Wise men in Washington have claimed for years that defeat in Afghanistan is what pushed the Soviet Union to collapse. Now that the US has done much worse, the world is about to see whether their theories hold water.
The last US military flight out of the Hamid Karzai International Airport (HKIA) took off on Monday, a minute before the clocks struck midnight in Kabul. The 20-year war had come to an end, and the Taliban lit up the night skies with celebratory gunfire.
To hear President Joe Biden tell it, “the largest airlift in US history” was an “unparalleled” success, executed by the US military, diplomats, veterans and volunteers “with unmatched courage, professionalism, and resolve.”
In the minds of just about everyone else who could watch the events unfold over the past two weeks, it was a mad scramble to evacuate over 100,000 Afghans eager to emigrate, with fewer than 6,000 Americans making the flights – and several hundred being left behind for diplomats to try and save.
In fact, while 82nd Airborne Division commander General Christopher Donahue and US ambassador to Afghanistan Ross Wilson were the last two people to step on the last plane, no American civilians were on board the last five flights out of Kabul. This was the startling admission by General Kenneth McKenzie of CENTCOM to Pentagon reporters on Monday evening.
“We did not get everybody out that we wanted to get out,” McKenzie said.
Compare that to the Soviet pullout from Afghanistan, which ended in February 1989. The USSR took nine months to draw down over 100,000 troops. The last man across the Bridge of Friendship into present-day Uzbekistan was General Boris V. Gromov, who turned to a TV crew and said, “There is not a single Soviet soldier or officer left behind me.”
The government of Dr. Najibullah, whom the Soviets intervened to support against the US-backed Islamists a decade earlier, fought on for three more years – collapsing only after the USSR itself imploded and stopped sending aid. By contrast, the US-backed government in Kabul vanished into thin air before the US withdrawal was even complete.
President Ashraf Ghani flew out of Kabul on August 14, letting the Taliban take over without firing a shot. The Afghan National Army, which Biden himself touted as 300,000-strong and equipped with some of the best US weaponry, simply surrendered and melted away, all that equipment taken by Taliban as trophies. The Taliban then surrounded HKIA with checkpoints, leaving the 6,000 or so US troops there to keep out desperate Afghan civilians. There were no more disturbing images of men stuck in airplane wheels – or falling to their deaths after clinging onto planes as they took off – but something worse was yet to come.
Last Thursday, a suicide bomber allegedly belonging to the ISIS-K terrorist group made it all the way to the line of US troops before blowing himself up – killing up to 200 Afghan civilians as well as 14 US troops in the process.
Biden’s response was to order two drone strikes. One reportedly killed unspecified ISIS-K leaders in another province, while another was said to have stopped a car bomb in Kabul. Except the Afghans said it killed ten civilians, seven of them children, instead.
Yet the only member of the US military sacked during this fiasco has been the Marine colonel who spoke out publicly and demanded accountability. The leadership at the Pentagon, the CIA, the State Department, and the White House that got just about everything wrong when it came to Afghanistan, remains in place.
While the Biden administration is now claiming credit for ending the 20-year war, it’s clear that its grip on the narrative – both at home and abroad – has been shaken, perhaps fatally.
For years it was thought that the US aided the Islamist mujahideen in Afghanistan only after the Soviets intervened. Until January 1998, that is, when former US national security adviser Zbigniew Brzezinski told a French publication that Washington’s support started months earlier, as part of his own plan to “give the USSR its Vietnam war.” Brzezinski outright boasted that the resulting conflict “brought about the demoralization and finally the breakup of the Soviet empire.” Many US scholars agreed.
Fast forward to the present day, and it’s the American empire that’s facing demoralization, including a political and economic crisis at home. Biden was inaugurated with 25,000 troops lining the empty streets of Washington, and declared the alleged “extremism” of his political opponents as the greatest threat to the country, now rebranded as Our Democracy. He pitched the retreat from Afghanistan to the American public as a heroic decision to end the endless war before anyone else gets hurt. It was supposed to be a feather in his cap.
With the US now exiting Afghanistan after a 20-year nation-building effort and absolutely nothing to show for it but “complete disgrace and total humiliation” – as one commentator put it – Brzezinski’s theory is about to be put to a test.
Nebojsa Malic is a Serbian-American journalist, blogger and translator, who wrote a regular column for Antiwar.com from 2000 to 2015, and is now senior writer at RT. Follow him on Telegram @TheNebulator.
Thank you to Dr Doshi for raising the profile of T-cells. Incidentally, German researchers found that a staggering 81 percent of individuals had pre-existing T-cells that cross-react with SARS-CoV-2 epitopes [1].
This fits with modelling in May by Imperial College’s Professor Friston, a world authority in mathematical modelling of complex dynamic biological systems, indicating that around 80% and 50% of the German and UK populations, respectively, are resistant to COVID-19: https://unherd.com/2020/06/karl-friston-up-to-80-not-even-susceptible-to…
Antibodies can only latch onto and help destroy pathogens outside cells and may also occasionally, paradoxically, enhance a pathogen’s ability to infect cell instead by antibody dependent ”enhancement” or ADE. It is only the T-cell that can cleverly sense and destroy pathogens inside infected cells using “sensors” which detect foreign protein fragments.
In the late 60’s the Lancet described a case of a child with agammaglobulinemia, a condition in which absence of B cells prevent them from producing antibodies, who overcame a measles infection quite normally and did not become re-infected thereafter. We now know that, although this condition can compromise immunity, in that particular case the rest of the immune functions, including T-cells, must have been perfectly up to the job of clearing infection and establishing immune memory without help from antibodies.
The importance of T-cells in fighting SARS-CoV-1 and establishing immune memory has also been well documented and discussed in a number of pre-COVID papers from 2017 and earlier [2].
Then, early in April, it was reported that two patients with agammaglobulinemia overcame COVID-19 infections without requiring ventilation [3], prompting the Italian authors to write: “This observation suggests that T‐cell response is probably important for immune protection against the virus, while B‐cell response might be unessential”.
All this should have shifted the focus of efforts towards T-cells at an early stage – the real question is why mainstream media and others continued to focus efforts and narrative on antibodies. Is it because vaccines are good at provoking antibody responses but not so great at generating T-cells? Some of the vaccines presently under trial do elicit some T-cells but it seems that neither the quantity nor variety are hugely impressive.
Does this matter? Apparently so: Research establishments including Yale found that in mild or asymptomatic cases, many T-cells are produced. These were highly varied, responding not just to parts of the Spike, S protein or Receptor Binding Domain but to many other parts of the virus [1, 4-6]. Notably, in these mild cases there were few or no detectable antibodies.
Conversely, the severely ill produced few T-cells with less variety but had plenty of antibodies. What is also of interest is that men produced fewer T-cells than women, and unlike women, their T-cell response reduced with age [7].
So why are some people unable to mount a good protective T-cell response? The key to this question might be a 10-year-old Danish study led by Carsten Geisler, head of the Department of International Health, Immunology and Microbiology at the University of Copenhagen [8].
Geisler noted that “When a T cell is exposed to a foreign pathogen, it extends a signalling device or ‘antenna’ known as a vitamin D receptor, with which it searches for vitamin D,”, and if there is an inadequate vitamin D level, “they won’t even begin to mobilize.” In other words, adequate vitamin D is critically important for the activation of T-cells from their inactive naïve state.
The question of whether T-cells might also need a continuing supply of vitamin D to prevent the T-cell exhaustion and apoptosis observed in some serious COVID-19 cases [9] deserves further research.
High levels of vitamin D are also critical for first line immune defences including physical mucosal defences, human antiviral production, modulating cytokines, reducing blood clotting and a whole host of other important immune system functions [10]. The obese, diabetics and people of BAME origin are far more deficient in vitamin D and men have lower levels than women [10].
Another intriguing clue is that Japan has the highest proportion of elderly on the planet but despite lack of lockdowns, little mask wearing and high population densities in cities, it escaped with few COVID deaths. Could this, at least in part, be because of extraordinarily high vitamin D levels of over 30 ng/ml in 95% of the active elderly [11]? By comparison, UK average levels are below 20ng/ml [10].
Vitamin D is made in the skin from the action of UV sunlight, food usually being a poor source, but the Japanese diet includes unusually high levels. Sunny countries near the equator (e.g. Nigeria, Singapore, Sri Lanka) also have very low COVID related deaths.
The results of the first vitamin D intervention double blind RCT for COVID was published on 29 August by researchers in Córdoba, Spain. This very well conducted study produced spectacular outcomes for the vitamin D group (n=50), virtually eliminating the need for ICU (reducing it by 96%) and eliminating deaths (8% in the n=26 control group). Although this was a small trial, the ICU results are so dramatic that they are statistically highly significant [12].
