Legal Information About How To Refuse Vaccine Mandates, Etc.
Weston A Price Foundation, London Chapter | July 27, 2021
Below is a helpful guide for anyone in the common law nations (UK, US, Canada, NZ, Australia, etc) concerned about unlawful impositions of COVID19 government mandates on vaccines, masks, exemptions, etc.
Vaccines in UK are not mandatory. There is an exemption on evidence of medical reasons and the Supreme Court recognises at common law that denial of free and informed consent is a self certified medical reason. See Montgomery v Lanarkshire [2015] UKSC 11 https://www.supremecourt.uk/cases/docs/uksc-2013-0136-judgment.pdf …In R Wilkinson v Broadmoor : [2001] EWCA Civ 1545
In that case Lady Justice Hale, Supreme Court President, confirmed that forced medical procedure without informed consent “may be sued in the ordinary way for the (common law) tort of battery”. https://www.bailii.org/ew/cases/EWCA/Civ/2001/1545.html …In the judgement it was held that acting under statutory authority provides no defence, therefore the Employer will be guilty of coercion on the threat of battery with regards to unlawful dismissal if express evidence of denial of informed consent are unlawfully rejected.This will result in a breach of contract and also a Tort that can be sued.
The Above Is Why Mask “Mandate” Exemptions Were Self Certified.
It is unlawful for Doctors to interfere with the process of free and informed consent. Informed consent is defined in Montgomery as follows:
- That the patient is given sufficient information – to allow individuals to make choices that will affect their health and well being on proper information.
- Sufficient information means informing the patient of the availability of other treatments (and forms of testing).
- That the patient is informed of the material risks of taking the medical intervention and the material risks of declining it.If consent is given but the Patient subsequently proves that information provided at the time breached the above common law test of informed consent, the Tort of battery is committed and the medication is unlawful.
The High Court has found children incapable of providing Gillick Competency for experimental medicines with unknown long term effects. Schools therefore risk being sued for battery if ignoring Parental preferences.
See Bell v Tavistock [2020] EWHC 3274 https://www.judiciary.uk/wp-content/uploads/2020/12/Bell-v-Tavistock-Judgment.pdf …
These principles are discussed without reference to case law on this important NHS page on Free and Informed Consent and Gillick Competency. See:
https://www.nhs.uk/conditions/consent-to-treatment/ …
The fundamental common law right to free and informed consent, based on the ancient Tort of battery (tresspass to the person), are valid in all 16 Commonwealth Realms and both the Republic of Ireland and USA, where English common law is retained as a body of law.
In Ireland, evidence that English common law rights are retained can be found in the Statute Revision Act (2007) which retained Magna Carta and most of the English Bill of Rights (1688) and much, much more. http://www.irishstatutebook.ie/eli/2007/act/28/enacted/en/html …
In USA, English common law rights are retained by the 9th Amendment of the Constitution
“The enumeration in the Constitution, of certain rights, shall not be construed to deny or disparage others retained by the people.”, hence why US courts refer to them. https://constitution.congress.gov/constitution/amendment-
9/ … Law that provides rights sit above normal laws in English law and provide lawful excuse to statutory obligations with this acknowledged by courts. see Art.29 Magna Carta (1297), which states: “we will not deny or defer to any man either Justice or Right.” https://www.legislation.gov.uk/aep/Edw1cc1929/25/9/section/XXIX …
Another case to read is Burton Hospitals NHS Foundation Trust [2017] EWCA Civ 62 regarding Doctor’s obligation to provide information to inform consent. https://www.bailii.org/ew/cases/EWCA/Civ/2017/62.html …
Happy for Solicitors to DM and work with me or folk who want to work on template letters to send out.For those not familiar with our organisation, here are the articles we have written on Covid. See: https://www.westonaprice.org/coronavirus/
Covid passports also recognise self certified free and informed consent.
“If you have a medical reason which means you cannot be vaccinated or tested, you may be asked to self-declare this medical exemption.” https://www.gov.uk/guidance/nhs-covid-pass …
Also see Art.IV Acts of Union (1706-7):
“That all the Subjects of the UK of GB shall from & after the Union have full freedom & Intercourse of Trade & Navigation to & from any port or place within the said UK & the Dominions” https://www.legislation.gov.uk/aep/Ann/6/11/part/4 …
For our friends in New Zealand, you also have these common law rights, but additionally, Art.11 of your 1990 Bill of Rights states: ”Everyone has the right to refuse to undergo any medical treatment.” https://www.legislation.govt.nz/act/public/1990/0109/latest/DLM224792.html …
Tories collaborate with Sturgeon to impose vaccine passports on Scotland
By Gary Oliver | TCW Defending Freedom | September 3, 2021
UNLESS a majority of MSPs are prepared to defend freedom – don’t laugh – Scotland will soon become the first part of the UK to impose vaccine passports.
Subject to the formality of a vote next week at Holyrood, from later this month Scots who wish to enter nightclubs, attend music festivals and large-scale concerts or be part of a five-figure football crowd, must be double-jabbed – and, crucially, be willing to prove it.
The foregoing are just some of the social activities in Scotland which First Minister Nicola Sturgeon has decreed off-limits to healthy people.
Addressing the Scottish Parliament on Wednesday, Sturgeon justified her malevolent measure because ‘case levels are 80 per cent higher now than they were last week and they are five times higher than four weeks ago’. Yet that five-fold rise over the past month continues to have negligible impact on the more important statistics: of 1,099 deaths in Scotland during week ending August 29, only 48 were ‘involving Covid’ – a weekly total and proportion (under 5 per cent) which has been consistent since mid-July.
The spiralling number of so-called cases is largely irrelevant and says only that Covid is circulating in Scotland amongst an adult population which already is overwhelmingly double-jabbed. This seems entirely consistent with recent findings that the fully vaccinated are just as likely to transmit the virus – a fact which, alone, renders redundant Sturgeon’s case for vaccine passports.
Spuriously presented as the benevolent alternative to another lockdown, the principal purpose of the policy is of course what health secretary Humza Yousaf euphemistically terms ‘incentivising vaccination’ – code for coercion of the reticent. Indeed, this week Nicola Sturgeon reiterated her amoral aim of unnecessary universal vaccination and restated her dastardly desire to stick needles into schoolchildren for whom the Covid vaccine is all risk and no personal benefit: ‘We still await advice from the JCVI [Joint Committee on Vaccination and Immunisation] on vaccinating all 12- to 15-year-olds and I very much hope the evidence will allow the JCVI to give a positive recommendation very soon, and we stand ready to implement that if it is the case.’
Shameful. We are also expected to welcome Sturgeon’s assurance that her forthcoming medical apartheid will apply only ‘in very limited settings and never for public services such as transport, hospitals and education’.
Never? Believe that at your peril.
She expects us to be pathetically grateful that ‘certification rules in several other countries cover a far wider range of venues than the ones we are currently considering for Scotland’, and take comfort from her tartan tyranny being less draconian than elsewhere – at least for the moment.
Far from defending freedom, the spineless Scottish Conservatives are contemptible collaborators. Murdo Fraser, the shadow spokesman for Covid Recovery, was already a proponent of vaccine passports: when the SNP had earlier expressed scepticism, fatuous Fraser advocated the abomination as a ‘reasonable proposition’ and a ‘reasonable trade-off for people’.
His leader’s response to the First Minister’s statement was even more lamentable. Instead of speaking up for liberty and personal autonomy, the complaint from Douglas Ross was that ‘the SNP Government is now introducing vaccine passports at the last minute’; depressingly, he bemoaned the Nats ‘wasting months that could have been spent making proper preparations’. https://www.dailymail.co.uk/news/article-9947533/Nicola-Sturgeon-wants-Scots-use-vaccine-passports-enter-clubs-attend-Premiership-games.html
Pathetic. The only party at Holyrood seemingly prepared to oppose these biometric badges is the Scottish Liberal Democrats.
