New Zealand Used Selective Science and Force to Drive High Vaccination Rates
By J.R. Bruning | Brownstone Institute | April 26, 2022
We expect that knowledge produced and applied in a health emergency will produce information that is protective of health. But it is increasingly apparent that over the last two years New Zealand’s Ardern government has designed policy, regulation, and information to coercively steward citizens to accept a drug under provisional consent.
Strict lockdowns were promised to end when 90% of the population was vaccinated. This was unprecedented: policy endpoints required population-level uptake of novel technology, no matter whether the individual was at risk or not.
In addition, data production was contracted by the department intent on a 90% vaccination rate. For decades governments have promoted ‘evidence-based science’ as the gold standard for public reasoning and risk deliberation. What we saw was internally produced and contracted science that focused on case rates, while (inconvenient) information in the published scientific literature on vaccine risk, waning and breakthrough was ignored.
This produced a tightly controlled scope of knowledge production that then failed to adhere to long-established democratic and public health principles. Responsible risk governance requires that governments must be responsive to data that indicates a technology is not as effective or is possibly more harmful than estimated, – for a democratic government’s primary role is the protection and safety of all citizens. Technology must not be valorized, and uncertainty set aside, in order to achieve policy ends.
Universal Vaccination Assumed from April 2021
New Zealand’s Unite Against Covid-19 ‘elimination’ strategy was confirmed in the first quarter of 2020. Policy, propaganda and legislation predominantly centred around the case, or infection rate, rather than the fatality rate as the measure of risk.
Even though the clinical trials did not demonstrate that the vaccine prevented transmission and infection, the Government promoted ‘the jab’ as a way to protect families in the Unite Against Covid-19 campaign. Persistent reporting of case rates fostered a perpetual state of fear and uncertainty among the population, who perceived infection from the SARS-CoV-2 virus to be something more like Ebola.
The Ardern government’s intention for the entire population to get the mRNA vaccine was declared through the signing of a supply agreement. This intention was then embedded in policy and regulation via the Traffic Light system, designed to nudge the population over 12 into compliance.
It was known by July 2021 that the vaccine waned and was leaky. Breakthrough infections were relatively common and for many. The clinical trials remain incomplete, lacking long-term safety data. The trials did not demonstrate that the vaccine prevented hospitalization and death.
However, in April 2022 in New Zealand, mandatory vaccinations remain compulsory for border workers, and workers in health and disability; corrections; defence; Fire and Emergency New Zealand (FENZ) and Police. These professions must be vaccinated and have received a booster vaccination against COVID-19.
At ‘Traffic Light Orange’ Kiwis ‘must wear a face mask’ in retail businesses, on shared and public transport, in government facilities and when visiting a healthcare service. This is despite the fact that Omicron ripped through New Zealand in February.
In the first week back at school and university after the summer holidays –the obedient mask-wearing young friends of my kids, including my son, from Otago and Canterbury down on the South Island up to the capital Wellington and Auckland – were locked down with Omicron in their first weeks back at university. No evaluation of Omicron and mask efficacy has been provided by the state.
The Risk Modellers
Government policy processes have persistently excluded uncomfortable knowledge that suggested uncertainty or risk. First, the policy accompanying and justifying Covid-19 legislation and Orders, and modelling by the contracted institution Te Pūnaha Matatini (TPM) contained narrow reasoning central to the state’s claims, locking in the narrative that infection was the predicator of risk, modelling wave after wave of infection.
Second, policy supporting the legislation excluded consideration of age-stratified risk and failed to address common principles of infectious disease management embedded in the New Zealand Health Act. Third, reviews of the scientific literature that could publicly identify and communicate risk relating to vaccine-related harm and issues relating to efficacy simply never occurred.
The gaps are considerable. The Government’s Covid-19 Unite campaign failed to communicate age-stratified risk of hospitalization and death as the pandemic evolved. New evidence on infection fatality rates were not reported to the public. In modelling papers, TPM used old infection fatality rate statistics that overestimated death rates.
The potential for the vaccine to wane or for breakthrough infection to occur was ignored in a major policy paper focussed on elimination and by the modellers at TPM. The role of natural infection in producing a broader, and protective structural response, assisting populations to shift to herd immunity status was downplayed. While herd immunity was recognized, testing and data modelling was undertaken to identify naturally derived herd immunity in the population. Later modelling exclusively associated herd immunity with vaccination.
Perhaps the problems addressed here are not surprising, when most modelling was undertaken outside of New Zealand’s public health institutions. Instead, number-crunching was carried out by data analysts, mathematicians affiliated with TPM, with scarce few infectious disease epidemiologists trained in public health ethics participating. And of course, the science and data modelling were directly funded by the government departments and Ministries dedicated to over 90% vaccine compliance.
Global vaccination policies ignored the fact that infection-related risk always centered on the aged and infirm and those with complex multimorbid conditions. Disconcertingly, the clinical trial data had conceded that vaccine efficacy remained uncertain for the most at-risk of harm from Covid-19 – the immunocompromised, autoimmune and people who were frail, and those with inflammatory conditions (see p.115). In addition, as coronaviruses readily mutate, it was highly probable the vaccine would have a short shelf life.
Early Treatments Sidelined
Governments are entrusted with an overarching obligation to protect health – this includes putting populations directly at risk through bad policy. There was always a role for safe, established drugs with a long history of safe use that had undergone complete testing before launching onto the market.
Early treatments could have been integrated as a major tool to prevent hospitalisation and death. Early treatments avoid the dilemma of mutating variants while acting to protect at-risk groups whose immune systems might not be as responsive to a vaccine.
Conventionally doctors are at liberty to repurpose drugs for their patients, such as antivirals with a long history of safe use. However, in July 2021, the government locked in approved drugs for treatment.
