It has been obvious since early 2020 that there has been an organized cult outreach that has permeated the world as a whole. It’s possible that this formed out of a gigantic error, rooted in a sudden ignorance of cell biology and long experience of public health. It is also possible that a seasonal respiratory virus was deployed by some people as an opportunity to seize power for some other purpose.
Follow the money and influence trails and the latter conclusion is hard to dismiss.
The clues were there early. Even before the WHO declared a pandemic in March 2020 (at least several months behind the actual fact of a pandemic) and before any lockdowns, there were media blitzes talking about the “New Normal” and talk of the “Great Reset” (which was rebranded as “Build Back Better”).
Pharmaceutical companies such as Pfizer, Johnson & Johnson, Moderna, and Astra-Zeneca were actively lobbying governments to buy their vaccines as early as February 2020, supposedly less than a month after the genetic sequence (or partial sequence) was made available by China.
As a person who spent his whole professional career in pharmaceutical and vaccine development, I found the whole concept of going from scratch to a ready-to-use vaccine in a few months simply preposterous.
Something did not add up.
I knew of the names with which everyone has become familiar. Bill Gates, Neil Ferguson, Jeremy Farrar, Anthony Fauci, and others had either been lobbying for or pursuing the lockdown strategies for many years. But still, the scope of the actions seemed too large to even be explained by those names alone.
So, the fundamental questions that I have been asking myself have been why and who? The “Why” seems to always come back to issues besides public health. Of course the “Who” had the obvious players such as the WHO, China, CDC, NIH/NIAID, and various governments but there seemed to be more behind it than that. These players have been connected to the “public health” aspect but that seemed to be only scratching the surface.
I am not an investigative journalist and I would never claim that role, but even I can do some simple internet searches and start to see patterns evolve. The searches that I have done have yielded some very interesting “coincidences.”
If I give you the names of the following people – Biden, Trudeau, Ardern, Merkel, Macron, Draghi, Morrison, Xi Jinping – what do you think that they have in common? Yes, they are all pampered and stumble over themselves, but that is also not the connection.
One can see very quickly that these names certainly connect to lockdown countries and individuals who have ignored their own laws and/or tried in some way to usurp them. But, there is more to it than that and I will give a hint by providing a link with each name.
They are all associated with the World Economic Forum (WEF), a “nonprofit” private organization started (in 1971) and headed by Klaus “You will own nothing and be happy” Schwab and his family. This is a private organization that has no official bearing with any world governance body, despite the implication of the name. It could just as well have been called the “Church of Schwabies.” The WEF was the origin of the “Great Reset” and I would guess that it was the origin of “Build Back Better” (since most of the above names have used that term recently).
If you think that the WEF membership ends with just leaders of countries, here are a few more names:
Allow me to introduce more of the WEF by giving a list of names for the Board of Trustees.
Al Gore, Former WP of the US
Mark Caney, UN Special Envoy for Climate Action
T. Shanmugaratnam, Seminar Minister Singapore
Christine Lagarde, President, European Central Bank
Ngozi Okonja-Iweala, Director General, WTO
Kristalian Georggieva, Managing Director, IMF
Chrystia Freeland, Deputy Minister of Canada
Laurence Fink, CEO, BlackRock
You can see a cross section of political and economic leaders on the board. The leader of the organization, that is the leader of the Board, is still Klaus Schwab. He has built an impressive array of followers.
If you want to really see the extent of influence, go to the website and pick out the corporate name of your choice; there are many to choose from: Abbott Laboratories, Astra-Zeneca, Biogen, Johnson & Johnson, Moderna, Merck, Novartis, Pfizer, Serum Institute of India, BASF, Mayo Clinic, Kaiser Permanente, Bill and Melinda Gates Foundation, Wellcome Trust, Blackrock, CISCO, Dell, Google, Huawei, IBM, Intel, Microsoft, Zoom, Yahoo, Amazon, Airbus, Boeing, Honda, Rakuten, Walmart, UPS, Coca-Cola, UBER, Bank of China. Bank of America. Deutsche Bank, State Bank of India, Royal Bank of Canada, Lloyds Banking, JP Morgan-Chase, Equifax, Goldman-Sachs, Hong Kong Exchanges, Bloomberg, VISA, New York Times, Ontario (Canada) Teacher’s Pension Plan
The extent of reach is huge even beyond the worldwide leader network. For example, we all know what Bill Gates has been doing with his wealth via the Bill and Melinda Gates Foundation (BMGF). But, the Wellcome Trust is equal to the task. Who is the Director of the Wellcome Trust? One named Jeremy Farrar, of the United Kingdom SAGE and lockdown fame – arguably the architect of the US-UK lockdowns in 2020 – is closely associated with WEF.
Concerning the reach that can occur, let me give some examples from the BMGF alone, and it comes from the time that I spent in 2020 reading their extensive funding list.
A few years ago, the BMGF awarded the Institute for Health Metric Evaluation (IHME) a ten-year, almost $280 million award. IHME (associated with the University of Washington in Seattle) was at the forefront of the computer modeling that was driving the lockdowns and the nonpharmaceutical Interventions during 2020. People have seen their name often in print or on MSNBC or CNN.
In 2019, IHME awarded the Editor of the Lancet (Dr. Richard Horton) a $100,000 award and described him as an “activist editor.” The Lancet, once considered one of the best medical journals, has been at the forefront of censoring opposing scientific viewpoints since 2020 and publishing “papers” that were not fit to be published. I never could understand what it meant to be an “activist” editor in a respected scientific/medical journal because, stupid me, I always thought that the first job of the editor was to be impartial. I guess I learned in 2020 how wrong I was.
Of course, the Lancet is also heavily funded from pharmaceutical companies such as Pfizer (also a member of the WEF).
But, the BMGF reach goes far beyond just IHME and these connections have been quite recognizable. Here are some examples of the organizations and moneys received during 2020 alone broken down by areas.
Bill and Melinda Gates Foundation Grants 2020
Organization Name
Amount USD
Johns Hopkins Bloomberg School of Public Health
20+ million
World Health Organization (WHO)
100+ million
Oregon Health Sciences Univ.
15+ million
CDC Foundation
3.5+ million
Imperial College of London
7+ million
Chinese CDC
2+ million
Harvard TH Chan School of Public Health
5+ million
Institute of Health Metric Evaluation (IHME)
28 million (part of a 10 yr/279 million USD grant)
Nigeria CDC
1.1 million
Deutsche Gesellschaft für Internationale Z. (Gmbh)
5+ million
Novartis
7+ million
Lumira Dx UK LTD
37+ million
Serum Institute of India
4+ million
Icosavac
10 million
Novavax
15 million
BBC
2 million
CNN
4 million
Guardian
3+ million
NPR
4 million
Financial Times LTD
0.5 million
National Newspaper Publishers Assoc.
0.75 million
Bill Gates has also invested heavily in Moderna and his investments have paid out nicely for him. The BMGF has also given close to $100 million to the Clinton Health Access Initiative.
The questions now have to be asked:
Is this some beginning of a controlled authoritarian society intertwined via the WEF?
Has the Covid panic been staged to set the stage? Please note, I am not a “Covid Denier” since the virus is real. But, has a normal seasonal respiratory virus been used as an excuse to activate the web?
