Vaccine Rollout Correlates With 25% Spike in Cardiac Arrest Emergency Calls for Young Adults, Study Finds

By Will Jones | The Daily Sceptic | April 29, 2022
Emergency calls for cardiac arrest and acute coronary syndrome in young people in Israel were significantly associated with the vaccine rollout, both first and second doses, spiking 25% higher than in earlier years, but not with COVID-19 prevalence, a study in the Nature journal Scientific Reports has found.
Using data from the Israel National Emergency Medical Services (EMS) from 2019 to 2021, the study looked at the volume of cardiac arrest and acute coronary syndrome EMS calls in the 16-39 year-old population. It found an increase of over 25% in both call types during January-May 2021, compared with 2019-2020, but no significant increase in calls correlating with COVID-19 infection rates.
The main finding of this study concerns with increases of over 25% in both the number of CA [cardiac arrest] calls and ACS [acute coronary syndrome] calls of people in the 16-39 age group during the COVID-19 vaccination rollout in Israel (January-May, 2021), compared with the same period of time in prior years (2019 and 2020). Moreover, there is a robust and statistically significant association between the weekly CA and ACS call counts, and the rates of first and second vaccine doses administered to this age group. At the same time there is no observed statistically significant association between COVID-19 infection rates and the CA and ACS call counts. This result is aligned with previous findings which show increases in overall CA incidence were not always associated with higher COVID-19 infections rates at a population level, as well as the stability of hospitalisation rates related to myocardial infarction throughout the initial COVID-19 wave compared to pre-pandemic baselines in Israel. These results also are mirrored by a report of increased emergency department visits with cardiovascular complaints during the vaccination rollout in Germany as well as increased EMS calls for cardiac incidents in Scotland.
While several studies have found severe myocarditis to be a rare adverse effect of the vaccines, the study authors note that myocarditis is often missed, and in fact has been found to be likely responsible for 12-20% of unexpected deaths in adults under 40 in normal times.
Myocarditis is a particularly insidious disease with multiple reported manifestations. There is vast literature that highlights asymptomatic cases of myocarditis, which are often underdiagnosed, as well as cases in which myocarditis can possibly be misdiagnosed as acute coronary syndrome (ACS). Moreover, several comprehensive studies demonstrate that myocarditis is a major cause of sudden, unexpected deaths in adults less than 40 years of age, and assess that it is responsible for 12-20% of these deaths. Thus, it is a plausible concern that increased rates of myocarditis among young people could lead to an increase in other severe cardiovascular adverse events, such as cardiac arrest (CA) and ACS. Anecdotal evidence suggests that this might not be only a theoretical concern.
The results, shown visually in the following graphs, are unmistakable, with clear corresponding spikes in vaccination numbers and emergency calls.


The study does not look at death rates in the age group, but data elsewhere show a clear spike in deaths during the period.

SPR/CBS
Surely it’s well past time these experimental vaccines (in Israel’s case, Pfizer), rushed to market in record time, are withdrawn for younger people.
1.2 Million Reports of Injuries After COVID Vaccines, VAERS Data Show
By Megan Redshaw – The Defender – April 29, 2022
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,247,131 reports of adverse events following COVID-19 vaccines were submitted between Dec. 14, 2020, and April 22, 2022, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 27,532 reports of deaths — an increase of 183 over the previous week — and 224,766 serious injuries, including deaths, during the same time period — up 1,930 compared with the previous week.
Excluding “foreign reports” to VAERS, 810,171 adverse events, including 12,672 deaths and 80,743 serious injuries, were reported in the U.S. between Dec. 14, 2020, and April 22, 2022.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 12,672 U.S. deaths reported as of April 22, 16% occurred within 24 hours of vaccination, 20% occurred within 48 hours of vaccination and 59% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 572 million COVID-19 vaccine doses had been administered as of April 23, including 338 million doses of Pfizer, 215 million doses of Moderna and 19 million doses of Johnson & Johnson (J&J).

Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to April 22, 2022, for 5- to 11-year-olds show:
- 10,348 adverse events, including 256 rated as serious and 5 reported deaths.
- 19 reports of myocarditis and pericarditis (heart inflammation).
The CDC uses a narrowed case definition of “myocarditis,” which excludes cases of cardiac arrest, ischemic strokes and deaths due to heart problems that occur before one has the chance to go to the emergency department.The Defender has noticed over previous weeks that several reports of myocarditis and pericarditis have been removed by the CDC from the VAERS system in this age group. No explanation was provided. - 42 reports of blood clotting disorders.
U.S. VAERS data from Dec. 14, 2020, to April 22, 2022, for 12- to 17-year-olds show:
- 31,455 adverse events, including 1,803 rated as serious and 44 reported deaths. The most recent reported death involves a 14-year-old girl from Tennessee (VAERS I.D. 2238618) who died after receiving her second dose of Pfizer’s COVID-19 vaccine. According to the VAERS report, the girl had a previous history of cancer but was hospitalized 29 days after receiving her second dose of Pfizer with severe COVID-19 and COVID pneumonia. She became “critically ill,” developed respiratory failure and bradycardia and later died.
- 65 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
- 649 reports of myocarditis and pericarditis — two fewer than last week — with 637 cases attributed to Pfizer’s vaccine.
- 165 reports of blood clotting disorders — 1 fewer than last week — with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to April 22, 2022, for all age groups combined, show:
- 20% of deaths were related to cardiac disorders.
- 54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
- The average age of death was 73.
- As of April 22, 5,460 pregnant women reported adverse events related to COVID-19 vaccines, including 1,709 reports of miscarriage or premature birth.
- Of the 3,630 cases of Bell’s Palsy reported — three fewer than last week — 51% were attributed to Pfizer vaccinations, 40% to Moderna and 8% to J&J.
- 870 reports of Guillain-Barré syndrome, with 42% of cases attributed to Pfizer, 30% to Moderna and 28% to J&J.
- 2,343 reports of anaphylaxis — 12 fewer reports than last week — where the reaction was life-threatening, required treatment or resulted in death.
- 1,678 reports of myocardial infarction.
- 13,826 reports of blood-clotting disorders in the U.S. Of those, 6,199 reports were attributed to Pfizer, 4,925 reports to Moderna and 2,661 reports to J&J.
