According to the UK Government, as of 27 March 2021, 126,515 people have died as a result of contracting Covid-19, and an additional 21,610 people have died with COVID-19 on their death certificates.
The government alleges, therefore, that a total of 148,125 people in the UK have died as a result of COVID-19. As we shall see, this claim is not credible.
Justifiable Policy?
Claims about mortality have been used by both the government and the mainstream media to justify the policy response.
The pace of change driven by that policy response has been astonishing. With Health Secretary Matt Hancock’s recent announcement of the creation of the UK Health Security Agency and its commitment to take “action to mitigate infectious diseases and other hazards to health before they materialise,” it is clear the government’s new (ab)normal is here to stay.
There is clearly an agenda; one entirely founded upon the idea that COVID-19 presents a significant threat. The primary evidence offered to substantiate this claim is suggested COVID-19 mortality.
Age Standardised Mortality
Just like nearly every other mortality cause, COVID-19 risks increase proportionately with age. Statistics for those of working age show a population mortality risk of between 0.0166% and 0.0046%, depending upon who you believe. The COVID-19 risk to the working age population is statistically insignificant. For the under 18’s it is statistically zero.
Mortality risk disproportionately impacts men. In 2018 the average age of death for men was approximately 80, and 83 for women in England and Wales.
The average age of COVID-19 death is just over 82. When we look at standard mortality distribution, there is no observable impact from COVID-19.
UK all cause mortality doesn’t suggest any need to panic either.
The ONS released data estimating a total of 607,173 deaths from all causes in England and Wales for 2020. Given demographic changes over time, the ONS use Age Standardised Mortality Rates (ASMR’s) to calculate relative death rates. The ASMR showed that 2020 was the worst year for mortality in the last decade.
ASMR’s were in continual decline throughout the post war period. That decline stopped abruptly in 2009 as the economic impact of the global financial crisis took its toll on public health. Thereafter it showed a marginal rise to 2019. Mortality in 2020 and 2021 should be seen in the context of a global financial crisis that dwarfs the credit crunch of 2008.
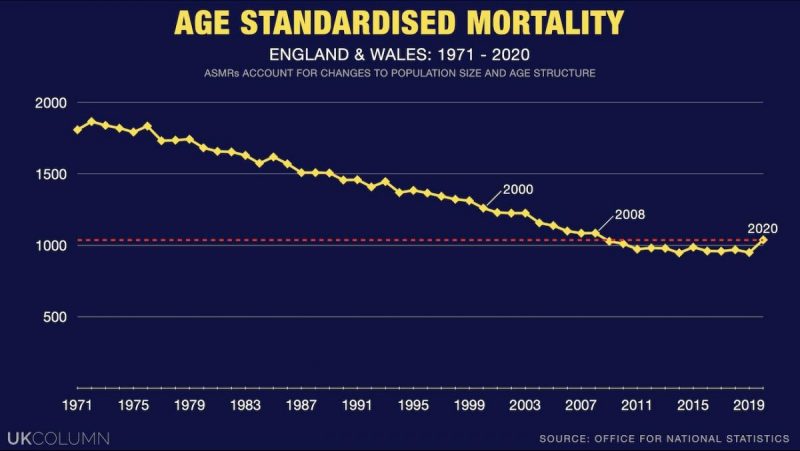
ASMR’s fluctuate annually and 2020 showed a significant increase above the 5 year average mortality rate. This was higher than most rises but by no means “unprecedented.” ASMR’s in England since 1938 show similar increases in 1947, 1949, 1951, 1958, 1963, 1970, 1972, 1976, 1985, 1993 and 2014.
Most of these spikes in ASMR’s were in the region of 35 to 45 points. For example, in 2014 the ASMR rose by 40.2, in 1993 by 38.4 and in 1985 by 46.3 points. It rose by 90.5 in 1947, by 83.5 in 1963, it went up by 104.9 in 1970 and in 1951 by 216.3. So the 2020 rise of 118.5 is by no means the worst.
The death toll in 1951 was attributed to the the influenza epidemic which struck some parts of the UK (most notably Liverpool) but left others relatively unscathed. To this day science has struggled to account for this.
2020 not only didn’t have the highest mortality rate in the post war period, it didn’t have the highest mortality rate in the 21st century either. 2020 ranked 9th, out of 20 consecutive years, for all cause mortality in England and Wales. It was the 11th least dangerous year in the last 50.
While there is no statistical evidence of an unprecedented global pandemic in England and Wales (nor in Scotland and Northern Ireland) this tells us little about how many deaths were genuinely attributable to COVID-19. Nor does it indicate at which point we should sacrifice our rights, freedoms, children’s educations and economy in the service of public health.
We certainly didn’t sacrifice them in 1947, 1963, 1970, nor even in 1951. Why was 2020 different?
PCR Does Not Mean COVID
For the purposes of this analysis, we will use the government’s higher claim of 148,000 deaths. The vast majority of these deaths were attributed based upon a positive RT-PCR test. The UK Coronavirus Act makes a clear distinction between the virus and the disease. It states:
Coronavirus means severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); coronavirus disease means COVID-19 (the official designation of the disease which can be caused by coronavirus).
SARS-CoV-2 and COVID-19 are not the same thing. The detected presence of SARS-CoV-2 does not mean the person has or will develop COVID-19.
Therefore the attribution of mortality based solely upon a positive test result in no way proves the person died of COVID-19. The extent to which the disease caused or contributed towards a death is a precise medical assessment. The UK government created a death certification and registration process where this did not occur in an unknown number of cases. We need to know what that number is.
COVID-19 has a distinct presentation that requires careful diagnosis. The unique symptoms are severe hypoxemia (low blood oxygen levels), hypercapnia (elevated blood Co2 saturation) and unusually no corresponding loss of respiratory system compliance.
Measurement of gaseous exchange and fluid retention in the lungs appears normal, meanwhile the patient, in serious cases, struggles to breath. This is unlike other influenza like illnesses (ILI’s).
Yet the NHS describe a list of COVID-19 symptoms that could be attributable to any ILI. A high temperature, continuous cough and loss of taste and smell are associated with many. While this is public information, intended to guide our decision to seek medical advice or a test, the list of possible causes expands further given that the NHS state just one of these symptoms possibly indicates COVID-19.
Without precise symptomatic diagnosis, it is difficult to distinguish COVID-19 from a range of other respiratory illnesses. A study from the University of Toronto found:
The symptoms can vary, with some patients remaining asymptomatic, while others present with fever, cough, fatigue, and a host of other symptoms. The symptoms may be similar to patients with influenza or the common cold.
A Cochran Review meta analysis of available studies looked for a clear definition of COVID-19 symptoms. Published in June 2020, the reviewers noted:
The individual signs and symptoms included in this review appear to have very poor diagnostic properties … Based on currently available data, neither absence nor presence of signs or symptoms are accurate enough to rule in or rule out disease.
Even using advanced diagnostics, such as a computer tomography (CT) scan, won’t always provide a clear result. A study attempting to improve differential diagnosis using CT scans found:
Although typical and atypical CT image findings of COVID-19 are reported in current studies, the CT image features of COVID-19 overlap with those of viral pneumonia and other respiratory diseases. Hence, it is difficult to make an exclusive diagnosis.
