Millions Face New Fluoridation Threats
By Stuart Cooper | Fluoride Action Network | June 21, 2022
The published science over the past decade has taught us a lot about water fluoridation, about both the very real and significant side effects inflicted on the public, but also about the credibility of those who continue to vouch for its safety.
At this point, the question we must ask isn’t whether the overwhelming risks outweigh the theoretical scant benefits, or whether more research is needed to draw strong conclusions. No, the only appropriate question now is: How much more harm will the promoters and regulators of fluoridation allow the practice to inflict on the public?
Without the Fluoride Action Network, our coalition partners, and people like you taking a stand, their answer will be a resounding, “a lot more harm!” With their credibility and influence at stake after defending fluoridation for more than 75 years, they’ve sadly shown that they’ll not only be the last to act, but that they plan to double down until we stop them.
As we speak, tens of millions of residents currently living on community water systems with no added fluoride throughout the United States, Canada, the United Kingdom, Australia and New Zealand are facing the imminent threat of having their water dosed with hazardous fluoridation chemicals.
The CDC has announced a new strategy and helped develop a new technology to fluoridate an addition 19+ million Americans, which will also eventually expand to Canadians, Australians and likely others.
Meanwhile, the governments in the U.K. and New Zealand have exploited the recent pandemic to pass sweeping health care reform bills that effectively include nationwide fluoridation mandates due to decades of strong pushback from residents and elected officials at the local level, keeping fluoridation at bay.
Fluoride Has Already Damaged the Teeth of Millions
The U.S. Centers for Disease Control’s own data taken from the National Health and Nutrition Examination Surveys (NHANES) has repeatedly found that our children in the United States are significantly overexposed to fluoride, evidenced by skyrocketing rates of dental fluorosis.
Fluorosis is a biomarker of toxicity from ingested fluoride, and is a permanent tooth defect, causing unsightly discoloration and mottling of the teeth, weakening the enamel and resulting in increased dental decay.

Ingesting fluoridated water — particularly in reconstituted infant formula — and processed foods made with fluoridated water are recognized as the primary sources of exposure, though swallowing toothpaste and fluoride prescriptions also contribute.
A 2015 review of the practice of fluoridation by the Cochrane Collaboration, the gold standard for evidence-based reviews of health interventions, found that “there is a significant association between dental fluorosis (of aesthetic concern or all levels of dental fluorosis) and [water] fluoride level.”
The CDC reported that 41% of adolescents (12 to 15) had dental fluorosis in 2004. At the time this was an increase of over 400% from the rates found 60 years prior. Then the 2012 survey found that the rate jumped significantly to 65+% of adolescents with dental fluorosis.
Now, according to a recent study (Yang, June 2021) published in the journal Ecotoxicology and Environmental Safety using the data from the NHANES 2015-16 survey, the “prevalence of dental fluorosis was 70% in the U.S. children.”
This means that the teeth of millions of children, teens and adults have already been damaged by overexposure to fluoride during development, and the CDC, along with the other promoters of fluoridation are fully aware. However, the teeth are not the only tissues in the body that are harmed by or accumulate fluoride. There is no apparent reason, therefore, why fluoride’s effects on the body would be limited to the teeth. As noted by renowned dentist and researcher Dr. Hardy Limeback:
… it is illogical to assume that tooth enamel is the only tissue affected by low daily doses of fluoride ingestion.
NHANES data has been used in recent published and peer-reviewed studies to link fluoridated water with a number of additional side-effects, including earlier onset of menstruation for black teens, sleep disorders in adolescents, increase uric acid levels in the blood, and kidney and liver impairment in adolescents.
Additional studies on fluoridation have also recently found higher rates of hip fractures, disruption of the endocrine system, and increased rates of hypothyroidism.
Fluoride Is the New Lead
There is now a large body of government-funded research indicating that fluoride is neurotoxic, and is associated with lowered IQ in children and a significant increase in ADHD diagnosis and related behaviors in children at doses experienced in fluoridated communities. Experts in the toxicology have likened the size of the effect to that from lead.
To date, 69 human studies, most from endemic fluorosis areas in China, have associated lowered IQ with fluoride exposure. The highest quality fluoride brain studies have been published since 2017, when the first of five NIEHS-NIH (National Institutes of Health) funded prospective-cohort studies was published (Bashash et al., 2017) finding an association between fetal exposure to fluoride and lowered IQ in Mexico.
A year later, another NIH-funded study found an increase in ADHD symptoms associated with in utero exposure to fluoride (Bashash et al., 2018).
Over the next two years, two more of these government-funded studies found similar results, linking fetal exposure to fluoridated water in Canada to lowered IQ (Green et al., 2019), and finding that bottle-fed infants in fluoridated communities in Canada had a significantly lowered IQ compared to bottle-fed infants in non-fluoridated communities (Till et al., 2020).
And just last year, the fifth NIH-funded study (Cantoral et al, 2021), found that for every 0.5 mg increase in dietary fluoride intake during pregnancy was associated with a 3.10 to 3.46-point lower cognitive score in boys. The authors stated:
“Fluoride is not an essential nutrient and … fluoride ingestion in pregnancy does not strengthen enamel during tooth formation in the fetus but has been associated with increased risk of neurotoxicity, even at optimal exposure levels …
These findings suggest that the development of nonverbal abilities in males may be more vulnerable to prenatal fluoride exposure than language or motor abilities, even at levels within the recommended intake range.”
I strongly urge you to watch and share this recent 20-minute PowerPoint presentation by professor Christine Till, Ph.D., lead author of some of these landmark fluoride studies, explaining her team’s research and findings.
In 2021, the first benchmark dose analysis conducted on maternal fluoride exposure and neurotoxicity to the fetus was published in the journal Risk Analysis (Grandjean, 2021). Benchmark doses analyses are used by the EPA and toxicologist to determine at what level a substance starts to cause harm. It is well established that a loss of one IQ point leads to a reduced lifetime earning ability of $18,000.
The analysis confirmed that extremely low fluoride exposure during pregnancy impairs fetal brain development, finding that a maternal urine fluoride concentration of only 0.2mg/L — which coincides with the level in water (0.2ppm) — was enough to lower IQ by at least 1 point.
This is four times lower than the current government “recommended” level of 0.8ppm in fluoridated communities. It’s also six times lower than the level that was recommended as “safe” by the CDC, HHS, and the American Dental Association for over 60-years up until 2011 (1.2ppm).
For perspective, A urinary fluoride (UF) concentration of 0.2mg/L is far below what a pregnant woman in a fluoridated community would have, as confirmed by two recent studies. A recent study of pregnant women in fluoridated San Francisco, California, found a mean UF concentration of 0.74mg/L. A second study with participants in fluoridated communities across Canada found a mean UF concentration of 1.06mg/L.
Both studies also found that the UF levels were significantly lower for the participants living in the non-fluoridated communities. The authors of the benchmark dose analysis stated:
“These findings suggest that fetal brain development is highly vulnerable to fluoride exposure … and provide additional evidence that fluoride is a developmental neurotoxicant (i.e., causing adverse effects on brain development in early life).
Given the ubiquity of fluoride exposure, the population impact of adverse effects from fluoride may be even greater than for other toxic elements like lead, mercury, and arsenic … and the benchmark results should inspire a revision of water fluoride recommendations aimed at protecting pregnant women and young children.”
These authors are hardly alone in comparing fluoride’s neurotoxic impact to the well-established harm of lead:
- Dr. Dimitri Christakis, MPH, and Dr. Frederick Rivara, MPH, editors for the Journal of the American Medical Association (JAMA) on their podcast (around 4:25): “[The 4.5 IQ loss is] An effect size which is sizeable — on par with lead.”
- Christine Till, PhD, co-author of several landmark fluoride/neurotoxicity studies, on Canada’s CTV: “4.5 points is a dramatic loss of IQ, comparable to what you’d see with lead exposure.”
- David Bellinger, Ph.D., MSc, Harvard professor of neurology, on NPR: “It’s actually very similar to the effect size that’s seen with childhood exposure to lead.”
Other experts, including Linda Birnbaum PhD, former Director of the National Toxicology Program, stress the need to avoid fluoride:
“Given the weight of evidence that fluoride is toxic to the developing brain, it is time [to] protect pregnant women and their children [and recommend they] reduce their fluoride intake.”
There are now nine fluoride mother-offspring studies linking fluoride exposure to harm, and 23 studies published on the association between fluoride exposure and reduced IQ since 2017.
How FAN Responded to the Science
Because of the growing list of published fluoride-IQ studies, and the downplaying of their importance by pro-fluoridation advocates such as the Division of Oral Health at the CDC and the American Dental Association, FAN embarked on two initiatives in 2016.
