More than a month has passed since Texas Gov. Greg Abbott shocked the Faucis of the world by scrapping COVID-inspired restrictions on businesses and individuals, including removing the mask mandate. The decisions prompted Dr. Anthony Fauci and legions of public health “experts” to warn about the devastating consequences – thousands of unnecessary deaths would result, they said – however, as the data show, practically every metric has shown that the Lone Star State’s outbreak has continued to recede, even as blue states like Michigan are seeing a new surge in infections (believed to be driven by “mutant” strains).
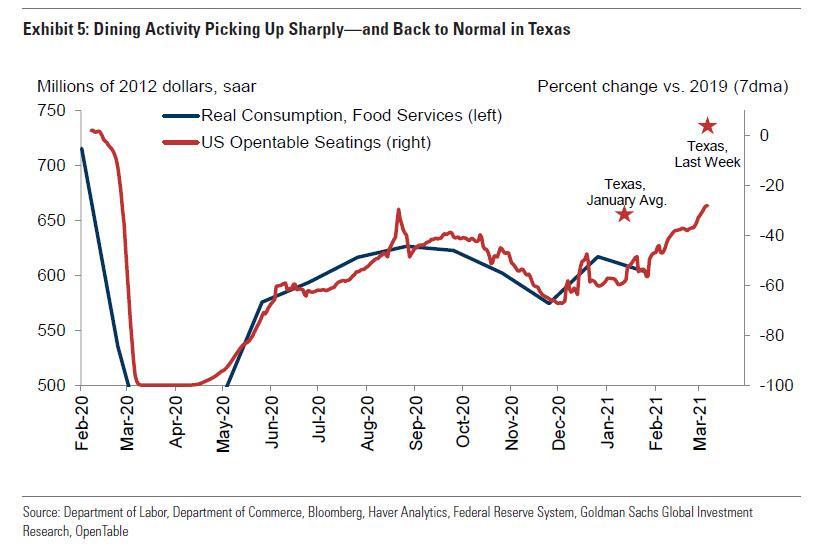
As epidemiologists everywhere have struggled to come up with an explanation, it’s worth noting that Texans are dining out more, according to Opentable seatings, which have become a closely watched proxy for post-quarantine economic activity.
As experts have struggled to come up with a satisfying answer, Dr. Fauci was asked about the phenomenon during an interview on MSNBC Tuesday morning as the senior advisor to President Biden made the rounds. As MSNBC noted, “if you go to Texas… it looks like 2019… the restaurants are full… the ballparks are full…” and yet, cases have continued to tick downward.
Dr. Fauci seemed dumbfounded. He first suggested that the surge in cases simply hadn’t manifested yet because of a “lag”. That might have made sense if the trend had only been in place for a week or two. But a month has passed, and Texas’ positivity rate – the share of new tests that yield positive results, seen as a more accurate representation of community spread – has continued to fall.
“It can be confusing because you may see a lag or a delay, because often you have to wait a few weeks… there’s a lot of things that go into that,” Dr. Fauci said.
“I’m not really sure, it could be because they’re doing things outdoors, you know it’s very difficult to just one-on-one compare that…I hope they continue to tick down, if they do that would be great. But there’s always the concern that when you pull back on methods, particularly things like indoor dining, or bars that are crowded…you could see a delay, then all of a sudden cases tick back up.”
“We’ve been fooled before with places opening up, then nothing happens, but all of a sudden a few weeks later cases explode on you.”
He concluded by saying “we’ve got to be careful we don’t prematurely judge” the situation in Texas.
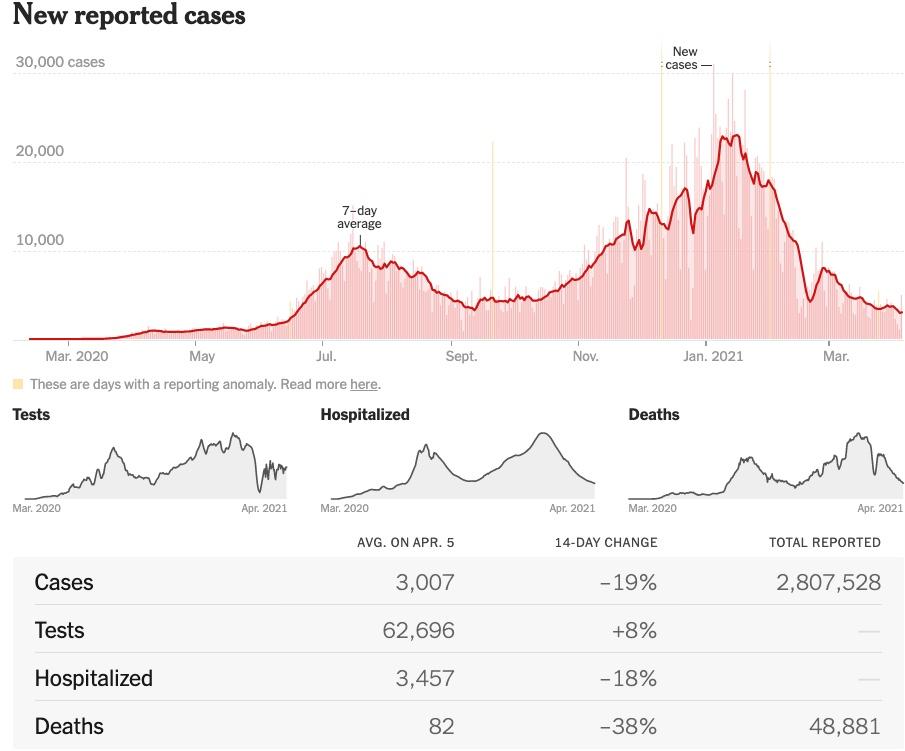
For those who haven’t been closely following the situation in Texas, 26 days have passed since the state “reopened 100%” with no mask mandate, and 34 days have passed since Gov. Abbott announced the reopening. The number of new cases, deaths, hospitalizations ICU occupancy and positivity rate have all fallen.
Once again, the UK government has been shown to have used ‘covert tactics’ in order to scare UK residents into staying at home for lockdown by increasing the ‘perceived threat’ of COVID’ rather than genuine science-backed risk assessment data, and also used ‘hard-hitting emotional messages’ designed to cower the public into complying with the government’s arbitrary diktats.
Due to the heightened level of public outrage, mainstream media outlets are finally being forced to admit what they have been systematically covering-up now for 12 months – that Government have been involved in active psychological and information warfare measures against their own population.
In a document presented to the UK government’s ‘SAGE’ confab, a scientific group meant to advise government on pandemic policies, it was revealed how technocrats sought to increase the ‘perceived threat’ of COVID-19 using aggressive psychological ‘hard-hitting emotional messages’ in order to brainwash the public into compliance.
Upon hearing the official admission, some psychology professionals have turned their sights on Downing Street, accusing bureaucrats of using “covert psychological strategies” in order to hype-up the threat of the virus, and offering no context as to the actual risk posed to the general public.