Regardless of their SARS-CoV-2 test status, without a very accurate diagnosis of symptoms, suspected COVID-19 patients could be suffering from one among a range of ILI’s. Again, a positive test result does not mean the patient died from COVID-19, even if they had corresponding symptoms.
Notifications of Infectious Diseases
In England and Wales it is a legal requirement for all registered medical practitioners to notify their local health authority of any suspected cases of notifiable diseases. The list of Notifiable Infectious Diseases (NOIDS) includes COVID-19. This is not optional.
All diagnosing doctors must complete a NOIDS report upon making a diagnosis. Testing laboratories are also required to notify Public Health England (PHE) of positive tests for notifiable diseases.
According to the fact checker FullFact there were 18,152 COVID-19 notifications made by doctors in the whole of 2020.
Yet the government claim that there were 70,853 COVID-19 deaths, never mind cases, in England and Wales in the same year.
Fullfact offered an explanation for this apparent huge discrepancy:
People with Covid symptoms are advised to get a test, but not to visit their doctor, which may be part of the reason why doctors reported so few cases of the disease through NOIDS. Since Covid became widespread in the UK, and began to be monitored in other ways, it is also possible that doctors felt there was little need to continue notifying PHE about each case.
This is not credible. While it is true that people were told not to go to a doctor if they suspected they had COVID-19, a diagnosis by a doctor was still necessary at some point. Self diagnosis doesn’t usually afford access to hospital treatment. The suggestion by FullFact that doctors unilaterally decided not to bother with their statutory obligations is ridiculous.
What this massive difference between claimed cases, subsequent COVID-19 mortality and NOIDS indicates, is that Doctors were largely reliant upon laboratory testing to fulfil the duty to notify the authorities. This adds considerable weight to the notion that laboratory testing was the leading determinant in the overwhelming majority of COVID-19 diagnosis.
Until mid August 2020, a UK COVID-19 death was reported if the decedent had tested positive at any point during the preceding months. An individual may have have tested positive for SARS-CoV-2 in March, have died of cancer in August and subsequently have been recorded as a COVID-19 statistic.
The scientific rationale for this did not exist. Research conducted by scientists at Oxford University analysed the COVID-19 Hospitalisation in England Surveillance System (CHESS) and calculated the average time between infection (positive test) and mortality to be 26.8 days.
And so, in response to public and scientific pressure this approach changed to only recording a COVID-19 death within 28 days of a positive test. Still the UK government would not let go of its inflated number system, adding nothing but statistical confusion, they announced:
In England, a new weekly set of figures will also be published, showing the number of deaths that occur within 60 days of a positive test. Deaths that occur after 60 days will also be added to this figure if COVID-19 appears on the death certificate.
The August methodological change reduced claimed COVID-19 deaths by 5,377 in England alone. This didn’t make any difference to the number of people who had died from COVID-19, it just changed the number of people who had reportedly died from COVID-19.
This wasn’t the only notable change to the data gathering process. Just before the significant spring spike in mortality, on the 30th March 2020, the MSM reported that the government had instructed the ONS to change the way they record COVID-19 deaths. Hitherto the ONS only reported a COVID-19 death if it was recorded as the direct or underlying cause. This was changed to recording “mentions” of COVID-19. A spokesperson for the ONS said:
It will be based on mentions of Covid-19 on death certificates. It will include suspected cases of Covid-19 where someone has not been tested positive for Covid-19.
The reporting of COVID-19 comorbidity rates was“paused” in July and has yet to resume. The final published ONS analysis that directly reported the number of pre-exiting conditions for deaths “with” COVID-19 mentioned on the death certificate, was released for the period ending 30 June 2020.
From this we learned that 91.1% of alleged COVID deaths had at least 1 serious additional comorbidity. The mean number of comorbidities for a those under 70 was 2.1 and for the vast majority over 70 it was 2.3.
It is preposterous to claim that a decedent who had cancer, pneumonia and had just had surgery, but tested positive for SARS-CoV-2 four weeks earlier, could reasonably be categorised as a COVID-19 death. Yet that is precisely what happened, and continues to happen to this day.
Covid-19 Cures the Flu
COVID-19 also cured influenza and other respiratory disease, such as adenovirus. Early January is always a period of notable influenza outbreaks, resultant hospital admissions and mortality. This is evident if we look at PHE’s Weekly Influenza Report for week 2 in any year prior to 2020.
In 2020, according to the newly combined PHE Weekly Influenza and COVID Report, there have been virtually no cases of influenza, treatment or related deaths.
The ONS note all the details on a death certificate. In their mortality roundup for the January to August 2020 period they stated:
Influenza and pneumonia was mentioned on more death certificates than COVID-19, however COVID-19 was the underlying cause of death in over three times as many deaths between January and August 2020.
How can flu and pneumonia possibly be on more death certificates than COVID-19 if, as the media and PHE allege, it has been wiped out? It seems the medical profession didn’t get the memo.
A Systemic Catch-22
A positive SARS-CoV-2 test appears to be the primary reason for attribution of mortality. Only the most fastidious diagnosis can differentiate between COVID-19 symptoms and other ILI’s. Is it credible to believe that flu and pneumonia are on more death certificates but that COVID-19 is deemed the cause of death on three times as many Medical Certificates of Cause of Death (MCCD’s)?
These are somewhat rhetorical questions. The reason why bizarre anomalies like this occurred is because recording COVID-19 as the cause of death was practically unavoidable.
The Coronavirus Act overhauled the MCCD and death registration processes. In addition, World Health Organisation Coding changes and guidance issued by the NHS and other medical authorities combined to create a systemic Catch-22.
In England and Wales an MCCD is completed online using the WHO’s recommended coding. The MCCD is split into sections. Part 1. a) “Disease or condition directly leading to death”; b) “Other disease or condition, if any, leading to (a)”; and c) “Other disease or condition, if any, leading to (b)”.
Part 2 records “Other significant conditions contributing to the death, but not related to the disease or condition causing it.” For example, a person may have died from heart failure caused by pneumonia but obesity, though not directly related to the immediate cause of death, could have contributed and would therefore be recorded in Part 2.
In the case of respiratory disease, the direct cause of death could be Acute Respiratory Distress Syndrome (ARDS). This may be brought on by, for example, pneumonia which was caused by influenza. In this instance the direct cause of death would be recorded in Part 1. a) as ARDS, prompted by pneumonia in Part1. b), and the underlying cause would be set as influenza in Part 1. c).
The WHO Family of International Classifications (WHOFIC) Network Classification and Statistics Advisory Committee (CSAC) created new International Classification of Diseases codes (ICD-10 codes) for COVID-19. If the decedent had tested positive, or had been in contact with anyone else who had, a recorded COVID-19 death was practically a fait accompli.
A “confirmed case” was dependent solely upon a positive test result and was given the code U07.1. Observable symptoms were not necessary for U07.1 code to be recorded on a death certificate.
A suspected COVID-19 case was coded as U07.2. A decedent known to have had contact with a SARS-CoV-2 positive person who, while neither testing positive nor having any symptoms themselves, was deemed a suspected/probable COVID-19 case and given the code U07.2.
Neither the U07.1 nor the U07.2 codes required any evidence that the decedent had COVID-19.
As the U07.1 code indicated a “confirmed case,” unless the decedent passed away from something obviously unrelated, such as head trauma, a SARS-CoV-2 positive test would almost automatically confirm COVID-19 as the underlying cause of death.
