What to Know Before Deciding to Take The Novavax Injection
Accepting an injection of spike protein hoping it is safe or effective is absurd. Yet, many are again forced to make a decision threatening their health and ability to support their family.
By Pierre Kory, MD, MPA | August 17, 2022
A subscriber asked me to write a post about my thoughts on Novavax because she “really trusts my judgement.” Flattered, I felt like I should share what they are. So here goes.
Before any medical intervention, but especially in the case of a novel or barely tested one, a long standing practice of medical ethics is that informed consent must be obtained. The emphasis should be on the informed part and not the consent part. Note that informed consent has been one of the foundations of medical ethics, essentially an inviolable standard, or at least it used to be before this “emergency” came along where now you have pharmacists injecting children with barely a mention of the risks, “because they might be too scared to take the shot.”
Informed consent discussions are simple in structure but often complex and time-consuming to conduct. It relies on providing the patient with as detailed and comprehensive a knowledge of the risks, benefits, and alternatives to the intervention.
So, should we go through an informed consent discussion with the novel Novavax injection? Actually, I would not. Why? Because I don’t hold informed consent discussions for interventions I do not recommend or would not want my patient to consider. I instead tell them not to consider and give them my reasons for that recommendation. Thus, I only conduct informed consent discussion for interventions that I feel would bring about greater benefits than risks (generally much greater), and I would only do so for patients with active illness in order to get them better. A vaccine is a much different proposition as they are given to patients without disease.
Why would I not even consider Novavax as a reasonable option? Simple:
- There has never been a successful or safe coronavirus vaccine. The last 18 months have shown that COVID vaccines lead to increased chances of getting ill, equal or increased chances of transmitting, and higher likelihood of entering hospital and dying. And that is leaving unmentioned the lethality and toxicity of the mRNA platform ones. See my “Vaccine Exemption Letter” post for the data to support these statements. The coronavirus is a rapidly mutating virus, thus vaccines will always be non-neutralizing because by the time they are manufactured and ready for injection, the virus has mutated into forms poorly responsive to older, narrower antibodies.
- Novavax is still formulated with a two and a half year-old protein for this rapidly mutagenic coronavirus, so it would be like giving a two and a half year old flu shot for this years flu (worse actually). Yet our health system, including every single academic medical center in the country is still mandating and eager to adopt use of an outdated viral protein. I would love to say this is beyond belief, but this is the world we live in now.
- We now have the omicron variant circulating, which is generally well tolerated by most, particularly those who are healthy or young (and even the old), and especially those with natural immunity.
- The country now has abundant natural immunity, which even the CDC now admits offers equal protection (actually, natural immunity offers better protection but let’s give the CDC some credit for telling at least a partial truth). So why are we still vaccinating and/or mandating in those who have recovered from COVID?
- Vaccinating against respiratory viruses works very poorly as the antibodies do not reach high concentrations in the nasal and respiratory mucosa which is where the virus enters. The flu vaccine is almost completely ineffective, even when you get this years flu shot. Not known by most.
- Vaccinating against respiratory viruses with non-neutralizing vaccines actually weakens and warps the immune system such that you are more likely to get other respiratory viruses or illnesses as well (this has been well reported after flu vaccinations given that those vaccinated against the flu are more susceptible to other respiratory viral infections).
- Proposing a novel and barely tested product coming out of the pharmaceutical industry to a patient is a wicked proposition in modern times. Note the pharmaceutical industry is a documented criminal industry which has repeatedly put out unsafe and ineffective products (even deadly, i.e opioids, Avandia, Vioxx, Bextra, the list goes on), followed by burying the adverse event data while pushing their wares through control of professional societies, federal/state legislation, and captured agencies. They have paid over $12 billion in criminal fines and over $16 billion in civil fines, just in the last 20 years across the 20 largest settlements. Their history of these actions stretches even longer.
- The history of criminality around the COVID vaccines dwarfs any actions the industry has done in the past. The Pfizer documents that the PFDA (the P is not a typo) tried to hide for 75 years reveal insane amounts of manipulations to try to show they work and are safe. They didn’t and weren’t. Further the testimony from the Ventavia/Pfizer whistleblower Brook Jackson reveals that the studies were so poorly done with such little follow-up of patients that they are simply not credible. Remember, Pharma. Does. Not. Care. About. Your. Health. Just your wallet (actually the government’s wallet, which I suppose is also your wallet).
So, conceptually, I think the idea of getting any coronavirus vaccine at this point is preposterous. However, let’s try to do a more traditional informed consent using the structure of risks/benefits/alternatives. The following is what I think other providers (or pharmacists egads) should be telling people prior to offering them Novavax, or more accurately, in order to get them to avoid it.
Yes, Novavax is a “non-mRNA” vaccine and is designed more along the line of a traditional vaccine in that an amount of viral protein is injected into the arm, it is then recognized as a “foreign” protein by our immune system which then makes antibodies against it. These antibodies are then thought (“hoped” remember) to help clear the virus rapidly and efficiently after exposure such that we avoid illness. Sounds good on paper. Not. Just ask Geert Vanden Bossche, one of the worlds top immunologists and vaccine experts.
RISKS
Novavax delivers the spike protein. As a self-described clinical expert in spike-protein induced disease, the spike protein is a pathogen. A pathogen is a substance or organism that is capable of inducing illness. Note that I call myself an expert because there are very few of us out here studying it’s pathogenicity, however I would argue Professor Paul Marik has taken the lead across the globe in amassing all the basic science and clinical research underlying the knowledge of the mechanisms and treatments of spike-protein induced diseases. That scholarly document is in evolution, and has over 300 scientific references at this point, with rapid evolutions and additions each week. Note that it appears to be the world’s sole “comprehensive” scholarly work on spike protein pathogenicity and empirically proposed treatments.
Another great sadness about the US COVID response is that almost the entire health system and all of academia have yet to recognize the spike as a pathogen or formulate any approach to treating Long-Haul or Post-Vaccine Injury. Until they do, they will continue to fail to recognize the causes or mechanisms of these syndromes as well as to offer effective treatments. And, it goes without saying, they will not be able to discuss this in thier ill-informed consent discussions. Their deplorable failure at treating these disabling diseases is astounding and will continue for the foreseeable future. Remember, the system docs won’t treat because they are all members of the Church of RCT Fundamentalism (a.k.a “evidence based medicine.”) You know, where they will sit there paralyzed until some massive randomized controlled trial is published in a high-impact medical journal and then is recommended by a federal agency or national medical society. You know what that system produces by now if you read my Substack. Not only will it leave patients untreated for months to years, but while the docs sit around waiting, Pharma, via the agencies and media, will suppress or attack any generic medicines or supplements that front-line doctors and patients have found effective. They will do this with ferocity and depravity until such a time they can “save the day” with the massive promotion of a novel, pricey Big Pharma pill which they will get our government to pay for at a price they set. Think about what happened to ivermectin and hydroxychloroquine until Pharma saved the day with the pathetic and poisonous Paxlovid using our government coffers. Rinse repeat here.
