“Preparing for Disease X”
WEF panel session on Jan. 17, 2024 will discuss preparations for “unknown disease.”
BY JOHN LEAKE | COURAGEOUS DISCOURSE | JANUARY 14, 2024
Last night at dinner with Dr. McCullough, he asked me to do some research on the dread “Disease X” about which we’ve been hearing a lot of chatter since it was announced that the Davos crowd will be talking about it at their annual WEF meeting this January.
I agree that it’s always a terribly ominous sign when the WEF talks about saving humanity from a hypothetical threat. When those guys start chatting about saving us from an “unknown” pathogen, it’s a safe bet that bio-labs are already tinkering around with a “candidate pathogen.” The stated objective of their work is to develop vaccines against the candidate pathogen should it (God forbid) evolve to infect humanity.
To get a sense of how this industry works, check out this Sky News report from August 7, 2023 headlined: ‘Disease X’: UK scientists begin developing vaccines against new pandemic.
Further investigation of the literature on Disease X led me to a book, published about a year ago, titled Disease X: The 100 Days Mission to End Pandemics, by Kate Kelland with a Forward by Tony Blair.
Ms. Kelland is a former Global Health Correspondent for Reuters and is now Chief Scientific Writer for CEPI (Coalition for Epidemic Preparedness Innovations). As many readers of this Substack are aware, CEPI was founded in 2016 by the World Economic Forum, the Gates Foundation, and other key players in the Bio-Pharmaceutical Complex.
Its Preliminary Business Plan, published in 2017, is a blueprint of what I call the Pandemic Predicting and Planning Industry, which positions itself to rake in billions of public money when the next infectious disease pathogen strikes humanity.
An attractive Englishwoman who studied French and German at Durham University, Ms. Kelland’s career as a news correspondent seems to have really taken off around the time of the 9/11 attacks. As she put it on her LinkedIn profile: “Two years in the lobby tracking the Blair government during the crisis surrounding the 9/11 attacks on the United States.” In 2009—probably with the arrival of the grossly overblown Swine Flu Pandemic—she became a Health and Science correspondent for Reuters.
A conference on Disease X at the WEF’s annual meeting is scheduled to take place in Davos on January 17, 2024. As it is described on the WEF website:
With fresh warnings from the World Health Organization that an unknown “Disease X” could result in 20 times more fatalities than the coronavirus pandemic, what novel efforts are needed to prepare healthcare systems for the multiple challenges ahead?
This session is linked to the Partnership for Health System Sustainability and Resilience and the Collaborative Surveillance Initiative of the World Economic Forum.
This first sentence raises the question: Why is the WHO issuing “fresh warnings… that an unknown “Disease X” could result in 20 times more fatalities than the coronavirus pandemic”? On what intelligence is the WHO basing its fresh warning? A Google search for “WHO issues fresh warning about Disease X” resulted in this report of 26 May 2023 headlined After WHO chief’s warning, ‘Disease X’ raises concern
It seems to me that all reasonable adults are justified in asking the question: What are these gangsters cooking up now?
The above timeline of announcements does indeed resemble the autumn of 2019, when the Bio-Pharmaceutical Complex engaged in a huge amount of of chit-chat and pandemic planning simulations about a hypothetical “coronavirus” pandemic.
To make matters even more ominous, the chatter about Disease X is happening at the beginning of another election year, with Donald Trump once again leading in the polls and the representation of a man named “Joe Biden” challenging him.
Heaven help us.
New Zealand’s “Warming” Is Based On Temperature Adjustments & Artificial Airport Heat Islands
By Paul Homewood | Not A Lot Of People Know That | January 13, 2024
Graeme Hook left this comment yesterday:

Unfortunately Wayback does not have a copy of the earlier Berkeley Earth graph; if anybody can track it down, give me a shout.
However what I have found is just as interesting.
Let’s start with the current Berkeley Earth graph for New Zealand:

https://berkeleyearth.org/temperature-region/new-zealand
Since the 1880s, temperatures have risen by about 1C, up to 2020. Most of this increase has occurred since the 1950s.
This is more or less in line with the GISS chart of adjusted temperature data for Auckland Int Airport – (ignore the 2023 spike):

https://data.giss.nasa.gov/cgi-bin/gistemp/stdata_show_v4.cgi?id=NZM00093110&ds=15&dt=1
However the unadjusted data tells a completely different story; as is often the case, GISS have cooled the past, by about half a degree. In particular, there appears to have been little increase since the 1950, prior to last year:

