CDC REFUSING TO PUBLISH DATA
And:
BY JEFFREY A. TUCKER | BROWNSTONE INSTITUTE | FEBRUARY 26, 2022
One day I’m reading an internal memo commissioned by the Democratic Party to provide advice to dealing with Covid policy. The next day I’m reading headlines about how the CDC has drastically altered its advice on how to deal with Covid.
Is there a relationship? At this point, only the hopelessly naive would think otherwise.
Let’s look at the memo produced by Impact Research. Some excerpts:
A few points.
This memo is not epidemiology but politics, most strongly illustrated by the idea that polling should make the difference as to whether a pathogen is pandemic or endemic. The constant incantation of “vaccines” here has nothing to do with the known data: they have nowhere stopped infection or spread, a point which the memo obscures with the line about how they “minimize illness.” They minimize serious outcomes for some strains so long as they last.
From a policy point of view, there are two main features that stand out: Covid is here to stay and “most people in the US will eventually get COVID-19” (thereby hinting at the reality that vaccines are not effective in the way that Biden/Fauci/Walensky promised) and therefore the focus should be on protecting the vulnerable.
There is nothing new about this. It was always true! You can shout “Omicron” all day but it was also true with Alpha and Delta as well. The virus should have been treated rationally the entire time and policies that have wrecked public health should have been off the table from 2020. The memo writers did not cite the Great Barrington Declaration but they might as well have.
As for how the Democrats somehow prevented an economic freefall, the worst economic outcomes are very clearly in Democratic-controlled states that retained restrictions for nearly two years in some places, including keeping schools closed. There is a reason for the mass migration that this has inspired.
If we are looking for thriving economies, look to the states that never closed up or opened earliest: South Dakota, Florida, Texas, Georgia, and so on. So none of this is remotely true but, hey, this is politics, right?, so it doesn’t have to be true.
The real problem that the Democrats need to solve is revealed in this chart:

Now, let us consider the dramatic turnaround at the CDC that came out the very next day. The full PDF is embedded below.
Here are the talking points handed to the director. It’s not just about masking, which is being relaxed. The CDC says there needs to be a dramatic shift away from endless monitoring of cases that are overwhelmingly mild and instead focus only on actual sickness that lands people in the hospital and threatens life. We need to stop obsessing about cases and start looking mainly at “medically significant disease.” The focus should be on “protecting the most vulnerable.”
This makes all of us want to say, shout, scream: THANK YOU!
In order to justify this change, the CDC posts four sets of charts on Covid prevalence during episodes of the pandemic. The last chart illustrates the point that an exclusive focus on controlling the spread is utterly preposterous at this point. Under the old protocols, the whole country should be back in lockdown. It’s unimaginable what attempting this now would cause.

To be sure, all of this is enormously frustrating for those of us engaged in this battle for two years. Instead of focusing on getting sick people well, the CDC experimented with wild guidelines that imagined some kind of society-wide solution that seemed designed to crush the virus while vast amounts of social and economic activity were shut down by law. This necessitated a crushing of freedoms, including of travel, association, commerce, religion, and, eventually even speech.
The CDC nowhere admits this much less apologizes for it. Two years in, the CDC seems to have rediscovered the traditional practice of public health, and has justified this new wisdom based on changed conditions, while never even bothering to claim that its previous measures and guidelines achieved anything along the way.
We’ve seen a massive collapse in public health, economic vitality, and essential rights, while closing schools and wrecking education and so much more, all in the name of virus control, even as the evidence is now overwhelming that the entire enterprise was not only a distraction from what should have happened (therapeutics and protecting the vulnerable) but also an astonishing failure.
Why the change? It had to happen at some point. The entire machinery of lockdowns and mandates were destined to fail. As to the timing of the reversal, it’s hard to resist the speculation that it is entirely political. See the memo above.
Still, there is a worrisome aspect to the CDC’s announcement. They reserve the right to do it all over again. “We want to give people a break from things like mask-wearing, when these metrics are better, and then have the ability to reach for them again should things worsen,” she said.
No one should be satisfied with a politically motivated change in the messaging. We need fundamental regime change to make sure that nothing like this can ever happen again.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
The Highwire with Del Bigtree | February 24, 2022
Freedom Convoy USA 2022 Organizer, Kyle Sefcik, went viral this week with his video message to President Biden to end the mandates, and his plan for peaceful protest of the draconian measures.
Convoy updates.
#FreedomConvoyUSA #KyleSefcik #TruckerConvoy #FreedomConvoyUSA2022
See also:
BY IAN MILLER | BROWNSTONE INSTITUTE | FEBRUARY 26, 2022
An infuriatingly consistent aspect of the mainstream media’s COVID coverage was their determination to prematurely credit a country with a wildly successful set of policy interventions.
While there has been no track record of universally accurate predictions or expectations, the desire to claim victory as far back as spring 2020 has led to subsequent embarrassments as trends change.
Naturally, New Zealand is no stranger to such untimely praise, with the BBC in July 2020 doing an in-depth look at how New Zealand became “COVID free.”
Of course, it was because New Zealand “… locked down early and aimed for elimination” and achieved “effective communication and public compliance.”
This is really the whole problem in a nutshell, isn’t it?
Assuming that elimination was possible through effective communication, compliance and early lockdowns ignores the inevitably that COVID will eventually spread throughout the population, whenever you “open up.”
Elimination of COVID throughout the world is and always was impossible, and therefore Fauci’s assertion that COVID could be “eliminated in certain countries” was inane and virtually impossible.
So how successful has New Zealand been in eliminating COVID in the long term through effective communication, public compliance and early lockdowns?
Well. The numbers speak for themselves.

When the BBC wrote the article explaining New Zealand’s remarkable success in eliminating the virus, they were averaging 1.5 cases each day. It’s now 2,918 cases each day.
That’s an increase of nearly 195,000%.
Elimination is a pipe dream.
No matter what policy interventions they’ve added, no matter how many early lockdowns they’ve tried, COVID has not been eliminated.
Remember how New Zealand’s amazing tracking and tracing system allowed them to identify transmission that could have only occurred via aerosols? And recall how all of the pre-pandemic guidance on masking suggested that masks could not stop aerosols? Did that stop New Zealand from using mask mandates to try and continue their elimination goals?
Of course not!
The following are the currently enforced rules on face masks in New Zealand:
We know New Zealanders are complying because the BBC assured us that their success was due to population compliance, but the survey data backs that up as well:

Mask wearing has been consistently high since the mandate came into effect in August, yet cases have exploded anyway.
None of it has mattered.
And this isn’t an insignificant increase. New Zealand’s now reporting more new cases adjusted for population than the United States, and identical numbers to the United Kingdom:

Working perfectly!
Elimination Through Vaccination
In the previously referenced interview, Fauci said that the most successful way to “eliminate” COVID was to reach extraordinary levels of vaccination uptake in the population.
While the Our World in Data download hasn’t been updated in the past week, over 88% of the population had received at least one vaccination dose in New Zealand by February 15th.
The numbers are even more impressive when considering only those over 12 years of age. 95% of everyone over in that demographic has been at least partially vaccinated or booked their appointment. 94% are fully vaccinated:

Nearly 2.3 million people over 12 have been given boosters, roughly 53% of that entire population.
Clearly those incredible rates of uptake must have been enough to maintain the “blanket of herd immunity” that Fauci claimed would be achievable with 75-85% of the population vaccinated.