The WHO clearly described this process in their International MCCD coding guidelines. They defined what death “due” to COVID-19 was:
A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death. A death due to COVID-19 may not be attributed to another disease (e.g. cancer).
A clinically compatible illness could be any ILI. Even if the individual died from cancer, as long as they tested positive for SARS-CoV-2, or the Doctor suspected respiratory distress, the death would be registered as “due to” COVID-19. COVID-19 would again be the reported as the underlying cause.
Additional WHO guidance stated:
COVID-19 should be recorded on the medical certificate of cause of death for ALL decedents where the disease caused, or is assumed to have caused, or contributed to death. Although both categories, U07.1 … and U07.2 … are suitable for cause of death coding … it is recommended, for mortality purposes only, to code COVID-19 provisionally to U07.1 unless it is stated as probable or suspected.
If a doctor was uncertain and merely suspected a probable COVID-19 case, they were clearly advised to record it on the MCCD as a confirmed case (U07.1 and not U07.2). Again, ensuring it would be reported as the “underlying cause.”
The Office of National Statistics stated:
Deaths involving the coronavirus (COVID-19) include those with an underlying cause, or any mention, of U07.1 (COVID-19, virus identified) or U07.2 (COVID-19, virus not identified) …
If the Doctor held firm and coded COVID-19 as U07.2 on Part 2 of the MCCD, the ONS (and the NRS and NISA) would still report it as a COVID-19 death.
In the Clear
The Coronavirus Act indemnified all NHS doctors against any claims of malpractice or negligence. It removed the need for a second medical opinion (Medical Examiner), it effectively ruled out both post-mortem examinations and jury-led coroner’s inquests, allowed virtually anyone to act as the qualified informant and facilitated rapid cremation.
In response to the Coronavirus Act and WHO IC10 coding, the NHS issued guidance to doctors for the completion of the Medical Certificate of Cause of Death (MCCD). The COVID-19 death certification and registration process they produced beggars belief. Under the guidance, acting on their own without any corroborating opinion:
Any medical practitioner with GMC registration can sign the MCCD, even if they did not attend the deceased during their last illness.
Attend doesn’t mean examine either. Checking in with the decedent via Zoom is sufficient. Failing that, if the MCCD signing doctor has only seen the decedent after death, providing they have tested positive, a review of their notes is still sufficient to record a COVID-19 death. The NHS stated COVID-19 could be recorded wherever:
A medical practitioner has attended the deceased (including visual/video consultation) within 28 days before death, or viewed the body in person after death.
In keeping with the WHO coding guidelines, there isn’t even any need for a positive test result. The NHS guidance added:
If before death the patient had symptoms typical of COVID-19 infection, but the test result has not been received, it would be satisfactory to give ‘COVID-19’ as the cause of death … In the circumstances of there being no swab, it is satisfactory to apply clinical judgement.
The NHS then created a system of remote death certification:
During periods of excess deaths due to COVID-19, healthcare providers are encouraged to redeploy medical practitioners whose role does not usually include direct patient care, such as some medical examiners, to provide indirect support by working as dedicated certifiers, completing MCCDs.
These dedicated certifiers, though medically qualified, are tasked with signing off COVID-19 MCCD’s. GP’s and hospital physicians gather reports, perhaps from a review of the deceased’s medical notes or a video conference with a care home provider, and pass that information to the dedicated COVID-19 certifier for MCCD completion.
The NHS advised that no proof was required for the attribution of a COVID-19 death. They stated:
Without diagnostic proof, if appropriate and to avoid delay, medical practitioners can circle ‘2’ in the MCCD (information from post-mortem may be available later)
This suggestion that a post mortem may be available is implausible.
Additional guidance issued by the Royal College of Pathologists states:
If a death is believed to be due to confirmed COVID-19 infection, there is unlikely to be any need for a post-mortem examination to be conducted and the Medical Certificate of Cause of Death should be issued.
Bearing in mind that the WHO had instructed suspected U07.2 deaths to be coded as confirmed U07.1 deaths, the chance of anything other than confirmed COVID-19 death reaching a pathologist is extremely remote. Any MCCD signed “without diagnostic proof” would almost certainly be agreed by the pathologist without further scrutiny. The mere act of putting COVID-19 anywhere on the MCCD was enough to negate the need for a post mortem.
This new death certification system, specifically designed for COVID-19, has understandably caused confusion. The British Medical Association’s verification of death guidance advises that if no signing doctor has seen the decedent prior to completing the MCCD they should refer it to the coroner. However, this was only a policy recommendation not a legal requirement.
Contradicting this, the Chief Coroner advised:
COVID-19 is a naturally occurring disease and therefore is capable of being a natural cause of death … The aim of the system should be that every death from COVID-19 which does not in law require referral to the coroner should be dealt with via the MCCD process.
This means that even if a coroner receives a referral from a doctor, they will be highly likely to automatically approve the MCCD without further inquiry. Since a post mortem has already effectively been ruled out, there will be little point in the coroner investigating further.
NHS staff and carers who may have been uncomfortable with all this have been under no illusions. The use of draconian Hospital Trust gagging orders (non disclosure agreements) are widely reported. Carers who have spoken out have been sacked.
To finalise this unbelievable COVID-19 death registration system, the Coronavirus Act also withdrew the standard second opinion required prior to cremation. The need to complete Cremation form 5 was suspended for all COVID-19 deaths.
Alleged COVID-19 decedents can be cremated without any clear evidence that they ever had the disease, regardless of their family’s wishes, swiftly ending any chance of any investigation by sceptical family members.
What was the Cause of Death?
SAGE assessed the UK mean operational false positive rate (FPR) for RT-PCR to be 2.3% of all conducted tests. The government say they have conducted just over 118M tests of which 4.3M were positive. This includes an unknown number of multiple tests of the same individual. A mean FPR of 2.3% suggests 2.7M of those 4.3M positive tests were false positives. This equates to 62.7% of all positive test results.
As we have already discussed it is highly likely that laboratory testing was the primary determinant for a diagnosis of COVID-19. Therefore it is not unreasonable to surmise that at least 50% of claimed COVID-19 deaths were attributed on the basis of false positives. We can halve the claimed 148,000 to 74,000 COVID-19 deaths.
The 2020 ONS mortality data for England showed a reduction in deaths from a number of other causes.
Deaths from Ischaemic heart diseases were 1,450 below the 5 year average. Cerebrovascular disease was down by 2,276, malignant respiratory neoplasm by 1,537, chronic lower respiratory disease by 2,764 and influenza and pneumonia deaths were 7,313 below the 5 year average. An apparent reduction of 15,340 deaths from other causes.
It seems highly likely that these deaths were wrongly recorded as COVID-19.
As we have seen above, approximately 90% of supposed COVID-19 decedents had at least one other comorbidity. Using the Government’s 148,125 figure, we might claim, therefore that only something like 15,000 of these died of, rather than with.
Is this claim justifiable? Well, consider this:
The Department of Health and Social Care published a study of residents in care homes which purported to show the total number of confirmed cases. Among this number they claimed:
80.9% of residents who tested positive were asymptomatic.
A meta analysis by the Oxford Centre for Evidence Based Medicine found that asymptomatic rates among those who tested positive varied between 5% – 80%. If there are no symptoms, then the disease cannot have contributed towards a death.
