The Historic Suppression of Scientific Debate in COVID
Never before in modern history have entire topics in Medicine been actively prevented from discussion in public forums
By Pierre Kory, MD, MPA | Medical Musings | August 30, 2022
I started reading about the definition, history, and legal background of censorship. The entry on Wikipedia (ugh) was quite revealing:
Censorship is the suppression of speech, public communication, or other information. This may be done on the basis that such material is considered objectionable, harmful, or sensitive. Censorship can be conducted by governments, private institutions and other controlling bodies.
But get this, look at the examples of topics that have traditionally been censored:
General censorship occurs for a variety of claimed reasons including national security, to control obscenity, pornography, and hate speech, to protect children or other vulnerable groups, to promote or restrict political or religious views, and to prevent slander and libel.
Note that “scientific opinion” is not on there. Because scientific data nor interpretations of that data, should ever be considered offensive. You can argue that wrong interpretations of data can be harmful, but debate is how you resolve that, not censorship! Science literally rests on open debate and the sharing of data and exchanging of interpretations amongst not only experts, but the wider public.
Now, also from Wikipedia:
Censorship has been criticized throughout history for being unfair and hindering progress. Censorship is counterproductive as it prevents the censored topic from being discussed. Those who impose censorship must consider what they censor to be true, as individuals believing themselves to be correct would welcome the opportunity to disprove those with opposing views (just ask Steve Kirsch).
But again, science is not on there as a category of discourse to censor. Although history is replete with attempts to censor individuals with scientific views contrary to established orthodoxy, in all the instances I can think of, the person being censored was eventually proven correct! Galileo (earth is round), Seimelwess (importance of handwashing), Scopes (teaching of evolutionary theory) etc.
Yet, in the last 2 years we have undergone a massive censorship of the discussion and sharing of scientific data in public forums. I believe this was the proximate cause of what can now only be viewed as humanitarian catastrophes resulting from 1) the suppression of knowledge of early treatment with effective repurposed drugs and 2) the suppression of data showing the toxicity, lethality, and ineffectiveness of the vaccines.
This period should serve as one of the most damning arguments against censorship.
We were not allowed to openly discuss our data or our interpretations and applications of that scientific data (i.e. scientific opinions) in major media or social media. The journalist Matt Taibbi called me “the ghost of the internet” because whenever I had scientific discussions with folks who are now dear friends and colleagues, their content and podcasts were de-platformed or demonetized (as in the case of my dear friend Dr. Been), and/or they immediately founds their posted videos of those discussions taken down, like immediately (the speed in which I “disappeared” was astonishingly fast at times). All because we had a scientific discussion where I had shared data and interpretations of that data. I was honored with the opportunity to make my case in front of some truly expert and deep thinkers. Folks who could challenge me, ask questions, express concerns or offer alternative interpretations or hypotheses. I would say that the only problem with those discussions is that the data in support of ivermectin was just so overwhelming. It is a drug with proven efficacy in COVID. Note that conclusion is shared by some of the most highly published doctors in the history of our specialty (the FLCCC) as well as by a group of some of the top evidence-based medicine researchers in the world (Tess Lawrie, Andrew Bryant, Edmund Fordham et al. of EBMc2).
And therein lay the problem. The data could not be debated because any other interpretation than ivermectin being effective was pretty much indefensible in the face of a mountain of repeatedly and almost universally supportive data from myriad sources. So, instead, such discussions were banned from wider public view. Strong move. I think the only thing that saved a good portion of humanity was that individual and organizational websites (like the FLCCC’s, AAPS, c19early.com, and others) were largely secure and not taken down or booted off of hosting servers. But I imagine they could have been.
So, in COVID, Big Pharma and Big Government literally got media companies to shut down debate and discussion on certain topics like HCQ and IVM and vaccine toxicity and ineffectiveness. See YouTube’s community guidelines, which are so absurd, I literally turn purple with rage every time I read it. But it is also sort of comical because they literally put it in writing, right out in the open, plain to see, essentially saying “thou shalt not discuss these medicines on our platform.” And they did it while their efficacy was still being debated. In a global pandemic with thousands dying each day. Safe medicines.
Check it out:
Insane. Crazy town. Clown world. Now, keep in mind that these “guidelines” restricting any discussion of the efficacy, even potential efficacy during a global pandemic, were employed by every major media company in the world with few exceptions, like Trial Site News (although massively impactful, not yet “major media”) and maybe on a few occasions Fox News or some conservative radio hosts.
But all was not lost. Independent podcasters and some radio hosts saved the day, contributing to the dissemination of life-saving information to millions of people in this country and world. Folks like Bret Weinstein, Joe Rogan, John Campbell, Dr. Been, Dr. Mercola, Greg Hunter, Vicki McKenna and countless others. But the print and TV media giants did not have that policy written and made public for all to see (and laugh at). It was under the table, understood by all media that ivermectin should instead only be referred to as a horse dewormer. Not subtle. Alex Berenson’s recent sharing of evidence that the White House was behind his Twitter de-platforming shows how high up the censorship was coming from.
So you literally had the government and Pharma pressuring all the media and social media giants (all of them – Facebook, Linked in, Instagram, Twitter etc) to outlaw, yes, outlaw discussion of even the possibility these medications were effective. Never, ever forget this. Note how YouTube wrote that their guidelines were based on WHO recommendations. Control the top, you control everything beneath it. Read my detailed deep dive uncovering the corruption of ivermectin at the WHO here and here.
Now, one of the reasons Paul Marik was such a famous critical care doctor is that he had long been successful at debunking prevailing orthodoxy supporting standard of care practices in our specialty. He did it via lecturing and debating at national conferences and in publications within medical journals. It was how he and I met, when he congratulated me on an editorial I wrote in a major journal, where I argued against using ultrasound to measure the size of the inferior vena cava to estimate central venous pressure (CVP), largely drawing on the science and rationale he had compiled and published.
Talking to Paul this morning, he told me he is most proud of his work (note he accomplished this feat on his own) in teaching a global generation of critical care doctors that measuring the CVP to estimate the fluid needs of a patient was useless outside of a very narrow set of circumstances like hemorrhage (in those circumstances though, you don’t need the CVP to estimate fluid needs as the patients vitals and clinical presentation will tell you all you need to do.
You have to understand that the CVP was used for decades by critical care doctors in ICU patients who were in states of shock (dangerously low blood pressure). It was the standard of care in ICU’s. Paul did a deep dive into the published literature and especially into the complex physiology of the factors which influence CVP and wrote pretty much the coolest and most impactful paper ever called “Does Central Venous Pressure Predict Fluid Responsiveness?: A Systematic Review of the Literature and the Tale of Seven Mares.” The papers most memorable sentence was “the only study we could find demonstrating the utility of CVP in predicting volume status was performed in seven standing, awake mares undergoing controlled hemorrhage.” Brilliant. Funny.
His paper triggered fierce and I mean, fierce debate in critical care… for years. Reversing established orthodoxy in medicine (and anywhere really) is nearly impossible. But Paul singlehandedly pulled it off with his papers and lectures (helped by a lot of folks like me who followed his work closely). I would argue that today, the obsession with using the CVP to guide fluid resuscitation has largely (but never completely) been abandoned. Wow.
But, again, back then, you could have “debates” on controversial topics, in fact, such topics demanded them! I remember when the United Hospital Fund used to put on this terrific conference in Manhattan where they invited experts in the field to debate “controversies” in critical care (like CVP). Each speaker was given ten minutes and were assigned the pro side or the con side of a topic, but the assigned debaters could not choose the side to argue! After both speakers were heard, the audience voted on which conclusion was based on the more compelling data and argument. I was invited several years in a row and sometimes had to argue the side I was not on intellectually. Which made it even more enlightening an exercise – imagine getting Berenson to have to argue in support of ivermectin? It just might happen that he learns something important. Also, it was a “hard” ten minutes they gave you. So much so, I remember one year I got the whole room laughing because I did not shut up when the big timer hit ten minutes and the big red stoplight turned on, so a close colleague of mine ran up to the podium, put me in a headlock and started to drag me away from the podium as I was still yelling my final points. That was fun. Now, not so much.
More trips down the memory lane of debates. One of the first “corruptions” by Pharma that I experienced in my career was when Eli Lilly invented a national campaign called “Surviving Sepsis” in an attempt to create guidelines supporting optimal care practices. They involved all the professional societies in critical care to participate. Leaders in the field all with a seat at the table.
Yep, you guessed it, it turned out to be cover for their efforts in making a $5,000 harmful drug (Xygris) the standard of care in sepsis. Every single one of those committee members got money. The entire campaign and strategy was developed by a PR firm. Recall that Disinformation tactics were first invented by a PR firm in the 1950’s working for the Tobacco Industry at a time when their products were starting to look bad in the scientific literature.
I would argue that Pharma is the most skilled practitioner of Disinformation amongst all industries. I mean 20 years ago already, the entire country’s critical care doctors gave a very expensive, harmful drug to every septic patient for years based on a manipulated trial with the tiniest of mortality benefits amidst a splashy “public health” campaign concocted by a PR firm working for a pharmaceutical company.
When Xygris was eventually shown to be harmful it was abandoned. But that decision occurred on the back of fierce debates and constant re-analysis and discussion of the accumulating data. Hmm, I wonder when that will happen to Remdesivir? Fun fact: during my fellowship training in pulmonary and critical care, my mentors, Dr. Paul Mayo and Dr. Samual Acquah essentially forbade the use of Xygris at a time when every other fellow in training was using it like water. I never once ordered it for any patient.
But there were other controversial aspects of the sepsis guidelines that Paul was a beast in demolishing at national conferences. He was so good, his take on the data so expert and compelling that his lectures were always packed, like standing room only type packed. For a medical lecture.
The most debated aspect of sepsis treatment (and yes, it was debated repeatedly at national conferences) was called “early goal directed therapy” (EGDT) which required that you resuscitate patients using fluids and vasopressors to a target central venous pressure (CVP) and a target central venous oxygen saturation (SCV02), but to monitor the latter continuously, you had to insert a special catheter into the large neck veins to do it. I will not go into the detailed physiology of those parameters but the need to measure them was nonsense.
I knew it (even as a fellow), my mentors knew it, Paul knew it, yet EGDT was widely adopted across the country and world. The protocol was based on a single center study whose Principal Investigator Manny Rivers held the patent on that catheter (unknown by most at the time). Further, information later came out that the data were manipulated. That information was leaked by a whistleblower who was a fellow of Rivers at the time. The fellow was threatened by the hospital with the ending of his career if he were to continue to speak publicly about it. They even apparently threatened to “kill his kids.”
