Comirnaty, liability, and how the HHS lies, cheats and steals
By Meryl Nass, MD | December 12, 2021
I checked the Federal Register and there has been no notice that Comirnaty has been added to the National Childhood Vaccine injury Program (NVICP). I confirmed this by checking whether Comirnaty had been added to the childhood schedule, and according to the HRSA, which manages both compensation programs, it has not.
So, if you receive the licensed Comirnaty vaccine, correctly labeled as the brand-name product and not the vaccine being fobbed off as licensed product, and you are injured, you are free to sue the manufacturer for your injury. Could this be why Pfizer wrote, “Pfizer does not plan to produce any product with these new [Comirnaty National Drug Codes] and labels over the next few months while EUA authorized product is still available and being made available for U.S. distribution.”
If, however, you receive the Pfizer-BioNTech vaccine under Emergency Use Authorization, or the Moderna or J and J vaccine, you can’t sue anyone. You have the right to beg HRSA for compensation of lost wages and unpaid medical bills, period. So far, HRSA and the Countermeasures Injury Compensation Program it administers have not paid out one dime for the approximately one million injuries and 20,000 deaths reported to VAERS for any COVID vaccine.
In other words, the federal government (DHHS) has not admitted a single injury was caused by a COVID vaccine. CDC says it has not linked a single death to a COVID vaccine–not even when the patient walked into the vaccination center but got carried out to the morgue. FDA doesn’t know much about myocarditis, Bell’s Palsy, thrombosis, thrombocytopenia, pulmonary emboli, etc. There are no black box warnings on any of the COVID vaccines.
HRSA, FDA, CDC and NIH are all agencies within the federal Department of Health and Human Services. They have all gotten their stories straight. They know nothing and they are just following orders. Heil HHS!
They can’t find a doggone problem in the 20 or so databases they are spending many $millions of your money to “study.”
Want to know the biggest conspiracy in the US right now? It is the HHS.
FDA has access to a bunch of electronic databases it has termed the “BEST” Initiative, and it published a plan to use them to study heart attacks, pulmonary embolism, thrombocytopenia, etc. back in July. Where are the results, FDA? What are you waiting for? (According to CDC, “More than 459 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through November 29, 2021.”). It seems clear that we aren’t supposed to be informed of FDA’s findings until everyone possible has been vaccinated, at which point the results will be irrelevant.
In October 2020, FDA’s Steve Anderson told us there were even more databases that would be studied.
On August 23, 2021, FDA announced its databases were inadequate to assess myocarditis, so BioNTech would have to do it for them. Here is what FDA wrote about its inability to use VAERS and its many other databases:
- As noted above, the FDA acknowledges that “We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA [in other words, VAERS–Nass] will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
- Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA [in other words, FDA’s many other databases that cost the taxpayer zillions–Nass] is not sufficient to assess these serious risks.”
NOT SUFFICIENT???
Unsaid, but implied, is that if FDA is incapable of studying thousands of reported cases of myocarditis, it probably cannot study the other serious adverse events that have been reported in conjunction with COVID vaccines.
VAERS has operated for 30 years, collecting reports of vaccine adverse events. It averaged under 100 cases of myocarditis reported yearly until this year. Through November, CDC reports it received 1949 reports of myocarditis and pericarditis, in those under 30. CDC didn’t say what the total number of reports for all ages was.
Somehow, these HHS don’t seem all that concerned that the admitted reporting rate of myocarditis is over 20 times the average during the past 30 years. Why?
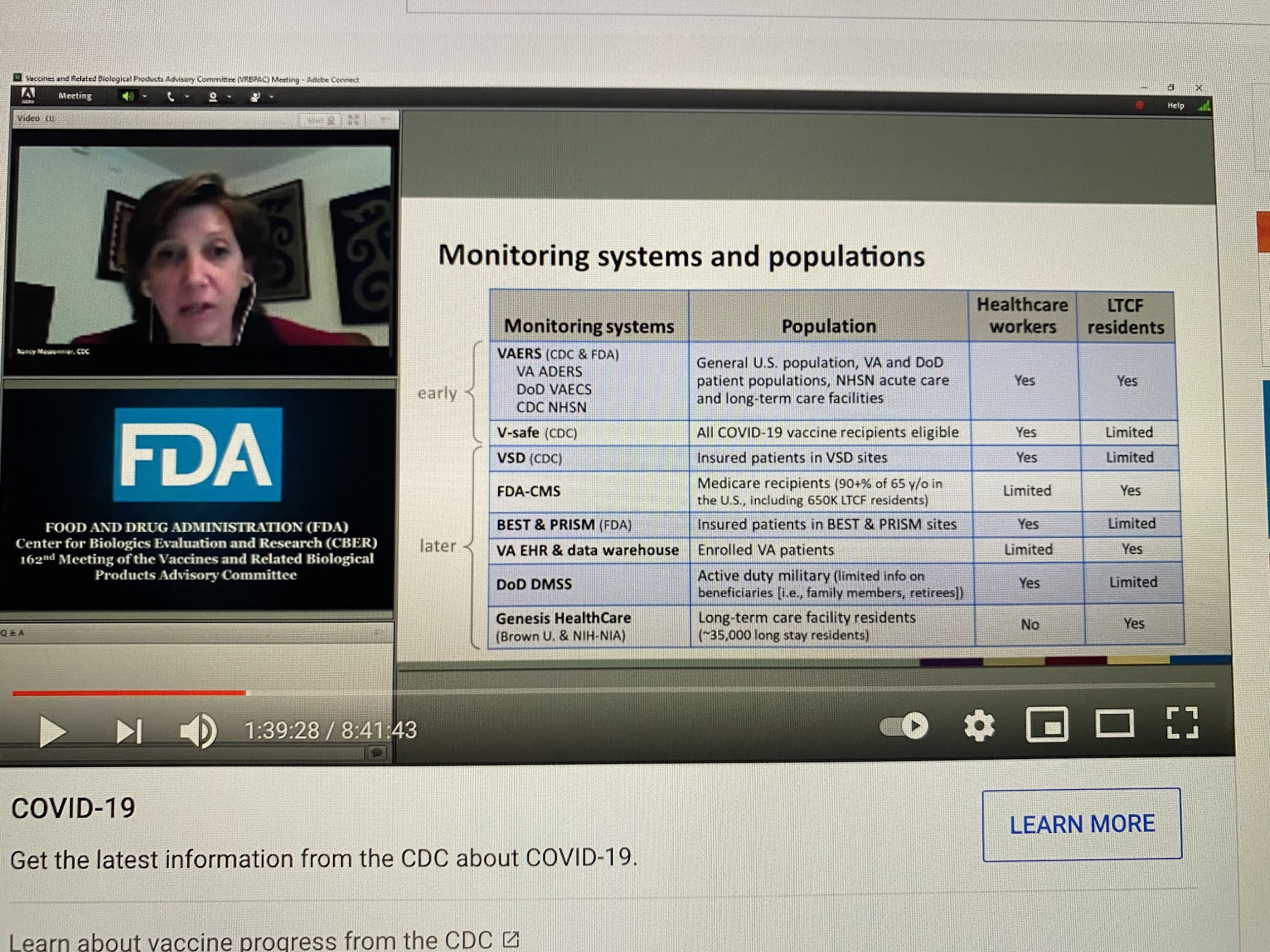
CDC has been even more shady in its analyses of safety as FDA, if that is even possible. Below, Nancy Messonier, then head of Immunizations and Respiratory Diseases at CDC, presented this list of databases that CDC would be using in the evaluation of COVID vaccine safety, on December 10, 2020. Apart from the V-safe (which they stopped talking about last January), VSD (which somehow can’t find any problems, not even myocarditis) and VAERS, all these other databases have been MIA.
NIH, whose job has never been to issue treatment guidelines, but instead to do and fund research, suddenly took over the treatment guidelines for COVID early in 2020. It formed a committee of internal and eternal “experts” to make up the guidelines. How were they chosen? That is not clear, but what is clear is that 16 of these so-called experts had current or recent financial entanglements with Gilead, the maker of remdesivir. NIH and the US Army also owned pieces of remdesivir. A number of other had financial conflicts with Merck. While NIH is the biggest single funder of medical research in the world, I cannot recall seeing a single study it funded on the safety of COVID vaccines. But somehow vaccines are its number one recommendation.
But it is not even clear that the committee is functional. The NIH has been sued to learn whether a vote was even taken by the committee regarding its ivermectin guidelines, which fly in the face of the evidence on ivermectin. How was NIH somehow authorized to issue guidelines in the first place?