- 4,152 cases of myocarditis and pericarditis with 2,544 cases attributed to Pfizer’s, 1,415 cases to Moderna’s and 181 cases to J&J’s COVID-19 vaccine.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
D.C. Schools Can’t Vaccinate Kids 11 and Up Without Parents’ Consent Until Lawsuits Settled
The Defender | April 28, 2022
A preliminary injunction prohibiting the mayor of the District of Columbia, the D.C. Department of Health and D.C. public schools from enforcing the D.C. Minor Consent for Vaccination Amendment Act of 2020 (D.C. Minor Consent Act) will remain in place after the defendants declined to file an appeal within the required 30-day period.
The preliminary injunction reverts D.C. to the standard age of consent of 18, at least until the conclusion of the case.
The injunction stemmed from two lawsuits filed against the D.C. Minor Consent Act, which allows children 11 and older to consent to vaccinations without their parents’ knowledge or consent.
The law, passed on Dec. 17, 2020, specifically targets children whose parents filed religious exemptions for their children.
“This is a significant legal victory,” said Rolf Hazlehurst, senior staff attorney for Children’s Health Defense (CHD). “But the legal battle is by no means over.”
D.C. is the legal testing ground for mandatory vaccinations, according to Hazlehurst, which makes this a “high-stakes” battle.
“The defendants and other states are twisting and distorting the ‘mature minor’ doctrine to push the limits of government overreach at the expense of parental rights,” Hazlehurst said. “They will not abandon this tactic or their assault upon our children or parental rights.”
The two lawsuits challenging the D.C. Minor Consent Act include one filed by CHD and the Parental Rights Foundation and a second brought by Informed Consent Action Network.
Both lawsuits sought a preliminary injunction to immediately prohibit D.C. schools and public health officials from enforcing the law until the lawsuits are concluded.
During oral arguments on March 3, Hazlehurst argued the D.C. Minor Consent Act violates the Supremacy Clause of the U.S. Constitution because it contains multiple provisions that strip away the meager protections guaranteed to parents under the National Childhood Vaccine Injury Act of 1986.
Hazlehurst also argued the law violates the right to freedom of religion guaranteed by the First Amendment to the U.S. Constitution.
Hazlehurst told the court the mayor of D.C. created a “pressure-cooker environment,” enticing and psychologically manipulating minor children to defy their parents and take vaccinations against their parents’ will.
To make his point, Hazlehurst relied on a drawing, “Peer Pressure,” by a child of one of the plaintiffs. The drawing depicts the dilemma children face at school when they don’t want to get the COVID-19 vaccine.
On March 18, the U.S. District Court for the District of Columbia ordered the preliminary injunction.
In obtaining the preliminary injunction, the plaintiffs overcame a high legal hurdle that the “threatened injury must be certainly impending” as established by the U.S. Supreme Court precedent Clapper v. Amnesty Int’l, Hazlehurst said.
The court also ruled the plaintiffs in both lawsuits have legal standing based on preemption because the D.C. Minor Consent Act conflicts with the National Childhood Vaccine Injury Act.
In CHD’s case, U.S. District Judge Trevor N. McFadden made the additional finding that the plaintiffs have standing based upon the fact that they are likely to succeed on the merits that the law violates the free exercise of religion clause in the First Amendment.
“This preliminary injunction is part of ongoing litigation in an extremely important national precedent-setting case,” said Hazlehurst. “The rights of parents to decide what is best for their children’s health is at stake. Government can’t be allowed to make such decisions for minor children.”
The D.C. Minor Consent Act contains several provisions designed to deceive parents by hiding the fact that their children have been vaccinated against their parental judgment, authority or religious convictions.
The law requires healthcare providers to falsify records by leaving the child’s school vaccination records blank.
It also allows doctors to bill parents’ insurance companies for vaccines administered to children against their parents’ written directive. However, insurance companies may not send parents of those children an explanation of benefits.
Doctors Could Be Struck Off For Questioning Government Line on Lockdowns and Vaccines Under New Guidance
By Will Jones | The Daily Sceptic | April 27, 2022
Doctors who criticise vaccines or lockdown policies on social media could face being struck off if regulators rule they are guilty of spreading ‘fake news’, according to new guidance from the GMC. The Telegraph has the story.
The core guidance for medics has been updated for the first time in almost a decade to cover media such as Twitter, Facebook and Instagram. The rules on use of social media include a duty to be “honest” and “not to mislead”, as well as to avoid abuse or bullying.
The draft regulations from the General Medical Council (GMC) – which the watchdog describes as a 21st-century version of the Hippocratic Oath – also say doctors must speak out if they encounter “toxic” workplace cultures that threaten patient safety. And they say medics must take action if they encounter workplace bullying, harassment or discrimination.
The watchdog regulates doctors, who can face a range of sanctions – including being struck off the medical register – if they are found to have failed in their duties.
Charlie Massey, the Chief Executive of the GMC, said… the fundamental principles of the guidance remained the same, but had been updated to reflect the modern world.
“We’ve had feedback that doctors want more clarity on using social media. We are already clear that doctors must be honest and trustworthy in their communications, and are now emphasising that this applies to all forms of communication. The principles remain the same whether the communication is written, spoken or via social media,” he said.
The use of social media by medics has become an increasingly vexed issue during the pandemic, the report adds.
In December a judge ruled that the GMC’s interim orders tribunal had made an “error of law” when it ordered a GP accused of spreading misinformation to stop discussing Covid on social media.
Dr. Samuel White, who was a partner at a practice in Hampshire, raised concerns about vaccines and claimed “masks do nothing” in a video posted last June.
The GMC’s Interim Orders Tribunal imposed restrictions on Dr. White’s registration as a result. But the High Court said this decision was “wrong” under human rights law.
He had claimed “lies” around the NHS and Government approach to the pandemic were “so vast” that he could no longer “stomach or tolerate” them.
In August, the tribunal concluded Dr. White’s way of sharing his views “may have a real impact on patient safety”. It found Dr. White allegedly shared information to a “wide and possibly uninformed audience” and did not give an opportunity for “a holistic consideration of COVID-19, its implications and possible treatments”.