Government officials are accused of creating ‘a state of heightened anxiety’ which led to many people becoming ‘too frightened to attend hospital’.
This rebuke of the government’s active measures is given further credence by the fact that the majority of hospital beds in the UK remained largely empty in 2020, especially during the first few months of the ‘pandemic.’ This is especially relevant because it was at this same time when the government and mainstream media were relentlessly pushing out the idea that health services were ‘under threat’ of being overrun by Covid, only it never happened.
As a result of the government’s fear campaign, along with the overall throttling of the NHS, there have been an estimated 4.66 million people left waiting many months to begin even routine treatment, as well as thousands of pre-cancer screening appoints abandoned or pushed back – all because of the constant ramping-up of the fear of Covid.
The question still remains: will cabinet ministers be held to account for this unprecedented over-reach of state power?
Experts fear Britons have been the subject of an experiment in the use of tactics which operate ‘below their level of awareness,’ it was said.
They have now made a formal complaint to an organisation which will rule on whether Government advisers are guilty of a breach of ethics.
Downing street denies this, claiming it simply presented the facts.
Complainants point to a document handed to the Scientific Advisory Group for Emergencies last March, when the pandemic began to rapidly grow in Britain.
The paper, written by Scientific Pandemic Influenza Group on Behaviours, said: ‘A substantial number of people still do not feel sufficiently personally threatened; it could be that they are reassured by the low death rate in their demographic group, although levels of concern may be rising.
‘The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging. To be effective this must also empower people by making clear the actions they can take to reduce the threat.’
The document, seen by the Telegraph, allegedly then gave 14 options for improving compliance including ‘use media to increase sense of personal threat’, which they said would be highly effective but runs the risk of ‘negative’ side effects.
SAGE members have since claimed the British public have been ‘subjected to an unevaluated psychological experiment without being told that is what’s happening.’
They added that SPI-B reports are often not ‘challenged’ by SAGE because many of those involved are ‘not very well equipped to evaluate it.’
‘When someone from SPI-B is saying we need to ramp up the fear and keep it ramped up – there wasn’t much questioning of that at the beginning and most of the questioning came from external sources, not from within.’
SPI-B is described as providing behavioural science advice aimed at anticipating and helping people adhere to interventions that are recommended by medical or epidemiological experts.
(…) Last November, Sir Patrick Vallance admitted he had ‘regrets’ over frightening people with a doomsday dossier that forecasted as many as 4,000 Covid-19 deaths a day over winter and was used to justify a second national lockdown.
Number 10’s top scientific adviser made the comments alongside Professor Chris Whitty, England’s chief medical officer, after the pair were hauled before MPs to defend SAGE’s modelling that also predicted hospitals would be overrun with virus patients by the end of this month.
During the grilling by members of the House of Commons Science and Technology Committee, Labour MP Graham Stringer asked Sir Patrick if he believed he had frightened people with the bleak deaths data presented during Saturday night’s press briefing.
The Chief Scientific Adviser said: ‘I hope not and that’s certainly not the aim… I think I positioned that as a scenario from a couple of weeks ago, based on an assumption to try and get a new reasonable worst-case scenario. And if that didn’t come across then I regret that.
PANDA (Pandemics – data and analysis) has been outspoken with regards to the policy-makers’ reaction to Covid-19, lockdowns and other approaches to the virus. Its viewpoints have ruffled feathers over the past year, with many in the establishment openly hostile towards the group of actuaries, accountants, economists and other professionals who participate in the global think tank. Nick Hudson, co-founder of PANDA, spoke at the inaugural BizNews Investment Conference in March 2021. Here’s his keynote address.
The British public’s widespread compliance with lockdown restrictions and the subsequent vaccine rollout has been the most remarkable aspect of the coronavirus crisis.
The removal of our basic freedoms — in the form of lockdowns, travel bans and mandatory mask wearing — have been passively accepted by the large majority of people. Furthermore, the proportion of the general public expressing a willingness to accept the Covid-19 vaccines has been greater in the UK than almost anywhere else in the world. But has the government achieved this widespread conformity through the unethical use of covert psychological strategies — “nudges” — in their messaging campaign?
A major contributor to the mass obedience of the British people is likely to have been the activities of government-employed psychologists working as part of the “Behavioural Insights Team” (BIT). The BIT was conceived in 2010 as “the world’s first government institution dedicated to the application of behavioural science to policy.” In collaboration with governments and other stakeholders, the team aspire to use behavioural insights to “improve people’s lives and communities”. Several members of BIT, together with other psychologists, currently sit on the Scientific Pandemic Insights Group on Behaviours (SPI-B), a subgroup of SAGE, which offers advice to the government about how to maximise the impact of its Covid-19 communications.
A comprehensive account of the psychological approaches deployed by BIT is provided by an Institute of Government document titled MINDSPACE: Influencing behaviour through public policy, where it is claimed that these strategies can achieve “low cost, low pain ways of ‘nudging’ citizens … into new ways of acting by going with the grain of how we think and act”. Several interventions of this type have been woven into the Covid-19 messaging campaign, including fear (inflating perceived threat levels), shame (conflating compliance with virtue) and peer pressure (portraying non-compliers as a deviant minority) – or “affect”, “ego” and “norms”, to use the language of behavioural science.
Behavioural scientists know that a frightened population is a compliant one, so this was exploited as a way of compelling us to abide by the coronavirus restrictions. The minutes of the SPI-B meeting on 22 March 2020 stated: “The perceived level of personal threat needs to be increased … using hard-hitting emotional messaging.” Aided by the mainstream media, the British public were subsequently bombarded with fear-inducing information, images and mantras: Covid-19 daily death counts reported without context; inflated predictions of future casualties; recurrent footage of dying patients in Intensive Care Units; and scary slogans like, “If you go out you can spread it”, or “People will die”, often accompanied by images of emergency personnel wearing PPE.
We all strive to maintain a positive view of ourselves. Utilising this human tendency, behavioural scientists have recommended messaging that equates virtue with adherence to the Covid-19 restrictions, so that following the rules preserves the integrity of our egos while any deviation evokes shame. Examples of these nudges in action include: slogans such as, “Stay home, Protect the NHS, Save lives” and “Protect yourselves, Protect your loved ones”; TV advertisements where an actor tells us, “I wear a face covering to protect my mates”; the pre-orchestrated Clap for Carers ritual; ministers telling students not to “kill your gran”; and close-up images of acutely unwell hospital patients with the voice-over, “Can you look them in the eyes and tell them you’re doing all you can to stop the spread of coronavirus?”
And then there’s what the psychologists euphemistically refer to as “normative pressure”: awareness of the prevalent views and behaviour of our fellow citizens — through peer pressure and scapegoating — can prise us into compliance. The simplest example is ministers repeatedly telling us that the vast majority of people are “obeying the rules”. But normative pressure is less effective in changing the behaviour of the deviant minority if there is no visible indicator of pro-social conformity rooted in communities. The mandating of masks in summer 2020 — in the absence of strong evidence that they reduce viral transmission in the community — enabled the rule breakers to be instantly distinguished from the followers. Appearing unmasked in public places now felt comparable to failing to display the icon of a dominant religion while being among devout followers; even if no explicit challenge ensues, the implicit demand to conform is palpable.
