Scientists are developing a proprietary “early warning system” — powered by CRISPR gene-editing technology — to “detect and characterize deadly pathogens” in Africa “before they spread across the globe,” STAT News reported.
The surveillance system — dubbed Sentinel — was launched with funding from the Bill & Melinda Gates Foundation and others. It uses “participatory” digital health tools developed with funding from the U.S. Department of Defense’s Defense Advanced Research Projects Agency, or DARPA.
Sabeti is a World Economic Forum Young Global Leader, Harvard professor and director of the Broad Institute’s Sabeti Lab. Happi is a professor of molecular biology and genomics at Redeemer’s University in Nigeria, an adjunct professor of immunology and infectious diseases at Harvard and director of the African Centre of Excellence for Genomics of Infectious Diseases (ACEGID), a genomic research institute focused on Africa, which he co-founded with Sabeti in Nigeria.
Sentinel aims to use rapid testing at “points-of-care” — anywhere tests can be administered, including non-clinical settings — across rural Africa to identify and genetically sequence pathogens. Then researchers will use cloud-based technology to share that information across the public health information sphere.
Global public health researchers can then track and predict “threats” and use that information to rapidly develop new diagnostics and vaccines — what the researchers call a “virtuous cycle,” according to a 2021 paper published in Viruses by the developers.
The Sentinel project was officially launched in 2020 with funding from TED’s Audacious Project, backed by Jeff Bezos’ ex-wife MacKenzie Scott, Open Philanthropy, the Skoll Foundation and the Gates Foundation.
But DARPA, the National Institutes of Health (NIH), the Wellcome Trust and others funded the development of the CRISPR technology the project will use to detect pathogenic threats.
“They fully intend to use synthetic biology to research, develop and test biological warfare weapons. That’s DARPA’s motivation for funding this.
“It fits in with Predict and its successor, also funded by USAID [U.S. Agency for International Development], which is a front organization for the CIA, to go out into the world and find every exotic disease, fungus, toxin, virus they possibly can and bring them back here and then weaponize them in their BSL3 [biosafety level 3] and BSL4 labs.”
According to Boyle, the Broad Institute is one of the country’s leading DARPA-funded synthetic biology research centers.
Happi and Sabeti officially launched Sentinel in West Africa one month before the World Health Organization declared COVID-19 a pandemic. By early February 2020, they were using it to deploy COVID-19 rapid testing and genomic sequencing in hospitals across Sierra Leone, Senegal and Nigeria — before anywhere in the U.S. was doing so, STAT reported.
“Experts” told STAT that Africa is a “hot spot for emerging infectious diseases” because the existing system of disease surveillance is too centralized and top-down.
Happi and Sabeti aim to change that, they said, by making disease surveillance “bottom-up” — getting “everyday Africans” and community frontline workers working as “sentinels” to surveil their friends and communities for diseases.
They said their project can change how disease surveillance works globally. “Everybody in the world should be a sentinel, a sentinel not only for his own immediate community, for his own country — but a sentinel for the globe,” said Happi.
‘Very wealthy people have figured out how they can get extremely rich from this’
The developers said the Sentinel program is needed because viruses can mutate at any time to become pandemic threats, and this system is designed to find them early.
Sabeti described the work in a video tweeted last year by Bill Gates.
Sentinel is designed to identify pathogens at the most localized level possible and then disperse diagnostic and genomic information as quickly as possible to public health officials and researchers designing treatments, vaccines and new tests.
Clinicians or others are meant to administer “point-of-care” tests that use CRISPR gene-editing technology, which turns gene editors into pathogen detectors through different techniques, some of which are still in development.
Sentinel’s first line of intervention is the SHINE (SHERLOCK and HUDSON Integration to Navigate Epidemics) diagnostic tool, easily administered at almost any location. It tests blood or urine samples and reveals the results on a piece of paper without any high-tech equipment.
Happi told STAT that administering the test is like “doing a PCR on a sheet of paper” and that it is so simple that his grandmother could do it in her village.
But SHINE — an improvement on Sabeti’s earlier Specific High-sensitivity Enzymatic Reporter UnLOCKing, or SHERLOCK test — can test for only one pathogen at a time.
If that test fails to detect anything, Sentinel researchers launch their next-level test, CARMEN (Combinatorial Arrayed Reactions for Multiplexed Evaluation of Nucleic acids), which can screen for up to 16 pathogens at a time and must be implemented at a nearby rural hospital.
Research on the CARMEN technique was funded by DARPA, NIH, and Wellcome and published in Nature in 2020.
If CARMEN fails, the sample is “escalated” to a regional genomics hub, where every virus in the sample, “known or unknown,” is sequenced.
Researchers can use those sequences to quickly make new diagnostic tests for the newly identified pathogens, STAT reported.
The data collected through Sentinel is shared across healthcare clinics and public health officials’ proprietary mobile apps and cloud-based reporting systems developed by Dimagi — a Gates Foundation-funded for-profit tech company that targets low-income communities — and Fathom — a for-profit software developer funded by Sabeti labs.
Sabeti filed patents for the technology and co-founded a biotech startup, Sherlock Biosciences, to commercialize these tests for use in the U.S.
Sherlock also has startup funding from the Gates Foundation, Open Philanthropy and a number of other biotech venture capitalist companies.
With funding from DARPA, Battelle National Biodefense Institute, the U.S. Department of Homeland Security, the NIH and others, the Broad Institute and Princeton University researchers also used SHINE to create a rapid test for COVID-19.
Sabeti sits on the board and serves as a shareholder of the Danaher corporation, which develops research tools determining the causes of disease and identifies new therapies and tests of drugs and vaccines.
Happi also collaborates with the Rockefeller Foundation’s Pandemic Prevention Institute and bioengineering firm Ginkgo Bioworks to deploy Ginko’s automation technologies to his lab to sequence genomes.
But Sabeti told STAT that providing people with access to testing is her true priority. And she is on the board of a nonprofit that will work to send the tests her new company makes to low- and middle-income countries “at cost.”
Sentinel’s real contribution, Sabeti said, is its focus on “empowerment.”
Sabeti and Happi are currently field testing SHINE and CARMEN. In the process, they are training scientists in genomic surveillance and collecting hundreds of thousands of genomes.
STAT didn’t specify whether those are virus genomes or people’s genomes, but Boyle said the testing would make it possible to also collect the genomes of African people, which he said is a form of biopiracy.
Other notable collaborators on the 2021 Viruses paper that helped publicly launch Sentinel include Scripps Research Institute virologist Kristian Andersen, Ph.D., co-author of the now infamous Nature “Proximal Origins” paper used to promote the theory that COVID-19 evolved in nature. Andersen’s private communications later revealed he suspected a segment of the SARS-CoV-2 genome may have been engineered in a lab.
Examples of conflicts of interest among the Virus paper’s co-authors also include Anthony Philippakis, M.D., Ph.D., a venture partner at Google Ventures; Jonathan Jackson, CEO of Dimagi; and Robert Garry, Ph.D., Matthew L. Boisen, Ph.D., and Luis M. Branco, Ph.D., who all work for Zalgen Labs, a “biotechnology company developing countermeasures to emerging viruses.”
Garry also co-authored the “Proximal Origins” paper.
Dr. David Bell, a public health physician and biotech consultant in global health, told The Defender the Sentinel program reflected a broader problem with global public health priorities.
“Public health has become a for-profit industry that’s very, very lucrative,” Bell said. As a result, the field no longer works to provide people with better economies, sanitation, nutrition, access to basic medicines and research on major endemic infectious diseases, such as tuberculosis and malaria.
Instead, research funding is diverted to “pandemic preparedness,” diseases that kill relatively few people.
Bell said:
“We’ve got to a point where very wealthy people have figured out how they can get extremely rich from this and they have enough money to completely control the agenda. So now they essentially control the agenda of global health.
“So you don’t hear much about sanitation and nutrition any more because that’s not where the people who are running the agenda can make their money.”
What they’re doing is not “intrinsically bad,” Bell said. “The question is whether it is proportionate to the need or is it a diversion of resources that in doing so will cause a net harm? And that’s a question that people won’t talk about.”
Sabeti, Happi and Broad Institute at forefront of viral hemorrhagic research in Africa for years
Sabeti, Happi and the Broad Institute have also been at the forefront of viral hemorrhagic fever research in Africa, including Lassa virus and Ebola.
Andersen, Garry, Sabeti and Happi all serve on the board of the Viral Hemorrhagic Fever Consortium (VHFC), founded in 2010 with funding from the NIH, the National Institute of Allergy and Infectious Diseases (NIAID) and Tulane University.
Sabeti and Happi began working together in 2008, studying the virus that causes a viral hemorrhagic fever known as Lassa fever, which infects hundreds of thousands — most of whom recover — and kills about 5,000 people globally per year, according to recent estimates. Lassa fever is considered a category A (most dangerous) bioterror threat.
The Viruses paper provides an account of Sabeti and Happi’s work on Lassa. By mapping human genomic variation in West Africa, they found the Lassa virus existed for half a millennia there, but had gone undetected because people had developed genetic resistance to it.
And many people with Lassa were being misdiagnosed because they had nonspecific symptoms.
This work led them to an epiphany moment — “the realization that in many parts of the world, we are largely blind both to the prevalence of known infectious diseases and to the appearance of new threats,” the paper said.
By developing better diagnostic tools for local healthcare workers, the paper concluded, diseases can be detected and better treatments and vaccines and then even better diagnostic tools can be created, “instead of awaiting the next outbreak.”
Lassa virus is a BSL4 pathogen, the paper notes — although in West Africa it is studied at a research facility without that safety level — and it makes a plug for BSL4 research in Africa.
“With increased globalization and an ever-expanding human population, the need for large-scale research initiatives on BSL-4 pathogens remains acute,” it says.
“Further, as only one BSL-4 lab exists in the entire region of West Africa … even today, transnational partnerships are critical to allow ongoing investigation of BSL-4 pathogen samples.”
Their work on Lassa led the researchers to begin developing a broader surveillance model and then to establish ACEGID at Redeemer University with support from Tulane, the NIH and the World Bank.
ACEGID then, according to the article, played a key role during the 2014 Ebola outbreak in West Africa, which happened just as ACEGID was launched in March of that year.
Happi’s team identified the first case of Ebola in Nigeria and sequenced the genome of the Ebola virus in 2014, it said.
The mainstream press reported that the 2014 Ebola outbreak — which claimed 11,000 lives in West Africa — came from a two-year-old boy in Guinea playing in a bat-infested tree stump.
But U.S. Right to Know reported that independent evidence and phylogenetic analysis cast doubt on that narrative.
Chernoh Bah, an independent journalist and historian from Sierra Leone, reported errors in the established narrative identified through his interviews.
Research by investigative journalist Sam Husseini and virologist Jonathan Latham, Ph.D., built on Bah’s research and pointed to a leak at the U.S. government-supported research laboratory in Kenema, Sierra Leone, where the VHFC was doing research on Ebola and Lassa.
An article co-authored by VHFC’s Sabeti, Happi, Andersen and dozens of others published in Science argued that the Ebola outbreak had a zoonotic origin in Central Africa.
Happi’s lab also sequenced the Lassa virus in a 2018 outbreak.
According to an article in Nature, Happi’s sequencing also provided evidence that the Lassa outbreak had a zoonotic origin, rather than being from a mutation that made the disease more transmissible.
The Viruses paper said the success of ACEGID in addressing the Ebola crisis, along with its work on Lassa, laid the groundwork for Sentinel, launched just a few months before the COVID-19 pandemic.
Given that history, Boyle said:
“I wouldn’t trust anything Sabeti’s doing. And I’d be very skeptical of any claims that are being made [about Sentinel] given the involvement of DARPA, the involvement of Broad and Broad’s previous involvement at that Kenema lab with the outbreak of the Ebola pandemic.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
The Kremlin reported that Ukrainian drones were downed in the Moscow region for a sixth consecutive day. Kiev has launched a series of attacks on Russia as it has failed to retake territory during its Spring counteroffensive.