Substantially more vitamin D is required for optimal immune function than for bone health. It seems Dr Fauci is not ignorant of this, having apparently confirmed on TV and by email that he takes 6,000 IU daily! (see Dr John Campbell on YouTube Vitamin D and pandemic science, 16 September 2020). Meanwhile the US’s health body continues to recommend only 600-800 IU and the UK’s, only 400 IU.
It is high time for joined up solid scientific rationale to overthrow mainstream narratives based on an alternative “science” controlled by industry interests/politics. Beda M Stadler, the former Director of the Institute for Immunology at the University of Bern, a biologist and Professor Emeritus, certainly appears to think so (see Ivor Cummins Ep91 Emeritus Professor of Immunology… Reveals Crucial Viral Immunity Reality on YouTube, 28 July 2020).
In the same way that prior infections protect us against future infections by means of cross-reacting T-cells, overcoming COVID-19 naturally offers potential for greater protection against future coronaviruses. Vaccines have their place but so do our amazingly complex, sophisticated, highly effective immune systems which have evolved over millennia to protect us from a world teeming with trillions of pathogens.
References
Annika Nelde, Tatjana Bilich, Jonas S. Heitmann et al. SARS-CoV-2 T-cell epitopes define heterologous and COVID-19-induced T-cell recognition, 16 June 2020, Research Square https://www.researchsquare.com/article/rs-35331/v1%20
William J.Liuabc et al. T-cell immunity of SARS-CoV: Implications for vaccine development against MERS-CoV.Antiviral Research. Volume 137, January 2017, Pages 82-92 https://doi.org/10.1016/j.antiviral.2016.11.006
Soresina, A, Moratto, D, Chiarini, M, et al. Two X‐linked agammaglobulinemia patients develop pneumonia as COVID‐19 manifestation but recover. Pediatr Allergy Immunol. 2020; 31: 565– 569. https://doi.org/10.1111/pai.13263
Avraham Unterman, et al. Single-Cell Omics Reveals Dyssynchrony of the Innate and Adaptive Immune System in Progressive COVID-19. medRxiv 2020.07.16.20153437; doi: https://doi.org/10.1101/2020.07.16.20153437
Leticia Kuri-Cervantes, et al. Immunologic perturbations in severe COVID-19/SARS-CoV-2 infection. bioRxiv 2020.05.18.101717; doi: https://doi.org/10.1101/2020.05.18.101717
Floriane Gallais, Aurelie Velay, Marie-Josee Wendling, Charlotte Nazon, Marialuisa Partisani, Jean Sibilia, Sophie Candon, Samira Fafi-Kremer. Intrafamilial Exposure to SARS-CoV-2 Induces Cellular Immune Response without Seroconversion. medRxiv 2020.06.21.20132449; doi: https://doi.org/10.1101/2020.06.21.20132449
Takahashi T, Wong P, Ellingson M, et al. Sex differences in immune responses to SARS-CoV-2 that underlie disease outcomes. Preprint. medRxiv. 2020;2020.06.06.20123414. Published 2020 Jun 9. doi:10.1101/2020.06.06.20123414
Von Essen MR, Kongsbak M, Schjerling P, Olgaard K, Odum N, Geisler C. Vitamin D controls T cell antigen receptor signaling and activation of human T cells. Nat Immunol. 2010;11(4):344-349. doi:10.1038/ni.1851
Diao B, Wang C, Tan Y, et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front Immunol. 2020;11:827. Published 2020 May 1. doi:10.3389/fimmu.2020.00827
King, E.. The Role of Vitamin D deficiency in COVID-19 related deaths in BAME, Obese and Other High-risk Categories. 2020, June 17. https://doi.org/10.31232/osf.io/73whx
Nakamura K. Vitamin D insufficiency in Japanese populations: from the viewpoint of the prevention of osteoporosis. J Bone Miner Metab. 2006;24(1):1-6. doi:10.1007/s00774-005-0637-0
Marta Entrenas Castillo et al. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. The Journal of Steroid Biochemistry and Molecular Biology. Volume 203, October 2020, 105751. https://doi.org/10.1016/j.jsbmb.2020.105751
Two things. First, economic growth saves children’s lives. That is one of the most basic, starkest facts about the modern world.
Second, there is a thing called the “degrowth movement”, which wants to stop economic growth. And, yes, this would lead almost inevitably to the unnecessary deaths of thousands of children a day.
As child mortality has gone down, so has global poverty — while global economic output has increased. Correlation is not causation, of course – but this isn’t just true at a global level, but at a country-by-country level. Nowadays, if your country is rich, your children are more likely to live. That is amazingly obvious on this chart. If you live in the rich Iceland, for example, your child is 60 or 70 times less likely to die before its fifth birthday than if you live in the poor Central African Republic or Democratic Republic of Congo, where about one child in every 10 dies in its first five years.
And on that second point: some people really think that that economic growth should stop, right now. Jason Hickel is an anthropologist and one of the key voices in what is known as the “degrowth” movement. He argues that — in rich countries, at least1 — we ought to stop aiming for economic growth immediately. He thinks that “green” growth, the idea that we can grow our economies while reducing carbon emissions, is a chimera, or at least that it cannot happen fast enough to avoid disastrous outcomes from climate change.
Hickel, of course, denies that economic growth saves lives. In fact, he doubly denies it. First, he denies that global poverty has gone down as a result of economic growth. In 2019, he argued that all those famous charts showing a huge decline in global poverty are false, because they focus on very extreme poverty — people living on the equivalent of $1.90 a day or less. If you look at some more reasonable threshold of “poverty”, he says, such as $15 a day, the decline disappears.
This is straightforwardly untrue, for the record. Whatever threshold you use, people are getting richer. People have generally shifted from lower incomes to higher incomes, and as a result fewer children are dying.
And secondly, Hickel denies that economic growth does save children’s lives: or, rather, that it does beyond a certain, quite low level. “Past a certain point, the relationship between GDP and social outcomes breaks down or becomes irrelevant,” he says. “After that, what matters is distribution and access to public services.”
But this doesn’t seem to be true either. If it were, you’d see that very poor countries have consistently high child mortality, but that as you reach the middle-income and rich countries, it would be much more mixed. But in fact there’s still a strong relationship, and middle-income countries like China and Brazil have much higher infant mortality than rich countries like the UK and Japan. If you live in Brazil, there’s about a one in 60 chance that your child will die before its fifth birthday. In China, one in 100. In the UK, it’s way down at one in 250-ish.
You could look at the reduction in child mortality over time, as the world has become richer, as one of the great success stories of our time. In a way you’d be right to do so, but it is a hugely unfinished story. Children are still dying at an awful, unacceptable rate of about 14,000 a day — Max Roser of Our World In Data describes it as “equivalent to a crash of a jumbo jet with only children on board, every hour of every day of the year”.
Nonetheless, it is true that economic growth appears to have saved millions of children’s lives. That 14,000 a day would be something more like 100,000 a day, if children were dying at the rate they used to.
Also note that “economic growth” doesn’t necessarily mean “free-market capitalism”. As Noah Smith points out, a lot of the reduction in global poverty has been about smart government action (especially in Latin America), or China’s complicated industrial and economic reform, not simply free-market policies – although at the very least it’s fair to say that global capitalism hasn’t got in the way.
But this broadly positive story is a closed book to Hickel and the degrowth movement. It’s instinctively difficult to understand why anyone would want to deny it, but I have two theories.
One is that it’s very hard to acknowledge that things can get better without being good. It’s a common problem. It is, for instance, almost certainly true that the UK is much less racist and sexist than it used to be. But it’s also clearly true that there are real problems that continue to exist. It is extremely hard to say “the UK has become better with regards to racism and sexism” without people hearing “the UK is not racist or sexist”.
If you’re Jason Hickel, you might see people arguing that poverty has decreased, and assume that they mean “and therefore global poverty is no longer a problem”. That is, of course, absolutely not the case.
The second hypothesis is a more complicated one — and has to do with something called “prevalence-induced concept change”. Imagine that you have dedicated your life to some problem: say, reducing littering in a local park. You work really hard. You set up a charity and solicit donations; you put together a workforce. And, bit by bit, you successfully reduce the problem. The park becomes a bit less litter-filled. What do you do? Do you say to your charity’s staff, “The park is doing a bit better now, we probably don’t need so many of you. And we should probably reduce our demands for donations, as well”?
Human nature being what it is, probably not. More likely (and as happens in laboratory settings), you will simply start focusing on smaller and smaller things. Before, you had shopping trolleys in the pond and a dead sheep in the playground, and you focused on them. But now that they’ve gone, your attention will focus on the crisp packets and fag butts. Partly that’s because you now have the attention to spare, because the bigger problems have been solved; but it’s also partly because, if you start saying “actually the situation is a bit better now”, it will be harder to rally support for your cause.
