V-Safe Part 1: After 464 Days, CDC Finally Coughed up Covid-19 Vaccine Safety Data Showing 7.7% of People Reported Needing Medical Care
First part of an incredible story that shows just how broken our public “health” apparatus is: very, very broken
By Aaron Siri | Injecting Freedom | November 23, 2022
Last year, I wrote to let you know that the CDC was refusing to release its post-marketing safety data for Covid-19 vaccines from its v-safe system to the public, despite our legal demands for this data on behalf of the Informed Consent Action Network (ICAN).
The CDC refused to release this data even though it had documented the data was in a form that could already be released to the public (meaning, it was “deidentified” or clear of any personally identifying information) because Oracle, a private company, already had access to this deidentified data.
Well, after multiple legal demands, appeals, and two federal lawsuits, the CDC finally capitulated and agreed to a court ordered schedule compelling it to produce the data. Now that ICAN, and therefore the public, have received the check-the-box portions (as opposed to the free-text field portions) of this data, the data itself may explain why the CDC refused to release it without a fight.
V-safe’s data shows that 7.7% of its approximate 10 million users reported having to receive medical care after receipt of a Covid-19 vaccine, and over 70% of those users sought outpatient/urgent clinical care, emergency room care, and/or were hospitalized.
I can already hear the retort: surely these were anti-vaxxers reporting the need for medical care! Far from. All v-safe users received the Covid-19 vaccine. Anti-vaxxers don’t get the shot. Not only were these folks not against the shot – again, because every one of them got the shot – they are likely mostly vaccine enthusiasts. This is evidenced by the fact that most of the individuals who registered for v-safe did so between December 2020 and April 2021; in fact, around 9 million of the approximate 10 million users registered during this period. This was the time, you may recall, when many people were clamoring over each other to get the shot. When they were spending hours online searching for vaccine availability and making appointments. When love songs were literally being sung about the vaccine.

This was also early in the rollout when CDC recommended, and many states followed, a phased rollout, offering the first vaccines to healthcare workers and to long-term care facility residents. It was during this period that people signed up for v-safe to participate in its rollout, excited to be part of the vaccine program. (One can assume that more healthcare workers than elderly long-term care residents signed up for a smartphone-based program). This also pre-dates most vaccine mandates in the country.
The data submitted by the 10 million v-safe users therefore may be a good reflection of the experience of the larger population of 265 million Americans who received at least one dose of a Covid-19 vaccine. To the extent it is not, if anything, these people (as enthusiasts and/or healthcare workers) were arguably more prone to underreport symptoms than to overreport.
The data itself is disconcerting but even more incredible is the CDC’s stonewalling the release of the data, the process needed to obtain the data, and how the CDC used, or dare I say misused, the data over the last year and a half. This story, in many ways, reflects all that is wrong with so-called public “health” authorities. It shows the serious danger resulting when the CDC’s policies, public claims, and reputation become indistinguishable from its need to defend a product at almost all costs.
To make it manageable to tell and digestible to folks with busy schedules, I will tell the story in several parts released over the coming days and weeks.
The v-safe story continues in Part 2, which will explain what is in v-safe and why you should care. And trust me, you should care, as v-safe is likely the best evidence that exists regarding the safety profile of this product. As I tell the story, I will endeavor through these posts to respond to the torrent of inquiries regarding v-safe, the fight to get the data, and the data itself, which I have already received.
I will leave you with a short appearance I had on Fox News discussing the v-safe data.
As an Oncologist I Am Seeing People With Stable Cancer Rapidly Progress After Being Forced to Have a Booster
BY DR ANGUS DALGLEISH | THE DAILY SCEPTIC | NOVEMBER 26, 2022
There follows a letter from Dr. Angus Dalgleish, Professor of Oncology at St George’s University of London, to Dr. Kamran Abbasi, the Editor in Chief of the BMJ. It was written in support of a colleague’s plea to Dr. Abbasi that the BMJ make valid informed consent for Covid vaccination a priority topic.
Dear Kamran Abbasi,
Covid no longer needs a vaccine programme given the average age of death of Covid in the U.K. is 82 and from all other causes is 81 and falling.
The link with clots, myocarditis, heart attacks and strokes is now well accepted, as is the link with myelitis and neuropathy. (We predicted these side effects in our June 2020 QRBD article Sorensen et al. 2020, as the blast analysis revealed 79% homologies to human epitopes, especially PF4 and myelin.)
However, there is now another reason to halt all vaccine programmes. As a practising oncologist I am seeing people with stable disease rapidly progress after being forced to have a booster, usually so they can travel.
Even within my own personal contacts I am seeing B cell-based disease after the boosters. They describe being distinctly unwell a few days to weeks after the booster – one developing leukaemia, two work colleagues Non-Hodgkin’s lymphoma, and an old friend who has felt like he has had Long Covid since receiving his booster and who, after getting severe bone pain, has been diagnosed as having multiple metastases from a rare B cell disorder.
I am experienced enough to know that these are not the coincidental anecdotes that many suggest, especially as the same pattern is being seen in Germany, Australia and the USA.
The reports of innate immune suppression after mRNA for several weeks would fit, as all these patients to date have melanoma or B cell based cancers, which are very susceptible to immune control – and that is before the reports of suppressor gene suppression by mRNA in laboratory experiments.
This must be aired and debated immediately.
Angus Dalgleish MD FRACP FRCP FRCPath FMedSci
Angus Dalgleish is a Professor of Oncology at St George’s, University of London.
The Doctor Who Can Rebuild Trust: Joseph Ladapo
By Jeffrey A. Tucker | Brownstone Institute | November 22, 2022
If you are like me, you are exhausted of the lies. Every day seems to bring new revelations about how our lives came to be upended. The connections are becoming clearer between the pandemic response and the growing economic crisis, the ballooning debt, the growth of the surveillance state, the corruption and scams, chilling absence of integrity in public life, and, with the failure of FTX, the way in which an outright financial scam was integral to the calamity.