But the GP’s barrister, Francis Hoar, argued the restrictions imposed on his client’s registration were a “severe imposition” on his freedom of expression.
The draft guidance says doctors can be held accountable for promoting misleading information or stepping outside areas of their expertise. They are told to “be honest and trustworthy … make clear the limits of your knowledge… [and to] make reasonable checks to make sure any information you give is not misleading.
“This applies to all forms of written, spoken and digital communication,” the draft guidance states. And doctors are warned that online rows and trolling could jeopardise their professional futures.
It is of course outrageous that medics should be at risk of losing their career for questioning on Twitter the Government line on its draconian public health interventions. If there’s one thing we were lacking during the pandemic it was not an excess of conformity amongst doctors. The right of medics to ‘informed dissent’ should be strengthened, as per the High Court ruling in favour of Dr. White, not weakened.
On the other hand, there are plenty of Government advisers I can think of who could do with being penalised for “stepping outside areas of their expertise”. Somehow I doubt anything similar will ever be applied to them, however.
Worth reading in full.
Stop Press: The GMC guidance is still the subject of a public consultation – and anyone can contribute. Click here to begin the process.
Denmark Suspends COVID Vaccine Campaign, EU Set to End Mass Testing
By Michael Nevradakis, Ph.D. | The Defender | April 27, 2022
Denmark on Tuesday became the first country to suspend its national COVID-19 vaccine campaign after health officials said the pandemic is under control there.
Bolette Soborg, director of the Danish Health Authority’s department of infectious diseases, on Tuesday said Denmark is “winding down” the mass vaccination program, and that invitations for vaccinations would no longer be issued after May 15.
“We plan to reopen the vaccination programme in the autumn,” Soborg said, adding: “This will be preceded by a thorough professional assessment of who and when to vaccinate and with which vaccines.”
Public health authorities cited several factors contributing to the decision to end the national vaccination campaign. These include a decline in the number of new reported infections, stabilized hospitalization rates and an overall high level of vaccination.
This decision comes just a few months after Denmark eliminated all COVID-19-related restrictions, becoming the first European Union (EU) member state to do so.
On February 1, the country dropped restrictions ranging from vaccine passports to mask mandates. Public health authorities at the time said COVID-19 was no longer considered a critical threat to public health.
Despite a “surge” in reported infections in Denmark, attributed to the Omicron variant, health authorities said these cases are not placing a heavy burden on the country’s health system.
Denmark’s health authorities are the first to explicitly state that future COVID-19 vaccination drives will be targeted, rather than universal.
EU set to announce ‘post-emergency’ phase of pandemic, Fauci says U.S. out of ‘pandemic phase’
Denmark’s decision comes as several other countries appear to be walking back mass-scale COVID-19 vaccination and related public health initiatives.
In an interview Tuesday on PBS NewsHour, Dr. Anthony Fauci said, “We [the United States] are certainly right now in this country out of the pandemic phase.”
However, when asked whether there will be an end to the COVID-19 pandemic, he said that’s “an unanswerable question.”
In the U.K., the country’s Health Security agency this week announced it is slashing its staff by almost half, and reducing its COVID-19 budget by nearly 90% compared to 2021 levels.
And the European Commission — the executive branch of the EU — is reportedly preparing to announce the EU has entered a new “post-emergency phase” of the COVID-19 pandemic, Reuters reported today, citing a draft document the news agency said it reviewed.
Despite there being no official statements yet from EU officials, according to Reuters, the draft document, prepared by EU Health Commissioner Stella Kyriakides, states:
“This Communication puts forward an approach for the management of the pandemic in the coming months, moving from emergency to a more sustainable model.”
In practical terms, this would mean an end to mass COVID-19 testing, already shut down in several EU countries.
This approach contrasts with China’s “zero-COVID” policies — which have resulted in mass testing and a renewed wave of mass lockdowns.
In a possible reflection of the EU’s new policy direction — and its stark differentiation from China’s COVID policies — Greek health minister Thanos Plevris said recently “we are entering the phase of co-existing with COVID … we don’t believe in the zero-COVID policy, like in China.”
According to Reuters, the EU’s draft document is non-binding on member-states and states that “COVID-19 is here to stay,” with a likely emergence of new variants and “surges,” necessitating that “vigilance and preparedness remain essential.”
The document asks EU governments to be ready to re-enact emergency measures if deemed necessary, though the nature of these “emergency measures” does not appear to be specified.
However, the draft document does address the introduction of more sophisticated means of detecting outbreaks of — and the spread of — COVID-19, highlighting that “[t]argeted diagnostic testing should be put into place.”
Such “targeted” testing would focus on “priority groups,” such as people close to outbreaks, those at risk of developing severe COVID-19 symptoms and medical staff who are in regular contact with vulnerable populations.
The draft document also suggests surveillance and tracking of COVID-19 infections should be adapted and targeted, focusing more on genomic sequencing and less on the mass reporting of “cases.”
This new surveillance system would amount to one that, according to Reuters, is “similar to that used to monitor seasonal flu, in which a limited number of selected healthcare providers collect and share relevant data.”
As reportedly stated by the document, “[t]he objective of surveillance should no longer be based on the identification and reporting of all cases, but rather on obtaining reliable estimates of the intensity of community transmission, of the impact of severe disease and on vaccine effectiveness.”
However, unlike Denmark’s approach, the document states that vaccines remain essential, with a recommendation that EU member states consider enacting strategies to bolster vaccination levels among children age 5 and up prior to the start of the new school year.
Some EU member states, such as Greece, have strongly hinted wide-scale COVID-19 vaccinations and restrictions may resume in September.
Michael Nevradakis, Ph.D., is an independent journalist and researcher based in Athens, Greece.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
New Zealand Used Selective Science and Force to Drive High Vaccination Rates
By J.R. Bruning | Brownstone Institute | April 26, 2022
We expect that knowledge produced and applied in a health emergency will produce information that is protective of health. But it is increasingly apparent that over the last two years New Zealand’s Ardern government has designed policy, regulation, and information to coercively steward citizens to accept a drug under provisional consent.
Strict lockdowns were promised to end when 90% of the population was vaccinated. This was unprecedented: policy endpoints required population-level uptake of novel technology, no matter whether the individual was at risk or not.