But the point is, the debates were fierce, in the open, and at conferences and hospital auditoriums across the country and world. They were data driven arguments by experts with decades of scientific inquiry and clinical expertise who reviewed the physiology and published literature. And sometimes led to conflicting interpretations. Yes, we all had biases when interpreting the data (all humans do), but we debated. It was not outlawed to say that SCV02 and IVC were unnecessary. Or to say they were critical. And you were not forced to use all aspects of EGDT in the care of patients back then as they were just “guidelines,” not rigid protocols supported by Federal government funded bonuses in every patient you used it in like we have now with Remdesivir.
Interestingly, widespread EGDT adoption actually showed consistent impacts in reducing mortality, but we knew it was not from the targeting of those parameters but instead just from the early recognition and resuscitation of sepsis. Might even be the one instance in history where a corrupt action by Big Pharma actually led to a benefit in public health. Anyway, eventually studies showed that targeting those parameters versus simply using clinical judgement led to the same outcomes and the practice was abandoned. Paul was right again.
Another aspect of the U.S resuscitation guidelines that Paul was absolutely brilliant in debunking was the decision to target a reduction in lactate as a resuscitation endpoint. This was another fiction like the CVP. Again, almost all of emergency and critical care medicine had been indoctrinated with the physiologic concept that lactate is a marker of hypo-perfusion (reduction in blood flow to organs). Now, in certain, specific clinical instances (ischemic bowel etc), a rise in lactate can reflect hypo-perfusion. But in most septic patients it is simply a marker of illness and stress. It is not harmful, in fact, if anything, lactate is better utilized by organs to maintain function and energy. However, doctors were taught to target lactate as a resuscitation endpoint instead of simply interpreting it as a marker of disease severity.
But, in this instance, that practice and belief was not the result of corruption. No-one as far as I can tell was making money off of dumb doctors and nurses being forced to check lactates repeatedly. It simply stemmed from ignorance and established practice, with leading “experts” (dotards) arrogantly teaching that it was important to target (because they were taught that and did not critically think about it). Paul’s research revealed that targeting lactate was the result of a gross misunderstanding of lactic acid physiology. It was again one of the most masterful papers I have read. He marshaled tons of physiologic knowledge and logically presented the concepts and data which defined the cause and purpose of lactic acid production.
Just like with his teachings on CVP, again you had one man arguing against an entire generation of doctors who believed that reducing lactate was important in the general septic patient. I totally agreed with Paul’s papers and conclusions. Which made my life difficult because I tried in vain to disseminate this knowledge among my trainees, trying to stop what I saw as the pervasive “lacto-bolo reflex” they were all exhibiting. Paul actually invented the term, and it was brilliant: “bolo” refers to a bolus of fluids, and the “reflex” was the ordering of an infusion of a half liter or liter of fluids every time a high lactate was measured.
Lacto-bolo reflexes unfortunately led to what he also brilliantly coined as “salt water drowning,” i.e the receipt of excessive amounts of saline fluids by patients. Every time a doctor or nurse received a report of a high lactate… the doc ordered fluids. Lacto-bolo reflex. What is crazy is that the excess fluid administration that resulted paradoxically worsened kidney function and led to more kidney failure despite the fact the doctors were trying to preserve kidney function with fluid infusions! It was insane and I knew it because of Paul’s research and teaching. I also tried for years to fight the lacto-bolo reflex in my trainees and colleagues with little success except for when I was physically present in the ICU. When I went home for the night though, my fellows and residents all continued with their lacto-bolo reflexes. When the cat’s away the mice will play.
However, in this instance, despite Paul’s papers and lectures on the topic, the unthinkable became true. “Experts” (dotards) eventually established the checking of repeated lactate as a national quality of care standard. Those standards are what hospitals are judged on which affects their reimbursement and accreditation.
So, doctors across the country are now literally mandated to repeatedly check and respond to lactates in septic patients. Again, another example of an orthodoxy based on fiction. Despite all of Pauls efforts in teaching, lecturing, and publishing on the topic, this time, he was unsuccessful in changing orthodoxy. He may have been if his career didn’t end but History marches on. I would argue that his efforts in singlehandedly trying to reverse orthodoxies unfounded by “the science” led to a widespread respect, admiration, and reverence for the deep knowledge and scientific acumen he consistently displayed. But not so much anymore it seems.
And that is solely because Paul’s final effort in academic medicine was in trying to reverse the fiction that ivermectin was ineffective in COVID. That effort ended his career because for the first time, unrealized by him at the time, instead of fighting ignorant knowledge of physiology, he was poking The Bear, i.e tackling a subject that threatened Big Pharma. In a big, big way. Thus, that effort ended his career. But let’s be specific about that – his former hospital (SENTARA GENERAL IN NORFOLK, VIRGINA) was the one who actually ended his career.
Now, how they ended it is pretty interesting, as my last job was ended in the same way. They did it by using a process that hospitals have long employed when a physician “doesn’t toe the line.” In COVID, Paul was a clinical leader in a major hospital and was employing a highly effective protocol using a combination of repurposed drugs and not using Remdesivir. And he was vocal about it. And he was teaching the doctors in training about the harms of Remdesivir and all of the data supporting “unapproved therapies.” So, they invoked a process called “sham peer review” to get rid of him. What the heck is “sham peer review?”
From a seminal paper on the topic:
In 1986, the United States Congress enacted the Healthcare Quality Improvement Act (HCQIA). which granted immunity to hospitals and reviewers participating in “good faith” peer review of physicians and dentists. These reviews were envisioned to be vehicles by which it could be determined if any actions or recommendations against a physician should become necessary on the measures of incompetence, unprofessional conduct, or behaviors that impact the doctors’ clinical privileges. However, of late, HCQIA has resulted in many unforeseen consequences, not the least of which is the rise of ‘sham peer reviews’ —and the consignment of guiltless, lifesaving, pre-eminent physicians into obscurity.
What is “Sham” Peer Review?
Sham peer review is an adverse action taken in bad faith by a hospital for purposes other than the furtherance of quality health care. It is a process that is disguised to look like legitimate peer review. But sham peer review is not objectively reasonable, precisely because it is not performed to advance the quality of health care (violation of safe harbor provision).
A sham peer review happens when the hospital invents some pretext on which to attack the physician and acts to disguise the adverse action against the targeted physician by conducting a such a review—where the truth and the facts do not matter, because the process is contrived to be rigged, and the outcome is predetermined.
Over the years, sham peer reviews have unfortunately become fairly well-known. Hospitals in the United States have mounted these proceedings for at least four decades to rid themselves of physicians who “get in their way.” Often, they are doctors who don’t ”follow the party line” and whom they consider “disruptive.” Hospital officials are resistant to physicians who bring patient safety or care quality concerns to their attention. Some hospitals retaliate against these whistleblowers, by instigating these sham peer reviews.
How Sham Peer Review works
Hospitals that use sham peer review bring trumped up, fabricated, and thoroughly false charges against the targeted physician. Although no court of law would permit depriving an accused person of files or records needed to defend himself, as it is fundamentally unfair and in violation of due process, hospitals that employ sham peer review frequently refuse to provide records required to the physician under review. Based on these totally erroneous and phony charges the physician’s hospital privileges are summarily suspended. The physician is usually given 14 days to respond in writing to the sham charges. The charges and the physician’s response are then supposedly shared with the Medical Executive Committee (MEC). The physician then meets with the Medical Executive Committee. The physician is usually denied legal representation (which is unlawful), and the meeting takes the form of a Kangaroo court.
And the above, is EXACTLY what happened to Paul. Like.. to the T. Most importantly, he had no rights during the process. No ability to bring a lawyer in to help defend him. No ability to discover the identity of the complainant or exact documentation of the complaint. That is how they can just make shit up.
I won’t go into the details because the above explains everything that happened to Paul but his was particularly egregious (mine was short and simple). They generated at least 8 anonymous, invented complaints by other providers, nurses and employees inventing things he said or did and characterizing his behavior as “disruptive.” He had never gotten a single complaint from a patient or colleague in his entire career. They even accused him of malpractice for treating a patient for severe COVID who had tested negative for COVID. I saw the patient’s films and labs, heard his history, and presentation. The guy had COVID, period. Plus, the guy was super sick, on a ventilator, and Paul saved him with his protocol. No small feat for a COVID patient on a ventilator. The patient survived yet the hospital used the case as a mark against him. Insane.
Everything was right out of the sham peer review playbook. And it resulted in the ending of his career.
My “sham peer review” was different given that I was working as an independent contractor running an ICU for a hospital in central Wisconsin. The hospital administration had been asking my partners who hired me to get rid of me as soon as they heard I had been hired, likely due to my public profile (ya think?). My partners refused as we got along great and they deeply appreciated my skills, contributions, COVID expertise and protocols. They told the administration “if he goes, we go.” And this was a hospital with a long track record of difficulty recruiting physicians. Yet, my partners were continually harassed by the administration who kept sending them “hit pieces” they found about me in newspapers and magazines.
Six months later, in November 2021, the Chief Medical Officer of the hospital knew I was not vaccinated and that a mandate was about to start. So he called me and asked if I was going to be vaccinated because he had to plan for contingencies. I asked him for a couple of days to think about it. I decided I would just get a vaccine card instead. Not proud of that plan but I knew the vaccines were built on unconscionable lies. He called me two days later, and I told him I would get vaccinated.
The next morning after my shift, my lead partner called and told me “they didn’t need me anymore.” I asked what happened (I knew they needed me, badly). He explained that I had told some ER patient to not get vaccinated and that their practice believed in vaccination so could not be associated with someone who was not. One catch – I had not been in the ER for two weeks. I defended myself, to no avail. My partner knew I was telling the truth, but I knew he was likely under an ultimatum. He apologized and said, “I am so sorry, but there is a war going on and you are unfortunately a casualty of that.” We said pleasant goodbyes and wished each other well. Pretty quick sham peer review because I was not an employee so they had the right to cancel my contract at anytime. Done. Gone.
So, as you can see from the above, COVID is not our first rodeo battling ignorance and corruption in Medicine. But we battled with debate using data, published literature, and deep knowledge of physiology. Now, no more.
Steve Kirsch has been offering 1-2 million dollars for anyone in academia or the agencies to participate in a public or even privately recorded, moderated debate of the evidence to support vaccine safety and efficacy. No-one took him up on it.
