Sliding doors
The publication of Prozac Nation was a societal inflection point that ushered in multiple pharmacological disasters
By Toby Rogers | October 5, 2022
I. The Promise
In the late 1980s/early 1990s my parents spent a small fortune to send me to what was, at the time, the top-ranked small liberal arts college in the country. While the Ivies train up the future ruling class, small private liberal arts colleges offered something far more alluring.
Hanging in the air at these small private colleges was a promise that went something like this: the social sciences, particularly psychology and sociology, have figured things out. If we just follow their wise teachings, we will emerge in a utopian society where there is depth and meaning, people are decent and real with each other, differences are worked out (through “I” statements and “position switching” amongst other tools), and above all people are happy.
I imagine it began with Freud and Jung, accelerated with Foucault and Butler, but it was also present in the pragmatic psychologists including Barry Schwartz and the later happiness researchers.
The promise co-opted the central notion of many 20th century revolutions — that a new man and new woman were being born from the ashes of the old system and that we would find better ways of relating to each other than any society heretofore.
This promise was EVERYWHERE — from the new student orientation to the mandatory date rape prevention workshops to resident advisor trainings to student clubs and late-night conversations in the common areas of the dorms. A better world was possible and we were the ones to usher it in. The promise was going to radiate out to the rest of society like a pebble dropped into a pond.
It’s heartbreaking to reflect on this now because: 1.) the promise was never fulfilled (perhaps because it was always just a fantasy); and, 2.) to the extent that this vision soldiers on in some form it has taken an incredibly dark turn and now resembles fascism more than anything else.
II. An inflection point
Elizabeth Wurtzel was a fierce talent. Yes, she went to Harvard but she was the embodiment of the promise. A third wave feminist, she was unabashed in her celebration of sexuality and pleasure. As a writer she was a sorceress — able to pull magic, truth, and wisdom out of thin air.

Ms. Wurtzel popularized the Pain & Suffering Memoir genre with the publication of her book Prozac Nation in 1994. The book was raw, confessional, and witty. It felt like she had discovered capital T Truth. She went inside, as the psychologists (and Buddhists) had trained us to do, explored her emotional pain with all of its searing intensity, and redeemed it by giving it meaning. Ms. Wurtzel modeled how to be vulnerable, ironic, and strong. By the end of the book she was our friend and shrink. She had gone through the dark night of the soul and had come out on the other side, victorious.

I loved Prozac Nation and I’m devastated by what has transpired since.
III. The misuse of a once-in-a-generation talent
There was always a strange sleight of hand involved in Prozac Nation. In spite of the extraordinary psychological heavy lifting for over three hundred pages — the remedy in the end was a magic little pill.
In retrospect, Elizabeth Wurtzel and all of us got played by the most corrupt industry in the history of the world.
The success of Prozac Nation was not an accident. For a while, the book was everywhere — on magazine covers, on all of the chatty morning shows, and in doctors’ waiting rooms. It was part of a wave of books including Listening to Prozac that assured the public that the scientists have it figured out and this magic little pill will make all of your troubles go away. I am almost certain that behind the scenes Pharma spent millions of dollars to promote this book and turn Ms. Wurtzel into a household name.
With the success of Prozac Nation an entire generation abandoned the century-long promise of the social sciences and said, “just write me that script doc.”
The tragedy of Elizabeth Wurtzel is that Pharma took a spectacularly talented thinker and writer and used her to betray her whole generation. The end result has been the gradual enslavement of Generation X (and the rest of society) to the cartel.
IV. The demise of Elizabeth Wurtzel
Things did not turn out well for Ms. Wurtzel. Her next book was Bitch: In Praise of Difficult Women. Apparently, the Prozac had stopped working so she resorted to snorting upwards of 40 crushed Ritalin tablets a day — and when that didn’t work she turned to cocaine. That led to rehab and another memoir — this time about dealing with addiction (More, Now, Again: A Memoir of Addiction). By this point she had lost the plot to her own story. She managed a brief reset by going to Yale Law School (always the best) and working for super lawyer David Boies for a few years. At 47 she developed breast cancer and she wrote about that in her trademark style. At 52 she was dead from leptomeningeal cancer.

(Photo credit: Dan Callister/Shutterstock)
In all of her brilliant writing, Ms. Wurtzel never criticized the white coats nor their pharmaceutical handlers in spite of the myriad ways that they failed her. Ms. Wurtzel blamed the BRCA gene mutation for her breast cancer and praised the heroic doctors and scientists who identified it and treated it (with a double mastectomy and reconstruction surgery).
The BRCA gene mutation very well could be the cause of her death. But there is another explanation that is also plausible — one that is not allowed in the mainstream media. Prozac is a fluoride compound (fluoxetine). Fluoxetine is 18.5% fluoride by weight.

Fluoride is toxic. Ms. Wurtzel’s miracle pill was actually depositing poison into her bone marrow, brain, thyroid gland, lymph nodes, fatty tissue, and vital organs, day after day, year after year.
It never cured her depression — any gains were short-lived and supplemented by drugs and alcohol.
The entire story of Prozac Nation was based a toxic and deadly lie.
V. The legacy of Prozac Nation
Things did not turn out well for the rest of us either.
Psychiatrist David Healy figured out the scam early on and went to great lengths to alert others with books including Let Them Eat Prozac (2002) and Pharmageddon (2004). He was later joined by Peter Gøtzsche (Deadly Medicines and Organized Crime, 2017) and many others.
But it took 30 years before the mainstream media admitted what was knowable on the first day — these products do not work as advertised. Even the usually reliable Pharma mouthpiece, The Guardian, was recently forced to admit that the entire theory of the case in connection with Selective Serotonin Reuptake Inhibitors was just glorified marketing copy:

The study in Molecular Psychiatry on which that article is based is (here). If you click through to read The Guardian article you’ll see defenders of the status quo at the end explaining that ‘it works even though there is no evidence that it works.’ Sound familiar?
By this point, about 1 in 5 American women and 1 in 10 men are on these drugs. They are given to pregnant women even though they are linked with autism (see literature review in my thesis). People are on them for decades in spite of no safety studies on long term use. They create dependency and once started, it is very difficult to stop.
It was not a foregone conclusion that Prozac would take off in the United States. German regulators (who actually examined the underlying data) rejected it and it was only approved in Sweden through outright bribery. But FDA regulators were primed to look the other way. In the meantime, Ms. Wurtzel made mental illness and these magic fluoride capsules sexy and cool. One can see how this set the stage for normalizing the other mass poisoning events that followed.
The adoption of SSRIs followed a pattern. Pharma pushed them, the FDA blessed them based on shoddy studies, the media and trusted messengers promoted them, and society gobbled up that snake oil like candy. Anyone who questioned the grift was shunned.
There was just too much money to be made for anyone to do the right thing. Once the pattern was set, more pharmacological disasters soon followed.
Next we were told that opioids, including OxyContin®, were not addictive. Once again the FDA blessed them based on shoddy data, the media promoted them, and society took these pills in massive quantities. On average, every year the U.S. now loses more Americans to opioids than died in combat in the entire (decade-long) Vietnam War.
Now it is happening yet again with Safe & Effective™️ Covid-19 shots that disable and kill at an astonishing rate. There is just so much money to be made from poisoning society that Pharma (+ the media and the political system that they own) cannot resist.
And millions of people who once believed in the promise of a better society are now mindless zombies who just want more pills, more injections, and more drugs to cure the human condition. But even that’s not enough — they want a society where Pharma idolatry is enshrined in law and everyone is forced to obey (setting up Pharma totalitarianism is basically the entire purpose of the California Democratic Party at this point).
VI. Sliding doors: imagine if Elizabeth Wurtzel had chosen differently
Hindsight is 20/20 and Ms. Wurtzel is not here to defend herself. But she was so incredibly talented. One can imagine a world where she might have chosen differently. Imagine if she had said, now wait, hang on, you’re telling me that several millennia of philosophy and a century of psychology are nonsense and that these drug dealers can solve the human condition with fluoride? That seems far-fetched.
One can imagine a world where Ms. Wurtzel used her fierce intellect to actually read the junk science clinical trials and study the FDA sham regulatory process instead of just surfing the zeitgeist. Any amount of honest due diligence would have quickly raised extraordinary doubts.
But the promise of magic pills was irresistible — for Ms. Wurtzel, society, and the drug dealers in white coats who stood to gain billions of dollars.
I want to be clear that it is not the responsibility of a 26 year old creative writer to save civilization. There should have been some adults in the room at her publisher (Houghton Mifflin) or the FDA who could have tapped the brakes on the rush to promote a fluoride compound as some sort of miracle cure. Ms. Wurtzel was uniquely influential but there were hundreds of thousands of others who also made ethically questionable choices in connection with this product. Furthermore, Ms. Wurtzel’s impulsiveness suggests that she may have already had some neurological damage, perhaps from the 10 to 13 shots that were common for Generation X. So perhaps she physically could not have chosen otherwise.