The Kremlin reports that it downed three Ukrainian drones targeting Moscow on Wednesday. TASS, Russian state media, said that no one in the Moscow region was killed or injured. One building, currently being constructed, was hit by a drone after it was disabled by Russian electronic warfare systems.
“The glazing of the Neva Tower in the Moscow City district was damaged on the 11th, 12th and 13th floors on an area of about 100 square meters after the crash of the downed drone,” TASS reported.
The drones have caused Moscow to shut down traffic at its airports for short windows for three straight days.
Additionally, Ukraine attacked the Belgorod region of Russia, killing three. Belgorod’s governor said a drone was used in the attack. Several Russian civilians have been killed by Ukrainian fire in Belgorod since Kiev decided it would begin targeting Russia.
Earlier this month, Ukrainian President Volodymyr Zelensky announced Kiev would increase strikes on Russia. “Gradually, the war is returning to the territory of Russia — to its symbolic centers and military bases,” he said. “And this is an inevitable, natural and absolutely fair process.”
In the months after Russia invaded Ukraine, the White House sought assurances from Kiev that it would not use American weapons to target Russia. However, officials in the Joe Biden administration appear to be less concerned the attacks will risk escalation with Moscow. American weapons have been documented to be used in cross-border raids conducted by Kiev-backed neo-Nazi militias.
In the past, Moscow has said that the Ukrainian attacks on Russia would not be possible without US support. “These attacks would not be possible without the help provided to the Kyiv regime by the US and its NATO allies,” the Russian foreign ministry said. The West is “training drone operators and providing the necessary intelligence to commit such crimes.”
The Kremlin has warned it will take harsh measures in response to the attacks on Moscow. “We regard what happened as yet another use of terrorist methods and intimidation of the civilian population by the military and political leadership of Ukraine,” the Foreign Ministry explained. “The Russian Federation reserves the right to take tough retaliatory measures.”
Russia’s top diplomat, Sergei Lavrov, recently said the greatest danger posed by the war in Ukraine is a direct conflict between Moscow and NATO breaking out. The Russian Foreign Minister said the war would lead to nuclear weapons being used.
I was honored to present to PANDA earlier this summer regarding my ongoing independent study of New York City’s spring 2020 mass-casualty event. Content is similar to what I shared with Jonathan Couey in our conversation a few weeks ago. – Jessica Hockett
New York City’s spring 2020 mass-casualty event is a global and domestic outlier that warrants closer scrutiny. How do common explanations for a weekly death rate that peaked at 600% above normal hold up against daily events and data points? In this two-part presentation, Dr. Jessica Hockett shares aspects of her hypothesis in progress about what happened – and what it suggests about whether the New York mortality experience is evidence that a global viral pandemic occurred. Content includes data Dr. Hockett has obtained via public records requests, as well as already-public datasets that media and researchers overlook.
Dr. Hockett has a PhD in educational psychology from the University of Virginia. For over 20 years, she worked in and with schools and agencies in the U.S., Canada, and South America, to improve curriculum, instruction, and programmes. Her publications include numerous articles related to the education field, as well as three books: Exam Schools: Inside America’s Most Selective Public High Schools, Differentiation in Middle and High School: Strategies to Engage All Learners Differentiation in the Elementary Grades: Strategies to Engage & Equip All Learners. Jessica’s current work involves policy research and analysis for the National Opportunity Project, a government watchdog and education nonprofit. Her paper on the implementation of federal Covid relief funds for nonpublic schools was released this spring https://www.nationalopportunity.org/eans-funding-report/ A forthcoming paper focuses on politically/ideologically-biased teacher-hiring practices in K12 public schools.
In the Covid-response era, Jessica used her Twitter account and Substack to push against mandates and for common sense. She leveraged her research skills and investigative tenacity to obtain public records, communicate directly with government officials, and gather data that uncovered illegalities and inefficacies of harmful orders and policies. Highlights of her research was exposing the University of Illinois’ false claims to FDA EUA for its Covid saliva test; assisting with a lawsuit against Chicago’s vaccine passport; testifying as a data analyst in a vaccine mandate arbitration case; helping lead the fight for mask choice in schools and churches; homeschooling her two children in 2020-21; and being censored by and banned for almost six months from Twitter.
In an interview with The Defender, Constantine’s son, Andy Kotsanis, said that in the 1980s, his father helped transform what was previously the Grapevine Medical Center into the Baylor Scott & White Medical Center — Grapevine, affiliated with Baylor University. It is now the largest not-for-profit health system in Texas.
It was in that same hospital, that on March 14, 2021, Constantine “violently lost his life,” his son said — days after being admitted with respiratory problems and a subsequent COVID-19 diagnosis.
Andy said he believes his father’s death resulted from the treatment he received, including remdesivir, fentanyl and other drugs Constantine and his family had not authorized.
Andy also alleges he was “threatened and assaulted by the police and the hospital administrator” as his father was dying, and barred from the room as his father passed away.
Today, Andy is raising awareness about his father’s death — and the stories of others who endured similar treatment — through his own activism and as a social media outreach coordinator for the FormerFedsGroup Freedom Foundation.
Andy discussed his family’s experience around his father’s hospitalization and subsequent death at Baylor Scott & White, and the activism he is now involved in as a result. He shared extensive documentation and photos with The Defender to corroborate his story.
Hospital president to victim’s family: ‘I’m not letting you see him’
Andy told The Defender that he was the very first baby born at Baylor Scott & White’s then-new outpatient operating room. Just days earlier, his father “was the first physician to do a procedure in that operating room,” he said. “So, there’s a very long history with my father and Baylor.”
“This is a story of tragedy, but also betrayal, because he helped build that place,” Andy said.
According to Andy, his father was not vaccinated for COVID-19. “He was not a fan of it,” he said. He said he now believes his father’s vaccination status may have played a crucial role in the treatment he received in the hospital.
After hearing about Gail Seiler’s story, Andy said, “Maybe they played that same game with him and did not tell the truth completely to us,” he said.
Andy said his father spent “a little over six days” in the hospital. He was admitted when “he had a hard time breathing. … He was really struggling, [in] a great state of hypoxia, almost to the point where he was exhausted with breathing.”
At the hospital, his father tested positive for COVID-19 and was admitted. According to Andy, the pulmonologist assigned to his father, Dr. Jagadeshwar Gummi Reddy, administered four rounds of remdesivir daily.
“At first, my father was calling me, saying ‘I feel a little bit better, everything’s fine,’” Andy said. “Then things started to go downhill very quickly. … I didn’t understand at the time what remdesivir was, how powerful it was and what it did to people or how deadly it was.”
A few days later, another phone call came from the hospital, this time from nurse Sarah Grice, who told Andy’s mother, “I had to put your husband in restraints, because he was confused about why he had tubes in his lungs.”
After his father’s death, Andy discovered that hospital medical records claimed no restraints were used.
“At the time, I didn’t know that there’s a formula that they follow: They sedate you and they’ll put you in restraints if they have to put remdesivir in you,” Andy said. “We requested to speak to the hospital administrator, Chris York, president of Baylor Grapevine at the time.”
According to Andy, York “arrogantly” told them, “‘I don’t care who your dad was or who your husband was, I’m not letting you see him.’ I said, ‘I think this is criminal. You’re not letting me see my dad. I don’t know what’s going on. Please let me see my father.’”
But York told them, “If you think it’s a crime, call the police,” according to Andy, who said, “I’ll never forget that sentence for the rest of my life.”
Nurse ‘started performing the most violent chest compressions I’ve ever seen’
Grice called the family again, telling Andy’s mother, “Your husband said he wants to die and be put on a ventilator.” This sounded nothing like my dad, Andy said, “because all over his chart, it says he didn’t want to be intubated. No ventilator, no remdesivir.”
“So how do you go from ‘No, I don’t want to be on a ventilator’ to ‘I want to die, put me on the ventilator’ in a matter of less than six days?” Andy asked.
On what turned out to be the day before his father’s death, Andy, his mother and their attorney “barged in the front door … demanding to see my father,” Andy said. “We were ready to press charges if they didn’t let us in.”
Subsequently, York “made the decision to only let my mother in,” Andy said, while Reddy spoke to him in person. According to Andy, this discussion was peculiar.
“He came downstairs with his mask off, with his hands shaking like he was scared, like someone was after him,” Andy said. “He introduced himself [and said] ‘My hands are tied. There’s nothing I can do.’ I said, ‘That’s not a good answer, sir,’ and he just walked away. It was almost like he was being bullied.”
Reluctantly, Andy’s mother approved the use of the ventilator that day, Andy said. But at 5 a.m. the next morning, the hospital called to say his dad was coding.
Again, only one family member was allowed into Andy’s father’s hospital room, so the family decided to let Katerina, his sister, be that person.
Expecting “some humane treatment,” Andy said they were instead met at the front door by Donna, an older nurse, and Demorrius Jones, a policeman, who “arrogantly greeted us in a very rude way.”
According to Andy, they got York on the phone, who said, “No one can go into the room. You have to watch him die through the glass.”
Andy told The Defender that, through the glass, they saw nurse practitioner Rommel Villas Lantajo handing a syringe to Grice, who then injected Constantine.
“Before she injected him, I saw the heart monitor,” Andy said. “He had a pulse of 122. So, I’m thinking to myself ‘Why is he coding? He has a heartbeat.’”
After the injection, “his pulse started to drop rapidly, and she [the nurse] started to do the most violent chest compressions I’ve ever seen,” Andy said.
“His body was bouncing 10 inches off the table. It was like watching someone get chainsawed in half. It was very violent and brutal, and looked more like she was trying to kill him, not save his life,” Andy said.
Andy said his father’s health was “already compromised with all those drugs they gave him” in the preceding day, which included fentanyl, adding that “he was still on the ventilator when she [Grice] was doing what she was doing.”
Grice subsequently stopped administering chest compressions and, according to Andy’s mother, “turned off all the machines.” Immediately following this, “My dad lifted his chest off the table, and then he had a seizure and died in front of my mother” while she was screaming “Stop, stop, stop!”
Andy was not present as his father died, though, because the police officer had “forced me out of the ICU. He threatened to arrest me if I didn’t leave the hospital immediately.”
Father’s death ‘malicious and arbitrary’
“They did this to a very kind, gentle soul,” Andy said, adding that his father’s death was “malicious and arbitrary, on behalf of Chris York, the administrator.”
“I’m still in shock,” Andy said, telling The Defender :
“The aftermath was so bad. I’m still in therapy over it. I’m very sad. I can’t put into words what a panic attack is like. I didn’t have irritable bowel syndrome until my dad died. You only get that when you experience something traumatic. Some people consider that a form of PTSD [post-traumatic stress disorder].”
“I’ve had several panic attacks,” Andy added. “I’ve lost count.” He said he’s “almost had to institutionalize” his mom. “I put my whole life on hold and I’m still, to this day, at her aid, trying to help her. She’s still not the same,” he said.
Andy also noted the anomaly of an extraordinary number of pages — many of them duplicates — in his father’s medical charts. “You’re in the hospital for six days but the chart is 948 pages long?” he asked. Another anomalous document dealt with “permission to be filmed,” he said, calling it “a very suspicious document.”
‘This is a huge cover-up’
His father’s experience led Andy to become an activist, he said.
“I’m trying to promote my story on my website and to inform everyone, the whole planet, that we’re witnessing the collapse of the healthcare system. … They’re using drugs in hospitals that are clearly not working,” he said. “I’m trying to show people that this is what they did to me. This is what they probably plan to do to you if you’re in there.”