Not exactly!
Whenever you reference the dramatic failure of Australia or New Zealand to maintain “zero COVID” lockdowns and “elimination” strategies, adherents to the cult of inaccurate expertise will respond by claiming their goal was only to eliminate cases until widespread vaccination.
By allowing for vaccines to blunt the impact of cases, these countries would prevent surges in hospitalizations. We already saw that this was wildly off in Australia:

But what about New Zealand? Maybe they’ve been able to successfully stave off any surge in severe cases due to their exceptional vaccination rate:

Well. Not exactly.
Hospitalizations have risen dramatically since January and continue to rise significantly each day.
News reports from New Zealand sound like those from any generic location in the US where local doctors report concerns of hospitals being overwhelmed:
Authorities anticipate Omicron will become the predominant Covid-19 variant in New Zealand within just two to four weeks of it being introduced into the community – and hospitals are bracing to be “swamped”.
Dr John Bonning, a frontline emergency department doctor and immediate past president of the Australasian College for Emergency Medicine, said EDs were already under “enormous duress”.
So their elimination strategy did not prevent a dramatic increase in cases, nor a concerning, overwhelming surge of hospitalizations.
And deaths, while thankfully still low, have increased in recent months as well:

New Zealand’s supposed “elimination” through their zero COVID policy has completely collapsed.
Mask mandates, as their own research indicated, have not prevented surges. Elimination until vaccination has not prevented surges. Zero COVID has been an unmitigated failure, as any rational person would have known and suggested as far back as summer 2020.
They’ve maintained an unearned sense of superiority, exemplified in this quote from the BBC’s story:
He says it is “a bit of a puzzle for us at a distance to understand why” with the UK’s extensive scientific expertise and health care, “you haven’t looked at the evidence and worked out a pattern like New Zealand’s”.
The UK government has previously defended its coronavirus strategy, saying its approach was “being guided by the science.”
That undeserved attitude can no longer be maintained.
The policies that never had the slightest possibility of long term success, the policies that Fauci claimed could be successful in “certain countries,” have turned into yet another example of the delusions of hubris.
While many areas are lifting mandates, they’re doing so without acknowledging the underlying flaws in their strategy. Iceland’s health ministry summed up the inescapable reality of COVID while announcing an end to all restrictions:
“Widespread societal resistance to COVID-19 is the main route out of the epidemic,” the ministry said in a statement, citing infectious disease authorities.
“To achieve this, as many people as possible need to be infected with the virus as the vaccines are not enough, even though they provide good protection against serious illness,” it added.
Until they understand and accept those sentiments, there will always be excuses for politicians and public health officials to bring back their prized, ineffectual interventions.
New Zealand is the latest in a long list of countries to be hailed as showing the world the “right” way to prevent surges; to keep COVID under control.
But as with masks, vaccine passports and “early” lockdowns, zero COVID never had a chance of working — despite the endless media and expert praise.
As always, Eric Feigl-Ding had absolutely no idea what he was talking about:

It is time for a taste of its own medicine
By Vinay Prasad MD MPH | February 26, 2022
Just yesterday, I read that NYC public schools will remove the OUTDOOR mask mandate starting Monday. How Brave!
Let’s reflect on this for a moment. NYC school district has been requiring children wear masks OUTSIDE all this time. Years after we knew the virus almost never spreads outside. During recess when kids play, forced to wear a mask while exerting themselves. Wow!
Whoever made the policy is an idiot. No way around it. They are not fit for policymaking. They abused the power of government to coerce children (at incredibly low risk of bad outcomes) to wear a mask in a setting where the virus simply does not spread. In other words, they participated in something done in the name of public health, which actually made human beings worse off. Worse, they used coercive force to do it.
Post-COVID we need to seriously talk about setting restrictions. But not on people. We need to place restrictions on public health and things done in the name of public health. We cannot allow individuals who are poor at weighing risk and benefit and uncertainty to coerce human beings, disproportionately the young and powerless (waiters/ servers) to participate in interventions that have no data supporting them, for years on end.
Public health be the subject of restrictions; a taste of its own medicine. Some of those restrictions should be placed on governments, but others on private actors who are appealing to public health. Here is what that might look like:
Cal Academy is a museum in Golden Gate Park. Do they have any business nor ability to mandate boosters in adolescents? No, it is absurd. Two senior officials with the FDA— Gruber and Krause- resigned over this decision. Paul Offit and Luciano Boro and others have been publicly critical of boosters for young people, and Cal Academy mandates it? Cal Academy is not qualified to make this decision.
These are just a few examples of where governments or institutions have overreached in the name of public health, but there are many more. Post COVID, the group that needs to face the strongest restrictions is public health itself. We must careful remove the power we have granted public health, which has often been misused.
Vinay Prasad MD MPH is a hematologist-oncologist and Associate Professor in the Department of Epidemiology and Biostatistics at the University of California San Francisco. He runs the VKPrasad lab at UCSF, which studies cancer drugs, health policy, clinical trials and better decision making. He is author of over 300 academic articles, and the books Ending Medical Reversal (2015), and Malignant (2020).
Professor Sunetra Gupta explains the concept of herd immunity threshold and how seasonality affects the way a virus spreads.
Collateral Global | February 16, 2022
Transcript
Many viruses are better able to spread at particular times of the year. How does this seasonality in transmission affect the way that a new virus will spread through the population?
In order to answer this question, we need to first understand the concept of a herd immunity threshold.
Herd immunity refers to the accumulation of immune individuals in a population.
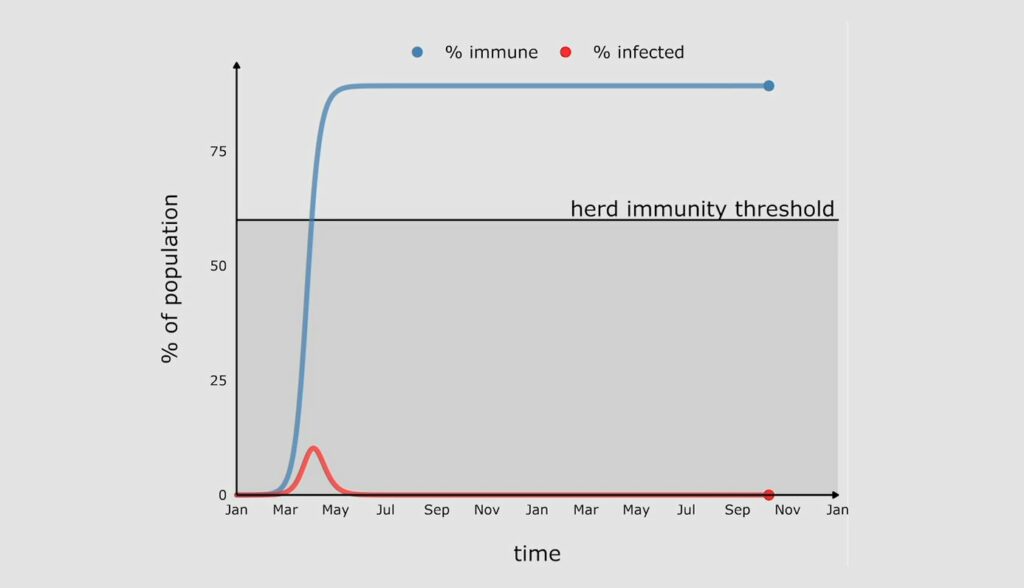
When a new virus enters a population, it muddles along for a while, and then it really starts to take off, as you can see here in this red line, which is tracking the proportion of the population infected by this new virus. And as you can see, after a while, this peaks, and the proportion infected starts to come down again.

