Covid experts: there is another way
Three eminent epidemiologists met in Massachusetts to plan a better response to the pandemic
By Sunetra Gupta, Jay Bhattacharya and Martin Kulldorff | UnHerd | October 5, 2020
As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical, and mental health impacts of the prevailing COVID-19 policies and recommend an approach we call Focused Protection.
“This is the saner approach, the more scientific approach,” the authors tell Freddie Sayers
Coming from both the left and right, and around the world, we have devoted our careers to protecting people. Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
Fortunately, our understanding of the virus is growing. We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.
As immunity builds in the population, the risk of infection to all – including the vulnerable – falls. We know that all populations will eventually reach herd immunity – i.e. the point at which the rate of new infections is stable – and that this can be assisted by (but is not dependent upon) a vaccine. Our goal should therefore be to minimize mortality and social harm until we reach herd immunity.
The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
Adopting measures to protect the vulnerable should be the central aim of public health responses to COVID-19. By way of example, nursing homes should use staff with acquired immunity and perform frequent PCR testing of other staff and all visitors. Staff rotation should be minimized. Retired people living at home should have groceries and other essentials delivered to their home. When possible, they should meet family members outside rather than inside. A comprehensive and detailed list of measures, including approaches to multi-generational households, can be implemented, and is well within the scope and capability of public health professionals.
Those who are not vulnerable should immediately be allowed to resume life as normal. Simple hygiene measures, such as hand washing and staying home when sick should be practiced by everyone to reduce the herd immunity threshold. Schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.
Great Barrington, Massachusetts, 4th October 2020
To sign the declaration, follow this link (will be live later today): www.GBdeclaration.org
Dr Sunetra Gupta is a professor at Oxford University, an epidemiologist with expertise in immunology, vaccine development, and mathematical modelling of infectious diseases
Dr Bhattacharya is a professor at Stanford University Medical School, a physician, epidemiologist, health economist, and public health policy expert focusing on infectious diseases and vulnerable populations.
Dr Kulldorff is a Professor of medicine at Harvard University, a biostatistician, and epidemiologist with expertise in detecting and monitoring of infectious disease outbreaks and vaccine safety evaluations.
Vaccines Are Complicated
By Donna Laframboise | Big Picture News | September 30, 2020
 Eager as we are for a COVID vaccine, we need to be realistic about possible harms – and about a plausible timeline.
Eager as we are for a COVID vaccine, we need to be realistic about possible harms – and about a plausible timeline.
There’s a phrase being tossed around with abandon these days. Everywhere we turn, there’s talk of a “safe and effective” COVID-19 vaccine.
USA Today quotes infectious disease chief Anthony Fauci: “We feel cautiously optimistic that we will be able to have a safe and effective vaccine.”
Two days ago, former US Food and Drug Administration (FDA) commissioners, and
Canada’s Prime Minister, Justin Trudeau, similarly declared recently: “Canadians must have access to a safe and effective vaccine against COVID-19…”
Let us now turn to Vaccines: Truth, Lies and Controversy, a book written by Peter Gotzsche, a Danish physician who has spent decades evaluating the quality of published medical research. 27 years ago, he was among those who founded the Cochrane Collaboration, an organization that systematically assesses healthcare interventions.
In the context of discussing Japanese encephalitis, Gotzsche writes:
according to the WHO “safe and effective vaccines are available.” You should never believe such reassuring statements, which is [drug] industry jargon. Nothing is both safe and effective; effectiveness always comes with a price.
He continues:
In healthcare, people rarely use the term harms. They talk about side effects, which is a euphemism for the inevitable – some people will be harmed and in rare cases even die after having received a vaccine.
Generally speaking, Gotzsche considers vaccines “the most valuable interventions and the best buy for money we can offer.” But the overriding message of his book is that every vaccine must be judged on its own merits. In his view, some vaccines promoted by health authorities are “marginal at best.”
He’s skeptical, for example, of annual flu vaccines, to the point of accusing the website of the US Centers for Disease Control (CDC) of promulgating a “massive amount of misinformation” on this topic. When discussing whether medical personnel and others should be forced to get an annual flu shot, he says:
No vaccine is entirely harmless, and in the worst case, the healthcare worker might die, e.g. because of an anaphylactic shock caused by the vaccine, or fainting with head trauma after the injection, or development of the Guillain-Barre syndrome…
… A common argument for mandatory flu shots is that they prevent transmission of the virus to other people. However, there is no evidence that the vaccine does this…
… Many people will think that their chance of benefitting from the vaccination exceeds 50%, but it is less than 2%…Furthermore, the vaccine does not reduce admission to hospital or days off work…
… It has never been shown in reliable research that flu shots reduce deaths.
Which brings us to COVID-19. The fact that 160 different teams are currently working on a vaccine is immensely encouraging. Surely one of them will hit the target. On the other hand, we must be sensible.
In a July interview, Kenneth Frazier, the CEO of Merck pharmaceutical company, had some words of caution:
What worries me the most is that the public is so hungry, so desperate to go back to normalcy, that they are pushing us to move things faster and faster. But ultimately, if you’re going to use a vaccine in billions of people, you better know what that vaccine does.
… There are a lot of examples of vaccines in the past that have stimulated the immune system, but ultimately didn’t confer protection. And unfortunately, there are some cases where it stimulated the immune system and…actually helped the virus invade the cell…
… I think when people tell the public that there’s going to be a vaccine by the end of 2020, for example, I think they do a grave disservice to the public. I think at the end of the day, we don’t want to rush the vaccine before we’ve done rigorous science. We’ve seen in the past, for example, with the swine flu, that that vaccine did more harm than good. We don’t have a great history of introducing vaccines quickly in the middle of a pandemic.
Where Did Covid-19 Come From?
By Paul Craig Roberts | Institute For Political Economy | September 30, 2020
Evidence indicates that it came from NIH funding of EcoHealth Alliance, an entity doing “gain-of-function” research in collaboration with the Wuhan Institute of Virology. Many experts believe that the virus was created by that research and escaped from the Wuhan lab.
Gain-of-function research involves enhancing the pathogenicity and transmissibility of pathogens. Many scientists are opposed to this research as it amounts in effect to bioweapons research. The rationale for the research is that it enhances with pre-knowledge the ability to respond to some emerging pandemic. In the case of the research at Wuhan, it might have caused one.
There are other explanations of the Covid pandemic, as it is called. Ron Unz based on circumstantial evidence makes a rational case that the US unleashed the virus on China from where it blew back on the US and the rest of the world. Having watched Washington destroy in whole or part seven countries in the past 20 years, it is not difficult to believe that Washington would unleash Covid on China. However, the fact that the NIH itself was financing the research in China is inconsistent with the US having created and unleashed the virus.
Dr. Anthony Fauci, director of the National Institute of Alergy and Infectious Diseases, which is part of NIH, supports gain-of-function research. Last April 28 Newsweek reported:
“Just last year [2019], the National Institute for Allergy and Infectious Diseases [NIAID], the organization led by Dr. Fauci, funded scientists at the Wuhan Institute of Virology and other institutions for work on gain-of-function research on bat coronaviruses.
“In 2019, with the backing of NIAID, the National Institutes of Health committed $3.7 million over six years for research that included some gain-of-function work. The program followed another $3.7 million, 5-year project for collecting and studying bat coronaviruses, which ended in 2019, bringing the total to $7.4 million.
“Many scientists have criticized gain of function research, which involves manipulating viruses in the lab to explore their potential for infecting humans, because it creates a risk of starting a pandemic from accidental release.”
Dr. Joseph Mercola presents views of experts who are critical of the ongoing gain-of-function research in this article: Bioweapon Labs Get More NIH Funding for Deadly ‘Research’
Although it is difficult for those of us who are not experts to have a confident opinion, we should be aware that many experts are convinced that research funded by NIH gave us the Covid pandemic.
The question whether in effect gain-of-function research amounts to banned bioweapons research needs to be taken up by Congress, the UN, and governments around the world. Covid, largely from its mishandling by public authorities, has done a great deal of economic and other damage to many countries that is larger than the cost of the virus itself.
Scientists love to monkey around with things that probably should be left alone. For example, humanity certainly does not need nuclear weapons. Neither does it need weaponized coronaviruses.
Engineering Contagion: UPMC, Corona-thrax and “the Darkest Winter”
Researchers at a BSL-3 lab tied to the organizers of the 2001 Dark Winter simulation, DARPA, and the post-9/11 biodefense industrial complex are genetically modifying anthrax to express Covid-19 components, according to FOIA documents.
By Whitney Webb | The Last American Vagabond | September 25, 2020
Soon after having been fired from his post as secretary of the treasury in December 2002, after a policy clash with the president, Paul O’Neill became a trustee of the University of Pittsburgh Medical Center. Despite having just worked under and clashed with George W. Bush and Dick Cheney, it wasn’t until O’Neill began answering to UPMC CEO Jeffrey Romoff as a member of the Center’s board that he chose to publicly denounce a superior as “evil.”
“He wants to destroy competition. He wants to be the only game in town,” O’Neill would later state of Romoff, adding that “after 18 months I quit [the UPMC board] in disgust” due to Romoff’s “absolute control” over the board’s actions. O’Neill subsequently noted that UPMC “board members who have wealth of hundreds of millions of dollars are not willing to take this guy on.” When pressed by a local reporter, O’Neill further elaborated that he had been told by other board members that they were “afraid” of Romoff because Romoff might “harm them in some way.”
O’Neill’s criticisms of Romoff are hardly an outlier, as local community activists and even a state attorney general have noted that UPMC’s board lets Romoff do as he pleases.
Jeffrey Romoff has ruled UPMC with an iron fist since his predecessor, Thomas Detre, had a heart attack in 1992. As a result of the Center’s massive wealth accumulation, at first spurred by his magic touch for receiving National Institutes of Health (NIH) grants, Detre was able to use the financial power afforded to him to consolidate control over enough of the University of Pittsburgh to create his “own personal fiefdom,” which is now the stand-alone corporation known as UPMC.
