Courts around the country are striking down vaccine mandates and even Covid restrictions in general. Protests against both have erupted the world over. There is a trend in which major names and faces that imposed lockdowns on the country are resigning from their positions and otherwise dropping out of politics. The Biden administration in general has sunk in the polls. The resistance to the entire regime of command and control that seized the world in March 2020 is growing by the day.
But none of this seems to matter to the dominant Internal portals of Google and YouTube, which Google owns. They occupy the number one and number two spots for global traffic and reach. That’s some serious power over what the majority of people read, see, hear, and believe. It’s true that critically thinking people have already shifted to DuckDuckGo, Rumble, and many other platforms, and their market share is growing, to be sure. But nothing can compare to the 75% market share of YouTube, or the 86% share of search controlled by Google.
Often individual users can develop a distorted sense of that whole based on their own browsing habits. You like Brownstone.org, for example, and you get great information from this site. It is easy to forget that its 4 million users seem nearly invisible compared with the traffic enjoyed by the larger sites. Being on the admin side, it is much easier to observe how a myth spread, for example, by CNN can reach tens of millions of people whereas its refutation on a small site might only reach a few thousand. The myth stands.
For this reason, their Terms of Use seriously matter for culture, politics, intellectual life, and public opinion in general. And Google has just changed its terms as they apply to YouTube. It’s a fair presumption that Google’s search results will reflect these same terms. They pertain directly to the science behind Covid, mitigation policies, and mandates on the vaccines. These new terms go into effect on January 6, 2022 (why that date?). If they are truly enforced, freedom of speech and the ability of the scientific process to operate unimpeded will be severely curtailed.
Under the new rules, you cannot claim “that the pandemic is over.” Which is to say, the pandemic is now declared to last forever. You cannot make “claims that any group or individual has immunity to the virus or cannot transmit the virus,” which means that all the science on naturally acquired immunity can be deleted.
You cannot claim that ”vaccines do not reduce risk of contracting COVID-19,” which directly contradicts the FDA: “The scientific community does not yet know if the Pfizer-BioNTech COVID-19 Vaccine will reduce such transmission.” You cannot post “videos alleging that social distancing and self-isolation are not effective in reducing the spread of the virus” and you cannot claim that “wearing a mask causes oxygen levels to drop to dangerous levels.”
And there is this one: you cannot make claims that “achieving herd immunity through natural infection is safer than vaccinating the population,” even though endemicity is inevitable and the vaccines cannot make a substantial contribution to its achievement due to their inability to protect fully against infection and transmission.
As usual, the long list of Do Nots also includes statements that are patently false and otherwise ridiculous – so much so that it seems not dangerous to permit them! The full list is extremely long and includes many fully open questions that Google/YouTube wants to be declared closed. Some of the Do Nots also include statements that are contradicted by statements from Fauci and Biden, such as the rule that you cannot make “claims that any vaccine is a guaranteed prevention method for COVID-19.” The head of the CDC made exactly this claim!
If these rules are strenuously enforced, millions of videos, interviews, television shows, lectures, press conferences, and scientific presentations will disappear. Maybe tens of millions actually. And all in the name of protecting “science” against its corruption, as if YouTube should be the determinant of what constitutes good science.
Here is what Google says about the consequences of violating the rules:
We may allow content that violates the misinformation policies noted on this page if that content includes additional context in the video, audio, title, or description. This is not a free pass to promote misinformation. Additional context may include countervailing views from local health authorities or medical experts. We may also make exceptions if the purpose of the content is to condemn, dispute, or satirize misinformation that violates our policies. We may also make exceptions for content showing an open public forum, like a protest or public hearing, provided the content does not aim to promote misinformation that violates our policies.
If your content violates this policy, we’ll remove the content and send you an email to let you know. If this is your first time violating our Community Guidelines, you’ll likely get a warning with no penalty to your channel. If it’s not, we may issue a strike against your channel. If you get 3 strikes within 90 days, your channel will be terminated.
An intriguing question for any defender of private enterprise – I am certainly that – is why Google would so willingly turn over its platform to a branch of the state and its medical/policy priorities. It cannot be simply the desire to only say true things because there is plenty that is thoroughly disputable in these rules and much has already been challenged by vast quantities of peer-reviewed studies.
How does it come to be that such a huge business can become fully captured by government? I have friends who say it is the reverse actually, that Google has fully captured government, and is driving forward the agenda of politics. Regardless, it becomes a troubled world in which one can no longer distinguish business from the state, or either from big pharmaceutical companies. The state finds it more advantageous to enlist business in its rights violations than risk the court challenges that come with directly violating the First Amendment. The law restricts states in ways that do not apply to private companies, so the answer for the state seems obvious: use the private sector to achieve state policy priorities, particularly as it pertains to controlling the information to which the public has access.
Others might observe that Google has everything to gain from its investment in lockdown policies and mandates, all the better to keep people glued to their personal computers. Even granting that big tech benefited enormously from lockdowns, that’s an outlook on enterprise that is too cynical for me to believe at this stage. Or maybe I’m naive.
What seems clear is that these censorious moves could seriously erode market share and give rise to new platforms that will eventually compete more directly. But before we get too optimistic about this, the time between now and then is a very long time away, while the change in the scientific culture that this move will enact starts next month.
Here is the full text of Google Terms of Use as it pertains to the most critical issues affecting freedom, free speech, and science in the world today. For your research amusement, you can see via the WaybackMachine how this page has expanded over time from its initial page on May 2, 2020, to today.
COVID-19 medical misinformation policy
The safety of our creators, viewers, and partners is our highest priority. We look to each of you to help us protect this unique and vibrant community. It’s important you understand our Community Guidelines, and the role they play in our shared responsibility to keep YouTube safe. Take the time to carefully read the policy below. You can also check out this page for a full list of our guidelines.
YouTube doesn’t allow content about COVID-19 that poses a serious risk of egregious harm.
YouTube doesn’t allow content that spreads medical misinformation that contradicts local health authorities’ (LHA) or the World Health Organization’s (WHO) medical information about COVID-19. This is limited to content that contradicts WHO or local health authorities’ guidance on:
- Treatment
- Prevention
- Diagnosis
- Transmission
- Social distancing and self isolation guidelines
- The existence of COVID-19
Note: YouTube’s policies on COVID-19 are subject to change in response to changes to global or local health authorities’ guidance on the virus. There may be a delay between new LHA/WHO guidance and policy updates given the frequency with which this guidance changes, and our policies may not cover all LHA/WHO guidance related to COVID-19.