On the other hand, warrior mamas and Covid critical thinkers perform proper due diligence every day. As a result we are attacked by the mainstream media, hunted by the cartel, censored by the Stasi, and blacklisted by corporations and government. I guess if Elizabeth Wurtzel had chosen otherwise we never would have heard of her and they would have promoted someone else to fill that trusted spokesmodel role.
Here’s what I cannot figure out. Was the promise (that I began this article with) always a lie? Is the human condition such that we are always at the mercy of primitive instinct? Conservative Presbyterians believe in the doctrine of “total depravity” — that human beings are always flawed and fallen and the best we can hope for is divine grace that cannot be earned. Are they right?
I confess that I still believe in the promise (even though the last two years have shown me mountains of evidence that it’s not possible). I want to believe in a world where people are decent to each other, where we can find better ways to relate to each other that reduce strife and provide meaning and connection. It’s a far cry better than the alternative — magic pills & injections that are actually deadly, promoted by an entire society built on lies.
Evidence of harm
By Steve Kirsch | September 21, 2022
A short collection of key pieces of evidence showing the COVID vaccines are not “safe and effective.” Not even close. They are the most deadly vaccines we’ve ever produced.
Here’s a high level collection of some of the most compelling pieces of evidence I’ve seen to date. This is not an exhaustive list, but just the key pieces of data that are impossible to explain if the vaccines are safe and effective.
I’ve divided the collection into sections and I’ve tried to limit each section to the most compelling data points. So don’t be disappointed if your favorite item isn’t mentioned in this article; I wanted to keep it short enough to be read..
I’ll try to keep this updated over time. It can be found in the Reference section of my Substack.
- The Pfizer trial 6 month report showed absolutely no all-cause morbidity or mortality benefit. There were no all-cause benefits at all. It was all negative. Ask your doctor why you should take a new, unproven medical intervention that is not shown to have an overall benefit. Even if there was a benefit of fewer COVID infections (which is seriously suspect due to the gaming below), the fact that the total all-cause numbers for both mortality and morbidity were negative means the intervention should not be recommended by any doctor.
- The Pfizer trial 6 month report showed that more people died (and were injured) who got the drug than who got the placebo. In other words, the cure was worse than the disease. The drug maker claimed that none of the people in the vaccine group were killed by the vaccine. They do not reveal the tests they did and explain how they were able to make that assessment. Why the secrecy here, especially in light of the study by Bhakdi and Burkhardt showing that trained medical examiners missed the causality link in 93% of the cases they looked at? The Pfizer vaccine had 4X as many cardiac arrests in the treatment group than the placebo (see page 12 of the Supplemental Appendix). This lines up very well with the numerous cardiac-related problems related to the vaccine as documented in the study by Retsef Levi and in the VAERS data which showed that the “cardiac arrest” reports were elevated by a factor of 93X higher than the annual baseline rate (VAERS reports from all vaccines combined in previous years). For some reason, the CDC wasn’t able to detect that signal (it was only 100 times higher than normal so they ignored it for some reason; they won’t let me ask them about it). In short, the claims from the manufacturer that none of the deaths were caused by the vaccine are highly suspect since all the evidence for those claims remains hidden from public view for some reason.
- The Pfizer trial 6 month report showed that at best, the drug saved only 1 COVID life per 22,000 recipients. This means that at best, after vaccinating 220M Americans, we might save 10,000 lives from COVID. But the VAERS reports show an excess death toll of well over 10,000 people and that’s before applying the minimum estimated under-reporting factor of 41. So there isn’t a mortality benefit: it’s actually the reverse. Furthermore, VAERS reports will likely only be filed for deaths in temporal proximity to the shot and is highly unlikely to report those deaths happening 5 months after the shot which appear to be the bulk of the deaths. This makes the comparison even worse. In short, we aren’t anywhere close to saving any lives at all.
- The Classen paper analyzed the clinical trial data for all three US vaccines and confirmed the lack of any overall benefit. There was an increase in morbidity which was highly statistically significant in all three vaccines. It concluded, “Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe.” This is exactly right.
- The paper by Christine Stabell Benn entitled, “Randomised Clinical Trials of COVID-19 Vaccines: Do Adenovirus-Vector Vaccines Have Beneficial Non-Specific Effects?” confirmed that there was no mortality benefit by taking the COVID mRNA vaccines. “Based on the RCTs with the longest possible follow-up, mRNA vaccines had no effect on overall mortality despite protecting against fatal COVID-19.” See this article by Daniel Horowitz for more information. In other words, these vaccines have no death benefit. Period. Full stop. This is exactly what the Canadian analysis below showed.
- Serious adverse reactions, including paralysis, were not reported to the FDA and there were other very serious discrepancies in the trials. For some reason, nobody seems to be interested in exploring or explaining these very serious issues. Some are very clear cut such as the case of Maddie de Garay who was one of 1,000 kids in the clinical trial. She’s paralyzed now and has to eat with a feeding tube. The FDA and Pfizer never investigated, but reported her results as mild abdominal pain in the trial results. This is fraud. Also, there were 5 times as many exclusions in the treatment arm as in the placebo arm of the trial: 311 vs. 60. Do the p-value computation on that one and you’ll find that it could not possibly have happened by chance (1e-40). It means the trial was not blinded. Why didn’t anyone in the medical community ever point this out? Nobody will tell me.
- Pfizer admitted to clinical trial fraud in federal court. Their defense was that the FDA was in on it.
- The VAERS data, which is the official adverse event reporting system used by the US government, shows that an estimated hundreds of thousands have died and millions have been injured. If these weren’t caused by the vaccine, what caused them? Why are there more adverse events reported for these vaccines than for all other vaccines in history combined? Nobody can answer that question. See this tutorial and this recent confirmation and this article on VAERS and causality. Here’s how these numbers were calculated. Here is independent confirmation of the estimates by Dr. Naomi Wolf who used different datasets. No fact checker was interested in contacting me to challenge the facts since I always insist on recording any calls. Also, the causality of events was confirmed by the Israeli safety studies, but nobody wants to look at those.
 Can you spot the unsafe vaccine? People at the CDC don’t see any problem with this mortality chart: all the vaccines look perfectly safe.
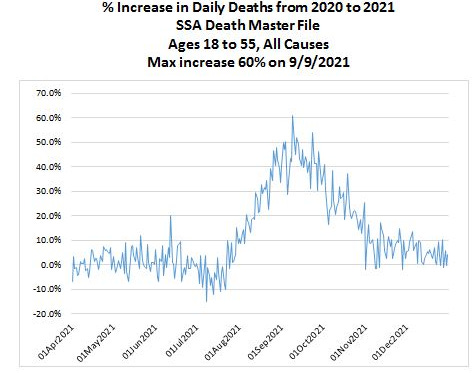
Can you spot the unsafe vaccine? People at the CDC don’t see any problem with this mortality chart: all the vaccines look perfectly safe. - The US Social Security Death Master File showed a 60% increase in the all-cause death rate in September 2021 vs. September 2020 for ages 18 to 55. According to the insurance companies, it wasn’t COVID. COVID kills only a small fraction of people in this age range so even if the COVID death rate doubled, it would be a minor blip on the all-cause death rate. A five month delay in death vs. vaccination was discovered in multiple countries, not just the US. Different studies found nearly identical delays. Also, I find it very troubling that the insurance companies aren’t asking the family of the policyholders who died whether they were vaccinated with the COVID vaccine and when. They don’t want to collect this information for some odd reason. So let’s be clear that a 60% increase in all-cause death rate makes this intervention extremely dangerous. I’m not aware of anything that comes close to killing people in such massive numbers. The CDC is silent on this. They don’t even want to show the public this chart:
- US disability rose dramatically soon after the vaccines rolled out (Y axis is Z-score). A 3 sigma increase is hard to explain.

- As of Sep 2, 2022, the vaccination rate in Israel is now just 2.4%. They used to be one of the world’s most vaccinated countries. Today, very few people in Israel are considered to be vaccinated. If the vaccines are so beneficial, why has nearly the entire country shifted from extremely pro-vax to extremely anti-vax in such a short period of time?

- The Israeli Ministry of Health revealed in a confidential meeting with scientists that the reason that they never notified the people of Israel about the safety issues from the vaccines was because of budget/staffing issues. Apparently, while they had millions of dollars to promote the vaccines as safe and effective, they forgot to budget for the possibility they were wrong.
