Official Data shows Deaths of male Children are up 54% since they were offered the Covid-19 Vaccine
THE EXPOSÉ | DECEMBER 4, 2021
An investigation of official ONS data has revealed that since the Covid-19 vaccine was offered and administered to kids in England and Wales there has been a 54% rise in deaths among male children compared to the same period in 2020.
The UK’s Medicine and Healthcare product Regulatory Agency (MHRA) have openly admitted that they suspect myocarditis and pericarditis are potential side effects of the Pfizer and Moderna Covid-19 vaccines, especially among young males. A suspicion that has been strong enough for the UK Medicine Regulator to officially add warnings about myocarditis and pericarditis to the safety labels of the Covid-19 vaccines.
Myocarditis is inflammation of the heart muscle, whereas pericarditis is inflammation of the protective sacs surrounding the heart. Both are extremely serious conditions due to the vital role the heart plays in keeping a person alive, and the fact that the heart muscle cannot regenerate. Serious myocarditis can lead to cardiac arrest and knock years off a persons life.

The UK Government have now also admitted in official documents that a high percentage of all hospitalised children are presenting to hospital with Myocarditis following Covid-19 vaccination.

Source
This fact adds greater concern for data published by Public Health England on the number of 999 calls made requesting an ambulance due to cardiac arrest. The stats show that they have skyrocketed against the expected average since young adults and teens began receiving the Covid-19 vaccine.

Chris Whitty advised the UK Government to roll-out the Pfizer Covid-19 vaccine to all children over the age of 12 in week 37 of 2021. Thanks to preparations already being made by the NHS to intrude on education in schools and administer the jab to children, the roll-out got underway the following week (week 38).
The 2020 edition of ‘Deaths registered weekly in England and Wales, which can be downloaded here, and accessed on the ONS website here shows the number of deaths registered weekly by age group.

Source
The ONS data shows that between September 18th and November 13th 2020 a total of 24 deaths occurred among male children aged between 10 and 14.
However, the 2021 edition of ‘Deaths registered weekly in England and Wales, which can be downloaded here, and accessed on the ONS website here, shows a significantly higher number of deaths have occurred among male children in 2021 following Chris Whitty’s decision to offer them the Covid-19 vaccine.
The data shows that between week 38 (week beginning 18th September) and week 46 (week ending 19th November) of 2021, a total of 37 deaths occurred among male children aged between 10 and 14.

This shows that since the Covid-19 vaccines began being given to kids over the age of 12, deaths among male children have increased by 54% compared to the same period in 2020.
We compiled the following graph on ONS figures so that we were able to easily compare the number of deaths per week among male children in 2020 and 2021.

The data is there now for the authorities to see, a 54% increase in deaths of male children compared to 2020 since they started to be given the Covid-19 vaccine, they must investigate this and cease the roll-out of the jabs to kids immediately.
2,809 Dead Babies in VAERS Following COVID Shots as New Documents Prove Pfizer, the FDA, and the CDC Knew the Shots Were Not Safe for Pregnant Women
By Brian Shilhavy | Health Impact News | December 4, 2021
The latest data dump into the U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) happened yesterday (12/3/21) and covers data through 11/26/2021.