From at least October, New Zealand doctors were instructed to ‘not use any other antiviral outside of a clinical trial’ while Medsafe warned against use of the safe antiviral Ivermectin for a respiratory virus. Yet the clinical guidelines were intended as last resort medicine for the hospitalized, rather than designed as protective nor preventative at home therapies.
These directives have fractured the practice of informed consent, which forms the basis of trust in the doctor-patient relationships. Even the New Zealand Medical Council, the organisation that grants licences to practice medicine, declared that there was ‘no place for anti-vaccination messages in professional practice.’ These actions may unwittingly undermine trust in vaccines and the doctor-patient relationship for years to come.
The implications of silencing doctors, some who have had their medical licenses suspended, when observed alongside the above-mentioned data gaps, are extraordinary.
Ethical questions continue to be sidelined. The principle of proportionality, embedded in the 1956 Health Act, has been effectively dropped. Proportionality, which allows for individual risk, is a core consideration in public health. Medicine is a technology, and the space where biology meets technology – including medicine – is never constant, and requires value-based judgement. Risk management of a medical intervention for a pregnant woman, young person or child requires significantly different deliberation to a 75-year-old.
Democratically Unaccountable Legislation
Since January 2020, a tsunami of rights-limiting has been rolled out purposefully and consistently. There was scant citizen consultation with public input limited to a few short days in most cases. The unprecedented barrage of rules and orders released by the Ardern government entrenched requirements for almost everybody to get the mRNA vaccine.
By mid-2021 – before most mandates – the scientific literature was revealing that the vaccine waned; that breakthrough infection occurred and that there was extensive evidence that it produced a wide range of side effects, and even death. This knowledge should have invalidated any workforce vaccine mandate, but instead by October, the state doubled down and locked in mandates and regulations that would legally and socially coerce most of the population over 12 into accepting the shot.
It’s probable that the mountain of legislation produced over the last two years never fulfilled democratic norms of accountability and transparency. For science in a pandemic to be harnessed to serve the public interest, the institutions that set those terms of reference must be guided by principles that protect health.
The failure of government agencies to draw on peer-reviewed scientific literature while prioritizing internal modelling is clear from tracking the literature stored online with the relevant agencies. Most compellingly, it is documented in the policy supplied in support of the unprecedented quantity of law-making.
It appears that from late 2019, institutional interests anticipated that there would be hesitancy around vaccine safety. Yet there was no public forum. Instead, groups who sought to question the safety of the novel mRNA vaccine remained outside ‘accredited’ media, possibly due to the chilling effect of unprecedented Covid-19 funding and advertising boosts which effectively captured mainstream media.
That the New Zealand state mandated not-at-risk people accept a novel technology, creating rules (as nudge policies) that limited economic and social life for the non-vaccinated when there was early evidence the vaccine was leaky and potentially harmful, will take years to unpick. As mandates continue, injured groups continue to face barriers to justice following vaccine injury and death.
Ultimately, practices such as this raise nagging doubts concerning the state’s capacity to honor broader obligations to protect health and the public interest in future emergency situations. New Zealand’s response to the Covid-19 pandemic serves as a case study – a precedent, for future health emergencies.
A deeper dive on this discussion can be found in the paper, Covid-19 Emergency Powers and on Rumble. The paper is offered to assist academic and legal experts, citizens and communities to consider use of policy and science by the Ardern Government from 2020-2022. I question the potential for the New Zealand state to navigate future pandemics, and future techno-controversies, in the public interest.
J.R. Bruning is a consultant sociologist (B.Bus.Agribusiness; MA Sociology) based in New Zealand. Her work explores governance cultures, policy and the production of scientific and technical knowledge. Her Master’s thesis explored the ways science policy creates barriers to funding, stymying scientists’ efforts to explore upstream drivers of harm. Bruning is a trustee of Physicians & Scientists for Global Responsibility (PSGR.org.nz). Papers and writing can be found at TalkingRisk.NZ and at JRBruning.Substack.com and at Talking Risk on Rumble.
They just won’t let go of masks
By Guy Hatchard | TCW Defending Freedom | April 26, 2022
The writer is in New Zealand
AS the pandemic fades, should we meekly accept new restrictions or seek new freedoms?
An article in the New Zealand autumn 2022 AA Directions magazine advises that ‘masks are going to be part of our day-to-day lives for the foreseeable future’, and teaches us how to recognise whether someone is smiling behind their mask.
Yesterday in Stuff, science columnist Dr Siouxsie Wiles finally gets around to admitting that ‘you can’t rely on mRNA vaccines’. Her answer? Be stricter about mask wearing.
Dr Wiles, a British microbiologist who received the 2021 New Zealander of the Year Award for pandemic science communication, cites a new study which she says supports continuing use of masks at gatherings. Click on the link (most people don’t) and you arrive at a study that involves theoretical modelling rather than verified effects.
Mask studies (of which there are many) have not demonstrated large reductions in Covid transmission. They tend to be very technical in nature and focus on the comparative viral loads found in nasal and mask swabs. These measurements can be connected to Covid transmission only via theoretical modelling.
Back in the real world, the near universal combination of vaccination and mask wearing to date in New Zealand has not stopped Omicron transmission.
A study published in ClinMed entitled ‘Adverse Effects of Prolonged Mask Use among Healthcare Professionals during Covid-19’surveyed 343 healthcare professionals in New York City hospitals obliged to wear masks throughout most of their working day. They reported: headaches (71 per cent), skin breakdown (50 per cent), and impaired cognition (24 per cent). Yes, you did read that right, one quarter of medical professionals wearing masks suffer decreased intellectual capacity.
