A few thoughts on COVID19 vaccination
By Dr. Malcolm Kendrick | February 23, 2022
The first thing I want to say here is that there should be nothing in science that is beyond analysis and potential criticism. Because, once this happens, we can find ourselves in a very dangerous situation indeed. A place of unquestioned acceptance of the accepted narrative, with criticism enforced by the authorities.
Unfortunately, I believe this is the place we have reached with COVID19 vaccination. Here is just one example from the UK.
‘GPs have been warned that criticising the Covid vaccine or other pandemic measures via social media could leave them ‘vulnerable’ to GMC* investigation.’1
*GMC = General Medical Council. This is the body that can strike doctors from the medical register so they cannot work as a doctor.
‘Vulnerable to GMC investigation’. What a deliciously creepy phrase that is, dripping with unspoken menace, whilst pretending to be helpful. It sounds like something the Mafia would come up with.
‘I would keep quiet about this, if I were you.’ Baseball bat tapping gently on the floor. ‘No, this is not a threat, think of it as advice from a friend. We don’t like to see anybody making themselves, or their family, vulnerable, and getting seriously injured now, would we?’
It seems that, unless you prostrate yourself before the mighty vaccine, and intone ‘Our vaccine, which art in heaven, hallowed be thy name…’ and suchlike, you will be attacked from all sides … simultaneously. Indeed, to suggest that vaccines are not perfect in every way is the twenty first century’s equivalent of blasphemy.
‘he said Jehovah. Stone him.’
This does make any discussion on vaccines somewhat tricky. To criticize any individual vaccine, indeed any aspect of any individual vaccine, is also to be instantly defined as an anti-vaxxer. Then you will be furiously fact-checked by someone with a fine arts degree, or suchlike, who will decree that you are ‘wrong’.
At which point you will be unceremoniously booted off various internet platforms – amongst other sanctions open to the ‘vulnerable’. This includes, for example, finding yourself struck off the medical register, and unable to earn any money:
‘Hell, we ain’t like that around here. We don’t just string people up, son. First, we have a trial to find ‘em guilty, only then do we string ‘em up. Yeeee Ha!’
Spit … ding!
Yes, it seems you must support the position that all vaccines are equally wonderful, no exceptions. Try this with any other pharmaceutical product. ‘He doesn’t think statins are that great, so he obviously believes that antibiotics are useless.’ Would this sound utterly ridiculous?
But with vaccines… All are the same, all are great, not a problem in sight? I said, NOT! a problem in sight. However, I genuinely believe there are some questions which still have not been answered and simply because of the different types of vaccines that are available, no, not all vaccines are the same.
Just for starters, vaccines come in many different forms. Live, dead, those only containing specific bits of the virus, and suchlike. Now we have the brand new, never used on humans before, messenger RNA (mRNA) vaccines. So no, all vaccines are not alike. Not even remotely.
In addition to the major difference between vaccines, the diseases we vaccinate against vary hugely. Some are viruses, others bacteria, others somewhere in between, TB for example.
Some, like influenza, mutate madly in all directions. Others, such as measles, do not. Some viruses are DNA viruses – which tend to remain unchanged over the years. Others, e.g. influenza, are single strand RNA viruses, and they mutate each year.
Adding to this variety, some of those viruses which mutate very little, also have no other host species to hide in. Smallpox, for example. Which means that the virus was unable to run away and hide in, say, a chicken, or a bat. Others are fully capable of flitting from animal species to animal species. Bird flu and Ebola spring to mind.
Some vaccines just haven’t worked at all. For over thirty years, people have tried to develop an HIV vaccine, and have thus far failed. Early trials on animal coronavirus vaccines also showed some concerning results. Here from the paper ‘Early death after feline infectious peritonitis virus challenge due to recombinant vaccinia virus immunization.’
‘The gene encoding the fusogenic spike protein of the coronavirus causing feline infectious peritonitis was recombined into the genome of vaccinia virus. The recombinant induced spike-protein-specific, in vitro neutralizing antibodies in mice. When kittens were immunized with the recombinant, low titers of neutralizing antibodies were obtained. After challenge with feline infectious peritonitis virus, these animals succumbed earlier than did the control group immunized with wild-type vaccinia virus (early death syndrome).’2
Yet, despite all this massive variety flying in all directions, with some spike protein vaccines found to increase the risk of death (in a few animal studies), attach the word vaccine to any substance, and it suddenly has miraculous properties that transcend all critical thought. Vaccines move in mysterious ways, their wonders to perform.
Yes, of course, some have worked extremely well. The polio vaccine, for example, although I have seen some valid criticisms. Smallpox… I am less certain about. Even though it is held up as the greatest vaccine success story of all. Maybe it was. Smallpox has certainly gone, for which we should be truly thankful. It was a truly terrible disease.
My doubts about the unmatched efficacy of smallpox vaccine simply arise from the fact that diseases come, and diseases go. The plague, for example. This was the scourge of mankind at one time. It tore round and round the world and leaving millions of dead in its wake, over a period of hundreds of years.
We do not vaccinate against the plague, yet it is virtually unknown today. Cholera killed millions and millions, thousands each year in the UK alone. Now … gone. In the UK at least. This had nothing to do with vaccination either. Measles. There seems little doubt that the measles vaccine is effective. But vaccination cannot explain the fact that measles deaths fell off a cliff and were bumping along the bottom for years and long before we started vaccination programmes.

In the US vaccination did not begin until 1963. So, what happened here? The virus did not mutate, so far as we know. It did not mutate because apparently it cannot. Or, if it did, it would no longer be able to be infective. At least not to humans:
‘While the influenza virus mutates constantly and requires a yearly shot that offers a certain percentage of protection, old reliable measles needs only a two-dose vaccine during childhood for lifelong immunity. A new study publishing May 21 in Cell Reports has an explanation: The surface proteins that the measles virus uses to enter cells are ineffective if they suffer any mutation, meaning that any changes to the virus come at a major cost.’3
So, measles didn’t change, but it did become far less damaging. From around ten deaths per one hundred thousand in the first two decades of the twentieth century, down to much less than one.
Why? What I believe happened with measles is primarily that the ‘terrain’ changed. Nutrition greatly improved. Vitamins, perhaps most importantly vitamin D, were discovered and added to the food supply. Rickets and other manifestation of vitamin D deficiency were rife in the late nineteenth and early twentieth centuries. Virtually gone by 1940.
Of course treatments improved as well, although antibiotics (to treat secondary bacteria pneumonia following measles), did not come into play until the late 1940s, at the earliest.
What we see with measles is simply the fact that infectious diseases have far less impact when they hit a healthy, well nourished person (healthy terrain), than when they hit an impoverished and undernourished child caught in the war in the Yemen, for example.
So, yes, vaccines have played a role in improving human health and wellbeing, but we shouldn’t inflate their impact to the point where they have become the unmatched saviours of humankind. They have certainly not been the only thing that reduced the impact of infectious diseases. They were probably not even the most important thing. ‘Yes … how dare you say this… string up the unbeliever, I know, I know.’
Moving on, and I think this is even more pertinant to the disucssion that follows. If we cannot accept the possiblility that, at least some vaccines, may have significant adverse effects, if we will not permit anyone to look into this, in any meaningful way. Then we can never improve them. Criticism is good, not bad.
Speaking personally, I do not criticize things that I do not care about. Primarily, because I don’t care if they improve, or not. I only criticize things when I want them to be as good as they possibly can be. It is a character trait of mine to hunt for flaws, and potential problems. Both real and imagined.
Some criticism is, of course, close to bonkers. Suggesting that COVID19 vaccines contain transhuman nanotechnology and microchips of some kind that will become activated by 5G phones … to what end? ‘World domination Mr Bond. Mwahahahahaha etc.’ Quantum dots? Yes, these do exist. But they would be pretty useless at collecting informaiton, and suchlike. Give it fifty years and … maybe.
The problem here is that wild conspiracy theories are simply gathered together with reasonable science-based criticism, to be dismissed as a package of equally mad, unscientific woo-woo tin-foil hat wearing, conspiracy theorist, gibberish.
Which means that, when people (such as me) suggested that COVID19 mRNA vaccination could, potentially, lead to an increased risk of blood clots – this was treated with utter scathing dismissal. I did not understand ‘the science’ apparently. Fact check number one. ‘Oh, look… clots.’
When people questioned the ‘fact’ that the safety phases of the normal clincial trial pathway had been seriously truncated, and that some parts were just non-existent, they were told that they knew nothing of ‘the science’ either.
I looked on the BBC website to find out the ‘official’ party line on vaccine safety information, sanctioned and approved by HM Govt, and SAGE I presume. It was an article entitled ‘How do I know if the vaccine is safe?’ The information rapidly contradicts reality. They say:
- There are different approved types and brands available and all have undergone rigorous testing and safety checks
- Safety trials begin in the lab, with tests and research on cells and animals, before moving on to human studies
- The principle is to start small and only move to the next stage of testing if there are no outstanding safety concerns
The article then looks at fast track approval for vaccines against new variants
- The UK’s drug regulator says new vaccines can be fast tracked for approval if needed.
- No corners will be cut, with safety paramount.
- But lengthy clinical trials with thousands of volunteers will not be needed4
What is wrong here? Well, ‘if the principle is to start small and only move to the next stage of testing if there are no outstanding safety concerns,’ then this principle was not followed. After pre-clinical and animal testing, we move onto trials in humans. Phase I, then II and then III.
Phase I may include as few as twenty people to check that humans don’t simply drop dead on contact with the new agent (it has happened).
Phase II may include a couple of hundred individuals, and usually lasts a few months… a bit more safety, and an attempt to establish the potential size of any health benefit.