There are now 927,740 cases reported to VAERS following COVID-19 shots for the past 11 months, out of the total of 1,782,453 cases in the entire VAERS database filed for the past 30+ years.
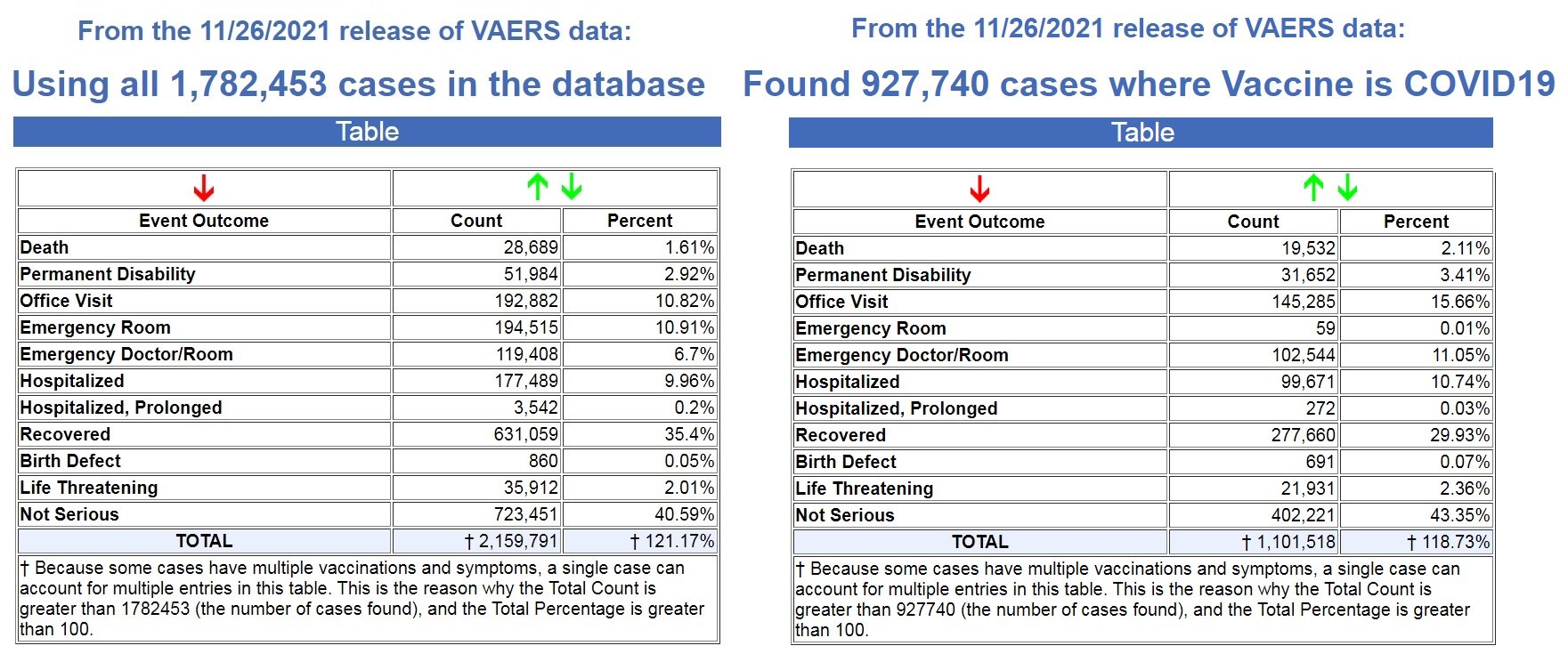
Left image source, Right image source.
That means that 52% off ALL vaccine adverse reaction cases in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
In addition, 68% of all deaths following vaccines reported in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
We are on pace to see 21,307 deaths reported in the first year following the experimental COVID-19 shots, while the average yearly deaths reported after FDA-approved vaccines for the past 30+ years is 305 deaths.
That is an astounding 86% increase in reported deaths following the COVID-19 shots, a 70X increase over the average reported deaths following vaccinations for the past 30+ years!
- FDA-approved vaccines: 305 deaths per year
- COVID-19 EUA shots: 21,307 deaths per year
And as Dr. Jessica Rose has previously reported, the under-reporting factor in VAERS for the COVID-19 shots is 41X, as a conservative number, which means that at least 800,812 people have now died following COVID-19 shots based on the VAERS data.
Most, if not all, of those deaths are being reported in the pharma-owned corporate media as “COVID” deaths, as there are now more recorded “COVID deaths” for the first 11 months of 2021 than there were for the entire year in 2020, when there were no COVID vaccines until December. (Source.)

Record Number of Fetal Deaths Following COVID-19 Shots
As of this most recent update in VAERS, we have now found 2,809 fetal deaths following COVID-19 shots injected into pregnant and child-bearing women for the past 11 months. (Source.)
By way of contrast, using the exact same search parameters in VAERS, but excluding the COVID-19 shots, we found 2,168 fetal deaths following all FDA-approved vaccines for the past 30+ years. (Source.)
That’s an average of 72 fetal deaths per year following all FDA-approved vaccines for the past 30+ years, compared to what is on pace to be 3064 fetal deaths in 1 year following COVID-19 shots.
- FDA-approved vaccines: 72 fetal deaths per year
- COVID-19 EUA shots: 3064 fetal deaths per year
That is an 80% increase in fetal deaths recorded in VAERS following the COVID-19 shots. And yet, the CDC and FDA continue to recommend these EUA shots for pregnant women and nursing mothers.
Not only do they recommend these shots for pregnant women, we now have ample evidence that they have known since earlier this year that these shots are dangerous to pregnant women, and causing fetal deaths.
In a March 4, 2021 Advisory Commission on Childhood Vaccines (ACCV) meeting, the CDC submitted a report that contained a section titled: Maternal vaccination safety summary (starting on p. 39).
They stated (emphasis mine – my comments in red):
* Pregnant women were not specifically included in pre-authorization clinical trials of COVID-19 vaccines
– Post-authorization safety monitoring and research are the primary ways to obtain safety data on COVID-19 vaccination during pregnancy
* Larger than expected numbers of self-reported pregnant women have registered in v-safe
* The reactogenicity profile and adverse events observed among pregnant women in v-safe did not indicate any safety problems (based on what criteria???)
* Most reports to VAERS among pregnant women (73%) involved non-pregnancy specific adverse events (e.g., local and systemic reactions)
* Miscarriage was the most frequently reported pregnancy-specific adverse event to VAERS; numbers are within the known background rates based on presumed COVID-19 vaccine doses administered to pregnant women (no supporting evidence to backup these claims)
It is important to note through all of this reporting by the CDC that these are based on self-reporting data from pregnant women.