Even costly N95 masks do not stop the passage of air around them essentially negating their purpose and prompting the observation that it is like trying to stop mosquitos with chicken wire. Surgical masks or their equivalent are mainly required in hospitals and dirty environments such as sawmills or building sites to protect the wearer from inhaling human tissue or large particulates.
So will Dr Wiles advise us next week to wear a full deep-sea diving suit? In the crazy world of the new subnormal apparently nothing absurd can be ruled out.
Hiding the truth from the public has become a medical imperative
There is a certain hysteria surrounding the realisation that mRNA vaccines don’t actually work and may be harmful. When my kids were growing up we used to read an amusing book to them, Lies My Mother Told Me. How many lies have we been told? Too many.
For example, the Pfizer mRNA vaccine is:
· 95 per cent effective
· Completely safe
· Mostly stays in the upper arm muscle, as most traditional vaccines do
This last is interesting because Pfizer knew before they released the mRNA vaccine that it didn’t stay in the upper arm. They had completed an animal study which suggested that most of the mRNA vaccine spread throughout the body instead of staying at the injection site. The lipid nanoparticles (LNP), which encase the mRNA and help to breach cell walls are highly mobile and ensure that the mRNA spreads rapidly to all the organ systems in the body. If you want the full story see this article by clinical immunologist Dr Byram Bridle.
If we had known this, we would have realised early on that adverse reactions such as liver and kidney damage, strokes, cardiac events, neurological conditions and sudden-onset cancers were not unrelated to vaccination, as many victims were assured at the time by the NZ Ministry of Health, GPs and hospital staff.
Medical professionals assessing the causal connections between mRNA vaccination and subsequent adverse events were relying upon their prior knowledge about traditional vaccines. They thought they knew that vaccine ingredients mostly stayed at the injection site and eventually appeared in lymph nodes as they were cleaned up by the immune system. Pfizer neglected to tell them this was not the case. In fact Pfizer didn’t seem to inform anybody: the damning data was hidden in an obscure study buried in the requirements of the various national regulatory processes supposedly scrutinising safety. Anyone sounding the alarm seemed to be cancelled by the media and relegated to the ranks of conspiracy theorists.
Now that we have some hard NZ data showing that the protective effect of mRNA vaccination is a myth, there appears to be a rush on the part of seasoned and highly decorated Covid science communicators like Dr Siouxsie Wiles, member of the NZ Order of Merit, to throw us a lifeline. We may not actually choose to be saved. We might instead get on with our own lives and make the best of what opportunities we can discover for ourselves. At least we will be rowing our own boat, not sinking in the good ship misinformation.
The Nation’s Top Scientists Lied
By Dr. Scott Atlas | Brownstone Institute | April 13, 2022
This adapted excerpt is from Dr. Scott W. Atlas’ bestselling book, A Plague Upon Our House, published by Bombardier.
CDC Director Robert Redfield’s congressional testimony on September 23, 2020, immediately caught my attention. I watched in disbelief as Redfield told Congress that “more than 90 percent of the population”—more than three hundred million people in the US—remains susceptible to the illness.
The statement was based on incomplete and outdated data, as well as an apparent lack of understanding of the literature, and it struck me as one of the most erroneous and fear-inducing proclamations of any public health official to that moment. Approximately two hundred thousand Americans had already died from COVID; the last thing the public needed was an exaggeration of the future risks, implying to some that ten times that number could still die.
First of all, the numbers didn’t add up. At that point, confirmed cases in the US already totaled approximately seven million, and the CDC itself had estimated that approximately ten times the number of confirmed cases, a very conservative estimate, were likely to have had the infection. A Stanford seropositivity study back in April had shown that confirmed cases underestimated the total infections by a factor of approximately forty times. It made no sense that only 9 percent, or thirty million Americans, had been infected.
Second, the 9 percent calculation was blatantly wrong. That number came from antibody testing by the states. I looked at the CDC website myself, and sure enough, the data was based on antiquated testing from several states.
Some antibody totals were pulled from several months earlier, before many of those states had experienced a significant number of cases. It therefore grossly underestimated the number of cases that had already occurred. The data was simply not valid, but you needed to pay attention to the details.
More importantly, Redfield’s basic claim was fundamentally flawed. The conclusion that serum antibody testing revealed the entire population of those protected from COVID was counter to an entire body of published literature and contrary to fundamental knowledge of immunology, including other coronavirus infections.
It was well known that antibody tests showed one cross-section in time—they were transient—even though immune protection can last. From studies on SARS-2 and most other viruses, antibody levels change over a span of months. They typically appear in the first couple of weeks, peak in a few months, and then decrease over a span of several months.
The literature on COVID had already shown these patterns. A month before this press conference, a Nature Reviews Immunology study on COVID-19 explicitly stated, “The absence of specific antibodies in the serum does not necessarily mean an absence of immune memory,” and explained, “memory B-cells and T-cells may be maintained even if there are not measurable levels of serum antibodies.”
Japan’s study demonstrated this dramatically. In their study, antibody levels increased from 5.8 percent to 46.8 percent over the course of the summer. The most dramatic increase occurred in late June and early July, paralleling the rise in daily confirmed cases within Tokyo, which peaked on August 4.
Out of the 350 individuals who completed both offered tests, 21.4 percent of those who tested negative became positive, and 12.2 percent of initially positive participants became negative for antibodies. A striking 81.1 percent of IgM-antibody-positive cases at first testing became negative in only one month. They stated that “[antibody tests] may significantly underestimate previous COVID-19 infections.” It had also been widely reported in several major scientific journals that antibody responses are not necessarily detectable in all COVID patients, especially those with less severe forms.
But the flaws in Redfield’s estimate extended deeper. Even those familiar with first-year college biology know that other components of the immune system, memory B-cell and T-cells, provide protection from virus infections. Some T-cells kill the virus, and they also help antibodies form. T-cells develop and provide protection that lasts far longer, even after antibodies disappear—sometimes for years in other SARS viruses.