Phase III may have up to thirty or forty thousand participants. This phase often lasts for several years.
Well, with the Pfizer Biontech vaccine, the concept of waiting to move to the next stage of testing did not truly occur. Because phase II and III were combined… and the phase III trials have now been, effectively abandoned. They were not supposed to finish until May 2022 at the earliest, and now apparently, they are not going to finish at all. At least not as a double-blind placebo controlled trial.
Yet, we are still informed by the BBC, in all seriousness, that no corners were cut, or will be cut. The fact is that corners were absolutely one hundred per cent cut. Slashed to the bone would perhaps be more accurate. To pretend otherwise is simply to deny reality.
It normally takes around ten years for any drug, or vaccine, to move through the clinical trials process, with each step done in series. COVID19 vaccines took around six months from start to finish, with critical steps done in parallel, and the animal testing was rushed – to say the least. To claim that no corners were cut is nonsense. Nonsense that we are virtually forced to believe?
It is possible/quite likely/probable that vaccine development can be shortened, but please do not tell us that all the normal processes were followed. No-one is that easily fooled.
‘Freedom is the freedom to say that two plus two make four[NK1] . If that is granted, all else follows.’ That freedom disappeared pretty early on in the COVID19 pandemic. I enjoyed the slant that ‘Important quotes explained’ had on the quote from Orwell’s 1984.
By weakening the independence and strength of individuals’ minds and forcing them to live in a constant state of propaganda-induced fear, the Party is able to force its subjects to accept anything it decrees, even if it is entirely illogical.
Of course, it could be that despite the speed with which these vaccines were pushed through nothing important was missed. It is almost certainly true that the standard ten years from start to finish in vaccine and drug development can be compressed, if everyone really wished. Bureaucracy expands to fill the space available.
But in general we are talking about a ten-year process, cut down to six months, or thereabouts. An additional concern is that this happened using mRNA vaccines, which represent a completely new form of technology. One that has never been used on humans before at all, ever.
We are not talking about the sixth drug in a long line of very similar drugs e.g. the statins.
- Lovastatin
- Fluvastatin
- Simvastatin
- Pravastatin
- Atorvastatin
- Cerivastatin
- Rosuvastatin etc.
Statins all do pretty much the exact same thing, in exactly the same way. Yet, each one of them still had to go through the entire laborious clincial trial process. Years and years.
‘Can we not just skip this phase…. please?’
‘No.’
‘Please?’
‘No.’
Hold on one moment, just step back, what was that at number six on this list, I hear you say… cerivastatin. You mean you’ve never heard of it. Well, it got through all the pre-clinical trials, then the animal trials. It then sailed through the human Phase II and III trials without a murmur. It was then was launched to wild acclaim. In truth that may be over-egging its real impact, which was a bit more ‘who cares, do we really need another one?’
Here from a 1998 paper: ‘Clinical efficacy and safety of cerivastatin: summary of pivotal phase IIb/III studies.’
‘In conclusion, these studies indicate that cerivastatin is a safe and effective long-term treatment for patients with primary hypercholesterolemia and also suggest that higher doses should be investigated.’ 5
Here from 2001, and an article entitled: ‘Withdrawal of cerivastatin from the world market.’
‘Rhabdomyolysis was 10 times more common with cerivastatin than the other five approved statins. We address three important questions raised by this withdrawal. Should we continue to approve drugs on surrogate efficacy? Are all statins interchangeable? Do the benefits outweigh the risks of statins? We conclude that decisions regarding the use of drugs should be based on direct evidence from long-term clinical outcome trials.’ 6
Yes, as it turns out, cerivastatin caused far more cases of severe muscle breakdown, and death, in a significant number of people. Which meant that it was hoiked from the market.
The moral of this particular story is that, even if you DO do all the clinical studies, fully and completely, one step at a time, over many years, in a widely used class of drug, your particular drug may still be found in the long term, not to be safe. Not even if it is the sixth of its class to launch.
The cerivastatin withdrawal is not an isolated event. You can, if you wish, read this paper ‘Post-marketing withdrawal of 462 medicinal products because of adverse drug reactions: a systematic review of the world literature.’7. So, what happens if you try to compress the entire ten year clinical trial process into around six months, on a completely new type of agent?
… Well then, it may be time to cross your fingers and hope for the best. But please do not insult my intelligence, or the intelligence of anyone else, by trying to tell me that vaccines have undergone: Rigorous testing and safety checks. Compared to what, exactly? Certainly not any other drug or vaccine launched in the last fifty years. ‘We rushed them through, and launched two years before the phase III clinical trials were due to finish.’ would be considerably more accurate.
Two plus two does not equal five, it never has, and it never will. However much you try to browbeat me, and everyone else, into accepting that it does. Indeed, as I write this, the simple fact is that not a single phase III clinical trial has yet ever been completed, on any mRNA COVID19 vaccine, and possibly not ever will be, in truth.
To repeat, this does not mean that mRNA vaccines may not be entirely safe. However, it has become impossible to claim that we have not seen significant adverse effects from the mRNA vaccines. Effects that were not picked up in any phase of the clincial trials. Here, from the Journal of the American Medical Association in February. One of the most highly cited medical journals in the world:
‘Based on passive surveillance reporting in the US, the risk of myocarditis after receiving mRNA-based COVID-19 vaccines was increased across multiple age and sex strata and was highest after the second vaccination dose in adolescent males and young men.’ 8
I highlighted the first bit here. Namely, the words ‘based on passive surveillance reporting in the US.’ Whilst this adverse effect was not seen, or reported in the clinical trials it was picked up by the passive surveillance reporting system a.k.a. spontaneous reporting systems.
Drug adverse event reporting systems
Frankly, it is surprising that anything at all is ever seen using passive surviellance. In the UK we have the passive/spontaneous reporting system, known as the ‘Yellow Card system.’ In this US (specifically for vaccines) there is ‘VAERS’ (Vaccine Adverse Event Reporting System).
When I use the term ‘spontaneous reporting’, I mean a system whereby someone may (or more likely may not) report an adverse effect to a healthcare professional. They may (or more likely may not) fill in a form, whereupon it goes through to VAERS, who then look at it and can decide whether or not the adverse effect may (or more likely may not) be due to the vaccine. Same basic principle in the UK.
How good are these types of spontaneous reporting system in picking up adverse effects?
Well, as far as I am aware, only one serious attempt has been made to look at how many drug and vaccine-related events were actually reported in the US. Here, from a study by The Agency for Healthcare Research and Quality:
‘Adverse events from drugs and vaccines are common, but under-reported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported.’ 9
Fewer than one per cent of vaccine adverse events are reported. Their words, not mine. Even though, in the US, unlike the UK, there is a legal responsibility to report adverse events – I believe.
When the authors of this report tried to follow up with the CDC and perform further assessment of the system, with testing and evaluation, the doors quietly, but firmly, shut:
‘Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.’
This study was done over ten years ago, but nothing about the VAERS system has changed since, as far as I know, or can find out.
In the UK the Yellow Card system may be better, or it may not be. No-one has carried out the sort of detailed analysis that was attempted in the US. However it has been accepted that:
… all spontaneous reporting schemes have a problem with numbers: the MHRA (Medicines and Healthcare products Regulatory Agency) itself says that only 10% of serious reactions and 2 – 4% of all reactions are reported using the Yellow Card Scheme. This means that most iatrogenic* morbidity goes unreported.’ 10
*Iatrogenic means – damage/disease caused by the treatment itself.
Frankly, I see no reason why the Yellow Card system would be any better than VAERS. The barriers to reporting are exactly the same. As the US report states:
‘Barriers to reporting include a lack of clinician awareness, uncertainty about when and what to report, as well as the burdens of reporting: reporting is not part of clinicians’ usual workflow, takes time, and is duplicative.’9
In other words, reporting an adverse event takes an enormous amount of time and effort. You don’t get paid for doing it, you certainly don’t get thanked for it, and you have no idea if anyone paid any attention to it. All made worse if you are not sure if the adverse event was due to the vaccine, or not.
I have filled in yellow cards three times, and several hours of work followed each one. As directed, I searched though patient notes for all previous drugs prescribed, the patient’s medical conditions, a review of the consultations and on, and on. Back and forth from the pharmaceutical company the questions went. Until the will to live was very nearly lost.
If you wanted to devise a system to ensure that adverse effects were under-reported, you could not devise anything better. Yes, doctor, please do report adverse effects to us. The result will be endless hours of work, with no attempt to report back that what you did had the slightest effect, on anything. Thank you for your continued and future co-operation. And yet this, ladies and gentlemen, is the system we have in place to monitor and review all drug and vaccine-related adverse effects.
Which becomes even more worrying because, as mentioned before a couple of times so far, nothing else of much use is going to come out of the clinical trials. With the Pfizer BioNTech trial, crossover occurred in Oct 2020. By crossover I mean the point at which they started giving the vaccine to those in the placebo group as well. End of randomisation, end of useful data. End of … well of anything of any use.
mRNA vaccines and myocarditis
Anyway, getting back to the JAMA study. Even with all the formidable barriers in place to reporting adverse events, JAMA reported an increase in the rate of myocarditis of around thirty-two-fold, as reported via the VAERS system.
I should make it clear that this was the increase seen in the most highly affected population. Males aged eighteen to twenty-four. [Myocarditis = inflammation and damage to heart muscle]. The risk was lower in females, and also in other age groups, although still high. But, to keep things simple, I am going to focus on this, the highest risk group, as far as possible.