In addition, data production was contracted by the department intent on a 90% vaccination rate. For decades governments have promoted ‘evidence-based science’ as the gold standard for public reasoning and risk deliberation. What we saw was internally produced and contracted science that focused on case rates, while (inconvenient) information in the published scientific literature on vaccine risk, waning and breakthrough was ignored.
This produced a tightly controlled scope of knowledge production that then failed to adhere to long-established democratic and public health principles. Responsible risk governance requires that governments must be responsive to data that indicates a technology is not as effective or is possibly more harmful than estimated, – for a democratic government’s primary role is the protection and safety of all citizens. Technology must not be valorized, and uncertainty set aside, in order to achieve policy ends.
Universal Vaccination Assumed from April 2021
New Zealand’s Unite Against Covid-19 ‘elimination’ strategy was confirmed in the first quarter of 2020. Policy, propaganda and legislation predominantly centred around the case, or infection rate, rather than the fatality rate as the measure of risk.
Even though the clinical trials did not demonstrate that the vaccine prevented transmission and infection, the Government promoted ‘the jab’ as a way to protect families in the Unite Against Covid-19 campaign. Persistent reporting of case rates fostered a perpetual state of fear and uncertainty among the population, who perceived infection from the SARS-CoV-2 virus to be something more like Ebola.
The Ardern government’s intention for the entire population to get the mRNA vaccine was declared through the signing of a supply agreement. This intention was then embedded in policy and regulation via the Traffic Light system, designed to nudge the population over 12 into compliance.
It was known by July 2021 that the vaccine waned and was leaky. Breakthrough infections were relatively common and for many. The clinical trials remain incomplete, lacking long-term safety data. The trials did not demonstrate that the vaccine prevented hospitalization and death.
However, in April 2022 in New Zealand, mandatory vaccinations remain compulsory for border workers, and workers in health and disability; corrections; defence; Fire and Emergency New Zealand (FENZ) and Police. These professions must be vaccinated and have received a booster vaccination against COVID-19.
At ‘Traffic Light Orange’ Kiwis ‘must wear a face mask’ in retail businesses, on shared and public transport, in government facilities and when visiting a healthcare service. This is despite the fact that Omicron ripped through New Zealand in February.
In the first week back at school and university after the summer holidays –the obedient mask-wearing young friends of my kids, including my son, from Otago and Canterbury down on the South Island up to the capital Wellington and Auckland – were locked down with Omicron in their first weeks back at university. No evaluation of Omicron and mask efficacy has been provided by the state.
The Risk Modellers
Government policy processes have persistently excluded uncomfortable knowledge that suggested uncertainty or risk. First, the policy accompanying and justifying Covid-19 legislation and Orders, and modelling by the contracted institution Te Pūnaha Matatini (TPM) contained narrow reasoning central to the state’s claims, locking in the narrative that infection was the predicator of risk, modelling wave after wave of infection.
Second, policy supporting the legislation excluded consideration of age-stratified risk and failed to address common principles of infectious disease management embedded in the New Zealand Health Act. Third, reviews of the scientific literature that could publicly identify and communicate risk relating to vaccine-related harm and issues relating to efficacy simply never occurred.
The gaps are considerable. The Government’s Covid-19 Unite campaign failed to communicate age-stratified risk of hospitalization and death as the pandemic evolved. New evidence on infection fatality rates were not reported to the public. In modelling papers, TPM used old infection fatality rate statistics that overestimated death rates.
The potential for the vaccine to wane or for breakthrough infection to occur was ignored in a major policy paper focussed on elimination and by the modellers at TPM. The role of natural infection in producing a broader, and protective structural response, assisting populations to shift to herd immunity status was downplayed. While herd immunity was recognized, testing and data modelling was undertaken to identify naturally derived herd immunity in the population. Later modelling exclusively associated herd immunity with vaccination.
Perhaps the problems addressed here are not surprising, when most modelling was undertaken outside of New Zealand’s public health institutions. Instead, number-crunching was carried out by data analysts, mathematicians affiliated with TPM, with scarce few infectious disease epidemiologists trained in public health ethics participating. And of course, the science and data modelling were directly funded by the government departments and Ministries dedicated to over 90% vaccine compliance.
Global vaccination policies ignored the fact that infection-related risk always centered on the aged and infirm and those with complex multimorbid conditions. Disconcertingly, the clinical trial data had conceded that vaccine efficacy remained uncertain for the most at-risk of harm from Covid-19 – the immunocompromised, autoimmune and people who were frail, and those with inflammatory conditions (see p.115). In addition, as coronaviruses readily mutate, it was highly probable the vaccine would have a short shelf life.
Early Treatments Sidelined
Governments are entrusted with an overarching obligation to protect health – this includes putting populations directly at risk through bad policy. There was always a role for safe, established drugs with a long history of safe use that had undergone complete testing before launching onto the market.
Early treatments could have been integrated as a major tool to prevent hospitalisation and death. Early treatments avoid the dilemma of mutating variants while acting to protect at-risk groups whose immune systems might not be as responsive to a vaccine.
Conventionally doctors are at liberty to repurpose drugs for their patients, such as antivirals with a long history of safe use. However, in July 2021, the government locked in approved drugs for treatment.
From at least October, New Zealand doctors were instructed to ‘not use any other antiviral outside of a clinical trial’ while Medsafe warned against use of the safe antiviral Ivermectin for a respiratory virus. Yet the clinical guidelines were intended as last resort medicine for the hospitalized, rather than designed as protective nor preventative at home therapies.
These directives have fractured the practice of informed consent, which forms the basis of trust in the doctor-patient relationships. Even the New Zealand Medical Council, the organisation that grants licences to practice medicine, declared that there was ‘no place for anti-vaccination messages in professional practice.’ These actions may unwittingly undermine trust in vaccines and the doctor-patient relationship for years to come.
The implications of silencing doctors, some who have had their medical licenses suspended, when observed alongside the above-mentioned data gaps, are extraordinary.