First, we requested the National Toxicology Program undertake a systematic review of ALL the studies (animal, human and cellular) pertaining to fluoride’s potential to damage the brain. The NTP agreed with our request, and they plan to publish the final results of their multiyear review of fluoride neurotoxicity any day now. In the two first drafts the NTP concluded, “that fluoride is presumed to be a cognitive neurodevelopmental hazard to humans …”
The review drafts identified over 100 studies showing adverse effects including IQ loss and increased ADHD. Among 27 studies designated as high quality, 15 show fluoride injury at the same exposure levels found in community fluoridation programs.
Second, we petitioned the EPA under provisions in the Toxic Substances and Control Act to ban the deliberate addition of fluoridation chemicals to the drinking water supply because it poses an unreasonable risk to the developing brains of children. The EPA’s lack of action led to FAN suing them in federal court.
The initial phase of the trial was held in June 2020, concluding with the judge saying, “I don’t think anyone disputes that fluoride is a hazard.” However, the court is awaiting the final NTP report before moving forward with the final phase of the trial. Here is a short video update on the lawsuit from FAN’s attorney.
This past year, FAN embarked on a two more initiatives. We communicated with the U.S. surgeon general about the risk posed by fluoridation to developing children, and asked that he take action to warn parents.
We also initiated a dialogue with CDC officials (see initial letter signed by 112 professionals) that ultimately led to them organizing presentations for their leadership from several fluoride/neurotoxicity study authors, Dr. Bruce Lanphear, Christine Till, Ph.D., and Dr. Philippe Grandjean on their research.
How Promoters Have Responded to the Science: A New Threat
It has been six months since the CDC heard the presentations on neurotoxicity from the three veteran researchers, and it’s been over a decade since the CDC acknowledged that fluoridation has damaged the teeth of millions.
Yet, the CDC, along with the EPA, World Health Organization, American Academy of Pediatrics, American Dental Association and their state level peers not only have failed to warn residents about the dangers posed by fluoridation, but have continued advocating for fluoridation expansion in spite of the science.
The CDC has partnered with the chemical industry to target 19 million residents in 32,000 small and medium sized communities across the United States that do not add fluoridation chemicals to the public drinking water. Using your tax dollars, the CDC provided upward of $2 million dollars in funds to private business to develop a fluoridation delivery product for water systems serving between 50 and 10,000 people.
The widespread sale and promotion of this new product began in January throughout the U.S., but is also planned for Canada and Australia in the near future. The American Dental Association has joined the CDC in pushing this new strategy.
In July of 2021, the CDC held a “Public Health Grand Rounds” presentation on fluoridation. While there was no mention of the large number of new studies linking low levels of fluoridated water to neurotoxicity, it was an infomercial for a new technology that the CDC and ADA were calling “a game changer” in their efforts to expand fluoridation.
Below is a slide from that presentation, where you can see they intend to increase the percentage of fluoridated water systems from 73% to 77% — representing 19 million people on 32,000 water systems — by 2030.

This goal isn’t exactly new. The CDC and ADA have utilized a number of strategies over the past decade to expand the practice, but largely due to FAN and our network of local volunteers and professionals, the number of fluoridating communities has actually decreased, while the population served has increased slightly due to urban growth.
To accomplish this significant increase over the next eight years, they intend to utilize a new fluoridation system specifically designed to be simple and cheap enough for even the smallest water systems, which could include private systems, or even colleges and public schools.
They’re calling it the “New Wave Fluoridation System.” It utilizes compacted sodium fluorosilicate in a tablet form designed to dissolve over time in a small amount of water, much like the deodorizer tablets used in urinals.

We have learned that this process started in 2013, when CDC’s chief fluoridation engineer, Kip Duchon, suggested that the CDC help develop a product that was feasible for small and rural communities. Soon thereafter the CDC announced a Small Business Innovation Research grant opportunity — providing upward of $2 million — for private business to develop and test the idea.
KC Industries, of Mulberry, Florida, was awarded at least two large grants, one to develop the tablet and the other to develop the injection/feeder system.
KC Industries is a small chemical manufacturer with a handful of employees. According to their website, “The plant was built by Kaiser Aluminum & Chemical Corporation and began producing Sodium Fluorosilicate in 1957 as a raw material to manufacture aluminum.”
KC Industries purchased the facility in 1999 and appears to have focused heavily on the “dry” fluoride drinking water additive market with sodium fluoride. Here is their page on their sodium fluoride product; it’s worth a quick look.
Over the past 20 years, more communities have switched their additive to fluorosilicic acid, which is an incredibly dangerous and corrosive liquid, but is cheaper. This led to a massive decline in sales of dry additives, and KC Industries’ profits.
According to their press release, they were struggling until the CDC’s grant, which they say provided “a new lease on life” for the chemical company. They’re expecting “an immediate return on investment” as communities clamor for the new system.
KC Industry representatives have said that interest in the system has come from around the world. The first community to use the product as part of a free pilot project is Cleveland, Georgia. Other communities that have signed on include Marathon, Wisconsin; Center, Colorado; and Aulander, North Carolina. The Missouri state legislature has also included nearly $4 million in funding over the next few years to go toward grants to expand the program in their state.
The CDC employee who initiated this process, Kip Duchon, has retired from the CDC and is now a consultant to the ADA’s National Fluoridation Advisory Committee.
The ADA has already called it a “game-changer” and lobbied Congressional members to include taxpayer funding for this technology in the recent infrastructure bill intended to help economy out of the pandemic.
Meanwhile, the CDC also continues to give very large taxpayer-funded grants to states to pay for public relations campaigns to promote fluoridation.
Pandemic Exploited to Mandate Fluoridation in UK, New Zealand
Even worse than what is happening in North America with the new tablet fluoridation system, is the recent passage of legislation in both the United Kingdom and New Zealand, transferring authority over fluoridation from local officials (and indirectly the public) to unelected public health bureaucrats who have vowed to mandate the practice throughout their respective nations without concern for what the public wants.
Both nations include fluoridation resolutions as part of a much broader legislative effort to centralize public health decisions in response to the pandemic. The U.K. and New Zealand will now join Ireland and Singapore as the four public health outliers in a world that has overwhelmingly rejected fluoridated water.
Last year, the New Zealand government revived, amended and passed a bill that was introduced in 2016, but lacked enough support for passage. As introduced, the bill would have moved fluoridation decisions from local councils — where they reside presently — to district health boards.
However, the current government amended the language to centralize fluoridation authority even further, by giving full control to the director-general of health, Dr. Ashley Bloomfield. Using this process defied the normal democratic process, with no select committee, community consultation or public input. Local councils (and local taxpayers) will be responsible for all capital and operational costs.
Like the CDC, government officials and public health officials were warned in advance of the harm their decision would cause, yet they ignored it.
Some local leaders have quickly made their opposition to this proposal heard, including the mayor of Whangarei, Sheryl Mai, who said, “People who drink water from the tap will be mass medicated whether they want to be or not.”
Mayor Greg Lang of Carterton, and Mayor Alex Beijen of South Wairarapa, both opposed the measure because it took councils, consumers and ratepayers out of the decision. Officials in Christchurch and Southland have also recently voiced opposition, saying safety is a greater priority than fluoride. Clearly, there is still a chance for those communities that push back against this proposal.
In the U.K., decades of efforts by the government to expand fluoridation stalled having reached only 10% of the population. Efforts to fluoridate Northern Ireland failed miserably with 22 councils voting against the measure. Scotland too remained unfluoridated. Efforts over the last two decades to fluoridate Southampton, Manchester, and Hull also failed.
As a result, Prime Minister Boris Johnson proposed an addition to the large Health and Care Act that would effectively mandate fluoridation by giving the health secretary, Sajid Javid, unilateral power to force communities throughout the country to add fluoridation chemicals to the public water supplies.
FAN coordinated with locals to mount opposition to this proposal, including a series of public letters from British scientists accusing public health officials of ignoring the science. The opposition culminated on the floor of the House of Lords, where a number of members spoke out against the proposal, including Lord Reay, who warned of the dangers posed to developing children.
Since passage into law, FAN has made an official submission to the government urging the Department of Health and Social Care to perform a health risk assessment on the effects of fluoridated water on the pregnant woman, the fetus and the formula-fed infant, before implementing fluoridation into the U.K. No regulatory agency in any fluoridating country has ever done this.
However, as the U.K. is contemplating expanding fluoridation to the whole country, it is essential that this is done before they embark on this program.
The Last Line of Defense
I want to conclude by asking the same question I asked at the beginning of this article, but rephrased: How much more harm will YOU allow the promoters and regulators of fluoridation to inflict on the public?