The first thing to say is that a thirty-two-fold increase probably does sound enormous. Another way to report this would be, a three thousand one hundred per cent increase, which may sound even more dramatic?
However, myocarditis is not exactly common. In this age group, over a seven-day period, you would expect to see around one and three-quarter cases per million of the population. Multiplying this by thirty-two still only gets you to fifty-six cases per million.
Which is not exactly the end of the world. In addition, most cases may fully recover. Although, having just said this, I have no long-term data to support that statement. The closest condition we have to go on as a comparator, is post-viral infectious myocarditis. And this has a mortality rate of 20% after one year and 50% after five years.11
Which means that myocarditis is certainly not a benign condition of little concern.
Anyway, at this point, you could argue that if around only one in twenty thousand men, in the highest risk population, suffer from myocarditis post-vaccination, then this does not represent a major problem.
It could indeed be worse to allow them to catch COVID19, where the risk of myocarditis is even higher than with vaccination. In reality, we may be protecting them from myocarditis through vaccination. This certainly seems to be the current party line. I might even agree with it… maybe. So, as is my wont, I looked deeper.
I looked for the highest rate of (reported) post-viral infection myocarditis, in younger people. I believe it can be found here. ‘Risk of Myocarditis from COVID-19 Infection in People Under Age 20: A Population-Based Analysis’ 12
Here, the reported rate was around four-hundred-and-fifty cases per million. On the face of it, this is much higher than the fifty-six cases per million post-vaccination. Approximately ten times as high. But … there are, as always, several very important buts here. There were two key factors that alter the equation.
First, in the JAMA post-vaccine study, the time period for reporting myocarditis was limited to seven days after vaccination. Any case appearing after that was not considered to be anything to do with the vaccine and was thus ‘censored’. In the study above, the time period was far longer. Anything up to ninety days post-infection was counted. A period thirteen times as long.
In addition, although it is difficult to work out exactly what was done from the details provided, the four-hundred-and fifty study only looked at young people who attended outpatients at hospital. These would have been the most severely affected by COVID19, or who had other underlying medical conditions. So, they represent a small proportion, of a small proportion …. of everyone who was actually infected. The vast majority of whom would only have suffered very mild symptoms, or none at all.
In short, we are not remotely comparing like with like here. I find that we very rarely are. We are not only going to vaccinate a small proportion, of a small proportion, of the population who are at high risk of myocarditis. We are going to vaccinate virtually everybody. So, the two populations are completely different.
Leaving that to one side, where else can we look for a comparison between the risk of post-vaccine myocarditis vs post-infection myocarditis. The CDC published this statement.
‘During March 2020–January 2021, patients with COVID-19 had nearly 16 times the risk for myocarditis compared with patients who did not have COVID-19, and risk varied by sex and age.’ 13
Their figure appears to have been entirely derived from a paper published in the British Medical Journal : ‘Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: retrospective cohort study’ 14. Different age groups were studied here which, again, makes any direct comparison tricky.
This study found a sixteen-fold increased risk, rather than a four hundred and fifty-times risk. A sixteen times risk is around half of the post-vaccination myocarditis risk reported in JAMA, in the eighteen-to twenty-four-year-old group.
Again, though, there were major differences. In the BMJ paper the observation period for inclusion of myocarditis considered to be ‘caused by’ COVID19, was one hundred- and forty-days post infection, not seven days. Twenty times as long for cases to build up.
Equally, after looking at nine million patients records over a year, slightly over two hundred thousand were diagnosed as having had COVID19. Of these, only fourteen thousand had post-infection problems, known as clinical sequelae. In this sub-group, which represents, one point two per-cent of one per-cent of the total, population there were so few cases of myocarditis that they didn’t even appear in the chart published in the main paper. You had to go to supplemental tables and figures 15
To be frank, there are far too many unknowns and uncontrolled variables kicking around here to make any accurate comparisons. However, I do not think it would be unreasonable to suggest that the risk of myocarditis post-vaccination, from these studies, is roughly the same as if you are infected with COVID19.
Once again though, we need to take a further step back. All of our figures here only make sense if all – or the majority of cases of myocarditis – are actually being picked up. What if they are not?
Worst case scenario
SAGE – the UK Governments scientific advisory group for emergencies – have been accused of scaremongering, and only presenting worst case scenarios for COVID19 hospital admissions and deaths. They are not the only ones. This is a worldwide phenomenon.
However, as Sir Patrick Vallance – one of the key members of (SAGE) – has stated, in response to such criticism.
‘It’s not my job to be an optimist’: Sir Patrick Vallance takes swipe at critics accusing scientists of scaremongering over Covid saying ministers need to ‘hear the information whether uncomfortable or encouraging.’ 16
SAGE believe it is their role to highlight the worst possible scenarios, the highest possible death tolls, and such like. So, let us now do the same, and focus on the worst-case scenario regarding mRNA vaccines and myocarditis. Whether ‘uncomfortable or encouraging’.
The worst-case scenario starts like this. If the VAERS system only picks up one per cent of vaccine related adverse effects, this means that we can start by multiplying the JAMA figures by one hundred.
Thus, instead of fifty-six cases per million, the reality is that we could be looking at five thousand six hundred cases per million, post-vaccination. Or very nearly one in two hundred.
If, in this model, we then include the possibility that post-vaccination myocarditis is as damaging as post-viral infection myocarditis, it means that one in four hundred eighteen to twenty-four-year-olds could be dead five years after vaccination.
Do I think that this is likely? I have to say that no, I don’t, really. Although this is where the figures, such as they can be relied upon, inevitably take you. Just to run you through the process a bit more slowly.
- Relying on the VAERS system, JAMA reported a thirty-three-fold increase in myocarditis post COVID19 vaccination. An increase from 1.76, to 56.31 cases per million (in the seven-day period post vaccination)
- It has been established that VAERS may pick up only one per cent of all vaccine related adverse effects
- Therefore, the actual number could be as high as five-thousand six-hundred cases per million ~ 1 in 200.
- Myocarditis (post viral infection) has a mortality rate of 50% over 5 years. So, we need to consider the possibility that post-vaccination myocarditis will carry the same mortality.
- Therefore, the rate of death after five years could be one in four hundred (males aged 18-24)
There are approximately sixteen million men aged between eighteen and twenty-four in the US.
Total number of deaths within five years (men aged eighteen to twenty-four in the US)
16,000,000 ÷ 400 = 40,000
(Divide by five for the UK) = 8,000.
Now, if I were in charge of anything, which I am not, which is probably a good thing, I would hope to have been made aware of these worst-case scenario figures. I would then immediately have begun to do everything I possibly could to verify them.
For starters I would want to know two critical things:
1: Is the VAERS system truly only picking up one per cent of vaccine related adverse effects?
2: Does vaccine related myocarditis lead to the same mortality and morbidity as caused by a viral infection?
If the answer to both of these questions were, yes, then I would have to decide what to do. And that could not possibly, be nothing. At least I would hope not. Yet, nothing appears to be exactly what is currently happening.
As you can tell, I still cling to the concept of ‘first do no harm.’ Today, with COVID19, it seems this this idea has become hopelessly naïve. The current attitude seems to be. ‘We are at war; you must expect casualties’ ‘Also, careless talk costs lives.’ So, my friend, I advise you to keep your ‘vulnerable’ mouth shut, if you know what is good for you.’
Well then, I just hope for everyone’s sake, that these figures are completely wrong. They are, after all, only a model. A worst-case scenario created using the most accurate information available at this time. However, as per the SAGE underlying philosophy, I believe it is important to present the information whether uncomfortable or encouraging.
The thing that concerns me the most is that we have a worrying signal emerging about the mRNA vaccines. A signal surrounded by a lot of noise, admittedly. Yet, the ‘official’ response continues to be to sweep the entire thing under the carpet. ‘Nothing to see here, move along.’
Postscript
As with regard to the GMC, and the threat of sanctions, as you can see, I am only following their guidance
‘Healthcare professionals must also be open and honest with their colleagues, employers and relevant organisations, and take part in reviews and investigations when requested. They must also be open and honest with their regulators, raising concerns where appropriate. They must support and encourage each other to be open and honest, and not stop someone from raising concerns.’ 17
What do you do if it is the GMC itself that may be stopping someone from raising concerns. Should I report the GMC to the GMC? I imagine they will find themselves innocent of any wrongdoing. Quis custodiet Ipsos custodes?
2: https://europepmc.org/article/MED/2154621
3: https://www.sciencedaily.com/releases/2015/05/150521133628.htm
4: https://www.bbc.co.uk/news/health-55056016
6: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC59524/
7: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4740994/
8: https://jamanetwork.com/journals/jama/fullarticle/2788346
10: https://wchh.onlinelibrary.wiley.com/doi/pdf/10.1002/psb.1789
12: https://pubmed.ncbi.nlm.nih.gov/34341797/
13: https://www.cdc.gov/mmwr/volumes/70/wr/mm7035e5.htm
14: https://www.bmj.com/content/373/bmj.n1098
15: https://www.bmj.com/content/bmj/suppl/2021/05/19/bmj.n1098.DC1/daus063716.wt.pdf
German Public Health Insurer: Vaccine Side Effects Maybe 8 to 10 Times More Frequent Than Officially Reported
eugyppius | February 23, 2022
German publicly regulated health insurers, the Betriebskrankenkassen, report substantially higher vaccine adverse effects than the Paul-Ehrlich-Institut, our vaccine regulatory body.
Andreas Schöfbeck, board member of BKK ProVita, one of these insurers, told Welt in the linked article that “The figures we have found are substantial and demand urgent verification.”