The two major and complex diseases unleashed by the spike are what we call “long haul” and “post-vaccine injury” syndromes. I probably should differentiate post-vaccine into two subtypes, with one being an acute, sudden death syndrome caused by massive heart attacks, myocarditis (which can cause lethal arrhythmias or pump failure), and/or massive strokes. Excess mortality amongst the vaccinated in 2021 skyrocketed and is showing up in Life Insurance industry data in both the U.S and other countries. However I don’t see those events in my practice because they are sudden deaths occurring in asymptomatic patients (who are often swimming or running or doing something else fun until they suddenly drop dead). My practice instead sees patients who suffer with the more chronic subtype consisting of myriad, disabling symptoms across multiple organ systems. Now, whether there is enough spike in Novavax to produce similar deadly events or chronic syndromes in the future, who knows. More on that below.
SHORT TERM RISK DATA
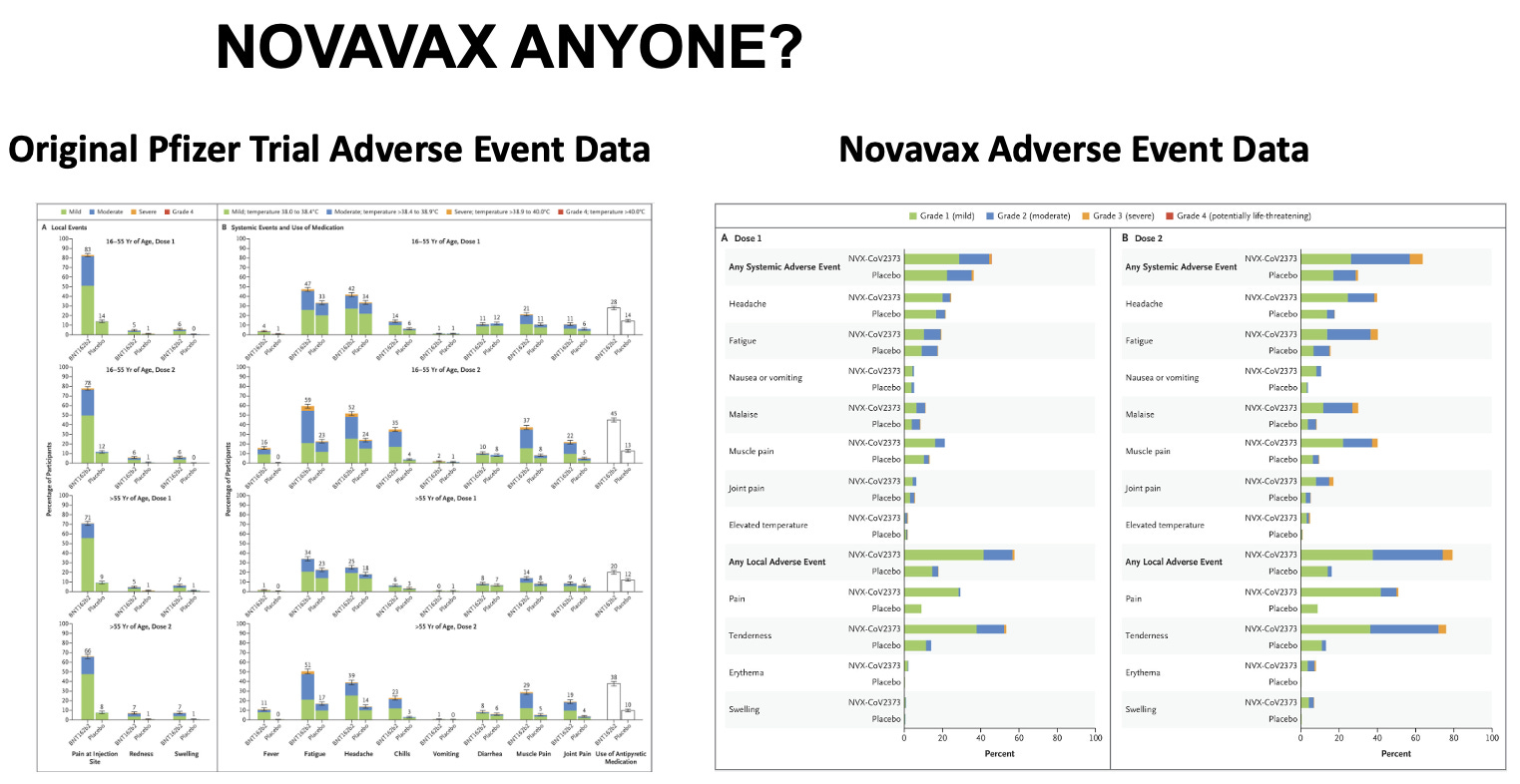
Not looking good here folks. Let’s take a look at the actual published trial of Novavax, and their chart detailing the “side effects.” Then let’s compare it to Pfizers mRNA “vaccine” trial published in December 2020. Look carefully. I will interpret these charts below.
Click for full size
Here is how I interpret the data:
- The “local” and “systemic” adverse events are absurdly high in both. I remember thinking back in December 2020 when I was reading the Pfizer trial, I said to myself, “Wow, that does NOT look friendly!” Not just the wickedly high frequency of really sore arms with redness and swelling, but the very high rates of “systemic symptoms” of fatigue, headache, chills, vomiting, muscle pain. Very high rates of those. Ouch.
- Next, look at the “dose response,” meaning look at the incidence of adverse events after the 2nd shot compared to the 1st shot. If it is higher after the 2nd, it indicates a “dose-response relationship,” which, when we are talking about a therapeutic, is a pillar of evidence to support the efficacy of the drug. For instance, ivermectin in COVID has a strong dose response relationship, meaning the higher the dose, the more effective it is (that is why all the high impact trials tried as much as they could to limit the dose of ivermectin, in particular during history’s most fraudulent trial called the TOGETHER trial).
Conversely, a dose-response in terms of side effects is a pillar of the measure of toxicity. The more you give, the sicker you get. Not cool. Now take a look at Pfizers published chart above, keeping in mind, these are only the short term systemic side effects.
