In 2015 a team of researchers employed by the medical services of the US military published a peer-reviewed paper on the incidence of myocarditis and pericarditis after smallpox vaccination (SPX) and vaccination with an inactivated trivalent influenza vaccine (TIV).
Despite being published 7 years ago before anyone had heard of “covid”, the findings in this study could have very significant implications for the Covid-19 mRNA injections.
In this study, the researchers found that:
When active surveillance systems are used, significantly more myocarditis cases were identified than in earlier studies which had relied on more passive reporting.
The incidence of cases of possible myocarditis without symptoms – detected by testing all subjects vaccinated regardless of symptoms – was far higher than the cases in which subjects developed symptoms such that they would seek medical help.
Given these observations, it seems highly likely that the incidence rates of myocarditis following Covid vaccination have to date been severely underestimated.
The background to the study was that the US military rolled out a limited program of SPX following a perceived threat that smallpox might be used as a weapon in a bioterrorism incident. By the time of the paper’s publication, >2m doses had been administered, but the US had 290m doses in reserve to use for the general population if required. Concerns had been raised about a possible risk of myocarditis after this vaccination. This study sought to quantify these risks.
Key aspects of the study design:
Subjects were selected from previously healthy military personnel presenting for either SPX (1081 subjects) or TIV (189 subjects). A battery of baseline tests were performed and these were repeated either once or twice 5-8 days after vaccination and / or 9-28 after vaccination.
The notable difference between this and other studies assessing myocarditis and pericarditis rates was that the assessments were performed on all subjects and they included measurements of cardiac troponin levels (a protein which is released by damaged heart muscle cells) and ECG, in an attempt to detect possible “subclinical” cases of myocarditis – ie those which did not result in symptoms and so ordinarily would not gain the attention of healthcare systems.
Clinical myocarditis and pericarditis were determined according to published epidemiological case definitions that require the development of new onset cardiac symptoms soon after vaccine exposure, and each case was confirmed by an independent adjudicator.
Possible subclinical myocarditis and pericarditis were diagnosed whenever troponin levels rose by or to a certain level[1], or by ECG changes respectively, in the absence of symptoms.
Incidence rates were compared to background incidence rates calculated from a 2002 study among 1,390,352 service members (no exposure to any vaccines).
Key results:
Subjects receiving SPX were predominantly young (mean 23 years) and male (88%), those in the TIV cohort were more evenly balanced (54% male) and older (mean 36 years)
8.8% of the SPX recipients reported severe cardiac symptoms (defined as >3 out of 10 on a visual scale for at least 2 days).The most frequently reported cardiac symptoms were chest pain and dyspnea on exertion.
Despite no significant differences in pre-vaccine health self-assessment between the cohorts and fewer reported physical limitations in the SPX cohort, there was a significantly higher incidence of new onset cardiac symptom(s) post-SPX (10.6%) compared to the older post-TIV cohort (2.6%), p<0.001. These differences remained 4-5 fold higher in the SPX cohort after adjusting for group differences in age, sex, weight, race, smoking, and physical limitations, and also when symptoms were limited to consideration of those above 3 out of 10 on the visual scale.
The incidence rate of clinical myocarditis / pericarditis after SPX was 5 cases out of 1081 (4 were myocarditis and one pericarditis), equating to 463 per 100,000, which was >200 x background expected rates.
The incidence of possible subclinical myocarditis / pericarditis after SPX was 2868 per 100,000, or nearly 3%, which was 6 x the rate of clinical myocarditis.[2] This could not be compared to an expected background rate as this had never been measured before in this way.
No cases of either clinical or subclinical myocarditis were detected after TIV.
Implications.
Before going on to discuss the implications of this study for the Covid-era, it must be emphasised that “full recovery” from myocarditis is a misleading term: whilst the patients may initially become symptom-free, all should ideally receive regular cardiological follow-up to detect cardiomyopathy and / or arrhythmias later in life, and there is a significantly raised risk of cardiac morbidity and mortality.
Moreover, in several case series, for example this one published in JAMA, “Late Gadolinium Enhancement” on cardiac MRI[3] indicative of long term heart damage was found in the majority of clinical myocarditis cases which underwent detailed investigation. This finding is not consistent with mRNA-induced myocarditis having a more benign course than other forms, as was originally hoped.
For the above reasons, it is important to try to accurately capture all possible cases of myocarditis, both for the individuals concerned (so they can receive proper follow-up) and for calculating the extent of any added risks from vaccination.
In respect of the accurate detection of myocarditis cases, this study raises several important concerns relevant to the Covid injections:
Passive surveillance misses many cases.
Before this study, the rate of clinically diagnosed myocarditis / pericarditis had been previously estimated to be 16.1 cases per 100,000 in a cohort of US service members receiving smallpox vaccination, nearly 7.5-fold higher than the expected background rate of 2.16 per 100,000 observed among comparable unvaccinated service members.
The rate of clinical myocarditis observed in this SPX study was approximately 28 times higher than the previous estimate, at 463 per 100,000 – several hundred times the expected background rate. The higher incidence rate detected is almost certainly due to the active surveillance systems in place, where cases were pro-actively sought out and participants and their physicians made aware of their possibility.
As the authors state:
Prior to the present study, the incidence of myocarditis / pericarditis following smallpox vaccination was estimated from passive surveillance registries and population databases, with an inherent bias towards underestimation of disease incidence.
Myocarditis cases may be easily dismissed as musculoskeletal in origin.
Myocarditis is usually self-limiting in its acute phase, improving with self-treatment by a non-steroidal anti-inflammatory drug such as ibuprofen. It could quite easily be confused with “expected” aches and pains following injection, or with musculoskeletal injury, and this would be more frequent in the young, especially if active in sport.
The authors make the point that:
“3 of the 5 clinical cases would not have sought medical care without study interventions including enhanced education and surveillance.”
With the Covid mRNA injections, not only have we experienced a lack of active surveillance and a reliance on passive adverse event reporting, but there has been an atmosphere of discouragement of reporting. Many physicians have reported censure by hospitals or other health authorities for even discussing a possible vaccine origin for adverse events, and even subjects themselves have received opprobrium online after questioning the origin of their symptoms.
Hence, whatever factors the authors noted in 2015 in relation to underreporting of myocarditis following SPX are likely to be even more in evidence now for the Covid vaccines.
Because of this, there must be a very significant possibility that the actual numbers of clinical myocarditis cases caused by the mRNA injections have to date been very significantly underestimated.
The frequency of subclinical cases may dwarf the clinical cases.
This was actually the first study to attempt to detect possible subclinical cases of myocarditis (ie those without discernible symptoms) following vaccination. It is highly likely that, just as there is a spectrum of outcomes with symptomatic cases, such that a proportion have zero long-term problems, so with the subclinical cases an unknown proportion may well go on to have cardiac problems. Given that heart cells are irreplaceable and that scar tissue in the heart can disrupt electrical conduction the degree of concern about heart damage must be much more than with, say, damage to the skin, which can self-repair and still perform its primary function.
The actual proportion of subclinical cases which go on to manifest in cardiac disease later in life is unknown, however the authors selected a threshold for the measured troponin levels by which to define a subclinical case which is known to be associated with an increased risk of adverse outcomes. In the paper cited by the authors in support of their chosen troponin criterion it had been concluded that:
“In the general population, cTnT [troponin – protein released from heart damage] elevation is rare in subjects without CHF, LVH, CKD, or DM, [Congestive Heart Failure, Left Ventricular Hypertrophy, Chronic Kidney Disease or Diabetes Mellitus] suggesting that the upper limit of normal for the immunoassay should be <0.01 μg/L. Even minimally increased cTnT may represent subclinical cardiac injury and have important clinical implications, a hypothesis that should be tested in longitudinal outcome studies.”
*Definitions in [ ] with bold added by this author
The rate of possible subclinical myocarditis detected after SPX (3% of subjects) was 6 x the rate of symptomatic myocarditis. That these findings are or might be significant rather than chance fluctuations is supported by the fact that zero such cases were detected in the TIV cohort.
Moreover, the authors point out that even this may be an underestimate (bold added):
“While assumptions about benign troponin release from the myocardium have been made, there is a growing body of literature suggesting that even in generally healthy populations with no known cardiac disease risk, small elevations in troponin (stratified below the levels measured by the assay in this study) are associated with increased risk of all cause and cardiovascular mortality. Therefore, the rate of reported elevations in this study may actually be an underestimate of the true incidence of vaccine related subclinical myocarditis.“
There seem no reasons to suggest that possible subclinical myocarditis might not also be occurring after Covid injections, and also at higher rates than clinical cases. In fact, given the use of active surveillance for clinical cases employed in the SPX study, it is likely that the ratio between possible subclinical and reported clinical myocarditis cases for the Covid vaccines may in fact be higher than the 6-fold seen after SPX, because of the significant underreporting of clinical cases after Covid vaccines for the reasons mentioned above.
It should be stressed that little is known about the long-term prognosis of myocarditis / pericarditis, whether infective in origin or otherwise. No follow-up to the Engler et al paper (now 7 years old) measuring cardiac status in either the clinical or possible subclinical cases has been published to date.