An organization in Kansas City asked me, Peter McCullough and two other experts to participate in a debate with the clinical leaders at KU. They refused to show. Their table sat empty on the stage while we debated the public statements they had made with a local TV program instead. They literally told the TV presenter that “we do not debate in public forums, only in journal clubs amongst fellow doctors.” Note he said this on TV then went on to support their policies citing what we know are corrupt and easily disprovable evidence-free narratives. What a farce.
Just as sad as the above is that Paul had long been invited every year by a medical education organization to lecture to anesthesiologists as he was a perennial favorite lecturer. This past year, he gave a masterful lecture on the data supporting the use of ivermectin in COVID. Soon after, he was told that he will never again be invited to give lectures.
He also gave the same lecture to the Anesthesia Department at Mass General (Harvard). The evaluations by attendees all complained that his lecture was full of mis-information. He will never be invited back.
Twitter, which describes itself as a “public square” has de-platformed many of my colleagues (multiple times) for sharing newly emerging data supporting the efficacy of ivermectin. Hey Juan Chamie, how many times have you been Twitterwhacked? One of life’s greatest mysteries (slight overstatement) is how I am still alive on Twitter, although to be accurate, I am only half-alive as they severely shadow ban me on that platform.
I guess we just have to accept the fact that two new commandments have come down from the mountaintop:
- Thou shalt not share favorable ivermectin data in any public media sphere
- Thou shalt not present analyses of the scientific data supporting ivermectin in lectures to physicians
The world has gone mad.
Next post, I will delve more specifically into the tactics Pharma deployed in pulling off their massive Disinformation campaign against ivermectin using propaganda as well as censorship of the FLCCC .
The Great Lab Leak Cover-Up By the U.S. Government
BY WILL JONES | THE DAILY SCEPTIC | AUGUST 30, 2022
Thomas Fazi, who has a book on The Covid Consensus coming out shortly with Toby Green, has written an excellent summary in UnHerd of the evidence of a cover-up of the possible lab origin of SARS-CoV-2 by those behind the kind of research that would have produced it.
Much of the work on SARS-like CoVs performed in Wuhan was part of an active and highly collaborative U.S.-China scientific research programme funded by the U.S. Government – primarily through the National Institute of Allergy and Infectious Diseases (NIAID), directed by Anthony Fauci, which is part of the NIH – and coordinated by the U.S.-based non-governmental organisation EcoHealth Alliance (EHA). The group’s research work went beyond the simple analysis of existing coronaviruses, and actually involved the engineering of ‘chimeric’ bat coronaviruses, some of which proved to be potentially more infectious to humans – a highly risky technique known as gain-of-function.
In 2018, EcoHealth and the WIV (in collaboration with other institutions) sent a grant proposal to the Defense Advanced Research Projects Agency (DARPA), which included a plan to insert furin cleavage sites into existing bat coronaviruses – spots in the surface protein of a virus that can boost its entry into human cells. The DARPA proposal was rejected – and yet the presence of a furin cleavage site is precisely what sets SARS-CoV-2 apart from all known SARS-like coronaviruses. Did the researchers carry out the research anyway, possibly using other sources of funding? Nobel Prize-winning virologist David Baltimore stated that he considered this to be “the smoking gun for the origin of the virus”.
In light of all this, it’s hardly surprising that in the early days of the pandemic, at the highest levels of the U.S. establishment, the question of whether the virus might have been engineered at the WIV, possibly through research part-funded by the U.S. Government, was taken very seriously. As a result of an FoIA request, we know that on February 1st 2020, Anthony Fauci convened a “totally confidential” conference call with at least a dozen high-level experts from around the world, many of whom privately admitted that there was a very high probability that the virus had been artificially engineered and had then “escaped” from the Wuhan lab.
Yet not only did the NIH fail to disclose this to the public or to Congress, but the emails released under the FoIA suggest that it took an early and active role in promoting the ‘zoonotic hypothesis’ and the rejection of the laboratory-associated hypothesis. Indeed, within days of the February 1st call, a group of virologists, including some who were on it and had endorsed the ‘artificial origin’ theory, prepared the first draft of a hugely influential paper on The proximal origin of SARS-CoV-2 – subsequently published in Nature – that argued for the exact opposite.
Moreover, the NIH has resisted the release of important evidence, such as the grant proposals and project reports of EHA, and has continued to redact materials released under FoIA, including a remarkable 290-page redaction in a recent release. Even more incredibly, at some point after March 2020 a number of early SARS-CoV-2 genomic sequences were deleted from the NIH’s own archive at the request of researchers in Wuhan.
The strangeness doesn’t end here. In February 2020, an influential letter signed by 27 global experts was published in the Lancet, strongly condemning “conspiracy theories suggesting that Covid-19 does not have a natural origin”. The letter proved crucial, alongside the aforementioned Nature paper, in nipping in the bud the lab-leak hypothesis and giving the illusion of scientific consensus. In late 2020, however, emails released following a FoIA request showed that the Lancet statement had been orchestrated by one of the 27 co-authors – none other than Peter Daszak, President of EcoHealth Alliance. It was also revealed that all but one of the other 26 scientists were linked to the Wuhan lab, their colleagues or funders.
Daszak was first appointed in late 2020 as Chair of the task force created by the Lancet COVID-19 Commission with the aim of establishing none other than “the origins of COVID-19”; and shortly thereafter as the only U.S. representative to a WHO fact-finding mission to China tasked with the same goal. Unsurprisingly, both task forces found that the virus was most likely zoonotic (i.e., natural) in origin, and that transmission through a laboratory incident was extremely unlikely.
The WHO report, in particular, came under heavy criticism, leading to the establishment of a specific work group tasked with ascertaining the origins of SARS-CoV-2, the Scientific Advisory Group on the Origins of Novel Pathogens, which published its first preliminary report in June 2022. The results were inconclusive, largely because “key pieces of data” from China were missing, leading the WHO to recommend in its strongest terms yet that a deeper probe was required into whether a lab accident may be to blame. As we have seen, however, it’s not only the Chinese government that is covering up its tracks about its possible involvement in the engineering of SARS-CoV-2 – but the American one as well.
Thomas notes that a new campaign is now underway to try to finally discredit the lab-leak theory, with two new studies that purport to provide more evidence that SARS-CoV-2 came from the Huanan Seafood Market leading several outlets to claim that “the Covid lab leak theory is dead” – a claim to which the Daily Sceptic‘s Dr. Noah Carl has responded here.
The question is, with those involved having closed ranks and refusing to speak or cooperate, who can force them to reveal their secrets, or must we accept that their cover-up has succeeded?
Follow the Science or Follow the Evidence?
Comment on Lord Sumptions’s Times editorial
By Tom Jefferson and Carl Heneghan | Trust the Evidence | August 29, 2022
Throughout restrictions which Lord Sumption called a “catastrophe”, we were exposed to the mantra of “follow the science”. But unfortunately, the only “science” that seems to have been followed in the major decisions is that of modellers and government departments.
Models are akin to opinions. If they are science, the evidence they provide sits on the lowest rung of the ladder. Modellers are accountable to no one; most have never seen a patient in their lives as they have no clinical background, which impedes their understanding of how people behave. Individuals are not herds of buffalos. Some modellers have a consistent track record of getting their predictions dramatically wrong with (again) catastrophic consequences.
Since the start, we have looked at the evidence underpinning the fear-generating narrative pushed by the government, some politicians, the media and many Twitterati, who overnight forgot the principles of scientific investigation, equipoise or uncertainty and the work of many pioneers in respiratory virus epidemiology spanning a century.
The psychotic narrative rests on three legs of what we call the Covid narrative stool.
The first leg is the number of cases. We have shown that misuse of polymerase chain reaction based on a superficial understanding amplified the number of “cases” as many of these were not likely to be infectious at all.
The second leg was the hospital pressure theme. Here using data which should have been available (but is not), we have shown that up to 40% of hospital cases were infected, a phenomenon which shows no sign of abating.
The data from three devolved nations and our interpretation have been serialised on this website.
Finally deaths. A death in epidemiology is the one inevitable outcome you can observe and tally. The question is: what caused it? This is called attribution. Looking at the data from freedom of information requests made by an alert public and the response at times by patronising authorities, we counted 14 different ways of attributing deaths to Covid-19. The first prize for the most bizarre was the Care Quality Commission’s: they left it to the care provider to decide the cause of death. So it is possible that administrators decided what role SARS-CoV-2 played in your grandmother’s death. In one health authority’s case, deaths of people who tested “negative” were rolled into the Covid total.
So the catastrophe described by Lord Sumption was underpinned by very weak evidence; science was nowhere to be seen. Consequently, it remains impossible to separate the impact of SARS-CoV-2 from that of the policies designed to “combat” it.
As the usual sources start gearing up to call for a new round of interventions and restrictions, have these massive cracks in evidence gathering and interpretation been tackled?
Hands up, who’s got the answer?
The narrative managers have done their best to memory-hole the Nurenberg Codes

By Helen of desTroy | August 28, 2022
You would be forgiven for not knowing that last Friday was the 75th anniversary of the Doctors’ Trial, one of 13 Nazi war crimes trials conducted at Nuremberg after World War II and the event that birthed the Nuremberg Codes, the most important medical ethics document of the modern era. The Codes set ground rules for requiring informed consent from experimental test subjects; they anchor international agreements like the Helsinki Declaration, the Geneva Convention and the United Nations’ International Covenant on Civil and Political Rights and have been codified into law in the US and other countries.
Sixteen doctors were found guilty at Nuremberg of murder and torture for carrying out a euthanasia program on mentally and physically disabled German citizens deemed “unworthy of life” and experimenting on concentration camp inmates; nine were jailed and seven were executed. Yet the expected flood of commemoratory articles and events marking the anniversary of the Allies’ crowning (if illusory) moment of moral superiority over those Evil Nazis™ has not materialized. It’s downright unnatural for the US and Europe to miss a chance to give the dead Nazi horse a good beating, but any attempts to even discuss the Nuremberg Codes in the last two years have been squelched by militant fact-checkers. Meanwhile, a coterie of corrupt “public health professionals” and the international financial cartels who control them have pulled off perhaps the most shocking and deadly crime against humanity ever committed.
The Big Lie
Mentioning Nuremberg during Covid-19 was asking to be pilloried in the “respectable” press as an anti-science, horse-paste-guzzling right-wing extremist. Fact-checkers came out of the woodwork to reflexively deny that the Nuremberg Codes applied to any aspect of the Covid-19 response, from forced masking to vaccine mandates, sometimes issuing two denials in a single day in their compulsion to keep the claim from spreading. One particularly tenacious fact-check even took issue with the claim “It was the doctors on trial in Nuremberg,” arguing that because the other 12 trials put Nazi Party officials, lawyers, and corporate executives in the dock, the statement “lacked context.”
