Israel occupation forces bulldoze Greek Orthodox land in occupied Jerusalem
MEMO | January 16, 2023
The Israeli occupation authorities yesterday started to bulldoze a 5,000 square metre plot of land owned by the Greek Orthodox Church in occupied Jerusalem’s Silwan neighbourhood, the Wadi Hilweh Information Centre has reported. The operators of the bulldozers were protected by a large number of Israeli occupation security forces and police.
According to the centre, the Israeli Nature and Parks Authority as well as settler organisations commissioned the bulldozers to uproot fruit-bearing trees and level the land. Illegal settlers and police seized the land on 22 December. The Jewish settlers fenced it off and installed surveillance cameras under police protection.
When Silwan residents rushed to the scene to stop the land theft, they were assaulted by security forces, said the centre, which monitors Israeli violations in the area. The land is owned by the Greek Orthodox Monastery in Silwan, which is part of the city’s Greek Orthodox Patriarchate.
Silwan is home to more than 60,000 Palestinians and is located strategically to the south of Al-Aqsa Mosque. The area has been the target of Israeli settler expansion for years, with hundreds of Palestinian families facing the threat of expulsion, either through lawsuits by powerful settler groups or administrative eviction orders by the Israeli-run Jerusalem municipality.
Middle East Eye has reported that the Greek Orthodox Church has been criticised heavily by Palestinian groups for its dealings with settlers and allegations of bribery and fraud. In 1951, church-owned land in West Jerusalem was rented to the Jewish National Fund for a period of 99 years. Today, the land houses most Israeli state institutions, including Israel’s parliament, the Knesset.
The Lancet has become a laughing stock
By Norman Fenton and Martin Neil | Where are the numbers? | January 14, 2023
In summary:
- On 6 May 2021 The Lancet published a blatantly flawed study of the effectiveness of the Pfizer covid vaccine on the population of Israel, claiming it was 95% effective.
- On 17 May 2021 we submitted a rapid response 250 word letter explaining why the study was flawed.
- After an initial response saying they would ask the authors for a response to our letter we heard nothing until 20 months later.
- On 8 January 2023 we got an email out of the blue from The Lancet Senior Editor Josefine Gibson apologising for never having got back to us about the letter, saying that they had asked the lead author Dr Sharon Alroy-Preis (SA-P) to respond to our letter but, because she did not provide any formal response, they have decided not to publish our letter.
- We tweeted The Lancet’s response and within 24 hours it got over one million impressions. We also published a substack article highlighting the fact we were now aware of additional problems with the paper relating to SA-P’s relationship with Pfizer.
- On 10 January 2023 we got an unsolicited email from Josefine Gibson (which we can only assume was a result of the reputation hit they got from our tweet) saying “Thank you for bringing your letter from May 2021 back to our attention. We are looking into next steps and will get back to you as soon as we can.”
- On 11 January 2023 (at 10:58) we sent an email to The Lancet’s Editor-in-Chief Richard Horton directing him to our substack article (which highlighted these new problems relating to SA-P’s relationship with Pfizer) stating that The Lancet was clearly taking a credibility hit surrounding the publication of the Israel-Pfizer study and its response to criticisms of it.
- On 11 January 2023 (at 11:21) we got an email from Josefine Gibson apologising for the ‘sub standard experience’ we had with The Lancet. She said that, after discussing it with Horton, they were now inviting us to publish the original letter or an update to it, suggesting the update ‘reflect more current experience with the vaccine’.
- On 12 January 2023 we submitted our updated letter (of an agreed 350 words).
- On 13 January 2023 we got a response from Josefine Gibson saying they had decided against publishing the letter.
Here is the full narrative and January 2023 correspondence in date order (personal details redacted)… continue
Insider reveals truth about Covid-19 pandemic from within the National Health Service
How the misdiagnosis of deaths occurred and was due to changes from 2016
The Naked Emperor’s Newsletter | January 15, 2023
An ex-director at one of the largest hospital trusts in the UK decided they wanted to reveal what really happened during the pandemic. They have kindly allow me to reproduce their thoughts. The catalyst for this revelation, according to the insider, was Dr. Malhotra speaking out about cardiac problems post vaccination.
This is an interesting take on what happened inside the National Health Service (NHS) and confirms, with more details, what we already knew and suspected.
Introduction (Long but important to understand the rest)
In 2016, the British Government proposed & piloted a change to the process of how deaths were certified across all hospitals in the UK. I have attached a link to this Department of Health (DoH) document.
The DoH document proposed a switch to the “Medical Examiner” (ME) System and was sent to a number of different audiences for feedback and consultation. The ME system was already being piloted at two hospitals up north. The results of the consultation are here.
Prior to the Covid-19 Pandemic, the death certification process involved treating doctors of a patient to attend Bereavement Services/Patient Affairs to discuss the death and either:
a) refer the death to the Coroner or
b) write a Medical Certificate of Cause of Death (MCCD).
The MCCD states the cause of death. Whereby a direct cause (1a) or contributing causes (1b) (1c) (1d) are stated along with co-morbidities (not directly causing the death) being written in (2) on the MCCD. The MCCD is only ever a probable cause of death, it is not definitive.
The only definitive way of determining an accurate and plausible cause of death is to refer the deceased patient to HM Coroner (if certain criteria is met), for HM Coroner to accept and take on the case, resulting in a Post Mortem (PM) being conducted by a Histopathologist. When a death is seen as natural and there is nothing untoward, the MCCD is written by the treating doctor of a deceased patient. Usually this is an F1, F2, SHO or Registrar that attends. It is rare for a treating Consultant to attend, but they will finalise the cause of death.