Taking everything into account, from high rates of comorbidity, to low rates of symptomatic individuals, the impact of false positives on testing and a death certification regime heavily biased towards recording COVID-19 as the underlying cause, then it is reasonable to conclude that the total number of deaths from Covid-19 is not 148,000, nor 126,000, but much closer to 15,000.
April 10, 2021
Posted by aletho |
Civil Liberties, Deception, Economics | Covid-19, Human rights, UK |
Leave a comment
IN THE early stages of the ongoing ‘war on terror’, which started twenty years ago, a nebulous conception of the enemy, non-existent victory conditions and the consistent dishonesty of warmongering politicians such as Blair led some to wonder if the threat of the global ‘Axis of Evil’ had been exaggerated to achieve some other set of goals.
Today, in similar circumstances of unanswered questions and ambiguous realities underpinned by systematic deception, reinforced by Boris Johnson on Monday as he launched the new phase of the psychological and economic war he is waging on the British people – vaccine passports (and after that?) – this question is being asked:
Is there a pandemic? Was there ever a pandemic?
Perhaps the most important point to grasp is that a pandemic is a construct, not an object. There is nothing you can point at which is the pandemic, only various data points indicating that one exists.
The World Health Organisation changed its definition in 2008 to exclude the criterion of ‘enormous numbers of deaths and illness’. In other words, the definition of a pandemic is ultimately a matter of interpretation. There is no data that currently supports the claim there is a pandemic in Britain at this moment, and whether any data ever did is doubtful..
The scientific process has happened in reverse. Starting in January last year, the existence of a deadly new pandemic, unlike anything previously confronted, was conjectured on the basis of terrifying rumours and unreliable reports from China, not scientifically established facts.
Once the existence of an extraordinary pandemic was assumed, extraordinary measures were justified to fight it, including the rapid deployment of highly unreliable PCR protocols developed by the Gates Foundation-funded Christian Drosten, shock propaganda messaging, a massive and drastic reduction in health care provision (which has functionally destroyed the NHS in order to ‘protect’ it) and de facto euthanasia policies in care homes, based on Neil Ferguson’s Gates Foundation-funded models.
Compromised administrative procedures recorded deaths as lives lost to the pandemic, providing further evidence for its existence.
As is now well known, an overwhelming majority of pandemic casualties also suffered from other conditions and the average age of victims tracks life expectancy in every country.
If the pandemic had not been assumed to exist, and the reckless and cynical interventions against it had not taken place, how would anyone know there was one?
Data clearly demonstrates that lockdowns and related policies were never necessary or effective. Experimental therapies have been deployed which are unreliable and potentially dangerous. Vaccination may or may not prevent contagion or transmission. The fact that governments and their paid experts are unable or unwilling to incorporate these matters into their thinking testifies either to their sinister intentions or the extent to which their mental processes have been corrupted.
Either they believe that some clandestine end justifies repressive and deceptive means, or else they are insane, or mindless through conformism: there is no other explanation.
Phenomenologically, the most important evidence for the existence of the pandemic is its external signifiers, especially face masks, this mass psychological theatre.
Here again, the conjecture of the pandemic itself justified the imposition of the mandate, and nothing else: no evidence supports the thesis that masks have any positive medical effect and the more plausible scenario is their medical effect is negative. Nonetheless the Gates Foundation-funded behavioural psychologists of Sage and their equivalents in other countries argued that mandating them was necessary (‘because most people still did not feel sufficiently threatened’).
The vague objective of an incomprehensible ambition, opposed against a nightmare, discloses a more concrete aim: control.
Why the authors of this initiative want control presents a complex question. Either they just want it without even knowing why, or they want it for another reason. Perhaps they have a broader plan which demands dramatically upgraded repression.
Either way, what they seem to desire is control over the bodies of their populations. In the idea of vaccine passports, what is being implemented is a political and legal climate in which experimental genetic therapies on human populations are normalised and inescapable. Armed with vaccine passports, global governments and their corporate allies would be able to establish the foundations of a global surveillance state, with the power to monitor every social interaction.
Vaccine passports are the gateway to the most radical slavery the world has ever seen. It now seems likely that creating a psychological and social climate in which to impose them was always the aim behind the engineered pandemic. The pandemic was needed to impose the vaccinations, and the vaccinations are needed to impose the passport.
This transformation of one part of the population into the vaccinated simultaneously invents the unvaccinated, a problem which could eventually be resolved through liquidation, but meanwhile offering opportunity for politically profitable stigmatisation. The vaccinated (via vaccine passports) are granted ‘privileges’ that the unvaccinated are denied in order to compel compliance.
Like accepting being forced to wear a government mandated gimp mask, for no reason whatsoever, a person accepting vaccination implicitly accepts the terms of the new normal. At the same time, vaccination is a ritual, substantiating membership in a psychological community.
Anyone who supposes the vaccine passport could lead to discrimination fails to grasp that this is the whole purpose of this document. The entire point is to divide society, to rule it. By creating checkpoints everywhere, power flows to the authority controlling access, in this case Johnson and his faction: a criminal cartel.
Accepting vaccination does not automatically imply a happy ending. The privilege to resume the semblance of a normal life (a ’new normal’ life) is linked to vaccination status now, but the reasoning behind this privilege is contingent on the existence of the non-vaccinated. Once non-vaxxers vanish, the reason for continuing to offer privileges is also gone. At this point a new status category can be introduced, and the same selective sequence played again. In this way, it would be possible progressively to eliminate a significant percentage of the population.
So far the theatre of the pandemic has been organised as a campaign of psychological manipulation with policies conceived to ‘nudge’ compliance by alternately dangling rewards (which are usually snatched away) and making threats. This campaign has also featured systematic censorship and intimidation directed against some of the most accomplished scientists in the world.
Although these tactics make a mockery of the principle of informed consent, they are of the ‘softer’ variety. Ultimately, more aggressive tactics will be deployed. The intensifying lawlessness of the police now points in this direction.
What can be done? The government is ruling via a threadbare fraud. When that disintegrates what will remain is force, but the real command authority of Johnson and his collaborators over the monopoly of violence that defines the British state has barely been tested.
Would British police or soldiers open fire on peaceful protesters on Johnson’s, Gove’s or Starmer’s orders? The question may arise. So far, the Territorial Support Group have been used by Johnson to attack protesters, and a strategy of tension is being used to increase antagonism between the people and the police, but further escalation would be risky.
What is needed in the meantime is urgently to unwind the cycle of compliance, beginning with the mass removal of the mask, extending to the deconstruction of the narrative, and culminating in total disobedience against the tyranny now represented by this illegitimate and shameful government.
April 10, 2021
Posted by aletho |
Civil Liberties, Corruption, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, Human rights, UK |
Leave a comment
The WEF’s promotion of a Chinese ‘smart face mask’ that tracks every breath its wearer takes is further evidence that the changes to Western society over the last 12 months of Covid are intended to be permanent.
“It’s only for when you pop into Tesco’s to do your weekly shop, what‘s your problem with that, you selfish ‘right-wing’ libertarian?” That’s how the introduction of mandatory face-masks was sold to us in Britain last summer, by its virtue-signalling, “Look at me, I’m such a good citizen” supporters.
Masks would be temporary – restricted to shops – and as soon as the Covid threat had passed they would be dispensed with, like social distancing. Anyone who said these measures were designed to be permanent – and were part of the global elite’s plan to keep the plebs muzzled up forever – was dismissed as a ‘crank’ and ‘a conspiracy theorist’.