As I write this, millions of developing babies and infants are being overexposed to fluoride from their fluoridated tap water. The research has shown that there is no safe amount of fluoride for the fetus or infant. All will be impacted, some significantly more than others.
Please help us defend these vulnerable children and give them the gift of normal brain development. Help us also protect other vulnerable subpopulations, including those with hypersensitivities, dental fluorosis, bone brittleness and kidney, liver, or thyroid impairment.
The Fluoride Action Network is a nonprofit advocacy group set up in 2000 to broaden awareness among citizens, scientists and policymakers on the toxicity of fluoride compounds. It maintains the largest online database for fluoride toxicity studies, and has helped many of the 300+ communities that have ended or rejected fluoridation chemicals since 2010.
We’re amplifying the voices of a growing chorus of renowned international experts in toxicology, neurology and environmental toxins, warning the public about fluoridation, and educating and recruiting more to speak out.
We’ve captured the surgeon general’s and the CDCs’ attention, made progress with our federal lawsuit against the EPA, helped communities come together to fight fluoridation, and worked with state legislators to defeat mandate bills and support prohibition efforts.
Can you help us continue defend our water and our health, and expand our efforts as new threats arise here in North America and around the world in the United Kingdom and New Zealand? Will you stand with FAN?
Fluoride Awareness Week – Your Help Is Needed
On June 20 to June 26, we launch Fluoride Awareness Week. We set aside an entire week dedicated to ending the practice of fluoridation. There’s no doubt about it: Fluoride should not be ingested. Even scientists from the Environmental Protection Agency’s (EPA) National Health and Environmental Effects Research Laboratory have classified fluoride as a “chemical having substantial evidence of developmental neurotoxicity.”
The only real solution is to stop the archaic practice of artificial water fluoridation in the first place. Fortunately, the Fluoride Action Network (FAN), has a game plan to END fluoridation worldwide.
Clean pure water is a prerequisite to optimal health. Industrial chemicals, drugs and other toxic additives really have no place in our water supplies. So please, protect your drinking water and support the fluoride-free movement by making a tax-deductible donation to the Fluoride Action Network today.
The Covid vaccine paper on declining sperm counts is even worse than it seems at first
By Alex Berenson | Unreported Truths | June 20, 2022
On Friday, the journal Andrology published a peer-reviewed paper showing large decreases in sperm counts among men after the second dose of Pfizer’s mRNA Covid jab.
Based on counts from men who donated sperm to three fertility clinics in Israel, this finding is devastating – medically and politically.
It cuts to the heart of the hottest button question of all about the mRNA shots, whether they have hidden fertility risks. That issue has simmered since early 2021, following my reporting that data showed the shots had caused excess miscarriages in rats – and other reports showing that measurable amounts of vaccine reached the ovaries and testes in tests in rats.
Ever since, media “fact-checkers” and public health authorities have dismissed and mocked the concerns and anyone who raises them:
—
Now – after a half-billion men have received mRNA shots – the skeptics appear to be right. Again. The Israeli paper offers hard evidence that the vaccines may present a systemic risk to men’s sperm counts. What was a conspiracy theory is now just a theory. AGAIN.
The paper raises questions about mechanism of action that must be answered immediately. And on top of the myocarditis risk, the finding is more evidence that encouraging – much less forcing – men under 40 to take the mRNA vaccines was a catastrophic mistake.
—
However, the authors qualified their findings by reporting that after five months, sperm levels recovered. Thus the decreases were only temporary, they wrote.
Put aside the fact that a five-month decrease hardly qualifies as temporary for someone trying to start a family – or compared to a “vaccine” that loses effectiveness against Omicron within weeks or months.
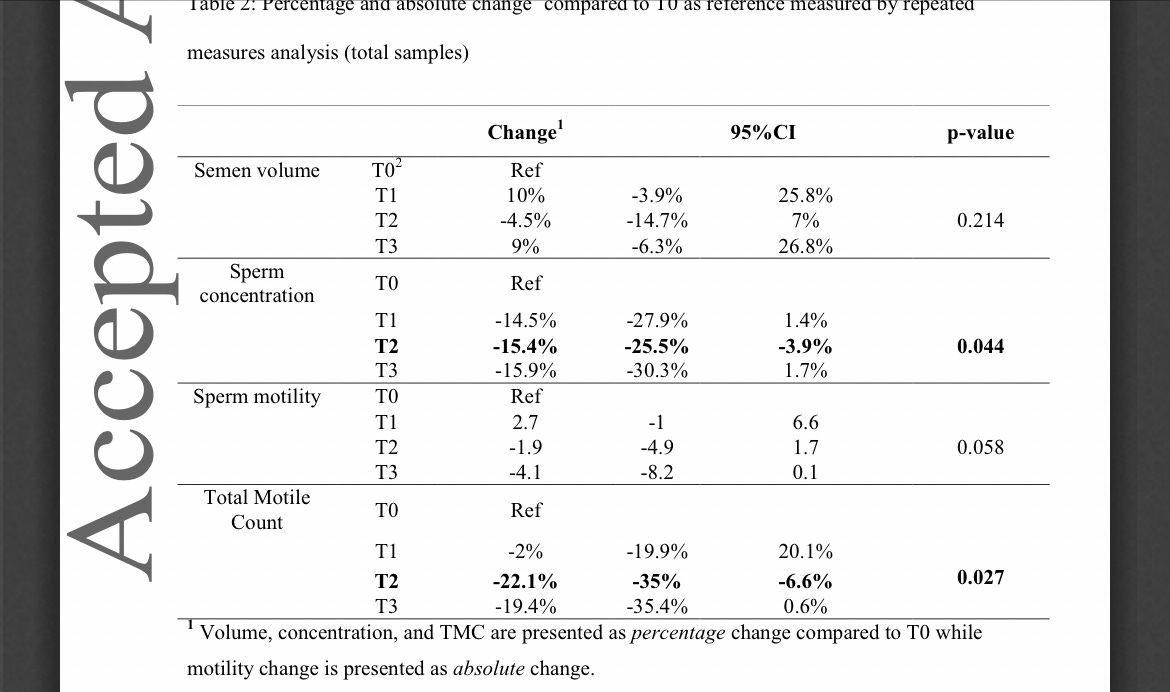
As other writers have pointed out, the actual data in the paper do not really support the argument that sperm levels returned to normal after five months. In fact, by some measures, levels continued to decline.
Rather than acknowledging this fact, the authors offered the best possible spin on their data, while at the same time publishing the figures themselves near the end of the paper so that other researchers could see the reality for themselves.
This tactic is now commonplace among researchers putting out data that might raise concerns about the mRNA shots. It is likely a response to the overwhelming political pressure to hide the deepening crisis around the safety and efficacy of shots that governments have given to over a billion people worldwide.
Below is the crucial chart, which shows that “total motile count” – the number of sperm in the ejaculated semen – plunged 22 percent three to five months after the second shot (T2) and barely recovered during the final count (T3), when it was still 19 percent below the pre-shot level.
SOURCE
Even more importantly, the fall in sperm counts CANNOT be blamed on short- or even medium-term inflammation as mRNA-generated spike proteins causes our immune cells to ramp up the systemic production of anti-spike antibodies. If that were the case, one would expect to see a short term decrease in sperm count that reverses over time. Instead, total sperm counts are unaffected shortly after the mRNA shots, then decrease months later and hardly recover.
To play down this unpleasant reality, the researchers instead focused on the fact that median rather than average counts did recover after five months. (The median is the numerical midpoint of a series; If a series goes 1, 2, 3, 4, 20, the median will be 3, but the average will be 30 divided by 5, or 6.)
Both the median and the average can be valuable statistics. Using the median rather than the average will hide extreme outliers. In this case, the fact that the average fell much more than the median is a sign that some of the men probably had near-zero sperm counts in both the second and third time periods – and that fact is arguably more important than the median change.
All of which is to say that this data cannot be easily explained away and should not be ignored, as badly as the media would like to do so. The fall in sperm counts is part of an emerging and increasingly dark picture about the long-term health impacts of the mRNA shots – and should all by itself convince parents not to risk exposing their children to these powerful biotechnologies.
Wake up, everyone!

By Paul Weston | TCW Defending Freedom | June 21, 2022
AFTER two years of Covid-19 insanity, the West has several new crises to deal with. Rampant inflation, coming food shortages and fuel shortages, monkeypox, a mystifying confusion about XX and XY chromosomes and a strange war in Ukraine which appears to be a proxy war between nuclear armed America and nuclear armed Russia.
I say a strange war because no one seems remotely interested in stopping it, no matter that it could lead to Armageddon. I think this is because Putin can be blamed for some of the deliberately engineered crises we are currently experiencing, so don’t expect it to end soon. Our armchair warrior political class seems more than happy to supply weapons to prolong the inevitable and are valiantly prepared to fight to the last surviving Ukrainian.