The same covert strategies are now being used to promote the uptake of the Covid-19 vaccines. The tactic of fear inflation is evident in a recent NHS England document that recommends healthcare staff “leverage anticipated regret” on the over-65s cohort by telling them they are “over three times more likely to die”. The recommended follow-up statement is, “Think about how you will feel if you do not get vaccinated and end up with Covid-19?” For young people — who are at vanishingly small risk of suffering serious illness should they contract Covid-19 — shame is the selected tool from the behavioural-science armoury; the recommendation is that they should be told “normality can only return, for you and others, with your vaccination.” As for the healthcare staff who will administer the jabs, the psychological experts suggest an ego boost from being hailed as the, “latest ‘NHS Heroes’”.
So, what’s wrong with using these covert psychological strategies to improve compliance with public health policy?
In comparison to the government’s traditional tools of persuasion (such as information provision and rational argument) these methods of influence differ in their nature and subconscious mode of action. Consequently, three sources of ethical concern emerge: problems with the methods per se; problems with the goals to which they are applied; and problems with the lack of consent.
It is questionable whether a civilised society should knowingly increase the emotional discomfort of its citizens as a means of gaining their compliance. State scientists deploying fear, shame and scapegoating to change minds is an ethically dubious practice that in some respects resembles the tactics used by totalitarian regimes such as China, where the state inflicts pain on a subset of its population in an attempt to eliminate beliefs and behaviour they perceive to be deviant.
Another ethical issue associated with the methods of covert nudging used in the Covid-19 communications campaign concerns the unintended consequences. Shaming and scapegoating has emboldened some people to harass those unable or unwilling to wear a face covering. More disturbingly, fear inflation has led to many people being too scared to attend hospital with non-Covid illness, while many old people, rendered housebound by fear, will have died prematurely from loneliness. Collateral damage of this sort is likely to be responsible for many of the tens of thousands of excess non-Covid deaths in private homes. In a civilised society, is it morally acceptable to use psychological strategies that are associated with this level of collateral damage?
The perceived legitimacy of using covert psychological strategies to influence people may also depend upon the behavioural goals that are being pursued. It seems likely that a higher proportion of the general public would be comfortable with the government resorting to subconscious nudges to reduce violent crime – for example, to discourage young men from stabbing each other – as compared to the purpose of imposing unprecedented and non-evidenced public-health restrictions. Would British citizens have agreed to the furtive deployment of fear, shame and peer pressure as a way of levering compliance with lockdowns and mask mandates? Maybe they should be asked before the Government considers any future imposition of these techniques.
In 2010, the authors of the MINDSPACE document — one of whom is Dr David Halpern, a member of SAGE and the SPI-B — recognised the significant ethical dilemmas arising from the use of influencing strategies that impact subconsciously on the country’s citizens and emphasised the importance of consent. Indeed, they could not be clearer: “policymakers wishing to use these tools … need the approval of the public to do so.” They go on to suggest some practical ways of acquiring this consent, including the facilitation of “deliberative forums” where a representative sample of several hundred people are brought together for a day or more to explore an issue and reach a collective decision. I am unaware of any public consultation of this type being conducted to gain the public’s permission to use covert psychological strategies.
At an individual level, obtaining a recipient’s permission prior to an intervention is a long-established principle of ethical clinical practice. Informed consent is an essential precursor to any medical procedure, including vaccination. To ensure ethical integrity, healthcare staff should be encouraging each potential recipient to, consciously and rationally, weigh up the pros and cons of accepting the Covid-19 vaccine rather than nudging them towards compliance.
The covert psychological strategies incorporated into the state’s coronavirus information campaign have achieved their aims of inducing a majority of the population to obey the draconian public health restrictions and accept vaccination. The nature of the tactics deployed — with their subconscious modes of action and the emotional discomfort generated — do, however, raise some pressing concerns about the legitimacy of using these kinds of psychological techniques for this purpose. The government, and their expert advisors, are operating in morally murky waters. An open, public-wide debate about the ethical integrity of these approaches — and the extensive collateral damage associated with them — is urgently required.
Dr Gary Sidley is a retired clinical psychologist with over 30 years’ experience working for the NHS. He is a member of the Health Advisory and Recovery Team (HART).
HART vs SAGE
HART Pathology Lead Dr John Lee appeared on Good Morning Britain this week alongside Professor Susan Michie who sits on SAGE and the Scientific Pandemic Insights Group on Behaviours (SPI-B).
Dr Lee noted the lack of evidence for asymptomatic spread of SARS-CoV-2 and also pointed out the absence of diverse scientific discussion in the media. Susanna Reid denied this, stating that the other side was being heard on social media and in the papers. However, these avenues are not the same as trusted mainstream TV programmes and the void of diverse thinking here has no doubt hampered the public’s understanding of ‘the science’.
Reid went on to say that ‘we know from the evidence that lockdown does work’. This is simply not true. Increasingly, the body of evidence points to the exact opposite as can be seen here and in dozens of published peer-reviewed papers, in stark contrast to the absence of evidence demonstrating significant benefits from lockdown when examining the real-world (as opposed to modelled) evidence. In addition, these models neglect to adequately assess the collateral harms.
Reid highlighted the figure of 126,000 COVID-19 deaths. However, there is a serious issue with excess, mainly non-Covid deaths at home which have reached over 50,000 in total. Here in the UK this figure currently sits at roughly 1,000 people each week. Perhaps many of these people would not have been put off seeking medical treatment had Michie, and her behavioural science colleagues, not terrified them into ‘staying at home’. A review of these covert, ethically questionable, psychological strategies was recently published by a member of HART here.
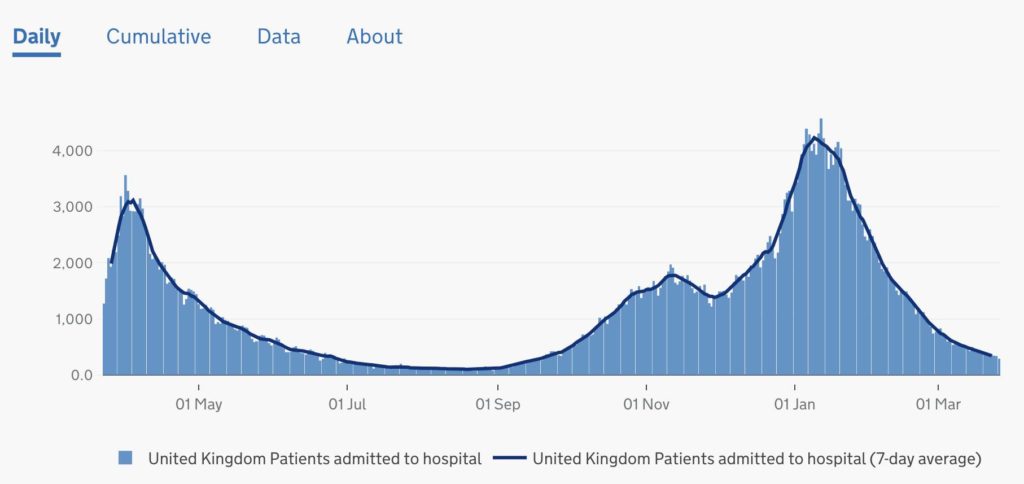
Michie also talked about mutant variants and how many people it is or is not ‘safe’ to interact with. It is a shame that these questions were addressed to a psychologist, rather than to a pathologist with medical training. No mention was made of the inevitable seasonal decline of the virus and Michie mentioned several thousand new cases a day, neglecting to outline how these figures relate to hospital statistics (currently at September levels).