Basically, BKK ProVita noticed anomalous diagnoses indicating adverse vaccine side effects, particularly surrounding these codes: T88.0: Infection or sepsis after vaccination; T88.1: Other complications or skin rash following vaccination; Y59.9: Complications due to vaccines or biologically active substances; and U12.9: Undesirable side effects from Covid-19 vaccines.
Meanwhile, the official PEI reports figures almost one magnitude lower.
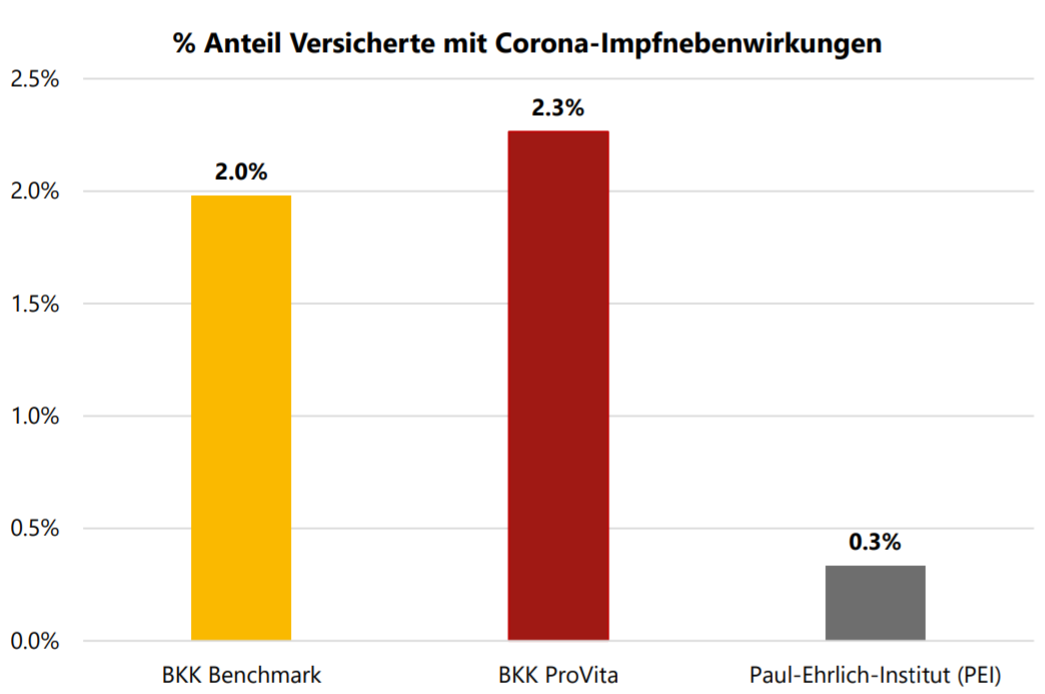
Percent of insured with vaccine side-effects. Yellow: All BKK-insured side-effects. Red: BKK ProVita insured side-effects. Grey: Side effects publicly acknowledged by PEI.
Schöfbeck says that probably there have been 400,000 clinical consultations by BKK insured alone due to vaccine complications. “Extrapolated to the total [German] population, the number would be three million.”
UPDATE: The data represents 10,937,716 German insured, over 13% of the country. The data comprises the first six months of 2021, and about half of the billing records for the third quarter of 2021. This is an extremely partial picture of the vaccine side effects, excluding much of the booster campaign here.
See also: el gato malo
The Lie That Net Zero is ‘Settled Science’

By Chris Morrison | The Daily Sceptic | February 22, 2022
Historically, the claim of consensus is the first refuge of the scoundrel; it is a way to avoid debate by claiming the matter is already settled. Whenever you hear the consensus of scientists agrees on something or other, reach for your wallet, because you’re being had. Let’s be clear: the work of science has nothing whatever to do with consensus. Consensus is the business of politics.
Michael Crichton, PhD, MD, author, screenwriter and academic
Humans cause all or most of the changes in the climate by burning fossil fuel. We must stop using the most efficient fuel we have, one that supplies 85% of our energy needs, and sign up for a so-called Net Zero future. The rich will get richer, since they will control state-mandated transfers of once-productive capital into new untried technologies, and the poor will get poorer. Holidays, personal travel and energy will be rationed (for the masses), while meat-free diets will be the order of the day. There are disadvantages, admit the green, politically motivated zealots, but it has to be done. The Earth is on fire – the science is settled.
Except that it isn’t. The idea that humans are largely responsible for climate change is an unproven hypothesis. The claim that it is ‘settled science’ on which all specialists in the field agree is a political con. Over 40 years, climate models have produced wildly inaccurate warming forecasts that have never been right.
The political narrative of global warming got going in the 1980s, following the failure of the 1970s global cooling scare. The warming narrative had a good ride for 15 years, until the recent warming started to run out of steam. Over the last seven years, there has been a standstill in temperatures. This is part of what lies behind the recent rebranding of bad weather as ‘extreme’, and unscientific attempts to link solo events to long-term aggregate climate change. Record high temperatures among the jet aircraft at Heathrow, record “gusts” of wind off isolated sea cliffs – all are used to craft a political Armageddon narrative.
At the heart of the debate, or rather the public non-debate, is the role of carbon dioxide as a warming gas. CO2 does warm the planet and the Earth would be about 33°C cooler without it and the other greenhouse gases. But its warming properties become less effective as more of it enters the atmosphere. Doubling atmospheric CO2 does not double the warming – a point which the IPCC accepts. Climate models guess that such doubling causes global temperature to rise in a range from 1.5°C to 6°C. Recent scientific work suggests this estimate is way too high. The simple ‘settled’ science deduction that rising CO2 levels automatically lead to significantly higher temperatures fails to take much account of natural climatic variations. In addition, little cause and effect between CO2 and temperature can be seen in current, historical or geological records.
CO2, methane and ozone, along with the much more common water vapour, produce a greenhouse effect of reflecting heat back to the Earth only within certain bands on the infrared spectrum. This has led some scientists to suggest that CO2 becomes ‘saturated’ once it reaches a certain level. Most of the heat that is going to be trapped is already being radiated back by the CO2 molecules evenly distributed in the existing atmosphere.
It is fascinating science, but it is conducted away from mainstream media, most political circles and the Earth Sciences/Geography university departments. It is the last that seem to provide many of the vocal scientists promoting the ‘settled science’ narrative. Such ground-breaking work holds out the promise of a better understanding of the role of CO2 in the atmosphere. Only a blinkered following of a political agenda can explain why it is ignored.
The idea that the science surrounding changes in the climate is settled goes back a long time. In 2006, the BBC ran a one day seminar in secret to decide on its future climate editorial policy. The meeting was crucial in plotting future editorial guidelines. According to the former Sunday Telegraph journalist Christopher Booker, the new guidelines “would allow it to make its coverage of any issues relating to climate change more actively partisan than ever”. Booker continued: “Its obligations to remain impartial could be put aside, it argued, on the grounds that the official orthodoxy was now so overwhelmingly accepted that any dissent from it could be dismissed as too insignificant to be worthy of notice.”
In 2013, John Cook came up with the suggestion that 97% of scientists believed that humans cause global warming. Mr. Cook is a green activist, who runs a site called Skeptical Science with the intriguing strapline: “Getting sceptical about global warming scepticism”. His notion was given a huge boost when Barack Obama tweeted that 97% of scientists agree that climate change is “real, man-made and dangerous”. In fact the 97% figure, which is still widely quoted today, was quickly debunked. It was found that of the 12,000 abstracts rated, only 0.5%, or 65 papers, suggested that humans were responsible for more than 50% of global warming.
Since scientists differ widely in their view on the human contribution to climate change, the attempt to put a number on a so-called consensus is futile and meaningless. But it makes a good headline. Step forward Mark Lynas, with a recent raise on 97% to 99%. In fact, his study found only that 99% of scientists failed to explicitly quantify the effect humans were having on the climate.
Mr. Lynas has had a lively career in green activism and journalism, first coming to attention in 2001 when he threw a pie into the face of the sceptical climate economist, Bjørn Lomborg. He was behind the PR stunt in 2009 when the Government of the Maldives met under water to draw attention to rising sea levels. Happily, this is not a problem for the Maldives, since overall the islands have grown in recent years. In 2007 he wrote an article in the Guardian reporting on the possibility of global warming producing fuel air bombs caused by oceanic methane eruptions. These would be equivalent to 10,000 times the world’s stockpile of nuclear weapons, he claimed.
These days, Mr. Lynas is the Communications Strategist and Climate Lead for the Alliance for Science, a non-profit operation linked with Cornell University. Its primary source of funding is said to be the Bill and Melinda Gates Foundation – another case, it appears, of following the money to find the billionaires pushing their pet green narratives and causes.
We the people, demand to see the data!
CDC withholding evidence concerning COVID vaccine safety is scientific fraud
By Robert W Malone MD, MS | February 21, 2022
The C.D.C. Isn’t Publishing Large Portions of the Covid Data It Collects New York Times, February 21, 2022
The agency has withheld critical data on boosters, hospitalizations…
“Two full years into the pandemic, the agency leading the country’s response to the public health emergency has published only a tiny fraction of the data it has collected, several people familiar with the data said. Much of the withheld information could help state and local health officials better target their efforts to bring the virus under control”…
Two full years into the pandemic, the agency leading the country’s response to the public health emergency has published only a tiny fraction of the data it has collected, several people familiar with the data said…
“The C.D.C. is a political organization as much as it is a public health organization,” said Samuel Scarpino, managing director of pathogen surveillance at the Rockefeller Foundation’s Pandemic Prevention Institute. “The steps that it takes to get something like this released are often well outside of the control of many of the scientists that work at the C.D.C.”