“If that’s how you want to say goodbye to a loved one, go to Baylor Scott & White,” Andy said. “They’ll be more than happy to accommodate you if that’s your desire. That’s how I feel about this organization.”
“Hopefully, in the future, this can be a reference point for people to go, ‘We don’t want to be like Baylor, don’t pull a Baylor, don’t be like Baylor.’ That’s where I’m going with this,” Andy said. “This was so vicious and atrocious. I’ll never forget it.”
Aside from his website, Andy’s activism has included “putting road signs out, [placing] cards on doors,” he said, adding that such acts are “perfectly legal in the state of Texas” due to the Texas Citizens’ Participation Act.
However, just weeks after Andy began these activities, he was warned by local police and a local detective to “be careful” where he placed his signs and cards because his “First Amendment rights are limited.”
Andy said he experienced more difficulty with police when he attempted to press manslaughter charges against Baylor Scott & White. Local police referred him to Baylor Police and the Texas Rangers. When Andy contacted the Rangers, they advised him to “start a paper trail” by calling Baylor Police.
Yet, Baylor Police refused to take a report, telling him to “call our legal department.”
“So, this is a huge cover-up,” Andy told The Defender. “The police are covering up, in my opinion, what I would consider a homicide.”
Andy said his efforts, though, have managed to secure a degree of professional difficulty for York. According to Andy, “He orchestrated this, and now he’s no longer in the state of Texas. For a small while, he was an administrator in Arkansas, but thanks to my efforts informing his new employer, he’s no longer [there].”
In addition to his individual activism, Andy joined the FormerFedsGroup Freedom Foundation, which advocates on behalf of victims of COVID-19 hospital protocols and others with similar experiences. He described them as “the best group you can find if you’re a victim.”
“We’re on a mission,” Andy said. “We’re here to help as many people get as many stories out there and turn the narrative around.”
Many people have reached out to him through the FormerFeds Group but also through his own website, said Andy, describing similar treatment that they or loved ones experienced at hospitals, including at Baylor Scott & White.
Referring to the COVID-19-related hospital protocol prescribed by the Centers for Disease Control and Prevention, Andy said he is not certain if it was followed by Baylor Scott & White in his father’s case. But he noted that his and other victims’ experience make it sound like “there’s a formula they’re following.”
Andy said these efforts are important to everyone, even if they haven’t been victims of COVID-19 hospital protocols or similar treatment.
“We all get old and will need a little extra attention,” he said. “The question is, what kind of attention is that going to be? I’m hoping it’s going to be a real standard of care.”
Andy shared some words of advice for individuals who have had similar experiences or who may end up in the hospital for similar reasons.
“If you can get the chart, get the chart, print the chart. Read it before you do any reporting. Do your own homework,” he said.
He also recommends seeking professional help to grieve. “It’s okay to ask for help.”
“Also, understand that there are people like me out there, a lot of us that are going to, for as long as we’re alive, try to turn this thing around,” he added. “Don’t give up because you feel like you’re going nowhere. I have felt that way many times. … Believe in yourself. Don’t give up. Be persistent.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
The debate as to how much “pandemic” harm was caused not by a virus, but rather by the dystopian response to the perceived threat of a virus, has been raging for some time now.
Jonathan tweeted about this last year in relation to Lombardy and that thread was turned into this Panda article.
An analysis of the spatial characteristics of deaths during the spring 2020 wave in Northern Italy was carried out by him along with a Panda colleague; this suggested that it looked nothing like a spreading virus, and more like the sudden imposition of a policy response.
More recently, Jessica has essentially come to the same conclusions about New York: that something terrifyingly unnatural appears to have happened, which cannot be explained by the sudden spread of a deadly virus.
It surely does not require any scientific understanding whatsoever to glance at the below graph of total mortality rate in NYC going back to 2015 and see that what happened in a few weeks during spring 2020 suggests an abrupt episode of ferocious lethality which was at odds not only with anything observed anywhere at the time or thereafter, but also with even the highest estimates of the infection fatality rate alleged to have caused “the pandemic”.
If we look back even further, it can be seen that the reported spring 2020 mortality spike in New York is actually around double that observed in the autumn of the 1918 pandemic. But other places in 2020 did not see waves of deaths anywhere near those observed during the 1918 pandemic.
Moreover, unlike elsewhere, the increase in deaths was seen across a younger demographic, not exclusively in the elderly.
As shown in the graph below, all-cause hospital inpatient weekly death counts in the 20-59 age group were dramatically elevated for a short period, by a shocking 6-fold at their peak, with nearly all these deaths being coded as ‘covid’.
In fact, in New York, the % increase in all-cause deaths during the spring “1st wave” period was the same in the 20-69 year old age group as in the 70s and over:
In other places, however, what we were told was the same disease caused by the same virus left the younger age groups largely untouched, with nearly all deaths being in the elderly.
This discrepancy remains completely unexplained. It seems unarguable that certain difficult questions certainly need asking about what happened in New York in 2020 if we are to unravel the truth about what happened there.
Of course, the narratives emerging from Northern Italy and New York in 2020 were instrumental in driving fear and hysteria worldwide. Moreover, the number of deaths in both places informed early estimates of the IFR. These inciting incidents directly sparked much of the worldwide exaggerated, fear-driven response to what we now know was (if anything) a virus mainly affecting the frail and elderly, to which most people already had sufficient immunity to prevent severe illness.
For these reasons, it is essential that particular attention is paid to try to ascertain precisely what happened in these specific places.
It’s worth detailing – as evidence for the deeply dystopian mindset operating at the time – just some of the many deviations from normality that adversely affected human health and immunity, or which constituted sudden changes to healthcare practice.
These included (but were not limited to):
Stress and anxiety from confinement (being told to stay home) and fear propaganda
Discouragement to attend hospitals if ill
Reduced community prescribing of broad-spectrum antibiotics
Low staff levels in healthcare settings due to self-isolation of those “testing positive,” even with no symptoms
Isolating the elderly
Barring loved ones from hospital and care homes
Fear (on the part of HCWs) of tending to covid positive patients, compromising basic medical and care needs.
Early and inappropriate invasive ventilation
Overuse of midazolam and opiates
Inevitably, and rightly, some researchers have started to perform post-pandemic autopsies analysing the motives and reasoning used to justify policies and other changes in behaviour and to examine their real world consequences.
Some medical practitioners have taken umbrage at any suggestion that the stressful environment and sudden expectations and pressures laid upon them may have resulted in well-meaning medical staff crossing ethical lines, or violating the Hippocratic Oath.
Those who wish to point out that there is historical precedent for medical staff behaving diabolically while thinking they are doing good often invoke atrocities during the 1930s and 1940s (and receive opprobrium as a result).
However, there is a much more recent example, and one which we were oblivious to until recently, despite this incident being totally “out in the open”, the subject of a lengthy investigative article, book, and a TV mini-series: the post Hurricane Katrina incident at Memorial Hospital Center in New Orleans in 2006.
In the hurricane aftermath, the basement of Memorial Hospital Center flooded, power failed, and battery power for essential equipment started to run out. Most, but not all, patients were successfully evacuated.
The hurricane occurred on 29th August. A shocking finding was made in the aftermath, as described in the Wikipedia article:
On September 11, mortuary workers recovered 45 bodies from the hospital. Toxicology tests were performed on 41 bodies, and 23 tested positive for one or both of morphine and the fast-acting sedative midazolam [branded as Versed in the US], although few of these patients had been prescribed morphine for pain.
In the following weeks, it was reported that staff had discussed euthanizing patients. Some reports went further; Bryant King, an internist at Memorial, told CNN that he believed “the discussion of euthanasia was more than talk.”
LifeCare told the state Attorney General’s office that nine of their patients might “have been given lethal doses of medicines by a Memorial doctor and nurses.”
King publicly charged that one or more healthcare workers had killed patients, based on conversations with other health care workers. King told CNN that when he believed a doctor was about to kill patients, he boarded a boat and left the hospital. King explained his actions in terms of his opposition to Pou’s alleged actions, arguing “I’d rather be considered a person who abandoned patients than someone who aided in eliminating patients.”
Following an investigation into the deaths described above, the local DA (“District Attorney”) decided there was sufficient evidence to charge three medical staff with four counts of second-degree murder. Charges against two were later dropped in exchange for testimony.
The prosecution was deeply unpopular. Despite substantial evidence of deliberate actions taken to terminate lives – indeed, enough to satisfy the legal definition for homicide – many members of the public felt medical staff were simply “doing their best” under very trying circumstances. According to a local reporter the incident “ignited a furious debate in New Orleans and elsewhere about whether sharp ethical boundaries can be drawn around decisions on patient comfort made in a crisis.”
The DA failed to win re-election, and when the new DA convened a Grand Jury* at an undisclosed location, much of the previously amassed evidence was not presented and some of the key witnesses not called. The Grand Jury decided that charges should be dropped.
Unsurprisingly, several commentators (e.g., Loyola University Law Professor Dane Ciolono) opined that the Grand Jury was convened and run in such a way as to ensure charges would be dropped while providing “cover” for such an outcome.
Whatever actually occurred at Memorial Hospital, or whatever the staff’s motives, the incident speaks to an unsettling, yet undeniable truth: during a crisis, “ethical red lines” – however deeply held and valued – may be easily crossed. Society may judge those decisions acceptable or understandable, as appears to have happened with the Memorial Hospital case.
In summary, it would appear that the legal process was manipulated to assure an outcome which accorded with public opinion – that is to say to extinguish the possibility of prosecution while maintaining the pretence of due legal process. In this way, facing up to the stark reality – that as a society we mete out justice arbitrarily when we wish to – was avoided. Perhaps the well-ordered rules-based system suggested by statutory definitions of what actions constitute crimes, is to some extent just “for show”.
The Memorial Hospital case obliterates – with a relatively recent example – the notion that doctors and nurses all have the same ethical boundaries which they simply will not cross under any circumstances.
Could such boundaries have been crossed during the recent covid event?
A number of commentators are considering the possibility that changes in the policies and practices around the use of certain drugs (midazolam and opiates), and procedures (invasive ventilation) – sometimes in combination – may have contributed to the high mortality reported, at least in some specific places.
In relation to drugs, in an article published on his Substack last year, the blogger known as Bartram’s Folly explored the possibility that (in the UK) sheer fear and panic may well have driven medical staff to use midazolam and opiates more liberally in patients with covid, which may have encompassed anyone with a positive covid test.
In the UK one such mechanism which may have encouraged this measure is the NICE Guideline NG163 (no longer on their website but available here or as PDF download here), about which others have also written in detail. This guideline effectively transposed the advice for treating end-stage cancer patients with midazolam and opiates into that for covid patients. More detail on this here.
Of the guideline, Bartram said,
“… the NICE guidelines appear to have introduced a pathway for doctors which allowed for (perhaps even encouraged) more than a gentle nudge for those who were ill with Covid towards death, some of whom might well have survived given the chance. This iatrogenesis hypothesis would mean that at least some of the deaths recorded as with Covid might well have been a direct result of the care guidelines as set out by NICE.“
Later, Bartram makes the point that the pretext of a crisis situation or emergency may establish the grounds for ethical boundaries to be crossed or disregarded, at least temporarily, under the auspices of ignorance or ‘doing one’s best’ with the information said to be known or available at the time:
It is important to note that in the iatrogenesis hypothesis it isn’t necessary for some people to have had an evil intent – it is entirely possible that individuals promoted and exercised a policy that resulted in needless deaths while believing that they were ‘doing the right thing’ (e.g., see Hannah Arendt’s concept of the banality of evil).
In particular, ‘petty bureaucrats’ appear to be readily able to think up policies without seeing the need to consider the full consequences, and when these consequences are eventually revealed will usually point to the minutes from endless meetings with other petty bureaucrats to show that they weren’t personally responsible for the policy and they were simply following process.