We know that it is politically incorrect to blame any health issue on a COVID-19 “vaccine,” and that doctors and nurses are pressured to NOT report these, so how many pregnant women had an adverse reaction, like a miscarriage, and never even thought to link it to their COVID-19 shot?
So back in March of this year (2021), there were already major concerns about the effects of the shots on pregnant women, as “larger than expected” pregnant women were reporting adverse reactions, and “the most frequently reported pregnancy-specific adverse event to VAERS” was “miscarriage.”
Then in August of this year (2021), the CDC presented a “new study” with “new data.”
Again, this “data” is dependent on pregnant women “self-reporting” adverse reactions, so we know these reports will be well below what was actually happening in the population, as it is politically incorrect to report any adverse reactions related to the experimental COVID-19 shots. To do so is to be branded an “anti-vaxxer” and shame you for life.
The August update admitted that 13% of the pregnant women who had received a COVID-19 shot reported a miscarriage. The CDC brushed this aside by stating “miscarriage typically occurs in about 11-16% of pregnancies.”
But of course ALL miscarriages are reported somewhere in the medical files, which is why they can even come up with a number range like this. So this figure is based on 100% of the reported data, while the COVID-19 related miscarriages are only based on what was self-reported, and we have no idea how many women never reported their miscarriages because they never related it to their COVID-19 shot.
One the main studies the CDC allegedly relied upon to declare that COVID-19 shots were safe for pregnant women, was a study published in the New England Journal of Medicine on June 17, 2021.
But on October 14, 2021, they issued a statement stating that some of their data was wrong in the June 17th study. (Source.) It dealt specifically with pregnancies in their 20th week or earlier.
“No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for gestational week–specific risk of spontaneous abortion.” (Source.)
Why hide what happens in the first two weeks after vaccination?
Hiding part of the data leads to wrong conclusions
Health Advisory and Recovery Team | December 1, 2021
There have been numerous papers published showing how well the vaccines protect people after the second dose. Some of this effect is an illusion. The effect happens as a result of inaccurate measuring and a phenomenon called survivorship bias.
Survivorship bias happens when a group is compared at two time points, but the members of the group change between the time points. It would be like assessing the quality of a swimming school which favours the technique of throwing people into the middle of the ocean, leaving them for a couple of hours and claiming credit for how well the remaining students can swim. After two hours, the only people left would be the ones who could already swim and possibly a few who learnt to swim the hard way! The poor souls who drowned in the interim don’t even make the count. Attributing the remaining people’s swimming ability to the coach who turned up 2 hours later would obviously give a very misleading picture. Pointing out that no-one drowned in later lessons would be equally misleading in determining the success of the ‘teaching technique’.
With covid vaccination there is a two week period after vaccination that is not included in the data. The rationale given for this is that vaccines take a while to induce antibodies and therefore the first two weeks’ data are not relevant. Obviously this is flawed. What if the vaccines have deleterious effects that are visible straightaway, that have nothing to do with antibody production? An example is the high rate of shingles seen after covid vaccination, suggesting there is a problem with viral reactivation. This may explain why Sars-CoV-2 infection rates are actually higher in the vaccinated than in the unvaccinated in the first two weeks after vaccination.
The effect of eliminating the first two weeks is a misleading data bias. If people become infected and are dying during that period, this needs to be included. The possibility that the vaccine itself may exert an effect on infection rate cannot be overlooked and the entire dataset needs to be included in order to accurately assess effectiveness. By only measuring the period after the higher risk of infection (0-14 days) it is possible to be deceived. Any signal would be missed.
Aside from it being nonsensical in terms of individual risk to remove this period of time, there will also be an impact on the wider community. If the vaccine in fact causes a spike in infections during the first two weeks, this will inevitably increase spread and will lead to an increased number of infections in that community during that time. Therefore, the assessment of the impact of the vaccination programme must include not only the effect on the individual, but the impact on the wider community.
This point is of particular relevance for close-knit communities where many are being vaccinated at the same time, such as schools and in particular communities with a high number of vulnerable people such as care homes and hospitals. What we are effectively doing is ‘speeding up’ the wave of infections (and deaths). Ultimately at the end of the viral season, the same number of people died. Because of excluding the earlier deaths (1-14 days), we are misled into thinking that the vaccines were more effective than they actually were. By only looking at the later period and seeing fewer deaths during that time, the illusion was created that lives were saved. This is evident in data from many countries following vaccine roll-out. The graph below showing the UK versus Europe illustrates this point, as the UK was the fastest to roll out the vaccine. The total number of deaths, represented by the area under the curve, was similar to other countries, but is just compressed into a shorter time period.