The next questions, for those of us who at least pretend to live in “Democratic” societies, have to be:
Is this what you expected and/or want from the people you elect?
How many people knew of the “Associations” of the people that they voted for? (I certainly did not know of the associations until I did the searches but maybe I am just out of touch)
Can we anticipate their next moves? There may be some hints.
The Next Move
Jeremy Farrar of The Wellcome Trust recently wrote an article for the WEF with the CEO of Novo Nordisk Foundation, Mads Krogsgaard Thomsen. It is a summary of a larger piece written for and published by the Boston Consulting Group.
In this article, they propose that the way to “fix” the problem of antibiotic resistant bacteria is via a subscription service. That is, you pay a fee and when you need an antibiotic, presumably an effective one will be available for you.
My guess is that they have the same philosophy for vaccines and that certainly seems to be the approach with Coronavirus. Keep paying for and taking boosters.
In view of this philosophy, the vaccine mandates make sense. Get society “addicted” to an intervention, effective or not, and then keep feeding them. This becomes especially effective if you can keep the fear going.
This approach is so shortsighted, from a scientific viewpoint, it astounds me. But, like much of recent history, I think science has little to do with it. The goal is not scientifically founded but control founded.
After the discovery of penicillin almost one century ago, there were scientists who warned that antibiotic usage should be considered very carefully in practice because evolutionary pressures would lead to antibiotic resistant species of bacteria. At that time, they were considered to be rogue scientists; after all, didn’t we suddenly have a miracle cure for many deadly problems?
From the time of discovery, it took over a decade before fermentation methods were developed to produce sufficient quantities of antibiotics to be practical. These methods allowed for the use of penicillin on the battlefield towards the end of WWII and undoubtedly saved many lives then and later in subsequent wars (Korea and Vietnam) by preventing serious infections resulting from wounds sustained during battle.
However, it did not take long before the medical establishment was handing out antibiotics like candy. I experienced this myself when I was a child in the 1960s. It seemed like every time we went to the doctor, no matter what the problem, I was given a series (not just one) of injections of penicillin. There were never any attempts to determine if I had a virus, bacteria, or even an allergy. The answer was: in with the needle. I cannot count how many times I was “jabbed” as a child.
It didn’t take long before resistant species started to appear. The result was that more and more money was pumped into R&D for antibiotics. When I was in graduate school during the 1980s, one sure way to get some NIH funding was to tie the research into the “antibiotic” search. Antibiotics became big business.
We now have several classes of antibiotics that are used for specific cases. We have Aminoglycosides (Streptomycin, Neomycin, etc.), Beta-Lactams Cephalosporins (four generations including Cefadroxil-G1, Cefaclor-G2, Cefotaxime-G3, Cefepime-G4 , Beta-Lactams Penicillins (including Ampicillin, Amoxicillin, and Penicillin), Other Beta-Lactams (Meropenem), Fluoroquinolones (Levofloxacin, Gemifloxicin, etc.), Macrolides (Azithromycin, Clarithromycin, etc.), Sulfonamides (Sulfisoxazole, etc.), Tetracyclines, and others such as Clindamycin and Vancomycin (typically reserved for resistant bacteria). All in all, physicians have over 50 different choices for antibiotics.
The most common place to encounter antibiotic resistant bacteria is in a hospital. Most people who get some sort of infection in the normal routine of life, like a sinus infection or skin infection, will not likely encounter an antibiotic resistant species.
Except there has been another source of the problem and that has been in the food supply. Antibiotics have become very popular with large scale meat production facilities of all types including beef, poultry, swine, and even fish. These include actual farms where the animals are raised as well as in the processing of the meat. The overuse of antibiotics in these industries has also produced resistant forms of bacteria.
For example, in attempts to limit the bacteria e. coli, common to mammalians, antibiotics have been used and this has resulted in some antibiotic resistant forms of e. coli. An infection via e. coli (antibiotic resistant or not) can be avoided by proper cooking and handling of meats. However, sometimes that does not happen and there are e. coli outbreaks (also from improperly washed vegetables that may use contaminated irrigation water).
For most healthy people, experiencing e. coli (either resistant or not) is only a passing discomfort that includes intestinal cramps, diarrhea, and other GI complaints. Depending on the amount of contamination, a person may suffer for a day or two or for several days.
But, with some people, it can be serious or deadly (such as in elderly people in poor health and young children). If that occurs, then the presence of an antibiotic resistant form can be a serious matter. Presence of a non-resistant form can be treated more readily.
A few years ago I had pneumonia; a relatively mild case. I was given a choice of in-patient treatment or out-patient and it was a no-brainer. If I wanted to make sure that my pneumonia could be handled by the normal course of antibiotics (I was given a quinolone), staying at home and away from the hospital was important. I knew that hospital-acquired pneumonia could be a much more serious situation. So, I stayed at home and easily recovered. That did not mean I was guaranteed getting a more serious resistant form in the hospital but I understood that the risk was much greater.
Producing more antibiotics and giving them on subscription to the users is not the answer. That will only lead to more resistant forms and there will be this continuing loop of antibiotic use. But, if the actual goal is societal addiction to antibiotics out of fear, just like addiction to universal Covid vaccines out of fear, then it makes sense.
Finding a few universal antibiotics that deal with the resistant forms is important and it is also important to use those sparingly and only as a last resort. In addition, better management of antibiotic use in our society would go a long way to attenuating the problem.
There is nothing particularly controversial about that observation. It was accepted by nearly every responsible health professional only two years ago. But we live now in different times of extreme experimentation, such as the deployment of world-wide lockdowns for a virus that had a highly focused impact, with catastrophic results for the world.
It was the WEF on March 21, 2020 that assured us “lockdowns can halt the spread of Covid-19.” Today that article, never pulled much less repudiated, stands as probably the most ridiculous and destructive suggestion and prediction of the 21st century. And yet, the WEF is still at it, suggesting that same year that at least lockdowns reduced carbon emissions.
We can easily predict that the WEF’s call for a universal and mandated subscription plan for antibiotics – pushed with the overt intention of shoring up financial capitalization of major drug manufacturers – will meet the same fate: poor health outcomes, more power to entrenched elites, and ever less liberty for the people.
Roger W. Koops holds a Ph.D. in Chemistry from the University of California, Riverside as well as Master and Bachelor degrees from Western Washington University. He worked in the Pharmaceutical and Biotechnology Industry for over 25 years. Before retiring in 2017, he spent 12 years as a Consultant focused on Quality Assurance/Control and issues related to Regulatory Compliance. He has authored or co-authored several papers in the areas of pharmaceutical technology and chemistry.
Below, Dr. Meryl Nass reviews a long list of corrupt practices that undermine the integrity of medical science and the practice of medicine during the current medical crisis. The coronavirus crisis has been made significantly worse by stakeholders who are preventing doctors from prescribing for their patients, existing, safe and effective medicines, because the stakeholders are invested on garnering projected future profits from not-yet-developed vaccines and “countermeasures” specifically developed against COVID-19.