Here is what has obviously occurred. All these agencies were told they had to keep quiet on vaccine problems (and perhaps problems of other COVID treatments), and they had to fiddle with their data or their analytic methods, or both, to get the required results. And there was to be NO BAD NEWS, no matter what. And no good news regarding generic treatments.
As we have seen, the so-called scientists and physicians working as bureaucrats in these agencies all caved, sucked it up, did the dirty work, kept their jobs, and betrayed their oaths and the trust of the people of the USA and the world.
2,809 Dead Babies in VAERS Following COVID Shots as New Documents Prove Pfizer, the FDA, and the CDC Knew the Shots Were Not Safe for Pregnant Women
By Brian Shilhavy | Health Impact News | December 4, 2021
The latest data dump into the U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) happened yesterday (12/3/21) and covers data through 11/26/2021.
There are now 927,740 cases reported to VAERS following COVID-19 shots for the past 11 months, out of the total of 1,782,453 cases in the entire VAERS database filed for the past 30+ years.
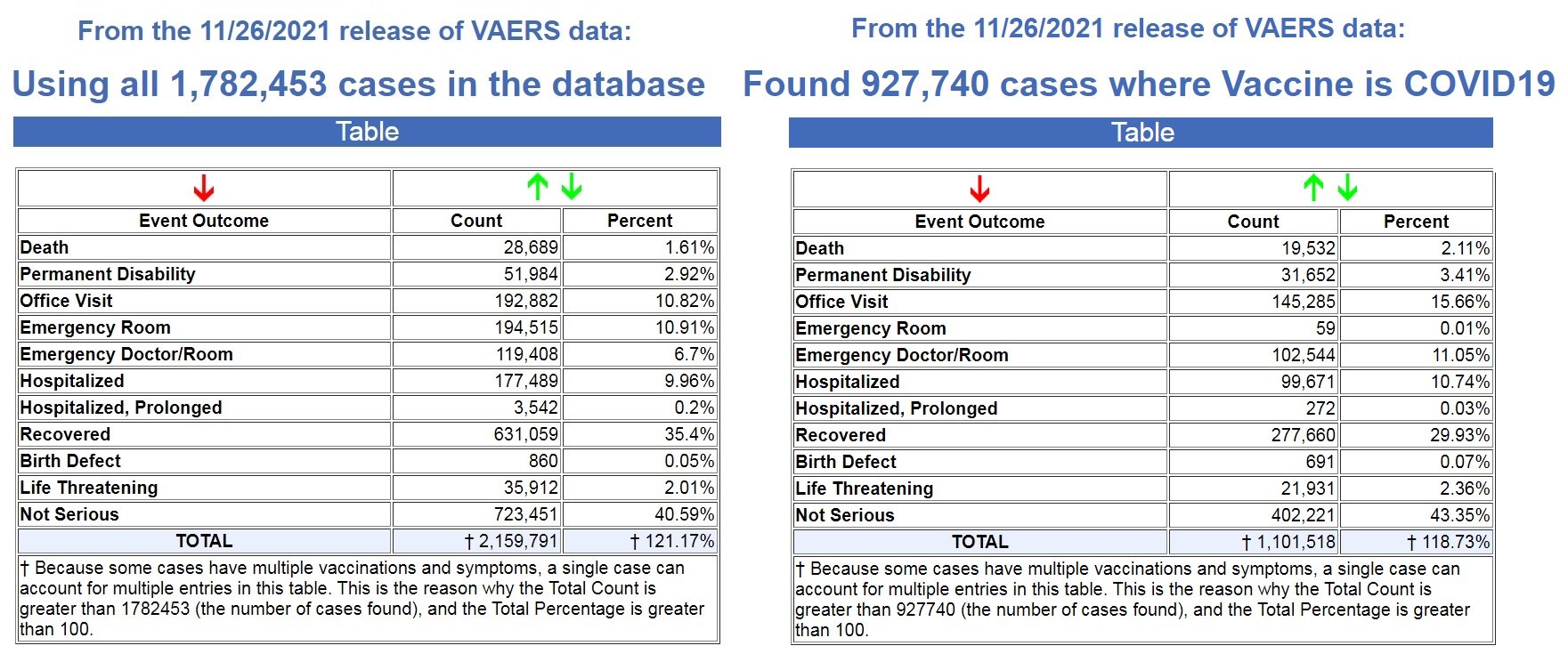
Left image source, Right image source.
That means that 52% off ALL vaccine adverse reaction cases in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
In addition, 68% of all deaths following vaccines reported in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
We are on pace to see 21,307 deaths reported in the first year following the experimental COVID-19 shots, while the average yearly deaths reported after FDA-approved vaccines for the past 30+ years is 305 deaths.
That is an astounding 86% increase in reported deaths following the COVID-19 shots, a 70X increase over the average reported deaths following vaccinations for the past 30+ years!
- FDA-approved vaccines: 305 deaths per year
- COVID-19 EUA shots: 21,307 deaths per year
And as Dr. Jessica Rose has previously reported, the under-reporting factor in VAERS for the COVID-19 shots is 41X, as a conservative number, which means that at least 800,812 people have now died following COVID-19 shots based on the VAERS data.
Most, if not all, of those deaths are being reported in the pharma-owned corporate media as “COVID” deaths, as there are now more recorded “COVID deaths” for the first 11 months of 2021 than there were for the entire year in 2020, when there were no COVID vaccines until December. (Source.)

Record Number of Fetal Deaths Following COVID-19 Shots
As of this most recent update in VAERS, we have now found 2,809 fetal deaths following COVID-19 shots injected into pregnant and child-bearing women for the past 11 months. (Source.)
By way of contrast, using the exact same search parameters in VAERS, but excluding the COVID-19 shots, we found 2,168 fetal deaths following all FDA-approved vaccines for the past 30+ years. (Source.)
That’s an average of 72 fetal deaths per year following all FDA-approved vaccines for the past 30+ years, compared to what is on pace to be 3064 fetal deaths in 1 year following COVID-19 shots.
- FDA-approved vaccines: 72 fetal deaths per year
- COVID-19 EUA shots: 3064 fetal deaths per year
That is an 80% increase in fetal deaths recorded in VAERS following the COVID-19 shots. And yet, the CDC and FDA continue to recommend these EUA shots for pregnant women and nursing mothers.
Not only do they recommend these shots for pregnant women, we now have ample evidence that they have known since earlier this year that these shots are dangerous to pregnant women, and causing fetal deaths.
In a March 4, 2021 Advisory Commission on Childhood Vaccines (ACCV) meeting, the CDC submitted a report that contained a section titled: Maternal vaccination safety summary (starting on p. 39).
They stated (emphasis mine – my comments in red):
* Pregnant women were not specifically included in pre-authorization clinical trials of COVID-19 vaccines
– Post-authorization safety monitoring and research are the primary ways to obtain safety data on COVID-19 vaccination during pregnancy
* Larger than expected numbers of self-reported pregnant women have registered in v-safe
* The reactogenicity profile and adverse events observed among pregnant women in v-safe did not indicate any safety problems (based on what criteria???)
* Most reports to VAERS among pregnant women (73%) involved non-pregnancy specific adverse events (e.g., local and systemic reactions)
* Miscarriage was the most frequently reported pregnancy-specific adverse event to VAERS; numbers are within the known background rates based on presumed COVID-19 vaccine doses administered to pregnant women (no supporting evidence to backup these claims)
It is important to note through all of this reporting by the CDC that these are based on self-reporting data from pregnant women.
We know that it is politically incorrect to blame any health issue on a COVID-19 “vaccine,” and that doctors and nurses are pressured to NOT report these, so how many pregnant women had an adverse reaction, like a miscarriage, and never even thought to link it to their COVID-19 shot?
So back in March of this year (2021), there were already major concerns about the effects of the shots on pregnant women, as “larger than expected” pregnant women were reporting adverse reactions, and “the most frequently reported pregnancy-specific adverse event to VAERS” was “miscarriage.”
Then in August of this year (2021), the CDC presented a “new study” with “new data.”
Again, this “data” is dependent on pregnant women “self-reporting” adverse reactions, so we know these reports will be well below what was actually happening in the population, as it is politically incorrect to report any adverse reactions related to the experimental COVID-19 shots. To do so is to be branded an “anti-vaxxer” and shame you for life.
The August update admitted that 13% of the pregnant women who had received a COVID-19 shot reported a miscarriage. The CDC brushed this aside by stating “miscarriage typically occurs in about 11-16% of pregnancies.”
But of course ALL miscarriages are reported somewhere in the medical files, which is why they can even come up with a number range like this. So this figure is based on 100% of the reported data, while the COVID-19 related miscarriages are only based on what was self-reported, and we have no idea how many women never reported their miscarriages because they never related it to their COVID-19 shot.