- Pfizer: fatigue goes from 47% after the 1st to 59% after the 2nd in young folks and 34% up to 51% in older folks. Chills: 14% to 35% in young, 6% to 23% in old. Same pattern and increases with muscle pains and also joint pains and use of anti-pyretic medications.
- Now, take a look at Novavax. Note how they don’t give you the numeral percentages and instead make you crane your neck and use a ruler to estimate the actual incidences and increases. But just looking at the height of the bars from shot 1 to shot 2 and the increases in the yellow at the tops of the bars (yellow = “Grade 3” reactions – i.e. more severe), you see again what looks like a scary shot to me with some of the local and systemic events reported even higher than with Pfizer’s mRNA shot! So, is Novavax safer?
LONG TERM SIDE EFFECTS. Unknown. Remember the famous, “I guess we will just have to give it to see how safe it is” by one of the nations top vaccine experts. I swear, again, and I say this often, you just cannot make this stuff up. So, an informed consent discussion should relate that long term side effects are unknown. Remember as well, we are not in a supposed “emergency” anymore, despite the fact our government keeps renewing its emergency powers. If the person conducting this discussion tries to argue that in terms of long term effects, it is safe and effective because the mRNA vaccines were safe and effective, that is so categorically ridiculous it does not even bare addressing. Again, read my “Vaccine Exemption Letter” post for the data on toxicity and lethality of those vaccines. Do not proceed. My caution would be that spike protein is a pathogen with sequences that we know generate antibodies that then are capable of attacking many tissues (what are called autoantibodies which cause a category of diseases called “auto-immune” diseases). Also, spike protein, when broken down by the body is known to generate amyloid like fragments which are highly thrombogenic (i.e. cause clotting). Spike protein also stimulates immune cells called monocytes and macrophages which disturb numerous organ functions. Spike protein is also toxic to mitochondria which are the energy producing parts of each cell. In summary, don’t sign up for any more spike protein than is already circulating in the world.
Also, Novavax, like the mRNA vaccines uses “nanoparticles” in a “saponin-based adjuvant” solution which is novel and proprietary, patented only in 2020. Well, thats reassuring no? Their published paper states that the adjuvant and the vaccine was found to be “safe and immunogenic” in Phase 1 and 2 trials. Then I found this in the supplementary appendix from one of the earlier trials, ”the mechanism of Matrix-M1 (the adjuvant) is not well defined, but it has been associated with a potent induction of leukocyte activation and migration into the draining lymph nodes in their previous study.” Not reassuring.
EFFICACY
Unknown, but likely ineffective as it has not been tested against Omicron, or any of its sub-variants or whatever future variant will be circulating when it rolls out. Plus, as we know now, all the predicted efficacy reported from COVID-19 vaccine trials were never observed in the real-world, again likely due to trial shenanigans and data manipulations and removal and/or miscategorization of those who fell ill during the trial or simply due to the fact the virus is rapidly mutating. Even if it were effective, we know from the past two years, it would be short lived. I again have to mention natural immunity. It already protects against severe disease and reasonably well from re-infection, and there is no credible data to suggest adding an even older spike protein vaccine using a newly patented adjuvant will better protect you or make you healthier.
ALTERNATIVES TO VACCINATION
For readers of my Substack, you all know that you can always just skip the vaccine and instead just rely on early treatment which has been shown to be near perfectly effective in achieving rapid recovery and avoidance of hospitalization and death, especially when given in synergistic combinations like the FLCCC’s or the AAPS’s protocols. In fact, as you know, no vaccine would ever get an EUA or approval if effective treatments were available. Further, there are now over three dozen effective treatments supported by controlled trials, with many of them repurposed and/or over the counter. I suppose you could also just rely on Paxlovid given its demonstration of such incredible efficacy in treating President Biden and Dr. Fauci.
Hope this helps.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S. I am getting professional help (hah!) to write a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:

RNA for Moderna’s Omicron Booster Manufactured by CIA-Linked Company
BY WHITNEY WEBB |
UNLIMITED HANGOUT| AUGUST 17, 2022
Since late last year, messenger RNA for Moderna’s COVID-19 vaccines, including its recently reformulated Omicron booster, has been exclusively manufactured by a little known company with significant ties to US intelligence.
Earlier this week, the United Kingdom became the first country to approve Moderna’s reformulated version of its COVID-19 vaccine, which claims to provide protection against both the original form of the virus and the significantly less lethal but more transmissible Omicron variant. The product was approved by the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) with the support of the UK government’s Commission on Human Medicines.
Described by UK officials as a “sharpened tool” in the nation’s continued vaccination campaign, the reformulated vaccine combines the previously approved COVID-19 vaccine with a “vaccine candidate” targeting the Omicron variant BA.1. That vaccine candidate has never been previously approved and has not been the subject of independent study. The MHRA approved the vaccine based on a single, incomplete human trial currently being conducted by Moderna. The company promoted incomplete data from that trial in company press releases in June and July. The study has yet to be published in a medical journal or peer reviewed. No concerns have been raised by any regulatory agency, including the MHRA, regarding Moderna’s past history of engaging in suspect and likely illegal activity in past product trials, including for its original COVID-19 vaccine.
The approval comes shortly before several Western countries, including the UK, plan to conduct a massive COVID-19 booster vaccination campaign this fall. Moderna has also noted that approval for its Omicron booster vaccine are pending in the US, EU, Australia and Canada – all of which are also planning fall vaccination campaigns focused on COVID-19. The company’s CEO, Stéphane Bancel, has called the reformulated vaccine “our lead candidate for a Fall 2022 booster.”

Moderna CEO Stéphane Bancel, Source: ClockworkOrange
However, unlike the company’s original COVID-19 vaccine, the genetic material, or messenger RNA (mRNA), for this new vaccine, including the newly formulated genetic material meant to provide protection against the Omicron variant, is being manufactured, not by Moderna, but by a relatively new company that has received hardly any media attention, despite its overt links to US intelligence. Last September, it was quietly announced that a company called National Resilience (often referred to simply as Resilience) would begin manufacturing the mRNA for Moderna COVID-19 vaccine products. Under the terms of the multi-year agreement, “Resilience will produce mRNA for the Moderna COVID-19 vaccine at its facility in Mississauga, Ontario, for distribution worldwide.”
“Reinventing Biomanufacturing”
National Resilience was founded relatively recently, in November 2020, and describes itself as “a manufacturing and technology company dedicated to broadening access to complex medicines and protecting biopharmaceutical supply chains against disruption.” It has since been building “a sustainable network of high-tech, end-to-end manufacturing solutions with the aim to ensure the medicines of today and tomorrow can be made quickly, safely, and at scale.” It further plans to “reinvent biomanufacturing” and “democratize access to medicines,” namely gene therapies, experimental vaccines and other “medicines of tomorrow.”