For once, the lack of LibDem representation in parliament – the party currently has only four MSPs – is a matter of regret. New leader Alex Cole-Hamilton has at least been refreshingly forthright: ‘I will state this clearly where others have not: I and my party are fundamentally opposed to vaccine passports as a matter of principle.’
This is the correct stance. Unfortunately, operators who will be most affected, such as the hospitality and entertainment sectors, are already falling into the trap of questioning the inconsistencies and impracticalities of implementation. Instead of conceding ground by quibbling over detail, it is the principle of vaccine passports which must vehemently be resisted. … Full article
Pro Forma Legal Letter For Parents of 12-15 Year-Olds Who Don’t Want Them to Get Jabbed
Lawyers For Liberty UK | September 2, 2021
Are you a parent? Is your 12-15 year old going back to school today? Are you worried about your child being given a Covid vaccine without your permission? Have you communicated with the school, but feel like you are being ignored?
Maybe you are concerned that ‘Gillick Competence‘ will be used to get your 12-15 year-old to make this complex decision alone?
Or that your child will be coerced or peer-pressured into making a decision without access to the full facts?
Lawyers for Liberty in association with the Jonathan Lea Network and Powerless 2 Powerful Parenting have created an anonymous “request a letter” to go from Lawyers for Liberty to your child’s school to let them know of the legal consequences of relying upon a child’s consent for a Covid vaccine, especially if a parent has specifically not consented.
We, as Lawyers For Liberty UK, will send an anonymous letter or email to schools on behalf of parents who are concerned about schools relying on their child to make a decision about whether or not to get jabbed.
If you’d like Lawyers For Liberty to send a letter or email on your behalf, fill in this form. You can read a note on the legal issues involved here and the pro forma letter here.
Named, shamed and fined – the maskless marauders

By Frederick Edward | TCW Defending Freedom | September 2, 2021
MAGISTRATES have been busy enforcing the laws of Covid-land, with more than 20 miscreants in Northamptonshire fined last week for failing to abide by the rules. They are named and shamed in the Northamptonshire Telegraph, the digital equivalent of the village stocks.
There are a few things to glean from the list of those convicted. We have a small insight, firstly, into the demographic shifts that are happening in the small towns of England such as Corby, Kettering and Wellingborough, with M Jatczak, K Marjani and P Blaga making an appearance.
The relative youth of those who found themselves in court is telling. J Ayre, 22, went to an outdoor gathering of more than two souls, for which he must pay £248. C Hulse, also 22, went to an indoor gathering of more than two. She has to pay £344.
While we do not know the circumstances of these individuals, it is a reminder of the price the youth have been made to pay throughout the last 18 months or so. Stuck in small accommodation or at home with their parents, they have suffered a disproportionate impact from restriction on movement. Moreover, the fines are not insignificant for those unlikely to have much disposable income.
Those caught refusing to abide by Covid regulations include:
U Aurica, 51, fined £344 for being in a corner shop without a mask;
C Oxlade, 21, found maskless in Budgens, as was E McIlreavy, 29, at Asda. Both fined £344;
L Stachura, 29, fined £344 for not wearing a face mask in a pizza takeaway.
R Gilderleft, 26, ‘left his home . . . without reasonable excuse’. He must pay £344.
The local paper website does not make it clear, but the prosecutions are likely to have been under the Coronavirus Act and Health Protection Regulations. Both pieces of legislation were passed in March 2020, the former without a vote in the Commons and the latter presented to the House only after it had come into force.
This is just a snapshot of cases involving Covid-19 rules. The Crown Prosecution Service reported in May 2021 – more than one year into the pandemic – that more than 1,800 had been brought to court, though a high proportion were subsequently identified as incorrectly charged. Indeed, between March 2020 and March 2021, all charges brought under the Coronavirus Act were incorrect, with not a single prosecution resulting from this large expenditure of police and court time.
Around 80 per cent of prosecutions brought under the Health Protection (Coronavirus, Restrictions) Regulations were correctly charged: it is under this legislation, which includes restrictions on leaving home, social gatherings and the enforcement of mask-wearing, that our Northamptonshire rebels were probably charged.
That a man living in England can be sentenced for leaving his own home is a sign of how far down the path of illiberalism we have strayed: never before in our history have we accepted such perverse rules, a fact made all the more unconscionable by their disproportionality.
What concerns me doubly is that they are enforced with such officiousness and subsequently reported so eagerly by an unquestioning and uncritical press. The Northamptonshire Telegraph says sanctimoniously: ‘The defendants were the latest to be convicted after violating emergency rules – which were designed to slow the spread of coronavirus – between January and April. Many of them were punished after failing to stick to the laws in January or February, at a time when many thousands died as the virus spiraled [sic] out of control.’
In any society which abandons the precepts of freedom, there will be a large group of people who willingly become the enforcers of the new regime. Intoxicated with power, they thrive amid a sea of petty regulations.
Naturally, one will not find names such as Matt Hancock of Neil Ferguson on the lists of those convicted. While the man on the street has the book thrown at him for daring to venture into a supermarket without a mask or seeing some friends, those in the right places and with the right connections can carry out their assignations without repercussion.
We can be convicted and fined for going to a takeaway without a mask, while our elites philander and jet around the world.
How much longer will we tolerate these glaring double standards?
UK Schoolchildren To Be Covid Vaxxed With Or Without Parental Consent
ALERT: ALL PARENTS IN U.K. WITH CHILDREN AGED 12 – 15 years
By Dr. Mike Yeadon | Health Impact News | August 26, 2021
I’ve just been informed via someone senior in the vaccination authorities that they will begin VACCINATING ALL SCHOOL CHILDREN AGED 12 – 15 years old STARTING SEPTEMBER 6th 2021.
WITH OR WITHOUT YOUR CONSENT.
Children are at no measurable risk from SARS-CoV-2 & no previously healthy child has died in U.K. after infection. Not one.
The vaccines are NOT SAFE. The USA reporting system VAERS is showing around 13,000 deaths in days to a few weeks after administration. A high % occur in the first 3 days. Around 70% of serious adverse events are thromboembolic in nature (blood clotting- or bleeding-related).
We know why this is: all of the gene-based vaccines cause our bodies to manufacture the virus spike protein & that spike protein triggers blood coagulation.
The next most common type of adverse events are neurological.
Death rates per million vaccinations are running everywhere at around 60X more than any previous vaccine.
Worse, thromboembolic events such as pulmonary embolisms, appear at over 400X the typical low rate after vaccination.
These events are serious, occur at a hideously elevated level & are at least as common in young people as in elderly people. The tendency is that younger people are having MORE SEVERE adverse events than older people.
There is literally no benefit whatsoever from this intervention. As stated, the children are unquestionably NOT AT RISK & vaccinating them WILL ONLY RESULT IN PAIN, SUFFERING, LASTING INJURIES AND DEATH.
Children rarely even become symptomatic & are very poor transmitters of the virus. This isn’t theory. It’s been studied & it pretty much doesn’t happen that children bring the virus into the home. In a large study, on not one occasion was a child the ‘index case’ – the first infected person in a household.
So if you’re told “it’s to protect vulnerable family members”, THAT IS A LIE.
The information emerging over time from U.K. & Israel is now showing clearly that the vaccines DO NOT EVEN WORK WELL. If there’s any benefit, it wanes.
Finally, the vaccines ARE NOT EVEN NECESSARY. There are good, safe & effective treatments.
IF YOU PERMIT THIS TO GO AHEAD I GUARANTEE THIS: THERE WILL BE AVOIDABLE DEATHS OF PERFECTLY HEALTHY CHILDREN, and severe illnesses in ten times as many.
And for no possible benefit.