T-cells for this virus had already been documented, even in people unexposed to SARS-2, meaning that in these cases, cross-protection was present from T-cells originating in response to other coronaviruses. T-cells had also been found in individuals with completely asymptomatic SARS-2 infections.
NIH Director Francis Collins had highlighted that very data in his Director’s Blog a few weeks earlier, writing, “In fact, immune cells known as memory T cells also play an important role in the ability of our immune systems to protect us against many viral infections, including—it now appears—COVID-19.”
Scientists from some of the top research institutions in the world, like Sweden’s Karolinska Institute, San Diego’s La Jolla Institute, Duke University, Berlin, and others had published this evidence. Karolinska demonstrated T-cell immunity in both asymptomatic and mild cases of COVID—even if antibody-negative.
Singapore researchers had noted robust T-cell responses to this virus, SARS2, from seventeen-year-old SARS1 samples. Since T-cells are obviously not discovered by antibody tests, those individuals were not included in Redfield’s count. Yet he apparently had not considered this essential, indeed fundamental, point as he testified to Congress and made headlines.
After watching this debacle on TV, I knew full well what was coming later that day. The media would latch on to this and create even more public panic. I also knew that the responsibility for clarifying this grossly erroneous statement would be mine. There was no question it would come up at the president’s press conference, and even if it did not, it still needed to be explained.
I rushed over to Derek Lyons’s office to update him and to make sure we would alert the president beforehand. A few others in the West Wing were there, so I summarized to them what had been said to Congress.
The mood ranged from amazement to dejection to frustration. An advisor to the president on legal matters warned me, with a smile on his face, “Scott, don’t just bluntly say, ‘Redfield is wrong!’ Say something softer, like ‘He misstated things.’”
I nodded, knowing that I needed to restrain my words, even though this was the same man who had tried to destroy me in the national press a few days earlier. But this wasn’t personal at all. Clarifying the facts about the pandemic and countering the unending barrage of misinformation and pseudoscience about it, in this case coming from within the administration itself, was one of my most important roles in this national crisis.
During the pre-brief in the Oval Office a few hours later, I outlined the issue to the president. It was decided, as expected, that I would answer the question when it came up. And so it did.
A reporter from ABC News directly asked me if Redfield’s statement that more than 90 percent of Americans remained susceptible to the disease was true. I took the friendly advice I had received earlier in the day.
“I think that Dr. Redfield misstated something there,” I said, and then did my best to calmly explain the problems with outdated information and the contribution of cross-reactive T-cells and T-cell protection that would not have been included in his data. I correctly stated what was widely known and factual—that the protection from the virus “is not solely determined by the percent of people who have antibodies.” During my answer, as I fended off interruptions, I tried to explain in understandable language as best I could.
I also made a serious effort to be somewhat delicate, because I felt extremely uncomfortable about having to correct the director of the CDC on the national stage.
Unfortunately, my disgust with the confrontational mood in that press room prevented me from being more diplomatic when that reporter asked, “Who are we to believe?” My reflexive answer was “You’re supposed to believe in the science, and I am telling you the science.” Then I referred him to several expert scientists by name. However, I had the strong sense that he was not really interested in the facts at all. Rather, it was another attempt to amplify discord.
After exiting the press room, I walked alongside the president. He briefly stopped to check the news coverage on the set of TV monitors outside the briefing room, as he typically chose to do. After some banter between the president and the staff standing in the area, we began walking back toward the Oval Office.
President Trump turned to me on his right, smiling wryly but with a genuinely puzzled look on his face. “Is Redfield political or just stupid?” he asked, subtly shaking his head. I looked right back at the president and hesitated. The answer was obvious to both of us.
Needless to say, the media immediately played up the disagreement between me and Redfield. It fed into their narrative of conflict between me and the other Task Force doctors, one that Redfield personally caused with his offensive and unwarranted remark that everything I said was “false.”
Later, Dr. Fauci appeared on TV and criticized my straightforward attempt to clarify important information as “extraordinarily inappropriate.” I wondered if he was more concerned with protecting his bureaucrat colleague’s reputation and undermining mine than ensuring that correct information was being told to the American public.
Martin Kulldorff, the world-renowned Harvard epidemiologist, posted his reaction on Twitter: “Scott Atlas stated the simple fact that immunity is higher than those with antibodies, whereupon Dr. Fauci criticizes him without contradicting what was actually said. Stating a simple scientific fact is not ‘extraordinarily inappropriate.’ What is going on?”
Scott W. Atlas, M.D., is the Robert Wesson Senior Fellow in health care policy at the Hoover Institution of Stanford University and a fellow at Hillsdale College’s Academy for Science and Freedom.
Christian Drosten, Karl Lauterbach try to block Health Ministry committee set to evaluate lockdowns and other containment measures

Health minister Karl Lauterbach caught maskless on a train
eugyppius | April 25, 2022
In March 2021, the German Bundestag ordered the Ministry of Health to set up an expert committee to evaluate the effectiveness of containment measures in Germany, from lockdowns to masks. They required this committee to complete their evaluation by 30 June 2022, and to publish a report before the end of September.
The committee finally convened on 22 April via video conference, delayed apparently because communicating with Karl Lauterbach’s ministry has been a huge problem. In the hours after that meeting, the committee chair notified its members that he had finally heard from Lauterbach. The health minister had raised the idea of extending the evaluation deadline to 31 December, and suggested that the committee mandate might end up being redefined.
As Welt explains, Christian Drosten had previously voiced staunch opposition to the project of investigating the efficacy of containment measures:
… [A]n internal virtual meeting in March, Charité virologist Christian Drosten argued against individually evaluating the containment measures. In a nine-minute speech, he said there was too little data, it was too early for such a study, and one could end up “in hot water,” according to WELT information. In view of this intervention from Drosten, who has been one of the most important advisers to political decision-makers since the start of the pandemic, the committee turned to the Ministry of Health for further instructions.