Ethical questions continue to be sidelined. The principle of proportionality, embedded in the 1956 Health Act, has been effectively dropped. Proportionality, which allows for individual risk, is a core consideration in public health. Medicine is a technology, and the space where biology meets technology – including medicine – is never constant, and requires value-based judgement. Risk management of a medical intervention for a pregnant woman, young person or child requires significantly different deliberation to a 75-year-old.
Democratically Unaccountable Legislation
Since January 2020, a tsunami of rights-limiting has been rolled out purposefully and consistently. There was scant citizen consultation with public input limited to a few short days in most cases. The unprecedented barrage of rules and orders released by the Ardern government entrenched requirements for almost everybody to get the mRNA vaccine.
By mid-2021 – before most mandates – the scientific literature was revealing that the vaccine waned; that breakthrough infection occurred and that there was extensive evidence that it produced a wide range of side effects, and even death. This knowledge should have invalidated any workforce vaccine mandate, but instead by October, the state doubled down and locked in mandates and regulations that would legally and socially coerce most of the population over 12 into accepting the shot.
It’s probable that the mountain of legislation produced over the last two years never fulfilled democratic norms of accountability and transparency. For science in a pandemic to be harnessed to serve the public interest, the institutions that set those terms of reference must be guided by principles that protect health.
The failure of government agencies to draw on peer-reviewed scientific literature while prioritizing internal modelling is clear from tracking the literature stored online with the relevant agencies. Most compellingly, it is documented in the policy supplied in support of the unprecedented quantity of law-making.
It appears that from late 2019, institutional interests anticipated that there would be hesitancy around vaccine safety. Yet there was no public forum. Instead, groups who sought to question the safety of the novel mRNA vaccine remained outside ‘accredited’ media, possibly due to the chilling effect of unprecedented Covid-19 funding and advertising boosts which effectively captured mainstream media.
That the New Zealand state mandated not-at-risk people accept a novel technology, creating rules (as nudge policies) that limited economic and social life for the non-vaccinated when there was early evidence the vaccine was leaky and potentially harmful, will take years to unpick. As mandates continue, injured groups continue to face barriers to justice following vaccine injury and death.
Ultimately, practices such as this raise nagging doubts concerning the state’s capacity to honor broader obligations to protect health and the public interest in future emergency situations. New Zealand’s response to the Covid-19 pandemic serves as a case study – a precedent, for future health emergencies.
A deeper dive on this discussion can be found in the paper, Covid-19 Emergency Powers and on Rumble. The paper is offered to assist academic and legal experts, citizens and communities to consider use of policy and science by the Ardern Government from 2020-2022. I question the potential for the New Zealand state to navigate future pandemics, and future techno-controversies, in the public interest.
J.R. Bruning is a consultant sociologist (B.Bus.Agribusiness; MA Sociology) based in New Zealand. Her work explores governance cultures, policy and the production of scientific and technical knowledge. Her Master’s thesis explored the ways science policy creates barriers to funding, stymying scientists’ efforts to explore upstream drivers of harm. Bruning is a trustee of Physicians & Scientists for Global Responsibility (PSGR.org.nz). Papers and writing can be found at TalkingRisk.NZ and at JRBruning.Substack.com and at Talking Risk on Rumble.
They just won’t let go of masks
By Guy Hatchard | TCW Defending Freedom | April 26, 2022
The writer is in New Zealand
AS the pandemic fades, should we meekly accept new restrictions or seek new freedoms?
An article in the New Zealand autumn 2022 AA Directions magazine advises that ‘masks are going to be part of our day-to-day lives for the foreseeable future’, and teaches us how to recognise whether someone is smiling behind their mask.
Yesterday in Stuff, science columnist Dr Siouxsie Wiles finally gets around to admitting that ‘you can’t rely on mRNA vaccines’. Her answer? Be stricter about mask wearing.
Dr Wiles, a British microbiologist who received the 2021 New Zealander of the Year Award for pandemic science communication, cites a new study which she says supports continuing use of masks at gatherings. Click on the link (most people don’t) and you arrive at a study that involves theoretical modelling rather than verified effects.
Mask studies (of which there are many) have not demonstrated large reductions in Covid transmission. They tend to be very technical in nature and focus on the comparative viral loads found in nasal and mask swabs. These measurements can be connected to Covid transmission only via theoretical modelling.
Back in the real world, the near universal combination of vaccination and mask wearing to date in New Zealand has not stopped Omicron transmission.
A study published in ClinMed entitled ‘Adverse Effects of Prolonged Mask Use among Healthcare Professionals during Covid-19’surveyed 343 healthcare professionals in New York City hospitals obliged to wear masks throughout most of their working day. They reported: headaches (71 per cent), skin breakdown (50 per cent), and impaired cognition (24 per cent). Yes, you did read that right, one quarter of medical professionals wearing masks suffer decreased intellectual capacity.
Even costly N95 masks do not stop the passage of air around them essentially negating their purpose and prompting the observation that it is like trying to stop mosquitos with chicken wire. Surgical masks or their equivalent are mainly required in hospitals and dirty environments such as sawmills or building sites to protect the wearer from inhaling human tissue or large particulates.
So will Dr Wiles advise us next week to wear a full deep-sea diving suit? In the crazy world of the new subnormal apparently nothing absurd can be ruled out.
Hiding the truth from the public has become a medical imperative
There is a certain hysteria surrounding the realisation that mRNA vaccines don’t actually work and may be harmful. When my kids were growing up we used to read an amusing book to them, Lies My Mother Told Me. How many lies have we been told? Too many.
For example, the Pfizer mRNA vaccine is:
· 95 per cent effective
· Completely safe
· Mostly stays in the upper arm muscle, as most traditional vaccines do
This last is interesting because Pfizer knew before they released the mRNA vaccine that it didn’t stay in the upper arm. They had completed an animal study which suggested that most of the mRNA vaccine spread throughout the body instead of staying at the injection site. The lipid nanoparticles (LNP), which encase the mRNA and help to breach cell walls are highly mobile and ensure that the mRNA spreads rapidly to all the organ systems in the body. If you want the full story see this article by clinical immunologist Dr Byram Bridle.
If we had known this, we would have realised early on that adverse reactions such as liver and kidney damage, strokes, cardiac events, neurological conditions and sudden-onset cancers were not unrelated to vaccination, as many victims were assured at the time by the NZ Ministry of Health, GPs and hospital staff.