Patients admitted to hospital in the UK
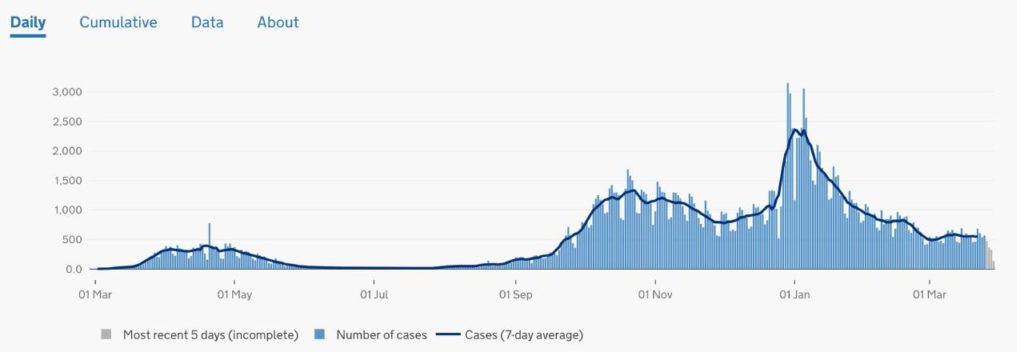
In fact, we know from numerous studies that there will be a significant number of post infectious positives at this stage with patients admitted to hospital for other reasons, incidentally testing positive. In the community, the expected surge in cases in the secondary school population has not materialised and the results of testing show that there is no active SARS-CoV-2 in that population. Overall, there is minimal evidence of residual coronavirus in the community. Mitchie went on to say cases are rising in Scotland. Again, this simply is not true.
Cases in Scotland
Michie then described the possibility of exponential growth if we remove measures too quickly, which shows a misunderstanding of the current immunity status of the population. With so many now having antibodies through natural infection or vaccination, it seems highly unlikely that this virus could now spread in an epidemic fashion. A transition into an endemic phase, as with seasonal flu in which there may be localised outbreaks, mainly in specific institutionalised settings, is much more likely.
The problems with Michie’s thesis are underpinned by the false assumption that asymptomatic spread is a major driver of transmission. There is no robust evidence for this phenomenon, and it would go against decades of understanding of respiratory viruses and how they are transmitted. By continuing to disseminate this questionable hypothesis to the British public, she is continuing to spread unnecessary fear. A far more balanced approach would be to focus on:
1. The viral season rapidly waning
2. The huge percentages of vaccinated people & those with acquired or innate immunity
3. The fact that children are not a significant driver of the disease
4. The fact that clinical symptoms are the driver of transmission of respiratory viruses
We need to stop ‘acting like we’ve got it’ and start living what is left of our finite lives.
Data not dates
It was reported this week that the weekly COVID-19-related death toll has fallen to the lowest rate since October. However, in a scenario of ever-decreasing death rates and diminishing prevalence of the virus, a comparison to the COVID mortality rate at the beginning of the winter wave seems somewhat arbitrary and of no relevance to the current situation. Once deaths reach minimal levels, this indicates that cases must have been minimal 18 days earlier.
A far more sensible metric for comparison would be the current test positivity rate. Since 21 March the PCR positivity rate has been only 2.1% i.e. only 1% higher than the baseline positivity rate we saw in summer. Including all testing, only 0.43% of 1.2 million tests were positive on 29 March. To put this in perspective, 9,957 people tested negative out of every 10,000 tests done. Remaining locked down under these circumstances indicates that the Government has adopted a “Zero Covid” strategy, despite their own admission of the futility and harm that would be caused by attempting this policy. Patrick Vallance himself said: “I think the chance of eradication, true eradication – ie zero – are in themselves close to zero.”
Tracking the success of the vaccine and maintaining confidence Last week, Sir Christopher Chope MP and William Wragg MP raised important questions in the House of Commons regarding COVID-19 deaths following coronavirus vaccination. Health Secretary Matt Hancock responded ‘I think we do have it’. Hancock also referred to the SIREN study but this only covers healthcare workers and therefore does not provide the complete information required for monitoring adverse effects, safety and efficacy. HART would urge active data capture, including a simple vaccine history taken at every unscheduled attendance at a hospital.
We must not forget that these are experimental vaccines, without full regulatory approval but issued under emergency waivers. It would be concerning in the extreme if data were not being collected or if the level of scrutiny of vaccine effects was not sufficient. The availability and rapid access to this data is vital in maintaining the public’s confidence in the vaccination programme.
US states continuing to open up Governors across the US are continuing to open up their states and remove COVID-19 restrictions. Earlier this month, Mississippi and Texas both announced the end of business restrictions and mask mandates, while North Dakota went a step further and implemented legislation to make mask mandates illegal. In Florida, Governor DeSantis is to forbid vaccine passports with an executive order.
In Texas, COVID-19 cases and hospitalisations carry on their downward trajectory despite their removal of measures being described variously as: “absolutely reckless” by California Governor Gavin Newsom, “it just is inexplicable why you would want to pull back now” by Dr Fauci and “neanderthal thinking” by President Joe Biden.
Essential viewing Nick Hudson, co-founder of the international group Pandemics ~ Data & Analytics (PANDA), has given a keynote address at the inaugural BizNews Investment Conference in South Africa. In his speech, Hudson gives a comprehensive overview of the COVID-19 pandemic and explores how instead of helping to slow the spread of the virus, lockdowns have led to infant mortality, poverty, starvation, joblessness and a major upsurge of psychological disorders. Well worth taking 30 minutes to watch in full, here. This video is currently being viewed by several thousand people per hour.
24 March 2021
There is no emergency COVID-19 cases are low and all-cause deaths are now back to normal pre-pandemic rates and falling. All vulnerable groups have been offered a vaccination. There are no longer any justifiable or ethical reasons for prolonging Covid-related statutory ‘emergency powers’.
It is anticipated that all phase 1 priority groups (approximately 32 million people) will have been offered a vaccine by 15 April, a group accounting for 99% of the deaths last spring. This will be an amazing achievement. The virus is now endemic and will circulate at very low levels this summer and is then likely to join the range of respiratory viruses circulating each winter. Talk of continuing social distancing and masks for several years is therefore unnecessary and unhelpful. We urgently need to reduce fear and increase hope as we recover from this crisis.