Not long after Romoff took over the Center’s reins, he made his intentions clear to faculty and staff, stating at one 1995 UPMC meeting that his “vision” for the future of American health care was “the conversion of health care from social good to a commodity.” Motivated by profit above all else, Romoff aggressively expanded UPMC, gobbling up community hospitals, surgery centers, and private practices to create a “health-care network” that has expanded throughout much of Pennsylvania and even abroad to other countries, including China. Under Romoff, UPMC has also expanded into the health-insurance business, with 40 percent of the medical claims it pays out going straight back into places of care that are owned by UPMC—meaning UPMC is essentially paying itself.
In addition, since UPMC is officially a “charitable nonprofit corporation,” it is exempt from property taxes and has special access to the tax-exempt municipal bond market. UPMC can also solicit tax-deductible grants from private individuals and organizations, as well as governments. These grants totaled over $1 billion dollars between 2005 and 2017.
Despite these perks being officially justified because of UPMC’s “charitable institution” status, the UPMC board, with Romoff at the top, have seen their own multimillion-dollar-per-year salaries continue to climb. Perhaps this perk also comes from UPMC being a nonprofit corporation, as there are no stockholders to whom Romoff and the board must explain their increasingly exorbitant salaries. For instance, Romoff made $8.97 million last year as UPMC’s CEO, a marked increase over the $6.12 million he had raked in the prior year.
UPMC’s financial chicanery is so out of control that even Pennsylvania’s attorney general has taken action against it, suing UPMC in February 2019 for violations of the state’s charity laws based on their “unjust enrichment” and engaging in “unfair, fraudulent or deceptive acts or practices.” Though UPMC decided to settle out of court, the Center and Romoff came out of the affair relatively unscathed.
Now, thanks to the crisis caused by Covid-19, UPMC is once again on the path toward growing even larger and more powerful in pursuit of Romoff’s ultimate goal, which is, in his own words, to make UPMC the “Amazon of health care.”
In this fourth installment of the The Last American Vagabond series “Engineering Contagion: Amerithrax, Coronavirus and the Rise of the Biotech-Industrial Complex”, the “nonprofit” health-care behemoth that is UPMC is squarely placed at the intersection of post-9/11 “biodefense” public-private partnerships; corporate-funded academics who shape public policy on behalf of their private-sector benefactors; and risky research on dangerous pathogens that threatens to unleash the very “bioterror” that these institutions claim to guard against.
The Odd Trajectory of UPMC’s Covid-19 Vaccine Efforts
In January 2020, when much of the world remained blissfully unaware of the coming global pandemic, UPMC was already at work developing a vaccine to protect against the novel coronavirus that causes Covid-19, known as SARS-CoV-2. That month, before the state of Pennsylvania had a single case of Covid-19, UPMC formed a “coronavirus task force,” which was initially focused on lobbying the US Centers for Disease Control and Prevention (CDC) to obtain samples of live SARS-CoV-2 for research purposes. That research was to be conducted at the Biosafety Level 3 (BSL-3) Regional Biocontainment Laboratory (RBL) housed within UPMC’s Center for Vaccine Research. A day after the director of UPMC’s Center for Vaccine Research, W. Paul Duprex, revealed UPMC’s efforts to access the SARS-CoV-2 virus, he announced that the virus samples, containing an estimated 50 to 60 million coronavirus particles, were already en route to the university. At the time, UPMC was one of only a handful of institutions on the CDC’s short list to receive live SARS-CoV-2 samples.
UPMC later stated that they began work on a vaccine for Covid-19 on January 21st, weeks before the February 14th announcement that the virus was on its way to the university. That original vaccine candidate used the published genetic sequence of SARS-CoV-2, released in early January 2020 by Chinese researchers, to synthetically produce SARS-CoV-2 spike proteins that would be transported into cells by an adenoviral vector, which is commonly used in a variety of vaccines. The vaccine candidate was nicknamed PittCoVacc, short for Pittsburgh Coronavirus Vaccine.
A little over a month after the live SARS-CoV-2 samples were received by UPMC’s Center for Vaccine Research, UPMC received a $5 million grant from the Coalition for Epidemic Preparedness Innovations (CEPI), an international organization founded in 2017 by the governments of Norway and India along with the World Economic Forum and the Bill and Melinda Gates Foundation. The grant was officially awarded to “an international academic-industry partnership” that the Center for Vaccine Research had recently formed with the Institut Pasteur in France and Austrian vaccine manufacturer Themis. Soon after, in May, Themis was acquired by vaccine giant Merck, which began recruiting volunteers for human trials earlier this month on September 11. Merck has incredibly close ties with UPMC, particularly its commercialization arm known as UPMC Enterprises.
The CEPI grant seems to have drastically altered the Center for Vaccine Research’s interest in the original adenovirus-vector vaccine candidate, PittCoVacc, as the CEPI grant was specifically aimed at funding a different vaccine candidate that instead uses the measles virus as a vector. The measles virus and the genetic manipulation of measles for use in the measles vaccine is, notably, the principal research interest and expertise of Center for Vaccine Research director Paul Duprex.
This measles-based vaccine candidate has been described as “a modified [genetically altered] measles virus that delivers bits of the new coronavirus into the body to prevent Covid-19” as well as an “attenuated [genetically modified yet weakened] measles virus as a vector with which to introduce genetic material from SARS-[CoV-]2 to the immune system.” The combination of this weakened measles virus and SARS-CoV-2, per Duprex, will produce a “more benign version of coronavirus [that] will acquaint a person’s immune system” with SARS-CoV-2. No vaccine using this modality has ever been licensed.
On April 2nd, less than a week after the CEPI award had been announced, the UPMC researchers who had developed the original vaccine candidate using the more traditional adenovirus-vector approach published a study in EBioMedicine (a publication of the medical journal Lancet) that reported promising results of their vaccine candidate in animal studies. The news that a US institution was among the first in the world to develop a Covid-19 vaccine candidate with promising results from an animal study was heavily amplified by mainstream US media outlets, with those reports noting that UMPC was requesting government permission to quickly move onto human trials.
This original vaccine candidate, however, was mysteriously dropped from subsequent reports and statements from UPMC regarding its Covid-19 vaccine efforts. Indeed, in recent months, Duprex’s statements on the center’s Covid-19 vaccine candidates no longer mention the once-promising PittCoVacc at all. Instead, new reports, citing Duprex, claim that the only UPMC vaccine candidates are the CEPI-funded measles-vaccine candidate and another, more mysterious vaccine candidate, whose nature has only been recently revealed by documents obtained through a Freedom of Information Act (FOIA) request.
Equally odd is that recent media reports on the original vaccine candidate have stopped mentioning UPMC at all, instead citing only Themis, its new owner Merck, and France’s Institut Pasteur. There are no reports indicating a break-up of the original “academic-industry partnership” that had received the CEPI grant. It seems that this is what may have come to pass, as Duprex stated that the UPMC measles-vector vaccine candidate had partnered with the Serum Institute of India for mass production, first for trials and then for public use, depending on how the vaccine advances through the regulatory process. In contrast, Themis/Merck have stated that their vaccine is being produced in France. It remains unclear what the relation is between these two, and apparently analogous, vaccine candidates.
Though Duprex has been relatively forthcoming about the nature of the first UPMC vaccine candidate (i. e., the CEPI-funded measles-vector vaccine), he has been much more tight-lipped about its second vaccine candidate. In late August, he told the Pittsburgh Business Times that the second vaccine candidate that UPMC was developing “works by delivering genetic material coding for a viral protein instead of the entire weakened or killed virus as is standard in other vaccines.” Yet Duprex declined to state what vector will be used to deliver the genetic material into human cells. Recent FOIA revelations, nevertheless, have revealed that UPMC’s second vaccine candidate involves genetically engineering a combination of SARS-Cov-2 and anthrax, a substance better known for its potential use as a bioweapon.
Corona-thrax
The recently obtained documents reveal that the BSL-3 lab that is part of UPMC’s Center for Vaccine Research is conducting eyebrow-raising research involving combining SARS-CoV-2 with Bacillus anthracis, the causative agent of anthrax infection. Per the documents, anthrax is being genetically engineered by a researcher, whose name was redacted in the release, so that it will express the SARS-CoV-2 spike protein, which is the part of the coronavirus that allows it to gain access into human cells. The researcher asserts that “the [genetically engineered anthrax/SARS-CoV-2 hybrid] can [be] used as a host strain to make SARS-CoV-2 recombinant S protein vaccine,” and the creation of said vaccine is the officially stated purpose of the research project. The documents were produced by the University of Pittsburgh’s Institutional Biosafety Committee (IBC), which held an emergency meeting on June 22nd of this year to “discuss specific protocols involving research with the coronavirus,” which included a vote on the aforementioned proposal.
Edward Hammond, the former director of the Sunshine Project, an organization that opposed chemical and biological weapons and the expansion of “dual use” biodefense/bioweapon research, obtained the documents. Other FOIA documents recently obtained by Hammond have revealed an “explosion” of risky Covid-19-related research at other academic institutions, such as the University of North Carolina, which has already had lab accidents involving genetically engineered variants of SARS-CoV-2.
Hammond told The Last American Vagabond that the experiment, which he dubs “Corona-thrax,” is “emblematic of the pointless research excesses that often characterize the response of scientists to the federal government throwing billions of dollars at health crises.” Hammond added, “While I don’t think that Corona-thrax would be infectious, it falls into the categories of pointless and crazy. The biggest immediate risk of all this activity is that a researcher will deliberately or inadvertently create a modified form of SARS-CoV-2 that is even more difficult to treat, or more deadly, and this virus will escape the lab. It only takes a stray droplet.”
Jonathan Latham, a virologist who previously taught at the University of Wisconsin and who is the current editor of Independent Science News, agreed with Hammond that the Corona-thrax experiment is odd and said that he was “concerned here specifically about the research process and the risks of these specific experiments at Pittsburgh.” In an interview with The Last American Vagabond, Latham asserted that it is “unusual by historical standards . . . the combining of two highly pathogenic organisms in a single experiment.” He did note, however, that such studies for the purposes of vaccine research have become more common in recent years, as is made clear in a 2012 study.