A strict hospital hierarchy exists within the NHS for doctors. It is as follows – from lowest to highest rank: Foundation Year 1 (FY1), Foundation Year 2 (FY2), Senior House Officer (SHO), Registrar (Reg), Consultant, Clinical Lead, Medical Director. Junior doctors will very rarely speak up or challenge their seniors. A senior decision is seen as final and it will be carried out and executed without any hesitance or questioning. In my 5.5 years of experience in End of Life Care, I have only ever seen one junior doctor disagree with a proposed cause of death and challenge their consultant.
With the number of deaths that occur in a hospital, as you can imagine, there is a great deal of variation with regards to causes of death, as we have numerous different doctors writing an MCCD and coming up with various different potential diseases in different orders.
The proposed ME system would change this, as the government would now hire and pay one Medical Examiner, to sit in every hospital and write all MCCD’s for all deceased patients. This would effectively eliminate any variation in causes of death.
In 2016, when I heard of this proposal, I worked as a Bereavement Officer at a hospital in Central London. My mentor/line manager at the time was a former Chief Nurse who managed Bereavement Services and all hospital deaths would be controlled by her and the department.
We essentially carried a huge amount of power with regards to decision making, as we would go through all patient notes following the death of a patient, and essentially guide and advise doctors on what would need to be written with regards to an MCCD or Coroners Referral.
In my personal opinion, our role was to sit on the fence and act in the best interests of a deceased patient (and their families), but also protect the hospital and our doctors from any potential negligence. As you can imagine many battles were fought over decisions about a cause of death of a patient or a referral to the coroner with a vast amount of doctors over the years.
F2’s and SHO’s were particularly the worst with regards to carrying an arrogance of knowing what should be written on an MCCD or stating that a patient didn’t need to be referred to the Coroner (often stating that their Consultant had given them instructions). It is worth noting that Consultants are also only human and can be incorrect at times too. We have to remember that they are succeeded in hierarchy by a Clinical Lead and beyond that a Medical Director. Who have far more experience and knowledge.
When I asked my mentor in 2016, how the ME system would change things, I was told that Bereavement Services/Patient Affairs would become purely administrative and that the clinical judgement would fall to the Medical Examiner.
The power and decision making with regards to MCCD/Coroners Referrals was being taken away not only from treating doctors but also from Bereavement Services/Patient Affairs/Bereavement Officers/Bereavement Service Managers/Directors of End of Life Care.
This decision making power was being handed solely to the Medical Examiner, who has not been involved in the treatment of a patient during an admission. I took all this information in at the time and acquired as much knowledge as I could from my mentor/line manager.
In 2016, I also happened to make a move and take up an opportunity to manage my own Bereavement Services at one of the largest hospital trusts in the whole of the UK. On average, I would oversee MCCD/Coroner Referrals for approx 1750 deaths on an annual basis. I developed a very close working relationship and friendship with one of the Medical Directors (a doctor with the highest ranking in a hospital). This was especially helpful when having to challenge doctors with regards to MCCDs/Coroners Referrals.
Progressing to Director of End of Life Care, I became involved with the reporting of mortality rates, conducting mortality reviews and writing hospital policies. I had also developed an excellent working relationship with the HM Coroner who oversaw our Trust. HM Coroner holds the power to investigate any hospital or trust with regards to a death or a number of deaths. A slight problem may arise, in that HM Coroner has an allegiance to the Crown and the Government.
When a death is reported to the Coroner. This was previously reported via telephone call by the treating doctor. A discussion was had with the Coroners Office and a direct outcome and instruction would come from the Coroner’s Office, by way of HM Coroner (via a phone call).
There is a fundamental flaw to this system, as there is no documentation of the decision and instruction from the Coroner’s. It comes via word of mouth. There is always room for error without any electronic documentation. Every Hospital/Trust & HM Coroner will have a different system of reporting deaths. I personally made a decision to safeguard my hospital and the trust, by developing an electronic coroners referral form, which I proposed to our Coroner and developed after their agreement. We now had documentation of every death being reported and every outcome.
When reporting a death, the Coroner will look at a proposed cause of death and accept it, or reject the cause of death and take on the case (death of the patient), leading to an Inquest or a PM.
In 2019, our Medical Director, came into my office one morning and stated that the Board of Directors at the Hospital had made a decision to switch to the Medical Examiner System. Hearing the words ME system was a massive case of Déjà vu (conversation with my mentor in 2016). I knew exactly what the ME system was, but I chose instead, to play the fool and enquire what exactly the ME system was and what it meant for our service, my staff and our roles. Everything the Medical Director mentioned to me that day was a carbon copy of what I already knew
I knew that my time in End of Life Care had come to an end. I’d reached the top and there was no more progress for me. Losing all power and decision making to any ME coming into the hospital did not appeal to me. I’d already made up my mind that I needed to leave. Seeking a new challenge and experience, I made a move in 2019 to another major hospital in Central London, this time side tracking into operational management. I was in charge of the operational management of Nephrology, Rheumatology, Dermatology and Diabetes & Endocrinology.
2020 – Covid Arrives
In Jan 2020, I remember hearing about the first case of Covid-19 at our hospital, with a patient arriving from China and walking into our A&E. A&E was shutdown and steam cleaned that day, I recollect the moment I heard about this. In my mind, I saw the reporting of Covid-19 in the media as nothing more than Bird Flu or Ebola, which had caused panic but yet passed. I wasn’t worried in the slightest bit.