I feel as though we no longer exist as human beings in the eyes of our overlords. We are now just cattle being herded toward a dystopian future by a small number of immensely powerful individuals and global organisations who make no secret of the future they wish to build for us. This global coup d’état is driven by lies and corruption at every level of our national and international institutions. Nothing we have been told over the last couple of years is true.
For example, over the last thirty years in England and Wales an average 1.2 per cent of the population died every year, the vast majority of them old and ill. In 2020, the year of the alleged Covid-19 killer pandemic, just 1 per cent of the population died, and again the vast majority were old and ill. Yet despite experiencing a lower-than-average death rate, a Covid-19 emergency was declared which saw the biggest power grab by the state over the lives of its citizens since the dictatorships of Lenin, Hitler and Mao.
The most chilling aspect of this totalitarian takeover is that Western countries acted in unified lockstep as they tore up every tried and trusted historical public health protocol related to airborne viruses and replaced them with a tyranny that had no basis in medical or scientific reality.
People who recognised what was happening publicly protested and were met with state enforced paramilitary brutality never previously seen in the West. In Australia rubber bullets were used against peaceful protesters. In Canada, Justin Trudeau invoked the War Measures Act to beat, jail and pauperise peaceful protesters who preferred to live their lives according to the Nuremberg Code rather than Trudeau’s Mengele Code. In New Zealand huge posters of a beaming Jacinda Ardern were ruthlessly displayed on advertising hoardings across the country.
The biggest issues I can see in all this criminal insanity are two-fold. Firstly, our ruling class now know they can do whatever they want to us if they terrorise us sufficiently, as in carry out acts of genuine terrorism against their own citizens to achieve a political ambition. Secondly, we now know exactly what they want to do to us because they meet up in Davos every year and shamelessly talk about it in very loud voices.
Their power is immense, and for the first time in history they have the ability to build a revolutionary new society without having to carry out violent street revolutions. All they need is electronic data and digital IDs linked to a government-controlled central bank digital currency, which all Western governments are currently implementing. Covid-19, mass vaccinations and digital Covid passes – please don’t think they have been consigned to history – were a necessary pre-condition of course if a Digi-Tyranny could ever become a reality.
Western governments are also working on legislation to both silence dissent on social media and stifle physical public protest. New Ministries of Truth are being formed which will disappear and memory-hole any written and spoken words our ruling class considers to be misinformation or disinformation. This is Orwell’s 1984 and it is happening before our very eyes.
Who are the people/organisations enacting this totalitarian Western coup d’état? Well, it is primarily the World Economic Forum, the United Nations, the World Health Organisation, the World Bank, the International Monetary Fund, the EU, Big Tech social media, the pharmaceutical industry, the entire Western political class and three gargantuan financial institutions called BlackRock, Vanguard and State Street, along with a handful of monumentally wealthy billionaires including Soros and Gates.
The concerted power and wealth held by the above has completely corrupted politics, science, journalism, the judiciary, academia and medicine. There are still some brave souls from those professions who risk their careers by speaking out, but you will never see them via the mainstream media or the biggest social media platforms. Those we are allowed to see are bought and paid for propagandists who tell us nothing other than the revolutionary line.
I am fifty-eight years old now. I was born a long time after World War Two and my entire life – up until 2020 at least – was one of unimaginable ease and freedom compared to most humans who have ever lived. But the freedom I enjoyed is over now. Our future could be very grim indeed. Another pandemic will soon be coming our way and I suspect this one will be necessarily much more lethal than the last.
Also coming our way are ever rising interest rates to counter the deliberately engineered inflation. If these interest rates hit double figures, every average earning mortgage holder will lose their house. The manufacture of petrol and diesel cars will soon be phased out and extortionate taxes will be introduced to keep older ones on the road. Air travel for the masses is not part of the New World Order’s Green Agenda, nor is heating our homes with oil or gas.
They have told us what they want. A smaller population. A lower carbon footprint. A digital ID surveillance/social credit state capable of bending us to their dictatorial will. No more meat, just bugs; lots and lots of delicious bugs. The apparatchiks of the Green New World Order will still have their private jets, their beachside mansions, their haunches of venison and their champagne whilst we will own nothing, which I rather suspect will fail to induce delirious happiness whatever Herr Schwab might purportedly believe.
Can they achieve their publicly oft-stated agenda? Yes, they simply have to continue doing what they are already doing, although it will need to be substantially ramped up, hence my belief another pandemic is on the cards. In America they have the problem of gun ownership in the hands of ordinary citizens, so I think we will see huge efforts – by means more foul than fair – to urgently rectify this problematic issue for the New World Order.
Is it all doom and gloom? Not really. They have shown their hand and despite their seemingly limitless power and wealth there are only a few thousand of them whilst there are billions of us. I see our future as one of only two credible possibilities: freedom for us and jail for them, or slavery for us and even bigger yachts, private jets and sizzling steaks for them. It is up to us in other words. The very first thing the average person needs do is wake up. Before it is too late.
Fauci Finally Gets Covid: The Significance
BY JEFFREY A. TUCKER | BROWNSTONE INSTITUTE | JUNE 17, 2022
What precisely happened in the month of February 2020, when Anthony Fauci and cohorts were plotting their pandemic response, is still a mystery. Jeremy Farrar, of the Wellcome Trust, in his book on the topic says that during these weeks, they went to burner phones, clandestine video calls, and warned family members that something terrible could happen to them.
Their top concern was the possibility of the lab leak from Wuhan. They needed to get to the bottom of it and prepare the spin. We know that the initial draft of the academic article denying the lab leak came out February 4, 2020, later published in the Lancet on March 16. But what happened in these three weeks – apart from the mid-February NIH junket to China to learn how to control a virus – remains foggy.
But this much we do know: by March 2, 2020, Fauci had his game plan lined up. Michael Gerson of the Washington Post wrote him on that day and asked about the purpose of social distancing. This was weeks before most Americans had even heard this euphemism for forced human separation. Was the idea to wait for a vaccine, Gerson asked?
Fauci answered in a private email as follows:
“Social distancing is not really geared to wait for a vaccine. The major point is to prevent easy spread of infections in schools (closing them), crowded events such as theaters, stadiums (cancel events), work places (do teleworking where possible… The goal of social distancing is to prevent a single person who is infected to readily spread to several others, which is facilitated by close contact in crowds. Close proximity of people will keep the R0 higher than 1 and even as high as 2 to 3. If we can get the R0 to less than 1, the epidemic will gradually decline and stop on its own without a vaccine.”

There we have it: the Fauci theory of how we get rid of the virus. We don’t need a vaccine. Just close things. Stay away from people. Don’t gather. Shut schools. Lock businesses and churches. All people stay away from all people. The R-naught will drop.
Then the virus will… and this is where the theory gets murky. Does it just vanish? Get bored? Get frustrated, give up, and vanish into the ether? And how long does this new social system of “social distancing” have to last? Years? Forever? And what happens once people start acting normally again?
This is very clearly crank science, one that confuses ex post data collection with causation itself and also seems to deny the workability of the human immune system. That such things would be written by a person in Fauci’s position is truly mind boggling. But the press went along, and still does after all this time.
What Fauci was imagining – and very few people picked up on it at the time – was the construction of a new social system. It was not just about this virus. It was about all pathogens and the whole functioning of society. He believed – or he decided to come to believe – that a re-engineering of the social order could successfully beat back common pathogens and bring about universal health.
He finally revealed this in his August 15, 2020, article for Cell that received very little attention at all. He was on his own attempting to implement an entire new social system based on a new ideology.
Living in greater harmony with nature will require changes in human behavior as well as other radical changes that may take decades to achieve: rebuilding the infrastructures of human existence, from cities to homes to workplaces, to water and sewer systems, to recreational and gatherings venues. In such a transformation we will need to prioritize changes in those human behaviors that constitute risks for the emergence of infectious diseases. Chief among them are reducing crowding at home, work, and in public places as well as minimizing environmental perturbations such as deforestation, intense urbanization, and intensive animal farming.
This article reveals the most important point. The pandemic response was not just about this one pathogen. It was about what amounts to a political, economic, social, and cultural revolution.
It’s not socialism or capitalism. It’s something else entirely, something very strange, like a Rousseauian technocracy, simultaneously primitive and high tech, as managed by a scientific elite, an untested dystopia worthy of the most terrifying literature in the English language.
No one has voted for such a thing. It is something Fauci and his friends dreamed up on their own and deployed all their enormous power to enact just as a test, until it fell apart. The US and many parts of the world were in their grip for the better part of a year and two years in some places.