Few experiments have been conducted that specifically utilize anthrax in this way. Since 2000, the studies that have examined the use of genetically modified anthrax as a potential vaccine vector have been affiliated with Harvard University. One of these studies was on the use of anthrax as a vector in a potential HIV vaccine and was jointly conducted in 2000 by Harvard researchers and the vaccine company Avant Immunotherapeutics (now part of Celldex).
Despite reporting positive preliminary results in their experiments, Avant/Celldex did not fund further experiments into a vaccine that used this anthrax-based modality, and it does not currently market or have any such vaccine in its product pipeline. This suggests that, for whatever reason, this company did not see much value in this vaccine, despite the preliminary study with Harvard claiming that the methodology was safe and effective.
The Harvard researchers involved in that 2000 study, however, continued to investigate the possibility of an anthrax-based HIV vaccine in 2003, 2004, and 2005, though without corporate sponsorship. Related yet different research has explored the use of “disarmed” anthrax components as an adjuvant in vaccines and as the basis for enzyme-linked immunospot assays.
The aforementioned Harvard researchers patented their methodology of using anthrax in this way for the production of a vaccine in 2002. This means that the anthrax-based “vaccine” currently being developed by UPMC’s Center for Vaccine Research would have to develop a new method that utilizes anthrax in much the same way so as not to infringe on the patent, which is unlikely. The other alternative is that UPMC would pay the patent holders for use of their methodology if they want to commercialize it in a vaccine. Yet, given UPMC’s business model in general, as well as that of UPMC’s Center for Vaccine Research specifically, this also seems unlikely.
Also odd is what sort of incentive UPMC’s Center for Vaccine Research possesses for the Corona-thrax experiment. There are currently over a hundred vaccine candidates that use existing and tested vaccine platforms in pursuit of a Covid-19 vaccine, a fact Duprex himself has acknowledged. As Hammond told The Last American Vagabond, “It is perfectly obvious that there are numerous existing vaccine platforms for Covid-19 and that some of them will, sooner or more likely later, succeed. There is no serious need for some sort of quite strange bacterial platform, much less one that happens to be anthrax. It’s completely unnecessary and frankly bizarre.”
The Crown Jewel of the Biotech-Industrial Complex

Ribbon cutting for the Center for Vaccine Research – From left: Donald S. Burke, U. S. Congressman Mike Doyle, Arthur S. Levine, Dan Onorato, Mark A. Nordenberg.
The Corona-thrax experiment is being conducted at the Center for Vaccine Research’s Regional Biocontainment Laboratory (RBL), where the center’s work with pathogenic agents, such as anthrax and SARS-CoV-2, is conducted.
The creation of UPMC’s RBL was first announced in 2003, when the National Institute of Allergy and Infectious Diseases (NIAID, then and currently led by Anthony Fauci) stated it would fund the laboratory’s construction with an $18 million grant. It was originally planned to be mainly “dedicated to research on agents that cause naturally occurring and emerging infections, as well as potential agents of bioterrorism.” The plan to create the lab was part of the US government decision to dramatically ramp up “biodefense” research in the wake of the 2001 anthrax attacks.
The lab was also intended to work on “developing a vaccine program focusing on basic and translational research” related to viruses of pandemic potential that are at risk of being “weaponized,” including SARS. After the creation of the lab was initially announced, the project expanded, eventually becoming UPMC’s Center for Vaccine Research, which was launched in 2007. The Center for Vaccine Research was the second such institution to be officially added to the NIAID’s “biodefense” RBL network.
The opening of both this lab and UPMC’s Center for Vaccine Research was made reality thanks to the efforts of the main authors of the June 2001 Dark Winter bioterror simulation, a controversial exercise that eerily predicted the 2001 anthrax attacks as well as the initial, yet bogus, narrative that Iraq and Islamic extremist terror groups were responsible for those attacks. However, the anthrax used in the attacks was later revealed to be of US military origin. As noted in Part I of this series, participants in the Dark Winter exercise had foreknowledge of the anthrax attacks and others were involved in the subsequent “investigation,” which many experts and former FBI investigators describe as a cover-up.
Dark Winter was largely written by Tara O’Toole, Thomas Inglesby, and Randall Larsen, all three of whom played integral roles in the founding or operations of UPMC’s Center for Biosecurity, along with O’Toole’s mentor, D. A. Henderson. UPMC’s Center for Biosecurity was launched in September 2003, just days before the NIAID announced it would fund the RBL lab that would later become the UPMC’s Center for Vaccine Research.
Notably, just days after the attacks on September 11, 2001, O’Toole, Inglesby, and Larsen personally briefed Vice President Cheney on Dark Winter. Simultaneously, Cheney’s office at the White House began taking the antibiotic Ciprofloxacin to prevent anthrax infection. In the weeks between that briefing and the 2001 anthrax attacks, Dark Winter participants and several associates of Cheney, namely members of the Project for a New American Century (PNAC) like Donald Kagan and Richard Perle, asserted that a bioterror attack involving anthrax would soon take place.
In the aftermath of the 2001 anthrax attacks, Henderson “was tapped by the federal government to vastly increase the number of [biodefense] labs, both to detect suspected pathogens like anthrax and to conduct bio-defense research, such as developing vaccines,” with the announcement of UPMC’s RBL being part of the launch of the O’Toole-led Center for Biosecurity at UPMC, where Henderson was named senior adviser. In 2003, the Center for Biosecurity was set up at UPMC partially at the request of Jeffrey Romoff to be “the country’s only think tank and research center devoted to the prevention and handling of biological attacks,” with UPMC’s Center for Vaccine Research being the hub of a new “biodefense research” lab network Henderson was setting up and managing at the time. That network remains technically managed by the Fauci-led NIAID.
Also noteworthy is that the Center for Vaccine Research’s director, from its opening in 2007 until 2016, was Donald Burke. Burke is a former biodefense researcher for the US military at Fort Detrick and other installations and, immediately prior to heading the UPMC center, was a program director at the Johns Hopkins Bloomberg School of Public Health, where he worked closely with O’Toole and Inglesby.
At the time of the 2003 announcement regarding the creation of what would become UPMC’s Center for Vaccine Research, Tara O’Toole stated:
“This new laboratory will enable University of Pittsburgh medical researchers to delve further into possible treatments and to develop vaccines against diseases that might result from bioterrorist attack or from natural outbreaks.”
A few years later, after she was nominated to a top post at the Department of Homeland Security, O’Toole was slammed by experts over her excessive lobbying “for a massive biodefense expansion and relaxation of provisions for safety and security.” Rutgers microbiologist Richard Ebright remarked at the time that “she makes Dr. Strangelove look sane.” It was also noted in hearings that O’Toole had worked as a lobbyist for several “life sciences” companies specializing in the sale of biodefense products to the U.S. government, including Emergent Biosolutions – a very controversial company and a key suspect in the 2001 anthrax attacks.
The history of the Center for Vaccine Research’s RBL, particularly the network of people who prompted the lab’s creation, raises concerns about the nature of the Corona-thrax experiment currently being conducted within the facility. This is especially true because the researcher conducting the experiment appears to be ignorant about key parts of the research he or she is conducting.
For instance, the FOIA-redacted researcher incorrectly states that a recombinant virus proposed for use in the study is incapable of infecting human cells, while the IBC members note that this is not the case. In addition, the unnamed researcher falsely claimed that one of the viral vectors for use in the investigator’s study did not express Cas9 (a protein associated with CRISPR gene editing) and gRNA (“guide RNA,” also used in CRISPR) and was unaware that handling those agents requires an enhanced BSL-2 lab (BSL-2+) as opposed to a typical BSL-2 lab.
Apparently such errors among researchers involved in Covid-19 research at UPMC is not an anomaly. During another UPMC IBC meeting included in the FOIA release, the IBC noted the following about a separate research proposal:
“In the investigator’s notes in responses to changes requested by the IBC pre-reviewers, the investigator indicates that RNA from SARS-CoV-1 and SARS-CoV-2 infected cells will be obtained from BEI resources. Genomic RNA isolated from cells infected with SARS-CoV-1 is regulated as a Select Agent by the Federal Select Agent Program and neither the University nor this investigator are registered for possession and use of these materials [emphasis added] (SARS-CoV-1). The investigator must NOT obtain SARS-CoV-1 genomic RNA without prior consultation with the University’s RO/AROs for Select Agents.”
This part, in particular, caught the attention of Jonathan Latham, who noted that it was odd that “a university researcher is trying to obtain approval for an experiment which no one at the university is allowed to do.” Latham added in an interview that “apparently this applicant is totally ignorant of the regulatory environment and by extension the risks of SARS-CoV, which is a highly infectious virus whose escape from a lab has already led to at least one death.”
While Latham assumed that this was a “university researcher,” it is worth noting that the use of the UPMC Center for Vaccine Research’s RBL is not exclusive to researchers affiliated with the university. Indeed, as noted on the NIH website, “Investigators in academia, not-for-profit organizations, industry, and government studying biodefense and emerging infectious diseases may request the use of biocontainment laboratories,” including the RBL managed by the Center for Vaccine Research.
In addition, the Center for Vaccine Research website notes that “scientists from outside the University of Pittsburgh can work in the RBL through a collaboration or contract. Outside scientists must comply with all University of Pittsburgh training, documentation, regulatory, and medical requirements.” This means that outside scientists using the facility are also subject to IBC review. Both the NIH and Center for Vaccine Research sites note that, for an outside researcher to use the UPMC RBL facility, approval from the center’s director must be obtained.
Since the name of the Corona-thrax researcher is redacted, there is no way of knowing if he or she is affiliated with the university or a separate institution, corporation, or government agency. Regardless of who is conducting this experiment, however, it is possible to examine the history and motivations of the man who ultimately signed off on it—the Center for Vaccine Research’s director, Paul Duprex.
