other decades such as the 1910s and 1950s. The peak heat wave index in 1936 is a full three times higher than it was in 2012 and up to nine times higher than in many other years.
The heat wave index shown above actually appears on the same EPA website page as the mimimum-temperature chart. But it’s presented as a tiny Figure 3 that is only 20% as large as the much more prominent Figure 1 showing minimum temperatures. As pointed out recently by another writer, a full-size version of the index chart, from 1895 to 2015, was once featured on the website, before the site was updated this year with the new climate change indicators.
The EPA points out that the 1930s heat waves in North America, which were concentrated in the Great Plains states of the U.S. and southern Canada, were exacerbated by Dust Bowl drought that depleted soil moisture and reduced the moderating effects of evaporation. While this is undoubtedly true, it has been suggested by climate scientists that future droughts in a warming world could result in further record-breaking U.S. heat waves. The EPA has no justification for omitting 1930s heat waves from their data record, or for suppressing the heat wave index chart.
Although the Dust Bowl was unique to the U.S. and Canada, there are locations in other parts of North America and in other countries where substantial heat waves occurred before 1961 as well. In the summer of 1930 two record-setting, back-to-back scorchers, each lasting eight days, afflicted Washington, D.C.; while in 1936, the province of Ontario – also well removed from the Great Plains – experienced 43 degrees Celsius (109 degrees Fahrenheit) heat during the longest, deadliest Canadian heat wave on record. In Europe, France was baked during heat waves in both 1930 and 1947, and many eastern European countries suffered prolonged heat waves in 1946.
What all this means is that the EPA’s heat-wave indicator grossly misrepresents the actual science and defeats its stated goal for the indicators of “informing our understanding of climate change.”
The New Irish Soviet: State Bans Seniors from Traveling Until They’ve Had ‘Second Dose’ of AstraZeneca Jab
21st Century Wire | June 15, 2021
Since the crisis began in March 2020, there has been a distinct air of medical fascism which has gradually permeated Irish political rhetoric and policy – which has left many conscientious residents shocked.
This dark state of affairs appears to be coming to a head now, as technocrats in Dublin push the totalitarian envelope even further.
Suddenly, after 15 months of running an open-ended crisis narrative, the great and good are now saying, “Now is certainly not the time to be taking risks on travel,” as the government and media operatives begin ramping-up Project Fear once again.
As usual, the state has singled-out the most vulnerable target demographic upon which to leverage its power, and to mete out some of the most outlandish policies ever seen in the western world over the last 150 years, including policies that would even have been beyond the pale for Stalin’s Soviet Union.
Incredibly, after the Irish government pushed some 400,000 of its older citizens to inject the highly controversial, unlicensed experimental gene-based AstraZeneca jab, the government is now banning them from leaving the country – until they have received their second dose.
Irish Independent reports…
More than 400,000 people who are waiting for a second dose of the AstraZeneca Covid-19 vaccine have been told they cannot travel abroad.
The “vaccine bonus” for those who are a month on from their first AstraZeneca jab does not involve foreign travel, the updated advice from the HSE has warned.
People in their 60s, and a significant number of those with underlying conditions, have been left waiting for a second dose of the vaccine, which will take at least eight weeks, but may be even longer for many.
They can avail of the vaccine “bonus”, with one dose after 28 days, allowing certain limited meeting up with others indoors, but “this does not include foreign travel”.
By definition, this can be classed medical fascism – where state and corporations have codified policy in order to coerce and effectively enforce an experimental medical procedure. On paper, this is in direct violation of the Nuremberg Codes which have been recognised for decades as de facto international law. Moreover, citizens are being denied informed consent, which is also a violation of both Irish and European law and contravenes the human rights charter.
This is an incredibly dangerous move by the state, and while it may be done under the now acceptable auspices of fear and general hysteria – it has still been done with no actual scientific evidence to justify it – only often repeated conjecture and increasingly vague claims used to further underpin the ever-evolving self-licking ice cream cone which is the seemingly never-ending “variant” scare.
Intelligent, sober people can now see that the variant scare has been contrived to justify the government’s omnipresent threat of more lockdowns, restrictions and border closures, and above all: to force vaccine compliance.
Meanwhile, technocrats in Brussels are using these artificial travel obstacles created by member states in order to create an artificial demand for a new Vaccine Passport (or ‘COVID credentials’) regime, which they have recently rebranded as a “Digital Wallet” due to pushback against its previous vaccine “Green Pass”:
The EU Digital Certificate, paving the way for travel within the bloc, is due to be operational here from July 19.
The HSE does not specify the same travel restriction for people who received one dose of the other vaccines.