Let me translate that quote for you. Basically, a non-governmental spokesperson for the “official” public health scientific community is throwing Rochelle Walinsky under the bus, and saying that the politicians forced us to commit scientific fraud by withholding key data.
The Global Summit Doctors and other brave medical practitioners who have stood up to the lies and tyranny – who have been harassed, jobs lost, medical licenses lost, smeared and libeled are right. The data are being withheld.
The main stream media owes a whole lot of us scientists and physicians a huge apology. The main stream media has to stop being the mouthpiece for the government. This is not communist China!
The government owes the American people a huge apology. People in the government who have lied to the American people need to be charged and must be held legally accountable. We the people must demand to see ALL of the data from the CDC and the FDA.
Let’s talk data. The CDC is using cumulative data from the beginning of the vaccine roll-out in early 2021 to prop up the lie that these vaccines are effective against Omicron.
The CDC is clearly hiding the data about safety. The (thoroughly biased) NYT piece above writes further on this.
Pfizer’s data supported the safety of the vaccine, but researchers said the effectiveness wasn’t there with two shots.
“It was effective in the younger kids so those six months to two years but in the two to four-year-old age group it didn’t quite meet the levels of antibody response they expected to see,” said Dr. Christina Canody, BayCare Pediatric Service Line Medical Director.
Now instead of just having an EUA meeting about two doses, Pfizer is continuing their trial for three doses and will present that data once they have it.
Precisely what we have been saying.
Why is this important?
The FDA have not revealed what the efficacy of the boosters for children is. They have not released the safety data. They have withheld the safety data on the vaccines for children and adults.
This must stop. We are deep into outright Scientific Fraud territory.
Let’s remember where this started… We have been manipulated from the VERY start of this pandemic. The government has been deciding what has been written, removed, censored by media and the big tech giants. This is propaganda.
I am posting the HISTORIC references from the beginning of 2020 to show that our government has been involved in scientific fraud from the beginning. Do not forget – this goes back to 2020.
1. World Health Organization holds secretive talks with tech giants Google, Facebook and Amazon to tackle the spread of misinformation on coronavirus. February 17, 2020.
Google, Facebook, Amazon and other tech giants spent a day in secretive talks with the World Health Organization to tackle the spread of coronavirus misinformation.
Social media companies including Twitter and Youtube have already been working to remove post about the virus that are proved to be fake.
The World Health Organization (WHO) has offered to work directly with the companies on fact checking in a bid to speed up the process.
Posts on the virus that needed to be removed have ranged from those calling it a fad disease or created by the government to claims it can be treated with oregano oil.
Companies at the meeting agreed to work with WHO on collaborative tools, better content and a call centre for people to call for advice, CNBC reported.
2. Bloomburg. Amazon, Alphabet among tech firms meeting with White House on coronavirus response. LA Times. March 11, 2020.
White House officials discussed combating online misinformation about the coronavirus and other measures during a teleconference Wednesday with tech companies including Alphabet Inc.’s Google, Facebook Inc. and Twitter Inc.
U.S. Chief Technology Officer Michael Kratsios led the call, which also included representatives from Amazon.com Inc., Apple Inc., Microsoft Corp., IBM Corp. and other companies and tech trade groups.
The discussion focused on information-sharing with the federal government, coordination regarding telehealth and online education and the creation of new tools to help researchers review scholarship, according to a statement from the White House’s Office of Science and Technology Policy.
“Cutting edge technology companies and major online platforms will play a critical role in this all-hands-on-deck effort,” Kratsios said in a statement. He said his office would unveil a database of research on the virus in coming days
3. White House asks Silicon Valley for help to combat coronavirus, track its spread and stop misinformation. Washington Post. March 11, 2020.
The White House on Wednesday sought help from Amazon, Google and other tech giants in the fight against the coronavirus, hoping that Silicon Valley might augment the government’s efforts to track the outbreak, disseminate accurate information…
The requests came during a roughly two-hour-long meeting between top Trump administration aides, leading federal health authorities and representatives from companies including Cisco, Facebook, IBM, Microsoft and Twitter, as Washington sought to leverage the tech industry’s powerful tools to connect workers and analyze data to combat an outbreak that has already infected more than 1,000 in the United States.
Three participants described the phone-and-video conversation on the condition of anonymity because the session was private. Most tech companies in attendance either did not respond or declined to comment.
The evidence above makes it crystal clear that the government has been manipulating data from the start. Now that Omicron is here and the vaccines are clearly not working. That we have data from other countries that there are issues, we much demand transparency and put a stop to the manipulation of the American people. Free speech is free speech.
Scientists and physicians must be allowed to discuss data on the Internet. We ALL must be allowed to discuss data. It is time to stop the madness.
How this all ties into the globalists is becoming more and more clear.
The Next Step for the World Economic Forum Brownstone Institute, February 20, 2022
It has been obvious since early 2020 that there has been an organized cult outreach that has permeated the world as a whole. It’s possible that this formed out of a gigantic error, rooted in a sudden ignorance of cell biology and long experience of public health. It is also possible that a seasonal respiratory virus was deployed by some people as an opportunity to seize power for some other purpose.Follow the money and influence trails and the latter conclusion is hard to dismiss.
The clues were there early. Even before the WHO declared a pandemic in March 2020 (at least several months behind the actual fact of a pandemic) and before any lockdowns, there were media blitzes talking about the “New Normal” and talk of the “Great Reset” (which was rebranded as “Build Back Better”).
Pharmaceutical companies such as Pfizer, Johnson & Johnson, Moderna, and Astra-Zeneca were actively lobbying governments to buy their vaccines as early as February 2020, supposedly less than a month after the genetic sequence (or partial sequence) was made available by China.
As a person who spent his whole professional career in pharmaceutical and vaccine development, I found the whole concept of going from scratch to a ready-to-use vaccine in a few months simply preposterous.
Something did not add up. … Read more at Brownstone
My last thought for the day: The US government appears be complicit in the creation of this virus. Again, the people are being manipulated. The NIH and the Defense Threat Reduction Agency at the US Department of Defense must be held accountable and they must release the data as to what they have funded and what they knew when – about the creation of SARS-CoV-2. It is time for our government to come clean. It is time for an investigation. Congress must lead the way. They can not shirk their responsibility any longer.
Bill Gates is Ready to Capitalize on ‘The Next Pandemic’

21st Century Wire | February 20, 2022
As the old says goes: “there’s no rest for the wicked.”
That’s certainly the case with vaccine mogul Bill Gates.
As the world finally gets an opportunity to take a breath easy – after being suffocated by two years of pandemic theatre and 24/7 government and corporate pharmaceutical propaganda, the notorious architect the global COVID-19 ‘vaccine’ roll-out, billionaire tech monopolist turned pharmaceutical scion, Bill Gates, is still determined to realize his life’s ambition of achieve 100% global vaccine compliance.
To keep the game going, Gates has reemerged from the shadows this week to prepare the public for “the next pandemic.”
CNBC reports…
Bill Gates said Friday that the risks of severe disease from Covid-19 have “dramatically reduced” but another pandemic is all but certain.
Speaking to CNBC’s Hadley Gamble at Germany’s annual Munich Security Conference, Gates, co-chair of the Bill & Melinda Gates Foundation, said that a potential new pandemic would likely stem from a different pathogen to that of the coronavirus family.
But he added that advances in medical technology should help the world do a better job of fighting it — if investments are made now.
“We’ll have another pandemic. It will be a different pathogen next time,” Gates said.
Initially, Gates had been actively promoting each and every ‘variant’ – constantly talking-up the crisis in order to help maintain the perception of a constant demand for the highly controversial experimental COVID-19 ‘vaccine’ gene-jabs. This includes the most recent media creation known as the “Omicron” variant. But as the public began shunning the booster shots en masse, the media gradually began the abandon the Omicron narrative. Gates has clearly read the propaganda tea leaves, and has since started backtracking from some of his previous positions – and is even admitting that natural immunity is more effective than the dubious pharmaceutical-based synthetic immunity he’s been pushing for the last two years through the media and his proxy organizations the World Health Organization (WHO) and the GAVI vaccine alliance.
Two years into the coronavirus pandemic, Gates said the worst effects have faded as huge swathes of the global population have gained some level of immunity. Its severity has also waned with the latest omicron variant.
However, Gates said that in many places that was due to virus itself, which creates a level of immunity, and has “done a better job of getting out to the world population than we have with vaccines.”
In order to further shield him from an increasing public backlash for his role in shamelessly promoting the ‘global pandemic’ and vaccine narratives, Gates has also carefully admitted the existence of comorbidities among the alleged COVID deaths.
“The chance of severe disease, which is mainly associated with being elderly and having obesity or diabetes, those risks are now dramatically reduced because of that infection exposure,” he said.
However, the vaccine kingpin is still lamenting his failure to reach 70% ‘penetration’ of the experimental mRNA toxic injections into the arms of the global population.
Gates said it was already “too late” to reach the World Health Organization’s goal to vaccinate 70% of the global population by mid-2022. Currently, 61.9% of the world population has received at least one dose of a Covid-19 vaccine.
He added that the world should move faster in the future to develop and distribute vaccines, calling on governments to invest now.
“Next time we should try and make it, instead of two years, we should make it more like six months,” Gates said, adding that standardized platforms, including messenger RNA (mRNA) technology, would make that possible.
It’s important for people to realize that Gates and his network are not finished in their plan to establish a global conveyor belt for experimental gene-based pharmaceutical injections – and he is already eyeing ‘the next pandemic’ in order to roll out the next phase of this globalist agenda. There is no shortage of funds either:
“The cost of being ready for the next pandemic is not that large. It’s not like climate change. If we’re rational, yes, the next time we’ll catch it early.”