KNOWING WHAT I KNOW FROM 40 years TRAINING & PRACTISE IN TOXICOLOGY, BIOCHEMISTRY & PHARMACOLOGY, to participate in this extraordinary abuse of innocent children in our care can be classified in no other way than MURDER.
It’s up to you. If I had a secondary school age child in U.K., I would not be returning them to school next month, no matter what.
The state is going to vaccinate everyone. The gloves are off. This has never been about a virus or public health. It’s wholly about control, totalitarian & irreversible control at that, and they’re nearly there.
PLEASE SHARE THIS INFORMATION WIDELY.
With somber best wishes,
Mike
VACCINATION: THEY’RE BECOMING DESPERATE
Computing Forever | August 21, 2021
Support my work here: https://computingforever.com/donate/
Support my work on Subscribe Star: https://www.subscribestar.com/dave-cullen
Follow me on Bitchute: https://www.bitchute.com/channel/hybM74uIHJKf/
Buy How is This a Thing Mugs here: https://teespring.com/stores/computing-forever-store
Source links:
https://www.irishmirror.ie/news/irish-news/irish-community-mourning-tributes-paid-24786114
https://www.which.co.uk/news/2021/08/travel-croatia-austria-vaccine-expiry-booster/
http://www.computingforever.com
KEEP UP ON SOCIAL MEDIA:
Gab: https://gab.ai/DaveCullen
Subscribe on Gab TV: https://tv.gab.com/channel/DaveCullen
Minds.com: https://www.minds.com/davecullen
Subscribe on Odysee: https://odysee.com/@ComputingForever
Revealed, the vaccine safety alert that drugs watchdog is ignoring
By Sally Beck | TCW Defending Freedom | September 1, 2021
FOR nearly a decade, Dr Tess Lawrie, MBBCh, DFSRH, PhD, has run the Evidence-Based Medicine Consultancy, an independent company concerned with rigorous medical research in healthcare.
She produces reports that can be found in the Cochrane Library, a respected organisation providing unbiased scientific paper analyses.
Dr Lawrie is a frequent member of technical teams developing international guidelines in the healthcare sector, and her peer-reviewed publications have received more than 3,000 citations. In short, Dr Lawrie should not be ignored.
Unless of course you are the Medicines and Healthcare products Regulatory Agency, the deaf-eared UK body regulating the novel, experimental, and under-tested Covid-19 mRNA and traditional vaccines.
With vaccine-associated deaths passing 1,600 in Britain, the MHRA should suspend the vaccination programme, like it did after 47 deaths caused by the Pandemrix swine flu jab.
However, it has no intention of doing so and continues to insist that the vaccine is ‘safe and effective and the best protection against Covid-19’.
Dr Lawrie sent Dr June Raine, the MHRA’s chief executive, a 39-page, fully-referenced paper criticising the agency’s complicated Yellow Card Scheme, a government system designed to collate information about adverse events caused by new drugs, as ‘not fit for purpose.’
She reminded Dr Raine, and copied in 15 of her colleagues, that they had a duty to ‘take any necessary action to minimise risk to individuals, after weighing risks against expected benefits.’ She pointed out that because of omissions in their data collecting, such as age and gender, and the timeframe of reaction post vaccination, the Yellow Card Scheme is non-transparent.
She said: ‘These omissions mean that basic conclusions about safety cannot be drawn. Consequently, the public and trial participants are not fully informed of the potential risks of taking a Covid-19 vaccine and are unable to give fully informed consent.’
Dr Lawrie concluded that the voluntary reporting system needed a complete overhaul, saying the Vaccine Adverse Event Reporting System (VAERS) in the US was doing a much better job giving citizens and healthcare professionals detailed information.
From VAERS’ database, she was able to conclude that more than 90 per cent of deaths occurred afterfirst vaccination and there was a clear link between vaccination and death, something MHRA members frequently say they cannot prove and insist is more than likely ‘coincidental’.
Speaking of VAERS, Dr Lawrie said: ‘From that system it is apparent that sporadic event reporting is high in number, as in the UK, and that there is a tight temporal relationship between Covid-19 vaccination and deaths: 15 per cent of deaths occurring within 24 hours, 22 per cent within 48 hours and in 37 per cent of deaths, the patient became unwell within 48 hours of Covid-19 vaccination with an event that led to their death.
‘The deaths analysed followed an almost equal number of Pfizer and Moderna Covid-19 vaccinations, and 91 per cent of deaths occurred after administration of the first Covid-19 vaccine.’
With the AstraZeneca #clotshot, which has not been approved for use in the US, double the number of people are impacted compared with Pfizer.
Dr Lawrie said that, as well as vaccine-induced immune thrombotic thrombocytopaenia (VITT), the European Medicines Agency has identified Guillain-Barreì Syndrome as a potential risk from the AstraZeneca vaccine.
It is adding a warning to the product information that ‘vaccinated persons need to seek immediate medical attention if they develop weakness and paralysis in the extremities.’
In conclusion, Dr Lawrie asked Dr Raine a simple question, yet to be answered: ‘Why is this clear safety signal not being acted upon by MHRA?’
This is an updated report published on August 26, 2021, detailing MHRA Yellow Card Reporting up to August 18:
• Pfizer – 21.3million people, 37.9million doses. Yellow Card reporting rate, one in 199 impacted.
• AstraZeneca – 24.8million people, 48.7million doses. Yellow Card reporting rate, one in 108 impacted.
• Moderna – 1.4million people, 2.1million doses. Yellow Card reporting rate, one in 100 impacted.
Overall, one in 135 people experience a Yellow Card Adverse Event from the 47.5million injected (20.7million men, women and children remain not injected in UK).
The Yellow Card reporting rate may be approximately ten per cent of actual figures, according to MHRA.
Proportional to the number of weeks each brand has been administered, currently the reported toll is:
• Approximately 47 linked deaths reported per week
• More than 10,500 reported adverse event injuries per week with unknown long-term consequences.
A significant proportion of these adverse events require urgent medical care, may be life-changing or long-lasting. These figures represent immense distress for those 351,404 people suffering adverse events and their families.
Reactions: 302,146 (Pfizer) + 816,393 (AZ) + 43,949 (Moderna) + 3,148 (Unknown) = 1,165,636.
Reports: 107,215 (Pfizer) + 229,134 (AZ) + 14,019 (Moderna) + 1,036 (Unknown) = 351,404.
Fatal: 508 (Pfizer) + 1,056 (AZ) + 17 (Moderna) + 28 (Unknown) = 1,609.
Acute Cardiac: 4,831 (Pfizer) + 9,102 (AZ) + 495 (Moderna) + 35 (Unknown) = 14,463.
Pericarditis/Myocarditis (Heart inflammation): 362 (Pfizer) + 245 (AZ) + 65 (Moderna) + 2 (Unknown) = 674
Anaphylaxis: 466 (Pfizer) + 810 (AZ) + 32 (Moderna) + 1 (Unknown) = 1,309
Blood Disorders: 10,283 (Pfizer) + 7,354 (AZ) + 829 (Moderna) + 44 (Unknown) = 18,510.
Infections: 7,116 (Pfizer) + 18,102 (AZ) + 730 (Moderna) + 89 (Unknown) = 26,037
Herpes: 1,574 (Pfizer) + 2,475 (AZ) + 75 (Moderna) + 13 (Unknown) = 4,137.
Headaches: 21,646 (Pfizer) + 83,513 (AZ) + 2576 (Moderna) + 229 (Unknown) = 107,964
Migraine: 2,474 (Pfizer) + 8,015 (AZ) + 284 (Moderna) + 29 (Unknown) = 10,802.
Eye Disorders: 5,025 (Pfizer) + 13,718 (AZ) + 495 (Moderna) + 55 (Unknown) = 19,293.
Blindness: 99 (Pfizer) + 281 (AZ) + 12 (Moderna) + 4 (Unknown) = 396.