Far from cooling the past at Auckland, GISS should be doing the opposite.
There are, apparently, two weather stations at Auckland Int Airport. This is the location of the one that GISS quote:

https://www.ncei.noaa.gov/access/homr/#ncdcstnid=30095746&tab=LOCATIONS
It’s on top of a roof of an airport building, in the middle of the airport complex. But a closer look shows it is just yards from a number of air conditioning vents:

The other station is no better, about 20m from the tarmac:

https://www.ncei.noaa.gov/access/homr/#ncdcstnid=30151541&tab=LOCATIONS
What is absolutely certain is that the airport would have looked much different in the 1950s. It started life in 1928 as a dairy field with three Gypsy Moths.
In 1965, when the first commercial flight took off, a DC8 to Sydney, it looked like this:

Over the years, of course, the airport has been massively expanded, and now handles 16 million passengers a year, now looking like this:

The so-called New Zealand temperature record, which claims to show significant warming since the 19thC, is based on heavily adjusted data and artificial,warming at airports. It has no basis at all in reality.
Australia’s eSafety Commissioner Complains About X Reinstating Censored Accounts
By Didi Rankovic | Reclaim The Net | January 12, 2024
Without considering the possibility that there were perhaps too many of them to begin with – Australia’s eSafety Commissioner is complaining in a new report that X, since the Musk takeover, has fired too many “safety and public policy personnel.”
Another complaint from the commissioner’s “transparency report” is about previously censored accounts getting reinstated on the platform.
The sum of the new policy, according to this Australian office – a government agency that’s “independent (but) supported by the Australian Communications and Media Authority (ACMA)” – is that X is now less capable of “tackling online hate.”
It is no wonder that these accusations are made by eSafety, considering that it has been given powers to deal with what’s described as “cyberbullying, image-based abuse, and illegal and harmful online content.”
Basing the report on information obtained from X, eSafety writes that 80 percent of “safety engineers” have been let go since October 2022 (the same figure applies to global public policy staff). Moderators working for X have fared somewhat better – still, over 50 percent of them have been fired.
Considering that these employees were doing more than simply moderating – there have been many confirmed and very controversial cases on clear censorship against content and accounts – free speech supporters are likely fine to learn these precise numbers for the first time.
However, the Australian eSafety is not, taking a negative stance toward the developments and warning that they have “implications for Australian users.”
Commissioner Julie Inman Grant is quoted in the report as saying that, “It’s almost inevitable that any social media platform will become more toxic and less safe for users if you combine significant reductions to safety and local public policy personnel with thousands of account reinstatements of previously banned users.”
About that last point – we now know that the number of banned accounts that have been allowed back on X is at this point in excess of 6,100. But, the Australian office is not even sure if these figures concern X’s operations globally or just in Australia – although eSafety “understands” the latter to be the case, and draws this understanding from media saying earlier that a total of more than 62,000 accounts have been reinstated.
The commissioner is also displeased with the fact that X did not find it necessary to place “additional scrutiny” on these accounts – banned under previous ownership, and its policies.
Low RSV Vaccine Acceptance Among Pregnant Women
By Peter A. McCullough, MD, MPH | Courageous Discourse | January 10, 2024
Vaccination during the third trimester of pregnancy is unprecedented and risky, since a vaccine induced fever could precipitate stillbirth or premature delivery of the baby. The CDC and the Bio-Pharmaceutical Complex has told young mothers they should take the risk for theoretical protection of the newborn.
As of August 30, 2023, the CDC recommends: “Vaccination for pregnant people, 1 dose of maternal RSV vaccine during weeks 32 through 36 of pregnancy, administered immediately before or during RSV season. Abrysvo is the only RSV vaccine recommended during pregnancy.” Now the CDC is reporting that only Asian women in the US have topped 10% on the respiratory syncytial virus RSV vaccination rate while African American mothers remain the most conservative with under 5% rates of acceptance. For any mass vaccination campaign, these data would indicate a program failure. The mothers and families have been burned by genetic COVID-19 vaccines and unprecedented rates of injury, disability, and death. There is little appetite for a new vaccine during pregnancy among obstetricians, midwives, and expecting mothers.
These data on the lagging maternal RSV immunization campaign indicate that “vaccine mania” may be cooling in the United States. As a consulting internist and cardiologist, I do not recommend the new RSV vaccine for pregnant women. There are insufficient data on short and longer term safety. Theoretical protection of infants for an easily treatable illness is simply not compelling enough to risk the pregnancy altogether.
Censorship Investigation: Jim Jordan Subpoenas Director of National Intelligence Avril Haines
The agency ignored requests to hand over documents
By Dan Frieth | Reclaim The Net | January 12, 2024
House Judiciary Committee Chairman Jim Jordan has issued a subpoena to Director of National Intelligence Avril Haines. This action is part of a wider investigation by the committee into allegations that the federal government has been working in concert with Big Tech companies to suppress certain viewpoints on social media platforms. These allegations raise serious concerns about violations of First Amendment rights.
Chairman Jordan, in his communication to Haines, underscored the gravity of the situation. He cited evidence gathered by the Committee and its Select Subcommittee on the Weaponization of the Federal Government, along with other publicly available information, highlighting the federal government’s involvement in pressuring and collaborating with Big Tech and other intermediaries. This collaboration, as Jordan pointed out, has led to the censorship of specific viewpoints online, in direct opposition to the principles enshrined in the First Amendment.
We obtained a copy of the subpoena cover letter for you here.
He emphasized that the First Amendment explicitly forbids government officials from imposing restrictions on speech based on viewpoint. Moreover, he mentioned the state action doctrine, which prohibits government officials from bypassing constitutional limits by engaging private actors to do what the government itself cannot lawfully do.
“The investigative work performed by the Committee and its Select Subcommittee on the Weaponization of the Federal Government, along with other publicly available information, have revealed how the federal government has pressured and colluded with Big Tech and other intermediaries to censor certain viewpoints on social media in ways that undermine First Amendment principles,” the subpoena reads. “The First Amendment prohibits government officials from imposing viewpoint-based restrictions on speech. State action doctrine prohibits government officials from circumventing constitutional strictures by using private actors—whether through coercion, encouragement, entwinement, or joint participation—to accomplish what the government cannot directly.”
According to a press release from Chairman Jordan, in an ongoing investigation, the ODNI has come under scrutiny for not providing documents requested by the Committee, despite repeated efforts for voluntary cooperation. This is what has sparked the need for a subpoena.
The Committee’s request encompasses records concerning the activities of the ODNI’s Foreign Malign Influence Center, which, according to publicly available information, should be within the scope of their inquiry.
Additionally, the Committee has acquired documents indicating that ODNI personnel were participants in meetings with major social media companies and various federal government agencies. These gatherings, commonly referred to as “USG-Industry Sync” meetings, are of particular interest to the Committee. Despite these revelations, the ODNI has not yet submitted any records related to these meetings or any other related sessions, raising questions about their responsiveness and transparency in this matter.
The Embarrassing Pause In Arctic Sea Ice Loss Has Lasted 17 Years, Defying IPCC, NSIDC Predictions
By Kenneth Richard | No Tricks Zone | January 8, 2024
“[S]ince the dramatical decline of the ice extent in 2007, the summer Arctic sea ice area has not declined further.” – Astrup Jensen, 2023
Scientists have been using the year 2007 as the starting point for assessing Arctic sea ice trends for nearly a decade. A 2015 study published in Nature Climate Change reported a “near-zero trend” in summer sea ice over the 7 years from 2007-2013.