In pursuit of those goals, the company announced it would “actively invest in developing powerful new technologies to manufacture complex medicines that are defining the future of therapeutics, including cell and gene therapies, viral vectors, vaccines, and proteins.” It was founded with the reported intention “to build a better system for manufacturing complex medicines to fight deadly diseases” as a way to improve post-COVID “pandemic preparedness.”
The company initially marketed its manufacturing capabilities as “the Resilience platform”, and offers principally “RNA Modalities”, including RNA development for vaccines, gene editing and therapeutics; and “Virus Production”, including viral vectors, oncolytic viruses (i.e. a virus engineered to preferentially attack cancer cells), viruses for use in vaccine development and gene-edited viruses for unspecified purposes. It is worth noting that, to date, many controversial “gain-of-function” experiments have justified modifying viruses for the same purposes as described by National Resilience’s Virus Production capabilities. In addition, National Resilience offers product formulations and other modalities, such as biologics and cell therapies, to its clientele and the “Virus Production” of its website has since been removed.

Resilience CEO Rahul Singhvi, Source: Resilience
National Resilience, being such a young company, has very few clients and there is little publicly available information on its manufacturing capabilities aside from the company’s website. The firm only acquired its first commercial manufacturing plant in March 2021, located in Boston, MA and purchased from Sanofi, followed shortly thereafter by the acquisition of another separate plant located in Mississauga, Ontario, Canada. Makeovers were announced for the plants, but little is publicly known about their progress. Prior to the acquisitions, the company had been subleasing a Bay area facility in Fremont, California. Reporters were puzzled at the time as to why a company with roughly 700 employees at the time had acquired a total of 599,00 square feet of manufacturing space after having only emerged from stealth less than 6 months prior.
In April 2021, National Resilience acquired Ology Bioservices Inc., which had received a $37 million contract from the US military the previous November to develop an advanced anti-COVID-19 monoclonal antibody treatment. This acquisition also provided National Resilience with its first Biosafety Level 3 (BSL-3) laboratory and the ability to manufacture cell and gene therapies, live viral vaccines and vectors and oncolytic viruses.
Despite being in the earliest stages of developing its “revolutionary” manufacturing capabilities, National Resilience entered into a partnership with the Government of Canada in July of last year. Per that agreement, the Canadian government plans to invest CAD 199.2 million (about $154.9 million) into National Resilience’s Ontario-based subsidiary, Resilience Biotechnologies Inc. Most of those funds are destined for use in expanding the Ontario facility that Resilience acquired last March and which is now manufacturing the mRNA for Moderna’s COVID-19 products. Canada’s Minister of Innovation, Science and Industry, François-Philippe Champagne, asserted at the time that the investment would “build future pandemic preparedness” and help “to grow Canada’s life science ecosystem as an engine for our economic recovery.” More recently, in 2022, the company has announced a few new clients – Takeda, Opus Genetics and the US Department of Defense.
According to National Resilience’s executives, the company’s ambitions apparently go far beyond manufacturing RNA and viruses. For instance, Resilience CEO Rahul Singhvi has claimed that the company is seeking to build “the world’s most advanced biopharmaceutical manufacturing ecosystem.” Yet, Singhvi has declined to offer much in the way of specifics when it comes to exactly how the company plans to become the planet’s most elite biomanufacturing company.
In an interview with The San Francisco Business Times, Singhvi states that Resilience is looking to fill its massive manufacturing plants with “technologies and people that can set and apply new standards for manufacturing cell therapies and gene therapies as well as RNA-based treatments.” Prior to Resilience, Singhvi was CEO of NovaVax and an operating partner at Flagship Pioneering, which played a major role in the creation and rise of Moderna.
Singhvi has further insisted that National Resilience is “not a therapeutics company, not a contractor and not a tools company” and instead aims “to boost production using the new therapeutic modalities” such as RNA-based treatments, which have become normalized in the COVID-19 era. Whereas contract manufacturers “are like kitchens, with pots and pans ready for any recipe,” “what we’re trying to do is fix the recipes,” Singhvi has explained. One member of Resilience’s board of directors, former FDA Commissioner and Pfizer Board member Scott Gottlieb, has described the company as seeking to act as the equivalent of Amazon Web Services for the biotechnology industry.
Essentially, Resilience bills itself as offering solutions that will allow “futuristic” medicines, including mRNA vaccines, to be produced more quickly and more efficiently, with the apparent goal of monopolizing certain parts of the biomanufacturing process. It also appears poised to become the manufacturer of choice for mRNA vaccines and experimental therapeutics in the event of a future pandemic, which some public health “philanthropists” like Bill Gates have said is imminent.
Perhaps the company’s most noteworthy ambition relates to their claims that they support clients through the government regulatory process. Given the company’s emphasis on speedy mass production of experimental gene therapies, its stated intention of getting the “futuristic” medical products it manufactures to market as quickly as possible seems at odds with the slower, traditional regulatory processes. Indeed, one could easily argue that the approvals of mRNA vaccines for the first time in human history during the COVID-19 crisis were only possible because of the major relaxing of regulatory procedurse and safety testing due to the perceived urgency of the situation.
Resilience seems intent on seeing that phenomenon repeat itself. As previously mentioned, the company claims to allow for the setting and application of “new standards for manufacturing cell therapies and gene therapies” and also says it plans to become a “technology-aggregating standards bearer that helps therapies come to market more efficiently.” It previously offered on its website “regulatory support” and “strategy consulting” to clients, suggesting that it would seek to mediate between clients and government regulators in order to fulfill its goal of having the products it manufactures taken to market more quickly. In addition, upon launch, the company claimed it planned to obtain unspecified “regulatory capabilities.” If so, it is certainly notable that former top Food and Drug Administration (FDA) officials are either on the company’s board or, as will be noted shortly, played a major role in the company’s creation.
The People Behind Resilience
Resilience was co-founded by Biotech venture capitalist Robert Nelsen, who is known for listening “to science’s earliest whispers, even when data are too early for just about anyone else.” Nelsen was one of the earliest investors in Illumina, a California-based gene-sequencing hardware and software giant that is believed to currently dominate the field of genomics. As mentioned in a previous Unlimited Hangout investigation, Illumina is closely tied to the DARPA-equivalent of the Wellcome Trust known as Wellcome Leap, which is also focused on “futuristic” and transhumanist “medicines.” Nelsen is now chairman of National Resilience’s board, which is a “Who’s Who” of big players from the US National Security State, Big Pharma and Pharma-related “philanthropy.”