Gates, through the Bill & Melinda Gates Foundation, has partnered with the U.K.’s Wellcome Trust to donate $300 million to the Coalition for Epidemic Preparedness Innovations, which helped form the Covax program to deliver vaccines to low- and middle-income countries.
The CEPI is aiming to raise $3.5 billion in an effort cut the time required to develop a new vaccine to just 100 days.
It’s no coincidence either that Gates has just begun marketing his latest manifesto entitled, How to Prevent the Next Pandemic.
“I’ve been following COVID since the early days of the outbreak, working with experts from inside and out of the Gates Foundation who are championing a more equitable response and have been fighting infectious diseases for decades. I’ve learned a lot in the process—both about this pandemic and how we stop the next one—and I want to share what I’ve heard with people. So, I started writing a book about how we can make sure that no one suffers through a pandemic ever again.”
To mark the occasion, Gates released this disturbing propaganda video – littered with many of the staged images and government tropes used to reinforce the COVID ‘global pandemic’ crisis narrative since the winter of 2020. Watch:
An Open Letter to the Professional Bodies of Counsellors and Psychological Therapists in the UK
Therapists for Medical Freedom | February 17, 2022
We write as a group of registered counsellors, psychotherapists and psychologists in clinical practice in the United Kingdom.
We are contacting you to express our grave concerns around Vaccines as a Condition of Deployment (VCOD) mandates for health and social care professionals, and the implications that these could have for our profession.
Whilst we welcome the recent suspension of the NHS vaccine mandate [1] to allow space for further public consultation, we are also aware that Sajid Javid, the Secretary of State for Health and Social Care, has made it clear that the debate on mandatory vaccination is far from over. He was quoted in The Times on 7th February as demanding that medical regulators send the “clear message” that healthcare workers must be vaccinated against coronavirus. [2]
The implication here is that the onus of enforcing and policing the vaccination status of healthcare workers could be shifted from employers to professional/regulatory bodies. We are concerned about the silence of our professional bodies on this matter and now seek urgent clarification on their positions.
We call upon our professional bodies to publicly reject any policy of mandating COVID-19 vaccines as a condition of registration and/or deployment amongst their membership – either now or at a future point. Furthermore, we urge them to commit to protecting the right to informed consent and bodily autonomy, both for their professional membership and the clients we serve.
In particular, we would like the professional bodies to consider and respond to our professional concerns on the following points:
1. Mandatory vaccination policies conflict with our professional ethics as counsellors and psychological therapists.
One of the core principles common to the Ethical Frameworks of all our professional bodies is that of upholding client autonomy and their right to informed consent to treatment.
As health practitioners, we rightly understand that no medical or clinical intervention can be considered universally safe. We know from our own practice that even authorised, regulated and ethically sound medical treatments can still pose significant risks and have the potential to cause harm at an individual level.
As such, suitability for any medical treatment needs to be assessed on a case-by-case basis and can only be authorised with informed consent from the client (so long as they have the capacity to do so), after they have been given full and accurate information around any potential risks.
This principle of informed consent is not only vital to our ethical practice, it is upheld as a central principle within wider medical ethics and international human rights law. For example, in the UK all medical interventions in the NHS must be fully voluntary and in line with this principle of informed consent:
The decision to either consent or not to consent to treatment must be made by the person, and must not be influenced by pressure from medical staff, friends or family… If an adult has the capacity to make a voluntary and informed decision to consent to or refuse a particular treatment, their decision must be respected. [3]
In March 2015, a significant judgement about the nature of informed medical consent was made in the UK Supreme Court. [4] The court clarified that doctors must: “take reasonable care to ensure that the patient is aware of any material risks involved in any treatment,” in which, “a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is aware that the particular patient would be likely to attach significance to it”.
The court ruled that UK doctors can no longer rely on simply sharing the consensus of a body of medical opinion (‘the Bolam test’) as a basis for a patient’s informed consent, but a personalised risk assessment must be given. In the case of COVID-19 mandates, this means that generic claims that ‘the science is settled’ or ‘vaccines are safe and effective’ – cannot be used to justify their safety for an individual. [5]
The public and professional discourse on COVID-19 vaccination mandates are an example of how social pressure can be exerted on individuals to have a particular health intervention, even without a full individual risk assessment or any long-term safety data. As such, mandates can be considered medically coercive and in direct violation of the legal principle of informed consent.
We call on our professional bodies to recognise that coercion does not equal informed consent.
2. COVID-19 vaccines are far from universally ‘safe and effective’.
COVID-19 vaccinations use novel technologies which have been in widespread use for little more than a year, are still in clinical trials and for which by definition no long-term safety data is available.
Since the start of the vaccine rollout, we have already seen a significant shift from the COVID-19 jabs being promoted as being ‘safe and 100% effective’ [6][7][8][9] – to a recognition that there can be serious, even fatal side effects for a small minority of people. Their overall efficacy, especially in reducing transmission and preventing the spread of Coronavirus, is also far from what was originally hoped for.
Furthermore, since their general release, some COVID-19 injections have now been discontinued for use within certain demographics due to safety concerns. For example, the AZ and Moderna vaccines have been discontinued for young people in several countries after safety concerns arose around the risks of blood clots, following several high-profile deaths. In more recent months there have been emerging scientific studies showing the risks, particularly to younger males, of serious side effects such as myocarditis and pericarditis following vaccination, as well as ongoing concerns about the impact of vaccines on the female menstrual cycle. Both concerns have led to the commissioning of major safety investigations through additional clinical trials.
Whatever the outcome of these investigations, the fact remains that our understanding of these novel COVID-19 vaccines and the risks they pose to human health is far from comprehensive or complete.
Whenever there is risk of significant harm from a medical intervention, especially when the treatment is newly developed and those harms could be life-threatening, it is imperative that there is free choice for the individual to refuse that treatment without fear of negative consequences.
For professional bodies to require mandatory vaccination as a condition of professional registration, for acceptance on professional training courses, or as a condition of employment, would amount to unethical coercion of its professional members. To do so would place the professional bodies in direct violation of the principle of informed consent.
We ask that the professional bodies join us in speaking out against the unethical nature of mandatory vaccination policies, and publicly affirm their commitment to the ethical principle of informed medical consent.
3. Informed consent goes beyond issues of safety and risk.
As counsellors and therapists, we recognise that assessing the safety profile of a specific intervention is only one aspect of the complex decision-making process that informs our consent to medical treatment.
An individual’s moral, spiritual and political beliefs, as well as their cultural practices, life experiences and approach to managing their health, will also have an impact on their willingness to give, or withhold, informed medical consent.
Many of us take a holistic, person-centred approach to working with our clients. As such, we believe in the validity, authority and importance of these broader factors that can be drawn upon to inform medical consent. We see these wider factors as valuable, essential and equal; individuals have a right to refuse a medical treatment on wider grounds than its official safety profile or potential side effects. We are particularly concerned about the impact of mandates on those who have complex health conditions, those who have prior experiences of being harmed by medical treatments, those who favour their natural immunity, and those with religious or ethical concerns about the development process of the vaccines.
Current government guidelines for vaccine mandates only grant ‘medical exemption’ to staff with a tiny number of officially permitted medical conditions [10], with no allowance for many broader concerns that could be central to someone deciding not to consent to a COVID-19 injection. We believe that the government has no lawful right or moral authority to draw up a set of very limited medical criteria and then insist that these are the only permitted circumstances in which someone can be officially ‘exempted’ from vaccine mandates without facing redeployment or job loss.
As counsellors and psychological therapists, we uphold the right of every individual to make an informed choice about whether to take a COVID-19 vaccination, or indeed any other medical intervention, based on their own personal circumstances and medical history. We call on our professional bodies to uphold that right for practitioners and the clients we serve.
4. Professional bodies are failing in their duty of care to members who are affected by NHS vaccination mandates.
It would be incongruent for professional bodies to enshrine the principle of informed consent within their ethical codes of conduct for working with clients, whilst their professional members are not permitted to make autonomous decisions about their own medical treatment.
Mandatory vaccination policies, and the loss of the right to informed medical consent, is causing significant psychological distress to many UK counsellors and therapists, especially those working in the NHS. Many of these affected practitioners have been loyal, paying members of their respective professional bodies for decades. The silence and seeming lack of engagement from our professional bodies around this issue is both disturbing and disappointing given how severe the consequences are for members who face job loss.
The exact number of counsellors and psychological therapists who stand to be affected by NHS vaccine mandates is uncertain, as to our knowledge, there has been no formal consultation process around this issue by any of the professional bodies.
However, Therapists for Medical Freedom have now facilitated numerous free, volunteer-run support workshops for affected therapists, which have often been full to capacity. We have also had hundreds of communications from distressed members who are under significant stress from the vaccine mandate process. Many have complained to us about experiencing an utter lack of clarity, guidance or support from their professional body.
Professional bodies have a duty to represent the interests of their paying members, especially at times where their human and employment rights are under threat in a professional context.
Therapists affected by vaccine mandates deserve better treatment and representation than they are currently getting from professional bodies. This situation must change, and we appeal to professional bodies to address this with the utmost urgency.
5. Vaccine mandates will have negative consequences for clients accessing therapeutic services.
NHS England estimated that had the vaccine mandate policy been implemented in April as planned, this would have left the NHS down by at least 80,000 staff, as many planned to leave the profession rather than comply with the policy. [11]. This number would increase exponentially if vaccines were mandated as part of the professional registration process, thereby affecting health professionals working outside of NHS services, which applies to most therapists and counsellors in the UK.
