Suppose an individual is infected with a novel pathogen, and then sometime later is infected with a related version of the same pathogen. If ‘original antigenic sin’ is present, the individual’s immune system will respond to the antigens carried by the original version of the pathogen, resulting in weaker immunity.
The idea is that, for certain classes of pathogen, the immune system’s response to any particular exposure depends on an individual’s first exposure. If two versions of a pathogen, A and B, are circulating in a population, individuals who were first exposed to A may develop weaker immunity against B, and vice versa.
There is substantial evidence that original antigenic sin applies to influenza: those who gain immunity to one strain of influenza may develop weaker immunity to other strains.
It can also apply to vaccines. As a recent review notes, “if we only immunise to a single strain or epitope, and if that strain/epitope changes over time, then the immune system is unable to mount an accurate secondary response.”
At the end of last year, ‘mainstream’ commentators began discussing the possibility that original antigenic sin applies to the Covid vaccines. If it does, we may have vaccinated millions of young people against a version of Covid that poses little risk to them, at the cost of weakening their immunity to subsequent variants.
Now ‘original antigenic sin’ has been mentioned in the context of Covid vaccines in the pages of the New England Journal of Medicine – the world’s most ‘prestigious’ medical journal.
Noting that boosters are “not risk-free”, the American immunologist Paul Offit writes: “all age groups are at risk for the theoretical problem of an ‘original antigenic sin’ – a decreased ability to respond to a new immunogen because the immune system has locked onto the original immunogen.”
He cites a recent preprint by Matthew Gagne and colleagues, who carried out an experiment on nonhuman primates. They began by giving two groups of primates the Moderna vaccine. After 41 weeks, they gave each group a booster shot. One group received the Moderna vaccine again, while the other group received an Omicron-specific booster.
Finally, both groups were exposed to Covid. The researchers measured memory B cells and found that the Omicron-specific booster “provided no advantage” over the original Moderna vaccine. Indeed, they “did not observe a population of Omicron-only memory B cells before or after the boost that was clearly distinct from background staining”.
This means the Omicron-specific booster did not produce any detectable Omicron-only memory B cells at all, though it did trigger the production of more memory B cells specific to the original SARS-CoV-2 strain. It’s important to note, however, that both boosters did increase memory B cells (and neutralising antibodies) to some extent. (Neither was totally ineffective.)
As Gagne and colleagues note, the fact that memory B cells were no higher in the group that received the Omicron-specific booster “likely stems from the principle of original antigenic sin”. How serious this problem turns out to be will depend on several factors, not least subsequent viral evolution.
Offit writes in the NEJM that it “could limit our ability to respond to a new variant”.
Russia says Israel is supporting “the neo-Nazi regime in Kiev”, raising the stakes in its tensions with Tel Aviv over the raging war in Ukraine.
The spat began after Russian Foreign Minister Sergei Lavrov, speaking to Italian outlet Mediaset’s Rete 4 channel in an interview released Sunday, said that Adolf Hitler had Jewish origins.
Israeli foreign minister Yair Lapid on Monday accused Lavrov of making an “unforgivable and outrageous statement as well as a terrible historical error” and summoned Moscow’s ambassador for “clarifications”.
“We have paid attention to Foreign Minister Yair Lapid’s anti-historical remarks, which largely explain the current government’s decision to support the neo-Nazi regime in Kiev,” said the Russian foreign ministry in a statement on Tuesday.
“History unfortunately knows tragic examples of cooperation between Jews and Nazis,” it said.
In his interview, Lavrov said Ukrainian President Volodymyr Zelensky “puts forward an argument of what kind of Nazism can they have if he himself is Jewish”.
Lavrov, according to a transcript posted on the Russian foreign ministry website, then added: “I could be wrong, but Hitler also had Jewish blood”.
Israeli prime minister Naftali Bennett characterized Lavrov’s remarks as “lies” that he said effectively “accuse the Jews themselves of the most awful crimes in history”, perpetrated against themselves.
On Tuesday, the Russian foreign ministry said “the Jewish origins of the president (Zelensky) is not a guarantee of protection against rampant neo-Nazism in the country”.
“Ukraine, may it be said in passing, is not the only one in this case,” the ministry said, citing Latvian President Egils Levits who “has also Jewish roots and he also gives cover… to the rehabilitation of the Waffen SS in his country”.
Israel has expressed solidarity with Ukraine but unlike its Western allies, it has refrained from enforcing formal sanctions on Russia over its military operation in the neighboring country.
Last month, Lapid accused Russia of committing war crimes in Ukraine. Moscow hit back, accusing Israel of using Ukraine to “distract” the world from its ongoing aggression against Palestinians.
A week ago I wrote a piece describing how Israel’s power over the US government is such that no American official will confirm that the Israelis have, and have had for years, a secret nuclear arsenal consisting of as many as 200 nukes. The situation is particularly odd in that the United States is on record as being strongly opposed to nuclear proliferation, except for Israel, and the enriched uranium that was used to create Israel’s bombs as well as the nuclear triggers were stolen and exported illegally from the US. Former Israeli Prime Minister Benjamin Netanyahu himself was reportedly involved in the thefts. One lawyer friend has suggested that the reason for the reticence is that under US law by way of the Symington Amendment, no assistance or aid can be given to any country that has not signed the Nuclear Non-Proliferation Treaty (NPT). Israel has not signed and also has a widely acknowledged nuclear arsenal. To preserve Israel’s billions of dollars in annual largesse from the US taxpayer, silence over what goes on when the government breaks its own laws must be maintained. Some might consider that a case of pandering to Israel rather than taking steps to enhance United States security, but when it comes to the Jewish state that argument is a non-starter in Washington as Israel always comes first.
This week I am going to describe another aspect of the Zionist state’s policy that has been invisible if one relies on the mainstream media or the chattering magpies that occupy Capitol Hill and the White House. That is the ongoing elimination of Christianity in the region where it was born being carried out by Israel and its friends. The United States has been the enabler of much of the change in spite of the prevalence of self-described devout Christians in Congress, many of whom ironically are vocal and even enthusiastic supporters of Israeli “security” policies. Killing Palestinians is all too often justified in Congress and the White House with the meaningless expression “Israel has a right to defend itself.”
American power wielded on behalf of Israel has already destroyed a thriving Christian community in Iraq while still laboring to do the same in Syria and possibly even Lebanon. At Christianity’s very birthplace, in what was once Palestine, Israel has been engaged in making the lives of Palestinian so miserable that they frequently choose to emigrate. Israel’s first Prime Minister David Ben-Gurion famously declared in a letter to his son that “We must expel the Arabs and take their places…” and he exploited massacres of unarmed civilians carried out by the Haganah to create terror to accomplish that end. Since that time, Israel has refused to allow Palestinians driven from their homes by the 1948 fighting to return, has destroyed more than 400 Arab villages and confiscated other Palestinian properties, has appropriated additional land and water resources for its illegal settlements, has allowed armed settlers to destroy Palestinians crops and other forms of livelihood, and controlled Palestinian movements through a network of Jews only roads and numerous checkpoints. Even Palestinians who happen to be Israeli citizens are legally and in practice treated like second-class citizens with limited rights. There are more than 60 laws in Israel that discriminate against non-Jews while Israel now legally defines itself as a Jewish state. Israel has also imprisoned without any trial thousands of West Bank and Jerusalem Palestinians, including children, and shot dead hundreds more.
I could go on, but the point is that Israel wants Palestinians gone, a process that has particularly impacted on the Christian community. It has not been done by ethnic cleansing in the classic sense after the initial Nakba massacres and appropriations in 1948, but rather accomplished by creating incentives to leave. And it has been successful. At the end of the Second World War, an estimated one third of the Palestinian population identified as Christian, but the percentage is currently closer to 9% and continuing to decline. The numbers suggest that Christians in the former Palestine are verging on extinction. In fact, Christians have been able to become disproportionately emigrants from their homeland because they more frequently than Muslims have family already established in Europe and the US and have also been able to rely on networking through their churches for resettlement assistance in a new country.
Even by the wretched standards of the past 70 years, Israel’s seeking a “final solution” with the Palestinians recently has become particularly outrageous, focusing as it does on loosening their ties to their religious and cultural institutions while also destroying their livelihoods and appropriating their properties.
Hardly reported in the US media was the use of new Israeli imposed security restrictions to disrupt this year’s Palestinian Christian Orthodox Easter celebrations of Christ’s Resurrection at the Church of the Holy Sepulcher in Jerusalem. This comes on top of similar police action to support the usual crowd of rampaging settlers and other Jewish extremists at the most recent Ramadan services held by Palestinian Muslims at the al-Aqsa Mosque, which included using a drone to fire tear gas at worshipers.
What took place during Holy Week and more particularly on Easter Sunday has been described by Rod Dreher, who writes for The American Conservative. I will confess that I do not much like Dreher as he is fond of celebrating himself in everything he writes, full of navel gazing and smug sanctimonious twaddle, but as he was a participant and eye witness to what occurred his account is of necessity extremely valuable. To be sure, he makes it clear that readers understand that he is not criticizing Israelis in general, nor is he engaging in anything objectionable to Jewish sensitivities when he includes himself in how “we American Christians, especially those who support Israel,” also as “an American who cares about Israel,” and who refers to “my Israeli Jewish friends” and then goes on to assert “I condemn anti-Semitism unreservedly. Criticizing the Jewish settlers and official Israeli policy does not constitute anti-Semitism” before concluding that “most Israeli Jews wouldn’t support these hate-filled radical settlers.”