Our COVID-19 policies were first published on May 20, 2020.
What this policy means for you
If you’re posting content
Don’t post content on YouTube if it includes any of the following:
Treatment misinformation:
- Content that encourages the use of home remedies, prayer, or rituals in place of medical treatment such as consulting a doctor or going to the hospital
- Content that claims that there’s a guaranteed cure for COVID-19
- Content that recommends use of Ivermectin or Hydroxychloroquine for the treatment of COVID-19
- Claims that Hydroxychloroquine is an effective treatment for COVID-19
- Categorical claims that Ivermectin is an effective treatment for COVID-19
- Claims that Ivermectin and Hydroxychloroquine are safe to use in the treatment COVID-19
- Other content that discourages people from consulting a medical professional or seeking medical advice
Prevention misinformation: Content that promotes prevention methods that contradict local health authorities or WHO.
- Claims that there is a guaranteed prevention method for COVID-19
- Claims that any medication or vaccination is a guaranteed prevention method for COVID-19
- Content that recommends use of Ivermectin or Hydroxychloroquine for the prevention of COVID-19
- Claims that Ivermectin and Hydroxychloroquine are safe to use in the treatment COVID-19
- Claims that wearing a mask is dangerous or causes negative physical health effects
- Claims that masks do not play a role in preventing the contraction or transmission of COVID-19
- Claims about COVID-19 vaccinations that contradict expert consensus from local health authorities or WHO
- Claims that an approved COVID-19 vaccine will cause death, infertility, miscarriage, autism, or contraction of other infectious diseases
- Claims that an approved COVID-19 vaccine will contain substances that are not on the vaccine ingredient list, such as biological matter from fetuses (e.g. fetal tissue, fetal cell lines) or animal products
- Claims that an approved COVID-19 vaccine will contain substances or devices meant to track or identify those who’ve received it
- Claims that COVID-19 vaccines will make people who receive them magnetic
- Claims that an approved COVID-19 vaccine will alter a person’s genetic makeup
- Claims that COVID-19 vaccines do not reduce risk of contracting COVID-19
- Claims that any vaccine causes contraction of COVID-19
- Claims that a specific population will be required (by any entity except for a government) to take part in vaccine trials or receive the vaccine first
- Content that promotes the use of unapproved or homemade COVID-19 vaccines
- Instructions to counterfeit vaccine certificates, or offers of sale for such documents
Diagnostic misinformation: Content that promotes diagnostic methods that contradict local health authorities or WHO.
- Claims that approved COVID-19 tests are dangerous or cause negative physical health effects
- Claims that approved COVID-19 tests cannot diagnose COVID-19
Transmission misinformation: Content that promotes transmission information that contradicts local health authorities or WHO.
- Content that claims that COVID-19 is not caused by a viral infection
- Content that claims COVID-19 is not contagious
- Content that claims that COVID-19 cannot spread in certain climates or geographies
- Content that claims that any group or individual has immunity to the virus or cannot transmit the virus
Social distancing and self isolation misinformation: Content that disputes the efficacy of local health authorities’ or WHO’s guidance on physical distancing or self-isolation measures to reduce transmission of COVID-19.
Content that denies the existence of COVID-19:
- Denial that COVID-19 exists
- Claims that people have not died or gotten sick from COVID-19
- Claims that the virus no longer exists or that the pandemic is over
- Claims that the symptoms, death rates, or contagiousness of COVID-19 are less severe or equally as severe as the common cold or seasonal flu
- Claims that the symptoms of COVID-19 are never severe
This policy applies to videos, video descriptions, comments, live streams, and any other YouTube product or feature. Keep in mind that this isn’t a complete list. Please note these policies also apply to external links in your content. This can include clickable URLs, verbally directing users to other sites in video, as well as other forms.
Examples
Here are some examples of content that’s not allowed on YouTube:
- Denial that COVID-19 exists
- Claims that people have not died from COVID-19
- Claims that any vaccine is a guaranteed prevention method for COVID-19
- Claims that a specific treatment or medicine is a guaranteed cure for COVID-19
- Claims that hydroxychloroquine saves people from COVID-19
- Promotion of MMS (Miracle Mineral Solution) for the treatment of COVID-19
- Claims that certain people have immunity to COVID-19 due to their race or nationality
- Encouraging taking home remedies instead of getting medical treatment when sick
- Discouraging people from consulting a medical professional if they’re sick
- Content that claims that holding your breath can be used as a diagnostic test for COVID-19
- Videos alleging that if you avoid Asian food, you won’t get the coronavirus
- Videos alleging that setting off fireworks can clean the air of the virus and will prevent the spread of the virus
- Claims that COVID-19 is caused by radiation from 5G networks
- Videos alleging that the COVID-19 test is the cause of the virus
- Claims that countries with hot climates will not experience the spread of the virus
- Videos alleging that social distancing and self-isolation are not effective in reducing the spread of the virus
- Claims that wearing a mask causes oxygen levels to drop to dangerous levels
- Claims that masks cause lung cancer or brain damage
- Claims that wearing a mask gives you COVID-19
- Claims that the COVID-19 vaccine will kill people who receive it
- Claims that the COVID-19 vaccine will be used as a means of population reduction
- Videos claiming that the COVID-19 vaccine will contain fetal tissue
- Claims that the flu vaccine causes contraction of COVID-19
- Claims that COVID-19 vaccines are not effective in preventing the spread of COVID-19
- Claims that the COVID-19 vaccine causes contraction of other infectious diseases or makes people more vulnerable to contraction of other infectious diseases
- Claims that the COVID-19 vaccines contain a microchip or tracking device
- Claims that achieving herd immunity through natural infection is safer than vaccinating the population
- Claims that COVID-19 never causes serious symptoms or hospitalization
- Claims that the death rate from the seasonal flu is higher than the death rate of COVID-19
- Claims that people are immune to the virus based on their race
- Claims that children cannot or do not contract COVID-19
- Claims that there have not been cases or deaths in countries where cases or deaths have been confirmed by local health authorities or the WHO
Educational, documentary, scientific or artistic content
We may allow content that violates the misinformation policies noted on this page if that content includes additional context in the video, audio, title, or description. This is not a free pass to promote misinformation. Additional context may include countervailing views from local health authorities or medical experts. We may also make exceptions if the purpose of the content is to condemn, dispute, or satirize misinformation that violates our policies. We may also make exceptions for content showing an open public forum, like a protest or public hearing, provided the content does not aim to promote misinformation that violates our policies.