Image Source: Swart et al., 2015 (full paper)
Another 10 years have now passed and there is still no evidence of a further decline in sea ice.
This is interesting because since late 2007 scientists have predicted Arctic sea ice would decline rapidly as CO2 continued rising – from 385 ppm in 2007 to 422 ppm today. There were 20 models referenced by the IPCC (AR4) projecting a 40% loss of sea ice by 2050 due to an allegedly enhance greenhouse effect associated with anthropogenic CO2 emissions.
But a new study reveals there’s been no declining trend in summer sea ice area over the last 17 years, and “no apparent correlation” between CO2 and sea ice trends.
“The Arctic Sea ice extent is measured by satellites and varies by day, month and year, and the yearly minimum ice extent will occur in a day of September month every year. The ice extent is much lower now (2023) than in 1978, when the satellite measurements began. However, it has not been a gradual decline. A major decline happened during the years 1997 – 2007. Before that the decline was minimal and after that period, there was no significant downward trend.”
“These data show that there is no apparent correlation between the variable extent of the Arctic and the Antarctic Sea ice and the gradually increasing CO2-concentrations in the atmosphere as proposed by NSIDC, IPCC and others, also for these areas of cold climate.”
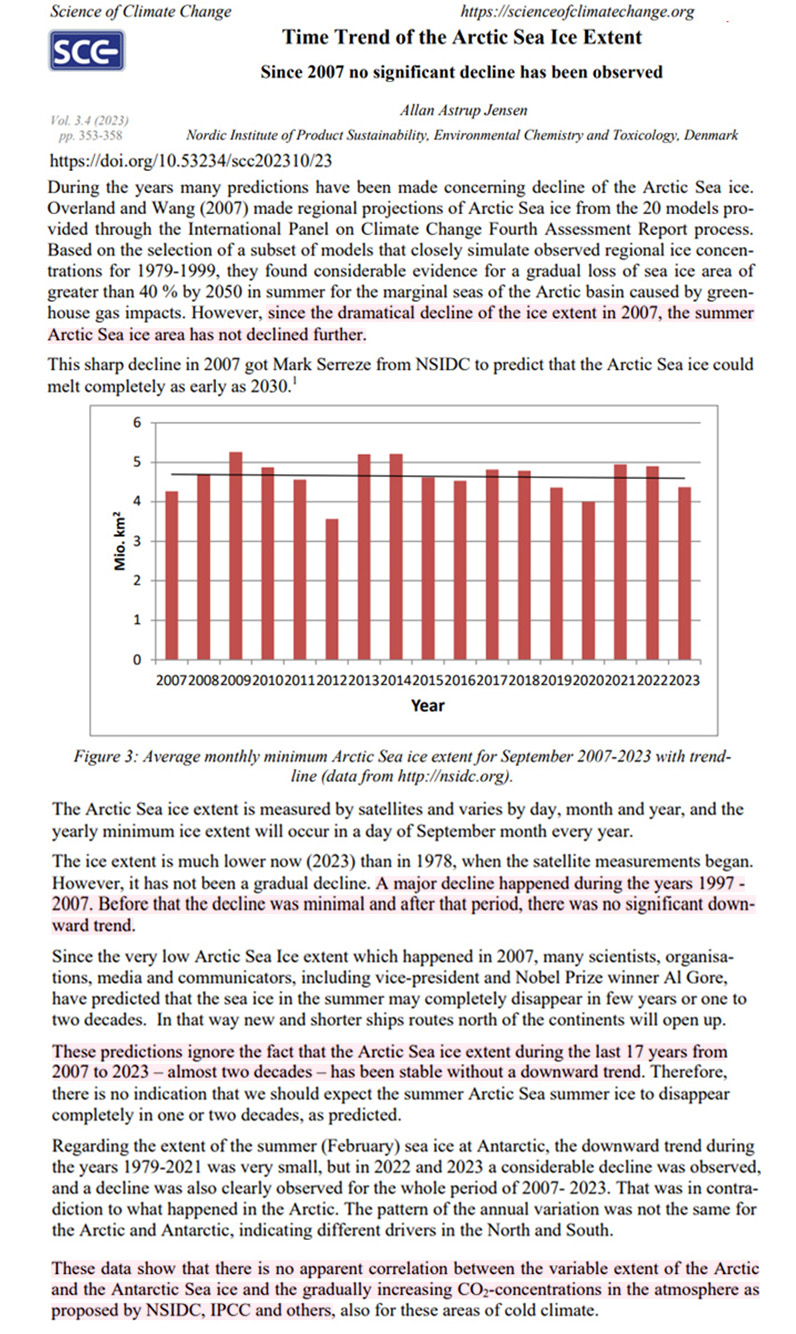
Image Source: Astrup Jensen, 2023
The Definition of Insanity
AARP: “Keep getting boosters even though previous ones didn’t work.”
BY JOHN LEAKE | COURAGEOUS DISCOURSE | JANUARY 9, 2024
This morning someone sent me a link to Alex Berenson’s post about the AARP advising its nearly 38 million members to get another COVID-19 booster shot, even if they have already had five boosters.
This prompted me to visit AARP’s website, which features an entire category of content titled Scams & Fraud—that is, warnings to older people about all the predators out there who wish to manipulate and deceive them in order to steal their money.
Under the category Caregiving is posted an articled titled COVID-19 Nursing Home Deaths Climb Ahead of Expected Winter Surge.
The article laments that nursing home residents and staff have lost interest in getting the latest booster, and suggests this is a likely explanation for why COVID-19 mortality in nursing homes has risen in recent months as we head into winter.
The author, Emily Paulin, does NOT mention the common experience of older people repeatedly falling ill with COVID-19 even after receiving multiple boosters. She also doesn’t mention a word about TREATING nursing home residents who fall ill with COVID-19. Four years after this mess began, an AARP writer about nursing home policy still has nothing to say about treating the illness.
Reading this article reminded me of a Joe Rogan podcast I watched yesterday in which his guest—an earnest and callow young man who says “like” every fourth word—asserts the following two propositions:
1). Most popular sports were conceived and developed to give men an advantage over women. For example, in basketball, “the way the ball moves” gives biological males an advantage.
2). Biological males who receive gender reassignment procedures to become women have NO advantage over women in sports.
The same kind of insanity is also evident among the foreign policy crowd that continues to advocate the war in Ukraine. No matter how many hundreds of thousands of Ukrainians are run into the meat grinder of Russian defensive positions in the eastern part of the country, these lunatics continue to insist that the Ukrainians KEEP DOING THIS until they get their desired result.
All of the above is further evidence of the mental illness underlying what I call the Holy Quadripartitus of Piffle:
1). COVID-19 vaccines are saving mankind. Anyone who questions the safety and efficacy of the vaccines is guilty of heresy.
2). The U.S. proxy war in Ukraine is a sacred mission and NO negotiated settlement with Russia shall be countenanced. Anyone who criticizes the Ukrainian and U.S. governments, and any attempt to understand the war from the Russian point of view, is guilty of heresy. Indeed, as Ukraine’s American, transgender military spokeswoman asserted back in September, journalists who question this article of faith should be hunted down and killed.
3). Human induced climate change will soon destroy the earth if trillions aren’t spent to overhaul our entire energy policy. Anyone who questions this proposition is guilty of heresy.
4). The concept of biological sex is a mere “construct.” Skilled surgeons and endocrinologists can transform a boy into a girl or vice versa. Anyone who questions this assertion is guilty of heresy.