It is vital that we harness the benefits of the rapid vaccine rollout by acknowledging we are no longer in an emergency. We can and must reopen society. Government and SAGE will need to undo the negative messaging, after a year in restrictions many people will still be fearful to pick up their lives again. News that a £2m Government contract has just been awarded for a COVID Public Information Campaign over the next two years is concerning. The repeal of the coronavirus emergency legislation would give a very positive message of confidence and hope to the British public. Therefore, HART continues to urge all MPs to vote against the renewal of the Coronavirus Act this week in Parliament.
No evidence of SARS-CoV-2 in schools HART predicted 24,000 false positive results in children in the first week of mass testing based on 4 million children being tested twice. In the week of 4 March, only 2.7 million tests were carried out on secondary school children and 0.05% of them were positive. Our previous prediction was based on the estimated false positive rate for the adult population of 0.3%. Testing of university students prior to Christmas showed a very low false positive rate of at or below 0.06% including Newcastle, Hull, Exeter and Birmingham. Testing among school children is demonstrating a similar rate. The good news is that these numbers are so low that no-one can be left in any doubt that they represent only false positive results and that there is no SARS-CoV-2 at present in the secondary school population. The ONS estimated that there would be SARS-CoV-2 in 0.4% (1 in 250) 12-24 year olds, so this is another instance of failed testing with PCR. With no virus in schools, there is now no justification for the mask mandate or mass testing.
Is mask wearing benign? This week, Dr Mary Ramsay from Public Health England told the BBC that face coverings were a ‘lower level restriction’ that ‘people can live with’ and they should continue to be worn ‘for a few years’. Her words are similar to those used by politicians to justify the introduction of the mask mandate in summer 2020, when it was portrayed as an extra layer of protection, a precautionary measure, a nothing-to-lose restriction.
While there is no evidence that masks significantly reduce transmission when worn routinely in real-world settings, there is recognition that they may constitute an infection hazard, particularly when used incorrectly. Masks potentially cause physical harms, while the social and psychological cost of concealing our faces from other people is considerable. Face coverings impair all forms of communication and human connection, make lip-reading impossible for the deaf and constitute a gross impediment to children’s social development.
A highly visible reminder that danger is supposedly all around, face coverings are fuelling widespread, irrational fear at a time when the current viral threat is very low and the vulnerable have been vaccinated. As we look to re-activate the economy and reopen our society, this mask-induced fear will act as a major obstacle. HART believes the Government should now lift the mandate and allow people to decide for themselves whether to wear one. It is time to trust the public with their own personal risk-based decision making.
The futility of border closures Summer holidays are in doubt again, with the news that a £5,000 fine will come into force for anyone trying to travel abroad without a ‘reasonable excuse’. Matt Hancock has said the restrictions are to ‘guard against’ new variants that might put the vaccine rollout at risk. Professor Neil Ferguson was also quoted as saying we ‘should be planning on summer holidays in the UK not overseas’. Closing international borders to keep out ‘foreign mutants’ of an already endemic virus is neither useful nor possible. It is worth noting that mutant variants from abroad pose no extra threat compared with any homegrown variants and are likely to have very similar sequences. Mutant variants, emerging overseas or domestically, are an inevitable biological reality once a virus is in the population, as is the case in the UK. The virus will mutate slowly over time, irrespective of borders.
Mandatory vaccination for care home workers The news that the government is considering making COVID-19 vaccination a legal requirement for all care workers is concerning and against international law. This would create a precedent of eroding informed consent, and is difficult to justify when the vulnerable population have themselves already been offered at least one dose of vaccine, especially in the light of Scottish data that suggests the Oxford-AstraZeneca vaccine reduces risk of hospitalisation by up to 94%. If this is case, would it be better to prioritise second doses for all vulnerable groups, thus rendering the vaccination of our younger, healthy population unnecessary?
And some good news… The number of patients admitted per day to intensive care units is now close to normal, pre-pandemic levels for the time of year. It appears we are well beyond the risk of overwhelming the NHS – further highlighting that now is the time to lift restrictions and allow the NHS to begin rapidly addressing the backlog of postponed appointments and operations. There is no sign of a virus resurgence in American states such as Florida and Texas which have lifted restrictions.
In 2000, everything about Bill Gates’ public persona changed. He morphed from a hardnosed and ruthless technology monopolizer into a soft, fuzzy and incredibly generous philanthropist when he and his wife launched the Bill & Melinda Gates Foundation.1
It was a public relations coup. May 18, 1998, the U.S. Justice Department, in collaboration with 20 state attorneys, filed an antitrust lawsuit against Microsoft.2 At that time, the company was 23 years old and was ruling the personal computer market. The Seattle Times described the fallout from the antitrust lawsuit:3
“The company barely escaped being split up after it was ruled an unlawful monopolist in 2000 for using its stranglehold on the PC market with its Windows operating system to cripple competitors, such as Netscape’s Navigator Web browser.”
How would the world be different today if the company had been split? Yale law professor George Priest described the antitrust lawsuit as “one of the most important antitrust cases of its generation.”4 In 2002, a court settlement placed restrictions on Microsoft to curb some of its practices for five years.
It was later extended twice and then expired May 12, 2011. The lawsuit had a dramatic effect on “the emergence of an entirely new field called IP (intellectual property) antitrust,” Iowa law professor Herbert Hovenkamp told the Seattle Times.5
Later, large sums donated from the foundation made the news multiple times, including $9.5 million to GAVI (Global Alliance for Vaccines), a second $7.5 million to GAVI and $6.8 million to the World Health Organization in 2017.6
By June 2020, in the middle of a global pandemic, the Gates Foundation’s donations totaled 45% of WHO’s funding from nongovernmental sources.7 Once mainstream media’s attention was no longer on Gates’ antitrust activities and focused on the philanthropist actions of the foundation, Gates publicly turned his attention to vaccinating the world, long before COVID-19.8
Event 201: A Preplanned Pandemic
In a deep dive into the Gates Foundation’s charitable donations, The Nation found there were $250 million in grants to companies where the foundation held corporate stocks, including Novartis, GlaxoSmithKline, Merck, Sanofi and Medtronic. The money was directed at supporting projects “like developing new drugs and health monitoring systems and creating mobile banking services.”9
What Gates had discovered was an easy path to political power, allowing him to shape public policy without being elected to office. In other words, favorable headlines could be bought with charitable contributions.10 One event that Gates has personally supported and participated in was Event 201.11
Writing in The Defender, Robert Kennedy Jr. describes the exercise that Gates organized in October 2019. Many high-ranking men and women with governmental authority participated in Event 201, which coincidentally simulated a worldwide pandemic triggered by a novel coronavirus, just months before SARS-CoV-2, the virus that causes COVID-19, changed the world.12
They included representatives from the World Economic Forum, the Centers for Disease Control and Prevention, Johns Hopkins University Population Center, the World Bank, the Chinese government and vaccine maker Johnson & Johnson. During the event, the group developed strategies to control a pandemic, the population and the narrative surrounding the event.