Paul Duprex: DARPA-Funded Researcher and Gain-of-Function Enthusiast

Director of UPMC’s Center for Vaccine Research, W. Paul Duprex
Paul Duprex is a former chief scientist for Johnson & Johnson whose subsequent foray into academia was largely funded with research grants from the NIH and the Pentagon’s Defense Advanced Research Projects Agency (DARPA). Much of Duprex’s research has focused on recombinant (i. e., genetically engineered) viruses or viral evolution.
In terms of his research funded by DARPA, Duprex was most closely associated with DARPA’s “Prophecy” program, the creation of which was overseen by Michael Callahan. Callahan’s suspect past and his ties to the origin of the current Covid-19 crisis in Wuhan, China, were the subject of a recent Unlimited Hangout article by Raul Diego.
In that article, Diego notes that the now-defunct Prophecy program had “sought to ‘transform the vaccine and drug development enterprise from observational and reactive to predictive and preemptive’ through algorithmic programming techniques” and that the program further “proposed that ‘viral mutations and outbreaks’ could be predicted in advance to more rapidly counter the unknown disease with preemptive drug and vaccine development.”
By all indications, Prophecy was DARPA’s first major foray into “predictive” AI-powered health care, which has expanded considerably in the years since. It also involved a component, which Duprex was particularly involved in advancing, whereby the “predictive” viral evolutions algorithms would be “validated and tested . . . by using multiple selective pressures on at least three closely related virus strains in an experimental setting.”
Such experiments, like this study by Duprex, involved the genetic engineering of three viral pathogen strains and then seeing which would become most transmissible and virulent in an animal host. Such studies are often referred to as gain-of-function (GOF) research and are incredibly controversial given that they often create pathogens that are more virulent and/or transmissible than they otherwise would be. It is also worth noting that UPMC, before Duprex joined the center, had also received millions in funding from DARPA’s Prophecy program “to develop in vitro and computational models for predicting viral evolution under selection pressure from multiple evolutionary stressors.”
Duprex has also been involved in conducting research for DARPA’s current INTERfering and Co-Evolving Prevention and Therapy (INTERCEPT) program, a successor to Prophecy that “aims to harness viral evolution to create a novel, adaptive form of medical countermeasure—therapeutic interfering particles (TIPs)—that outcompetes viruses in the body to prevent or treat infection.” TIPs are genetically engineered viruses with defective genomes that theoretically compete with real viruses for viral components in the human body but “evolve with” the viruses they are meant to protect the body against and are “susceptible to mutation over time.”
The goal of the INTERCEPT program is to use TIPs as “therapeutics” and have them injected into the human body to “preemptively” protect against the virus from which a particular TIP was developed. It is worth noting that, while DARPA frames much of its gene-editing research (including its “genetic extinction” technology research) as being aimed at promoting either human or environmental health, it has also openly admitted that these same technologies are of interest to DARPA for their ability to “subvert” the genes of human adversaries of the US military via “genetic weapons.”
Duprex led an INTERCEPT study published in February of this year in which he and his coauthors explored how to create a synthetic TIP of the Nipah virus, a deadly virus with a fatality rate of over 70 percent. In that study, they used both wild and genetically engineered strains of Nipah virus. Notably, the Clade X pandemic simulation, which will be discussed in detail in the next installment of this series, involved a genetically engineered combination of the Nipah virus and a parainfluenza disease.
Clade X took place in 2018 and was led by much of the same team that was responsible for the 2001 Dark Winter bioterrorism simulation, including former FDA commissioner Margaret Hamburg and Tara O’Toole and Thomas Inglesby of the UPMC Center for Biosecurity. Another notable participant at Clade X was Julie Gerberding, former CDC director and current executive vice president at Merck, which has close ties to UPMC as well as the Center for Biosecurity’s failed “21st Century Biodefense” project.
A few months after publishing the study funded by DARPA’s INTERCEPT program, Duprex coauthored another study on the use of synthetic “nanobodies” (i. e., bioengineered synthetic nanoparticles acting as antibodies) that was published in August. This effort mirrors other DARPA “health-focused” projects. That study was funded by the University of Pittsburgh, the NIH, and Israel’s Ministry of Science and Technology.
In addition to his ties to DARPA programs involving the genetic engineering of viral pathogens, Duprex is a leading advocate for controversial gain-of-function research and was appointed to direct UPMC’s Center for Vaccine Research less than three months after the federal moratorium on GOF research ended.
In October 2014, five days after that moratorium was first imposed, Duprex gave a talk to the National Science Advisory Board for Biosecurity entitled “Gain-of-Function Studies: Their History, Their Utility, and What They Can Tell Us.” In the talk, he asserted that “cross-species infection studies have already helped to improve surveillance in the field, have shed new light on basic influenza virus biology, and could assist in growing vaccine viruses better” and argues against the recently imposed moratorium.
In 2014, Duprex also wrote in a paper published in Nature that “GOF approaches are absolutely essential in infectious disease research; although alternative approaches can be very useful, these can never replace GOF experiments.” He added that, in his view, there were only two reasons for GOF research, the first being to “improve surveillance or to develop therapeutics” and the second being merely to learn “interesting biology.”
In that same paper, he also argued that “genetic engineering that is intended and likely to endow a low-pathogenicity, low-transmissibility agent with either enhanced pathogenicity or enhanced transmissibility may be appropriate if the benefits are substantial.” He also suggested in this 2014 paper that it “might” be necessary “to enhance pathogenicity of coronaviruses in order to develop a valid animal model for coronaviruses.” Years later, during the current coronavirus crisis, Duprex and other officials from the UPMC’s Center for Vaccine Research co-developed a Covid-19 research and development “blueprint” for the UN’s World Health Organization.
In addition, Duprex’s work for DARPA’s Prophecy program involved GOF research, as noted above, and the creator of that program, Michael Callahan – former head of DARPA’s biodefense therapeutics initiatives, is also a proponent of GOF who believes that such risky research is inseparable from “the research and development enterprise in the life sciences and for biotechnology.”
Duprex is also a founding member of Scientists for Science, a group of researchers (most of whom are involved in GOF research) who opposed the GOF moratorium and were “confident that biomedical research on potentially dangerous pathogens can be performed safely and is essential for a comprehensive understanding of microbial disease pathogenesis, prevention and treatment.” Another of the group’s founding members is Yoshihiro Kawaoka, whose controversial GOF experiments that made pathogenic viruses more deadly have garnered considerable media attention.
When the moratorium on GOF was lifted in December 2017, Duprex called it a “sign of progress,” adding that “on a personal level I’m really pleased these NIH funded scientists [conducting GOF research] get some clarity.” As previously mentioned, he became the Center for Vaccine Research’s director less than three months later, in March 2018.
The “Darkest Winter” Looms

After a cursory examination of the background of UPMC, its Regional Biocontainment Laboratory, and the man directing its Center for Vaccine Research, the question about the nature of the Corona-thrax experiment becomes: Is this yet another ill-advised experiment by a lab led by a GOF enthusiast and fueled by a feeding frenzy over the billions of dollars thrown by the government and other entities into Covid-19 research? Or is there perhaps a more nefarious motive to genetically engineering something as bizarre as Corona-thrax?
While the latter question may appear conspiratorial, it is worth pointing out that the institutions most likely to have been the sources for the anthrax used in the 2001 anthrax attacks were conducting GOF research on anthrax funded by the Pentagon and the CIA that was justified as “improving” the controversial anthrax vaccine known as BioThrax.
For instance, Battelle Memorial Institute—a Pentagon and CIA contractor—began genetically engineering a more virulent form of anthrax “to see if the [anthrax] vaccine the United States intends to supply to its armed forces is effective against that strain.” While these experiments were going on, the embattled manufacturer of the anthrax vaccine now known as Emergent Biosolutions, entered into a contract with Battelle that gave Battelle “immediate exposure to the vaccine” it was using in connection with the genetically modified anthrax program.
As noted in Part II of this series, BioPort was set to lose its Pentagon contract for anthrax vaccine entirely in September 2001, and the entirety of its anthrax vaccine business was rescued by the 2001 anthrax attacks, which saw concerns over BioPort’s corruption and its horrendous safety track record replaced with fervent demands for more of its anthrax vaccine. Furthermore, as noted in detail in Part III of this series, Battelle was the most likely source of the anthrax used in the 2001 attacks. The ties between UPMC’s Center for Biosecurity, Battelle, and Emergent Biosolutions will be discussed in the next installment in the series.
What is also notable about these Corona-thrax experiments occurring at UPMC are the ties of UPMC’s RBL and Center for Vaccine Research to another key component of the center’s “biodefense” complex, the UPMC Center for Biosecurity. As previously mentioned, the people recruited to head this center at its founding in 2003 were intimately involved in the 2001 bioterror simulation Dark Winter, namely Tara O’Toole and Thomas Inglesby.
While leading the UPMC’s Center for Biosecurity, O’Toole and/or her successor Inglesby engaged in other notable bioterror simulations, including one that took place last year— Event 201, which eerily predicted the coronavirus crisis that began this year. Inglesby, who is also the director of the Johns Hopkins Center for Health Security in addition to his post at UPMC, was the moderator at Event 201.
Though Event 201 has garnered considerable scrutiny in recent months, another but less well-known exercise in 2018 that involved O’Toole and Inglesby, examined how a bioterror attack involving a genetically engineered pathogen could trigger a Continuity of Government (CoG) scenario, a government roadmap for the imposition of martial law in the United States. As other investigative series of mine have noted, there have recently been a myriad of intelligence agency–linked simulations that predict the imminent imposition of martial law in the United States following the 2020 election.
It is also notable that George W. Bush’s controversial and classified update to CoG plans in 2007, known as Executive Directive 51, was directly inspired by Dark Winter, and Barack Obama’s subsequent executive orders on CoG gave near-complete control of American infrastructure to the Department of Homeland Security in a such a situation. At the time Obama issued those executive orders, O’Toole was the DHS undersecretary for science and technology and also influenced those updates to the CoG plans. O’Toole is currently the executive vice president of the CIA’s In-Q-tel.