I think this is a really important driver of human behaviour. It is very hard to ever admit things are getting better along any axis, because if you do, it feels like you’re saying: “So you can stop working hard to fix this problem.”
Similarly, if you’re Jason Hickel and you’ve dedicated your life to fighting global poverty (and to saying that global poverty is all because of capitalism and colonialism and that economic growth is bad), then it will be really inconvenient if someone says: “Actually, global poverty has decreased significantly, that reduction seems to be correlated with economic growth, and it has had amazing positive outcomes such as a huge reduction in child mortality.” It will be very tempting to find ways of ignoring that reality.
I worry, though, that it is counterproductive to tell people that all their hard work improving some situation has had no effect. If all those decades of buying low-energy lightbulbs and reducing flights and eating less meat have not improved the climate, then why shouldn’t I just stop bothering? If all those anti-racism campaigns and hate-speech laws and so on made no difference, what’s the point? And in the case of poverty, if economic growth doesn’t reduce global poverty, then it does indeed make sense to give up on growth altogether. But in reality, economic growth does reduce global poverty, and reduced poverty saves children’s lives.
But the degrowth movement is right, in one sense. Growth almost certainly can’t carry on forever. If the economy grows at 2% a year every year, which it roughly has for the last century or so, then it doubles in size every 35 years.
That’s not sustainable in the long term. In 8,250 years — as Holden Karnofsky of the Open Philanthropy Project points out — the economy would have grown to 3*1070 (that is, a 3 followed by 70 zeroes) times its current size. There are, for context, about one-third that many atoms in our galaxy. And 8,250 years isn’t very long: there are cities which have been around for longer.
Perhaps growth will continue into the far future. I could imagine some weird universe of simulated worlds and uploaded humans — and indeed others have. But probably, the more likely outcome is that growth slows or stops or reverses in the next few centuries.
The question, of course, is when it should stop. I, for one, would rather wait until the children stop dying so much. Hickel and the degrowth movement think it should be sooner. But if they want to make that case honestly, they should admit the reality of all the dead children.
FOOTNOTES
It’s worth noting that Hickel doesn’t think we should stop aiming for growth everywhere: just in rich countries. But rich countries that buy much of the goods produced in poor countries, driving their growth, so that would be a very difficult needle to thread.
AWESOME interview conducted by Vaccine Choice Canada, August 21. Dr. David Martin reveals shocking news everyone, especially Canadians must demand authorities investigate – potentially treasonous acts and crimes against humanity.
As you probably know, since 2020, this pandemic has poisoned the lives of billions of individuals across the world. Meanwhile, the World Economic Forum (WEF) cannot contain its excitement. Indeed, this powerful, influential, elite-owned organization keeps posting bizarrely upbeat videos about the “advantages” and “opportunities” of COVID-19.
Needless to say, people absolutely hate these videos. They are ruthlessly downvoted on YouTube and 99.85% of the comments express utter disgust. But that did stop the WEF from creating more absurdities.
On August 17th, the WEF posted a video titled “This is how our lives would soon look”. And it looks likes the trailer of a dystopian horror movie where people are treated like dehumanized cattle.
The first thing they make abundantly clear is that they don’t want you or your children to leave the house. They want you to work from home and they want your children to learn from home. And they believe that these changes will be so permanent that offices will need to be repurposed and entire neighborhoods will need to be redesigned.
They don’t even want you to leave the house to get food. Also, they want you to wear a mask in your own house when you get that food. “Analytics-driven services” implies that big tech companies will analyze your web searches and consuming habits to “predict” what you want and have it sent to you.
Same thing.
If you decide to go crazy and actually get out of the house to meet other people, they want it to be like this:
If you meet another human being, it’s going to be with hand sanitizer and permanent masks. Don’t forget to scan that QR code so they know exactly where you are and who you are meeting with.
They’ll also want to track you in the creepiest way possible.
I hate every word in this sentence.
According to the WEF, masks will be a permanent thing. And, because of that, their precious face recognition systems won’t work as well. So what’s the solution? Stop with the masks because pandemics are temporary? Of course not. Stop with the tracking of individuals? Are you crazy? Their answer: Shoot lasers right at our hearts and listen to our heartbeats to ID us. Yes, that’s the most insane answer to that question and that’s what they put in their video.
These creeps are also “laser-focused” on our children. They want to shape and mold them according to their dystopian principles. For this reason, the WEF promotes permanent remote learning on screens.
They want your children to be locked inside the house, staring at screens all day.
Although remote learning has been nothing less than disastrous for the development and mental well-being of children, the WEF wants it to become permanent. And to sell that insane idea, they claim that it would “improve their digital skills”.
That’s the weakest argument I’ve ever heard regarding anything in my life. Children today absolutely do not need to “improve their digital skills”. They learn how to use phones and tablets before they actually learn how to walk. If anything, they need to scale back their “digital skills” by a couple of notches and boost their “go outside and get dirty” skills by a couple of notches.
The WEF knows very well that children need to play, socialize and communicate with other children to develop properly. However, they do not want children to develop properly. That’s the scary, terrifying truth about their agenda. They’re looking to deny vital elements of a child’s development in order to create the kind of human they want living in their dystopian society.
They really want COVID hysteria to be permanent.
Not unlike previous WEF videos, this one was received with universal disgust. Here are some Twitter replies to the video (I didn’t cherrypick them, they’re literally all like that).
In Conclusion
As you might have noticed, these videos aggravate me, like they aggravate nearly everyone who watches them. And for several reasons. First, who voted for any of this? Did anyone see the name of Klaus Schwab – the head of the WEF – on any election ballot? Of course not. In fact, Schwab has been working for years to dismantle national democracies.
Schwab as publisher of the World Economic Forum’s 2010 “Global Redesign” report postulates that a globalized world is best managed by a coalition of multinational corporations, governments (including through the UN system) and select civil society organizations (CSOs). It argues that governments no longer are “the overwhelmingly dominant actors on the world stage” and that “the time has come for a new stakeholder paradigm of international governance”. The WEF’s vision includes a “public-private” UN, in which certain specialized agencies would operate under joint State and non-State governance systems.
According to the Transnational Institute (TNI), the Forum is hence planning to replace a recognised democratic model with a model where a self-selected group of ‘stakeholders’ make decisions on behalf of the people.The think tank summarises that we are increasingly entering a world where gatherings such as Davos are “a silent global coup d’etat” to capture governance.
– Wikiepdia, Klaus Schwab
Second, every single WEF video unironically promotes a joyless, freedomless world where everything that makes life worth living is banned. They want you to stay in your house while they extract what they need from you using technology. They want to train your children to be the same. They don’t want you to wander too far from your home and, if you do, they want to track you on a biological level. They especially don’t want you to interact with other human beings in a normal way because that might spark some humanity in you.
Is this how you want to live? Is this the world you want your children to grow up in? If not, we need to actively reject every attempt to make their plans a reality, on every level possible.
In this interview, Thomas Lewis, Ph.D., and Dr. Michael Carter explain how biomarker panels can help you take control of your health by identifying underlying chronic infections that might be sabotaging your health. Lewis is a microbiologist with a Ph.D. from MIT and certifications from the Harvard School of Public Health and Carter is an integrative physician.
They run a company that performs diagnostic testing to guide patients through a process of diagnosing various ailments. Biomarkers such as D-dimer, fibrinogen, clotting factors and auto antibodies, which are largely ignored by the mainstream, can clue you in on where you lie on a health/disease continuum.
Importantly, poor COVID outcomes are rare unless you have two or more comorbidities, and in the last year, they’ve developed a more refined way of assessing an individual’s COVID-19 risk using a panel of specific markers associated with inflammation and blood clotting.
Their testing helps YOU understand where you are on the health-disease continuum. In their model, you are not either sick or well — you are somewhere on this continuum. Find out where you are and then work to improve your status.
“Really, it’s your chronic health status that helps you figure out where you are in the continuum for COVID risk,” Lewis explains. The same goes for the COVID shot. According to Lewis, whether you got COVID-19 or the vaccine, the risk factors that determine whether you’ll have a serious bout of COVID-19 or experience more serious adverse events from the shot are identical.
The Role of Underlying Infections
Underlying or latent infections can play a significant role not only in chronic disease but also in SARS-CoV-2 infection. Judy Mikovits, Ph.D., has pointed out the role of retroviruses and coinfections with pathogens such as borellia and babesia in leading to less favorable outcomes in COVID.