Deafness: 185 (Pfizer) + 360 (AZ) + 13 (Moderna) + 2 (Unknown) = 560.
Psychiatric Disorders: 6,135 (Pfizer) + 17,011 (AZ) + 884 (Moderna) + 74 (Unknown) = 24,104.
Skin Disorders: 21,263 (Pfizer) + 50,240 (AZ) + 6,657 (Moderna) + 211 (Unknown) = 78,371.
Spontaneous Miscarriages: 278 + 6 stillbirth/foetal death (Pfizer) + 195 + 2 stillbirth (AZ) + 24 + 1 foetal death (Moderna) + 1 (Unknown) = 499 + 9 (figures imply 20 related maternal deaths – four more this week alone).
Vomiting: 3,242 (Pfizer) + 11,347 (AZ) + 496 (Moderna) + 41 (Unknown) = 15,126.
Facial Paralysis including Bell’s Palsy: 691 (Pfizer) + 860 (AZ) + 48 (Moderna) + 5 (Unknown) = 1,604.
Nervous System Disorders: 52,947 (Pfizer) + 173,935 (AZ) + 6788 (Moderna) + 600 (Unknown) = 234,270.
Strokes and CNS haemorrhages: 496 (Pfizer) + 1,993 (AZ) + 17 (Moderna) + 9 (Unknown) = 2,515
Guillain-Barré Syndrome: 42 (Pfizer) + 388 (AZ) + 2 (Moderna) + 5 (Unknown) = 437.
Tremor: 1,288 (Pfizer) + 9673 (AZ) + 153 (Moderna) + 38 (Unknown) = 11,152.
Pulmonary Embolism and Deep Vein Thrombosis: 601 (Pfizer) + 2,696 (AZ) + 25 (Moderna) + 18 (Unknown) = 3,340.
Respiratory Disorders: 12,950 (Pfizer) + 27,425 (AZ) + 1,138 (Moderna) + 109 (Unknown) = 41,622.
Seizures: 713 (Pfizer) + 1,874 (AZ) + 119 (Moderna) + 9 (Unknown) = 2715
Paralysis: 301 (Pfizer) + 735 (AZ) + 39 (Moderna) + 6 (Unknown) = 1,081.
Haemorrhage (All types): 2,568 (Pfizer) + 4713 (AZ) + 321 (Moderna) + 24 (Unknown) = 7,626.
Vertigo/Tinnitus: 2,692 (Pfizer) + 6313 (AZ) + 271 (Moderna) + 25 (Unknown) = 9,301.
Renal & Urinary Disorders: 795 (Pfizer) + 2,507 (AZ) + 93 (Moderna) + 23 (Unknown) = 3,418
Reproductive/Breast: 17,108 (Pfizer) + 16,689 (AZ) + 2,215 (Moderna) + 120 (Unknown) = 36,132.
For full reports see Annex One.
BOMBSHELL UK data destroys entire premise for vaccine push
By Chris Waldburger | August 21, 2021
This is an absolute game-changer.
The UK government just reported the following data, tucked away in their report on variants of concern:
Less than a third of delta variant deaths are in the unvaccinated.
Let me say that another way – two-thirds of Delta deaths in the UK are in the jabbed.
To be specific:
From the 1st of February to the 2nd of August, the UK recorded 742 Delta deaths (yes, the dreaded Delta has not taken that much life).
Out of the 742 deaths, 402 were fully vaccinated. 79 had received one shot. Only 253 were unvaccinated.
The report is here.
But this is the crucial page. Look at the bottom line.

Again, 402 deaths out of 47 008 cases in vaccinated; 253 deaths out of 151 054 cases in unvaccinated. If you get covid having been vaccinated, according to this data, you are much more likely to die than if you were not vaccinated!
Obviously some allowance must be made for more elderly people being vaccinated, but not enough to change the bottom line: this vaccine is not nearly as effective as advertised.
And with all its unknowns, and a much higher adverse reporting number than all other vaccines combined, a complete recalibration of global policy is the only moral option.
Countries around the world, as months pass since vaccinations, are experiencing a surge in vaccinated deaths and hospitalizations. 60% of hospitalizations in Israel are fully vaccinated patients. (Hence the mad rush for untested boosters.)
The powers that be will not admit there is something terribly wrong. They will not acknowledge the clear science that people with natural immunity, and the young and healthy, do not need to take the risks of these injections. Read this very important piece on natural immunity. Reliable studies showing the superiority of natural immunity are just ignored by our overlords.
Instead they will jab and jab and jab again. The vaccine passports will be renewable every six months. Countries are ordering up to 8 shots per citizen. The masks will not go away. Israel, the pre-eminent vaxxed nation, is in lockdown.
The report also made one other important admission:

In other words, getting vaccinated to protect others is not true!
This is NOT a sterilising vaccine that stops diseases like polio or hepatitis using live virus. This is for you alone. Which means, as experts like Martin Kulldorff, biostatistician, epidemiologist and professor of medicine at Harvard Medical School, and Jay Bhattacharya, professor of medicine at Stanford University and research associate at the National Bureau of Economic Research, have long said, it makes zero sense to vaccinate the young and healthy.
We are dealing with a world-historical error, and in fact a global assault on young bodies.
To be clear, I make no advice to anybody about taking the vaccine or not. I may well have decided to take it if I were in a risk category, or if I knew I did not have to wear a mask or get tested after taking a single shot. Your decision should be guided by consulting with a doctor, informed consent, and your own conscience.
And you should ask yourself why there is no explanation for the hundreds of thousands of women experiencing menstrual changes after the shot, or the way vaccines are being mandated at the same time they are under investigation for unknown risks.
What I will say categorically is that you will have to answer one day, in this life or the next, for where you stood on the issue of mandating medicine for the healthy without informed consent, on giving cover for governments to shove things down kids’ noses, and locking down all that makes life worthwhile. Where were you when kids’ freedoms were stolen from them? I doubt there will be much forgiveness from that generation.
Every time somebody posts a meme mocking vaccine hesitance, not only do they alienate the hesitant, and radicalize them, they implicitly endorse a new police state in which a liberal government like Australia feels empowered to pepper spray kids in the face for not wearing a mask that has not been conclusively shown to prevent viral transmission.
For crying out loud, this what even the World Health Organization admits about masks:

The vaccines will not end these measures, especially in countries with low vaccination rates. They cannot, unless these governments admit their massive errors. Their booster shot push makes this unlikely.
Finally, why does the media not even report on governmental data? Why am I reporting this stuff?
I have no idea, but it is truly sinister.
Ask yourself why the media will not even mention the fact that this 23-year-old Irish footballer below, in perfect health, received a vaccine three days before dropping dead:

Untimely indeed.
God have mercy.
The Latest Paper From Neil Ferguson et al. Defending the Lockdown Policy is Out of Date, Inaccurate and Misleading

By Mike Hearn • The Daily Sceptic • August 24, 2021
Neil Ferguson’s team at Imperial College London (ICL) has released a new paper, published in Nature, claiming that if Sweden had adopted U.K. or Danish lockdown policies its Covid mortality would have halved. Although we have reviewed many epidemiological papers on this site, and especially from this particular team, let us go unto the breach once more and see what we find. The primary author on this new paper is Swapnil Mishra.
The paper’s first sentence is this:
The U.K. and Sweden have among the worst per-capita Covid mortality in Europe.