- The Israeli vaccine safety data showed very clearly the side-effects are serious, long-lasting, and caused by the vaccines. Secondly, it showed that the Israeli authorities and the worldwide mainstream media are covering it all up. It also showed that US officials were not interested in seeing credible COVID vaccine safety that didn’t go along with the narrative. I tried to find out why, but nobody would talk to me. Harvard Professor Martin Kulldorff, a widely respected authority on vaccines, when asked why these people wouldn’t want to see the data, replied, “I don’t know.” This is the single most damaging report in the history of the COVID vaccines. Nobody wants to talk about it. They are hoping it will die. It won’t. Some people claim Israeli used a broad mix of vaccines, but that’s not true. Over 90% of the reports are from Pfizer, the bulk of the others are from Moderna. See also Israeli Investigators Find COVID-19 Vaccines Cause Side Effects: Leaked Video.
- The Canadian report prepared for the Liberal Party of Canada (Trudeau’s party) showed no benefit for infection, hospitalization, and death for those under 60. “The empirical evidence investigated in this report from PHO and PHAC does not support continuing mass vaccination programs, mandates, passports and travel bans for all age groups.” You can’t have a vaccine that doesn’t work in Canada work in other countries. The authors of the report had to hide their identities for fear of retribution. The statistics analyzed were those from Ontario which is not a small province (15M people). Naturally, the mainstream press ignored the report. Nobody has shown where the experts who wrote this made a mistake. The conclusion of the report is supported by independent analysis done by Mathew Crawford of the data from San Diego County, San Diego County Data Busts a Hole in Vaccine Efficacy Narrative. So apparently, the results are not limited to Ontario.
- The Harvard-Hopkins-UCSF study showed it is unethical to mandate vaccination for college students and anyone younger. The study clearly said, “University booster mandates are unethical.”
- The Thailand study did blood tests before vs. after the jab and determined that nearly 30% of young adults experienced cardiovascular injuries after the jab. How is that safe? And why didn’t anyone in the US ever do such a study? Do we not want to know? This was a simple blood test before and after the vaccine. Why did they not notify parents as soon as the study was published?
- The study by Bhakdi and Burkhardt showing 93% of deaths after vaccination were caused by the vaccine
- The data showing the vaccines cause prion diseases shortly after vaccination. This is impossible if the vaccines are truly safe. See the paper on ScienceOpen.com (after ResearchGate removed it).
- Determinants of COVID-19 Vaccine-Induced Myocarditis Requiring Hospitalization by Jessica Rose and Peter McCullough showing the myocarditis caused by the vaccine have distinct biomarkers.
- The Fraiman-Doshi paper looked at serious adverse event rates and found that the vaccines may not be as safe as has been claimed, but they cannot do a proper analysis because they are not allowed to see the data. “Full transparency of the COVID-19 vaccine clinical trial data is needed to properly evaluate these questions. Unfortunately, as we approach 2 years after release of COVID-19 vaccines, participant level data remain inaccessible.” You have to wonder: if the vaccine is so safe, why are the drug companies hiding the data?
- The Levi cardiac arrest rate elevation paper showed a troubling correlation between vaccine doses and increased cardiac events from January–May 2021. When they tried to get data after May 2021, they were refused access. This begs the question: if the vaccines are perfectly safe, what are they trying to hide?
- There are over 1,250 papers published in the scientific peer-reviewed literature showing the vaccines cause significant adverse events.
- The Walach paper found that the vaccines harm more people than they save.
- This news article published in the BMJ showed that 10 out of 100 deaths in elderly people they examined were “likely” caused by the vaccine. Funny, in America we think the number is 0. They can’t both be right. Someone should investigate why we have different results. This is very important. In fact, with a deeper investigation, over 90% of the deaths thought by medical examiners not to be caused by the vaccine were shown to be caused by the vaccine. This suggests that the US isn’t looking at the deaths.
- My colleagues and I are not misinformation spreaders according to this paper published in a peer-reviewed medical journal.
Are the Covid mRNA Vaccines Safe? was written by Harvard professor Martin Kulldorff who until recently was on vaccine committees of the FDA and CDC. He concluded:
Fraiman and colleagues have produced the best evidence yet regarding the overall safety of the mRNA vaccines. The results are concerning. It is the responsibility of the manufacturers and FDA to ensure that benefits outweigh harms. They have failed to do so.
Canadian court decisions on the constitutionality of Covid measures are invalid due to jurisdictional errors of law reviews court decisions on COVID and emphasizes the courts’ repeated over reliance on government expert testimony. Courts are supposed to find the truth and not rely on government representations or propaganda.
- The Watson et al. “modeling study”: did “COVID vaccinations” really prevent 14 million deaths? The original paper was clearly bogus since the vaccines kill more people than they save. This article examines the paper claiming the vaccines have been ridiculously effective.
There are specialized tests required to diagnose a death from the COVID vaccine.
The CDC has never told any medical examiner in the US about these tests.
So the medical examiners aren’t implicating the vaccine in any of the deaths.
The question is we know what the tests are, we know there is solid evidence from multiple countries that the vaccine causes death, yet we refuse to even consider the possibility that the vaccine caused the deaths. Why?
This paper, A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products, was retracted because the publisher didn’t like the result. So he unilaterally decided to retract the paper. This is unethical.
Here’s the “withdrawn” notice.
Here is the backstory as well as this censorship update.
The publisher hasn’t fixed the problem in over a year despite assurances it would be quickly resolved.
Here is another retracted paper that was correct:
Why are we vaccinating children against COVID-19? by Ron Kostoff
“Compared with the 28,000 deaths the CDC stated were due to COVID-19 and not associated morbidities for the 65+ age range, the inoculation-based deaths are an order-of-magnitude greater than the COVID-19 deaths!”
That is basically what I found: the vaccines kill >10X more people than the number of COVID deaths that they save. The paper passed peer review and was published. The editor of the journal quit after he was overridden by the publisher on the retraction.
The reason cited for the retraction:
- The use of key terminology, specifically the key terms “inoculation” and “vaccination” diverges from common use and are incorrect, indicating clear evidence of bias.
- Publicly available data from the United States Center for Disease Control (U.S. CDC) were concluded by the external reviewers to be misinterpreted to make the erroneous conclusion that the vast majority of reported deaths due to COVID-19 are actually due to other comorbidities. Such an egregious misinterpretation and misrepresentation are unacceptable.
This is completely bogus for two reasons:
- The editor could have easily normalized the terminology to eliminate any perceived “bias.” They simply ask the author to do a quick search and replace.
- The vast majority of COVID-19 deaths were in fact due to other comorbidities. For example, the New Mexico death records where COVID-19 was listed as the cause of death and 5 out 6 were not consistent with a COVID death. If anyone wants to challenge me on that, I have access to the death data. In Massachusetts, only 10% to 20% of the deaths listed as COVID were actually caused by COVID. Most people don’t have access to the death data, but I do. So I wonder if the journal is interested in fixing their error?
Can anyone explain how these anecdotes are possible?
- Why don’t Dr. Paul Offit (FDA vaccine outside committee) and Professor Grace Lee (Chair, CDC vaccine outside committee) want to see the Israeli safety data? They are deliberately avoiding answering the question. Why?
- In Canada, the #1 cause of death is now “unexplained.” See Deaths with unknown causes now Alberta’s top killer: province. If it isn’t the vaccine, what is causing this?
- There is data from over 1,000 vaccine injured people where 10% of the injured report 30 or more symptoms that are unique to the vaccine injured. How is that possible if the vaccine is so safe? Marsha Gee was perfectly healthy before her COVID vaccine. Less than 1 hour after her first Pfizer shot she experienced severe symptoms and experiences 78 of symptoms common with other vaccine injured. If Marsha wasn’t injured by the COVID vaccine, what caused all these symptoms?
- Why is it illegal to analyze the vaccine vials? Why hasn’t a single medical institution done an analysis of the content of the vaccines to see if there are placebos with saline solution and the amount of mRNA degradation, rendering the vaccines useless? Why the secrecy here? If we knew what was in the vaccines would this cause harm? How?
- Why are prominent people risking their careers to obtain fake vaccine cards? We know top people at Mass General Hospital have fake vaccine cards. We’ve heard that people at the highest levels of the DoD can get fake vaccine cards. It is well known that the CEO of a large pharmaceutical company bought a fake vaccine card. Why would he risk spending years in jail if the vaccines are perfectly safe?
- The Died Suddenly group on Facebook was adding users at 20,000 per day making it the fastest growing group in Facebook history. They had to throttle the growth rate due to attempts by the British military to infiltrate the group to cause it to be shut down.
- The average age of the people reported dead in the Died Suddenly group has been trending younger and younger over time. How can you explain that? The only worldwide massive intervention that goes to younger people is the COVID vaccine.
- The embalmer data (such as The Epoch Times article and this interview). These clots are not blood clots, but they are clots embalmers never saw before mid-2021 (since they take 3 months or more to form into large sizes). If the vaccines are not causing these killer clots, what is? They can be found in up to 93% of the embalming cases.