The simulation known as Clade X will be examined in greater detail in the next installment of this series as will the numerous and recent “predictions” from US government sources, controversial billionaires such as Bill Gates, and a web of individuals tied to UPMC who have warned that a bioterror attack or related public health catastrophe is set to take place in the United States in the latter half of 2020. As one high-ranking government official put it earlier this year, this allegedly imminent event will result in “the darkest winter in modern history.”
Cheaper Than Remdesivir: Russia to Supply Anti-COVID Avifavir to 17 Countries
In late May, Russia registered the world’s first anti-COVID-19 drug, based on favipiravir, an antiviral medication. The medicine has been extensively used in Russian clinics to treat coronavirus disease since June, and has since been obtained by hospitals in Belarus, Kazakhstan, Bolivia and a number of other countries.
The Russian Direct Investment Fund (RDIF), the investor which funded the development of the world’s first vaccine against coronavirus, and Moscow-based ChemRar Group have agreed to supply the anti-COVID drug Avifavir to 17 countries.
Avifavir, the world’s first favipiravir-based drug to be approved for the treatment of COVID-19, will now be delivered to Saudi Arabia, Brazil, Bulgaria, Serbia, Argentina, Chile, Colombia, Ecuador, El Salvador, Honduras, Kuwait, Panama, Paraguay, Slovakia, South Africa, the UAE and Uruguay.
After being first registered in Russia on 29 May 2020, it has already been used for COVID-19 treatment in more than 70 Russian regions and subsequently purchased by Belarus, Bolivia, Kazakhstan, Kyrgyzstan, Turkmenistan and Uzbekistan.The efficacy of favipiravir against COVID-19 has been confirmed by Japan’s Fujifilm Holdings Corp, several months after Avifavir trials in Russia.
Avifavir as the Leading Anti-Covid Drug in the Russian Market
RDIF notes that in comparison to other Russian manufacturers of favipiravir, Avifavir has proven to be more effective when treating more than 400 patients, who fell ill with the coronavirus disease since April. The drug has now been approved by European, Middle Eastern and Asian regulators, becoming Russia’s number one anti-coronavirus medication for export.
According to RDIF, it is also a much cheaper option in comparison to Remdesivir, a favipiravir-based drug produced in the United States.
“When we registered the first anti-coronavirus drug in the world based on favipiravir, there was a lot of scepticism as people were wondering how we could register it when Japan had not registered it yet,” says Kirill Dmitriev, CEO of the Russian Direct Investment Fund. “Now five months after our clinical trials, we see that Japan has confirmed the clinical efficacy of favipiravir.”
The RDIF CEO stresses that apart from clinical trials which were conducted at 35 medical centres in Russia, Avifavir’s efficiency has also been tested by 940 patients in observational post-registration studies, which made it “the largest clinical trial of a favipiravir-based drug against coronavirus in the world”.
“Based on our extensive clinical trials and the research in Japan confirming favipiravir’s efficacy against coronavirus we believe that Avifavir and other favipiravir-based products will be the leading antiviral medicines against COVID-19 in the world,” Dmitriev adds. “In addition to proven efficacy and safety Avifavir is also three to four times cheaper than Remdesivir.”
Trials Confirm Avifavir’s Efficiency
According to the results of post-registration clinical trials, those patients taking Avifavir recovered more quickly from COVID-19 symptoms, as in 30% of cases the virus was eliminated at an early stage, while the level of oxygen saturation in the patient’s blood was also restored to normal two times more quickly than when traditional therapy was applied. No adverse effects from the drug’s use have been reported. Meanwhile, the third phase of clinical trials of the Japanese favipiravir-based drug Avigan also showed a shorter time of recovery among patients with non-severe pneumonia, according to the results published on 23 September.
RDIF, Russia’s sovereign wealth fund, has also been involved in the development of the world’s first anti-coronavirus vaccine, dubbed Sputnik V, which was registered in Russia on 11 August. The country has now received a request for 1 billion doses of the vaccine from at least 20 countries, including the UAE, Saudi Arabia, Indonesia, Philippines, Mexico, Brazil and India.
Betrayal. Infuriating, Betrayal

By Mike Whitney • Unz Review • September 23, 2020
“The belief in a supernatural source of evil is not necessary; men alone are quite capable of every wickedness.” Joseph Conrad
Here’s your political puzzler for the day: Which of these two things poses a greater threat to the country:
- An incompetent and boastful president who has no previous government experience and who is rash and impulsive in his dealings with the media, foreign leaders and his critics?
- Or a political party that collaborates with senior-level officials in the Intel agencies, the FBI, the DOJ, the media, and former members of the White House to spy on the new administration with the intention of gathering damaging information that can be used to overthrow the elected government?
The answer is “2”, the greater threat to the country is a political party that engages in subversive activity aimed at toppling the government and seizing power. In fact, that’s the greatest danger that any country can face, an enemy from within. Foreign adversaries can be countered by diplomatic engagement and shoring up the nation’s military defenses, but traitors–who conduct their activities below the radar using a secret network of contacts and connections to inflict maximum damage on the government– are nearly unstoppable.
What the Russiagate investigation shows, is that high-ranking members of the Democrat party participated in the type of activities that are described above, they were part of an illicit coup d’etat aimed at removing Donald Trump from office and rolling back the results of the 2016 elections. It is a vast understatement to say that the operation was merely an attack on Donald Trump when, in fact, it was an attack on the system itself, a full-blown assault on the right of ordinary people to choose their own leaders. That’s what Russiagate is really all about; it was an attempt to torpedo democracy by invoking the flimsy and unverifiable claim that Trump was an agent of the Kremlin.
None of this, of course, has been discussed in a public forum because those platforms are all privately-owned media that are linked to the people who executed the junta. But for those who followed events closely, and who know what actually happened, there has never been a more serious crime in American history. What we discovered was that the permanent bureaucracy, the media and the Democrat party are riddled with strategically-placed quislings and collaborators that are willing to sabotage their own government if they are so directed. The question that immediately comes to mind is this: Who concocted this plot, who authorized the electronic eavesdropping, the confidential informants, the widespread spying, the improperly obtained warrants, the fake news, and the endless leaks to the media? Who?
What we witnessed was not just an attempted coup, it was a window into the inner-workings of a secret government operating independently from within the state. And the sedition was not confined to a few posts at the senior levels of the FBI, CIA, NSA, or DOJ. No. The corruption has saturated the entire structure, seeping down to the lower levels where career bureaucrats eagerly perform tasks that are designed to damage or incriminate elected officials. How did it ever get this bad?
And who is calling the shots? We still don’t know.
Let me pose a theory: The operation might have been concocted by former CIA-Director John Brennan, but Brennan surely is not the prime instigator, nor is Clapper, Comey or even Obama. The real person or persons who initiated the coup will likely never be known. These are the Big Money guys who operate in the shadows and who have a stranglehold on the Intelligence agencies. These are the gilded Mandarins who have their tentacles wrapped firmly around the entire state-power apparatus and who dictate policy from their leather-bound chairs at their high-end men’s clubs. These are the people who decided that Donald Trump “had to go” whatever the cost. They pulled out all the stops, engaged their assets across the bureaucracy, and launched a desperate 3 and half year-long regime change operation that blew up in their faces leaving behind a trail carnage from Washington, DC to Sydney, Australia. In contrast, Trump somehow slipped the noose and escaped largely unscathed. He was pummeled mercilessly in the media, disparaged by his political rivals, and raked over the coals by the chattering classes, but — at the end of the day– it was Trump who was left standing. Trump– who took on the entire political establishment, the Intel agencies, the FBI, the mainstream media, and the Democratic party– had beaten them all at their own game. Go figure??
Keep in mind, the Democrats have known that the Mueller probe was a fraud from as early as 2017 when the President of Crowdstrike, Shawn Henry, (who provided cyber security for the DNC) admitted to Congress that there was no forensic evidence that the DNC emails had been hacked by Russia or anyone else.
Think about that for a minute: The entire Mueller investigation was based on the assumption that Russia hacked into the DNC servers and stole the emails. We now know that never happened. The cyber-security team that conducted the investigation of the DNC computers admitted in sworn testimony before Congress that there was no evidence of “exfiltration” or pilfering of any kind. Repeat: There was no proof of hacking, no proof of Russian involvement, and no proof of foul play. The entire foundation upon which the Russia investigation was built, turned out to be false. More importantly, Democrat members of the Intelligence Committee knew it was false from the get-go, but opted to let the charade continue anyway. Why?
Because the truth didn’t matter, what mattered was getting rid of Trump by any means necessary. That’s why they used “opposition research” (Note– “Oppo” research is the hyperbolic nonsense political parties use to smear a political opponent.) to illegally obtain warrants to spy on members of the Trump team. It’s because the Democrat leadership will do anything to regain power.
By the way, we also have evidence that the warrants that were used to spy on Trump were obtained illegally. The FISA court was deliberately misled so the FBI could carry out its vendetta on Trump. Former FBI lawyer Kevin Clinesmith “did willfully and knowingly make and use a false writing and document, knowing the same to contain a materially false, fictitious, and fraudulent statement and entry in a matter before the jurisdiction of the executive branch and judicial branch of the Government of the United States.” Bottom line: Clinesmith deliberately altered emails so that FISA applications could be renewed and the spying on the Trump campaign could continue.
So, let’s summarize:
- The Democrats knew there was no proof the emails were stolen; thus, they knew the Russia probe was a hoax.
- The Democrats knew that their fraudulent “opposition research” was being used to illegally obtain warrants to spy on the Trump camp. This makes them accessory to a crime.
- Finally, the Democrats continue to spread (virtually) the same Russia-Trump collusion allegations today that they did before the Mueller investigation released its report. The lies and disinformation have persisted as if the “nation’s most expensive and exhaustive investigation” had never taken place. What does this tell us about the Democrats?