No citation is provided for this claim. The paper was submitted to Nature on March 31st, 2021. If we review a map of cumulative deaths per million on the received date then this opening statement looks very odd indeed:
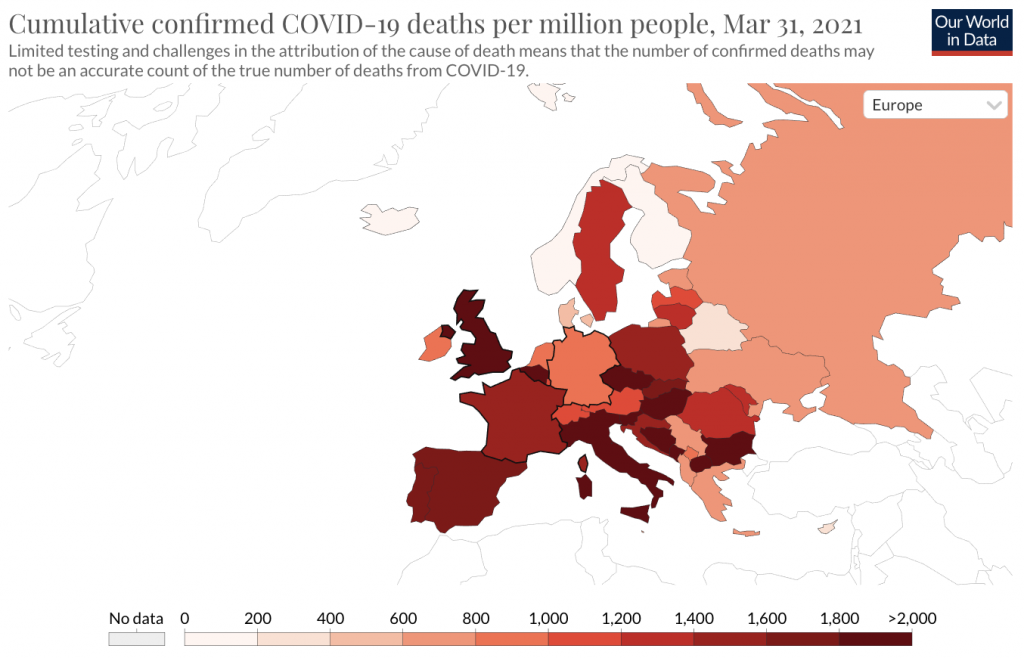
Sweden (with a cumulative total of 1,333 deaths/million) is by no means “among the worst in Europe” and indeed many European countries have higher totals. This is easier to see using a graph of cumulative results:
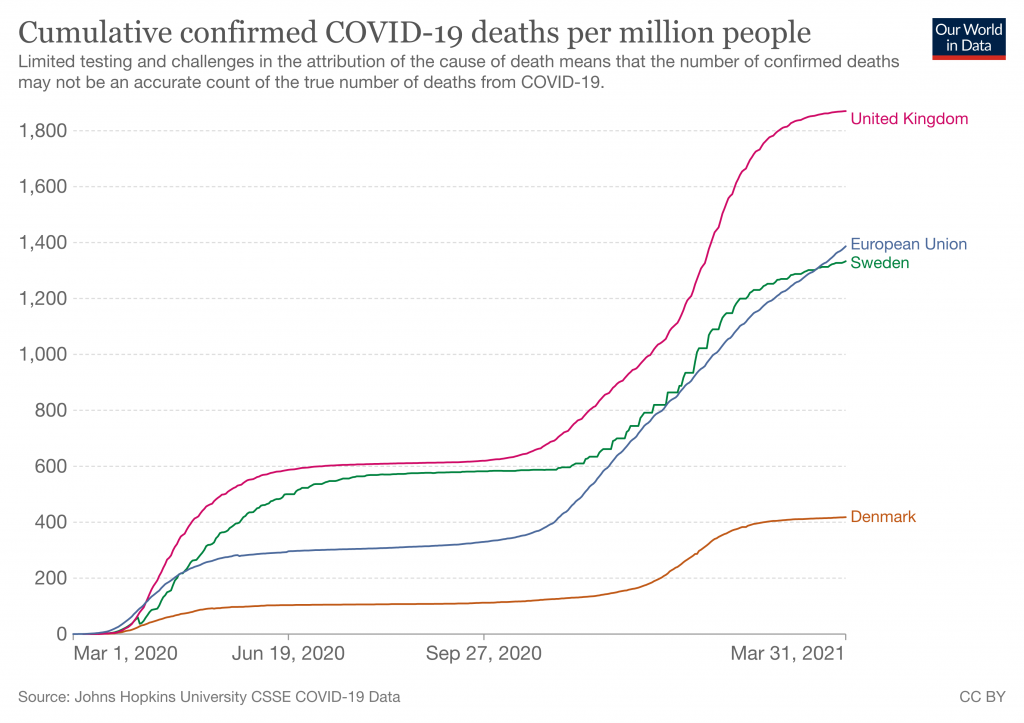
But that was in March, when the paper was submitted. We’re reviewing it in August because that’s when it was published. Over the duration of the journal’s review period this statement – already wrong at the start – became progressively more and more incorrect:
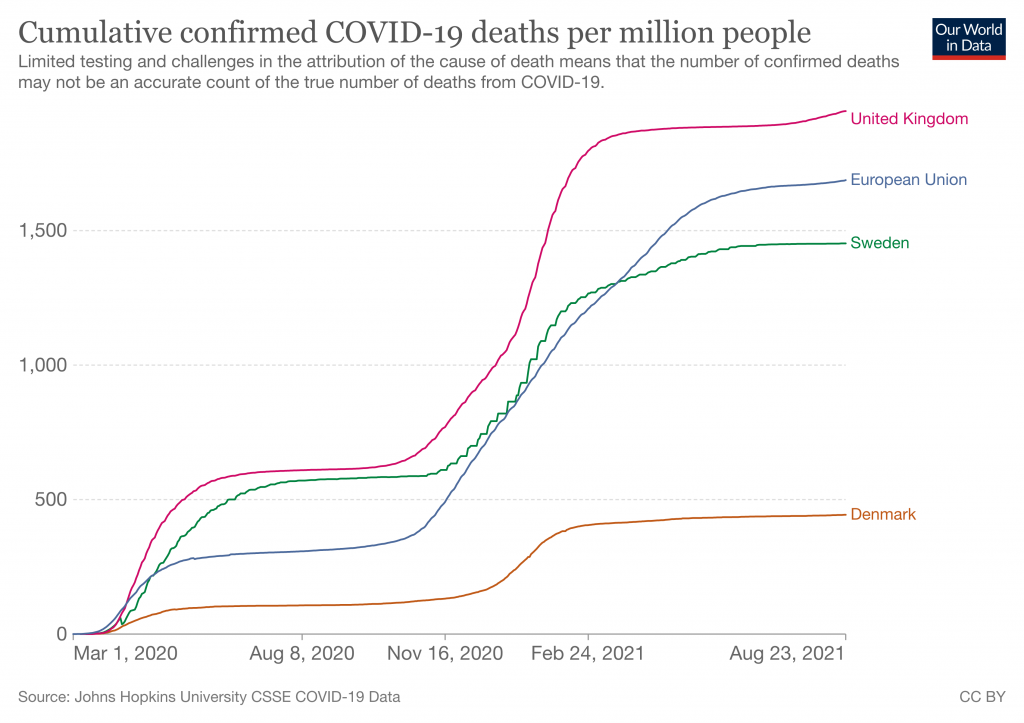
As always, we must note that these ‘death’ graphs can be heavily affected by testing levels, because Covid deaths are defined as any death within 28 days of a positive test. The U.K. tests much more than Sweden does. But putting that to one side, Sweden by now has significantly better results than the rest of the E.U. What’s going on here? A likely explanation is that although the paper was submitted in March it was actually written some time last year, probably starting around the end of the summer and finishing up in August. There then followed a strange many month gap before they submitted it, and then many more months were added by the glacial peer review process journals use. We can see evidence of this timeline in the abstract, where they say:
We use two approaches to evaluate counterfactuals which transpose the transmission profile from one country onto another, in each country’s first wave from March 13th (when stringent interventions began) until July 1st, 2020.