Now why does that happen? This is because once people recover from infection, they become immune, and this means that the virus starts to run out of susceptible people to infect. The blue line here is showing you how the proportion immune is growing at the same time.
There comes a point when the proportion of the population immune is high enough that the rate of growth of infection become negative, and that’s when the virus hits peak and the infections start to decline. This occurs when the proportion of the population immune has crossed a threshold, which is known as the herd immunity threshold. That herd immunity threshold is determined by the fundamental transmissibility of the pathogen itself.
If there’s no loss of immunity, the proportion immune, this blue line, will stay above the herd immunity threshold, which means that no new epidemics can occur and the virus will die out.
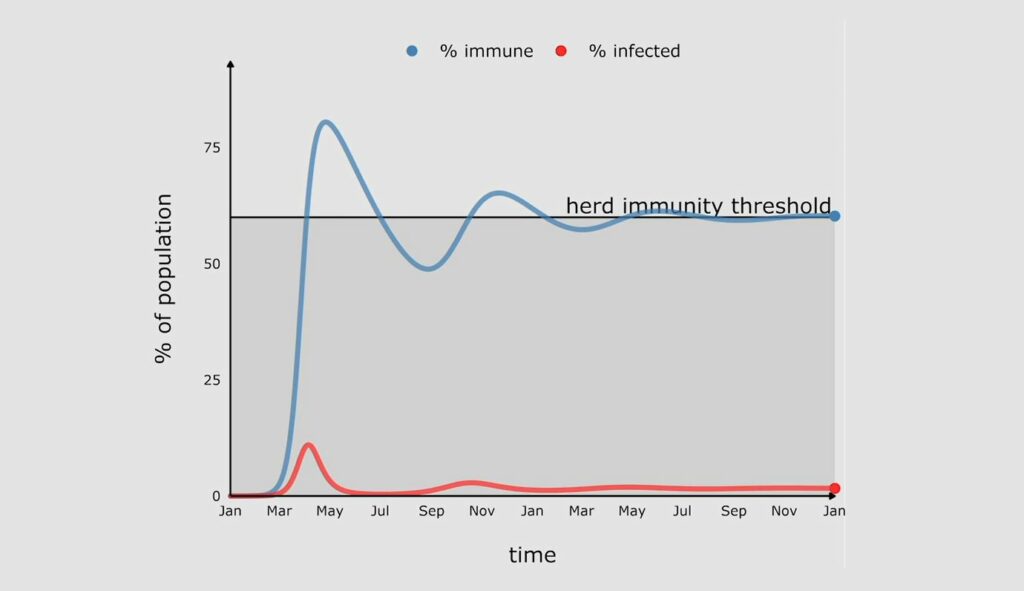
In reality the proportion immune will decline with time. For viruses like measles which give you lifelong immunity against infection, this will happen at a very slow pace. For many other viruses, like the coronaviruses, immunity against infection declines on a much shorter timescale. And as soon as it dips below the herd immunity threshold, infections will start to climb again, and we will see a second wave.

The second wave is smaller than the first wave because this time the gap between the proportion immune and the herd immunity threshold is much smaller and therefore more quickly closed.
The other thing to note about the second wave is that many infections are actually reinfections, so people who’ve lost immunity are becoming infected again. What this means is that the rates of severe disease and death are likely much lower, because people will retain the ability to resist disease even though they have lost their ability to resist infection.
Further waves will occur when the proportion immune falls below the herd immunity threshold again, but the gaps will get smaller and smaller and the waves will get smaller and smaller until they sort of flatten out at an endemic equilibrium.
Now let’s go back to our original question. What happens if there is seasonality in transmission?
As I’ve just explained, the herd immunity threshold is strongly dependent on the transmissibility of the virus, so as the transmissibility goes up and down with seasons, so will the herd immunity threshold. And that’s what’s show here by the gradated area.

So now you see a more complex picture emerging which is the result of an interaction between waning immunity and the changes in the herd immunity threshold.
After the first peak, immunity wanes, but because the herd immunity threshold is also declining it takes longer for the blue line to dip below the herd immunity threshold. And so the next peak is delayed. Eventually this settles into a pattern which is characteristic of the seasonal respiratory viruses which we live with at endemic equilibrium.
Without seasonality it doesn’t make much of a difference at what time of the year the virus arrives. But when you have seasonality in transmission, it makes a really big difference.
A virus that arrives just before peak season will have a very big first wave, because the proportion immune will have to reach a very high herd immunity threshold before we see a decline in infections.

But if the virus arrives in a low season, the first wave could be quite small because the proportion immune only has to reach that lower herd immunity threshold before a turning point occurs.

However, as the herd immunity threshold starts to climb again, we will get a second wave in order to catch up with the new higher herd immunity threshold. And in some instances this could actually be larger than the first wave.
Of course the virus could arrive at different times of the year in different regions of the same country. What that means is lumping all these patterns together can be quite misleading.
Eventually all viruses will reach a state of endemic equilibrium, but their journey to that state from the point of introduction depends crucially on the rate at which infection blocking immunity decays for that particular virus as well as seasonality in transmission.