Her hypothesis is that SARS-CoV-2 in and of itself is not the primary cause of COVID-19. She’s convinced there must be a coinfection along with SARS-CoV-2 that suppresses or compromises your immune system in order for symptomatic COVID-19 to occur.
Carter and Lewis have discovered a number of infectious pathogens that are even more prolific than those highlighted by Mikovits, and which appear central in triggering many chronic conditions that then predispose you to more severe COVID-19.
Primary among those are bacteria involved in periodontal disease (periodontitis). You don’t have to have oral issues or root canals to have a high burden of periodontal pathogens. The Lewis/Carter team test for these pathogens using an oral DNA home test kit.
Another is chlamydia pneumoniae, a respiratory pathogen that 60% to 70% of older adults have antibodies against. Chlamydia pneumoniae plays a role in several common age-related conditions, including Alzheimer’s disease, heart disease and rheumatoid arthritis. Unfortunately, few are ever tested for the presence of this organism.
According to Lewis and Carter, inflammatory markers and clotting markers such as C-reactive protein, fibrinogen, uric acid, the neutrophil-to-lymphocyte ratio, D-dimer, and sedimentation (SED) rate are strongly associated with innate immune response activity and chronic infections, which in turn correlate with COVID-19 severity.
“What’s tricky about these organisms is they don’t always show up from the classic acute perspective of diagnostic,” Lewis says. “If you talk to any infectious disease doctor that’s not functional in nature, they’ll say that the IgG antibody is historic. But I can guarantee you they’re completely wrong.
They’re not looking at things from a chronic, stealth [perspective]. Do we think chickenpox, the herpes zoster virus, is the only organism that can cause problems and then go dormant and reactivate when you’re immune-compromised later in life? No.
Every single one of these organisms has a potential opportunity to go from an acute phase to a chronic phase. Some never even express acute disease. They just hang out in biofilms and will express in the chronic phase later in life, causing disease of “unknown” origin!
It’s called crypticity, which makes it extremely difficult to create, in the minds of doctors and researchers, the association between the disease and the exposure. Sometimes these exposures are congenital. They happened pre-birth. So, that’s really the art.”
So, to clarify the hypothesis presented by Lewis and Carter, the conventional view is that these infections, once they’ve generated an IgG antibody response, no longer pose a threat to your body. But this isn’t the case.
They can indeed lay dormant only to later contribute to chronic diseases that, on the surface, appear to have nothing to do with a pathogenic infection. The book by Paul Ewald titled, “Plague Time: The New Germ Theory of Disease,” written in 2000, explains well this conundrum.
How to Identify Underlying Infections
The clinical approach to identifying whether an underlying infection is at play in a particular disease is to look at antibody levels. Immunoglobulin G (IgG) is reflective of long-term protection and also happens to be the most common antibody, found in blood and other body fluids. It protects against both viral and bacterial infections and tends to be elevated when the infection has reached a chronic state.
Immunoglobulin M (IgM) is associated with acute responses to infections and is found primarily in your blood and lymph. It’s the first antibody to be made when your body encounters a new pathogen. Carter explains:
“Everyone has a baseline level of IgG and IgM, especially in the acute phases, but the long-term IgG, once it is above the normal background level, then in many cases, especially in those who are symptomatic with various diseases, there is reactivation of that virus, bacteria, parasite or other pathogen, what have you — any grouping of these organisms that can smolder and cause disease patterns.
The driver is inflammation and tissue destruction. The mechanism is simple. We all have some “wear and tear.” These organisms increase wear and tear so your “repair and recovery” pathways cannot keep up.
We also — even without doing those IgG levels, just on our basic platform of biomarker testing — can see things in the complete blood count where, let’s say our white blood cell count has a ‘normal range’ somewhere between 3.8 and 10.8 depending on the lab. But that’s a very wide normal range.
Really, anything above 6.2, in terms of your white blood cell count, is an indicator that something is brewing. When we start looking deeper at the neutrophils, the lymphocytes, the basophils, the monocytes and eosinophils, when those values are increased or decreased beyond the optimal range, we can tell that there are critters being unruly even though you don’t have fever, chills or a classic increase in white blood cell count.
So, we know that these pathogens are present in everyone. It’s really incumbent upon your own immune system to be vigilant to keep them at bay and stop them from replicating.”
In summary, if you have elevations (or suppressions) in white blood cell markers, then you likely have an infectious process going on in your body. There’s also typically a direct correlation between your antibody level and the risk of disease, so the higher your antibody level, the greater your risk of chronic disease and poor COVID / JAB outcomes.
PCR testing can be useful for identifying a specific pathogen. However, if excessively high cycle thresholds (CTs) are used (as has been the rule when testing for SARS-CoV-2), the test becomes useless, as it can find even a single molecule if run at a high-enough CT. So, the CT needs to be below 26 to avoid false positives.
Review of Lewis and Carter’s Research
Before we go further, here’s how Lewis describes their research, and how it can improve your health and medical decisions:
“Carter and I are not researchers. We like to fancy ourselves translators of best clinical research. There’s really great science published, but medicine is a business decision. Less than 1% of the great medical research makes it to clinical practice.
We had the opportunity to evaluate 100 people at a Fortune1000 company. Based on that, we made an assumption that, because of their health status, 42 of them had some sort of an infectious process.
So, we were given license to test IgM, IgG, bacterial [and] viral. Forty-one of 42 were positive using our testing. Now, we’re not looking for everything in the universe. We’re telling the lab what to look for: what we call ‘usual suspects.’ Some of them had IgM and IgG, and some of them just had IgG with a negative IgM for a single or multiple pathogens.
When we treated them over nine months, everyone got better. What was remarkable is IgG levels [indicative of chronic infection] came down. When someone had a negative IgM but a positive IgG and symptoms, and their IgG level came down, they got better too. This proves that IgG is indicative of the presence of a “hidden” but chronically active infection.
So that’s not an extraordinarily scientific evaluation, but it’s completely consistent with the work of folks like Charles Stratton out of Vanderbilt, who’s written about chlamydia pneumoniae and its three different life forms.”
There are many other researchers and clinicians who have come to this conclusion. Lewis and Carter are in the process of publishing a peer-review medical paper that references many other publications explaining how important an IgG antibody test is.
Treating Chronic Versus Acute Infections
Carter and Lewis have developed a pretreatment program, followed by a variety of treatment strategies aimed at chronic infections. As you might expect, the chronic infection treatments involve more aggressive approaches, and will depend on whether the infection is caused by bacteria, viruses or parasites.
The biggest factor for effective treatment is eradicating pathogens hiding in biofilm, which takes time. (We do not address the use of specific remedies in this interview, as each patient must be tested, seeing how there’s such a broad array of potential causal factors.)
As noted by Lewis, even if you use a broad-spectrum anti-infective, such as ozone, you’ll rarely eradicate enough of the chronic phase of these organisms, as they shelter inside biofilms or inside your cells — including your white blood cells. that are very difficult to get into. These pathogens are often referred to as “obligate intracellular pathogens.” The “obligate” part infers that these harmful organisms rob your energy by mimicing to be your mitochondria. He explains:
“For long periods of time, you have to maintain a physiologically anti-infective dose. The other piece of it that we’ve learned, [and which] everybody knows much better now because of COVID-19, is the inflammatory component. There’s no question that the inflammatory response can override, go too far, even in chronic conditions.
There’s a brilliant paper by Australian groups that talk about cytokines, anti-inflammatory treatments and their clinical relevance.
The biggest problem we face is that, if you bang your elbow and your brain at the same time with the same sort of force, your elbow will recover in a couple weeks, but the brain perpetuates inflammation much longer, and sometimes forever. Consider traumatic brain injury as an example. It happened one time a while ago, but your brain stays “inflamed.”
So, every treatment has to consider an infectious [risk], has to consider lifestyle risks, and help you optimize those things. But generally, there has to be a very strong anti-inflammatory component, which … has to be rigorous and continuous. That’s the big challenge …
Dr. Stratton at Vanderbilt has shown that these organisms can live in an elementary body, a reticular body, and a “cryptic” phase. In some of these phases they’re completely refractory [i.e., resistant] to antibiotic treatment …
J. Thomas Grayson, 95 years old, [a doctor of] preventive medicine at University of Washington … showed that … when it comes to organisms like chlamydia pneumoniae, you have to treat for one year. That’s scary for people, so what we do is we do three-month segments and then retest. Obviously, we measure for symptoms, but also the IgG.”
The Role of Vitamin D
A basic intervention that is really important for shoring up your immune system is vitamin D. Vitamin D is really a pro-hormone and hormones regulate physiological processes. I believe vitamin D optimization — making sure your blood level is between 60 ng/mL and 80 ng/mL (150 nmol/L and 200 nmol/L) — is one of the easiest, least expensive and most important things you can do to avoid infections of all kinds, including COVID-19.