Things began to escalate around in Feb 2020, around the time I was going on holiday. Due to the reporting by the media, I bought N95 masks as a precaution for my trip and to give to my parents and younger sister. I was blessed to have had an opportunity to spend a few days in Sri Lanka for a wedding and then nearly a whole month in Australia (March 2020). I watched as the narrative of a deadly infectious disease continued to grow with every day that passed. I made a decision to cut my holiday short by a couple of days so that I could make sure I got back to my family and not end up being stranded in Australia.
Upon returning to the UK in late March 2020. One of the immediate things that struck me was the lack of any temperature monitoring or questioning at Heathrow Airport. This seemed odd for a potentially deadly infectious disease that was spreading around the world. This was especially odd, as Sri Lanka & Australia had questioned me/checked temperatures upon arrival, with even Singapore monitoring temperatures during transit.
My mother had just recovered from Cancer, my father was over 70 and my younger sister was born with Down’s Syndrome alongside having multiple other conditions. I had three high risk individuals to Covid-19 in my family and I was scared/fearful of giving them Covid-19. I asked my hospital to allow me to work from home. They refused. I wasn’t deemed high risk, although I lived with my parents at the time. I needed to help my mum and my sister. The hospital held no regard for the safety of it’s employees. They forced me to come into work. I spent two months isolating in my bedroom, I barely came out of my room, for fear of spreading an infectious disease. Never once did I think about the situation or my prior experience or knowledge, I was just reacting to the media frenzy. I was full of panic and stress.
The first irregularity I noticed, was the government and media stating that Covid-19 was an infectious disease. However just before the first lockdown was implemented, I noted that the government had downgraded the status of Covid-19 stating it was no longer infectious. This made no sense to me. Why would we need to isolate if they downgraded the status? My circle of friends contained many medics and dentists. They were all panicking at the time, saying they had inadequate surgical masks and that they needed N95 masks.
N95 masks were seen as the only way to prevent medical professionals from becoming infected with Covid-19. The public being asked to wear surgical masks made no sense to me. The virus would be able to go straight through. Something didn’t seem right.
I ended up meeting and dating an FY1 doctor (my ex gf) around October 2020. We clicked because she was different from every other doctor, I had previously spoken to about Covid-19. She also had her suspicions and believed it wasn’t as infectious as it was made out to be. We both started to slowly realise that Covid-19 was a real disease (as it was showing up on X-rays in patients) but that it wasn’t infectious at all [NE – I have since confirmed with them that they mean not as infectious as was being made out], despite all the reporting in the media.
I needed to experience working in a Covid-19 hotspot and see all the action for myself. In March 2021, I quit my job at the hospital in Central London and took up an opportunity to manage A&E and AMU (Acute Medical Unit) at a hospital in South London. The 6 months that I spent working in A&E/AMU confirmed all my suspicions and culminated in my decision to end my career in the NHS.
The entire 6 months, I was not tested once with a PCR Test, despite walking into wards full of Covid-19 Positive patients on a daily basis. Yet we were required to test multiple times when visiting another country.
The PCR Test that the NHS was using to test patients, is known to have false-positive results. This is shown in numerous studies which can be found online, an example of which is:
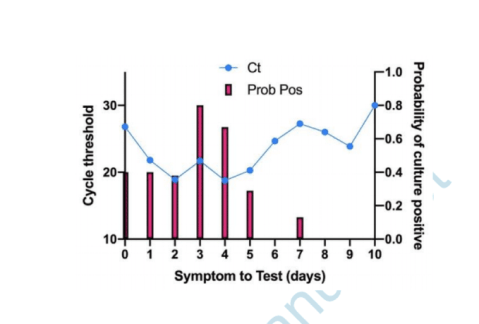
Are you infectious if you have a positive PCR test result for COVID-19? – The Centre for Evidence-Based Medicine.
If a patient tests positive for Covid-19 with a PCR Test, this doesn’t mean they are infected. If tested again, they may well turn out with a negative test. However in the NHS, patients are only tested once and this stays on their record throughout their admission. Hospital policies were changed alongside the implementation of the Medical Examiner System, to ensure that any patient who died within 30 days of positive test, would have to have Covid-19 as their primary cause of death. This was regulated by the Medical Examiner.
The highest cause of death at every hospital per annum pre Covid-19 is Pneumonia. Pneumonia is a Respiratory Disease like Covid-19. Pneumonia can be broken down into 4 different causes of death: Bronchopneumonia, Aspiration Pneumonia, Community Acquired Pneumonia & Hospital Acquired Pneumonia.
These four causes when added together kill the largest number of people on an annual basis prior to the pandemic.
The Medical Examiner (one individual in each hospital), was certifying all these Pneumonia deaths as Covid-19 deaths. When 4 different diseases being grouped and now being called Covid-19, you will inevitably see Covid-19 with a huge death rate.
The mainstream media was reporting on this huge increase in Covid-19 deaths due to the Medical Examiner system being in place. Patients being admitted and dying with very common conditions such as Old Age, Myocardial Infarctions, End Stage Kidney Failure, Haemorrhages, Strokes, COPD & Cancer etc were all now being certified as Covid-19 via the Medical Examiner System.
Hospitals were switching to and from the Medical Examiner system and the Pre Pandemic System as when they pleased. When Covid-19 deaths needed to be increased, the hospital would switch to the Medical Examiner System. Doctors were one week being told they needed to complete an MCCD, to then be told the following week that they weren’t required to fill out an MCCD, as the Medical Examiner was handling this.
Hospitals were incentivised to report Covid-19 deaths over normal deaths, as the government was paying hospitals additional money for every Covid-19 death that was being reported. The Medical Examiner system ensured that Covid-19 was being put down as the cause of death. The government sends out the annual NHS budget to Primary Care Trusts. This is split to fund Hospitals and GP Surgeries. A clinical coding team at each hospital will assign codes to each treatment or death, so that money is paid out to the hospitals.