More evidence comes from the upload dates on the released code, which is from 10 months ago. In other words, Nature is publishing a paper about the fast-moving coronavirus situation that builds its entire case on obsolete data more than a year old, without explicitly noting that anywhere. In July 2020, Sweden and the U.K. did indeed have worse results than the rest of the E.U. However as we now know, this meant nothing and a year on the data looked very different.
Why did ICL wait so long before submitting this paper to Nature? No obvious explanation occurs. And why didn’t anyone notice that the claims were no longer true? Not for the first time, it appears nobody can actually be reading these papers adversarially before publication. Time and again we see that at major scientific journals the lights are on, but nobody’s home.
Seeing this made me wonder if they were once more engaging in a favourite trick of this team, by using Verity et al.‘s obsolete infection:fatality ratio estimates from January 2020. And indeed they are:
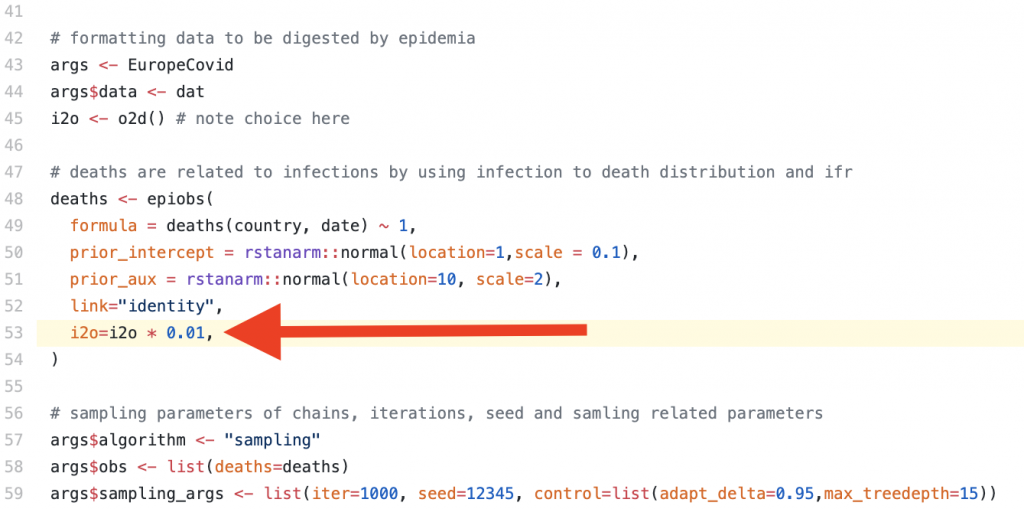
The idea that 1% of all SARS-CoV-2 infections would lead to death was later disputed as being ~4x too high by a meta-study of seroprevalence data published by the WHO. This newer estimate was based on far larger sample sizes, and serosurveys give an ability to detect people who recently had mild disease without getting tested or reporting it at the time. It’s thus a much more scientifically robust method of IFR estimation than Verity’s paper, which being written very early on had to rely on media reports and questionably reliable information coming out of China. As the authors discuss in the supplementary material, using a lower IFR (they try 0.5) means that the U.K.’s predicted mortality from adopting the Swedish strategy drops significantly due to the changed impact of herd immunity.
Who is responsible for this situation? Nature appears to be knowingly publishing a paper on Covid that makes claims in the present tense, but which is in reality so out of date that the very first sentence is factually false. This is not merely useless but actively damaging because non-academic readers (i.e., politicians and public health officials) will reasonably assume that claims published by scientists about Covid in August 2021 were actually written in August and have some relevance to the current situation. Nowhere is it explicitly stated at what time the analysis was believed to be accurate: it must instead be inferred from the choice of datasets and audit trails left on the source code hosting site they use.
Overall approach
Moving on. What does the model actually do?
The core concept is to try and calculate the changing infectiousness of SARS-CoV-2 for each of the U.K., Sweden and Denmark over time, then ‘graft’ the generated timeseries for R(t) onto the other countries. As is typical for this team, the authors assume that changes in Rt are driven only by government interventions or voluntary behavioural changes, and thus by transposing Rt onto other countries they claim to be calculating what would have happened if different countries had adopted each other’s policies. They try two different approaches to this, an ‘absolute’ and a ‘relative’ approach.
There are many problems with this methodology.
The study of only the U.K., Sweden and Denmark has no scientific basis. Why Denmark and not, say, France? This selection is very obviously politically motivated. In fact, the entire paper is basically a policy paper designed to influence politicians, not answer any question about viruses that a real scientist might ask.
With the benefit of 2021 hindsight we can argue persuasively that lockdowns had no real impact on Covid. The most recent and effective demonstration of that was the U.K.’s ‘Freedom Day’ in which cases dropped off a cliff just days after restrictions were relaxed, in defiance of the warnings of “international health leaders” that this would be “foolish” and “unethical”, a “threat to the world”, etc. There have been many other such events and analyses of global datasets show no correlation between lockdowns and health outcomes. Thus their underlying assumption that social policy is responsible for different outcomes is wrong. In fact, although they are well aware that there must be many factors influencing mortality outcomes, they explicitly disregard all of them: “While we cannot fully encompass the myriad of differences between each country, our analysis is nonetheless informative on best practice for control of future waves of the Covid pandemic.”
Despite asserting that their analysis can tell lawmakers what to do in future epidemics, they later admit that “our counterfactual scenarios should be interpreted as a exchange of both population behaviour and government policy between donor and recipient countries“. This is important for them to admit because they tried to explain why Covid has varying infectiousness in different countries by reference to “cultural differences“, which they boil down to a single statistic about the proportion of single person households in each country. But this is illogical nonsense. Even if we (wrongly) assume that all differences in observed outcomes are to do with policy and culture, governments cannot magically make the U.K. population become Danish or vice-versa. Any analysis that assumes this and claims to be “informative on best practice” is wrong and should have been dropped during peer review.
The paper has another difficulty with being “informative“. Although the authors propose two different approaches to try and answer the same underlying question, the two approaches give totally different answers. For example: “If Denmark followed U.K. policies, our relative approach estimates that mortality would not have been markedly different, although our absolute approach implies that mortality would have been more than twice that observed.” Their calculations aren’t even consistent with each other, yet the paper provides no specific recommendation on which approach is supposed to yield the best answer.
Other problems include an inability to actually calculate Rt from death data (“the high variance of this distribution leads to high uncertainty in Rt estimates“), even though their entire analysis is based on the presumed integrity of that calculation, and an implausibly high sensitivity to the exact starting date of policy changes (“a three-day difference in the introduction of measures can lead to twofold differences in mortality“). The strength of this connection in their model is absurd and would appear to be strongly motivated by ICL’s attempted rewriting of history to one of: “If only the Government had listened to us sooner everything would have been far better.”
Conclusion
Given the history of this department, it’s no surprise that ICL is still churning out delusional and misleading epidemiology papers. They will continue doing so for as long as they’re funded. Analysing each and every one is a futile effort due to the sheer scale at which academia operates (e.g. this paper alone has 19 authors). But we can nonetheless learn some more about bad science by reading them. This paper shows all the usual hallmarks of an academic sector that’s gone off the rails:
- A grotesque level of data cherry picking.
- A publishing process so slow that the claims are entirely wrong on the date of publication, and wrong from literally the first sentence.
- A delusional belief that their work is “informative” to policy makers, despite implicitly arguing that entire societies can be transplanted from one country to another.