The activated form of “vitamin” D is produced in your liver when you have an infection and it is strongly antibiotic. Lewis and Carter recently completed a study in which they looked at the vitamin D level compared to neutrophil and lymphocyte ratio. Lewis explains:
“Neutrophils go up with bacteria. Lymphocytes often go down with viral infections, so [your neutrophil to lymphocyte ratio] is sort of a measure of your overall infectious burden.
What we did recently, and we’re putting this into a paper we’ll be publishing, is a study of neutrophil-to-lymphocyte ratio versus blood 25 hydroxy vitamin D levels. We saw a very clear linear relationship between a bad neutrophil to lymphocyte ratio count and low vitamin D, and then just the opposite.”
They’ve also found a similar correlation between chronic infection and free cholesterol (not total cholesterol). This correlation appears particularly strong in those with cancer, who typically have a free cholesterol level of 50 ng/mL and above. An optimal level is thought to be somewhere between 5 ng/mL and 20 ng/mL, with the healthiest of people typically falling between 5 ng/mL and 15 ng/mL.
When free cholesterol is elevated, you’re more prone to tissue destruction, as cholesterol is an important repair molecule. Since your cholesterol level can indicate your tissue repair capability, it is also included in Lewis’ and Carter’s COVID panel.
“Cancer patients are, I think, just the tip of the iceberg in terms of people that have some virulent infectious process that is destroying tissue,” Lewis says. “I’m pretty sure we’re going to see a very strong correlation to your free cholesterol number as part of the portfolio of tests you want to do to investigate what is going on inside your body.”
How Do You Know if an Infection Is Chronic?
One way to determine whether you’re suffering from an acute or chronic infection is to look at the half-life of the factors being measured. Lewis explains:
“If you take a test now and in three months and you see a sustained trend of biomarker elevation, that’s obviously a way to relate it to chronic infection. But in a single test, every biomarker has a half-life. Red blood cell distribution width, because it’s tied to red blood cells, it’ll stick around for four months.
It has a much longer half-life than say C-reactive protein. If you bang your knee, [C-reactive protein] will go way up, then come down with the half-life of one and a half days.
Fibrinogen is seven days. When you understand half-lives, then when you look at a single lab and they’re all elevated to sort of the exact same extent above what we consider our baseline, then we know it’s chronic, or at least with a very educated guess, that it’s in the chronic phase.”
What’s in the Panel?
Speaking to the issue of what the panel Lewis and Carter developed contains, Carter explains:
“A typical panel … is a very concise panel of blood biomarkers. We expand that with the inflammatory markers that really play a role [in chronic infections].
So, if your homocysteine and C-reactive protein are up, these are key inflammatory markers that many people are walking around with that are high and that are really directly causing toxicity to the [blood]vessels, [thereby] leading to coronary artery disease, stroke, Alzheimer’s and a whole host of things. Almost every chronic disease starts in the vessels — more specifically the capillaries.
High sensitivity C-reactive protein is another inflammatory marker that when elevated is really indicative of pathogens in the mouth, among other things. That is one thing that is totally missed by traditional doctors [but] is a key component. The oral testing we do includes Interleukin-6 that tracks closely with C-reactive protein.
If you’ve had root canals or wisdom teeth taken out, or have bleeding gums, [we can] test to see the vast array of pathogens that we know are associated with pretty much every disease syndrome out there.
So, we take these things that have been invisible to the masses and bring it at an affordable cost structure. We have a very robust panel of 55 biomarkers that runs about $150, including vitamin D … If you were to take that same panel, it would be $400 to $500 if you were to go directly to LabCorp.
However, we highly recommend you get this testing from us with a one-hour consult included because of our unique way of explaining the “story” behind your biomarkers — and what you can do to take control of your health. Even with the consult, our pricing is less compared to the labs alone from most places.”
In addition to helping you evaluate your chronic disease risk, this panel will also help you assess your COVID-19 risk. They also offer an advanced panel that is even more comprehensive. It costs about $400 and includes a one-hour consultation to help you understand what all the markers mean.
As noted by Lewis, “It’s all about where do you lie on the health/disease continuum. We very accurately are placing people on that, and there’s not a marker we test for that’s not modifiable through lifestyle or other appropriate interventions. We’re not treating symptoms. We’re going right at the disease.”
Where to Get the Panel
If you’re interested in ordering this panel, go to HealthRevivalPartners.com. If you want to get the comprehensive COVID / JAB risk screening panel, go to www.healthrevivalpartners.com/post-jab-tests. You will be asked to fill out a questionnaire, after which you receive a requisition to have your blood drawn at a LabCorp.
The report you get will be a comprehensive and detailed report from Health Revival Partners in addition to the standard lab report. Carter explains:
“It really starts with the initial questionnaire and we give you a grade from A to F. We wanted to make it so that the average person could really see what is going on in a very tangible fashion. Obviously, you answer 125 questions that are much more probing than your traditional questionnaire.
If you end up with a grade of C, D or F, then that tells you your report card of health is not so good. Then we give guidelines on those questions. When you do your biomarker test, we give you a temperature. It’s called your chronic disease temperature and of course 98.6 is a normal temperature.
When we do the biomarkers, we look at optimal ranges, not just normal ranges. We want everyone to be optimal, not just normal. When those values are either too high or too low out of the optimal range, then you get a corresponding increase in your temperature.
Our “normal” ranges are best on early mortality data for each biomarker. Our normal levels are much tighter compared to the standard of care. We are looking for chronic (smoldering) whereas they are only looking to see if you are very sick or acutely sick.
So now you can have a temperature of, say, 103 based on high homocysteine, high C-reactive protein, high fibrinogen, high white blood cell count and various other biomarkers. We’re testing 55 biomarkers, but 21 of them really home in on and create that temperature setting … Even more biomarkers are part of the COVID panel.
When you correlate that to COVID, we have a little analogy of what’s in your glass. If your glass is a quarter-full, half-full, three-quarters full, you could be walking around with all of these different things: toxins, pesticides, subacute infections.
When your glass gets full and overflowing, then generally that’s going to express as disease. We show where people are on that continuum. How full is your glass of these different things? With the biomarker panel, that gives us a great window [into your COVID risk].”
Building a Stronger Foundation for Functional Medicine
Again, to learn more, and to join the Health Revival Partners’ chronic disease support program, go to HealthRevivalPartners.com. In closing, Lewis notes:
“Integrative and functional medicine is like herding cats. They got into that because they’re outliers, but I’ve been trying to get some of the highest-level leadership in functional medicine to create a core standard of labs that every doctor takes because the biggest reason why you’re not getting served well in medicine today is because the dark side is saying we don’t have the evidence.
One of Carter’s and my life’s goals is to herd the functional integrative cats together to build standards, and I think we’ve done a very good job of creating a very important end-point standard that I think anybody could hang their hat on. That’s early mortality. So, we really want to do that.
“The other part of it is we wrote a peer-reviewed paper1 last year, and we coined the term the ‘pre-cytokine storm.’ Carter talked about your glass being a quarter-full, half-full or overflowing. Measuring your pre-cytokine storm — which our panel incorporates, and then our COVID panel expands even more, so either of those panels are available to anybody that comes to our site — will tell you what your risk factors are.
Your blood doesn’t lie. So, what I’m hoping people will do is become part of the solution. Take the COVID and the vaccine survey, get your COVID risks labs drawn, and then we’ll be able to report back to you and publish peer-reviewed articles about this correlation that right now we’re all being marginalized on because we’re not creating enough evidence.
Judy [Mikovits] knows exactly what’s going on, but to convince the world, we’ve got to get more conventional and functional lab data in large sets to prove our point. That’s how we’re going to start winning, with evidence-based functional medicine.”
Over the past year and a half, hysterical media reporting on matters Covid-19 has reduced some people to a fearful state of unquestioning compliance – including a great number of otherwise critically-thinking journalists.
With screaming headlines in bold and large font such as, ‘Will this nightmare ever end?’ and ‘Mutant virus skyrockets…’ and ‘Fear grows across the country: VIRUS PANIC’, and ‘Coronavirus horror: Social media footage shows infected Wuhan residents ‘act like zombies’, it is no wonder many people are in a state of panic.
In times when many are suffering mentally and physically under unnecessary and prolonged lockdowns, the incessant fear porn is causing excessive anxiety, which in turn will affect the health & mental well-being of some, if not many.