Medical professionals assessing the causal connections between mRNA vaccination and subsequent adverse events were relying upon their prior knowledge about traditional vaccines. They thought they knew that vaccine ingredients mostly stayed at the injection site and eventually appeared in lymph nodes as they were cleaned up by the immune system. Pfizer neglected to tell them this was not the case. In fact Pfizer didn’t seem to inform anybody: the damning data was hidden in an obscure study buried in the requirements of the various national regulatory processes supposedly scrutinising safety. Anyone sounding the alarm seemed to be cancelled by the media and relegated to the ranks of conspiracy theorists.
Now that we have some hard NZ data showing that the protective effect of mRNA vaccination is a myth, there appears to be a rush on the part of seasoned and highly decorated Covid science communicators like Dr Siouxsie Wiles, member of the NZ Order of Merit, to throw us a lifeline. We may not actually choose to be saved. We might instead get on with our own lives and make the best of what opportunities we can discover for ourselves. At least we will be rowing our own boat, not sinking in the good ship misinformation.
When will these vaccine zealots wake up to the truth?
By Guy Hatchard | TCW Defending Freedom | April 24, 2022
WE should not understate the naivety of the government, media and scientists during the pandemic. The tabloid-style stories of severe Covid outcomes, the authoritative voice of Dr Anthony Fauci (who has financial conflicts of interest), the allure of the word vaccine, and the exaggerated death toll in foreign lands all combined into a convincing call for immediate and coercive action. Yet behind the stories, the highly profitable pharmaceutical PR system was running at full steam playing on the fear factor. New Zealand fell head over heels in love. Love knows no reason and that was certainly the case here.
New Zealand is a long way from the rest of the world. We have a tradition of proud independence and self-sufficiency, but we rolled over and played Follow the Leader. No one in a position of influence struck a note of caution, especially not our Prime Minister. We instituted the largest public borrowing programme in our history and spent it on a US mega corporation with a poor safety record and a history of punitive malpractice judgments. The government instituted saturation advertising of vaccine safety and efficacy, and then followed up with mandates, sackings and social exclusion. Our media shouted down those few asking questions.
Times, however, have changed. The respected and conservative Wall Street Journal (WSJ) has aired concerns about poor regulatory decisions at the US Food and Drug Agency (FDA) over booster shots. It joins a growing international chorus of highly qualified and influential voices.
On April 3, in an opinion piece entitled ‘FDA Shuts Out Its Own Experts in Authorising Another Vaccine Booster’, Dr Marty Makary, a surgeon and public policy researcher at Johns Hopkins University School of Medicine, wrote: ‘The FDA last week authorised Americans over 50 to get a fourth Covid vaccine dose. Some of the FDA’s own experts disagreed, but the agency simply ignored them.’
Eric Rubin, editor-in-chief of the New England Journal of Medicine (arguably the world’s most influential medical journal) and a member of the FDA advisory committee on vaccines told CNN last month: ‘I haven’t seen enough data to determine whether anyone needs a fourth dose.’
Dr Cody Meissner, also a member of the FDA vaccine advisory committee and chief of paediatric infectious diseases at Tufts Children’s Hospital in Boston, agreed: ‘The fourth dose is an unanswered question for people with a normal immune system.’
A third member of the committee, Dr Paul Offit of the Children’s Hospital of Philadelphia, went further. He told the Atlantic magazine that he advised his 20-something son to forgo the first booster.
Two top FDA officials, Marion Gruber, Director of the FDA Office of Vaccine Research and Review and her deputy Paul Krause, quit the FDA in September last year complaining of undue pressure to authorise boosters and a lack of data to support their use.
Unbelievably, the US Centers for Disease Control (CDC) rubber-stamped the FDA decision to approve a second booster without even convening its panel of external independent vaccine experts.
The WSJ article described the effect of boosters as fleeting, mild and short-lived. It sounded a note of alarm saying that neither the CDC nor the US National Institutes of Health (NIH) had made a priority of studying vaccine complications. Moreover their VAERS data collection and analysis process is incomplete and inadequate. In other words, the safety investigation to date of adverse effects of mRNA vaccination is incomplete and potentially misleading.
The central question raised by the WSJ opinion piece is, why wouldn’t the US regulators wish to undertake accurate and complete investigation of adverse effects of mRNA vaccination? Have pharmaceutical interests been able to influence decision-making at the FDA to their own commercial advantage at the expense of safety considerations?
The British Medical Journal agrees. On March 16 it published an article which said: ‘Evidence-based medicine has been corrupted by corporate interests, failed regulation and commercialisation of academia.’
The lessons are obvious. We have stifled debate and slavishly followed FDA advice. Now there is a need for revaluation and debate. We have travelled a long way down a one-way street, but it appears to be a dead end. The triumphant articles published about a survey of vaccine-resistant people born in Dunedin was a low point in uncritical mainstream media publishing. We have to regain an objective voice.
A paper published on April 5 in the New England Journal of Medicine found that any measurable protective effect of the fourth inoculation (which in any case, it found, is very small in absolute terms) disappeared after just eight weeks. Moreover a paper in the Lancet on April 8 admitted that boosters carry a risk of additional side-effects. Both these papers, however, skirted the obvious safety questions in favour of weak praise for vaccine orthodoxy.
In contrast the WSJ article asked the important question: ‘Who is actually getting serious about measuring the extent of adverse events, rather than continuing to urge uncritical acceptance of a largely ineffective vaccine?’
So far New Zealand media have steered clear of such questions. Dr Ashley Bloomfield, chief executive of the country’s Health Ministry, has refused to institute mandatory reporting of adverse events following mRNA Covid vaccination and he has excelled at denying vaccine exemptions to those injured by the first shot. Silence is no longer tenable, although in actuality it never was. Questions have to be asked. No ifs or buts. Overseas media outlets of the thinking kind are waking up.
If we can’t face debating rationally with our critics, we are drifting on to the rocks of ignorance and prejudice.
Time for us to wake up.
NEW DATA SHOWS TROUBLING TREND IN VACCINATED
The Highwire with Del Bigtree | April 21, 2022
The Highwire with Del Bigtree | April 21, 2022
Elon Musk’s attempt to buy the social media giant Twitter has sent shockwaves through the mainstream media. Why are they so threatened by free speech?