Who is ultimately responsible for stopping this? It must be the funders, who for this paper include:
- The National Institute for Health Research
- The Bill and Melinda Gates Foundation
- The U.K. Medical Research Council
- Community Jameel (a Saudi family foundation)
- Microsoft, who donated free compute time on Azure
- And finally, universities and other institutions who subscribe to Nature despite its history of publishing misleading papers
The theme here is that none of these organisations is paying close attention to what’s actually being written, apparently including the journals and peer reviewers. For funders, giving away money is not the means but the end. Until research is funded by people who actually care about the utility of the results our society will continue to be flooded with highly evolved scientism, of which the output of the ICL Epidemiology Department is a textbook example.
Mike Hearn is a former Google software engineer. You can read his blog here.
ALERT: All Parents In U.K. With Children Aged 12 – 15 years
By Dr. Mike Yeadon | August 26, 2021
I’ve just been informed via someone senior in the vaccination authorities that they will begin VACCINATING ALL SCHOOL CHILDREN AGED 12 – 15 years old STARTING SEPTEMBER 6th 2021.
WITH OR WITHOUT YOUR CONSENT.
Children are at no measurable risk from SARS-CoV-2 & no previously healthy child has died in U.K. after infection. Not one.
The vaccines are NOT SAFE. The USA reporting system VAERS is showing around 13,000 deaths in days to a few weeks after administration. A high % occur in the first 3 days. Around 70% of serious adverse events are thromboembolic in nature (blood clotting- or bleeding-related).
We know why this is: all of the gene-based vaccines cause our bodies to manufacture the virus spike protein & that spike protein triggers blood coagulation.
The next most common type of adverse events are neurological.
Death rates per million vaccinations are running everywhere at around 60X more than any previous vaccine.
Worse, thromboembolic events such as pulmonary embolisms, appear at over 400X the typical low rate after vaccination.
These events are serious, occur at a hideously elevated level & are at least as common in young people as in elderly people. The tendency is that younger people are having MORE SEVERE adverse events than older people.
There is literally no benefit whatsoever from this intervention. As stated, the children are unquestionably NOT AT RISK & vaccinating them WILL ONLY RESULT IN PAIN, SUFFERING, LASTING INJURIES AND DEATH.
Children rarely even become symptomatic & are very poor transmitters of the virus. This isn’t theory. It’s been studied & it pretty much doesn’t happen that children bring the virus into the home. In a large study, on not one occasion was a child the ‘index case’ – the first infected person in a household.
So if you’re told “it’s to protect vulnerable family members”, THAT IS A LIE.
The information emerging over time from U.K. & Israel is now showing clearly that the vaccines DO NOT EVEN WORK WELL. If there’s any benefit, it wanes.
Finally, the vaccines ARE NOT EVEN NECESSARY. There are good, safe & effective treatments.
IF YOU PERMIT THIS TO GO AHEAD I GUARANTEE THIS: THERE WILL BE AVOIDABLE DEATHS OF PERFECTLY HEALTHY CHILDREN, and severe illnesses in ten times as many.
And for no possible benefit.
KNOWING WHAT I KNOW FROM 40 years TRAINING & PRACTISE IN TOXICOLOGY, BIOCHEMISTRY & PHARMACOLOGY, to participate in this extraordinary abuse of innocent children in our care can be classified in no other way than MURDER.
It’s up to you. If I had a secondary school age child in U.K., I would not be returning them to school next month, no matter what.
The state is going to vaccinate everyone. The gloves are off. This has never been about a virus or public health. It’s wholly about control, totalitarian & irreversible control at that, and they’re nearly there.
PLEASE SHARE THIS INFORMATION WIDELY.
With somber best wishes,
Mike
Dr Mike Yeadon
The Dubious Ethics of ‘Nudging’ the Public to Comply With Covid Restrictions

By Dr. Gary Sidley | The Daily Sceptic | August 22, 2021
A middle-aged woman, walking along a pavement in the afternoon sunshine, sees a young family approaching and instantly becomes stricken with terror at the prospect of contracting a deadly infection. A man in a queue in a garage kiosk leans into the face of another and screams, “You selfish idiot! Hundreds of people will die because you don’t wear a mask.” The aggressor is oblivious to the fact that his victim suffers a history of asthma and anxiety problems. A neighbour puts on a face covering and plastic gloves before wheeling her dustbin to the end of her drive. These are three recent examples of many similar events I’ve observed or read. What could be the main reason for such extraordinary behaviour? Has the emergence of the SARS-COV-2 virus magically re-wired our brains, transforming many of us into vindictive germaphobes?
No, of course not. These extreme human reactions are, I believe, primarily the result of the Government’s deployment of covert psychological ‘nudges’, introduced as a means of increasing people’s compliance with the Covid restrictions.
In an article in the Critic, I discussed the remit of the Government’s behavioural scientists in the Scientific Pandemic Insights Group on Behaviours (SPI-B), a subgroup of SAGE which offers advice to the Government about how to maximise the impact of its Covid communications strategy. The methods of influence recommended by the SPI-B are drawn from a range of ‘nudges’ described in the Institute of Government document, MINDSPACE: Influencing behaviour through public policy, several of which primarily act on the subconscious of their targets – the British people – achieving a covert influence on their behaviour. The three ‘nudges’ to have evoked the most controversy, among both psychological practitioners and the general public, are: the strategic use of fear (inflating perceived threat levels); shame (conflating compliance with virtue); and peer pressure (portraying non-compliers as a deviant minority) – or ‘affect’, ‘ego’ and ‘norms’, to use the language of behavioural science. (Specific examples of how each of these covert strategies have been used throughout the Covid crisis are described here).
The British Psychological Society (BPS) is the leading professional body for psychologists in the U.K. According to their website, a central role of the BPS is: “To promote excellence and ethical practice in the science, education and application of the discipline.” In light of this remit, I – together with 46 other psychologists and therapists – wrote a letter to the BPS on January 6th, 2021, expressing our ethical concerns about the use of covert psychological strategies as a means of securing compliance with Covid restrictions. In particular, our alarm centred on three areas: the recommendation of ‘nudges’ that exploit heightened emotional discomfort as a means of securing compliance; implementing potent covert psychological strategies without any effort to gain the informed consent of the British public; and harnessing these interventions for the purpose of achieving adherence to contentious and unevidenced restrictions that infringe basic human rights.
Responses from the BPS to our initial letter were slow and circuitous. However, on July 1st we received an email from Dr. Roger Paxton, the Chair of the Ethics Committee, which clarified the BPS’s position: in the Committee’s view, there is nothing ethically questionable about deploying covert psychological strategies on the British people as a means of increasing compliance with public health restrictions.
An in-depth inspection of Dr. Paxton’s defence of the BPS reveals that it is evasive, disingenuous and wholly unconvincing.
First, he quibbles about the use of the word “covert”, arguing that the compliance techniques under scrutiny are more appropriately described as “indirect”. Behavioural-science documents routinely refer to the psychological strategies underpinning Government communication campaigns as evoking responses from people that are “unconscious”, “subconscious” or “automatic”. The crucial point is that the human targets of these ‘nudges’ are often unaware that the intention of the SPI-B psychologists is to scare, shame them and socially pressure them to conform. The MINDSPACE publication – co-authored by Professor David Halpern, an SPI-B and SAGE member – seems to concur: “Citizens may not fully realise that their behaviour is being changed… Clearly, this opens Government up to charges of manipulation… [as] it may offer little opportunity for citizens to opt-out.” (p. 66)
Second, Dr. Paxton rejects the idea that it would be ethical to offer citizens an opportunity to opt-out by asserting that the application of covert psychological strategies to shape people’s behaviour falls outside the realm of individual consent. The BPS appears to be claiming that an appeal to some nebulous, ideologically-driven concept of social decision-making exempts psychologists from the fundamental requirement to seek a person’s informed agreement before delivering an intervention. So according to the BPS – the formal guardians of ethical practice in the U.K. – the Covid communications strategy, aimed at achieving mass behavioural change, was intended to influence some anonymous collective rather than the actions of as many individuals as possible.