Of course, once a framework had been decided front-line staff might have been grateful for the guidance offered given the challenging times, at least until the negative consequences of the guidance became painfully clear.
It should also be remembered that – in the US at least – certain extraordinary policy measures may have been important factors. For example, during the emergency NYC Governor Cuomo issued executive orders and suspended laws which gave doctors and nurses immunity and absolved hospitals of the responsibility to keep close patient records. (The order itself can be found here, and some legal commentary on it here.) Articles in JAMA can be interpreted as giving ethical permission for physicians to issue unilateral DNR orders, avoid CPR, and ration ventilators and critical care beds.
Moreover there are numerous examples of doctors, nurses and others in the US who later said they were following guidance, learning as they went. (See this interesting essay by Dr Kory, for example.) Under these circumstances it is easy to see how they could assume that something which ordinarily might have been questionable would become acceptable as “everyone else was doing it”.
Evidence of increased midazolam use can be seen in the US as well as in the UK. This graph from a study describing the use of 7 specific drugs in 47 hospitals in NY shows the daily count of patients (blue) who received midazolam and the disproportionate quantities used (orange) between March 1 and May 16, 2020.
Moreover, midazolam is currently listed by the FDA to have been in short supply since 2 April 2020:
ThisGuardian article from 13 April 2020 reports on a letter sent by “a group of prominent medical practitioners and experts” to capital punishment states imploring them to:
“release their stocks of essential sedatives and paralytics that they hoard for executions” so that they can be “used for intubations and mechanical ventilation of the most severely ill coronavirus patients who cannot breathe for themselves”.
The tone of this letter can be taken to illustrate the sense of sheer panic prevailing at the time – certainly not conducive to rational decision-making – combined with the assumption that invasive ventilation was going to be extensively required and used.
This takes us to the question of invasive ventilation, whether it might have been used too often, inappropriately, and why.
As well as panic, the role of fear on the part of healthcare workers cannot be underestimated. Here is Dr Vinay Prasad stating that:
“It is a unique situation in medicine. In our whole medical career, doctors have never been personally afraid the way they were [with covid].”
Official guidance (see for example this from a British anaesthetists’ professional association) certainly reinforced the idea that one of the benefits of early intubation was to reduce the aerosolization of virus, such that it would be safer for those caring for the patients, compared to when non-invasive forms of ventilation were used.
ThisJAMA Clinical Update “Care for Critically Ill Patients With COVID-19” published on 11 March 2020 strongly supports the idea that the thinking was very much that non-invasive oxygen augmentation could be dangerous for healthcare workers:
The journalist Alex Berenson was early to point out that ventilator shortage may have more to do with overuse “to protect staff” than to being overwhelmed by patients in respiratory failure.
It seems like fear may well have been augmented by official guidance to result in significant overuse of this measure.
It is important to understand the differences between the Memorial Hospital incident and what may have happened in the early stages of the covid crisis. In New Orleans, it may indeed have been reasonable to assume that it was going to be impossible to evacuate the patients (who were given midazolam and opiates to ease suffering) in time, and that they were indeed unsaveable due to the extraordinary circumstances. (Whether or not this was actually the case will probably never be known, because of the legal shenanigans described above.)
However, whether that applies to all, some, or just a few of those who died in spring 2020 after being administered the same or other drugs (or placed on mechanical ventilators or issued a unilateral DNR, etc.) is still a matter of debate whereas for sure, Hurricane Katrina was self-evidently an extreme weather event that created devastation and emergency conditions in its fury and wake.
Certainly, it seems clear that personal fear and a belief in the lethality of this infection drove much medical decision-making in the early days. It is not hard to imagine actions being taken which were then rationalised by imagining the suffering that had been prevented, limited resources preserved, and many lives saved. The deaths witnessed could easily have acted as positive reinforcement in the minds of healthcare workers as to how serious the illness was. These protocols could lead to the deaths of patients who were not particularly old and frail and thus reinforce the message that the virus was potentially fatal even in such people
The decisions that healthcare workers made, and the influences on and factors involved in those decisions, will be discussed and dissected for decades to come. When humanity is ready to confront what occurred – and admit that ethical inversions in hospitals and care homes contributed to unintentional iatrogenic death, we can move toward keeping it from happening again.
* (A Grand Jury in the US is a specific type of court empowered by law to determine whether probable cause exists to support criminal charges for a suspect in a crime. Louisiana – in which New Orleans is situated – is one of 23 US states that use grand juries for indictments in serious crimes.)
The New World Order (NWO), is it a recipe for war or peace? That is the question Mahathir bin Mohamad asked in a speech made at the New World Order International Conference in 2015.
Before I continue, Wikipedia provides me with ‘Context’ under the video this article is based on – “The New World Order is a conspiracy theory that hypothesizes a secretly emerging totalitarian world government”. Just so that you are aware!
Mahathir was Prime Minister of Malaysia from 1981 to 2003 and then later from 2018 to 2020. His 24 years as Prime Minister make him the country’s longest serving Prime Minister. He has often been extremely critical of the West and the foreign policy of the US. The former Prime Minister has claimed that the US staged the war on terror to increase its powers and 9/11 was a false flag by the US Government.
So his comments at the 2015 conference won’t come as a surprise but some of the detail might.
He says the idea of a NWO is not new, it is very old. “Basically, it is about having a world government which will abolish all states, all nations, all borders. That world government is to be governed by certain people, elites, people who are very rich, very intelligent, very powerful. There was not much talk about democracy or choice of leaders, instead a government by elites who will impose the rules on everyone. And for those unwilling to submit to them there will be punishment”.
Mahathir tells the audience it is important to remember that this NWO is an Old World Order. It is something that was conceived more than 100 years ago.
Globalisation and a borderless world is an expression that relates to the concept of the NWO as it was first conceived. They don’t say whether it will be ruled democratically by the election of leaders.
To a certain extent, he says, this NWO is already with us. The world today is dominated by the powerful, the ones with the guns. The world is frightened of the countries with nuclear weapons which makes the world submissive. And when the world submits to them, effectively there is one government in this world.
Politically, there is no freedom for any nation. Internationally, there is no free speech. Say the wrong thing and you will be taken to task and vilified in the international press which is under their control. Action may be taken against you. You can criticise your own government but not the power that is running the world today.
Mahathir says they are urging every country to undergo regime change, except for those that are already submitting to them. If you refuse, you will be persuaded through propaganda and actions such as invasion and occupation and the removal of the head of that government will be replaced by one who will submit to the NWO. We see this in Middle East.
The economy is also being used to create a NWO. Free trade agreements just mean more rules than they have ever had previously. It is not about free trade, it is not free at all, it is about regulated trade. Once you have regulated trade then the most powerful economy will dominate.
If you don’t like to conform then you may have sanctions placed against you. We see this with countries like Iran and Russia.
The former Prime Minister says there are certain moral values that are being promoted. You are not allowed to have your own value system. I disagree with some of what he says here, in this part of his talk, including his comments on free speech. However, he says it is an attempt to undermine everything we believe in.
Mahathir says that what we are seeing today is the establishment of a world government that is responsible to nobody. The rulers consider themselves as the most suitable people to run the world.
Will this bring peace or will this cause wars? We already see wars being fought around the world so they can establish their NWO. Not only wars but subversion of moral values until we become helpless.
Towards the end of his speech, Mahathir makes his most inflammatory comments. The intention is to reduce the number of people in this world, he says. When the NWO was created, the world population was only 3 billion and the intention was to reduce it to 1 billion. Now the population is 7 billion, there will be a need to kill many billions of people, starve them to death or to prevent them from giving birth, in order to reduce the population. This is what is in store for most. For those that will suffer and die, there will be the peace of the grave.
There will be wars to weaken and destabilise small nations so that they will submit to the NWO. He concludes by saying there will either be the peace of the grave or war. The world will be in a state of turmoil.
An oil tanker seized by the US Navy for allegedly carrying sanctioned Iranian oil began transferring its cargo to another tanker off the coast of Texas on 20 August, despite threats from Tehran to target shipping in the Persian Gulf in response.
Ship-tracking data analyzed by The Associated Press showed the Marshall Islands-flagged Suez Rajan began the ship-to-ship transfer of its oil to the MR Euphrates, a tanker located some 70 kilometers southeast of Houston in the Gulf of Mexico. The value of the oil on the 800,000-barrel tanker is estimated to be $56 million.
Washington illegally seized the Marshall Islands-flagged Suez Rajan supertanker in April of this year in what was described by the Pentagon as “a sanctions-enforcement operation.” Washington also charged the ship’s owner with “sanctions evasion” and directed the stolen cargo to the waters off the Texas coast.
According to the Wall Street Journal, the Suez Rajan came under Washington’s radar after an anti-Iran organization – the New York-based United Against Nuclear Iran (UANI) – provided information about the ship’s cargo to government officials. Lawyers representing the families of victims of the 11 September attacks, “whom US courts have given the right to claim compensation from [Tehran],” filed a lawsuit against one of the ship’s former owners.
However, oil firms in the US had been reluctant to unload the shipment of stolen Iranian oil sitting, saying they were “too worried about Iranian reprisal” to touch the cargo, sources familiar with the matter told the WSJ.
“Companies with any exposure whatsoever in the Persian Gulf are literally afraid to do it,” a Houston-based energy executive told the US outlet, adding that companies fear “the Iranians would take retribution against them.”
“I don’t know if anybody’s going to touch it,” another executive at a shipping company had said.
The transfer of the Iranian oil comes as the US Navy has bolstered its forces in the Persian Gulf in recent weeks, including by sending the troop-and-aircraft-carrying USS Bataan through the Strait of Hormuz. Washington is also considering placing US troops on commercial vessels to prevent Tehran from seizing them in response to Washington’s own seizures of Iranian ships.
US theft of Iranian oil from the Suez Rajan also comes as Tehran and Washington seek to complete a prisoner exchange that also involves the US releasing between $6 and $10 billion in seized Iranian oil proceeds held in banks in South Korea and Europe.
Iran has been resisting US sanctions by continuing to sell its oil abroad, while the US has been seizing cargoes since 2019 after withdrawing from the nuclear deal negotiated between the two rival countries. The 2015 nuclear deal held that Iran would limit the enrichment of uranium for its nuclear program in exchange for sanctions relief. The US withdrew from the deal unilaterally in 2018. Washington accuses Iran of seeking to develop nuclear weapons, however, Iranian leaders have stated the nuclear program is for peaceful purposes and that developing nuclear weapons is forbidden by Islam.
Three utility workers were killed in the Russian city of Donetsk on Friday when a faulty Ukrainian cluster shell exploded, according to local officials. Another worker was injured in the blast.
The workers, who had been repairing water pipes in central Donetsk, were caught in the blast during their lunch break. They were killed on the spot in a “detonation of an explosive device,” Donetsk Mayor Aleksey Kulemzin said. Two others were hospitalized following the blast.
According to media reports and local officials, the explosion was caused by a Ukrainian cluster artillery shell. The unexploded device may have been hanging from a tree or in a trash can, local residents told the media. The shell suddenly detonated and released its sub munitions, which exploded, hitting the civilians.
In recent weeks, the Ukrainian military has ramped up its use of cluster munitions, repeatedly firing them at Donetsk and other locations near the front line. The shells have already caused multiple deaths and injuries among civilians.
The uptick in the use of cluster munitions comes after last month the US sent so-called dual-purpose improved conventional munitions (DPICM) for NATO-caliber 155mm howitzers. The controversial delivery, which was criticized even by some of the US’ closest allies, came as a stop-gap measure to compensate for a shortage of conventional artillery shells, as admitted by President Joe Biden.