At no time did they investigate using current therapeutic drugs and vitamins or communicating information about building immune systems. Instead, the aim was to develop and distribute patentable antiviral medications and a new wave of vaccines.
As Kennedy reports, Gates spoke to the BBC13 April 12, 2020, and claimed these types of simulations had not occurred, saying “Now here we are. You know we didn’t simulate this; we didn’t practice, so both the health policies and economic policies … we find ourselves in uncharted territories.”
Yet, videos of the event are available14 and Johns Hopkins Center for Health Security released a statement naming the Gates Foundation as a partner in sponsoring the pandemic simulation.15 It seems strange and alarming that a man with the responsibility of running the Gates Foundation and the powerful influence he has over global public policy decisions had forgotten an exercise he organized only six months before the interview.16 Or was it deception?
Uncanny Prediction or Planned Event?
During the pandemic exercise, the global experts “modeled a fictional coronavirus pandemic.”17 After questions arose about whether the exercise had “predicted the outbreak in China,” Johns Hopkins Center for Health Security released a thinly supported statement, saying:18
“… the exercise served to highlight preparedness and response challenges that would likely arise in a very severe pandemic … Although our tabletop exercise included a mock novel coronavirus, the inputs we use for modeling the potential impact of that fictional virus are not similar to nCoV-2019.”
Kennedy characterizes the fourth simulation in Event 201, writing that “the participants primarily focused on planning industry-centric, fear-mongering, police-state strategies for managing an imaginary global coronavirus contagion culminating in mass censorship of social media.”19
The transcript of the fourth simulation shows that the participants discussed communication strategies using dissemination of information and censorship on social media.20,21 Communication strategist Hasti Taghi, who works for a major media company and leads strategic initiatives with the World Economic Forum,22 said:
“So, I think a couple of things we have to consider are even before this began, the anti-vaccine movement was very strong and this is something specifically through social media that has spread.
So, as we do the research to come up with the right vaccines to help prevent the continuation of this, how do we get the right information out there? How do we communicate the right information to ensure that the public has trust in these vaccines that we’re creating?”
The question the group undertook wasn’t how to communicate the truth about the vaccine development, manufacture and distribution, but rather how to “communicate the right information to ensure the public has trust in these vaccines that we’re creating?”
The issue of gaining public trust to take a vaccine was significant in this simulation, even though the U.S. population is well indoctrinated in the perceived value of annual flu shots and childhood vaccinations. In fact, the Centers for Disease Control and Prevention has a list of 26 different types of vaccines currently in use in the U.S.
In addition to the long list of recommended childhood vaccinations, there are adult vaccines against shingles, tetanus and pneumococcal pneumonia that are routinely given. Why, then, did the global experts in communication and control believe communicating the “right information” would be necessary to “ensure the public trust”?
Group Calls for Social Media Censorship
This was only one of the highly predictive conversations during Event 201 that played out in 2020 as the global COVID-19 pandemic unfolded. George Gao, director-general, Chinese Center for Disease Control and Prevention,23 predicted:24
“By and long, we have more cases in China and also death cases reported. And also, my staff told me that before there’s misinformation and there’s some belief. People believe, ‘This is a manmade … some pharmaceutical company made the virus,’ so there’s some violations of human … That is because of this misinformation.”
Others agreed with the need for social media censorship as it may pertain to the spread of “disinformation” about the pandemic or vaccines and vaccine injury, without regard to the source. The idea was to remove any information that did not align with the government’s mandates and ideas. Kevin McAleese, who is a communications officer with a Gates-funded agricultural project, said:25
“To me, it is clear countries need to make strong efforts to manage both mis- and disinformation … If the solution means controlling and reducing access to information, I think it’s the right choice.”
During the ensuing conversation, Tom Inglesby, director of the Johns Hopkins Center for Health Security,26 replied, “In this case, do you think governments are at the point where they need to require social media companies to operate in a certain way?”27
At each step of the simulation, the global “experts” agreed that information censorship through media platforms would be necessary to control the flow of the “right information” in order for people to willingly follow the leader.
What is interesting about the transcript from Event 201 is that what was planned and shared was frighteningly close to what has happened since January 2020. It may have been a coincidence to predict one or two major public health decisions, but it appears that the group was either phenomenally prophetic or they shaped the decisions and events of 2020 from behind the scenes.
Framing the Vaccine Message to Trigger Action
From the outside, the driving force behind economically devastating lockdowns, warp speed vaccine development and population control and surveillance strategies has been to “flatten the curve” and lower the death rate of SARS-CoV-2. Yet, as I and others have exposed, when these strategies are analyzed, it’s apparent there is more than what meets the eye.
In July 2020, Yale University28 announced a study of the trigger words and phrases that would have a higher likelihood of promoting an otherwise individualistic society to quietly follow mandates (not laws) to control behavior. The phrases tested were believed to be most successful at conveying feelings about health, helping others and fear.
The hope was to manipulate behavior in such a way that it lowered the governmental risk for riots and dissidence. The study was conducted by Yale University using 4,000 participants who were randomized to receive one of 12 different messages. After the message, they were then evaluated to “compare the reported willingness to get a COVID-19 vaccine at three and six months of it becoming available.”29
The primary outcome of the study was to find the right combination of phrases and messaging that would increase the number of people who got the vaccine. The study began July 3, 2020, and the last participant underwent testing by July 8, 2020.30 To date, the results of the study have not been published.
The president of the U.S. announced in July 2020 that there would be an “overwhelming” vaccine campaign launched by November 2020.31 In December 2020, the National Institutes of Health released a COVID-19 vaccination communication recommending behavioral and social science actions that might address vaccine hesitancy and increase the number who take the vaccine, including:32
Framing accepting a vaccine as a social norm including “promotional materials that induced peer pressure to vaccinate.”
Encouraging those who vaccinate to share their positive experience on social media.
Nudging a person into accepting the vaccine by making it convenient and easy, leveraging electronic portals to send messages and using competition, gamification and incentives to encourage behavioral changes.
Assessing the values of the target audience and then embedding those values into messages about vaccinations. Examples might include being a protector of the community, building on desires to go back to normal activities or as a way of enacting equality and social justice by protecting vulnerable people.
In other words, many of the messages that you’ve been seeing in the media and your doctor’s office have been designed to trigger emotions that would lead you to take the vaccine. These same pressure tactics are not routinely used in the media for some of the more common adult vaccinations including pneumococcal, tetanus, hepatitis or shingles vaccines.
It’s Time to Speak With One Voice and Fight for Freedom
As I’ve written before, what we lose as a society when we acquiesce to these mandates and controls will be exponentially harder to get back. One of the freedoms we give away is allowing our thoughts and beliefs to be censored on social media without fighting back.
It is essential to safeguard your constitutional rights and civil liberties against unlawful overreach, and yet many appear to be willing to give up easily. Although the government has a duty to protect the health and welfare of its citizens, this must be balanced against the loss of civil rights and liberties.
We’re currently facing a battle of freedom versus tyranny. For example, multiple studies have demonstrated that long-term lockdowns are clearly not in the public’s best interest.33,34 Instead, it’s tantamount to abuse. And yet many have gone along with these mandates, which were not laws.