ELON MUSK BUYING TWITTER
You’ve probably heard that billionaire Tesla-founder Elon Musk is putting together a financial package to become the sole proprietor of Twitter. Having already purchased 10% of the social media giant’s shares, Musk turned down a seat on the board of directors and decided to just buy the whole place.
To be clear, we don’t much like Musk and trust him less. The whole story is likely just another non-issue for people to squabble over.
… that said, you’d have to be made of stone not to take some bitter pleasure in watching the squirming of “liberal” pundits who are suddenly having their own sophistry turned against them.
Remember how those of us concerned about corporate censorship have always been told that “private companies can do what they want” and “if you don’t like, go make your own platform”? Well, apparently those arguments no longer apply.
In fact, according to Robert Reich in the Guardian, “going to another platform” is not an option. Funny that.
Mehdi Hasan rants about Musk’s “problematic free speech escapade” in his latest show, setting up a strawman so large he could burn it and guarantee a bountiful harvest.
The Conversation hosts an article that argues allowing everyone equal room to express themselves is actually bad for free speech because it doesn’t protect “the vulnerable” from harassment.
But the prize for the most-revealing reaction goes to Max Boot of the Washington Post, who said on twitter:
It’s delightful. From the refusal to acknowledge that the paper he works for was only just recently purchased by Jeff Bezos, the second richest man in the world, to the coy euphemism for censorship, all good stuff.
But why is all this happening? And where is it all going?
There are a few ways this could go. For one, the government might step in and stop Musk from buying the company. Protecting social media from becoming a “monopoly”, scoring some points with the “left” for “standing up to billionaires”, and setting a precedent for state interference in private business.
It could be that Musk does buy twitter, and scraps any limitations in line with his “free speech absolutist” claims… but then nation-states will be “forced” to make new rules limiting speech since “irresponsible tech companies refuse to act to stop hate speech” or something along those lines.
Whatever happens, its easy to see how this could further the war on free speech, one way or another. Or maybe nothing will happen at all, and it’s just fun and games.
How to lie with statistics – Vaccine efficacy edition
The Naked Emperor’s Newsletter | April 23, 2022
Just a quick post to show another method of how to increase vaccine efficacy. This time looking at data from Switzerland and Liechtenstein (S&L).
By mid December 2021, S&L were at the peak of their third wave. It was ok though because 67% of the country had been fully vaccinated, 17% with a booster. 32% of selfish people had still not been vaccinated however.
As the vaccines stop people from going to hospital this would show up in the stats.
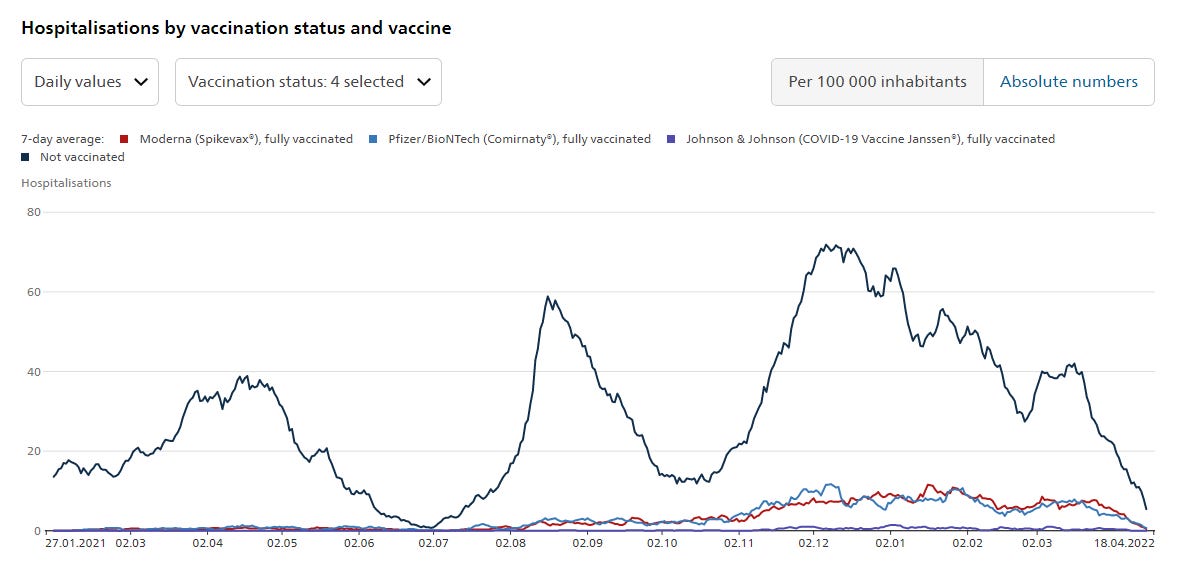
Yes, as predicted, there was a slight increase in hospitalisations for fully vaccinated citizens (Moderna – red line, Pfizer – light blue line) but a massive spike in hospitalisations for those pesky unvaccinated (dark blue line).
Job done, vaccine efficacy proven.
But hold on a second, there is another category. “Vaccine unknown, fully vaccinated”. Let’s add this to the graph.