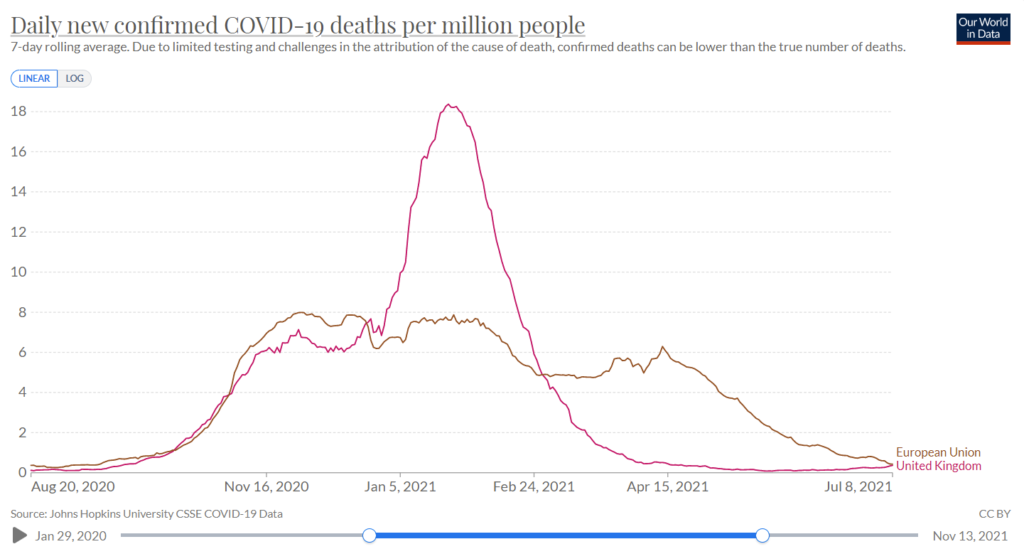
Figure 1: Covid Deaths in winter in UK and the European Union
Let’s now examine some specific examples, e.g. this study of nursing home residents in the United States. The results show that over the course of the study 6.8% of the vaccinated population were infected and 6.8% of the unvaccinated population were infected. However, by deciding that the first 14 days after vaccination should be excluded, the grey area for the vaccinated group is compared to the black and grey area combined for the unvaccinated. Doing so could lead to the claim of 66% vaccine efficacy against infection. The authors of this study were honest enough to share the raw data and did not claim 66% efficacy.
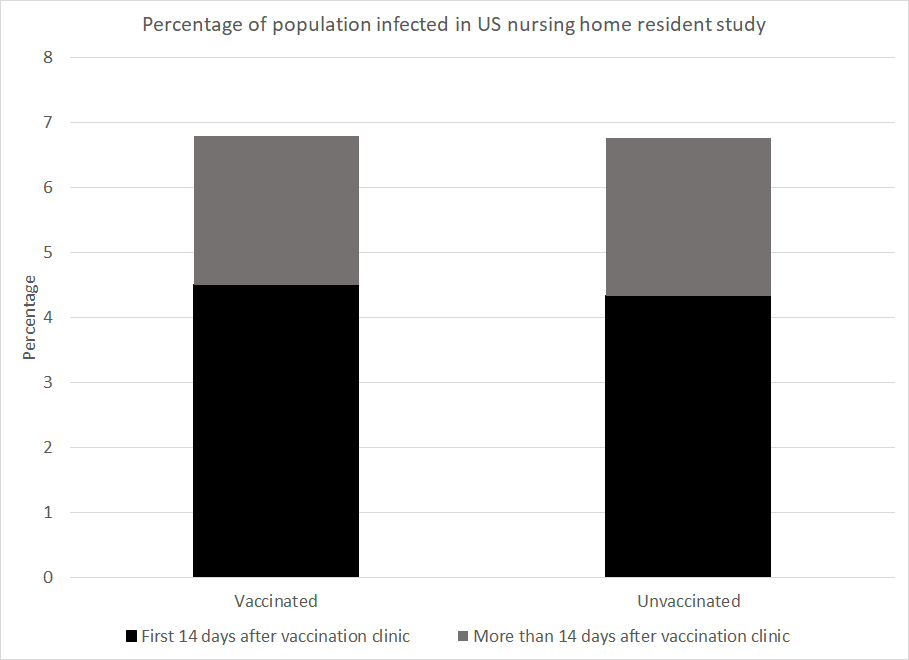
Figure 2: Data from US paper showing the percentage of the nursing home population to be infected by time after the clinic came to their home and by vaccination status
However, numerous studies have relied on this trick to make claims of vaccine efficacy. The most obvious examples of this are the original Pfizer trial study and the AstraZeneca trial.