Any doctor who argued against Covid-19 as a cause of death was bullied and vilified. The General Medical Council maintains a register of all doctors within the UK. This ensures that there is a fear of being struck off for speaking out against an agenda. The GMC effectively controls all doctors in the UK. Even if a doctor realises what is going on and wants to speak out. They will think twice about talking, as they would be risking their entire career and everything that they’ve worked so hard for.
Doctors essentially have their hands tied, many have families, kids, mortgages and mouths to feed. If I was in their situation, I would think twice about speaking out, for fear of being struck off by the GMC and losing everything.
The NHS Track & Trace App, which was introduced to try and control the spread of the virus, did not apply to medical professionals. We were all asked to turn this off, as Doctors and staff isolating for 14 days disrupted patient flow, beds and the discharge of patients.
Any doctor that I spoke to regarding taking the Covid-19 vaccine, were insistent that they were going to wait for a period of time, before taking it themselves, to ensure that it was safe. How is it ethical to give a vaccine to your patients, but not want to take it yourself? In my 12 years of NHS service, never has a doctor pushed or influenced the public to take a vaccine. Yet on social media, I was seeing close friends who were doctors, starting to post on social media that they have taken the vaccine and that the public should. I wouldn’t be surprised if doctors were being forced to promote the vaccine by their superiors or if they were receiving monetary gain in doing so.
I have no doubt in my mind, that the Government has planned the entire pandemic since 2016, when they first proposed the change to medical death certification. Stress leads to disease and illness. Panic leads to people following whatever orders and instructions that are given to them by authority, such as prolonged mask use, which leads to an increase in admissions in to the NHS system due to hypoxia and bacterial pneumonia.
The NHS treatment pathway involved patients being placed onto ventilators. There is a 50% chance of death from this clinical decision alone. How many innocent people have died from the clinical decision to place them onto a ventilator.
During boardrounds (where every admitted patient is discussed), we were seeing patients on a daily basis being admitted due to suffering from adverse affects of taking the vaccine. Patients were blacking out after taking the vaccine or suffering from clots or strokes.
The NHS is all about money and making money. The safety of a patient didn’t seem like the most important thing. It was more about how do we make more beds available so that another patient can be treated. Patients with no next of kin are discharged to nursing homes with care packages. I can’t comment on what happened to these patients in nursing homes, during the pandemic, as I have no experience of their inner workings.
Patients are seen as money, even upon death, hospitals receive money for each death. Is there an actual concern for patient health and safety? I know numerous doctors who are driven primarily by money and monetary gain.
THE REASON WHY I LEFT THE NHS in 2021
56 yr old male, admitted into A&E with end stage kidney failure, has a previous history of regular dialysis treatment for this. No respiratory symptoms on admission and no temperature. However when tested with a PCR Test he unfortunately tests positive. This stays on his record throughout his admission. Our hospital is relatively small in comparison to others I have worked at, we have no dialysis machine as a result. We urgently need to transfer this patient to another hospital otherwise this patient will die. Our treating doctor calls up larger hospitals with a dialysis machine to organise his transfer. All doctors pick up the phone and request the Covid-19 status of the patient. A transfer is declined due to a Covid-19 infection protocol. Our doctors again reiterate the point that this patient will die without dialysis. We are told there is nothing that can be done and that the patient cannot be accepted for transfer.
This gentleman ended up dying without dialysis. Now please tell me what goes on the MCCD….
1a) Covid-19
2) End Stage Kidney Failure
Not written by the treating doctor who disagreed with this cause of death, but by a medical examiner, put in place by the government and the hospital.
When innocent people are being killed by a corrupt organisation and system, for pure monetary gain, I can’t stand by and be part of this anymore. My conscience was clear and I no longer wanted to be a part of this anymore. I am very blessed and lucky that I was in a position to walk away. I’ve been able to speak out, because my hands are not tied and I am not regulated by any organisation or governing body. I believe in speaking the truth and in doing so, I am only just an instrument for God.
I joined the NHS, 12 years ago because I had a desire to help those in need, but the moment I realised that I was not doing this anymore was the time for me to walk away. I apologise to you all if the above thread is confusing with regards to terminology or you cannot understand it’s contents. I’m hoping that at the very least, it can be understood by my fellow medical professionals or by journalists who would like to report the truth.
Who designed global guidelines for puberty blockers?
Free West Media | January 13, 2023
Clinics around the world follow guidelines from the Netherlands for gender treatments in children. The basis for this is, among other things, a much-criticized study sponsored by a German hormone manufacturer.
More and more children and young people believe they have to question their gender identity. Some 60 minors were treated in the Netherlands in 2010, but the number has increased to around 1,600 last year. Another 1,800 people under the age of 18 were on the waiting list because gender clinics in the country are full.
Institutions around the world use a standard procedure developed in Amsterdam in the 1990s when it comes to the drug treatment of supposedly transsexual children.
A report by the Dutch newspaper NRC Handelsblad has meanwhile cast doubt on the directive and the independence of gender research at the Amsterdam UMC hospital. As strict as the conditions for treatment may appear, several complications have been overlooked: The terrible side effects of the heavy drug has been brushed off by doctors as being the lesser evil.
Hormone manufacturer sponsored ‘puberty blocker’ study
The approach with puberty inhibitors has since been known internationally as the “Dutch protocol”. The protocol has become the basis for the “gender-affirming standard of care” used throughout the world. Tens of thousands of children are affected worldwide, and in the Netherlands certainly several hundreds, although no precise figures are available.