While we await new revelations, depositions, coverups, pleas for amnesty, and bad economic news, whom can we trust? Is anyone telling the truth?
Today was Anthony Fauci’s last White House press conference, and he spoke as if life is all normal and everything is fine. It’s as if the whole disaster never happened. He never locked anyone down, he says. He is happy for any investigations, he says, because he has nothing to hide. And then he ended with a final push for everyone to get booster #5 or whatever number we are on.
It’s like we live in two universes: our own lives in which we read true things in some places, and official life, in which shills and publicists keep repeating the same nonsense over and over without flinching or providing anything like an honest account of these last three years.
Perhaps for this reason – and also because by any historical standard this is a tremendous autobiography – reading Dr. Joseph Ladapo’s Transcend Fear is a welcome relief from the nonsense of our times. It is brutally honest. It is emotionally affecting. It is careful and precise but also deeply radical in its observations. If what’s called the “public health world” has lost touch with both the public and health, this book provides a path to restoring it. In short, it is a beautiful and inspiring experience.
Dr. Ladapo is the Surgeon General of the State of Florida, picked by Governor Ron DeSantis to forge and explain the state’s health decisions and priorities to the public in the midst of a grave crisis. He has faced down the national press time and time again with Zen-like wisdom. He seems emotionally unflappable while also sticking to the science as he understands it. He is the only public health official in the country who has been upfront about the limits of the vaccines and warned healthy young people that they don’t need them.
What we learn from this book is that he has been a warrior against pseudoscience from the very beginning of this pandemic and the government response. After the lockdowns, most scientists and health professionals fell silent, fearing reputational and financial loss. Dr. Ladapo was different, On March 24, 2020, still within the window of “15 Days to Flatten the Curve,” he wrote in USA Today:
We are fretting and we are fuming. As a country, we have been caught miserably flat-footed after receiving warnings about what lay ahead when cases of Covid-19 began exploding in Wuhan, China. Messages from local and state leaders about how to respond to the pandemic change almost daily—a sure sign they have no idea what they are doing. Shutdowns are happening here in California and in New York, and will probably spread to the rest of the nation….
Here’s the problem: Because of the (understandable) fear and hysteria of the moment, few US leaders are seriously talking about the endgame. The epidemiologic models I’ve seen indicate that the shutdowns and school closures will temporarily slow the virus’ spread, but when they’re lifted, we will essentially emerge right back where we started. And, by the way, no matter what, our hospitals will still be overwhelmed. There has already been too much community spread to prevent this inevitability.
We don’t have a totalitarian government like China, and we value our civil liberties too much to take the measures (i.e., total lockdown) that would be needed to rapidly decrease the infection rate to zero. This means that, even with shutdowns, the virus will still spread. Unfortunately, this also means that rates of “community immunity,” often referred to as “herd immunity,” will slow. As a result, we will always be vulnerable to the virus spreading rapidly again as soon as shutdown measures are lifted, unless they are immediately reimplemented—over and over and over again.
Was he the first post-lockdown voice from public health profoundly to object in a public forum of this magnitude? Perhaps so. Consider the bravery and presence of mind it required to write those sentences. The entire country was on a wartime footing with unprecedented horribles taking place. The media was screaming “Run for your lives” but most of us weren’t even allowed out of our homes to do that.
These were utterly crazy times. The whole world was going bonkers. And yet this man kept his cool.
This book explains where his cool comes from. You see, he is the son of an immigrant from Nigeria, born 1979. A math and science whiz, he attended Wake Forest and then entered Harvard Medical School. While he was involved in his studies, he noted the existence of the Kennedy School of Government and enrolled there too. On graduation day, he was granted a MD plus a PhD in public policy. So essentially: the highest credentials in two fields that this country offers. He became professor of medicine at New York University and then the University of California, Los Angeles.
The trouble was that none of his training had prepared him to deal with medical issues closer to home, namely his wife’s unrelenting migraines that often landed her in the hospital and his own underlying psychological fears of social interaction. The details are very painful and told in this book with disarming detail. Long story short: his search for answers led him toward alternative medical paths that eventually fixed both issues, and burned a lesson in his mind. Health is individual, and the right path is not the same for everyone and not always found in expertise as codified in the textbooks and institutions.
It was soon after these difficult times that the pandemic broke and, along with it, the claims that the experts had all the answers in lockdowns and eventual universal mandates for vaccination.
Dr. Ladapo had meanwhile developed the self-confidence to speak about such matters truthfully and fearlessly. And he never stopped. He wrote for every venue he could, month after month, urging an end to the lockdowns, a focus on therapeutics, attention to the science we had, and genuine concern for the health of actual individuals, who are not lab rats but people with human rights and freedom.
Even though Dr. Joseph Ladapo is obviously a hero (and one for the ages, so far as I’m concerned), the prose here is remarkably lucid, humble, and precise. That’s why I say that the humane concern in this book is an inspiration. Moreover, reading it is a form of therapy because he connects with a common sense that we all had in 2019 before the world descended into utter madness.
What’s more, this book shows a path forward not only for public health but for all of us as individuals. He urges personal reflection as the first step in recovery, overcoming whatever hidden fears we had that caused too many among us to go along with the preposterous parade of dangerous nonsense that controlled our lives for so long.
In my own view, this book is a classic of our times. Its value added is not only the author’s credentials, though he has them galore, or even how it speaks so directly to issues that have profoundly affected all our lives. Its real value is as a model of autobiography that offers lessons for all of us without exception.
I write as Dr. Fauci just finished his last press conference without offering so much as a hint of apology for what has happened. Meanwhile, I’m sure Dr. Ladapo is tending to his work in Florida where he has been charged with dealing with public health policy with honesty, truth, and wisdom. I know who gets my vote for hero of the pandemic.