A 2005 paper reported a well-conducted follow-up study of 67 cases detected following smallpox vaccination of 540k military personnel and found normalisation of echocardiography, ECG, and functional status (measured by ECG exercise-testing) in all subjects including those who initially had depressed cardiac function. This is encouraging, although the median follow-up period was just a few months and none were followed for more than one year after the myocarditis; hence concerns must remain regarding cardiac function in later life, especially in those in whom cardiac reserve falls secondary to other cardiac pathology such as coronary artery disease.
Concluding remarks
The authors conclude their paper with this warning:
Our study identified a rate of myocarditis/pericarditis following SPX immunization that is significantly higher than previously described, and highlights the challenges of post-licensure vaccine safety surveillance to identify adverse events that are not well understood or previously unrecognized.
Applying the incidence described in this study to a SPX immunization program that has delivered over 2 million doses, largely to young, healthy primary vaccinees, there are potentially thousands of vaccine associated cases, many undiagnosed because of self-medication or lack of provider awareness].
In our study, 3 of the 5 clinical cases would not have sought medical care without study interventions including enhanced education and surveillance. The recognition of potential adverse events following immunization requires accurate diagnosis of new onset clinical symptoms.
Our study reinforces the need, as part of all post-vaccine (and potentially new drug related) adverse events surveillance, to include specific standardized inquiry about new onset cardiac symptoms and to highlight the value of dynamic pre to post immunization cardiac troponin increases as a potential biomarker of risk in future safety surveillance studies.
Two million doses of SPX sounds a large number, but it is sobering to consider where we are today in respect of our understanding of the association of the Covid vaccines to myocarditis, having rolled out several billion doses, a program which is now continuing with 3rd or even 4th doses (whereas the incidence studies published to date have been based on 2 doses only).
It is accepted now that there is a definite association between mRNA vaccination and myocarditis, yet the precise rates of increased risks reported vary hugely between different studies, which probably reflect vastly different methodologies between investigators and countries according to prevailing local reporting standards and customs.
Moreover, initial claims that myocarditis risk might be higher after Covid infection compared to vaccination have not held up to scrutiny. The latest study – based on a large (~200k) cohort of adults in Israel – found no increase in the incidence of pericarditis or myocarditis in adult patients recovering from COVID-19.
In addition to the high, yet underreported, rates of clinical myocarditis, there remains a distinct possibility that there may have been very large numbers of subclinical myocarditis cases caused by Covid vaccines, the long-term outcomes for which are uncertain.
Approximately 3% of those receiving a single SPX vaccination met the criteria for having developed possible subclinical myocarditis, and given that billions have now received Covid mRNA products (many multiple times), if the frequency is similar to SPX the number of such cases following mRNA injections could well be in the millions.
Despite these worrying data, we have inexplicably witnessed the rollout of multiple booster doses, including in many countries to young adults and even children, despite there having been:
No active surveillance for myocarditis, only passive reporting
No prospective studies of troponin levels (which would be relatively simple to perform).
No standardised inquiries about new onset cardiac symptoms
One could be forgiven for thinking that the reason for this is that those who have relentlessly pushed this program into younger and younger people at little to no risk from Covid, simply do not want to know, and prefer to maintain a degree of “plausible deniability”.
Footnotes:
For subclinical myocarditis, the criteria for diagnosis were: the development of any one of the following: a) elevated post-vaccine levels of cTnT ≥ 0.02 ng/ml with pre-vaccine cTnT levels <0.01 ng/ml; or b) a post-vaccine cTnT level of 0.02 ng/ml greater than the pre-vaccine level based on the imprecision profiles of the assay.
The absolute subclinical cTnT elevations post SPX vaccine ranged from 0.02 to 0.24 ng/ml with the majority (n = 28, 90.3%) ranging from 0.02 to 0.07 ng/ml
This is a radiological feature seen on cardiac imaging which is indicative of myocardial damage consistent with a high risk of poor long-term prognosis.
In 2020, government orders to stay home — along with lockdown-produced job losses, public fear of COVID-19 and other factors — led to dramatic declines in in-person utilization of healthcare services among adults and children, both in the United States and globally.
“Well-baby” and “well-child” visits were some of the noteworthy casualties.
In the U.S., children’s and teen’s vaccination rates plummeted dramatically, falling that year by as much as 91% depending on the age group, including a noticeably lower uptake of diphtheria, tetanus and pertussis vaccines (DTaP or DTP), meningitis shots and human papillomavirus (HPV) vaccines.
Public health officials expected this “pandemic hangover” to dissipate by 2021, but instead, the change in parents’ vaccine-seeking behavior for their kids persisted.
Internationally, 6 million fewer children worldwide got at least one dose of DTP vaccine in 2021 versus 2019, causing the head of UNICEF to lament “the largest sustained drop in childhood immunization in a generation.”
And in the Philippines — where the president threatened to jail COVID-19 vaccine refusers — 2021’s percentage of children receiving a first DTP dose was just 57% versus 92% a decade previously.
Stateside, Washington State reported flu shot uptake in children under age 5 was down by around 25% in November 2021, compared to the two previous flu seasons. And Michigan’s state registry for March 2022 showed that 24% fewer toddlers “were considered vaccinated” compared to March 2020.
When Michigan compared its 2020 vaccination data against the 2016-2019 period, it found vaccination coverage had declined in “all milestone age cohorts, except for birth-dose hepatitis B coverage.”
At this juncture, state officials are openly speculating that COVID-19 shots — thus far rejected by the parents of 97% of under-5-year-olds — are the reason parents are increasingly ambivalent about childhood vaccination more generally.
Referring to this “spillover doubt,” a Michigander public health spokesperson said parents who once accepted childhood vaccination without question are now saying, “Wait a minute. Do I really need these vaccines?” and asking, “How are these vaccines made?”
According to another Michigan official, “vaccination” — the “V-word” — has become a “trigger word” for irate parents who believe government not only overstepped its authority during COVID-19 but is fraudulently pushing unsafe vaccines on their little ones.
Fewer babies dying is no ‘disaster’
In October 2020, three scientists from the U.S. and U.K. authored the Great Barrington Declaration and condemned — quite gloomily — the steep decline in childhood vaccination resulting from COVID-19 lockdowns.
As long-time proponents of vaccination — professionally involved in vaccine development, promotion of the dangerous HPV vaccine and accepting of COVID-19 vaccines as a solution to lockdowns — the three declaration authors positioned the decline in childhood vaccination rates at the head of their list of “disastrous” lockdown consequences.
Far from witnessing a disaster, however, observers by June 2020 had begun noticing a wonderful silver lining — a “surprising” pandemic effect on the death rate among infants, in particular, with 200-plus fewer infants dying per week, amounting to a 30% reduction in expected child deaths within a few months.
To explain the “something mysterious” saving the lives of infants, these analysts, along with Children’s Health Defense (CHD) Chief Scientific Officer Brian Hooker, pointed out how the missed infant vaccines coincided with a “precipitous drop” in reports of sudden infant death syndrome (SIDS) to the Vaccine Adverse Event Reporting System (VAERS).
SIDS deaths — which by definition affect children who are normal and healthy — and sudden unexplained deaths in children over age 1 typically occur in close temporal proximity to vaccination, with nine out of 10 SIDS deaths following two- and four-month “well-baby” visits.
An analysis of three decades of VAERS data found 75% of reported post-vaccination SIDS cases occurred within seven days of childhood shots.
Japanese pathologists who identified SIDS cases taking place within a week of vaccination agree that “suspicious cases do exist,” leading them to encourage forensic pathologists to “devote more attention to vaccination” in SIDS events.
Naturally, “fact-checkers” dispute the hypothesized association between 2020’s lower vaccination rates and the decreased deaths in young children.
Additional clues
CHD has reviewed dozens of studies showing dramatically better health in unvaccinated children while finding “no studies that show superior health outcomes in vaccinated children.”
However, because the effects of vaccination are complex, cumulative and synergistic with other toxic exposures — and because most chronic disease data sets have not yet caught up to the pandemic — it is not so easy to tease out other upsides resulting from 2020’s lower childhood vaccination rates.
There are a few clues, however.
Consider the decline in emergency department (ED) visits and the fact that the largest declines were in persons under age 15.
Ordinarily, an estimated one in seven children experiences an ED visit every year.
An analysis comparing 2020’s pediatric ED visits to ED encounters over the previous decade found “substantial” decreases for certain diagnoses — notably abdominal pain, ear infections, asthma, pneumonia, upper respiratory and urinary tract infections and trauma — while visits for diagnoses such as seizures and complications of diabetes held steadier.
Although there is no surefire way to know why ED visits declined for those specific conditions, all of the diagnoses in question show up in vaccine package inserts as post-vaccination occurrences — along with nearly 400 other acute and chronic symptoms and conditions.
Abdominal pain may not sound serious, but it can be a sign of acute pancreatitis (sudden-onset inflammation of the pancreas), so much so that clinicians advise “always” considering acute pancreatitis “in the differential diagnosis of abdominal pain in children.
And case reports are now flooding in (for example, from the U.S., Japan, Poland and New Zealand) describing severe pancreatitis in the aftermath of COVID-19 vaccination.