Bob Nelsen of ARCH Venture Partners, Source: ARCH Venture Partners
However, while Nelsen has been given much of the credit for creating Resilience, he revealed in one interview that the idea for the company had actually come from someone else – Luciana Borio. In July of last year, Nelsen revealed that it was while talking to Borio about “her work running pandemic preparedness on the NSC [National Security Council]” that had “helped lead to the launch of Nelsen’s $800 million biologics manufacturing startup Resilience.”
At the time of their conversation, Borio was the vice president of In-Q-tel, the venture capital arm of the CIA that has been used since its creation in the early 2000s to found a number of companies, many of which act as Agency fronts. Prior to In-Q-Tel, she served as director for medical and biodefense preparedness at the National Security Council during the Trump administration and had previously been the acting chief scientist at the FDA from 2015 to 2017.
Borio is currently a senior fellow for global health at the Council on Foreign Relations, a consultant to Goldman Sachs, a member of the Bill Gates-funded vaccine alliance CEPI, and a partner at Nelsen’s venture capital firm ARCH Venture Partners, which funds Resilience. Nelsen’s ARCH previously funded Nanosys, the company of the controversial scientist Charles Lieber. Around the time of her conversation with Nelsen that led to Resilience’s creation, Borio was co-writing a policy paper for the Johns Hopkins Center for Health Security that recommended linking COVID-19 vaccination status with food stamp programs and rent assistance as a possible means of coercing certain populations to take the experimental vaccine.
Borio is hardly Resilience’s only In-Q-Tel connection, as the CEO of In-Q-Tel, Chris Darby, sits on the company’s board of directors. Darby is also on the board of directors of the CIA Officers Memorial Foundation. Darby was also recently a member of the National Security Commission on Artificial Intelligence (NSCAI), where members of the military, intelligence community and Silicon Valley’s top firms argued for the need to reduce the use of “legacy systems” in favor of AI-focused alternatives as a national security imperative. Among those “legacy systems” identified by the NSCAI were in-person doctor visits and even receiving medical care from a human doctor, as opposed to an AI “doctor.” The NSCAI also argued for the removal of “regulatory barriers” that prevent these new technologies from replacing “legacy systems.”

Resilience Board Member Drew Oetting, Source: 8VC
Another notable board member, in discussing Resilience’s intelligence ties, is Drew Oetting. Oetting works for Cerberus Capital Management, the firm headed by Steve Feinberg who previously led the President’s Intelligence Advisory Board under the Trump administration. Cerberus is notably the parent company of DynCorp, a controversial US national security contractor tied to numerous scandals, including scandals related to sex trafficking in conflict zones. Oetting is also part of the CIA-linked Thorn NGO ostensibly focused on tackling child trafficking that was the subject of a previous Unlimited Hangout investigation.
Oetting is also the co-founder of 8VC, a venture capital firm that is one of the main investors in Resilience. 8VC’s other co-founder is Joe Lonsdale and Oetting “started his career” as Lonsdale’s chief of staff. Lonsdale is the co-founder, alongside Peter Thiel and Alex Karp, of Palantir, a CIA front company and intelligence contractor that is the successor to DARPA’s controversial Total Information Awareness (TIA) mass surveillance and data-mining program. In addition, Oetting previously worked for Bill Gates’ investment fund.
Also worth noting is the presence of Joseph Robert Kerrey, former US Senator for Nebraska and a former member of the conflict-of-interest-ridden 9/11 Commission, on Resilience’s board. Kerrey is currently managing director of Allen & Co., a New York investment banking firm which has hosted an annual “summer camp for billionaires” since 1983. Allen & Co. has long been a major player in networks where organized crime and intelligence intersect, and is mentioned repeatedly throughout my upcoming book One Nation Under Blackmail. For instance, Charles and Herbert Allen, who ran the firm for decades, had considerable business dealings with organized crime kingpins and frontmen for notorious gangsters like Meyer Lansky, particularly in the Bahamas. They were also business partners of Leslie Wexner’s mentors A. Alfred Taubman and Max Fisher as well as associates of Earl Brian, one of the architects of the PROMIS software scandal – which saw organized crime and intelligence networks cooperate to steal and then compromise the PROMIS software for blackmail and clandestine intelligence-gathering purposes. Allen & Co. was a major investor in Brian’s business interests in the technology industry that Brian used in attempts to bankrupt the developers of PROMIS, Inslaw Inc. and to market versions of PROMIS that had been compromised first by Israeli intelligence and, later, the CIA.
In addition to these intelligence-linked individuals, the rest of Resilience’s board includes the former CEO of the Bill & Melinda Gates Foundation, Susan Desmond-Hellmann; former FDA Commissioner and Pfizer board member, Scott Gottlieb; two former executives at Johnson & Johnson; former president and CEO of Teva Pharmaceuticals North American branch, George Barrett; CalTech professor and board member of Alphabet (i.e. Google) and Illumina, Frances Arnold; former executive at Genentech and Merck, Patrick Yang; and Resilience CEO Rahul Singhvi.
To Boost or Not to Boost
It is certainly telling that the normally publicity hungry Moderna has said so little about its partnership with Resilience and that Resilience, despite its ambitious plans, has also avoided the media limelight. Considering Moderna’s history and Resilience’s connections, there may be more to this partnership that meets the eye and concerned members of the public would do well to keep a very close eye on Resilience, its partnerships, and the products it is manufacturing.
Given that we now live in a world where government regulatory decisions on the approval of medicines are increasingly influenced by corporate press releases and normal regulatory procedures have fallen by the wayside for being too “slow,” there is likely to be little scrutiny of the genetic material that Resilience produces for the “medicines of tomorrow.” This seems to be already true for Moderna’s recently retooled COVID-19 vaccine, as there has been no independent examination of the new genetic sequence of mRNA used in the Omicron-specific vaccine candidate or its effects on the human body in the short, medium or long term. For those who are skeptical of the outsized role that intelligence-linked companies are playing in the attempted technological “revolution” in the medical field, it is best to consider Resilience’s role in the upcoming fall vaccination campaign and in future pandemic and public health scenarios before trying its “futuristic” products.
Whitney Webb has been a professional writer, researcher and journalist since 2016. She has written for several websites and, from 2017 to 2020, was a staff writer and senior investigative reporter for Mint Press News. She currently writes for The Last American Vagabond.
Government employee offered euthanasia to veteran struggling with PTSD

By Thomas Lambert | The Counter Signal | August 16, 2022
Sources at Veterans Affairs Canada said one employee casually offered euthanasia to a CAF veteran struggling with a brain injury and PTSD.
Speaking to Global News, several sources from VAC say that the offer to provide “medical assistance in dying” (MAID), which is effectively euthanasia, was entirely unprovoked.