Actually, the US and other governments as well as many states do believe that criticism of Israel is anti-Semitism as defined by the International Holocaust Remembrance Alliance. And, depending on how the question is phrased many, possibly most Jews worldwide, support firm action against Muslims in particular, who are routinely described in the media and by the Israeli government as “terrorists.” Rod clearly understands that it is a bad idea to veer into areas that Jews are uncomfortable with as they can be surprisingly sensitive and unreasonably reactive to perceived slights. No need to bite the hand that feeds you, as one might put it, particularly if one wants to stay employed.
Dreher reports how he was “staying at a hotel inside the Old City, where I was advised to book a room out of fear that the Jerusalem police would not let Christians into the Old City on Holy Saturday. This turns out to have been very good advice.” Holy Saturday for Orthodox Christians features a “miracle” of the Holy Fire, which is believed to be the first sign of the Resurrection of Jesus. Normally, at 11 am, the Church of the Holy Sepulcher opens and is quickly packed with believers. After noon, the Greek Patriarch the “little house” built directly over the tomb of Christ, prays, and what is referred to as “divine energy” descends from heaven to light the Patriarch’s candles, the flames from which are shared with everyone present. He then emerges and passes the flame to everyone there.
Dreher and a friend reportedly left their hotel early to pray but when they arrived at the end of the street at the Jaffa Gate, two Jewish police officers refused to allow them to pass out of the Old City, warning that if they left they might not be able to come back in. They then walked over to an access point to the Jaffa Gate, and witnessed a large group of Christians behind a barrier on the other side, blocked from entering into the Old City where the Church of the Holy Sepulcher is situated. Dreher observed that at the same time Orthodox Jews wearing white prayer shawls, entered freely into the Old City on their way to the Western Wall to pray on the Jewish Sabbath. Later that morning, Dreher was only allowed to pass into the Church of the Holy Sepulcher because he had obtained a ticket to the “fire” service. The tickets, to control and limit attendance at the church was an innovation by the Israeli police. The Patriarch objected, observing that tickets had never before been required. The tickets allowed entry of only 1,800 worshipers in the church, which normally accommodates 10,000, a reduction of 82% of the faithful permitted to be in attendance on the highest of all holy days.
An Anglican priest from Virginia who spoke to Dreher at the service described that morning’s experience this way: “Police checkpoints were at every corner. Even when we reached the private property of the Greek Patriarchate, police had taken over there as well. They actually turned back nearly a dozen Consuls General and other diplomatic representatives, including ones from the United States. We had to take an alternative route to get inside. If that was the way it worked for VIPs, imagine you’re a local Palestinian Christian simply trying to worship on the holiest of Christian holidays inside the church built over the very Tomb of Christ.”
At issue are demands by radical Jewish groups, most notably the extremist Jewish settlers’ organization Ateret Cohanim, a type of Jewish Taliban, to “cleanse” Jerusalem of all non-Jews. They have been aggressively buying or otherwise occupying properties in and around the traditional Christian and Muslim quarters of the city and often use violence when they are resisted by local residents. Christians, unlike the Muslim community, notably do not tend to resort to violence in support of their property or civic rights even though recourse to the Israeli courts is useless as the judges have consistently sided with the settlers and police.
In Jerusalem there have been regular instances of verbal abuse, vandalism and spitting on Christian clergy, as well as sporadic violent assaults. In the Armenian Christian quarter a monk reports how “[The settlers] destroy the tires of our cars, graffiti ‘death to Christians’, break windows, they desecrate our cemetery, you know… ugly things, and it’s really invasive.” Some Christians have pointed to what happened to the former St John’s Hospice near the Jaffa Gate as a prime example of what the Christian churches fear could happen across the quarter. The building’s lintel still shows the tau-phi monogram of the Greek Patriarchate but in 1990, this pilgrims’ hostel was illegally occupied by Ateret Cohanim, and now the vast building is covered with multiple Israeli flags and houses violent armed Israeli settlers. The local Christians Dreher talked to “believe that this is part of a settler plot to choke off access to Christian holy sites within the city, and force Christians out.”
The Israeli authorities tend to ignore the settler activity as they have powerful supporters, including from the diaspora community in the US and some Evangelicals who help to fund them. Ateret Cohanim’s 2010 annual gathering featured as guest speaker no less than John Bolton and the Kushner Family Foundation has reportedly helped finance its activities. In addition, Israel’s religious conservative parties are a necessary component in the coalition government and their extreme behavior is tolerated and even aided and abetted on the sly. Nor will secular Jews stand up for their Christian brothers in Israel in enough numbers to matter. Also, many Israelis believe that increasingly hardline radical Jewish groups are actually the future of Israel based on demographic trends. All excuses aside, clearly enough of the ruling elite in America, and in Israel, support the radical settlers, or none of this would be happening.
And the situation is little better for Christians in Palestine outside Jerusalem. A Franciscan monk visitor to a monastery outside of the city reported how the Israeli authorities had cut off water to the building while the missionaries themselves were verbally abused and had rocks and other debris hurled at them by settlers. In Bethlehem, a Christian gift shop was deliberately put out of business after nearby Jewish settlements were allowed to erect walls blocking access to it. Other attacks on Christians have included a June 2015 arson incident at the Church of the Multiplication and a nearby Benedictine monastery in Tabgha, located 120 miles north of Jerusalem. The church is built on the site where Christ fed the 5,000 through the multiplication of loaves and fishes. The attackers left Hebrew graffiti on the walls, reading “all idols will be smashed.” In 2014 occurred vandalization of a Romanian Orthodox church, the Benedictine Abbey of the Dormition, and Catholic offices in Jerusalem, as well as a monastery in Beit Shemesh. The year before, more than 20 Christian sites of the Latin Patriarchate were attacked by vandals. And in 2012, a Trappist monastery in Latroun was subject to arson and graffiti, while the Convent of St. Francis on Mt. Zion was vandalized. Non-Jews in Bethlehem and on the West Bank meanwhile live under a system of Israeli military laws and check points established by government order number 101. In Hebron, non-Jews living on Jewish-only streets cannot even walk out their front doors and they are regularly bombarded by feces and other waste hurled down upon them by the settlers.
Israel’s anti-Christian policies are international and includes support of groups the US has called terrorists. Israel has given money and weapons to the jihadists fighting against Syria’s Bashar al-Assad, which includes al-Nusra Front, an al-Qaeda affiliate. Wounded jihadists even have crossed into Israel to received hospital treatment. Once, ISIS accidentally fired into Israel and then publicly apologized. Israel is intent on removing al-Assad, which will lead to an exodus of Christians from Syria, similar to what took place in neighboring Iraq after US forces deposed Saddam Hussein.
There is a certain irony in how the United States doggedly pursues China over its alleged maltreatment of the Uighurs while at the same time rewarding and protecting Israel even though it spies relentlessly on the US and very clearly persecutes Palestinians. Dreher asks the question why the US government, which gives Israel multiple billions of dollars a year, cannot stop Israel’s de facto official punishment of its Christians. The answer is at least in part simple, that most American Christians do not care about the plight of their co-religionists in the Middle East. Millions of true-blue Christians not unlike Dreher, many weaned on the Scofield Bible and its dispensationalism, and many of whom wind up in government or other positions of power, choose to disengage from the problem, accepting that Jews are the “chosen people” of God and, for some, part of End Time prophecy. They are therefore to be given a pass by both the media and government on all their exclusivism and bad behavior even as they meddle in US politics and work to hobble freedom of speech by criminalizing anyone who criticizes Israel or supports Palestinians by urging a boycott against it. Until all that changes, if it even can happen, Christians in the so-called Holy Land will be on the chopping block and when the churches and monasteries no longer have a community to sustain them, it will be the end of Christianity in the place where it was born. And more’s the pity, the United States will have played a major role in enabling that to happen.
Philip M. Giraldi, Ph.D., is Executive Director of the Council for the National Interest, a 501(c)3 tax deductible educational foundation (Federal ID Number #52-1739023) that seeks a more interests-based U.S. foreign policy in the Middle East. Website is councilforthenationalinterest.org, address is P.O. Box 2157, Purcellville VA 20134 and its email is inform@cnionline.org.
The struggle with weight gain and obesity is a common and costly health issue, leading to an increase in risk for heart disease, Type 2 diabetes and cancer, just to name a few.
According to CDC figures for 2017-18, 19.3% of American children1 and 42.4% of adults2 are now obese, not just overweight. That’s a significant increase over the 1999/2000 rates, when just under 16% of children ages 6 to 193 and 30.5% of adults were obese.
Research has linked growing waistlines to a number of different sources, including processed foods, sodas and high-carbohydrate diets. Risks associated with belly fat in aging adults includes an elevated risk of cardiovascular disease and cancer.4
Researchers have actually predicted obesity will overtake smoking as a leading cause of cancer deaths,5 and recent statistics suggest we’re well on our way to seeing that prediction come true as obesity among our youth is triggering a steep rise in obesity-related cancers at ever-younger ages.
Millennials More Prone to Obesity-Related Cancers
As obesity rates rise, so do related health problems, including cancer. According to a report6 published in 2014 on the global cancer burden, obesity is already responsible for an estimated 500,000 cancer cases worldwide each year, and that number is likely to rise further in coming decades.
As reported in a Lancet study7 by the American Cancer Society, rates of obesity-related cancers are rising at a far steeper rate among millennials than among baby boomers. According to the authors,8 this is the first study to systematically examine obesity-related cancer trends among young Americans.