For my part, I have lost all patience with people who subscribe to the Holy Quadripartitus of Piffle. In my view, they have become indistinguishable from sleep-deprived children. There is no sense in trying to have a conversation or reason with them. I can only hope that their insane assertions and conduct will ultimately be rejected by the great majority of adults in the United States and the rest of the world.
CDC study concludes most young children hospitalized for COVID were unvaccinated — after enrolling 7 times as many unvaxed kids in study
By Angelo DePalma, Ph.D. and Karl Jablonowski, Ph.D. | The Defender | January 9, 2024
A U.S. government-sponsored study published late last month in The Pediatric Infectious Disease Journal reported that most young children hospitalized for acute COVID-19 had not received an mRNA COVID-19 vaccination and were sicker to begin with than vaccinated children.
The authors’ conclusions are true on the surface, but their analysis ignored that more than 7 times as many unvaccinated as vaccinated children were enrolled in their study.
Only 4.5% of trial subjects completed primary COVID series
Investigators led by Laura Zambrano, Ph.D., a Centers for Disease Control and Prevention epidemiologist, recruited 597 children ages 8 months through under age 5 hospitalized for COVID-19 at 28 U.S. pediatric hospitals between Sept. 20, 2022, and May 31, 2023.
Unvaccinated subjects outnumbered subjects who had received at least one COVID-19 shot by 528 to 69, a more than 7-fold difference.
Children were grouped by demographic factors such as race, sex and geographic location, vaccination status (no vaccine, incomplete vaccine series or fully vaccinated) and underlying non-COVID-19 illnesses, or comorbidities.
Only 4.5% of the subjects had completed their primary COVID-19 vaccination series and 7% had received at least one dose.
Cases varied widely in severity, with 174 (29.1% of all subjects) admitted to intensive care and 75 progressing to life-threatening illness.
Fifty-one (8.5% of all subjects) required life support via invasive mechanical ventilation, and three required extracorporeal membrane oxygenation, a life-support treatment involving a heart-lung machine.
Based on results from both vaccinated and unvaccinated groups, infants 8 months to under age 2 were more vulnerable to serious outcomes than children ages 2 to 4 years.
For example, the youngest subjects had more life-threatening illnesses and the greatest need for high-level respiratory support involving vasoactive infusions — intravenous treatments to maintain normal blood pressure and heart rate. Yet they also had shorter hospital stays.
Investigators concluded that most children hospitalized for COVID-19, including most children with underlying medical conditions, were unvaccinated. On that basis, they called for “strategies to reduce barriers to vaccine access among young children.”
Researchers tested kids for COVID but not other respiratory infections
Zambrano et al. also compared the Pfizer mRNA shot to the Moderna product. They found that children who took the Moderna product were somewhat more likely to experience a serious outcome, however, the numbers from both groups were small and the authors did not subject them to statistical analysis.
Based on their analysis they also calculated and reported, in their “results” section, that mRNA COVID-19 vaccines were 40% effective in reducing serious outcomes. However, in their discussion (several sections later), they admitted that “vaccine coverage in this population was too low to evaluate vaccine effectiveness.”
There were two notable limitations to the Zambrano study. Even though the researchers recruited children who were only partially vaccinated the study’s design excluded children who had received any vaccination fewer than 14 days before hospital admission. Therefore no short-term post-vaccination adverse events were included.
Another limitation was that children were tested for COVID-19 but not for all possible respiratory infections, meaning “it is possible that RSV [respiratory syncytial virus], human metapneumovirus or other respiratory viral co-detections influenced disease severity.”
Media parroted authors’ conclusions
U.S. media (for example here and here) picked up on the Zambrano paper and repeated its conclusion that most hospitalized COVID-19 pediatric patients were unvaccinated — ignoring that the study included more than 7 times as many unvaccinated as vaccinated subjects.
A deeper dive into the data reveals the extent of this error and the discrepancies between what Zambrano et al. reported and what they saw.
Tables 1 and 2 illustrate what the authors got wrong.