Again, the BPS stance is at odds with Professor Halpern’s position. In his 2019 book, Inside the Nudge Unit, he states: “If Governments… wish to use behavioural insights, they must seek and maintain the permission of the public. Ultimately, you – the public, the citizen – need to decide what the objectives, and limits, of nudging and empirical testing should be.” (p. 375)
Third, Dr. Paxton’s claim that the levels of fear throughout the Covid pandemic were proportionate to the viral threat is ill-informed and does not stand up to scrutiny. The minutes of the SPI-B meeting of March 22nd, 2020, demonstrate that its endorsement of a covert psychological strategy was a calculated decision to scare the British people, recommending that: “The perceived level of personal threat needs to be increased among those who are complacent… using hard-hitting emotional messaging.” In her book, A State of Fear, Laura Dodsworth interviewed members of SPI-B who confirmed that there had been a concerted effort to elevate the fear levels of the general public. One committee member, Educational Psychologist Dr. Gavin Morgan, admitted: “They went overboard with the scary message to get compliance.” Another SPI-B member – who wished to remain anonymous – was even more forthright: “The way we have used fear is dystopian… The use of fear has definitely been ethically questionable. It’s been like a weird experiment. Ultimately, it backfired because people became too scared.”
The mission to indiscriminately instil fear in the British public has been highly effective. An opinion poll prior to ‘Freedom Day’ suggested most people were worried about the prospect of lifting the remaining Covid restrictions. Even now, when all the vulnerable groups have been offered vaccination, many of our citizens remain tormented by ‘Covid Anxiety Syndrome’ – a disabling combination of fear and maladaptive coping strategies – with 20% of the population ‘markedly affected’. And this psychology-assisted fear inflation will be responsible for a substantial proportion of the extensive collateral damage associated with the restrictions, including excess non-Covid deaths and mental health problems.
Fourth, Dr. Paxton’s response makes no reference to the use of shame and scapegoating, and whether these are acceptable strategies for a civilised society to use. One can only assume that the BPS either views these tactics as acceptable, or that they seek to avoid acknowledging that psychologists have recommended practices that, in some respects, resemble the methods used by totalitarian regimes such as China, where the state inflicts pain on a subset of its population in an attempt to eliminate beliefs and behaviour they perceive to be deviant.
The dismissal of our ethical concerns by the BPS was predictable: a cursory glance at the scientists comprising the SPI-B shows that several of its members are also influential figures in the BPS; a major conflict of interest that renders the impartiality of their views highly questionable. What was surprising was the strident tone of Dr. Paxton’s rejoinder, as exemplified by his assertion that the psychologists’ role in the pandemic response demonstrated “social responsibility and the competent and responsible employment of psychological expertise”. I suspect the lady trembling on the pavement, the young man being verbally abused in the garage, and the neighbour donning mask and gloves to wheel out her dustbin – along with the many others in similar positions – might all beg to differ.
Dr. Gary Sidley is a retired NHS Consultant Clinical Psychologist.
NHS plans Covid-19 vaccination for 12-year-olds that would NOT require parental permission – reports
RT | August 26, 2021
The UK National Health Service (NHS) has reportedly made plans to vaccinate children as young as 12 without the need for their parents’ permission – a plan that government advisers have not yet supported.
Under the NHS’ plan, children between the ages of 12 and 15 would start being vaccinated in less than two weeks’ time after returning to school following the summer holidays, according to The Telegraph, which obtained emails sent by the NHS’ regional offices. The newspaper also reported on Thursday that the children “would not need parental consent” to get vaccinated.
Though Pfizer’s Covid-19 vaccine has been approved in the UK for children aged 12 and over, the Department of Health said on Wednesday that a decision on the vaccination of young children had not yet been made.
Government advisers on the Joint Committee on Vaccination and Immunisation (JCVI) have been reviewing whether to approve widespread vaccination of children, but had earlier said only children with certain health conditions would receive jabs.
Earlier this month, England’s deputy chief medical officer, Jonathan Van-Tam, expressed his support for the vaccination of under 18s, claiming to be “very much in favour” of 16- and 17-year-olds getting jabbed.
Vam-Tam also said that it was “more likely rather than less likely” that the number of children between the ages of 12 and 15 who were eligible to get vaccinated would soon expand.
News of the NHS’ plan angered many people on social media who pointed out that the risk vs reward conclusion for vaccinating young children was still uncertain.
Reform Party leader Richard Tice called the plan “shocking” while pub entrepreneur Hugh Osmond called it “grotesque.” Conservative academic Adrian Hilton – a former adviser to Cabinet Office Minister Michael Gove – pointed out that “12-year-olds cannot consent to a medical procedure.”
Other Brits protested that “the government does not own my child” and threatened to pull their children out of public schooling.
Some supported the idea, with one Welsh social media user stating that she agreed 12- to 15-year-olds “can consent” and are “mature enough to make that call,” but thought it should be “done near to medical care like mine was, not in school.”
In the United States, the Centers for Disease Control and Prevention (CDC) advises all Americans aged 12 and over to get vaccinated against Covid-19. Roughly 600,000 children between the ages of 12 and 15 were vaccinated in less than a week after Pfizer’s vaccine was approved for under 16s in May.
Many European Union countries have also started vaccinating children, with the EU approving Pfizer for 12- to 15-year-olds in May and Moderna in July.
Featured Video

Seyed Marandi: Trump lost the Iran war – Must sell it as victory
or go to
Aletho News Archives – Video-Images
From the Archives
The Balfour Declaration – A Century of Jewish Power
By Gilad Atzmon | May 17, 2017
This year, Palestinians and their supporters mark the 100th anniversary of The Balfour Declaration, a written statement from the United Kingdom’s Foreign Secretary, Arthur James Balfour, to Walter Rothschild, a leader of the British Jewish community, in favour of the establishment of a Jewish national home in Palestine.
For Palestinians, The Balfour Declaration was the beginning of their plight: a century of ethnic cleansing at the hands of European newcomers who claim Palestine as their historic home. Yet, for some reason, supporters of the Palestinians are desperate to suppress discussion of the motivation for the Balfour Declaration – how and why did it come about? … continue
Blog Roll
 Aletho News
Aletho News- Seyed M. Marandi: Trump Lost the Iran War – Must Sell It as a Victory
- Iran, Saudi FMs hold phone talks as Persian Gulf states rethink US ties
- The Illusions of Western Virtue: Ursula von der Leyen and Europe’s Moral Bankruptcy
- AIPAC-backed candidates lose New York primaries as voters reject pro-genocide lobby
- The West’s Post-Soviet ‘Democracy’ Playbook
- UK suppressed intel on Sudan genocide to protect UAE ties: Report
- Starmer’s exit exposes dirty secret: UK can’t afford Ukraine War
- Putin Warns the West: Russia Is Ready
- BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
- There Are No Budget Constraints In New York City: “Coastal Resiliency” Edition
- If Americans Knew
- Israel’s Attacks on Gaza’s Children (Photos)
- ‘His only crime is that he is a Palestinian doctor’
- ‘Killed pursuing her dream’: Gaza girl on her way to school dies in Israeli drone strike
- Unbelievable pressure on Gaza from Israel, “Board of Peace” – Daily Update
- UN: Israel Continues to Commit Genocide and Other Atrocity Crimes by Deliberately Targeting Palestinian Children
- Bari Weiss, Free-Speech Fraud & Zionism Promoter, Would Rather Deport Than Debate
- ‘Doctor of the Poor’: Israeli Occupation Arrests Prominent Palestinian Physician
- Search for Your Church (and see if it has been targeted by the Israeli gov’t)
- Mark Levin Flying to Israel as Netanyahu Reportedly Seeks to ‘Leverage’ Levin to Trash Trump’s Iran Deal
- Watch: Zionist Brags about Israel’s Power to Get the World to Do What Israel Wants
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