This display of ideological lockstep was supposed to intimidate anyone who wasn’t already 100% allied with society’s enlightened institutions in defense of The Science™ against the irrational, emotionally-driven forces of ignorance. Those still on the fence about getting their “Warp Speed” car-crash of a shot were shamed by peer pressure psyops like the UK’s “Clap for our carers,” while social media was seeded with controlled but approachable “experts” who carefully crafted the illusion of overwhelming consensus that the measures being taken in the name of “stopping the spread” were not only scientifically but morally beyond reproach.
But this wasn’t an organic moment of unity. These “fact-checkers” have all received big money from the Bill & Melinda Gates Foundation, the eugenics enthusiasts who have rapidly become the most powerful force in global health policymaking and who also control huge chunks of the education, agriculture, and “green” energy spheres. Most fact-checking organizations pay lip service to the rules set by the International Fact-Checking Network, which while it sounds like an upstanding professional association that’s been around a while was actually launched less than a decade ago. The IFCN, which admits it doesn’t follow its own code of principles, has been funded since its 2015 beginnings by the Gates Foundation, the Omidyar Network, George Soros’ Open Society Foundations, Google, Facebook, the US State Department, and CIA cutout the National Endowment for Democracy, among others. It’s hard to think of a worse group of stewards for a gaggle of helpless facts, aside from perhaps the Wikimedia Foundation, about which more later.
The IFCN is run by the Poynter Institute, a “journalism education” nonprofit funded by many of the same entities as its IFCN subsidiary. Loaded down with enough conflicts of interest to make that code of principles swoon, Poynter selects, sponsors, and trains journalists, prioritizing obedience to authority, ideological inflexibility and a total absence of shame. They are then turned loose to mow the internet’s epistemological lawn in military fashion, doxxing some popular opposition voice while merely tagging others for later deplatforming, arrest, or worse. The tactic’s resemblance to the work of Ukrainian vigilante website Mirotvorets, unofficially operated by the country’s Ministry of Information, is unlikely to be an accident, given that Omidyar and Soros both poured billions of dollars into 2014’s Maidan Square color revolution, which was itself choreographed by the State Department’s Victoria Nuland, who knows the value of a well-placed bullet or a warm cookie.
It’s easy to see why Gates just had to buy the industry for himself. If these fact-checkers could reinvent the most corrupt government in Europe, whose military was exposed by dozens of major western media outlets as a hive of neo-Nazi thugs, as a democratic paradise, surely they could spin the vaccine tycoon’s Final Solution as the solution to all humanity’s problems. The Covid-19 experiment saw the closest collaboration yet between the fact-checkers, Big Tech and governments around the world to construct an epistemological roach motel that users could enter easily but would face growing barriers – warning screens, computer failures, personal attacks, deplatforming, financial hardship and a lowered social credit score – if they tried to leave.
It’s no exaggeration to say Poynter’s army of fact-checkers set the narrative of Covid-19 for the public from Day One (or should we call it Year Zero?). The IFCN’s “Coronavirus Alliance” launched in January 2020, before most Americans even knew what a coronavirus was. While the first Twitter users in the western hemisphere were stumbling across bizarre videos of Chinese people dropping to the ground and convulsing, explained in the accompanying broken-English text to be the result of an unknown virus, the fact-checkers were implementing orders from their paymasters. One of the first narrative touchstones, the red and white 3D model of the coronavirus, soon became as ubiquitous as the footage of planes hitting towers on 9/11, triggering intense fear and doubt directed both at the outside world and at the self. After all, they might be an “asymptomatic carrier,” and the only way to be sure was to isolate from their loved ones. As with 9/11, this unfamiliar terror pushed the individual to seek solace in an increasingly totalitarian state that insisted its ‘tough love’ – locking us in our homes, forbidding us from earning money, and keeping us from our families – was for our own good. Frightened and confused, many turned on the TV and sucked down its narcotizing propaganda. Even CNN’s ratings went up that first pandemic year, as Chris Cuomo demanded Americans “sacrifice the me to the we” and compared binge-watching Netflix to landing on the beaches of Normandy while his brother mass-murdered elderly New Yorkers.
The complex choreography of the Covid-19 response could not have unfolded as it did without premeditation. The plot was lifted – not plagiarized, as the authors were the same – from Event 201, the tabletop coronavirus simulation sponsored by the Gates Foundation at Johns Hopkins University’s Center for Public Health Security. This took place just a month after the Global Preparedness Monitoring Board – the product of an unholy marriage between the WHO and the World Bank earlier that year – released a report demanding all UN member countries “conduct at least two system-wide training and simulation exercises” by the following September, “including one for covering the deliberate release of a lethal respiratory pathogen.” Video of Event 201 shows players uninterested in minimizing harm from the virus instead exploring how the “emergency” might be used to stifle undesirable narratives and ram through major changes in society. The “real” pandemic – simulation number two, by the GPMB’s counting – played out months later exactly along the exercise’s script. The WHO, Gates, the World Economic Forum and Big Business took the reins, filling the power vacuum left while individual governments, seemingly baffled by the outbreak despite having repeatedly run their own simulations, ran around in circles.
How to treat an Infodemic
The crisis was planned and then used to crack down on unauthorized views under the reasoning that humanity was in the midst of an infodemic – a surfeit of information encouraging irresponsible beliefs – and careless talk could cost lives. Spreading dissenting opinions could infect friends and loved ones with the virus of doubt, which while perhaps less deadly than the virus itself (with its 99.7% survival rate), could cause society to fracture at a time when all humanity had to unite or be destroyed by the invisible enemy. Reading or hearing “disinformation” about Covid could reduce one’s likelihood of getting vaccinated, putting one’s very life at risk.
Convincing test subjects to discard their self-preservation instincts and their critical capacity and embrace the most absurd statements as gospel truth was the main goal of the first part of the Covid-19 experiment, and given the single-mindedness with which the WHO zeroed in on the “infodemic” before it had even officially declared the real virus to be a pandemic, it’s hard to believe they were making it up as they went along, especially given that the term was allegedly invented during the original SARS outbreak in 2003 (by a Washington Post writer no less) and then apparently put on ice until almost two decades later. Seeking input on how to respond to this new threat, the WHO reached out to professionals of all stripes, with more than a quarter of advisory input coming from academics eager to test out their juiciest hypotheses on real people with no repercussions. Everyone who used social media in 2020 to discuss the Covid-19 pandemic and its aftermath thus became a test subject, “nudged” and prodded for the Public Good, and some of those experiments – particularly those aimed at developing an FBI-style psychological profile of believers in “conspiracy theories” so they can be locked up as domestic terrorists or institutionalized as incurable monsters are very much ongoing.
Those early academic papers describe a chaotic infosphere in which the WHO’s narrative failed to dominate on its merits alone. The academics rose to the challenge, burnishing their half-baked speculations with scientific-looking graphs and charts. Their solutions ranged from Orwellian – deploying “freedom of expression officers” to censor and label rogue content as much as European human rights law would allow; re-education programs for “influencers,” teachers, priests, and other likely “superspreaders,” who could then be suspended from social media entirely if they refused to get their minds right – to the lesser evils of sending in fact-checkers as the equivalent of UN peacekeeping troops to help “inoculate” social media users against the disinformation they were about to see. With distrust in public and private institutions hitting new highs, society didn’t just need a vaccine against the scary new virus, it needed one against “disinformation” as well! But like the Covid vaccines themselves, these digital inoculations didn’t come with an informed consent notice, and the clinical trial results aren’t looking good.
Experiment #1: Shock “therapy”
As the WEF’s Klaus Schwab himself admitted in his pandemic tome The Great Reset, Covid-19 is the least deadly ‘pandemic’ in the last two millennia. But he’s quite open about wanting to use the largely self-inflicted Covid-19 “crisis” to bring about the Fourth Industrial Revolution, a transhumanist “green” dystopia lovingly crafted for “stakeholder capitalists” and inspired by technocratic parasites like Yuval Noah Harari. This is no experiment for the “good of society,” nor are any efforts made to “avoid unnecessary mental and physical suffering,” as Nuremberg demands. If anything, the experiment’s designers deliberately ratcheted up the suffering, believing this was necessary to unfreeze the fixed ideas of western civilization – free will, individuality, rationality, democracy (not to be confused with Our Democracy™) in our minds and replace them with the WEF’s preferred picks: obedience, “equity” (a Newspeak term meaning equality of outcome rather than equality of opportunity), credulity, communitarianism. The group has admitted on its own website that the lockdowns and the rest of the “touchless torture” the Covid response has supposedly required constitute the “world’s biggest psychological experiment.”

The Great Reset is an especially noxious experiment in that it violates the minds and bodies of test subjects on multiple levels, burrowing down into the way we think in its megalomania. It’s the spiritual offspring of CIA-funded Canadian psychiatrist Ewen Cameron, who “de-patterned” his patients’ personalities with high-voltage electroshock, induced coma, and mega-doses of LSD, then attempted to’ ‘build them back better’ by playing their comatose forms 16 hours of tape-recorded messages at a time; and Milton Friedman, the University of Chicago economist and godfather of neoliberalism whose students, the so-called “Chicago Boys,” conducted campaigns of economic “shock therapy” on third-world nations the US worried were too left-wing, assisting far-right leaders in seizing power, further impoverishing the masses with austerity programs, terrorizing what political opposition remained with death squads and disappearances, and privatizing all state-run industries so as to attract foreign investors. Neither Cameron’s patients, most of whom came in with simple problems like anxiety or depression (and one of whom wasn’t even seeking treatment but just looking for a job) and left as husks no longer able to even use the bathroom themselves; nor the inhabitants of Chile, Brazil, Uruguay, Indonesia, Russia, or any of the long list of other countries subject to some variation on Chicago School shock treatment over the years, were ever told they were part of an experiment, let alone asked if they wanted to be.