Jeffrey A. Tucker, Founder and President of the Brownstone Institute, is an economist and author. He has written 10 books, including Liberty or Lockdown, and thousands of articles in the scholarly and popular press.
Courage to Face COVID-19: Book Trailer
https://rumble.com/embed/v1uk8xs/?pub=4
Written by John Leake and produced by Daniel Hancock | November 25, 2022
At the beginning of 2020, Dr. Peter McCullough was a highly regarded practicing physician, program director, teacher, and clinical investigator at a major academic medical center in Dallas, TX. When COVID-19 arrived in March, he felt a duty to find a treatment for the disease. He wasn’t alone. Other doctors all over the world were also searching for a cure. They followed the longstanding principle that it’s best to tackle a sickness early, before it becomes life threatening. This is the story of how Dr. McCullough and his colleagues developed an early treatment protocol of generic, repurposed drugs and supplements that has saved millions of COVID-19 patients from hospitalization and death.
In spite of their success, their early treatment protocol was not welcomed by public health officials. On the contrary, the news of their promising results was dismissed as soon as it was reported. At first this seemed like conventional skepticism, but then fraudulent papers maligning the protocol’s repurposed drugs were published in academic medical journals. This and other acts of fraud revealed that a coordinated smear campaign against early treatment was being waged. Dr. McCullough and his colleagues soon found themselves censured, censored, vilified in the media, and fired from their jobs. The greatest victims of the smear campaign were COVID-19 patients who were consequently deprived of early treatment. Hundreds of thousands needlessly died of the disease.
At the same time early treatment was suppressed, the US government and mainstream media proclaimed that the cure to COVID-19 lay in a new generation of vaccines that were being developed at warp speed. These were heralded as a forthcoming panacea that would save mankind and restore normalcy. As soon as they were mass deployed, public health officials would lift the restrictions on social and economic life.
While many observers were thunderstruck by this turn of events, there were historical precedents. In his 1961 Farewell Address, President Eisenhower warned, “We must guard against the acquisition of unwarranted influence, whether sought or unsought, by the military-industrial complex. The potential for the disastrous rise of misplaced power exists and will persist. We must never let the weight of this combination endanger our liberties or democratic processes”. As Dr. McCullough and his colleagues learned, Eisenhower’s warning has become equally applicable to the Bio-Pharmaceutical Complex of multinational drug companies, the NIH and other federal agencies, research and virology labs, and the Gates Foundation. Since COVID-19 arrived, this Complex has obtained misplaced power over every aspect of our lives and taken our liberties. The Courage to Face Covid-19 recounts how Dr. McCullough and his colleagues began their work by fighting a novel infectious disease, and then became leaders in fighting the tyrannical regime that endangers our American way of life.
Who is Dr. Asish Jha (President Biden’s Covid Czar)?
Top public health empty suit is a pandemic planner and propagandist

Dr. Ashish Jha
By John Leake · Courageous Discourse · November 25, 2022
At at press briefing on November 22, White House COVID-19 Response Coordinator, Dr. Ashish Jha, reiterated that God gave us two arms in order to receive multiple vaccines and boosters. I write “reiterated” because he made the same stupid remark at a press briefing back in September.
I wasn’t surprised when the Biden Administration appointed Dr. Jha to serve as its Covid Czar. As we recount in our book, Dr. Jha was the minority witness at Senator Ron Johnson’s November 19, 2020 hearing on Early Outpatient Treatment. This hearing began with testimony from Drs. Peter McCullough, Harvey Risch, and George Fareed on the safety and efficacy of repurposed, FDA-approved drugs for treating COVID-19—especially in the disease’s early stage—to prevent hospitalization and death.
Following their testimony, Dr. Jha testified that their observations and findings were erroneous. In fact, he claimed, there were no effective early treatments for COVID-19, and that our best and only hope was the vaccine that was then in development.
An especially dramatic and somewhat comical moment in the hearing occurred when Dr. George Fareed said, “I wonder if Dr. Jha actually treats patients by the way he talks.” Senator Johnson took this remark as a cue for querying Dr. Jha.
“Have you treated any Covid patients,” Senator Johnson asked.
“I have not, sir,” Dr. Jha replied. We recount this scene in the following excerpt from The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex:
Dr. Jha had splendid academic credentials to match his splendid manners, but at this moment he lost a lot of credibility. It was perhaps the equivalent of an aeronautical engineer admitting that he’d never flown in a plane, or a marital counselor admitting he’d never been married.
He implied that Professor Risch—a distinguished epidemiologist twenty years his senior—was categorically wrong in his interpretation of the data. Then he implied that Dr. Fareed’s observations as a treating physician were an illusion—that the high-risk patients who received the Zelenko Protocol would have recovered in the same dramatic way without the intervention.
This was probably the most notable moment in the hearing. Since graduating from medical school in 1970, Dr. Fareed had logged fifty years as a medical researcher and treating physician. It would be hard to find a doctor in the entire country with more clinical experience. He testified to the U.S. Senate that he’d successfully treated 1,000 high-risk COVID-19 patients. A few minutes later, a doctor 25 years his junior—one who’d never treated a single COVID-19 patient—asserted that “there is now clear consensus in the medical and scientific community” that a key ingredient of Dr. Fareed’s treatment protocol doesn’t work. In effect, Dr. Jha told Dr. Fareed to reject the evidence of his own eyes and ears.
Shortly after the hearing, Dr. Jha published an opinion piece for the November 24, 2020, edition of the New York Times titled “The Snake-Oil Salesman of the Senate.” He opened with likening the event to a contagion.