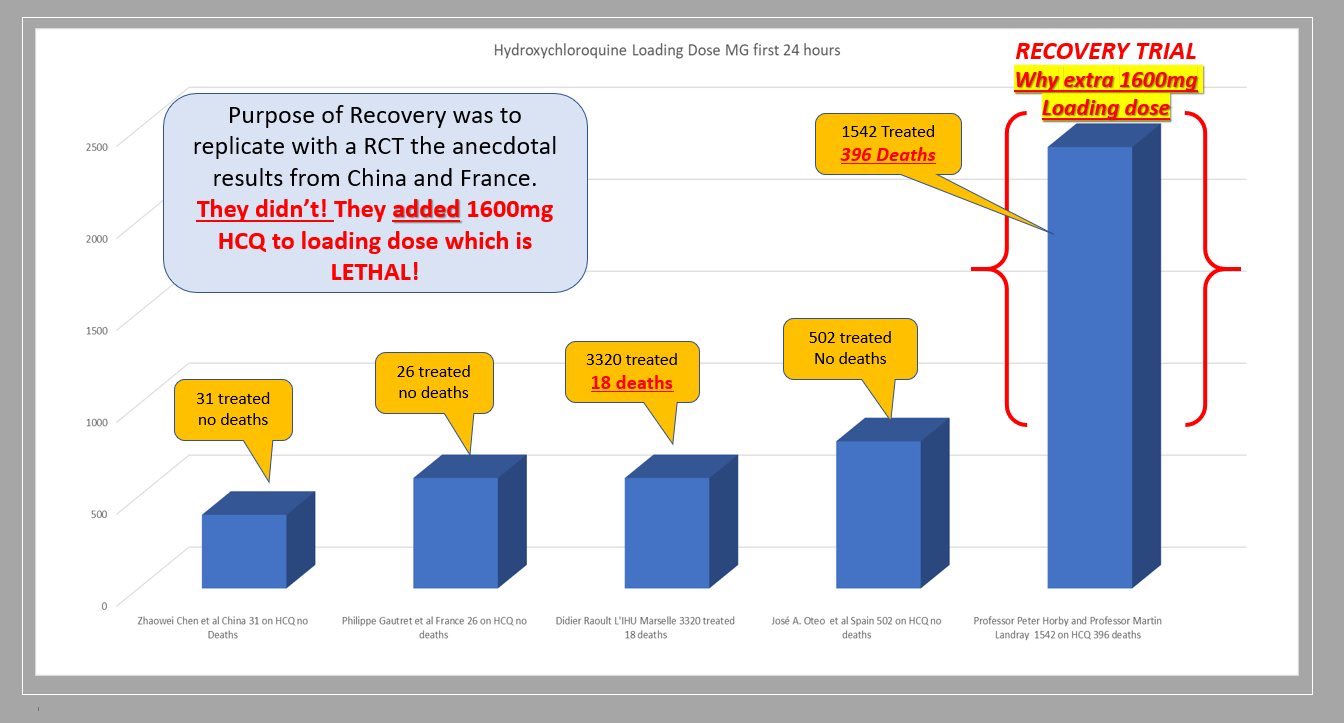
The stakeholders who influence and issue medical practice guidelines, include public health officials, global public health institutions, government advisory committees, and clinical trialists who design trials to provide commercially beneficial results. Editors of prestigious high impact, medical journals contribute to the corruption of medicine by publishing fraudulent studies, and reports of clinical trials that were designed to cause foreseeable deaths, The focus of Dr. Nass’ J’Accuse post are clinical trials that deliberately subjected some patients to toxic doses of Hydroxychloroquine. [Dr. Nass is a longtime member of the AHRP Board of Directors].
These collaborators engaged in an orchestrated effort to prevent physicians from utilizing an existing, off-patent, cheap and affordable drug, that thousands of clinicians attest to its therapeutic benefit.
The problem with Hydroxychloroquine, a drug with a 70-year safety track record, is that there is no profit to be made from this cheap, off-patent drug!
*****************
It is remarkable that a series of events taking place over the past 3 months produced a unified message about hydroxychloroquine, and produced similar policies about the drug in the US, Canada, Australia, NZ and western Europe. The message is that generic, inexpensive hydroxychloroquine is dangerous and should not be used to treat a potentially fatal disease, Covid-19, for which there are no (other) reliable treatments.
Were these acts carefully orchestrated? You decide.
Might these events have been planned to keep the pandemic going? To sell expensive drugs and vaccines to a captive population? Could these acts result in prolonged economic and social hardship, eventually transferring wealth from the middle class to the very rich? Are these events evidence of a conspiracy?
Here is a list of what happened, in no special order. Please help add to this list if you know of additional acts I should include. This will be a living document. I have penned this as if it is the “to do” list of items to be carried out by those who pull the strings. The items on the list have already been carried out. One wonders what else might be on their list, yet to be carried out, for this pandemic.
1. You stop doctors from using the drug in ways it is most likely to be effective (in outpatients at onset of illness). You prohibit use outside of situations you can control.
Situations that were controlled to show no benefit included 3 large, randomized, multi-center clinical trials (Recovery, Solidarity and REMAP-Covid), which are generally believed to yield the most reliable evidence. However, each of them used excessive doses that were known to be toxic; see my previous articles here and here.
2. You prevent or limit use in outpatients by controlling the supply of the drug, using different methods in different countries and states. In NY state, by order of the governor, hydroxychloroquine could only be prescribed for hospitalized patients. France has issued a series of different regulations to limit prescribers from using it. France also changed the drugs’ status from over-the-counter to a drug requiring a prescription.
3. You play up the danger of the drug, emphasizing side effects that are very rare when the drug is used correctly. You make sure everyone has heard about the man who died after consuming hydroxychloroquine in the form of fish tank cleaner.
5. You design clinical trials to give much too high a dose, ensuring the drug will cause harm in some subjects, sufficient to mask any possible beneficial effect. You make sure that dozens of trials in dozens of countries around the world use these dangerous doses.
6. You design clinical trials to collect almost no safety data, so any cause of death due to drug toxicity will be attributed to the disease instead of the drug.
7. You issue rules for use of the drug based on the results of the unethical, overdosing Recovery study.
8. You publish, in the world’s most-read medical journal, the Lancet, an observational study from a huge worldwide database that says use of chloroquine drugs caused significantly increased mortality. You make sure that all major media report on this result. Then 3 European countries announce they will not allow doctors to prescribe the drug. And Sanofi announces it will no longer supply the drug for use with Covid, and will halt its own clinical trials, based on a fabricated study.
9. Even after hundreds of people renounce this observational study due to easily identified fabrications–which, as James Todaro, MD, wrote was a “study out of thin air“–the Lancet held firm for two weeks, serving to muddy the waters about the trial, until finally 3 of its 4 coauthors (but not the journal) retracted the study. You make sure few media report that the data were fabricated and the “study” a fraud. You let people believe the original story: that hydroxychloroquine routinely kills.
10. You ensure federal agencies like FDA and CDC hew to your desired policies. For example, FDA advised use only in hospitalized patients (too late) or in clinical trials (which are limited, are difficult to enroll in, or use excessive doses). As of mid June, FDA now advises patients and doctors to only use the drug in a clinical trial!