Well, nine months on, and where are we?
The UK government has issued a ‘road map’ for taking us – with the speed of a 150-year-old Galapagos Island tortoise on sleeping tablets – out of lockdown. But there’s no mention of when masks and social distancing will be dispensed with.
Could that be because there’s no intention of masks and social distancing ever being dispensed with? It certainly appears that way.
Since last July, we’ve seen the mask mandate expanded. You are now asked to wear them not just in shops, but in all indoor areas, unless exempt. Even school children have to wear them in class. That decision was supposed to be reviewed at Easter, and, guess what, the government has just extended the school mask mandate until the summer. In addition, football fans will be expected to wear masks when they’re finally allowed back into grounds this spring at ‘trial’ events.
‘Following the science’? Hardly. We shouldn’t forget that in the week that masks were first introduced last summer, deaths with Covid literally reached zero.
The BBC’s Health Correspondent Deborah Cohen asked the World Health Organisation if their change of advice on masks had been due to political lobbying, and they did not deny.
Why, if masks were so important in preventing transmission, weren’t we told to wear them last March and April? In fact, government scientists advised us not to wear them.
Now, it seems not only must we wear them, but we need to get used to them being a permanent part of daily life in the ‘New Abnormal’. In their recent paper, ‘Evaluating England’s Road Map out of Lockdown‘, published on the UK government’s website, the Imperial College Covid-19 Response team state: “Whilst the impact of Test Trace Isolate, mask wearing, hand hygiene and COVID security on ‘R‘ is difficult to quantify it will be vital to emphasise the importance of normalising and ensuring adherence to all measures even after ‘full lifting’ is achieved.” Got that? Masks need to stay even after Boris Johnson says ‘Lockdown is over‘.
It’s in this context that the World Economic Forum’s (WEF) enthusiastic promotion of the Chinese ‘smart face mask’ needs to be seen. It apparently reminds users when to wash it and checks if they’re wearing it properly. If too much carbon dioxide builds up inside, a phone alert reminds the wearer to catch a few breaths of fresh air. If the user forgets to put it on, the same phone app sends them a reminder to mask up.
This is not about public health, but all about making sure that measures introduced ostensibly to stop the spread of Covid-19 become permanent. Yes, once again the much-derided ‘crackpot conspiracy theorists’ of 2020 have been proved right.
Remember how last summer, the WEF was promoting a ‘Common Pass‘ health passport scheme, not just for international travel but for access to domestic events too? It would never happen, we were told. That’s ‘David Icke stuff’, was the condescending brush-off. Well, that too has come to pass – no pun intended.
To find out why all this is happening, all we have to do is to follow the money trail. All the way to Davos. What does the pro-permanent mask Imperial College have in common with the pro-permanent mask WEF? Answer: the pro-permanent mask Bill Gates.
Last month, Gates himself likened putting on a face mask to putting on a pair of trousers. “I just don’t think wearing a mask is such a deep inconvenience. I mean we ask people to wear pants. You know, why was this politicised?” Back in November, he made the same comparison. “We ask you to wear pants and, you know, no American says — or very few Americans say — that that’s, like, some terrible thing.”
But is masking up whenever we go out really the same as putting on a pair of trousers, to use the English term?
Of course it isn’t. Unless you’re Batman or The Lone Ranger, or another Saturday morning cinema superhero, or indeed a bank-robber, wearing a mask in public isn’t normal, and no amount of WEF-spin makes it so. But what walking about with pieces of black cloth over our mouths and noses does do, is maintain the levels of fear in the community.
If cases and deaths with Covid have plummeted to zero, but we want to make people live as if there is a permanent pandemic, to keep control over them, and to introduce ‘Covid-certification’ to restrict where they can and cannot go, how else can we keep Project Fear going without masks? It’s the only way we’d know that these were not ‘normal’ times. Which is, of course, precisely why they were introduced when deaths had dwindled to very low numbers.
Smart masks? The really smart thing is to get wise to the WEF’s dystopian agenda.
Neil Clark is a journalist, writer, broadcaster and blogger. His award winning blog can be found at http://www.neilclark66.blogspot.com.
April 9, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Covid-19, Human rights, UK |
Leave a comment
 Early on in the COVID19 saga I came in contact with Sebastian Rushworth. He was, and is, working as an emergency care doctor in Sweden. It seemed we shared very similar ideas about what was going on. It was fascinating as he was working in Sweden, which has been attacked from all sides, for following WHO advice on the best actions to take in a pandemic.
Early on in the COVID19 saga I came in contact with Sebastian Rushworth. He was, and is, working as an emergency care doctor in Sweden. It seemed we shared very similar ideas about what was going on. It was fascinating as he was working in Sweden, which has been attacked from all sides, for following WHO advice on the best actions to take in a pandemic.
Sweden did not fully lockdown, most schools remained open, as did bars and restaurants etc. As a result of this everyone died… Start again. As a result of this Sweden suffered around the average number of deaths (per head of population) in Europe.
European countries, above a certain size, that have done worse than Sweden, so far, include:
Czechia
Hungary
Bosnia and Herzegovina
Bulgaria
Belgium
North Macedonia
Slovenia
Slovakia
Italy
UK
Portugal
Spain
Peru
Croatia
Poland
France
Lithuania
(NB: I left out micro-countries’ such as Gibraltar, San Marino, Andorra etc.)
You would think, from the howls of anguish that Sweden was now a smoking ruin, with hospitals full of the dead and dying. Which serves them bloody well right. They should have done what every other country did.
Anyway, it was interesting to link up with Sebastian to get a first-hand account of what was going on. You hear so much rubbish from the mainstream media, that it is difficult to know what is really going on. We live in a scary, censored world. Patrolled by self-appointed fact-checking dementors.
Sebastian has his own website at https://sebastianrushworth.com/ which I recommend as a good place for sensible thinking.
Now he has written a book. I should know, because he asked me to write the foreword for it, which I gladly did. It isn’t long, it is very readable, and you will learn a lot if you read it. It covers:
How Dangerous is COVID
Are the tests effective?
Does lockdown work?
Why did Sweden have more deaths than Norway?
Do face masks stop the virus?
Are the vaccines safe and effective?
I recommend it to everyone, and you can find a link to it on his website.
April 9, 2021
Posted by aletho |
Book Review | Covid-19 |
Leave a comment

We would not need a COVID19 vaccine if there is already a safe and effective treatment. Imagine that: No lockdowns, no masks, no destruction of jobs and livelihoods. Are there treatments for Covid-19 that are safe, cheap, and effective?
The Case for Ivermectin is Part 1 of an investigative series exploring the ever increasing fight against censorship, health freedom, and the medical professionals and researchers who dare to question the official narrative.
Please SHARE, DOWNLOAD, and FOLLOW @TheSAQproject on the following platforms:
IG – www.instagram.com/thesaqproject
TELEGRAM – t.me/TheSAQproject
GAB – gab.com/TheSAQproject
MeWe – mewe.com/i/thesaqproject
BitChute – www.bitchute.com/channel/the-saq-project/
April 8, 2021
Posted by aletho |
Corruption, Deception, Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular, Video | Covid-19, COVID-19 Vaccine |
Leave a comment
It’s April 2021 and we’re still being fed the same “stay home, save lives” line of 2020. But lockdowns are based on dodgy data and exaggerations, as well as causing more harm than they supposedly prevent.