- Insurance company data from insurance companies worldwide:
- Wayne Root’s wedding: 200 guests, half vaxxed, half unvaxxed. Only the vaxxed got injured (26%) or died (7%). I surveyed my readers and collected data from over 600 readers who collectively reported very similar stats. That’s hard to explain if there isn’t a huge effect.
- My neurologist stats: 11 years without needing to do a single VAERS report; this year, she needs to file 1,000 VAERS reports on 20,000 patients in the practice. How can anyone explain that if the vaccine is perfectly safe with mild, short term effects? This is similar to the 4.5% rate of neurological injury reported earlier by the Israeli Ministry of Health.
- The polling results using third party polling firms (so not my followers) consistently show that more people died from the vaccine than from the virus. The mainstream media refuses to do similar surveys and most survey firms refuse to even ask the questions.
- Ten different surveys I did all showed the vaccines are more harmful than helpful.
- Doctors in Canada died at a rate that was more than 10X normal after getting the fourth dose of the vaccine. And those are just the ones we know about.
- The fact that Paul Offit isn’t going to get the latest booster even though the CDC says he should. Why should any of us take the shot if Paul Offit is refusing to take the shot? He’s arguably the world’s most respected authority on vaccines and sits on the FDA outside advisory committee?
- Why are health authorities removing safety data on the latest shots? If they are so safe, why not release the data?
- Google searches show people became interested in topics related to vaccine safety before they became popular on social media
- When I ask data/statistics experts such as Joel Smalley and Professor Norman Fenton whether they’ve seen any credible data proving the vaccines are safe and effective, they are unable to cite a single reference.
- A local news station (WXYZ-TV) asked people to report on unvaxxed loved ones that became sick and died and instead they got hammered with hundreds of thousands of people saying they lost loved ones to the jab. See my video on the WXYZ-TV story and also this video.
- Woman collapses and dies 7 minutes after Booster shot… The stunning thing is the Twitter video documents that the pharmacy workers have been instructed to not bring it up when briefing patients and, if asked, not to comment on the death. Do you think they are looking out for your best interest by withholding adverse events like death 7 minutes after the shot from the public? That should never happen. Have you ever seen a video like this before the COVID vaccines rolled out? The death was ruled as “natural causes” which means it was from internal organ failure as opposed to being hit by a truck. However, the internal organ failure was due to an external event (vaccinated).
- Turbo-cancer is being reported now. It’s impossible to explain. Never been seen before.
- A reader wrote: I work in the financial services industry in Toronto. A co-worker of mine was recently diagnosed with cancer. He has been getting treated at Sunnybrook hospital for it. The doctors there told him they’ve seen a significant spike in cancer cases well above what could be explained by people missing getting screened due to the pandemic. What’s more though is that they catalogue the vaccine status of every cancer diagnosis and the spike in the number of cases is only occurring in those who are vaccinated– apparently they are researching it to try and find out why the vaxed have seen a spike in cancers vs the unvaxed who haven’t- obviously they are not ready to go public with this but they know about it and are researching it fwiw
- Turtles all the way down: Vaccine science and myth shows the vaccines are not nearly as safe as people think. This is the most damaging book ever written showing the safety of the vaccines is highly questionable. There isn’t a single risk-benefit trial on all cause mortality and morbidity vs. placebo for any of the 70 approved vaccines even though they’ve had 60 years to do this. If the vaccines are truly beneficial, why do you think it’s never been done for any vaccine? A team of Israeli scientists wrote this book over 5 years. It was recently translated into English and is available through purchase on Amazon.
- Dissolving Illusions: the history of vaccines shows they did a lot less than people think; probably next to nothing.
- The Real Anthony Fauci: illustrates the corruption in the medical community today. For example, they created a more accurate adverse event reporting system (ESP:VAERS) system and then scrapped it after it showed all the vaccines were unsafe.
- Vaccine Secrets: a 20 minute slide presentation from CHD
- The CCCA presentations:
- My mega-presentations:
Once I established a policy of always recording calls with “fact checkers,” I’ve not had a single call from them trying to refute anything I’ve written.
None of the drug companies that make these products will refute anything I’ve written or supply a representative to debate me or any of my colleagues in a live debate. They have immunity from liability and they are not willing to be held accountable in the court of public opinion either.
- The COVID lies by Dr. Michael Yeadon
This was a very well done study, but it is of course attacked by the pro narrative people. We’d love to have an open debate about this study, but the other side doesn’t want to talk about it in a neutral forum.
A LITERATURE REVIEW AND META-ANALYSIS OF THE EFFECTS OF LOCKDOWNS ON COVID-19 MORTALITY
Masks don’t work at all. See this article which has plenty of references. If anything, masks are more likely to hurt you than to benefit you.
There is no study at all on the 6 foot distance rule. They just made that one up.
Professor Jeffrey Sachs was tasked by The Lancet to lead an independent investigation into the source of the SARS-CoV-2 virus. After he determined it came from US biotechnology, all of a sudden nobody wanted to pursue the investigation any further.
Tony Fauci gets paid every time you get a Moderna shot. He won’t disclose how much he makes and you can’t get via FOIA (it’s blacked out). If the Republicans get control of the Senate, that will change. Watch this video from Sept 20, 2022 of Rand Paul commenting on this as well as the well founded accusation that Fauci created the virus in the first place and then desperately tried to make it look like it came from nature after top scientists said it was a lab leak (watch the video at 2:00 onwards). Rand Paul called it, quite rightly, “the biggest cover-up in the history of science.”
The question you have to ask yourself is why is Fauci keeping his funding of the gain of function research and also his compensation for each vaccine dose a secret?
Tony Fauci was the primary reason that all early treatments were ignored by the government. It appears he did that because it would cut into his revenue stream.
Early in the pandemic, two physicians, George Fareed and Brian Tyson, developed a treatment protocol using a variety of safe, low cost drugs and supplements with little to no side effects that had a near 100% success track record in preventing hospitalization, death, and long haul COVID if the patient started treatment shortly after realizing they were infected. They’ve treated over 10,000 patients. They wrote a best-selling book about it.
Today, more than two years later, the FDA and the CDC have not returned their calls.
- Why can’t we have open forums where our public health officials can be challenged by experts who disagree? Is there proof that having open debate results in worse outcomes?
- Why doesn’t anyone want to see the Israeli safety data?
- Why isn’t anyone asking for Fauci’s unredacted emails?
- Is there a scientific reason that the CDC is ignoring me and all the experts I work with?
- Questions I’d love to ask Congresswoman Anna Eshoo… that she’ll never answer
- Why hasn’t anyone calculated the minimum VAERS under-reporting factor (URF)?
- Did the propensity to report change in 2021 vs. previous years. What is the new number in 2021 and 2022 compared to previous years? How did you calculate it?
- Why do John Su and Tom Shimabukuro never talk about the URF in the ACIP meetings?
- There were over 14,000 excess deaths reported in VAERS. That’s before the URF is applied. If these weren’t caused by the vaccine, what caused them?
- If these vaccines are so safe, why are there more adverse events reported for these vaccines than for all other vaccines in history combined?
- I found thousands of adverse events that are elevated by these vaccines compared to all other vaccines combined in previous years. How many adverse events did the CDC find?
- There was a dramatic rise in adverse events reported in the VAERS system for the COVID vaccines. How could this not be a serious safety concern? The propensity to report did not increase. If you believe the propensity to report did increase, what data do you have to support that?
- My neurologist has been in practice for 11 years. She has 20,000 patients in her multi-physician practice. In that time, she’s never had to report a single event to VAERS. With the COVID vaccines, she now needs to make 1,000 reports. If the vaccines are safe and effective and most all the symptoms are mild and short term, how do you explain this? Her event rate similar to the 4.5% injury rate that the Israeli MoH found. So her reporting rate is more than 10,000 times higher than for any other vaccine. Couldn’t that be the explanation for the higher rate of VAERS reports? Doesn’t this suggest that the propensity to report is much lower this year because there are so many more events and doctors simply don’t have the time to report them all?
- The NEJM pregnancy paper by Tom Shimabukuro noted that the results on safety for pregnant women was preliminary since many of the women were still pregnant. What was the final result and why wasn’t it published?
- There was an analysis of the VAERS data by Hannah Rosenblum published in the Lancet. It never goes into explaining why there were elevated reporting rates and also the nature of the reported events are not normal background events. Couldn’t the elevated reporting rates be caused by a dangerous vaccine? Does she want to look at the Israeli safety data? If not, why not? The Israeli data directly contradicts the conclusion of the paper. Shouldn’t we figure out which conclusion is correct?
- Why does Carol Crawford not answer my questions about an open discussion with the top vaccine misinformation spreaders to resolve our differences and reduce vaccine hesitancy?