11. You make sure to avoid funding/encouraging clinical trials that test drug combinations like hydroxychloroquine with zinc, with azithromycin, or with both, although there is ample clinical evidence that such combinations provide a cumulative benefit to patients.
12. You have federal and UN agencies make false, illogical claims based on models rather than human data. For example, you have the FDA state on June 15 that the dose required to treat Covid is so high it is toxic, after the Recovery and Solidarity trials have been exposed for toxic dosing. This scientific double-speak gives some legal cover to the clinical trials that overdosed their patients.
”Under the assumption that in vivo cellular accumulation is similar to that from the in vitro cell-based assays, the calculated free lung concentrations that would result from the EUA suggested dosing regimens are well below the in vitro EC50/EC90 values, making the antiviral effect against SARS-CoV-2 not likely achievable with the dosing regimens recommended in the EUA. The substantial increase in dosing that would be needed to increase the likelihood of an antiviral effect would not be acceptable due to toxicity concerns.”
13. You have a WHO report claim toxic doses are needed. This of course is nonsense since
Toxicity was noted after only 3 days of treatment, during which 3.6 grams of chloroquine were administered. But the Solidarity (3.2 grams of hydroxychloroquine in 3 days), Recovery (3.6 grams of hydroxychloroquine in 3 days) and REMAP-Covid trials (3.6 grams of hydroxychloroquine in 3 days) continued overdoing patients until June, despite Brazil’s evidence of deaths by overdose.
Tellingly, JAMA editor Gordon Rubenfeld wrote about the Brazilian study, “if you are prescribing HCQ after these JAMA results, do yourself and your defense lawyer a favor. Document in your medical record that you informed the patient of the potential risks of HCQ including sudden death and its benefits (???).”
14. You create an NIH Guideline committee for Covid treatment recommendations, in which 16 members have or had financial entanglements with Gilead, maker of Remdesivir. The members were appointed by the CoChairs. Two of the three CoChairs are themselves financially entangled with Gilead. Are you surprised that their guidelines recommend specifically against the use of hydroxychloroquine and in favor of Remdesivir, and that they deem this the new “standard of care”?
15. You frighten doctors so they don’t prescribe hydroxychloroquine, if prescribing it is even allowed in their jurisdiction, because prescribing outside the “standard of care” leaves them open to malpractice lawsuits. You further tell them (through the FDA) they need to monitor a variety of lab parameters and EKG when using the drug, although this was never advised before, which makes it very difficult to use the drug in outpatients. You have the European Medicines Agency issue similar warnings.
16. You manage to control the conduct of most trials around the world by designing the WHO-managed Solidarity trials, currently conducted in 35 countries. WHO halted hydroxychloroquine clinical trials around the world, twice.
The first time, May 25, WHO claimed it was in response to the (fraudulent) Lancet study.
The second time, June 17, WHO claimed the stop was in response to the Recovery trial results.
Recovery used highly toxic doses of hydroxychloroquine in over 1500 patients, of whom 396 died.
WHO’s trial in over 400 hospitals was unlikely to provide useful results, as it too overdosed patients with hydroxychloroquine. The trial was halted days after the toxic doses were exposed.
21. You convince the public that the crisis will be long-lasting. You have the 2nd richest man in the world, and biggest funder of the WHO, Bill Gates, keep repeating to the media megaphone that we cannot go back to normal until there is a vaccine. (The Gates Foundation helped design the WHO clinical trials, and Gates is heavily invested in pharmaceuticals and vaccines.)
Bill Gates
You have CDC (with help from FDA) prevent the purchase of coronavirus test kits from Germany, China, WHO, etc, and fail to produce a valid test kit themselves. The result was that during January and February, US cases could not be reliably identified, and for several months thereafter insufficient and unreliable test kits made it impossible to track the epidemic and stop the spread.
Yet Dr. Fauci toldUSA Today on February 17 that Americans should worry more about the flu than about coronavirus, the danger of which was “just miniscule.” Then on February 28, Drs. Fauci and Robert Redfield (CDC Director) wrote in the New England Journal :
“… the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
You have social media platforms ban content that does not agree with the desired narrative. As YouTube CEO and ex-wife of Google founder Sergey Brin, Susan Wojcicki said,
“YouTube will ban any content containing medical advice that contradicts World Health Organisation (WHO) coronavirus recommendations. Anything that would go against World Health Organisation recommendations would be a violation of our policy.”
When your clinical trials are criticized for overdosing patients, you have Oxford-affiliated, Wellcome Trust-supported scientists at Mahidol University publish papers (a literature review with modeling and a modeling study) purporting to show that the doses used were not toxic. You develop a new method to measure hydroxychloroquine in a handful of Recovery patients who were not poisoned. However, there are 2 problems you forgot with this approach:
The Brazilian data, including 16 deaths, extensive clinical information and documented ventricular arrhythmias, are much more valuable than theoretical models of what might be happening in the body.
Either the drug is too toxic to use for a life-threatening disease, or even extremely high doses are safe. You can’t have it both ways.
Oxford is the institution running the Recovery trial, and invented a Covid vaccine that already has 400 million doses on order. The Wellcome Trust funded the Recovery trial.
You change your trial’s primary outcome measures after the trials have started, in order to prevent detection of drug-induced deaths (Recovery) or to make your drug appear to have efficacy (NIAID Remdesivir trial).
With every passing day, the list of people suffering tragic consequences from the COVID mRNA shots grows longer. Data1 show 23,149 people have died after a COVID jab as of January 28, 2022. There also are 13,575 reports of people with Bell’s palsy, 41,163 who are permanently disabled, 31,185 with myocarditis, 11,765 who have had heart attacks and 3,903 women who have lost their babies after getting the shots.
Many of these people and their stories have remained hidden from public view. YouTube, Instagram, Facebook and other social media platforms have censored the personal stories and videos of individuals documenting their injuries and permanent disabilities, so those who only read mainstream media are unaware of the overwhelming damage being done in the name of science.
However, there is a population of people whose injuries and death have been made public. In the past six months, a slew of professional and amateur athletes have collapsed and died on the field. Yet, mainstream media appear to take this in stride, acting as if what is happening is completely normal.
But, as described by Matt Le Tissier in the first seconds of the video above, this is far from normal. Le Tissier was a soccer legend2 (a sport called football in the U.K.). His prowess on the field earned him the nickname “Le God”3 before leaving the sport to become a sports commentator, most recently with Sky Sports.
As he describes in the interview, he lost that job for speaking out and bringing attention to the large number of unexplained sudden cardiac deaths happening to professional and amateur athletes around the world.
Athletes Are Dying on the Field in Large Numbers
Red Voice Media asks in a headline, “400 Athletes Collapsing & Dying Just in the Last 6 Months?”4 then mentions “small stories coming out about perfectly healthy athletes mysteriously dying.” During the interview, Le Tissier is asked about his thoughts on the surge of cardiac events in the sporting world, to which he responds:5
“I’ve never seen anything like it. I played for 17 years. I don’t think I saw one person in 17 years have to come off the football pitch with breathing difficulties, clutching their heart, heart problems …
The last year, it’s just been unbelievable how many people, not just footballers but sports people in general, tennis players, cricketers, basketball players, just how many are just keeling over. And at some point, surely you have to say this isn’t right, this needs to be investigated.”