There was a super-spreader event last week in the United States Senate. It wasn’t the coronavirus, however, that was spreading, but misinformation. … The Senate Homeland Security and Governmental Affairs Committee held a hearing about early treatment for COVID-19. Yet instead of a robust discussion about promising emerging therapies or what Congress might do to accelerate such treatments, the conversation was all about the malaria drug hydroxychloroquine. … Neither Ron Johnson, the Wisconsin Republican senator nor his chosen witnesses—three doctors who have pushed hydroxychloroquine—displayed more than a passing interest in evidence. Intuition and personal experiences of individual doctors were acclaimed as guiding principles.[i]
Dr. Jha didn’t mention that he himself had focused his Senate remarks on hydroxychloroquine and hadn’t mentioned any “promising emerging therapies” apart from vaccines. He also didn’t state the names or credentials of the hearing’s witnesses or a summary of their findings or experiences. He compared them to the snake oil salesmen from the frontier past with their advocacy of the drug that President Trump had touted in the spring, implying they were equally lacking in medical sophistication.
“I was called reckless because I pointed to facts that could prevent people from getting the treatment,” he wrote, but he didn’t state these facts. The online version of his essay hyperlinked the word “reckless” to a similar hatchet job report on the hearing in the Washington Post. He claimed the witnesses had expressed a distrust of science and had even “suggested that scientists were part of a ‘deep state’ conspiracy to deny Americans access to lifesaving therapies.” This was, he asserted, “a powerful reminder that not even Congress is immune to toxic conspiracy theories…”
Dr. Jha’s New York Times opinion was, itself, evidence that early treatment of COVID-19 was the subject of a well-orchestrated smear campaign. Why else would such a distinguished academic pen such rank propaganda against his colleagues and their work? That he was personally stung by the revelation that he’d never treated a single COVID-19 patient could only partly account for it.
A possible answer to this question may be gleaned from Dr. Jha’s remarks at a January 10, 2017, Georgetown University conference titled “Pandemic Preparedness in the Next Administration.”

Like the participants at the October 2019 Pandemic Simulation Exercise at Johns Hopkins, Dr. Jha predicted that a devastating pandemic “is going to come at some point.” Dr. Fauci, the keynote speaker, made a more precise prediction.
“There is no question that there will be a challenge to the coming administration in the arena of infectious diseases,” he proclaimed. “The thing we’re extraordinarily confident about is that we’re going to see this in the next few years.”[ii]
As psychiatrist and author Peter Breggin, MD, remarked in his extraordinary book COVID-19 and the Global Predators: We Are the Prey, Dr Jha did not speak in a somber tone about the coming devastation. On the contrary, he emphasized that he was excited about the ambitious project of helping the U.S. and other governments, and equally excited about the many pandemic preparation events in Georgetown and Cambridge that lay ahead. The conference was, he said, the “beginning of a journey.”[iii]
Dr. Jha and his colleagues were animated with the same excitement that denizens of the military-industrial complex would feel at the prospect of a coming war in which they would assume leadership positions. At last, they would be able to deploy all of their forces. With the recognition that the coming war was inevitable, they could call upon the government to allocate far more resources for new technologies, weapons systems, bases, and military organizations. In an atmosphere of such heady excitement, the suggestion of defusing the coming war with diplomacy wouldn’t be received with much enthusiasm.
The irony of Dr. Jha’s excitement is that, when the pandemic he predicted arrived three years later, he didn’t attempt to treat patients or scramble to find consultants to intervene against the disease before it wrecked bodies and imprisoned people in hospitals. Instead, he penned propaganda against hydroxychloroquine and against Drs. McCullough, Risch, and Fareed. Why was the New York Times Editorial Board compelled to publish his misleading account of the Senate hearing? Did the editors even watch the C-SPAN recording of it?
It’s not plausible that their motive was a concern about hydroxychloroquine’s safety. Dr. Jha himself conceded in his testimony that he wasn’t particularly concerned about safety, so why the vast and ceaseless quibbling about whether its efficacy for outpatients had been proven? As Senator Johnson had said in the hearing, this makes no sense.
[i] Jha, Ashish, MD. The Snake Oil Salesmen of the Senate. New York Times, Nov. 24, 2020. https://www.nytimes.com/2020/11/24/opinion/hydroxychloroquine-covid.html
[ii] Georgetown University Center for Global Health Science & Security, Pandemic Preparedness in the Next Administration. January 10, 2017. https://ghss.georgetown.edu/pandemicprep2017/
[iii] Breggin, Peter R, MD and Ginger Ross Breggin, COVID-19 AND THE GLOBAL PREDATORS: WE ARE THE PREY. Ithaca: Lake Edge Press, 2021, p. 259.
Alberta Premier suspends cooperation with WEF
Free West Media | November 25, 2022
The newly elected Premier Danielle Smith of the province of Alberta in Canada has recently made several powerful statements against the globalist foundation World Economic Forum and its leader Klaus Schwab. She has also decided to cancel a strange consulting agreement that WEF had with the province.
The now-revealed collaboration began in the middle of the alleged Corona pandemic and contributed to the draconian restrictions and lockdowns Canadians were subjected to. There are also those who believe that it is part of something much bigger. At the same time, she demanded that the Trudeau administration end the agenda-driven carbon tax.
On October 11, Danielle Smith was sworn in as Premier of the oil-producing province of Alberta in Canada. It came just five days after she won the leadership election of her United Conservative Party (UCP), largely on promises to stand up to the federal government in Ottawa led by the increasingly unpopular Justin Trudeau.
Trudeau has been leader of the Liberal Party of Canada since 2013 and Prime Minister of Canada since 2015. He distinguished himself during the alleged Corona pandemic as one of the most tyrannical leaders in the world, violently cracking down on peaceful popular protests. Trudeau is a member of the notorious globalist organization World Economic Forum (WEF) elite school Young Global Leaders (YGL).
YGL is a leadership program within the WEF, where politicians are schooled and initiated into the globalists’ plans and are then helped into leadership positions.
‘I find it offensive’
On October 24, barely two weeks after taking office, Danielle Smith made a move that sent the establishment in Canada into a tailspin. The new Premier harshly criticized the WEF and its chairman and founder Klaus Schwab.