As of today, Ontario is once again locked down. The last lockdown of two months was lifted only a month ago.
The province has endured the longest lockdowns in the country, thanks to politicians and medical officers pushing selective statistics.
The “Stay-at-Home” order (sounds so much nicer than lockdown!) requires people to imprison themselves again, except for “essential purposes” (exempt, of course, are Canadian politicians, who have repeatedly violated their own exhortations).
This latest draconian lockdown again impacts nearly every aspect of Ontarians’ ability to live their lives
It means: closed businesses; increasing poverty, loneliness, and depression; increased domestic abuse, a rise in suicides and self-harm; and utter media hysteria (actually, the media hysteria and fear mongering has not ceased since the announcement of a pandemic one year ago).
A petition to end Ontario’s lockdown of small businesses notes:
“There are over 440,000 small businesses in Ontario.
“Less than a week ago [state premier] Doug Ford told restaurants they would be allowed to operate outdoor dining even in grey zones; this caused restaurant owners to spend thousands of dollars on these spaces only to find out that this would not be the case in this current closure.
This level of carelessness and lack of foresight could be the demise of many locally owned restaurants.”
Alarmism and exaggerated ICU data
Premier Doug Ford, in his address yesterday, spoke of case rates, hospitalizations, and ICU occupancy “increasing rapidly, threatening to overwhelm the healthcare system.”
But, as I’ve written before, the whole concept of “cases rising” is meaningless: “Cases are determined by Covid-19 tests, which have proved to be unreliable and inaccurate, giving false positives and creating a false picture of reality. This faulty testing is exacerbating the media hype over ‘rising cases.’”
And according to a long-time employee at the Ottawa General hospital I corresponded with: “I work in a large hospital and I pass through the Covid-19 ICU unit every day. And it’s never been overflowing or too busy.”
Or, as a columnist for the Toronto Sun noted: “Toronto’s top doc said that data was showing younger people in ICUs. Asked about the data, she changed her tweet to say she was ‘hearing’ of younger Toronto ICU patients. Big difference between data showing and you hearing anecdotally.”
Or, as an Ontario MPP noted: “The @OntHospitalAssn keeps fear mongering about ICU capacity. But Critical Care Services Ontario ICU data for Apr 3 reveals: Toronto 375 of 496 beds taken (76%) Central: 398 of 513 (78%) Ontario: 1852 of 2418 (77%) The question to the OHA is why?”
In fact, every year in flu season, we’ve had reports of overcrowding in hospitals, hospitals bursting at seams. This never caused us to shut down our economy and lock down our citizens.
Finally, more and more journalists are asking for proof of the claims bandied about by the Fords and media.
Even Naomi Wolf, not your average “conspiracy theorist” or “right winger” (as those opposed to brutal lockdowns are often described by dinosaur media) tweeted, “How are Canadians still being told such gigantic lies? The whole ‘lockdown equals public safety’ mythology is fully deceased.”
Vested interests in vaccines?
While ordinary Canadians suffer tremendously under lockdowns, Canada’s unelected medical tyrants, the Medical Officers of Health (MOH) are doing quite well, earning $200,000 – $300,000, and more.
In addition to pushing for this latest lockdown, Ontario MOHs went the extra mile and called for “fewer businesses to be deemed essential and more operations shut down.”
Because a year-plus of lockdowns destroying small businesses’ ability to survive just wasn’t enough…
Some of these MOHs may even have financial links to the rollout of vaccines.
In his press conference yesterday, much of Premier Ford’s focus was on pushing jabs.
Ford promised, “better days are ahead of us,” followed by more calls for Ontarians to get jabbed with vaccines made faster than ever before which, technically, will not even be out of the clinical trials stage till next year at the earliest.
The AstraZeneca vaccine is being suspended by countries around the world for causing blood clotting, which could lead to death.
In spite of this, Ontario continues to push it. As of April first, Canada has bought around 24 million doses. In addition to its AstraZeneca purchases, Canada agreed to purchase at least 20 million doses of Pfizer’s hurried vaccine.
In March, the media reported that Toronto’s MOH, Eileen de Villa, is married to Dr Richard Choi, a cardiologist and lecturer at Unity Health Toronto, who lists Pfizer and AstraZeneca among his ‘Relationships with financial interests.’ Under de Villa’s leadership, “Toronto Public Health has been used as a tool to counter any ‘misinformation’ about vaccination,” and was allegedly “behind a call to ban vaccine exemptions because of religious or philosophical beliefs.”
Another article on the de Villa-Choi conflict of interest noted: “It’s not a good look when you lock down your city when you don’t have to and your husband has financial interests with AstraZeneca and Pfizer.”
In mid-March, Premier Ford said he isn’t making the decisions, the chief medical officers are. He also said it would essentially be political suicide to go against them.
“To be frank, there’s no politician in the country who’s going to disagree with their chief medical officer. They’re just not going to do it. They might as well throw a rope around their neck and jump off a bridge.”
Last December, Toronto’s Associate MOH, Dr. Barbara Yaffe, and Chief MOH, Dr. David Williams, admitted they are just reading a script, “I just say what they write down for me.” And laughed about it.
So, we have unelected medical officers running the show, essentially forcing government decisions on lockdowns and related issues. And as a Toronto lawyer opposed to lockdowns noted,“local Councils are legally powerless to stop” these unaccountable MOHs. How wonderfully democratic.
There is definitely a will and momentum to resist the brutal lockdown measures affecting all but the fat cats flouting them. With a new round of bullying by unelected medical officers, I hope the resistance to tyranny grows.
Eva Bartlett is a Canadian independent journalist and activist. She has spent years on the ground covering conflict zones in the Middle East, especially in Syria and Palestine (where she lived for nearly four years).
April 8, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Canada, Covid-19, Human rights |
Leave a comment
Diabolical events rolled out early last year took detailed long term planning.
Plans for the mother of all scams was hatched by US and complicit Western dark forces long before garden variety flu outbreaks were renamed covid.
Millions of unwitting Americans and others abroad were conned to believe what shows up annually requires draconian measures to protect against what for the great majority of people is a few days of illness that pass with no adverse side effects.
Readily available safe, effective, inexpensive drugs are needed at most for relief, for many people none at all.
Yet most people in the West have been brainwashed to self-inflict short and longer-term harm from hazardous covid jabs and other draconian policies on the phony pretext of self-protection not gotten.
Notably in the West, virtually all politicians lie. So do their complicit bureaucrats, public health handmaidens, and press agent media.
Renaming flu covid and draconian measures instituted were planned many months in advance, including vaccine passports for unrestricted access to public places.
In April 2018, the European Commission (EC) — the EU’s executive branch — proposed health passports in a document titled ‘Strengthened Cooperation against Vaccine Preventable Diseases.”
Months later, plans to implement the EC’s proposal “examine(d) the feasibility of developing a common vaccination card/passport” for European countries that’s “compatible with electronic immunization information systems and recognized for use across borders.”
Unmentioned in the West is that vaccines cause outbreaks of illnesses they’re supposed to protect against.
They’re hazardous to health, not the other way around.
Bioweaponized covid mass-jabbing to the rescue risks widespread harm, not protection.
What’s been going on since early last year has nothing to do with protecting and preserving health, just the opposite.
Growing numbers of covid jabbed individuals are falling ill from the virus.