- Why does Martha Sharan ignore my emails and phone messages when I attempted to ask for permission to talk to the authors of the Rosenblum paper? Can’t she reply with the reason questions are not allowed?
Questions I’d love to get the answer to. These were asked, but never answered.
- Why did the CDC never publish the follow up on the NEJM pregnancy paper by Tom Shimabukuro?
- The CEO of Moderna was asked how the 19 nucleotide sequence from a Moderna patent got into the SARS-CoV-2 genome. That sequence is never found in a virus. How did it get in this one? The CEO said he’d look into it, but never reported the explanation. I’d love to know what it was.
- Why hasn’t any Democratic committee chairman asked the NIH for Tony Fauci’s unredacted emails? Don’t we want to know the truth about whether there was a deliberate cover-up? If there was, shouldn’t Fauci be fired?
- Fauci wasn’t supposed to be funding gain of function research but he was. How is he being held accountable?
- How much is Fauci making every time someone gets a Moderna shot? He’s a public official… Why is this a secret?
People who disagree with the mainstream narrative are rewarded with censorship, permanent bans on posting on social media, demonetization of your YouTube account, revocation of your medical license, revocation of your medical certifications, loss of hospital privileges, loss of job, loss of funding, loss of friends, and a Wikipedia entry labeling you a “misinformation spreader” and/or “conspiracy theorist.”
This is a problem. I am not aware of any paper published in the medical literature that shows that such tactics result in better health decisions.
Should we use the same rules at the UN when nations disagree? Do you think that will result in better outcomes?
The way people resolve differences is by confronting the issues and talking through them. But we are not doing this:
- Why can’t we find anyone who will defend the CDC, FDA, and NIH on camera?
- Dr. Byram Bridle and 2 colleagues challenged Canada’s health authorities to a debate
- Vinay Prasad’s most important op-ed
This is objective proof of a broken system. It is indefensible. Caught on video camera. There is no reason that anyone in a position of authority on the COVID vaccines would refuse an opportunity to see the most thorough post-vaccine safety study ever done: one that shows causality of serious adverse events.
From Israeli Investigators Find COVID-19 Vaccines Cause Side Effects: Leaked Video:
Rechallenge changes a causal link “from possible to definitive,” Dr. Mati Berkovitch, head of the research team and a pediatric specialist, said at the meeting.
and
Many of the reported adverse events were found to be long-lasting, which researchers said in the meeting was surprising since the brochure handed to vaccine recipients says otherwise. They also said Pfizer officials told them that Pfizer did not know of any long-lasting symptoms.
and
In the official report later issued to the public, the MoH did not detail how researchers were caught off guard by the duration of the events and side effects. The health agency also stated that there were no new events identified.
It concludes:
The choice to omit some of the crucial findings discussed in the meeting from the public report is “a recipe to destroy” the entire vaccine program, according to Levi, an Israeli native and an expert in risk management.
“The more pro-vaccine, the more disturbed you need to be from something like this,” Levi told The Epoch Times. “And the reason is that the two most important enablers for vaccine programs … to be successful is trust and transparency, that you actually communicate to people the real risk-benefits and allow them to make choices about what they want to do. The second thing is that you take care of the people that were harmed by the vaccine because no vaccine has 100 percent safety.”
“I think we have in this example … where we violate these two very important principles,” he added. “This is a recipe to basically destroy all vaccine programs, so the more pro-vaccine you are, you should be more disturbed by this.”
How can you have the chair of a safety committee not interested in seeing important safety data? Professor Grace Lee should be removed from her position by the CDC. Why isn’t she? Does anyone care?
Why does Dr. Paul Offit ignore requests to see the same data?
According to the Epoch Times article, everyone declined to comment on the story: the scientists, the MOH officials, and the CDC’s Immunization Safety Office declined to comment on the Israeli findings.
If the above isn’t enough, there are hundreds more “hard to explain” data points.
- List of over 1,200 papers published in peer-reviewed scientific journals
- The safe and effective narrative is falling apart
- Think we got it wrong?
- How the authorities can INSTANTLY stop the spread of “COVID misinformation”
- Examining COVID Vaccine Efficacy
There is an excellent article written in August 2020 by Norman Doidge entitled “Medicine’s Fundamentalists” which talks about the “all-available-evidence approach.” It should be read by every doctor in America. This is how medical science should work.
The precautionary principle medicine seems to have been thrown under the bus during the pandemic. It says in the face of uncertainty, one should take reasonable measures to avoid threats that are serious and plausible.
For example, the Pfizer clinical trial showed the vaccine saved only one COVID death per 22,000 injected. That means we might only save around 10,000 lives if we inject 200M Americans. So if VAERS, which is at least 41 times under reported, is showing over 12,000 deaths associated with the vaccine, any reasonable person should say that killing more than 41 people to save 1 life is nonsensical… shouldn’t we put a PAUSE on this intervention until we resolve the uncertainty?
In the current system, questioning the CDC or other authorities results in serious retribution as mentioned earlier.
Is that really the right way to handle scientific dissent?
Are the vaccines “safe and effective” as claimed?
To answer this, science requires that we look at all the available data and see whether the data is more consistent with the hypothesis of “safe and effective” or “not safe and effective.”
All the data that I and my colleagues have seen end up being placed in the “not” bucket.
We are open to being shown we got it wrong on the hundreds of pieces of evidence we have examined, but nobody is willing to discuss the data with us to resolve the issue, not even for $1M dollars.
I even went to extraordinary lengths to offer the Israeli safety data to ACIP Chair Grace Lee. Her response: she called the police on me. That pretty much tells you everything you need to know: they simply refuse to look at any data that goes against their currently held beliefs. That’s the way science works.
Is That True Or Did You Hear It On The BBC?
By Paul Homewood | Not A Lot Of People Know That | August 19, 2022
 I have just bought this book, which includes some good stuff on the BBC’s climate lies and misinformation.
I have just bought this book, which includes some good stuff on the BBC’s climate lies and misinformation.
I have only read the first couple of chapters, but I would thoroughly recommend it.
This is the Amazon summary:
… not only does the BBC diligently protect power from scrutiny, it attacks and attempts to discredit those who dare to challenge the status quo.
Formed in 1922 by the British establishment, the BBC has always been a reliable ally of ultra-wealthy and powerful interests. Indeed, the broadcaster occupies a pivotal position within an international corporate-political alliance which promotes only those narratives which consolidate the ‘global order.’
Using multiple examples of BBC reporting, the author argues that the tax-payer funded broadcaster is a proxy which acts on behalf of a tiny, but very powerful clique – a role which compels it to pump out disinformation on an industrial scale, misleading all those who consume its content.
The book includes sections on:
- Climate Change
- Brexit
- COVID
- Trump
- NHS
Sedgwick’s premise is an interesting one that the BBC has always protected the establishment. One implication from this is that this same establishment has morphed over the years, from a reactionary one of the past to the left wing, big government, global world order one of today.
How We Have Been Misled About Antidepressants
By Joanna Moncrieff | Brownstone Institute | August 18, 2022
Our umbrella review that revealed no links between serotonin and depression has caused shock waves among the general public, but has been dismissed as old news by psychiatric opinion leaders. This disjunction begs the questions of why the public has been fed this narrative for so long, and what antidepressants are actually doing if they are not reversing a chemical imbalance.
Before I go on, I should stress that I am not against the use of drugs for mental health problems per se. I believe some psychiatric drugs can be useful in some situations, but the way these drugs are presented both to the public and among the psychiatric community is, in my view, fundamentally misleading. This means we have not been using them carefully enough, and crucially, that people have not been able to make properly informed decisions about them.
Much public information still claims that depression, or mental disorders in general, are caused by a chemical imbalance and that drugs work by putting this right. The American Psychiatric Association currently tells people that: “differences in certain chemicals in the brain may contribute to symptoms of depression.” The Royal Australian & New Zealand College of Psychiatrists tells people: “Medications work by rebalancing the chemicals in the brain. Different types of medication act on different chemical pathways.”
In response to our paper finding that such statements are not supported by evidence, psychiatric experts have desperately tried to put the genie back in the bottle. There are other possible biological mechanisms that could explain how antidepressants exert their effects, they say, but what really matters is that antidepressants ‘work.’
This claim is based on randomised trials that show that antidepressants are marginally better than a placebo at reducing depression scores over a few weeks. However, the difference is so small that it is not clear it is even noticeable, and there is evidence that it may be explained by artefacts of the design of the studies rather than the effects of the drugs.
The experts go on to suggest that it does not matter how antidepressants work. After all, we do not understand exactly how every medical drug works, so this should not worry us.
This position reveals a deep-seated assumption about the nature of depression and the action of antidepressants, which helps to explain why the myth of the chemical imbalance has been allowed to survive for so long. These psychiatrists assume that depression must be the result of some specific biological processes that we will eventually be able to identify, and that antidepressants must work by targeting these.