What’s more, while six of 12 obesity-related cancers (endometrial, gallbladder, kidney, multiple myeloma and pancreatic cancer) are on the rise, only two of 18 cancers unrelated to obesity are increasing. As noted in the press release:9
“The obesity epidemic over the past 40 years has led to younger generations experiencing an earlier and longer lasting exposure to excess adiposity over their lifetime than previous generations.
Excess body weight is a known carcinogen, associated with more than a dozen cancers and suspected in several more … Investigators led by Hyuna Sung, Ph.D., analyzed 20 years of incidence data (1995-2014) for 30 cancers … covering 67 percent of the population of the U.S. …
Incidence increased for 6 of the 12 obesity-related cancers … in young adults and in successively younger birth cohorts in a stepwise manner. For example, the risk of colorectal, uterine corpus [endometrial], pancreas and gallbladder cancers in millennials is about double the rate baby boomers had at the same age …
‘Although the absolute risk of these cancers is small in younger adults, these findings have important public health implications,’ said Ahmedin Jemal, D.V.M., Ph.D., scientific vice president of surveillance [and] health services research and senior/corresponding author of the paper.
‘Given the large increase in the prevalence of overweight and obesity among young people and increasing risks of obesity-related cancers in contemporary birth cohorts, the future burden of these cancers could worsen as younger cohorts age, potentially halting or reversing the progress achieved in reducing cancer mortality over the past several decades.
Cancer trends in young adults often serve as a sentinel for the future disease burden in older adults, among whom most cancer occurs.'”
Changes in Diet Are Driving the Obesity Epidemic
Studies10,11,12 have repeatedly demonstrated that when people switch from a traditional whole food diet to processed foods (which are high in refined flour, processed sugar and harmful vegetable oils), disease inevitably follows.
Below are just a few telling statistics. For more, see nutrition researcher Kris Gunnars’ 11 graphs published in Business Insider showing “what’s wrong with the modern diet.”13
Over the past 200 years, our sugar intake has risen from 2 pounds to 152 pounds per year.14 While Americans are advised to get only 10% of their calories from sugar,15 equating to about 13 teaspoons a day for a 2,000-calorie diet, the average intake is 42.5 teaspoons per day.16 It’s important to realize that it’s nearly impossible to achieve that on a processed food diet.
Not only that, you can’t exercise off the excess calories. For example, to burn off the calories in a single 12-ounce soda, you’d have to walk briskly for 35 minutes. To burn off a piece of apple pie, you’d be looking at a 75-minute walk.17
Soda and fruit juice consumption is particularly harmful, studies18,19 show, raising a child’s risk of obesity by 60% per daily serving.20 Research has also shown refined high-carb diets in general are as risky as smoking, increasing your risk for lung cancer by as much as 49%.21
Between 1970 and 2009, daily calorie intake rose by an average of 425 calories, a 20% increase, according to Stephan Guyenet, Ph.D.,22 who studies the neuroscience of obesity. This rise is largely driven by increased sugar and processed food consumption, and the routine advertising of junk food to children.23
To attract customers and compete with other restaurants, companies often add salt, sugar, fat and flavor chemicals to trigger your appetite. Unfortunately, it turns out additives and chemicals supplemented in processing kill off beneficial gut bacteria, which further exacerbates the problems created by a processed food diet.24
According to epidemiology professor Tim Spector, even eating a relatively small number of highly processed ingredients is toxic to your gut microbiome, which start to die off just days after eating a fast food heavy diet, suggesting excess calories from fast food may not be the only factor to blame for rising weight.
Processed vegetable oils, which are high in damaged omega-6 fats, are another important factor in chronic ill health. Aside from sugar, vegetable oils are a staple in processed foods, which is yet another reason why processed food diets are associated with higher rates of heart disease and other diseases.
Soybean oil, which is the most commonly consumed fat in the U.S.,25 has also been sh
“Ultraprocessed diets cause excess calorie intake and weight gain,” research26 concludes, showing that when people are allowed to eat as much as they want of either ultraprocessed foods or unprocessed food, their energy intake is far greater when eating processed fare.
In just two weeks, participants gained between 0.3 and 0.8 kilos (0.166 and 1.76 pounds) on the ultraprocessed diet, and lost 0.3 to 1.1 kilos (0.66 to 2.42 pounds) when eating unprocessed food.
As These Foods Became the Norm, so Did Chronic Illness
Unfortunately, Americans not only eat a preponderance of processed food, but 60% of it is ultraprocessed27 — products at the far end of the “significantly altered” spectrum, or what you could typically purchase at a gas station.
The developed world in general eats significant amounts of processed food, and disease statistics reveal the inherent folly of this trend. There’s really no doubt that decreasing your sugar consumption is at the top of the list if you’re overweight, insulin resistant, or struggle with any chronic disease.
It’s been estimated that as much as 40% of American health care expenditures are for diseases directly related to the overconsumption of sugar.28 In the U.S., more than $1 trillion is spent on treating sugar and junk food-related diseases each year.29
Any foods that aren’t whole foods directly from the vine, ground, bush or tree are considered processed. Depending on the amount of change the food undergoes, processing may be minimal or significant. For instance, frozen fruit is usually minimally processed, while pizza, soda, chips and microwave meals are ultraprocessed foods.
The difference in the amount of sugar between foods that are ultraprocessed and minimally processed is dramatic. Research30 has demonstrated that over 21% of calories in ultraprocessed foods comes from sugar, while unprocessed foods contain no refined or added sugar.
In a cross-sectional study31 using data from the National Health and Nutrition Examination Survey of over 9,000 participants, researchers concluded that “decreasing the consumption of ultraprocessed foods could be an effective way of reducing the excessive intake of added sugars in the USA.”
Definition of Ultraprocessed Food
As a general rule, ultraprocessed foods can be defined as food products containing one or more of the following:
Ingredients that are not traditionally used in cooking.
Unnaturally high amounts of sugar, salt, processed industrial oils and unhealthy fats.
Artificial flavors, colors, sweeteners and other additives that imitate sensorial qualities of unprocessed or minimally processed foods (examples include additives that create textures and pleasing mouth-feel).
Processing aids such as carbonating, firming, bulking, antibulking, defoaming, anticaking, glazing agents, emulsifiers, sequestrants and humectants.
Preservatives and chemicals that impart an unnaturally long shelf-life.
Genetically engineered ingredients, which in addition to carrying potential health risks also tend to be heavily contaminated with toxic herbicides such as glyphosate, 2,4-D and dicamba.
As described in the NOVA classification of food processing,32 “A multitude of sequences of processes is used to combine the usually many ingredients and to create the final product (hence ‘ultraprocessed’).” Examples include hydrogenation, hydrolysation, extrusion, molding and preprocessing for frying.
Ultraprocessed foods also tend to be far more addictive than other foods, thanks to high amounts of sugar (a substance shown to be more addictive than cocaine33), salt and fat. The processed food industry has also developed “craveabilty” into an art form. Nothing is left to chance, and by making their foods addictive, manufacturers ensure repeat sales.
Processed Food Diet Linked to Early Death
In related news, recent research34 involving more than 44,000 people followed for seven years warns that ultraprocessed foods raise your risk of early death. The French team looked at how much of each person’s diet was made up of ultraprocessed foods, and found that for each 10% increase in the amount of ultraprocessed food consumed, the risk of death rose by 14%.
This link remained even after taking confounding factors such as smoking, obesity and low educational background into account. As you’d expect, the primary factors driving the increased death rate was chronic diseases such as heart disease and cancer.
Nita Forouhi, a professor at the MRC Epidemiology Unit at the University of Cambridge, who was not part of the study, told The Guardian :35
“The case against highly processed foods is mounting up, with this study adding importantly to a growing body of evidence on the health harms of ultraprocessed foods … [W]e would ignore these findings at public health’s peril.
A vital takeaway message is that consumption of highly processed foods reflects social inequalities — they are consumed disproportionately more by individuals with lower incomes or education levels, or those living alone.
Such foods are attractive because they tend to be cheaper, are highly palatable due to high sugar, salt and saturated fat content, are widely available, highly marketed, ready to eat, and their use-by dates are lengthy, so they last longer. More needs to be done to address these inequalities.”
Ultraprocessed Foods Linked to Cancer
Another French study36,37 published last year also found that those who eat more ultraprocessed food have higher rates of obesity, heart problems, diabetes and cancer. Nearly 105,000 study participants, a majority of whom were middle-aged women, were followed for an average of five years.
On average, 18% of their diet was ultraprocessed, and the results showed that each 10% increase in ultraprocessed food raised the cancer rate by 12%, which worked out to nine additional cancer cases per 10,000 people per year.
The risk of breast cancer specifically went up by 11% for every 10% increase in ultraprocessed food. Sugary drinks, fatty foods and sauces were most strongly associated with cancer in general, while sugary foods had the strongest correlation to breast cancer.
According to the authors, “These results suggest that the rapidly increasing consumption of ultraprocessed foods may drive an increasing burden of cancer in the next decades.” Study co-author Mathilde Touvier told CNN:38
“It was quite surprising, the strength of the results. They were really strongly associated, and we did many sensitive analysis and adjusted the findings for many cofactors, and still, the results here were quite concerning.”
Diet Is a Key Factor Determining Your Health and Longevity
Research39 published in 2017 linked poor diet to an increased risk of cardiometabolic mortality (death resulting from Type 2 diabetes, heart disease and stroke).