What happens if content violates this policy
If your content violates this policy, we’ll remove the content and send you an email to let you know. If this is your first time violating our Community Guidelines, you’ll likely get a warning with no penalty to your channel. If it’s not, we may issue a strike against your channel. If you get 3 strikes within 90 days, your channel will be terminated. You can learn more about our strikes system here.
We may terminate your channel or account for repeated violations of the Community Guidelines or Terms of Service. We may also terminate your channel or account after a single case of severe abuse, or when the channel is dedicated to a policy violation. You can learn more about channel or account terminations here.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
December 3, 2021
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science | Google, YouTube |
Leave a comment
I HAVE just been alerted to the Government’s new Myocarditis and pericarditis after Covid 19 vaccination: guidance for healthcare professionals, published four days ago on Monday. It makes chilling reading.
You can read it here.
First, it is a clear admission of that myocarditis is a serious post-vaccine adverse reaction risk. Second, amongst the usual and increasingly implausible disclaimers like ‘it is a rare condition’ and ‘it is usually mild or stable and most patients typically recover fully without medical treatment’, comes the terrifying admission that ‘a high percentage of children admitted to hospital with myocarditis have significant left ventricular fibrosis and no follow-up data is available yet on hospitalised patients.’
So does it recommend halting the vaccine programme for children, given ‘that no follow-up data is available yet on hospitalised patients’?
No.
In complete defiance of any precautionary principle the subtext of this disturbing document is that these are reactions that are expected, not to be alarmed by and to be lived with as an inevitable consequence of the vaccination, giving what should be self-evident advice that though ‘the majority of cases appear to be mild and self-limiting; any acutely ill or unstable patients should be referred to hospital directly’. As though an acutely ill child was not normally treated as an emergency and rushed to hospital.
Furthermore, how they can claim to know at this stage that ‘ the majority of cases are mild and self-limiting’ in the absence of rigorous and systematic follow-up health checks on such children? It beggars belief and betrays an astonishingly cavalier attitude to children.
Even more chilling, if that were possible, is the publication of this document on the very same day that the JCVI decided to recommend second vaccine doses for 12-15s.
The opening few bullet points include these gems:
· Myocarditis – significant left ventricular (LV) fibrosis has been described in a high percentage of children admitted to hospital, with a small percentage of these having non-sustained ventricular tachycardia (VT);
· No follow-up data is available yet on hospitalised patients;
· The long-term consequences of this condition secondary to vaccination are yet unknown, so any screening recommendations need to be balanced against the frequency and severity of the disease with the aim to prevent complications, in particular of myocarditis (arrhythmias, long term myocardial damage or heart failure).
The question is also raised as to why would a GP not refer every child or youth with suspected myocarditis or pericarditis to the paediatric team for a full assessment, especially given this is a vaccine still under emergency use authorisation requiring proper post marketing surveillance? Perhaps the government doesn’t want to find too many cases?
Please, please do anything and everything you can to bring this to the attention of parents.
Some 80 per cent of school children* are estimated to have had Covid already and so have nothing to gain from vaccination, only the potential risk of harm.
*MRC Biostatistics Unit’s statistics on infections and deaths, which are updated once a week using ONS data, estimates that 5.53 million 5-14-year-olds in England have had Covid. This is of a total population of 6,975,037.
December 3, 2021
Posted by aletho |
Science and Pseudo-Science, War Crimes | COVID-19 Vaccine, UK |
Leave a comment
You may think that climate science is complicated and that the scientists who are alarmed about climate change know what they are doing. Well, yes and no. The climate is complicated but scientists have bought into some very silly science.
Happily this is all easy to see with no science involved. Seriously, don’t back away. There is no science coming, especially nothing hard. Happily the world’s top alarmists have provided everything we need in a very simple way. Of course they do not see it because they are committed to alarmism. But I will point it out and you can use your own judgement.
Here goes. Globally, climate alarmism is led by the United Nations. Huge sums of money are at stake but that is not the point here, although it does explain much of what is going on. On the science side alarmism is led by the UN’s Intergovernmental Panel on Climate Change, usually just called the IPCC.
“Intergovernmental” sounds like a word you might learn as a joke. In this case it means that the members of this Panel are most of the world’s national governments. Most or maybe all of these governments pay lip service to climate alarmism.
Every five years or so the IPCC puts out a monster report that claims to be an overview of the latest climate science. In reality they just pick the science that best supports alarmism. This year is one of those years and they outdid themselves. Instead of the usual 1,000 page report it is a whopping 4,000 pages. Of course no one in their right mind will read it, but it sure shows how smart they are, right?
Where it gets useful is that there is a 40 page Summary for Policy Makers, which means for ordinary people. Anyone who votes is a policy maker of sorts. It is here that we find the basic scientific arguments for alarmism and they don’t amount to much.
In fact there are just two arguments for alarmism, which occur as two windows in the very first figure. They are labeled figure 1a and 1b. They are easy to describe so you don’t have to look them up. If you want to see them go here: https://www.ipcc.ch/report/ar6/wg1/.
Figure 1a is called the Hockey Stick by skeptics of alarmism (like me). It claims to be the global average temperatures for the last 2,000 years (like we can know that). It is pretty much a flat line until about 150 years ago and this is the hockey stick handle. Then it suddenly shoots up with big rapid warming from then until now, making the hockey stick blade. Handle flat then blade pointing up.
In short they say there was no global warming until we started it 150 years ago. What makes this silly is that there is lots of evidence for two prior periods of warming that may have been just as warm as today’s. These are so well known that they have names — the medieval warm period (when Vikings farmed Greenland) and the Roman warm period (when civilization flourished).
In between there were really cold spells including the little ice age that ended with the recent warming. In fact our warming may be nothing but the natural end to the little ice age.