Scientists investigated whether hormone treatment in transsexuals is more successful if their puberty was initially suppressed with medication. The sponsor of the study was the German hormone manufacturer.
Ferring Pharmaceuticals, the company that markets the drug Triptorelin as a puberty inhibitor had a strong commercial interest in the outcome. Primarily, treatment relies on administering hormones from the opposite sex: men are given oestrogen to become more feminine, women testosterone to become more masculine. But teenagers are additionally administered puberty inhibitors, which prevent boys from developing a low voice and beard growth and girls from developing breasts and other feminine shapes.
There are many criticisms of the study. Questionnaires were inconsistent, there was no control group at all, and the researchers used random samples from the 196 treated children for the results.
Several countries are moving away from ‘puberty blockers’
In the meantime, there is objection in more and more countries to the treatment of children with “puberty blockers”. Not only are they said to impair the physical sexual development of minors, but they can also cause osteoporosis, anorgasmia and infertility. According to the NRC, the drug is said to sometimes even impair the ability to make rational decisions.
Worldwide, there is increasing criticism of the scientific content and non-existent empirical basis of the Dutch protocol developed at the gender clinic of the Free University of Amsterdam. In several countries, health authorities have already decided to treat children mainly psychologically and prescribe puberty inhibitors only exceptionally. In Sweden, they concluded that “the risks currently outweigh the possible benefits” and spoke of possibly the country’s “worst medical scandal”.
In the UK, criticism of the Dutch protocol was so serious that the Tavistock gender clinic, the largest in the world, was closed by the authorities.
Sweden, Finland and Great Britain only want to prescribe the drug in rare, particularly severe cases. Instead, they are increasingly relying on psychological support for patients.
Since February last year, Sweden’s National Board of Health and Welfare has followed the Karolinska Institute’s policy regarding hormonal interventions for gender-dysphoric minors. Karolinska’s pediatric gender services at Astrid Lindgren Children’s Hospital (ALB) has ended the practice of prescribing puberty blockers and cross-sex hormones to gender-dysphoric patients under the age of 18.
Marketing redundant drugs for the wrong condition
In the US, Texas Attorney General Ken Paxton has been investigating two pharmaceutical companies for advertising puberty blockers to children. This is a condition they are not approved to treat.
In December, Paxton announced investigations under the Texas Deceptive Trade Practices Act into Endo Pharmaceuticals and AbbVie Inc., the two companies that sell puberty blockers. The drugs were approved to treat precocious puberty and forms of prostate cancer but were being marketed and prescribed off-label to treat gender dysphoria.
“These drugs were approved for very different purposes and can have detrimental and even irreversible side effects,” Paxton said. “I will not allow pharmaceutical companies to take advantage of Texas children.”
Republicans Preparing to Move Forward With Ukraine Aid Audit, US Congresswoman Greene Says

Samizdat -13.01.2023
WASHINGTON – US Congresswoman Marjorie Taylor Greene said on Friday that she and other House Republican lawmakers are preparing to move forward with an audit of US aid to Ukraine, an idea first proposed late last year before the House Republican majority took effect.
“We don’t even have committees filled yet but [Congressman Michael McCaul] and I are already preparing to move forward with the audit of Ukraine. No more blank checks to Ukraine,” Greene said via Twitter.
House Republicans are committed to transparency for US taxpayers, Greene added.
In November, Greene and several other House Republicans introduced a resolution to initiate an audit of funds appropriated by Congress to Ukraine. The measure failed during the “lame duck” session of the 117th Congress, but Greene vowed to reintroduce the idea in the new 118th Congress.
House Republicans now hold a majority in the lower chamber, with Speaker Kevin McCarthy having started the party’s mantra of ending “blank checks” from the US to Ukraine. McCarthy also backed the initial Ukraine aid audit proposal.
On Thursday, Pentagon Press Secretary Pat Ryder said that the Defense Department is responsive to oversight by Congress, adding that he looks forward to further bipartisan support for Ukraine.
However, defense budget cuts proposed by the new House Republican majority could force hard questions about funding for foreign operations related to Ukraine and NATO, former Pentagon analyst and retired US Air Force Lt. Col. Karen Kwiatkowski told Sputnik.
Greene has also called for Ukraine to begin negotiations toward a peaceful resolution of the conflict, characterizing it as a “proxy war” between the United States and Russia.
Ivermectin’s Effectiveness Proven Again; 72% Efficacy
800,000 people died in the USA for nothing
By Igor Chudov | January 11, 2023
You are not a horse! You are not a cow! That’s what the FDA told us to dissuade us from taking Ivermectin.

Fortunately, we are also not sheep and did not believe the FDA. Many of us stocked up on Ivermectin, and most found it helpful. While I did not use it when I had my Covid in Nov 2020, it worked great for my wife in Dec 2021 and other family members during the summer of 2022.
Ivermectin, a cheap and safe generic medication, was of little interest to profit-minded pharmaceutical giants like Pfizer and Merck. Therefore, they conspired with the FDA to lie that it did not work and instead pushed expensive Covid vaccines and non-working drugs like mutagenic Molnupiravir and rebound-causing Paxlovid.
MedinCell conducted a randomized controlled trial of their version of Ivermectin and found that it reduces Covid infections by 72%!

The study was very well designed because the participants were EXPOSED to the Covid infection within five days. Given the exposure, the outcomes were more likely to happen and thus were easier to compare between groups, giving the trial greater statistical power.
The 72% reduction in infection is much MORE effective than the “covid vaccine.”
The trial encompassed the period of Mar-Nov 2022, thus giving us the real-world effectiveness of Ivermectin against the Omicron variant.
While I am happy at the finding, there are several things to be NOT happy about.