According to the authors, suboptimal intake of key foods such as fruits, vegetables, nuts and seeds, and animal-based omega-3, along with excessive consumption of processed foods such as meats and sugar-sweetened beverages accounted for more than 45% of all cardiometabolic deaths in 2012. In other words, the more processed foods you eat, and the less whole foods you consume, the greater your risk of chronic disease and death.
Other research published that same year found that eating fried potatoes (such as french fries, hash browns and potato chips) two or more times per week may double your risk of death from all causes.40 Eating potatoes that were not fried was not linked to an increase in mortality risk, suggesting frying — and most likely the choice of oil — is the main problem.
In a 2013 presentation41 at the European Ministerial Conference on Nutrition and Noncommunicable Diseases by Dr. Carlos Monteiro,42 professor of nutrition and public health at the University of Sao Paulo, Brazil, Monteiro stresses the importance of creating “policies aiming the reformulation of processed foods,” and limiting children’s exposure to junk food marketing, in order to tackle the rise in diet-related noncommunicable diseases.
In my view, eating a diet consisting of 90% real food and only 10% or less processed foods is an achievable goal for most that could make a significant difference in your weight and overall health. You simply need to make the commitment and place a high priority on it. To get started, consider the following guidelines:
Focus on raw, fresh foods, and avoid as many processed foods as possible (if it comes in a can, bottle or package, and has a list of ingredients, it’s processed).
Severely restrict carbohydrates from refined sugars, fructose and processed grains.
Increase healthy fat consumption. (Eating dietary fat isn’t what’s making you pack on pounds. It’s the sugar/fructose and grains that add the padding.)
You may eat an unlimited amount of nonstarchy vegetables. Because they are so low in calories, the majority of the food on your plate should be vegetables.
Limit protein to less than 0.5 gram per pound of lean body weight.
Replace sodas and other sweetened beverages with pure, filtered water.
Shop around the perimeter of the grocery store where most of the whole foods reside, such as meat, fruits, vegetables, eggs and cheese. Not everything around the perimeter is healthy, but you’ll avoid many of the ultraprocessed foods this way.
Vary the whole foods you purchase and the way you eat them. For instance, carrots and peppers are tasty dipped in hummus. You get the crunch of the vegetable and smooth texture of the hummus to satisfy your taste, your brain and your physical health.
Stress creates a physical craving for fats and sugar that may drive your addictive, stress-eating behavior. If you can recognize when you’re getting stressed and find another means of relieving the emotion, your eating habits will likely improve.
The Emotional Freedom Techniques (EFT) can help reduce your perceived stress, change your eating habits around stress and help you create new, healthier eating habits that support your long-term health. To discover more about EFT, watch the video at this referenced link on substack.43
*This article has been updated with new information.
One of the more pernicious and morally shocking developments surrounding the covid vaccines is hospitals forcing transplant recipients (and sometimes even their families) to be vaccinated with one of the covid vaccines.
I have heard a number of people defend this vile practice, who were genuinely convinced that there was nothing wrong with it. None of these individuals were “evil”, or anything close. Yet, they genuinely did not see a concern or dilemma that would disqualify the whole policy, or even one that would at least counsel a more thoughtful review before taking such a momentous and consequential step.
It is therefore worthwhile to present a clear explanation why, even assuming that transplant recipient vaccination is objectively beneficial as a purely scientific matter, mandating vaccination as a prerequisite for receiving a transplant is destructive to society and evil.
The following are a few of the more salient reasons why mandating recipient vaccination as a condition to remain eligible to receive a transplant, even assuming that transplant recipient vaccination are objectively beneficial as a purely scientific matter, is unjustifiable, destructive, and evil:
Breaks the Social Compact of Society:
Discriminates on the basis of a controversial political/social issue
Politicizes and undermines the trustworthiness of the medical community
Weaponizes the medical community / medical institutions in the “culture wars”
Drives the Balkanization of society
Is Intrinsically Immoral:
Such a mandate inflicts tremendous psychological torment upon people who are already suffering the stress and physical torment of a life-threatening disease
Erodes the ethics and character of medical professionals, so they regard some people as “inferior” and therefore undeserving of or not worth being treated
This is a policy that cannot be plausibly portrayed as being “in the best interests of patients”
Catch-all: Will cause considerable stress to the entire society
The Broader Context that Informs how People View Such a Mandate – The Medical Community no longer possesses the moral authority or credibility to make this sort of policy decision:
The already heavily damaged reputation and image of the medical community due to covid policies so far
A sizable minority today believes (if not outright majority) that hospitals and doctors are possibly complicit in the deaths of millions around the world and the unimaginable suffering of hundreds of millions more
Breaks the Social Compact of Society:
Discriminates on the basis of a controversial political/social issue
The reality of the current situation is that the covid vaccines are one of the preeminent issues at the forefront of the body politic in the country. This is therefore automatically a consideration when making policies on behalf of society, which any decisions regarding the prioritization scheme of transplant recipients are.
Decisions broadly affecting the whole of society that discriminate or persecute a faction/s of society break the social compact and erode or destroy the moral legitimacy of the major institutions through which political and social power and ideology are disseminated and enforced.
Specifically for this point, discriminating against a political or social minority – and surely where it is literally determining by proxy who lives and who dies – is by definition apartheid in both spirit and practice.
It goes without saying that apartheid policies are both harmful to a healthy and functioning society and evil.
Politicizes and undermines the trustworthiness of the medical community
Enacting a policy that is inextricably intertwined with a highly visible social or political controversy unavoidably conveys – regardless of whether it’s true – that the medical community is:
(A) a political actor that has
(B) vested political interests and objectives – such that it will
(C) pursue using the resources at its disposal
(D) even if/when they are in conflict with the neutral practice of medicine.
The damage from such overt political overtones and imaging (to say the least) to the practice of medicine, and the implications for the physical and mental health of the broader society, is something that does not require elaboration.
Importantly, this is true even for many of the people who agree with vaccination, because they also perceive that the medical community is “allying” with them to promote a political cause. The worse the reputation of the medical community is tarnished with political entanglements, the more difficult it becomes to rehabilitate subsequently.
Weaponizes the medical community & medical institutions in the “culture wars”
The participation of the medical community to coerce political compliance at gunpoint transforms the medical community (more than it is already) from a shared societal institution to a partisan one that one side views as a hostile force or enemy and the other views as a means to achieve political or social objectives.
The obvious (i.e. uncontroversial as factual observations regardless of whether one agrees or disagrees with the underlying position of either side here) societal harms that flow from this are manifold. Transforming the shared social institutions of science/medicine into a partisan weapon will cause the following negative consequences (among others; ‘shared’ is an increasingly tenuous proposition these days):
undermines trust in the practice of science
undermines the integrity of medical scientists by creating and incentivizing political objectives that take precedence over scientific integrity
causes a sizeable portion of society to regard doctors and medical professionals as enemies, which is harmful both to patients who will then not receive the same standards of medical care and to doctors who will suffer constant harassment and demoralizing stresses
encourages the propagation of propaganda as everyone is now incentivized to either deify or demonize medical practitioners and institutions regardless of the factual merits of any specific issue or incident
A society must have shared institutions that are not “playable characters” in the everyday social or political maelstroms that are the domain of politics in order to function and survive as a single political entity.
Drives the Balkanization of society
The most prominent consequence of the politicization and weaponization of the medical community and institutions is that it is a Balkanization of society. Regardless of the factual or scientific merits, even the perception by one faction that another faction is trying (and succeeding) in hijacking and corrupting the medical establishment is the fraying of the society as an organized political and social unit. To actually go ahead and do so is more damaging by orders of magnitude. Medical care is possibly the most foundational institution in a society – consider that the most consequential apartheid policy (besides for outright slavery) is the proscription of medical care by political or social affiliation. Thus proscribing medical care for a highly visible and prominent social faction within society – even if it wouldn’t be an outright death sentence for the patients restricted from medical treatment as is the case here – is tantamount to a declaration of [civil] war against anyone politically affiliated with the group targeted by the mandates.
It should also go without saying that you can’t have a functional society if whether your life and your human rights can be legally and socially vindicated depends upon on your political affiliation or ideological coadunation. There is no rational universe where this is an acceptable tradeoff for the conjectured benefits of restricting transplants to vaccinated patients.
Transplant Vaccine Mandates Are Intrinsically Immoral:
Such a mandate inflicts tremendous psychological torment upon people who are already suffering the stress and physical torment of a life-threatening disease
Any policy decision must consider the entire picture, not just the virtues of the preferred course of action.
Transplant vaccine mandates are dealing with a population that is exclusively comprised of people who are already under extreme suffering that is hard to contemplate or understand for someone bereft of this sort of experience. Adding distress to people already so tormented would therefore be warranted only if there was an exceptionally pressing concern. Even if the covid vaccines are somewhat beneficial as a purely scientific matter to patients awaiting an organ transplant, the marginal benefit of vaccination is hardly something that is so massive that imposing a vaccine mandate – in the context of everything else articulated in this article – can even be plausibly entertained let alone imposed. (The marginal benefit is the absolute risk reduction in all-cause morbidity/mortality gained from vaccination, not the “relative” risk reduction which is not relevant to assessing the real-world value of vaccination.)
Erodes the ethics and character of medical professionals, and influences and/or habituates them to regard some people as “inferior” and therefore undeserving of or not worth being treated
A policy of ‘either you acquiesce to vaccination or you die’ conveys to medical practitioners a clear message that people who reject the covid vaccines are not worthy of medical treatment. This is true regardless of the scientific merits of a (theoretically) objective cost/benefit analysis. Contingency of life-or-death treatment upon a political behavior or choice internalizes to medical practitioners and laypeople alike that it is appropriate to proscribe treatment to people because of political affiliation, so much so that we will even consign them to death. Medical apartheid on the basis of political or social faction characteristics is quite literally in the mold of the ideology and policies implemented in Germany in the 1930’s. Such a comparison is sufficient to retire any further consideration by itself of transplant vaccine mandates.