Le Tissier acknowledges there may be other factors that have caused this massive rise in cardiac events in athletes. He mentions that the athletes may have had COVID, and this could be a consequence of the illness, or it could be the vaccine. But the point he makes is that it should be investigated and it’s not.
This may cause you to wonder why health experts are not placing blame on the infection, but are in fact ignoring the issue completely. It begs the question: Do they already know the answer?
Le Tissier goes on to talk about player safety and how the sport protects the players from playing too long or too many games, yet they are watching players collapse on the field and apparently are content acting as if this is normal. He calls it a “massive dereliction of duty” that no one in a position of power is calling for an investigation.6
“It’s absolutely disgusting that they can sit there and do nothing about the increase in the amount of sports people who are collapsing on the field of play. And it’s not just what I’ve noticed this season as well. Again, in my career, I don’t remember a single game being halted because of an emergency in the crowd, a medical emergency in the crowd …
I would like somebody to look into that and go well, hang on a minute, can we go back for the last 15 or 20 years and … have a look and see how many times it happened 10 years ago and then how many times it happened in the last year. I’ve been watching a lot of sports and a lot of reports on football, and I’ve never seen anything like it, the amount of games that have been interrupted because of emergencies in the crowd.”
The interviewer pointed out that correlation does not necessarily mean causation, to which Le Tissier agreed, but stressed that an investigation is required to find out if it does. “To my naked eye, this is happening a lot more than it has in the past. I can’t be the only one who is seeing this.”7
FOLLOWING the decision to roll-out Covid vaccines to healthy children aged 5-11 from April, the Children’s Covid Vaccine Advisory Group (CCVAG), comprising a wide range of senior health professionals, have issued a statement urging an immediate halt to the policy.
Dr Ros Jones, chairwoman of the CCVAG, said: ‘Why are the governments of the four nations announcing a rollout of Covid vaccines to healthy children aged 5-11 when they still have not answered urgent questions about safety in 12-17-year-olds?
‘Presumably this “offer” is being made on a “non-urgent” basis because the government has not finished its investigation into the growing evidence of harms to children.
‘This has never been a more urgent matter. We must halt the vaccine roll out while further investigations take place.’
Since yesterday morning, more than 300 healthcare professionals have co-signed a letter to the government and its advisers, in a growing critique of policy by Britain’s medical establishment.
The letter, which you can read here with the full list of signatories, calls for an immediate halt to the UK Covid vaccine roll-out to children to allow time for a thorough investigation.
Data from Hong Kong shows the myocarditis (heart inflammation) risk to teenage boys as high as 1 in 2,680, and they have ceased giving a 2nd dose. ONS figures for the UK have shown a significant rise in non-Covid deaths, representing at least two young men aged 15-19 dying each week, the cause of which has yet to be investigated and correlating with the vaccine roll-out.
The CCVAG says: ‘Vaccinating children is all risk and no benefit. Yet governments are recommending vaccinating healthy 5-11s, most of whom have already had SARS-CoV-2 infection, providing excellent natural immunity.’
About the CCVAG
The Children’s Covid Vaccine Advisory Group comprises a wide number of health professionals and scientists including several of the country’s leading professors in medicine, microbiology and risk, as well as specialists in public health, emergency medicine, paediatrics, infectious disease and primary care.
Once the world’s sixth largest firm with a valuation of over $1 trillion, Facebook’s parent company Meta finished Thursday’s trading with a value of $565 billion. According to data compiled by Bloomberg, the social media giant has tumbled out of the world’s 10 largest companies by market value, hammered by its worst monthly stock decline ever.
The stock rout has placed Mark Zuckerberg’s company in 11th place behind Chinese Tencent Holdings. Chip giant Taiwan Semiconductor Manufacturing Company (TSMC) holds the ninth spot. The list of the world’s most-valuable companies, ranked by market capitalization, includes Apple, Microsoft, Aramco, Alphabet, Amazon, Tesla, Berkshire Hathaway, and Nvidia.
Data shows that the value wiped out by the selloff in Meta’s shares exceeds the market caps of all but eight companies in the S&P 500 Index. Meta’s share price is down about 40% year-to-date after the company reported two weeks ago that its social media platform Facebook lost about one million users from the third quarter to the fourth quarter of 2021. That’s the first such decline for the company in its 18-year history.
Meta’s stock plummeted 26.4% on February 3 after the company released its weaker-than-expected outlook. The $240 billion loss in market capitalization was the largest one-day loss in US corporate history. CEO Mark Zuckerberg’s personal net worth is down more than $46 billion from the beginning of the year, he’s currently worth $78.8 billion.
Since then, Meta’s share price has extended losses, losing another 13% to date. The company has warned that the rest of the year is shaping up to be a choppy one as it deals with “macroeconomic challenges” and continues its long-term strategic shift “towards building the metaverse.”
While all eyes have been on Canada, there also have been massive Freedom Convoys, and joyous multitudes applauding them, and turning out to help them, all around the world. We’re seeing it (despite the usual blackout by the quisling media) in Australia, where 1.4 million vehicles, and between one and two million protestors, have taken over Canberra, Australia’s capital, the people calling for an end to all restrictions, and the ouster of that once-free country’s quisling politicians. There, too, the biggest protest in that nation’s history has been just as peaceful as it is diverse—a wondrous mass display of solidarity, to re-assert our fundamental human rights, spontaneously led by many thousands of real workers.
So where’s “the left”? Australia’s “left” is on the other side—just like “the left” in the United States and Canada, there being no diversity among them, as they’re all one in their boiling hatred of that mass resistance, and in fanatical support of the state/corporate juggernaut coercing universal “vaccination.” So, on this unprecedented global confrontation, there is no disagreement whatsoever between US “leftists” like Noam Chomsky (the first public figure to propose detention of the “unvaccinated), Amy Goodman, Michael Moore (“Get off my fucking bridge!”), Chris Hedges, Thom Hartmann, the Trotskyites at WSWS, Sen. Bernie Sanders and Stalinist noisemaker Bob Avakian, the liberals at MoveOn, and many of the “woke” contributors to Truthout, Nation of Change, Truthdig, Counterpunch, Portside, the Progressive and The Nation. Nor, on this working-class resistance to the bio-fascist order, is the fearfully like-minded US “left” in any disagreement with its counterpart in Canada, typified by Naomi Klein (who deems the Great Reset a “boring” topic), Henry A. Giroux (who says the truckers are attempting to destroy democracy), “woke” neo-Nazi Justin Trudeau (whose government trained Ukraine’s feral National Guard), and the sanctimonious rabble of Canada’s “left” parties (and let’s throw Neil Young in there, too); so that “the left” throughout all North America is absolutely unified against the workers.