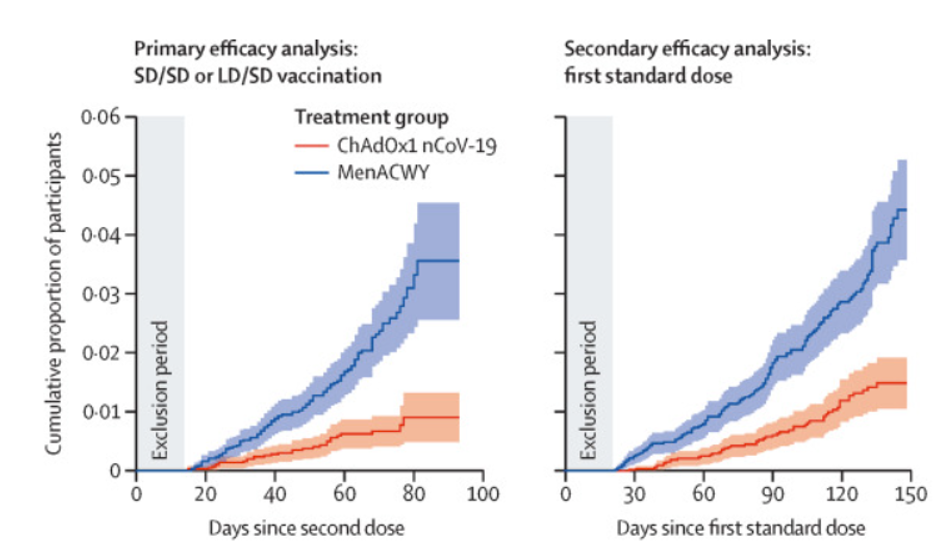
Figure 3: Graph from AstraZeneca trial showing censorship of early period (‘Exclusion Period’)
To take a second example, a Danish paper measured infection numbers in healthcare workers and care home residents. Prior to the beginning of the vaccination programme 4.8% of the healthcare workers had been infected and 3.8% of the care home residents had been. The study ended at the end of the Danish winter wave after 95% of the care home residents had been vaccinated and 28% of the healthcare workers had been. Given the worse position at the start and the lower vaccination rate in healthcare workers you might expect that they were worse off overall. However, the percentage infected by the end of the wave was 7.0% among healthcare workers but 7.7% among care home residents.
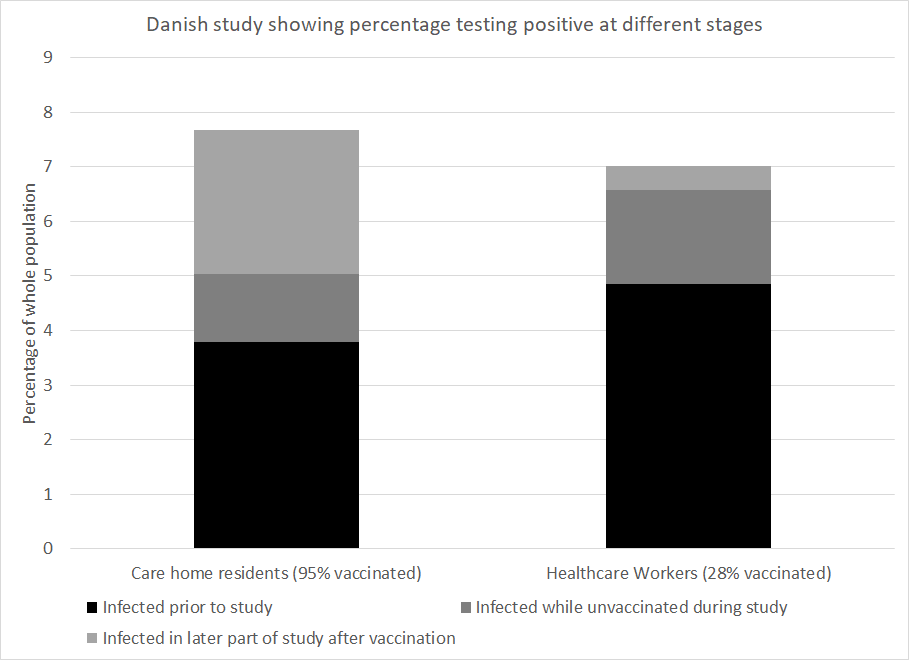
Figure 4: Data from Danish paper showing percentage of population infected among care home residents and healthcare workers
How much of the vaccine efficacy reported in covid research is really a measure of survivorship bias coupled with naturally acquired immunity? This is a critical question. No claim of vaccine efficacy should be made without first addressing this.
UK surgeon remains suspended a year after saying governments are using Covid to control people
By Christina Maas | Reclaim The Net | December 4, 2021
Last year, the UK medical register suspended a consultant surgeon for 12 months pending an investigation by the General Medical Council (GMC) for posting on social media that Covid-19 was being used by elites to control the world.
Colleagues wrote to the organization arguing he should not have been suspended for his personal opinion.