These assumptions are neither supported nor helpful. They are not supported because, although there are numerous hypotheses (or speculations) other than the low serotonin theory, no consistent body of research demonstrates any specific biological mechanism underpinning depression that might explain antidepressant action; they are unhelpful because they lead to overly optimistic views about the actions of antidepressants that cause their benefits to be overstated and their adverse effects to be dismissed.
Depression is not the same as pain or other bodily symptoms. While biology is involved in all human activity and experience, it is not self-evident that manipulating the brain with drugs is the most useful level at which to deal with emotions. This may be something akin to soldering the hard drive to fix a problem with the software.
We normally think of moods and emotions as being personal reactions to the things going on in our lives, which are shaped by our individual history and predispositions (including our genes), and are intimately related to our personal values and inclinations.
Therefore we explain emotions in terms of the circumstances that provoke them and the personality of the individual. To override this common-sense understanding and claim that diagnosed depression is something different requires an established body of evidence, not an assortment of possible theories.
Models of drug action
The idea that psychiatric drugs might work by reversing an underlying brain abnormality is what I have called the ‘disease-centred’ model of drug action. It was first proposed in the 1960s when the serotonin theory of depression and other similar theories were advanced. Before this, drugs were implicitly understood to work differently, in what I have called a ‘drug-centred’ model of drug action.
In the early 20th century, it was recognised that drugs prescribed to people with mental disorders produce alterations to normal mental processes and states of consciousness, which are superimposed onto the individual’s preexisting thoughts and feelings.
This is much the same as we understand the effects of alcohol and other recreational drugs. We recognise that these can temporarily override unpleasant feelings. Although many psychiatric drugs, including antidepressants, are not enjoyable to take like alcohol, they do produce more or less subtle mental alterations that are relevant to their use.
This is different from how drugs work in the rest of medicine. Although only a minority of medical drugs target the ultimate underlying cause of a disease, they work by targeting the physiological processes that produce the symptoms of a condition in a disease-centred way.
Painkillers, for example, work by targeting the underlying biological mechanisms that produce pain. But opiate painkillers may work in a drug-centred way too, because, unlike other painkillers, they have mind-altering properties. One of their effects is to numb emotions, and people who have taken opiates for pain often say they still have some pain, but they do not care about it anymore.
In contrast, paracetamol (so often cited by those defending the idea that it does not matter how antidepressants work) does not have mind-altering properties, and therefore although we may not fully understand its mechanism of action, we can safely presume it works on pain mechanisms, because there is no other way for it to work.
Like alcohol and recreational drugs, psychiatric drugs produce general mental alterations that occur in everyone regardless of whether they have mental health problems or not. The alterations produced by antidepressants vary according to the nature of the drug (antidepressants come from many different chemical classes – another indication that they are unlikely to be acting on an underlying mechanism), but include lethargy, restlessness, mental clouding, sexual dysfunction, including loss of libido, and numbing of emotions.
This suggests they produce a generalised state of reduced sensitivity and feeling. These alterations will obviously influence how people feel and may explain the slight difference between antidepressants and placebo observed in randomised trials.
Influences
In my book, The Myth of the Chemical Cure, I show how this ‘drug-centred’ view of psychiatric drugs was gradually replaced by the disease-centred view during the 1960s and 70s. The older view was erased so completely that it seemed people simply forgot that psychiatric drugs have mind-changing properties.
This switch did not occur because of scientific evidence. It occurred because psychiatry wanted to present itself as a modern medical enterprise, whose treatments were the same as other medical treatments. From the 1990s, the pharmaceutical industry also started to promote this view, and the two forces combined to insert this idea into the minds of the general public in what has to go down as one of the most successful marketing campaigns in history.
As well as wanting to align with the rest of medicine, in the 1960s the psychiatric profession needed to distance its treatments from the recreational drug scene. Best-selling prescription drugs of the period, amphetamines and barbiturates, were being widely diverted onto the street (the popular ‘purple hearts’ were a mixture of the two). So it was important to emphasise that psychiatric drugs were targeting an underlying disease, and to gloss over how they might be changing people’s ordinary state of mind.
The pharmaceutical industry took up the baton following the benzodiazepine scandal in the late 1980s. At this time it became apparent that benzodiazepines (drugs like Valium- ‘mother’s little helper’) caused physical dependence just like the barbiturates they had replaced. It was also clear they were being doled out by the bucket load to people (mostly women) to medicate away the stresses of life.
So when the pharmaceutical industry developed its next set of misery pills, it needed to present them not as new ways of ‘drowning one’s sorrows,’ but as proper medical treatments that worked by rectifying an underlying physical abnormality. So Pharma launched a massive campaign to persuade people that depression was caused by a lack of serotonin that could be corrected by the new SSRI antidepressants.
Psychiatric and medical associations helped out, including the message in their information for patients on official websites. Although marketing has died down with most antidepressants no longer on patent, the idea that depression is caused by low serotonin is still widely disseminated on pharmaceutical websites and doctors are still telling people that it is the case (two doctors have said this on national TV and radio in the UK in the last few months).
Neither Pharma nor the psychiatric profession has had any interest in bursting the chemical imbalance bubble. It is quite clear from psychiatrists’ responses to our serotonin paper that the profession wishes people to continue under the misapprehension that mental disorders such as depression have been shown to be biological conditions that can be treated with drugs that target the underlying mechanisms.
We haven’t worked out what those mechanisms are yet, they admit, but we have plenty of research that suggests this or that possibility. They do not want to contemplate that there might be other explanations for what drugs like antidepressants are actually doing, and they do not want the public to do so either.
And there is good reason for this. Millions of people are now taking antidepressants, and the implications of discarding the disease-centred view of their action are profound. If antidepressants are not reversing an underlying imbalance, but we know that they are modifying the serotonin system in some way (though we are not sure how), we have to conclude they are changing our normal brain chemistry – just like recreational drugs do.
Some of the mental alterations that result, such as emotional numbing, may bring short-term relief. But when we look at antidepressants in this light we immediately understand that taking them for a long time is probably not a good idea. Although there is little research on the consequences of long-term use, increasing evidence points to the occurrence of withdrawal effects which can be severe and prolonged, and cases of persistent sexual dysfunction.
Replacing the serotonin theory with vague assurances that more complex biological mechanisms can explain drug action only continues the obfuscation, and enables the marketing of other psychiatric drugs on equally spurious grounds.
Johns Hopkins, for example, is telling people that ‘untreated depression causes long-term brain damage’ and that ‘esketamine may counteract the harmful effects of depression.’ Quite apart from the damage to people’s mental health by being told they have, or will soon get brain damage, this message encourages the use of a drug with a flimsy evidence base and a worrying adverse effect profile.
The serotonin hypothesis was inspired by the desire of the psychiatric profession to regard its treatments as proper medical treatments and the need of the pharmaceutical industry to distinguish its new drugs from the benzodiazepines that, by the late 1980s, had brought the medicating of misery into disrepute.
It exemplifies the way that psychiatric drugs have been misunderstood and misrepresented in the interests of profit and professional status. It is time to let people know not only that the serotonin story is a myth, but that antidepressants change the normal state of the body, brain and mind in ways that may occasionally be experienced as useful, but may be harmful too.
Joanna Moncrieff is a Professor of Critical and Social Psychiatry at University College London, and works as a consultant psychiatrist in the NHS. She researchers and writes about the over-use and misrepresentation of psychiatric drugs and about the history, politics and philosophy of psychiatry more generally. She is currently leading UK government-funded research on reducing and discontinuing antipsychotic drug treatment (the RADAR study), and collaborating on a study to support antidepressant discontinuation. In the 1990s she co-founded the Critical Psychiatry Network to link up with other, like-minded psychiatrists. She is author of numerous papers and her books include A Straight Talking Introduction to Psychiatric Drugs Second edition (PCCS Books), published in September 2020, as well as The Bitterest Pills: The Troubling Story of Antipsychotic Drugs (2013) and The Myth of the Chemical Cure (2009) (Palgrave Macmillan). Her website is https://joannamoncrieff.com/.
RNA for Moderna’s Omicron Booster Manufactured by CIA-Linked Company
BY WHITNEY WEBB |
UNLIMITED HANGOUT| AUGUST 17, 2022
Since late last year, messenger RNA for Moderna’s COVID-19 vaccines, including its recently reformulated Omicron booster, has been exclusively manufactured by a little known company with significant ties to US intelligence.
Earlier this week, the United Kingdom became the first country to approve Moderna’s reformulated version of its COVID-19 vaccine, which claims to provide protection against both the original form of the virus and the significantly less lethal but more transmissible Omicron variant. The product was approved by the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) with the support of the UK government’s Commission on Human Medicines.