There are thousands of research reports on these natural periods of warming and cooling but the IPCC simply ignores them. Alarmism depends on the recent warming being unprecedented. Natural warming disappears. Do not look behind the curtain!
So much for the bogus hockey stick. Figure 1b then zooms in on the recent warming, with a fancy variation on the same disappearing act. This time it is about the computer models of climate change, which is where alarmism comes from. It is these silly computer models that say we are causing dangerous global warming, with worse to come.
Figure 1b shows two computer model outputs. Each line is the global temperature over the last 150 years, when the recent warming occurred. One is supposedly the temperature history as it would have been without human interference, the natural history, and the other is the history with human inputs. Guess what? The natural history has no warming, while the human history shows all the warming that has occurred over the period.
The IPCC says this proves all the warming is caused by us humans. What makes this silly is figure 2, which gives the game away. It is a list of all the things in the models that can cause warming. All are human! There are no natural causes.
This means the models are programmed so that only humans can cause warming. Thus what figure 1b really says is “If we assume that only humans can cause long term warming then we find that the long term warming is caused by humans”. This is called circular reasoning because the conclusion is just a restatement of the assumption. It is truly silly.
What is missing of course is just what was missing In the hockey stick, namely nature. There is actually a great deal of research on possible natural causes for some of the long term warming, maybe even all of it. Keep in mind that the recent warming is very small, just around one degree over 150 years. Small changes in the sun, or the ocean, or even just in the clouds, could easily cause this little bit of global warming.
The IPCC simply ignores all this research, just like it ignored the warm and cold periods in the 2,000 year hockey stick. In fact this extreme alarmist bias dominates government funded climate science, which is most of it.
That is really all there is to alarmist science and it sure is silly! No deep scientific mystery. Just assume that everything that happens is our fault, program the computers that way, and let the computer then predict worse to come. Ignore all the research that says otherwise. Ignore the little ice age and the medieval warm period. Ignore natural change even though it is right in front of us.
Ignoring nature is the silly science of climate alarmism.
Reprinted with added stuff from RANGE magazine, Winter 2021/2022 issue. For more information see http://www.rangemagazine.com
December 3, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | IPCC |
Leave a comment
WaPo : Less than a week after the new omicron variant of the coronavirus was reported to the World Health Organization, global leaders on Wednesday agreed to start negotiations to create an international agreement to prevent and deal with future pandemics — which some have dubbed a “pandemic treaty.” The special session of the World Health Assembly, only the second ever held by the WHO’s governing body, pledged by consensus to begin work on an agreement, amid a round of applause, after three days of talks. “I welcome the decision you have adopted today, to establish an intergovernmental negotiating body to draft and negotiate a WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response,” WHO Director General Tedros Adhanom Ghebreyesus said. The commitment by countries to negotiate a “global accord” would “help to keep future generations safer from the impacts of pandemics,” he added.
The assembly’s decision will see the creation of an “intergovernmental negotiating body” to draft and negotiate the final convention, which would then need to be adopted by member states. … Tedros said omicron “demonstrates just why the world needs a new accord on pandemics,” and called for a “legally binding” agreement.
#
Marc Morano’s comment: “This will be a virus version of the UN IPCC & Paris climate style pacts. The pandemic ‘crisis’ will become permanent just like the ‘climate crisis.’ Attempts to impose lockdowns for future COVID variants or new viruses may be internationally imposed instead of national, state or local. If you don’t like your governor, mayor or school board, you can vote them out, but if a ‘radical’ WHO ‘pandemic treaty’ that is ‘legally binding’ becomes reality, global mandates may be coming your way and local elections will cease to matter as unelected bureaucrats will be yielding the real power over your life, liberty, and pursuit of happiness. This must be stopped now. Even the Washington Post is calling a ‘pandemic treaty’ a ‘radical’ idea.
Once a ‘pandemic treaty’ is set in place, COVID mandates will become permanent as elite officials fly around the world to discuss how to further crush freedom to wage war on viruses. Just like the UN Intergovernmental Panel on Climate Change, the architects of a ‘pandemic treaty’ will seek more and more power and control and become a self-interested lobbying organization all while doing squat to prevent or mitigate future viruses. A ‘radical’ WHO ‘pandemic treaty’ may be just the ticket for the administrative state to reign in rogue anti-lockdown governors like Ron DeSantis.”
December 3, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Human rights, WHO |
Leave a comment
I’ve written about vitamin D as a potential treatment for covid-19 a couple of times before. In September of 2020 I wrote about a Spanish randomized trial that showed a massive reduction in ICU admissions in hospitalized patients treated with 25-hydroxyvitamin D (a part-activated form of vitamin D). However, that study had some major weaknesses – it was completely unblinded and it was small. In other words, although the results were promising, they hardly constituted conclusive proof of a benefit.
Then, in January, I wrote about a much larger double-blind Brazilian trial that failed to show any benefit when hospitalized patients were treated with vitamin D. For many in the mainstream medical community, this study constituted conclusive proof that vitamin D is ineffective as a treatment for covid-19. However, participants in the trial weren’t given vitamin D until late in the disease course, and unlike in the previous Spanish study, they were given regular vitamin D, not the part-activated form used in the Spanish study. Since it takes several days for regular vitamin D to become activated and usable by the body, the study was more or less designed to fail from the start – whether intentionally or unintentionally. There was no realistic chance that it was ever going to show a benefit, even if one exists.
So, when I last wrote about vitamin D, in January, it was still unclear whether it had any role in the treatment of covid-19 or not. Well, has anything changed since then?
Let’s start by taking a look at the observational data. Although the randomized trials of vitamin D have been few and far between, there has been a massive amount of observational data produced. In recent months, two meta-analyses of cohort studies have been published that look at the relationship between vitamin D levels and death, one in the journal Nutrients, and another in the Nutrition Journal. For those who are unaware, a meta-analysis is a pooled study, where you take lots of different studies and pool their results together in to one, in order to get more statistically significant results. And a cohort study is a type of observational study in which you take two or more groups that vary in some specific way, such as in their vitamin D levels, and then follow them over time to see if they have different outcomes.
Interestingly, the two meta-analyses reach the exact opposite conclusions, with one claiming that if we can just get everyone up to 50 ng/ml of vitamin D in the blood stream, then we can literally prevent all covid deaths, while the other says that there is no correlation whatsoever between vitamin D levels and covid mortality.