One the main studies the CDC allegedly relied upon to declare that COVID-19 shots were safe for pregnant women, was a study published in the New England Journal of Medicine on June 17, 2021.
But on October 14, 2021, they issued a statement stating that some of their data was wrong in the June 17th study. (Source.) It dealt specifically with pregnancies in their 20th week or earlier.
“No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for gestational week–specific risk of spontaneous abortion.” (Source.)
The Magical Thinking and Dangers of Masks
By Dr. Joseph Mercola | November 24, 2021
Are you prepared to wear masks forever? Some are, but their positive attitude toward masks is a likely result of deceptive and misleading information. The resulting magical thinking relating to masks has created one of the most polarized debates in U.S. history and led to anti-maskers being labeled as “grandma killers.”1
To be clear, the U.S. Centers for Disease Control and Prevention (CDC) has blatantly lied about masks’ effectiveness. November 5, 2021, CDC director Dr. Rochelle Walensky tweeted, “Masks can help reduce your chance of #COVID19 infection by more than 80%.”2
But as Dr. Vinay Rasad, MPH, a hematologist-oncologist and associate professor in the department of epidemiology and biostatistics at the University of California San Francisco, put it in the Brownstone Institute, “I don’t know how to put this politely, but it is a lie, and a truly unbelievable one at that … The idea that masks could reduce the chance of infection by 80% is simply untrue, implausible and cannot be supported by any reliable data.”3
Masks Have Meager Effectiveness, if Any
Walensky didn’t give a reference for her claim that masks reduce COVID-19 infection by 80%, but a large study4 from researchers at Yale, Stanford and the University of California Berkeley found much less impressive results from masks.
The trial involved 342,183 people from 600 villages in rural Bangladesh from November 2020 to April 2021. In villages that received masks, the number of symptomatic COVID-19 infections were 9.3% lower compared to villages without masks, or 11% lower in villages that received surgical masks instead of cloth masks.5
Why, then, hasn’t Walensky’s tweet been flagged for misinformation and targeted by “fact checkers” calling out the blatant lie? Rasad featured a tweet6 by Carnegie Mellon University mathematician Wesley Pegden, who said:7
“The head of the agency responsible for providing Americans with accurate and trustworthy information about interventions (like vaccines) that we actually know are really effective should not also be making fabricated quantitative statements in support of poorly evidenced ones.”
Antibiotic-Resistant Pathogens Live on Face Masks
While face masks continue to be recommended or mandated, little has been said about the risks inherent to covering your mouth and nose with fabric or other materials. Both cotton and surgical masks collect pathogens that may increase your risk of infectious illness — a factor that’s rarely taken into account when discussing their merits.
When researchers from the University of Antwerp, Belgium, analyzed the microbial community on surgical and cotton face masks from 13 healthy volunteers after being worn for four hours, bacteria including Bacillus, Staphylococcus and Acinetobacter were found — 43% of which were antibiotic-resistant.8
In order to best clean masks to remove the bacteria, the study found boiling at 100 degrees Celsius (212 degrees F), washing at 60 degrees Celsius (140 degrees F) with detergent or ironing with a steam iron worked best, but only 21% of survey respondents said they cleaned their cotton face masks daily.9 According to the researchers:
“Taken together, this study suggests that a considerable number of bacteria, including pathobionts and antibiotic resistant bacteria, accumulate on surgical and even more on cotton face masks after use. Based on our results, face masks should be properly disposed of or sterilized after intensive use. Clear guidelines for the general population are crucial to reduce the bacteria-related biosafety risk of face masks …”
Researchers from Germany similarly questioned whether a mask that covers your nose and mouth is “free from undesirable side effects” and potential hazards in everyday use.10 It turned out they were not and instead posed significant adverse effects and pathophysiological changes, including the following, which often occur in combination:11
- Increase in dead space volume
- Increase in breathing resistance
- Increase in blood carbon dioxide
- Decrease in blood oxygen saturation
- Increase in heart rate
- Decrease in cardiopulmonary capacity
- Feeling of exhaustion
- Increase in respiratory rate
- Difficulty breathing and shortness of breath
- Headache
- Dizziness
- Feeling of dampness and heat
- Drowsiness
- Decrease in empathy perception
- Impaired skin barrier function with acne, itching and skin lesions
Mask-Induced Exhaustion Syndrome Is Prevalent
The study referred to this cluster of symptoms as mask-induced exhaustion syndrome (MIES) and warned that children, pregnant women and those who are sick or suffering from certain chronic conditions may be particularly at risk from extended masking. While short-term effects include microbiological contamination, headaches, exhaustion, carbon dioxide retention and skin irritation, the long-term effects may lead to chronic issues:12
“Extended mask-wearing would have the potential, according to the facts and correlations we have found, to cause a chronic sympathetic stress response induced by blood gas modifications and controlled by brain centers. This in turn induces and triggers immune suppression and metabolic syndrome with cardiovascular and neurological diseases.”
Further, “it can be assumed,” they wrote, “that the potential adverse mask effects described for adults are all the more valid for children: … physiological internal, neurological, psychological, psychiatric, dermatological, ENT, dental, sociological, occupational and social medical, microbiological and epidemiological impairments …
The masks currently used for children are exclusively adult masks manufactured in smaller geometric dimensions and had neither been specially tested nor approved for this purpose.”13
Again, in taking on these unknown risks — both short- and long-term — to wear masks, the benefits are highly questionable and intended to thwart a pathogen with a low death rate for most populations:14
“[R]ecent studies on SARS-CoV-2 show both a significantly lower infectivity and a significantly lower case mortality than previously assumed, as it could be calculated that the median corrected infection fatality rate (IFR) was 0.10% in locations with a lower than average global COVID-19 population mortality rate.
In early October 2020, the WHO also publicly announced that projections show COVID-19 to be fatal for approximately 0.14% of those who become ill — compared to 0.10% for endemic influenza — again a figure far lower than expected. On the other hand, the side effects of masks are clinically relevant.”
‘The Mask of Your Enslavement’
 It’s clear that the evidence in support of masks for physical protection against disease is lacking, while their potential for psychological harm is immense. Brownstone Institute highlighted the story of folk saint Escrava Anastácia, a slave of African descent who lived in Brazil during the 19th century.15
It’s clear that the evidence in support of masks for physical protection against disease is lacking, while their potential for psychological harm is immense. Brownstone Institute highlighted the story of folk saint Escrava Anastácia, a slave of African descent who lived in Brazil during the 19th century.15
She was forced to wear a metal, muzzle-like mask during her lifetime in order to silence her from speaking out about the oppression and injustice she was facing. As written by Roberto Strongman, associate professor in the department of black studies at the University of California, Santa Barbara:16
“The apparition of Anastásia at anti-lockdown rallies represents an opportunity to understand the current medical tyranny as a form of enslavement and to forge links of solidarity between communities whose freedom is threatened across all racial groups. The claim of cooptation deserves to be unpacked for a valid claim of cultural usurpation could easily work towards severing important alliances in a divide-and-conquer model.
While there are clear specificities between the suffering of Africans under the system of chattel slavery and the deprivation of civil liberties endured by most citizens around the world during the current pandemic panic, Anastásia reminds us of certain transhistorical constants in the process of dehumanization and subjugation of populations through the gagging and muzzling of their bodies to quell their protestations.”
Strongman pointed out several undeniable reasons why face mask mandates “fashion the citizenry as slaves” and act as symbols of enslavement. Among them, they:17
- Lead to oxygen deprivation, promoting a state of physical and mental weakness
- Are symbols of submission and used as part of master-slave dynamics
- Enforce the creation of a carceral culture
- Erase personhood and homogenize the masses — “The collectivized wearing of masks results in an enforced uniformity in which the individual cedes way to the nameless collectivity as the neo-meta citizen.”18
- Are theatrical and act to conceal identities, rendering us alien to others and ourselves
- Delete facial expressions and inhibit nonverbal communication, including that necessary for social organization that can lead to revolution
- Reduce verbal output
- Are visible displays of allegiance to the “system of medicalizing technocratic control”
- Are part of preparing individuals for new societal roles — “However transitory the current regime of face masking might be, the population must face that we are beingforced to undergo a rite of passage, a process of resocialization into the new normal.”