Moreover, acute and chronic pancreatitis began mysteriously surging in children following the childhood vaccine schedule’s expansion in the 1990s and 2000s, and juvenile diabetes and pancreatic cancers in young adults — two conditions associated with pancreatitis — began escalating soon thereafter.
COVID vaccines — a line in the sand?
Most observers attributed the sudden drop-off in routine childhood vaccination in 2020 purely to circumstance-imposed foregone care (“the gap between perceived need and actual utilization of healthcare services”).
Now, however, it is COVID-19 vaccines — and particularly the unscientific authorization of the jabs for teens and young children — that appear to be the principal reason many parents no longer “perceive a need” to rush back into the vaccine fold.
Even the propagandistic New York Timesadmitted to a hardy new contingent of vaccine “skeptics” whose questioning was forged in the crucible of COVID-19 restrictions, COVID-19 vaccine mandates and, tragically for some, a child’s adverse reaction to the COVID-19 shots.
As a physician tweeted from the “frontlines of medicine” in early August, “Parents are DONE with giving their kids any and all [syringe emoji]. Not only that but they’re disgusted with what they had already allowed to be injected into their kids. They wish they could turn back.”
Public health’s tired old strategy for recapturing these wayward parents appears to be (surprise, surprise) badgering parents to “catch up as many vaccines as possible in a single visit” — bolstered by the false claim that it is to a child’s advantage to get a bunch of shots at once — while also stoking worries about a resurgence of so-called “vaccine-preventable” illnesses.
Thus, following a single case of paralysis ascribed to “polio,” New York State is busily trying to conjure up a polio outbreak, never mentioning the decades of manipulation of the “polio” diagnosis intended to mask nonviral causes of paralysis that include vaccination and poisoning.
Florida, meanwhile, is urging college students and other groups to get meningococcal vaccines following the deaths of seven gay and bisexual men, allegedly from meningococcal disease.
Why did the deceased men develop meningitis to begin with? No one has shared information about their COVID-19 vaccination status, but researchers around the world are reporting meningitis as a post-COVID-vaccination adverse event in adolescents and adults — for example, in Japan, Singapore, Korea, Iraq, Belgium and Germany.
Meningitis also is a listed adverse event for DTaP, hepatitis A and B, influenza and MMR vaccines, and vaccines containing Haemophilus influenzae type b (Hib) and polio components.
And a 28-year-old physician who volunteered in Brazil’s clinical trials for AstraZeneca’s COVID-19 vaccine died after receiving the meningitis vaccine given to the “control group.”
What kids really need
Sadly, whatever temporary or longer-lasting silver lining may have emerged from the COVID-19-induced lull in childhood vaccination, children and their parents still face many challenges.
According to a Centers for Disease Control and Prevention study, the weight status of children and adolescents who were already overweight or obese worsened significantly during 2020, and children’s food insecurity is rising both domestically and internationally.
In addition, the massive social and behavioral changes commanded through government restrictions have prompted dire headlines about young people’s mental health — although experts caution these could counterproductively lead to overdiagnosis and overmedication with black-box-warning drugs known to cause violence and suicide.
Rather than more vaccines or drugs that have never delivered on their hype or promises, what children and youth need to thrive are the slower-but-surer public health fundamentals — such as solid nutrition, safe housing and economic security — and the loving attention of their parents.
Europe’s biggest nuclear power plant is under repeated missile attacks by the NATO-backed Kiev regime. Let that appalling fact sink in for a moment. Can anything more criminal and reckless at this time be imagined?
Bear in mind that the very governments (regimes really) responsible for this abysmal situation are the same ones who proclaim “rules-based order” and “liberal democracy”. Evidently, their rhetoric is just a sick facade for totalitarianism and lawlessness.
What is going on is nuclear terrorism by the Nazi-infested Kiev regime and its Western sponsors. The missiles hitting the Zaporozhye nuclear plant (ZNPP) are supplied by the United States and its NATO allies. The power station has been under sustained artillery or drone attack since last week. A fire at the installation has already been reported although the Russian military and the Ukrainian civilian operators at the Zaporozhye plant managed to put the blaze out. The ZNPP is reckoned to contain hundreds of tonnes of enriched uranium and other spent nuclear fuel. Situated on the mighty Dnieper River in southeast Ukraine that flows into the Black Sea, if the ZNPP is fatally hit the damage would be catastrophic for Europe and the rest of the world. The resulting radioactive contamination would far exceed that of Chernobyl or the Fukushima disaster. The world is on the brink of a deliberately orchestrated cataclysm.
UN Secretary-General Antonio Guterres and the UN international nuclear supervising agency, the IAEA, have both condemned the attacks on Zaporozhye as “suicidal”. They have appealed for demilitarization of the area. The UN is being cowardly in its restraint by not specifically condemning the NATO-weaponized Kiev regime. The UN is hiding behind cynical claims that there are “conflicting reports” of who is to blame for the shelling of the nuclear plant.
The United States and its Kiev proxy are blaming Russia for the military strikes. Displaying twisted logic, they say Russia is carrying out the attacks in order to smear the Ukrainian regime. They also claim that Russia is using the plant as a cover for its military forces.
Russian forces commandeered the Zaporozhye NPP in early March, days after they invaded Ukraine on February 24. Russia’s military operation was compelled by the relentless build-up of NATO’s offensive threat in neighboring Ukraine since the CIA coup d’état in 2014. Securing the ZNPP was a top priority given the criminal recklessness of the NATO-backed Kiev regime. Now the United States and its Kiev catspaw are absurdly making out that Russia is hitting its own forces and territory under its control, including the vitally important ZNPP.
The trajectory of missiles fired on the ZNPP clearly shows that the attacks are coming from the territory under the control of the Ukrainian forces and its NATO accomplices. The rational suspicion is that the long-range multiple-launch rocket systems supplied and overseen by the U.S., Britain and Germany are involved.
Washington and its NATO allies are calling on Russia to relinquish control of the nuclear plant and give it back to the Kiev regime.
That preposterous demand exposes who the nuclear terrorists are. The United States and its NATO axis are responsible for holding Europe and the world hostage with the threat of nuclear catastrophe.
We should note that anything claimed by the Kiev regime and its Western handlers, including the entire news media acting as propaganda outlets, cannot be taken remotely seriously. This week, the Kiev puppet president Vladimir Zelensky admitted through his aide Mikhail Podolyak that all public statements are “information warfare” designed to deceive Russia. The alleged Russian massacres at Bucha and Mariupol, allegations of mass rapes by Russian soldiers, and allegations of bombing civilians all fit into this admission of lies.
The furor over a report by Amnesty International last week blaming the Kiev regime for using civilian centers such as hospitals, schools and homes as military shields is just the tip of a very dirty iceberg. But it illustrates the depravity and corruption of the NATO-backed Kiev regime.
The risible accusations that Russia is shelling the Zaporozhye nuclear power plant as some kind of propaganda stunt betray the guilt of projecting onto others what the accusers themselves are capable of doing.
Russian forces have secured Europe’s largest nuclear power station and up to now have averted disaster by protecting it. It is Russia that summoned the UN Security Council to convene this week in an emergency session to highlight the extreme danger. Moscow is calling for demilitarization and for IAEA inspectors to be allowed access to the ZNPP in order to report the circumstances. It is the Kiev regime and its Western sponsors who are preventing those calls. The United States and its NATO axis are supplying more and more long-range missiles to Ukraine and slandering Russia with claims of “nuclear terrorism”. The U.S. axis is in effect giving a green light to the Kiev regime to continue its criminal offensive.
This week saw the 77th anniversary of the U.S. atomic bombings of Hiroshima and Nagasaki. That horror was carried out as a criminal act of state terrorism. American justifications for the crimes on August 6 and 9, 1945, have always been known – albeit not widely known due to Western media lies – to be baseless propaganda. The intended effect of the U.S. imperial regime then was to terrorize the rest of the world into submitting to its presumed global dominance.
The same abominable, lawless logic is on show again with the situation in Ukraine over the Zaporozhye nuclear plant. The United States is using its Kiev proxy to hold the world hostage to its imperial objectives.
The psychopathic gambling by the U.S. regime is heinous. Russia has warned that if its territory comes under threat it will use nuclear forces to defend itself. Nuclear war is an increasing risk. If the U.S.-sponsored Kiev regime makes a fatal blow on Zaporozhye causing untold radioactive contamination of Europe, Russia and the rest of the world, what do the Americans expect Moscow to do? Yet this madness by Washington is being pursued.
A diplomatic end to the crisis over Zaporozhye as with the general war in Ukraine is being thwarted by NATO’s militarism. The world’s foremost nuclear terrorist regime – in Washington – is playing with fire and acting as the perverse God of Death again, holding the whole world to ransom for its pernicious ends.
A simple, urgent test beckons: stop the military attacks on Zaporozhye. Now, who is objecting?
In crisis after crisis, Western narrative control kicks into overdrive to shift blame, whitewash culprits, or make sure inconvenient lines of questioning are never pursued
Soon after US House Speaker Nancy Pelosi’s recent descent on Taiwan, the Russian Foreign Ministry’s spokeswoman, Maria Zakharova, called out Nicholas Burns, America’s ambassador to China, for “keeping an embarrassed silence” regarding the “insolent stunt.”