These calculations say nothing about the relative outcomes for vaccinated and unvaccinated children because Zambrano et al. either did not perform the relevant calculation — number of cases in each group divided by the number of subjects — or chose not to report the results it generated.
Instead of presenting the number of subjects experiencing the indicated outcome as a percentage of vaccinated or unvaccinated groups, they reported them as a percentage of all subjects experiencing that outcome. Since there were 7 times as many unvaccinated as vaccinated subjects, this approach all but guaranteed the numbers among the unvaxed would be higher.
Here’s an analogy: In a hypothetical study comparing 10 coffee drinkers to 100 abstainers, five drinkers and 10 abstainers reported feeling nervous. Using Zambrano’s logic, 67% of people feeling nervous were abstainers, and just 33% drank coffee. This “proves,” according to Zambrano’s logic, that not drinking coffee doubles (67% vs. 33%) the risk of getting the jitters.
The correct way to view this data is that 10 in 100 abstainers, or 10%, felt jittery but 5 in 10 (50%) of coffee drinkers felt jittery, and that drinking coffee raises the risk of nervousness fivefold (50% vs. 10%).
Table 2 uses the same raw data as Table 1. But instead of reporting vaccinated and unvaccinated data as a percentage of all data, it first calculates the occurrence of these conditions or outcomes in each group and compares the inter-group differences.