The Great Reset has not only targeted the entire world with economic shock therapy, triggering a massive depression the current financial system is unlikely to ever shake off (spoiler alert: another experiment coming…) – it funneled unprecedented amounts of fear into populations already thrown off balance by the blinding speed of policy shifts. First scolded for “selfishly” wearing a mask, then attacked for “selfishly” not wearing one; informed their city would be “locking down” at 10pm, when a peek out the window yielded crowds of restive youths hanging out on the corner with nary a cop in sight; told vaccinations were mandatory for school, then told their child could have just “masked up” when little Polly drops dead of a heart attack not 24 hours after her first shot of Moderna; the average person soon lapsed into learned helplessness and became a shut-in, depatterning daily in the glow of the television as they degenerated into an obedient vegetable, capable of “masking up” and socially distancing but little else. Despite leaving a horrific trail of devastation in their wake, the experimental lockdowns were praised by the WEF for the slight dip in carbon emissions they caused, all but guaranteeing phase II of the nonconsensual clinical trials – climate lockdowns – will be rolled out within the year.
Experiment #2: Hackable animals
Given the mountain of evidence against them, it’s perfectly logical that the ruling class would have tried to build up an impenetrable fort of bullshit using their captive fact-checking industry to deflect accusations of war crimes under the Codes. Several patterns pervade the apologist coverage, starting with the idea that these brand new mRNA Covid vaccines, tested on under 100,000 people by Pfizer and Moderna combined (and none who were pregnant or nursing) before receiving their coveted emergency authorization, are somehow not experimental procedures. They use the synonym investigational instead, as ‘experimental’ tends to trigger thoughts of, well, human experimentation, authoritarian regimes, the very Nuremberg Nazis the media establishment is trying its best to keep the average reader away from. But the effect is the same – mRNA vaccines of any kind weren’t tried on the general population until the end of 2020, and the torrent of side effects and death that has been unleashed in the meantime suggests neither Moderna nor Pfizer had informed consent from these gen-pop guinea pigs.
That’s a big deal, because Pfizer knew before it sought emergency authorization that more vaccinated test subjects had died than unvaccinated subjects – it even fudged the numbers for the FDA. Some 1,200 trial participants died in the 90 days following their injection, and Pfizer made sure to vaccinate the placebo group at the end of the trial in order to make sure further comparisons didn’t spoil its story. Indeed, it was so sure its vaccines were going to leave a pile of bodies behind that it refused to even sell them to countries whose governments wouldn’t shield them from liability for the damage caused. One should have expected this from a company with the dubious distinction of paying the largest fine in Justice Department history in 2009 for healthcare fraud, off-label prescribing, misleading marketing and miscellaneous criminality. Nevertheless, they won the “Warp Speed” lottery under Albert Bourla, a veterinarian with a doctorate in the biotechnology of reproduction who was for some reason promoted to CEO of the entire (human-focused) drug company a year before the Covid-19 outbreak. Given that his primary achievement prior to Operation Warp Speed was developing a “vaccine” that chemically castrated boars without ruining the meat, it becomes much more difficult to see the utter disaster the mRNA vaccines have created for both male and female fertility as an accident.
Still questioning authority? The fact-checkers then attempt to distance vaccine mandates – along with health passports, mask mandates, lockdowns and the other psychological aspects of the experiment conducted on the unwitting populace – from the Nuremberg zone by categorizing them as “public health interventions,” not research, or experiments. The Codes simply do not apply. Never mind that public health interventions are supposed to be evidence-based, and no western democracy has ever engaged in anything like the Covid lockdowns before, or that the CDC pulled the six-foot social distancing rule out of its ass, or even that the only “science” backing closing schools to “stop the spread” was a computer model from a 16 year old’s science project. Lockdowns arguably killed more people than Covid-19, and they have cut short many more lives by impoverishing, immiserating, and isolating millions. Arguing public health measures can’t be experimental because they’re public health measures is merely a last-ditch effort to wall the Codes off in a museum, inapplicable to anyone but those nasty Nazis who were – as the narrative managers never tire of reminding us – a unique and special case.
Discouraging cross-time contextualization is very important to the fact-checkers, who aren’t hesitant to shoot the messenger if all else fails. Anyone talking about the Nuremberg Codes in the context of Covid-19 is dismissed as an “alt-righter”, a “covid crazy,” dangerous “extremists,” “anti-vaxxers,” or even actual Nazis who apparently got confused about whose side their team was on back in WW2. In war, dehumanizing the enemy is key to beating him, and this is nothing if not a two-pronged war being fought in our brains and our bloodstreams. “Drawing a link between this final rollout of these vaccines and what the Nazi doctors were doing is morally grotesque,” the British Medical Association’s Dr Julian Sheather told FullFact ; he didn’t explain why, and it’s not apparent why one should not draw parallels between the two cases. According to the Vaccine Adverse Event Reporting System (VAERS), whose own creators admit it contains less than 1% of all adverse events associated with a given vaccine, the Covid shots have already caused nearly 30,000 deaths, over 170,000 hospitalizations, nearly 16,000 heart attacks (a common sight now on sports fields, where 60 times more athletes than normal are flatlining mid-game), and nearly 5,000 miscarriages in the US alone. Using tech entrepreneur Steven Kirsch’s calculations, the numbers are much higher: at least 478,000 Americans have been killed by Covid vaccines, to say nothing of millions permanently disabled, unable to work or function on a basic level. Worldwide, the number of deaths approaches 12 million.
While the number of victims the Nazi doctors left behind is not so meticulously recorded, especially given the high levels of typhus and malnutrition contributing to the mortality rate in the camps, one source has them consigning between 70,000 and 100,000 “unfit” Germans to death between 1939 and 1941 while sterilizing hundreds of thousands more – a detail that once again should send a chill down the spine of anyone who’s noticed the declining birthrates around the world. If the figures aren’t comparable, that’s only because the mRNA vaccine has been so much more efficient in its killing. There’s nothing “morally grotesque” about pointing that out. But since “everybody knows” the Nazis were the pinnacle of Evil™, the realization that Pfizer and Moderna’s death toll might have their doctors beat must be prevented at all costs. Thus even bringing up Nuremberg in relation to Covid-19 is deemed to be “trivializing” the crimes of the Nazis, even when the intention is to draw attention to the seriousness of their modern descendants’ crimes, and efforts are made to further poison the dialogue by suggesting there’s something antisemitic about the whole business.
In Part II: the war on “conspiracy theories,” why Nuremberg is to be memory-holed, infodemic terrorism, and more…
Exhaustive study of German mortality data finds excess deaths tightly correlated with mass vaccination
eugypius | August 27, 2022
Excess mortality in Germany 2020–2022 is a preprint by Christof Kuhbandner (a psychologist at Regensburg) and Matthias Reitzner (a statistician at Osnabrück) that applies sophisticated actuarial analysis to the publicly available all-cause mortality data provided by the German government. It turns out that when you account for historical mortality trends, the virus no longer looks so dangerous, and the vaccines no longer look so great.
From the abstract:
In 2020, the observed number of deaths was close to the expected number with respect to the empirical standard deviation. By contrast, in 2021, the observed number of deaths was two empirical standard deviations above the expected number. The high excess mortality in 2021 was almost entirely due to an increase in deaths in the age groups between 15 and 79 and started to accumulate only from April 2021 onwards. A similar mortality pattern was observed for stillbirths with an increase of about 11 percent in the second quarter of the year 2021.
Something must have happened in April 2021 that led to a sudden and sustained increase in mortality in the age groups below 80 years, although no such effects on mortality had been observed during the COVID-19 pandemic so far.
What happened in April 2021 was the beginning of mass vaccination across Germany.
Here’s an overview of mortality deficit or excess by age bracket:
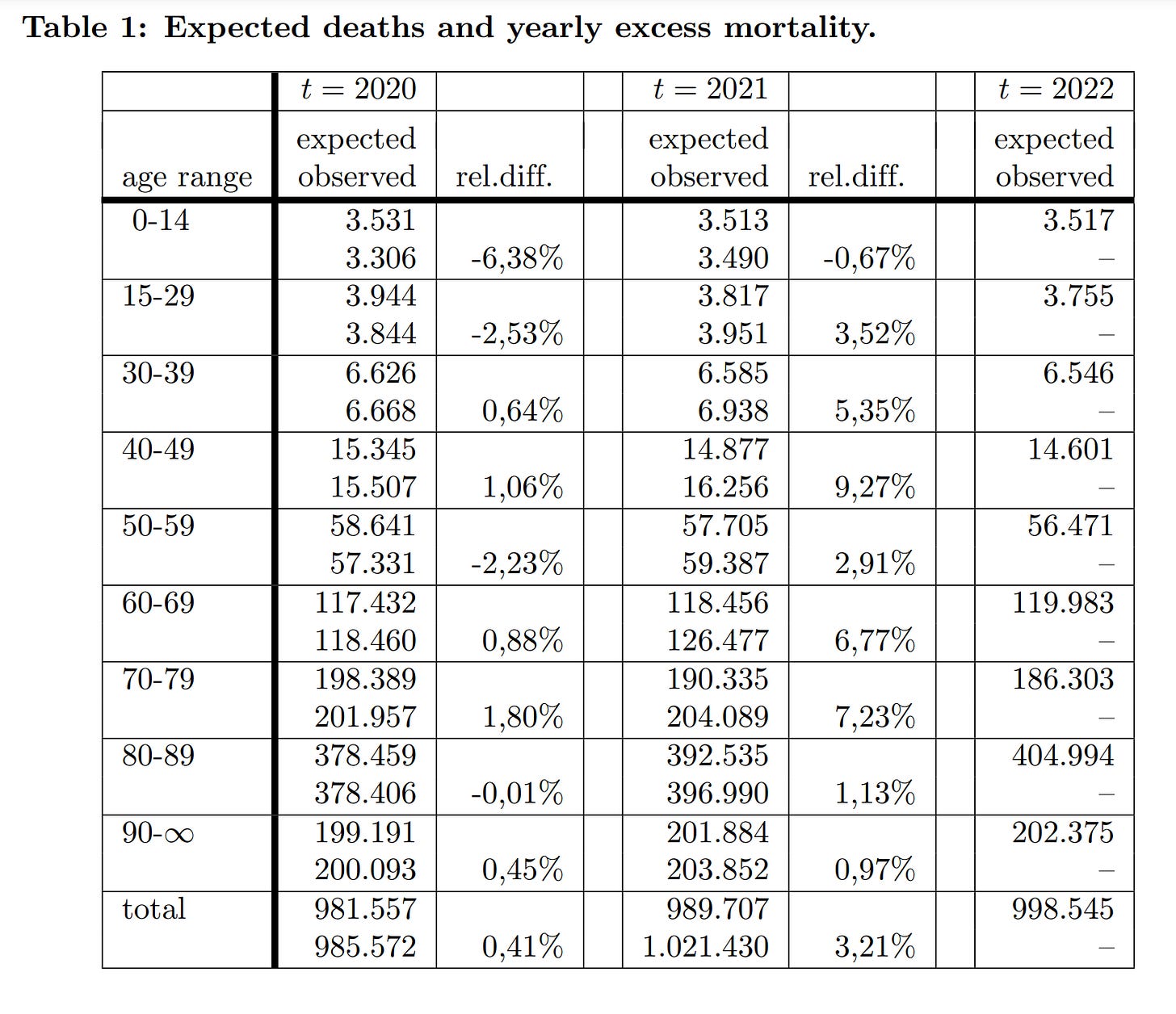
As I’ve said many times, the first year of the German pandemic was a total nothingburger. There was no heightened mortality trend save for among the oldest groups, briefly, in December. In 2021, however, the Year of Maximum Vaccination, the authors estimate almost 32,000 excess deaths. Mortality rose across the board, especially among youngs, with those in their 40s seeing 9% more deaths than expected by their model.