How is this possible?
Well, the first thing to note is that the two meta-analyses vary in terms of which particular studies they include. The Nutrients study performed its data search in March, while the Nutrition Journal study performed its data search in June. This means that the Nutrition Journal meta-analysis had access to a few extra studies, which weren’t available when the first data search was conducted in March.
But that isn’t the whole explanation. The researchers have also used somewhat different search strategies, which means that each includes some studies that the other lacks. In fact, there is amazingly little overlap between the two meta-analyses in terms of which studies are included. Only two of the seven studies in the Nutrients meta-analysis are included in the Nutrition Journal meta-analysis, and only two of the eleven studies in the Nutrition Journal meta-analysis are included in the Nutrients meta-analysis. No wonder they’re able to reach such divergent results!
This really showcases how easy it is to manipulate meta-analyses so that they show what you want them to show, just by choosing the date on which you extract data and by choosing which specific search terms to use. It’s easy to keep modifying search terms slightly until you get a list that includes the studies you want in, and excludes the studies you want out. Which is why we should always be skeptical of meta-analyses, just as we are with other types of studies.
This explains why we saw a similar phenomenon earlier this year, when half the meta-analyses of ivermectin seemed to show massive benefit and the other half seemed to show no benefit whatsoever.
Meta-analyses are often considered to be the pinnacle of evidence based medicine, but considering how easy they are to game, I think that is wrong. I’d rather have a single large, well done study than a meta-analysis that consists of lots of little studies, even if that meta-analysis includes more participants overall. If all scientists were honest, then meta-analyses would be an excellent tool for determining the truth. But since we know that many scientists aren’t honest, their use is far more limited. At the end of the day we all have to do our own due diligence. The only meta-analyses that I trust fully are the ones I do myself, such as one I did earlier this year on ivermectin.
It is interesting to note though, that the Nutrition Journal study, which came to the conclusion that vitamin D had no effect, actually had results that did suggest benefit. All the included studies showed fewer deaths in the group with a higher vitamin D level, although the results were not able to reach statistical significance overall.
So we have one meta-analysis which shows a large benefit, and one which shows a trend towards benefit. Which is encouraging. Of course, these are observational studies, and so can’t really say anything about cause and effect. People with low vitamin D levels probably spend less time outdoors, which means they’re probably less physically active. And they probably consume a different diet from people with high vitamin D levels. Correlation is not causation, and even if a correlation is seen between vitamin D and death from covid in observational studies, that doesn’t mean it’s the vitamin D that’s preventing the deaths.
So, what we need is good data from randomized trials. As mentioned, the data from randomized trials that existed last time I wrote about vitamin D was limited and mixed, with the Spanish study that gave 25-hydroxyvitamin D showing massive benefit, while the Brazilian study that gave regular inactivated vitamin D showed no benefit whatsoever.
Since then, three new randomized trials have been published, one from India, one from Mexico, and one from Saudi Arabia. Unfortunately, all three were small, with the largest of the three only including 87 patients. Additionally, all three gave regular inactivated vitamin D, not the part-activated form that was found to have an effect in the earlier Spanish study. In other words, the new studies don’t add anything on top of the store of knowledge that we already had in January.
So, we’re actually more or less in the same situation that we were in regarding vitamin D back in January. The observational data suggests that there is a benefit to supplementing with regular vitamin D for prophylaxis, which is in line with a systematic review that was published in the British Medical Journal in the pre-covid era, which found that people with low vitamin D levels who supplement daily with vitamin D reduce the frequency of respiratory infections by half. And the limited randomized trial data that exists suggests that the part-activated 25-hydroxyvitamin D formulation can reduce the risk of bad outcomes if given on admission to hospital. But the evidence is still too weak to draw any firm conclusions.
It’s quite shocking that more data isn’t available to answer this question conclusively at this late stage in the pandemic. I do personally think though, based on the evidence that is available, that it makes sense to take a daily vitamin D supplement. 4,000 IU (100 mcg) is a reasonable dose. It’s safe, it’s cheap, it might well help, and it can’t hurt.
December 3, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, Vitamin D |
Leave a comment
German physician-scientists reported Monday that not a single healthy child between the ages of 5 and 18 died of Covid in Germany in the first 15 months of the epidemic.
Not one.
Even including children and adolescents with preexisting conditions, only six in that age range died, the researchers found. Germany is Europe’s largest country, with more than 80 million people, including about 10 million school-age children and adolescents.
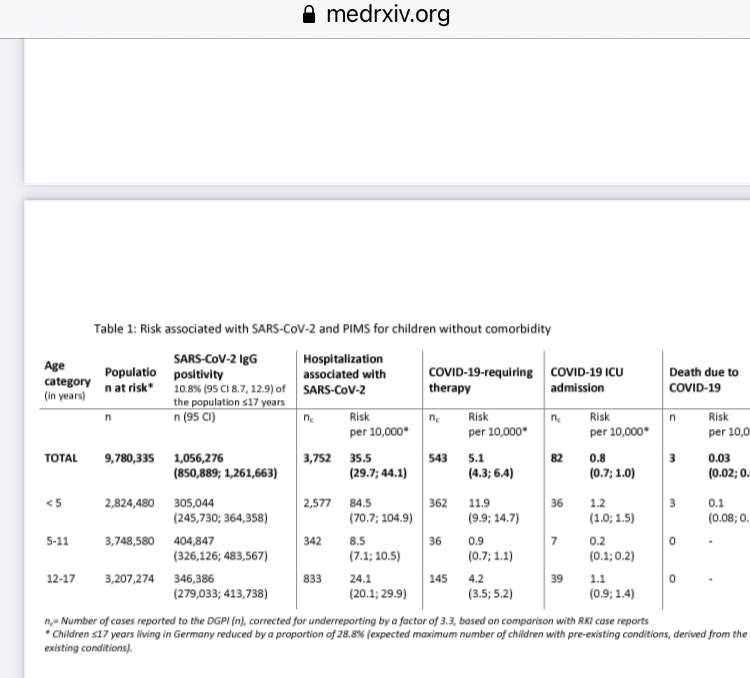
Serious illness was also extremely rare. The odds that a healthy child aged 5-11 would require intensive care for Covid were about 1 in 50,000, the researchers found. For older and younger children, the odds were somewhat higher, about 1 in 8,000.