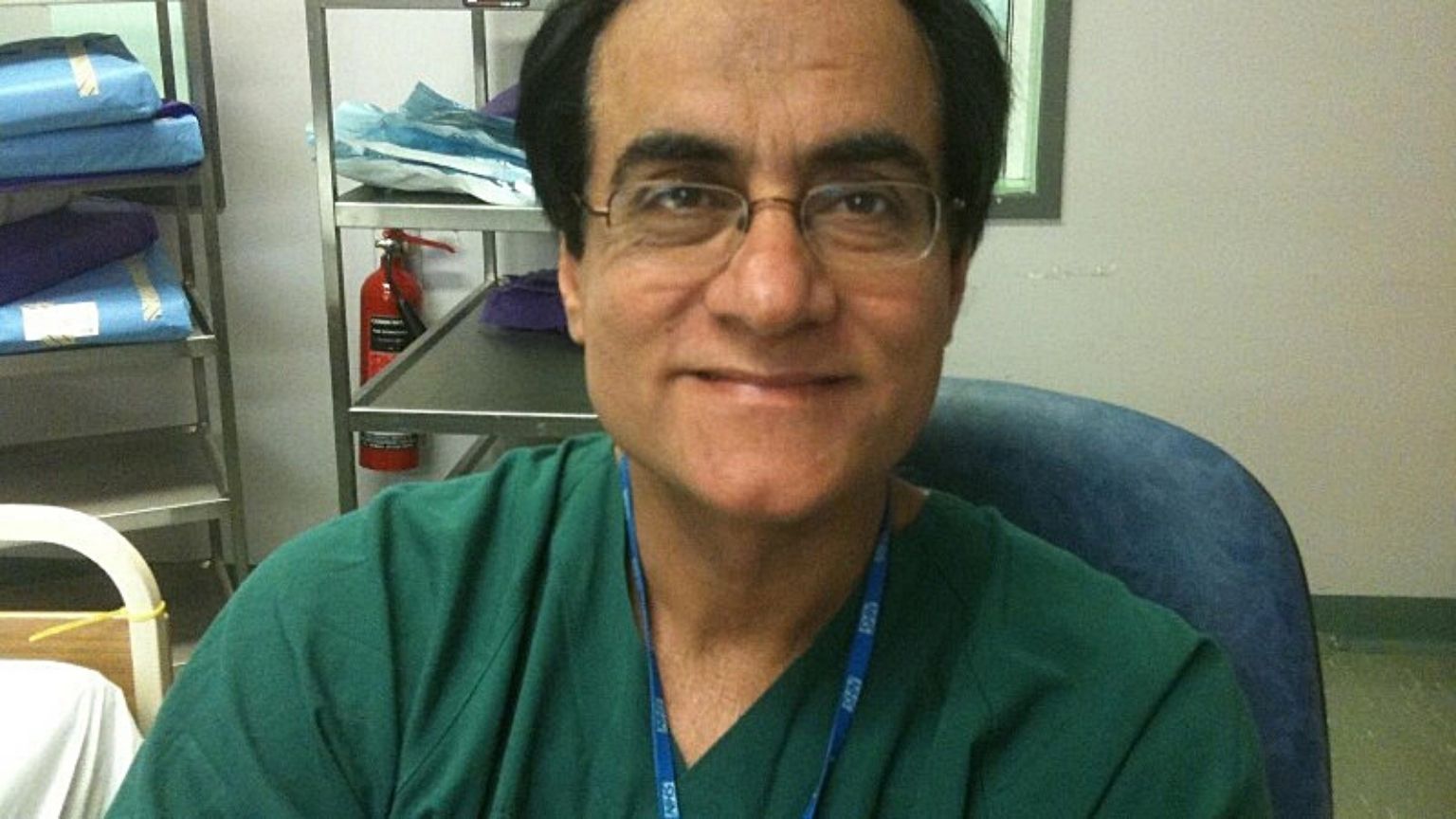
Mohammad Iqbal Adil, a Pakistan-born British doctor, has worked in the NHS for almost three decades. An interim orders tribunal suspended him for a year because of videos he posted on social media.
The doctor expressed “his point of view on the Covid-19 pandemic and the far-reaching effects of the lockdown on the economy, public health and wellbeing,” his campaign page states.
A spokesperson for the GMC at the time said: “The interim orders tribunal imposed an interim suspension on Dr Adil’s registration, following our referral, to protect patients and public confidence. This interim suspension remains in place while we consider concerns about Dr Adil’s fitness to practice.”
Some of his colleagues launched a petition on Change.org calling on the GMC to reinstate Dr. Adil. The petition argues that the GMC should have given him a chance to reflect on the videos “when the entire world is confused about the novel virus.”
The petition also noted that he had a family to support, adding, “UK needs doctors to work. It would not be in the best interest of the public and health system to lose [an] experienced and highly qualified surgeon like him.
“We, the doctors community within [the] UK and across the world, feel that it’s injustice to suspend Mr Adil on his personal point of view on the covid-19 without giving him [a] chance to reflect upon his video before enforcing suspension.