- Promote a culture of fear
- Act as deterrents of solidarity by making your neighbor into a “nameless pathogenic vector instead of your ally”
Magical Thinking on Masks
In addition to flat-out lies, the CDC also makes nonsensical statements, like this: “Cloth masks will not protect you from wildfire smoke … They might not catch small, harmful particles in smoke that can harm your health.”19
But we are to believe that they will protect us from an aerosolized virus? “The virus is 25X smaller than a smoke particle,” wrote Steve Kirsch, executive director of the Vaccine Safety Research Foundation. “So it’s like trying to stop a mosquito with a chain link fence.”20
Yet magical thinking — the belief that you can influence outcomes by doing something that has no causal connection to them — persists. Robert Dingwall, a consulting sociologist, questioned why the U.K.’s Health Security Agency expert panel used only a second-class evidence base that failed to demonstrate clear benefits on which to base their conclusion that face masks in the community help reduce transmission. He wrote:21
“The state of the face mask debate is rather as if Galileo had published his account of the heliocentric universe and then included a paragraph at the end telling the reader to ignore all the evidence because the Church had declared that everything revolved around the Earth.
In the absence of better-quality work — and we must ask why that research has not been done — some of the claims for face masks look much more like magical thinking than anything that demonstrates the sort of casual connection that might be recognizable as science.”
As the pandemic stretches on, science continues to be ignored and recommendations are primarily pushed based on emotional justifications and triggers. If science were actually followed, universal mask wearing by healthy people would not — indeed could not — be recommended.
In the beginning, health officials did, in fact, advise against masks for healthy people,22 but somewhere along the way — early on — they flip-flopped. Why? According to Strongman:23
“Just as masks function as liminal artifacts in rites of passage and as part of animal training, these covid mask are harbingers of further intrusions to our integrity.
Wearing the masks is just one step away from receiving the shots, then accepting the vaccine passports and the implantable neural links until one’s original persona is buried by a cyborg. The masks function as an empirical compliance test for the projected acceptability of future corporeal technologies of control. Where will you draw the line?”
Sources and References
- 1, 20 Steve Kirsch Newsletter November 7, 2021
- 2 Twitter, Rochelle Walensky November 5, 2021
- 3, 6 Brownstone Institute November 7, 2021
- 4 The Impact of Community Masking on COVID-19: A Cluster-Randomized Trial in Bangladesh November 8, 2021
- 5 ABC Action News September 1, 2021
- 7 Twitter, Wes Pegden November 5, 2021
- 8, 9 Frontiers in Medicine September 3, 2021
- 10, 11, 12, 13, 14 Int J Environ Res Public Health. 2021 Apr; 18(8): 4344
- 15 History Collection December 13, 2018
- 16, 17, 18, 23 Brownstone Institute November 4, 2021
- 19 U.S. CDC, Wildfire Smoke and COVID-19
- 21 Social Science Space October 25, 2021
- 22 Life Site News July 31, 2020
CDC Redefined Vaccine to Support Deficient Fake Vaccines Sold by Drug Companies
By Joel S. Hirschhorn | November 14, 2021
The CDC once was a federal agency that nearly everyone respected. That no longer is the case. Now there are many reasons why the CDC should be widely disrespected. Its latest debacle is how it changed the definition of vaccine.
Just imagine this: The entire push for COVID “vaccines” was based on a lie – they did not meet the official CDC definition of a vaccine. By doing this, the government could coerce the entire population to get the shot. Calling them “vaccines” was the biggest lie from Fauci and the key to drug companies making many billions of dollars.
Why would the government’s key public health agency change the definition of what a vaccine is in the midst of a pandemic? After millions of Americans have taken the shot? And millions more are being beaten into taking it for the first time and others to get booster shots.
Words matter
Here is the key point. It became widely recognized by medical experts and informed citizens that COVID vaccines clearly did not fit the official CDC vaccine definition. The CDC thought the answer was not to fix what was deficient with the COVID vaccines or stop their use by most people as so many medical experts advised. Their response was to change the vaccine definition to fit the so-called vaccines.
This was done so that vaccine mandates could keep getting pushed by the government. Of course, the COVID “vaccines” should be referred to as gene therapy products, even better than calling them experimental vaccines.
To see how corrupt this action by the CDC was, it is necessary to examine the details of the vaccine definition debacle.
Prior to September 1, 2021 here is how CDC defined vaccine:
A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease. Vaccines are usually administered through needle injections, but can also be administered by mouth or sprayed into the nose.
This definition had been used for years and it makes sense. No expert or sensible citizen would find fault with it. But did it honestly apply to the COVID vaccines?
Then this is what the CDC concocted:
A preparation that is used to stimulate the body’s immune response against diseases. Vaccines are usually administered through needle injections, but some can be administered by mouth or sprayed into the nose.
Here is what the CDC also said:
Immunity: Protection from an infectious disease. If you are immune to a disease, you can be exposed to it without becoming infected.
Think about that last sentence: You can be exposed to COVID without being infected; but we know that is not true for fully vaccinated people who still get infected.
This is the key language in the original definition:
“stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.”
How rational to invoke the purpose of a vaccine to stimulate an immune system to produce immunity to a specific disease that protects the recipient from that disease. Exactly what everyone for years thought was the correct way to think about a vaccine. People want permanent protection from the COVID infection disease.
But now the CDC has taken out the language referring to getting immunity for a specific disease and getting protection from that disease.
Now, COVID vaccines do not have to directly produce immunity. No, now they only have to stimulate the body’s immune system.
You don’t get immunity because COVID vaccines do not directly produce immunity. They do not directly kill the COVID virus. Vaccinated people can still have high viral loads and also transmit the virus to others. While some individuals may get some health benefits from COVID shots, they do not necessarily protect the entire population. This is why mandates to get everyone the shots really do not make sense from a public health perspective, that Dr. Paul Alexander has well substantiated.
Apparently, the only logical way to understand what the CDC has done is to accept the truth belatedly seen by the CDC that COVID vaccines do not, in fact, produce effective immunity for COVID infection and do not provide effective protection, once vaccinated, from that infection.
Much of the public surely does not yet know what the CDC has acknowledged for the COVID vaccines. Odds are that everyone who depends on mainstream media for good information about the pandemic has not been informed about what the CDC has done and its implications.
The new vaccine definition, if publicly known, would reduce public confidence in current COVID vaccines. You don’t have to be a medical expert to see how the new definition has been created to accommodate COVID shots.
In fact, these definition changes reflect what is now known about the limitations of the COVID vaccines.
Fully vaccinated people can still get COVID disease, referred to as breakthrough infections that, contrary to what the government says, can be very serious, often requiring hospitalization and sometimes causing death, as was the case for Colin Powell. Such serious effects have been well discussed by Dr. Günter Kampf. Other times, breakthrough infections greatly disrupt lives, as recently described by Madrigal, a strong proponent of COVID shots.
Moreover, the COVID vaccines are now widely known from considerable clinical evidence to lose their effectiveness typically in about six months. And even worse, they do not provide hardly any protection against variants like the delta variant. Same disease but from a different virus in terms of its complex genetic makeup. So, befitting the new CDC definition the COVID shots really do not have long lasting effective immunity to the specific COVID infection caused by all variants.
Elsewhere on the CDC website is a glossary of many terms; here is what is especially relevant to the debate about COVID vaccines:
Attenuated vaccine: A vaccine in which a live microbe is weakened (attenuated) through chemical or physical processes in order to produce an immune response without causing the severe effects of the disease. Attenuated vaccines currently licensed in the United States include measles, mumps, rubella, varicella, rotavirus, yellow fever, smallpox, and some formulations of influenza, and typhoid vaccines.
Most people would read this and find that it fits with what they think of as vaccines that have been routinely taken by most people, especially children. Clearly, COVID vaccines do not fit this definition. But seeing this established view of vaccines helps explain why so many people resist and reject the COVID shots. They are so fundamentally different than long accepted and used vaccines.
Natural immunity
One of the biggest pandemic scandals is that the government refuses to give full credit to natural immunity that people get from once being infected by the COVID virus. It should be officially recognized as equivalent to “vaccine” immunity.
The following CDC glossary definition is especially relevant:
Active immunity: The production of antibodies against a specific disease by the immune system. Active immunity can be acquired in two ways, either by contracting the disease or through vaccination. Active immunity is usually permanent, meaning an individual is protected from the disease for the duration of their lives.
This CDC definition of active immunity recognizes that you can get it by contracting the disease versus through vaccination. In other words, it recognizes what today is commonly called natural immunity achieved by once being infected by the COVID virus. And that such immunity is likely permanent and better than vaccine immunity, as recent clinical studies substantiate. But it also infers that active immunity obtained through vaccination is also permanent, which clearly is not the case for COVID shots, as evidenced by breakthrough infections.
Also note that it has recently been revealed that the CDC has not been able to provide any proof of at least one instance of an unvaccinated, naturally immune individual transmitting the COVID-19 virus to another individual.