To lose a significant number of counsellors and therapists at a time of national crisis could pose significant harm to clients. COVID-19 and the wide-ranging impact of restrictions on the population has left a legacy of new and worsening existing mental health problems. The Centre for Mental Health estimates that 8 million adults and 1.5 million children will need mental health support in the years following the pandemic. [12]
Those of us who have worked to provide psychological therapies throughout this challenging time are now seeing an unprecedented rise in demand for NHS and voluntary sector counselling and therapy services, to the point where people in need now face dangerously long waiting times. [13] Across the UK, even private therapy services and individual practitioners are in short supply, with many having to make difficult decisions to turn away people in need because they simply do not have the resources to treat them. At a time of increased mental health need, vaccine mandates would therefore be detrimental for current and future clients.
We call upon the professional bodies to provide reassurance that clients’ access to therapeutic support will not be restricted based on vaccination status, either now or in the future. We also call on them to reject policies that will risk the loss of experienced practitioners, put further strain on existing services and staff, and potentially dissuade others from training to enter the field.
6. It is essential to consider the wider context to mandatory vaccination policies and to remember the lessons of history.
As counsellors and psychological therapists, when faced with an ethical dilemma, we are encouraged to look beyond the issue itself and consider the wider field and context – including any relevant historical, sociological and political factors. Therefore, when considering the ethics of vaccine mandates, we must consider more than just the risk posed by COVID-19 vs the benefits and risks of vaccination.
When we step back and consider the wider socio-political context, we can clearly see that:
- Governments do not always act in the best interests of the public they are appointed to serve, whatever their political rhetoric might be. We are seeing numerous examples of this emerging now, for example the conflicts of interests in the awarding of PPE contracts and the flouting of COVID-19 rules by senior government figures. [14]
- There have been numerous instances in human history, especially at times of ‘national emergency’, where government bodies have actively lied to the population, exploited the situation to further their own aims, or have sought to conceal important information, especially when it could harm their wider political agenda. [15][16][17]
- The health care system has a long history of being vulnerable to exploitation by political lobbyists, corporate donors or becoming compromised by internal pressures from within government or from regulatory bodies. Consider examples from our recent history – public health advice given to reassure the public of the safety of tobacco, pesticides, GMOs – which have later been proven to be manifestly unsafe, despite the proclamations of the government-sanctioned public health experts of the time. [18][19][20]
- Many authorised medical treatments have later been discovered to be causing significant harm to human health and have been withdrawn from public use, despite having passed required safety checks and being widely embraced by the medical orthodoxy of the time. [21][22][23]
- We are being exhorted to “trust the science” when there is no such thing as ‘the’ science. Rather, science has always comprised a breadth of opinions, conclusions, methods and ethical standpoints. History has shown us that public trust has not always been as safe as we would hope for in the hands of scientists and medical professionals, especially when there are financial interests at stake. [24][25]
- Politicians, pharmaceutical companies, peer-reviewed medical research, clinical trials, regulatory bodies and individual expert opinion – all of these are vulnerable to human error, corruption and conflicts of interest which are not always declared or formalised. [26][27][28]
In the context of our collective history, as ethical health practitioners, we have a responsibility to ask difficult questions if we see draconian policies such as vaccination mandates being introduced in our society. We must continue to think critically about who would profit and benefit most from such policies. Might there also be vested interests, whether in government, science and medicine or the pharmaceutical industry, that could stand in the way of open and transparent discussion? [29][30]
It is not the terrain of ‘conspiracy theory’ for therapists and other health professionals to demand that government and medical experts are scrutinised and held to account for the policies they impose upon the public. As a profession, we must make room for alternative perspectives and difficult questions without these legitimate concerns being dismissed or slandered as ‘anti vax’, ‘dangerous disinformation’ or even more alarmingly, as ‘far-right extremism’.
It is not acceptable for our Professional Bodies to simply dismiss or silence any dissenting voices within their membership, or to ignore these difficult questions. Nor is it acceptable for heavy-handed policies such as COVID-19 vaccine mandates to be supported and justified by our professional bodies on the sole basis that they are acting in line with ‘official legislation or government guidance’ without any independent analysis of the actual effectiveness, ethics, or impact of the guidelines – or any acknowledgement that governments do not always act solely in the public interest.
Our professional bodies have a duty to carefully scrutinise any mandated public health measures that compromise our medical autonomy. They must not be accepted on face value as being in the public interest simply based on the assurances of government and its approved health advisors, or pharmaceutical companies with vested interests.
Recommended Actions:
It is time for the professional bodies who represent counsellors and psychological therapists in the UK to show courage and break their collective silence on the issue of mandatory vaccination in our profession.
In light of all the above, we call on our professional bodies to:
- Uphold the values that are written and protected within their own ethical codes by publicly affirming their commitment to protecting the right of therapists and clients to freely give or withhold their consent to medical treatment without fear of coercion or punishment.
- Affirm that their commitment to upholding the right to informed consent will stand regardless of the emergence of new future variants, waves of disease or novel medical treatments.
- Engage with Therapists for Medical Freedom and other groups of concerned professionals in a process of dialogue around the ethics and legality of vaccine mandates in our profession.
- Pledge to protect the rights of therapists and clients who have exercised their lawful right to informed consent to refuse COVID-19 vaccinations.
- Use their authority as professional membership bodies to prohibit the implementation of discriminatory policies around COVID-19 vaccinations within their organisational membership and associated training institutes – and to publicly speak out against such discriminatory practices in the wider field.
- Remind their members that we each have an ethical responsibility to think critically for ourselves when assessing any government health advice, especially when it is mandated. Professional bodies should help facilitate this broader risk assessment process within their membership, especially the potentially negative impact that any existing or future public health advice might have on practitioners and clients.
- Take into account the broader historical, social and political context when assessing the ethics of mandatory health interventions. We cannot forget the harm that has been caused to human health and civil liberties when the right to refuse medical treatment has been denied to populations at other times in history.
We await to hear your considered responses on these important matters of professional ethics, legislation and human rights, and look forward to beginning a process of dialogue with you.
Yours sincerely,
Therapists for Medical Freedom
Principal Signatories:
Jennifer Ayling, Psychotherapeutic Counsellor, UKCP
Clare Beatson, Counsellor, BACP
Elizabeth Bentley, Psychotherapist, BACP
Johann Burton, Counsellor, NCS
Paula Charnley, Counsellor, BACP
Ben Harris, Psychotherapist, MBACP
Julie Horsley, Counsellor, NCS
Frances Kandler-Singer, Psychotherapist, BACP
Naintara Land, Psychotherapist, UKCP
Rachel Maisey, Counsellor, BACP
Kate Morrissey, Psychotherapist, BACP
Melanie Pickles, Counsellor, BACP
Dr. Bruce Scott, Psychoanalyst, UKCP & CP-UK
Dr. Gary Sidley, Clinical Psychologist (Retired)
Deborah Short, Psychotherapist, UKCP
Elizabeth Smith, Psychotherapist, Pre-Accred
Leanne Ward, Clinical Psychologist, HCPC
Sarah Waters, Psychotherapist, MBACP
Supporting Signatories:
Marc Allen, Trainee Therapist, Pre-Accred
John Bates, Psychotherapist, UKCP
Antoine Bowes, Counsellor, BACP
Dr. Faye Bellanca, Clinical Psychologist, HCPC
Caroline Brett, Psychotherapist, BACP
Jacqueline O’Brien, Psychotherapist, (retired)
Sheila Burchell, Clinical Psychologist, HCPC
Dr. Erika Filova, Clinical Psychologist, HCPC
Dr. June Golding, Psychotherapist, UKCP
Andrew Harry, Counsellor, UKPTA
Susan Hayes, Psychotherapist
Jessica Horton, Counsellor, BACP & BPS
Isla Hunter, Psychotherapist, BABCP
Gabrielle Lake Mitchell, Trainee Therapist, BACP
Maggie Leathley, Psychotherapist, BACP
Jane Margerison, Psychotherapist, BACP
Jonathan Martin, Psychotherapist, UKCP
Gary McKeever, Counsellor, BACP
Caroline Montanaro, Psychotherapist, UKCP
Dr. Naomi Murphy, Clinical Psychologist, HCPC & A-CP
Dr. Rachel Newton, Clinical Psychologist, HCPC & BPS
Sue Parker Hall, Psychotherapist, UKCP
Kay Parkinson, Psychotherapist, UKCP
Dr. Helen Payne, Psychotherapist, UKCP & ADMP UK
Carolyn Polunin, Psychotherapist, UKCP
Dr. Kate Porter, Clinical Psychologist, HCPC
Tracy Rees, Trainee Therapist, Pre-Accred
Dr. Helen Ross, Clinical Psychologist, HCPC
David Scott, Clinical Psychologist, HCPC
Patricia Taddei, Psychotherapist, UKCP
Dr. Lucie Turner, Clinical Psychologist, HCPC
Dr. Alice Welham, Clinical Psychologist, HCPC
Tracy Williams, Counsellor, BACP
Dominique Wynn, Psychotherapist, (Retired)
Sign the Open Letter
Are you a Counsellor, Psychotherapist or Clinical Psychologist based in the UK who is concerned about the impact of vaccine mandates on the profession? (whether you are personally vaccinated or not).
If so, please sign the letter.
Most Published Studies Exaggerated the Effects of Ocean Acidification – and Covid, Etc.