Described by UK officials as a “sharpened tool” in the nation’s continued vaccination campaign, the reformulated vaccine combines the previously approved COVID-19 vaccine with a “vaccine candidate” targeting the Omicron variant BA.1. That vaccine candidate has never been previously approved and has not been the subject of independent study. The MHRA approved the vaccine based on a single, incomplete human trial currently being conducted by Moderna. The company promoted incomplete data from that trial in company press releases in June and July. The study has yet to be published in a medical journal or peer reviewed. No concerns have been raised by any regulatory agency, including the MHRA, regarding Moderna’s past history of engaging in suspect and likely illegal activity in past product trials, including for its original COVID-19 vaccine.
The approval comes shortly before several Western countries, including the UK, plan to conduct a massive COVID-19 booster vaccination campaign this fall. Moderna has also noted that approval for its Omicron booster vaccine are pending in the US, EU, Australia and Canada – all of which are also planning fall vaccination campaigns focused on COVID-19. The company’s CEO, Stéphane Bancel, has called the reformulated vaccine “our lead candidate for a Fall 2022 booster.”

Moderna CEO Stéphane Bancel, Source: ClockworkOrange
However, unlike the company’s original COVID-19 vaccine, the genetic material, or messenger RNA (mRNA), for this new vaccine, including the newly formulated genetic material meant to provide protection against the Omicron variant, is being manufactured, not by Moderna, but by a relatively new company that has received hardly any media attention, despite its overt links to US intelligence. Last September, it was quietly announced that a company called National Resilience (often referred to simply as Resilience) would begin manufacturing the mRNA for Moderna COVID-19 vaccine products. Under the terms of the multi-year agreement, “Resilience will produce mRNA for the Moderna COVID-19 vaccine at its facility in Mississauga, Ontario, for distribution worldwide.”
“Reinventing Biomanufacturing”
National Resilience was founded relatively recently, in November 2020, and describes itself as “a manufacturing and technology company dedicated to broadening access to complex medicines and protecting biopharmaceutical supply chains against disruption.” It has since been building “a sustainable network of high-tech, end-to-end manufacturing solutions with the aim to ensure the medicines of today and tomorrow can be made quickly, safely, and at scale.” It further plans to “reinvent biomanufacturing” and “democratize access to medicines,” namely gene therapies, experimental vaccines and other “medicines of tomorrow.”
In pursuit of those goals, the company announced it would “actively invest in developing powerful new technologies to manufacture complex medicines that are defining the future of therapeutics, including cell and gene therapies, viral vectors, vaccines, and proteins.” It was founded with the reported intention “to build a better system for manufacturing complex medicines to fight deadly diseases” as a way to improve post-COVID “pandemic preparedness.”
The company initially marketed its manufacturing capabilities as “the Resilience platform”, and offers principally “RNA Modalities”, including RNA development for vaccines, gene editing and therapeutics; and “Virus Production”, including viral vectors, oncolytic viruses (i.e. a virus engineered to preferentially attack cancer cells), viruses for use in vaccine development and gene-edited viruses for unspecified purposes. It is worth noting that, to date, many controversial “gain-of-function” experiments have justified modifying viruses for the same purposes as described by National Resilience’s Virus Production capabilities. In addition, National Resilience offers product formulations and other modalities, such as biologics and cell therapies, to its clientele and the “Virus Production” of its website has since been removed.

Resilience CEO Rahul Singhvi, Source: Resilience
National Resilience, being such a young company, has very few clients and there is little publicly available information on its manufacturing capabilities aside from the company’s website. The firm only acquired its first commercial manufacturing plant in March 2021, located in Boston, MA and purchased from Sanofi, followed shortly thereafter by the acquisition of another separate plant located in Mississauga, Ontario, Canada. Makeovers were announced for the plants, but little is publicly known about their progress. Prior to the acquisitions, the company had been subleasing a Bay area facility in Fremont, California. Reporters were puzzled at the time as to why a company with roughly 700 employees at the time had acquired a total of 599,00 square feet of manufacturing space after having only emerged from stealth less than 6 months prior.
In April 2021, National Resilience acquired Ology Bioservices Inc., which had received a $37 million contract from the US military the previous November to develop an advanced anti-COVID-19 monoclonal antibody treatment. This acquisition also provided National Resilience with its first Biosafety Level 3 (BSL-3) laboratory and the ability to manufacture cell and gene therapies, live viral vaccines and vectors and oncolytic viruses.
Despite being in the earliest stages of developing its “revolutionary” manufacturing capabilities, National Resilience entered into a partnership with the Government of Canada in July of last year. Per that agreement, the Canadian government plans to invest CAD 199.2 million (about $154.9 million) into National Resilience’s Ontario-based subsidiary, Resilience Biotechnologies Inc. Most of those funds are destined for use in expanding the Ontario facility that Resilience acquired last March and which is now manufacturing the mRNA for Moderna’s COVID-19 products. Canada’s Minister of Innovation, Science and Industry, François-Philippe Champagne, asserted at the time that the investment would “build future pandemic preparedness” and help “to grow Canada’s life science ecosystem as an engine for our economic recovery.” More recently, in 2022, the company has announced a few new clients – Takeda, Opus Genetics and the US Department of Defense.
According to National Resilience’s executives, the company’s ambitions apparently go far beyond manufacturing RNA and viruses. For instance, Resilience CEO Rahul Singhvi has claimed that the company is seeking to build “the world’s most advanced biopharmaceutical manufacturing ecosystem.” Yet, Singhvi has declined to offer much in the way of specifics when it comes to exactly how the company plans to become the planet’s most elite biomanufacturing company.
In an interview with The San Francisco Business Times, Singhvi states that Resilience is looking to fill its massive manufacturing plants with “technologies and people that can set and apply new standards for manufacturing cell therapies and gene therapies as well as RNA-based treatments.” Prior to Resilience, Singhvi was CEO of NovaVax and an operating partner at Flagship Pioneering, which played a major role in the creation and rise of Moderna.
Singhvi has further insisted that National Resilience is “not a therapeutics company, not a contractor and not a tools company” and instead aims “to boost production using the new therapeutic modalities” such as RNA-based treatments, which have become normalized in the COVID-19 era. Whereas contract manufacturers “are like kitchens, with pots and pans ready for any recipe,” “what we’re trying to do is fix the recipes,” Singhvi has explained. One member of Resilience’s board of directors, former FDA Commissioner and Pfizer Board member Scott Gottlieb, has described the company as seeking to act as the equivalent of Amazon Web Services for the biotechnology industry.
Essentially, Resilience bills itself as offering solutions that will allow “futuristic” medicines, including mRNA vaccines, to be produced more quickly and more efficiently, with the apparent goal of monopolizing certain parts of the biomanufacturing process. It also appears poised to become the manufacturer of choice for mRNA vaccines and experimental therapeutics in the event of a future pandemic, which some public health “philanthropists” like Bill Gates have said is imminent.
Perhaps the company’s most noteworthy ambition relates to their claims that they support clients through the government regulatory process. Given the company’s emphasis on speedy mass production of experimental gene therapies, its stated intention of getting the “futuristic” medical products it manufactures to market as quickly as possible seems at odds with the slower, traditional regulatory processes. Indeed, one could easily argue that the approvals of mRNA vaccines for the first time in human history during the COVID-19 crisis were only possible because of the major relaxing of regulatory procedurse and safety testing due to the perceived urgency of the situation.
Resilience seems intent on seeing that phenomenon repeat itself. As previously mentioned, the company claims to allow for the setting and application of “new standards for manufacturing cell therapies and gene therapies” and also says it plans to become a “technology-aggregating standards bearer that helps therapies come to market more efficiently.” It previously offered on its website “regulatory support” and “strategy consulting” to clients, suggesting that it would seek to mediate between clients and government regulators in order to fulfill its goal of having the products it manufactures taken to market more quickly. In addition, upon launch, the company claimed it planned to obtain unspecified “regulatory capabilities.” If so, it is certainly notable that former top Food and Drug Administration (FDA) officials are either on the company’s board or, as will be noted shortly, played a major role in the company’s creation.
The People Behind Resilience
Resilience was co-founded by Biotech venture capitalist Robert Nelsen, who is known for listening “to science’s earliest whispers, even when data are too early for just about anyone else.” Nelsen was one of the earliest investors in Illumina, a California-based gene-sequencing hardware and software giant that is believed to currently dominate the field of genomics. As mentioned in a previous Unlimited Hangout investigation, Illumina is closely tied to the DARPA-equivalent of the Wellcome Trust known as Wellcome Leap, which is also focused on “futuristic” and transhumanist “medicines.” Nelsen is now chairman of National Resilience’s board, which is a “Who’s Who” of big players from the US National Security State, Big Pharma and Pharma-related “philanthropy.”