Nothing came of that meeting; the committee had a mandate from the Bundestag, the legal force of which does not rest upon Drosten’s feelings.
When Welt asked the health ministry to comment on the latest delays, a Lauterbach spokesman said the experts don’t have sufficient data, and that the ministry is in discussions with the Bundestag about how to handle this. He even denied that there would be any delay in the committee’s work, which is plainly a lie, because Welt has documents and off-the-record statements from committee members to the opposite effect. One such member even complained to their reporter that “It shows great disrespect to try to withdraw our mandate to evaluate containment measures after so many hours of work.”
We are asked to believe that containment measures have been super successful in the past, and that they remain an important tool for future waves. Lauterbach himself has promised the return of containment in the Fall, because he did not get his vaccine mandate. At the same time, nobody must be permitted to evaluate the efficacy of these allegedly crucial measures. We can’t be allowed to know which ones work and which ones don’t. That would be dangerous somehow, even for an expert committee. In fact it would be so dangerous, that Christian Drosten, the public face of mass containment in Germany, felt compelled to deliver a secret lecture warning against any such evaluative process.
What’s really galling about all this, isn’t that they’re lying, but that they’re terrible at it.
AR6 Model Failure Affirmed: ‘No Model Group Succeeds Reproducing Observed Surface Warming Patterns’
By Kenneth Richard – No Tricks Zone – 25. April 2022
A new study published in Geophysical Research Letters highlights the abysmal model performance manifested in the latest Intergovernmental Panel on Climate Change report (AR6). The 38 CMIP6 general circulation models (GCMs) fail to adequately simulate even the most recent (1980-2021) warming patterns over 60 to 81% of the Earth’s surface.
Dr. Scafetta places particular emphasis on the poor performance of the highly uncertain estimates (somewhere between 1.83 and 5.67°C) of equilibrium climate sensitivity (ECS) and their data-model agreement relative to 1980-2021 global warming patterns.
The worst-performing ECS estimates are the ones projecting 3-4.5°C and 4.5-6°C warming in response to doubled CO2 concentrations (to 560 ppm) plus feedbacks, as the 1980-2021 temperature trends are nowhere close to aligning with these trajectories.
Instead, the projected global warming by 2050 (~2°C relative to 1750) associated with the lowest ECS estimates and implied by the warming observed over the last 40+ years is characterized as “unalarming” even with the most extreme greenhouse gas emissions (no mitigation efforts undertaken) growth rate.
In addition to the conclusion that “no model group succeeds reproducing observed surface warming patterns,” poor modeling of heat transfer physics, ocean and atmospheric circulation patterns, polar sea ice processes… is also evident in the latest IPCC report.
“Accurately reproducing regional temperature differences over the past 40+ years is beyond the capability of climate model simulations, and even fails for major ocean basins and continents.”
The fundamental modeling failures in simulating responses to sharply rising greenhouse gas emissions over the last 40+ years “calls into question model-based attribution of climate responses to anthropogenic forcing.”

When will these vaccine zealots wake up to the truth?
By Guy Hatchard | TCW Defending Freedom | April 24, 2022
WE should not understate the naivety of the government, media and scientists during the pandemic. The tabloid-style stories of severe Covid outcomes, the authoritative voice of Dr Anthony Fauci (who has financial conflicts of interest), the allure of the word vaccine, and the exaggerated death toll in foreign lands all combined into a convincing call for immediate and coercive action. Yet behind the stories, the highly profitable pharmaceutical PR system was running at full steam playing on the fear factor. New Zealand fell head over heels in love. Love knows no reason and that was certainly the case here.
New Zealand is a long way from the rest of the world. We have a tradition of proud independence and self-sufficiency, but we rolled over and played Follow the Leader. No one in a position of influence struck a note of caution, especially not our Prime Minister. We instituted the largest public borrowing programme in our history and spent it on a US mega corporation with a poor safety record and a history of punitive malpractice judgments. The government instituted saturation advertising of vaccine safety and efficacy, and then followed up with mandates, sackings and social exclusion. Our media shouted down those few asking questions.
Times, however, have changed. The respected and conservative Wall Street Journal (WSJ) has aired concerns about poor regulatory decisions at the US Food and Drug Agency (FDA) over booster shots. It joins a growing international chorus of highly qualified and influential voices.
On April 3, in an opinion piece entitled ‘FDA Shuts Out Its Own Experts in Authorising Another Vaccine Booster’, Dr Marty Makary, a surgeon and public policy researcher at Johns Hopkins University School of Medicine, wrote: ‘The FDA last week authorised Americans over 50 to get a fourth Covid vaccine dose. Some of the FDA’s own experts disagreed, but the agency simply ignored them.’
Eric Rubin, editor-in-chief of the New England Journal of Medicine (arguably the world’s most influential medical journal) and a member of the FDA advisory committee on vaccines told CNN last month: ‘I haven’t seen enough data to determine whether anyone needs a fourth dose.’
Dr Cody Meissner, also a member of the FDA vaccine advisory committee and chief of paediatric infectious diseases at Tufts Children’s Hospital in Boston, agreed: ‘The fourth dose is an unanswered question for people with a normal immune system.’
A third member of the committee, Dr Paul Offit of the Children’s Hospital of Philadelphia, went further. He told the Atlantic magazine that he advised his 20-something son to forgo the first booster.
Two top FDA officials, Marion Gruber, Director of the FDA Office of Vaccine Research and Review and her deputy Paul Krause, quit the FDA in September last year complaining of undue pressure to authorise boosters and a lack of data to support their use.