This is a scandal for the ages, one that far outstrips issues of tax-funded gain-of-function research, as important as that is. It’s even more important than reports that Fauci has been earning personal royalty payments from pharmaceutical companies that receive grants that he has personally approved. The real problem comes down to his power and the ability of elected representatives and courts to control him for many decades.
Regardless of Fauci’s millenarian vision, the course of the virus took the usual path but for one major exception: the waves of infection occurred based on class rank in society. There was a political hierarchy of infection that started with the working classes, moved to the bourgeoisie, hit the professional classes, then high-end journalists, and finally, at the very end came for the elite ruling class itself – Trudeau, Psaki, Ardern, Gates, and finally Fauci – regardless of their multiple vaccines.
And here is why Fauci’s covid infection is significant, 28 months after the first lockdowns. It’s a sign and symbol that his entire theory of virus control was wrong. He got his way with policy and it did not work. The virus finally landed on him, as if to reenact Edgar Allan Poe’s fictional story of Prince Prospero in his castle that he believed would protect him.
And as a result of his exposure, Fauci will surely (unless his repeated injection of the same vaccine harmed the operation of his immune system) gain the natural immunity that is already possessed by 78 percent of kids and likely two thirds of the general population.
It should also alert us to three points of moral urgency:
- We need to replace Fauci-style feudalism with a new theory of how to reconcile the freely functioning society with the presence of infectious disease, so that neither he nor people in his pay or sway can attempt this again.
- We need to act to disable the unmitigated power of administrative-state bureaucrats to seize control of the machinery of government.
- We need a new system to decentralize science away from privileged elites so that they can never again have monopoly control over what is considered to be the science much less posses the power to censor dissent.
These are the lessons, at least the start of them. This virus is either endemic or at least almost so, but we are left with astonishing social, cultural, and economic destruction from Fauci’s attempt to implement an experimental plan on the whole population not only in the US but all over the world.
We will suffer for many years or generations from it. And yet, in the end, infection is individual and probably unavoidable for most people. The immune system adapts. That’s how we evolved to coexist. To pretend otherwise is the very essence of denying the science.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
Disappearing MSN Article – Severe COVID-19 ‘Rare’ In Unvaccinated People, Survey Reveals
MSN quickly removes article along with the study itself

The Naked Emperor’s Newsletter | June 17, 2022
I am back after a disruptive week, flight cancelled, tech stolen etc.
The bonus about having limited access to the internet is that by the time I started to write about a news article I was reading, it had been removed. Normally I wouldn’t have noticed but my sporadic typing meant going back and forth to the article over a number of days.
I was going to write about the study in the article but instead I will preserve the original article itself which was published on MSN.com
*UPDATE – As I type the actual study has been removed as well*
Severe COVID-19 ‘Rare’ In Unvaccinated People, Survey Reveals
A survey has found that people who did not get the vaccine had a lower rate of suffering severe COVID-19 amid the pandemic.
The survey uploaded to the preprint server ResearchGate presented data from more than 18,500 respondents from the “Control Group” project with more than 300,000 overall participants. An analysis revealed that compared to those who got jabbed, unvaccinated people reported fewer hospitalizations.
The international survey also found that the unvaccinated people from more than 175 countries were more likely to self-care to prevent and manage COVID-19 infection. They used natural products like vitamin D, vitamin C, zinc, quercetin, and drugs, such as ivermectin and hydroxychloroquine.
Many participants experienced discrimination for refusing the administration of “genetic vaccines” and struggled with mental health burdens due to the stigma in the mostly “vaccinated” society.
The participants admitted to avoiding vaccines due to their preference for natural medicine interventions and skepticism of pharmaceutical interventions. They also voiced distrust of government information and fear of the possible adverse effects of the vaccines in the long run.
The survey was conducted from September 2021 through February 2022. During the period, participants experienced mild to moderate COVID-19 infection and were infrequently hospitalized.
A number of female participants suffered menstrual and bleeding abnormalities, prompting the researchers who analyzed the data to surmise that the issues might have been caused by spike protein exposure and shedding, as per The Epoch Times.
Data collected from the survey were analyzed and interpreted by an independent, international team of scientists led by Robert Verkerk, Ph.D., the founder and executive and scientific director of Alliance for Natural Health International.
The link to the original article is here but as you can see this just diverts back to the home page.
Wayback Machine seems to be empty but fortunately Google has cached it for now.
The study itself can be read on ResearchGate. (Update – this has now been removed). However, this one is still available on the Wayback Machine.
It used data from a UK citizen-led cooperative called the Control Group Cooperative (CGC). This was formed in July 2021 “to represent the interests of individuals and families around the world who have chosen to not receive COVID-19 ‘vaccine’. Among the aims of the CGC is to evaluate long-term health outcomes among the COVID-19 vaccine-free, as well as linking its members to country support networks and online community groups. Participants who join the ‘control group’ may obtain an ID card (Fig. 1), in the relevant language. The card includes the statement that the individual is part of a SARS-CoV-2 Control Group and “must not be vaccinated”. Many members have reported that these ID cards have been successful in allowing travel, preventing forced vaccination (vaccination without informed consent) or avoiding the loss of liberties, such as access to venues otherwise limited to COVID-19-vaccinated individuals.”
There were around 300,000 members of the CGC which were predominantly from Europe (40.2%) with 25% from North America and 27% from Oceania. Approximately 18,500 were part of the survey on which the study was based.
The study was independent to the CGC and looked at the first five months of survey data. By using data from this group there is an obvious bias but interesting to see the results nevertheless.
Findings included the fact that the unvaccinated did not place a disproportionate burden on health systems. In fact only 0.4% of the cohort were hospitalised with COVID-19 which compared with 0.6% for the US population as a whole.
Reasons for individuals not wanting to be vaccinated was an almost equal five way split between preferring natural medication (16.8%), distrust of pharmaceutical intervention (16.4%), distrust of government information (16.4%), poor/limited trial study data (16.3%) and fear of long-term adverse reactions (15.4%).
Almost 75% of respondents, who had COVID-19, engaged in self-care using vitamins (such as D and C), minerals (zinc), quercetin, as well as ivermectin and hydroxychloroquine. The amount of people using dietary supplements was highest in the USA with 71% of respondents but still relatively high at 60-65% in the rest of the Western world.
A surprising finding was that there were common reports of menstrual disturbances and bleeding abnormalities in the unvaccinated female cohort. The authors suggest a number of reasons this may have occurred, including: COVID-19, pandemic lifestyle changes, shedding exposure or chronic stress.
Around 40% of respondents reported mental health problems due to the psychological stress of the pandemic. It is suggested that “the mental health burden may be associated more to the human response to the pandemic, rather than psychological, fear-based reactions to any threat posed by the SARS-CoV-2 virus itself. This includes discrimination in the workplace, by peers or by family members, as well as victimisation by states (governments/health authorities) owing to ‘unvaccinated’ status.
Much of this disproportionate and discriminatory treatment is likely the result of widespread misunderstandings about, and over-stated benefits of, COVID-19 ‘vaccines’, false claims over societal risks posed by the unvaccinated, media and state propaganda and coercion to ensure high rates of COVID-19 vaccination, institutional mandates, and the desire for in-group identity as explained by social identity theory (Scheepers and Derks, 2016).”
As I said above, the study is clearly biased. However, there is some interesting data to look at (which public health authorities have largely hidden or not collected) and so this study should not be disappeared. It should remain to be dissected and analysed and if others decide the findings are nonsense, it is for them to argue the reasons why.
Why Won’t My State’s Largest News Organisation Look into These Vaccine Stories?

BY BILL RICE, JR. | THE DAILY SCEPTIC | JUNE 9, 2022
On June 8th 2022, I sent the following email to several reporters and one editor at al.com, which is the largest news organisation in my state of Alabama. I encourage other Daily Sceptic readers to send the same type of email to the major news organisations in their cities or states.
I don’t expect this news organisation to follow-up on my story suggestions and answer any of my questions, although I would be happy to be proven wrong. My main purpose is to create a record that shows that these reporters and editors are aware of many data points which strongly suggest that Covid vaccines are not ‘safe and effective’ (or necessary for children), and confirm that these ‘watchdog’ journalists will not share these types of stories with their readers. Nor will they pursue their own investigations that might corroborate (or impeach) these findings.
If enough readers participate in this similar experiment, this collective evidence (and the non-responses to our ‘story suggestions’) might provide strong evidence that the mainstream media are conspiring (or at least capitulating) in the cover-up of information that would debunk or challenge many elements of the alleged ‘settled science’ about Covid vaccines. In the opinion of this correspondent, such a finding – suggesting an obvious bias and censorship – would itself constitute an alarming and disturbing scandal.