Another eight infants and toddlers died, including five with preexisting conditions. In all, 14 Germans under 18 died of Covid, about one per month. About 1.5 million German children or adolescents were infected with Sars-Cov-2 between March 2020 and May 2021, the researchers found.
“Overall, the SARS-CoV-2-associated burden of a severe disease course or death in children and adolescents is low,” the researchers reported. “This seems particularly the case for 5-11-year-old children without comorbidities.”
The researchers reported their findings in an 18-page paper published to the medrxiv preprint server on Monday.
The data came from a registry Germany established in March 2020 intended to capture all hospitalizations of people under 18 with Covid. All German children’s hospitals, pediatric infectious disease specialists, and pediatric societies were invited to participate.
British researchers have posted similar findings, reporting that only six healthy children (including those under 18) out of 12 million died of Covid.
Given the known risks of vaccine-induced myocarditis in young men, the fact that Pfizer tested its mRNA vaccines on barely 3,000 children 5-11 and followed most of them for only weeks after the second dose, the German data again raises the question of how health authorities can possibly justify encouraging children or teenagers to be vaccinated.
But they have.
So parents will have to decide what’s best for their children (at least in those states that bar vaccine fanatics from trying to vaccinate teenagers without parental consent).
December 3, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Germany, Human rights |
Leave a comment
The Occupational Safety and Health Administration’s controversial plan to enforce COVID-19 vaccinations for large businesses—recently enjoined by the Fifth Circuit Court of Appeals— was ostensibly designed to minimize “deadly outbreaks of COVID-19.” The ability of COVID-19 vaccines to protect life is at the heart of the OSHA mandate and the fierce debate over similar mandates now embroiling much of the world.
Nearly 18,000 scientific papers have been published since last year on COVID-19 and vaccines, so the task of sifting through the evidence to help critically evaluate whether vaccines reduce risk of death seems daunting. It turns out, though, that two studies stand so far above the rest in terms of rigor and quality that they are uniquely suited to help us address the question of vaccine protection.
These two studies, published last month in the New England Journal of Medicine, are fundamentally distinct from the other studies in that they are the only clinical trials yet reported to randomize adults to receive either a COVID-19 vaccine (Pfizer or Moderna) or a placebo injection and then follow them over time. Why is this important? Because the randomized controlled study design they used is the gold standard and most rigorous scientific tool available to examine cause and effect relationships between an intervention and outcome (vaccination and death, in this case).
This design also limits as much as possible the influence of other factors, whether known or unknown, that could affect the outcome. Many studies have used other designs to try and understand how well the COVID-19 vaccine protects against death, but no matter how well planned or executed, none of these studies approaches the level of scientific rigor that a well-conducted randomized controlled trial offers.
So did these two clinical trials find that vaccination reduced the risk of dying from COVID-19? The Moderna study reported one death from COVID-19 in the vaccinated group and three in the unvaccinated group, far too few to make any statistical conclusion. The Pfizer trial was even more inconclusive because the findings published in the New England Journal report (one COVID-19 death in the vaccinated group and two in the unvaccinated group) differed from what Pfizer later reported to the Food and Drug Administration, and the FDA update did not specify the number of COVID-19 deaths.
Regardless, the most relevant study endpoint is not death from COVID-19 but all-cause mortality, which counts every death that occurred during the study period. All-cause mortality is the key outcome of interest not simply because it circumvents the oftentimes subjective decision as to why someone died but also because it balances all the possible effects of a COVID-19 vaccine, both good and bad, that could influence risk of death. In other words, it allows us to quantify lives saved by the COVID-19 vaccine while taking into account potential lives lost from vaccine-related heart disease, blood clots, severe allergic reactions, and perhaps other causes.
Because results from the two trials were so similar regardless of the type of vaccine used it is helpful to merge the results. Following a combined total of 74,580 individuals, half given the COVID-19 vaccination and half given a placebo shot, over six to seven months, the two studies reported that thirty-seven people who were vaccinated died as compared to thirty-three people who received placebo.
Simply put, the very best scientific evidence currently available to mankind does not support the widely held contention that COVID-19 vaccination using the Pfizer or Moderna brands lowers risk of death, at least over the first half-year after vaccination. Interestingly, these striking findings were not reported in the main body of the papers but in supplemental sections.
There are several additional points to consider.
First, the studies’ findings were limited by the fact that their design did not take into consideration previous infection leading to subsequent immunity from COVID-19 infection, which could very well have lowered risk of death in one or both study groups.
Second, there are serious concerns over falsification of data and other data integrity issues in the Pfizer trial so this could also have influenced results. Importantly, because both trials mostly excluded groups at highest risk of dying from COVID-19 such as the frail elderly, the very obese, or those with serious chronic illnesses, we cannot assume that the vaccines do not protect against death in these populations.
Based on my clinical judgment and lesser quality supportive evidence, I generally assume when treating such patients that the vaccine’s benefits outweigh its risks and so advocate for their use, though I cannot be absolutely certain they offer protection against death because of the lack of randomized controlled evidence.
Finally, the very low rates of death from COVID-19 observed in both studies should serve to remind us of how minimal this risk is in the general population.
Perhaps the key takeaway message is that absolutist, rigid COVID-19 vaccine mandates such as that put forth by OSHA are not based on best science. Such mandates run counter to the universal medical dictum of risk stratification, whereby treatment is tailored to individuals based on individual risks and benefits to be accrued. They also violate the dominant philosophy of evidence-based medicine, which supports the use of current best evidence when making decisions about patient care.
The Pfizer and Moderna trials show that in lower risk populations (which account for most of society) COVID-19 vaccines do not reduce mortality. Therefore, vaccine mandates, which are enormously costly and terribly divisive, are a cure worse than the disease.
Allon Friedman is a Professor of Medicine at Indiana University School of Medicine and a medical researcher focusing on topics related to kidney disease. The ideas expressed in the article are entirely his own and not necessarily those of his employer.
December 3, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | COVID-19 Vaccine, Human rights |
Leave a comment
ICYMI, here’s the URL to file your comments before the comment period closes on December 6, 2021.
In a nutshell, OSHA believes that:
- Face coverings work and should be used.