- If we are to believe official numbers, about 1,121,000 people died of Covid in the USA. Given published effectiveness estimates of Ivermectin coming from honest studies, Ivermectin could have saved eight hundred thousand of those lives. The intentional suppression of Ivermectin cost us so dearly.
- Given a 72% reduction in infection, natural immunity with Ivermectin would likely have stopped the pandemic entirely in 2020.
- Had Ivermectin been recognized as an effective antiviral, the “Covid vaccines” could not get EUA approval, and thus we would avoid thousands of vaccine victims and destroyed immune systems.
- Second-largest Democratic donor and the largest crypto thief Sam Bankman-Fried donated 18 million dollars to the Together trial after it falsely demonstrated a finding that Democrat-aligned Covid vaccine pushers wanted, namely that Ivermectin allegedly was useless.

The good news here is that Ivermectin works.
Here are some of my other articles about Ivermectin — with honest trials showing a comparable reduction in illness and death.
So, thousands of people died of Covid. Thousands of people died of Covid vaccines. The pandemic, prolonged by vaccination, is raging and reinfects people with immunity disabled by mystery genetic treatments. My prediction from last March, unfortunately, is coming true.
AIDS-Like “Chronic Covid” is Taking Over Europe, Australia and NZ
All of this happened because of the recklessness and greed of the biomedical-industrial complex, which developed Sars-Cov-2 and then pushed an unproven, ineffective vaccine that worsened the pandemic.
While the above paragraph is upsetting, the good news is that Ivermectin was validated, and “we have the tools” to manage a Covid infection or exposure.
Lastly, take a minute to think about millions of victims of suppression of Ivermectin worldwide, who died to make a few companies and foundations richer and more powerful.
Will Ivermectin ever be recommended officially? And do we even care about such approval if we can still order it online?
US House Establishes Panel to Investigate Potential Weaponization of Federal Government
Samizdat – 11.01.2023
WASHINGTON – The US House of Representatives on Tuesday passed a resolution establishing a select subcommittee to investigate whether components of the federal government have been weaponized against everyday citizens.
House lawmakers passed a resolution establishing the special Judiciary Committee panel in a vote of 221-211, falling along partisan lines.
“Congress hasn’t kept pace with the federal government’s potential to abuse new technology, and we need to better understand how US intelligence agencies work with each other and with the private sector to collect information on Americans or to undermine their fundamental constitutional rights,” House Majority Leader Steve Scalise said in a statement on the panel.
The subcommittee will investigate how the FBI, Justice Department, Department of Homeland Security and other executive branch agencies obtain information from and provide information to the private sector and other agencies to facilitate actions against US citizens.
The panel will be granted access to information shared with the House Intelligence Committee and the authority to review ongoing criminal investigations. The panel is styled after the Church Committee of 1975, which conducted similar oversight of federal agencies.
House Speaker Kevin McCarthy will name 13 members to the subcommittee, including five Democrats in consultation with Minority Leader Hakeem Jeffries.
A few months after their 16 year old student dies running track, Amherst school superintendent admits they’ll hold a COVID vaccine clinic for students and be paid $2,000 to do so
By Meryl Nass | January 10, 2023
Sacrificing virgins on the altar of the Scientism religion, Amherst MA (population 40,000 but housing 2 colleges and a major university) pledges loyalty to the shot, denying the reality of their own student’s recent death from myocarditis.
The Amherst-Pelham MA school superintendent admitted at a meeting streamed on closed circuit TV tonight that he is putting his students’ lives at risk for thirty pieces of silver.
What is wrong with Amherst, a small city chock full of MDs and PhDs, who are mindlessly going along and increasing their kids’ chance of death? Disclosure: I lived there for ten years. I lectured in the next town 3 days ago.
After losing one high school athlete already to the shot (and the parents of the deceased teenager are an MD and PhD) why aren’t people screaming NO!? What does it take to stop the carnage? If it’s such a great vaccine, why do you need to pay people to take it? The town of Amherst’s COVID vaccine website claims that 91% of the town is fully vaxxed. But the clinics won’t stop, even after everyone knows the darn things don’t work.
According to the NYT and CDC, only 15% of Americans have taken a bivalent booster and only 34% have taken any COVID booster. So a lot of us have figured out the scam. Too bad the good, overeducated people of Amherst haven’t yet.
Alzheimer’s drug approval raises the alarm
Data shows treatment can lead to ‘brain shrinkage’
By Maryanne Demasi, PhD | January 9, 2023
The US Food and Drug Administration (FDA) has granted an accelerated approval of a new treatment for Alzheimer’s disease, which aims to clear toxic amyloid protein build-up in the brain.
At a cost of $26,500 per year in the US (not covered by Medicare or Medicaid), people with early Alzheimer’s disease can receive a twice-monthly monoclonal antibody infusion called lecanemab (marketed as LEQEMBI™), co-developed by Eisai, a Japanese biotech firm, and Biogen.
In the lead up to the FDA’s approval, there was intense lobbying for the drug.
A ‘consensus statement’ signed by over 200 scientists, many of whom had financial ties to the drug companies, described lecanemab as a “foundational gamechanger” for the disease, calling for “no barrier” to the widespread availability of the treatment.
Now that the drug has been approved, advocacy groups like the Alzheimer’s Association, which are heavily funded by the drug industry, have welcomed the news, saying the FDA made “the right decision.”
But critics doubt the benefits of lecanemab outweigh its harms, and are dismayed that the FDA approved the drug without input from its own advisory panel.
Kim Witczak, a drug safety advocate, and member of the FDA’s Psychopharmacologic Drugs Advisory Committee, says she is “shocked” by the latest FDA stunt.