And so is the Australian “left,” as the doggedly Marxist Red Fire demonstrates in “Straw Man: ‘Fascism’ in the Freedom Movement,” a devastating piece out just today, nailing the Socialist Equality Party (SEP), Socialist Alternative (SAlt), Solidarity, the Australian Council of Trade Unions (ACTU), the Trostkyist Platform (TP), the Communist Workers Party of Australia (CWPA), the Communist Party of Australia (CPA) and the Socialist Alliance (SA) for their hostility to the assembly in Canberra—a multitude “largely middle-aged and Anglo-European,” as SA’s Green Left Weekly airily (and inaccurately) sneers. While it’s hard to picture Julian Assange condemning the protesters in his country (what they’ve done to him is what they also plan to do, eventually, to every COVID dissident), it’s even harder to hear Caitlin Johnstone’s voice amid the protest in Australia—since she’s written nothing on what’s happening in her country (though she lives in Melbourne, right under Dan Andrews’ iron heel).
Red Fire admirably nails what’s happening everywhere:
Despite the largest political movement in modern history consistently mobilising against government repression which is a clear move to replace liberal democracy with fascism, the Covid left (formerly the lockdown left) have instead decided to double and triple down on their abject betrayal of the working class. As we have previously argued, the treachery of the ostensible left parties on Covid surpasses that of August 4, 1914. At that time, virtually all “socialist” parties the world over backed “their own” ruling class and marched into the slaughter of the first World War.[6] Today the Covid left, from the very start of the civil war launched by big finance capital, have aggressively sided with “their own” imperialism while having the temerity to lambaste millions of working and oppressed people as “far-right” or “fascist” for mobilising against Covid fascism.
Thus “the left” has finally moved beyond the fatal splintering tendency that paralyzed the (real) left from the days of Marx and Engels through the Sixties and Seventies (when such splintering was deftly aggravated by the FBI and CIA and their affiliates worldwide). Whereas such total solidarity was once envisioned as the surest means of liberating all the “workers of the world,” this “left” has come to it at last by squaring off against the working class— and so against the rest of us as well.
And so it’s time now for the rest of us to recognize that this “left” is itself the enemy it used to warn against—a “left” that hates the working class, and wants to see its independence smashed, its peaceful protests halted everywhere, whatever that may take, so that those “far right” truckers stop insisting on their “freedom,” get their boosters and go back to work, delivering the goods that “leftists” need from Amazon. Thus this “left” is on exactly the same page as John D. Rockefeller when he had the miners massacred in Ludlow, Colorado in 1914, and as Leon Trotsky when his troops crushed the Kronstadt insurrection in 1921. To put the case in a more timely way, this “left” wants to see the working class throughout the West controlled as tightly as it is in China, where there are no strikes or labor unions, guns are not allowed, everyone is always under absolute surveillance, and dissidence is likely to be punished with financial strangulation, as Justin Trudeau is now trying to starve the truckers into silence, in collusion with GoFundMe and the banks—a fascist combination that this fascist “left” applauds, to its eternal shame.
So let’s agree that this “left” has to go, along with all the predatory players that it now serves with such unprecedented unity and livid zeal. And as we call it out for what it really is, let’s also stop dividing We the People into “left” and “right,” because those terms are finally meaningless in this apocalyptic fight, in which you’re either on the side of right, or in the wrong.
Project Veritas published Part Two of its series on the FDA on Wednesday night which featured FDA Executive Officer, Christopher Cole, speaking about the inner workings of the agency including the FDA’s conflicts of interest, overspending, and why it’s hard for those within the agency to speak out on such abuses.
In the footage, Cole talks about the impact that pharmaceutical companies have on the agency including the process for approving drugs.
“A long time ago, Congress approved user fees for [the] FDA. Basically, we charge the industry millions of dollars in order to hire more drug reviewers and vaccine reviewers, which will speed up the approval process, so they make more money,” Cole says in the hidden camera footage.
He then reveals that the FDA tones down the impact that these user fees have on the agency’s operations because, “they’re dependent on the drug companies, and the vaccine companies and these other companies for their agency to operate.”
The incendiary footage, which features Cole talking about how the additional money the FDA brings in “gets banked” to be spent on “whatever you can, whether it’s right or wrong,’’ also features Cole discussing reasons why it’s difficult for anyone in government to speak out about practices he sees as “probably excessive.”
“I don’t think there’s enough people saying they’re, like, ‘Look, that’s fine, but that’s not right. So, we’re not going to charge that.’ You don’t want to be that person. You’re not going to have a long shelf life in the agency if you’re always that person,” Cole said.
“There’s not an incentive to speak out in government, surprisingly. You would think there would be, but there’s not. It’s better just to just not say anything and just ignore it. The whistleblower, well, it’s high-profile whistleblower statutes and everything, that’s kind of ridiculous,” Cole said before adding “it’s better to just stay quiet and accept.”
Cole’s LinkedIn page lists him as an Executive Officer within the agency’s Countermeasures Initiatives, which plays a critical role in ensuring that drugs, vaccines, and other measures to counter infectious diseases and viruses are safe. He made these revelations on a hidden camera to an undercover Project Veritas reporter.
A spokesperson for FDA issued a statement yesterday saying, “The person purportedly in the video does not work on vaccine matters and does not represent the views of the FDA.”
This statement appears to contradict a phone call released Wednesday afternoon by Project Veritas wherein Cole reiterated, during the conversation with Project Veritas Founder and CEO, James O’Keefe, that he is “a manager in the office that helps oversee the approval of the COVID vaccines for emergency approval.”
YouTube, the world’s dominant video sharing platform, has already removed over one million videos for violating its strict and controversial “misinformation” rules. But in a new announcement, the tech giant has revealed that it’s going to be getting even stricter and suppressing “new misinformation” preemptively before it has the chance to gain traction.
YouTube’s Chief Product Officer Neal Mohan described how the video-sharing platform will start “catching new misinformation before it goes viral” in a blog post. The process will involve continuously training YouTube’s machine learning systems with “an even more targeted mix of classifiers, keywords in additional languages, and information from regional analysts” to identify “narratives” that YouTube’s main classifier doesn’t catch.
Mohan added: “Over time, this will make us faster and more accurate at catching these viral misinfo narratives.”
When YouTube does catch what it calls “viral misinfo narratives,” it will reduce the reach of some videos and push viewers towards “authoritative” videos (videos from brands, mainstream media outlets, and health authorities that YouTube has deemed to be authoritative) in search and recommendations.
For topics where there’s no authoritative content, YouTube is considering using news panels being developed (which direct viewers to text articles for major news events), “fact check” boxes (which direct viewers to content from fact-checkers), and new types of labels that add “a disclaimer warning viewers there’s a lack of high quality information.”
However, YouTube has yet to finalize how these labels will work because “surfacing a label could unintentionally put a spotlight on a topic that might not otherwise gain traction.”
Mohan justified these new censorship measures by claiming that “the fresher the misinfo, the fewer examples we have to train our systems” and noted that new narratives often “quickly crop up and gain views.” He added: “Narratives can slide from one topic to another—for example, some general wellness content can lead to vaccine hesitancy.”
YouTube has been proactively targeting “emerging” misinformation since at least 2020 via its “Intelligence Desk.” The Intelligence Desk initiative launched in 2018 to proactively police “inappropriate or offensive content” and in a 2020 interview, Mohan revealed that it was also being used to look “over the horizon” and “stay ahead of” emerging “conspiracy” and misinformation content before it “becomes a challenge” on YouTube.