Moreover, government ministers continue to make assertive claims about the alleged “effectiveness” of these unlicensed experimental injections against the newly branded “variants” which are now being deceptively sold to the public as ‘deadly mutations’ of the previously touted ‘novel’ coronavirus:
Public Health England has previously found that one dose of vaccine gives just 33pc protection against the more infectious Delta variant that originated in India.
It said yesterday that two doses of the Pfizer vaccine give 96pc protection while the AstraZeneca gives 92pc.
It comes amid concern at the inevitable rise in the Delta variant, with around 140 cases detected here so far. Another 242 cases of coronavirus were diagnosed yesterday.
How the UK government could make any such claims about the level of “protection” any COVID vaccine actually provides against the alleged ‘variants’ may be more a feat of political science and propaganda than actual clinical science, because the source of these sweeping claims emanates from the pharmaceutical manufacturers themselves. Does anyone seriously doubt by now that these private interests have captured European governments’ regulatory and political institutions?
Still, Irish ‘science’ experts appear to be confused as to how to play the new variant-vaccine narrative. Luke O’Neill, professor of biochemistry at Trinity College, spoke with the Irish Independent, claims to know how the rebranded ‘Delta variant’ virus behaves, while at the same time admitting that, ‘there doesn’t seem to be a huge amount it around’. He then defers to the UK experts and their own spurious Delta claims, whilst advising hapless Irish citizens who have had one dose of the experimental AstraZeneca injection to ‘take care’. By now, this contortionist feat of ‘public health’ gymnastics has become commonplace:
“We know from the UK that one shot of AstraZeneca is not giving the same level of protection from the Delta variant as two shots, so I would think those who have had one shot of AstraZeneca will have to take some precautions until they’ve had their second shot,” he said.
“We’re lucky in that there doesn’t seem to be a huge amount of the Delta variant around, at least currently. The goal has to be to get the second shot into the vulnerable people – including the over-60s – as quickly as possible.”
Of course there is no mention by any government officials about the fact that this problematic AstraZeneca jab has already been halted in multiple countries (and it hasn’t been allowed to be released in the United States either) due to confirmed risks of maiming or death due to fatal blood clotting – a fact now accepted by experts worldwide. This is now accepted as a clear and present danger for any members of the public taking part in this unprecedented human experiment.
In Europe, health officials have stated that countries should also avoid giving the AstraZeneca vaccines to people over 60, as said by the head of the EU drug regulator’s COVID-19 task force on Sunday. But for some strange reason, no Irish politician or mainstream media outlets want to talk about this serious problem.
All of this comes amid the backdrop of British PM Boris Johnson announcing the delaying of an end to the UK government’s indefinite ‘state of emergency’ and lingering lockdown policies. The government claims this is because of fears of the alleged Indian Variant (recently rebranded to ‘Delta Variant’), while claiming that somehow COVID-19 “cases” (not actual clinical cases, but PCR and lateral flow ‘positive’ tests) are now at a three-month high. Britain was scheduled to lift all remaining restrictions on June 21st, but now says that it needs more time to vaccinate more of its population – as extremist voices in political and media circles continue to blame these alleged new ‘outbreaks’ of COVID-19 on ‘the unvaccinated.’
Based purely on its words and polices, Ireland’s ruling Fine Gael-Fianna Fail regime (from the onset, ‘opposition’ party Sinn Fein has also supported these same draconian policies) now finds itself as the vanguard of a new European Soviet.
Needless to say, this level of medical tyranny and mass-hysteria is unprecedented.
The real question remains: will the public at large and conscientious members of the press and government, come to their senses and wake up before the damage to democracy and freedom becomes irreparable?
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s recurring use of terror on civilians

By Bob Finch | January 26, 2009
Insanely disproportionate use of violence against unarmed civilians… continue
Blog Roll
 Aletho News
Aletho News- China issues first prohibition order to safeguard international trade order under rule of law
- Iran rejects Trump’s ‘Project Freedom,’ warns US over Hormuz role
- TRUMP ANNOUNCES OPERATION TO ESCORT SHIPS – Fmr. CIA Analyst Larry Johnson
- A few observations on Iran’s latest proposal to Trump
- ‘I urged that our objective be regime change… so did Netanyahu’ – ex-Trump adviser on Iran
- “STAGED”: Conspiracy Theories Are Everywhere!
- NATO courts screenwriters to embed alliance messaging in film, TV
- Iran replaces UAE ports with Pakistan corridor to break US blockade
- Iran sets one-month deadline for end to US-Israeli war, blockade: Report
- At the edge of the Strait: A superpower in a narrow sea
- If Americans Knew
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- No Tricks Zone
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