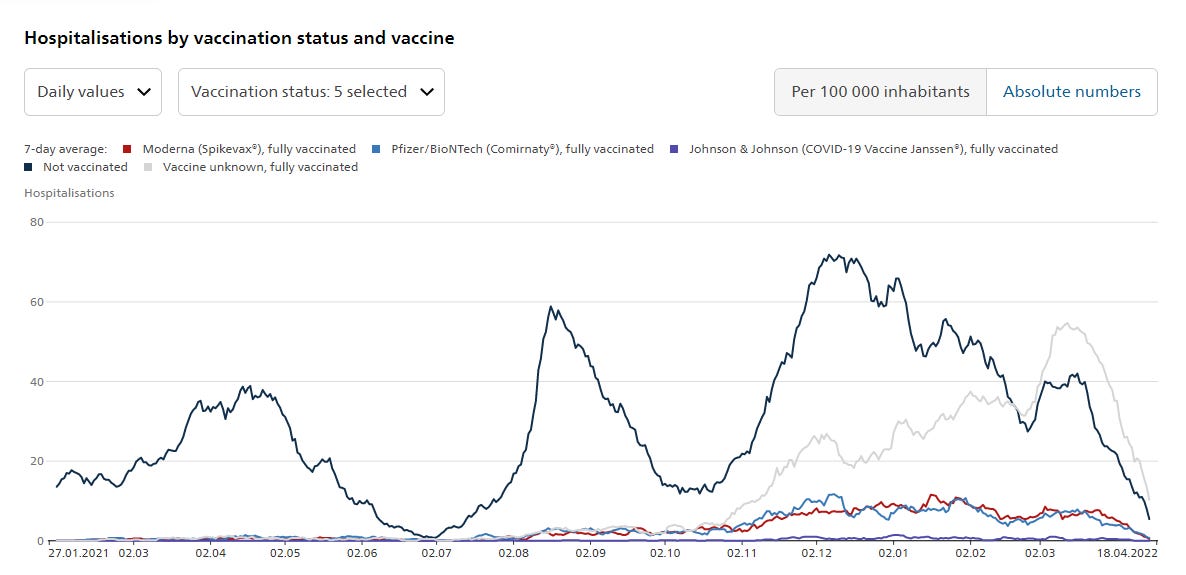
They don’t really want you to see this line so have made it a faint grey colour. However much they would like to pretend it wasn’t there, it is. And it shows a lot of fully vaccinated people going to hospital, and continuing to go to hospital, until March 2022, well after the peak for unvaccinated individuals.
Lot’s of fully vaccinated people going into hospital who have forgotten which vaccines they had. Did they forget or were they too ill? Is this an admin issue or are these people who had a combination of vaccines and so couldn’t be put in one category?
Either way, this grey lined category shifts a lot of people out of the Pfizer and Moderna vaccinated categories. It makes vaccine efficacy look much better than it actually is by saying only this many Pfizer or Moderna vaccinees were hospitalised.
Another great example of how to lie with statistics.
EU commission sued over Covid-19 vaccine secrecy
Samizdat | April 23, 2022
Five Green MEPs are suing the European Commission over its ultra-secretive vaccine contracts, arguing that the heavily redacted versions released by the EC “made it impossible to understand the content of the agreements,” in a statement published Friday.
“Secrecy is a breeding ground for distrust and skepticism, and it has no place in public agreements with pharmaceutical companies,” Margrete Auken, a Danish MEP involved in the suit, declared, adding that “the European Commission’s refusal to provide transparency on its vaccine contracts affects the public’s confidence in the EU’s ability to obtain the best possible outcome for its citizens.”
The MEPs are demanding the details of the contracts the EC signed with vaccine-makers BioNTech, Pfizer, Moderna, AstraZeneca, Johnson & Johnson, and Novavax, including price per dose, advance payments, conditions for vaccine donations, liability, and indemnification matters.
“Purchases made with public money should come with public information, definitely in matters of health,” Dutch MEP and party to the lawsuit Kim van Sparrentak said in the group’s statement, noting that “confidentiality under the guise of trade secrets only fuels uncertainty and fear.”
In addition to Auken and van Sparrentak, the MEPs signing on to the suit are Tilly Metz (Luxembourg), Jutta Paulus (Germany), and Michele Rivasi (France), the chair of the parliament’s committee on Covid-19.
The lawsuit, filed in the European Court of Justice in Luxembourg, comes as EC President Ursula von der Leyen revealed that every EU member state would be required to adopt EU Digital Covid Certificates, a digital health passport issued to those with proof of vaccination, a negative PCR test, or proof of recovery from Covid-19. While the validity period for such certificates was due to lapse at the end of June, the EC is not only renewing it another year, but making it mandatory for all 27 EU countries from July 1. Only 15 are currently using it, according to von der Leyen.
The move comes despite many EU states winding down their Covid-19 restrictions, moving away from some of the stricter measures imposed in the first 18 months of the pandemic. Germany, which had initially sought to require all citizens over the age of 60 to receive a Covid-19 vaccine, has been forced to axe those plans after they were voted down in the Bundestag, though the country’s health minister has warned that the government may reimpose mask mandates, as he expects infections to increase in the fall.
In response to the lawsuit, the EC has insisted it cannot reveal the contracts it signed with the vaccine-makers back in 2020, claiming “the commission is in the business of respecting contracts.” At the time, EU lawmakers who wanted to see the contracts were prohibited from taking notes and forced to sign non-disclosure agreements.
Much of the world seemed to be headed for mandatory Covid-19 vaccination six months ago. However, the realization that despite their manufacturers’ initial promises, the vaccines were no magic bullet – not only incapable of stopping the spread, but incapable of preventing further infection – has cooled public fervor for mandates. Health concerns and complaints of discrimination against the unvaccinated have also contributed to the backlash. However, the manufacturers, as well as most officials, continue to insist that the vaccines are “safe and effective.”
Featured Video

IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
or go to
Aletho News Archives – Video-Images
From the Archives
Because no animal reservoir has been found for SARS-CoV-2, it cannot properly be termed a zoonosis.* Should we call it a labnosis? And what does that mean?
By Meryl Nass, MD | July 12, 2021
After a year and a half of seeking but not finding SARS-2 in any wildlife anywhere (apart from domesticated or zoo animals that appear to have caught it from humans) is it time to say, yes, it didn’t just escape from a lab. It was created, built, assembled in a lab. Or many labs
Coronavirus scientists have been constructing new viruses out of bits and pieces of other viruses for a long time.
Why did they do it? … continue
Blog Roll
 Aletho News
Aletho News- The Targeted Assassination of Studies Showing Vaccines Cause Injury
- BMJ Probe Into Excess Mortality Study Drags On for Two Years With No Resolution
- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- Strait of Hormuz closed over Israeli aggression on Lebanon
- Keir Starmer arson mysteries multiply
- IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
- Zelensky threatens to attack Belarus
- UK to send Ukraine 150,000 drones
- ‘Biased censorship’: Iran deputy FM slams X for stripping him of blue tick
- If Americans Knew
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- Old Iraq war architects rise up against Trump’s Iran deal
- No Tricks Zone
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines

{kind=link}