Such a dynamic is also corrosive to compassion and empathy — two attributes that are already in short supply in healthcare settings these days. The deprivation of treatment, especially in circumstances that are exceptionally heartwrenching, forces practitioners at minimum to suppress their sense of compassion. For many, the internal dissonance between their sense of compassion and the cruelty being inflicted on defenseless patients (& the relegation of a political class to “2nd class citizens”) that some would be complicit in will lead them to zealously embrace rationalizing that the unvaccinated are less than fully human. This is precisely how otherwise civilized people can be indoctrinated into an ideology that if unchecked ultimately enables them to commit or be complicit in the commission of atrocities.
(Requiring adherence to personal behavior standards – such as not consuming alcohol or drugs – whose medical rationale is obvious and apparent to everyone and which have already been standard requirements for decades is an entirely separate matter that has nothing to do with this discussion, and is something that requires its own lengthy dissertation to properly explore and flesh out.)
Like every other enumerated argument here, this point is true regardless of the factual merits of vaccination for transplant patients.
This is a policy that cannot be plausibly portrayed as being “in the best interests of patients”
Medical ethics is organized around the proposition that all decisions or policies must be in the best interests of patients. It is hard to imagine more blatant disregard of patients’ welfare than compromising the integrity and viability of the entire edifice of healthcare provision in the country as millions of people are less able and/or willing to seek and receive medical care as a result of all of the other points articulated above and below (and it is also not in the patients’ best interests for medical treatment to be withheld without which the patient will perish).
Contumeliously discarding the millennia-old foundational ethical principium of medicine ominously portends the possibility of medicine and healthcare unanchored to an ethical North Star.
Catch-all: This will cause considerable stress to the entire society
Polls consistently reveal that people of all social and political affiliations are suffering considerable stress. Policies that antagonize or that are erosive to the body politic spur or inflame the already burdened and fraying psyche of the populace. Even those advantaged by politically prejudicial persecution cannot escape the stresses that beset even those that have the upper hand politically, such as the worry that someday you will become a victim to the same social or political forces, or the stresses of living in a society where the social fabric is frazzled and fragmented. Especially in light of the current mental health apocalypse presently afflicting the country, it surely behooves the medical community to avoid further exacerbating the already overwrought stressors in people’s lives.
The Broader Context that Informs how People View Such a Mandate – The Medical Community no longer possesses the moral authority or credibility to make this sort of policy decision:
The reputation and image of the medical community has already been brutally savaged by the performance of the medical establishment throughout the covid crisis, especially the govt health agencies which are the backbone of the medical community’s authority and credibility. Moreover, at least a sizeable minority of the country believes that hospitals and doctors are complicit in the deaths of millions around the world and the unimaginable suffering of hundreds of millions more through draconian isolation of psychologically/emotionally vulnerable patients, denial of covid treatment, society-wide lockdowns, and vaccine carnage.
As a result, the medical community has lost the moral legitimacy and expert authority that until now was taken for granted. This is a monumental shift that is hard to overstate. The medical community previously was accorded the considerable latitude and deference by society they needed to make life-and-death policy decisions that society wouldn’t reflexively view as illegitimate or political. Without unambiguous and widely conceded moral authority to make controversial life-and-death policy decisions, the medical community ceases to be trusted and neutral stewards whose decisions can determine who lives and dies. Instead, they are no better than any other partisan and unobjective actor with their own biases and agenda. Empowering what is rationally perceived by one half of society as a conflicted and dishonest political actor to determine who lives and dies on the basis of a political characteristic is inherently evil and lacks even a semblance of moral credibility.
This last point is worth restating: This is akin to having a republican decide that democrats are not eligible for transplants unless they switch party affiliation or vice versa. The disfavored group would rightly and accurately perceive that a government that proscribes them from receiving lifesaving treatment lacks legitimacy.
Caveats:
It is important to note that there are many heroic doctors and nurses who do not agree with these policies. In a similar vein, the impact of such a policy (and the other covid policies that are similarly evil or just plainly irrational) is not uniform on all healthcare practitioners – there is a wide range of resiliency and resistance to the mental and psychological influence of this sort of policy.
It is also important to note that there is already considerable damage along the lines of everything stipulated above, so for the most part transplant mandates are aggravating already belabored destructive social pathologies as opposed to initiating or creating new ones.
However, this does not detract from the intensity or imperative of the arguments raised. The fact of the already-widespread devastation underscores how critical it is to reverse these developments – meaning that exacerbating them is that much more unconscionable.
Conclusion
Medical institutions are integral to the translation of medical and scientific knowledge into practice in a manner that will be accepted by the various major factions of society (there are always going to be fringe lunatic groups or cults that repudiate any sort of governing political bodies no matter what). A society without a shared epistemology cannot survive, as there can be no agreement on how to determine factual truth. The medical establishment institutions are fiduciaries to the entire population, granted awesome powers over society, and therefore commensurately responsible for the broader social impact of their actions (something that the medical literature en masse freely embraces, one need only look at the hundreds of papers condemning the medical community for their role in promoting “health inequities” and systemic racism).
It is not just prudent but obligatory to consider the political climate when weighing a policy choice that implicates and will resonate through the exigent political and social realities on the ground such as they are. One would think it would be common sense to go to the farthest practical extreme to avoid even the hint of appearing partisan or political, never mind actually further inflaming the divisive and increasingly weaponized political tensions. This is by no means even remotely controversial. The typical standards that society holds critical non-partisan institutions to is that they must avoid “even the appearance of” conflicts of interest, partisanship, etc. – recusals for these reasons are routine in the legal world for instance.
One would also be forgiven for thinking that the medical community would be embarrassed to be caught openly embracing the same fundamental political philosophy that animated the Nazi’s systematic denudement of the medical community back then of the ethical code synonymous with the practice of medicine.
Enacting a policy that in practice is political discrimination is irreconcilable with both basic medical ethics and the responsibility of the medical community to scrupulously avoid even the appearance of partisanship or other non-medical entanglements. There is no justification or defense for such an egregious lapse of judgement.
The ever-sharp Zacki on Twitter points to this intriguing 2018 study out of New York. The authors administered PCR tests to 2,685 people at a tourist attraction in New York City, between the months of January and July. Over 6% tested positive for one of seven common human respiratory viruses. In the winter, human coronaviruses were the most common; in the summer, rhinoviruses took the lead. By design, the study targeted healthy populations, and so we must imagine that it substantially understates the true rate of virus infection.
The authors don’t find a significant difference in the overall prevalence of positivity between winter and summer. In their small sample, it’s only the mix of viruses that changes. This is another piece of evidence in favour of my crazy theory, that a great part – perhaps a majority – of spring and summer allergies are in fact persistent low-grade rhinovirus infections.
Other studies, particularly on rhinovirus, find even larger incidences of infection. There is this paper, which looks at rhinovirus in infants and finds that 20% of their sample are asymptomatic positives; or this case-control study of all ages, which finds rhinovirus in 17% of their asymptomatic controls.
For perspective: At the height of the alpha wave in the United Kingdom, only about 0.3% of the population was testing positive for SARS-2 every day. School antigen testing in Germany, which is done multiple times a week and finds nearly every detectable infection in school-age children, found Delta 7-day incidences of around 1%, and Omicron 7-day incidences peaking in February at near 4% in specific age cohorts (see the the graph on p. 5). The allegedly hypercontagious SARS-2 looks like it was doing substantially worse, in other words, than garden-variety human coronaviruses in the same month in the New York study.
Respiratory viruses are extremely pervasive; they’re everywhere and this is totally normal. What isn’t pervasive, is virus testing. We’ve only ever tested widely for a single virus. So much of Corona mythology depends upon presenting data in isolation from what we know about the behaviour of all the other pathogens we’ve lived with for centuries. Our governments have spent two years hyperventilating about incidences of infection that turn out to be minuscule, or at worst normal, when compared to the other pathogens that infect us. This should also make you very, very sceptical of uncontrolled studies cataloguing alleged Long-Covid symptoms. If we tested this widely for rhinovirus, imagine all the totally unrelated symptoms we’d find in our vast pool of positive results.
THE business magazine Forbes has published a story with the arresting headline: ‘Unvaccinated People Increase Risk Of Covid Infection Among Vaccinated, Study Finds.’
The work to which it refers is not in the normal sense a study but is actually a modelling exercise published by the journal of the Canadian Medical Association. Did the Forbes staff writer read the paper very well? I am quite sure not. At the end of paragraph one of the Method section of the original paper, it describes its model, saying: ‘A vaccine that is 80 per cent efficacious would result in 80 per cent of vaccinated people becoming immune, with the remaining 20 per cent being susceptible to infection. We did not model waning immunity.’
Now I am sure you know that the mRNA vaccines do not stop infection and also wane in effectiveness. In other words mRNA vaccination does not confer immunity and its effectiveness does not remain constant as the paper assumes. So what use is this paper and to what do its conclusions apply? Apparently not to the mRNA Covid vaccines.
Lo and behold, one of the paper’s authors, David Fisman, declares competing interests: ‘He has served on advisory boards related to SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca and Sanofi-Pasteur Vaccines.’
Another author, Ashleigh Tuite, was ‘employed by the Public Health Agency of Canada when the research was conducted’ (aka the domain of Justin Trudeau).