On a superficial level, it tells us that they can’t be trusted because they don’t tell the truth. But on a deeper level, it expresses the party’s Ruling Doctrine, which is to control the public by means of deceit, disinformation, propaganda and lies. Only the powerful and well-connected are entitled to know the truth, everyone else must be subjected to fabrications that are crafted in a way that best coincides with the overall objectives of ruling elites. That’s why the Democrats stick with the shopworn mantra that Trump is in bed with Russia. It doesn’t matter that the theory has been thoroughly discredited and disproved. It doesn’t even matter that the theory was never the slightest bit believable to begin with. What matters is that party leaders are preventing ordinary people from knowing the truth, which is an essential part of their governing doctrine. It’s surprising that this doesn’t piss-off more Democrats, after all, it’s the ultimate expression of contempt and condescension. When someone lies to your face relentlessly, repeatedly and shamelessly, they are expressing their loathing for you. Can’t they see that?
But maybe you think this is overstating the case? Maybe you think the Dems are just trying to “cover their backside” on a matter that is purely political?
Okay, but answer this: Were the Democrats involved in a plot to overthrow the President of the United States?
Yes, they were.
Is that treason?
Yes, it is.
Then, are we really prepared to say that treason is “purely political”?
No, especially since Russiagate was not a one-off, but just the first shocking example of how the Democrats operate. If we examine the Dems approach to the Covid-19 crisis, we see that their policy is actually more destructive than the 4-year Russia fiasco.
For example, which party has imposed the most brutal, economy-eviscerating lockdowns and the most punitive mask mandates, while steadily ratcheting up the fearmongering at every opportunity? Which states suffered the most catastrophic economic damage due in large part to the edicts issued by their Democrat governors? Which party is using a public health emergency to advance the global “Reset” agenda announced at the World Economic Forum (WEF)? Which party is using the Covid-19 fraud to crash the economy, eliminate 40 million jobs, roll-back basic civil liberties and turn the United States into a NWO slave-state ruled by Wall Street bankers, Silicon Valley technocrats and Davos elites? Which party?
And which party has aligned itself with Black Lives Matter, the faux-social justice organization that is funded by foreign oligarchs that are working tirelessly to crush the emerging populist movement that supports “America First” ideals? Which party applauded while American cities burned and small businesses across the country were looted and razed by masses of hooligans engaged in an orgy of destruction? Which party’s mayors and governors rejected federal assistance to put down the riots and reestablish order so ordinary people could get back to work to provide for themselves and their families? And which party now is threatening widespread social unrest and anarchy if the upcoming presidential election does not produce the result that they or their globalist puppet-masters seek?
The Democrat party has undergone a sea-change in the last four years. There’s no trace of the party that was once headed by progressive-thinking idealists like John F Kennedy. What’s left now is a shell of its former self; a cynical, self-aggrandizing, cutthroat organization that has betrayed its base, the American people, and the country. Indeed, for all its many failings, it is the ‘betrayal’ that is the most infuriating.
Lies, Damned Lies and Health Statistics – the Deadly Danger of False Positives
By Dr Michael Yeadon | Lockdown Sceptics | September 20, 2020
I never expected to be writing something like this. I am an ordinary person, recently semi-retired from a career in the pharmaceutical industry and biotech, where I spent over 30 years trying to solve problems of disease understanding and seek new treatments for allergic and inflammatory disorders of lung and skin. I’ve always been interested in problem solving, so when anything biological comes along, my attention is drawn to it. Come 2020, came SARS-CoV-2. I’ve written about the pandemic as objectively as I could. The scientific method never leaves a person who trained and worked as a professional scientist. Please do read that piece. My co-authors & I will submit it to the normal rigours of peer review, but that process is slow and many pieces of new science this year have come to attention through pre-print servers and other less conventional outlets.
While paying close attention to data, we all initially focused on the sad matter of deaths. I found it remarkable that, in discussing the COVID-19 related deaths, most people I spoke to had no idea of large numbers. Asked approximately how many people a year die in the UK in the ordinary course of events, each a personal tragedy, they usually didn’t know. I had to inform them it is around 620,000, sometimes less if we had a mild winter, sometimes quite a bit higher if we had a severe ’flu season. I mention this number because we know that around 42,000 people have died with or of COVID-19. While it’s a huge number of people, its ‘only’ 0.06% of the UK population. Its not a coincidence that this is almost the same proportion who have died with or of COVID-19 in each of the heavily infected European countries – for example, Sweden. The annual all-causes mortality of 620,000 amounts to 1,700 per day, lower in summer and higher in winter. That has always been the lot of humans in the temperate zones. So for context, 42,000 is about ~24 days worth of normal mortality. Please know I am not minimising it, just trying to get some perspective on it. Deaths of this magnitude are not uncommon, and can occur in the more severe flu seasons. Flu vaccines help a little, but on only three occasions in the last decade did vaccination reach 50% effectiveness. They’re good, but they’ve never been magic bullets for respiratory viruses. Instead, we have learned to live with such viruses, ranging from numerous common colds all the way to pneumonias which can kill. Medicines and human caring do their best.
So, to this article. Its about the testing we do with something called PCR, an amplification technique, better known to biologists as a research tool used in our labs, when trying to unpick mechanisms of disease. I was frankly astonished to realise they’re sometimes used in population screening for diseases – astonished because it is a very exacting technique, prone to invisible errors and it’s quite a tall order to get reliable information out of it, especially because of the prodigious amounts of amplification involved in attempting to pick up a strand of viral genetic code. The test cannot distinguish between a living virus and a short strand of RNA from a virus which broke into pieces weeks or months ago.
I believe I have identified a serious, really a fatal flaw in the PCR test used in what is called by the UK Government the Pillar 2 screening – that is, testing many people out in their communities. I’m going to go through this with care and in detail because I’m a scientist and dislike where this investigation takes me. I’m not particularly political and my preference is for competent, honest administration over the actual policies chosen. We’re a reasonable lot in UK and not much given to extremes. What I’m particularly reluctant about is that, by following the evidence, I have no choice but to show that the Health Secretary, Matt Hancock, misled the House of Commons and also made misleading statements in a radio interview. Those are serious accusations. I know that. I’m not a ruthless person. But I’m writing this anyway, because what I have uncovered is of monumental importance to the health and wellbeing of all the people living in the nation I have always called home.
Back to the story, and then to the evidence. When the first (and I think, only) wave of COVID-19 hit the UK, I was with almost everyone else in being very afraid. I’m 60 and in reasonable health, but on learning that I had about a 1% additional risk of perishing if I caught the virus, I discovered I was far from ready to go. So, I wasn’t surprised or angry when the first lockdown arrived. It must have been a very difficult thing to decide. However, before the first three-week period was over, I’d begun to develop an understanding of what was happening. The rate of infection, which has been calculated to have infected well over 100,000 new people every day around the peak, began to fall, and was declining before lockdown. Infection continued to spread out, at an ever-reducing rate and we saw this in the turning point of daily deaths, at a grim press conference each afternoon. We now know that lockdown made no difference at all to the spread of the virus. We can tell this because the interval between catching the virus and, in those who don’t make it, their death is longer than the interval between lockdown and peak daily deaths. There isn’t any controversy about this fact, which is easily demonstrated, but I’m aware some people like to pretend it was lockdown that turned the pandemic, perhaps to justify the extraordinary price we have all paid to do it. That price wasn’t just economic. It involved avoidable deaths from diseases other than COVID-19, as medical services were restricted, in order to focus on the virus. Some say that lockdown, directly and indirectly, killed as many as the virus. I don’t know. Its not something I’ve sought to learn. But I mention because interventions in all our lives should not be made lightly. Its not only inconvenience, but real suffering, loss of livelihoods, friendships, anchors of huge importance to us all, that are severed by such acts. We need to be certain that the prize is worth the price. While it is uncertain it was, even for the first lockdown, I too supported it, because we did not know what we faced, and frankly, almost everyone else did it, except Sweden. I am now resolutely against further interventions in what I have become convinced is a fruitless attempt to ‘control the virus’. We are, in my opinion – shared by others, some of whom are well placed to assess the situation – closer to the end of the pandemic in terms of deaths, than we are to its middle. I believe we should provide the best protection we can for any vulnerable people, and otherwise cautiously get on with our lives. I think we are all going to get a little more Swedish over time.
In recent weeks, though, it cannot have escaped anyone’s attention that there has been a drum beat which feels for all the world like a prelude to yet more fruitless and damaging restrictions. Think back to mid-summer. We were newly out of lockdown and despite concerns for crowded beaches, large demonstrations, opening of shops and pubs, the main item on the news in relation to COVID-19 was the reassuring and relentless fall in daily deaths. I noticed that, as compared to the slopes of the declining death tolls in many nearby countries, that our slope was too flat. I even mentioned to scientist friends that inferred the presence of some fixed signal that was being mixed up with genuine COVID-19 deaths. Imagine how gratifying it was when the definition of a COVID-19 death was changed to line up with that in other countries and in a heartbeat our declining death toll line became matched with that elsewhere. I was sure it would: what we have experienced and witnessed is a terrible kind of equilibrium. A virus that kills few, then leaves survivors who are almost certainly immune – a virus to which perhaps 30-50% were already immune because it has relatives and some of us have already encountered them – accounts for the whole terrible but also fascinating biological process. There was a very interesting piece in the BMJ in recent days that offers potential support for this contention.
Now we have learned some of the unusual characteristics of the new virus, better treatments (anti-inflammatory steroids, anti-coagulants and in particular, oxygen masks and not ventilators in the main) the ‘case fatality rate’ even for the most hard-hit individuals is far lower now than it was six months ago.
As there is no foundational, medical or scientific literature which tells us to expect a ‘second wave’, I began to pay more attention to the phrase as it appeared on TV, radio and print media – all on the same day – and has been relentlessly repeated ever since. I was interviewed recently by Julia Hartley-Brewer on her talkRADIO show and on that occasion I called on the Government to disclose to us the evidence upon which they were relying to predict this second wave. Surely they have some evidence? I don’t think they do. I searched and am very qualified to do so, drawing on academic friends, and we were all surprised to find that there is nothing at all. The last two novel coronaviruses, Sar (2003) and MERS (2012), were of one wave each. Even the WW1 flu ‘waves’ were almost certainly a series of single waves involving more than one virus. I believe any second wave talk is pure speculation. Or perhaps it is in a model somewhere, disconnected from the world of evidence to me? It would be reasonable to expect some limited ‘resurgence’ of a virus given we don’t mix like cordial in a glass of water, but in a more lumpy, human fashion. You’re most in contact with family, friends and workmates and they are the people with whom you generally exchange colds.