Sunetra Gupta is Professor of Theoretical Epidemiology in the Department of Zoology, University of Oxford and a member of Collateral Global’s Scientific Advisory Board.
By Professor Paul R. Goddard | GM Watch | February 19, 2022
Two myths have hindered investigations into the origins of the SARS-CoV-2 virus: one, that viruses seldom escape from laboratories; and two, that most pandemics are zoonotic, caused by a natural spillover of a virus from animals to humans.
Promoters of the first myth include the World Health Organization (WHO). At a press conference in Wuhan, China, in February 2021, Peter Ben Embarek, the head of the WHO inspection team tasked with looking into the origins of the virus, said it was “extremely unlikely” that it had leaked from a lab and as a result the lab escape hypothesis would no longer form part of the WHO’s continuing investigations.[1]
Dr Peter Daszak, president of the EcoHealth Alliance, has promoted both myths. As long ago as 2012, Dr Daszak co-authored a paper in The Lancet claiming that “Most pandemics – e.g. HIV/AIDS, severe acute respiratory syndrome, pandemic influenza – originate in animals”.[2] Since the start of the pandemic, he has claimed that “lab accidents are extremely rare”, and that they “have never led to large scale [disease] outbreaks”. He also said that suggestions that SARS-CoV-2 might have come out of a lab are “preposterous”, “baseless”, “crackpot”, “conspiracy theories”, and “pure baloney”.[3]
In September 2020 Dr Anthony Fauci, director of the US National Institutes of Health’s (NIH) National Institute of Allergy and Infectious Diseases (NIAID), and his co-author wrote in a paper about COVID’s origins, “Infectious diseases prevalent in humans and animals are caused by pathogens that once emerged from other animal hosts.”[4] Fauci has tried to quash the notion that SARS-CoV-2 could have come from a lab. In May 2020 he said that the virus “could not have been artificially or deliberately manipulated” and in October 2020 that year that the lab leak theory was “molecularly impossible”.[5]
But emails uncovered this year by a Freedom of Information request in the US reveal a wide gap between what Fauci was being told by experts about the virus’s origins and what he was saying publicly. In January 2020, a group of four virologists led by Kristian G. Andersen of the Scripps Research Institute told Fauci that they all “find the genome inconsistent with expectations from evolutionary theory”[6] – in other words, it likely didn’t come from nature and could have come from a lab.
Fauci hastily convened a teleconference with the virologists on 1 February 2020.[7] As the New York Post reported, “Something remarkable happened at the conference, because within three days, Andersen was singing a different tune. In a Feb. 4, 2020, email, he derided ideas about a lab leak as ‘crackpot theories’ that ‘relate to this virus being somehow engineered with intent and that is demonstrably not the case’.”[8]
Andersen and his colleagues then published an article on 17 March 2020 in the journal Nature Medicine that declared, “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.”[9] The article was highly influential in persuading the mainstream press not to investigate lab leak theories.[10]
While the emails do not prove a conspiracy to mislead the public, they certainly make it more plausible. Just one day after the teleconference at which his experts explained why they thought the virus seemed manipulated, Francis Collins, then-director of the NIH, complained about the damage such an idea might cause.
“The voices of conspiracy will quickly dominate, doing great potential harm to science and international harmony,” he wrote on 2 February 2020, according to the emails.[11]
But there is another reason why Fauci and Collins might not want the lab leak idea to take hold. Dr Daszak’s EcoHealth Alliance had channelled funding from the NIH’s NIAID to the Wuhan Institute of Virology (WIV) in China, for dangerous gain-of-function (GoF) research on bat coronaviruses. So money from organisations headed by Fauci, Collins, and Daszak funded research that could have led to the lab leak that some believe caused the pandemic.[12]
While it should have been clear from the beginning that Drs Fauci and Daszak have strong vested interests in denying the lab leak theory, until recently their assertions were taken as objective fact by most science writers and media.
But a brief look at the history of lab leaks and the origins of pandemics confirms that their claims are highly misleading. Research shows that the escape of viruses from laboratories and supposedly contained experiments, such as vaccine research and programmes, is a common occurrence. In addition, many pandemics have arisen from lab escapes and almost all have not been directly zoonotic. Even when viruses do ultimately originate in animals and make the jump into humans, they mostly fester in a separated community of human beings for many years – centuries or millennia – before spreading during abnormal movements of people due to wars and famines.
What is GoF research?
In its broadest definition, GoF research provides a virus or other microbe with a new function, such as making it more virulent or transmissible, or widening its host range (the types of hosts that the organism can infect).[13] Through GoF, researchers can create new diseases in the laboratory.
GoF can be achieved by any selection process that results in changes in the genes of the organism and as a result, its characteristics. One example of such a process is passing a virus through different animal cells, which can result in a loss of function (weakening it) or a gain of function (making it more able to replicate in a new host species). The researcher can then select the altered organism, depending on the purpose of the research.
In the last decade, GoF researchers have used genetic engineering to directly intervene in the genome of viruses to enhance a desired function.
But long before GoF studies involving deliberate genetic alteration, researchers had started to experiment with widening the host range of certain viruses, in order to develop vaccines. Often these experiments had unintended outcomes, including causing outbreaks of the disease being targeted.
Smallpox
An example is the development of the smallpox vaccine. Most of us are aware of how Edward Jenner in 1796 put cowpox to work in a new way, to infect humans. This led to the successful vaccination programme that eventually eliminated smallpox from the world.
But what many people do not know is that the experiments of 1796 were not his first attempts at using an animal pox in humans. His first subject was his baby son, who had been born in 1789. He inoculated the lad with swinepox and later tested the inoculation’s effectiveness with smallpox. As Greer Williams pointed out in the book Virus Hunters, “The best we can say for this experiment is that it muddied the water… whether the experimental infections had anything to do with [the son’s] mental retardation it is impossible to say.”[14]
Vaccination does not give immunity from smallpox for life: A booster is required every few years. The last person to die from smallpox was Janet Parker, a photographer who worked on the floor above a lab in Birmingham, UK, where research on the virus was being conducted. She had been vaccinated against smallpox in 1966 but contracted the disease in 1978 when the virus escaped from the lab by an unknown route. She died some days later (see Table 1).
Introducing a virus or other microbe to a new host has historically been associated with problems. Before Jenner, inoculation with variola minor (smallpox from a sufferer with minor disease), had been used as a preventive measure in China as early as the tenth century.[15] Variolation, as it was termed, was introduced to the UK in 1717, but is reported to have killed 1 in 25. So Jenner’s experiments have to be viewed in the light of the contemporary practice, which was killing 4% of those inoculated.
What is more, as Greer Williams noted, variolation was an “excellent way of spreading the disease and starting new epidemics”.[16]
Yellow fever
In 1900 the French had given up on building the Panama Canal due to yellow fever decimating the workers. Eventually the disease was conquered in the region by a mosquito eradication programme based on the experiments of the US Army surgeon Major Walter Reed.[17] This success was crucial to the completion of the project in 1914.
But what is often forgotten is that a series of doctors and laboratory workers died trying to combat yellow fever. In 1900 Dr Jesse W. Lazear was the first researcher to die from yellow fever after he apparently allowed himself to be bitten by an infected mosquito as part of his experiments.[18] Between 1927 and 1930, yellow fever caused 32 laboratory infections, killing five people.[19]
As the research into viruses continued, so did the infection rate amongst the researchers and the death toll of researchers and those inoculated against diseases rose. I do not doubt that the final outcome was to the good of mankind, but occasionally a “vaccine” would go spectacularly wrong.
Polio
In the 1930s, 40s and 50s the infection that seemed to most frighten Western society was poliomyelitis. Perhaps it was because unlike with most infectious diseases, cleanliness did not seem to be a protection and exercising could be positively harmful. In fact polio struck those who were healthy and wealthy and was worse if the person was fit and active. Much effort was put into finding a vaccine and among the first to succeed was Dr Jonas Salk. There had been abortive attempts in the 1930s but the 1935 vaccination programme had actually killed people.
Salk was a meticulous researcher and his technique was excellent. Unfortunately this was not the case with all of the laboratories that prepared the vaccine for public use. In particular, the Cutter Laboratories failed to kill the virus and poliomyelitis was spread by their version of the Salk vaccine, paralysing and killing the recipients. Eventually the proper controls permitted the successful rollout of the killed vaccine. It was later replaced by an attenuated polio virus vaccine, which has nearly eliminated polio from the world. It will not, however, succeed in completely eliminating the disease, as the attenuated virus can revert to a wild form. Thus the final push may require the use, once again, of the killed virus polio vaccine.
The infection of laboratory workers with the microbes they were working on was so common that steps were introduced in the 1940s to prevent escape of the organisms. According to Wikipedia, the first prototype Class III (maximum containment) biosafety cabinet was fashioned in 1943 by Hubert Kaempf Jr., then a US Army soldier.[20] The regulations were enhanced and the escape of dangerous organisms decreased, but has never disappeared. This is clearly demonstrated in Table 1, which lists some, but by no means all, of the known lab leaks since the 1960s.
Escapes from bioweapons facilities
Whilst all of the incidents in the table are of interest, some are more worrying than others. In 1971 and 1979 there were outbreaks of smallpox and anthrax in the Soviet Union, caused by escapes of weaponised smallpox and weaponised anthrax from their own bioweapons facilities. In 1977 it is believed that a laboratory somewhere on the border of China and Russia put the H1N1 virus back together and it escaped and caused at least two pandemics. SARS1, which erupted first in 2003, later escaped from laboratories six times, four of which were in China, plus Singapore and Taiwan.[21]
The more you look at the table, the more you wonder if there is any virus that has not at some time escaped from a laboratory. Laboratory workers have told me that it is common for technicians to become infected with the organisms they are working with and their usual response in the past has been to take multivitamins and hydroxychloroquine.