Here are the same figures visualised:
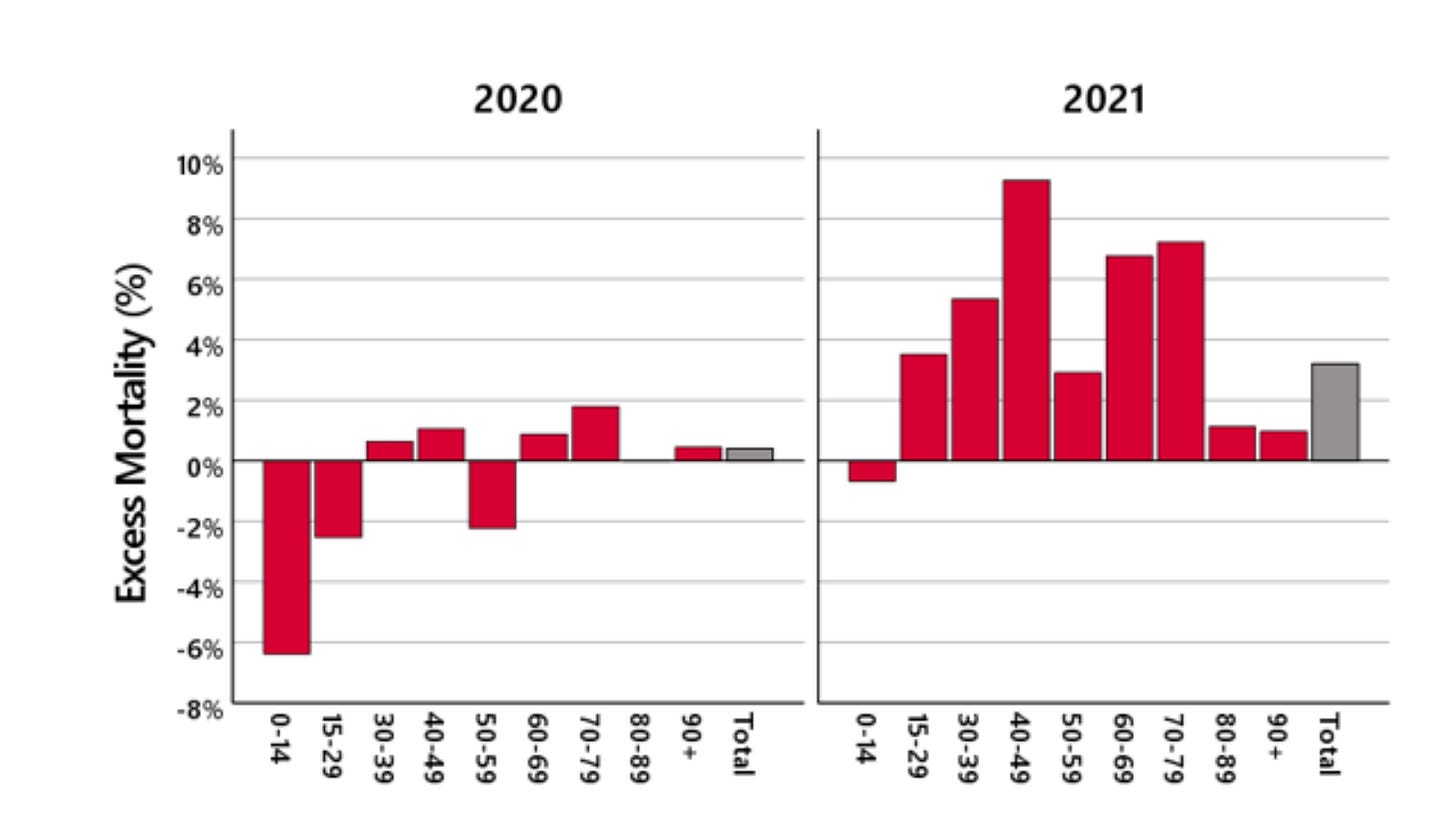
Just looking at that 2021 graph, you can tell there’s something really wrong here. If it’s virus doing all this killing, why is it hardest on people aged 15 to 79? How is it leaving the oldest Germans almost entirely unscathed?
The authors also provide a month-by-month breakdown for the 15-59 age-group:
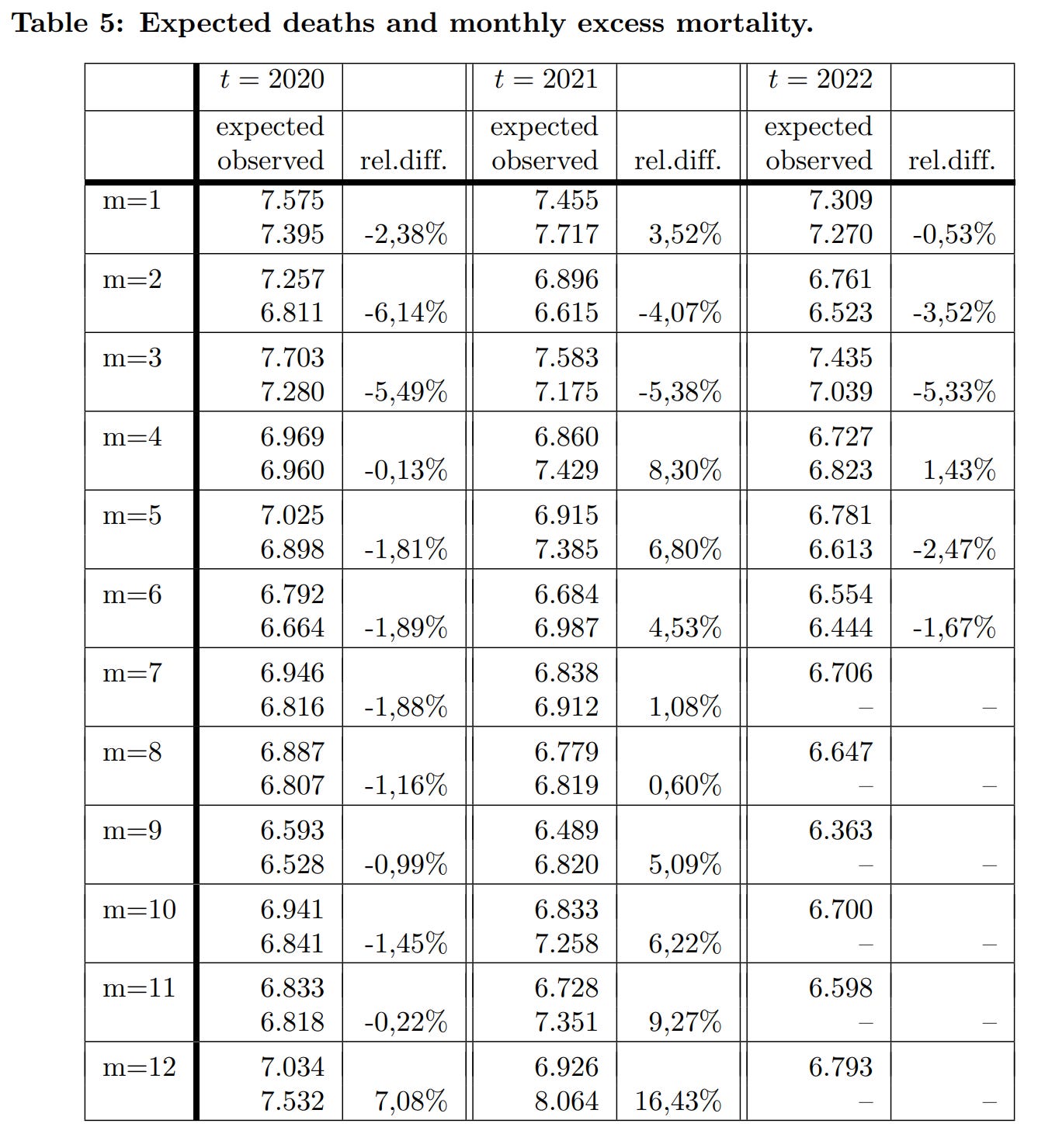
They note that “The significant excess mortality in December 2020 continues slightly in January 2021, and then is mostly compensated until March 2021. That is, by the end of March, the cumulative excess mortality was close to zero.” These are what the funeral industry would call “pull-forward” deaths. In Germany, the virus mainly kills people who are about to die anyway, such that mortality spikes are followed by counterbalancing mortality deficits.
The authors continue:
In April and May 2021, a significant increase in excess mortality is observed, followed by a decrease up to August. However … the increase in excess mortality in April and May is not compensated for. In September there is again a significant excess mortality, which increases in November and is more than doubled in December 2021.
The April increase obviously coincides with the vaccine rollout, while the Fall increase aligns fairly well with the booster campaign. It’s noteworthy that dose 2 doesn’t seem as dangerous as dose 1 or 3; and that the mortality signal is very tightly correlated with the date of vaccination. As soon as you stop vaccinating, excess deaths recede.