The veteran never brought up MAID, and he and his family “were disgusted by the conversation and feel betrayed by the agency mandated to assist veterans,” reports Global News.
Sources say that the veteran had been improving both physically and mentally following a traumatic brain injury received while serving in the line of duty and that the casual offer to be euthanized has impeded his progress.
Veterans Affairs Canada has since issued an apology for the employee’s behaviour.
“VAC deeply regrets what transpired,” VAC wrote in a statement, adding that MAID was discussed “inappropriately,” and the organization plans to take “appropriate administrative action.”
The most recent report from Health Canada on MAID has revealed that death from MAID has skyrocketed since being made legal in 2016 and constituted 3.3% of all deaths (10,064) in Canada in 2021.
As noted by University of Toronto Law professor Trudo Lemmens, the incidents of MAID “is rising remarkably fast.”
He also noted several times when those dealing with issues relating to poverty and non-terminal were offered MAID as a solution to their ailments, which should never happen under the current guidelines for offering and approving MAID.
Veterans now say they’re concerned about VAC members offering MAID to struggling veterans, especially considering that veterans are already at higher risk of suicide. Thus, an offer of MAID may be seized upon when other care could be provided.
Keira Bell: My Story

After a landmark court ruling in December, the name “Keira Bell” was cited worldwide, admiringly by some, with hostility by others. (Photo: Paul Cooper/Shutterstock)
By Keira Bell | April 7, 2021
From the earliest days, my home life was unhappy. My parents—a white Englishwoman and a black American who got together while he was in Britain with the U.S. Air Force—divorced when I was about 5. My mother, who was on welfare, descended into alcoholism and mental illness. Although my father remained in England, he was emotionally distant to me and my younger sister.
I was a classic tomboy, which was one of the healthier parts of my early life in Letchworth, a town of about 30,000 people, an hour outside London. Early in childhood, I was accepted by the boys—I dressed in typically boy clothing and was athletic. I never had an issue with my gender; it wasn’t on my mind.
(Courtesy: Keira Bell)
Then puberty hit, and everything changed for the worse. A lot of teenagers, especially girls, have a hard time with puberty, but I didn’t know this. I thought I was the only one who hated how my hips and breasts were growing. Then my periods started, and they were disabling. I was often in pain and drained of energy.
Also, I could no longer pass as “one of the boys,” so lost my community of male friends. But I didn’t feel I really belonged with the girls either. My mother’s alcoholism had gotten so bad that I didn’t want to bring friends home. Eventually, I had no friends to invite. I became more alienated and solitary. I had been moving a lot too, and I had to start over at different schools, which compounded my problems.
By the time I was 14, I was severely depressed and had given up: I stopped going to school; I stopped going outside. I just stayed in my room, avoiding my mother, playing video games, getting lost in my favorite music, and surfing the internet.
Something else was happening: I became attracted to girls. I had never had a positive association with the term “lesbian” or the idea that two girls could be in a relationship. This made me wonder if there was something inherently wrong with me. Around this time, out of the blue, my mother asked if I wanted to be a boy, something that hadn’t even crossed my mind. I then found some websites about females transitioning to male. Shortly after, I moved in with my father and his then-partner. She asked me the same question my mother had. I told her that I thought I was a boy and that I wanted to become one.
As I look back, I see how everything led me to conclude it would be best if I stopped becoming a woman. My thinking was that, if I took hormones, I’d grow taller and wouldn’t look much different from biological men.
I began seeing a psychologist through the National Health Service, or NHS. When I was 15—because I kept insisting that I wanted to be a boy—I was referred to the Gender Identity Development Service, at the Tavistock and Portman clinic in London. There, I was diagnosed with gender dysphoria, which is psychological distress because of a mismatch between your biological sex and your perceived gender identity.
By the time I got to the Tavistock, I was adamant that I needed to transition. It was the kind of brash assertion that’s typical of teenagers. What was really going on was that I was a girl insecure in my body who had experienced parental abandonment, felt alienated from my peers, suffered from anxiety and depression, and struggled with my sexual orientation.
After a series of superficial conversations with social workers, I was put on puberty blockers at age 16. A year later, I was receiving testosterone shots. When 20, I had a double mastectomy. By then, I appeared to have a more masculine build, as well as a man’s voice, a man’s beard, and a man’s name: Quincy, after Quincy Jones.

(Courtesy: Keira Bell)
But the further my transition went, the more I realized that I wasn’t a man, and never would be. We are told these days that when someone presents with gender dysphoria, this reflects a person’s “real” or “true” self, that the desire to change genders is set. But this was not the case for me. As I matured, I recognized that gender dysphoria was a symptom of my overall misery, not its cause.
Five years after beginning my medical transition to becoming male, I began the process of detransitioning. A lot of trans men talk about how you can’t cry with a high dose of testosterone in your body, and this affected me too: I couldn’t release my emotions. One of the first signs that I was becoming Keira again was that—thankfully, at last—I was able to cry. And I had a lot to cry about.
The consequences of what happened to me have been profound: possible infertility, loss of my breasts and inability to breastfeed, atrophied genitals, a permanently changed voice, facial hair. When I was seen at the Tavistock clinic, I had so many issues that it was comforting to think I really had only one that needed solving: I was a male in a female body. But it was the job of the professionals to consider all my co-morbidities, not just to affirm my naïve hope that everything could be solved with hormones and surgery.
Last year, I became a claimant against the Tavistock and Portman NHS Foundation Trust in a judicial-review case, which allows petitioners in Britain to bring action against a public body they deem to have violated its legal duties. Few judicial reviews get anywhere; only a fraction obtain a full hearing. But ours did, with a panel of three High Court judges considering whether youths under treatment at the clinic could meaningfully consent to such medical interventions.
Bell in January 2020, after she brought legal action against the clinic. (Photo: Sam Tobin/PA Wire)
My team argued that the Tavistock had failed to protect young patients who sought its services, and that—instead of careful, individualized treatment—the clinic had conducted what amounted to uncontrolled experiments on us. Last December, we won a unanimous verdict. The judges expressed serious doubts that the clinic’s youngest patients could understand the implications of what amounted to experimental treatment with life-altering outcomes.
In their ruling, the judges repeatedly expressed surprise at what had been going on at the Tavistock, particularly its failure to gather basic data on its patients. They noted the lack of evidence for putting children as young as 10 years old on drugs to block puberty, a treatment that is almost universally followed by cross-sex hormones, which must be taken for life to maintain the transition. They also had concerns about the lack of follow-up data, given “the experimental nature of the treatment and the profound impact that it has.”