Over the course of the ongoing conflict, Russia has accused the Ukrainian military of repeatedly using cluster munitions from its domestic stockpiles to target civilian areas. In particular, Kiev’s forces have on many occasions shelled Donetsk and its surroundings with unguided multiple rocket artillery projectiles containing the controversial anti-personnel PFM-1 petal mines.
This report is designed to help readers think about some big topics: how to really prevent pandemics and biological warfare, how to assess proposals by the WHO and its members for preventing and responding to pandemics, and whether we can rely on our health officials to navigate these areas in ways that make sense and will help their populations. We start with a history of biological arms control and rapidly move to the COVID pandemic, eventually arriving at plans to protect the future.
Weapons of Mass Destruction: Chem/Bio
Traditionally, the Weapons of Mass Destruction (WMD) have been labelled Chemical, Biological, Radiologic, and Nuclear (CBRN).
The people of the world don’t want them used on us—for they are cheap ways to kill and maim large numbers of people quickly. And so international treaties were created to try to prevent their development (only in the later treaties) and use (in all the biological arms control treaties). First was the Geneva Protocol of 1925, following the use of poison gases and limited biological weapons in World War I, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, and during those 50 years the US asserted it was not bound by the treaty.
The US used both biological and chemical weapons during those 50 years. The US almost certainly used biological weapons in the Korean War (see this, this, this and this) and perhaps used both in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and probably other chemical weapons like BZ (a hallucinogen/incapacitant) led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968 and 1969, two important books were published that had a great influence on the American psyche regarding our massive stockpiling and use of these agents. The first book, written by a young Seymour Hersh about the US chemical and biological warfare program, was titled Chemical and Biological Warfare; America’s Hidden Arsenal. In 1969 Congressman Richard D. McCarthy, a former newspaperman from Buffalo, NY wrote the book The Ultimate Folly: War by Pestilence, Asphyxiation and Defoliation about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand,” has sprayed anti-plant chemicals over an area almost the size of the state of Massachusetts, over 10 per cent of its cropland. “Ranch Hand” no longer has much to do with the official justification of preventing ambush. Rather, it has become a kind of environmental warfare, devastating vast tracts of forest in order to facilitate our aerial reconnaissance. Our use of “super tear gas” (it is also a powerful lung irritant) has escalated from the originally announced purpose of saving lives in “riot control-like situations” to the full-scale combat use of gas artillery shells, gas rockets and gas bombs to enhance the killing power of conventional high explosive and flame weapons. Fourteen million pounds have been used thus far, enough to cover all of Vietnam with a field effective concentration. Many nations, including some of our own allies have expressed the opinion that this kind of gas warfare violates the Geneva Protocol, a view shared by McCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, and seeking to burnish his presidency, President Nixon announced to the world in November 1969 that the US was going to end its biowarfare program (but not the chemical program). Following pointed reminders that Nixon had not eschewed the use of toxins, in February 1970 Nixon announced we would also get rid of our toxin weapons, which included snake, snail, frog, fish, bacterial, and fungal toxins that could be used for assassinations and other purposes.
It has been claimed that these declarations resulted from careful calculations that the US was far ahead technically of most other nations in its chemical and nuclear weapons. But biological weapons were considered the “poor man’s atomic bomb” and required much less sophistication to produce. Therefore, the US was not far ahead in the biological weapons arena. By banning this class of weapon, the US would gain strategically.
But in 1973 genetic engineering (recombinant DNA) was discovered by Americans Herbert Boyer and Stanley Cohen, which changed the biological warfare calculus. Now the US had regained a technological advantage for this type of endeavor.
The Biological Weapons Convention established conferences to be held every 5 years to strengthen the treaty. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent nations from cheating and would add sanctions (punishments) if nations failed to comply with the treaty. However, since 1991 the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone accepts that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. While the USSR tried a sloppy cover-up, blaming contaminated black market meat, this was a clear BWC violation to all those knowledgeable about anthrax.
US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs, were also thought by experts to have transgressed the BWC.
It has taken over 40 years, but in 2022 all declared stocks of chemical weapons had been destroyed by the USA, by Russia, and the other 193 member nation signatories. The chemical weapons convention does include provisions for surprise inspections and sanctions.
Pandemics and Biological Warfare Receive Funding from Same Stream
It is now 2023, and during the 48 years the Biological Weapons Convention has been in force the wall it was supposed to build against the development, production, and use of biological weapons has been steadily eroded. Meanwhile, especially since the 2001 anthrax letters, nations (with the US at the forefront) have been building up their “biodefense” and “pandemic preparedness” capacities.
Under the guise of preparing their defenses against biowarfare and pandemics, nations have conducted “dual-use” (both offensive and defensive) research and development, which has led to the creation of more deadly and more transmissible microorganisms. And employing new verbiage to shield this effort from scrutiny, biological warfare research was renamed as “gain-of-function” research.
Gain-of-function is a euphemism for biological warfare research aka germ warfare research. It is so risky that funding it was banned by the US government (but only for SARS coronaviruses and avian flu viruses) in 2014 after a public outcry from hundreds of scientists. Then in 2017 Drs. Tony Fauci and Francis Collins lifted the moratorium, with no real safeguards in place. Fauci and Collins even had the temerity to publish their opinion that the risk from this gain-of-function research was ‘worth it.’
What does gain-of-function actually mean? It means that scientists are able to use a variety of techniques to turn ordinary or pathogenic viruses and bacteria into biological weapons. The research is justified by the claim that scientists can get out ahead of nature and predict what might be a future pandemic threat, or what another nation might use as a bioweapon. The functions gained by the viruses or other microorganisms to turn them into biological warfare agents consist of two categories: enhanced transmission or enhanced pathogenicity (illness severity).
1) improved transmissibility may result from:
a) needing fewer viral or bacterial copies to cause infection,
b) causing the generation of higher viral or bacterial titers,
c) a new mode of spread, such as adding airborne transmission to a virus that previously only spread through bodily fluids,
d) expanded range of susceptible organs (aka tissue tropism); for example, not only respiratory secretions but also urine or stool might transmit the virus, which was found in SARS-CoV-2,
e) expanded host range; for example, instead of infecting bats, the virus is passaged through humanized mice and thus acclimated to the human ACE-2 receptor, which was found in SARS-CoV-2,
f) improved cellular entry; for example, by adding a furin cleavage site, which was found in SARS-CoV-2,
2) increased pathogenicity, so instead of causing a milder illness, the pathogen would be made to cause severe illness or death, using various methods. SARS-CoV-2 had unusual homologies (identical short segments) to human tissues and the HIV virus, which may have caused or contributed to the late autoimmune stage of illness, impaired immune response and ‘long COVID.’
Funding for (Natural) Pandemics, Including Yearly Influenza, was Lumped Together with Biological Defense Funding
Perhaps the comingling of funding was designed to make it harder for Congress and the public to understand what was being funded, and how much taxpayer funding was going to gain-of-function work, which might lead them to question why it was being done at all, given its prohibition in the Biological Weapons Convention, and additional questions about its value. Former CDC Director Robert Redfield, a physician and virologist, told Congress in March of 2023 that gain-of-function research had not resulted in a single beneficial drug, vaccine, or therapeutic to his knowledge.
Nonprofits and universities like EcoHealth Alliance and its affiliated University of California, Davis veterinary school were used as intermediaries to obscure the fact that US taxpayers were supporting scientists in dozens of foreign countries, including China, for research that included gain-of-function work on coronaviruses.
Perhaps to keep the lucrative funding going, fears about pandemics have been deliberately amplified over the past several decades. The federal government has been spending huge sums on pandemic preparedness over the past 20 years, routing it through many federal and state agencies. President Biden’s proposed 2024 budget requested “$20 billion in mandatory funding across DHHS for pandemic preparedness” while the DHS, DOD, and the State Department have additional budgets for pandemic preparedness for both domestic and international spending.
Although the 20th century experienced only 3 significant pandemics (the Spanish flu of 1918-19 and 2 influenza pandemics in 1957 and 1968) the mass media have presented us with almost non-stop pandemics during the 21st century: SARS-1 (2002-3), avian flu (2004-on), swine flu (2009-10), Ebola (2014, 2018-19), Zika (2016), COVID (2020-2023), and monkeypox (2022-23). And we are incessantly told that more are coming, and that they are likely to be worse.
We have been assaulted with warnings and threats for over 2 decades to induce a deep fear of infectious diseases. It seems to have worked.
The genomes of both SARS-CoV-2 and the 2022 monkeypox (MPOX) virus lead to suspicion that both were bioengineered pathogens originating in laboratories. The group of virologists assembled by Drs. Fauci and Farrar identified 6 unusual (probably lab-derived) parts of the SARS-CoV-2 genome as early as February 1, 2020 and more have been suggested subsequently.
I do not know if these viruses leaked accidentally or were deliberately released, but I am leaning toward the conclusion that both were deliberately released, based on the locations where they first appeared, the well-orchestrated but faked videos rolled out by the mass media for COVID, and the illogical and harmful official responses to each. In neither case was the public given accurate information about the infections’ severity or treatments, and the responses by Western governments never made scientific sense. Why wouldn’t you treat cases early, the way doctors treat everything else? It seemed that our governments were trading on the fact that few people knew enough about viruses and therapeutics to make independent assessments about the information they were being fed.
Yet by August 2021, there was no corresponding course correction. Instead, the federal government doubled down, imposing vaccine mandates on 100 million Americans in September 2021 in spite of ‘the science.’ There has been no accurate statement yet from any federal agency about the lack of utility of masking for an airborne virus (which is probably why the US government and WHO delayed acknowledging airborne spread by COVID for 18 months), the lack of efficacy of social distancing for an airborne virus, and the risks and poor efficacy of 2 dangerous oral drugs (paxlovid and molnupiravir) purchased by the US government for COVID treatment, even without a doctor’s prescription.
Never have any federal agencies acknowledged the truth about the COVID vaccines’ safety and efficacy. Instead, the CDC turns definitional and statistical cartwheels so it can continue to claim they are “safe and effective.” Even worse, with all that we know, a third generation COVID vaccine is to be rolled out for this fall and the FDA has announced that yearly boosters are planned.
All this goes on, even a year after we learned (with continuing corroborations) that children and working age adults are dying at rates 25 percent or more above the expected averages, and the vascular side effects of vaccination are the only reasonable explanation.
Maiming with Myocarditis
Both of the two US monkeypox/smallpox vaccines (Jynneos and ACAM2000) are known to cause myocarditis, as do all 3 COVID vaccines currently available in the US: the Pfizer and Moderna COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial, but this was downplayed and it was authorized and rolled out anyway, intended for those who refused the mRNA vaccines due to the use of fetal tissue in their manufacture.
Here is what the FDA’s reviewers wrote about the cardiac side effects noted in the Jynneos clinical trials:
Up to 18.4% of subjects in 2 studies developed post-vaccination elevation of troponin [a cardiac muscle enzyme signifying cardiac damage]. However, all of these troponin elevations were asymptomatic and without a clinically associated event or other sign of myopericarditis. p. 198
The applicant has committed to conduct an observational, post-marketing study as part of their routine PVP. The sponsor will collect data on cardiac events that occur and are assessed as a routine part of medical care. p. 200
In other words, while the only way to cause an elevated troponin level is to break down cardiac muscle cells, the FDA did not require a specific study to evaluate the extent of cardiac damage that might be caused by Jynneos when it issued its 2019 license. How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. I have not seen a study with rates of myocarditis for Jynneos, but there was an unspecified elevation of cardiac enzymes in 10 percent and 18 percent of Jynneos recipients in two unpublished prelicensure studies available on the FDA website. My guess for the mRNA COVID vaccines is that they cause myocarditis in this general range, the vast majority of which remain undiagnosed and probably asymptomatic.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work—Jynneos didn’t prevent infection in the monkeys in whom it was tested nor did it do well in people. And the CDC has failed to publish its trial of Jynneos vaccine in the ~1,600 Congolese healthcare workers on whom the CDC tested it for efficacy and safety in 2017. The CDC made the mistake of announcing the trial, and posting it to clinicaltrials.gov as required, but has not informed its advisory committee that reviewed the vaccine, nor the public, of the trial’s results.