Table 1: Some serious leaks of viruses from laboratories[22]k
The recent history of gain-of-function studies
Since 2010, GoF studies have increasingly focused on finding out whether non-pathogenic strains of viruses could be made infective and harmful to human beings.[23] This was supposedly in order to know whether or not the microbe was likely to be hazardous to human beings and then, if it was, devise vaccines and drugs against it.
In my opinion, such work simply increases the sum total of different pathogens that can affect human beings. When medical doctors are made aware of this type of research, they are usually speechless at the stupidity that anybody would contemplate doing such work. I now call such studies Make Another Disease (MAD) research.
This type of MAD research dramatically increased in laboratories in the USA between 2012 and 2014. The resulting accidents in which small outbreaks of novel viral diseases occurred led to three hundred scientists writing to the Obama administration asking for GoF to be stopped. The US Government responded by announcing a pause on the research in 2014 because of the inherent dangers.[24]
In the same year Dr Fauci, whose recorded belief was that the studies were worth the risk,[25] gave money from the NIH to Dr Daszak of Ecohealth Alliance to continue GoF research on coronaviruses.[26] This was carried out at the Wuhan Institute of Virology using genetically engineered humanized mice, culminating in reports in 2017 and 2018 that the researchers had successfully made harmless coronaviruses pathogenic to humans.[27]
In the autumn of 2019 the Covid-19 pandemic of SARS-2 started in Wuhan and, to date, over five million people across the world have died from the virus.
Are pandemics ever zoonotic?
In addition to stating erroneously that viruses only rarely escape from laboratories and/or that SARS-Cov-2 was unlikely to have done so, Drs Daszak and Fauci hold that most pandemics are zoonotic in origin. They say that pandemics start from a disease spreading from an animal but they do not state the time period involved. I would suggest that pandemics never occur from the immediate spread from an animal. In order for a pandemic to occur, a reservoir of the infection, adapted to human beings, must develop. This usually takes many years. Moreover the spread usually occurs due to the unnaturally large movement of people that occurs due to wars and famines.
I will give just a couple of well known examples.
When the Europeans invaded the Americas, 90% or more of the indigenous people of America died from the introduced diseases, which included measles, smallpox and mumps. In return, syphilis spread to Europe. Yes, the diseases had all arisen from animals initially, but the adaptation to make them pathogenic enough to cause a pandemic must have occurred over a period of the several thousand years during which the populations of Europe and America were separated.
AIDS was discovered in the early 1980s and it was soon clear that the Human Immunodeficiency Virus had arisen from the Simian Immunodeficiency Virus. However, studies have concluded that the first transmission of SIV to HIV in humans took place around 1920 in Kinshasa in the Democratic Republic of Congo (DR Congo),[28] so that it had at least 40–50 years of sporadic infection of human beings before it started to spread round the world as a pandemic. During that time there were many local wars in Africa and, of course, the 2nd World War.
In my book PANDEMIC, I document the world’s worst pandemics and conclude that it is only malaria that seems to be indifferent to wars, killing people whether or not there are hostilities. All other historical pandemics have at least some connection with war and occur when isolated groups with an endemic disease meet another group without the disease.
Conclusion
Thus historically we come to an impasse with SARS-CoV-2. This arose in a city many miles away from an animal population that might have harboured a similar virus, at a time when the supposed original host was dormant (late autumn), near a laboratory known to be working on the viruses. It then spread from person to person at an alarming rate and was seen to be totally adapted to human beings, to the extent that it was unable to even infect the bat it was supposed to have arisen from.
As a person who has studied the history of pandemics and lab leaks, imagine my surprise when authorities, not only in China but also in the USA and UK, stated categorically that the virus was obviously zoonotic and we were conspiracy theorists if we proposed the opposite. I had to conclude that they were misguided or purposely lying.
References
1. Matthews J (2021). WHO investigation descends into farce in rush to rule out a lab leak. GMWatch. 10 Feb. https://www.gmwatch.org/en/news/archive/2021-articles2/19691
2. Morse SS et al (2012). Prediction and prevention of the next pandemic zoonosis. The Lancet 1-7 Dec; 380(9857):1956–1965. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3712877/
3. Matthews J (2020). Why are the lab escape denialists telling such brazen lies? GMWatch. 17 Jun. https://gmwatch.org/en/news/archive/2020-articles/19437
4. Morens DM, Fauci AS (2020). Emerging pandemic diseases: How we got to COVID-19. Cell 182. 3 Dec. https://www.cell.com/cell/pdf/S0092-8674(20)31012-6.pdf
5. Chaffetz J (2022). Fauci, Feds tried to quash COVID lab leak origin theory – protecting Chinese interests over American lives. Fox News. 27 Jan. https://www.foxnews.com/opinion/fauci-covid-lab-leak-origin-theory-china-jason-chaffetz
6. Wade N (2022). Emails reveal scientists suspected COVID leaked from Wuhan lab – then quickly censored themselves. New York Post. 17 Feb. https://nypost.com/2022/01/24/emails-reveal-suspected-covid-leaked-from-a-wuhan-lab-then-censored-themselves/
7. Carlson J, Mahncke H (2021). Behind the scenes of the natural origin narrative. Epoch Times. 30 Sep. https://www.theepochtimes.com/behind-the-scenes-of-the-natural-origin-narrative_4023181.html
8. Wade N (2022). As above.
9. Andersen KG et al (2020). The proximal origin of SARS-CoV-2. Nature Medicine 26:450–452. 17 Mar. https://www.nature.com/articles/s41591-020-0820-9
10. Wade N (2022). As above.
11. Wade N (2022). As above.
12. Lerner S, Hvistendahl M, Hibbett M (2021). NIH documents provide new evidence US funded gain-of-function research in Wuhan. The Intercept. 10 Sep. https://theintercept.com/2021/09/09/covid-origins-gain-of-function-research/
13. Board on Life Sciences et al (2015). Gain-of-function research: Background and alternatives. In: Potential Risks and Benefits of Gain-of-Function Research: Summary of a Workshop. National Academies Press (US). Apr 13. https://www.ncbi.nlm.nih.gov/books/NBK285579/
14. Williams G (1959). Virus Hunters. Knopf.
15. Goddard PR (2020). PANDEMIC: Plagues, Pestilence and War: A Personalised History. Clinical Press. https://www.amazon.co.uk/PANDEMIC-Paul-Goddard-MD-FRCR/dp/1854570994
16. Williams G (1959). Virus Hunters. As above.
17. Feng P (undated). Yellow fever. National Museum of the United States Army. https://armyhistory.org/major-walter-reed-and-the-eradication-of-yellow-fever/