In government documents from the UK’s Scientific Advisory Group for Emergencies (SAGE) dated from March 2020 advice was given saying:
“The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging… This could potentially be done by trained community support volunteers, by targeted media campaigns, social media”
I’d say the UK media campaigns weren’t so much ‘targeted’ as ‘blanket’ but they certainly did the job, and other Western nations got similar directives. The UK government also became the nation’s biggest advertiser in 2020, make what you will of the potential ramifications that could have on cash-strapped newspapers and their supposed ‘independence’.
Having myself been deeply focused on exposing war propaganda and other media lies around Syria, Palestine, Venezuela, and elsewhere over the years, my default position has become one of deep cynicism on mass media reporting. Yes, you can find nuggets of truth, or even excellent journalists in mainstream publications, honestly challenging the narratives.
But those are few and far between, generally you find copy-paste propaganda emanating largely from the bowels of the USA and the UK.
A study by Swiss Propaganda Research (SPR) noted, “most of the international news coverage in Western media is provided by only three global news agencies based in New York, London and Paris.”
Those agencies are AP, Reuters, and AFP. SPR notes:
“The key role played by these agencies means Western media often report on the same topics, even using the same wording. In addition, governments, military and intelligence services use these global news agencies as multipliers to spread their messages around the world.”
Given all of this, I’ve come to believe that with regard to media reporting on Covid-19, my cynicism is well-deserved.
Covid-19 reporting has increasingly been utterly absurd, with stories of people dropping dead in the streets, ice rink morgues to cope with the mountains of bodies, footage of an overcrowded New York hospital (that just happened to be of an Italian hospital), claims of animals testing positive for SARS-CoV-2, and more recently reports of people dying post-jab but we are told ‘it could have been worse!’
This campaign of fear caused the public to massively overestimate the lethality of Covid-19, which as un-alarmist voices note has a survival rate of over 99%.
When months into the outbreak it became apparent that SARS-CoV-2 was far less lethal than first predicted, the media and talking heads moved from talking about ‘Covid deaths’ to ‘positive cases’.
Although relatively early on a goat and pawpaw tested positive for Covid-19, instead of then scrutinizing the accuracy of the PCR test as a means of ‘detecting Covid-19’, the media continued to hype the rise in Covid ‘cases’.
In lockstep, ‘Covid testing’ was increased dramatically using the PCR test (recently revoked by the CDC). This inevitably pumped up the number of ‘cases’, which mass media have in turn promoted non-stop, this in turn gave ammunition to those enforcing lockdowns and vaccines.
By now hundreds of vocal doctors, nurses, virologists, immunologists, and other professionals actually worth listening to, whose data and experience counter the hype pumped out in media have very quickly disappeared from social media, or otherwise deemed quacks, and are thus largely silenced. This leaves the general public mainly getting their information via hyped-up media.
Alongside this, there have been relentless ad hominem attacks on journalists who pose legitimate questions and uncomfortable truths about the official narratives around Covid-19.
For offering perspectives which contradict the standard narratives around Covid-19, journalists have been deemed conspiracy theorists, pandemic-deniers, right-wingers, selfish… I’m sure I’ve missed quite a few slurs.
When it comes to matters Covid-19, it is suddenly unacceptable to question ‘The Science’, question the authorities, or question the same media that sold us WMDs in Iraq and chemical attacks in Syria.
Media are the drivers of Covid hysteria, and it is the daily bombardment of fear porn that confuses average people and enables tyrannical powers to be brought in, largely unchallenged.
As it is the responsibility of journalists to expose lies around wars of aggression, it is also the duty of journalists to do so around Covid-19. For some journalists who have stubbornly refused to hold power to account, instead toeing the line on all things Covid, it appears their fear is of losing an audience and not of a virus.
Whether or not you agree with dissenting voices’ questions and criticisms, we have the right to ask and make them. We do so, knowing that remaining silent in the face of the brutal Covid measures is a guaranteed path to tyranny.
Eva Bartlett is a Canadian independent journalist and activist. She has spent years on the ground covering conflict zones in the Middle East, especially in Syria and Palestine (where she lived for nearly four years).
A huge amount of opprobrium was heaped on the Americans for allowing this sensitive data to fall ‘into the wrong hands’. However, surely a better question is why had they gathered all this deeply personal data in the first place?
It’s been reported that the Taliban has seized US military biometric devices in the wake of Washington’s flight from Afghanistan, which could put civilians who assisted coalition forces at significant risk.
The devices, known as HIIDE, for Handheld Interagency Identity Detection Equipment, contain identifying biometric data such as iris scans and fingerprints, as well as biographical information – while their primary stated purpose is to track insurgents, biometric data was also collected and stored on Afghans who assisted the US occupation forces.
The story sparked outcry, widely invoked by both opponents and advocates of the 20-year war as yet another deplorable example of Washington leaving its allies high and dry. While it seems clear there was no consideration given to what could happen if the technology fell into the ‘wrong’ hands, critics have nonetheless overwhelmingly failed to consider the terrifying ramifications of this data being in the right hands, and how the US came into possession of it in the first place.
When precisely the practice of collecting Afghans’ biometric data began isn’t certain, although at a 2010 conference in Kabul, US military officials laid out the terms of Afghan 1,000, a program which sought to collate information on 80% of the country’s population, around 25 million people. It was framed in extremely positive terms, not merely as a means to identify terrorists and criminals, but “enable progress in society” due to its “countless applications for the provision of services” to citizens.
It’s uncertain if that target was reached before Washington’s withdrawal, but the strategy remained in operation for over a decade. The next year, it was reported that Washington ultimately sought to gather biometric data on all living Afghans.
To achieve the lofty goal, a policy of mandatory data collection was imposed for every traveler entering the country via any means, and a dedicated Population Registration Department was created, with offices throughout the country. Even foreign journalists covering the war were fingerprinted, and their irises scanned. Moreover, occupation forces conducted innumerable “enrolment missions”, entering towns and villages and forcing locals to hand over their biometric data at literal gunpoint.
A US Army guide states emphatically that “all combat outposts and checkpoints throughout Afghanistan make it a priority to collect biometric data from as many local nationals as possible.” In the aftermath of a bombing or skirmish, soldiers are told to “enroll everyone”, including the dead, their DNA to be collected using buccal swabs to capture cells lining the mouth. The “payoff” for coalition forces was said to be so great, “commanders must be creative and persistent in their efforts to enroll as many Afghans as possible.”
In a section disturbingly titled “Population Management”, the guide recommends that everyone who lives within an operational area “should be identified and fully biometrically enrolled with facial photos, iris scans, and all ten fingerprints (if present).” Soldiers must also record “good contextual data” about individuals, such as “where they live, what they do, and to which tribe or clan they belong.” Citizens were to be told the collection protected them from potentially violent elements and troublemakers.
A lengthy article in the January 2014 edition of Military journal Joint Forces Quarterly offers a glowing appraisal of the “biometric-enabled intelligence” system rolled out in Kabul, declaring it to be a “key enabling factor” in US counterinsurgency efforts, and “an invaluable part of the campaign that has even greater potential in the future.” It documents how enrolment was often carried out using colorful trucks with jingling bells, in the manner of an ice cream van, in order to make the process “more culturally appealing” – particularly in respect of children, presumably.
Also included are several alleged “success stories”, such as one instance in which two Afghan police officers, neither of whom could read or write, spotted an individual on a “biometrically developed insurgent watch list” approaching their checkpoint.
One of the officers is said to have taken the man – identified as having been involved in “multiple IED events” – into custody “with a broad smile,” and the anecdote ends on an upbeat note, hailing how the officers’ illiteracy was no barrier to them removing a dangerous insurgent from the battlefield due to the miracle of biometric intelligence. Cheery stuff, although journalist Annie Jacobsen has exposed in chilling detail just how fallible biometric evidence can be.
In July 2012, US Army First Lieutenant Clint Lorance ordered his platoon to shoot three unarmed motorcycle riders in Kandahar province. The next year, a court martial found him guilty of two counts of second-degree murder, attempted murder, wrongfully communicating a threat, reckless endangerment, soliciting a false statement, and obstructing justice, sentencing him to 20 years in prison. However, in November 2019, he received a pardon from Donald Trump.
The then-president released Lorance after he was shown fingerprints and DNA data that purportedly indicated the Afghan men killed were Taliban bomb makers, not civilians. However, after some determined digging, Jacobsen found that one set of fingerprints allegedly found on an exploded IED said to prove one of the dead men was a bomber actually belonged to a police officer, who was likely to have contaminated the evidence in the line of duty. The other set did indeed belong to a bomber – who was still alive.