The silence was quite a change from how vocal Burns had been a mere month prior at the World Peace Forum in Beijing, where he demanded that China stop relaying “Russian propaganda” by “accusing NATO of starting” the conflict in Ukraine. He used the opportunity to accuse the Chinese Foreign Ministry’s spokesperson of “telling lies about American bioweapons labs, which do not exist in Ukraine.”
But that was then and this is now in the West’s ‘rules-based order’, where each occasion requires a new set of rules. Thus, it goes without saying that, for the time being, Burns will also keep an ‘embarrassed silence’ about another potentially tectonic event – the latest, even more damning statement regarding alleged US-run biolabs in Ukraine made by the Russian Defense Ministry on August 4. Lieutenant-General Igor Kirillov, the head of the Nuclear, Biological and Chemical Protection Troops of the Russian Armed Forces, said Moscow was assessing the possibility of US involvement in the Covid-19 pandemic, as well as investigating US-funded research of various other pathogens.
The reason for Burns’ silence is not difficult to guess – the serious allegations made in Kirillov’s presentation, if properly investigated and proven true, could serve as an indictment of what could be America’s use of Ukraine as a vast pathogen testing ground. And since the Western media mostly chose to ignore it, the ambassador was certainly not going to make a statement they would have to quote, drawing attention to the issue. And now that Twitter has suspended the Russian Foreign Ministry’s account for daring to quote key parts of Kirillov’s media presentation about the possible origins of Covid-19, Burns and company don’t have to say anything at all. If it’s memory-holed by the social media, then it’s as if it never happened.
That’s the modus operandi of the Western elites – it’s not the truth that matters, but successfully managing the narrative so that it doesn’t leave room for doubt in people’s minds. In other words, they think they can do whatever they want.
Perhaps we should remind ourselves of the post-Cold War Western formula announced during the heady days of the early 2000s, an era marked by another famous American political quote, Karl Rove’s “we’re an empire now and, when we act, we create our own reality.” As Tony Blair’s policy adviser, Robert Cooper, nonchalantly put it on the pages of The Guardian in April 2002: “The challenge to the postmodern world is to get used to the idea of double standards. Among ourselves, we operate on the basis of laws and open cooperative security. But when dealing with more old-fashioned kinds of states outside the postmodern continent of Europe, we need to revert to the rougher methods of an earlier era – force, pre-emptive attack, deception, whatever is necessary to deal with those who still live in the 19th century world of every state for itself. Among ourselves, we keep the law but when we are operating in the jungle, we must also use the laws of the jungle.”
Two decades later, despite the rise of both China and Russia and the world’s inexorable evolution to multipolarity, imperial habits die hard – usually until they hit a wall of reality, as is currently happening in Ukraine and is bound to happen in Taiwan. But back to Burns for a moment. He’s far from new in enforcing double standards in the ‘jungle’. Before his present work on poking the Dragon regarding Taiwan, and the Bear regarding just about everything, he distinguished himself as a partisan and apologist of NATO’s illegal aggression against Serbia back in the 1990s, which resulted in Kosovo’s unilateral secession.
Meanwhile, in 2009, when he was the US under-secretary of state for political affairs, Burns explained to the media that the recognition of Pristina’s independence was in fact an expression of the US’ “interest in good relations with Serbia.” Will he, in due time, express himself similarly vis-à-vis China and Taiwan? Outside the West, it’s all still a jungle to Burns and his ilk, and the ‘natives’ are to be dealt with accordingly. So, in Burns-talk, Pelosi’s Taiwan sojourn and pledge of continuing US support for the island is actually a sign of America’s interest in good relations with China.
Another notable Anglo-American figure visible across the Kosovo-China-Ukraine crisis landscape is the Englishman Geoffrey Nice, who gained international notoriety as a prosecutor of the International Criminal Tribunal for the former Yugoslavia (ICTY), whose sole purpose was to shift the blame for the Western-inspired bloody breakup of that multinational country solely onto the Serbs. In addition to his selective prosecution of former Serbian President Slobodan Milosevic for ‘crimes against humanity’, Nice’s ICTY legacy also includes accusations of destroying evidence related to human organ trafficking in Kosovo.
Nice subsequently offered his legal services to former Kosovo President Hashim Thaci, one of the main figures in not just the trafficking but the alleged “forcible extraction” of human organs of still-living, mostly Serb prisoners, as outlined in a stunning Council of Europe 2011 report, ‘Inhuman treatment of people and illicit trafficking in human organs in Kosovo’. The report also cites anti-drug agencies of “at least five countries” as saying Thaci “exerted violent control over the trade in heroin and other narcotics.” Nice’s subsequent attempt to discredit the report was, however, brilliantly dissected and exposed by American journalist Diana Johnstone as the latest attempt by a representative of “self-righteous Western democracies” to reserve the privileges of a “culture of impunity” exclusively for themselves and their clients. Of course, the clients in the ‘jungle’ still have to pay for the imperial ‘double standards’ umbrella, so in the end, Nice reportedly accused Thaci of owing him “almost a half a million euros” for his work for the Kosovo government.
Zakharova just recently more fully described the house of horrors over which Thaci allegedly presided: “Kosovo is the territory of ‘black’ transplantation. People were dissected alive, taking out internal organs for sale to those people in the West… In the West they stood in line for organ transplant operations. And they began to receive these organs when Kosovo turned into a terrible black hole in which people disappeared, who were not just killed, but killed to sell their internal organs.”
To paraphrase Franklin D. Roosevelt’s immortal words justifying US support for Nicaraguan dictator Anastasio Somoza, they may be sons of b****es, but they’re the West’s sons of b****es.
‘We need a new plague’ was the sentiment in the early 1980s in the corridors of America’s Centers for Disease Prevention and Control (CDC), because the agency was facing closure. In his book The Real Anthony Fauci Robert F Kennedy Jr cites Dr Kary Mullis recalling the institutional desperation reflected in circulating memos which said: ‘We need to find something to scare the American people into giving us more money.’
The events which followed, and the panoply of artifices used to secure this end, became a template for amassing unbridled power over the population, the institutions, and even the White House.
Kennedy recounts that in the summer of 1981 the CDC reported that approximately 50 gay men in Los Angeles, San Francisco and New York had presented with Kaposi’s sarcoma (a skin cancer associated with immune suppression) and other immune deficiency-related health problems including a rare form of pneumonia (PCP).
As cases starting appearing in other major cities in the same cohort, the hunt was on for the cause of this new disease, dubbed Acquired Immune Deficiency Syndrome (Aids).
Responsibility for it fell under the US National Cancer Institute (NCI). In 1983 the French virologist Dr Luc Montagnier identified signals of a retrovirus in some Aids patients, which he believed could be responsible for causing the disease. Dr Robert Gallo of the NCI persuaded Montagnier to send him a sample of the virus in exchange for fast-tracking the publishing of Montagnier’s work in the journal Science.
Before doing so, Gallo cultured the sample, gave it a different name, patented an antibody kit he claimed capable of detecting it, and in April 1984 called a press conference to announce to the world that the probable cause of Aids had been found in the form of a ‘known human cancer virus’, claiming the discovery as his own. Once the announcement was made, no one could review Gallo’s work which was published subsequently.
A bitter row ensued between Montagnier and Gallo, which eventually led to an ‘accommodation’, whereby the researchers agreed to share the discovery, and the virus was given the name HIV (Human Immunodeficiency Virus).
The hypothesis that HIV caused Aids, however, had not been subject to the normal processes of independent replication, verification, dissent and rebuttal. A nascent hypothesis had been seized and hurriedly converted into accepted fact. ‘Science by announcement’ was a dangerous development which has had grave repercussions to the present day.
Robert Gallo’s overt ambition to be awarded a Nobel Prize made him a natural ally of Anthony Fauci. So once the HIV story of a worldwide lethal virus was launched, claiming the highly infectious nature of it, Fauci wrested jurisdiction for the disease away from NCI and into his moribund National Institute for Allergies and Infectious Diseases (NAID), thus capturing the flood of congressional funds that would be made available to combat it.
Many eminent scientists had misgivings about the hypothesis. Foremost was Professor Peter Duesberg, a world-respected molecular biologist. Duesberg was a consummate scientist and an applied scholar. At thirty-three, having discovered the ‘oncogene’ which appeared to cause cancer, he subjected his own theory to more rigorous tests than his critics had, and became convinced his discovery had been a lab fluke. He therefore publicly abandoned his own hypothesis, at the height of his acclaim. Colleagues praised him for his ‘integrity, his genius, his kindness and his intelligence’.
Duesberg, Kary Mullis and their school of critics believed the first generation of Aids was a complex illness which had its cause in a variety of chemicals. The profusion of recreational drugs used by the homosexual community, particularly amyl nitrate (poppers) known to cause immune suppression, in combination with the constant use of antibiotics to treat infections, were strong factors in immunity collapse. But after Robert Gallo’s April 1984 press conference Fauci moved to quash all talk of toxic causation to attribute Aids uniquely to the deadly virus.