A long period of imposed restrictions, in addition to those of our ordinary lives did prevent the final few percent of virus mixing with the population. With the movements of holidays, new jobs, visiting distant relatives, starting new terms at universities and schools, that final mixing is under way. It should not be a terrifying process. It happens with every new virus, flu included. It’s just that we’ve never before in our history chased it around the countryside with a technique more suited to the biology lab than to a supermarket car park.
A very long prelude, but necessary. Part of the ‘project fear’ that is rather too obvious, involving second waves, has been the daily count of ‘cases’. Its important to understand that, according to the infectious disease specialists I’ve spoken to, the word ‘case’ has to mean more than merely the presence of some foreign organism. It must present signs (things medics notice) and symptoms (things you notice). And in most so-called cases, those testing positive had no signs or symptoms of illness at all. There was much talk of asymptomatic spreading, and as a biologist this surprised me. In almost every case, a person is symptomatic because they have a high viral load and either it is attacking their body or their immune system is fighting it, generally a mix. I don’t doubt there have been some cases of asymptomatic transmission, but I’m confident it is not important.
That all said, Government decided to call a person a ‘case’ if their swab sample was positive for viral RNA, which is what is measured in PCR. A person’s sample can be positive if they have the virus, and so it should. They can also be positive if they’ve had the virus some weeks or months ago and recovered. It’s faintly possible that high loads of related, but different coronaviruses, which can cause some of the common colds we get, might also react in the PCR test, though it’s unclear to me if it does.
But there’s a final setting in which a person can be positive and that’s a random process. This may have multiple causes, such as the amplification technique not being perfect and so amplifying the ‘bait’ sequences placed in with the sample, with the aim of marrying up with related SARS-CoV-2 viral RNA. There will be many other contributions to such positives. These are what are called false positives.
Think of any diagnostic test a doctor might use on you. The ideal diagnostic test correctly confirms all who have the disease and never wrongly indicates that healthy people have the disease. There is no such test. All tests have some degree of weakness in generating false positives. The important thing is to know how often this happens, and this is called the false positive rate. If 1 in 100 disease-free samples are wrongly coming up positive, the disease is not present, we call that a 1% false positive rate. The actual or operational false positive rate differs, sometimes substantially, under different settings, technical operators, detection methods and equipment. I’m focusing solely on the false positive rate in Pillar 2, because most people do not have the virus (recently around 1 in 1000 people and earlier in summer it was around 1 in 2000 people). It is when the amount of disease, its so-called prevalence, is low that any amount of a false positive rate can be a major problem. This problem can be so severe that unless changes are made, the test is hopelessly unsuitable to the job asked of it. In this case, the test in Pillar 2 was and remains charged with the job of identifying people with the virus, yet as I will show, it is unable to do so.
Because of the high false positive rate and the low prevalence, almost every positive test, a so-called case, identified by Pillar 2 since May of this year has been a FALSE POSITIVE. Not just a few percent. Not a quarter or even a half of the positives are FALSE, but around 90% of them. Put simply, the number of people Mr Hancock sombrely tells us about is an overestimate by a factor of about ten-fold. Earlier in the summer, it was an overestimate by about 20-fold.
Let me take you through this, though if you’re able to read Prof Carl Heneghan’s clearly written piece first, I’m more confident that I’ll be successful in explaining this dramatic conclusion to you. (Here is a link to the record of numbers of tests, combining Pillar 1 (hospital) and Pillar 2 (community).)
Imagine 10,000 people getting tested using those swabs you see on TV. We have a good estimate of the general prevalence of the virus from the ONS, who are wholly independent (from Pillar 2 testing) and are testing only a few people a day, around one per cent of the numbers recently tested in Pillar 2. It is reasonable to assume that most of the time, those being tested do not have symptoms. People were asked to only seek a test if they have symptoms. However, we know from TV news and stories on social media from sampling staff, from stern guidance from the Health Minister and the surprising fact that in numerous locations around the country, the local council is leafleting people’s houses, street by street to come and get tested.
The bottom line is that it is reasonable to expect the prevalence of the virus to be close to the number found by ONS, because they sample randomly, and would pick up symptomatic and asymptomatic people in proportion to their presence in the community. As of the most recent ONS survey, to a first approximation, the virus was found in 1 in every 1000 people. This can also be written as 0.1%. So when all these 10,000 people are tested in Pillar 2, you’d expect 10 true positives to be found (false negatives can be an issue when the virus is very common, but in this community setting, it is statistically unimportant and so I have chosen to ignore it, better to focus only on false positives).
So, what is the false positive rate of testing in Pillar 2? For months, this has been a concern. It appears that it isn’t known, even though as I’ve mentioned, you absolutely need to know it in order to work out whether the diagnostic test has any value! What do we know about the false positive rate? Well, we do know that the Government’s own scientists were very concerned about it, and a report on this problem was sent to SAGE dated June 3rd 2020. I quote: “Unless we understand the operational false positive rate of the UK’s RT-PCR testing system, we risk over-estimating the COVID-19 incidence, the demand on track and trace and the extent of asymptomatic infection”. In that same report, the authors helpfully listed the lowest to highest false positive rate of dozens of tests using the same technology. The lowest value for false positive rate was 0.8%.
Allow me to explain the impact of a false positive rate of 0.8% on Pillar 2. We return to our 10,000 people who’ve volunteered to get tested, and the expected ten with virus (0.1% prevalence or 1:1000) have been identified by the PCR test. But now we’ve to calculate how many false positives are accompanying them. The shocking answer is 80. 80 is 0.8% of 10,000. That’s how many false positives you’d get every time you were to use a Pillar 2 test on a group of that size.
The effect of this is, in this example, where 10,000 people have been tested in Pillar 2, could be summarised in a headline like this: “90 new cases were identified today” (10 real positive cases and 80 false positives). But we know this is wildly incorrect. Unknown to the poor technician, there were in this example, only 10 real cases. 80 did not even have a piece of viral RNA in their sample. They are really false positives.
I’m going to explain how bad this is another way, back to diagnostics. If you’d submitted to a test and it was positive, you’d expect the doctor to tell you that you had a disease, whatever it was testing for. Usually, though, they’ll answer a slightly different question: “If the patient is positive in this test, what is the probability they have the disease?” Typically, for a good diagnostic test, the doctor will be able to say something like 95% and you and they can live with that. You might take a different, confirmatory test, if the result was very serious, like cancer. But in our Pillar 2 example, what is the probability a person testing positive in Pillar 2 actually has COVID-19? The awful answer is 11% (10 divided by 80 + 10). The test exaggerates the number of covid-19 cases by almost ten-fold (90 divided by 10). Scared yet? That daily picture they show you, with the ‘cases’ climbing up on the right-hand side? Its horribly exaggerated. Its not a mistake, as I shall show.
Earlier in the summer, the ONS showed the virus prevalence was a little lower, 1 in 2000 or 0.05%. That doesn’t sound much of a difference, but it is. Now the Pillar 2 test will find half as many real cases from our notional 10,000 volunteers, so 5 real cases. But the flaw in the test means it will still find 80 false positives (0.8% of 10,000). So its even worse. The headline would be “85 new cases identified today”. But now the probability a person testing positive has the virus is an absurdly low 6% (5 divided by 80 + 5). Earlier in the summer, this same test exaggerated the number of COVID-19 cases by 17-fold (85 divided by 5). Its so easy to generate an apparently large epidemic this way. Just ignore the problem of false positives. Pretend its zero. But it is never zero.
This test is fatally flawed and MUST immediately be withdrawn and never used again in this setting unless shown to be fixed. The examples I gave are very close to what is actually happening every day as you read this.
I’m bound to ask, did Mr Hancock know of this fatal flaw? Did he know of the effect it would inevitably have, and is still having, not only on the reported case load, but the nation’s state of anxiety. I’d love to believe it is all an innocent mistake. If it was, though, he’d have to resign over sheer incompetence. But is it? We know that internal scientists wrote to SAGE, in terms, and, surely, this short but shocking warning document would have been drawn to the Health Secretary’s attention? If that was the only bit of evidence, you might be inclined to give him the benefit of the doubt. But the evidence grows more damning.
Recently, I published with my co-authors a short Position Paper. I don’t think by then, a month ago or so, the penny had quite dropped with me. And I’m an experienced biomedical research scientist, used to dealing with complex datasets and probabilities.
On September 11th 2020, I was a guest on Julia Hartley-Brewer’s talkRADIO show. Among other things, I called upon Mr Hancock to release the evidence underscoring his confidence in and planning for ‘the second wave’. This evidence has not yet been shown to the public by anyone. I also demanded he disclose the operational false positive rate in Pillar 2 testing.
On September 16th, I was back on Julia’s show and this time focused on the false positive rate issue (1m 45s – 2min 30s). I had read Carl Heneghan’s analysis showing that even if the false positive rate was as low as 0.1%, 8 times lower than any similar test, it still yields a majority of false positives. So, my critique doesn’t fall if the actual false positive rate is lower than my assumed 0.8%.
On September 18th, Mr Hancock again appeared, as often he does, on Julia Hartley-Brewer’s show. Julia asked him directly (1min 50s – on) what the false positive rate in Pillar 2 is. Mr Hancock said “It’s under 1%”. Julia again asked him exactly what it was, and did he even know it? He didn’t answer that, but then said “it means that, for all the positive cases, the likelihood of one being a false positive is very small”.
That is a seriously misleading statement as it is incorrect. The likelihood of an apparently positive case being a false positive is between 89-94%, or near-certainty. Of note, even when ONS was recording its lowest-ever prevalence, the positive rate in Pillar 2 testing never fell below 0.8%.
It gets worse for the Health Secretary. On September the 17th, I believe, Mr Hancock took a question from Sir Desmond Swayne about false positives. It is clear that Sir Desmond is asking about Pillar 2.