In this essay, I explain in simple terms why The Great Reset concept of the WEF (which not only includes a large climate change component but is also linked to Covid-19 restrictions) is conceptually unsound but so dangerous that it sparked a Canadian uprising that is spreading around the world.
Ottawa, Canada. 11 February 2022. Donna Laframboise, BigPicNews.
The World Economic Forum (WEF) held a special virtual meeting in early June 2020 to announce the publication of a book written by Klaus Schwab and Thierry Malleret that laid out a grand manifesto called ‘Covid-19: The Great Reset’. This is what Schwab had to say:
We can emerge from this crisis a better world, if we act quickly and jointly. The changes we have already seen in response to COVID-19 prove that a reset of our economic and social foundations is possible. This is our best chance to instigate stakeholder capitalism – and here’s how it can be achieved.
Schwab and the WEF have promoted the concept of ‘stakeholder capitalism’ for decades but it appears that very early in the pandemic he saw the Covid-19 crisis as a perfect opportunity to implement his vision sooner rather than later. This was a red flag for me because it mirrored the actions of David Attenborough that I’d been documenting for my book, Fallen Icon: Sir David Attenborough and the Walrus Deception. Attenborough saw the shocking film footage of walrus falling to their deaths presented in the Netflix/WWF extravaganza Our Planet as the leverage he needed to kick-start an aggressive campaign to promote action on climate change and curb capitalism.
The topics may seem unrelated but statements made by Attenborough last year were barely distinguishable from those made by the Duke of Edinburgh (Prince Charles) in his support of the WEF’s plan for a total revamping of society. While some have dismissed The Great Reset as a conspiracy theory, the concept is very real but esoteric enough to invite wide interpretation.
Worryingly, as critic Justin Honse has pointed out, the WEF has not been forthcoming about the fact that the stakeholder capitalism idea is “not exactly compatible with democracy”. In addition, it’s easy to see that their aim of having huge societal changes fully implemented by 2030 – a scant eight years from now – would cause concern.
I have read Schwab and Malleret’s book. Contrary to my expectations, I did not find it to be a totally irrational rant. However, three core concepts upon which The Great Reset rests are undeniably false, which renders the manifesto invalid and the proposed ‘solutions’ colossally inappropriate as well as unnecessary:
That “… there is nothing new about the confinement and lockdowns imposed upon much of the world to manage Covid-19. They have been common practice for centuries.” (pg. 13)
False: Chinese-style lockdowns of millions of healthy citizens are not the same thing as localized quarantines of sick people and their contacts used in modern times to control epidemics.
That all previous pandemics were followed by a total reorganization of society. (pg. 13-15, and 38)
False: a reorganization of society after a pandemic has not happened since the ‘Black Death’ bubonic plague in the 1300s.
That future climate catastrophes – but especially ‘extreme weather’ – are inevitable unless extraordinary measures are taken to reduce emissions of CO2. (pg. 25, 141)
False: there is no plausible evidence that ‘extreme weather’ has increased in recent years, despite groundless statements to the contrary. Outputs from modelling regarding possible future conditions are not scientific facts and are based on assumptions that may not be correct.
Since these core concepts are false, The Great Reset and all the societal changes it calls for can be dismissed as ideological drivel. But the ideas are dangerous nevertheless because a large number of very rich and powerful people have bought into the plan. Attenborough and Prince Charles are only two of them: there are many others.
When Attenborough said to the WEF in January 2019, regarding his Netflix ‘Our Planet’ documentary, “If people can truly understand what is at stake, I believe they will give permission to business and governments to get on with the practical solutions,” he implied that democratic votes would be involved.
However, it is easy to see how many people would interpret ‘The Great Reset’ manifesto as a grand plan to circumvent democracy.
In part, this is because they have seen how easy it was for governments around the world to use hastily-declared public health emergency powers to enforce drastic restrictions on people’s movements and their ability to make a living, including the imposition of vaccine passports that pave the way toward more generalized digital ID systems. It doesn’t take much imagination to realize that similar legislation might be enacted to deal with a perceived climate change ‘emergency’.
This seems like a reasonable concern to me, especially when activists have already been insisting governments declare a climate emergency, which many governments have already agreed to do.
It is apparent that Schwab and his supporters realized by April 2020 that mandating the most rigid restrictions imaginable on people’s lives was not only possible in democratic countries but much easier than they anticipated – provided that populations were sufficiently frightened by coordinated media reports and government announcements.
When people around the world submitted with virtually no resistance to lockdowns imposed to protect their lives, it appeared that Schwab and his confederates assumed those same people would readily submit to mandated, communist-style restriction on their freedom to mitigate climate change since it would also be for their own good. However, convincing people that a climate emergency would require acquiescence with even more draconian regulations might be a more difficult challenge. Insisting on 100% compliance with vaccine passports and mask wearing now might make compliance with climate emergency measures and other social changes easier a few years down the line.
Vaccine passports have been defended by many as a necessary mitigation strategy to reduce illness while others have more honestly admitted they are simply a way to coerce the unvaccinated to submit. However, now that it’s apparent that none of the Covid-19 vaccines prevent infection or transmission, many people are interpreting continued insistence on vaccine passports as irrational and dangerous. They are starting to wonder if this is a ploy by governments to advance Great Reset ideology by stealth. Others simply see the danger in governments having so much power to restrict people’s lives.
And now, the assumption that people will continue to comply with mandates and restrictions has hit a giant roadblock – quite literally. A few weeks ago, working class people across Canada said they’d had enough of Covid-19 mandates and backed up their convictions with strategically parked big-rig trucks, farm tractors, and other vehicles. They amassed an astonishing amount of support very quickly, proving it was not a fringe minority opinion.
After three weeks of massive disruption across the country, the truckers continue to insist they will not stop their protests until all mandates and restrictions are lifted: Prime Minister Justin Trudeau has steadfastly refused to do so, resorting instead to deriding and slandering the protesters. This week, he invoked Canada’s Emergencies Act to quell the peaceful protests even though the act was never intended for this purpose. Under this authority, Trudeau has threatened every Canadian who donated even $10 to support the peaceful truckers protest with freezing their bank accounts.
No wonder the Canadian truckers Freedom Convoy has inspired citizens in other countries such as Australia and France to rise up and fight back against tyrannical ‘health’ restrictions: they understand now that it’s not about Covid-19 anymore.
IT gives me no pleasure to be the fortnightly bearer of bad tidings. It gives me even less pleasure to know that TCW Defending Freedom has been the only media outlet since last July to have regularly published MHRA Yellow Card reports – the records of adverse effects from the Covid vaccines.
We commission a detailed and professional analysis of the data each time, so that we can properly track the consequences of the jabs – including the rising list of fatalities – and freely pass on the information to our readers.
We believe it remains vital that we keep the data accessible in the public domain, with the details that most people would neither be able to find or calculate on their own.
The Yellow Card headlines this week are that deaths have topped 2,000 and now stand at 2,010.
The percentage of reactions to injections stands at one in 118, up from the one in 123 recorded before Christmas.
Reported cases of myocarditis (heart muscle inflammation) are significantly up again, now at 1,941. This compares with 1,362 reported by the beginning of December.