And a new study found that almost 60 percent of the people with antibodies had no idea they had even had COVID at all. But they would have natural immunity. Quite consistent with the reality that most people suffer no significant health impacts from being infected with the COVID virus, regardless of all the fear mongering by Fauci and others.
Conclusions
To sum up, a close look at what the CDC has done lately reinforces the thinking of millions of people who have reservations and concerns about getting COVID genetic therapy shots that pose myriad adverse impacts and sometimes death.
There is a rational, science basis for thinking that the limited benefits of those shots do not adequately offset their risks. This is true for the vast majority of healthy people, especially children, who have extremely low risk from COVID infection for serious illness, hospitalization or death.
Mandates that do not recognize natural immunity are merely a sham tactic to make money for drug companies.
How interesting it would be, in the context of informed consent, if people were shown the original and new CDC vaccine definitions as a means to stimulate productive discussion with medical providers of COVID shots.
Dr. Joel S. Hirschhorn, author of Pandemic Blunder and many articles, podcasts and radio shows on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.
New VAERS analysis reveals hundreds of serious adverse events that the CDC and FDA never told us about
Serious adverse events that are more elevated than myocarditis. New VAERS analysis by Albert Benavides blows the “safe and effective” narrative away.
By Steve Kirsch | November 9, 2021
The CDC and FDA have said the vaccines are “safe and effective.” They haven’t found any serious issues with the COVID vaccines. Zero. Zip. Nada. It was the DoD that found myocarditis.
The evidence in plain sight shows that they are either lying or incompetent. Or both. But of course, the medical community is never going to call them on this.
So that’s where our team of vaccine safety experts comes in; to reveal the truth about what is really going on.
In a brand new VAERS data analysis performed by our friend Albert Benavides (aka WelcomeTheEagle88), we found hundreds of serious adverse events that were completely missed by the CDC that should have been mentioned in the informed consent document that are given to patients. And we found over 200 symptoms that occur at a higher relative rate than myocarditis (relative to all previous vaccines over the last 5 years). All together, there were over 4,000 VAERS adverse event codes that were elevated by these vaccines by a factor of 10 or more over baseline that the CDC should have warned people about.
As of November 1, 2021, there have been more adverse events reported for the COVID vaccines than for all 70+ vaccines combined since they started tracking adverse events 30 years ago. That’s a stunning statistic, nobody can deny it, but nobody in the mainstream medical community (or mainstream media) seems to care much. It’s not even worth noting in passing. Wow.
Here’s what the evidence shows:
- The COVID vaccines are the most dangerous vaccines in human history. They are 800 times more deadly than the smallpox vaccine which was the previous record holder. The vaccines have killed over 150,000 Americans and permanently disabled even more. They don’t make sense for anyone of any age. The younger you are, the worse it gets. For kids, it is estimated that we kill 117 kids for every COVID death we prevent.
- The Pfizer 6 month trial showed the drug can save 1 life for every 22,000 people vaccinated. It also appeared from the trial that the drug killed more people than it saved (there were 20 deaths in the treatment group vs. 14 in placebo after unblinding). So we are “saving” fewer than 10,000 lives at the expense of over 150,000 deaths. In short, we kill 15 people to save 1. That’s incredibly stupid. But nobody in the Biden administration wants to meet with our team. They basically don’t want to hear the truth. Instead, they focus on deplatforming and censoring us which are techniques that are effective when the data doesn’t work out for you.
- Both the FDA and CDC have proven inept in spotting safety signals. They can’t even compute the VAERS URF which is a number that is required for any serious risk-benefit analysis. So the FDA and CDC outside committee members are all flying blind in approving the vaccines. Even after this deficiency is pointed out in the public comments by yours truly (and direct emails to the committee members), it makes no difference. We are ignored. The CDC safety monitoring is so bad that they even admitted at the last ACIP meeting that it was the DoD that spotted the myocarditis signal. So the FDA and CDC have basically been batting .000 in terms of spotting safety signals that have been sitting in plain sight the entire time.
- They can’t admit that they missed the signals now because that would be an admission they missed them before. So they will try to discredit this article with ad hominem attacks (this is a technique used to win an argument when you cannot win on the evidence).
- The serious events we highlight below are all consistent with the mechanism of action that Robert Malone and I first described in the Darkhorse podcast. Namely, that the spike protein that is produced in response to the delivery of the mRNA is cytotoxic and results in blood clots, inflammation and scarring throughout your body which then creates a wider range of severe adverse events than any vaccine in human history.
- The medical community is trained by the CDC to believe the vaccines are safe, so they interpret all the adverse events as not vaccine related. But if it wasn’t the vaccine that caused all these events, what was it? What’s worse is they tell their patients, “this is all in your head” or that “your baby died because you had a genetic defect.”
- In general, patients believe their doctors and never figure out where to get a cytokine panel to discover that they are vaccine injured (go to www.covidlonghaulers.com to get the cytokine panel and IncellDx to get the spike protein assay). So people never learn how to rid their body of the spike protein either (see my article on vaccine treatment for the drugs they use to do this) which is the first step in the road to recovery.
- The high adverse event rates aren’t “excess reporting.” It is due to excess events. For example, one neurologist had 0 cases of vaccine adverse events in her entire career, but this year, she has 2,000. Another physician I know has had 0 events in 29 years in his 700 patients. This year he needs to report 25 events. Physicians themselves have experienced stunningly higher incidence rates of reproductive, neurological, and cardiac events since the vaccines rolled in 2021. We couldn’t find a single cardiologist who actually had fewer cases of myocarditis after the vaccines rolled out as the members of the FDA and CDC claim.
- The serious events are primarily centered around menstruation, blood clots, inflammation and scarring, cardiovascular damage, and neurological damage, just as we predicted in the podcast in June of 2021.
- There are hundreds of serious adverse events that are caused by these vaccines. This of course is shocking to people since the CDC has repeatedly said you can’t ascribe causality to data in VAERS. Not true. The VAERS data analysis (temporal data, the dose dependency, and the elevated reporting rates compared to baseline) provide ample signal to enable us to show causality on all of these events using the five Bradford-Hill criteria applicable to vaccines.
- Nicki Minaj was right to complain about elevated rates of testicular swelling, impotence (erectile dysfunction), and orchitis. Every world authority who opined on the matter belittled her and said she was wrong, but all the symptoms she talked about are strongly elevated as you’ll see from the data below. None of these so-called experts of course ever looks at the data; it’s all based on arguing from their belief system rather than the scientific evidence. And even if those authorities disagreed with the VAERS data, it was irresponsible not to have pointed out the raw data to people and then explain why they totally ignored the elevated signal in the VAERS data. Today, we do science based on our belief system rather than the old-fashioned way of looking at what the data actually says. Our team is old-fashioned.
- There is a pretty good chance that the vaccines don’t really work at all and never did. We know the Pfizer Phase 3 trials were gamed in many ways. There is no doubt that the vaccines elevate antibodies, but it seems that it is quite possible that the immunity they confer is actually the result of killing off (or excluding as in the case of the trials) people with weaker immune systems. The people who are left are thus more resistant to the virus. Mathew Crawford will be coming out shortly with an analysis that makes a compelling case for this novel hypothesis. Subscribe to his substack here.
- It is unlikely that anyone in the world will want to debate us publicly on any of the claims above (or on any of my articles or on any of Mathew’s articles), but if you are a prominent supporter of the false narrative and want a public debate, we are here for you. Our team would be thrilled to accept the challenge as we have no desire to spread misinformation. If we got it wrong, we are happy to correct our mistakes if you can explain to us clearly the mistake we made and the correction you suggest (e.g., the “right” answer). Yet even with multiple million dollar incentives (listed in this article), nobody seems to be interested in showing how we got it wrong. Everyone talks about how bad the vaccine misinformation problem is, but nobody is willing to do anything to show that we got it wrong. For example, I’ve asked any prominent scientist in America who disagrees with my analysis (showing eight different ways to validate that over 150,000 Americans have been killed by the vaccines) to let me see their “correct” analysis showing the “correct” number, but nobody will. They won’t even come on a recorded call to show us how we got it wrong. It’s baffling. They all want to do it in slow motion via documents because that way it’s easier to obfuscate the truth and they can avoid answering questions. The latter is key.
- It’s really easy to tell who is telling you the truth here. John Su is the CDC expert on VAERS. If he’s wrong, the entire narrative falls apart. I personally attacked Dr. Su in a widely read article accusing him of being corrupt. I offered to publish his response in the article. He said nothing. I offered to debate him. No dice. TrialSiteNews tried to interview him. He refused to reply. Seriously? If the CDC gave us 2 hours to ask John Su questions, we would destroy his credibility and the credibility of the CDC. That’s why he’s not talking and that’s why the CDC will never let him talk to anyone on our team. Because we don’t ask softball questions like what John gets at the ACIP meetings. We play hardball.