So why publish this story which on the face of it has little relevance to the real-world data of the current pandemic? Forbes magazine is 51 per cent owned by a Hong Kong-based company, Integrated Whale Investments, about which little is known. The Washington Post has suggested that Forbes’s editorial policy has been influenced as a result, but by whom no one really knows.
At this point in the pandemic, it has become clear that boosted individuals are becoming more vulnerable to Omicron than the unvaccinated. So I can only suggest that it might be advantageous for some scientists and politicians to blame the unvaccinated for everything in order to cover up their own mistaken ideas. Or perhaps there are commercial interests anxious to sell more arguably useless vaccines for billions of dollars. You decide.
If the government and their compliant media friends are our one source of truth, as has happened in New Zealand (by decree), then you have no option except to blame the unvaccinated whatever happens.
The actual situation is that the unvaccinated are currently less likely to be hospitalised than the boosted. Thank you to Grant Dixon for compiling and graphing NZ Ministry of Health data, below.
This morning my mask-exempt friend entered a haberdashery shop, whereupon two other potential customers turned and fled. Yesterday she was turned away from a fabric store. I am sure many of you have had similar experiences. The fact of the matter is that almost the whole of the New Zealand population has become subject to fear-based government-sponsored groupthink.
Are we all being conditioned to vote for Jacinda Ardern in next year’s election based on the carefully constructed myth that she is keeping us all safe? We should be keeping our feet on the ground. We should recognise that public relations experts and propaganda promoters are at work full-time, but they are working out of touch with reality.
Meanwhile our whole economy is becoming ever more dysfunctional. As people are too afraid to associate with one another in public, the whole basis of commercial activity is being undermined.
The two large supermarket chains are laughing all the way to the bank. As small businesses are forced to close and their monopoly grows, supermarket prices and profits are entering the stratosphere. Smart individuals are now ordering their vegetables and groceries direct from Australia (as far away from us as Moscow is from London) because they are so much cheaper.
The government is clueless to control this rampant price inflation, along with most things including the pandemic. The public is hoodwinked, queueing fully masked and fully vaccinated to pay through the nose for everyday items without a squeak of dissent.
The ten-year-old son of a friend asked his mother the other day: ‘Which do you think our society is more like – Brave New World or 1984?’ I doubt if either Aldous Huxley or George Orwell could ever have imagined anything so incomprehensibly doublethinking as 2022 New Zealand.
This is the state we have reached through our government’s careful rationing of information and saturation conditioning.
Time we reopened the floodgates of free speech and social media – hold your horses, we might endanger our one source of truth.
Respiratory viruses are both unpredictable and commonplace. The name of the most well-known one, Influenza, originated in 15th century Italy, and comes from the old Italian expression influenza dei pianeti or influence of the planets. They could not explain its sudden and unaccountable behavior and ascribed its capricious nature to the influence of planets.
However, influenza is just one of the many agents involved in active respiratory infections; there are scores of known ones which give a spectrum of clinical presentations, from a mild cold to severe pneumonia. We have no idea how many agents there are. Since 1970, 1,500 pathogens have been discovered – 70% have come from animals. Some authors report that up to 40% of respiratory infections have no recognised causes.
Over 30 years, we have studied physical interventions, vaccines, and antivirals for registered compounds and ones which never made it to market. In 2014 we encouraged Roche and GSK to give up the business part of their regulatory submissions for their antivirals, opening up a whole new source of clinical study report evidence that is infinitely more reliable and complete than biomedical journal publications.
So when SARS-CoV-2 struck, we watched unfolding events with curiosity. We try to understand the effects of the agent and those of our leaders’ responses. To achieve this, you need reasonably good data.
We are used to wastage, error, and poor quality research underpinning patient care. The influenza field is further affected by flawed science, pandemic conspiracies and political contamination that leads to the inevitable box thinking with the advent of a newly identified agent.
In the UK, like in most other countries, the daily situation briefings delivered by top scientific advisers who we knew had little experience of respiratory virus epidemiology set the pace of the pandemic and the subsequent hysteria.
The briefings were devised to illustrate the seriousness of the COVID-19 situation by presenting running totals of new cases, hospital admissions and deaths. We call this the three-legged stool of the COVID narrative. The stool provided the rationale for an unprecedented level of restrictions on civil liberties and governmental diktats designed to control the unruly populace in the hope of managing – or even eradicating – the agent.
After exploring aggregate data, we looked in-depth into the science of the three legs: Speaking daily, we discussed and analyzed the certainty behind the summary figures and trends presented every night. Finally, we asked ourselves: what props the stool up?
We tried making sense of the various government websites, the relevant papers in biomedical journals, and the tests applied to identify “cases.” We soon understood that the PCR was inappropriately used as a mass screening tool. Its limits were not understood by those reporting its results or those presenting aggregate data.
Even with correct specimen management and a competent laboratory process, a simple PCR test cannot distinguish active cases from those recovering from SARS-CoV-2 infection who are no longer infectious and a danger to no one.
We used our systematic review skills to analyse the studies comparing the culture of SARS-CoV-2, the best indicator of current active infection and infectiousness, with the results of PCR.
Complete viable viruses are necessary for transmission, not the fragments identified by PCR. PCR picks up minute particles which take weeks to be cleared by our immune systems, not complete viruses, so governments were locking up the contagious with the non-contagious.
Misuse of PCR underpinned the whole narrative. Its very high sensitivity and robotic acceptance as a gold standard created the illusion of many more cases (i.e. active infections) than were really present and prompted long quarantines, disrupting society and lives.
Therefore, the first leg of the stool is unstable, made worse by the absolute refusal to link PCR results to the reporting of viral load estimates, which could (coupled with accurate history and thorough epidemiology) give a likelihood of infectivity.
The second leg, attribution of death, was affected by bureaucratic bungling and PCR misuse. We discovered that UK public health bodies had 14 different ways of attributing the role of SARS-CoV-2 to a death. Some totals included deceased who had tested negative. Post-mortem examinations were uncommon, as was independent verification of causes of death. So aggregate attribution of mortality figures was questionable – the second leg started teetering too.
We are currently analyzing the last leg of the stool: hospital capacity. Hospital episodes take time to reconstruct, but they are also underscored by PCR misuse, poor definitions, and confusing messaging. A coherent dataset is unlikely to exist, so we have to piece the puzzle together.
We reported our findings in a series of web reports for a charity and the mainstream media, the only avenues that evade some censorship.
Where did our data come from? From the only section of society which had an idea of what was going on, or at least were asking questions instead of accepting the “rule of six” or supermarket trolley police checks like obedient cattle, the public.
Freedom of Information (FOI) request sites in the UK are sources of amazingly bright questions and bureaucratic and sometimes misleading answers. Here are some examples. Public Health England does not know whether hospitals have a financial incentive to classify an admission episode as COVID-related, so how can they interpret the data?
Some deaths are classified as COVID-related, even though negative. The Department of Health has no idea how many and which of the PCR kits are in use, all with a different performance which has not been standardized. So they were adding apples with trees and hay bales and reporting the consequent nonsense daily.
The power of FOI host websites like WhatDoTheyKnow is immense and underutilized. The questions and responses are public for everyone to see, and most of the public’s questions are pin-sharp.
The FOI ACT provides access to information held by public authorities who are obliged to publish certain information about their activities; and members of the public are entitled to request information from public authorities.
However, the FOI respondents show poor science, bureaucracy, delegation to juniors to respond to “nuisance” questions and a lack of coherent vision – at times, the response is dismissive. Still, there are occasional nuggets of vital information.
Why not set up a similar FOI portal in every country? We think it is the only way to make these people accountable to voters. You can follow our attempts at getting to the bottom of hospital episodes in England, Wales and Northern Ireland by following our correspondence: 1234.
The stool’s three legs remain vital to understanding the rationale for restrictions imposed throughout the pandemic.
Conflict of interest statements
TJ’s competing interests are accessible here. CJH holds grant funding from the NIHR, the NIHR School of Primary Care Research, the NIHR BRC Oxford and the World Health Organization for a series of Living rapid review on the modes of transmission of SARs-CoV-2 reference WHO registration No 2020/1077093. He has received financial remuneration from an asbestos case and given legal advice on mesh and hormone pregnancy tests cases. He has received expenses and fees for his media work including occasional payments from BBC Radio 4 Inside Health and The Spectator. He receives expenses for teaching EBM and is also paid for his GP work in NHS out of hours (contract Oxford Health NHS Foundation Trust). He has also received income from the publication of a series of toolkit books and for appraising treatment recommendations in non-NHS settings. He is Director of CEBM and is an NIHR Senior Investigator.
Authors
Carl Heneghan is Director of the Centre for Evidence-Based Medicine and a practising GP. A clinical epidemiologist, he studies patients receiving care from clinicians, especially those with common problems, with the aim of improving the evidence base used in clinical practice.
Tom Jefferson, Department for Continuing Education, University of Oxford, UK
It began with the strange decision of state media to elevate Christian Drosten at Berlin Charité to national prominence, by granting him the Coronavirus Update podcast on 26 February 2020. The WHO had just endorsed lockdowns two days before, and various countries were acquiring new Corona tsars – random virus wizards who would become the face of containment policy to panicking domestic audiences. Every day, Drosten’s banal podcast interviews were reported breathlessly across the German media, as if they meant anything.
It’s important to remember that Drosten is a virologist. He’s not a statistician, and for what it’s worth, he’s not a public health expert either. He studies how very small proteins work and how they interact with human cells. Nevertheless, Drosten had (or claimed to have) a wide range of opinions on matters outside of his field, including the question of whether closing schools would slow down SARS-2.