Following Gallo’s announcement, Duesberg studied every scientific publication on HIV and Aids, and in 1987 published his observations in the journal Cancer Research. He argued that retroviruses were not, by accepted definition, a life form, and HIV was not capable of causing either cancer or Aids. Referring to the supposed indeterminate incubation period of HIV he said: ‘There are no slow viruses causing Aids, only slow scientists.’ Duesberg was committed to clean functional proof at a time when electron microscopy and other technologies for detecting new viruses were making biology – particularly the study of viruses – increasingly murky. Fame and finance were driving the frenzy in viral research. With official and commercial encouragement, researchers were blaming newly discovered viruses for an assortment of ancient diseases. Duesberg argued that the apparent high incidence of HIV-Aids in Africa was a function of the now notorious PCR to produce false diagnoses of infection, and the broad definition of Aids, which captured everything in its net from malnutrition to endemic diseases.
The second generation of Aids in the early 1990s is now widely recognised to have been caused by the poisonous drug Azidothymidine (AZT) pushed by Fauci on to ‘HIV positive cases’. AZT was developed in the 1960s as a leukaemia chemotherapy drug but abandoned when government researchers deemed it too toxic even for short-term use. Described by Joseph Sonnabend as ‘incompatible with life’, AZT randomly destroys bones, kidneys, livers, muscle tissue, the brain and the central nervous system.
After Peter Duesberg’s compelling 1987 article, which challenged point by point the basis of the HIV-Aids hypothesis, the scientific world waited for answers to Duesberg’s probing questions, but Gallo never attempted a reply. Instead Fauci moved ruthlessly to annihilate Duesberg’s voice. His stature and the respect he commanded were an existential threat to Fauci’s plans for control and grandeur through the theory of a dangerous virus.
Marshalled by Fauci, the self-interested scientific press banished Duesberg. John Maddox, editor of the journal Nature, invited Duesberg’s colleagues to slander him without fear of response, writing an editorial stating that the virologist, by his heresy, had forfeited the standard scientific practice of ‘right of reply’.
Scientific conferences disinvited Duesberg. His graduate students were warned by their university that working with him would render them irrelevant, and the fawning mass media followed the instructions handed down from on high. As the reporter Celia Farber wrote, ‘Duesberg’s problem transcended science: It was career protection to partake in his bullying and degradation. The Fauci serf scientists were driven by fear that if they did not publicly denounce Duesberg in sufficiently disgusted tones they themselves would be punished.’
In 1994 a senior geneticist, Dr Stephen O’Brien, was dispatched by the very same editor of Nature, John Maddox, to try to persuade Duesberg to change his position, in exchange for ‘reinstatement’. O’Brien rang Duesberg on the pretext of needing to speak to him urgently and the two met at the opera in San Francisco. O’Brien pulled from his pocket a paper entitled ‘HIV Causes Aids: Koch’s Postulates Fulfilled’ with his own name and that of Duesberg printed at the bottom, and begged Duesberg to sign it. To his undying credit, Duesberg refused.
Duesberg’s remarkable lack of bitterness towards his persecutors is the sign of a man at peace with his soul. It is likely that Fauci’s rancour, and the depths to which he sank to humiliate and denigrate Duesberg, sprang from a hatred of his ability and integrity, qualities Fauci could not bear to contemplate.
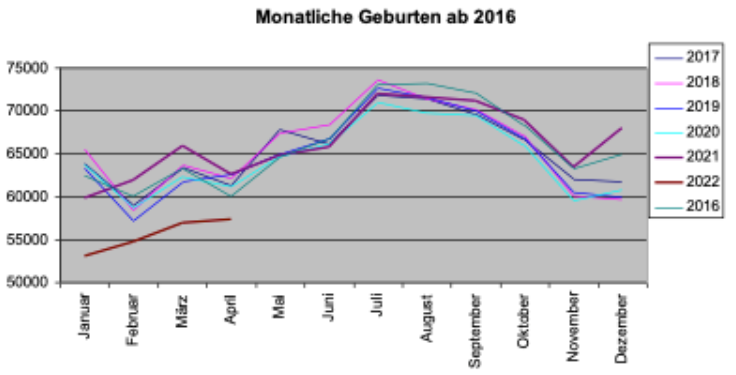
Germany has seen a “dramatic drop” in birthrate during the first 4 months of 2022, according to transitionnews.de, leading to rising suspicions over COVID vaccine safety.
“Compared to the previous year, the number of births has fallen by 12 percent – that’s about 25,000 fewer births in the first four months of 2022,” reports Sternfried Müller of transitionnews.de.
The above chart shows the number of births for the January-April period each year since 2018. During the Corona years of 2020 and 2021, Germany saw a rise in the number of births, climbing to 250,000 births. But in 2022, the number of births mysteriously plummeted a whopping 12%!
Something unusual must have triggered the phenomenon. Going back 9 months prior to the January-April 2022 period takes us to the April to July 2021 period, which coincides to COVID vaccination of younger adults in earnest. Remarkably, Germany’s media have been silent on the latest published statistics, issued by the German Federal Statistical Office (Destatis).
The next transitionnews.de chart shows the monthly number of births and just how dismally 2022 lags so far compared to the previous years:
A number of reasons have been proposed to explain the dramatic decline, among them fewer marriages. But that remains highly doubtful.
There are increasing suspicions that it is vaccine linked, as some studies already suggest: see here and here.
For the time being German authorities obstinately continue to remain in denial mode when it comes the the adverse effects of the COVID vaccines. Currently the Ministry of Health is gearing up to roll out another mass wave of vaccinations and restrictions in the run-up to the fall flu season.
A former Washington State University football coach is seeking $25 million from the university for wrongful termination after he was fired last year for refusing to get vaccinated against COVID-19, The Seattle Times reported Tuesday.
A tort claim was filed April 27 on behalf of Nick Rolovich with the state’s risk management office. Filing a claim is a prerequisite to filing a lawsuit against a state agency.
There’s a 60-day waiting period between when a claim is filed and when the claimant can file a lawsuit. As of Wednesday, a spokesperson for Attorney General Bob Ferguson said no suit had been filed, according to The Washington Post.
After denying Rolovich’s request for a religious exemption from Gov. Jay Inslee’s COVID-19 vaccine mandate for state employees, the university in October 2021 fired Rolovich.
At the time of his firing, Rolovich was subject to a five-year contract with three seasons remaining and was paid $3.2 million per year — the highest public salary in the state. He had coached 11 games with the Cougars over two seasons.
Rolovich’s attorney, Brian Fahling, said at the time his client would take legal action for religious discrimination. He filed a 34-page letter with the university appealing the university’s decision to fire Rolovich, but the appeal was denied.
Rolovich, a Catholic, is not the first person to file a claim for wrongful termination or religious discrimination over an employer’s failure to grant a religious exemption to a COVID-19 vaccine mandate.
Liberty Counsel on July 29 settled the nation’s first class action lawsuit on behalf of healthcare workers who were unlawfully discriminated against and denied religious exemptions to the COVID-19 vaccine mandate by their employer, Chicago-based NorthShore University HealthSystem.
The $10,337,500 settlement, filed in the federal Northern District Court of Illinois, compensates NorthShore employees who were “punished for their religious beliefs against taking an injection associated with aborted fetal cells.”
As part of the settlement agreement, NorthShore also will change its unlawful “no religious accommodations” policy to make it consistent with the law and must provide religious accommodations in every position across its numerous facilities.
In addition, employees who were terminated because they refused to receive a COVID-19 vaccine on religious grounds will be eligible for rehire if they apply within 90 days of the final settlement approved by the court, and they will retain their previous seniority level.
The amount of individual payments from the settlement fund will depend on how many valid and timely claim forms are submitted during the claims process.
If the settlement is approved by the court and nearly all of the affected employees file valid and timely claims, it is estimated employees who were terminated or resigned because of their religious refusal of a COVID-19 vaccine will receive approximately $25,000 each.
Also under the settlement, employees who were forced to get the shot against their religious beliefs to keep their jobs will receive approximately $3,000 each.
The 13 healthcare workers who are lead plaintiffs in the lawsuit will receive an additional approximate payment of $20,000 each for their role in bringing this lawsuit and representing the class of NorthShore healthcare workers.
Lawsuits over denied exemptions or insufficient accommodations to COVID-19 vaccine requirements began last September after the U.S. Food and Drug Administration granted full approval to the Pfizer-BioNTech Comirnaty vaccine, allowing more employers to enact vaccine mandates.
Workers as of May 19, 2022, had filed at least 66 lawsuits since September 2021 against private employers for refusing to grant exemptions to COVID-19 vaccine requirements, according to Bloomberg Law.
Judges rejected workers’ requests for immediate court orders blocking enforcement of mandates in 22 cases.
In one case involving United Airlines Inc., the airline changed its policy allowing accommodations rather than contest the lawsuit.
According to Bloomberg Law, 59% of lawsuits filed over COVID-19 vaccine mandates are related to an employer’s response to faith-based requests for accommodation.