“By approving this new drug without a public advisory committee meeting, the FDA once again has shown a lack of concern for the public, patients, and healthcare providers. Convening its advisory panel would have helped reassure everyone that the FDA’s decision was scientifically sound and transparent,” said Witczak.
“Advisory committee meetings offer the opportunity to discuss the data in an open and public forum, to challenge methods, study endpoints (surrogate vs clinically meaningful), and safety findings before the general committee member discussion. But in this case, none of that was possible,” she added.
The FDA’s accelerated approval process used to green-light lecanemab is known for accepting lower evidentiary standards for drug efficacy, so that patients can gain access to experimental drugs sooner.
Critics say its reminiscent of the FDA’s approval of aducanumab – Biogen’s other Alzheimer’s drug. It was approved on the basis of lowering amyloid protein (a surrogate marker) in the brain, despite no clinically meaningful benefit for patients.
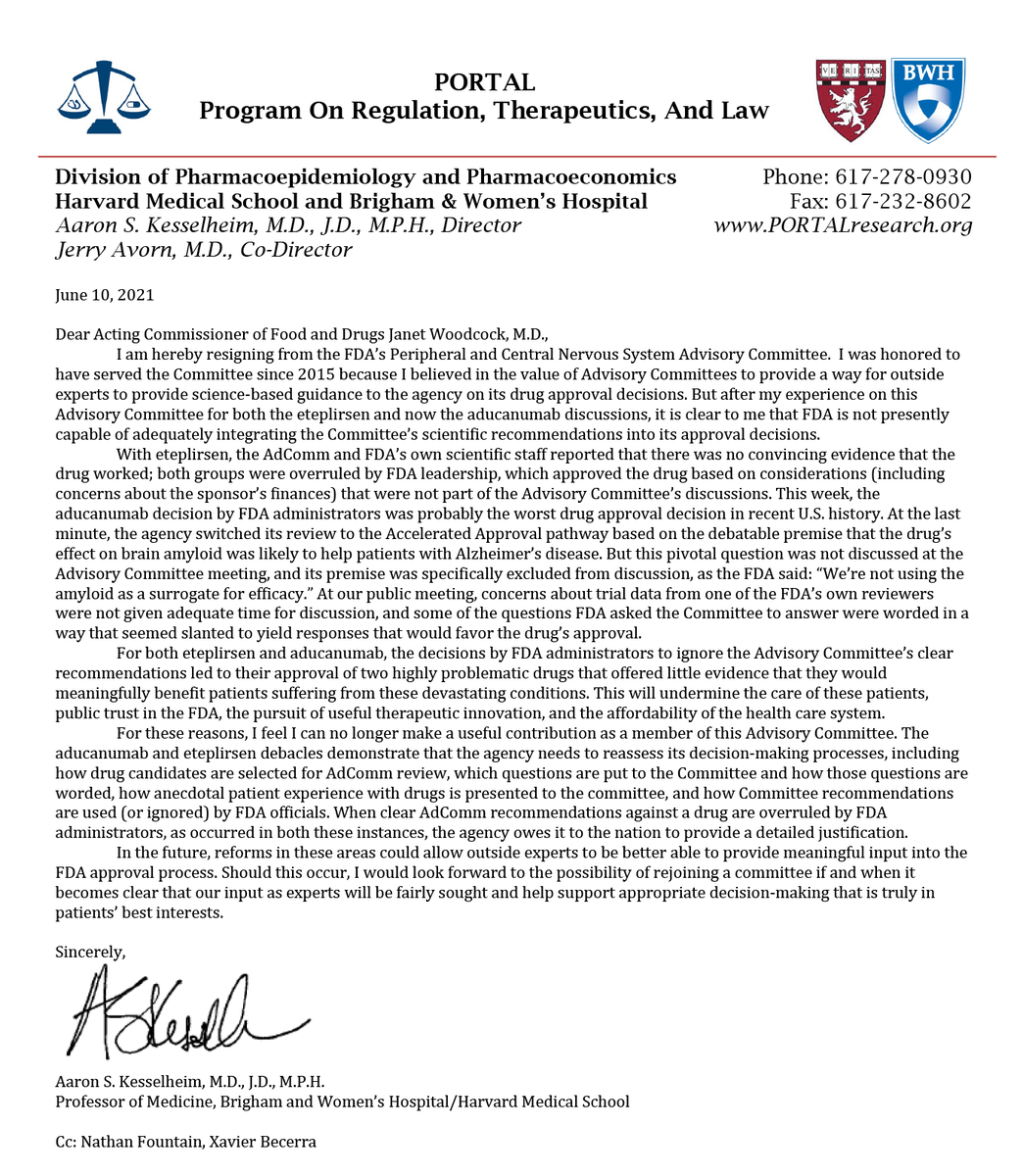
At the time, the controversial decision led to the resignation of FDA advisory member Aaron Kesselheim, who labelled it “probably the worst drug approval decision in recent U.S. history.”
Linda Furlini, a research ethics advisor based in Montreal, Canada says it essentially gives the rubber stamp to similar drugs down the track. “Once you grant accelerated approval of a drug in that class, then it’s easier to get the second drug, and then the third drug approved.”
Jessica Adams, an expert in drug regulatory affairs, agrees. She said, “Lecanemab’s approval shows the power of precedent in regulatory approvals. This is why I scoff whenever the FDA says it still reviews drugs on a case-by-case basis.”
The industry-funded study published in the New England Journal of Medicine, involving almost 1800 people with early Alzheimer’s disease, found that lecanemab could slow the decline of cognition and function by 27% over 18 months compared to placebo.