It’s vital to understand that the vast majority of information you consume in mainstream media is carefully designed propaganda that has been crafted from nearly two decades of personal data collected from you.
Although Yale University undertook a study with 4,000 participants for a COVID-19 messaging campaign, that data had been gathered and collated through your use of social media.
As I have carefully identified in many previous articles, this plan will result in a progressive loss of your freedom and liberty that eventually results in tyranny and slavery. It is crucial to be vigilant and seek the truth so that you can understand how to distinguish between fact and a fictional narrative that promises you liberation but eventually enslaves you.
My newest book, “The Truth About COVID-19,” will be available April 29, 2021, on Amazon. In it, I investigate the origins of the virus and how the elite has used it to slowly erode your personal liberty and freedom. In addition, I’ll also show you how to protect yourself against the disease and what you can do to fight back against the technocratic overlords.
The country of Nicaragua never instituted a lockdown, never required masks, and yet crushed the Corona virus? Major protests in Germany, Switzerland, and the UK as people are saying ‘no’ to more lockdowns.
—————-
Support Truth in Media by visiting our sponsors:
Pulse Cellular: Use code “TRUTH” for 10% every plan for life. https://truthinmedia.com/phone
WHO updated “Therapeutics and COVID-19” on March 31, 2021 to include a recommendation on ivermectin. The recommendation was:
“We recommend not to use ivermectin in patients with COVID-19 except in the context of a clinical trial.”
The recommendation was made by the Guideline Development Group; 63 members consisting of “content experts, clinicians, patients, ethicists and methodologists”.
WHO explained that a vote on the recommendation was not necessary:
“While a priori voting rules informed procedures if the panel failed to reach consensus, these procedures proved unnecessary for this recommendation.”
Two questions:
Was there an “a priori” system in place for deciding when and how to abandon the “a priori” voting rules?
How was consensus determined?
Is it too late to take a vote?
WHO explained how they reached their “transparent and trustworthy recommendations”. They need to understand that bypassing a vote on the recommendation is the opposite of transparent and trustworthy.
According to the latest figures derived from the European Medicines Agency’s database of Covid-19 vaccine adverse reactions, 162,610 injurious events and 3,964 deaths have now been reported. Among the three major vaccines approved and deployed in Europe, Pfizer-Biontech’s vaccine accounts for over two-thirds of reported injuries and mortalities, or 102,100 and 2,540 events respectively. Curiously, women disproportionately account for 77% of adverse events; this greater than 1:4 gender ratio is also being observed for Moderna’s and AstraZeneca’s vaccines. So far there seems to be no scientific explanation to account for this gender disparity.
Recently, we have been alerted that AZ’s adenovirus vaccine is particularly worrisome. It has been less than two months since its administration in the EU commenced; already there have been over 54,000 injuries and 451 deaths registered. Consequently, many European nations, which are more committed to protecting their citizens than increasing pharmaceutical profits, have placed moratoriums on administering AZ’s Covid vaccine. In the UK, over 114,000 adverse reactions from AZ’s product or 4.6 reactions per 1,000 recipients have been reported.
However, the EU’s vaccine injury statistics are disturbing for another reason. It seems very apparent in our review of government and institutional figures that the EU has a far more robust and accurate vaccine injury reporting system in place. Given that the US started vaccinating adults against SARS-CoV-2 before the EU, we would expect to observe the number of reported adverse effects higher or at least proportionate. However, this is not the case. Since December 14, 2020, the CDC’s Vaccine Adverse Event Reporting System (VAERS) has only reported 44,606 adverse events and 2,050 deaths – a small fraction compared to Europe and where the average European citizen is generally healthier and where far fewer doses have been administered.
Consider two other anomalies. According to Oxford University’s global Covid-19 vaccine tracker, as of March 27th, the US has administered over 136 million doses, which accounts for about 25 percent of all Covid-19 vaccines administered worldwide. On the other hand, the EU nations have only administered 66 million doses — less than a half compared to the US. In addition, the US vaccination rate is now approximately 41 per 100 Americans. EU nations have individually vaccinated 17 per 100 citizens or less. Therefore, why is there such an enormous discrepancy of adverse vaccine reactions between the US and EU? The EU is reporting a 0.2 percent adverse reaction rate whereas the US is claiming only 0.03 percent, almost a ten-fold difference.
Various studies have estimated that only between 1 to 10 percent of vaccine injuries are reported in VAERS. In the past, the CDC has relied upon the conservative 10 percent estimate, which may account for the ten-fold discrepancy in adverse Covid-19 vaccine events in the EU and US. A 2011 Harvard study in collaboration with the Federal Agency for Health Care Research has estimated actual adverse event reporting may be as low as 1 percent. The study states,
“Adverse events from drugs and vaccines are common, but underreported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.”
If we assume the European Medicines Agency’s statistics are relatively accurate, we would therefore expect that the actual number of US adverse reactions should be in the neighborhood of 335,000 injuries and over 8,100 deaths.
Something is very seriously amiss with this scenario.
First, we can surely agree that Covid vaccines do not hold a personal vendetta against Europeans. Nor does owning an EU passport make one more susceptible to a serious vaccine reaction.
Although anyone can report an adverse reaction to VAERS, very few Americans know it exists. The CDC notes that reporting vaccine injuries and deaths in the database is completely voluntary. Consequently, there is no requirement for a vaccine administering physician or health professional to report an injury or death. In fact, many doctors and healthcare workers are largely ignorant about VAERS’ existence as is the public. Because VAERS is an extremely flawed passive surveillance system, it provides an extremely inaccurate picture for risks associated with every approved vaccine, let alone those against the SARS-CoV-2 virus. The CDC’s National Immunization Program has acknowledged VAERS’ glaring limitations for over 25 years, but nothing has fundamentally changed in mandating its use throughout the medical establishment. As millions of Americans are rushing to get their shots, our health officials have been relying upon “a patchwork of existing programs that they acknowledge are inadequate because of small sample size, missing critical data or other problems.” Anthony Fauci and the heads of our health agencies have known for many months that these vaccines were forthcoming. However they have been utterly negligent, according to a New York Times article, to put in place a robust monitoring system to record adverse vaccine reactions and to undertake appropriate analysis.
VAERS has served as a highly successful propaganda tool to mask and hide actual vaccine risks instead of a reliable monitoring system. Anyone can access the database, and it is the most common resource for those who follow and report adverse vaccine reaction trends.
Yet, the CDC also relies upon other monitoring sources, notably the Vaccine Safety Datalink (VSD), a database controlled in a collaboration between the CDC and nine large managed healthcare organizations. In fact, the CDC states that it relies upon VSD “to evaluate vaccine safety issues.” The Institute of Medicine ranks VSD as the best resource for conducting necessary analysis on vaccine safety and contains the electronic records of over 9 million Americans. It is also relied upon for comparing the health status of vaccinated versus unvaccinated groups and for investigating long-term adverse vaccine risks. However, despite our tax dollars going towards the funding of VSD, the database’s content is inaccessible to the public. Federal agencies have assured that its data remain the proprietary property of the private healthcare organizations to prevent it being used by independent researchers and journalists.