By Jennifer Marohasy | February 20, 2022
The concept of ocean acidification, and human-caused global warming more generally, could be described as containing a grain of truth embedded in a mountain of nonsense. Indeed, the projected large increase in atmospheric CO2 will at most cause a small reduction in pH – it will not turn the ocean acidic. Yet this is what is implied by the term ocean acidification. True acidification would require average pH to be reduced below 7.0, at which point seashells would indeed begin to dissolve. This is an impossible scenario, however, because of the ocean’s effectively limitless buffering capacity.
There is a newly published study by Jeff Clements and team that concludes many of the published studies on ocean acidification, especially those studies published in high impact journals and accompanied by sensational media reporting, have turned-out to be wrong, or at least exaggerated.
My colleague Peter Ridd describes the situation:
This problem with exaggeration of threats applies to many areas of science and has a name: The Decline Effect.
The Decline Effect goes like this: an early report, usually attracting huge media interest, predicts some sort of catastrophe. But when follow up work is done, usually with far better experimental procedure and far greater numbers of samples, the original report turns out to be wrong.
Jeff Clements’ team included Timothy Clark, Josefin Sundin and Frederik Jutfelt who were involved in a study last year proving that numerous reports by James Cook University’s coral reef centres on reef fish was totally wrong.
I co-authored a book chapter with John Abbot some years ago that explained:
Initial concerns about ocean acidification focused on organisms that construct their shells or skeletons from calcium carbonate. Such organisms are referred to as marine calcifiers and include not only corals, but also crabs, clams and conchs (sea snails).
Theoretically, and according to popular science magazines, all corals are already severely and negatively affected by ocean acidification. But this is not evident from methodologically sound studies undertaken at the Great Barrier Reef. A review of the growth rates of six, hard coral species at Lord Howe Island (Anderson et al. 2015) found marked variation in the growth rates of branching coral, while growth rates of the massive Porites coral were unchanged. The researchers suggested that a decline in the growth rates of the branching species could be attributable to a reduction in the calcium carbonate saturation state as a consequence of higher summer temperatures. A study measuring calcification rates for 41 long-lived Porites corals from seven reefs from the central Great Barrier Reef (D’Olivio et al. 2009), showed good recovery from the major 1998 bleaching event, with no significant trend in calcification rates for the inner reefs. Corals from the mid-shelf central Great Barrier Reef, however, did show a decline of 3.3%.
While most ocean acidification research has been focused on physiological processes, in particular calcification, there have also been studies on three common hard corals to look at their fertilisation, embryonic development, larval survivorship, and metamorphosis (Chua et al. 2013a; Chua et al. 2013b). These studies have found the early life-history stages were unaffected by reduced pH; there was no consistent effect of elevated CO2 alone, nor in combination with temperature.
Studies of the effect of very high CO2 levels (up to 2,850 ppm) on molluscs – including oysters, clams, scallops and conchs – have shown that these species will generally build their shells more slowly as CO2 levels increase (Ries et al. 2009). This same study showed that crabs and lobsters respond quite differently to the same elevated CO2 levels, showing a general increase in calcification rates.
This chart shows how quickly scientists could meet the demand for commentary in the new area of ocean acidification, including to support the theory of human-caused global warming.
The varied responses among different organisms reflect their differing abilities to regulate pH at the site of calcification, and:
- the extent to which their outer shell layer is protected by an organic covering
- the solubility of their shell, or skeletal mineral
- the extent to which they use photosynthesis (Ries et al. 2009).
Of course, many marine organisms are not calcifiers, and some of these organisms have also been tested for a response to ocean acidification.
When seagrasses collected from three locations in the Great Barrier Reef region – Cockle Bay, Magnetic Island, and Green Island – were exposed to four different CO2 concentration levels for two weeks – with water temperature and salinity in the experimental tanks near-constant throughout – all three seagrass species exhibited enhanced photosynthetic responses (Ow et al. 2015). That is growth rates, observed after two weeks of exposure to an enriched CO2 environment in an indoor aquarium, were higher. This suggests that ocean acidification could mean more seagrass, which would be good for large marine mammals like dugongs (dugongs are vulnerable to extinction because of issues unrelated to changing ocean chemistry).
Also, contrary to expectations, laboratory investigations into the effects of three different CO2 treatments on anemonefish (commonly known as the clownfish) found that higher CO2 levels stimulated breeding activity (Miller et al. 2013). The breeding pairs from the fringing reefs of Orpheus Island on the Great Barrier Reef, where they are exposed to the highest CO2 levels, produced double the number of clutches per breeding pair, and 67% more eggs per clutch than the control. However, young anemonefish that were bred in high CO2 levels and high temperatures showed decreases in their length, weight, condition, and survival (Miller et al. 2012). Though these effects were absent or reversed when their parents also experienced the higher concentrations (Miller et al. 2013).

We concluded:
Most studies have been on single species in contrived laboratory conditions. They have been of short duration, and they have not considered the potential for adaptation. In the few instances where adaptation has been considered, it has been shown to significantly modify the impact of varying pH as a consequence of elevated levels of CO2.
All of this needs to be assessed against the reality that along the length and breadth of the Great Barrier Reef there are naturally occurring large daily fluctuations in pH, and that it is unclear as to what extent the current trends of apparent pH decline are part of existing natural cycles.
Most of the articles describe the effects of changes of pH on biological organisms; many of the claims are based exclusively on laboratory experiments (Riebesell & Gattuso 2015). However, a problem with laboratory experiments is that they cannot capture the complexities of the real world, not even the tremendous natural variability in ocean pH – which is a measure of ocean acidification.
Statistician John P.A. Ioannidis published a review of medical research back in 2005 entitled ‘Why most published research findings are false’ (Plos Medicine ). It included a comment that:
The majority of modern biomedical research is operating in areas with very low pre- and post-study probability for true findings.
The review by John Ioannidis is a devastating critic of the sad state of biomedical research. It is this same profession, biomedical research, that concluded we should fear Covid-19 and get vaccinated – with the results from the Pfizer trials withheld while emergency approvals were granted for the mass vaccination of citizens across the world against Covid-19.
We will no doubt have better insights, when studies like those by Jeff Clements into ocean acidification, are undertaken into the recent Covid-19 vaccine research. We may then be in a position to judge whether the apparent ineffectiveness of these particular Covid-19 vaccines, despite all the promises, can be best explained by corporate greed and mendacity, or simply flaws in the scientific method. Certainly there was pressure on medical researchers to find a quick cure, that could be administered as part of a global public health response, to what appeared in the beginning to be a deadly new virus much worse than the seasonal flu.
The British Medical Journal in an editorial dated 19thJanuary includes commentary that we don’t know enough about Covid-19 vaccines.
‘Today, despite the global rollout of Covid-19 vaccines and treatments, the anonymised participant-level data underlying the trials for these new products remain inaccessible to doctors, researchers, and the public—and are likely to remain that way for years to come,’ the editorial states. ‘This is morally indefensible for all trials, but especially for those involving major public health interventions.’
The editorial also accuses pharmaceutical companies of ‘reaping vast profits without adequate independent scrutiny of their scientific claims,’ pointing to Pfizer, whose Covid vaccine trial was ‘funded by the company and designed, run, analysed, and authored by Pfizer employees’.
Of course, Peter Ridd lost his job at James Cook University for speaking truth to power. Those who continue to publish studies on ocean acidification, especially those studies published in high impact journals and accompanied by sensational media reporting, have most recently been rewarded by the Australian government with an additional $1billion in funding. Some of this money will end-up funding more nonsense ocean acidification projects at James Cook University. It is unlikely that any of this grant money will be used to ensure that there is some quality assurance of the same research.
Featured Video

The Sordid History of the CIA – Part 3
or go to
Aletho News Archives – Video-Images
From the Archives
The Mysterious Death of UN Secretary General Dag Hammarskjold
By Lisa Pease | Consortium News | September 16, 2013
More than a half century ago, just after midnight on Sept. 18, 1961, the plane carrying UN Secretary-General Dag Hammarskjöld and 15 others went down in a plane crash over Northern Rhodesia (now Zambia). All 16 died, but the facts of the crash were provocatively mysterious. … continue
Blog Roll
 Aletho News
Aletho News- The Sordid History of the CIA – Part 3
- West Bank is Defenseless – This is Why Israeli Settler Attacks Continue
- Systematic Israeli targeting of Gaza police seen as deliberate prelude to chaos
- Netanyahu destabilizing region, US hindering talks: Pakistani official
- Iran FM to hold no talks with Americans in Islamabad; US media lied again: Report
- When It Comes to Using Proxies, The US Far Surpasses Iran as a Sponsor of Terrorism
- Hidden history: How Mossad infiltrated Italy
- Promises, pressure, pullout: Why US nuclear talks with Iran were never about a deal
- Somalia bans Israeli-linked vessels from Bab al-Mandab Strait
- ‘Profound moral failure’: Iran denounces US endorsement of assassinations amid fragile ceasefire
- If Americans Knew
- Christians in Israel and Palestine, past and present
- Israel eager to restart Iran war, Gaza genocide – Daily Update
- Meet the Top “Content” Producers Linked to Canary Mission
- Lebanese Journalist Amal Khalil Bombed and Left to Die by Israel
- Israel Moves to Re-establish Ganim Colony In Jenin
- Two Iranian Women in ICE Detention Are Not, In Fact, Related to Qasem Soleimani, Documents Show
- “The shooting was not in the air”: Testimonies from the Flour Massacre
- Israel chases down, kills Lebanese journalist, massacres 5 in Gaza, all during “ceasefires” – Daily Update
- Gaza’s unseen casualties: A surge in stillbirths and birth defects
- ‘Day of Ordinary Terror’: Israeli Attack on West Bank School Kills Man, Child
- No Tricks Zone
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