Note: Story links and excerpts (several from the Daily Sceptic) are provided below this post.
Dear [journalists who routinely write Covid stories and an editor]:
I write to bring to your attention six articles that strongly suggest that Covid vaccines are not “safe and effective” nor necessary for many people. See story links below.
My real purpose in writing is to encourage al.com to do its own reporting to see if your reporters can confirm that the trends depicted in this quantifiable data are, perhaps, also being seen in Alabama.
Specifically:
- Are Alabama ambulance companies responding to more calls from individuals suffering health emergencies related to cardiac events than they did prior to widespread Covid vaccination?
- Are life insurance companies doing business in Alabama reporting more excess deaths in policy holders since vaccines became widespread, especially in the ages 18 to 64? What are these numbers?
- Are funeral homes in Alabama performing more funerals and cremations compared to time periods before Covid vaccines had been widely administered?
- Are doctors seeing more complications in vaccinated patients?
- Do vaccinated Alabamians now comprise the greatest percentage of PCR-confirmed Covid cases? Are the percentage of vaccinated patients being treated in hospitals now higher than the unvaccinated cohort (as appears to be the case in the U.K., whose data are much more comprehensive and transparent)? Are the percentages of deaths in older age groups (60 plus) now higher among the vaccinated class (as is also the case in the U.K. and other countries)?
- How many Alabama children under the age of 18 without serious pre-existing medical conditions have died from Covid in the past 27 months (this would be the mortality figure for ‘healthy’ children)? How many healthy Alabama children died from Covid in the first 12 months of the pandemic? Is death from Covid actually one of the ‘top eight’ or ‘top 10 causes of death of Alabama children in a given year (as has been quoted by public health officials and officials at pediatrician groups)? What are the top 10 annual killers of Alabama children with the number of annual deaths per year?
- If I wrote a 1,000-word article, listing several of the ‘accepted Covid narratives’ that I believe are false or dubious and why I believe they are, would you publish this piece?
I’ve come to believe that journalism or independent investigations that would challenge key parts of the ‘Covid narrative’ is not allowed at mainstream news organisations. Can you provide examples from your own reporting that would debunk or refute this theory? Is al.com going to follow up on these articles with your own reporting? If not, why not? Have reporters been told that certain Covid stories cannot be reported? Which al.com journalists have written any story that challenges or questions key parts of the CDC’s ‘settled science’?
Thank you for your consideration.
Bill Rice, Jr.
Supporting link and excerpts:
Virology Journal has published a letter from a cardiovascular surgeon, Kenji Yamamoto, setting out the case for ceasing all Covid vaccine booster programmes on safety grounds, calling Covid vaccines a “major risk factor for infections in critically ill patients”. His own cardiovascular surgery department at Okamura Memorial Hospital, Japan, has seen numerous complications in vaccinated patients, including some deaths, he says.
The National Health Service has confirmed in response to a freedom of information request that ambulance call-outs relating to immediate care required for a debilitating condition affecting the heart nearly doubled in the whole of 2021 and are still on the rise further in 2022. But the most concerning published figures show that they have also doubled among people under the age of 30.
“Indiana Life Insurance CEO Says Deaths Are Up Among people Ages 18-64“:
We are seeing, right now, the highest death rates we have seen in the history of this business – not just at OneAmerica,” the company’s CEO Scott Davison said during an online news conference this week. “The data is consistent across every player in that business.” …
Davison said the increase in deaths represents “huge, huge numbers,” and that’s it’s not elderly people who are dying, but “primarily working-age people 18 to 64” … “Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic,” he said. “So 40% is just unheard of.
On Wednesday, Dowd noted that funeral home company Carriage Services saw a 28% increase in September 2021 vs. 2020, and a 13% increase in August vs. the same period. Funerals and cremations are up 12% and 13% respectively on the quarter.
“Unbelievable U.K. Vaccine Report Update“:
Already evident in previous weeks is that for all but the youngest group, the vaccinated were getting infected at higher rates than the unvaccinated … In several age groups, it would appear the double vaccinated are infected at four to five time the rate of the unvaccinated …
Looking at double (not triple) vaccinated, it appears they have higher rates of hospitalisation for all ages over 60, and comparable rates for ages 18-59.
In this case, the rate of death of the unboosted fully vaccinated is basically twice as high for the over 70 year olds.
“For Majority of U.K. children, Covid Mortality is 0.000“:
Only six of the 25 Covid deaths in the U.K. in the first 12 month of the pandemic occurred among children without pre-existing serious medical conditions … This represents a mortality risk to ‘healthy’ children of approximately 0.0001%.
Should the patient really get the drug?
By Sebastian Rushworth, M.D. | June 14, 2022
I recently gave a lecture to 70 primary care physicians here in Stockholm, titled “should the patient really get the drug?”. The lecture seemed to generate quite a bit of cognitive dissonance among some in the audience, based on the somewhat aggressive discussion that followed the lecture, which suggests to me that much of what I was saying was stuff they had literally never been exposed to before – not at any point in medical school, and not at any point during their careers after medical school either. Cognitive dissonance is good. It’s the first step towards change.
I thought it would be interesting to re-write the lecture as an article, so that more people can hopefully achieve similar levels of cognitive dissonance. Please feel free to share it with any doctors you know that you think might benefit from an expanded perspective. Anyway, here we go.
Let’s imagine a common patient. Every primary care physician meets this patient, or someone much like her, on an almost daily basis. She’s 75 years old, and overweight. She experienced a wrist fracture two years ago, and was subsequently diagnosed with osteoporosis. She has high cholesterol levels, but she’s never had a heart attack or other “cardiovascular event”. On top of that, she has type 2 diabetes, chronic knee pain due to osteoarthritis, and high blood pressure. She was diagnosed with depression a few years ago, after her husband died.
Our patient takes seven drugs every day:
- Alendronate, because of her weak bones.
- Atorvastatin, because of her high cholesterol levels.
- Sertraline, because of her depression.
- Metformin, because of her type 2 diabetes.
- Insulin, also because of her type 2 diabetes.
- Paracetamol (a.k.a. acetaminophen), because of her knee pain.
- Enalapril, because of her high blood pressure.
So, the question is, are these drugs doing her any good?
Well, to answer that question, we need to consider NNT (Number Needed to Treat). NNT is the number of patients who need to take a drug for one patient to achieve a noticeable benefit.
For alendronate, the NNT is 20, i.e. if you treat 20 people for a couple of years, you prevent one fracture. For atorvastatin the NNT is 200, i.e. you need to treat 200 people for five years or so in order to prevent one heart attack. For sertraline, the NNT is 7, which means that you need to treat seven people in order to have a noticeable effect on depression in one patient. Note that this doesn’t mean that one out of seven gets cured of their depression, it just means that there is a noticeable difference on a rating scale for depression.
For metformin, the NNT is 14 – If you treat 14 type 2 diabetics with metformin for ten years, you prevent one death. For enalapril, the NNT is 70 – If you treat 70 people with high blood pressure with enalapril for five years or so, you prevent one stroke.
For insulin, however, there is no NNT, because insulin has not been shown to result in any benefit on any clinically relevant outcome, even though big studies have been carried out that have included thousands of patients and followed them for five or ten years. Note here that we’re talking about insulin for type 2 diabetics. When it comes to type 1 diabetes, insulin is pretty much magical – you don’t even need to do a randomised trial in order to show benefit. People with type 1 diabetes virtually return from the dead when treated with insulin. But when it comes to type 2 diabetes, there is no benefit, at least not to any hard outcomes. All insulin has been shown to do is reduce blood sugar, but it’s never been shown to result in any meaningful patient oriented benefit for type 2 diabetics.
The same is true for paracetamol/acetaminophen. When it comes to patients with knee pain due to osteoarthritis, the drug doesn’t provide any benefit whatsoever.
Ok, so we have seven drugs, and we know what their NNT’s are. If we plus the probabilities of benefit together, then we get the probability that our 75-year old woman will benefit in some way from at least one of the drugs she’s taking. So, what probability of benefit do we get?
We get 30%. Only 30%.
What that means is that there is a 70% probability that this woman doesn’t benefit at all from any of the seven drugs that she takes every day for years on end!
If you told her, I’d say there are pretty good odds she’d decide to stop taking her pills. Seven drugs a day, every day, and two to one odds of zero benefit.
And we haven’t even talked about harms yet. Because none of these pills are inert. All have widespread biological effects. And all can cause harms. So any rational treatment decision must include not just the potential benefits, but also the potential harms.
For figuring out harms, we have NNH (Number Needed to Harm), which is the counterpoint to NNT. NNH is the number of patients who need to get a drug for one to be harmed. Like I said, the drugs all have widespread biological effects, so there isn’t just one NNH – there is an NNH for each possible harm. That means that there are multiple NNH’s for each drug.