Notably, a growing wave of girls has been seeking treatment for gender dysphoria. In 2009-10, 77 children were referred to the Gender Identity Development Service, 52% of whom were boys. That ratio started to reverse a few years later as the overall number of referrals soared. In England in 2018-19, 624 boys were referred and 1,740 girls, or 74% of the total. Over half of referrals were for those aged 14 or under; some were as young as 3 years old. The court noted the practitioners at the Tavistock did not put forward “any clinical explanation” for the dramatic rise in girls, and expressed surprise at its failure to collate data on the age of patients when they began puberty blockers.
The ruling does not completely prevent a minor from beginning a medical transition. But the judges recommended that doctors consider getting court permission before starting such treatment for those 16 to 17; they concluded it was “very doubtful” that patients aged 14 and 15 could have sufficient understanding of the consequences of the treatment to give consent; and that it was “highly unlikely” for those aged 13 and under.
In response, the NHS said that the Tavistock had “immediately suspended new referrals for puberty blockers and cross-sex hormones for the under-16s, which in future will only be permitted where a court specifically authorizes it.” The Tavistock appealed the ruling, and the court will hear its appeal in June.
The puberty blockers that I received at 16 were designed to stop my sexual maturation: The idea was that this would give me a “pause” to think about whether I wanted to continue to a further gender transition. This so-called “pause” put me into what felt like menopause, with hot flushes, night sweats, and brain fog. All this made it more difficult to think clearly about what I should do.
By the end of a year of this treatment, when I was presented with the option of moving on to testosterone, I jumped at it—I wanted to feel like a young man, not an old woman. I was eager for the shots to start, and the changes this would bring. At first, the testosterone gave me a big boost in confidence. One of the earliest effects was that my voice dropped, which made me feel more commanding.
Over the next couple of years, my voice deepened further, my beard came in, and my fat redistributed. I continued to wear my breast binder every day, especially now that I was completely passing as male, but it was painful and obstructed my breathing. By the time I was 20, I was being treated at the adult clinic. The testosterone and the binder affected the appearance of my breasts, and I hated them even more. I also wanted to align my face and my body, so got a referral for a double mastectomy.
My relationship with my parents continued to be difficult. I was no longer speaking to my mother. My father had kicked me out of his apartment shortly after I turned 17, and I went to live in a youth hostel. He and I were still in touch, though he was adamantly opposed to my transition. Reluctantly, he took me for the surgery. I was a legal adult when it took place, and I don’t relieve myself of responsibility. But I had been put on a pathway—puberty blockers to testosterone to surgery—when I was a troubled teen. As a result of the surgery, there’s nerve damage to my chest, and I don’t have sensation the way I used to. If I am able to have children, I will never breastfeed them.
Around the end of that first year post-surgery, something started happening: My brain was maturing. I thought about how I’d gotten where I was, and gave myself questions to contemplate. A big one was: “What makes me a man?”
I started realizing how many flaws there had been in my thought process, and how they had interacted with claims about gender that are increasingly found in the larger culture and that have been adopted at the Tavistock. I remembered my idea as a 14-year-old, that hormones and surgery would turn me into someone who appeared to be a man. Now, I was that person. But I recognized that I was very physically different from men. Living as a trans man helped me acknowledge that I was still a woman.
I also started to see what I was living out was based on stereotypes, that I was trying to assume the narrow identity of “masculine guy.” It was all making less and less sense. I was also concerned about the effect my transition would have on my ability to find a sexual partner.
Then there was the fact that no one really knew the long-term effects of the treatment. For instance, the puberty blockers and testosterone caused me to have to deal with vaginal atrophy, a thinning and fragility of the vaginal walls that normally occurs after menopause. I started feeling really bad about myself again.
I decided to stop, cold turkey. When I was due for my next testosterone shot, I canceled the appointment.
After I came to this decision, I found a subreddit for detransitioners. The number of people on it started rising, as if all these young women had come to a collective realization of the medical scandal we had been a part of. It was a place we could talk about our experiences and support each other. I felt liberated.
What happened to me is happening across the Western world. Little of my case was a surprise to those paying attention to the Tavistock whistle-blowers who in recent years have spoken out in alarm to the media, sometimes anonymously. Some have left the service because of these concerns. But the transgender issue is now highly political and wrapped up in questions of identity politics. It can be perilous to raise questions or doubts about young people’s medical gender transitions. Some who have done so have been vilified and had their careers threatened.
At the Tavistock, practitioners provide “gender affirmative care”—in practice, this means that when children and teens declare a desire to transition, their assertions are typically accepted as conclusive. Affirmative care is being adopted as a model in many places. In 2018, the American Academy of Pediatrics released a policy statement on the treatment of young people who identify as transgender and gender diverse that advocated for “gender-affirmative care.”
But former Tavistock practitioners have cited varied problems suffered by the kids who sought help, such as sexual abuse, trauma, parental abandonment, homophobia in the family or at school, depression, anxiety, being on the autism spectrum, having ADHD. These profound issues, and how they might be tied up with feelings of dysphoria, have often been ignored in favor of making transition the all-purpose solution.
As the High Court found, much of the clinic’s treatment is not even based on solid evidence. At the time our case was accepted, the NHS was asserting that the effects of puberty blockers are “fully reversible.” But recently, the NHS reversed itself, acknowledging “that ‘little is known about the long-term side-effects’ on a teenager’s body or brain.” That didn’t stop them from prescribing these drugs to people like me.
Dr. Christopher Gillberg, a professor of child and adolescent psychiatry at Gothenburg University in Sweden and a specialist in autism, was an expert witness for our case. Gillberg said in his court statement that over his 45 years of treating children with autism, it was rare to have patients with gender dysphoria—but their numbers started exploding in 2013, and most were biological girls. Gillberg told the court that what was happening at the Tavistock was a “live experiment” on children and adolescents.
Parents who are reluctant or even alarmed about starting their children on a medical transition may be warned, “Would you rather have a dead daughter or a live son?” (Or vice versa.) I had suicidal thoughts as a teen. Suicidal thoughts indicate serious mental health problems that need assessment and proper care. When I told them at the Tavistock about these thoughts, that became another reason to put me on hormones quickly to improve my well-being. But after the court ruling, the Tavistock released an internal study of a group of 44 patients who had started taking puberty blockers at ages 12 to 15. It said that this treatment had failed to improve the mental state of patients, having “no significant effect on their psychological function, thoughts of self-harm, or body image.” Additionally, of those 44 patients, 43 went on to cross-sex hormones. This suggests blocking puberty isn’t providing a pause. It is giving a push.