At first, Drosten said that he didn’t think this would accomplish very much. Like everyone else of his ilk, he had an early history of saying basically correct and sensible things before he went crazy. On 11 March 2020, he went home and read this paper on Nonpharmaceutical Interventions Implemented by US Cities During the 1918–1919 Influenza Pandemic. It wasn’t his field; his assessment of its analysis is worth no more than mine or yours. But after reading it, he decided that actually closing schools would be a great idea, especially when used in combination with other interventions, such as banning mass gatherings. This was wind in the sails of hystericists like Markus Söder, minister president of Bavaria. And so we closed our schools, and our kids endured months of social isolation and mental anguish, because Drosten read a thing and had a brilliant idea.
But, that’s only the official story. It may be vastly worse than that. I really doubt, for example, that Drosten’s ridiculous podcast was a spontaneous programming idea by Norddeutscher Rundfunk. I suspect, instead, that there’s a reason lockdowns and Corona tsars went together in those early days. Primary was the political or bureaucratic decision to do all this crazy stuff, in the absence of any evidence aside from some dodgy numbers out of Wuhan. Thus the genius smart guys who run our institutions had to find celebrity virus astrologers, who could become the public face of novel policies and provide a simulacrum of science for the politicians to pretend they were following. It’s even odds, whether Drosten really did change his mind because of a paper he read one night; or whether it was rather the political or bureaucratic faction behind Drosten that changed their minds and gave him a paper or two to read.
Science isn’t some objective reasonable force outside of politics. Scientists spend most of their careers chasing government grant funding, and fighting for appointments and promotions in government-funded university systems. Science follows politics, and nobody knows this as much as the disingenuous politicians who claim that their policies are subordinate to scientific findings.
The Centers for Disease Control (CDC) was founded in 1946 as a backwater quasi-governmental agency with a negligible budget and a handful of employees tasked with a simple mission: “prevent malaria from spreading across the nation.”
Seventy-five years later it has metastasized into a multi-billion dollar bureaucratic behemoth that oversees and controls virtually all aspects of public health programs, policies and practices across the United States.
The CDC is the primary US national public health agency tasked with“protecting America from health, safety and security threats” and advertises that it will “increase the health security of our nation.”
Guidelines and recommendations by the CDC set the standards for mainstream medicine in America and are considered the de facto rules by which public health departments and most institutions throughout the country must operate.
“be a diligent steward of the funds entrusted to our agency, base all public health decisions on the highest quality scientific data that is derived openly and objectively and place the benefits to society above the benefits to our institution.”
This high-minded mission statement gives the impression that the CDC will, above all else, work diligently and honestly to protect the health of all Americans. A careful review of the CDC’s history and current mode of operation indicate a stark contrast between these noble words and how the CDC actually functions.
OZ HAS SPOKEN
“The CDC has enormous credibility among physicians, in no small part because the agency is generally thought to be free of industry bias. Financial dealings with bio-pharmaceutical companies threaten that reputation.”
Marcia Angell, former editor in chief of the New England Journal of Medicine
In the mainstream media vortex, questioning the state religion of CDC decrees and guidelines lands one firmly in the camp of the “conspiracy-minded,” accused of practicing sorcery or some manner of medieval medical quackery.
In the minds of many Americans the CDC represents the final word on “all matters health-related.” To question this omnipotent bureaucratic agency is to challenge sacred health commandments and cast doubt on the medical establishment itself.
The widely accepted belief about the CDC holds that it is a governmental agency which functions outside of health industry relationships and consequently operates free from the monied interests of the health management sector. Nothing could be further from the truth.
Despite this reputation, further scrutiny reveals that the CDC falls far short of its stated purpose. As the scope and budget of this agency has ballooned over the years, including a war chest of corporate contributions, we have to ask ourselves, “Does the CDC fulfill its mission statement of protecting public health or is it now just another bloated quasi-governmental agency that works on behalf of its donors?”
Contrary to its disclaimer that “the CDC does not accept commercial support”, the British Medical Journal (BMJ)reported, in 2015, that “the CDC does receive millions of dollars in industry gifts and funding, both directly and indirectly.”
A petition filed in 2019 by several watchdog groups contends that the CDC’s assertion that it is free from influence peddling and has “no financial interests or other relationships with the manufacturers of commercial products” are “indisputably false.”
The petition goes a step further asserting that the CDC, “knows the claims are false, because it has procedures to address from whom and under what circumstances it accepts millions of dollars from contributors, including manufacturers of commercial products.”
This allegation is supported by multiple examples from the CDC’s own Active Program’s Report.
For instance, Pfizer Inc. contributed $3.435 million since 2016 to the CDC Foundation for a program on the prevention of Cryptococcal disease.
Programs like these became commonplace as early as 1983 largely due to Congressional authorization which allowed the CDC to accept “external” gifts:
made unconditionally… for the benefit of the [Public Health] Service or for the carrying out of any of its functions.”
Despite the caveat that these donations must be geared towards public health, the reality is these contributions come with strings attached. As noted earlier in the BMJ report, Pharma funds given to the CDC for specific projects return to Pharma pockets via marketing and sales.
The spigot of funding initiated through Congressional permission would open full blast a decade later, with the creation of the CDC Foundation.
THE CDC FOUNDATION
The CDC Foundation was created by Congress in 1992 and incorporated two years later to “mobilize philanthropic and private-sector resources.”
Once established, the CDC Foundation became the primary pass-through mechanism utilized by a cornucopia of corporate interests to exert influence over various aspects of the CDC. Large pharmaceutical companies contributed millions of dollars each year to the “separate, philanthropic CDC Foundation.“
The CDC Foundation would then “donate philanthropically” Big Pharma contributions to the CDC itself. This sleight of hand ensured the CDC could maintain they never accepted money directly from Big Pharma.
Some have argued that once this avalanche of monied interests was unleashed, the agency itself was transformed into the primary marketing arm of the Pharmaceutical Industry creating a hornet’s nest of ethics violations, outright corruption and opened up a slew of questions as to who the CDC actually works for.
Was the CDC Foundation truly established as a philanthropic enterprise or as a way to conceal conflicts of interest?
Did this massive influx of corporate cash cede control of the CDC to the medical and pharmaceutical industry and their financiers, allowing them to control the direction of “public” health policy?
Would business oriented, for-profit medical programs, using the CDC’s imprimatur, come to dominate public health policy?
Those questions seemed to have their answer in the CDC Foundation’s donor list which reads like a ‘Who’s Who’ of pandemic profiteers and philanthropic mercenaries.
Major sources of cash for the Foundation include the GAVI Alliance, Bloomberg Philanthropies, Fidelity Investments, Morgan Stanley Global Impact Funding Trust, Microsoft Corporation, Imperial College London, Johns Hopkins University, Google, Facebook, Merck Sharp & Dohme Corp., Johnson & Johnson Foundation and the omnipresent ‘do-gooders’ at the Bill and Melinda Gates Foundation.
INTERNAL PROBLEMS
In 2016 a group of concerned senior scientists from within the CDC wrote a letter to then CDC Chief of Staff Carmen Villar alleging that the CDC “is being influenced and shaped by outside parties… [and this] is becoming the norm and not the rare exception.”
The transgressions cited in that letter include: “questionable and unethical practices,” “cover up of inaccurate screening data” and “definitions changed and data cooked to make the results look better than they were.”
The scientists went on to note that the CDC, “essentially suppressed [findings] so media and/or Congressional staff would not become aware of the problems” and “CDC staff [went] out of their way to delay FOIAs and obstruct any inquiry.”
The indictment also claimed that CDC representatives had “irregular relationships” with corporate entities that suggested direct conflicts of interest.
While criticisms of the CDC have increased in recent years, a look back at their history reveals a long list of misconduct and questionable practices.
SCANDALS ‘R’ US
As far back as 1976 the CDC was creating mass medical terror campaigns in order to procure increased funding and justify mass vaccination programs. The infamous 1976 swine flu scandal sought to inoculate 213 million Americans for a pandemic that didn’t exist. By the time the program collapsed in late 1976, 46 million Americans were needlessly injected– despite the knowledge that neurological disorders were associated with the vaccines. This resulted in thousands of adverse events including hundreds of incidents of Guillain-Barre Syndrome.
At the onset of the mass vaccination program, Dr. David Sencer – then head of the CDC – when pushed on national TV, admitted there had only been “several [swine flu] cases reported worldwide and none confirmed.” When asked if he had encountered “any other outbreaks of swine flu anywhere in the world”, he bluntly answered, “No.”
The program moved forward.
In contrast to the CDC’s publicly stated position as “protector of public health,” this type of misconduct would become standard operating procedure and serve as the template for future invented pandemics.
A growing rap sheet of scandals would come to define the CDC’s existence.
In 1999 the CDC was accused of misspending $22.7 million appropriated for chronic fatigue syndrome. Government auditors said they could not determine what happened to $4.1 million of that money and the CDC could not explain where the money went.
In 2000, the agency essentially lied to Congress about how it spent $7.5 million that had been appropriated for research on the hantavirus. Instead the CDC diverted much of that money into other programs. “One official said the total diverted is almost impossible to trace because of CDC bookkeeping practices, but he estimated the diversions involved several million dollars.”
In 2010 Congress discovered that the CDC “knowingly endangered DC residents regarding lead in the drinking water.” A Congressional report found that the CDC did not properly warn residents of high levels of lead in the DC drinking water and “left the public health community with the dangerous and wrong impression that lead-contaminated water is safe for children to drink.”