With our 75-year old woman and her seven drugs, we don’t have time to go through the NNH for every possible side effect, so we’re just going to look at a few, and put them side by side with the NNT, to get a somewhat more complete picture of benefits vs harms. I’ve tried to make sure that the NNH numbers apply to the same time period as the NNT numbers, since otherwise it’s an apples to oranges comparison.
If we do that, we get something like this:
Alendronate
NNT: 20 (fractures)
NNH: 200 (esophagitis), 260 (atrial fibrillation), 4,000 (osteonecrosis)
Atorvastatin
NNT: 200 (cardiac infarction)
NNH: 20 (myalgia), 20 (type 2 diabetes)
Sertraline
NNT: 7 (depression)
NNH: 2 (sexual disturbance), 10 (hyponatremia)
Metformin
NNT: 14 (death)
NNH: 2 (stomach upset), 5 (B12 deficiency), 1,000 (lactic acidosis)
Enalapril
NNT: 70 (stroke), 125 (death)
NNH: hyperkalemia (10), acute kidney failure (100)
Insulin
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: severe hypoglycemia (5), weight gain (1)
Paracetamol/acetaminophen
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: Hypertension (30), liver damage (?)
It’s possible to quibble here about specific NNT and NNH numbers. Different studies show different things. And many of the numbers come from studies carried out by pharmaceutical companies, which generally means that the risk of a certain side effect is massively underestimated (as we will discuss shortly). The point here isn’t to get hung up on any of the specific numbers. It’s to illustrate that we quickly end up with a very complex equation, where it in many cases isn’t clear at all whether the benefits outweigh the harms.
Take alendronate, as an example. We know that it decreases fractures in elderly osteoporotic women. But it doesn’t decrease hospitalisations. The only reasonable conclusion is that the reduction in hospitalisations that is seen due to the reduction in fractures is made up for by an increase in hospitalisations due to the many and varied side effects. So at the end of the day the only way to decide whether or not to take the drug is to have a detailed discussion with the patient and get them to decide which set of risks they’d rather be taking.
Hippocrates is supposed to have said “primum non nocere”, which is latin for “first, do no harm”. Actually he didn’t say that, and couldn’t have even if he wanted to. Hippocrates was greek, and didn’t speak latin. The quote comes from a 19th century American physician, Worthington Hooker.
Of course, as doctors, we all know that “first, do no harm” is completely unrealistic. Every intervention we do carries some measure of risk. If our primary guiding principle was to never do harm, we literally would never be able to do anything. A more reasonable principle is “only do something if the benefits clearly outweigh the risks”. If it isn’t clear to you that the benefits of a drug outweigh the harms, then don’t give it to the patient.
That’s a good general rule to stick by. However, it probably isn’t enough, for a few reasons we’re now going to discuss.
A study was published in JAMA Internal Medicine in 2021 that sought to establish how good physicians are at estimating the likelihood that a patient has a certain disease. 500 primary care physicians in the US were asked to consider various hypothetical scenarios, and then answer what they thought the probability of disease was. Here’s an example of a scenario that they were asked to consider:
Ms. Smith, a previously healthy 35-year-old woman who smokes tobacco presents with five days of fatigue, productive cough, worsening shortness of breath, fevers to 102 degrees Fahrenheit (38.9 degrees centigrade) and decreased breath sounds in the lower right field. She has a heart rate of 105 but otherwise vital signs are normal. She has no particular preference for testing and wants your advice.
How likely is it that Ms. Smith has pneumonia based on this information? ___%
Ms. Smith’s chest X-ray is consistent with pneumonia. How likely is she to have pneumonia? ___%
Ms. Smith’s chest X-ray is negative. How likely is she to have pneumonia? ___%
Go ahead and make your own guesses in relation to each of the three questions.
Once you’ve done that, you can take a look at the table below, and the answers will be revealed.

So, for our pneumonia example above, we see that the actual initial risk of disease based on the presented information was around 35%. If we then move along and look at what the doctors answered, they thought the risk was 80-85%. In other words, they thought pneumonia was more than twice as likely as it actually was!
The same phenomenon was seen in all clinical scenarios tested. The doctors consistently overestimated the initial risk, and they continued to overestimate the risk after both a positive and a negative test result. In some cases the difference between reality and what the doctors thought was huge, with the doctors overestimating risk by a factor of ten or more.
What can we conclude from this?
Doctors consistently overestimate disease risk.
Hold that thought, as we move on to take a quick look at another study, which was published in BMJ Open in 2015. This study sought to do something about a problem inherent in statin trials (and for that matter, all trials in medicine), which is that the results they produce, in the form of percent absolute risk, percent relative risk, and NNT, are so abstract that they’re completely meaningless to patients (and for that matter, to doctors as well). We know that statins have an NNT of 200 when used for primary prevention (to prevent a heart attack in someone who has risk factors but hasn’t already has a heart attack), and 40 when used for secondary prevention (to prevent additional heart attacks in someone who has already experienced a heart attack). But what do those numbers actually mean? Are they good or bad?
What the patient really wants to know is “how much longer will I live if I take this drug?”
So, what the researchers did was gather together data from all the big randomised trials of statins, and use the survival curves provided to estimate how much longer the patients actually lived. Here’s what they came up with:

All the big statin trials are included here. What’s interesting to do is look at the NNT provided, and then compare that with the number to the right of it, which is how much longer the patients actually lived, on average. So, for the ALLHAT trial, to take the topmost example, we have an NNT (for primary prevention) of 250, which comes down to a postponement of death of 4.96… well, 4.96 what?
Is it years? No.
Is it months? No
The patients in the statin group lived 4.96 days longer than the patients in the placebo group. That is what the NNT of 250 means in real terms.
Let’s look instead at 4S, which was published in 1994 and is the statin trial that has produced the best results of any statin trial ever. It’s the trial that initiated the massive boom in statin prescribing that we still see today. In 4S, the NNT (for secondary prevention) is 27.8. So, in other words, one in 27.8 patients benefited from the treatment.
But what does that actually mean in terms of life extension?
It means 27 days.
Not as impressive as you would have thought, right?
When the researchers put all the data together, from all the trials, in order to get an overall average, what they found was that when statins are used for primary prevention they prolong life by 3 days. When they are used for secondary prevention, they prolong life by 4 days.
I can imagine quite a few patients turning down the offer of a statin if they knew that it will on average only prolong their life by days.
The purpose of bringing up this study was to illustrate the following general point:
Doctors consistently overestimate the benefit of the drugs they prescribe.
Hold that thought in your mind as we move on and look at a third study.
This one was published in The Lancet Healthy Longevity in 2021. It compared the rate of serious side effects seen in randomised trials with that seen in the real world. If randomised trials give us good information about what to expect in reality, then the rate of serious side effects in the trials should be the same as that seen in reality.
But that isn’t what the researchers found. What they found was that serious side effects were three to four times more common in reality than they are in the randomised trials! Three to four times!
How is this possible?
Well it’s important to remember that the randomised trials are funded and run by the drug companies, and the drug companies want to sell their drugs, so they will do what they can to make side effects appear as rare as possible.
Why is this a problem? Because it’s the randomised trials that doctors mostly use as a basis for determining whether a drug is safe to give to a patient or not.
So, what can we conclude from the study?
Doctors consistently underestimate side effects of drugs.
Ok, so we have three conclusions, that are all pointing us in the same direction:
- Doctors consistently overestimate disease risk.
- Doctors consistently overestimate drug benefit.
- Doctors consistently underestimate drug harm.
What does this lead to?
Massive overprescribing of drugs.
Peter Gotzche, a founding member of the Cochrane Collaboration and former director of the Nordic Cochrane Center, has estimated that prescription drugs are now the third biggest cause of death in the western world, after heart disease and cancer.
That on its own should lead to massive humility among all doctors about our drug prescribing. It should make us much more careful every time we think about prescribing a drug to a patient.
Ok, so we’ve identified the problem. The causes of this problem are many and complex, so I’m just going to bring up one that each of us as doctors can actually do something about – industry sponsored meals.
A study was published in JAMA Internal Medicine in August 2016 that sought to estimate the extent to which physicians are influenced by partaking in industry sponsored meals, which often take the form of a lecture about a specific drug given by an drug company salesperson, which the physician is supposed to sit and listen to in return for getting a free meal. Industry sponsored meals are very common. Most physicians probably take part in at least a couple of these per year, and many take part in far more than that.
As the saying goes, “there’s no such thing as a free lunch”. The drug companies are not charities whose goal it is to keep starving doctors alive. If they spend vast sums of money of sponsored meals, it’s because they’re pretty damn sure that it increases sales of their drugs, and thereby their profits.