Before beginning on testosterone, I was asked if I wanted children, or if I wanted to consider freezing my eggs because of the possibility that transition would make me infertile. As a teenager, I couldn’t imagine having kids, and the procedure wouldn’t have been covered by the NHS. I said I was fine if I couldn’t, and I didn’t need to freeze my eggs. But now as a young adult, I see that I didn’t truly understand back then the implications of infertility. Having children is a basic right, and I don’t know if that has been taken from me.
As part of its defense, the Tavistock put forth statements from a few young trans people who are happy with their care. One is S, a 13-year-old trans boy who got puberty blockers from a private provider because the waiting list at the Gender Identity Development Service was so long. S told the court that he had “no idea what me in the future is going to think” about being able to have children and that since he has never been in “a romantic relationship,” the idea of one is not “on my radar at the moment.”
Lots of teenagers, when contemplating future sexual relationships, feel baffled and even disturbed at the thought. Those same people, when adults, often feel very differently. I know, because this happened to me. I’d never been in a sexual relationship at the time of my transition, so I didn’t truly understand what the transition would mean sexually.
S’s statement demonstrates how difficult it is for minors to give consent for procedures they can’t yet understand. As the judges wrote, “There is no age-appropriate way to explain to many of these children what losing their fertility or full sexual function may mean to them in later years.”

Bell speaking to the media after the court ruling last December. (Photo: Sam Tobin/PA Wire)
Today, at 24, I’m in my first serious relationship. My partner is very supportive of everything I do, and I am the same for her. She has a large group of female friends who accept me; it’s been very healing. For now, I don’t speak to either of my parents or have a relationship with them.
I still get taken for male sometimes. I expect that, and I’m not angry about it. I know that I will live with that for the rest of my life. What I am angry about is how my body was changed at such a young age. People want to know if I’m going to have reconstructive surgery of my breasts or do other things to make me look more female. But I haven’t fully processed the surgery I had to remove my breasts. For now, I want to avoid more such surgical procedures.
When I joined the case, I didn’t realize how big it would become. What has happened since the ruling has been a rollercoaster. Many people have thanked me. I have also been attacked online. If you’re someone who regrets transitioning and decides to speak out about your experiences, you’re considered a bigot. You may be told that you’re trying to take away trans rights, that children know what’s best for themselves and their bodies, and that you’re ruining kids’ lives.
But I am focused on what is best for distressed young people. A lot of girls are transitioning because they’re in pain, whether it’s from mental-health disorders, or life trauma, or other reasons. I know what it’s like to get caught up in dreaming that transitioning will fix all of this.
Although sharing my story has been cathartic, I still struggle, and have yet to receive appropriate therapy. As I go on with my life, I plan to continue to be an activist on behalf of this cause. I want the message of cases like mine to help protect other kids from taking a mistaken path. This year, I helped create the first Detrans Awareness Day, on March 12. I hope that, in years to come, this day can be a beacon to empower others.
I do not believe in rigid gender expression. People should be comfortable and feel accepted if they explore different ways of presenting themselves. As I said in my statement after the ruling, this means stopping the homophobia, the misogyny, and the bullying of those who are different.
I also call on professionals and clinicians to create better mental health services and models to help those dealing with gender dysphoria. I do not want any other young person who is distressed, confused, and lonely as I was to be driven to conclude transition is the only possible answer.
I was an unhappy girl who needed help. Instead, I was treated like an experiment.
Featured Video

Israel furious at Trump over Turkey, Syria to invade Lebanon
or go to
Aletho News Archives – Video-Images
From the Archives
Bum Rap for the Rapa Nui
By Thomas Riggins | Dissident Voice | February 5, 2014
A new report in Science News Magazine (1-25-2014) by Bruce Bower details a reevaluation of the view that the Rapa Nuians, the native inhabitants of Easter Island (Rapa Nui), were responsible for the collapse of their population and society due to over exploitation of natural resources and the destruction of the rain forest on their island, a view recently popularized by Jared Diamond in his book Collapse (2005).
As Bower reports, the anthropologist Maria Mulrooney has published the results of her studies of the Rapa Nui culture (Journal of Archeological Science, December 2013) based on new radiocarbon dates from archeological sites on the island. She has concluded that after the clear cutting of the forest in the 1500s, to make room for agricultural production, the population of Rapa Nui remained sufficiently vibrant to carry on food production and continue their cultural development.
Exactly when the Rapa Nui arrived on Easter Island is unknown but it was on or before 1200 A.D. or so. Mulrooney maintains they had a thriving culture which was still going strong even after their “discovery” by the Dutch explorer Jacob Roggeveen on Easter Sunday 1722. This would indicate that they had not suffered “collapse” as a result of forest clearance. … continue
Blog Roll
 Aletho News
Aletho News- Israeli occupation forces advance in southern Lebanese towns after truce deal with Beirut
- Abelardo De la Espriella’s Victory Renews Pressure on Venezuela
- Israel furious at Trump over Turkey, Syria to invade Lebanon – w/ Col. Macgregor
- IRGC says it struck US military positions, warns of broader response
- Russia stops record number of Ukrainian drones overnight – MOD
- Denmark admits ‘no evidence’ for Russian drone hysteria
- Washington agreement ‘will not pass’: MP Fadlallah
- Iran mocks US for ‘solving’ domestic hunger problem, lecturing others on issue
- Germany, Israel hold joint naval drill off Haifa amid Gaza genocide
- Trump’s war on Iran becomes ‘most unpopular conflict’ in US history
- If Americans Knew
- Israel kills Gaza’s public servants again – this time it’s police – Daily Update
- Four Reasons the Netanyahu-Backed Plan to ‘End’ U.S. Military Aid to Israel Is a Scam
- Archbishop of Canterbury vows to help Palestinians achieve ‘freedom you deserve,’ calls for end to Israeli occupation
- The scars left behind by Israel’s white phosphorus in Lebanon
- Drones and decomposing babies: What’s in UN report on Israel’s genocide of Palestinian children
- Crimson Thread: The new Israeli separation wall that cuts through the ‘breadbasket of Palestine’
- Gaza ceasefire talks back to square one as Israel changes the rules – Daily Update
- The NDAA Proposed Merger of the U.S. and Israeli Military is Strategically Unwise and Inherently Unconstitutional
- Victories by Pro-Palestinian Democrats Show the Party’s Shift on Israel
- Massie moves to strike $3.3B in Israel military aid from the budget
- No Tricks Zone
- Lousy Station Siting: Swirling Controversy Surrorunds Germany’s Latest “New Alltime Record High” Temperature
- 2025 Study: Cloud Effects Reduce Downwelling Longwave Radiation, Overriding The CO2 Impact
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