“I find it uncomfortable when billionaires brag about how much control they have over political leaders like the head [Schwab] of that organization [WEF] has,” Smith said after a ceremony where her ministers were sworn in to the new provincial government.
“I find it offensive. The people who should be running the [provincial] government are the people who vote for them. And the people who vote for me and my colleagues are people who live in Alberta and who are affected by our decisions,” explained the Premier.
“So quite frankly, until that organization [WEF] stops bragging about how much control they have over political leaders, I have no interest in being involved with them. My focus is here in Alberta, to solve problems for the people of Alberta, with the mandate I received from the people of Alberta,” said Smith, announcing the suspension of the province’s cooperation with the globalist foundation.
Alberta’s new leader was referring to provocative statements made by WEF chief Klaus Schwab. One of these that specifically concerned Canada was done in 2017 at the Harvard Kennedy School’s Institute of Politics where political commentator David Gergen interviewed Schwab. The WEF chief then said that his organization had “infiltrated governments” all over the world. A visibly proud Schwab then also named several heads of state, including Canadian Prime Minister Justin Trudeau, as examples of the WEF’s global power and influence.
“Yesterday I was at a reception for Prime Minister Trudeau and I learned that half of his ministers or even more than half are actually our Young Global Leaders (YGL) of the World Economic Forum,” said the arch-globalist Schwab.
WEF health experts?
Danielle Smith further revealed that it has emerged that the province of Alberta has a cooperation agreement with the globalist foundation WEF, something she wanted to end right away.
“They signed a kind of partnership with the World Economic Forum in the middle of the pandemic; we have to deal with it. Why on earth do we have anything to do with the World Economic Forum? It must end,” the new Premier declared firmly.
She was immediately harshly attacked by mainstream media in Canada, who accused her of espousing “extreme right-wing conspiracy theories”, while mainstream media abroad tried to black out her statements.
Many Canadians were surprised to learn that the globalist organization WEF had a direct contract with one of their provincial governments. They were even more surprised when they heard what the agreement was. It did not concern consultation regarding economic issues or even “Agenda 2030 and the global goals for sustainable development”, where the WEF works closely with the UN – or as many critics believe rather dictates to the UN.
Instead, it turned out that early in the alleged 2020 Corona pandemic, the WEF stepped in as health consultants to effectively dictate the pandemic measures taken by the Canadian province of Alberta’s health authority, Alberta Health Services (AHS). Danielle Smith has been a strong critic of this authority and how it, like the previous provincial government, handled the pandemic.
On October 21, ten days after taking office as prime minister and three days before the sensational announcement, Smith commented during the “Question Period with Premier Danielle Smith” on the Western Standard media website that the health authority AHS would be held accountable for both the cooperation with the WEF and the “health councils” which they had given to the provincial government over the last two years. Canada stood out during the pandemic as one of the countries that had the most repressive restrictions and lockdowns in the world. Not least, vaccine-free citizens were grossly discriminated against.
“I think Alberta Health Services is the source of many of the problems we’ve had,” explained Smith, who also described the cooperation with the WEF as “useless”.
Many Albertans were well aware that the health authority AHS was driving the very unpopular restrictions and regulations, as were many other health authorities around the world, but they did not know that the globalist organization WEF was the one pulling the strings. It came as a shock to many and some questioned how the WEF could contribute medical expertise.
Some pundits also cited the example of globalist billionaire Bill Gates, who has been portrayed by the establishment and its media as a pandemic expert in general and a vaccine expert in particular, despite his lack of a relevant education, and where his only direct link is that he has earned multi-billion sums from investing in vaccines in particular.
Globalist puppets
However, there are those who believe that the secret agreement is part of something bigger that is happening beyond public knowledge. One of these is George Gammon, an economist and analyst who made a name for himself by explaining complex economic and political events in an accurate and easy-to-understand manner.
He commented on the news that the WEF had a consulting engagement – on health issues – with the Canadian province of Alberta in a November 5 interview with Daniela Cambone. He did not express the same surprise as many others, but stated that the heads of state and ministers who are in power today have the WEF and its head Schwab to thank for it, that is to say, they are indebted and possibly even dependent on them.
They devote large amounts of their countries’ tax dollars to covert programs that involve the WEF in such a way that the globalist organization can directly influence the country’s policies on issues important to them in order to drive their globalist agenda forward.
Economist Gammon further explained that the arrangement not only brought global power but also revenue to the WEF, which is on paper a Swiss non-profit foundation, and thus also to Schwab personally. These not infrequently very large amounts can then be used to train new leaders in the elite Young Global Leaders (YGL) school, and so on.
For the WEF it is a win-win situation, while for the taxpayers in Canada and other countries it is a double loss, where they lose both their tax money and, in the case of the Corona response, freedoms. Gammon concluded by pointing out that it is probably a common scheme in several countries and described it as pure fraud.
“This is the scam that is going on right now and it is something that most people are not aware of,” said Gammon about the WEF-Alberta agreement
‘Hostile politics’
On November 10, Premier Smith tweeted: “It is time to put people’s needs before politics. I have asked Prime Minister @justintrudeau to consider the financial hardships facing so many Canadian families right now.”
The Prime Minister’s tweet referred to a letter she had sent to Justin Trudeau the day before. In it, she stated that the number one problem for Albertans and all Canadians was the rapidly rising cost of living. Smith wrote that “with runaway inflation, many Canadians are struggling to feed their families, pay their rent and utility bills, and afford to get to work.”
She asked Trudeau to change course: “The long-term solution to this cost-of-living crisis involves the federal government changing course to actively promote and deliver more affordable, reliable and responsibly produced energy and food. Current federal energy and agricultural policies have the opposite effect”.
Critics believe that these nefarious policies are also dictated by the WEF.
Smith further wrote that her province of Alberta has already taken steps to deal with rising costs, including pausing the fuel tax and subsidizing electricity and natural gas. She urged Trudeau to do the same and completely eliminate the federal carbon tax, which Trudeau instead wants to raise further. Smith further wrote that “the answer to reducing emissions is not more taxes on consumers or limiting economic growth in our food and energy sectors”.