There can be no question about it: our health agencies are guilty of malfeasance, misrepresentation, and deliberate infliction of harm on their own populations. The health agencies first incited terror with apocalyptic predictions, then demanded patients be medically neglected, and finally enforced vaccinations and treatments that were tantamount to malpractice.
COVID Vaccines: The Chicken or the Egg?
The health authorities could have just been ignorant — that could possibly explain the first few months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did our health authorities still push COVID vaccines on low-risk populations who were clearly at greater risk from a vaccine side effect than from COVID? Particularly as time went on and newer variants were less and less virulent?
Once you acknowledge these basic facts, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. While we cannot be certain, we should at least be suspicious. And the fact that the US contracted for 10 doses per person (review purchases here, here, here, here and here) and so did the European Union (here and here) and Canada should make us even more suspicious – there is no justification for agreeing to purchase so many doses for vaccines at a time when the vaccines’ ability to prevent infection and transmission was questionable, and its safety suspect or worrying.
Why would governments want ten doses per person? Three maybe. But ten? Even if yearly boosters were expected, there was no reason to sign contracts for enough vaccine for the next nine years for a rapidly mutating virus. Australia bought 8 doses per person. By December 20, 2020 New Zealand had secured triple the vaccines it needed, and offered to share some with nearby nations. No one has come forward to explain the reason for these excessive purchases.
Furthermore, you don’t need a vaccine passport (aka digital ID, aka a phone app that in Europe included a mechanism for an electronic payments system) unless you are giving out regular boosters. Were the vaccines conceived of as the means for putting our vaccinations, health records, official documents–and most importantly, shifting our financial transactions online, all managed on a phone app? This would be an attack on privacy as well as the enabling step to a social credit system in the West. Interestingly, vaccine passports were already being planned for the European Union by 2018.
A Pandemic Treaty and Amendments: Brought to You by the Same People who Mismanaged the Past 3 Years, to Save us from Themselves?
The same US and other governments and the WHO that imposed draconian measures on citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs, withheld effective treatments, and refused to tell us that most people who required ICU care for COVID were vitamin D-deficient and that taking vitamin D would lessen COVID’s severity–decided in 2021 we suddenly needed an international pandemic treaty. Why? To prevent and ameliorate future pandemics or biological warfare events… so we would not suffer again as we did with the COVID pandemic, they insisted. The WHO would manage it.
To paraphrase Ronald Reagan, the words, “I’m from the WHO, and I’m here to help” should be the most terrifying words in the English language after the COVID fiasco.
What the WHO and our governments conveniently failed to mention is that we suffered so badly because oftheir medical mismanagement and our governments’ merciless economic shutdowns and mismanagement. According to the World Bank, an additional 70 million people were forced into extreme poverty in 2020 alone. This was due to policies issued by our nations’ rulers, their elite advisers and the World Health Organization, which came out with guidance to shut down economic activity that most nations adopted without question. The WHO is acutely aware of the consequences of economic lockdowns, having published the following:
Malnutrition persisted in all its forms, with children paying a high price: in 2020, over 149 million under-fives are estimated to have been stunted, or too short for their age; more than 45 million – wasted, or too thin for their height…
Starvation may have killed more people than COVID, and they were disproportionately the youngest, rather than the oldest. Yet the WHO prattles on about equity, diversity, and solidarity—having itself caused the worst food crisis in our lifetime, which was not due to nature but was man-made.
How can anyone take seriously claims by the same officials who mishandled COVID that they want to spare us from another medical and economic disaster–by using the same strategies they applied to COVID, after they masterminded the last disaster? And the fact that no governments or health officials have admitted their errors should convince us never to let them manage anything ever again. Why would we let them draw up an international treaty and new amendments to the existing International Health Regulations (IHR) that will bind our governments to obey the WHO’s dictates forever?
Those dictates, by the way, include vaccine development at breakneck speed, the power to enforce which drugs we will be directed to use, and which drugs will be prohibited, and the requirement to monitor media for “misinformation” and impose censorship so that only the WHO’s public health narrative will be conveyed to the public.
The WHO’s Pandemic Treaty Draft Requires the Sharing of Potential Pandemic Pathogens. This is a Euphemism for Bioweapons Proliferation.
Obviously, the best way to spare us from another pandemic is to immediately stop funding gain-of-function (GOF) research and get rid of all existing GOF organisms. Let all nations build huge bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its June 2023 Bureau Text of the Draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s draft treaty, which most nations’ rulers appear to have bought into, all governments will share all viruses and bacteria they come up with that are determined to have “pandemic potential” — share them with the WHO and other governments, putting their genomic sequences online. No, I am not making this up. (See screenshots from the draft treaty below.) Then the WHO and all the Fauci’s of the world would gain access to all the newly identified dangerous viruses. Would hackers also gain access to the sequences? This pandemic plan should make you feel anything but secure.
Fauci, Tedros, and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to ever more potential biological weapons, and the rest of us are on the other, at their mercy.
This poorly conceptualized plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. (For example, see Security Council resolution 1540 adopted in 2004.) But this is the plan of the WHO and of many of our leaders. Governments will all share the weapons.
The Genomic Sequencing Conundrum
And governments are to commit to building biolabs that must include genomic sequencing. No explanation has been forthcoming about why each nation needs to install its own genome sequencing laboratories. Of course, they would sequence the many viruses that will be detected as a result of the pathogen surveillance activities nations must perform, according to the WHO treaty draft. But the same techniques can be used to sequence human genomes. The fact that the EU, UK, and US are currently engaged in projects to sequence about 2 million of their citizens’ genomes provides a hint they may want to collect additional genomes of Africans, Asians, and others.
This might fly as simply sharing state-of-the-art science with our less-developed neighbors. But it is curious that there is so much emphasis on genomics, compared to an absence of discussion about developing repurposed drugs for pandemics in the draft treaty or IHR amendments.
But we can’t forget that virtually all developed nations, in lockstep, restricted the use of safe generic hydroxychloroquine, ivermectin, and related drugs during the pandemic. In retrospect, the only logical explanation for this unprecedented action was to preserve the market for expensive patentable drugs and vaccines, and possibly to prolong the pandemic.
Genomes offer great potential profits, as well as providing the substrate for transhumanist experiments that could include designer babies.
The latest version (aka the WHO Bureau draft) of the pandemic treaty can be accessed here. I provide screenshots to illustrate additional points.
Draft pages 10 and 11:
The WHO Treaty Draft Incentivizes Gain-of-Function Research
What else is in the Treaty? Gain-of-Function research (designed to make microorganisms more transmissible or more pathogenic) is explicitly incentivized by the treaty. The treaty demands that administrative hurdles to such research must be minimized, while unintended consequences (aka pandemics) should be prevented. But of course, when you perform this type of research, leaks and losses of agents can’t always be prevented. The joint CDC-USDA Federal Select Agent Program (FSAP) which keeps track of research on potential pandemic pathogens collects reports of about 200 accidents or escapes yearly from labs situated in the US. The FSAP annual report for 2021 notes:
“In 2021, FSAP received 8 reports of losses, 177 reports of releases, and no reports of thefts.”
Research on deadly pathogens cannot be performed without risks both to the researchers and the outside world.
Draft page 14:
Vaccines Will be Rolled Out Speedily Under Abbreviated Future Testing Protocols
Vaccines normally take 10-15 years to be developed. In case you thought the COVID vaccines took too long to be rolled out (326 days from availability of the viral sequence to authorization of the first US COVID vaccine) the WHO treaty draft has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way places like Africa, for example?) And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.”
Draft page 14:
Manufacturer and Government Liability for Vaccine Injuries Must be “Managed”
Nations are supposed to use “existing relevant models” as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal.
Is the US government’s program to be a model of what gets implemented internationally?
The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated exactly 4 (yes, four) of the 12,000 claimants for COVID product-related injuries as of August 1, 2023. All pandemic EUA drugs and vaccines convey a liability shield to the government and manufacturers (this includes monoclonal antibodies, pre-licensure remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines) and the only avenue for injury compensation is through this program.
Slightly over 1,000 of the 12,000 claims have been adjudicated while 10,887 are pending review. Twenty claims were deemed eligible and await a benefits review. Benefits are only paid for uncovered medical expenses or lost income. A total of 983 people, or 98 percent of those whose claims have been adjudicated had their claims denied, many because they missed the brief one-year statute of limitations. Below are the latest data from this program:
The treaty draft also demands weakening the strict regulation of medical drugs and vaccines during emergencies, under the rubric of “Regulatory Strengthening.” As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25).
Next Up: Vaccines Developed in 100 Days
A plan to develop vaccines in 100 days and have them manufactured in 30 additional days has been widely publicized by the vaccine nonprofit CEPI, founded in 2017 by Sir Dr. Jeremy Farrar, who is now the WHO’s Chief Scientist. The plan has been echoed by the US and UK governments and received some buy-in from the G7 in 2021. This timeframe would only allow for very brief testing in humans, or would, more likely, limit testing to animals. Why would any country sign up for this? Is this what we the people want?
The plan furthermore depends on the vaccines only being tested for their ability to induce antibodies, which is termed immunogenicity, rather than being shown to actually prevent disease, at least for the initial rollout. My understanding of FDA regulation was that antibody levels were not an acceptable surrogate for immunity unless they had been demonstrated to actually correlate with protection. However, the FDA’s recent vaccine decisions have scrapped all that and vaccines are now being approved based on antibody titers alone. The FDA’s vaccine advisory committee has asked it for better indicators of efficacy than this, but the advisers have also voted to approve or authorize vaccines in the absence of any real measures showing that they work. I learned this because I watch the FDA vaccine advisory meetings and provide a live blog of them.
We all know how long it took for the public to become aware that the COVID vaccines failed to prevent transmission and only prevented cases for a period of weeks to months. The US government has still not officially admitted this, even though CDC Director Rochelle Walensky told CNN’s Wolf Blitzer the truth about transmission on August 6, 2021.
It is critical for the public to understand that safety testing can only be accomplished in human beings, as animals react differently to drugs and vaccines than humans do. Therefore, limited testing in animals would mean there was no actual safety testing. But testing vaccines in humans for only short periods is also unacceptable.
Testing vaccines during brief trials in humans (the Pfizer trials only followed a “safety subset” of trial subjects for a median of two months for safety) allowed COVID vaccines to be rolled out without the public being aware they could cause myocarditis and sudden deaths, most commonly in athletic young males in their teens and twenties, or a myriad of other conditions.
Finally, following this rapid manufacturing plan, thorough testing for potential failures in the manufacturing process could not be performed. With the current plan for far-flung, decentralized manufacturing facilities that are said to be necessary to achieve vaccine equity for all, there are nowhere near enough regulators who could inspect and approve them.
Will the WHO Respect Human Rights?
The need to respect “human rights, dignity, and freedom of persons” is embedded in the current International Health Regulations (IHR), as well as other UN treaties. However, the language guaranteeing human rights, dignity, and freedom of persons was peremptorily removed from the proposed IHR Amendments, without explanation. The removal of human rights protections did not go unnoticed, and the WHO has been widely criticized for it.
The WHO apparently is responding to these criticisms, and so the language guaranteeing human rights that was removed from the drafts of the International Health Regulations has been inserted into the newest version of the pandemic treaty.
Conclusions
As long predicted by science fiction, our bio- and cyber-scientific achievements have finally gotten away from us. We can produce vaccines in 100 days and manufacture them in 130 days–but there will be no guarantees that the products will be safe, effective, or adequately manufactured. And we can expect large profits but no consequences for the manufacturers.