Lorance isn’t an isolated example either. Staff Sergeant Robert Bales is serving life for killing 16 Afghan villagers in cold blood in March 2012. While he pleaded guilty to the charges and admitted his tours of Afghanistan and Iraq had instilled a loathing of the local population within him, he’s now appealing his sentence. The case rests on data provided by a biometrics expert who also worked on the Lorance case, which he claims proves witnesses to Bales’ crimes were Taliban bomb makers who left their fingerprints on bomb components.
Evidently though, Afghanistan was just an experiment – and Washington was enamored with the results. The White House’s proposed Army budget for 2022 seeks over $11 million to purchase 95 new biometric collection devices, meaning the policy will almost inevitably be rolled out again in whichever country is next in the US crosshairs.
Where that will be is unknown, but there’s also the question of what implications the Afghan test run has for the Western world. Governments, police forces, security services and even big business are increasingly using cutting-edge technology to amass, store and analyze vast reams of sensitive personal data – much of it was similarly trialed during the War on Terror, and sold to home audiences on the basis of convenience and security, just as the military’s biometric data harvest was sold to Afghans. Now the troops are finally home, has the fight been brought back with them?
Kit Klarenberg is an investigative journalist exploring the role of intelligence services in shaping politics and perceptions.
Since invading Afghanistan in 2001, the United States has spent $2.313 trillion on the war, which includes operations in both Afghanistan and Pakistan. Note that this total does not include funds that the United States government is obligated to spend on lifetime care for American veterans of this war, nor does it include future interest payments on money borrowed to fund the war. This $2.313 trillion spent on Afghanistan is a portion of the total estimated cost of the post-9/11 wars.
The Costs of War Project also estimates that 241,000 people have died as a direct result of this war. These figures do not include deaths caused by disease, loss of access to food, water, infrastructure, and/or other indirect consequences of the war.
The figures for Afghanistan are part of the larger costs of the U.S. post-9/11 wars, which extend to Iraq, Syria, Yemen, Somalia and elsewhere. The numbers are approximations based on the reporting of several data sources.
For decades, true scientists have warned that pivotal clinical trial designs for vaccines are dangerously flawed and outdated [1]. Vaccines have been promoted and widely utilized under the false claim they have been shown to improve health.
However, this claim is only a philosophical argument and not science based. In a true scientific fashion to show a health benefit one would need to show fewer overall deaths during an extended period in the vaccinated group compared to a control group.
Less stringent indicators of a health benefit would include fewer severe events of all kinds, fewer days hospitalized for any reason, lower heath care expenses of all types, fewer missed days from work for any health reason. No pivotal clinical trial for a vaccine preventing an infectious disease has ever demonstrated an improvement in health using these scientific measurements of health as a primary endpoint.
Instead, vaccine clinical trials have relied on misleading surrogate endpoints of health such as infection rates with a specific infectious agent. Manufactures and government agents have made the scientifically disproved and dangerous philosophical argument that these surrogate endpoints equate to a health benefit.
True medical scientists, outside the vaccine fields, have embraced the use of true health measurements as the proven proper scientific endpoint of clinical trials. Decades ago, a pharmaceutical manufacturer would only need to show that a chemotherapeutic agent shrank a tumor or reduces cancer deaths to obtain FDA approval. Manufacturers would market their products under the fraudulent philosophical argument that shrinking tumors or reducing cancer deaths equates to improved survival.
However, many of the toxic chemotherapeutic agents would destroy vital organs and actually reduce survival while decreasing cancer deaths at the same time. The FDA and comparable agencies around the world switched to “all cause mortality” as the primary endpoint for pivotal cancer drug trails. The gold standard for marketing approval is to show that those receiving a cancer drug actually live longer than those who do not.
Typically, new “miracle” anticancer drugs only prolong survival about 2 months but this added time may be spent severely ill suffering from adverse events caused by the chemotherapy. Application of true scientific principles often severely deflates the hype promoting pharmaceutical products.
All previous vaccine trials have suffered not only from lacking a proper primary clinical endpoint but also from insufficient perspective follow up of adverse events. The trials have failed to account for the well-established toxicity data and epidemiology data that vaccines are associated with chronic immune mediated disorders that may not develop for years after immunization.
These adverse events, for example type 1 diabetes, are quite common, develop 3 or more years after immunization, and can exceed the reduction in infectious complications induced by the vaccine as was shown with a hemophilus vaccine [1]. Pivotal trials for the recombinant hepatitis B vaccine prospectively recorded adverse events for about 7 days after immunization and newer vaccines typically prospectively follow patients 6 months for adverse events.
Method Data from all three US COVID-19 vaccines was published in the New England Journal of Medicine [4-6]. Data from these three publications and the accompanying published appendixes provided the bulk of the information analyzed. On rare occasions supplemental data was found on the FDA’s website (https://www.fda.gov/advisory-committees/advisory-committee-calendar) in briefing documents pertaining to FDA advisory panel committees for COVID-19 vaccines from Pfizer-BioNTech, Moderna, and Janssen.
The scientific primary endpoint, “all severe events”, in the treatment group and controls was calculated by adding all severe or life threatening events reported in the clinical trials by the manufacturers. Severe events included both severe cases of COVID-19 and all other severe events in the treatment arm and control arm respectively.
A Chi square analysis using a 2×2 table was used to calculate statistical p values. An online statistical chi square calculatorwas used. Statistical calculations ignored small differences in total subject number between efficacy and adverse event populations. The randomized number, shown in Table 1, was used as the study population for statistical calculations.
In general, the population for adverse events was slightly higher than that for efficacy. Given the statistical significant p, values generated (see Table 1), these small differences do not appear to be material. The FDA document entitled Guidance for Industry Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials, 2007, provided the following definitions for adverse events.
Grades 3, Severe: Prevents daily activity and requires medical intervention.
Grades 4, Potentially life threatening: ER visit or hospitalization.
Results
Moderna The Moderna pivotal Phase III trial results and protocol are published in the New England Journal of Medicine (NEJM) [5].The primary endpoint was COVID-19 illness starting 14 days after the second dose of vaccine however the trial had a secondary endpoint which was patients developing severe COVID-19 symptoms. This later endpoint allowed for a direct comparison to severe adverse events.
The study randomized 30,420 individuals, 15,210 were randomized to receive injections with Moderna’s mRNA-1273 vaccine and 15,210 were randomized to receive injections with placebo. Two shots were administered 28 days apart. “Solicited” adverse events were collected 7 days after immunization and “unsolicited” adverse events were reported up to 28 days after administration of each vaccine or approximately 56 days after the first dose according to protocol.
Because of dropouts, adverse events were recorded on 15,185 vaccinated patients and 15,166 placebo patients (reference 5, appendix table S8). The treatment group had 11 cases of symptomatic COVID-19 infections and 0 cases severe COVID-19 infections (reference 5, appendix table S13). There were 234 cases of severe “unsolicited” adverse events in the treatment group (reference 5, appendix table S8), and an additional 3,751 “solicited” severe or life threatening (Grade 3 or Grade 4) adverse events (reference 5, appendix table S3 and S4).
By contrast, the control group had 185 cases of symptomatic COVID-19 infections and 30 cases of severe COVID-19 infections. However, only one of these case of COVID-19 out of 15,166 controls required admission to an intensive care unit (see reference 5, appendix table S13). There were 202 cases of severe “unsolicited” adverse events in the placebo group and an additional 711 “solicited” severe or life threatening (Grade 3 or Grade 4) adverse events.
There were 3 deaths in the placebo groupand 2 in the vaccinated group (reference 5, appendix table S8).
Pfizer-BioNTech The Pfizer-BioNTech (Pfizer) pivotal Phase III trial results are published in the New England Journal of Medicine [6].The Pfizer trial was classified as a Phase 1/2/3 trial. Two shots were administered 21 days apart. The primary endpoint was confirmed COVID-19 infections 7 days after the second dose. A post hoc analysis of severe COVID-19 infections was included in the appendix published by the NEJM. The study randomized 43,548 individuals of which 100 did not receive injections, 21,720 received injections with the vaccine and 21,728 received injections with placebo.
“Solicited” adverse events were collected 7 days after immunization and “unsolicited” severe adverse events were reported up to 14 weeks after administration of the second dose. However, median safety follow up for “unsolicited” events was only approximately 2 months after the second dose at the time of publication in the NEJM. In the treatment arm there was 1 case of severe Covid-19 (reference 6, appendix table S5), 240 “unsolicited” severe adverse events and 21 “unsolicited” life threatening adverse events (reference 6, appendix table S3).
In the placebo arm, there were 9 cases of severe COVID-19, 139 “unsolicited” severe adverse events and 24 “unsolicited” life threatening adverse events. Pfizer used a safety subset of approximately 8,183 (both vaccinated and unvaccinated) to record “solicited” adverse events at 7 days. These data that are not shown in Table 1 in part because the data was depicted graphically in the NEJM manuscript.