About 22% of lawsuits involve contesting a company’s handling of both religious and disability requests and 5% involve health-related accommodations.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
I joined the Tavistock Clinic in North London as a clinical nurse therapist in 2003. Back then, Tavistock was prestigious—known all over the world for its professional seminars and specialized psychological treatments for mental-health patients. Before I ever worked there, I would attend lectures and training workshops to hear from renowned psychoanalysts, who were considered some of the best in the field.
A lot can change in a decade.
Last week, the National Health Service ordered that the gender youth clinic at Tavistock to shut its doors by next spring. And I am part of the reason why.
The story of what happened at Tavistock is the story of how a small group of whistleblowers—doctors, nurses, parents and patients, together with the help of journalists and reporters—were able to relentlessly expose activist-driven medicine that they knew was irresponsible. It’s also an object lesson for others who are deeply concerned about a one-size-fit-all approach to transgender healthcare and wonder what they should do about it.
I was delighted when I started working at Tavistock back in the early 2000s. My role as senior clinical lecturer was to devise and deliver training courses for mental-health staff. Shortly after I joined, I took on another part-time role working with children and adolescents in what was called the Gender Identity Development Service.
There were, as I recall, seven of us on the team back then. We would have clinical meetings each week in which we would discuss our referrals and caseloads. Back then we had fewer than 100 referrals per year in the entire country and they were mostly biological boys.
Sometime during my first few weeks we were discussing a newly referred patient, a 16-year-old boy with a complex history, who felt he had been born in the wrong body. My colleague took on the case. Four months later, the boy’s name came up again in the meeting, and my colleague announced that she was recommending him for puberty blockers (gonadotropin-releasing hormone agonists), which are used to suppress the further development of secondary-sex characteristics like breast tissue in females or facial hair in males. Puberty blockers are almost always followed by cross-sex hormones (testosterone or estrogen).
Usually, when new patients arrived at the service, they would come in for an hour or so once a month for the first few months. So I was surprised to hear that my coworker was recommending drugs when, in my view, no meaningful understanding of his internal world could have been reached. I knew from my experience in working with adolescents that any diagnostic assessment arrived at after such a short time span would have been superficial.
It’s worth pointing out that Tavistock specialized in therapy—talking through problems with patients—and that we did not generally prescribe drugs. For that reason, I had expected the same approach when it came to treating children and teens with gender dysphoria. But it seemed that, even back then, certain staff didn’t hesitate to recommend puberty blockers—even for vulnerable kids contending with anxiety, autism, internalized homophobia or other challenges.
I had also noticed that senior clinicians in the service would regularly meet with Mermaids, a transgender patient-advocacy group. At the time, various patient-advocacy groups were springing up alongside mental-health services so that patients would have a voice in the examination room. At first, I viewed all of this as an overdue development. But as time progressed, it seemed clear that groups like Mermaids were exerting influence over doctors and clinicians in the service—sometimes dictating the expectations of care for our patients.
One small anecdote: I was once instructed by a superior to rewrite a letter I’d written to a male patient’s referring doctor—making sure to use the patient’s chosen, female name and new pronouns. I understood the sensitivities around this subject, but I pointed out that using a female name and female pronouns might be confusing to the clinical team, since we had been talking about a male child with gender dysphoria..
I was informed that failure to use the right name and pronouns might result in problems or even litigation for me and the gender clinic at Tavistock.
The external influence of the advocacy groups increased. Instead of being a clinical, research-focused service where we were learning and developing ideas, it felt like it was a fait accompli that we had to go along with what Mermaids and patients wanted—even if we, the mental-health-care professionals, had legitimate questions about the appropriateness of the treatments that patients and patient advocates were demanding.
For example, a weird paradox arose at a conference on transgender health care hosted by Tavistock around 2005: the opening speaker declared that we were no longer supposed to think of gender dysphoria as a mental illness. But we were a mental-health team working at a mental-health facility. What were we supposed to be doing if not treating patients with psychological conditions?
Remember, this was all before the internet took hold of an entire generation of teenagers. There were no online groups dedicated to gender affirmation and coaching kids on what to say to their providers to secure cross-sex hormones. We mostly saw younger boys who believed themselves to be girls from an early age and a few teenagers who felt like they were trapped in the wrong bodies. So, although I felt aware of the gathering force of thinking around the area of gender dysphoria and transgender identity, it was hard to foresee the slow-motion avalanche that would hit over the next two decades.
Yet even what I saw in those years worried me deeply and working on the Gender Identity Development Service started to affect my personal well-being. I would come home with a headache on the days that I worked in the unit, and my heart would beat quickly when I went in the next morning. It felt like every time I raised a concern about us rushing prematurely to prescribe drugs that would have permanent effects on our patients, I’d be met with an eye roll and the unstated “Oh, here she goes again,” or “Can’t she just fit in?”
There were a few colleagues who shared my views. One colleague, Dr. Az Hakeem, would also speak up at team meetings. But for the most part I felt alone, and I felt very anxious about some of the children who had been referred for body-altering medications. I began to feel as though I might be part of something unethical. I tried to take on only children who were legally too young to commence the blockers, which would allow me more time to do long-term therapeutic work while avoiding the dilemma of the fact I worked in a so-called “gateway service” to medicalization.
I spoke a lot to my husband, Marcus, who is a psychoanalyst and who was by now a senior member of staff in the Adult Department of Tavistock. He suggested I go to the clinical director at theTavistock, which I did. She listened and took my concerns seriously. I later learned that she reached out to Dr. David Taylor, the Medical Director of the Trust, who was asked to launch an investigation into the work of the gender clinic. That was issued in 2006.
I do not remember being shown the report then, and don’t recall any in depth discussion about the contents of it or how the recommendations would be implemented. The only change that I remember was that a senior staff member from the more general Adolescent Department began overseeing our work. That oversight petered out when this staff member retired.
It was only in 2019 that I saw the full report when Hannah Barnes, a BBC journalist, obtained it via a Freedom of Information request. It confirmed all the disturbing things I had reported: Our data was poor; it wasn’t being stored properly; and there were not sufficient follow-ups with patients once they left the service—meaning we didn’t know how our patients were faring unless they voluntarily wrote to us.
As we have now learned from more recent whistleblowers, the recommendations in the report were buried, and when any criticism or difficult questions arose in the press, the Tavistock management would repeat the same mantra about how they were “a world-class service.” It’s important to acknowledge that there might have been some staff still struggling to deliver thoughtful, measured care, but the noise around our standards was growing louder.
I had tried hard to help the Gender Identity Development Service from the inside, but it felt like I was swimming against a stronger and stronger tide. I didn’t want to be part of something that felt wrong, and I knew that each time I spoke up I was being cast in a darker shadow of suspicion by my colleagues.
So in 2007, I quit.
After I left the gender clinic, I continued to work in other departments at Tavistock. I continued my clinical lecturing and practiced psychoanalytic psychotherapy. Life was satisfying and busy, and I tried to put the experience out of my mind.
But it became increasingly impossible to ignore.
In the past decade, there has been an explosion in referral numbers to the gender clinic at the Tavistock—over 3,000 in 2019—and the service came under mounting pressure to get through the long waiting lists. This resulted in even more children getting fast-tracked and put on blockers if they expressed a wish for them.
The profile of the patients changed significantly, too. Many were adolescent girls who had never exhibited signs of gender dysphoria. Often, their feelings of wanting to be a boy developed along with their breasts, or when they got their period. They were horrified by their bodies, and they wanted control over the changes taking place in them.
Between then and now, there were more whistleblowers, like Dr. David Bell, a psychiatrist and psychoanalyst at Tavistock, who issued yet another report on the service in 2018 that raised a lot of the same concerns that I had raised back in 2005. Sonia Appleby, whose job title was Safeguarding Children Lead, spoke out in November 2019, claiming that she was being blocked from doing her job by management. By then, the political pressure, the institutional capture, and the influence of social media had become much more intense, and about 40 people were working on the youth gender care team. Shortly after Dave’s report came out, my husband Marcus resigned from the Tavistock Board.
His resignation gained national publicity, and Marcus was invited to present at a 2019 House of Lords meeting, which I attended with him. A representative of the Tavistock Trust who was also at the meeting read a statement claiming that no one was being rushed through treatment, that Tavistock was a best-in-class facility. This was my second Damascene moment. I raised my hand to speak. “Look, that is not correct,” I said. “I worked there. And I saw that children were being pushed to transition very quickly.”
After that meeting, a group of us met, and we learned that a mother of a girl with autism and gender dysphoria was seeking support as a claimant in a judicial review of Tavistock’s practice of giving puberty blockers to minors. (Adults who transition are also prescribed blockers prior to starting on cross-sex hormones.) She had contacted a lawyer and he arranged a meeting with several of us who had attended the House of Lords meeting. The mother was worried about her daughter’s referral to the Gender Identity Development Service, as she did not feel that her daughter would be able to fully understand the ramifications of the treatment and give informed consent to it. She needed to remain anonymous and, therefore, needed a co-claimant who could afford to go public. Dave was still at Tavistock and was being threatened by the administration there. My husband had his hands full with his own patients. I did not relish the idea of sticking my neck out, but I knew I had to get back into the ring. By now, the whistleblowers’ reports felt grave. I signed onto the suit.