Unbelievably, the US Centers for Disease Control (CDC) rubber-stamped the FDA decision to approve a second booster without even convening its panel of external independent vaccine experts.
The WSJ article described the effect of boosters as fleeting, mild and short-lived. It sounded a note of alarm saying that neither the CDC nor the US National Institutes of Health (NIH) had made a priority of studying vaccine complications. Moreover their VAERS data collection and analysis process is incomplete and inadequate. In other words, the safety investigation to date of adverse effects of mRNA vaccination is incomplete and potentially misleading.
The central question raised by the WSJ opinion piece is, why wouldn’t the US regulators wish to undertake accurate and complete investigation of adverse effects of mRNA vaccination? Have pharmaceutical interests been able to influence decision-making at the FDA to their own commercial advantage at the expense of safety considerations?
The British Medical Journal agrees. On March 16 it published an article which said: ‘Evidence-based medicine has been corrupted by corporate interests, failed regulation and commercialisation of academia.’
The lessons are obvious. We have stifled debate and slavishly followed FDA advice. Now there is a need for revaluation and debate. We have travelled a long way down a one-way street, but it appears to be a dead end. The triumphant articles published about a survey of vaccine-resistant people born in Dunedin was a low point in uncritical mainstream media publishing. We have to regain an objective voice.
A paper published on April 5 in the New England Journal of Medicine found that any measurable protective effect of the fourth inoculation (which in any case, it found, is very small in absolute terms) disappeared after just eight weeks. Moreover a paper in the Lancet on April 8 admitted that boosters carry a risk of additional side-effects. Both these papers, however, skirted the obvious safety questions in favour of weak praise for vaccine orthodoxy.
In contrast the WSJ article asked the important question: ‘Who is actually getting serious about measuring the extent of adverse events, rather than continuing to urge uncritical acceptance of a largely ineffective vaccine?’
So far New Zealand media have steered clear of such questions. Dr Ashley Bloomfield, chief executive of the country’s Health Ministry, has refused to institute mandatory reporting of adverse events following mRNA Covid vaccination and he has excelled at denying vaccine exemptions to those injured by the first shot. Silence is no longer tenable, although in actuality it never was. Questions have to be asked. No ifs or buts. Overseas media outlets of the thinking kind are waking up.
If we can’t face debating rationally with our critics, we are drifting on to the rocks of ignorance and prejudice.
Time for us to wake up.
NEW DATA SHOWS TROUBLING TREND IN VACCINATED
The Highwire with Del Bigtree | April 21, 2022
The Highwire with Del Bigtree | April 21, 2022
Elon Musk’s attempt to buy the social media giant Twitter has sent shockwaves through the mainstream media. Why are they so threatened by free speech?
ELON MUSK BUYING TWITTER
You’ve probably heard that billionaire Tesla-founder Elon Musk is putting together a financial package to become the sole proprietor of Twitter. Having already purchased 10% of the social media giant’s shares, Musk turned down a seat on the board of directors and decided to just buy the whole place.
To be clear, we don’t much like Musk and trust him less. The whole story is likely just another non-issue for people to squabble over.
… that said, you’d have to be made of stone not to take some bitter pleasure in watching the squirming of “liberal” pundits who are suddenly having their own sophistry turned against them.
Remember how those of us concerned about corporate censorship have always been told that “private companies can do what they want” and “if you don’t like, go make your own platform”? Well, apparently those arguments no longer apply.
In fact, according to Robert Reich in the Guardian, “going to another platform” is not an option. Funny that.
Mehdi Hasan rants about Musk’s “problematic free speech escapade” in his latest show, setting up a strawman so large he could burn it and guarantee a bountiful harvest.
The Conversation hosts an article that argues allowing everyone equal room to express themselves is actually bad for free speech because it doesn’t protect “the vulnerable” from harassment.
But the prize for the most-revealing reaction goes to Max Boot of the Washington Post, who said on twitter:
It’s delightful. From the refusal to acknowledge that the paper he works for was only just recently purchased by Jeff Bezos, the second richest man in the world, to the coy euphemism for censorship, all good stuff.
But why is all this happening? And where is it all going?
There are a few ways this could go. For one, the government might step in and stop Musk from buying the company. Protecting social media from becoming a “monopoly”, scoring some points with the “left” for “standing up to billionaires”, and setting a precedent for state interference in private business.
It could be that Musk does buy twitter, and scraps any limitations in line with his “free speech absolutist” claims… but then nation-states will be “forced” to make new rules limiting speech since “irresponsible tech companies refuse to act to stop hate speech” or something along those lines.
Whatever happens, its easy to see how this could further the war on free speech, one way or another. Or maybe nothing will happen at all, and it’s just fun and games.
Why We Sued to Overturn the Federal Travel Mask Mandate — And Why We Won
By Leslie Manookian | The Defender | April 22, 2022
In America, the ends don’t justify the means. There are legal guardrails in place to protect our basic liberties and rights — even during a pandemic.
That was the message in the decision handed down Monday by a federal judge in our lawsuit to overturn the federal travel mask mandate.
Since early 2021, anyone traveling on a plane, bus or train, or anyone who used a shared ride service — or even walked into an airport or train station — was compelled to wear a face covering, often for hours at a time.
President Biden, on his first full day in office, signed an executive order on mandatory masking.
The Centers for Disease Control and Prevention (CDC), citing a public health emergency, promulgated the order just eight days later.
The CDC circumvented a required notice and comment period and issued no scientific justifications for the specifics of the order.
Americans were supposed to take the government’s word for it, put on our masks and ask no questions.
But when flight attendants announced — repeatedly on each flight — that compliance is required “by federal law,” did you ever wonder: what federal law?
I did. And it led us at the Health Freedom Defense Fund to file suit against the mandate in federal court.