They used a “Clinical Dementia Rating” scale to show lecanemab patients declined by 1.21 points compared to 1.66 point in the placebo group – a 0.45 point difference in lecanemab’s favour.
But experts question whether the small difference will have any impact on how the patient actually feels.
Madhav Thambisetty, a neurologist at Johns Hopkins University and the National Institute on Aging said, “The benefit appears to be quite small, and it’s unclear how meaningful this might be for patients.”
In fact, the FDA’s own statistician Dr Tristan Massie was uncertain whether “the treatment effect on amyloid is reasonably likely to predict change on the clinical outcome” and considered the results of the study to be “exploratory”.
As a physician who cares for people with Alzheimer’s disease, Thambisetty spoke about the harms of the drug. “These patients can experience headaches, falls, confusion, vision disturbances and it’s unclear if patients will be able to see obvious benefits on a day-to-day basis,” he said.
The data showed an increased risk of brain bleeds and swelling, i.e. amyloid-related imaging abnormalities (ARIA) occurred in 126 (14.0%) of subjects in the lecanemab group and only 69 (7.7%) of subjects in the placebo group.
This prompted the FDA to include a warning on the drug about the risk of swelling and bleeding in the brain.
The drugmakers have also highlighted that people carrying two copies of the APOE4 gene (which predisposes someone to Alzheimer’s) puts them at a particularly “high risk of life-threatening brain haemorrhage.”
Three deaths have been reported in people taking lecanemab; an 80-yr old phase 3 trial participant who suffered intracranial haemorrhage, a 65-yr old who experienced brain swelling and bleeding and a 79-yr old who reportedly had seizures and brain bleed in the open-label phase of the trial.
Two of the three people who died were taking blood thinners, and experts who reviewed the lecanemab death cases suggested that anticoagulant use may have exacerbated the fatal outcomes.
Furlini’s research career has focused on the need to educate and support caregivers of people with dementia-type illnesses.
“You read the list of side effects – you might have gait problems, you might have brain swelling, visual disturbances… I mean, what are we doing here?” asks Furlini, “The patient is already confused and losing their cognitive capacity. How are these serious side effects helping them? It runs counter to any ethical semblance of what is wanted or expected.”
Thambisetty has also expressed concerns about the “brain shrinkage” seen in trial participants taking either lecanemab or aducanumab – increasing doses of the drug correlate to a decrease in brain volume.
“The observation of brain shrinkage is worrisome because, in the absence of compelling evidence to the contrary, it suggests a potential worsening of degenerative changes in the brains of people with Alzheimer’s disease,” wrote Thambisetty in a recent opinion piece for STAT.
The observation has been explained away by researchers who say that a reduced brain volume is due to the clearance of amyloid protein from the brain. But Thambisetty says there is little empirical evidence to support this theory.
Instead, he points to an Australian study which calculated that the clearance of amyloid plaque from the brain was too small to represent a plausible explanation for the loss of brain volume.
US lawmakers launched an investigation into the FDA after the agency’s controversial approval of aducanumab. Last month, a US House of Representatives panel released the report following an 18-month investigation.
The report said the process was “rife with irregularities” and that FDA officials “inappropriately collaborated” with the drugmaker during the approval process which “exceeded the norm in some respects.”
Representatives from the FDA and Biogen engaged in over 100 phone calls or meetings dating back to 2019 in order to expedite the drug’s approval, which lawmakers say, “consisted of atypical procedures and deviated from the agency’s own guidance.”
The congressional report recommended the agency “must take swift action to ensure that its processes for reviewing future Alzheimer’s disease treatments do not lead to the same doubts about the integrity of FDA’s review.”
But critics now say, it’s too late for an agency that has not taken accountability for its actions.
“These drug approvals have just created confusion, uncertainty, fear and misinformation. Then they wonder why people have no trust in their institutions, like the FDA. The world looks to the FDA for leadership. That it does not fulfill its responsibilities, remains the challenge of our times,” said Furlini.
Furlini has followed this area of research for decades and says the drug industry needs to move on from the ‘amyloid theory’ of Alzheimer’s disease and refocus its attention on other causes.
“After so many years, I’m fed up with the exclusive focus on the amyloid theory to the exclusion of other research theories, it’s a disservice to people with Alzheimer’s, and their families,” said Furlini
“There are a lot of buzzwords and marketing propaganda being put out there. And they justify it by saying that you have to give people hope. But you’re giving people false hope. It plays with people’s emotions, which I find horrendous,” added Furlini.
Featured Video
Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
Because no animal reservoir has been found for SARS-CoV-2, it cannot properly be termed a zoonosis.* Should we call it a labnosis? And what does that mean?
By Meryl Nass, MD | July 12, 2021
After a year and a half of seeking but not finding SARS-2 in any wildlife anywhere (apart from domesticated or zoo animals that appear to have caught it from humans) is it time to say, yes, it didn’t just escape from a lab. It was created, built, assembled in a lab. Or many labs
Coronavirus scientists have been constructing new viruses out of bits and pieces of other viruses for a long time.
Why did they do it? … continue
Blog Roll
 Aletho News
Aletho News- The Story the Media — and the Government — Don’t Want You to Hear
- Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
- The Targeted Assassination of Studies Showing Vaccines Cause Injury
- BMJ Probe Into Excess Mortality Study Drags On for Two Years With No Resolution
- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- Strait of Hormuz closed over Israeli aggression on Lebanon
- Keir Starmer arson mysteries multiply
- IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
- Zelensky threatens to attack Belarus
- If Americans Knew
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- Old Iraq war architects rise up against Trump’s Iran deal
- No Tricks Zone
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines

{kind=link}