What we found in the VAERS analysis below can be verified by anyone because it is all publicly accessible. Albert spent only a few hours to produce the tables. So the CDC should have been able to do the same work Albert did.
You can easily verify any entry yourself via manual queries to any VAERS interface (my favorite is MedAlerts, but others such as openvaers and the HHS site give the same results).
Before we get to Albert’s analysis of the VAERS data, let’s do a little background.
The Darkhorse Podcast
On June 10, 2021, my friend Robert Malone and I appeared on Bret Weinstein’s Darkhorse Podcast to tell the world what we had learned about the COVID vaccines. You can watch the 3 hour version here or the condensed 1 hour version here if you haven’t already seen it. I highly recommend the whole thing; I know a lot of people who watched it multiple times and raved about it.
Basically, we said the COVID vaccines were super dangerous, they had killed a lot of people at the time, the Pfizer bio-distribution data that Dr. Byram Bridle obtained from the Japanese government using a FOIA request showed the lipid nanoparticles delivered a very substantial dose of mRNA to female ovaries, and that the spike protein that is subsequently produced causes blood clots, inflammation, and scarring leading to a large number of cardiovascular and neurological symptoms, a number of which would be irreversible. Robert in particular noted that we had no clue about the amount, dose, and duration of the spike protein that is produced (we still don’t) because this testing was never done in animals (they looked only at the distribution of the nanoparticles which is not the same thing). Bret referenced a very long article I had written on May 25, 2021 for TrialSiteNews entitled “Should you get vaccinated?”
For reference, here is the bio-distribution graph that Bret showed in that podcast:

See anything wrong? Note that we deliberately omitted areas of the body where the vaccine was expected to accumulate in order to highlight areas of the body where it wasn’t supposed to go. Naturally, those supporting the mainstream narrative that the vaccines are safe and effective went into overdrive to suppress the episode and discredit what we said. They said we were dishonest not to include everything in the chart. YouTube censored the video after nearly 1M views. Wikipedia accused both of us of spreading misinformation and then blocked me when I tried to point out that the scientific evidence supported what I said. Wikipedia relies on fact checks for science.
We were right about everything we said in the podcast, and now, thanks to the work Albert did, it’s now easier to see we were telling the truth: the top elevated events were neurological, cardiovascular, and related to the female reproductive system, just like we said. I was stunned at the sheer number of menstrual events that made it to the very top of the list. That was a surprise to me.
Openvaers has been highlighting the damaging effects on both male and female reproductive systems for months with a page dedicated to reproductive health, but the medical community, Congress, and mainstream press wasn’t paying any attention at all. These event counts are not normal, but nobody really seems to care. President Biden not only doesn’t care; he wants to force all our kids to be vaccinated with the most dangerous vaccine in human history.

With the new analysis, the counts are much easier to interpret because instead of being just raw counts, they are numbers relative to a baseline rate so we can instantly see what symptoms are “abnormal” meaning 10X or more higher than “expected.” The answer: over 4,000 adverse events.
The X factor analysis (November 7, 2021)
Before I give you the link to the spreadsheet of VAERS symptoms sorted by X factor, you need to know a few things to properly interpret the data.
First, let’s address the myth that is promoted by the FDA that the VAERS database is “over reported.” As we said above, there are more events this year than any previous year, so that’s why the events are up. But there still could be a component of overreporting as well, i.e., that people this year are more likely to make a report on an event compared to last year since everyone is so “highly aware” of the vaccines. Nice theory. No data to back it up. Nobody making that argument has ever included any data to back up their assertion. We call that a hand-waving argument. Doctor surveys we’ve done show that, if anything, they are less likely to report an adverse event this year for a variety of reasons (hospital frowns on it, no time, still too frustrating, too many events to report). The other way we can tell is to look at the rates of events that are not comorbidities or causal. We find that events like Musculoskeletal pain, Screaming, Head banging, Local reaction, Diet refusal, Croup infectious, Hepatitis A, Eyelid oedema, and more occur at pretty much the same rate this year as in previous years.
Now let’s tackle the columns:
Symptom
This is the VAERS symptom name. These are coded by HHS upon receipt of the report based on the contents of the report. Some of these symptoms are tests that are ordered. An elevation of a test is a good signal something is amiss. Other symptoms are not causal, but are comorbidities. For example, it might be that diabetes is there more often not because it makes diabetes worse, but because diabetic people are more likely to report symptoms. So for these symptoms, we have to be careful about the analysis. But for many of these symptoms such as cancer, herpes zoster (shingles), diabetes and more, these are all exacerbated by the vaccine as we know from talking directly to doctors. Finally, some symptoms like “rib fracture” or “suicide” are elevated because they are caused by the vaccine. For example, the vaccine can make you lose consciousness and fall and fracture your hip. The vaccine can give you tinnitus which is so bad that you want to kill yourself. So we have to be extremely careful to examine each one of these symptoms carefully because in most cases, we’ll find that they are indeed caused by the vaccine. I’ve coded a bunch of symptoms red that I thought were serious/interesting. I’m not done yet, so the redness coding was only methodically done on the first 100 symptoms and sporadically after that. When I get more time, I’ll go through them and update the file. Note that myocarditis is located on row 274, i.e., way way down.
Also, when looking at deaths, we never look at a “symptom” of death since death is coded in a separate field. So the event count for the “death” symptom (6,487) is lower than the over 8,000 domestic deaths.
Guillain-Barre syndrome is only elevated by a factor of 6 from baseline, likely because other vaccines also elevate GBS; this vaccine elevates it even more.
C19 count
This is the raw number of VAERS events in 2020 and 2021 due to the COVID vaccines for that symptom. The key here is that this count should be multiplied by 41 (known as the underreporting factor or URF to estimate the absolute number of events that occurred). See this article for how that is computed.
Baseline count
The baseline rate is the # of incidents occurring in a 5 year period from 2015-2019 for all vaccines given in that time period.
X-factor
The X-factor is the (C19 count*5/Baseline count). This is because the baseline is 5 years so we compare the COVID counts in a year vs. the average count in a typical year. So an X-factor of 10 or more would mean that the symptom is very likely to be caused by the vaccine since it is highly elevated from the “normal” rate.
Now let’s tackle the tabs. There are two tabs:
match tab
On the match tab are symptoms where the baseline count !=0
no match tab
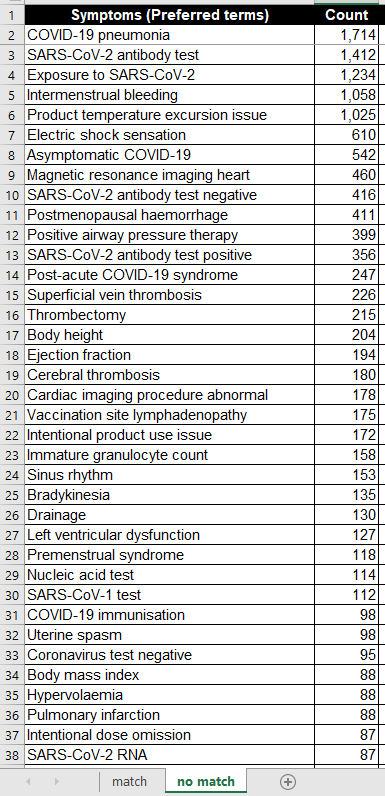
On the “no match” tab are symptoms where the baseline count=0. So these are quite extraordinary since these symptoms are not typically seen even once in 5 years. So here, even a small value in the “count” field is very significant, e.g., 2 or more would be comparable to a 10X or more on the “match tab.”