With assistance from our lawyers at the Davillier Law Group, we learned there is no “federal law” compelling masks for travel.
The CDC does not have the statutory authority to issue a sweeping mandate requiring masking. Nor does the agency have the authority to penalize Americans for non-compliance.
The Biden administration claimed its mask mandate was rooted in authority granted under the Public Health Service Act.
However, a careful reading of that law shows Congress never intended to grant such sweeping powers. In fact, the law is limited and specific, as the court pointed out in its decision.
One of the bigger red flags for the court was the CDC’s claim it could bypass a period of public notice and comment.
The CDC cited the pandemic “emergency” as justification for bypassing notice and comment.
Yet, as we all recall, by early 2021, the pandemic had been wreaking its havoc for nearly a year, yet the agency had proposed no such travel mask mandate.
It is hard to justify requiring emergency powers and circumventing all citizen comments when the CDC was marking time on masks for more than a year.
Indeed, if a mask mandate was key to the pandemic battle, Congress could have enacted such a bill, with debate, transparency and accountability. It did not.
In fact, public comment is at the core of credible and transparent regulatory policy because it allows for flaws and pitfalls to be cited and hopefully corrected.
Despite telling us all for years to “follow the science,” the CDC cited no scientific research to justify the mandate, nor did it offer justification for choosing the age of 2 for its exemption — clearly indicating the agency arbitrarily chose that age.
An abundance of research in major medical and scientific publications, including in the Journal of the American Medical Association, details the negative effects of prolonged mask-wearing, including among medical professionals and the military.
The CDC also ignored the serious, and medically verified, concerns voiced by Americans about how mask-wearing creates severe anxiety, as the two individual plaintiffs in our case detailed.
Clearly the federal government simply brushed away bona fide questions about mask efficacy and risk, and chose not to cite rationale of its own.
The government’s rationale is what we parents say often when our children question our demands: “Because I said so.”
That approach usually doesn’t work well with kids — and it sure falls short in setting policy for hundreds of millions of Americans.
As our lawsuit pointed out, never has a president entered an executive order mandating that every American citizen be required to don a type of garment or device, whether when traveling or otherwise, for any reason whatsoever.
And the U.S. Constitution certainly doesn’t grant the president power to enact nationwide edicts just because Congress failed to pass legislation he deems needed.
So now that you can choose to fly or ride mask-free, remember: Even in response to a pandemic, your government cannot do what it wants, when it wants and to whom it wants.
We are governed by laws, not the preferences of elites, and the Constitution is not suspended in an emergency.
Leslie Manookian is president and founder of Health Freedom Defense Fund, a nonprofit which seeks to rectify health injustice through education, advocacy and legal challenges to unjust mandates, laws and policies that undermine our health freedoms and human rights.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
How to lie with statistics – Vaccine efficacy edition
The Naked Emperor’s Newsletter | April 23, 2022
Just a quick post to show another method of how to increase vaccine efficacy. This time looking at data from Switzerland and Liechtenstein (S&L).
By mid December 2021, S&L were at the peak of their third wave. It was ok though because 67% of the country had been fully vaccinated, 17% with a booster. 32% of selfish people had still not been vaccinated however.
As the vaccines stop people from going to hospital this would show up in the stats.
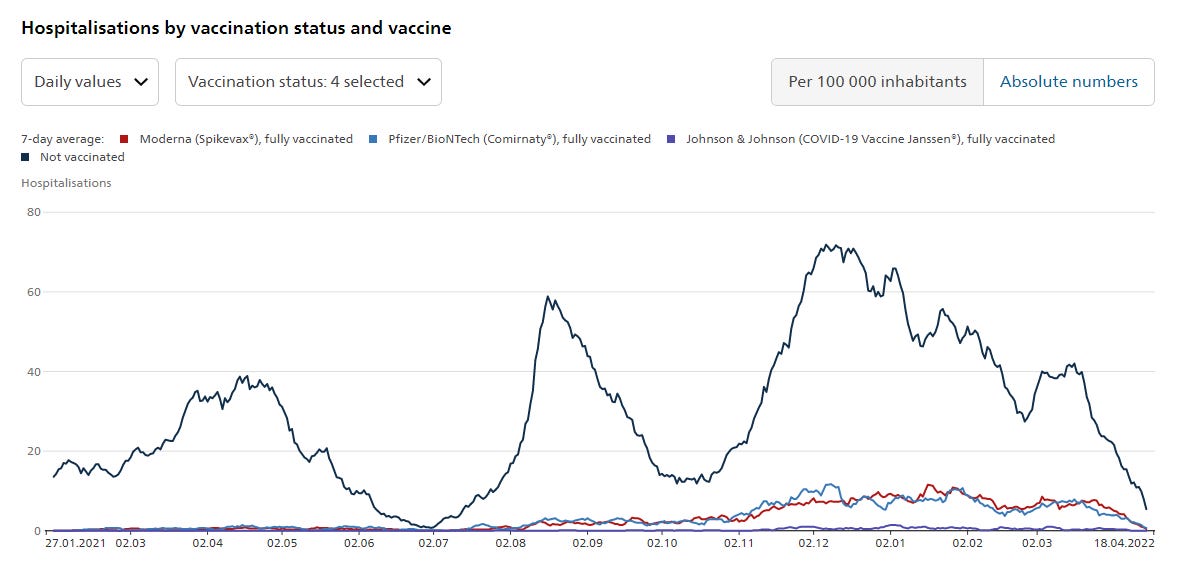
Yes, as predicted, there was a slight increase in hospitalisations for fully vaccinated citizens (Moderna – red line, Pfizer – light blue line) but a massive spike in hospitalisations for those pesky unvaccinated (dark blue line).
Job done, vaccine efficacy proven.