18. College of Physicians of Philadelphia (undated). Jesse Lazear. https://www.historyofvaccines.org/content/jesse-lazear
19. Berry GP and Kitchen SF (1931). Yellow fever accidentally contracted in the laboratory: A study of seven cases. The American Journal of Tropical Medicine and Hygiene s1–11(6):365–434. https://www.ajtmh.org/view/journals/tpmd/s1-11/6/article-p365.xml
20. Wikipedia (undated). Biosafety level. https://en.wikipedia.org/wiki/Biosafety_level#:~:text=The%20first%20prototype%20Class%20III,Laboratories%2C%20Camp%20Detrick%2C%20Maryland.
21. Mihm S (2021). The history of lab leaks has lots of entries. Bloomberg. 27 May. https://www.bloomberg.com/opinion/articles/2021-05-27/covid-19-and-lab-leak-history-smallpox-h1n1-sars
22. Sources:
* 1967 https://www.who.int/news-room/fact-sheets/detail/marburg-virus-disease
* 1966 and 1978 https://en.wikipedia.org/wiki/1978_smallpox_outbreak_in_the_United_Kingdom
* 1971 Aral smallpox incident: https://en.wikipedia.org/wiki/1971_Aral_smallpox_incident; 1973 https://api.parliament.uk/historic-hansard/written-answers/1973/apr/12/smallpox
* 1977, 1979 The history of lab leaks has lots of entries: https://www.bloomberg.com/opinion/articles/2021-05-27/covid-19-and-lab-leak-history-smallpox-h1n1-sars
* 2003-2017 Breaches of safety regulations are probable cause of recent SARS outbreak, WHO says BMJ. 2004 May 22; 328(7450): 1222 and The Origin of the Virus (Clinical Press, Bristol) 2021;
* 2007 https://en.wikipedia.org/wiki/2007_United_Kingdom_foot-and-mouth_outbreak
* 2015 US military accidentally ships live anthrax to labs. https://doi.org/10.1038/nature.2015.17653
23. Herfst S et al (2012). Airborne transmission of influenza A/H5N1 virus between ferrets. Science 336(6088):1534-41. https://pubmed.ncbi.nlm.nih.gov/22723413/
24. The White House (2014). Doing diligence to assess the risks and benefits of life sciences gain-of-function research. 17 Oct. https://obamawhitehouse.archives.gov/blog/2014/10/17/doing-diligence-assess-risks-and-benefits-life-sciences-gain-function-research
25. Fonrouge G (2021). Fauci once argued for risky viral experiments – even if they can lead to pandemic. New York Post. 28 May. https://nypost.com/2021/05/28/fauci-once-argued-viral-experiments-worth-the-risk-of-pandemic/ ; Barnard P, Quay S, Dalgleish A (2021). The Origin of the Virus. Clinical Press.
26. NIH (2014). Understanding the Risk of Bat Coronavirus Emergence. Project Number 1R01AI110964-01. https://reporter.nih.gov/search/-bvPCvB7zkyvb1AjAgW5Yg/project-details/8674931
27. Barnard P, Quay S, Dalgleish A (2021). The Origin of the Virus. Clinical Press.
28. Avert (2019). Origin of HIV and AIDS. https://www.avert.org/professionals/history-hiv-aids/origin
About the author: Professor Paul R Goddard BSc, MBBS, MD, DMRD, FRCR, FBIR, FHEA is Emeritus Professor, University of the West of England, Bristol; retired consultant radiologist; and former president of the Radiology Section of the Royal Society of Medicine. He is the author of PANDEMIC, A Personalised History of Plagues, Pestilence and War, Clinical Press Ltd, August 2020, and PANDEMIC, 2nd Edition 2021, Clinical Press, Bristol, available from Gazelle Book Services Ltd and good bookshops, ISBN 978-1-85-457105-2. On a similar theme, see The Origin of the Virus, Clinical Press 2021.
The above article is adapted from material that was first presented as the Long Fox lecture to The Bristol Medico-Chirurgical Society and Bristol University (2017) and to the British Society for the History of Medicine Biennial Congress (September 2021).
JCVI – don’t bite the hand…
Health Advisory & Recovery Team | February 25, 2022
There’s a well known expression “Don’t bite the hand that feeds you.” It can be taken literally – if an animal bites the hand that feeds it, it won’t get fed. In the business or academic world, it means don’t upset your funder. It’s obvious really – if you do, they won’t fund you anymore. The bigger the amount received, the less of a good idea it is to upset the funder.
The Joint Committee on Vaccination and Immunisation (JCVI) “advises UK health departments on immunisation.”[i] The JCVI has a sub-committee specifically to advise on COVID-19 vaccines. The chair of the JCVI, Professor Andrew Pollard, recused himself from all JCVI COVID-19 meetings because he is involved in the development of a SARS-CoV-2 vaccine at Oxford University – where he works. This was done to avoid any “perceived conflict of interest.”
Professor Lim Wei Shen was appointed chair of the JCVI sub-committee on COVID-19 vaccines. In August 2021, he stated categorically that 12-15 year olds would not be offered COVID-19 vaccines.[ii] Barely 6 weeks after that statement, 12-15 year olds were offered jabs.[iii] Barely 6 months later, on February 16th, 2022, the sub-committee issued a statement saying that, although 5-11 year olds are “generally at very low risk of serious illness from the virus”, they would be offered 2 doses of the Pfizer mRNA jab.[iv] This recommendation occurred despite the trials in children not being due for completion until May 2026.[v] We have previously noted that Professor Lim has a substantial conflict of interest: he has direct responsibility for material levels of funding received by his department from Pfizer.
At the time of writing, the most recent minutes for the sub-committee meetings are from May 2021. The sub-committee and main JCVI minutes report “Declarations of Interest” for the committee members. The Code of Practice describes the JCVI as “an independent Departmental Expert Committee and a statutory body.”[vi] Independent being the word of interest. One would expect this to mean “free from conflicts of interest”, but a closer look revealed that this was not the case.
The COVID-19 sub-committee of the JCVI has 15 core members (1 lay member). None of the members of this sub-committee declared conflicts of interests. Five of the 14 non-lay members provided additional information in their ‘non-declaration’ that revealed conflicts of interest. One, for example, declared funding from “the National Institute for Health Research, the Medical Research Council, the Wellcome Trust and Gavi, The Vaccine Alliance, and the Bill & Melinda Gates Foundation”, but didn’t consider any of that vaccine funding as a conflict of interest. A cursory search on the remaining nine members revealed that six had conflicts of interest – from running a COVID-19 vaccine trial to being their organisation’s representative for Pfizer. One member failed to declare that he leads the Pfizer Vaccine Centre of Excellence in Bristol.
The members work for organisations, which collectively have received approximately $1,000,000,000 – one billion dollars – from the Bill and Melinda Gates Foundation. The Gates Foundation aims to “accelerate the development and commercialization of novel vaccines and the sustainable manufacture of existing vaccines.”[vii] No doubt the Gates Foundation would have welcomed the sub-committee’s decision.
The majority of the COVID-19 JCVI sub-committee members have conflicts of interest. These members don’t seem to realise that their research or institution receiving huge sums of money from pharmaceutical companies and/or the Gates Foundation is a conflict of interest.