Almost no one in the U.K. wanted to get involved, so I set about finding expert witnesses in the United States, Australia and Scandinavia. Gradually, we put together statements and evidence to support our claim that children could not give fully informed consent to an experimental treatment with lifelong, as yet unknown consequences. I found, among many others, Kiera Bell through a journalist, and I was immediately taken by her story.
Keira is a young woman who went on puberty blockers at 16, testosterone at 17, and then had a double mastectomy—only to realize, at 21, that she wasn’t, in fact, a man trapped in a woman’s body. She argued that, as a minor, she hadn’t been able to consent in any meaningful way to the treatment. Eventually, she became a co-claimant in the case against Tavistock.
In December 2020, we won. The court ruled that minors under 16 could not give informed consent to having their puberty blocked. The ruling came as a great relief. I thought, Finally, people will have to pay attention and examine the evidence base for treatment of childhood gender dysphoria.
It’s hard to deal with the feeling of being hated. I’m aware how contentious this area is, and while I was only ever trying to do my best for our young patients, there was a loud group of people who would only hear my concerns as transphobia or bigotry or that I was a proponent of conversion therapy. The win felt like such a victory—not just legally, but culturally. It felt like an honest conversation was finally beginning to happen.
But then, in September 2021, we lost on appeal. It was awful—deflating.
The only thing that softened the blow was the fact that the government commissioned yet another report into Tavistock. And the results were devastating. It vindicated everything we had been saying for years.
But this time, the NHS decided they were going to do something about it. On July 28, the NHS announced that Tavistock Gender Identity Development Service would be closed and that, from now on, regional clinics would handle cases of transgender kids. I was blown away. I still can hardly believe it. The aim is that the new services should be more holistic, taking into consideration the whole child, and adopt better clinical standards according to the new report’s findings.
I didn’t seek any of this. It has been a pretty stressful few years. When I get a letter from patients or parents from around the world, and they tell me, “Well done, thank you for speaking up, you didn’t give up,” I sometimes get a lump in my throat. It’s been hard to be suspected of being prejudiced when all I wanted was safer clinical practice, more scrutiny and evidence collecting, and improved data storage.
Because what I am is a nurse. And my job as a nurse is to treat all my patients with respect and an open mind. I try to think about who they are as people, and to relate to their experience and empathize with them. I also believe we need to keep an open and curious clinical mind when something is occurring in society that seems novel or not yet fully understood. It should never be that doctors and nurses are unable to question diagnoses and prescriptions.
If my actions all those years ago have made a contribution, then I am proud. I made the right decision to raise my hand to ask another unwanted question.
Sue and Marcus Evans run a private psychotherapy practice in London. They are the authors of “Gender Dysphoria: A Therapeutic Model for Working with Children, Adolescents and Young Adults,” which you can buy here.
Richard Smith, editor of the British Medical Journal (BMJ) until 2004 posted an interesting opinion piece in the BMJ last year.
I have posted it below for you to read.
Time to assume that health research is fraudulent until proven otherwise?
Health research is based on trust. Health professionals and journal editors reading the results of a clinical trial assume that the trial happened and that the results were honestly reported. But about 20% of the time, said Ben Mol, professor of obstetrics and gynaecology at Monash Health, they would be wrong. As I’ve been concerned about research fraud for 40 years, I wasn’t that surprised as many would be by this figure, but it led me to think that the time may have come to stop assuming that research actually happened and is honestly reported, and assume that the research is fraudulent until there is some evidence to support it having happened and been honestly reported. The Cochrane Collaboration, which purveys “trusted information,” has now taken a step in that direction.
As he described in a webinar last week, Ian Roberts, professor of epidemiology at the London School of Hygiene & Tropical Medicine, began to have doubts about the honest reporting of trials after a colleague asked if he knew that his systematic review showing the mannitol halved death from head injury was based on trials that had never happened. He didn’t, but he set about investigating the trials and confirmed that they hadn’t ever happened. They all had a lead author who purported to come from an institution that didn’t exist and who killed himself a few years later. The trials were all published in prestigious neurosurgery journals and had multiple co-authors. None of the co-authors had contributed patients to the trials, and some didn’t know that they were co-authors until after the trials were published. When Roberts contacted one of the journals the editor responded that “I wouldn’t trust the data.” Why, Roberts wondered, did he publish the trial? None of the trials have been retracted.
Later Roberts, who headed one of the Cochrane groups, did a systematic review of colloids versus crystalloids only to discover again that many of the trials that were included in the review could not be trusted. He is now sceptical about all systematic reviews, particularly those that are mostly reviews of multiple small trials. He compared the original idea of systematic reviews as searching for diamonds, knowledge that was available if brought together in systematic reviews; now he thinks of systematic reviewing as searching through rubbish. He proposed that small, single centre trials should be discarded, not combined in systematic reviews.
Mol, like Roberts, has conducted systematic reviews only to realise that most of the trials included either were zombie trials that were fatally flawed or were untrustworthy. What, he asked, is the scale of the problem? Although retractions are increasing, only about 0.04% of biomedical studies have been retracted, suggesting the problem is small. But the anaesthetist John Carlisle analysed 526 trials submitted to Anaesthesia and found that 73 (14%) had false data, and 43 (8%) he categorised as zombie. When he was able to examine individual patient data in 153 studies, 67 (44%) had untrustworthy data and 40 (26%) were zombie trials. Many of the trials came from the same countries (Egypt, China, India, Iran, Japan, South Korea, and Turkey), and when John Ioannidis, a professor at Stanford University, examined individual patient data from trials submitted from those countries to Anaesthesia during a year he found that many were false: 100% (7/7) in Egypt; 75% (3/ 4) in Iran; 54% (7/13) in India; 46% (22/48) in China; 40% (2/5) in Turkey; 25% (5/20) in South Korea; and 18% (2/11) in Japan. Most of the trials were zombies. Ioannidis concluded that there are hundreds of thousands of zombie trials published from those countries alone.
Others have found similar results, and Mol’s best guess is that about 20% of trials are false. Very few of these papers are retracted.
We have long known that peer review is ineffective at detecting fraud, especially if the reviewers start, as most have until now, by assuming that the research is honestly reported. I remember being part of a panel in the 1990s investigating one of Britain’s most outrageous cases of fraud, when the statistical reviewer of the study told us that he had found multiple problems with the study and only hoped that it was better done than it was reported. We asked if he had ever considered that the study might be fraudulent, and he told us that he hadn’t.
We have now reached a point where those doing systematic reviews must start by assuming that a study is fraudulent until they can have some evidence to the contrary. Some supporting evidence comes from the trial having been registered and having ethics committee approval. Andrew Grey, an associate professor of medicine at the University of Auckland, and others have developed a checklist with around 40 items that can be used as a screening tool for fraud (you can view the checklist here). The REAPPRAISED checklist (Research governance, Ethics, Authorship, Plagiarism, Research conduct, Analyses and methods, Image manipulation, Statistics, Errors, Data manipulation and reporting) covers issues like “ethical oversight and funding, research productivity and investigator workload, validity of randomisation, plausibility of results and duplicate data reporting.” The checklist has been used to detect studies that have subsequently been retracted but hasn’t been through the full evaluation that you would expect for a clinical screening tool. (But I must congratulate the authors on a clever acronym: some say that dreaming up the acronym for a study is the most difficult part of the whole process.)
Roberts and others wrote about the problem of the many untrustworthy and zombie trials in The BMJ six years ago with the provocative title: “The knowledge system underpinning healthcare is not fit for purpose and must change.” They wanted the Cochrane Collaboration and anybody conducting systematic reviews to take very seriously the problem of fraud. It was perhaps coincidence, but a few weeks before the webinar the Cochrane Collaboration produced guidelines on reviewing studies where there has been a retraction, an expression of concern, or the reviewers are worried about the trustworthiness of the data.
Retractions are the easiest to deal with, but they are, as Mol said, only a tiny fraction of untrustworthy or zombie studies. An editorial in the Cochrane Library accompanying the new guidelines recognises that there is no agreement on what constitutes an untrustworthy study, screening tools are not reliable, and “Misclassification could also lead to reputational damage to authors, legal consequences, and ethical issues associated with participants having taken part in research, only for it to be discounted.” The Collaboration is being cautious but does stand to lose credibility—and income—if the world ceases to trust Cochrane Reviews because they are thought to be based on untrustworthy trials.
Research fraud is often viewed as a problem of “bad apples,” but Barbara K Redman, who spoke at the webinar insists that it is not a problem of bad apples but bad barrels if not, she said, of rotten forests or orchards. In her book Research Misconduct Policy in Biomedicine: Beyond the Bad-Apple Approach she argues that research misconduct is a systems problem—the system provides incentives to publish fraudulent research and does not have adequate regulatory processes. Researchers progress by publishing research, and because the publication system is built on trust and peer review is not designed to detect fraud it is easy to publish fraudulent research. The business model of journals and publishers depends on publishing, preferably lots of studies as cheaply as possible. They have little incentive to check for fraud and a positive disincentive to experience reputational damage—and possibly legal risk—from retracting studies. Funders, universities, and other research institutions similarly have incentives to fund and publish studies and disincentives to make a fuss about fraudulent research they may have funded or had undertaken in their institution—perhaps by one of their star researchers. Regulators often lack the legal standing and the resources to respond to what is clearly extensive fraud, recognising that proving a study to be fraudulent (as opposed to suspecting it of being fraudulent) is a skilled, complex, and time consuming process. Another problem is that research is increasingly international with participants from many institutions in many countries: who then takes on the unenviable task of investigating fraud? Science really needs global governance.