Numbers of adverse events and deaths are suppressed, the tip of the iceberg alone reported.
Throughout the West alone, millions of unwitting guinea pigs were harmed, many seriously.
As long as mass-jabbing continues unchecked, numbers of harmed individuals will increase exponentially.
Unreported by major media, a September 2019 mass-jabbing summit was held in Brussels — Western nations and the complicit WHO involved, supporting the scam instead of exposing and debunking it.
Weeks before seasonal flu-renamed covid outbreaks began, a global pandemic exercise was held.
So-called Event 201 “simulated a series of dramatic, scenario-based facilitated discussions, confronting difficult, true-to-life dilemmas associated with response to a hypothetical, but scientifically plausible, pandemic.”
The Bill & Melinda Gates Foundation, WHO, and Johns Hopkins Center for Health Security supported the diabolical scheme.
Political leaders, senior UN officials, scientific, public health, and medical experts, Pharma, other private sector figures, and NGO’s attended summit discussions.
They were titled “In Vaccines We Trust” “The Magic Of Science,” and ‘Vaccines Protecting Everyone, Everywhere” — knowing they afford no protection and risk great harm when used as directed.
Plans were laid in Europe and the US for what was unleashed at year-end 2019.
Seasonal flu-renamed covid was planned as part of the diabolical Great Reset New World Order plot.
It’s all about transforming the world community of nations into ruler-serf societies — ruling class interests owning everything, ordinary people nothing.
Events rolled out in early 2020 took months of detailed planning.
What’s going on is the most diabolical ever plot against public health, free and open societies, and fundamental freedoms too precious to lose.
A new abnormal in the West and elsewhere is eliminating what just societies hold dear.
Protecting public health and fundamental freedoms demands mass resistance against ongoing horrors no one should tolerate.
If eliminated, they’ll likely be lost for good in our lifetimes — dystopian hell replacing them, much of it already in place.
April 8, 2021
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
In 2020, Florida took the lead in rejecting lockdowns. The effort was led by Governor Ron DeSantis, who in the course of the pandemic became a master of knowledge and erudition on matters of public health and the cell biological issues concerning immunity. In removing mandates and restrictions, he was under the influence of the signatories of the Great Barrington Declaration along with public health scholar Scott Atlas.
The efforts in Florida to protect the elderly while permitting the rest of society to function normally led to a success that has been celebrated the world over. It causes major disruption to the lockdown narrative that the only way to suppress a virus is to suppress rights and freedoms.
As a retrospective on the policy, the governor held a roundtable with all four scientists. Lasting an hour and a half, they covered all the major issues. The video itself came to serve as a tutorial in the relationship between public policy and virus mitigation.
With no warning, no announcement, and no explanation, YouTube on April 7, 2021, suddenly deleted the entire video from its platform. Once hosted by WTSP Tampa Bay, an NBC affiliate, it originally appeared as embedded in a story on WTSP.com. The video that once lived here is now replaced by this.
AIER embedded that same video on our story about the event, along with the first and still the only full transcript of the event. In the late afternoon, the video appeared completely blanked out.
After the lockdowns last spring, YouTube announced that it would pull any video with coronavirus information that was at odds with the recommendations by the Centers for Disease Control and the World Health Organization, organizations that aggressively backed lockdowns in 2020 (after ten years of opposing them). When the CDC and WHO began to contradict themselves on many issues, among which included immunities and their source, YouTube took a different direction, curating the “science” themselves and deleting any video that its employees didn’t like.
This policy has now run afoul of the basic needs of public health messaging, science, and sound policy decision making, even to the point of removing a serious forum of a popular government along with his scientific advisors from Harvard, Stanford, and Oxford universities.
AIER has dealt with problems of censorship for the better part of a year. We began to find alternative sources to host our content, companies that would not engage in sudden takedowns and censorship. Our own choice has been LBRY, which hosts all our videos on a channel.
This sounds like a good solution to censorship, but there is a vulnerability. The Securities and Exchange Commission has singled out LBRY for investigation and fines as high as $11 million for unlawful distribution of securities. The complaint is about the protocol ownership tokens that are distributed to those who use the platform, as a way of incentivizing and monetizing the creation of content. LBRY is only one of many thousands of companies that are using this new method, which is made possible by blockchain technology and the tokenization of internet finance. The SEC has been ambiguous on the question of whether a token is a security but states such as Wyoming have specifically legislated against this claim that fundamentally threatens the entire crypto industry.
Why is LBRY being singled out for investigation? Is it possible that the complaint against the company was initiated by YouTube as a way of tightening the tech giant’s control over internet content? We do not know but it is not crazy to suspect that this is what’s going on.
This latest attack on public health information comes barely one week after Twitter aggressively censored one of the scientists on DeSantis’s panel, Martin Kulldorff, one of the original creators of the Great Barrington Declaration. Meanwhile, Twitter itself has bragged about its new tools for removing anything that contradicts the government/corporate agenda.
And to mention one more case of big-tech/big-media manipulation, Governor DeSantis himself was subjected to an outrageous case of editing by 60 Minutes. The show deliberately distorted its broadcast version of a question and answer session, completely leaving out of its account an extended explanation by the governor that proved that the nature of the question was completely false.
The pulling of the roundtable video comes a day after the total humiliation of 60 Minutes in many stories that defended the governor. Its deletion of the most viewed version online denies viewers the opportunity to observe DeSantis’s impressive knowledge on the subject of the coronavirus and the public policy response.
A new version of the original video of the DeSantis roundtable still appears at AIER, along with a complete transcript.
April 8, 2021
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science, Timeless or most popular, Video | Covid-19, United States |
Leave a comment
Digital vaccine passports are all-about pushing unwitting people to be jabbed with experimental, hazardous to heath drugs that risk potentially irreversible harm short-or-longer-term when taken as directed.
Already rolled out in Israel, Denmark, and Estonia by late April, they’re coming to the US and other Western states.
Apartheid in new form, they’ll create two-tiered societies — jabbed individuals afforded rights everyone deserves and unjabbed social outcasts denied them.
Where vaccine/health passports are instituted, they’ll likely be required for employment, attending school, air travel, other public transportation, hotel reservations, restaurant dining, in-store shopping, attending sporting events, and other social interactions.
Normal daily lives and routines will likely be denied without proof of covid jabs.
What was inconceivable not long ago already became the new abnormal.
Refuseniks will become untouchable social outcasts.
Draconian brave new world conditions will be more intolerable, unsafe and unfit to live in than already.
Nothing remotely justifies lockdowns, quarantines, face masks that don’t protect and risk harm from longterm use, PCR tests not designed to diagnose viral infections, social distancing that destroys normal human interactions, and hazardous experimental drugs that risk contracting diseases they’re supposed to protect against, but don’t.
What’s happening in real time is all-about replacing free and open societies with dystopian ones.
It’s about transforming world community states into ruler-serf societies.
It’s about instituting social control — enforced by police state harshness.
It’s about powerful monied interests owning everything, exploited ordinary people nothing.
It’s the worst of Orwell’s 1984 and Huxley’s Brave New World combined.
Florida Governor Ron DeSantis and Texas Governor Greg Abbott banned the transformation of their states into two-tiered ones.
On April 2, DeSantis banned businesses from requiring customers to show proof of covid jabs (by executive order) to enter their premises and be served.