Has this committee truly been able to provide an independent assessment of the risk and reward of the main products of interest of the Gates Foundation? Or has it made a decision to not bite the hand that feeds it?
Read full article here:
The people who know this stuff the best (the industrial hygienists) weigh in on the flawed CDC mask guidance
By Steve Kirsch | February 22, 2022
Eight industrial hygienists, including my friends Stephen Petty and Tyson Gabriel, wrote a 27-page letter to the CDC, NIH, and other top US government officials that points out serious flaws in the CDC mask guidance.
The key points in their letter
The letter starts out with:
They made four key points :
They also sent email to scientificIntegrity@cdc.gov
They also emailed scientificIntegrity@cdc.gov the following:
We have conducted a peer review of the CDC’s “Types of Masks and Respirators” that was updated on January 28, 2022. Our findings have shown that this publication does not meet the scientific integrity that we have come to expect from HHS and all affiliated agencies. Please review the findings in our report. We strongly encourage your team to remove this publication from use and publish an acknowledgement of the concerns. We are willing to discuss our findings further at your request. We appreciate your time and look forward to a response.
However, I’m pretty sure that there isn’t any scientific integrity left at the CDC and there will be nobody there to answer their complaint.
Their conclusion
The CDC is doing enormous damage to science and scientists by allowing politics to dictate public health policy rather than actual science. Increasingly, and for good reason as we have illustrated, the public does not trust the CDC and its science; this must change.
Their offer to help
We recognize that it is easy to judge from afar and know that you and your team are under tremendous stress during this period. Our desire is to see the CDC and our country succeed in these efforts. As such, instead of just being critical, we want to offer our time to your organization to find solutions together. We would be willing to collaborate in the creation of a competent plan that will be based on the Hierarchy of Controls and will be tailored to various work and living environments. We will also help develop data points we can use to monitor and measure this program to enable proper adjustments as needed.
Summary
The industrial hygienists are right. The CDC is wrong.
I predict that the CDC isn’t going to admit they are wrong. When was the last time you saw that happen?
And they aren’t going to accept help from the experts who know this stuff because it would be a tacit admission that they’ve been giving out crappy advice through the entire pandemic that has made the problem worse.
By David Charbonneau, Ph.D. | The Defender | February 23, 2022
Before the U.S. Supreme Court last month blocked the Biden administration’s COVID-19 vaccine mandates for large employers and allowed the mandate for healthcare workers to stand, all eyes were on the feds when it came to COVID-related policies.
But state lawmakers also have been busy drafting bills in an effort to shape COVID policies closer to home.
The California Assembly, for example, introduced over the past six months a flurry of bills designed to strengthen vaccination mandates and regulate treatment options for patients.
For example, Sen. Richard Pan (D-Sacramento) last month introduced legislation proposing COVID vaccine mandates for all K-12 students in California schools.
And this month, Assembly Member Evan Low (D-Campbell) introduced legislation (AB 2098) that, according to the Los Angeles Times, would “make it easier for the Medical Board of California to discipline doctors who promote COVID-19 misinformation by classifying it as unprofessional conduct.”
The bill defines “unprofessional conduct” as any action a physician or surgeon takes “to disseminate or promote misinformation or disinformation related to COVID-19, including false or misleading information regarding the nature and risks of the virus, its prevention and treatment; and the development, safety, and effectiveness of COVID-19 vaccines.”
Under the bill, disciplinary action could be brought against a physician for disseminating information that “resulted in an individual declining opportunities for COVID-19 treatment or prevention that was not justified by the individual’s medical history or condition.”
Additionally, doctors could be disciplined for “misinformation or disinformation” that is contradicted by contemporary scientific consensus to an extent where its dissemination constitutes gross negligence” by the physician.
Commenting on the criteria, Dr. Meryl Nass, an expert in epidemiology and vaccine injury and member of the Children’s Health Defense scientific advisory committee, said:
“I think this is clearly an attempt to legislate that the government of California or the Medical Board of California will define what is truth and what is misinformation, and medical providers will have to follow lockstep with that definition.
“This, of course, is the same thing as the Ministry of Truth in George Orwell’s “1984,” and if the California legislature actually votes for this bill, the intent of the action will be to enforce a one and only truth.
“Nowhere does this legislature define what is misinformation and disinformation. They do talk about contemporary scientific consensus but as we know in the last two years, the so-called scientific consensus — or the public health agency consensus — on masks, on vaccination, on boosters, etc. has flip-flopped all over the place. So we have adequate examples that the concept of “contemporary scientific consensus” is basically meaningless in this context.”
Contrary to typical board practice, under AB 2098, physicians could also be disciplined for public speech, including social media posts, unrelated to the actual treatment of patients.
Supporters of Low’s bill insist the legislation does not impinge on doctors’ freedom of speech.
“This isn’t a call for a policing of free speech,” Nick Sawyer, an emergency room doctor who founded a group called No License for Disinformation, told the LA Times. “This is a call for protecting the public against dangerous misinformation, which patients are parroting back to us in our emergency room departments every day.”
Nass disagreed:
“The result is removing options from doctors and patients. And the longer-term consequence is that doctors will become irrelevant if they are not needed to assess each individual’s personal risks and benefits from each type of medical care.
“The government and its partners in the healthcare industries can simply prescribe one-size-fits-all healthcare for everyone.”
Low’s bill, introduced as part of a larger effort by a group of Democratic state legislators to strengthen vaccination laws, set off a contentious debate over how far the state should go in pursuing COVID mandates.
Other COVID-related bills introduced in California include:
Other states pursue efforts to support alternative treatments
In contrast to California, several state legislatures are moving to provide legal support for off-label prescriptions and alternative approaches supported by physicians.