Later, she sent out another tweet reiterating the main points of the two-page letter: “The carbon tax is hurting Canadians. Families and businesses need a reprieve from high utility bills, prohibitively expensive food and rising gas prices. It is time to end the carbon tax.”
The next day, on November 11, she called the Trudeau administration hostile in a new tweet: “Today our [provincial] government took a step forward to stand up and defend Alberta’s interests against hostile federal government legislation and policies.”
Alberta’s Deputy Premier, Kaycee Madu, has also been highly critical of Ottawa’s “tyrannical” pandemic restrictions and also thanked the Freedom Convoy participants for their efforts to protest them. In a tweet on September 20, he wrote that the pandemic measures were “never about science but about political control and power”.
He saluted all the Canadians who at the beginning of the year stood up against the oppression of the WEF-schooled Trudeau in the name of public health: “Thank you to all those citizens of the Freedom Convoy who had the courage to mobilize against this tyrannical policy. They endured much hatred, abuse, suffering and slander for all of us. I thank them.”
There are many Canadians and people around the world who share his opinion of the brave who dared to stand up for freedom; despite having their bank accounts frozen, being threatened with having their vehicles impounded and ultimately in several cases enduring the brutality of the Trudeau regime.
The globalists and their handy politicians and journalists can now be expected to come down very hard on Smith and Madu, who have taken the side of their constituents and challenged the WEF and Trudeau – something very unusual in modern politics.
DANGER: “ANTI-VACCINE” THOUGHTS ARE A MENTAL ILLNESS REQUIRING “TREATMENT”
Amazing Polly | November 24, 2022
Building blocks are being put into place so that political dissidents can be drugged or locked up much like the Soviets did with Sluggish Schizophrenia.
Can you support my work with a financial gift? If so click here, thank you! https://amazingpolly.net/contact-support.php
References:
-CPSO Guidelines on vaccine ‘hesitancy’: https://www.cpso.on.ca/Physicians/Your-Practice/Physician-Advisory-Services/COVID-19-FAQs-for-Physicians
-Canadian Psychiatric Association Seminar on New Delusions: https://archive.ph/Eg1rV
-Euthanasia Article from Associated Press, Aug 2022: https://apnews.com/article/covid-science-health-toronto-7c631558a457188d2bd2b5cfd360a867
-VIDEO: Are Leaders Being Threatened by the Medical Mafia?: https://www.bitchute.com/video/8QClDbzxpt22/
-Study Claiming anti-vaccine info is causing blood clots, heart attacks, etc in the vaccinated: Covid 19 vaccines and the misinterpretation of perceived side effects clarity on the safety of vaccines. | Biomedicine (Taipei);12(3): 1-4, 2022. | MEDLINE (bvsalud.org)
Time to come clean about Covid’s lab origins

By Neville Hodgkinson | TCW Defending Freedom | November 24, 2022
More than two years ago, an Anglo-Norwegian team of scientists demonstrated unique ‘fingerprints’ of laboratory manipulation in the Covid virus. They argued that the evidence as good as proved that the virus had originated in a lab rather than evolving naturally. The manipulation, which made a bat virus a danger to humans, was exactly as envisaged by American and Chinese researchers who had been working on a vaccine aimed at reducing the impact of any such future outbreaks.
A paper describing these findings, co-authored by London University vaccines expert Professor Angus Dalgleish, was suppressed in both the US and UK. Internationally, the World Health Organisation, leading science journals and others made a huge effort to persuade us that Covid was a natural occurrence – and that we should spend a lot more money to fight any such future threats.
However the paper was uploaded by the Norwegian website Minerva in July 2020, and an update appeared on the website in May 2021 which I reported here.
Now an American expert in the field, who previously dismissed the lab-origin theory, has reached exactly the same conclusion. ‘The body of evidence supporting a lab origin of SARS-CoV-2 is overwhelming, far more so than most realise,’ says biologist and analyst Dr Alex Washburne in a newly published ten-page report.
He studied transmission of infections from bats to people for many years before Covid. ‘Pathogen spillover is common,’ he writes, ‘and so for much of the pandemic I kept an open mind about a laboratory origin yet remained firmly entrenched in my prior belief of a zoonotic [animal] origin. However . . . the totality of evidence has completely changed my mind.’
Before Covid, Dr Washburne was working with a team funded by a US Defense Department grant aimed at pre-empting pandemics by studying whether some strains of animal viruses were more likely to cause human disease than others.
He says it takes a lot of effort to find and examine naturally occurring viruses, and so ‘there is a clear temptation to make new viruses, such as chimeric viruses or viruses passaged in human cells. If we made a virus more capable of infecting people, it might reveal the essence of human-infective viruses and help us prepare vaccines before a pandemic ever happens.
‘Engineer and evolve a novel pandemic-capable virus to create a vaccine against the virus before it causes a pandemic, and you might win a Nobel Prize . . . provided nothing goes wrong.’
He describes how in March 2018 a proposal to do just that was drawn up by EcoHealth Alliance (a global non-profit with the slogan ‘Standing Between You and the Next Pandemic’) with the Wuhan Institute of Virology in China and other international collaborators.
The plan was to sample bat coronaviruses, assemble cloned copies of the viruses in the lab, introduce genes that might make them a threat to humans, and test the resulting chimeric viruses in the lab at Wuhan.
‘Find, engineer, and evolve human-infectious viruses capable of causing a pandemic, develop a vaccine against them, and pre-empt a pandemic . . . provided nothing goes wrong.’
DARPA, the US Defense Advanced Research Projects Agency, turned down the proposal on safety grounds.
But the group had alternative sources of funding, including a biodefence grant from the US National Institute of Allergy and Infectious Diseases. The fact that SARS-CoV-2 emerged in Wuhan, with an exact fingerprint of the proposed manipulation, and a geographic pattern inconsistent with its having emerged from animal trade, ‘ought to tilt the scales towards a laboratory origin’, Washburne says.