Bob Nelsen of ARCH Venture Partners, Source: ARCH Venture Partners
However, while Nelsen has been given much of the credit for creating Resilience, he revealed in one interview that the idea for the company had actually come from someone else – Luciana Borio. In July of last year, Nelsen revealed that it was while talking to Borio about “her work running pandemic preparedness on the NSC [National Security Council]” that had “helped lead to the launch of Nelsen’s $800 million biologics manufacturing startup Resilience.”
At the time of their conversation, Borio was the vice president of In-Q-tel, the venture capital arm of the CIA that has been used since its creation in the early 2000s to found a number of companies, many of which act as Agency fronts. Prior to In-Q-Tel, she served as director for medical and biodefense preparedness at the National Security Council during the Trump administration and had previously been the acting chief scientist at the FDA from 2015 to 2017.
Borio is currently a senior fellow for global health at the Council on Foreign Relations, a consultant to Goldman Sachs, a member of the Bill Gates-funded vaccine alliance CEPI, and a partner at Nelsen’s venture capital firm ARCH Venture Partners, which funds Resilience. Nelsen’s ARCH previously funded Nanosys, the company of the controversial scientist Charles Lieber. Around the time of her conversation with Nelsen that led to Resilience’s creation, Borio was co-writing a policy paper for the Johns Hopkins Center for Health Security that recommended linking COVID-19 vaccination status with food stamp programs and rent assistance as a possible means of coercing certain populations to take the experimental vaccine.
Borio is hardly Resilience’s only In-Q-Tel connection, as the CEO of In-Q-Tel, Chris Darby, sits on the company’s board of directors. Darby is also on the board of directors of the CIA Officers Memorial Foundation. Darby was also recently a member of the National Security Commission on Artificial Intelligence (NSCAI), where members of the military, intelligence community and Silicon Valley’s top firms argued for the need to reduce the use of “legacy systems” in favor of AI-focused alternatives as a national security imperative. Among those “legacy systems” identified by the NSCAI were in-person doctor visits and even receiving medical care from a human doctor, as opposed to an AI “doctor.” The NSCAI also argued for the removal of “regulatory barriers” that prevent these new technologies from replacing “legacy systems.”

Resilience Board Member Drew Oetting, Source: 8VC
Another notable board member, in discussing Resilience’s intelligence ties, is Drew Oetting. Oetting works for Cerberus Capital Management, the firm headed by Steve Feinberg who previously led the President’s Intelligence Advisory Board under the Trump administration. Cerberus is notably the parent company of DynCorp, a controversial US national security contractor tied to numerous scandals, including scandals related to sex trafficking in conflict zones. Oetting is also part of the CIA-linked Thorn NGO ostensibly focused on tackling child trafficking that was the subject of a previous Unlimited Hangout investigation.
Oetting is also the co-founder of 8VC, a venture capital firm that is one of the main investors in Resilience. 8VC’s other co-founder is Joe Lonsdale and Oetting “started his career” as Lonsdale’s chief of staff. Lonsdale is the co-founder, alongside Peter Thiel and Alex Karp, of Palantir, a CIA front company and intelligence contractor that is the successor to DARPA’s controversial Total Information Awareness (TIA) mass surveillance and data-mining program. In addition, Oetting previously worked for Bill Gates’ investment fund.
Also worth noting is the presence of Joseph Robert Kerrey, former US Senator for Nebraska and a former member of the conflict-of-interest-ridden 9/11 Commission, on Resilience’s board. Kerrey is currently managing director of Allen & Co., a New York investment banking firm which has hosted an annual “summer camp for billionaires” since 1983. Allen & Co. has long been a major player in networks where organized crime and intelligence intersect, and is mentioned repeatedly throughout my upcoming book One Nation Under Blackmail. For instance, Charles and Herbert Allen, who ran the firm for decades, had considerable business dealings with organized crime kingpins and frontmen for notorious gangsters like Meyer Lansky, particularly in the Bahamas. They were also business partners of Leslie Wexner’s mentors A. Alfred Taubman and Max Fisher as well as associates of Earl Brian, one of the architects of the PROMIS software scandal – which saw organized crime and intelligence networks cooperate to steal and then compromise the PROMIS software for blackmail and clandestine intelligence-gathering purposes. Allen & Co. was a major investor in Brian’s business interests in the technology industry that Brian used in attempts to bankrupt the developers of PROMIS, Inslaw Inc. and to market versions of PROMIS that had been compromised first by Israeli intelligence and, later, the CIA.
In addition to these intelligence-linked individuals, the rest of Resilience’s board includes the former CEO of the Bill & Melinda Gates Foundation, Susan Desmond-Hellmann; former FDA Commissioner and Pfizer board member, Scott Gottlieb; two former executives at Johnson & Johnson; former president and CEO of Teva Pharmaceuticals North American branch, George Barrett; CalTech professor and board member of Alphabet (i.e. Google) and Illumina, Frances Arnold; former executive at Genentech and Merck, Patrick Yang; and Resilience CEO Rahul Singhvi.
To Boost or Not to Boost
It is certainly telling that the normally publicity hungry Moderna has said so little about its partnership with Resilience and that Resilience, despite its ambitious plans, has also avoided the media limelight. Considering Moderna’s history and Resilience’s connections, there may be more to this partnership that meets the eye and concerned members of the public would do well to keep a very close eye on Resilience, its partnerships, and the products it is manufacturing.
Given that we now live in a world where government regulatory decisions on the approval of medicines are increasingly influenced by corporate press releases and normal regulatory procedures have fallen by the wayside for being too “slow,” there is likely to be little scrutiny of the genetic material that Resilience produces for the “medicines of tomorrow.” This seems to be already true for Moderna’s recently retooled COVID-19 vaccine, as there has been no independent examination of the new genetic sequence of mRNA used in the Omicron-specific vaccine candidate or its effects on the human body in the short, medium or long term. For those who are skeptical of the outsized role that intelligence-linked companies are playing in the attempted technological “revolution” in the medical field, it is best to consider Resilience’s role in the upcoming fall vaccination campaign and in future pandemic and public health scenarios before trying its “futuristic” products.
Whitney Webb has been a professional writer, researcher and journalist since 2016. She has written for several websites and, from 2017 to 2020, was a staff writer and senior investigative reporter for Mint Press News. She currently writes for The Last American Vagabond.
Featured Video

Pressure to REMOVE TRUMP FROM OFFICE Growing
or go to
Aletho News Archives – Video-Images
From the Archives
UK Researchers: Tax Food to Reduce Climate Change

I doubt these professors have anything to fear from a food tax
By Eric Worrall | Watts Up With That? | November 19, 2016
A group of researchers in Oxford University, England have suggested that imposing a massive tax on carbon intensive foods – specifically protein rich foods like meat and dairy – could help combat climate change. […]
This proposal, from a group of people who have probably never missed a meal in their lives, is totally obscene. High income countries often have a lot of poor people who would be hard hit by increases in the price of food.
Needlessly exacerbating the risk poor people don’t get enough to eat, especially children and pregnant mothers, who are especially vulnerable to adverse health impacts from lack of protein in their diet – if this ghastly proposal is ever implemented, future generations will look upon it as a crime against humanity. – Read full article
Blog Roll
 Aletho News
Aletho News- Iran, Saudi FMs hold phone talks as Persian Gulf states rethink US ties
- The Illusions of Western Virtue: Ursula von der Leyen and Europe’s Moral Bankruptcy
- AIPAC-backed candidates lose New York primaries as voters reject pro-genocide lobby
- The West’s Post-Soviet ‘Democracy’ Playbook
- UK suppressed intel on Sudan genocide to protect UAE ties: Report
- Starmer’s exit exposes dirty secret: UK can’t afford Ukraine War
- Putin Warns the West: Russia Is Ready
- BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
- There Are No Budget Constraints In New York City: “Coastal Resiliency” Edition
- The UN’s plan to levy taxes on global trade is a sinister power grab
- If Americans Knew
- Israel’s Attacks on Gaza’s Children (Photos)
- ‘His only crime is that he is a Palestinian doctor’
- ‘Killed pursuing her dream’: Gaza girl on her way to school dies in Israeli drone strike
- Unbelievable pressure on Gaza from Israel, “Board of Peace” – Daily Update
- UN: Israel Continues to Commit Genocide and Other Atrocity Crimes by Deliberately Targeting Palestinian Children
- Bari Weiss, Free-Speech Fraud & Zionism Promoter, Would Rather Deport Than Debate
- ‘Doctor of the Poor’: Israeli Occupation Arrests Prominent Palestinian Physician
- Search for Your Church (and see if it has been targeted by the Israeli gov’t)
- Mark Levin Flying to Israel as Netanyahu Reportedly Seeks to ‘Leverage’ Levin to Trash Trump’s Iran Deal
- Watch: Zionist Brags about Israel’s Power to Get the World to Do What Israel Wants
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