This last development is worrying indeed. First, because of the unexplained excess young male deaths last year that the Government now acknowledges, as Dr Ros Jones reported in TCW yesterday. Second, because it is now well-established that the likelihood of this reaction in young men is higher than their risk of myocarditis from Covid infection.
In this context I would point readers and health professionals to the Government’s own ‘information for health care professionals’ published on January 17.
It emphasises that all suspected cases must be reported to the MHRA using the Yellow Card scheme. It specifically demands that ‘in addition, a serum sample should be collected from any patient that is suspected of experiencing myocarditis or pericarditis following any Covid-19 vaccination and sent to the UK Health Security Agency, Colindale. Please use the code “Heart Inflammation” or “Myocarditis” for easy identification and which vaccine dose (and vaccine brand) the symptoms developed after.’
Despite this admission of urgency, we have yet to see any alert by the Government to pause the vaccine for younger men, women and children.
We can only conclude that ministers are choosing to disregard a serious risk that they themselves warn of – a worrying display of acute cognitive dissonance.
‘Anyone who develops these symptoms within ten days of a Covid-19 vaccination should urgently seek medical assistance,’ the information alert adjures.
But from the tone of the message, all is seemingly okay, because ‘the existing evidence base shows that most patients with myocarditis post-vaccination respond well to standard treatment for the acute episode, and the prognosis of the myocarditis is good’.
However, it adds that ‘it may have long-term consequences and studies are in progress to further understand the potential longer-term consequences with follow-up at three months and six months’.
Well, we’ll just have to pray that each individual strikes lucky, won’t we? Becausewhile myocarditis may be mild, bringing few or no symptoms, it can also be severe, causing life-threatening heart failure.
Furthermore, no one can deny that its immediate complications include ventricular dysrhythmias (abnormal heart rhythm), left ventricular aneurysm (swelling of a weakened muscular wall), congestive heart failure, and dilated cardiomyopathy (thinning of the left ventricle). Or that, despite optimal medical management, overall mortality has not changed in the last 30 years. The mortality rate is up to 20 per cent at one year and 50 per cent at five years.
Why on Earth would any government actively inflict this hazard on healthy young people who are effectively at zero risk of dying from Covid?
Such breathtaking complacency is alarming. It is as though simply acknowledging myocarditis as a reaction makes everything all right and no further action is needed. In effect, the Government can’t ignore the problem, so it neutralises it by normalising it. That may be convenient, but it is mendacious and dangerously disingenuous.
Here is our latest MHRA Yellow Card combination reporting summary up to February 2, 2022 (data published February 10, 2022):
Adult – Primary and Booster/Third Dose, Child Administration
* Pfizer: 25.8million people, 48.7million doses. Yellow Card reporting rate, one in 158 people impacted.
* Astrazeneca: 24.9million people, 49.1million doses. Yellow Card reporting rate, one in 102 people impacted.
* Moderna: 1.6million people, three million doses. Yellow Card reporting rate, one in 45 people impacted
Overall one in 118 people injected experienced a Yellow Card Adverse Event, which may be fewer than 10 per cent of actual figures, according to MHRA.
Adult Booster or 3rd Doses given = 37,419,104 people
One of the major frustrations throughout the COVID-19 crisis has been the failure of high-profile journalists to ask ministers and SAGE scientists challenging questions about the rationale for their – often unprecedented – decisions. When they were not baying for earlier and harder restrictions, the journalists who participated in the numerous coronavirus press conferences typically restricted themselves to questions seeking clarification about the detail of a new rule or imposition rather than imploring the experts to justify the reasoning that led to their non-evidenced diktats.
I am sure I’m not alone in fantasising about the sort of questions I would like to put to the key rule-makers responsible for this extraordinary two-year assault on our basic human rights. Consider, for instance, Professor Chris Whitty, England’s Chief Medical Officer, and his belated support for requiring people to wear masks in community settings, arguably the most insidious of all the COVID-19 restrictions.
This is not an academic issue. Thanks to the Government’s relentless messaging about the purported benefits of face coverings, there is a real danger that widespread community masking – with all the attendant physical, social, psychological and environmental harms – could become a permanent feature, at least in certain sections of our society.
Prof. Whitty’s track record on the contentious issue of masking healthy people is, like that of many of the high-profile political and scientific rule-makers, characterised by contradiction. In early March 2020, he unequivocally stated that healthy people should not be wearing face-coverings. One month later, he was faltering, saying that, “The evidence is weak, but the evidence of a small effect is there under certain circumstances”. Since this time he has supported – or, at least silently colluded – with the pro-mask lobby. What changed his mind? No robust evidence supporting mask efficacy emerged in spring 2020, nor any time since, so what ‘nudged’ him to relinquish his anti-mask stance?
To clarify the reasons for his change of mind, I would be keen to be given the opportunity to ask our Chief Medical Officer the following questions:
Around April/May 2020, what piece of robust real-world research made you change your mind about the ineffectiveness of masking healthy people in the community?
As late as December 2020, a WHO document concluded that: “There is only limited and inconsistent scientific evidence to support the effectiveness of masking healthy people in the community.” Do you agree with the BBC Newsnight reporter Deborah Cohen that the WHO’s U-turn on masks was likely to have been the result of political lobbying?
With regard to the imposition of masks, what has been the specific rationale offered to you by the Government’s behavioural scientists, such as Professor David Halpern?
Is it merely a coincidence that masks powerfully help enforce the main ‘nudges’ promoted by behavioural scientists to achieve compliance with COVID-19 restrictions?
Do you agree that the most robust type of scientific evidence is that provided by real-world, randomised controlled trials? If so, how can you reconcile your promotion of mask wearing with the results of such trials that consistently show that masks do not significantly reduce the transmission of respiratory viruses, including SARS-CoV-2?
Do you agree that, in a democratic free society, the evidential bar for mandating an intervention (such as masking the healthy) should be set very high? If so, do you believe that the empirical evidence for the benefits of masks as a means of reducing viral transmission reaches this threshold?
There are a wide range of harms (physical, social, psychological and environmental) associated with masking healthy people, including the maintenance of inflated levels of fear that will have contributed significantly to the tens-of-thousands of non-Covid excess deaths and the current mental health crisis. Do you believe that a marginal reduction in viral transmission can compensate for this extensive collateral damage?
If the Government’s behavioural scientists had not promoted masks as a way of increasing a sense of ‘solidarity’ that encouraged general compliance with the COVID-19 restrictions, can you confirm whether you would have changed your advice?
Growing numbers of people would like to hear Whitty’s answers to these important questions. Given the opportunity, I would be very happy to directly put them to our Chief Medical Officer in a public forum. Failing this, maybe a high-profile journalist will rise to the challenge. Ah, we can but dream.
Dr. Gary Sidley is a retired NHS Consultant Clinical Psychologist, a member of HART and co-founder of the Smile Free campaign.
By Lisa Pease | Consortium News | September 16, 2013
More than a half century ago, just after midnight on Sept. 18, 1961, the plane carrying UN Secretary-General Dag Hammarskjöld and 15 others went down in a plane crash over Northern Rhodesia (now Zambia). All 16 died, but the facts of the crash were provocatively mysterious. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.