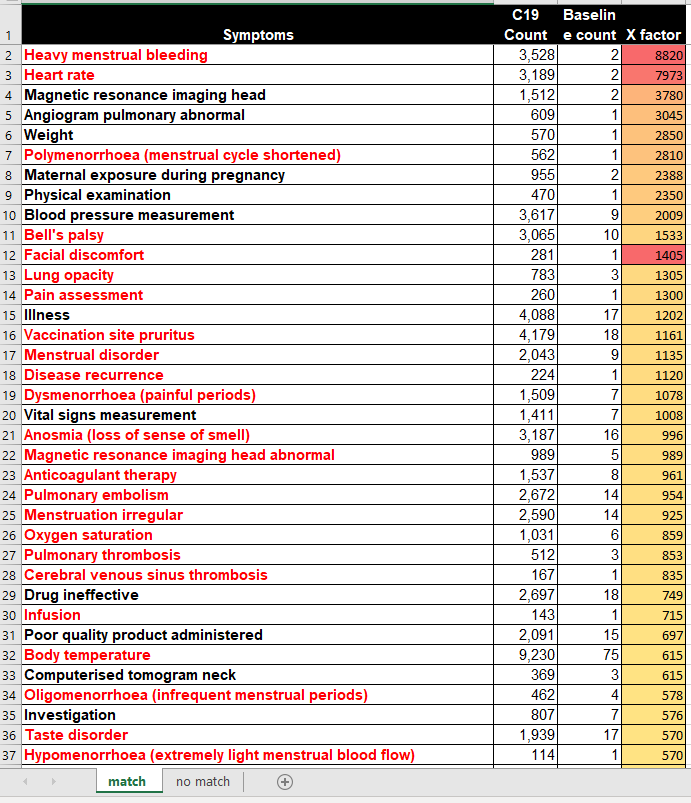
Now here are some screenshots of the first page of the two tabs:
And the no match tab:
What the data tells us
Here are a few quick observations from the complete data set (see next section for downloading):
- Female reproductive issues top the list. These are strongly elevated by these vaccines. Many of the top symptoms are all related to the menstrual process.
- There are an enormous number of cardiovascular and neurological events that are strongly elevated, many of them serious.
- Fibrin D dimer increased is #53 on the list, elevated by a factor of over 400x above baseline. Charles Hoffe discovered D-dimer was elevated in over 60% of the patients he measured. This is very serious as D-dimer is a lagging indicator of blood clots.
- Troponin increased was #130, elevated by a factor of 205. Troponin indicates heart damage and it is elevated to extreme levels (10X heart attack levels or more) and can stay elevated for months at a time (with a heart attack, the levels start returning back to normal immediately after the incident)
- Death as a symptom (which is pretty unusual coding since it isn’t a symptom), is #433 and elevated by 96X. Hardly a “safe” vaccine.
- Brain herniation at #405 is elevated by a factor of 100X over baseline. However, this is not considered a big deal at the CDC (perhaps because many people there don’t use their brain).
- Cardiac arrest at #450 is elevated by 93X. This is when your heart stops. This is a relatively serious condition since you don’t last for too long after that. It’s a bit surprising that the CDC missed that one. Perhaps because they don’t have a heart?
- Pulmonary embolism #24 is elevated by 954 times normal. How the CDC can miss that one is simply astonishing! This was the cause of death of 2 of the 14 kids that the CDC looked at in their death analysis. Mainstream press will never ask them that question as to why the CDC would not find causality here. They wrote: “CDC reviewed 14 reports of death after vaccination. Among the decedents, four were aged 12–15 years and 10 were aged 16–17 years. All death reports were reviewed by CDC physicians; impressions regarding cause of death were pulmonary embolism (two), …” 954 times normal is hard to explain, isn’t it? So no causality? That’s hard to explain, so they didn’t. They just moved on as if there is nothing to see.
- Intracranial haemorrhage (their spelling) is at #604 and is elevated by 79X. Two of the 14 kids from the CDC analysis died from that. How could that not be causal? They never explained that.
- Tinnitus at #362 is elevated by 105X. This can be so bad that people can kill themselves from this alone. One of the people who work at Vaccine Safety Research Foundation (VSRF) had to talk a friend out of suicide.
- There are many many more issues to be concerned with, but I wanted to get the list out quickly so there can be more eyes on this.
- For months, I’ve offered to discuss our data and analyses to both the FDA and CDC outside committees as well as the CDC and FDA themselves, but nobody wanted to see it. Most hit delete on my emails. A few told me to wait for the public comment period and submit it then (which I’ve done). Nobody followed up.
The Excel file with the full results
I’m trying to increase the number of paying subscribers I have as this supports the substack community. All proceeds will go to paying the salaries of people working for the Vaccine Safety Research Foundation (vacsafety.org) as well as buying ads so we can get the message out.
You can find the full Excel file and Albert’s analysis in this article.
CDC Admits Crushing Rights of Naturally Immune Without Proof They Transmit the Virus
By Aaron Siri | Injecting Freedom | November 11, 2021
You would assume that if the CDC was going to crush the civil and individual rights of those with natural immunity by having them expelled from school, fired from their jobs, separated from the military, and worse, the CDC would have proof of at least one instance of an unvaccinated, naturally immune individual transmitting the COVID-19 virus to another individual. If you thought this, you would be wrong.
My firm, on behalf of ICAN, asked the CDC for precisely this proof (see below). ICAN wanted to see proof of any instance in which someone who previously had COVID-19 became reinfected with and transmitted the virus to someone else. The CDC’s incredible response is that it does not have a single document reflecting that this has ever occurred. Not one. (See below.)
In contrast, there are endless documents reflecting cases of vaccinated individuals becoming infected with and transmitting the virus to others. Such as this study. And this study. And this study. And this study. It goes on and on…
But it gets worse. The CDC’s excuse for not having a shred of evidence of the naturally immune transmitting the virus is that “this information is not collected.” What?! No proof! But yet the CDC is actively crushing the rights of millions of naturally immune individuals in this country if they do not get the vaccine on the assumption they can transmit the virus. But despite clear proof the vaccinated spread the virus, the CDC lifts restrictions on the vaccinated?! That is dystopian.
The facts about natural immunity are simple. Every single peer reviewed study has found that the naturally immune have far greater than 99% protection from having COVID-19, and this immunity does not wane. In contrast, the COVID-19 vaccine provides, at best, 95% protection and this immunity wanes rapidly. I am no mathematician, but a constant 99% seems preferable to a 95% that quickly drops. And, while the vaccinated readily transmit the virus, not so for the naturally immune.
The lesson yet again is not that health authorities should never make mistakes. They will. It happens. The lesson is that civil and individual rights should never be contingent upon a medical procedure. Everyone, the naturally immune or otherwise, who wants to get vaccinated and boosted should be free to do so. But nobody should be coerced by the government to partake in any medical procedure.
FOIA Request
FOIA Response
CDC lies again–it will now try to impose universal Hepatitis B vaccination of adults!
By Meryl Nass, MD | November 7, 2021
The criminals at CDC began 30 years ago to appropriately target iv drug abusers, sex workers and others with a high risk of Hepatitis B to be vaccinated. There were not enough takers, according to CDC, so the public health officials set their sites on newborns, aimed and fired.
Hepatitis B is a viral disease transmitted via intercourse, iv drugs, or from mother to baby. All mothers are supposed to be tested for it during pregnancy, and less than 1% are positive. Mothers and their newborns who test positive are treated for it with vaccinations and immune globulin.
But that did not suffice for the science-light, pharma-heavy CDC. So some dim bulb decided that ALL newborns should be vaccinated for hepatitis B, within a few hours after birth. This practice was never shown to be safe, but it pleased public health officials, who could impose the vaccinations on babies while their moms were still recovering and dopey from the birth, the babies were stuck in a hospital, and the newborns were basically chickens to be plucked.
No one ever explained why newborns whose moms were negative needed to be protected from a disease that only affected those with more than one sex partner (primarily gay men) and those using dirty needles. But the CDC decided this was a great way to get everyone vaccinated, and it would protect those newborns when they did become old enough for sex and needles.
A bell should have gone off when it turned out their immunity waned after a few years–even though those poor infants had suffered 3 doses of a vaccine they had no need for, starting in the first moments of life. But the dim bulbs at CDC ignored it.
The thing is, rates of Hepatitis B in the US are low. They are high in east Asia, but the US is not east Asia. Rates have fallen since vaccine has been available over the past 30 years.
If you look at CDC’s Figure 2.5 below you will see that reported new Hepatitis B cases are 1 per 100,000 per year in women, and 1.5 per 100,000 in men in 2018, the last year for which CDC provides data.

In 2018, a total of 3,322 cases of acute hepatitis B were reported to CDC, for an overall incidence rate of 1.0 cases per 100,000 population.
The rate of reported acute HBV infections declined approximately 90% since recommendations for HepB vaccination were first issued, from 9.6 cases per 100,000 population in 1982 to 1.0 cases per 100,000 population in 2018.
So why in heaven’s name would CDC want to start vaccinating everyone when rates are very low and have fallen dramatically? However…
On Wednesday November 3, CDC briefed its supine advisory committee on the imaginary need for hepatitis vaccines. CDC briefers are trained to scare the pants off you to get the votes they want. Here is what was said:
CDC medical officer Mark K. Weng, MD, MSc, FAAP, who leads the ACIP’s hepatitis vaccines work group, presented data on the importance of vaccinating adults against HBV.