Hospital stays were also on average one day shorter for the unvaccinated. The only area where unvaccinated children faired slightly worse was in underlying cardiac issues, but the authors did not address this small difference in their discussion.
Previous study used same tactic
A study preceding the Zambrano paper by three weeks used the same tactic to arrive at the same conclusion.
Tannis et al. compared many of the same outcomes as Zambrano in 6,337 unvaccinated and 281 vaccinated children ages 6 months to under 5 years.
All subjects had visited emergency departments for acute respiratory illness from July 2022 to September 2023.
By coincidence, Tannis also calculated vaccine effectiveness to be 40%.
Table 3 presents data from Tannis et al. with percentages reported by Tannis (Tannis %) and the actual values (Actual %).

Vaccinated children were also 68.3% more likely to harbor HCoV, an endemic coronavirus, than the unvaccinated. Similar to SARS-CoV-2 (the COVID-19 virus), HCoV can cause serious illness in immunocompromised individuals and the elderly.
Angelo DePalma, Ph.D., is a science reporter/editor for The Defender.
Karl Jablonowski, Ph.D., holds a master’s degree in computer science and a doctorate in biomedical and health informatics. He practices data science by asking questions of databases that can reveal population-based adverse outcomes of medical interventions.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video
Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
As Hillary Clinton kisses up to Henry Kissinger, RT looks at 4 of his most heinous acts
RT | September 3, 2016
… While Clinton retains the ultimate warmongering seal, RT examines some of Kissinger’s most memorable acts… Read full article
Blog Roll
 Aletho News
Aletho News- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
- The Targeted Assassination of Studies Showing Vaccines Cause Injury
- BMJ Probe Into Excess Mortality Study Drags On for Two Years With No Resolution
- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- Strait of Hormuz closed over Israeli aggression on Lebanon
- Keir Starmer arson mysteries multiply
- IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
- If Americans Knew
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- Old Iraq war architects rise up against Trump’s Iran deal
- No Tricks Zone
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