But hold on a second, there is another category. “Vaccine unknown, fully vaccinated”. Let’s add this to the graph.
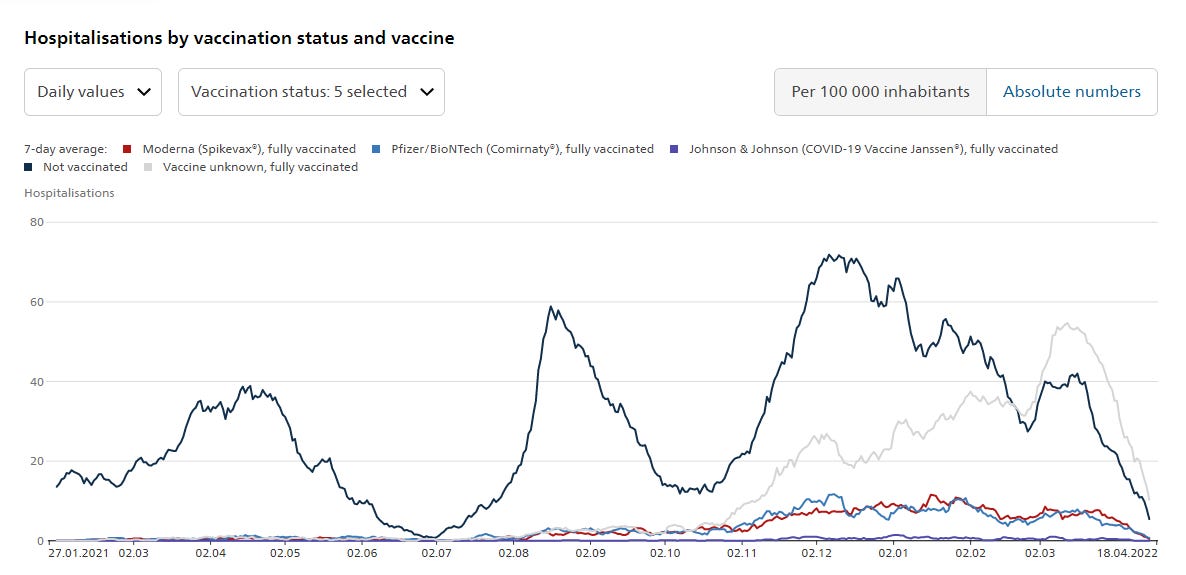
They don’t really want you to see this line so have made it a faint grey colour. However much they would like to pretend it wasn’t there, it is. And it shows a lot of fully vaccinated people going to hospital, and continuing to go to hospital, until March 2022, well after the peak for unvaccinated individuals.
Lot’s of fully vaccinated people going into hospital who have forgotten which vaccines they had. Did they forget or were they too ill? Is this an admin issue or are these people who had a combination of vaccines and so couldn’t be put in one category?
Either way, this grey lined category shifts a lot of people out of the Pfizer and Moderna vaccinated categories. It makes vaccine efficacy look much better than it actually is by saying only this many Pfizer or Moderna vaccinees were hospitalised.
Another great example of how to lie with statistics.
Featured Video
First Photographs Ever Taken of Iran [1848-1858] + Persepolis, Old World
or go to
Aletho News Archives – Video-Images
Book Review
A Palantir Manifesto
By Alan Mosley | The Libertarian Institute | April 22, 2026
Palantir CEO Alex Karp’s book, The Technological Republic, is a clarion call for Silicon Valley to abandon its consumer trinkets and rush headlong into the arms of the military-industrial complex. According to Karp, America’s future depends on wielding hard power through technology—arming soldiers, AI-weaponry, and mass surveillance systems—rather than on the “soft” influence demonstrated by free markets and liberty-first principles. The book claims that “the survival of the American experiment depends on the technological revitalization of the military-industrial complex” and urges the country’s engineering talent to focus on national defense. Karp and his co-author, Nicholas Zamiska, argue that tech bros should “grow up” and start killing America’s enemies before they kill us. … continue
Blog Roll
 Aletho News
Aletho News- The First Photographs Ever Taken of Iran [1848-1858] by Colonel Luigi Pesce + Persepolis, Old World
- Confusion, delusion, and how Israel drives the Iran War
- After the ceasefire illusion: Why Gaza’s “Day After” still has no buyer?
- Shifting to Guerilla Warfare, Hezbollah Delivers Massive Blows to Israel
- Wired for War: Israel’s Black Cube and the infiltration of Europe
- Monitoring group finds UK media guilty of ‘systematic’ dehumanization of Palestinians
- Al-Akhbar’s Amal Khalil assassinated by Israel, left to die under rubble
- US naval blockade has disrupted but ‘not broken’ Iran’s oil exports: Kpler
- On Mass Surveillance, Will the Deep State Win Again?
- Fire breaks out aboard identity-fluid $8bn USS Zumwalt
- If Americans Knew
- Meet the Top “Content” Producers Linked to Canary Mission
- Lebanese Journalist Amal Khalil Bombed and Left to Die by Israel
- Israel Moves to Re-establish Ganim Colony In Jenin
- Two Iranian Women in ICE Detention Are Not, In Fact, Related to Qasem Soleimani, Documents Show
- “The shooting was not in the air”: Testimonies from the Flour Massacre
- Israel chases down, kills Lebanese journalist, massacres 5 in Gaza, all during “ceasefires” – Daily Update
- Gaza’s unseen casualties: A surge in stillbirths and birth defects
- ‘Day of Ordinary Terror’: Israeli Attack on West Bank School Kills Man, Child
- Final Gaza Rapid Damage and Needs Assessment
- Zionist Doxxing Campaigns Upended Their Lives. Now They’re Suing for Damages.
- No Tricks Zone
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