Mr Hancock replied: “I like my right honourable friend very much and I wish it were true. The reason we have surveillance testing, done by ONS, is to ensure that we’re constantly looking at a nationally representative sample at what the case rate is. The latest ONS survey, published on Friday, does show a rise consummate (sic) with the increased number of tests that have come back positive.”
He did not answer Sir Desmond’s question, but instead answered a question of his choosing. Did the Health Secretary knowingly mislead the House? By referring only to ONS and not even mentioning the false positive rate of the test in Pillar 2 he was, as it were, stealing the garb of ONS’s more careful work which has a lower false positive rate, in order to smuggle through the hidden and very much higher, false positive rate in Pillar 2. The reader will have to decide for themselves.
Pillar 2 testing has been ongoing since May but it’s only in recent weeks that it has reached several hundreds of thousands of tests per day. The effect of the day by day climb in the number of people that are being described as ‘cases’ cannot be overstated. I know it is inducing fear, anxiety and concern for the possibility of new and unjustified restrictions, including lockdowns. I have no idea what Mr Hancock’s motivations are. But he has and continues to use the hugely inflated output from a fatally flawed Pillar 2 test and appears often on media, gravely intoning the need for additional interventions (none of which, I repeat, are proven to be effective).
You will be very familiar with the cases plot which is shown on most TV broadcasts at the moment. It purports to show the numbers of cases which rose then fell in the spring, and the recent rise in cases. This graph is always accompanied by the headline that “so many thousands of new cases were detected in the last 24 hours”.
You should know that there are two major deceptions, in that picture, which combined are very likely both to mislead and to induce anxiety. Its ubiquity indicates that it is a deliberate choice.
Firstly, it is very misleading in relation to the spring peak of cases. This is because we had no community screening capacity at that time. A colleague has adjusted the plot to show the number of cases we would have detected, had there been a well-behaved community test capability available. The effect is to greatly increase the size of the spring cases peak, because there are very many cases for each hospitalisation and many hospitalisations for every death.
Secondly, as I hope I have shown and persuaded you, the cases in summer and at present, generated by seriously flawed Pillar 2 tests, should be corrected downwards by around ten-fold.
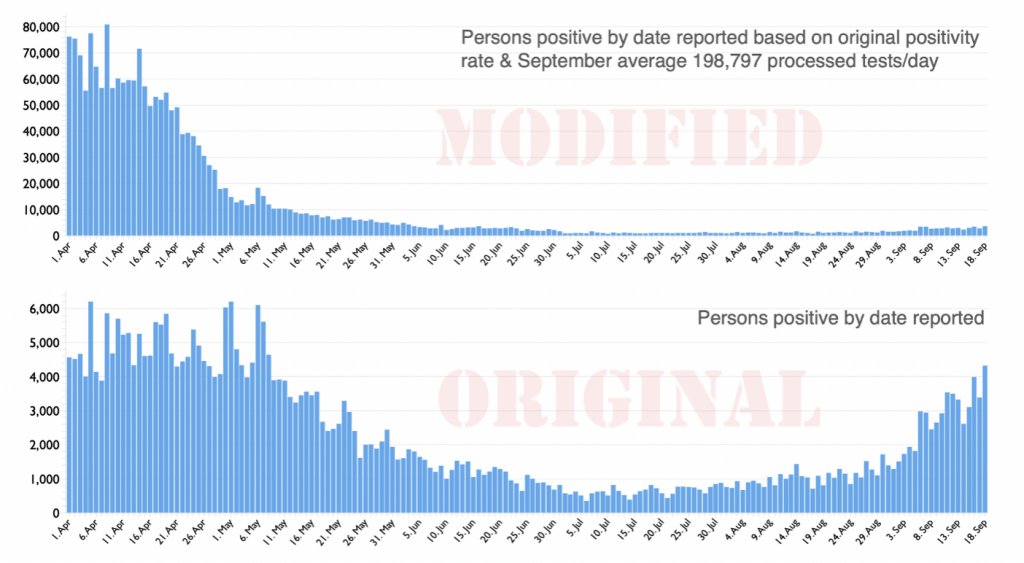
I do believe genuine cases are rising somewhat. This is, however, also true for flu, which we neither measure daily nor report on every news bulletin. If we did, you would appreciate that, going forward, it is quite likely that flu is a greater risk to public health than COVID-19. The corrected cases plot (above) does, I believe, put the recent rises in incidence of COVID-19 in a much more reasonable context. I thought you should see that difference before arriving at your own verdict on this sorry tale.
There are very serious consequences arising from grotesque over-estimation of so-called cases in Pillar 2 community testing, which I believe was put in place knowingly. Perhaps Mr Hancock believes his own copy about the level of risk now faced by the general public? Its not for me to deduce. What this huge over-estimation has done is to have slowed the normalisation of the NHS. We are all aware that access to medical services is, to varying degrees, restricted. Many specialities were greatly curtailed in spring and after some recovery, some are still between a third and a half below their normal capacities. This has led both to continuing delays and growth of waiting lists for numerous operations and treatments. I am not qualified to assess the damage to the nation’s and individuals’ health as a direct consequence of this extended wait for a second wave. Going into winter with this configuration will, on top of the already restricted access for six months, lead inevitably to a large number of avoidable, non-Covid deaths. That is already a serious enough charge. Less obvious but, in aggregate, additional impacts arise from fear of the virus, inappropriately heightened in my view, which include: damage to or even destruction of large numbers of businesses, especially small businesses, with attendant loss of livelihoods, loss of educational opportunities, strains on family relationships, eating disorders, increasing alcoholism and domestic abuse and even suicides, to name but a few.
In closing, I wish to note that in the last 40 years alone the UK has had seven official epidemics/pandemics; AIDS, Swine flu, CJD, SARS, MERS, Bird flu as well as annual, seasonal flu. All were very worrying but schools remained open and the NHS treated everybody and most of the population were unaffected. The country would rarely have been open if it had been shut down every time.
I have explained how a hopelessly-performing diagnostic test has been, and continues to be used, not for diagnosis of disease but, it seems, solely to create fear.
This misuse of power must cease. All the above costs are on the ledger, too, when weighing up the residual risks to society from COVID-19 and the appropriate actions to take, if any. Whatever else happens, the test used in Pillar 2 must be immediately withdrawn as it provides no useful information. In the absence of vastly inflated case numbers arising from this test, the pandemic would be seen and felt to be almost over.
Dr Mike Yeadon is the former CSO and VP, Allergy and Respiratory Research Head with Pfizer Global R&D and co-Founder of Ziarco Pharma Ltd.
Top UK scientists urge govt to protect most vulnerable from Covid-19 instead of carpet-bombing virus
RT | September 21, 2020
The UK should focus on helping the most vulnerable – including residents in care homes worst affected by Covid-19 – instead of pursuing an “unfeasible” goal of suppressing the virus until a vaccine arrives, top scientists urged.
British scholars penned an open letter to PM Boris Johnson, Chancellor of the Exchequer Rishi Sunak, as well as health chiefs in England, Scotland, Wales and Northern Ireland, asking them to urgently reconsider the current epidemic strategy.
Authored by Oxford professors Sunetra Gupta and Carl Heneghan, as well as Karol Sikora of the University of Buckingham and Sam Williams of the Economic Insight consultancy, the letter says the “existing policy path is inconsistent with the known risk-profile of Covid-19.” The appeal has been signed by dozens of academics from the UK’s leading educational institutions.
“The unstated objective currently appears to be one of suppression of the virus, until such a time that a vaccine can be deployed. This objective is increasingly unfeasible… and is leading to significant harm across all age groups, which likely offsets all benefits.”
The letter comes days after Health Secretary Matt Hancock pledged “to do what it takes” in order to fight Covid-19. After the UK recorded close to 4,000 confirmed coronavirus cases on Sunday, the government is considering a “circuit-breaking” period of tightened measures which could be announced later this week, UK media revealed.
Such a move could reportedly involve bringing back restrictions in public spaces for a few weeks, most of which were relaxed throughout May and June. Pubs and restaurants could be mandated to close earlier across the country, but schools and most workplaces would be kept open. Closing some parts of the hospitality industry is also one of the options.
According to the authors of the open letter, blanket measures aren’t the way to go. “Instead, more targeted measures that protect the most vulnerable from Covid, whilst not adversely impacting those not at risk, are more supportable,” they wrote.
“Given the high proportion of Covid-19 deaths in care homes, these should be a priority,” the scientists pointed out. The pandemic hit the UK’s nursing facilities exceptionally hard, claiming 19,394 lives between March and June, which accounted for 29.3 percent of all deaths in care homes during that time, according to government figures.
Last month, it emerged that care home staff were allegedly pressured by the NHS to admit coronavirus-positive or untested patients at the height of the crisis this spring. Nurses were reportedly instructed to change the status of all residents to “do not resuscitate.”
However, the government seems to have learned its lesson. Care facilities will receive £546 million ($702.5 million) to upgrade, reduce all but essential movements of staff between nursing homes to prevent the spread of the virus, and allow for the distribution of free PPE – masks and gloves – to the elderly and workers.
The UK has reported more than 394,000 coronavirus cases since the start of the epidemic, claiming close to 42,000 lives.
Featured Video
House Resolution Calls for Tech Companies to Censor Speech
or go to
Aletho News Archives – Video-Images
Book Review
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran unveils new control measures over Strait of Hormuz transit
- House Resolution Calls for Tech Companies to Censor Speech
- Ceasefire no longer viable after 200 days of Israeli violations: Hamas
- Israeli strikes intensify across southern Lebanon, casualties reported
- Left in Disbelief: Israel in Panic over Hezbollah FPV Drone Nightmare
- Trump Taps Israel Lobbyist From Mossad Cutout FDD To Join Iran Negotiations
- Trump’s Blockade Snatches Defeat from the Jaws of Victory
- Geopolitics and Geoeconomics of the Strait of Hormuz
- Mali: a new front in the Western war on multipolarism
- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- If Americans Knew
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