“In the U.S. every year, there are 20,700 estimated acute hepatitis B infections, and over $1 billion dollars spent on hepatitis B-related hospitalizations,” Weng said. “There are almost two million people estimated to be living with chronic hepatitis B in the U.S., of whom there’s a [15% to 25%] risk of premature death from cirrhosis or liver cancer.”
How did he get these deadly numbers? Well, CDC claimed that only about one tenth of the cases get reported, that is how. CDC used its dubious estimates to claim cases were ten times greater than reported–something they never claimed before. How do they know this? They never tell. They can’t give us a number to multiply the VAERS reports by to find out the rate of adverse vaccine events, but they are quick to come up with a magic multiplier when they want new vaccine programs to be approved.
What happened? The ACIP sleepwalkers voted to vaccinate all adults for hepatitis B–even those who are monogamous and don’t take any drugs. Why? Because they can, and they get pharma contracts when the advisory committee members behave.
So, this is what is next. Get ready to fight against more mandates. The elites are making war on us.
ACIP recommends universal hepatitis B vaccination for adults aged 19 to 59 years
CDC Advisors Unanimously Endorse Pfizer’s COVID Vaccine for Kids 5-11 Despite Expert Concerns Over Clinical Data
By Megan Redshaw | The Defender | November 2, 2021
The Centers for Disease Control and Prevention’s (CDC) vaccine advisory panel today unanimously recommended Pfizer’s COVID vaccine for children 5 to 11, despite concerns raised during the meeting about Pfizer’s clinical data, the fact that children who previously acquired natural immunity to COVID were included in clinical trials and evidence showing COVID poses little risk to children.
If Dr. Rochelle Walensky, the CDC’s director signs off on the decision, children ages 5 through 11 could start receiving COVID vaccines as early as tonight.
The younger age group will receive one-third of the dose authorized for those 12 and older in two shots at least three weeks apart. The doses will be delivered by smaller needles and stored in smaller vials to avoid a mix-up with adult doses.
The CDC’s guidelines for the vaccine’s use are not legally binding, but heavily influence the medical community’s practice.
Prior to today’s decision by the CDC’s Advisory Committee on Immunization Practices (ACIP) the Biden administration enlisted more than 20,000 pediatricians, family doctors and pharmacies to administer the vaccines — with 15 million doses already packed with dry ice, loaded into small specialized containers and shipped via airplanes and trucks to vaccination sites across the country, federal officials said on Monday.
Walensky sent a clear signal during the ACIP meeting about where she stands, CNN reported. “We have been asking when we will be able to expand this protection to our younger children,” Walensky said in opening comments to the committee.
“As you review the data today, it will be key to keep in mind the specific risks to children from this virus and the pandemic, and to put that risk into context of other vaccine-preventable diseases,” Walensky said.
Walensky noted that children are routinely vaccinated against diseases like chickenpox — which results in far fewer hospitalizations and deaths in children compared to COVID.
During today’s meeting, ACIP members reviewed and discussed the science behind the U.S. Food and Drug Administration’s (FDA) authorization last week of Pfizer’s COVID vaccine in all children 5-11 years old.
That authorization was based mostly on a Pfizer-BioNTech study of 4,600 children worldwide, of whom approximately 3,100 got the low-dose vaccine and about 1,500 got a placebo.
These studies showed the vaccine is about 91% effective against COVID. The immune system response to the vaccine, as measured by antibodies, was comparable to the response seen in 16- to 25-year-olds, NPR reported.
During the meeting, the CDC said 745 children under 18 have died of COVID since the beginning of the pandemic — although the COVID-19 team admitted 79% were confirmed to be hospitalized for COVID, while the rest were hospital admissions for other causes.
“The chance that a child will have severe COVID, require hospitalization or develop a long-term complication like MIS-C [multisystem inflammatory syndrome] remains low, but still the risk is too high and too devastating to our children, and far higher than for many other diseases for which we vaccinate children,” Walensky said.
Efficacy of Pfizer’s COVID vaccine in children
The CDC said Pfizer’s COVID vaccine was 90.9% effective against symptomatic COVID and none of the adverse events experienced during clinical trials were assessed by “the investigator” as related to the vaccine.
To determine the efficacy of the Pfizer-BioNTech COVID vaccine, Pfizer measured the blood of 264 children for antibodies.
“There were 3,000 vaccinated children in the trial. Why isn’t blood from the other 2,700-plus being measured for antibodies?” asked Dr. Meryl Nass, a member of the Children’s Health Defense Scientific Advisory Panel.
“Pfizer never explains why, when they have an important clinical trial in which over 3,000 children were injected in this age group, only a subset of less than 10% were used to assess efficacy,” Nass said.
Nass explained:
“Pfizer claims three cases of COVID in the vaccinated group versus 16 in the placebo group show efficacy of the vaccine. But the FDA did not accept this claim. Note that all cases were mild, none hospitalized or died. So are they planning to vaccinate 28 million kids to prevent colds?”
Nass noted Pfizer also enrolled kids who had prior evidence of having had COVID in the clinical trial, “which should never have been allowed.”
“Of the kids who were already immune at the start of the trials, none developed COVID,” Nass said. “About 150 kids in the placebo group were recovered and none got COVID.”
Nass said kids with preceding COVID infection did not have their antibody levels checked after the first dose, as Pfizer stated they did not collect the data because they “tried to minimize blood draws in children.”
“The real reason they did not want to collect data is because it might support the fact that kids who already had COVID might only need one vaccine dose, or none at all,” Nass said.
During the brief public comment session, Patricia Neuenschwander, a registered nurse noted there was no prevention of hospitalization, death or multisystem inflammatory syndrome in children — a condition being used to justify vaccinating younger children against COVID, despite numerous cases of MIS-C having been reported after receipt of a COVID vaccine.
Neuenschwander reminded the ACIP that vaccinations do not prevent infection or transmission. It is a mild illness in the vast majority of children, she said, and prior immunity is being ignored — the expansion group was only followed for 17 days.
David Wiseman, a research scientist with a background in pharmacy, pharmacology and experimental pathology, asked the CDC panel why the efficacy study was not validated by the FDA, and why Pfizer changed the buffer [see page 14] in the vaccine but did not test it in animals or kids — planning to use an untested version of the vaccine in 5 to 11-year-olds.
Wiseman said the FDA abandoned its responsibility, and he asked if the ACIP would do the same.
Myocarditis and COVID in 5- to 11-year-olds
One side effect that generated considerable discussion at today’s meeting was myocarditis — a form of heart inflammation.
The CDC said 1,640 cases of myocarditis have been reported to the CDC’s Vaccine Adverse Event Reporting System in people under age 30 after having received a COVID vaccine, but only 877 met the CDC’s case definition.
The CDC said there were nine reported deaths in people with myocarditis, but then the agency reduced the number to three, with two cases pending evaluation and one case without adequate information.
“I have to say that it is beyond belief that CDC could whittle down 877 cases reported in young people to three actual cases. Where did the rest go?” Nass asked.
“According to the CDC’s Vaccine Safety Datalink, 7 of 16 12- to 17-year-olds with myocarditis were still on exercise restriction three months after diagnosis — that is 44% could not exercise three months later,” Nass said. “This is huge.”
Nass further noted 25% of 250 myocarditis cases were still symptomatic at three months, and only 74% of cases were designated by cardiologists as definitely resolved at 3 months.
As it pertains to safety, some who testified during a public comment period, as well as other commentators, questioned whether the study used by the FDA to grant Emergency Use Authorization is large enough to assure parents that the vaccine is safe in young children.
“The bottom line is getting COVID, I think, is much riskier to the heart than getting this vaccine,” said Dr. Matthew Oster, a pediatric cardiologist at Children’s Hospital of Atlanta.
Dr. Tom Shimabukuro covered vaccine safety monitoring from the CDC’s surveillance system in children. Shimabukuro said COVID is getting the “most intensive vaccine monitoring program in history,” yet he did not go into detail on surveillance data.
Acknowledging that some parents are hesitant about vaccinating their children right away, Dr. Matthew Daley, a member of the ACIP said, “we hear you loud and clear and of course you only want what’s best for your child. I encourage you to talk to your family physician or pediatrician, they can walk through this with you.”
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- US sent ‘a lot’ of arms to Iranian protesters – Trump
- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- REWRITING THE RISK? INSIDE THE GOVERNMENT’S VACCINE SAFETY MESSAGING
- “Davos Can Really Replace the UN”
- NIAID/NIH and USDA Fund Bioengineered Chimeric Influenza Viruses Built Using Pandemic H1N1 Components: Journal ‘Science Advances’
- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- If Americans Knew
- Trump poised to “blow everything up” (ie. commit war crimes) in Iran – Daily Update
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