So, anyway, the study sought to estimate the extent to which industry sponsored meals influence physician prescribing patterns, by comparing participation in such meals with later prescribing behaviour. Here’s what they found:

They looked at four different drugs. As I think is clear from the tables, participation in industry sponsored meals increased prescribing of the drug the meal was about, and the more such meals a doctor participated in, the more often he or she prescribed that drug.
The purpose of these meals is not to educate us, or make us better doctors. It’s the opposite – the purpose is to make us do a specific profit-driven company’s bidding. And it works.
If you’re a doctor, and you think you don’t get influenced by participating in industry sponsored meals, then you are very naive. The more industry sponsored meals we participate in, the worse doctors we become.
Doctors in general massively underestimate the extent to which their thoughts, beliefs, and opinions are influenced by the pharmaceutical industry. We like to think that we are evidence based. But the truth is that much of what we think we know is not based on sound scientific knowledge, but on pharmaceutical industry propaganda, which quickly becomes clear to anyone who starts going through the studies in detail themselves.
On that note, I strongly recommend reading these three books, all written by physicians, to help get some perspective on the scale of the problem we face in relation to the pharmaceutical industry.
- Bad Pharma by Dr. Ben Goldacre
- Doctoring data by Dr. Malcolm Kendrick
- Deadly medicines and organised crime by Dr. Peter Gotzsche
There is one very simple thing every doctor can do, to at least partially free themselves from the onslaught of drug company propaganda, and that is to refuse to take part in industry sponsored lunches, and all other forms of industry sponsored “education”. Just say No.
Ok, so, that’s number one: refuse to take part in industry sponsored lunches.
What else can you do as a doctor?
Well, something that was once considered standard, but has fallen by the wayside in recent decades, is to never have a patient on more than five drugs at the same time. With drugs, as with everything else, there is a state of diminishing returns – the more you add, the less benefit (and more harm) each additional drug confers. So try to keep a patient on at most five simultaneous drugs. If you want to add a sixth, then rank them all, and get rid of the one that you think is least important. Most likely, the sixth least important drug in a list of six is not going to do anything useful for the patient anyway, just increase their risk of harm.
Ok, so that’s number two: try to avoid having your patients on more than five drugs simultaneously.
Number three: go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit. As any doctor will know, it’s common for patients to stay on drugs for years, even though the original reason they were put on the drug resolved itself a long time ago. The patient often doesn’t remember why they were put on the drug in the first place, but they keep taking it dutifully. Drug lists require regular pruning or they will become increasingly bloated as the years go by, which is one reason why so many elderly people are on 15 simultaneous drugs or more.
Number four: only prescribe a drug if the benefits clearly outweigh the harms. This should be obvious, but it requires a deep knowledge of the size of both potential benefit and potential harm, which unfortunately most doctors lack. And what they think they know is often incorrect because it’s based more on pharma propaganda than real science.
As a doctor, the only way to get around this is to start doing your due diligence and getting in to the weeds of the scientific studies. Do that for the ten drugs you prescribe most commonly, so that you’re an expert on those ten drugs, and you’ve already done a lot. If a patient asks you about the probability of benefit and the probability of harm, you should be able to answer that question correctly, at least for the ten drugs you use most frequently. It requires an up-front investment of time, but it will pay massive dividends to your patients over the remainder of your career.
Ok, so that was number four: only prescribe a drug if the benefit clearly outweighs the harm.
Here’s number five: prioritise lifestyle changes. Most of the diseases that doctors spend most of their time dealing with are caused by poor lifestyle choices. And most can be rectified by switching to good lifestyle choices, which invariably produce greater benefits than any drug can, with less risk of harm.
Doctors can accomplish a lot with their patients with simple lifestyle coaching. To take one example, a primary care clinic in the UK decided to try putting their type 2 diabetic patients on a ketogenic diet, since the drugs they were using clearly weren’t making the patients better. They published their six year follow up results in BMJ Nutrition, Prevention, and Health in 2020.
Over six years, the patients following the ketogenic diet decreased their median HbA1c (a measure of average blood sugar over the preceding few months) from 66 to 48. Normally, that would be unheard of. HbA1c doesn’t decrease over time in a type 2 diabetic. It increases. Yet here it was far better at the end of the six years than at the beginning. The same goes for body weight. Normally it goes up over time. But here the median decreased from 99 kg to 91 kg. And on top of that, median systolic blood pressure dropped from 152 to 141.
All this just with a simple diet intervention. Thanks to the improvements in all health markers, the patients were able to get off a lot of their drugs. This meant that after six years, the clinic was spending less than half as much money on anti-diabetic drugs as the other primary care clinics in the region.
To take another example of a simple lifestyle intervention, a randomised trial published in BMJ in 2021 that was carried out in nursing homes in Australia found that a diet high in protein has an effect on fracture risk that is equivalent to that seen with bisphosphonates.
There is a massive amount that can be accomplished with simple lifestyle interventions, and since they are much less risky than drugs, and actually treat the underlying problem rather than just putting a patch on top of it, they should be the primary intervention we use whenever possible. Drugs should be viewed as a complement to lifestyle interventions. It shouldn’t be the other way around.
Ok, so that was my fifth and final point. I’ll repeat the five points here again. These are five things that you as a doctor can do about the situation we currently find ourselves in, where prescription drugs are the third biggest killer in the western world:
- Refuse to participate in industry sponsored lunches and other industry sponsored “education”.
- Try to avoid having your patients on more than five drugs simultaneously.
- Go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit.
- Only prescribe a drug if the benefits clearly outweigh the harms.
- Prioritise lifestyle changes.
Featured Video

Israel furious at Trump over Turkey, Syria to invade Lebanon
or go to
Aletho News Archives – Video-Images
From the Archives
The toxic legacy of nuclear weapons testing serves as a stark warning of the danger these weapons pose
By Scott Ritter | RT | March 11, 2021
Millions of people suffer and die from the effects of radiation exposure from decades of nuclear weapons testing. Their experience should give serious pause to those who continue to embrace the viability of a nuclear deterrent.
A dust storm originating in the Sahara Desert swept across parts of Spain, France, the UK, and Ireland last month. In addition to bringing a red tinge to the sky, the dust caused a slight, yet noticeable, spike in radiation in the areas it reached. This radiation spike was caused by the presence of cesium-137, a radioactive isotope produced through the nuclear fission of uranium-235 in nuclear weapons. A legacy of French nuclear weapons testing that occurred in Algeria during the 1960s, the cesium-137 contamination is a reminder that while the testing of nuclear weapons may have been halted for the time being, the consequences of these tests live on through the poisoning of the planet mankind calls home.
The Saharan radioactive dust cloud is but the most recent visible phenomenon of a plague that has infected much of the world. … continue
Blog Roll
 Aletho News
Aletho News- Abelardo De la Espriella’s Victory Renews Pressure on Venezuela
- Israel furious at Trump over Turkey, Syria to invade Lebanon – w/ Col. Macgregor
- IRGC says it struck US military positions, warns of broader response
- Russia stops record number of Ukrainian drones overnight – MOD
- Denmark admits ‘no evidence’ for Russian drone hysteria
- Washington agreement ‘will not pass’: MP Fadlallah
- Iran mocks US for ‘solving’ domestic hunger problem, lecturing others on issue
- Germany, Israel hold joint naval drill off Haifa amid Gaza genocide
- Trump’s war on Iran becomes ‘most unpopular conflict’ in US history
- The Middle East is wringing its hands of Washington. Finally
- If Americans Knew
- Four Reasons the Netanyahu-Backed Plan to ‘End’ U.S. Military Aid to Israel Is a Scam
- Archbishop of Canterbury vows to help Palestinians achieve ‘freedom you deserve,’ calls for end to Israeli occupation
- The scars left behind by Israel’s white phosphorus in Lebanon
- Drones and decomposing babies: What’s in UN report on Israel’s genocide of Palestinian children
- Crimson Thread: The new Israeli separation wall that cuts through the ‘breadbasket of Palestine’
- Gaza ceasefire talks back to square one as Israel changes the rules – Daily Update
- The NDAA Proposed Merger of the U.S. and Israeli Military is Strategically Unwise and Inherently Unconstitutional
- Victories by Pro-Palestinian Democrats Show the Party’s Shift on Israel
- Massie moves to strike $3.3B in Israel military aid from the budget
- How Jeffrey Epstein’s Israeli Network Shaped Congo’s Deadly Mineral Trade
- No Tricks Zone
- 2025 Study: Cloud Effects Reduce Downwelling Longwave Radiation, Overriding The CO2 Impact
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