“We request to the GMC to revoke his unfair 12 months suspension . . . and allow him fair chance to work in this country [for the benefit of] the health system, communities, and medical graduates.”
“Dr Adil has been making a stand for freedom of speech for all doctors and nurses to speak their truth without fear of recrimination or persecution,” his campaign page states.
Researchers Acknowledge SARS-CoV-2 Is Gaining Vaccine Resistance
By Dr. Joseph Mercola | December 3, 2021
Looking at the viral evolution of SARS-CoV-2, researchers from the prestigious universities Harvard and MIT have found that the virus not only will continue to mutate and create new variants in the future, but will become resistant to the vaccines as it adapts to humans.
Their study, published December 2, 2021, in the journal Science, shows that the mutations serve as bridges to conferring resistance to neutralizing antibodies. “The severity of the phenotypes we observed in vitro suggest that further evolved variants will more adeptly escape therapeutic antibody neutralization than currently circulating variants of concern, with potential resistance to two-component antibody cocktails,” the study authors wrote.
The scientists urged that “proactively examining the consequences of further viral evolution before the next highly antibody resistant strain emerges is of utmost importance.”
A brief reminder: Health agencies were not always deranged
a trip down memory lane
el gato malo – bad cattitude – december 4, 2021
it was february of 2020, a kinder time. a gentler time.
and the WHO was putting out guidelines to avoid stigmatizing people who got covid…
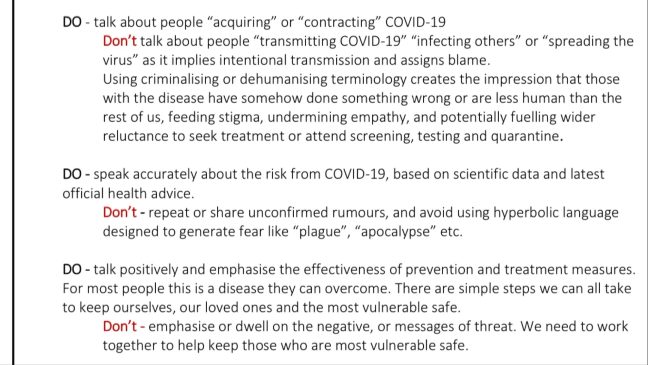
never forget this.
they knew before 2020 than none of these interventions worked, that their prices were insanely high, and that they should never be undertaken.
they knew the dangers of vilification and polarization.
standing pandemic guidelines vehemently warned against any of this and especially against making pariahs of the infected and cultivating exaggerated fear to drive compliance.
this has NOT been “following the science” is has been the abrogation of a century of evidence based epidemiology and social mores in order to take a devastating and self-serving joy ride with the world’s populace like it was some sort of video game.
and all the health agencies were aware of that.
these were choices.
this was done to you, not for you.
and it was done by people who damn well knew better.
if you learn one thing from this, learn that, because these malefactors and agencies are still around and they are not done with you…
“Post Pandemic Stress Disorder”… seriously?
By Kit Knightly | OffGuardian | December 3, 2021
There’s a reason heart attacks and blood clots are about to become a LOT more common… but the vaccine has nothing to do with it. Apparently.
Doctors are warning that hundreds of thousands of people in the UK could be at increased risk of heart disease or cardiac events.
Speaking to the Evening Standard, psychological therapist Mark Rayner and vascular surgeon Tahir Hussein said that the UK could see “300,000 new patients with heart issues” in the near future.
What’s to blame? Well, that would be “Post Pandemic Stress Disorder”. A new condition “yet to be recognised”, even though “many experts believe it should be”.
It’s a totally real thing. They didn’t just completely make it up. Don’t be cynical.
You see, all the “pandemic” related anxiety and stress has taken such a toll on the public that doctors are predicting a 5% increase in heart disease, nationwide, and not just in the elderly or infirm.
According to Dr Hussein, he is already seeing…
a big increase in thrombotic-related vascular conditions in my practice. Far younger patients are being admitted and requiring surgical and medical intervention than prior to the pandemic.
Now, some of you demented anti-vaxxers out there might be asking crazy questions like “could this increase in blood clots and heart disease be linked to injecting millions of people with an untested vaccine?”
But that’s absurd. And I told you to stop being cynical.
Yes, fine, in the interests of fairness, we should mention it was recently reported that the Astra Zeneca jab can cause blood clots.
It turns out all the people saying that back in March weren’t just conspiracy theorists spreading misinformation after all. They were totally right. But the clots are only rare, so don’t worry. And they sort of know what causes it now, so future batches might be fine.
And yes, also in the interests of fairness, it’s true that both the Pfizer and Moderna shots can cause heart issues too. Both, according to the CDC, can cause pericarditis and myocarditis, the complications of which include heart attacks, heart failure and strokes.
The UK government has even produced special guidelines for dealing with myocardits, “following Covid19 vaccination”.