- COVID recovered people who have not been fully vaccinated still face a grave danger from workplace exposure to SARS-CoV-2.
- They should impose a strict vaccination mandate ( i.e., all employers required to implement mandatory vaccination policies as defined in this ETS) with no alternative compliance option.
I believe:
- The scientific evidence (Danish mask study, Bangladesh mask study) shows that face coverings are completely ineffective.
- COVID recovered people should be exempt from all rules. If COVID recovered people are re-infected, they don’t get hospitalized, don’t die, and don’t spread the virus to others. The CDC has no counter-examples.
- The vaccines kill more people than they save for all age groups according to the VAERS data. And even in Pfizer’s own study, there were significantly more deaths in the vaccine group than then in the placebo group. There is ZERO scientific evidence the vaccines save lives when you are looking for a reduction in all cause mortality. Businesses should BE PROHIBITED from requiring vaccination.
One of us is wrong. If you agree with me, please consider taking a few minutes to file a comment.
December 3, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science, Solidarity and Activism | Covid-19, COVID-19 Vaccine, Human rights, United States |
Leave a comment
THIS is just staggering in its predatory mendacity.
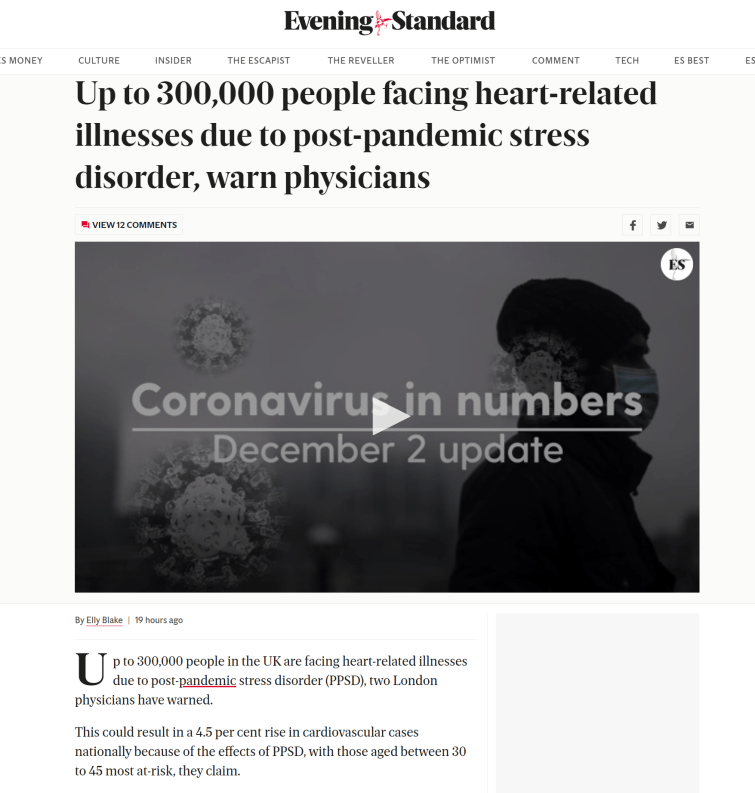
there is not a shred of evidence to support it nor any remotely plausible reason to even put forward such a hypothesis.
frankly, it’s patently absurd and has no precedent in other stressful events. being bombed nightly during the blitz did not cause this.
this is a desperate lie from a desperate class of state run doctors desperate to shift the blame for that which they have wrought.
nothing more.
you can tell a lot about what people are afraid of when they start answering questions that were not really asked.
it goes double when the answers don’t make any sense.
there is no question that lockdowns, social alienation and ostracization, etc have caused piles of mental health problems. this is what makes it a great smokescreen. but there is no way that’s translating to heart attacks, strokes, blood clots, and myo- and pericarditis in young people like this. it doesn’t do that (or at least not to any meaningful extent).
what DOES do that are these vaccines. and it concentrates MOST in the young and, seemingly, in athletes.
these truths are gaining currency. this is a clear counter-lie/backfire set to try to head them off and provide a false explanation for these increasingly unavoidably obvious outcomes.
there is a point where one cannot plead incompetence any longer, a line across which one becomes deliberately pernicious and predatory and seeks to lie to save their own hide at the expense of others.
reasonable people might argue about where that is.
but this is WAY over that line. it’s pure propaganda and cannot even be couched as “it’s for their own good.” this is an attempt to mask and shift the cause of serious harm while allowing that harm to continue.
it’s just the next extension of this already failing lie: (previously debunked HERE)

it’s really very simple. this heart risk outcome has become too prevalent to hide. so they need to shift the blame and they are willing to lie to the people and keep harming them to do so.
period.
Full article
December 3, 2021
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine |
Leave a comment
It took the U.S. Food and Drug Administration 108 days to review all the data Pfizer/BioNTech submitted in order to gain FDA approval for its Comirnaty COVID shot, which was licensed August 3, 2021.
Considering the agency claims there are 329,000 pages of data, the fact that they were able to read, analyze and draw conclusions about its safety and effectiveness in just 108 days — about 80,000 pages a month — is no small miracle. They must employ some very efficient speed readers.
And that is why the FDA’s claim that it now needs half a century to review the documents before they can release them to the public doesn’t seem very credible. Even Reuters has expressed shock, and its former CEO is on the board of Pfizer.1
Expedited FOIA Request for Comirnaty Data
In September 2021, a group called Public Health and Medical Professionals for Transparency (PHMPT) filed a Freedom of Information Act (FOIA) request with the FDA to obtain the documentation used to approve Comirnaty.
This includes safety and effectiveness data, adverse reaction reports and lists of active and inactive ingredients. Approximately 400 additional FOIA requests by other individuals for all or part of this information have also been filed.2
In their FOIA application, the PHMPT asked the agency to expedite release of the documents — a reasonable request, considering we have no raw data and the shots are being pushed on children as young as 5.
FOIA guidelines include two conditions upon which a request may be expedited. One is “if the lack of expedited treatment could reasonably be expected to pose a threat to someone’s life or physical safety,” which one could easily argue is the case here.
The second condition is “if there is an urgency to inform the public about an actual or alleged federal government activity, if made by a person who is primarily engaged in disseminating information.” This too is clearly applicable.