In 2016 The Hill reported on two scandals at the CDC. One involved the “cover up” of “the poor performance of a women’s health program called WISEWOMAN.” The allegations asserted that within the program, “definitions were changed and data ‘cooked’ to make the results look better than they were” and the CDC actively suppressed this information.
The other scandal involved ties between Coca-Cola and two ‘high-ranking’ CDC officials. The two scientists were accused of manipulating studies about the safety of sugar laden soft drinks. Two days after these connections were revealed one of the accused CDC scientists retired.
These scandals were brought to light by the CDC Scientists Preserving Integrity, Diligence and Ethics in Research, or CDC SPIDER.
As part of their statement these scientists remarked:
our mission is being influenced and shaped by outside parties and rogue interests…. What concerns us most, is that it is becoming the norm and not the rare exception.”
Their complaints were filed anonymously “for fear of retribution.”
Another dodgy, yet textbook, example of the incestuous nature of Big Pharma’s Revolving Door was the case of former CDC commander Julie Gerberding. As director of the CDC from 2002 to 2009 Gerberding, “shepherded Merck’s highly controversial and highly profitable Gardasil vaccine through the regulatory maze.”
Another in a series of collusion scandals hit the CDC in 2018 when director Brenda Fitzgerald was forced to resign as she was caught buying stock in cigarette and junk food companies, the very companies the CDC regulates.
THE CDC AND THE VACCINE INDUSTRY
Although the CDC does not regulate the pharmaceutical industry, the agency’s policies and recommendations have profound implications for drug makers. Nowhere is this more apparent than national vaccination policy- in particular the CDC Child and Adolescent Immunization Schedule.
Despite pushing the world’s most aggressive vaccination campaign the facts on the ground show a decidedly different reality than CDC advertisements would lead us to believe on the efficacy of this campaign.
With the expanded vaccine schedule no demonstrable positive returns in children’s health outcomes have accompanied the windfalls to the pharmaceutical industry. Chronic disease in American children has skyrocketed from 6% to 54% in the past 40 years and the United States holds the lamentable distinction of the highest infant mortality rates in the developed world.
Some point out that the CDC currently operates as chief vaccine sales and marketing agent for Big Pharma buying, selling and distributing vaccines even as the agency has direct conflicts of interest by holding multiple patents on vaccines and various aspects of vaccine technologies. Compounding this deceptive state of affairs, the CDC poses as a neutral scientific body that assesses vaccine safety while mandating increased vaccine doses to the American people.
While the CDC does not sell vaccines directly, it does receive royalties from companies who acquire licenses to their technologies.
The CDC’s Advisory Committee on Immunization Practices (ACIP) plays a major role in this scheme. The 12 member ACIP Committee has extraordinary influence on the health of virtually all US citizens as it is the body tasked with “adding to and/or altering the national vaccine schedule.”
THE CDC AND COVID: THE ROAD TO COVID HELL IS PAVED WITH CDC OBFUSCATIONS
Besides, as the vilest Writer has his Readers, so the greatest Liar has his Believers; and it often happens, that if a Lie be believ’d only for an Hour, it has done its Work, and there is no farther occasion for it. Falsehood flies, and the Truth comes limping after it; so that when Men come to be undeceiv’d, it is too late; the Jest is over, and the Tale has had its Effect. – Jonathan Swift
As the central organization commissioned with “protecting America from health, safety and security threats,” the CDC was presented its most significant assignment in its controversial history when the Covid Crisis of 2020 spread to the shores of the United States.
The CDC would shift into hyperdrive offering up all manner of advice, guidelines, regulations, decrees and laws impacting virtually every aspect of life across the country. Most of these decrees represented radical departures from past epidemiological principles.
No stone was left un-micromanaged— even the mundane task of washing hands was transformed into a 4 page baroque ritual, video included, via CDC guidelines. It seemed the only thing notably omitted from CDC “expert guidelines” during this teachable moment was nutrition and exercise.
CHANGE WITH THE CHANGING SCIENCE™
This onslaught of edicts and definitions shifted on a weekly basis creating a climate of confusion and chaos. When questioned, the CDC would sternly proclaim “the science is settled.”
One of the more egregious examples of CDC duplicity occurred on March 24,2020 when the CDC changed well established protocols on ‘how cause of death’ would now be reported on death certificates, exclusively for COVID-19.
This seemingly benign modification became a watershed moment launching a process by which many deaths would be erroneously coded as U07.1 COVID-19. This led to massive COVID-19 death misattribution, was used to ramp up the fear and used as justification for the assemblage of draconian Covid policies.
Critics have called for a full audit of the CDC noting that, “These changes in data definition, collection, and analysis were made only for Covid” in violation of Federal guidelines. In a statement to Reuters, the CDC said:
it made adjustments to its COVID Data Tracker’s mortality data on March 14 because its algorithm was accidentally counting deaths that were not COVID-19-related.”
Two years after the problematic change in certification, the CDC would commence the process of removing tens of thousands from its “Covid death” toll.
THE COVID VACCINE
As the Covid crisis unfolded, all of the long and winding roads ended up in the same place: experimental mRNA gene therapies which were sold as ‘vaccines’ and advertised as a panacea to extricate the world from this ‘crisis.’ The CDC, as trusted go-to government body and chief marketing representative, was tasked with leading the country to safer shores and peddling Pharma’s latest cash cow to the American public.
To sell these experimental injections the CDC relied on the ever handy marketing mantra of “safe and effective”. Consistent with past maneuverings, CDC communiques on the mRNA injections were chaotic when not outright duplicitous.
Certain problems cropped up almost immediately as it was discovered that this sales pitch was dependent on flawed study designs and data that was clearly massaged and manipulated.
The very same CDC that originally touted Covid injections as being able to “stop transmission” took an abrupt U-Turn admitting they couldn’t.
Once the “vaccine” rollout was in full swing the CDC, true to form, ignored all warning signs.
As early as January 2021 safety signals pointed towards potential dangers of these controversial injections. Adverse reactions were either downplayed or completely ignored. Risk-benefit analysis was also kept off the table even as the data painted a not-so-rosy portrayal of “safe and effective.”
The CDC’s reputation took another hit when it was reported that large swaths of Covid data had been hidden from public scrutiny and independent analysis. This added to the pile of pandemic policy scandals and further tarnished the CDC’s veneer as a reliable public health agency.
POSTSCRIPT
The story of CDC kleptocracy parallels the story of contemporary US government institutions. From its humble beginnings as an agency with a mission to manage the swamp, it has degenerated into a bloated bureaucracy that has become a full fledged member of the swamp.
That the CDC isn’t telling the truth to Americans on important matters of public health is in plain sight. It is no surprise that polls show public confidence in the CDC plummeting and, in the mind’s of many, the agency’s once honorable bubble has burst.
Accusations of CDC corruption no longer exist exclusively in the skeptical minds of government critics; they have become commonplace denunciations backed by mountains of easy-to-access evidence. No conspiracy is needed as a litany of scandals have come to characterize ‘business as usual’ at the CDC.
“Can we trust the CDC?”
To find the answer ask a different question.
“Who owns the CDC?”
Michael Bryant is a freelance journalist/activist and researcher who presently focuses primarily on issues surrounding health freedom. His work has appeared on HealthFreedomDefense.org
This year, Palestinians and their supporters mark the 100th anniversary of The Balfour Declaration, a written statement from the United Kingdom’s Foreign Secretary, Arthur James Balfour, to Walter Rothschild, a leader of the British Jewish community, in favour of the establishment of a Jewish national home in Palestine.
For Palestinians, The Balfour Declaration was the beginning of their plight: a century of ethnic cleansing at the hands of European newcomers who claim Palestine as their historic home. Yet, for some reason, supporters of the Palestinians are desperate to suppress discussion of the motivation for the Balfour Declaration – how and why did it come about? … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

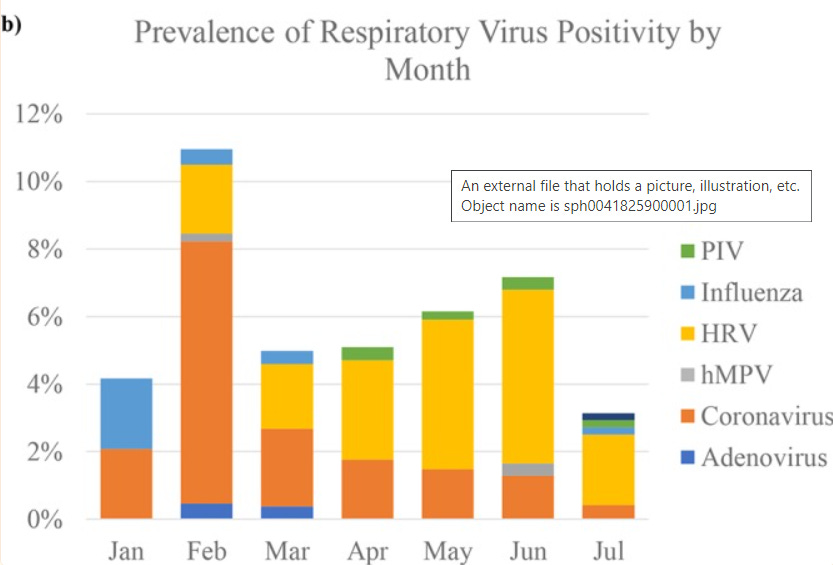



 Aletho News
Aletho News