But, just like the blood clots, this is very rare. Obviously not so rare you don’t need a special guiding document on how to deal with it, but still very very rare.
… the point is, yes, all the major Covid vaccines are known to have cardiac-related side effects, and yes, some doctors are now predicting a major spike in heart-related health problems, but these are totally unrelated.
Frankly, the very idea this could be a media psy-op designed to do pre-emptive damage control is ridiculous.
Stop. Being. Cynical.
Any connection between heart problems and vaccines is just bad luck or a coincidence. It’s really just the stress.
Don’t ask questions about the vaccine. Don’t decide to not get the vaccine. And certainly don’t worry about what’s in the vaccine. Worrying causes stress which, unlike vaccines, causes heart problems.
Just get the shot. And the second dose. And the booster, every three months. And the updated doses, for the variants.
Just to be safe, get four shots a year, every year, for the rest of your natural life, and/or until you drop dead of a heart attack.
… due to stress.
Don’t be cynical.
Featured Video
Drone Strike on Egypt, War Widens /Lt Col Daniel Davis & Matt Bracken
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s threat of nukes shows us who is running U.S. foreign policy
By Martin Jay | Strategic Culture Foundation | November 27, 2025
It is a long-debated subject. Whether it is the U.S. which controls Israel or the other way around. In the 70s, under President Nixon, many analysts firmly believed, despite the JFK assassination, that it was still the U.S. who called the shots and used Israel as a useful tool in the Middle East to keep a rowdy group of Arab states in check and subservient to America’s interests. But it is in recent years where we have to see if Israel has done that effectively and meticulously in America’s interests, given that most analysts agree that Israel and the U.S. are both preparing for war with Iran.
Given that Israel’s main task was to keep the region in order to serve America’s hegemony and its energy needs, one has to ask isn’t it a failure of both U.S. foreign policy and of Israel that a war with Iran is seen as a solution to America’s failing hegemony? And doesn’t this tail wagging the dog scenario show itself in the clear light once and for all? … continue
Blog Roll
 Aletho News
Aletho News- Drone Strike on Egypt, War Widens /Lt Col Daniel Davis & Matt Bracken
- Pfizer Freezes Air Traffic Control Funds Over COVID Vaccine Contract Dispute With Poland, Romania
- Mafia buying up some of 800,000 weapons missing from Ukraine – Italian prosecutors
- NATO deploys Italian, Spanish, Turkish jets to eastern flank
- From Tehran to Riyadh: How Israel Draws the Red Lines America Can’t Cross
- Iran warns Bulgaria against hosting US warplanes, secures assurances from Cyprus on base neutrality
- Leaked: How Britain exploits US Empire
- Ukraine’s ‘turned tide’ doesn’t comport ‘with basic military reality’
- How NIH Silenced Its Critics Without Telling Them
- American journalist reveals role of Jolani regime’s Washington envoy in her 2016 kidnapping
- If Americans Knew
- Israeli Media: Israel’s Defense Chief Is Enabling Jewish Terror: 2 Articles
- Why the New York Times story on Mossad recruiting Ahmadinejad doesn’t add up
- The Facts on ICC’s Karim Khan’s Dismissal after Court’s Arrest Warrant for Netanyahu
- By 22-Point Margin, Americans Think Netanyahu Should Be Arrested on US Soil
- What an Israeli settler pogrom feels like
- As Gaza draws closer to possible ceasefire, Netanyahu draws closer to Trump – Daily Update
- Zelensky’s big idea for Trump: Ukraine is the Israel of Europe
- In Michigan’s Primary, Abdul El-Sayed Puts AIPAC on the Ballot
- Trump and Netanyahu’s Meetings: A Trail of Broken Promises
- ‘A disaster for America First’: Trump allies fear Netanyahu meeting will pull US deeper into war with Iran
- No Tricks Zone
- ECMWF Models Throwing Cold Water On Extreme Germany Heat Wave Forecast Next Week
- Greenland’s Ice Sheet Was Supposed To Be Rapidly Melting Away. It Hasn’t Been.
- Global Temperature Trend Has Cooled Over The Past 6500 Years, Scientists Have Found
- Wind Energy Means Going Back To The Middle Ages, Says German Professor Horst-Joachim Lüdecke
- New Study: A 40-Fold Increase In Earth’s Main Greenhouse Gas Contributes To Cooling The Ocean
- New Study Highlights The ‘Dominant Role’ Of Aerosol/Cloud Interactions In Shaping Climate
- Munich’s First-Ever Green Party Mayor Declares First Ever City Water Use Restrictions… Fines Up to 50,000 €!
- Experimental Lab Research: The Climate Sensitivity To A 400-Fold Increase In CO2 Is 0.1°C
- Fatal Snobbery: In France, It’s Better To Die From A Heatwave Than To Do As Americans
- New Study: NASA’s Models Wildly Underestimate The Capacity Of Clouds To Alter Solar Radiation