Everybody gains from the publication game, concluded Roberts, apart from the patients who suffer from being given treatments based on fraudulent data.
Stephen Lock, my predecessor as editor of The BMJ, became worried about research fraud in the 1980s, but people thought his concerns eccentric. Research authorities insisted that fraud was rare, didn’t matter because science was self-correcting, and that no patients had suffered because of scientific fraud. All those reasons for not taking research fraud seriously have proved to be false, and, 40 years on from Lock’s concerns, we are realising that the problem is huge, the system encourages fraud, and we have no adequate way to respond. It may be time to move from assuming that research has been honestly conducted and reported to assuming it to be untrustworthy until there is some evidence to the contrary.
In this in-depth interview series with Kirsten Murfitt of NZLSOS, we highlight the key points and outline the crucial yet-to-be-answered questions from Kirsten’s excellent Open Letter to Parliament, which she penned on 22 July 2022. This is Part 1.
Please share this interview. Please also utilise the steps involved at the end of the interview in order to put pressure on the government to answer our important questions:
The 3 main questions are:
1.) Why doesn’t the Government require mandatory reporting of deaths and serious adverse reactions, following the administration of a vaccine which has only provisional approval?
2.) Why does the Government refuse to investigate the safety and contents of the vaccine, given both the emerging overseas data and the court-ordered release of Pfizer’s documents?
3.) Why did the Government market the vaccine as “Safe and Effective”, when it knew that neither of those statements was true?
On this day, August 10, 1961, the United States began chemical warfare in Vietnam War, having sprayed 77 million liters of defoliants over South Vietnam by the end of 1971. Of that amount, 44 million liters contained dioxin, which causes various diseases and genetic mutations in humans and other living beings exposed to it.
Some three million Vietnamese were affected by direct contact with dioxin in that decade.
14% of the territory of South Vietnam was exposed to this toxin, causing severe consequences for the land and nature. Five thousand square kilometers of mangrove forests were almost completely destroyed; about 10,000 square kilometers of jungle and more than a thousand square kilometers of lowland forests were affected. American troops destroyed 70% of the coconut plantations and 60% of the Gewea plantations; they also changed the ecological balance of Vietnam.
The affected areas lost 18 out of 150 bird species; nearly all amphibians and insects disappeared; the number of fish in rivers decreased, and their composition changed. The microbiological composition of soils was disturbed. Changes in the fauna resulted in the replacement of black rats, which are safe for humans, with other species that were plague carriers. Alterations in the mosquito species composition led to the introduction of malaria-carrying ones. Dioxin: A Permanently Exploding Bomb The large-scale US use of chemical warfare in Vietnam lasted until late 1971. But this war was not over for Vietnam itself, said Professor Andrei Kuznetsov, director general of the Russian Division of the Joint Russo-Vietnamese Research and Technology Tropical Center, in an interview with Sputnik.
“This is because dioxins, once inside the human body, begin to work like an HIV infection. If a person is completely healthy, they do not affect him. As soon as the human immune system weakens and any disease begins, dioxins immediately get integrated into the disease chains and start working in their own way. No one knows just how. They can cause cancer, damage to the liver, skin, respiratory system, and much more. Dioxin pathology is very diverse. And the most tragic thing is that it is inherited through mother’s milk. More than a million and a half Vietnamese in the three postwar generations have suffered from it. For an extremely long time, for many generations, dioxins will continue to be passed on from women to their children. Moreover, there is no minimum permissible dose for dioxins,” says Andrei Kuznetsov.
Today, Vietnam faces the ever-present threat that children will be born with a wide variety of defects. To this day, several villages there are closed to the public, where children are born into families with various deformities. There are several specialized boarding schools where children with genetic defects live. Scientists from different countries have been studying the effects of dioxin on soil for a long time, but only in temperate and northern climates. No one has studied its impact in the tropics. There have been no studies on what happens when dioxin molecules enter the soil under tropical conditions, continued Professor Kuznetsov.
“The Joint Russo-Vietnamese Research and Tropical Technology Center is the first and only one to address this issue. It was commonly believed that dioxin molecules were insoluble. Supposedly, humus binds them and they remain in the top layer of the soil. One could bulldoze or even shovel it and burn it. But it turns out that things are different in the tropics. Dioxin molecules bind with various acids in the soil, forming new dioxin-containing molecules that become water-soluble and water-permeable. They mix with rainfall streams, sink into the soil, get transported by subsurface water, and subsequently enter wells, lakes, rivers, and seas hundreds of kilometers away from where they were sprayed. This situation persists in Vietnam to this day. There are several ‘hot spots’; places where, during the aggression, the Americans stored barrels with chemical agents. When they left Vietnam, they shot these barrels with large-caliber machine guns and left them there. For example, this happened in Da Nang, which was one of the largest US military bases. And the same happened at the US military base in Bien Hoa. These two former bases are still the largest and scariest hotbeds of contamination,” said Andrei Kuznetsov.
The expert also noted that the Americans recently have conducted a demonstrative action in Da Nang – and have now begun it in Bien Hoa – to decontaminate the soil to a depth of two meters in those places where barrels with warfare agents were stored. But they don`t check the level of dioxin contamination even within the radius of 200-300 meters from the storage sites. Meanwhile, subsurface water transports pesticides far beyond those limits.
The Mission of Joint Tropical Center The Joint Russo-Vietnamese Research and Technology Tropical Center has been studying the consequences of the US chemical war in Vietnam since its founding. In fact, it was established precisely for this work, noted Professor Kuznetsov.
“We were tasked with determining whether contact with dioxin leads to genetic changes in humans and has a detrimental effect on soil, flora, and fauna. Our conclusion – yes, it does. The results of our work were published and reported to the leadership of Vietnam’s Ministry of National Defense and Ministry of Health, together with our scientific and practical recommendations on combating various dioxin-related effects. At the same time, we noted that the most effective, global way to prevent dioxins from damaging people is to take maximum care of their health. That is, Vietnam needs to invest much more in health care than countries that have not been exposed to this toxic chemical. We cannot yet say when the effects of US chemical warfare will cease in Vietnam. After all, Vietnam is the first and only country to have been exposed to such massive amounts of poisonous substances,” Kuznetsov concluded.
Germany’s Hauke publishing house has published an open letter from 413 physicians, addressed to Thuringia’s Prime Minister, harshly criticizing the government’s Corona policy and call for the immediate suspension of Covid vaccinations due to “serious side effects and consequential damage”.
The signatories are all from one single German state, Thuringia, and were brought together by the fear of “the so-called facility-based mandatory vaccination” which they claim “has long been scientifically untenable, and thereby continue to bring suffering to those affected and their patients.”
The 413 physicians blast the government for ignoring the “growing number of studies critical of the measures or studies on side effects of the so-called vaccinations” and how “the so-called vaccinations continue to be touted as the only ‘panacea’ against the SARS-Cov2 virus.”
The group of physicians and health professionals also remind the government that they are “endangering the health of people” and doing so “to an unprecedented degree”. They expressed grave concerns over the safety of the COVID vaccines, stating that their harmful effects have now gone far beyond “suspicion” in terms of risk, and: “Colleagues from our group could tell you here about the growing number of patients with vaccine-related serious side effects and consequential damage.”
The group of 413 are calling for an investigation on the vaccine’s safety and blast the authorities for remaining silent, even that they have been abundantly warned, writing: “This does nothing to build confidence in your government’s policies.”
They add: “The answers of the state government to the many small inquiries of the member of the state parliament Dr. Ute Bergner on the subject of Corona show a shocking picture of ignorance, many data are not available to the state government again and again. ”
The signatories also share the opinion that “parts of science, politics, leading media, pharmaceutical industry have failed.”
By Thomas Riggins | Dissident Voice | February 5, 2014
A new report in Science News Magazine (1-25-2014) by Bruce Bower details a reevaluation of the view that the Rapa Nuians, the native inhabitants of Easter Island (Rapa Nui), were responsible for the collapse of their population and society due to over exploitation of natural resources and the destruction of the rain forest on their island, a view recently popularized by Jared Diamond in his book Collapse (2005).
As Bower reports, the anthropologist Maria Mulrooney has published the results of her studies of the Rapa Nui culture (Journal of Archeological Science, December 2013) based on new radiocarbon dates from archeological sites on the island. She has concluded that after the clear cutting of the forest in the 1500s, to make room for agricultural production, the population of Rapa Nui remained sufficiently vibrant to carry on food production and continue their cultural development.
Exactly when the Rapa Nui arrived on Easter Island is unknown but it was on or before 1200 A.D. or so. Mulrooney maintains they had a thriving culture which was still going strong even after their “discovery” by the Dutch explorer Jacob Roggeveen on Easter Sunday 1722. This would indicate that they had not suffered “collapse” as a result of forest clearance. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.