As for people 60 and older, there are two distinct trends: Rising mortality coinciding, again, with the mass administration of doses 1 and 3 in the 60-79 bracket, and nothing special in the 80+ bracket:
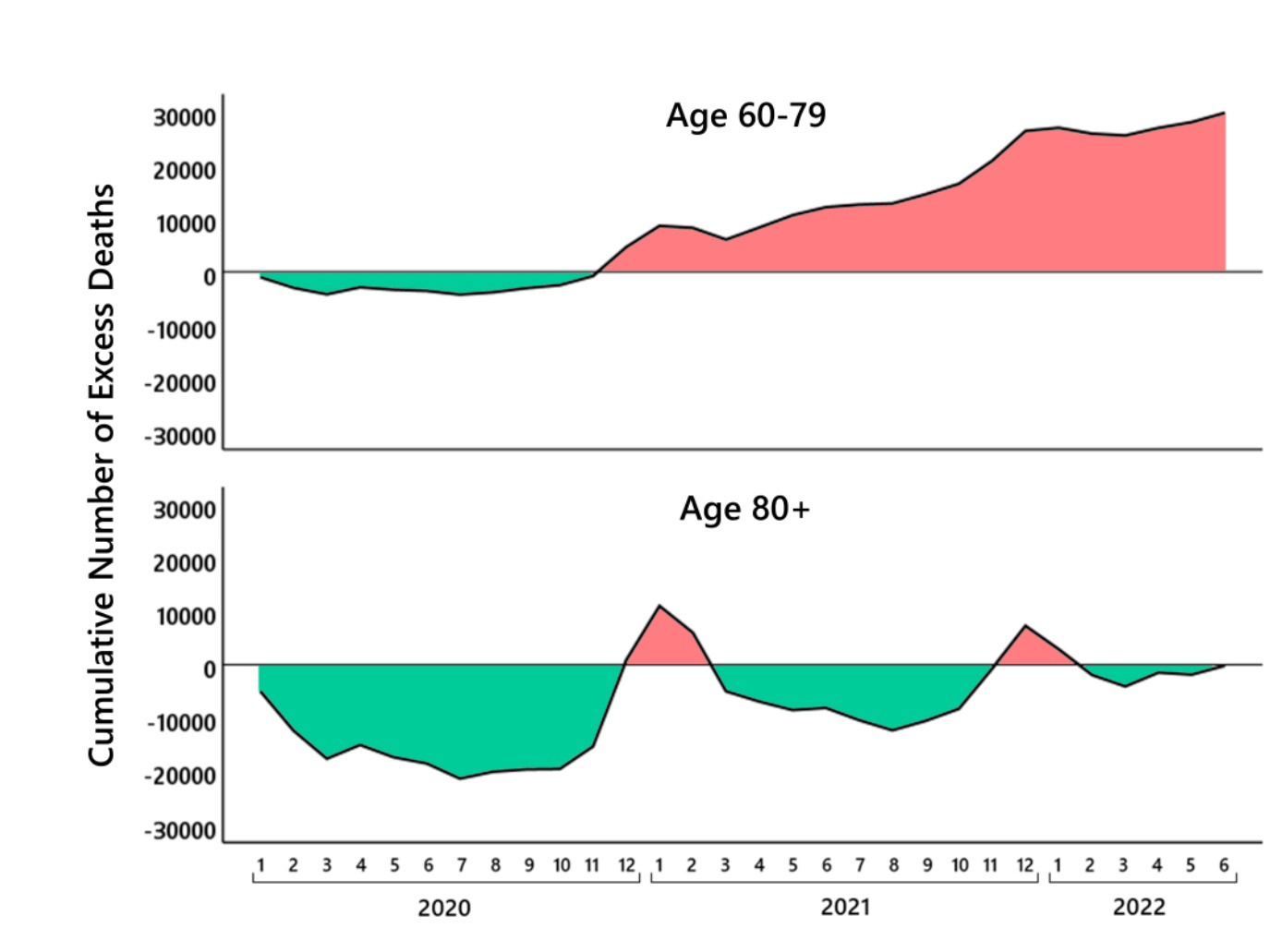
The vaccines obviously do most of their harm by inducing adverse immune reactions, and thus they’re relatively safe in the very elderly, who have weaker immune systems. This makes the oldest Germans a useful control, as they are the most sensitive to virus-associated mortality, and the least sensitive to vaccine-associated mortality. Thus, to anyone who objects that it’s really the April case spike that’s making the vaccines look bad here, or that it’s Delta causing those problems in the Fall, the reply is simple: The olds aren’t dying in April or September 2021, just the youngs. What kills mainly the youngs and spares mainly the olds? The answer is not SARS-2.
As the authors note:
The maybe most surprising fact is that [2021] produces in all age groups a significant mortality increase, which is in sharp contrast to the expectation that the vaccination should decrease the number of COVID-19 deaths. The only exception is the last age group [80+] … However, when interpreting this finding, it has to be taken into account that there wa sa huge mortality deficit in 2019 and until October 2020 which was compensated in November [and] December 2020 and January 2021.
It becomes very hard to doubt that the excess mortality of 2021 is vaccine related, when you compare the relative chronology of deaths and mass vaccination:

There are also more specific mortality correlations by age bracket. Thus the authors note the “further hint” that the vaccines are implicated in these deaths, “is the fact that the age group 0–29 has a peak in the excess mortality in June 2021 instead of April 2021,” precisely when these younger cohorts were lining up for their first dose.
A final intriguing finding relates to the relationship between official Corona death numbers and excess mortality. Nobody will be surprised to learn that the SARS-2 death toll is egregiously inflated, but the age-cohort patterns are worth a look:

The official figures are most accurate for those in their 60s and 70s. For those over 80 years old, they are almost entirely meaningless. This group saw less than 20,000 excess deaths in two-and-a-half years of Corona, while their official death count is approaching 100,000.
It’s no wonder that nothing—not lockdowns, not vaccines, not masks, not all the tests in the world—can drive down all-cause mortality in Germany. Most of the people the virus kills are on the verge of dying anyway, and if you spare them a death from SARS-2, they’ll just die of something else next month.
If It’s Okay for Mice, It’s Good Enough for People, Right?
By Madhava Setty, M.D. | The Defender | August 26, 2022
Its audacity on full display, Pfizer — arguably the most criminal corporation in history — has asked the U.S. Food and Drug Administration (FDA) to greenlight its new bivalent COVID-19 vaccine that targets the Omicron BA.4 and BA.5 subvariants for people 12 and older “to help the country prepare for potential fall and winter surges of the coronavirus,” Pfizer CEO Albert Bourla said in a statement.
Bourla’s good intentions are sadly thwarted by FDA regulations that require an Investigational New Drug (IND) application be submitted and approved before a drug can be tested in humans.
Luckily, the FDA can circumvent the inconvenience of its own regulatory processes by allowing itself the ability “to authorize use of an experimental drug in an emergency situation that does not allow time for submission of an IND in accordance with 21CFR, Sec. 312.23 or Sec. 312.20.”
Section 312.20 of the Code of Federal Regulations specifies that a clinical investigation cannot commence until an IND application has been submitted and approved. Nevertheless, Pfizer on Monday submitted an IND for its new formulation.
Now that the FDA and Pfizer have crossed their Ts and dotted their Is to make sure all the rules are followed, how do we know these products are safe and will work?
This is where the rodents come in — the products seem to work on mice.
As NPR reported, “For the first time, the FDA is planning to base its decision about whether to authorize new boosters on studies involving mice instead of humans.”
Yes, it’s an unprecedented move by the FDA, but Dr. Ofer Levy, professor of pediatrics at Harvard and advisor to the FDA argues that the country has had enough experience with the vaccines at this point to be confident the shots are safe and that there’s not enough time to wait for data from human studies.
He has a point. There were still only 30,479 uninvestigated deaths reported in VAERS after administration of the shots as of Aug. 19.
In any case, why should the FDA be concerned with such things as human studies in the first place?
This maneuver by the FDA may finally unshackle the agency from its overly restrictive responsibility to fulfill its own mission and become more agile in bringing products to market.
Not to be left behind, Moderna also requested the FDA authorize its bivalent vaccine for human beings over the age of 17.
Similar to the Pfizer vaccine, Moderna’s vaccine also, for good measure, will encode for the spike protein for the original ancestral SARS-CoV-2 strain, which for all intents and purposes, does not exist on our planet any longer.
Meryl Nass, M.D., summarized it this way:
“No clinical trials. (You need to obtain an IND before you can start testing the vaccine in humans. Pfizer applied 4 days ago.)”
Taking no chances, the FDA will not convene the Vaccines and Related Biological Products Advisory Committee (just like the first time the FDA authorized boosters) and has announced this today to see how much opposition the agency gets.
Can we dispense with the pretense any of this is about health?
No sane person vaccinates the entire country with an experimental vaccine without trials — particularly since the whole country already has some immunity, the virulence is low and the evidence supports higher all-cause mortality with an increasing number of vaccine doses.
What is in the vaccine that they are desperate to inject us with?
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Norwegian Schools Are Disseminating Government-Approved Covid Misinformation

BY KATHRINE JEBSEN MOORE | THE DAILY SCEPTIC | AUGUST 26, 2022
Who needs conspiracy theorists when you’ve got school books teaching children that Covid vaccines are “95% effective”?
This autumn, a new school book was introduced for the ninth grade in Norway. Fabel 10 was revised in 2021/22, but has only now been introduced in schools across Norway. Not only does the book overstate the effectiveness of the novel mRNA vaccines, it decries anyone questioning that as conspiracy theorists.
One excerpt reads:
Since the Covid pandemic broke loose, Covid deniers and vaccine sceptics have spread disinformation about coronavirus through social media. They claimed among other things that COVID-19 was no more deadly than the flu, that the vaccine was dangerous, and that restrictions were unnecessary. On Saturday March 20th 2021, 200 Covid deniers gathered in front of the Parliament. They burnt face masks to show that they thought they were unnecessary.
This short paragraph is easily debunked. Readers of the Daily Sceptic know that Covid now has an infection fatality rate about the same as influenza. We also know that side effects from the Covid vaccines – both the mRNA and the viral vector vaccines such as AstraZeneca’s – are more common than for other tried and tested vaccines. Remember when the Pandemrix vaccine rollout was halted because of a link to rare instances of narcolepsy? Multiple studies show Pfizer and Moderna’s Covid vaccines increase the risk of myocarditis and pericarditis in especially younger males – the demographic who make up precisely half the readership of Fabel 10. The German Government even admits that as many as one in 300 doses of the mRNA jabs produce serious injury. Compared to the danger that Covid poses to most people, does that make vaccines worth having?
And as for restrictions, a new consensus is gaining momentum. Whereas back in 2021, when the book was written, it was mainly agreed that lockdowns and other Covid restrictions were necessary to halt the spread, and countries with low Covid fatalities would credit these non-pharmaceutical interventions for their comparatively low excess mortality, studies later proved them incorrect. Lockdowns and excess mortality were not correlated. Whereas back in the early days of the pandemic, only a few, brave voices spoke up about their concerns, now even Rishi Sunak, who helped implement Britain’s lockdowns, admit they were detrimental to overall health and the economy and did little to stop infection. Yet in Norway, pupils are stuck in the reality curated more than a year ago, a reality that has now been revealed to most as bonkers.