Given the CDC’s and FDA’s long history of secrecy and lack of transparency, and its long public relations arm that infiltrates every mainstream media source, it is not surprising that we never hear public service announcements notifying viewers and readership that the CDC has a system in place to report any adverse effects from Covid-vaccination. Now that the vaccines are being rolled en masse, we would expect our government to enforce due diligence to track vaccine injuries in the public interest. But we will never hear this information coming from the lips of the pharmaceutical media shills such as Sanjay Gupta and George Stephanopoulos. Not even during flu seasons when the media follows its marching orders from federal health agencies to persuade the public to roll up their sleeves.
In the meantime, the medical establishment gives lukewarm condolences towards those unfortunate to have become seriously ill or have died from the virus. But think of all the others, Fauci and his federal colleagues consistently tell us over the media waves, who have been lucky enough to be vaccinated and can return to a normal life. Just take these experimental vaccines despite the shoddy evidence to convince any objective reviewer that they prevent transmission or protect anyone from contracting the virus. Nor were they tested to determine rates of hospitalization or deaths. Yet the media makes every effort to assure us that we are being given the best information science can provide. And sadly, all this science is preferentially cherry picked to strengthen the false narrative to increase vaccination compliance. And since lockdowns, masks, social distancing and quarantining remain in place, it is near impossible to conduct any vigorous scientific study to determine how much or how little these vaccines are contributing to the rise and fall of infectious rates. Is it vaccination or all of the mandatory social restrictions that is the major contributing factor?
“The greatest enemy of knowledge,” wrote renowned historian Daniel Boorstein, “is not ignorance, it is the illusion of knowledge.” Today, this illusion of authoritative knowledge pervades the medical establishment and brainwashes the sleeping media. In our opinion, it is becoming a dangerous collective mental disorder. The good news is that more and more scientists, researchers and doctors within the towering medical citadel are exiting rapidly in order to publicly speak out against the litany of falsehoods, lies and corruption spewed from the orifices of the CDC, the FDA, World Health Organization and Big Pharma.
Gary Null is an internationally recognized thought leader and activist who holds a Ph.D. in human nutrition and public health science and Richard Gall is the Executive Producer for the Progressive Radio Network.
Disclaimer: This article is not intended to provide medical advice, diagnosis or treatment.
“Wow. But don’t those cost a fortune? How can you afford them, with just the Universal Basic Income?”
“Well, duh. I didn’t buy them, dude. I’m just renting them from Amazon Prime, of course. All of my clothes are rented, including the original Calvin Klein underwear.”
“Nothing, just remembering an old joke here. So, what’s new? What are your plans for next week?”
“Not sure. Maybe I’ll go to the City Hall Yearly Masked Ball. You want to come? The masks are all N95 compliant, so it’s safe.”
“No, thanks. I thought you were travelling to Italy for the holidays?”
“Nah, I can’t board a plane this month. I didn’t get my Moderna monthly booster shots. I wanted to, but the lines were so big, the next appointment available for me is only next month.”
“This Covid-29 is really pesky, isn’t it?”
“You bet. But I’m sure the vaccine is working. Just give it time. It takes a few years to achieve full immunization, but of course, with the new variants and viruses that appear every month, it’s always a game of catching up. We got to be patient. So, yeah, no travel this month for me.”
“Well, you know, you could always travel around your own room.”
“What?”
“Oh. I just got reminded of an old 18th century novel. ‘Voyage around my room,’ by Xavier de Maistre.”
“What it’s about?”
“It’s about a guy who, well, travels around his room.”
“18th century? Man, that’s like, old. When was that exactly? I guess that’s when the first lockdowns happened, right? In the first Covid era?”
“Yeah, sort of… Anyway, forget it, you just reminded me of that book. But I guess reading is not really your thing.”
“Nah. Is there a YouTube version? You are funny, you’re one of those guys who still read, right? You’re really old-fashioned. I bet you don’t even have a microchip in your brain, L.O.L.”
“Thankfully not…”
“…”
“What’s wrong?”
“Don’t get close to me.”
“What? Why? Who are you calling?”
“Who am I calling? Who am I calling? The police, dude. Not having a brain chip is a felony, and it’s my duty as a citizen to report you, sorry. I know you’re a friend and neighbour and all, but, that’s just sick, dude. That’s really fucked-up.”
“No, No… Wait, stop! I meant that I don’t have the latest version of he chip. But I still have the 2029 model. As you said, I’m old-fashioned…”
“Ah… Ok… But… I don’t see the scar in your head…”
“Oh, it’s there, trust me. It’s just that I got a hair implant on top of it, so, it’s not visible.”
“Ah, OK. That’s cool. You were starting to scare me, dude. I mean, not having a brain chip, in this day and age… I was starting to think you were a radical or something…”
“Well…”
“Oh man, it’s getting late. It was nice seeing you, but, sorry, I got to go now. I have a Zoom meeting with my family. But, see you another time, I guess. Should we do an elbow bump, or a foot shake?”
“…”
“What’s up dude? What’s wrong with you?”
“Nothing, you know, memories. I’m kind of old now, and sometimes I get flashes of images from previous times. And now I was thinking of an old movie I saw once, long ago…“The Flowers of Saint Francis”, it was called. By Roberto Rossellini, about Saint Francis of Assisi. There is one scene in which a leper comes, ringing a bell… You know, at that time, in the Middle Ages, lepers were forced to wear bells on their clothes to announce their arrival… And so this leper comes, his little bell ringing, asking for some money, but all people move away from him, and he’s there all alone, looking so forlorn. So Saint Francis sees this, and he is so overcome with pity, that he approaches the leper and hugs him. A long hug, for several minutes. And when the poor leper goes away, he starts to cry.”
“Eew… That’s sick, man. I mean, hugging someone. That’s just gross! What’s a leper?”
“Oh… it’s a… Leprosy was a disease that existed a long time ago. I mean, it still exists, but it was more common then.”
“Oh. I guess mRNA vaccines cured it, right? Man, viruses are evil. But thankfully we have those magic vaccines today.”
“Sort of. It’s not really caused by a virus, and the treatment is not a vaccine. But anyway, I was just reminded of that scene, I don’t know why…”
“OK. So, elbow bump or foot shake, then?”
“Honestly, I prefer neither.”
“Sure, that’s the safest way. See you around then, man. And get that 2030 brain chip, bro, for Satan’s sake. I mean, we’re in 2030, dude. We are not in the Middle Ages anymore.”
New research suggests that four billion people globally will be overweight in 2050. This trend can be traced back to the ‘low-fat, high-carb’ guidelines first issued in the 70s, and should prompt a major U-turn on dietary advice.
A recent report from the Potsdam Institute predicts that by 2050 there will be four billion overweight people in the world, with one-and-a-half billion of them obese. This is not entirely surprising. The world has been getting fatter for years, and things do not seem to be slowing down.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.