Janssen The Janssen pivotal Phase III trial design and trial results are published in the New England Journal of Medicine [4].The primary endpoint was prevention of molecularly confirmed, moderate to severe–critical COVID-19 14 days post vaccination however a secondary endpoint was prevention of molecularly confirmed, severe–critical COVID-19 14 days post vaccination. This later endpoint allowed for a direct comparison to severe adverse events.
The study randomized 19,630 to receive a single injection with Janssen’s adenovirus COVID-19 vaccine and randomized 19,691 to receive a single injection with placebo. “Solicited” adverse events were collected 7 days after immunization and “unsolicited” adverse events were reported up to 28 days after administration of the single dose of vaccine. The treatment group had 21 cases of severe or critical COVID-19 infections while the placebo control group had 78 (reference 4, appendix table S9).
Further analysis shows that only 2 of 19,514 immunized patients needed medical intervention for COVID-19 infections starting 14 days after immunization, while only 8 of 19,544 controls needed medical intervention for COVID-19 infections starting 14 days after placebo injection where the COVID-19 infection was confirmed by a central lab (reference 4, appendix table S10).
There were 83 “unsolicited” and approximately 492 “solicited” serious adverse events in the vaccinated group compared to 96 “unsolicited” and approximately 157 “solicited” serious adverse events in the control group (reference 4, appendix table S7). There were 3 deaths in the treatment group and 16 in the control group (reference 4, appendix table S7).
Discussion
Scientific analysis of the data from pivotal clinical trials for US COVID-19 vaccines indicates the vaccines fail to show any health benefit and in fact, all the vaccines cause a decline in health in the immunized groups. Health is the sum of all medical events or lack there of. COVID-19 vaccines are promoted as improving health while in fact there is no evidence that these vaccines actual improve health in the individual or population as a whole.
The current analysis used the proper scientific endpoint of “all cause severe morbidity”, a true measure of health. By contrast, manufactures and government officials promote the vaccines using a surrogate measure of health, severe infections with COVID-19, and the disproved philosophical argument that this surrogate endpoint equates to health. This substitution of philosophy for science is extremely dangerous and is certainly leading to a catastrophic public health event.
Review of data from the three COVID-19 vaccines marketed in the US shows complete lack of a health benefit and even an increase in severe events among vaccine recipients. The proper scientific clinical trial endpoint, “all cause severe morbidity” was created by combing all severe and or life threatening events, both infectious and non-infectious, occurring in the vaccinated and placebo control groups respectively.
The data (Table 1) shows there are clearly more severe events in the vaccinated groups. The results are highly statistically significant. The use of a true scientific measure of health as an endpoint for a vaccine trial gives a contrasting result compared to the use of a non-scientific surrogate endpoint of heath, severe infections with COVID-19.
There is an old saying, fool me once shame on you, fool me twice shame on me. This saying can be applied to the COVID-19 mass immunization program. The US anthrax attack of 2001, which originated at US army is Fort Detrick, has demonstrated that there are people in the US government who desire to attack US citizens with bioweapons [10].
According to the chief FBI agent leading the investigation of the US anthrax attack, conspirators were likely not apprehended in part because the investigation was prematurely ended and prior to stopping the investigation, people at the top of the FBI deliberately tried to sabotage the investigation [11]. In the US anthrax attack of 2001, people high in the US government publicly anticipated the anthrax attack as early as 1999 [10].
Similarly with the COVID-19 attack, people high in government anticipated the COVID-19 attack [12,13] several years before the attack took place [10]. There is even data that an effort was made in 2018 to protect certain populations against COVID-19 by immunizing them with MMR vaccine [14].In such a hostile government environment, the citizens need to individually evaluate the science of immunization with COVID-19 vaccines and not rely on philosophical arguments propagated by government officials.
In this case there is no scientific evidence that the COVID-19 vaccines improve the health of the individual, much less of the population as a whole. Mass immunization with COVID-19 vaccines is certainly leading to a catastrophic public health event.
The Bottom Line
These Covid vaccines have been promoted and widely utilized under the false claim they have been shown to improve health, but the claim is only a philosophical argument and not science based, and in a mounting numnber of cases, these vaccines can be shown to be detrimental to your health.
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

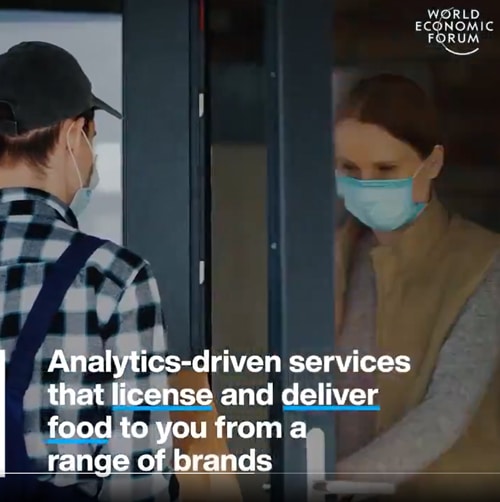


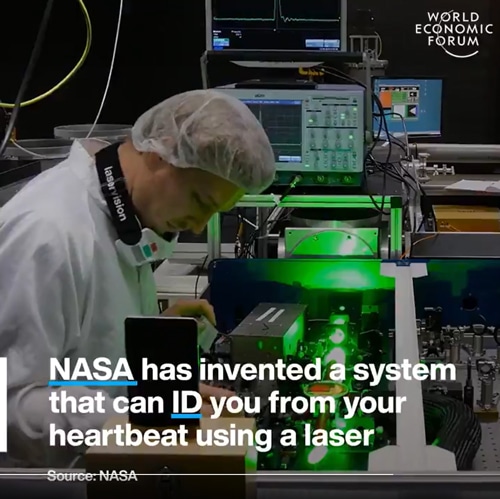
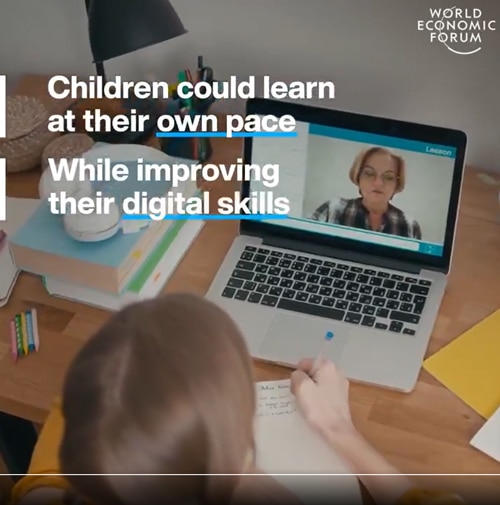



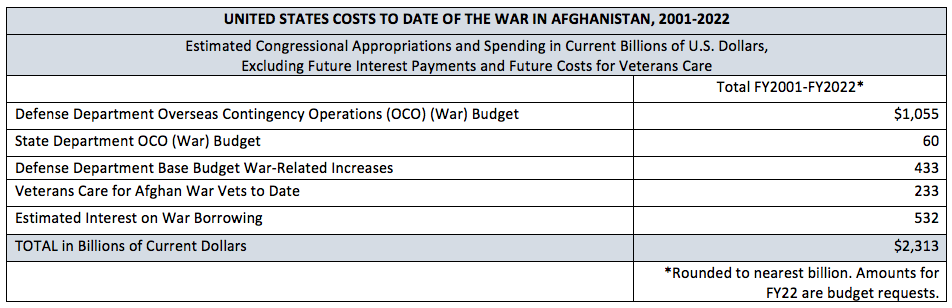
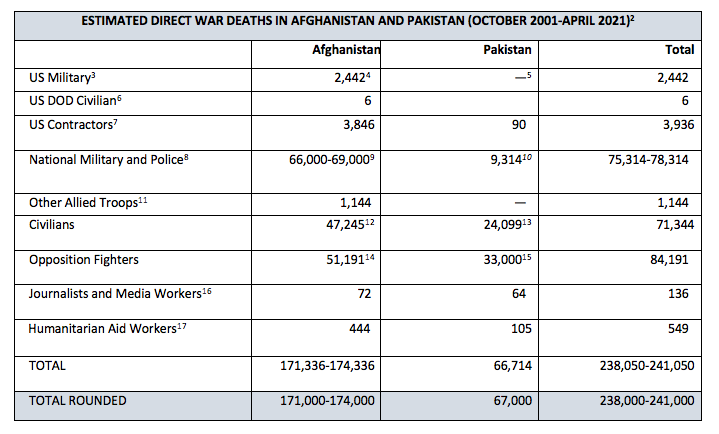

 Aletho News
Aletho News