“During a time when COVID-19 vaccine mandates are being implemented over the objection of those that have questions about the data and information supporting the safety and efficacy of the Pfizer Vaccine, and individuals with these questions are being expelled from employment, school, transportation, and the military, the public has an urgent and immediate need to have access to this data,” the PHMPT said in its request.3
FDA Now Wants 55 Years to Release COVID Jab Data
When, after a month, the FDA still had not responded to the FOIA request, the PHMPT sued.4 The FDA is now asking a federal judge to allow them to delay the full release of all documents until 2076 — 55 years from now.
According to the U.S. Department of Justice (DOJ) attorney who represents the FDA in this case, the agency will be able to “provide more pages to more requesters” if allowed to stick to a rolling schedule of 500 pages per month, “thus avoiding a system where a few large requests monopolize finite processing resources.”
They claim they only have 10 employees assigned to FOIA releases, and before material can be released, an FDA official has to go through them and redact any information that might reveal personal information about clinical trial participants and any confidential business or trade secret information.
The 1967 FOIA law requires federal agencies to respond to FOIAs within 20 days unless “unusual circumstances” exist that prevent a timely release. Circumstances that might warrant an extended release schedule include:
- Instances where response records must be searched for and collected from an entity other than the office processing the request
- Situations involving “voluminous” amounts of records that must be compiled, and
- Instances requiring consultation with another federal agency that has a substantial interest in the information
The DOJ attorney points out that the court has allowed for a 500-page maximum per month release schedule in other cases, and should allow the FDA the same leeway here.
Plaintiffs, on the other hand, argue the agency should be able to release everything by early March 2022, noting the FDA employs 18,000 people and has an annual budget of $6 billion. Between 2008 and 2017, the agency processed 114,938 FOIA requests, of which it granted 72.4%, either fully or partially.
Of those, 39.8% were designated as “complex,” and 81.5% of these complex FOIA requests were granted in 61 days or more. Considering these historical statistics, a backlog of 400 FOIA requests doesn’t appear excessively burdensome.
FDA’s Foot-Dragging Is Suspicious
Then there’s the sticky issue that it has already proven its capacity for rapid review. Aaron Siri of the law firm Siri & Glimstad wrote in the PHMPT’s court filing:5,6,7,8
“This 108-day period is the same amount of time it took the FDA to review the responsive documents for the far more intricate task of licensing Pfizer’s COVID-19 vaccine …
It took the FDA precisely 108 days from when Pfizer started producing the records for licensure to when the FDA licensed the Pfizer vaccine. Taking the FDA at its word, it conducted an intense, robust, thorough, and complete review and analysis of those documents in order to assure that the Pfizer vaccine was safe and effective for licensure.
While it can conduct that intense review of Pfizer’s documents in 108 days, it now asks for over 20,000 days to make these documents available to the public …
The entire purpose of the FOIA is to assure government transparency. It is difficult to imagine a greater need for transparency than immediate disclosure of the documents relied upon by the FDA to license a product that is now being mandated to over 100 million Americans under penalty of losing their careers, their income, their military service status, and far worse.”
Shocking Revelations in First Batch of FOIA Docs
Two months after the lawsuit against it was filed, the FDA released a batch of 91 pages,9 and if this batch is any indication, it’s not surprising that the FDA wants to slow-walk the release of the rest. In a November 21, 2021, substack article, Kyle Becker cites directly from the released documents:10
“’It is estimated that approximately [REDACTED] doses of BNT162b2 were shipped worldwide from the receipt of the first temporary authorization for emergency supply on 01 December 2020 through 28 February 2021,’ the document states. ‘Cumulatively, through 28 February 2021, there was a total of 42,086 case reports (25,379 medically confirmed and 16,707 non-medically confirmed) containing 158,893 events …
Most cases (34,762) were received from United States (13,739), United Kingdom (13,404) Italy (2,578), Germany (1913), France (1506), Portugal (866).’ Below is a General Overview of the reported outcomes to the Adverse Events:
The chart lists 1,223 fatal outcomes in the Relevant Cases. Interestingly, the age range with the most relevant cases was 31-50 years old, which is not the age group considered to be at high risk from COVID-19.”
It’s worth noting that by redacting the specified number of doses shipped, it becomes more difficult to assess the potential ratio of injury. Still, even without that, 42,086 reports of injury, including 1,223 fatalities, are a significant signal in and of itself, especially when you consider that the 1976 swine flu vaccine was pulled after 25 deaths.
Glaring Disregard for Life
It’s even more disturbing when you consider that those 42,086 reports were received by Pfizer in just the first 2.5 months of the shot being rolled out. Pfizer even acknowledges the abnormal rate of injuries, but then sweeps it aside as being of no consequence. As noted by Siri, in a November 19, 2021 substack article, in which he discusses this first batch of documents:11
“Pfizer explains, on page 6, that ‘Due to the large numbers of spontaneous adverse event reports received for the product, [Pfizer] has prioritized the processing of serious cases…’
Pfizer ‘has also taken a [sic] multiple actions to help alleviate the large increase of adverse event reports’ including ‘increasing the number of data entry and case processing colleagues’ and ‘has onboarded approximately [REDACTED] additional fulltime employees (FTEs).’
Query why it is proprietary to share how many people Pfizer had to hire to track all of the adverse events being reported shortly after launching its product …
But no cause for alarm since Pfizer explains to the FDA: ‘The findings of these signal detection analyses are consistent with the known safety profile of the vaccine.’ So, if they knew these issues were going to arise, then why didn’t they appear to have enough staff to process this expected volume of reports?
The grand conclusion by Pfizer to the FDA: ‘The data do not reveal any novel safety concerns or risks requiring label changes and support a favorable benefit risk profile of to the BNT162b2 vaccine.’ Nothing to see here.”
Clearly, there’s plenty to be seen in the hundreds of thousands of documents Pfizer/BioNTech submitted to the FDA. The fact that the FDA is stonewalling and wants 55 years to redact them before they’re fit for public view is telling in and of itself.
You don’t need a fanciful imagination to comprehend what they might be hiding. It almost seems they want to make sure the responsible parties are all dead by the time the full data set is out in the open and people can be held to account for their decisions. Let’s hope the judge is more interested in public health than protecting the FDA’s dirty secrets.
Sources and References
December 3, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, FDA, United States |
Leave a comment