And those 200 “Covid deniers” who burnt face masks deserve praise for being a tiny minority speaking up for science at a time where “the science” became an allegory for anything the authorities wanted us to do without having to prove why.
The book also states that vaccines are “95% effective against COVID-19 infections”. This is clearly nonsense, and doesn’t need further debunking. We all know of multiple-jabbed people getting infected several times over, and that infection rates in highly vaccinated countries went through the roof after the vaccine rollout.
Perhaps the book will serve as a test to pupils old enough to gather information from multiple sources. Some might agree with what they’re presented with, while others will see through this Government-approved misinformation. But that’s not really the sort of education you want in a free, democratic country. The book doesn’t invite 14-15 year-olds to question or discuss – it presents them with all the (wrong) answers. That’s bad enough in itself, but what’s worse is it tells them to ridicule those who don’t agree. The chapter on Covid and conspiracy theories could have been a great opportunity to teach children about academic freedom, online censorship, tolerance, debate, dissent and freedom of speech. Instead, it serves straight-up, Orwellian newspeak to young minds in a way the CCP would be proud of.
Senators demand NIH, HHS preserve all related documents, communications, promise ‘full-throated investigation’ of Fauci
By Suzanne Burdick, Ph.D. | The Defender | August 24, 2022
Two U.S. senators on Tuesday — the day after Dr. Anthony Fauci announced plans to leave his government posts in December — formally requested the National Institutes of Health (NIH) and the U.S. Department of Health and Human Services (HHS) preserve all documents and communications related to Fauci.
Fauci on Monday said he will retire as director of the National Institute of Allergy and Infectious Diseases (NIAID) and as chief medical adviser to President Joe Biden in December to pursue “the next chapter” of his career.
In a letter to HHS Secretary Xavier Becerra, Sen. Roger Marshall (R-Kan.) demanded Becerra “immediately confirm” that HHS is preserving all records related to Fauci and Dr. Francis Collins, who was director of the NIH from August 2009 to December 2021.
“This request applies to all documents, records, memoranda, research, correspondence, or other communication or any portion thereof relevant to any involvement of Dr. Fauci or Dr. Collins,” the letter stated.
Sen. Rand Paul (R-Ky.), in a letter to Lawrence Tabak, D.D.S., Ph.D., acting director of the NIH, asked Tabak to “ensure the preservation of all documents and communications within Dr. Fauci’s possession related to his tenure at the National Institutes of Health (NIH).”
Marshall stressed that it is “imperative” that all HHS workers are made aware of their “legal responsibilities to collect, retain, and preserve all documents, communications, and other records in accordance with federal law.”
He also reminded Tabak of his obligation, as the head of HHS, to ensure the preservation of all records and that any employee “who conceals, destroys, or attempts to conceal or destroy a federal record may be subject to fine and imprisonment for up to three years.”
Marshall pointed out that HHS previously refused to provide information to Congress:
“HHS and component agencies, including NIH in particular, continue to obstruct numerous congressional investigations through refusal to provide responsive information.
“In addition to withholding information from Congress, private parties note that NIH refuses to comply with Freedom of Information Act (FOIA) requests until forced to do so by court order.”
Marshall went on to list “recent egregious examples” of NIH’s failure to meet record-keeping requirements and said that “even one” such example “should instigate immediate oversight action by HHS.”
Marshall’s letter outlined four “notable recent concerns” with NIH’s record-keeping, including past accusations that NIH destroyed records, potential conflicts of interest within the HHS Office of Inspector General, NIH’s practice of “self-policing” and NIH’s failure to ensure required reporting of clinical trial results.
‘Fauci’s resignation will not prevent full-throated investigation into origins of pandemic’ — Rand Paul
Paul, in his letter to Tabak, also emphasized the need to preserve NIH documents for investigation purposes.
Paul wrote:
“This information is critical to ensure that Congress has access to information necessary to conduct proper oversight regarding events that took place during Dr. Fauci’s tenure with the agency.
“Specifically, I request you preserve all records, e-mail, electronic documents, and data created by or shared with Dr. Fauci during his tenure at NIH that relate to COVID-19 including, but not limited to, NIAID-funded coronavirus research.”
In an email today, Paul told The Defender :
“Dr. Fauci misled the American people on public health guidance throughout the pandemic, lied to Congress under oath, and funneled tax dollars to fund dangerous research in communist China.
“The American people deserve transparency and accountability from the NIH regarding the COVID-19 pandemic regardless of Dr. Fauci’s future employment plans.”
On Monday, Paul tweeted, “Fauci’s resignation will not prevent a full-throated investigation into the origins of the pandemic. He will be asked to testify under oath regarding any discussions he participated in concerning the lab leak.”
For more than a year, Paul has advocated for a thorough investigation into the origins of COVID-19 and pushed for a criminal investigation of Fauci, whose NIAID research at the Wuhan Institute of Virology in China Paul suggested may have been involved in creating the virus.
Following up on a threat he made in mid-July of 2021, Rand sent an official criminal referral on Fauci to the U.S. Department of Justice on July 26, 2021.
Paul asked Attorney General Merrick Garland to investigate Fauci for allegedly lying to Congress when he said the NIH “has not ever and does not now fund gain-of-function research in the Wuhan Institute of Virology.”
The week before he sent the official criminal referral, Paul asked Fauci if he wanted to retract the statement he made to Congress during a May 11 hearing. Paul said, “Dr. Fauci, knowing that it is a crime to lie to Congress, do you wish to retract your statement of May 11, where you claimed the NIH never funded gain-of-function research and move on?”
Fauci replied he would not retract the statement and was adamant he never lied before Congress.
However, Fox News commentator Tucker Carlson said on June 2, 2021, that evidence showed Fauci was “implicated in the very pandemic he had been charged with fighting.”
Emails obtained by BuzzFeed via the Freedom of Information Act show “Fauci supported the grotesque and dangerous experiments that appeared to have made COVID possible,” Carlson said.
The emails, which date back to the early winter of 2020, show Fauci was worried the public would think COVID-19 originated at the Wuhan lab. Why?
“Possibly because Tony Fauci knew perfectly well he had funded gain-of-function experiments at that very same laboratory,” Carlson said.
The emails showed Fauci and other top virologists shared an article from ZeroHedge suggesting COVID-19 was a man-made bioweapon. Despite it being a “plausible explanation,” said Carlson, ZeroHedge was banned from social media.
Carlson said:
“Until recently, you were not allowed to suggest that COVID might be man-made. Why couldn’t you suggest that? The fact checkers wouldn’t allow it. Why wouldn’t they? Because Tony Fauci assured the tech monopolies that the coronavirus could not have been manmade. And so the tech monopolies shut down the topic.”
NIAID has, for years, provided grants to the EcoHealth Alliance and others to conduct gain-of-function research on coronaviruses, as The Defender previously reported.
In March 2021, the Wuhan lab deleted mentions of its collaboration with the NIAID/NIH and other American research partners from its website. It also deleted descriptions of gain-of-function experiments on the SARS virus, according to Dr. Joseph Mercola.
“The NIH/NIAID has funded GOF [gain-of-function] research to the tune of at least $41.7 million,” Mercola said. “Up until 2014, this research was conducted by Ralph Baric at the University of North Carolina.”
After 2014, when federal funding of gain-of-function research was banned, the research was funneled to the Wuhan lab via the EcoHealth Alliance.
Mercola added:
“In August 2020, the NIAID announced a five-year, $82-million investment in a new global network of Centers for Research in Emerging Infectious Diseases that will conduct GOF experiments to ‘determine what genetic or other changes make [animal] pathogens capable of infecting humans.’”
Suzanne Burdick, Ph.D., is an independent journalist and researcher based in Fairfield, Iowa.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Download for Free: Robert F. Kennedy’s New Book — ‘A Letter to Liberals’
CDC Director deflects blame for lockdowns towards predecessors

By Mike Campbell | The Counter Signal | August 25, 2022
CDC Director Rochelle Walensky admitted organizational shortcomings on Fox News while deflecting blame toward predecessors for their lockdown recommendation.
“Many of those lockdowns pre-dated me at the CDC,” she said.
Walensky, who once used ‘Trust the science’ to persuade the public, carried a humbler tone while reflecting on her organization’s decisions.
“There were important decisions that we had to make in imperfect times, with imperfect data, and we always updated those decisions as those data were evolving…”
“So, I don’t really want to re-visit the questions of lockdowns that pre-dated me, but what I will say is, we’ve updated our guidance in the context of new information, and sometimes we have to make a decision before we have all the information that we want…”
Indeed, the CDC updated guidance by removing special quarantine recommendations for unvaccinated persons, effectively admitting that vaccination status is no longer relevant when it comes to infection or spread of the Covid virus.
In fact, on July 23, the CDC deleted a ‘fact’ from their “Facts about mRNA Covid-19 Vaccines”, and they did so without explanation. Last time I checked, facts don’t change — but apparently, they do for the CDC.
Walensky further stated that “[their] science” indicated hybrid immunity was superior to natural immunity. However, we’ve reported on a scientific study that accounted for more than 5.7 million people, which showed that natural immunity is just as effective as hybrid immunity.
To this point, Walensky’s usage of science in the possessive sense — by calling it “our science” — denotes a departure from “the science,” of which they’re either arbitrarily picking from or are completely unaware.
Between Fauci stepping down and Walenski pointing fingers, it appears the blame game has officially started.
Disappearing YouTube Misinformation Prevention Policies on Masks and Social Distancing

The Naked Emperor’s Newsletter | August 23, 2022
Earlier in the year YouTube’s COIVD-19 medical misinformation policy wouldn’t allow you to post content which contradicted the WHO’s or local health authorities’ guidance on various issues including:
- Social distancing;
- Claims that wearing a mask is dangerous or causes negative physical health effects;
- Claims that masks do not play a role in preventing the contraction or transmission of COVID-19

Now, it’s perfectly fine, signalling that those claims are no longer misinformation. Too bad if you previously had your account cancelled for questioning those policies. You should know by now when it is ok to question The Science™ and when it is verboten. Do keep up.

Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- The Straight of Hormuz is Open for Iranian Business… Oil is Moving and Iran is Getting Paid
- Biden’s Closed Circle on Russia
- Lebanon Accuses Israel Of Violating The Chemical Weapons Convention By Spraying Toxic Herbicide Over Farmland
- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- If Americans Knew
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- No Tricks Zone
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