Our genes can be decoded, and the fruits of personalized medicine made available to us. Or perhaps our genes will be patented and sold to the highest bidder. We might be able to select for special characteristics in our children, but at the same time, a human underclass could be created.
Our electronic communications can be completely monitored and censored, and uniform messaging can be imposed on everyone. But for whom would this be good?
New biological weapons can be engineered. They can be shared. Maybe that will speed up the development of vaccines and therapeutics. But who really benefits from this scheme? Who pays the price of accidents or deliberate use? Wouldn’t it be better to end so-called gain-of-function research entirely through restrictions on funding and other regulations, rather than encouraging its proliferation?
These are important issues for humanity, and I encourage everyone to become part of the conversation.
Dr. Meryl Nass, MD is an internal medicine specialist in Ellsworth, ME, and has over 42 years of experience in the medical field. She graduated from University of Mississippi School of Medicine in 1980.
The government and the people of Ukraine should not allow the use of depleted uranium shells on their soil as these could have long-term consequences for the health of future generations, Serbian Health Danica Grujicic said in an interview with Sputnik on Tuesday.
“Previously, in several interviews, I have tried to reach out to the decision-makers in Ukraine and especially to the citizens of Ukraine who will continue to live there to make them realize that all this [radioactive] contamination will have consequences for their health and the health of their offspring,” she said.
The minister added that “it is scary to use such weapons in terms of health.”
“How can you allow the use of depleted uranium on your territory? Does it mean that you are planning to go somewhere else, and do not want to live here? The health consequences will remain for many years to come. Worst of all, it will affect children as well,” the minister said.
She said that cancer in patients in Serbia after the 1999 NATO bombing became less predictable and more likely to be fatal.
“I am sure that an experiment has been conducted that continues to affect not only our people but also Croats, Hungarians and Albanians. If you look at the statistics, you will see that the highest mortality from cancer is in these countries: Serbia, Hungary and Croatia. We swap places within the top three,” Grujicic said.
The minister believes that high mortality rates are not due to poor treatment, as innovative therapy tools and methods have been introduced and applied in Serbia in recent years.
“I believe that ‘our’ tumors are more aggressive. There are young people who die in a month or month and a half, although with the new therapy and by all indications they could have lived for a long time. They just die suddenly, and you do not know why it happened. For this, we need to carry out research, we need projects. I call on all medical and scientific institutions that want to do this to submit their projects to be included in the next year’s budget,” she said.
In 1999, an armed confrontation between Albanian separatists from the Kosovo Liberation Army and the Serbian army led to a bombing of what was then the Socialist Federal Republic of Yugoslavia, consisting of Serbia and Montenegro, by NATO forces. The operation was undertaken without the approval of the UN Security Council and was based on allegations by Western countries that the Yugoslav authorities were carrying out ethnic cleansing of Kosovo Albanians.
Grujicic is a renowned neurosurgeon who served as the director of the Institute of Oncology and Radiology of Serbia before she was appointed the health minister. She has been calling attention to the increase in cancer cases and other pathologies in Serbia since the 1999 NATO bombing of Serbia with depleted uranium shells.
WASHINGTON – The United States has established bio-laboratories in Ukraine as part of programs involving biological weapons, said Robert Kennedy Jr, a Democratic Party presidential candidate.
“We have bio-labs in Ukraine because we are developing bioweapons, and these weapons involve all sorts of cutting-edge synthetic biology technologies like CRISPR and genetic engineering methods that were not available to the previous generation,” the politician said.
He noted that in 2001, the US began investing heavily in bioweapons again, but had concerns because “violating the Geneva Convention is a crime,” so it transferred management of biological security to the US Department of Health and Human Services.
Kennedy added that the development of any biological weapon requires a vaccine, since there is a “100 percent chance” of blowback when bioweapons are used.
In a stunning revelation from February 2022, the Russian Defense Ministry unveiled the presence of 30 military biological labs in Ukraine, allegedly funded by the US with a staggering $200 million. Moscow claimed that these were only a fraction of a global network of 300 similar facilities. The US denied the allegations, escalating tensions between the two nations.
🚨BOMBSHELL: @TuckerCarlson asked @RobertKennedyJr about the shadowy biolabs in Ukraine. RFK's jaw-dropping answer, if proven true, could shake the very foundations of trust and demands unparalleled consequences for both Anthony Fauci and Ralph Baric.
The Epoch Timesrecently reported an astonishing statement by a U.S. government lawyer in a federal court in Texas, where the FDA is being sued by Dr. Paul Marik of Virginia, Dr. Mary Bowden of Texas, and Dr. Robert Apter of Arizona. The three plaintiffs claim the FDA illegally prohibited them from prescribing the drug to their patients. At a November 1 hearing, U.S. lawyer Isaac Belfer argued for the defendant:
The cited statements were not directives. They were not mandatory. They were recommendations. They said what parties should do. They said, for example, why you should not take ivermectin to treat COVID-19. They did not say you may not do it, you must not do it. They did not say it’s prohibited or it’s unlawful. They also did not say that doctors may not prescribe ivermectin.”
If Belfer’s assertion is true, it raises a very urgent question: On what legal grounds did hospitals all over the United States refuse to administer ivermectin to severely ill COVID-19 patients, even when patients and their family members begged for the drug to be administered?
If ivermectin was not prohibited by the FDA or any other U.S. medical authority for treating COVID-19, why did Dr. Paul Marik’s hospital prohibit him from administering the drug to his dying patients? Why was Dr. Mary Bowden reported to the Texas Medical Board for disciplinary action when she prescribed it? Why did many pharmacists fear losing their licenses if they filled ivermectin prescriptions for treating COVID-19?
All these patients asked for was to be allowed to try the drug (FDA-approved for River Blindness, Elephantiasis, and Scabies) for COVID-19. The patients and their kin gladly indemnified the hospitals and arranged to have their independent primary care doctors deliver and administer the drug. Nevertheless:
Hospital administrators absolutely refused to grant this wish.
Hospital attorneys fought tooth and nail against using ivermectin to treat COVID-19 patients, doing everything in their power to challenge patient lawsuits and appeal court orders to administer the drug.
Even when hospital doctors acknowledged that the patients were dying, they insisted it was better to let the disease take its natural course rather than allow patients to try ivermectin.
Even when patients’ families succeeded in getting a court orders to administer the drug, many hospitals still refused, even at the risk of being held in contempt of court.
Several readers have told us that our chapters covering this shameful scandal— Chapters 38: Begging for the Wonder Drug and Chapter 40: Graduating into Eternity—are horrifying beyond belief.
Now we hear U.S. government lawyers arguing in court that the FDA never prohibited using ivermectin to treat COVID-19 patients, but merely recommended not using it. This indicates that hospitals had no legal grounds for denying sick patients a drug that could have helped them. How is withholding medicine from a sick man any different from withholding a life ring from a man who has fallen overboard in high seas?
For families who watched their loved ones slip away after being denied the right to try ivermectin, U.S. attorney Isaac Belfer’s statement may be interpreted as declaring open season for lawsuits against hospital administrators and doctors.
Nevertheless, Dr. Marik and his co-plaintiffs, Robert L. Apter and Mary Talley Bowden, appealed the dismissal and are now being heard before a three-judge panel of the 5th U.S. Circuit Court of Appeals.
Once again, attorneys for the U.S. government are in the hot seat about their mendacious claims about the FDA’s directive to doctors and hospitals against prescribing or administering Ivermectin, either to outpatients or to patients dying in hospital.
Instead of acknowledging the obvious reality that the FDA did indeed DIRECT doctors and hospitals against administering Ivermectin, U.S. attorneys continue to insist that the FDA’s communiques were mere advice.
This preposterous argument not only overlooks the plain language of the FDA’s communiques, it also overlooks the salient fact that numerous doctors (like Paul Marik) were fired from their jobs for administering ivermectin to their dying patients, and the fact that many State Medical Boards revoked doctors’ licenses for doing the same. If these punitive actions taken against doctors were NOT based on the FDA’s directives, on what grounds were they taken?
As was just reported by Just the News columnist Greg Piper:
The 5th Circuit panel seemed skeptical of Civil Division Appellate Attorney Ashley Honold’s argument that the FDA’s “informational statements” against ivermectin, including its conflation of human and animal dosages, were “merely quips” about reported problems after “self-medicating” rather than “prohibit[ing] anyone” from using ivermectin.
Judge Jennifer Walker Elrod cited the phrase “Stop it” in the agency’s viral “You are not a horse” post on X, then known as Twitter. “If you were in English class, they would say that was a command. … That is different than ‘we’re providing helpful information,'” she told Honold.
Readers of this Substack will probably agree with my sentiment that enough is enough of lying and obfuscating U.S. government agency officials and their mercenary lawyers. It’s time for the grown-up, reasonable citizenry of this country to join Marik, Bowden, et al. in suing the pants off the FDA and other U.S. agencies against whom there is a preponderance of evidence that they have unlawfully interfered with the doctor-patient relationship and committed negligent homicide, fraud, and concealment.
Cry havoc and let slip the plaintiffs’ attorneys! Sue the FDA; sue doctors and hospital administrators; and sue the medical boards. Let them pay for the damages they have inflicted on the families of patients who were denied ivermectin until their last breaths. Let them pay for the massive damage and distress they have caused for courageous doctors like Paul Marik and his colleagues who tried to help their patients.