Barring government agencies from requiring proof of jabs, he said “vaccination passports reduce individual freedom and will harm patient privacy.”
His order doesn’t prevent businesses from establishing screening protocols and other policies recommended by state and federal public health officials.
On Tuesday, Texas Governor Abbott banned state agencies, political organizations receiving public funds, and some private entities from requiring vaccine passports or other proof of jabbing for covid to receive services.
His executive order overrides local ones that call for mandating what infringes on civil liberties.
“We will continue to (jab) Texans (for covid) and protect public health, (but) will do (it) without treading on Texans’ personal freedoms,” Abbott said, adding:
The US Constitution does not permit the federal government to mandate proof of inoculations.
The Biden regime ruled out establishing a national mandate to show proof of covid jabs — so far.
At this time, it’s up to states and local communities to set their own standards.
That policy isn’t written in stone and could change ahead — notably if millions of refuseniks refuse jabs to protect their health and well-being.
Pre-2020, no one could have imagined what’s going on now.
Draconian policies may harden ahead. Guidelines being developed by the White House could be stiffened after in place.
Free and open societies in the West are being replaced by draconian ones.
Based on what happened since early last year, what remains of personal freedoms may disappear entirely ahead — full-blown tyranny replacing them.
A Final Comment
Since Texas scrapped mandatory mask-wearing in public weeks earlier, seasonal flu-renamed covid outbreaks and deaths declined in numbers.
Days earlier, MSNBC noted that Texas today resembles 2019, adding:
“(R)estaurants are full. Ballparks are full.” Yet covid outbreaks declined.
Asked for an explanation, pro-mass-jabbing huckster, fraudster, profiteer, chief Biden regime medical adviser Fauci — a doctor who never treated a patient — failed to explain what’s clear to truth-telling medical and scientific experts.
Policies imposed since early last year did infinitely more harm than any number of serious diseases combined — notably by creating deeper Main Street Depression conditions than in the 1930s and deceiving the public to self-inflict harm from toxic covid jabs.
Former Trump regime trade representative Peter Navarro slammed Fauci, saying the following:
“From the first time I met him, he just did not make a lot of sense.”
“We’ve seen all of his flipflops.”
“My new theory is that he’s simply a sociopath. He just lies to advance his own interest.”
Navarro wants him held accountable for serial lying that contributed to inflicting enormous harm on millions of Americans and countless others abroad.
For what I call crimes against humanity, US and other Western political hardliners, their public health handmaidens, Pharma and media press agents for all of the above share guilt.
April 8, 2021
Posted by aletho |
Civil Liberties | Covid-19, COVID-19 Vaccine, Denmark, Estonia, Human rights, Israel, United States |
Leave a comment
Dr Peter McCullough is the leading published medical doctor of his speciality in the world. He is regarded as an impeccable expert and someone to be listened to on COVID19 treatments.
In this testimony before the Texas Senate he bemoans that too little is being done to educate ourselves on non-vaccine alternative treatments.
VIDEO SOURCE: “Peter McCullough, MD testifies to Texas Senate HHS Committee”, released by Association of American Physicians and Surgeons: https://youtu.be/QAHi3lX3oGM (March 11, 2021). Original description: “Testimony given March 10, 2021. Patient Guide at https://aapsonline.org/covidpatientguide/ ”
QUOTE:
”Lets not have a single person going home with a test result with a fatal diagnosis sitting at home going into two weeks of despair before they succumb to hospitalization and death. … There is not a single media doctor on tv who has ever treated a covid patient. Not a single one! … There was a silencing of any information on treatment! You can’t get papers published on this! … All effort has to be on vaccinations! … You cannot beat natural immunity. You cannot vaccinate and make it better! … There is no scientific rationale to vaccinate young and healthy people. … There is no asymptomatic spread of covid-19. … Covid19 has always been a treatable illness. … 85% of deaths could have been prohibited with early treatment.”
More at www.bitchute.com
April 7, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, Video | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Tyrannical World Economic Forum head Klaus Schwab, the pro-Western/pro-Pharma/pro-mass-jabbing with toxic drugs WHO, and over two dozen hardline world leaders allied with US imperial aims are calling for establishment of a draconian pandemic treaty.
Wrapped in deceptive equitable socioeconomic rhetoric, their scheme all about wanting free and open societies abolished — police state enforced neoliberal harshness on steroids replacing them.
The scheme calls for mandatory global mass-jabbing with experimental, unapproved hazardous to health mRNA technology or vaccines for covid that increase the risk of contracting the disease they’re supposed to protect against, but don’t.
Their plot also increases the chance developing any one or more of a number of serious autoimmune and other diseases near-or-longer-term.
Their diabolical scheme is all risk and no rewards, nothing beneficial from these experimental, rushed to market drugs to be rejected, not used as directed.
A joint press release by Schwab, the WHO, and complicit world leaders defied reality.
It falsely called garden variety seasonal flu-renamed covid “the biggest challenge to the global community since…political leaders came together to forge the multilateral system” in the aftermath of two world wars.
They’re pushing a diabolical Great Reset scheme to transform the world community of nations into ruler/serf societies.
It’s polar opposite “the spirit of solidarity and cooperation (that includes) peace, prosperity, health and security.”
Seasonal flu now called covid shows up annually like clockwork — 2020 and this year no different from earlier ones.
Diabolical dark forces like Schwab, the WHO, and leaders of US vassal states aim to destroy public health, well-being, and fundamental freedoms, not protect and preserve them.
They oppose peace, equity, justice, the rule of law and societies safe and fit to live in.
When ill from seasonal flu now called covid, readily available safe, effective, inexpensive remedies exist — free from hazards posed by toxic mRNA technology and vaccines.
Nothing justifies an international pandemic treaty to combat the common cold or flu — that for the vast majority of people are minor health issues.
They’re in sharp contrast to cancer, heart disease, diabetes, and many other serious ones the above dark forces oppose combatting because their widespread outbreaks let Pharma and large hospital chains cash in big from expensive treatments.
Extensive writing and activism by the late cancer expert Dr. Samuel Epstein explained the following:
The cancer industry is “indifferent (toward and) hostile to “prevention (because it) conflicts” with bottom-line priorities.
The National Cancer Institute (NCI), National Cancer Society (NCS), and American Cancer Society (ACS) are “incestuously tied to the “drug industry, the mammography industry, the pesticide industry, and other such industries” that profit from cancer proliferation.
It’s big business. The more illness, the greater the bottom line benefits.
The same goes for many other major diseases.
The illness industry in the US and West profit from sickness. Health protection and wellness harm their bottom line priorities.
Epstein slammed the cancer industry for “losing the winnable war (on) the disease.”
The same goes for many other curable diseases.
Seasonal flu-renamed covid is being used to fear-monger countless millions of people in the West and elsewhere to self-inflict harm by unneeded/unsafe/toxic drugs to reject, not use as directed.
US federal law prohibits mandatory use of experimental drugs.
Ways around the law include approving use of hazardous drugs by the FDA and/or new legislation to mandate what formerly was prohibited.
Western dark forces will stop at nothing to get their way.
The only solution is mass resistance and revolution.
The alternative risks loss of health, well-being, and free and open societies safe and fit to live in.
That’s where things are heading if not challenged and stopped while there’s time.
April 7, 2021
Posted by aletho |
Deception, Science and Pseudo-Science | Covid-19 |
Leave a comment