He adds that ‘as a scientist, I can’t tell you how badly I want scientists to have not opened Pandora’s Box. It took enormous amounts of self-examination and self-criticism to question my own cherished belief in the theory of a zoonotic origin’.
He might have been able to change his mind sooner if the findings of the Anglo-Norwegian team had been examined at the pandemic’s outset.
The team’s findings were exactly in line with those now highlighted by Washburne. They found that the virus’s so-called spike protein had six inserts, ‘unique fingerprints . . . indicative of purposive manipulation’, which allowed it to infect and damage a wide range of human cells. They showed how these and other features of the virus were linked to laboratory work published by the Chinese and American researchers.
The authors wrote: ‘Since, regrettably, international access has not been allowed to the relevant laboratories or materials, since Chinese scientists who wished to share their knowledge have not been able to do so and indeed since it appears that preserved virus material and related information have been destroyed, we are compelled to apply deduction to the published scientific literature, informed by our own biochemical analyses.
‘We refute pre-emptively objection that this methodology does not result in absolute proof by observing that to make such a statement is to misunderstand scientific logic. The longer the chain of causation of individual findings that is shown, especially converging from different disciplines, the greater the confidence in the whole.’
The team also warned that vaccine-makers who failed to acknowledge the chimeric nature of the virus, and the toxicity of the spike protein, might unwittingly put the public at risk.
We now know that wittingly or not the vaccine-makers put out products which present an even bigger threat to health for some than the virus itself, and have been linked to tens of thousands of deaths and millions of adverse events. But because of the obstacles put in the way of a genuine understanding of the virus’s nature, regulators continue to assure the public that the products are ‘safe and effective’.
I believe there was high-level knowledge from the very start that this was not a naturally evolved virus, but a chimera – originally native to Chinese bats but manipulated in the laboratory to see if it could become a threat to humans.
If Covid really was a straightforward zoonosis – an infectious disease of animal origin – why was a global panic button pressed, leading to the ruinous lockdowns and other crisis measures which were to cost the UK £500billion over the next two and a half years?
Why did top scientists and public health officials persist in demanding panic measures long after it was clear that the threat from Covid was not as bad as had been feared?
Why did the G20 countries at their recent meeting in Bali sing the praises of Covid immunisation as a ‘global public good’, and flag up digital and non-digital ‘proof of vaccinations’ to facilitate ‘seamless international travel’?
Is it because of fears that another, more dangerous genetically engineered pathogen is in the pipeline?
Chinese scientists and public health officials are said to have predicted that World War Three will be fought with ‘a new era of genetic weapons’ which can be ‘artificially manipulated into an emerging human disease virus, then weaponised and unleashed in a way never seen before’.
This is clearly a subject with which governments and their intelligence agencies worldwide must be familiar. May I suggest that if that is the real fear, they should come clean about it, and stop treating us like idiots? That would do a lot to improve understanding, and help end a damaging crisis of confidence in science that could prove a lot more damaging than SARS-CoV-2 itself.
Covid-19 Vaccines in Pregnancy
How much do we really know about safety?
Health Advisory & Recovery Team | November 20, 2022
There are gaps in our knowledge about the risk from covid infection in pregnancy but even larger gaps regarding the risks of vaccination. What we do know, however, is that there have always been very good reasons to be cautious of giving medication in pregnancy.
How risky is SARS-CoV-2 infection during pregnancy?
Early in the pandemic, the fear was raised that Covid-19 was more severe during pregnancy. This would not be surprising, as that is true for any infection. There are several reasons for this. The immune system is relatively down-regulated in pregnancy (vital so that the mother does not reject the developing fetus which of course is 50% genetically ‘non-self’) making women more susceptible to infections. It is known that some viral infections, such as rubella and cytomegalovirus cause fetal abnormalities if caught early in pregnancy. In late pregnancy, respiratory infections are likely to be more problematic, as the diaphragm may be splinted by the growing uterus, making breathing shallower. Also any febrile illness may tip the mother into preterm labour. And finally there was the concern that passage of the virus across the placenta could infect the baby, as may be seen in untreated HIV infection.
Thus, there were good theoretical reasons to be concerned. On the other hand, Covid-19 severity was known to be highly related to older age groups and serious comorbidities whereas the majority of pregnant women will be young and healthy. In all, nine pregnant women died with Covid-19 between March and December 2020 from a total of 683,191 births that year. SARS-CoV-2 infections with the recent omicron variants are known to be much milder, including during pregnancy.
One problem with quantifying the risk of Covdi-19 in pregnancy arises from the routine testing – thus anyone admitted for obstetric reasons was tested and so hospitalisations in pregnancy will have all been counted as pregnant covid admissions where in reality many were admissions for pregnancy complications at a time of high SARS-CoV-2 prevalence.
Finally, the evidence that vaccination has reduced risk from covid in pregnant women is lacking.
What do we know about covid vaccine safety in pregnancy?
The honest answer to this is ‘very little’. All the randomised clinical trials have specifically excluded pregnant women. Indeed, participants in the trials had to affirm that they were not trying to become pregnant and that if sexually active they would take contraceptive precautions. These rules were also applied to potential fathers and an obligation to inform the trial investigators should pregnancy occur. Invariably, some participants in the trials did become pregnant but full information on the outcomes is not available.
It was known that Pfizer’s animal studies showed the lipid nanoparticles were detectable in the ovaries (see Table 4-2). Moreover, SARS-CoV-2 spike glycoprotein was found to share similarities with 27 human proteins that relate to egg production (oogenesis), uterine receptivity and placentation. It is also known that the pregnancy studies in rats involved a higher rate of pregnancy losses and fetal anomalies in the vaccine than the placebo arm, despite which, these limited studies were reported as showing no concerns. See this analysis of recently released Pfizer data.