In New Hampshire, legislators last month held public hearings on a bill that would allow for over-the-counter dissemination of ivermectin at pharmacies, provided certain treatment plan requirements were met.
New Hampshire HB 1022 would permit pharmacists to dispense the ivermectin by means of a standing order entered into by licensed healthcare professionals.
Sponsors of the bill argued many healthcare workers are unable to prescribe ivermectin, either because of hospital politics or outside professional pressures.
The bill has support from Dr. Paul Marik, who traveled from Virginia to testify at the public hearing.
A former professor of medicine and chief of pulmonary and critical care medicine at Eastern Virginia Medical School, Marik sued the hospital he worked for after it banned physicians from prescribing ivermectin for COVID patients.
Marik resigned late last year in protest of the ban.
During his testimony in New Hampshire, Marik described ivermectin as “cheap, exceedingly safe and exceedingly effective.”
“If ivermectin had been promoted at the beginning of this pandemic, we would not be sitting here today,” Marik said.
Kansas lawmakers last month advanced a bill supporting the prescribing of ivermectin and hydroxychloroquine. The model legislation, also introduced in Tennessee, would require pharmacists to fill prescriptions for the off-label use of ivermectin and hydroxychloroquine.
In direct contrast to the California legislation, the Kansas bill also would mandate that doctors not be subject to disciplinary action for any “recommendation, prescription, use or opinion … related to a treatment for COVID-19, including a treatment that is not recommended or regulated by the licensing board,” Kansas Department of Health and Environment or the U.S. Food and Drug Administration.
“Such actions,” the bill states, “could not be considered unprofessional conduct.”
Kansas lawmaker Sen. Mark Steffen (R-Hutchinson) supports the bill. Steffen, an anesthesiologist, said he’s under investigation by the University of Kansas Health System with which he is affiliated for prescribing ivermectin to COVID patients.
Dr. Festus Krebs III, a physician representing the Catholic Medical Association of Kansas City, also spoke in favor of the bill:
“With ivermectin and hydroxychloroquine, we now have 76 ivermectin COVID-19 controlled studies which show 66 percent overall improvement and 57 percent decreased mortality.”
Meanwhile, in Florida, legislation that would extend protection for hospitals against patient lawsuits over COVID care sits on the desk of Gov. Ron DeSantis, awaiting signature or a veto.
And in New York, the state’s comptroller — citing the investment of the state’s public pension plan in Spotify — sent a letter to the company asking it to increase its screening of “misinformation” on their platform.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
eugyppius | February 24, 2022
Because available statistics have been so terrible, I’ve not written very much about vaccine injuries, but evidence is mounting, from sources beyond the American VAERS database, that they are vastly more frequent and severe than anybody will acknowledge.
Many of my readers have not been vaccinated, but many others have been. I’d like to compile a post or two of reader experience with the vaccines. If you have something to report, please write to me at containment@tutanota.com. I’m not only interested in severe side effects; reports of mild reactions will help to build a full picture. I’m also interested in infection following vaccination, and any other related matters you deem of interest. It’s most helpful if you can report about your own direct experiences, that is to say, things that happened to you or to people you know personally.
Otherwise, to complete yesterday evening’s hasty update, I provide a translation of Andreas Schöfbeck’s letter to the Paul Ehrlich Institute, on the underreporting of vaccine side effects in Germany. Apparently the PEI has responded, but exactly what they’ve said has yet to be released, as far as I know.
Dear Prof. Dr. Cichutek,
the Paul Ehrlich Institute has issued a press release announcing 244,576 suspected cases of adverse reactions to the Corona vaccines for the calendar year 2021.
Our company has data that give us reason to believe that there is a very pronounced under-reporting of suspected adverse reactions following Corona vaccination. I attach an analysis to this letter.
Physicians’ billing data provide the basis for this analysis. We have sampled data from the anonymised records of company health insurers, totalling 10,937,716 insured persons. So far, we have billing data for the first half of 2021, and about half of the billing data for the third quarter of 2021. We queried this data for the ICD codes valid for vaccination side effects. Although we do not yet have the complete data for 2021, our analysis of the available data reveals 216,695 treated cases of vaccination side effects following Corona vaccination. If these figures are extrapolated to the whole year and to the total German population, perahps 2.5 to 3 million people have received medical treatment for side effects following Corona vaccination.
For us, this is a serious wake-up call, that must be considered for the further administration of vaccines. We think it would be relatively easy and quick to confirm these figures, by asking the other health insurers (AOKs [general regional insurers], the alternative insurers, etc.) for a corresponding anylsis of their data. Extrapolated to the number of vaccinations across Germany, this would mean that about 4-5% of the vaccinated have been treated by a doctor because of side effects from the vaccines.
We believe that vaccine side effects are being substantially under-reported. It is crucial to identify the reasons for this as soon as possible. Since there is no remuneration for reporting adverse reactions to the vaccine, our primary assumption is that doctors often neglect to report adverse reactions to the Paul Ehrlich Institute, because of the effort involved. Doctors tell us that reporting a suspected vaccine injury takes about half an hour, which means that 3 million suspected cases of adverse reactions would require doctors to work 1.5 million hours. That would correspond to the annual labour of around 1,000 doctors. This should also be quickly confirmed. A copy of this letter will also be sent to the German Medical Association and the Federal Association of Statutory Health Insurance Physicians.
The Central Association of Health Insurers will also receive a copy of this letter with a request to obtain corresponding data analyses from all health insurers.
Since we cannot rule out the danger to human life, we ask you for your report on your response by 6pm on 22 February 2022.
Regards,
Andreas Schöfbeck

or go to
Aletho News Archives – Video-Images
By Lisa Pease | Consortium News | September 16, 2013
More than a half century ago, just after midnight on Sept. 18, 1961, the plane carrying UN Secretary-General Dag Hammarskjöld and 15 others went down in a plane crash over Northern Rhodesia (now Zambia). All 16 died, but the facts of the crash were provocatively mysterious. … continue