For quite some time the British have accepted that British Jewish organizations have hijacked the political discourse. As has happened in other Western countries, the British political establishment has engaged is a relentless rant against antisemitsm. Sometime the focus drifts for a day or two. An alleged ‘Russian nerve gas attack’ provided a 48 hour pause. Occasionally we bomb Arabs in the name of ‘human intervention’ only to realize a day or two later that we have, once again, followed a premeditated foreign agenda. But, somehow, we always return to the antisemitism debate, as if our media and politicians are a herd of flies gravitating to a pile of poop. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
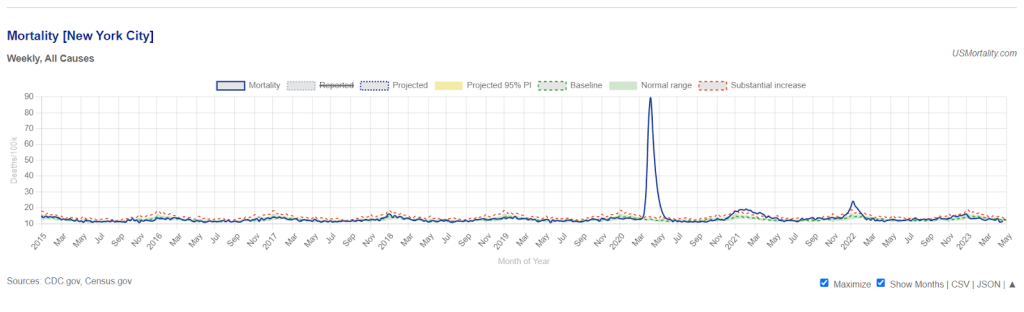
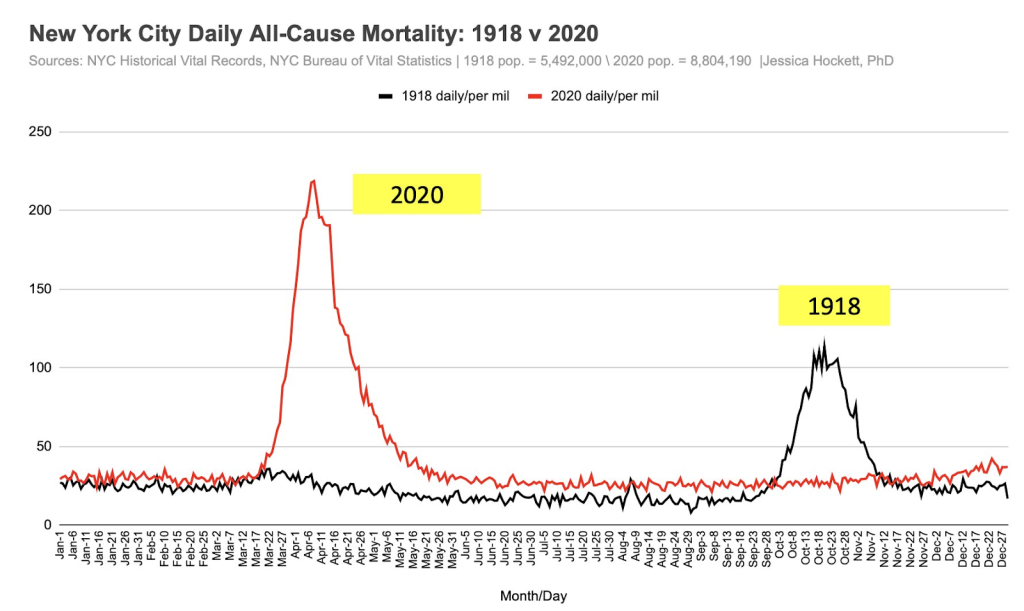
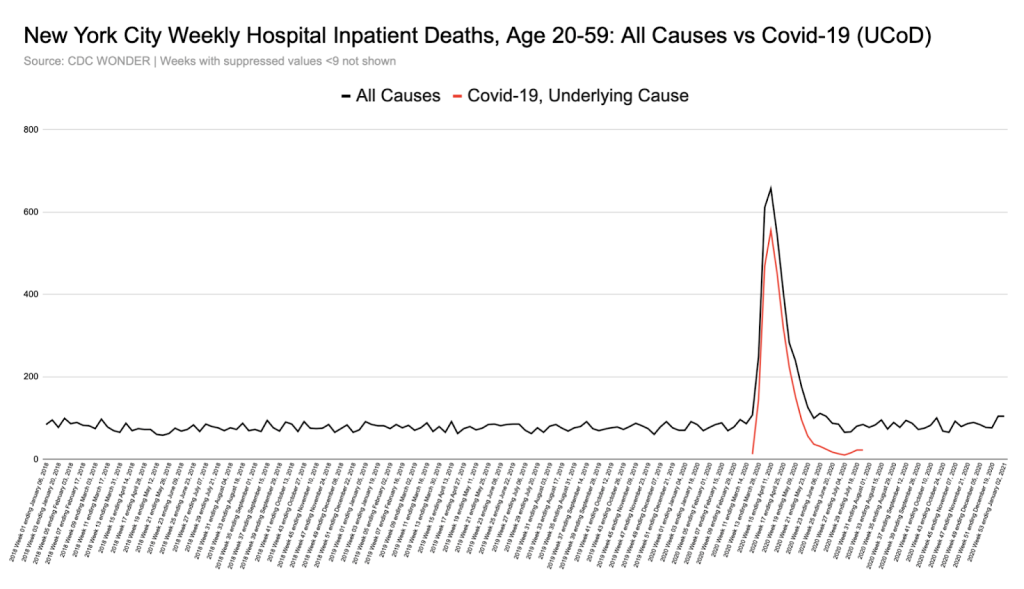
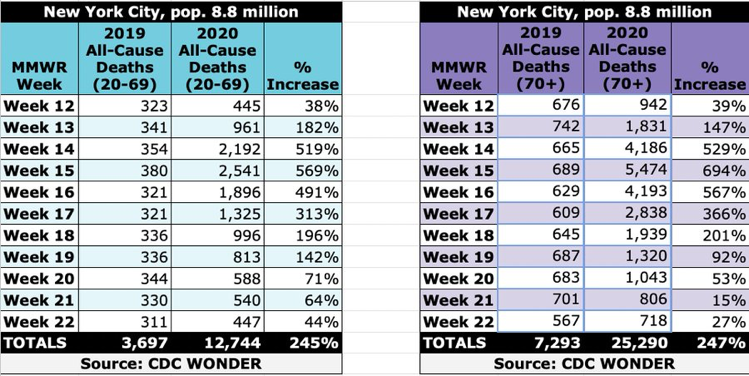
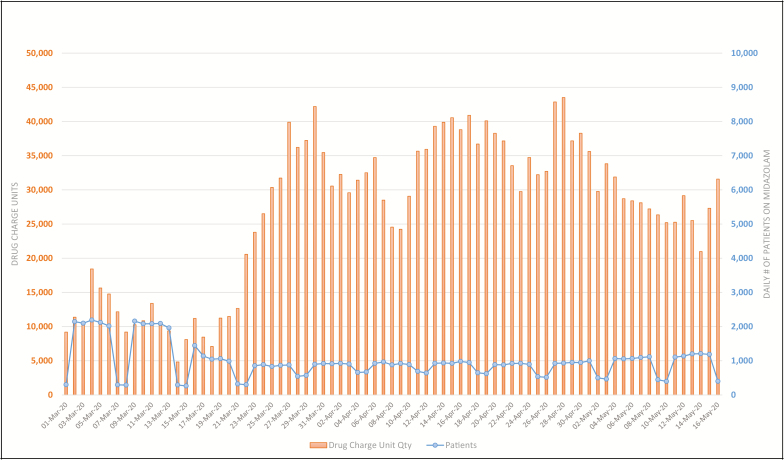
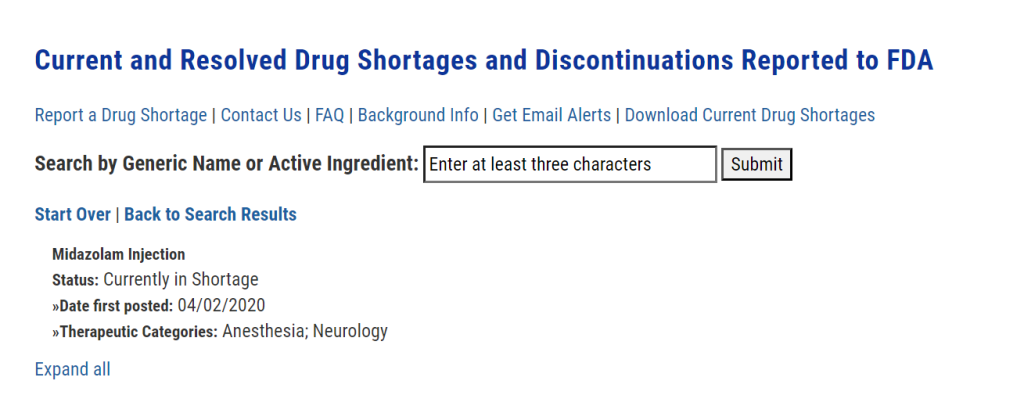
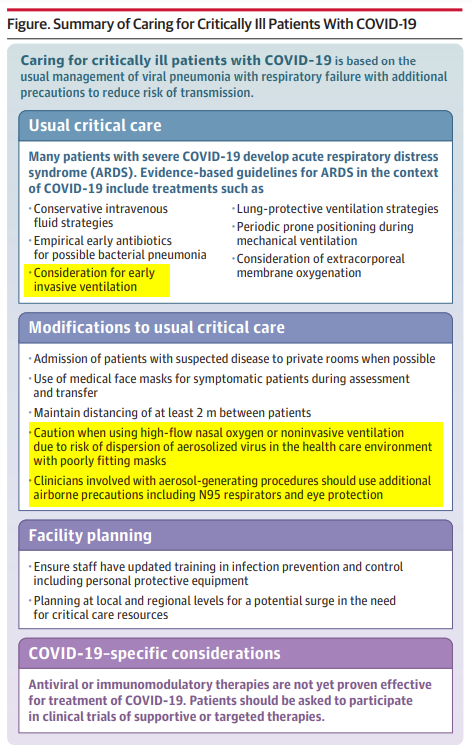





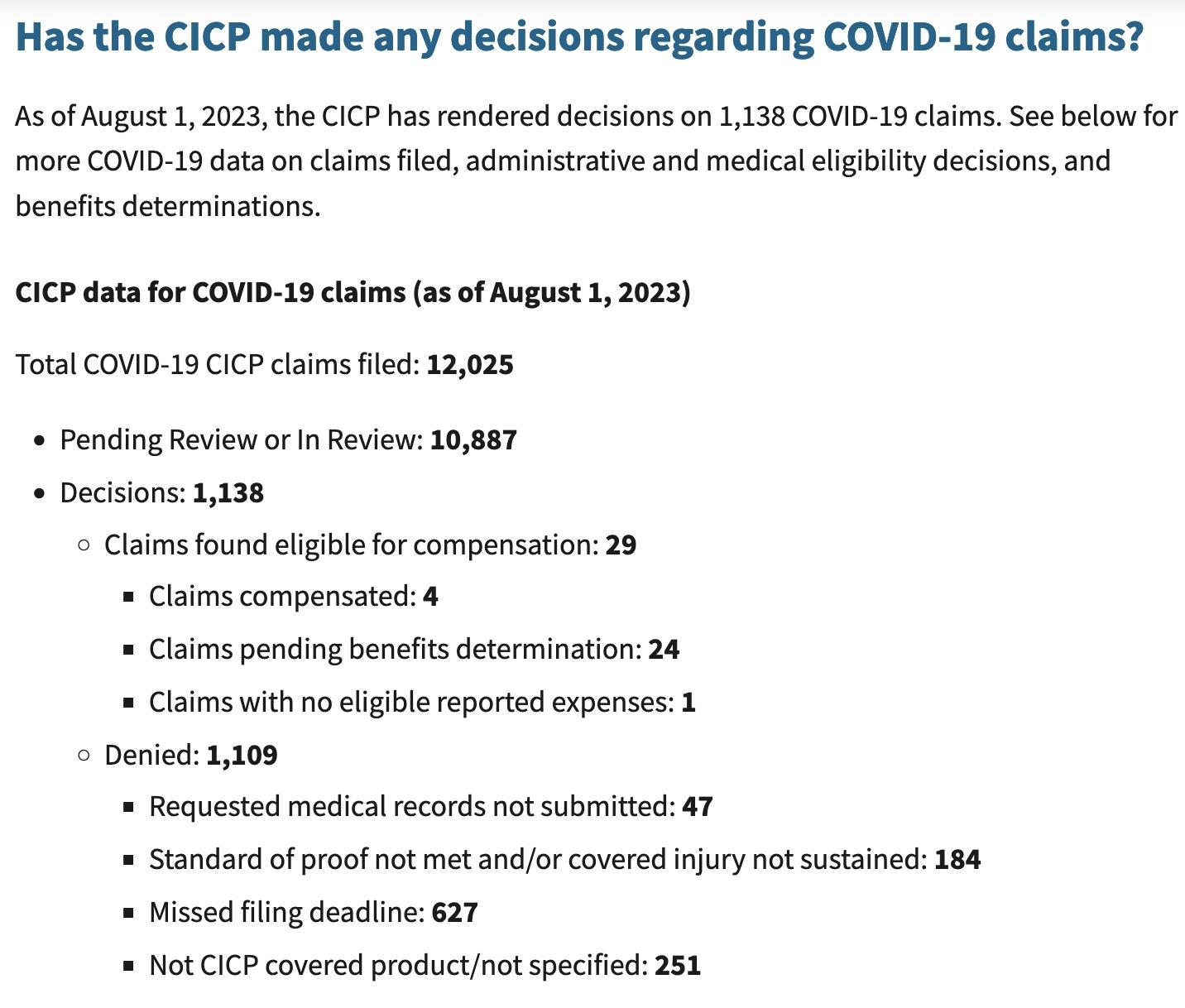



{kind=link}
{kind=link}
{kind=link}