A detailed open letter to the president of the RCOG highlights the lack of information and some worrying signals of potential harm. One such signal is the increase in neonatal deaths in Scotland. It has already been concluded that these deaths were not related to Covid-19 itself but, like the excess deaths in the whole population, the officials and the MSM are ‘baffled’. Oddly, no-one has looked at the effect of vaccination beyond 28 days. Public Health Scotland declared there was no “plausible link” to vaccination to justify investigation, adding, “the outcomes of such analysis, whilst being uninformative for public health decision making, had the potential to be used to harm vaccine confidence at this critical time.” Indeed, Professor Sarah Stock, expert in maternal and fetal medicine at the University of Edinburgh, commented in May 2022: “The numbers are really troubling, and I don’t think we know the reasons why yet” but “stressed the Covid vaccine, which studies have consistently shown to be safe in pregnancy, was not a factor”. Professor Richard Ennos, also from Edinburgh University, has written challenging her logic.
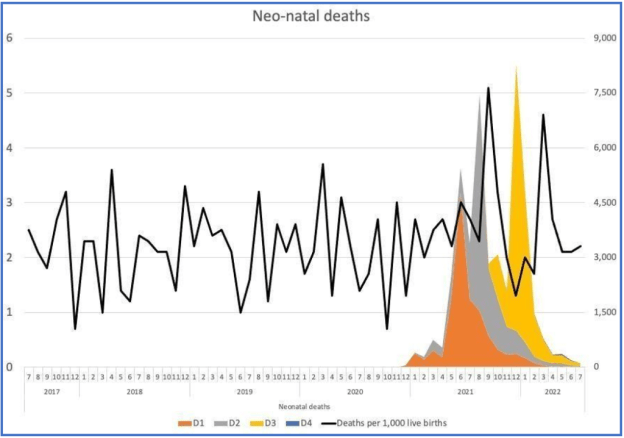
Figure 1: Scottish data on neonatal death rate per 1,000 live births per month (left axis) and doses given to pregnant women (right axis).
An inquiry has been launched in September 2022, but is likely to take 6-9 months – the temporal link to the vaccines would at least suggest a much more urgent need for investigation.
It is not only in the UK that concerns have been raised. Australia has had an extraordinary fall in live birth rate in the last two months of 2021 (2022 figures are not yet available). The results are so extreme that it must surely be some sort of reporting error. But Germany and Sweden have also seen a sharp drop in fertility rates in recent months which have been analysed here, looking a Covid-19 infections, unemployment rates and vaccination rates.
A hugely concerning peer-reviewed preprint has been published showing reduction in stem-cells from umbilical cord samples after Covid-19 infection but much more marked effects following vaccination. The paper has been reviewed here. These cells are an integral part of the newborn infants developing immune system.
Historical pharmaceutical catastrophes and cautions
The most widely known example of severe harm resulting from a drug used in pregnancy is Thalidomide. Launched in 1953 as a tranquiliser, the drug company was taken over the following year and it was relaunched in 1958 as an anti-sickness medication, despite undergoing no specific testing in pregnancy. Over the next 3 years, over 10,000 babies were born with severe limb defects and some also deaf or blind and many thousands are thought to have died. Women had trusted the authorities that all safety checks had been carried out, but sadly irreversible and catastrophic harm resulted before the drug was eventually withdrawn. It was the Thalidomide scandal which led to the setting up of the UK Yellow Card system.
The prescribing of diethylstilbestrol to pregnant women resulted in harm to female fetuses, which only became apparent when the exposed girls themselves reached adulthood. It took 30 years before the late cancer risks were fully recognised and the use of diethylstilboestrol in pregnancy was stopped. Similarly, sodium valproate, an effective anticonvulsant, when given in pregnancy can cause ‘fetal valproate syndrome’, with severe effects on cognitive function. Its teratogenic potential was known from animal studies prior to its launch in 1972, yet even as recently as 2020, women were still not fully informed. It is noteworthy that a BMJ letter in 1981 sounding caution came from a group in Finland – the same country who first noted narcolepsy in children following Pandemrix vaccination. The shortcomings of our healthcare system, described as “disjointed, siloed, unresponsive and defensive” are evident in the Cumberlege Review published July 2020 – ‘First Do No Harm’.
It is against this background that the British National Formulary has strict cautions on prescribing in pregnancy, stating:
“Drugs can have harmful effects on the embryo or fetus at any time during pregnancy. … Drugs should be prescribed in pregnancy only if the expected benefit to the mother is thought to be greater than the risk to the fetus, and all drugs should be avoided if possible during the first trimester. During the second and third trimesters drugs can affect the growth or functional development of the fetus, or they can have toxic effects on fetal tissues.”
“Not all the damaging effects of intrauterine exposure to drugs are obvious at birth, some may only manifest later in life. Such late-onset effects include malignancy, e.g. adenocarcinoma of the vagina after puberty in females exposed to diethylstilbestrol in the womb, and adverse effects on intellectual, social, and functional development.”
Most vitally the BNF reminds us, “Absence of information does not imply safety.”
We can only hope that in the case of the Covid-19 vaccines, this does not turn out to be prophetic.
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- Historic blow to South Korea’s military intelligence agency
- Russian frigate fires warning shots in English Channel
- Radio Free Europe, the Cold War ‘Weapon’ Congress Still Funds
- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- The Straight of Hormuz is Open for Iranian Business… Oil is Moving and Iran is Getting Paid
- Biden’s Closed Circle on Russia
- Lebanon Accuses Israel Of Violating The Chemical Weapons Convention By Spraying Toxic Herbicide Over Farmland
- Did the 9/11 Hijackers Really Fly the Planes?
- If Americans Knew
- Israeli army ‘murdered child’ in Gaza and then dumped body on a roadside
- The Forward’s Hit Piece on Thomas Massie and USS Liberty Veterans
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- No Tricks Zone
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
